employment characteristics and salaries of psychologists in united states medical schools: past and...
TRANSCRIPT

Journal of Clinical Psychology in Medical Settings, Vol. 6, No. 2, 1999
Employment Characteristics and Salaries ofPsychologists in United States Medical Schools:Past and Current Trends
Steven Williams1,3 and Danny Wedding2
In 1997 the Research Office of the American Psychological Association(APA) collaborated with the Association of Medical School Psychologists(AMSP) to conduct a comprehensive employment and salary survey ofpsychologists employed in medical schools and academic health centers.Questionnaires were mailed to 3894 psychologists; postcard reminders anda follow-up mailing to nonresponders resulted in a final 50% response rate.The questionnaire addressed appointment characteristics, department andschool characteristics, employment activities, salary information, demograph-ics, and changes in the medical school work environment that have occurredas a result of managed care. This survey, the 1997 Employment Characteris-tics and Salaries of Medical School Psychologists, is the most comprehensiveanalysis to date of the practice of psychology in U.S. schools of medicineand academic health centers. This article reports the most salient findingsfrom this survey.
KEY WORDS: psychologists; medical schools; employment; salaries.
INTRODUCTION
A 1911 recommendation and a 1912 symposium prompted the exami-nation of professional psychology within medical schools by the AmericanPsychological Association (Nathan, Lubin, Matarazzo, & Persely, 1979).Until the end of World War II, the representation of psychologists within
1American Psychological Association, Research Office, 750 First Street, NE, Washington,DC 20002.
2Missouri Institute of Mental Health, School of Medicine, University of Missouri—Columbia,540 Arsenal Street, St. Louis, Missouri 68139.To whom correspondence should be addressed.
221
1068-9583/99/0600-0221$16.00/0 © 1999 Plenum Publishing Corporation
222 Williams and Wedding
these settings was sparse (Nathan, Lubin, Matarazzo, & Persely, 1979).Nevertheless, beginning in the mid-1940s and throughout the next fourdecades, the number of psychologists in such settings soared. In the early1950s, for example, there was a conservative estimate of 255 psychologistsemployed within medical schools (Mensh, 1953). By the mid-1960s, thisnumber had more than tripled, to 993 (Wagner & Stegeman, 1964), andby 1976 it had risen to 2336 (Lubin, Nathan, & Matarazzo, 1978). Matarazzo(1994) estimated that there were 3500 psychologists on medical schoolfaculties in 1993. Today, more than 3900 psychologists are employed withinmedical schools and academic health centers.
The surge in the number of medical school psychologists in the lastfour decades was accompanied by a rise in the number of medical schoolsthat employ professional psychologists. In 1953, psychlogists were em-ployed in 73% of the medical schools that existed at that time (Mensh,1953). A little more than two decades later, psychologists were representedin 98% of the existing medical schools (Lubin et al, 1978).
It is perhaps no surprise that the demographic composition, departmen-tal settings, activities, roles, status, and salaries of psychologists withinmedical schools have shifted over the past four decades. Several scholarshave monitored these changes by conducting employment surveys or engag-ing in discussion on topics that are relevant to these psychologists (Lubin,Nathan, Gildenberg, & Matarazzo, 1980; Lubin et al, 1978; Matarazzo,1994; Matarazzo & Daniel, 1957a, 1957b; Matarazzo, Lubin, & Nathan,1978; Mensh, 1953; Nathan, Lubin, Matarazzo, & Persely, 1979; Routh, 1972;Rozensky, 1994; Thompson & Matarazzo, 1984; Wagner, 1968; Wagner &Stegeman, 1964; Witkin, Mensh, & Gates, 1972). Many of these studies anddiscussions reflected the employment of medical school psychologists ofthe 1960s and 1970s. Only a few studies have examined employment charac-teristics of psychologists during the 1980s (e.g., Thompson & Matarazzo,1984), and most of these have had a limited focus (e.g., medical staffmembership, voting privileges). Furthermore, there is a paucity of researchthat has examined the salaries of these psychologists. Although severalemployment and salary surveys of psychologists have been conducted re-cently (e.g., Wicherski & Kohout, 1997a; Wicherski, Williams, & Kohout,1998a,b), they have not specifically focused on this group of psychologists.No comprehensive study has examined employment characteristics andsalaries of medical school psychologists in the 1990s.
Relative to other work settings for professional psychology, only asmall number of psychologists are employed within medical schools (Wich-erski & Kohout, 1997b). So that these psychologists are not eclipsed in anenvironment that is inundated by other nonpsychological health profession-als, it is essential that these psychologists be identified and that their currentcircumstances be evaluated; even more attention to this group may be

Employment Characteristics and Salaries 223
warranted given the changes and cutbacks that medical schools may beexperiencing due to the health care reforms of the last decade. Hence,the goal of this study was to provide a comprehensive description of theemployment characteristics and salaries of psychologists within medicalschool settings and to view these results in the context of past employmentand salary trends derived from previous surveys (e.g., Lubin et al., 1978;Matarazzo & Daniel, 1957a; Wagner & Stegeman,1964).
METHOD
Participants
Membership lists of the American Psychological Association (APA),the Association of American Medical Colleges (AAMC), and the Councilof Deans of the American Association of Colleges of Osteopathic Medicine(AACOM) were used to identify psychologists who were employed withinmedical school settings. After eliminating duplicate names, a final list of3894 psychologists was obtained. The sample used in this study was definedas all doctoral-level psychologists working in U.S. medical schools. Thissample included psychologists with various subfield specialties (e.g., clinicalpsychology, neuropsychology), licensure status, and degree types (e.g.,Ph.D., Psy.D., M.D./Ph.D.). Participants were employed full-time and part-time, but only those participants who were employed full-time (albeit notnecessarily full-time in a school of medicine) were selected for this study.Finally, participants came from various geographic regions of the UnitedStates.
Measures
The 1997 Medical School Psychologists Employment Survey4 comprisedmostly closed-ended items/questions. The survey was used to obtain infor-mation about the demographic characteristics, employment arrangement(e.g., full-time versus part-time, 9-10 versus 11-12 months), rank, tenurestatus, departmental characteristics, employment activities, and salaries ofmedical school psychologists. Most of the survey items and questions werefashioned after previous surveys (e.g., Arnett & Martin, 1981; Johnson &Williams, 1979; Lubin et al., 1978; Matarazzo & Daiel, 1957a; Wagner &
4Copies of the survey and the final report, 1997 Employment Characteristics and Salaries ofMedical School Psychologists, are available from the American Psychological Association,Research Office, 750 First Street, NE, Washington, DC 20002.

