enodmetrial carcinoma: special & not so special …
TRANSCRIPT
Pacific Northwest Society of Pathologists Vancouver, B.C.
September 26, 2015
Teri A. Longacre, M.D. [email protected]
Stanford University, Stanford, CA
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL
VARIANTS
Disclosure of Relevant Financial Relationships
ASCP requires that anyone in a position to influence or control the content of all CME activities disclose any relevant relationship(s) which they or their spouse/partner have, or have had within the past 12 months with a commercial interest(s) [or the products or services of a commercial interest] that relate to the content of this educational activity and create a conflict of interest. Complete disclosure information is maintained in the ASCP office and has been reviewed by the CME Advisory Committee.
Teri Longacre declares no conflict(s) of interest to disclose.
Special Variants: When Does It Matter?
• Serous carcinoma • Clear cell carcinoma • Locational issues (endocervix vs
endometrium): mucinous • Unusual transformation (trophoblast,
yolk sac) • Squamous cell carcinoma • Neuroendocrine carcinoma
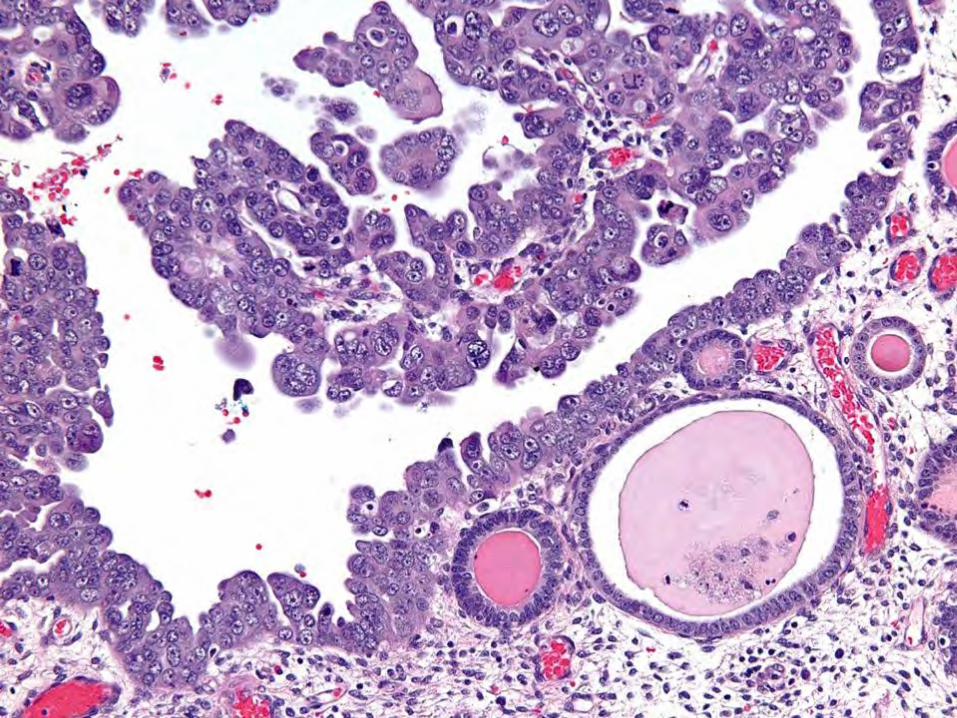
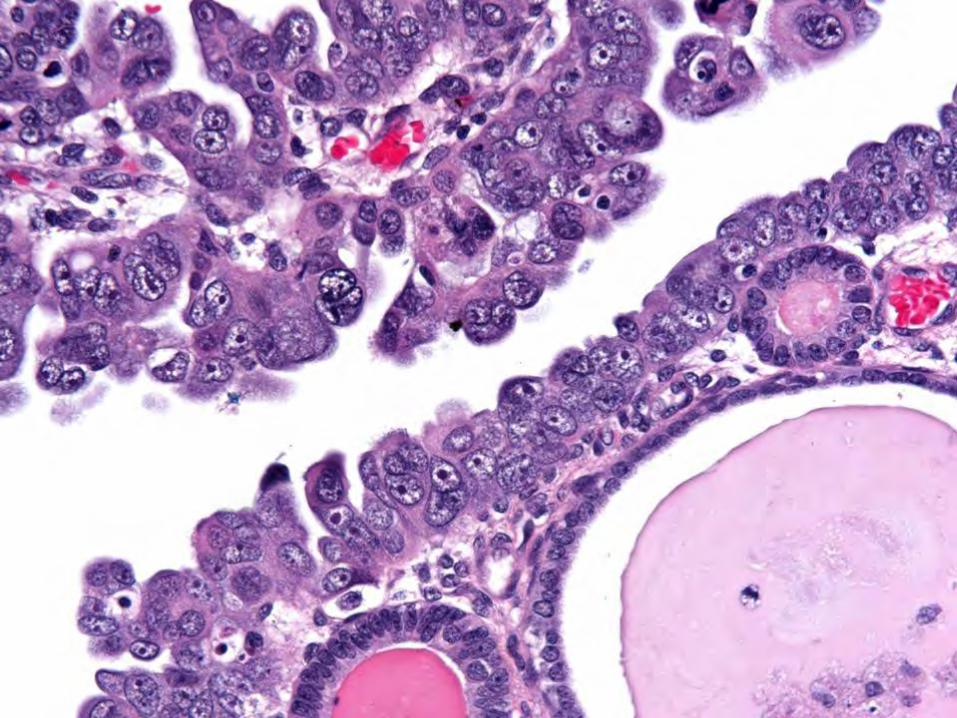
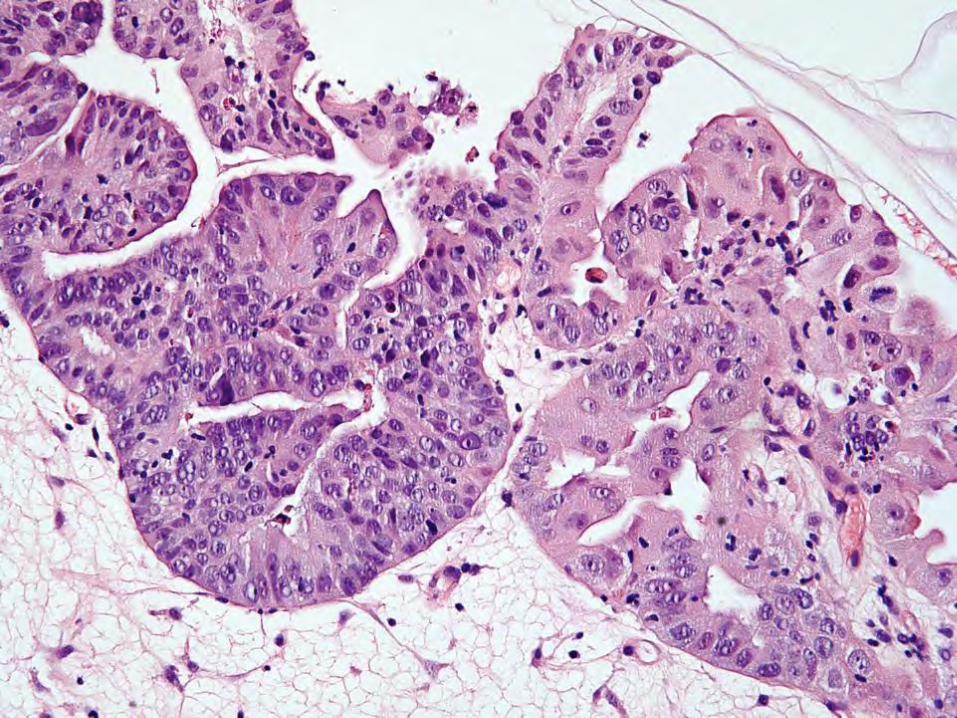
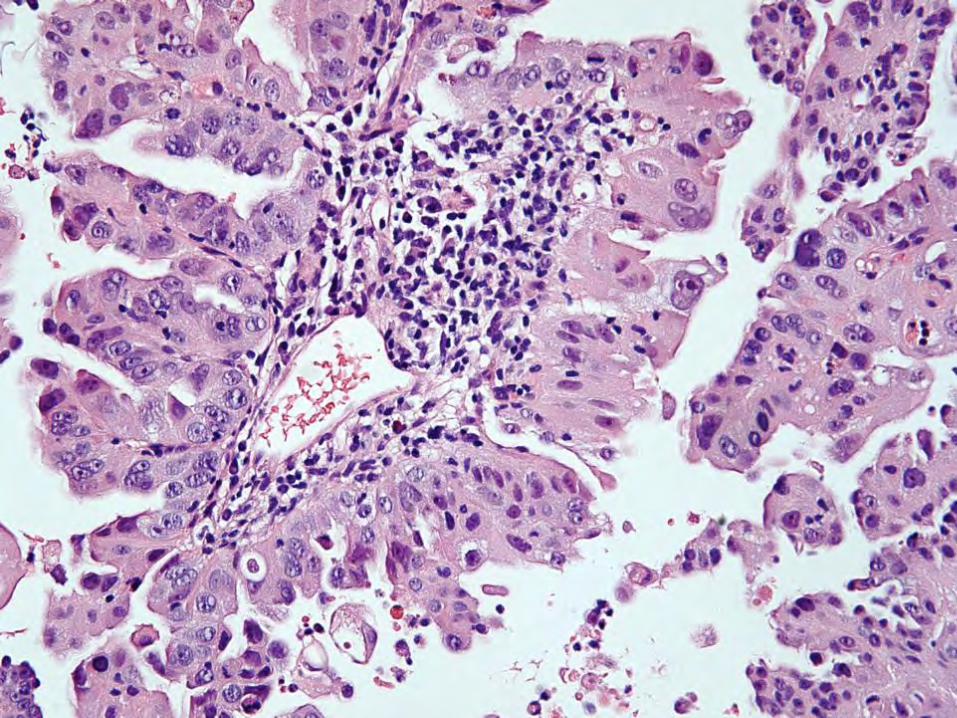
Serous Cancer
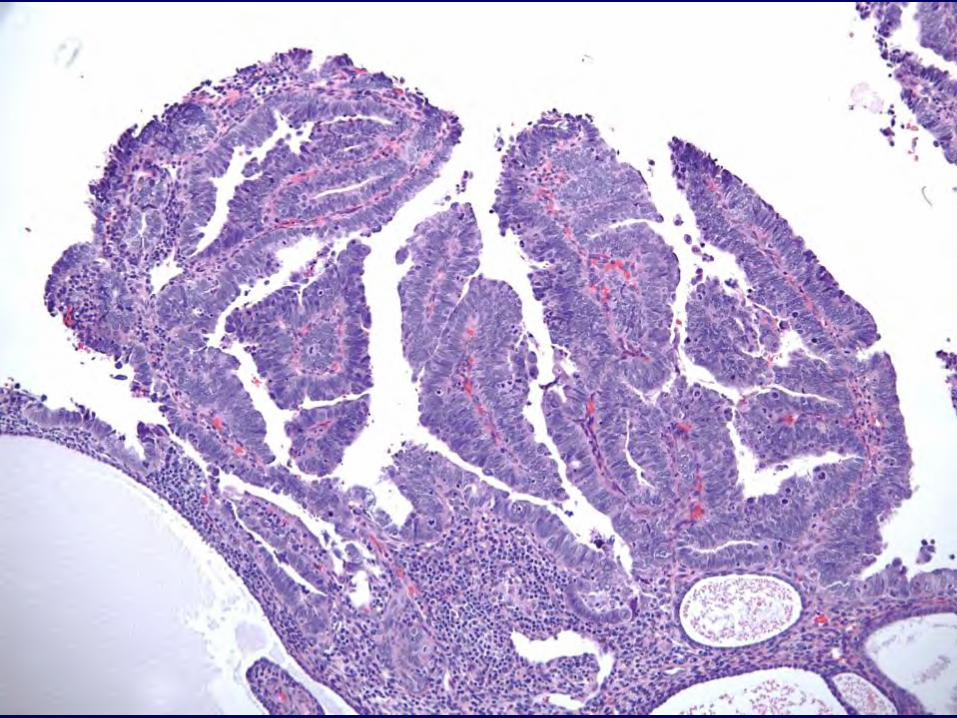
Uterine Serous Carcinoma • Type II cancer – High grade! • Mean age decade older than usual
adenocarcinoma • No background hyperplasia - traditionally • Uterus may not be enlarged; “scanty”
sampling • May be minimally invasive with widespread
disease
S08-23452 03
S08-23452 04
S08-23452 08
S08-23452 09
S08-23452 10
S08-23452 11
S08-23452 07
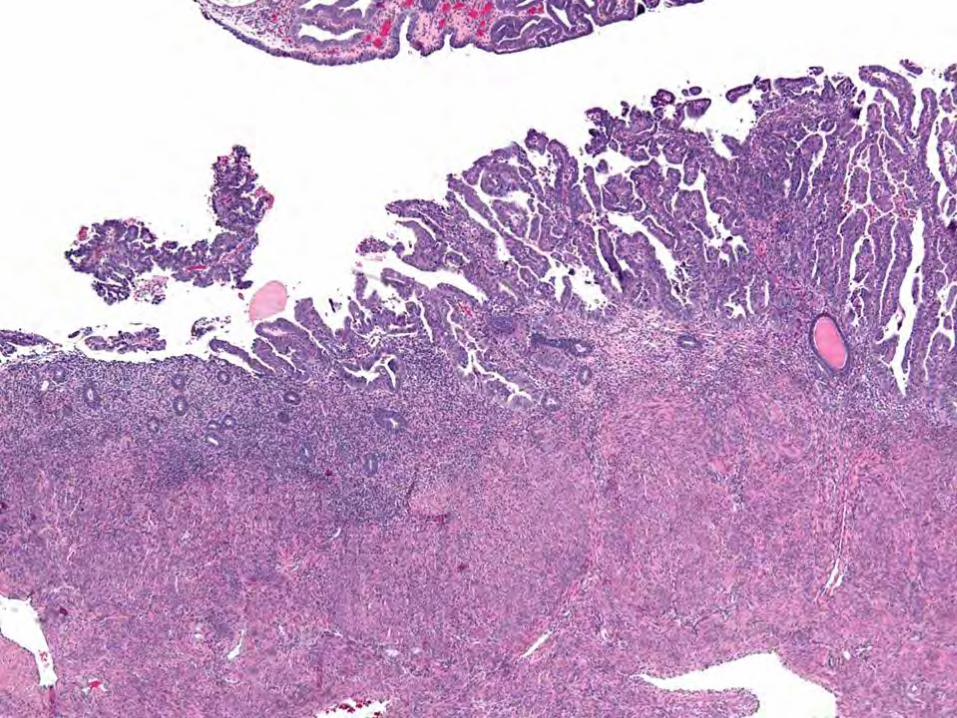
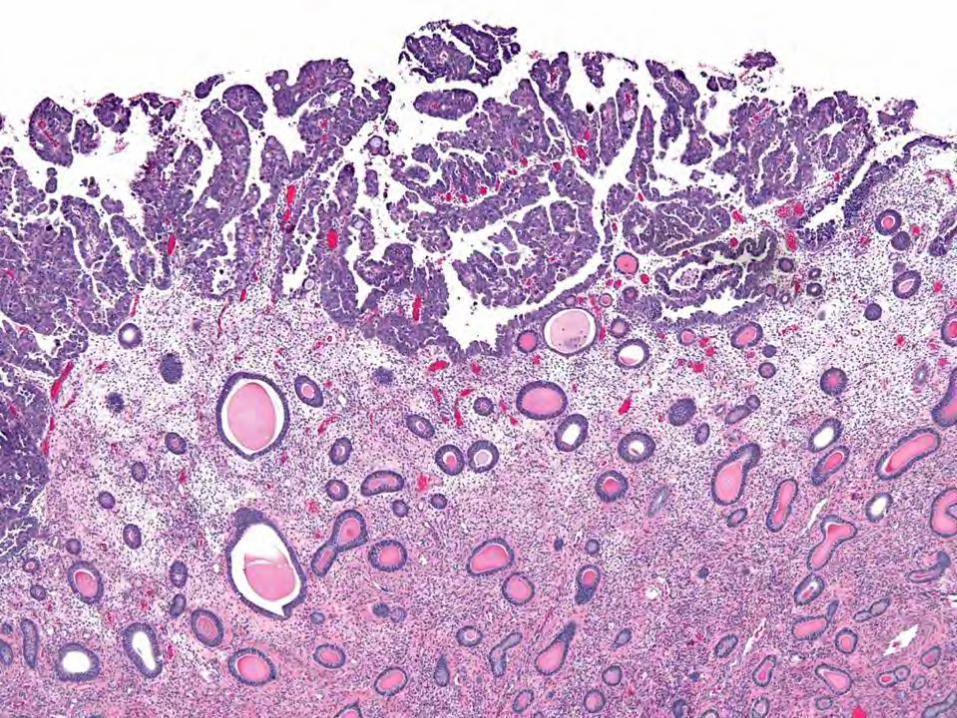
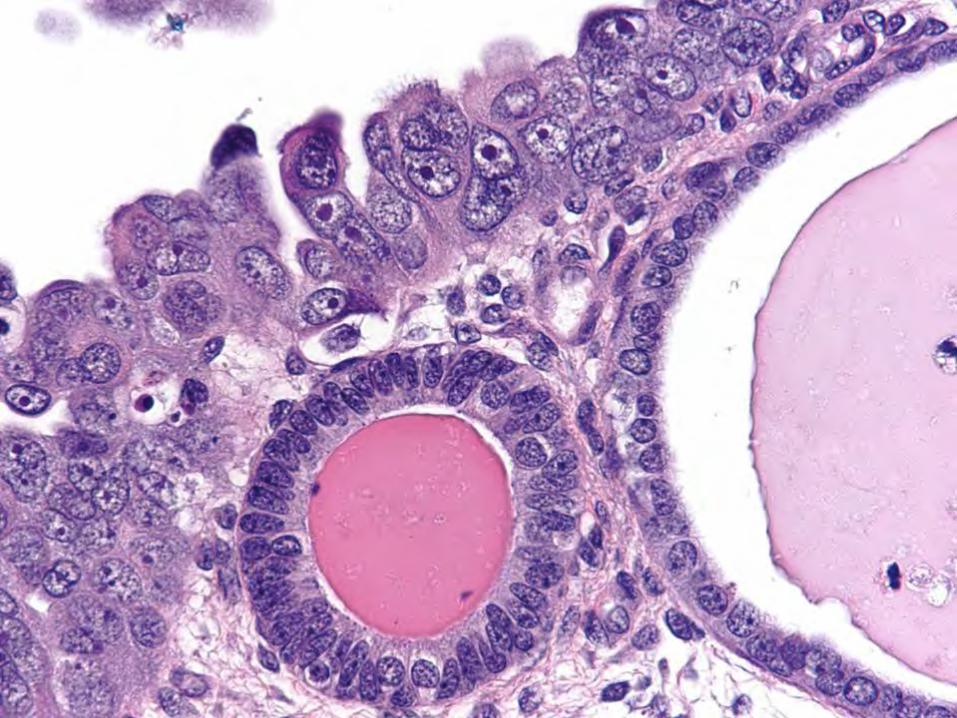
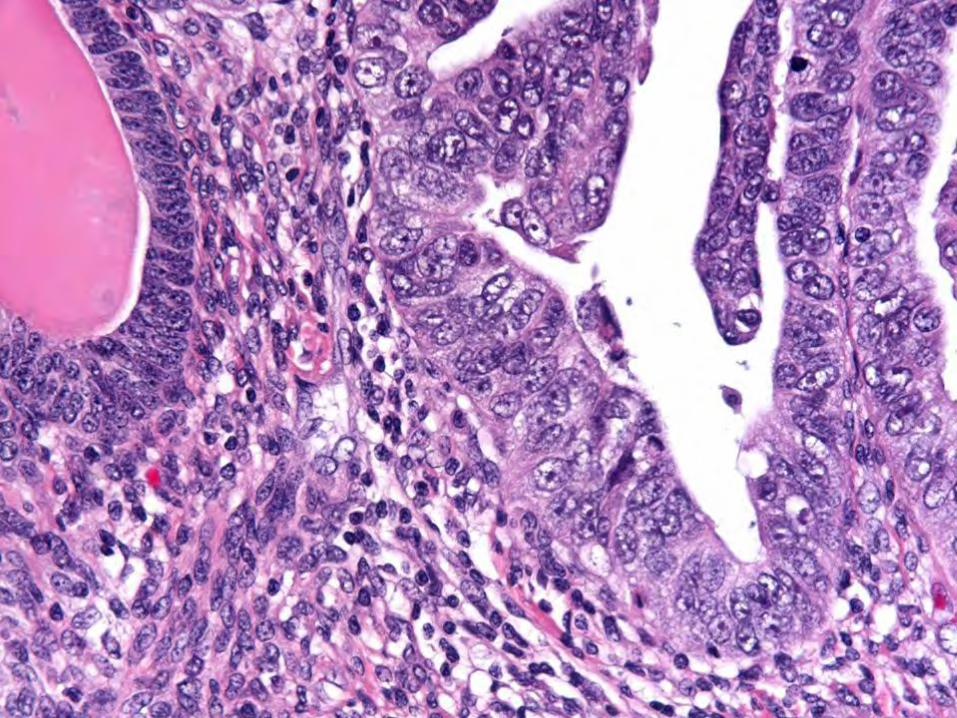
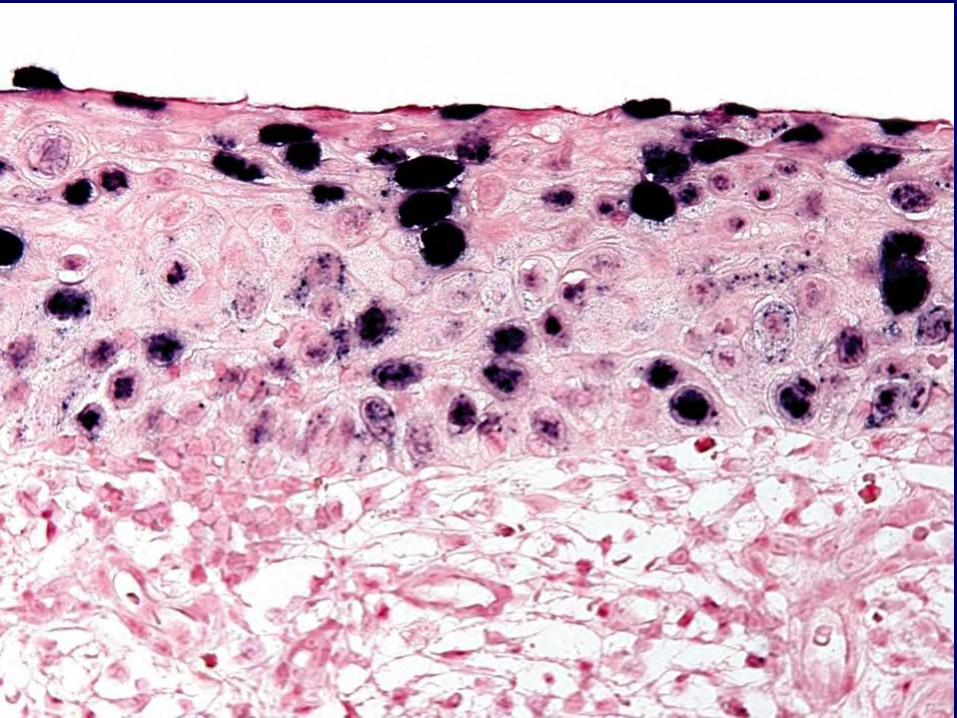
Serous Endometrial Intraepithelial Carcinoma (SEIC): “Non-invasive” Serous Carcinoma
