endobronchial ultrasound-guided fine needle aspiration biopsy: role of the cytopathologist in use...
TRANSCRIPT
S64 Abstracts
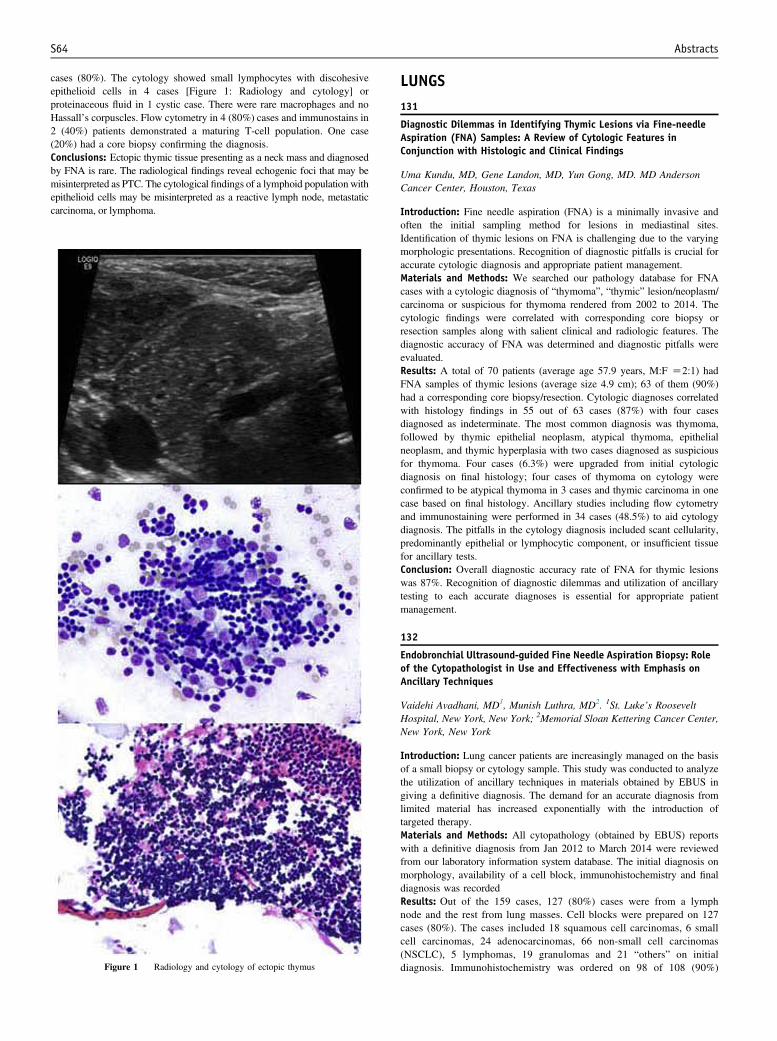
cases (80%). The cytology showed small lymphocytes with discohesiveepithelioid cells in 4 cases [Figure 1: Radiology and cytology] orproteinaceous fluid in 1 cystic case. There were rare macrophages and noHassall’s corpuscles. Flow cytometry in 4 (80%) cases and immunostains in2 (40%) patients demonstrated a maturing T-cell population. One case(20%) had a core biopsy confirming the diagnosis.Conclusions: Ectopic thymic tissue presenting as a neck mass and diagnosedby FNA is rare. The radiological findings reveal echogenic foci that may bemisinterpreted as PTC. The cytological findings of a lymphoid population withepithelioid cells may be misinterpreted as a reactive lymph node, metastaticcarcinoma, or lymphoma.
Figure 1 Radiology and cytology of ectopic thymus
LUNGS131
Diagnostic Dilemmas in Identifying Thymic Lesions via Fine-needleAspiration (FNA) Samples: A Review of Cytologic Features inConjunction with Histologic and Clinical Findings
Uma Kundu, MD, Gene Landon, MD, Yun Gong, MD. MD AndersonCancer Center, Houston, Texas
Introduction: Fine needle aspiration (FNA) is a minimally invasive andoften the initial sampling method for lesions in mediastinal sites.Identification of thymic lesions on FNA is challenging due to the varyingmorphologic presentations. Recognition of diagnostic pitfalls is crucial foraccurate cytologic diagnosis and appropriate patient management.Materials and Methods: We searched our pathology database for FNAcases with a cytologic diagnosis of “thymoma”, “thymic” lesion/neoplasm/carcinoma or suspicious for thymoma rendered from 2002 to 2014. Thecytologic findings were correlated with corresponding core biopsy orresection samples along with salient clinical and radiologic features. Thediagnostic accuracy of FNA was determined and diagnostic pitfalls wereevaluated.Results: A total of 70 patients (average age 57.9 years, M:F Z2:1) hadFNA samples of thymic lesions (average size 4.9 cm); 63 of them (90%)had a corresponding core biopsy/resection. Cytologic diagnoses correlatedwith histology findings in 55 out of 63 cases (87%) with four casesdiagnosed as indeterminate. The most common diagnosis was thymoma,followed by thymic epithelial neoplasm, atypical thymoma, epithelialneoplasm, and thymic hyperplasia with two cases diagnosed as suspiciousfor thymoma. Four cases (6.3%) were upgraded from initial cytologicdiagnosis on final histology; four cases of thymoma on cytology wereconfirmed to be atypical thymoma in 3 cases and thymic carcinoma in onecase based on final histology. Ancillary studies including flow cytometryand immunostaining were performed in 34 cases (48.5%) to aid cytologydiagnosis. The pitfalls in the cytology diagnosis included scant cellularity,predominantly epithelial or lymphocytic component, or insufficient tissuefor ancillary tests.Conclusion: Overall diagnostic accuracy rate of FNA for thymic lesionswas 87%. Recognition of diagnostic dilemmas and utilization of ancillarytesting to each accurate diagnoses is essential for appropriate patientmanagement.