Stegeman, 1964) to facilitate comparison between the current findings andthose of earlier surveys.
Procedure
In March 1997 the survey and a cover letter explaining the purposeof the study were mailed to the sampled psychologists who met selectioncriteria. Each was provided a postage-paid envelope to return his or hersurvey. Anonymity was not preserved so that nonrespondents could betracked. Nonrespondents were mailed postcard reminders 1 month follow-ing the initial contact. A final attempt to contact nonrespondents was made1 month after the postcard reminders and a second survey and reminderletter was mailed to all nonrespondents.
RESULTS
Response Rate and Demographic Characteristics
A 50% response rate (N = 1938) was obtained. Fifty-six percent ofthe responding psychologists were men, compared to 44% who were women.The majority of the respondents were white (92%). Each of the other racial/ethnic groups represented less than 2% of the respondents. These data arecomparable with those of Black and Holden (1998), who surveyed a smallersample of medical school psychologists in which 56% of the sample weremen and 94% were white. As shown in Table I, the highest proportions of
Table I. Geographical Distribution of MedicalSchool Psychologists
Geographic region
New EnglandMid AtlanticEast North CentralWest North CentralSouth AtlanticEast South CentralWest South CentralMountainPacificUnspecified
%
11.322.012.04.9
20.14.67.62.59.95.2
N
21942623295
39089
14748
191101
Note. States that comprise geographic regionsare based on the categorization used by theU.S. Department of Commerce’s Bureau of theCensus. Colupercentages ay not sum to100 due to rounding.
224 Williams and Wedding

medical school psychologists were employed in institutions located in theMiddle Atlantic (22%) and South Atlantic regions (20%). The smallestsingle proportion of psychologists (3%) was employed in the Mountainstates.5
Previous researchers have noted the changes in the demographic pat-tern of medical school psychologists that have occurred over the last severalyears. The presence of female psychologists within medical schools hasincreased dramatically, from 15% in the 1950s and 22-24% in the 1970s toaround 41% in the mid-1990s (Black & Holden, 1998; Holden & Black,1996; Matarazzo, Carmody, & Gentry, 1981; Nathan, Lubin, Matarazzo, &Persely, 1979). In contrast, the racial/ethnic distribution of medical schoolpsychologists has remained relatively stable over the past several years(Black & Holden, 1998; Holden & Black, 1996; Nathan, Lubin, Matara-zzo, & Persely, 1979). The geographic dispersion of these psychologists,however, has shifted somewhat. Using a different geographical classificationsystem, Johnson and Williams (1979) found that the single highest propor-tions of psychologists in the mid-1970s were employed in the Northeastand North Central regions (30% each). This was followed by 15% in theSouthwest region, 11% in the Southeast, 8% in the South Central states,and 6% in the Northwest.
Departmental Distribution of Medical School Psychologists
Departments of psychiatry and behavioral sciences provided academichomes for the majority of psychologists (56%) within medical schools,followed by departments of pediatrics (9%), departments of neurology/biology/physiology/anatomy (8%), and departments of family/health/community/preventive medicine (7%). Only 5% of medical school psycholo-gists were found in departments involving other medical specialties suchas cardiology, oncology, surgery, and obstetrics/gynecology. About 3% ofmedical school psychologists were placed in departments of rehabilitation/pain management, and another 3% were housed in autonomous depart-ments of psychology.
Slightly more than one-third (36%) of these psychologists were em-ployed in a department or college that had a separate administrative unit
5States that comprise geographic regions were based on the categorization used by the U.S.Department of Commerce’s Bureau of the Census. Geographic regions comprise the followingstates: New England (CT, ME, MA, NH, RI, VT); Middle Atlantic (NJ, NY, PA); East NorthCentral (IL, IN, MI, OH, WI); West North Central (IA, KS, MN, M, NE, ND, SD); SouthAtlantic (DE, DC, FL, GA, MD, NC, SC, VA, WV); East South Central (AL, KY, MS,TN); West South Central (AR, LA, OK, TX); Mountain (AZ, CO, ID, MT, NV, NM, UT,WY); and Pacific (AK, CA, HI, OR, WA)
Employment Characteristics and Salaries 225

226 Williams and Wedding
Table II. Departmental Distribution of Psychologists in MedicalSchool Settings
Department
Psychiatry and Behavioral SciencesPediatricsNeurology/Biology/Physiology/AnatomyFamily/Health/Community/PieventionOther medical specialties (e.g., Cardiology)Rehabilitation and Pain ManagementPsychologyOther
%
56.28.77.87.15.13.33.26.6
N
1089169151137996362
127
Note. Departmental affiliation was not indicated by 2% of the respon-dents.
for psychology. Almost half (48%) were employed in a department orcollege where there was a chief psychologist or administrative head ofpsychology. Table II presents the distribution of psychologists across depart-ments.
Departments of psychiatry and behavioral sciences (formerly nameddepartments of neuropsychiatry) have been the primary jurisdiction forpsychologists within medical school settings since the 1950s. In 1953, forexample, 73% of these psychologists were employed in departments ofpsychiatry (Matarazzo & Daniel, 1957a). By the mid-1960s, 68% of medicalschool psychologists could be found within departments of psychiatry(Wagner, 1968; Wagner & Stegeman, 1964). This figure had climbed to80% by the mid-1970s (Nathan, Lubin, Matarazzo, & Persely, 1979) andthen dropped again to 59% in the mid-1990s (Holden & Black, 1996). Seime(1998) recently described an effective model for the organization of medicalschool psychologists within a Department of Behavioral Medicine and Psy-chiatry.
Since the 1960s, psychologists have increasingly found academic homesin other departments within medical schools such as neurology,rehabilitation/pain management, and pediatrics. As is the case today, pedi-atrics emerged as a second popular setting for medical school psychologistsfrom the 1950s to the 1970s. During these years, 6%-7% of psychologistswere placed in these departments (Matarazzo & Daniel, 1957a; Nathan,Lubin, Matarazzo, & Persely, 1979; Wagner, 1968;Wagner & Stegeman,1964).
Employment Arrangement
An 11- to 12-month academic year is the norm for the mjority (85%)of medical school psychologists; in contrast, 1% operated on a 9- to 10-