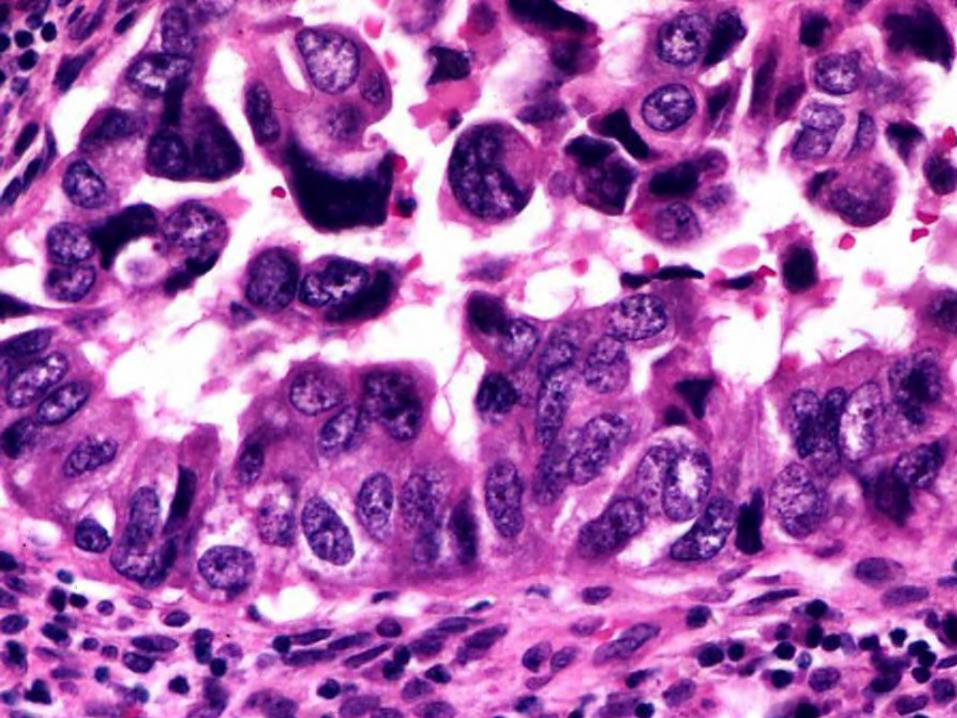
• Typically elderly woman • Normal endometrial (often atrophic)
glandular structure is preserved • Lining cells exhibit marked nuclear atypia,
enlargement, and hyperchromasia • Strong nuclear p53 overexpression • Assoc w/ high grade serous-type disease
elsewhere – often peritoneal Am J Surg Pathol 2000;24:726-732

MICRO: EIN
Serous Cancer
• P53-positive (every single cell or null pattern)
• P16-positive • WT1-negative (mostly) • ER-positive/negative • PR-positive/negative • HER2-positive (subset)
High Single Copy Number Abnormalities
• TP53
• MYC
• ERBB2
• CCNE1
• FGFR3
• SOX17
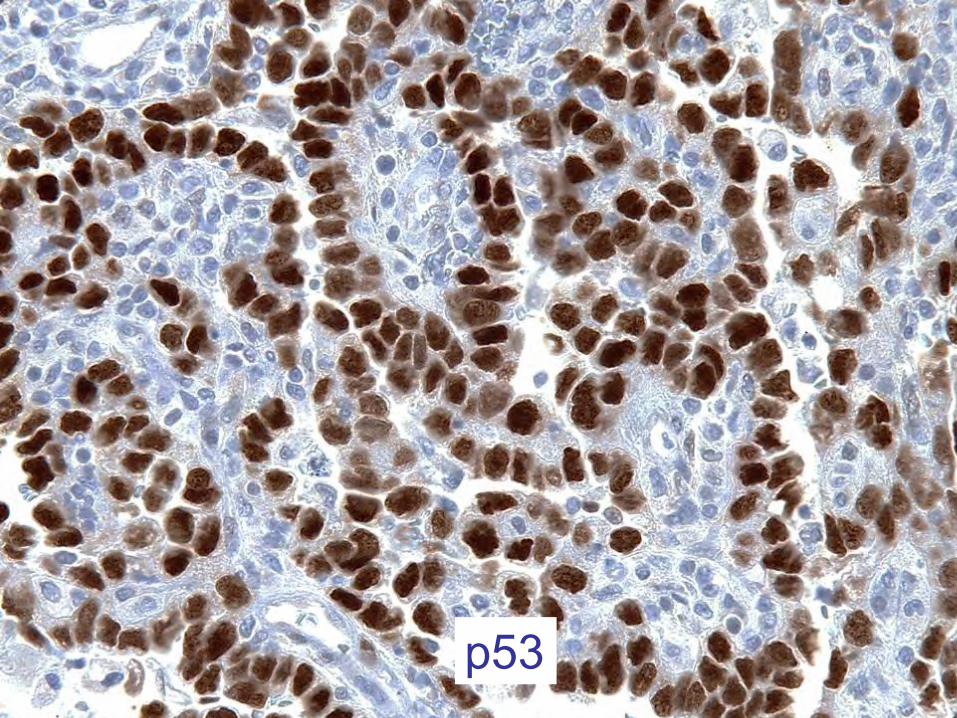
p53
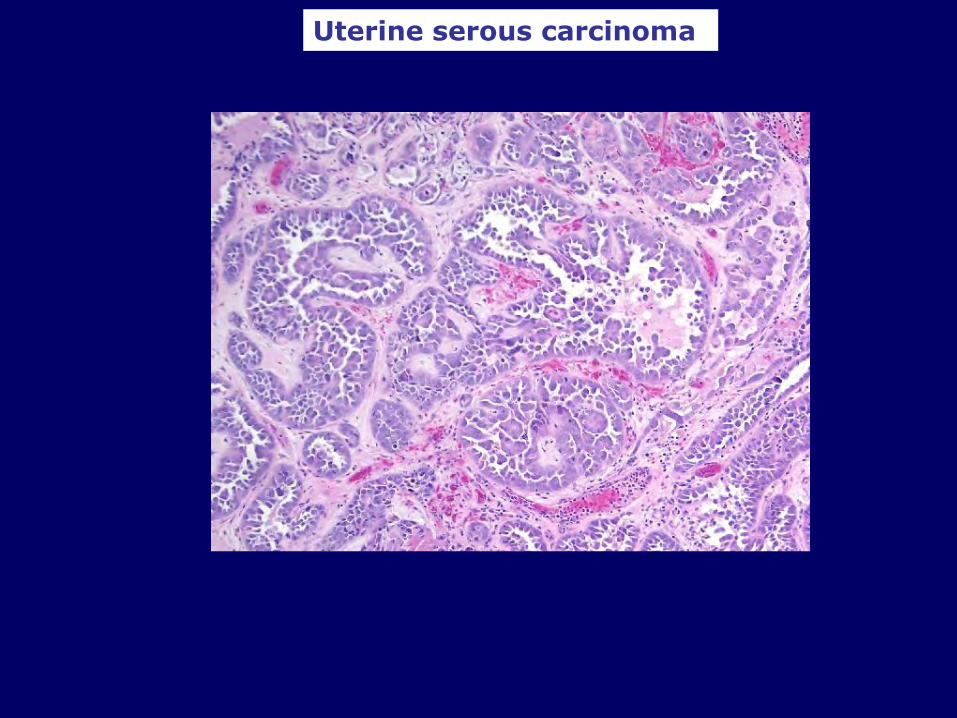
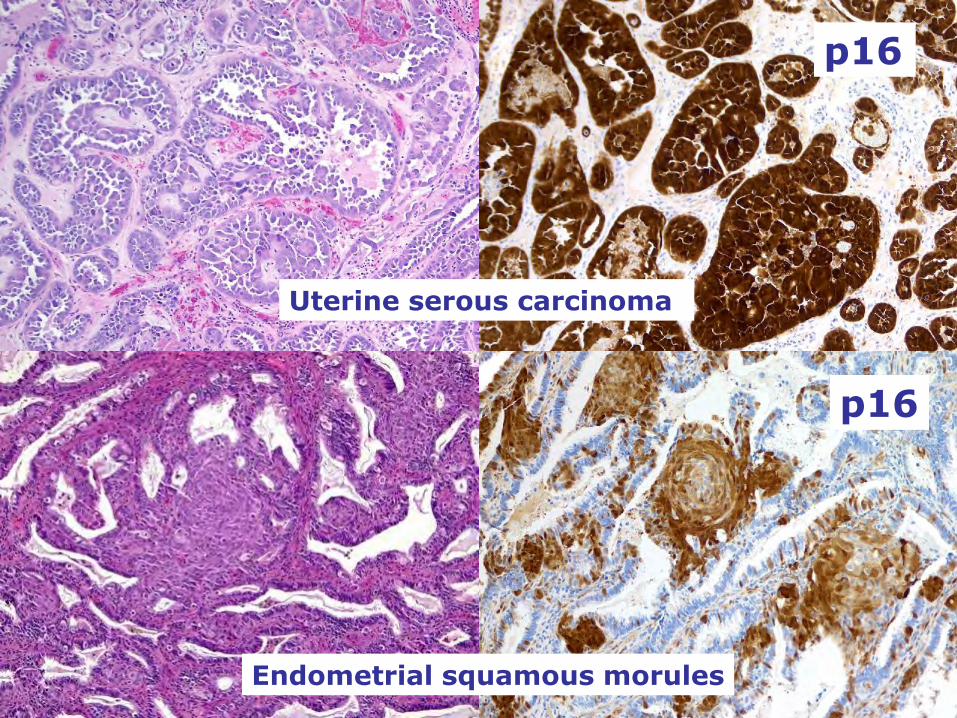
Uterine serous carcinoma
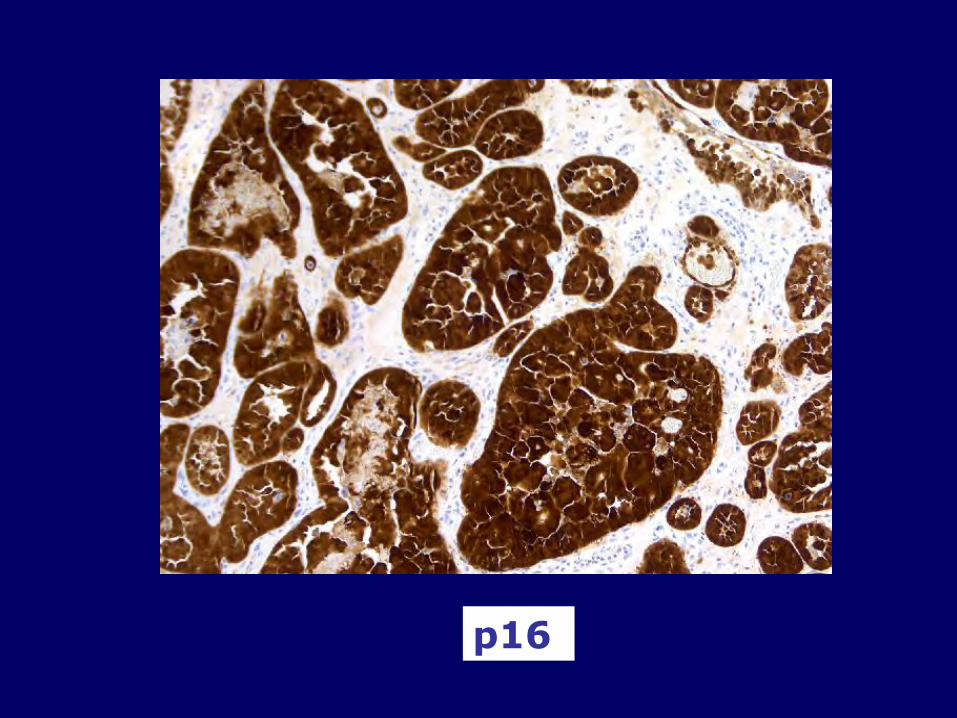
p16
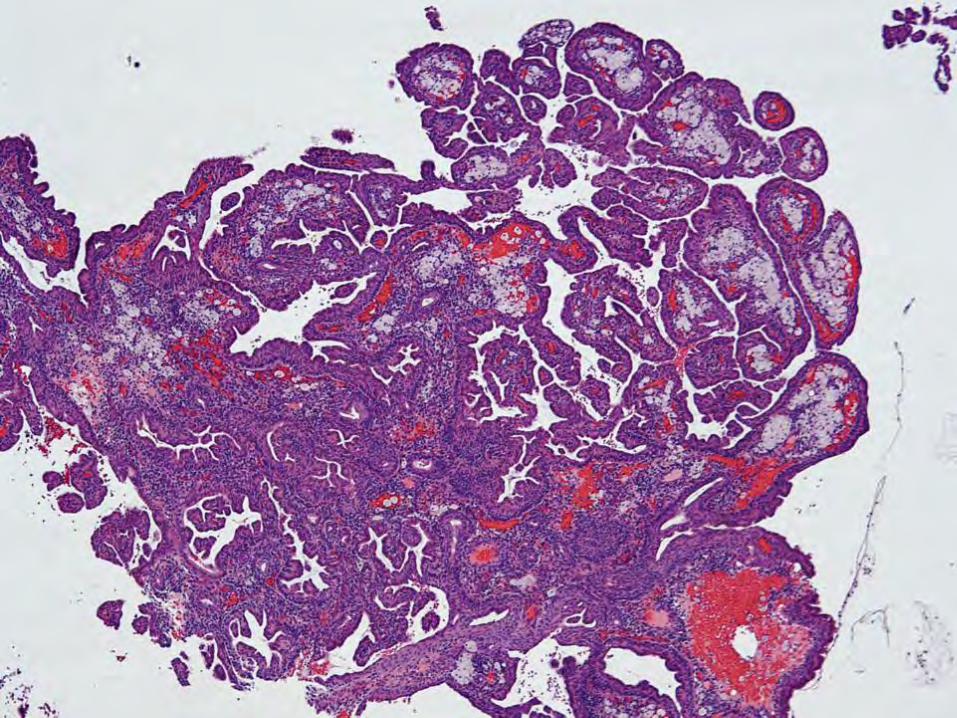
Serous Carcinoma Mimics: The Good, The Bad and The Ugly
