empowerment in mental health practice: behavioural means … · empowerment in mental health...
TRANSCRIPT

EMPOWERMENT IN MENTAL HEALTH
PRACTICE: Behavioural Means of
Client Empowerment
By: Courtney Brennan
April 2011

2 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
Health professionals are powerful. Each carries with them a power exercised unconsciously
over others as a result of their designation, their knowledge-base, and their status. But in addition to
this contextual power, individuals in dominant positions have a tendency to display certain
dominance behaviours through their nonverbal communication, though the relationship between
these behaviours and dominance is unclear (Knapp & Hall, 2002). What’s interesting is how these
dominance behaviours can affect the behaviour of others. For example, B.F. Skinner and Erich
Fromm once attended a symposium together, where Skinner found himself in a disagreement with
Fromm and opted to use his behavioural theories to make his point:
On a scrap of paper I wrote ‘Watch Fromm’s left hand. I am going to shape a chopping
motion’ and passed it down the table to [Halleck Hoffman]. Fromm was sitting directly across
from the table and speaking mainly to me. I turned my chair slightly so that I could see him
out of the corner of my eye. He gesticulated a great deal as he talked, and whenever his left
hand came up, I looked straight at him. If he brought the hand down, I nodded and smiled.
Within five minutes he was chopping the air so vigorously that his wristwatch kept slipping
out over his hand. William Lederer had seen my note, and he whispered to Halleck. The note
came back with an addendum: ‘Let’s see you extinguish it.’ I stopped looking directly across
the table, but the chopping went on for a long time. (Skinner, 1983, pp. 54)
This quote from Skinner readily demonstrates the concept of pervasively influencing the
behaviour of others through dominance behaviours and positive reinforcement. This demonstration
raises questions on how individuals in positions of power can exert that power non-verbally over
others, and this can potentially influence the actions of others.
Powerlessness is a result of another individual exercising power-over another individual and
presents as alienation, disenfranchisement from resources, rights, and privileges, and potentially
learned helplessness (Clark & Krupa, 2000). Because health professionals take a powerful

3 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
leadership role in mental health practice, mental health clients may be especially vulnerable to the
effects of the power imbalance created by that role, compounded by the awareness of the
designation of ‘health professional’, altering their behaviour and increasing their sense of
powerlessness. However this powerlessness is the antithesis of the goal of current mental health
practice, a field attempting to embody the idea of empowerment, the increase of the holistic strength
of individuals and communities through developing confidence in one’s capacities (Townsend,
2000). However the actual practice of empowerment in mental health is often met with tension and
undermined by organizational process and objectification of the client. In order to challenge the
routine organization of power within mental health practice, Townsend (1998) recommends that
“With awareness of their participating in ruling institutions, professionals might reduce their
dominance and become translators, transmitters, facilitators, and activists who work with and on
behalf of the people they want to help.” This quote calls for action on the part of professionals to
take responsibility over their own dominance and demonstrate an individualized commitment to the
empowerment philosophy they are attempting to embody. As such, this paper will examine concrete
changes in objective behaviours professionals can analyze and adjust accordingly to increase their
client’s sense of empowerment during therapist-client discussions.
When looking objectively at human interaction, an examination from the behavioural frame of
reference is necessary. The behavioural frame of reference looks at how behaviours are formed by
observable environmental responses and the use of reinforcement and punishment to influence
behaviours in terms of intensity, duration, and frequency (Firor et al., 2009). This perspective
emphasizes an individual’s behaviours as they are objectively observable and can be manipulated
directly, facilitating research and objective assessments and outcomes. Clinician behaviour during
client interactions is an important area of practice health professionals have direct control over and
can improve and adjust with self-awareness and reflection. In taking this perspective, I hope to