Employment Characteristics and Salaries 227
month schedule. The remaining proportion of psychologists either had analternative academic year arrangement or did not specify their employmentarrangement. Seventy-four percent were employed full-time by the medicalschool or academic health center, compared to 20% whose academic ap-pointment was part-time. Approximately 6% of medical school psycholo-gists reported no academic appointment or did not specify their appoint-ment status.
Full-time appointments have only recently become the standard. In1951, 44% of the psychologists in this setting were appointed full-time(Mensh, 1953). This percentage rose to 70%-71% by the mid-1960s andmid-1970s (Buck, 1961; Nathan, Lubin, Matarazzo, & Persely, 1979;Wagner, 1968; Wagner & Stegeman, 1964). A concomitant decline in part-time faculty appointments was witnessed with the rise of full-time appoint-ments.
Years in Current Position, Rank, and Tenure Status
The job security of psychologists within medical schools is often corre-lated with the number of years one holds a position, academic rank, andtenure status. The results indicated that psychologists within this settinghave held their current position for a median of 8 years. In terms of rank,Table III reveals that the highest single proportion of these psychologistsheld the rank of assistant professor (34%), followed by associate professorsand full professors at similar levels of representation (26% and 22%, respec-tively). Lecturers and psychologists with“other ranks”each comprised only6% of these psychologists. Seven percent of medical school psychologistsreported that they did not have an acdemic appointment or did not specifytheir academic rank.
Table III. Academic Rank of Medical School Psychologists: 1964, 1976, and 1997
Academic rank
Full professorAssociate professorAssistant professorLecturers/instructorsOther
1955a
% N
4183322
3152718
1964b
% N
5183316
1662
11657
1976c
% N
131939228
10915732618664
1997d
% N
22263466
424500664111106
aFrom Matarazzo and Daniel (1957a).bFrom Wagner (1968) and Wagner and Stegeman (1964).cFrom Lubin et al. (1978).dFrom the current study.eData not available.