• Papillary metaplasia • Syncytial papillary metaplasia • Villoglandular endometrioid • Glandular serous vs endometrioid with
grade 3 nuclei • Serous carcinoma from elsewhere in the
genital tract

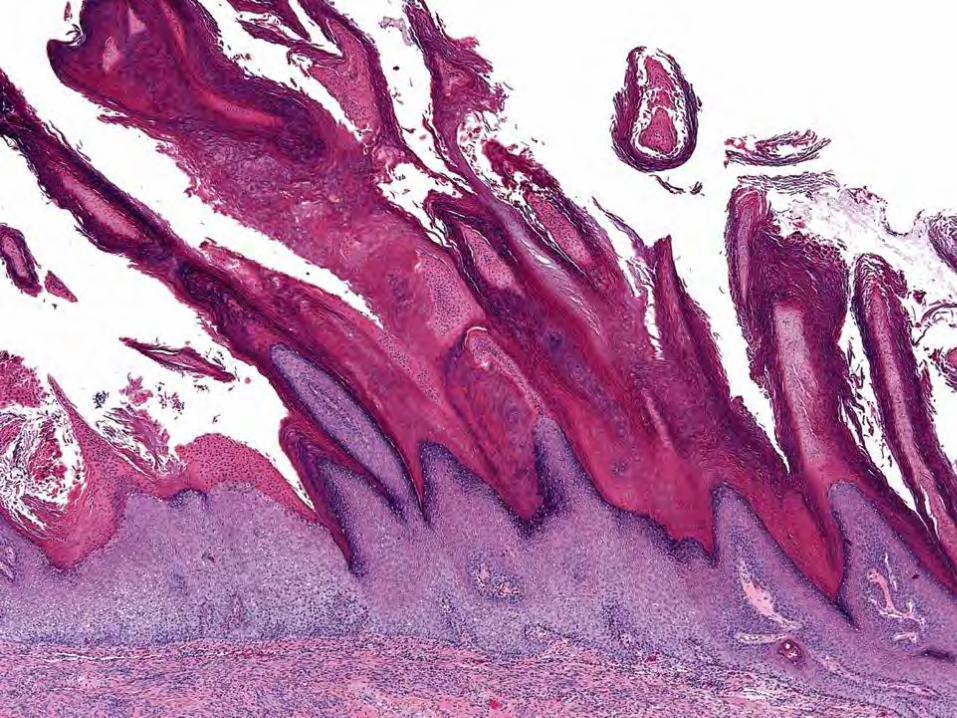
Simple Papillary Proliferations • Atrophic, weakly proliferative, or
proliferative cells without atypia lining coarse connective tissue papillary cores
• Spectrum of metaplastic changes • Frequently focal, in endometrial polyps in
atrophic endometria • “Benign papillary hyperplasia/proliferation”
Am J Surg Pathol 2013;37:167-77
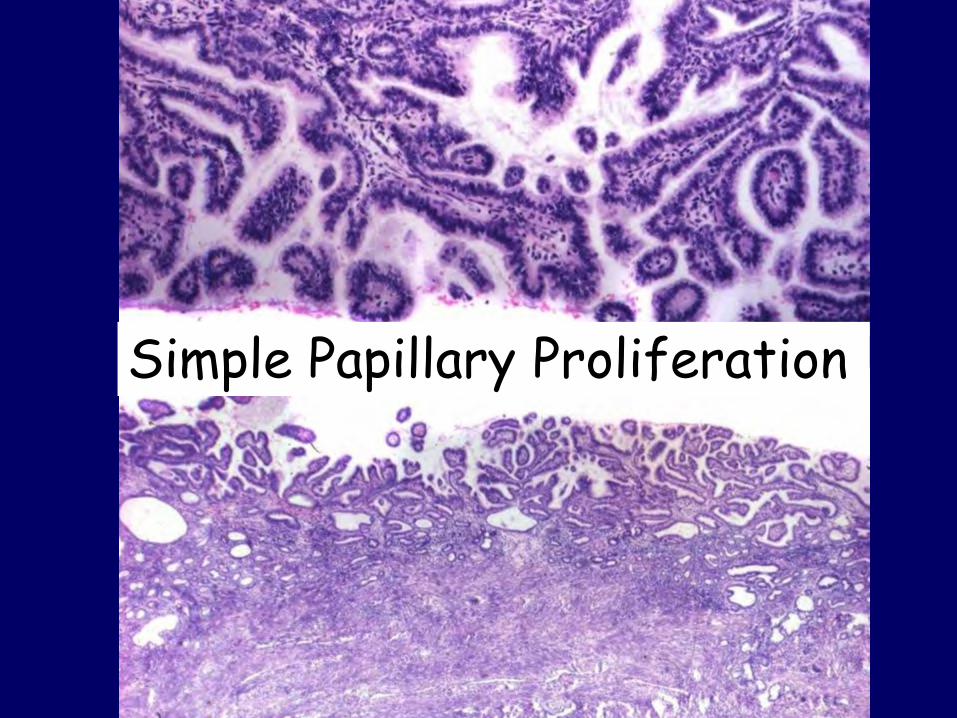
Simple Papillary Proliferation
Complex Papillary Proliferations
• May be associated with concurrent or subsequent endometrial hyperplasia and carcinoma
• Analogous to atypical hyperplasia (even in the absence of significant cytological atypia)
• “Complex papillary hyperplasia/proliferation"
Am J Surg Pathol 2013;37:167-77
p53
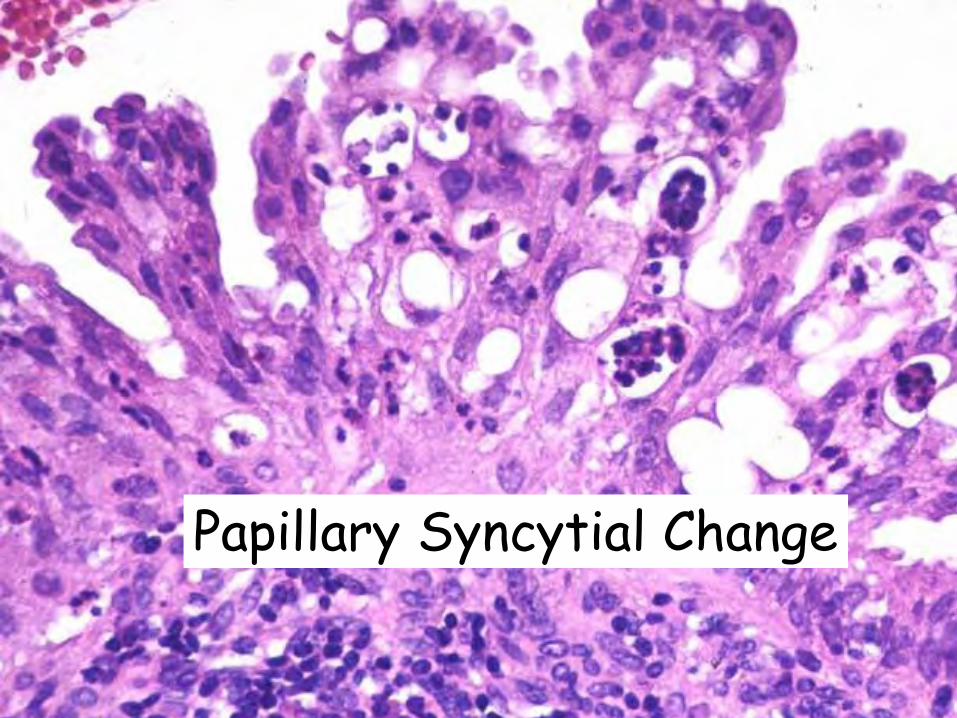
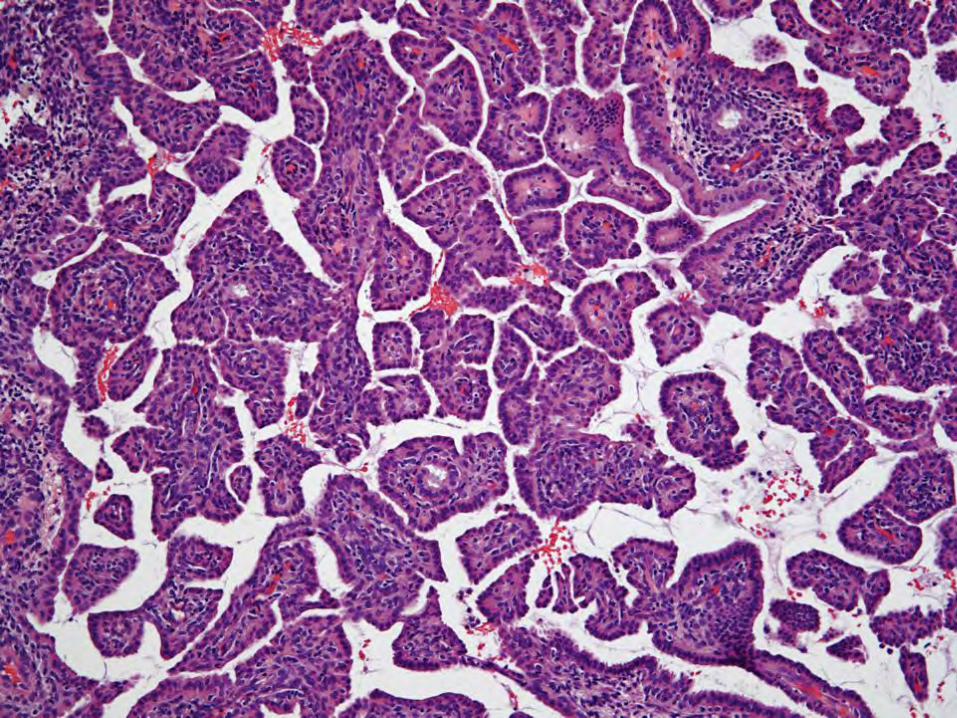