132
Endobronchial Ultrasound-guided Fine Needle Aspiration Biopsy: Roleof the Cytopathologist in Use and Effectiveness with Emphasis onAncillary Techniques
Vaidehi Avadhani, MD1, Munish Luthra, MD2. 1St. Luke’s RooseveltHospital, New York, New York; 2Memorial Sloan Kettering Cancer Center,New York, New York
Introduction: Lung cancer patients are increasingly managed on the basisof a small biopsy or cytology sample. This study was conducted to analyzethe utilization of ancillary techniques in materials obtained by EBUS ingiving a definitive diagnosis. The demand for an accurate diagnosis fromlimited material has increased exponentially with the introduction oftargeted therapy.Materials and Methods: All cytopathology (obtained by EBUS) reportswith a definitive diagnosis from Jan 2012 to March 2014 were reviewedfrom our laboratory information system database. The initial diagnosis onmorphology, availability of a cell block, immunohistochemistry and finaldiagnosis was recordedResults: Out of the 159 cases, 127 (80%) cases were from a lymphnode and the rest from lung masses. Cell blocks were prepared on 127cases (80%). The cases included 18 squamous cell carcinomas, 6 smallcell carcinomas, 24 adenocarcinomas, 66 non-small cell carcinomas(NSCLC), 5 lymphomas, 19 granulomas and 21 “others” on initialdiagnosis. Immunohistochemistry was ordered on 98 of 108 (90%)

Abstracts S65
malignant cases with cell blocks. Out of the 66 NSCLC, 57 (86.3) hadadequate cell blocks and 100% of these had immunohistochemistry.Out of the 9 with inadequate cell blocks, 7 were finally givena diagnosis of NSCLC (10.6%).Conclusions: Cell blocks have become an essential part of thearmamentarium of the cytopathologist in both benign and malignantcases. Immunohistochemistry has also become an essential ancillarytool and is being used not only to get to a definitive diagnosis but alsoto confirm the morphological diagnosis. Without IHC support, the rateof NSCLC was 58% and with IHC the rate of NSCLC decreased to6%. Hence, effective communication with the clinician regardinggetting adequate material, adequacy assessment and purpose is thecornerstone of the role of the cytopathologist and ancillary staff aseffective members of the clinical team.
133
The Correlation of Concomitant Fungal Culture and GMS Staining ofBronchoalveolar Lavage Specimens: A 100 Case Institutional Review
Ariana Beck, MD, Frances Cate, MD, Alice Coogan, MD. VanderbiltUniversity Medical Center, Nashville, Tennessee
Introduction: Bronchoalveolar lavage (BAL) is a common procedure usedfor the diagnosis of fungal respiratory tract infections. Although microbi-ologic culture is the gold standard in the diagnosis and characterization offungal species, the time frame is not ideal clinically. Therefore, Grocott’smethenamine silver (GMS) staining of concomitant cytologic specimens isused to screen for the presence of fungal elements. Our study aims to lookat the correlation between GMS staining and culture results at ourinstitution.Materials and Methods: Our database was queried for cytologic casesprocured during BAL procedures with fungal elements seen on GMSstaining from 2009 to 2013. 100 unique cases were retrieved. Cultureresults were ascertained from the medical record. Cases were consideredconsistent when the organism cultured matched the organism identified bycytology and inconsistent when the culture was negative or a differentorganism was identified.Results: Of 100 cases, 93 had concomitant fungal culture results. Of thosecases, 68% had consistent cytology and microbiology and 32% of caseswere inconsistent. 73% of inconsistent cases were due to negativemicrobiology (22 cases). This is attributed to sampling error or decreasedviability secondary to treatment. In the remaining 8 inconsistent cases, theorganism identified was different than that cultured. In 5 of these cases, theless commonly seen organisms Chrysosporium sp, Saccharomyces cerevi-siae, Scopulariopsis brumptii, Scedosporium prolificans, and Penicillium spwere identified as Candida sp or Aspergillus sp by cytology. In 3 cases,commonly seen organisms were discrepant. In 2 of these cases, Aspergillussp was incorrectly identified as Candida sp which is a common diagnosticpitfall.Conclusions: GMS staining of cytologic preparations collected duringBAL is a pragmatic diagnostic test for the presence of fungalpathogens and correlates well with cultures. Inconsistencies in whichincorrect organisms were identified were primarily seen withuncommon organisms.