228 Williams and Wedding
The largest single proportion of psychologists reported that they werenot on a tenure track (40%), even though the tenure system was used attheir institutions. On the other hand, about 23% reported that they weretenured, and about 15% said that although they were not tenured, theywere currently on a tenure track. Thirteen percent of medical school psy-chologists claimed that the tenure syste was not used within their institu-tions, and the remaining psychologists either did not specify their tenurestatus or claimed some other status. Bodner (1997) has noted that tenuredoes not necessarily protect faculty salaries, especially in a medicalschool environment.
Today, as in the 1970s, the majority of psychologists have held theirpositions for less than a decade. Smaller proportions of psychologists heldtheir positions for more than 10 years—only 5% in 1955 (Matarazzo &Daniel, 1957a) and 23% in 1977 (Nathan, Lubin, Matarazzo, & Persely,1979). As shown in Table III, there have been substantial changes in thedistribution of academic rank over the last three decades. In the mid-1950s, mid-1960s, and mid-1970s, as today, the single highest proportionof psychologists was at the assistant professor level (33%, 33%, and 39%,respectively). This was followed by the associate professor rank, at 18%-19% during that period. However, the proportion of full professors inschools of medicine has more than quadrupled since the mid-1950s, andthe presence of lecturers has declined considerably (Johnson & Williams,1979; Wagner, 1968; Wagner & Stegeman, 1964).
Activities and Roles
The findings illustrate the breadth of activities and roles of psycholo-gists located in medical schools. The greatest median block of time reportedwas devoted to research (30%). One-quarter of the time was spent providingclinical services, 15% was allocated to training, and 10% was devoted toadministrative tasks. Wedding (1997) has discussed the critical role playedby research psychologists in medical school settings.
Most psychologists in medical school settings functioned in trainingcapacities. Seventy percent of these psychologists reported involvement inpredoctoral psychology internship training and about 62% reported thatthey participated in postdoctoral psychology fellowship training. Approxi-mately 6% of medical school psychologists were responsible for teachingnursing students, and about 3% each taught physician’s assistants and den-tists. Medical students and other students (consisting of mostly psychiatricresidents) were the health professional trainees outside of psychology wompsychologists were mostly likely to train. Fifty-four percent and 47% of
Employment Characteristics and Salaries 229
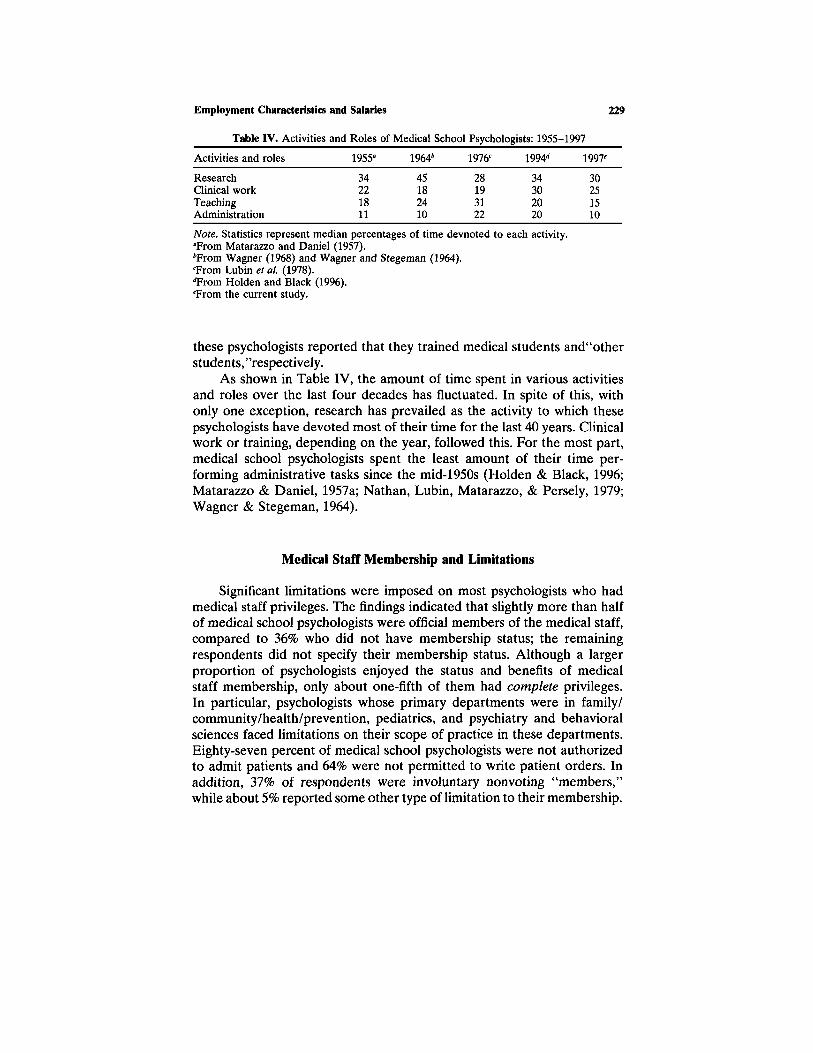
Table IV. Activities and Roles of Medical School Psychologists: 1955-1997
Activities and roles
ResearchClinical workTeachingAdministration
1955a
34221811
1964b
45182410
1976c
28193122
1994d
34302020
1997e
30251510
Note. Statistics represent median percentages of time devnoted to each activity.aFrom Matarazzo and Daniel (1957).bFrom Wagner (1968) and Wagner and Stegeman (1964).cFrom Lubin et al. (1978).dTFrom Holden and Black (1996).eFrom the current study.
these psychologists reported that they trained medical students and“otherstudents, ”respectively.
As shown in Table IV, the amount of time spent in various activitiesand roles over the last four decades has fluctuated. In spite of this, ithonly one exception, research has prevailed as the activity to which thesepsychologists have devoted most of their time for the last 40 years. Clinicalwork or training, depending on the year, followed this. For the most part,medical school psychologists spent the least amount of their time per-forming administrative tasks since the mid-1950s (Holden & Black, 1996;Matarazzo & Daniel, 1957a; Nathan, Lubin, Matarazzo, & Persely, 1979;Wagner & Stegeman, 1964).
Medical Staff Membership and Limitations
Significant limitations were imposed on most psychologists who hadmedical staff privileges. The findings indicated that slightly more than halfof medical school psychologists were official members of the medical staff,compared to 36% who did not have membership status; the remainingrespondents did not specify their membership status. Although a largerproportion of psychologists enjoyed the sttus and benefits of medicalstaff membership, only about one-fifth of them had complete privileges.In particular, psychologists whose primary departments were in family/community/health/prevention, pediatrics, and psychiatry and behavioralsciences faced limitations on their scope of practice in these departments.Eighty-seven percent of medical school psychologists were not authorizedto admit patients and 64% were not permitted to write patient orders. Inaddition, 37% of respondents were involuntary nonvoting “members,”while about 5% reported some other type of limitation to their membership.