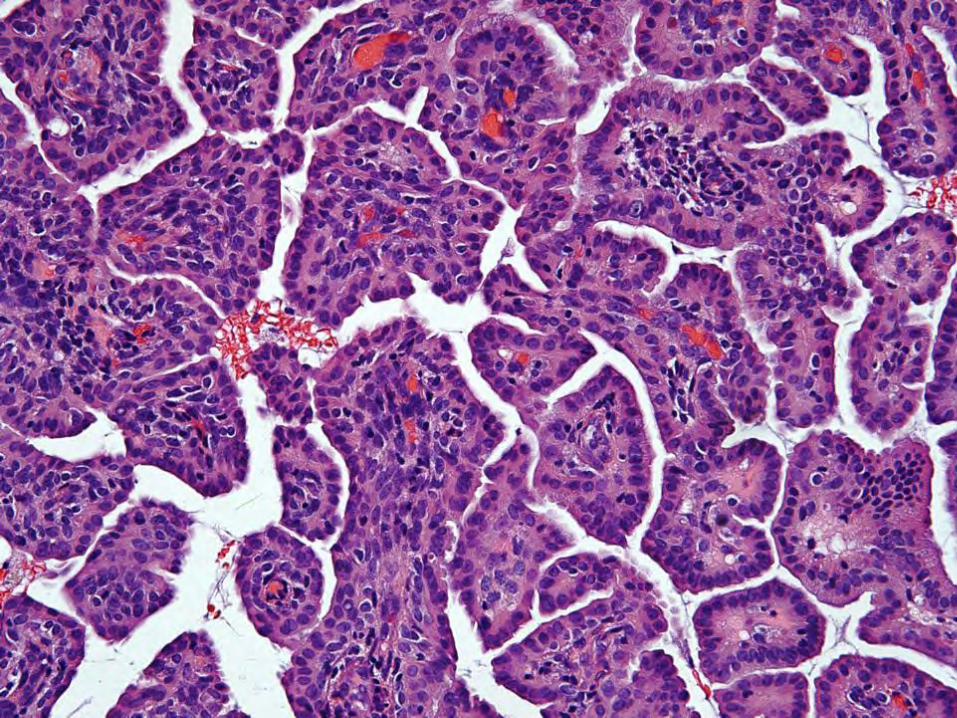
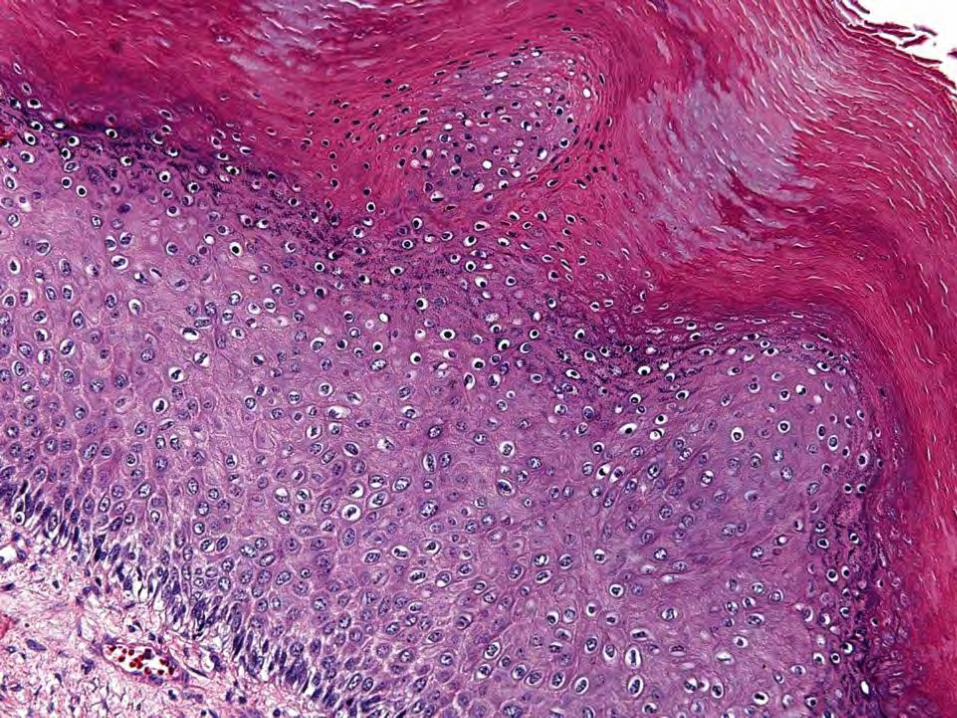
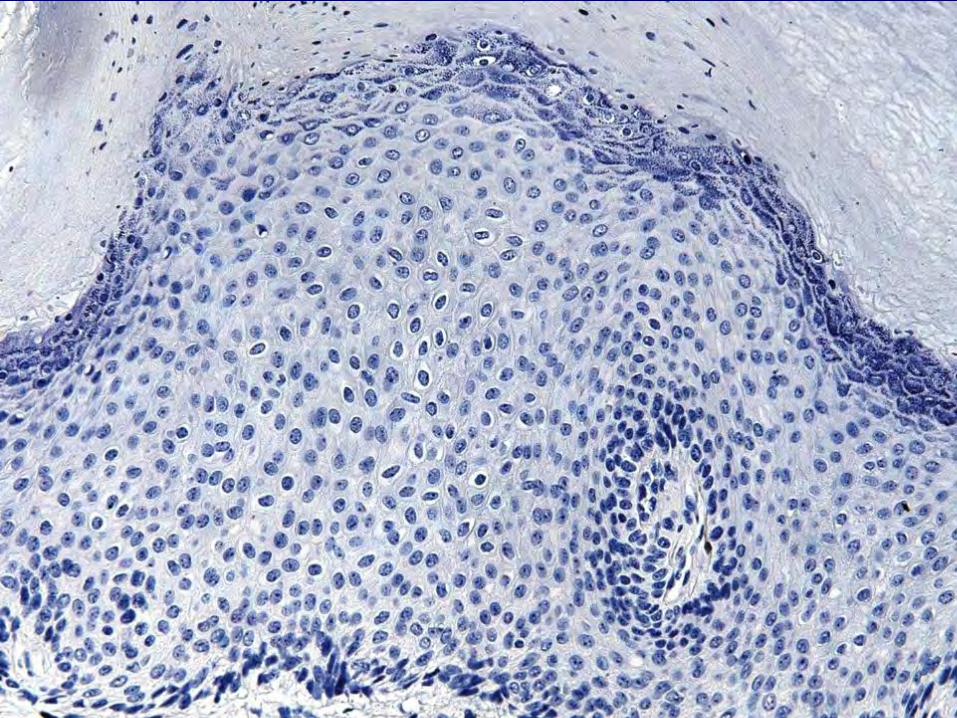
MICRO: Papillary syncytial metaplasia
Papillary Syncytial Change
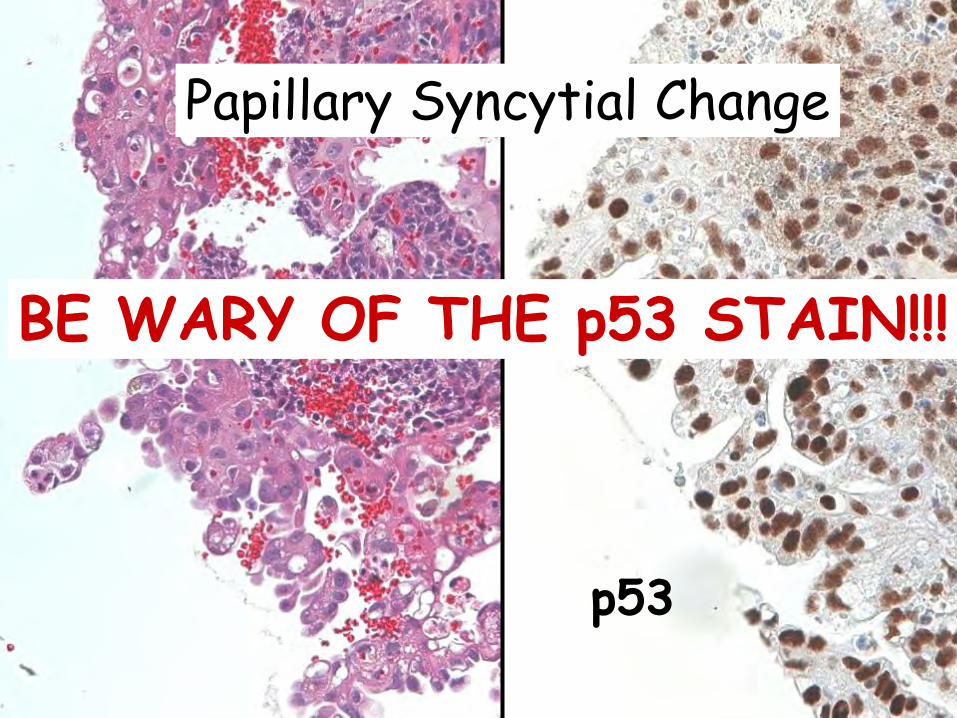
Papillary Syncytial Change
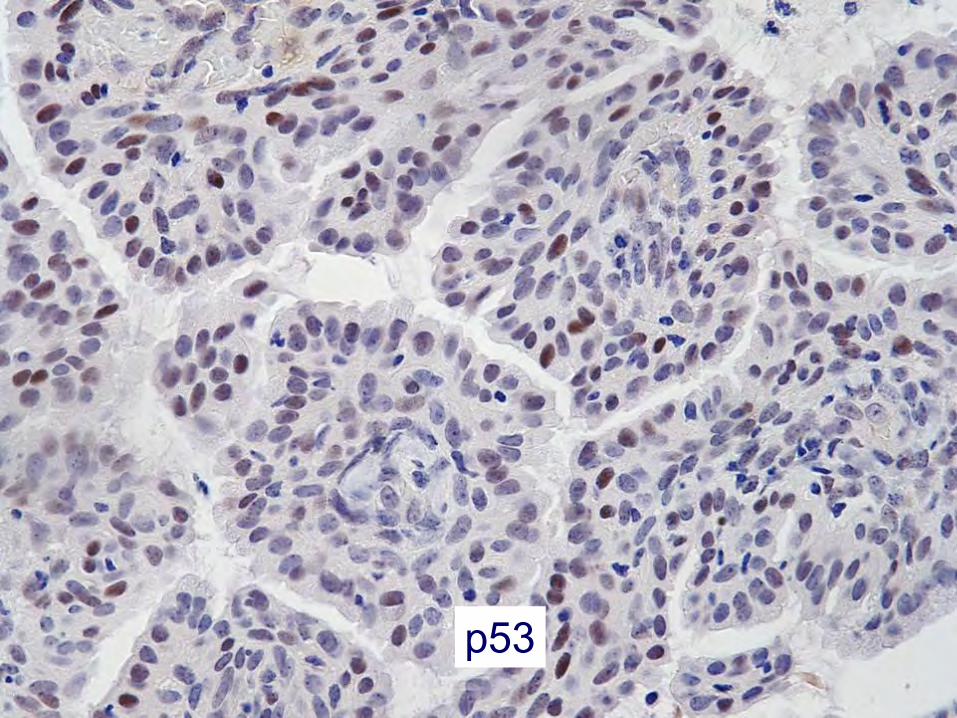
p53
BE WARY OF THE p53 STAIN!!!
Papillary Syncytial Change (Metaplasia)
• Decreased expression of ER • Increased expression of p53 (although still
wild-type staining) and p16, the latter marker typically being diffusely positive
• Low MIB1 proliferation index • In problematic cases, IHC may result in a
misdiagnosis
Int J Gynecol Pathol 2012;31:206-10
Papillary Problems: Strategy • Mixed epithelium argues benignancy • Some degree of cytologic atypia is
permitted in metaplastic papillary lesions (even expected) – but marked nucleomegaly & pleomorphism is not
• Serous carcinoma is a cytologic diagnosis • p53 & p16 should be used with caution
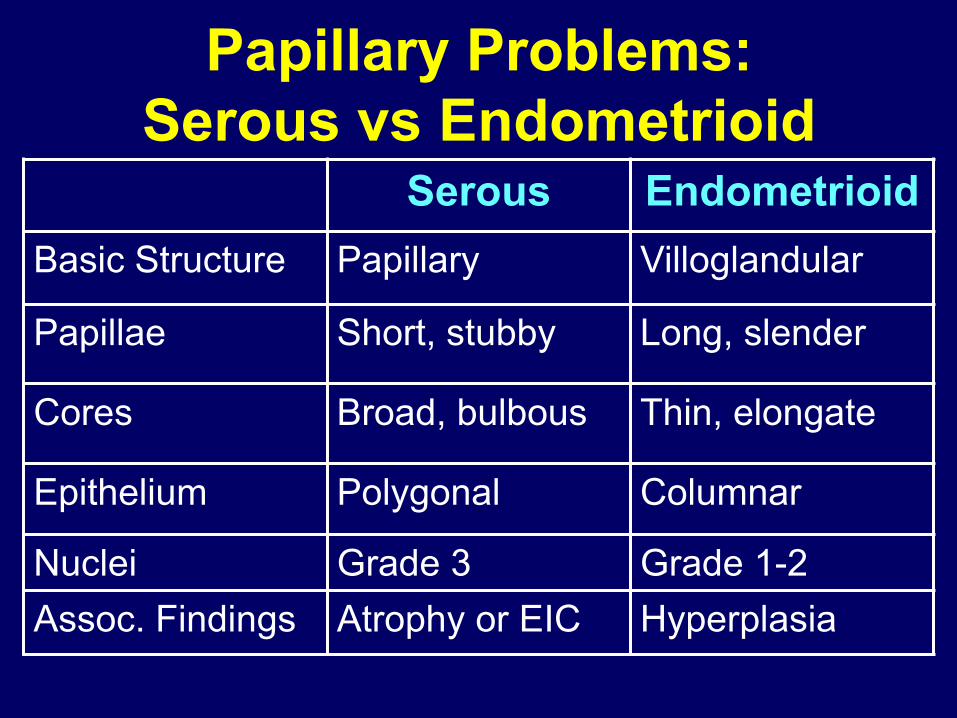