134
Correlation of p16 Expression with p53, Cyclin D1 as Well as ClinicalOutcomes in Non-small Cell Lung Carcinoma (NSCLC)
Jamal Carter, MD, Susan Geddes, CT(ASCP), Zhen Zhang, PhD,Hui Zhang, PhD, Frederic Askin, MD, Edward Gabrielson, MD,Qing Kay Li, MD, PhD. The Johns Hopkins Medical Institutes, Baltimore,Maryland
Introduction: Recent studies have identified a multitude of genetic andepigenetic changes affecting CDKN2A signaling in lung cancers, includingmutations of CDKN2A, deletions or inactivating of p16INK4, mutations ofRB1, and mutations affecting CDKN2A and RB1. These genetic alterations
can result in an elevated p16 protein. The clinical significance of elevatedp16 in lung cancer is not well understood. In this study, we correlatedexpressions of p16 with levels of p53 and cyclinD1 as well as clinicaloutcomes in NSCLC patients.Materials and Methods: Primary lung cancer TMAs (0.6 mm indiameter, 3-4 cores per cases) were constructed using surgicallyresected specimens retrieved from department archives, including 75cases of pulmonary adenocarcinoma (ADC), 88 cases of pulmonarysquamous cell carcinoma (SQCC), and 60 tumor-matched normal lungtissues. Immunohistochemistry (IHC) of p16 (clone INK4a/E6H4), p53and cyclinD1 were performed. Nuclear staining patterns were scoredsemi-quantitatively as 0-3+ (from negative to strong positive staining).Clinical information was correlated.Results: The overall frequency of expression of p16 in ADCs andSQCCs was 50.7% and 35.2%, respectively. In ADCs, patients withp16 positive tumors had smaller tumor size, earlier tumor stage andlonger survival compared to patients with p16 negative tumors, withmean survival of 41.1 vs. 28.9 month (PZ0.047). In SQCCs, a slightlyworse survival for patients with p16 positive tumors (30.1 vs. 37.3months) did not reach statistical significance (PZ0.382). In bothSQCCs and ADCs, p16 expression was not significantly correlatedwith expressions of p53 and cyclinD1.Conclusions: p16 is aberrantly expressed in a large subset of ADC andSQCC. Elevated p16 levels appear to be correlated with better prognosis inpatients with ADCs, suggesting that p16 expression might play differentroles in different subtypes of NSCLC. Further studies are necessary tocharacterize the molecular role of p16 in lung cancers.
135
Utility of Endobronchial Ultrasound-Guided Transbronchial NeedleAspiration (EBUS-TBNA) for the Diagnosis of Mediastinal Lymphoma
Arivarasan Karunamurthy, MD1, Walid Khalbuss, MD, PhD, FIAC2,Liron Pantanowitz, MD1, Sara Monaco, MD1. 1University of PittsburghMedical Center, Pittsburgh, Pennsylvania; 2GE Clarient DiagnosticServices, Aliso Viejo, California
Introduction: Endobronchial ultrasound-guided transbronchial needleaspiration (EBUS-TBNA) is a minimally invasive modality to evaluatethoracic malignancies and mediastinal lymph nodes. The utility of EBUS-TBNA in the diagnosis and subtyping lymphomas is not as well defined.Our aim was to study the utility of EBUS-TBNA in the diagnosis andmanagement of lymphoproliferative disorders.Materials and Methods: A retrospective review of all EBUS-TBNAsprocured at our institution over a six-year period (2007 to 2013) wasperformed to find cases with a lymphoproliferative disorder. The adequacy,cytological diagnosis, histological follow-up and available ancillary studieswere reviewed.Results: A total of 766 EBUS FNA specimens were obtained from 462patients with a mean age of 53 years (range 23-90 years). There were 17(4%) patients with a final diagnosis of lymphoma confirmed by histologyand/or ancillary studies. Non-Hodgkin lymphomas (NHL; 11 cases) weremore frequent than Hodgkin lymphoma (HL; 5 cases) and post-transplantlymphoproliferative disorder (PTLD; 1 case). [Table 1] A prior history oflymphoma was available in 11 cases (65%). EBUS-TBNA was diagnosticfor lymphoma in 10 (58%) of these cases, indeterminate in 3 (18%),unsatisfactory in 3 (18%), and negative in one (6%). Histological follow-upwas available in 8 (47%) cases. Confirmatory ancillary study results(immunostains, flow cytometry or FISH) were available in 6 (35%) cases.The sensitivity was 91% in adequate specimens.Conclusions: Lymphoproliferative disorders at our institution areuncommonly encountered in EBUS-TBNA, but pose a diagnosticchallenge due to the high incidence of suboptimal or unsatisfactoryspecimens, particularly in large cell lymphomas. However, adequatespecimens have a high sensitivity and low false negative rate forlymphoproliferative disorders in the setting of on-site evaluation anduse of ancillary studies.