230 Williams and Wedding
Although limitations remain, there has been steady progress in medicalstaff membership among psychologists since the 1970s, when only 5% ofthe medical schools that existed at that time had bylaws that permittedpsychologists to be voting members (Lubin et al., 1978; Matarazzo et al.,1978). Ten years later, 13% of the medical schools passed bylaws favoringpsychologists’ participation as voting members (Thompson & Matarazzo,1984).
Salaries
The median base salary for full-time psychologists within medicalschools was $66,100 in 1996. Opportunities for supplementary income wereavailable to 43% of these psychologists who provided clinical services out-side of their academic appointments or engaged in other nonclinical activi-ties. Forty-three percent of the respondents supplemented their salarieswith clinical income and 47% were able to add to their income by servingin non-clinically-based roles such as teaching or consulting. The medianclinical supplementary income of all psychologists within medical schoolswas $13,700, and the median nonclinical, additional income was $4000.After combining all sources of psychology-related income, medical schoolpsychologists reported a total median income of $75,000 in 1996.
Salaries of medical school psychologists varied considerably as a func-tion of academic rank and years since the doctorate. Tables V and VIillustrate the base salaries, clinical income, nonclinical income, and totalincome by academic rank and years since the doctorate, respectively. Asshown in Table V, salary steadily increased with increasing academic rank.Similarly, as would be expected, salaries continued to rise with increasingyears since the doctorate (Table VI).
Medical school psychologists who are male continue to earn consider-ably more than their female colleagues. The median total income in 1996for men in the sample was $83,500; the comparable ttal income for women
Table V. 1996 Base, Clinical, Additional, and Total Income of Medical School Psychologistsby Academic Rank
Rank
All ranksFullAssociateAssistantLecturerOther
Base
66,10098,00070,00055,00048,50051,000
N
1,3713534014994753
Clinical
13,70017,50020,00010,00011,0009,086
N
34562
1061381514
Additional
4,0006,0003,0002,5003,0002,500
N
7452522342201716
Total
75,000108,50077,00060,10051,65060,000
N
13353453914834553
Employment Characteristics and Salaries 231
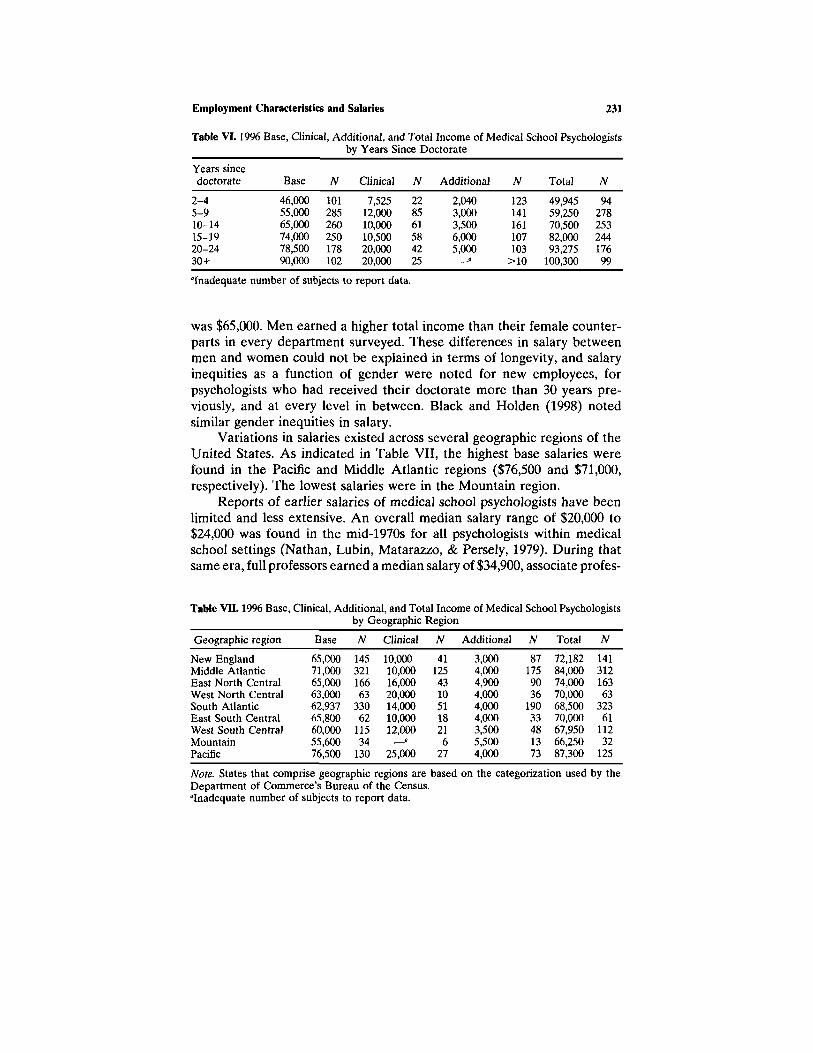
Table VI. 1996 Base, Clinical, Additional, and Total Income of Medical School Psychologistsby Years Since Doctorate
Years sincedoctorate
2-45-910-1415-1920-2430+
Base
46,00055,00065,00074,00078,50090,000
N
101285260250178102
Clinical
7,52512,00010,00010,50020,00020,000
N
228561584225
Additional
2,0403,0003,5006,0005,000
N
123141161107103
>10
Total
49,94559,25070,50082,00093,275
100,300
N
9427825324417699
aInadequate number of subjects to report data.
was $65,000. Men earned a higher total income than their female counter-parts in every department surveyed. These differences in salary betweenmen and women could not be explained in terms of longevity, and salaryinequities as a function of gender were noted for new employees, forpsychologists who had received their doctorate more than 30 years pre-viously, and at every level in between. Black and Holden (1998) notedsimilar gender inequities in salary.
Variations in salaries existed across several geographic regions of theUnited States. As indicated in Table VII, the highest base salaries werefound in the Pacific and Middle Atlantic regions ($76,500 and $71,000,respectively). The lowest salaries were in the Mountain region.
Reports of earlier salaries of medical school psychologists have beenlimited and less extensive. An overall median salary range of $20,000 to$24,000 was found in the mid-1970s for all psychologists within medicalschool settings (Nathan, Lubin, Matarazzo, & Persely, 1979). During thatsame era, full professors earned a median salary of $34,900, associate profes-
Table VII. 1996 Base
Geographic region
New EnglandMiddle AtlanticEast North CentralWest North CentralSouth AtlanticEast South CentralWest South CentralMountainPacific
, Clinical, Additional, and Total Income of Medical School Psychologistsby Geographic Region
Base
65,00071,00065,00063,00062,93765,80060,00055,60076,500
N
14532116663
33062
11534
130
Clinical
10,00010,00016,00020,00014,00010,00012,000
— a25,000
N
4112543105118216
27
Additional
3,0004,0004,9004,0004,0004,0003,5005,5004,000
N
871759036
19033481373
Total
72,18284,00074,00070,00068,50070,00067,95066,25087,300
N
14131216363
32361
11232
125
Note. States that comprise geographic regions are based on the catgorization used by theDepartment of Commerce’s Bureau of the Census.aInadequate number of subjects to report data.