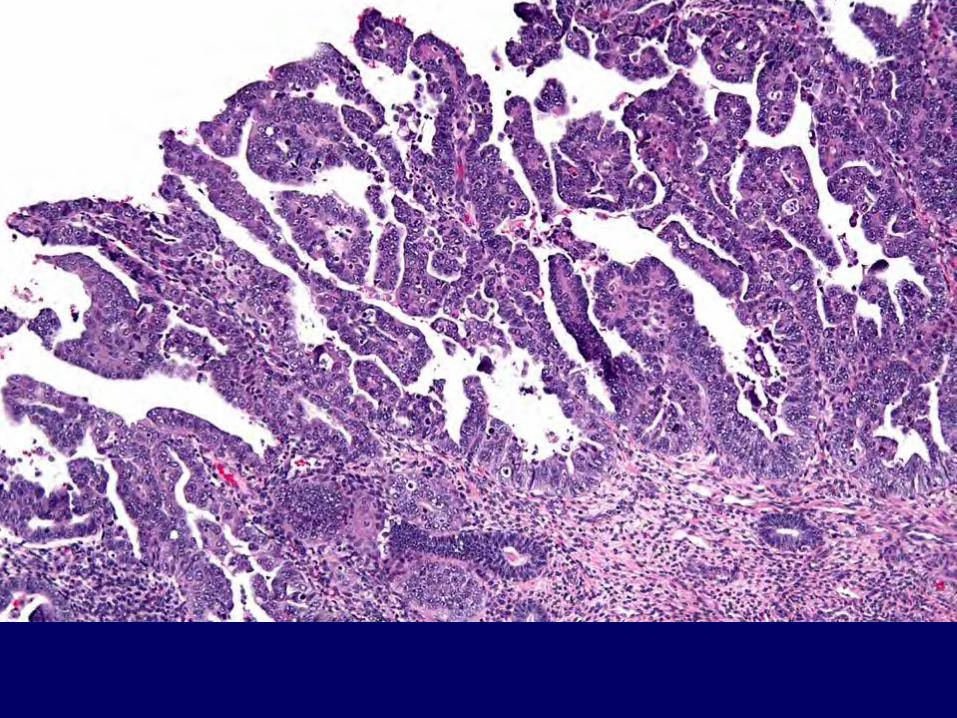
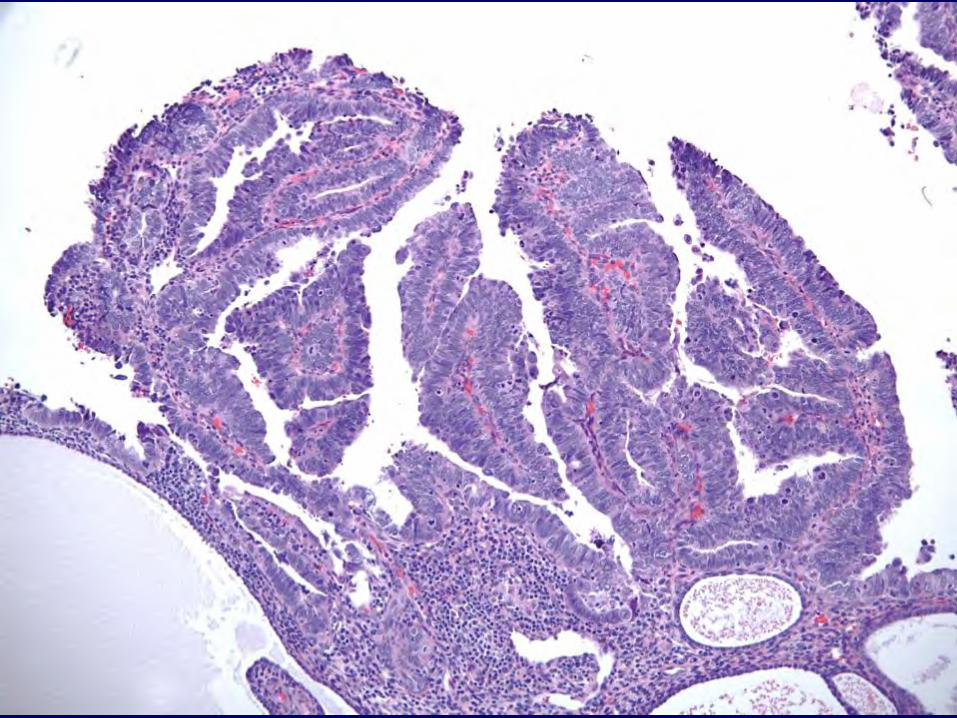
Papillary Problems: Serous vs Endometrioid
Serous Endometrioid Basic Structure Papillary Villoglandular
Papillae Short, stubby Long, slender
Cores Broad, bulbous Thin, elongate
Epithelium Polygonal Columnar
Nuclei Grade 3 Grade 1-2 Assoc. Findings Atrophy or EIC Hyperplasia
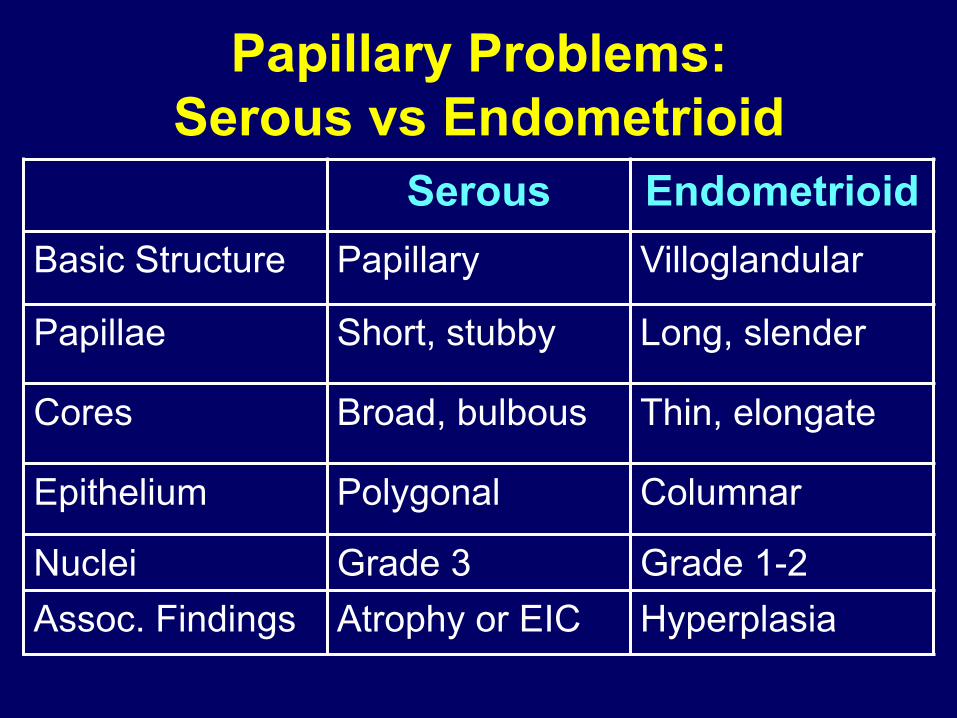
Papillary Problems: Serous vs Endometrioid
Serous Endometrioid Basic Structure Papillary Villoglandular
Papillae Short, stubby Long, slender
Cores Broad, bulbous Thin, elongate
Epithelium Polygonal Columnar
Nuclei Grade 3 Grade 1-2 Assoc. Findings Atrophy or EIC Hyperplasia
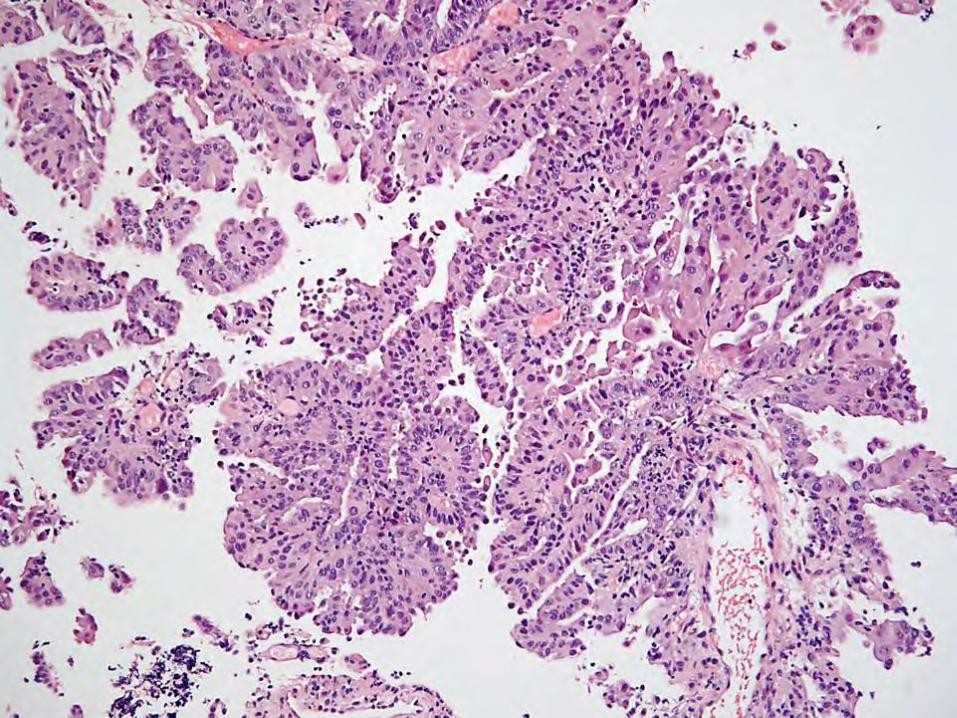
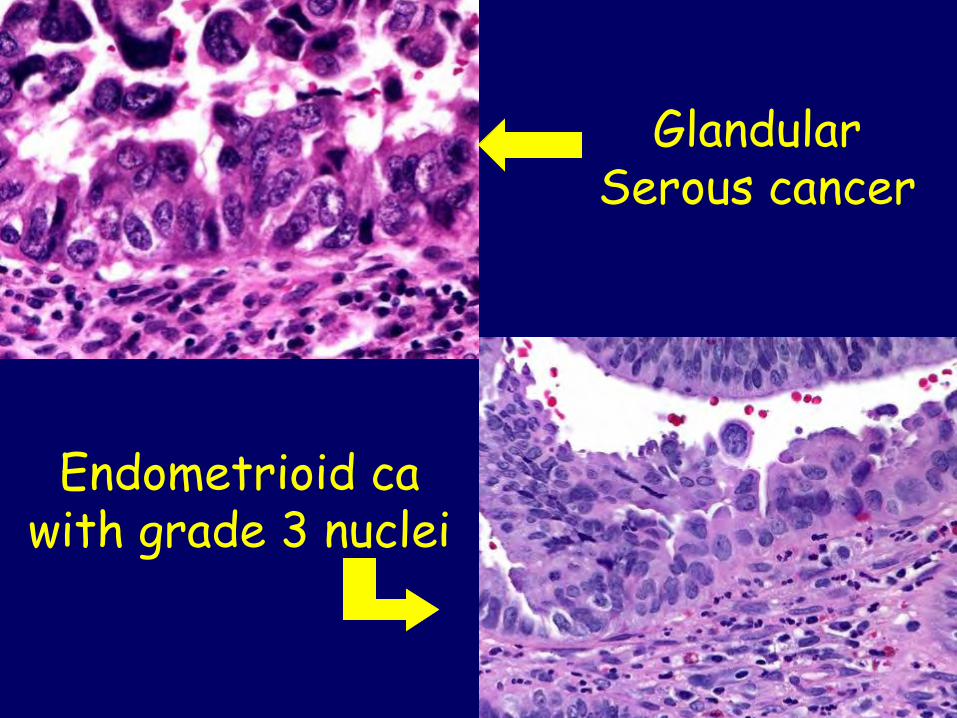
Glandular Serous cancer
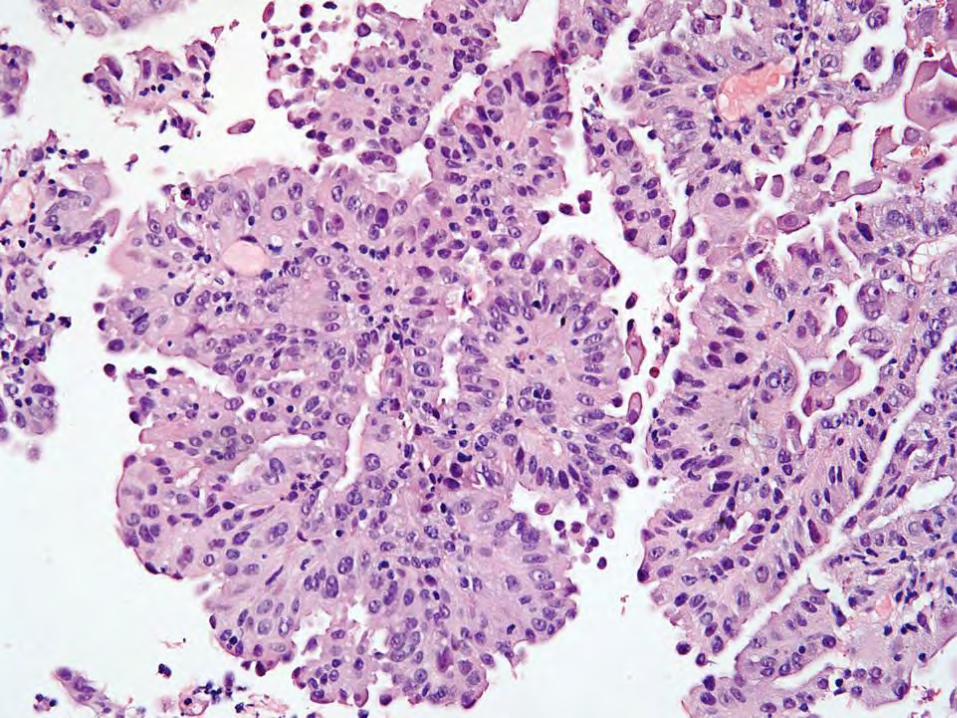
Endometrioid ca with grade 3 nuclei
Serous Carcinoma Staging • What to do with “intraepithelial” serous
carcinoma in endometrium, cervix, fallopian tube, peritoneum?