4 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
examine how to adjust objective clinician behaviours to influence the behaviour of clients to enable
empowerment.
An understanding of occupation is key to this topic as occupational therapy presents as a unique
health profession, as it often resembles and is based on empowerment education, and occupational
therapists may enable empowerment by helping people to feel more powerful and to act with greater
power in everything from self-care to work hardening programmes, or through guidance in
occupations such as meeting attendance, public speaking, film making, or advocating for change in
disability benefits (Townsend, 2000). As such, occupational therapists working in mental health
settings are well positioned to be leaders in the empowerment of their clients, and should take it
upon themselves to meet this challenge.
For my paper I intend to investigate tangible and concrete methods of increasing a client’s sense
of empowerment. As such, this topic will fit well with the compendium’s chapter on Considering
Power and Empowerment. My objective is to investigate the various non-verbal behaviours implying
dominance and power, as well as avoidance and dependence. This will be obtained through a review
of non-verbal communication literature. Following this investigation, my second objective is to
examine how these behaviours can be applied in clinical practice to influence behaviour, namely by
decreasing dominance behaviours in clinicians to foster empowerment in clients.
Many self-help books praise the endless power of exhibiting dominant behaviours in persuasion,
conflict management, and debate, however the relationship between nonverbal dominance
behaviours and power status is less clear cut than it is made out to be due to the complexity of the
constructs and alternating use of concepts like dominance, power, and status (Knapp & Hall, 2002).
In personality research, the DISC (Dominance, Influence, Steadiness, & Compliance) model has been
translated into a formal standardized assessment measure of dominance in personality (See
Appendix A; Chapman, 2011). This assessment can be used to provide professionals with a general

5 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
understanding of how dominance influences their individual behaviour. In addition to the personality
psychology realm, behavioural psychologists, organizational behaviourists, and evolutionary
psychologists have conducted a great deal of research on human interaction paradigms and
dominance/avoidance behaviours exhibited in social interactions. From this research, there have
been several key behaviours associated with social dominance and power in human interaction, as
shown in Table 1.
Table 1: Common Dominance Behaviours
Voice Speak clearer, louder, and more well-articulated
Touch
Relaxed & expansive postures
Initiating touch
Gaze
Increased gaze is associated with credibility and dominance
High status people are looked at, and look more while talking than listening
Timing Waiting time increases for dominant people
Dominant people talk more and interrupt more
(Knapp & Hall, 2002).
Because lacking power implies increased dependence on others, those who lack power are
especially sensitive to how other people evaluate them and encounter more constraints and
interference (Keltner, Gruenfeld, & Anderson, 2003). This suggests that clients in mental health
settings may be more attuned to dominance behaviours and react more strongly to them.
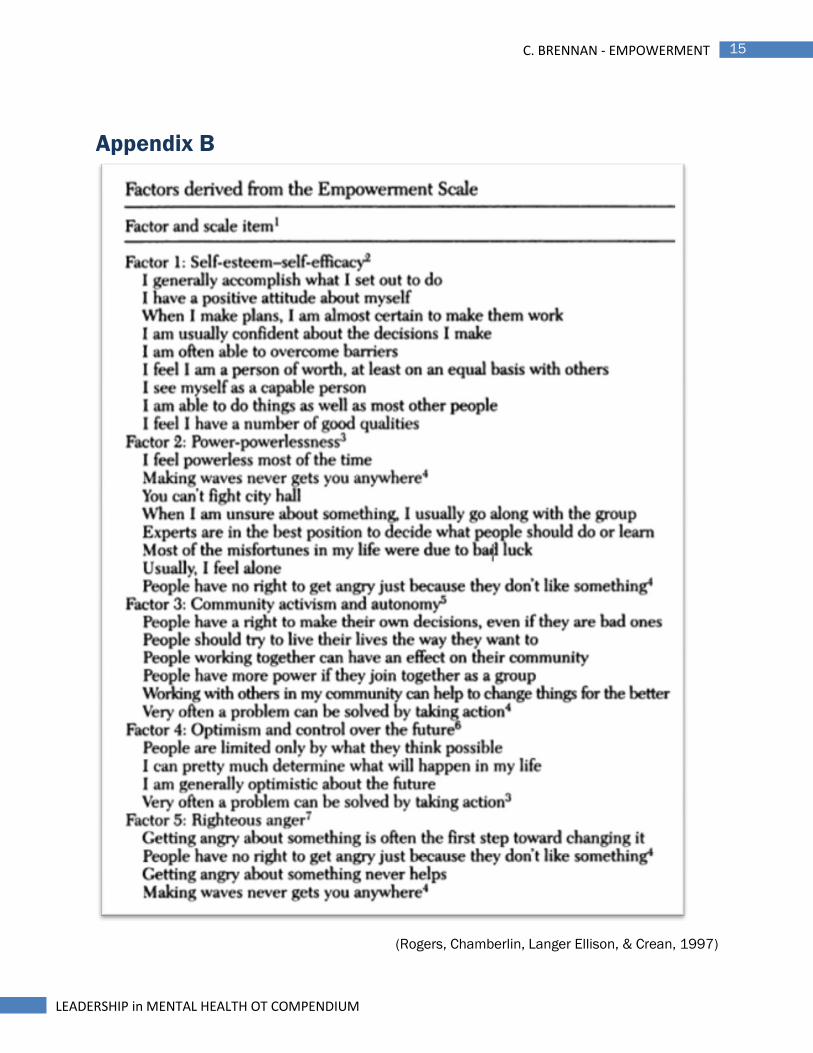
Additionally, this information demonstrates the need for mental health workers to be educated about
dominance behaviours and how they manifest in everyday interactions, potentially through staff
education sessions (See Appendix B). Mental health clients have been noted to demonstrate
decreased duration of eye contact, increased downward gaze, and lack body language, which may
lead to negative evaluations in daily social interactions and signal a lack of power (Tickle-Degnen &