232 Williams and Wedding
Table VIII. Comparison of Medical School Base Salaries and Non-Medical School AcademicSalaries: 1975-1976 and 1996-1997
FullAssociateAssistantLecturer
University graduate departments ofMedical school faculty psychology faculty
1975a
34,90027,00021,40017,500
1996b
98,00070,00055,00048,500
Percentagedifference
181159157177
1975-1976c
30,75722,75018,09416,456
1996-1997d
83,72260,23750,11143,878
Percentagedifference
172165177167
Note. Salaries of faculty within university departments of psychoogy have been converted to11- to 12-month salaries.aFrom Johnson and Wiliams (1979).bFrom the current study.cFrom Stang (1977).dFrom Wicherski and Kohout (1997c).
sors earned $27,000, assistant professors earned $21,400, andlecturersearned a median salary of $17,500 (Johnson & Williams, 1979); as wouldbe expected, salaries are positively related to academic rank and years sincethe doctorate (Nathan, Lubin, & Matarazzo, 1981).
Although it is difficult to make meaningful comparisons across surveys,psychologists working in medical schools have maintained a higher salarythan psychology faculty in university graduate departments of psychologyin the mid-1970s and 1990s at all academic ranks (Table VIII). The rateof growth of salaries from 1975 to 1996 was higher for full professors andlecturers in medical schools than for faculty with similar ranks in universitygraduate departments of psychology. In contrast, associate and assistantprofessors within university graduate departments of psychology enjoyeda higher salary growth rate than medical school faculty of comparable rank.
DISCUSSION
The results of this study accentuated several key characteristics rele-vant to the employment and salaries of medical school psychologists. First,compared to female psychologists, a slightly higher proportion of malepsychologists is employed in this setting, and whites represented a largerproportion of medical school psychologists than any other racial/ethnicgroup. Additionally, the highest proportions of psychologists could be foundin Middle and South Atlantic regions of the United States. Second, mostof these psychologists were administratively housed in departments of psy-chiatry and behavioral sciences. Third, the majority of these psychologists

Employment Characteristics and Salaries 233
worked an 11- to 12-month academic appointment and were appointed fulltime in a medical school or academic health center. Fourth, academic rankat the assistant professor level and non-tenure-track status were the normfor most of these professionals. Fifth, most of the time of these psychologistswas consumed by conducting research and providing clinical services; lesstime was spent on education and training or performing administrativeduties. Sixth, although a larger proportion of these psychologists weremembers of the medical staff (compared to those who were not officialmembers), a large number of them had restrictions to their membershipprivileges. Finally, as one would expect, the salaries of psychologists withinmedical school settings increased steadily with increasing academic rankand years of work experience but varied by gender and geographic region.
Several factors may contribute to the employment treds for this groupof psychologists. The rapid growth of female psychologists within medicalschools is likely due, in part, to the feminization of psychology as a whole[APA, 1995; Goodheart & Markham, 1992; Howard et al., 1986; NationalScience Foundation (NSF), 1993a,b, 1994; Ostertag & McNamara, 1991].In 1977, for instance, females comprised slightly more than one-fourth(27%) of the membership of the American Psychological Association(APA); by 1998, they represented almost one-half (48%) of the APA mem-bership (APA, 1998). Likewise, graduate enrollment of women has morethan doubled (NSF, 1994), and the number of doctoral degrees awardedto women has quadrupled (NSF, 1993b) from the 1970s to the 1990s, inthe face of declining male enrollees and doctorate recipients during thattime period. Despite the impressive increase in the number of womenpsychologists working in medical schools, marked salary disparities arepresent. This relationship appeared consistent and robust and was presentfor inexperienced, midlevel, and senior medical school psychologists.
The racial/ethnic and geographic distributions of medical school psy-chologists are fairly parallel to the racial/ethnic and geographic configura-tion of psychologists in general (Wicherski & Kohout, 1997b). Becauseabout one-third of psychologists are required to generate a median of 90%of their income through research grants (Williams, Wicherski, & Kohout,1998a,b), it is no surprise that research activities are an important compo-nent of the role of most medical school psychologists.
Other trends may be attributed to psychology’s socialization withinthe medical school setting. Full-time employment for psychologists rapidlyhas become the norm in medical school settings, perhaps due to the realiza-tion that psychology is an integral and legitimate part of health care andnot a peripheral part of the health care delivery system. This appreciationfor psychology within these settings is also apparent when one examinesthe increasing rates of medical staff membership for psychologists and the

234 Williams and Wedding
introduction of psychologists within departments other than psychiatry.The dispersion of psychologists across general medical departments hasbeen correlated with the decreasing percentage of psychologists workingwithin departments of psychiatry over the past several years. Due to a lackof longevity, full professorship in medical schools was rarely achieved bypsychologists prior to 1965. The marked increase in the numbers of medicalschool psychologists who have earned the rank of full professor is associatedwith both an increase in the number of psychologists working in this venueand enhanced respect and appreciation for the contributions made by medi-cal school psychologists.
Several caveats to the results should be noted. Although this surveyeffort was confined to medical school psychologists, this group is quiteheterogeneous, and these psychologists have varying types of doctoral de-grees, areas of expertise, and licensure status. Further, these psychologistsare employed in different departments and there are marked differencesacross geographic regions in the United States.
Comparisons of the current results to previous survey results shouldbe viewed cautiously. In some cases, previous studies differed from thecurrent study in the design, analysis of certain variables, sample size, andform in which questions were posed. This was especially the case with thosestudies that examined variables such as salaries and geographic distribution.
Based on historical trends, the future for psychologists within medicalschools appears promising. Clearly, the number, status, and salaries of thesepsychologists have increased dramatically over the past 30 years. Moreover,about two-thirds of these psychologists expressed satisfaction with theircurrent employment and 85% of them reported that they would recommendthe career to beginning professionals (Holden & Black, 1996). Graduatepsychology programs (e.g., clinical, counseling, experimental, neuropsy-chology, physiological) continue to provide curricula and train studentsin a manner that prepares them for clinical, research, and administrativepositions within medical school settings. Related, medical school settingsrepresent the location in which the largest number of predoctoral internsand postdoctoral fellows apply, and 50% of predoctoral interns are placedin hospital/medical settings (APPIC, 1997). As a result, large numbers ofpsychology trainees work in environments that promote psychology withinmedical schools and settings that recruit young professionals for careers asmedical school psychologists.
Several recent proposals augur well for the future of medical schoolpsychologists as they approach the millennium. Ever since the first indepen-dent department of medical psyhology was established at the University ofOregon Health Sciences Center in 1961, psychologists within other medicalschools have advocated for administratively independent and autonomous