• Describe distribution of disease • We don’t use the term “EIC” or “minimal
volume serous carcinoma” • Stage according to distribution, but admit
outcome data sparse
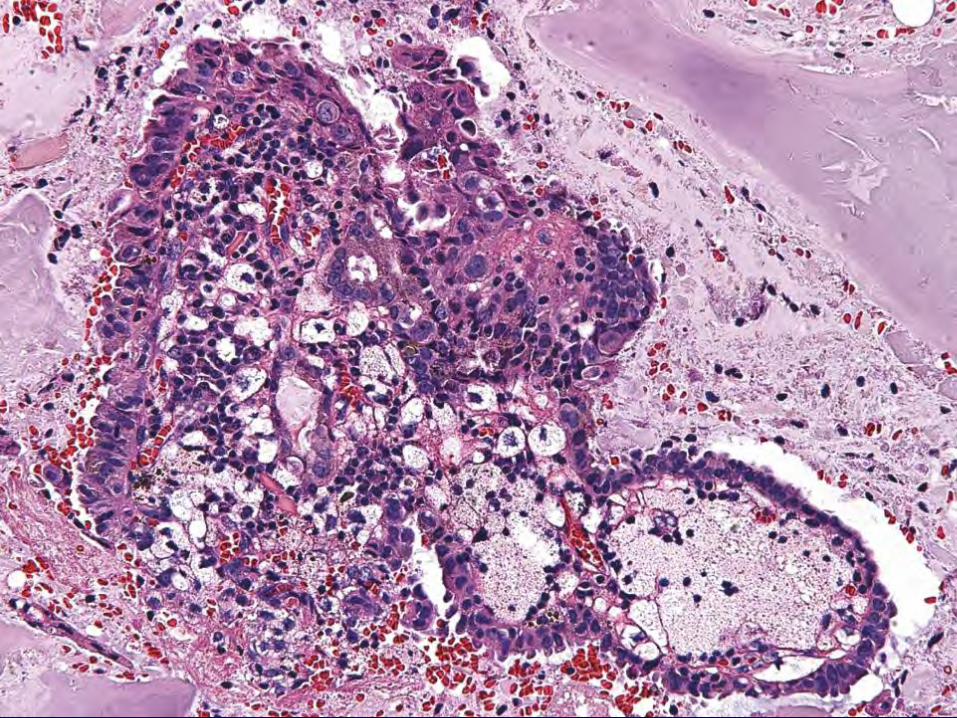
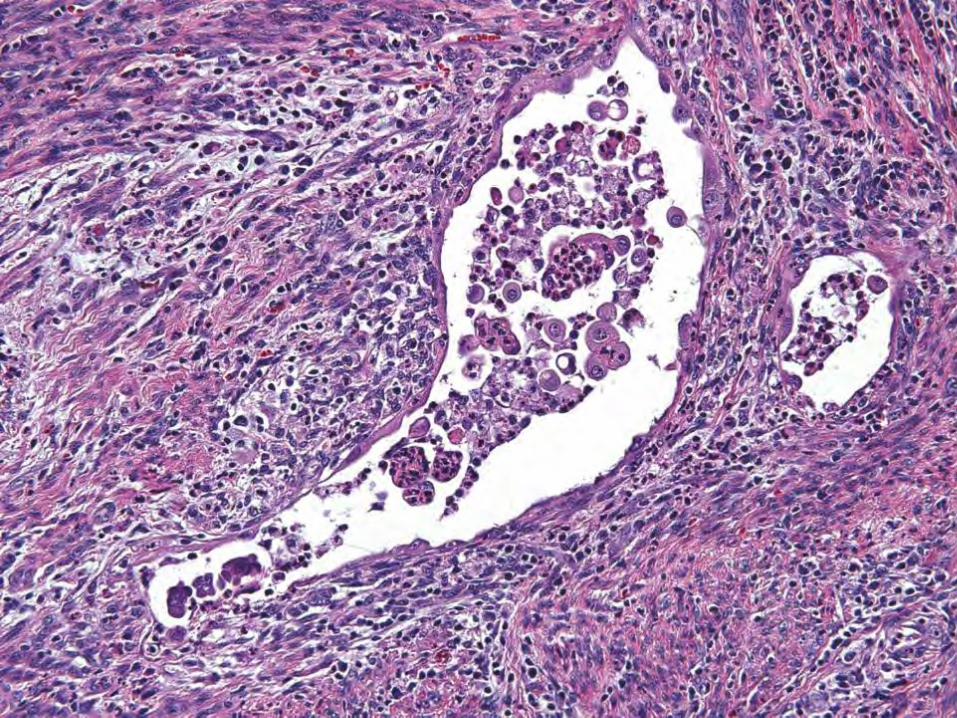
Don’t Forget Carcinosarcoma
• Often misdiagnosed as serous carcinoma • Stromal component may be focal – look
for the cartilage (or bone) • Stromal component may be overlooked as
“reactive” stroma – look for pink hyalin droplets
• May recur as serous cancer, carcinosarcoma or rarely, sarcoma

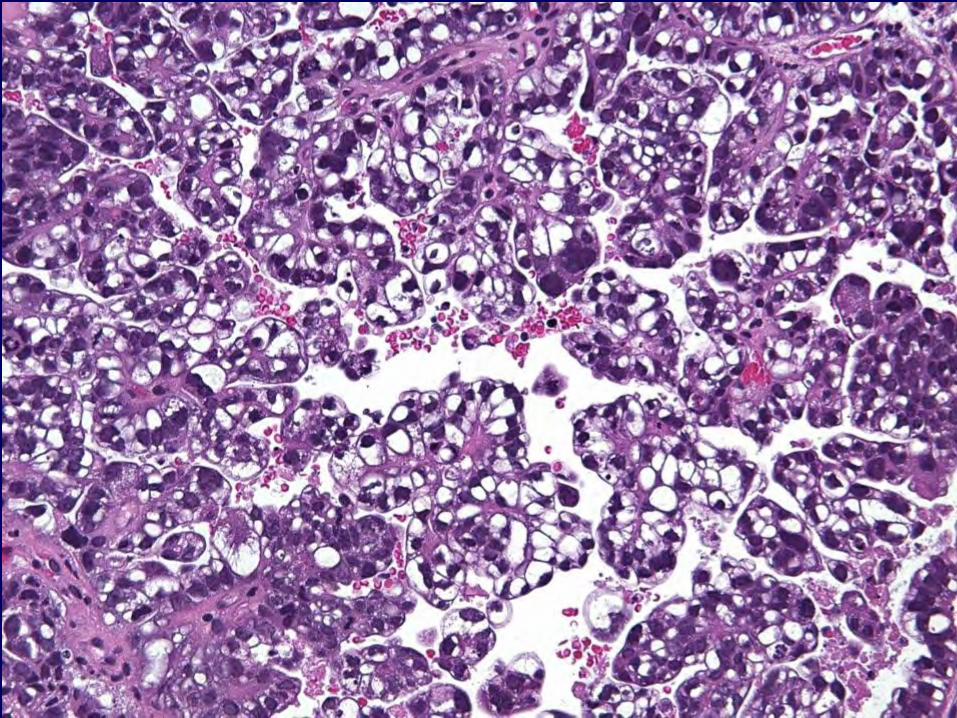
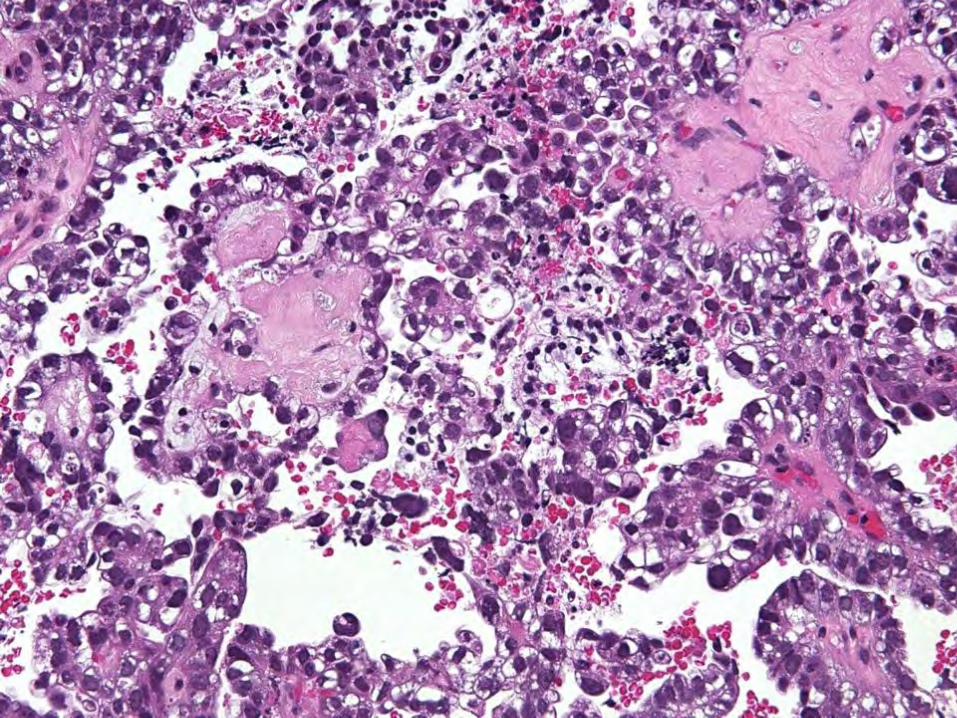
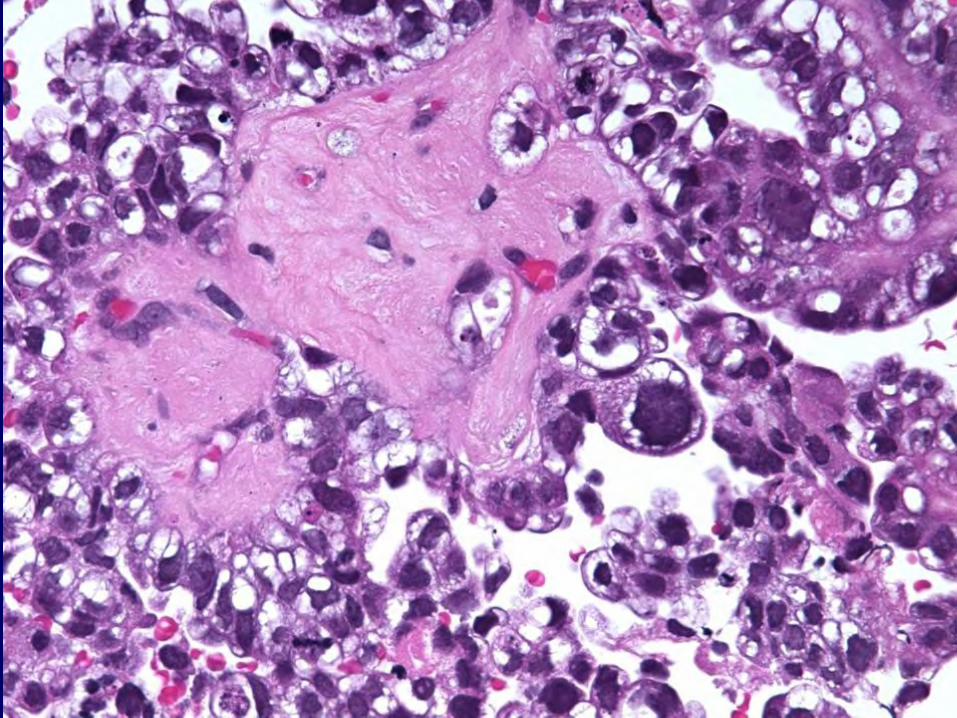
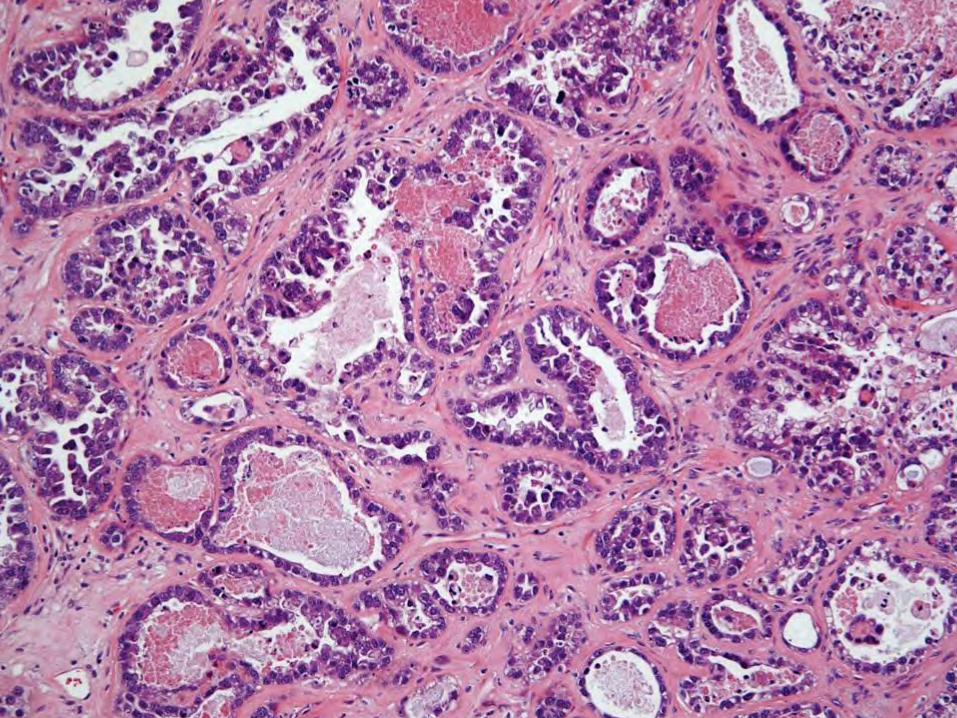
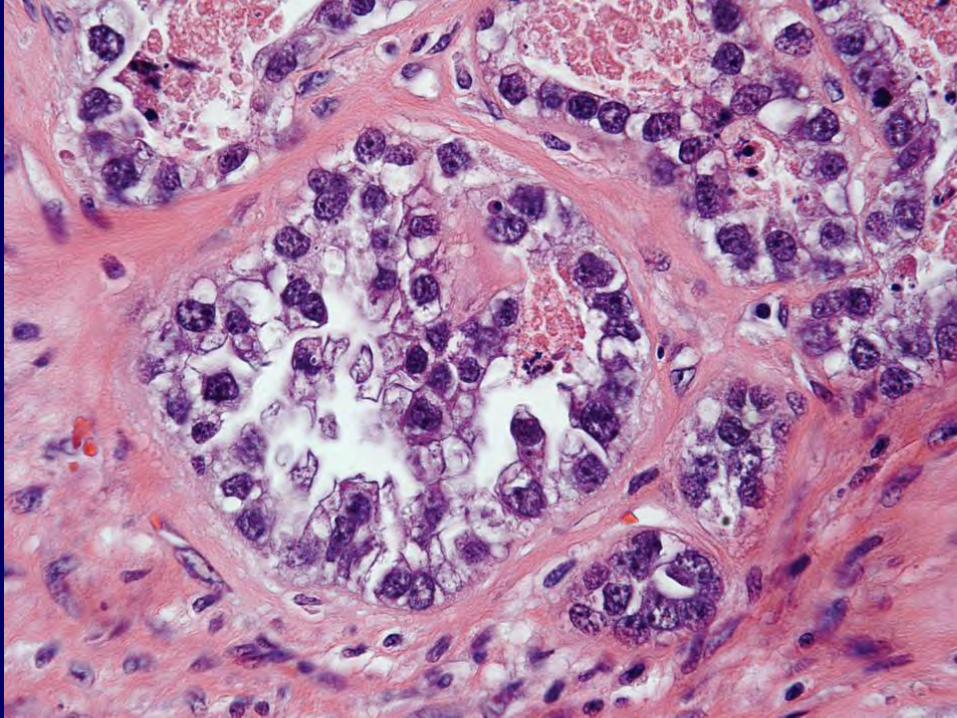
Clear Cell Carcinoma
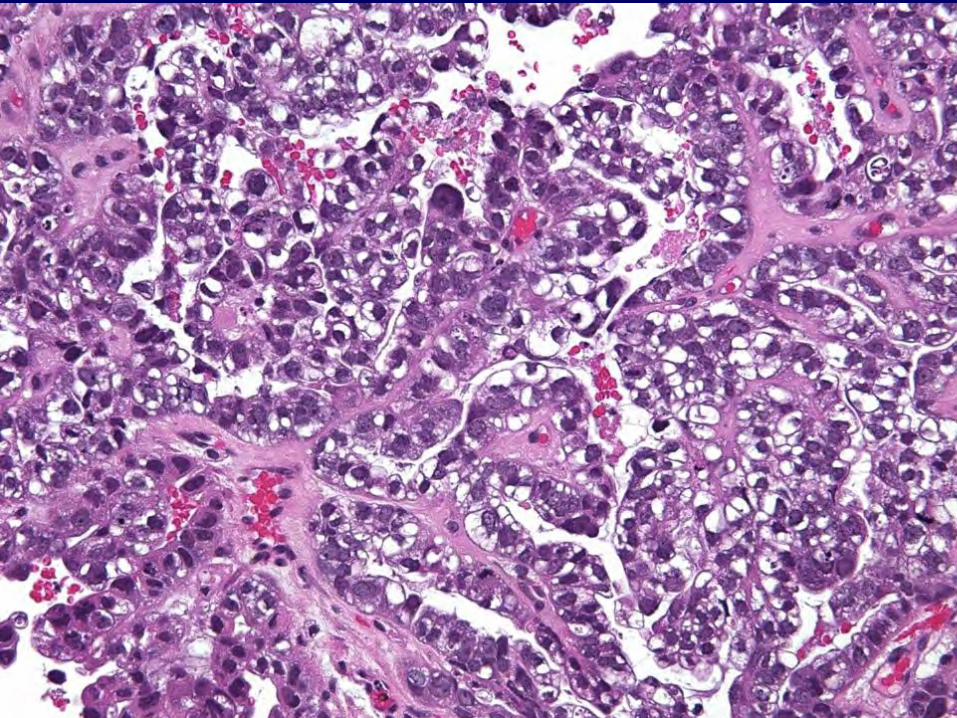
Clear Cell Carcinoma • RARE in uterus, esp. pure variety • Histologically similar to clear cell cancer in
ovary: papillary, tubulocystic, diffuse (solid)
• Clear or eosinophilic cytoplasm • Hobnail cells • Almost a diagnosis of exclusion in the
uterus – High grade!!!