6 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
Rosenthal, 1992). Lacking power means a person not only has less access to resources, material
and otherwise, but also is more subject to social threats and punishments, creating the type of
negative, threatening context that would activate the avoidance system (Smith & Bargh, 2008).
These findings demonstrate that individuals with mental illness are often pathologically powerless in
their actions, and this affects how the world reacts to them, furthering their lack of power. As such, it
is important as clinicians to make strides to return that power to our clients by enabling them to
participate in their care and experience empowerment. Table 2 shows attributes of empowerment as
described by mental health services consumers, outlining key actions that give them a sense of
empowerment.
Table 2
(Rogers, Chamberlin, Langer Ellison, & Crean, 1997)
When looking for potential applications of nonverbal communication to the concept of
empowerment, there was no direct research to establish this connection. The book Empowerment
Overruled by Elizabeth Townsend (1998) provided some guidance in terms of how empowerment
7 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
should manifest through collaborative decision making, facilitated risk taking, and empowerment
education, and highlighted the importance of reducing dominance of the clinician, but had no
mention of directly observable dominance behaviours. As such, by comparing and categorizing
nonverbal behaviours as facilitating different components of consumer-identified attributes
empowerment, I identified a few potential categories of concrete means of potentially fulfilling
empowerment: Decrease Objectification, Reduce Exclusivity, Monitor Dominance, and Reinforce
Power Use (See Appendix C).
In terms of decreasing objectification, the institutional processes of assessment, diagnosis, and
medication largely objectify the individual as a broken item requiring repair. The individual is lost in
these processes as they are labelled and shuffled around between professionals. A concrete means
of avoiding this pitfall includes using person-first language and referring to the consumers of the
mental health system as Clients, Members, Consumers, or Residents to decrease the client’s
potential sense of objectification (Townsend, 1998). Additionally, inviting participation to involve
client in collaborative decision-making & practicing in a client-centred manner helps to empower the
individual as a director of their own care and remind them of their rights as a person.
Reducing the exclusiveness afforded to professionals by access to knowledge and resources
enables clients to further direct their care. By sharing privileges, eating areas, washrooms, library
materials, educational opportunities, and chores, implicit dominance relayed by context and position
is decreased by an equalization of physical forms of power. Additional resources can also be
provided to equalize interactions further, for example providing clients with a notebook to make their
own notes while you make documentation notes enable them to keep track of the decisions made
during sessions and equalizes visually manifested power imbalances.
The theme of monitoring clinician dominance behaviours also became apparent through the
literature, looking at ways to increase the client’s positive self-image and reduce stigma by acting