departments of psychology. Independent departments of psychology werethe preferred choice of two thirds of these psychologists (Nathan, Mill-ham, & Lubin, 1979). Several other medical schools have moved in thisdirection since the 1960s.6 Next, many psychologists have advocated for andendorsed medication prescribing privileges for psychologists (Ax, Forbes, &Thompson, 1997; Cullen & Newman, 1997; DeLeon, DeNelsky et al., 1998;DeLeon, Fox, & Graham, 1991; Smyer, et al, 1993; Tuckman, 1996). Theprospect of psychologists receiving prescribing privileges would undoubt-edly create a new and larger role for psychologists in general, but especiallyfor those psychologists practicing within medical school settings. Third,growing numbers of patients and physicians are expressing interest in theprovision of psychological services as an integral component of primarycare (Cummings, Cummings, & Johnson, 1997; Nethercut & Piccione, 1984),and it is increasingly clear that physical problems are related to psychologi-cal distress (Levant, 1996; Nethercut & Piccione, 1984; Wilson-Barnett,1992). It is also likely that increasing numbers of experimental psychologists,biopsychologists, physiological psychologists, neuropsychologists, and pro-fessionals from other psychological subfields will play a larger role in theresearch conducted within this setting. Finally, the APA is currently em-barking upon a media campaign to promote psychology to the generalpublic, and specific recommendations for marketing psychology in academichealth centers have been proposed (Frank, 1997). As the public becomesmore aware of the breadth of services that psychologists have to offer,medical school psychologists could benefit tremendously from this increasedawareness of their role in preventing and treating physical illness.
There is still substantial information to be gleaned from the employ-ment and salary data collected on this group of psychologists. Given thatmedical school psychologists are increasingly becoming integrated withinthe medical school milieu, more research in this area is necessary. Forexample, it would be useful if future studies examined employment andsalary characteristics of psychologists in comparison to other comparablebut nonpsychological health care professions within medical schools.
ACKNOWLEDGMENTS
The authors would like to express their gratitude to Richard Evenson,Ph.D. for his scholarly revew of the manuscript, and Jessica L. Kohout,
The medical schools with independent departments of psychology are the Uniformed ServicesUniversity of the Health Sciences (USUS), the University of Florida, Rush-Presbyterian-St.Lukes, Pennsylvania State University, the Chicago Medical School, and the University ofManitoba School of Medicine.
Employment Characteristics and Salaries 235

236 Williams and Wedding
Ph.D., Paul D. Nelson, Ph.D., and Marlene Wicherski for their ongoinginvolvement in the design of the survey, database development, analysesof data, and review of the manuscript.
REFERENCES
American Psychological Association (APA) (1995). Report of the Task Force on ChangingGender Composition of Psychology. Washington, DC: APA.
American Psychological Association (APA) (1998). 1974-1998 membership register/directory.Washington, DC: APA.
Arnett, J. L., & Martin, R. M. (1981). Psychologists in Canadian medical schools. ProfessionalPsychology, 12, 237-245.
Association of Psychology Postdoctoral and Internship Centers (APPIC) (1997). Internshipand postdoctoral programs in professional psychology: Washington, DC: APPIC.
Ax, R. K., Forbes, M. R., & Thompson, D. D. (1997). Prescription privileges for psychologists:A survey of predoctoral interns and directors of training. Professional Psychology: Re-search and Practice, 28, 509-514.
Black, M. M., & Holden, E. W. (1998). The impact of gender on productivity and satisfactionamong medical school psychologists. Journal of Clinical Psychology in Medical Settings,5, 117-131.
Bodner, G. (1997). Does tenure protect the salaries of medical school faculty? AcademicMedicine, 72, 966-971.
Buck, R. L. (1961). Behavioral scientists in the schools of medicine. Journal of Health andHuman Behavior, 2, 59-64.
Cullen, E. A., and Newman, R. (1997). In pursuit of prescription privileges. ProfessionalPsychology: Research and Practice, 28, 101-106.
Cummings, N. A., Cummings, J. L., & Johnson, J. N. (1997). Behavioral health in primarycare. Madison, CT: Psychosocial Press.
DeLeon, P. H., Fox, R. E., & Graham, S. R. (1991). Prescription privileges: Psychology’s nextfrontier? 98th Annual Convention of the American Psychological Association Distin-guished Professional Contributions Award Address (1990, Boston Massachusetts). Ameri-can Psychologist, 46, 384-393.
DeLeon, P. H., DeNelsky, G. Y., et al. (1998). Should psychologists be allowed to prescribedrugs? In S. Noelen-Hoeksema (Ed.), Clashing Views on Abnormal Psychology: A TakingSides Custom Reader (pp. 36-53). Westport, CT: Dushkin/McGraw-Hill.
Frank, R. G. (1997). Marketing psychology at academic health centers. Journal of ClinicalPsychology in Medical Settings, 4, 41-49.
Goodheart, C. D., & Markham B. (1992). The feminization of psychology: Implications forpsychotherapy. Special Issue: The future of psychotherapy. Psychotherapy, 29, 130-138.
Holden, E. W., & Black, M. D. (1996). Psychologists in medical schools—Professional issuesfor the future: How are rank and tenure associated with productivity and satisfaction?Professional Psychology: Research & Practice, 27, 407-414.
Howard, A., Pion, G. M., Gottfredson, G. D., Flattau, P. E., Oskamp, S., Pfafflin, S. M., Bray,D. W., & Burstein, A. G. (1986). The changing face of American Psychology. AmericanPsychologist, 41, 1311-1327.
Johnson, J. J., & Williams, T. A. (1979). The psychologists in the department of psychiatry.Professional Psychiatry, 10, 318-323.
Levant, R. F. (1996). The psychological physician: Onward to the future. Journal of ClinicalPsychology in Medical Settings, 3, 167-172.
Lubin, B., Nathan, R. G., & Matarazzo, J. D. (1978). Psychologists in medical education:1976. American Psychologist, 33, 339-343.
Lubin, B., Nathan, R. G., Gildenberg, S., Matarazzo, J. D. (1980). Medical school characteris-tics associated with the employment of psychologists. Professional Psychology, 11, 1-2.