8 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
towards them in a way that is not overbearing and powerful, but instead as equals. Avoiding
inequality in seating and positioning may play a role in this realm through ensuring the clinician
doesn’t stand over the seated client or positions themselves in a higher plan or in a seat of
prominence, such as that at the head of a table. By enabling the client to take a position of power,
this may have affects on their behaviour in terms of increasing assertiveness. Additionally, Knapp
and Hall (2002) spoke to the importance of avoid dominant timing patterns, in terms of making a
client wait for your presence. Being waited for signals power and dominance, as well as disrespect
and unimportance of the client’s issues, so practicing punctuality may prevent the client from
sensing the clinician as being powerful over them and additionally like their issues are not worth the
clinicians time. Furthermore, in conversation, avoiding interrupting and allowing silence for the client
to interject is key to the empowerment process, as interrupting and dominating conversation are very
dominant behaviours. Providing clients with the time to express their opinions and ideas without
being interrupted enables them to participate more fully in their decision making and may help them
to come out of their shell and open up.
Finally, reinforcing the client’s use of powerful behaviours through nonverbal communication
may be a key means of objective empowerment. This can be done through displaying positive
feedback cues in response to client demonstrating empowerment, or dominant behaviours. These
positive feedback behaviours may include smiling, nodding, providing eye contact, as well as verbal
cues to alert the client to their use of these behaviours, and how they help to improve
communication skills as well as portrayed competence, a reoccurring theme in the consumer-
identified empowerment attributes. Additionally, the clinician must monitor their use of negative
feedback cues in response to client behaviours, avoiding forceful gestures, standing over the client,
and making unconscious negative facial displays (ex., frowns) in response to the client seeking
empowerment opportunities and demonstrating dominance behaviours, as this may undermine the

9 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
empowerment the client feels and reverse progress that has been made. Furthermore, sharing
knowledge with the client of these tactics may play a role in their empowerment education, as
dominance behaviours the clinician utilizes may be incorporated into the client’s behavioural
repertoire with facilitated reflection.
While these categories of objective empowerment are not directly based in research, there
have been studies to demonstrate the nonverbal benefits of control. Research has found that
participants assigned control over resources expressed their true attitudes, experienced more
positive and less negative emotion, were more likely to perceive rewards (ex. that their partner liked
them), and were less likely to perceive threats (ex. that their partner felt anger toward them)
(Anderson & Berdahl, 2002). Most of these effects were mediated by the sense of power, suggesting
that subjective feelings of power are an important component in the effects of power. That is,
through empowerment clients would be better situated to participate actively in therapy processes.
By incorporating these behavioural changes and organizational adjustments, there is the potential
for greater empowerment among clients, and as such, greater participation in the therapy process.
Further research is necessary to determine the explicit effects of these empowerment strategies;
however the benefit of the strategies suggested is that, due to their non-verbal nature, they are
neither time nor resource intensive and merely require greater reflection on the part of the clinician
regarding their behaviour and whether they are truly ‘talking the talk and walking the walk’ of client
empowerment.
A key component of acting as a change agent is the ability to monitor and modify one’s
progress to assess change and outcome in this area or based on experience. Rogers, Chamberlin,
Langer Ellison, & Crean (1997) have psychometrically tested the Empowerment Scale (see Appendix
D) for use with consumers, which analyzes attributes such as having access to
information/resources, having a range of options to make choices, learning skills, increasing positive

10 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
self-image, and changing other’s perceptions of competency on a 4 point Likert-scale ranging from
strongly disagree to strongly agree . Utilizing a measure of empowerment such as this one will inform
clinicians as to whether their clients feel empowered, and whether they need to adjust and modify
their practice to improve this state. Utilizing an assessment tool such as this one enables clinicians
to quantify their empowerment practices and gain objective data on the changes in client
empowerment they are potentially fostering.
In summary, it is important for clinicians to realize that mental health clients are pathologically
disempowered and this is reflected in their demeanour and non-verbal communication. Additionally,
as professionals placed in dominant positions with a specialization in enabling occupation,
occupational therapists hold a unique position to lead a paradigm shift of empowerment within
mental health contexts. Though clinicians have the best intentions for client empowerment,
organizational constraints often limit the actions of those with the best intentions and create
unbalanced power dynamics preventing client empowerment. As such, the onus of empowerment is
on us as clinicians to take necessary measures to offset these unbalanced power dynamics and
empower clients through our own behaviour. It is not enough to merely intend on empowering
clients, but it is necessary to literally ‘walk the walk’ of empowerment by making conscious
behavioural adjustments to foster the best intentions of clinicians, while reinforcing the behavioural
changes of our clients that are leading them to be more assertive, appear more competent, and feel
able to make a difference in their own lives.
Reflecting on the process of this paper, I found I discovered more objective means of
empowerment than I expected, and far more input from the perspective of the client regarding
empowerment than I thought would exist. I initially chose this topic because I find I personally often
manifest a number of dominant behaviours in my own social interactions, and as someone of
imposing stature, tend to be viewed as dominant in interactions even if I make an attempt not to be.

11 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
I wanted to explore this area of practice because I realize the importance of empowerment in mental
health settings and I wanted to find concrete measures I could take to downplay my own nonverbal
dominance and encourage the empowerment of the client. Initially as I approached this paper I
assumed I would be looking at means of directly altering my own nonverbal behaviours, but as I
researched nonverbal communication I realized that what was more important was empowering the
client to demonstrate dominance behaviours of their own through positive reinforcement of their
nonverbal behaviours. As opposed to adjusting my own non-verbal dominance practices being the
focus, I had to modify my plan to additionally include a reinforcement component for the client’s
empowered behaviours, which I was not expecting. I feel that putting the tips I established into
practice would require a great deal of conscious cognition over my own behaviour, which is not an
area I’m strong in, but I feel that the process of writing up this paper and having to find all of the
ways myself will benefit my future practice greatly and enable me to lead others in the field of mental
health to empower their clients through their actions as well as their words.
12 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
References
Anderson, C. & Berdahl, J. L. (2002). The experience of power: Examining the effects of power on
approach and inhibition tendencies. Journal of Personality and Social Psychology, 83(6), 1362-
1377. doi: 10.1037/0022-3514.83.6.1362
Chapman, A. (2011). DISC: DISC basic personality types model. Retrieved from
http://www.businessballs.com/personalitystylesmodels.htm#DISC personality systems
Clark, C. C. & Krupa, T. (2002). Reflections on empowerment in community mental health: Giving
shape to an elusive idea. Psychiatric Rehabilitation Journal, 25(4), 341-349.
Firor, E., Perras, E., Zimmerman, K., McCarthy, K., & Kronk, P. (2009). Frames of reference used in
occupational therapy. In K. Jacobs & L. Jacobs (Eds.), Quick reference dictionary for
occupational therapy (5th ed.)(pp. 312-314). Thorofare, NJ: SLACK Inc.
Keltner, D., Gruenfeld, D. H., & Anderson, C. (2003). Power, approach, and inhibition. Psychology
Reviews, 110(2). 256-284. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12747524
Knapp, M. L. & Hall, J. A. (2002). Nonverbal communication in human interaction. (5th edition).
Toronto, ON: Nelson Thomson Learning.
Rogers, E., Chamberlin, J., Langer Ellison, M., & Crean, T. (1997). A consumer-constructed scale to
measure empowerment among users of mental health services. Psychiatric Services 48,
1042-1047.
Skinner, B. F. (1985). A matter of consequence. New York, NY: New York University Press.

13 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
Smith, P. K., & Bargh, J. A. (2008). Nonconscious effects of power on basic approach and avoidance
tendencies. Social Cognition, 26(1): 1-24. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2435045/
Tickle-Degnen, L., & Rosenthal, R. (1992). Nonverbal aspects of therapeutic rapport. In R. S.
Feldman (Ed.). Applications of nonverbal behavioural theories and research. Hillsdale, NJ:
Lawrence Erlbaum Associates Inc.
Townsend, E. (1998). Good intentions overruled: A critique of empowerment in the routine
organization of mental health services. Toronto, ON: University of Toronto Press.
Townsend, E. (2001). Enabling empowerment: Using simulations versus real occupations. Canadian
Journal of Occupational Therapy, 63(2), 114-128.

14 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
Appendix A
(Chapman, 2011)
15 C. BRENNAN - EMPOWERMENT
LEADERSHIP in MENTAL HEALTH OT COMPENDIUM
Appendix B
(Rogers, Chamberlin, Langer Ellison, & Crean, 1997)