Employment Characteristics and Salaries 237
Matarazzo, J. D. (1994). Psychology in a medical school: A personal account of a department’s35-year history. Journal of Clinical Psychology, 50, 7-36.
Matarazzo, J. D., & Daniel, R. S. (1957a). Psychologists in medical schools: Personal, profes-sional, academic, and scientific characteristics. Journal of Neuropsychiatry, 4, 93-107.
Matarazzo, J. D., & Daniel, R. S. (1957b). The teaching of psychology by psychologists inmedical schools. Journal of Medical Education, 32, 410-415.
Matarazzo, J. D., Lubin, B., & Nathan, R. G. (1978). Psychologists membership on the medicalstaff of university teaching hospitals. American Psychologist, 33, 23-29.
Matarazzo, J. D., Carmody, T, P., & Gentry, W. D. (1981). Psychologists on the faculties ofUnited States schools of medicine: Past, present, and possible future. Clinical PsychologyReview, 1, 293-317.
Mensh, I. N. (1962). Psychology and other professions. In W. B. Webb (Ed.), The professionof psychology. New York: Holt, Rinehart & Winston.
Mensh, I. N. (1953). Psychology in medical education. American Psychologist, 8, 83-85.Nathan, R. G., Lubin, B., Matarazzo, J. D., & Persely, G. W. (1979). Psychologists in schools
of medicine: 1955, 1964, and 1977. American Psychologist, 34, 622-627.Nathan, R. G., Millham, J., & Lubin, B. (1979). Organizational structure and roles of psycholo-
gists in schools of medicine. Professional Psychology, 10, 97-103.Nathan, R. G., Lubin, B., & Matarazzo, J. D. (1981). Salaries and satisfactions of medical
school psychologists. Professional Psychology, 12, 420-425.National Science Foundation (1993a). Federal funds for research & development: Fiscal years
1991, 1992, and 1993. Washington, DC: NSF.National Science Foundation (1993b). Science and engineering doctorates: 1960-91, detailed
statistical tables (NSF-93-301). Washington, DC: NSF.National Science Foundation (1994). Special analyses of the data from 1973-1991, survey of
doctorate recipients, Unpublished raw data.Nethercut, G., & Piccione, A. (1984). The physician perspective of health psychologists in
medical settings. Health Psychology, 3, 175-184.Ostertag, P. A., & McNamara, J. R. (1991). “Feminization” of psychology: The changing sex
ratio and its implications for the profession. Psychology of Women Quarterly, 15, 349-369.Routh, D. K. (1972). Psychological training in medical school departments of pediatrics: A
second look. American Psychologist, 27, 587-589.Rozensky, R. H. (1994). Clinical psychology in medical settings: Psychology’s role in health
care. Journal of Clinical Psychology in Medical Settings, 1, 1-5.Seime, R. J. (1998). The section of psychology: Psychology in an academic health sciences
center’s department of behavioral medicine and psychiatry. Journal of Clinical Psychologyin Medical Settings, 5, 215-233.
Smyer, M. A., Balster, R. L., Egli, D., Johnson, D. L., et al. (1993). Summary of the reportof the Ad Hoc Task Force on Psychopharmacology of the American Psychological Associ-ation. Professional Psychology: Research and Practice, 24, 394-403.
Stang, D. J. (1977). Salaries of graduate faculty in Psychology: 1966-67 through 1976-77.Washington, DC: American Psychological Association.
Thompson, R. J., & Matarazzo, J. D. (1984). Psychology in Untied States medical schools:1983. American Psychologists, 39, 988-955.
Tuckman, A. (1996). Isn’t it about time psychologists were granted prescription privileges?Psychotherapy in Private Practice, 15, 1-14.
Wagner, N. N. (1968). Psychologists in medical education: A 9-year comparison. Social Scienceand Medicine, 2, 81-86.
Wagner, N. N., & Stegeman, K. L. (1964). Psychologists in medical education. AmericanPsychologist, 19, 689-690.
Wedding, D. (1997). Creating a research-friendly workplace. Journal of Clinical Psychologyin Medical Settings, 4, 51-60.
Wicherski, M., & Kohout, J. (1997a). 1995 Doctorate Employment Survey. Washington, DC:American Psychological Association.
Wicherski, M., & Kohout, J. (1997b). 1997 profiles of APA members, Unpublishe raw data.

238 Williams and Wedding
Wicherski, M., & Kohout, J. (1997c). 1996-97 faculty salaries in graduate departments ofpsychology. Washington, DC: American Psychological Association.
Wicherski, M., Williams, S., & Kohout, J. (1998). 1997-98 faculty salaries in graduate depart-ments of psychology. Washington, DC: American Psychological Association.
Williams, S., Wicherski, M., & Kohout, J. (1998a). 1997 salaries in psychology. Washington,DC: American Psychological Association.
Williams, S., Wicherski, M., & Kohout, J. (1998b). 1997 employment characteristics and salariesof medicat school psychologists. Washington, DC: American sychological Association.
Wilson-Barnett, J. (1992). Psychological reactions to medical procedures. Psychotherapy andPsychosomatics, 57, 118-127.
Witkin, H. A., Mensh, I. N., & Gates, J. (1972). Psychologists in medical schools. AmericanPsychologist, 27, 434-440.
U.S. Bureau of the Census. (1997), Statistical abstract of the Unied States, 117th ed. Washington,DC: Author.