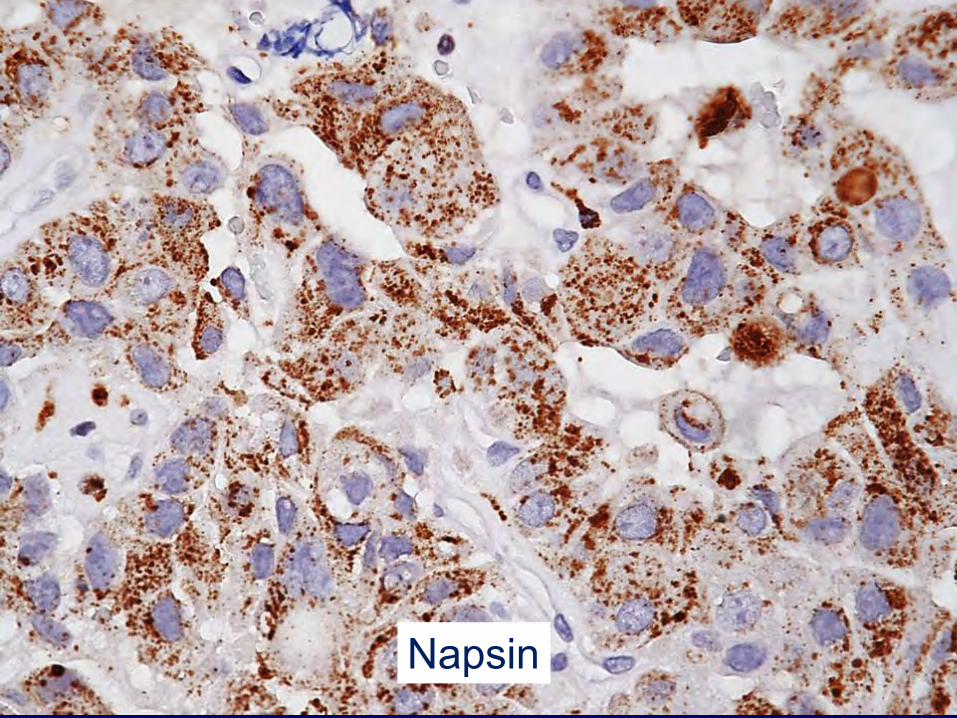
Napsin
Clear Cell Carcinoma • ER-negative • PR-negative • P16-negative • P53-negative • HNF1-beta-positive • Napsin-positive
…but can see variable patterns
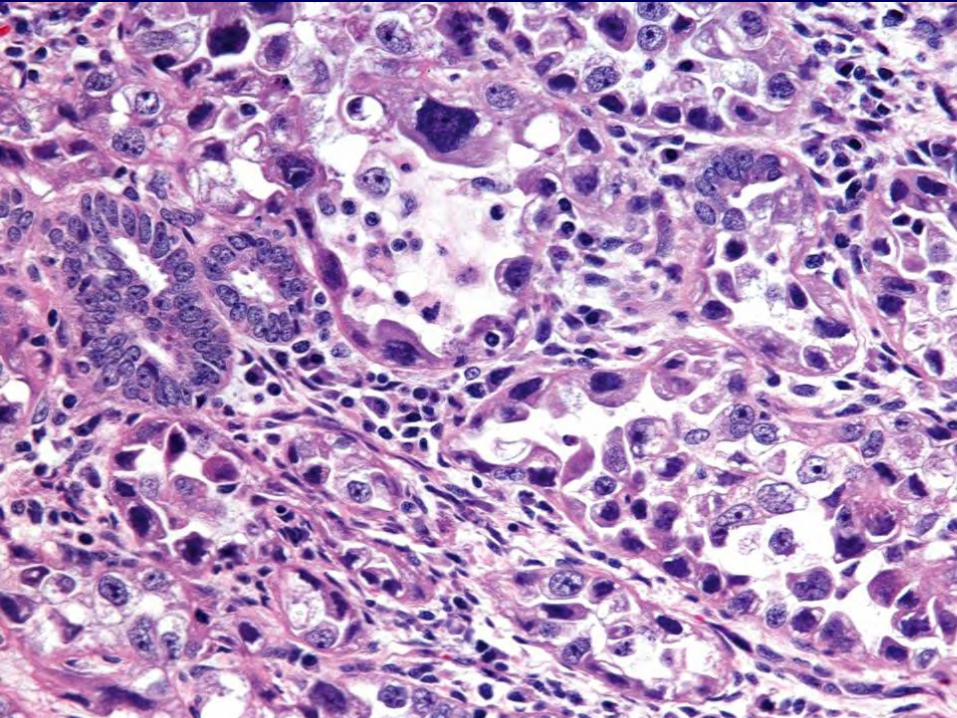
Clear Cell Carcinoma Mimics • Arias-Stella reaction & “pill effect” • Endometrioid carcinoma with clear
cytoplasm • Serous carcinoma with clear cells –
tough differential diagnosis - original Stanford series of uterine serous carcinoma featured tumors with areas of clear cell: does it matter?
• Mucinous carcinoma (less likely)

MICRO: Arias-Stella reaction
Endometrioid Carcinomas with Clear Cytoplasm
• “Secretory” carcinoma - subnuclear and supranuclear vacuoles, low grade (nuclear grade 1-2) cytology
• Endometrioid carcinoma with clear cytoplasm, due to glycogen, lipid, other
• Squamous glycogenization has other areas of classic squamous differentiation
• Lipid, other causes of artifactually clear cytoplasm have low grade nuclear features, merge with classic endometroid carcinoma Am J Surg Pathol 2007;31:1203-8
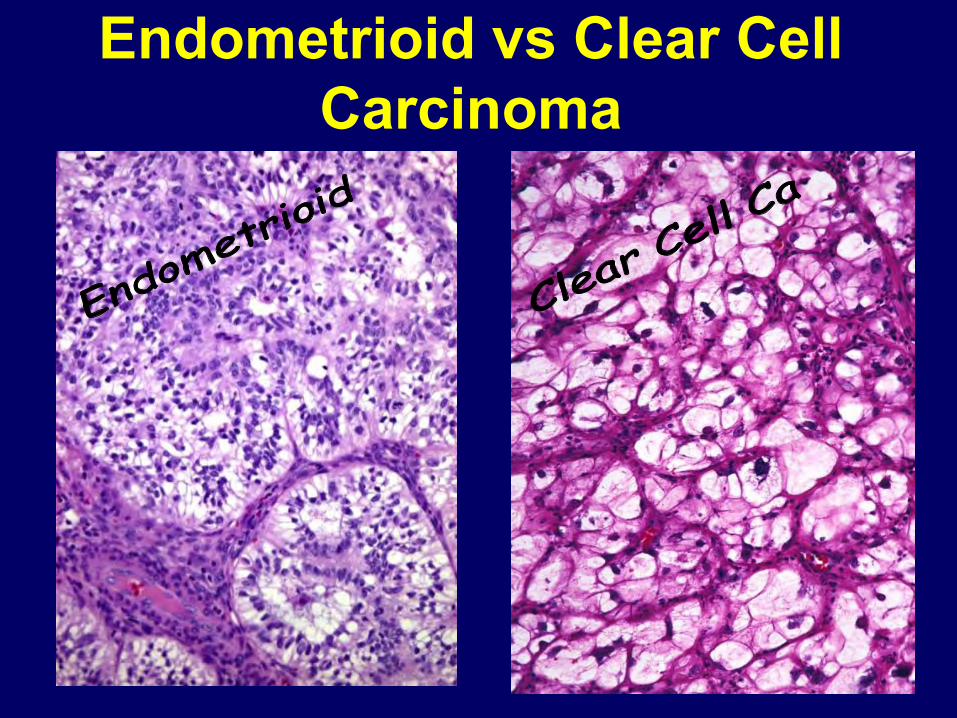
Endometrioid vs Clear Cell Carcinoma
Mucinous Carcinoma
Mucinous Adenocarcinoma, Endometrial Origin
• Less than 10% of all endometrial cancer • Definitions vary – WHO uses >90% mucin
component • Most mixed with endometrioid • Type 1 cancer (estrogen) • Most low grade (FIGO 1 or 2) • Most low stage
Low Single Copy Number Abnormalities
• CTNNB1
• KRAS
• SOX17
Mutually exclusive, so different mechanisms activating WNT signaling
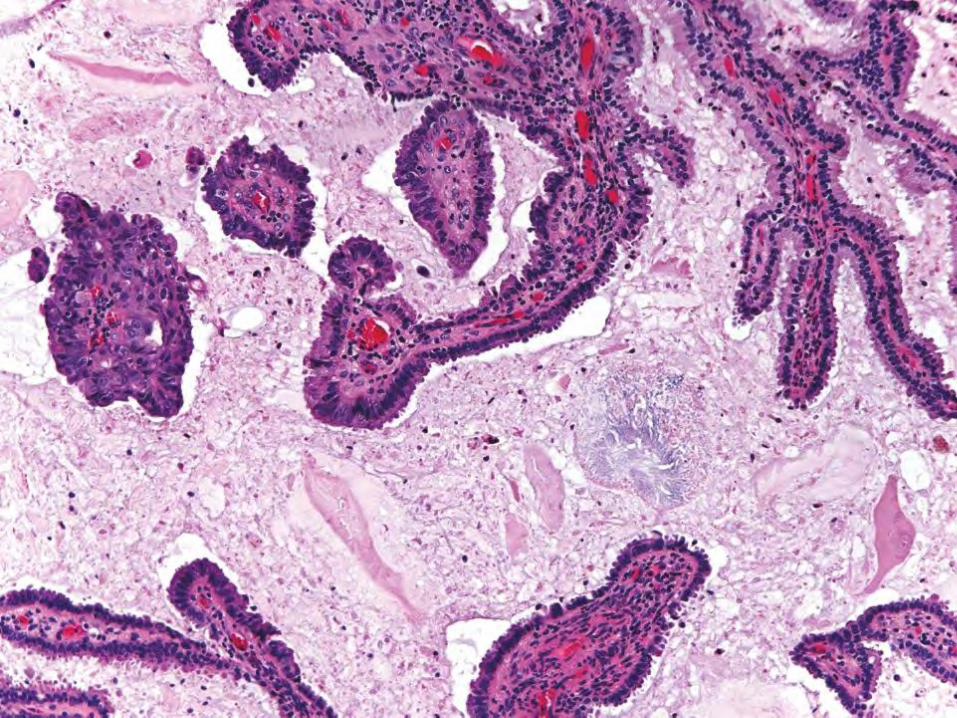
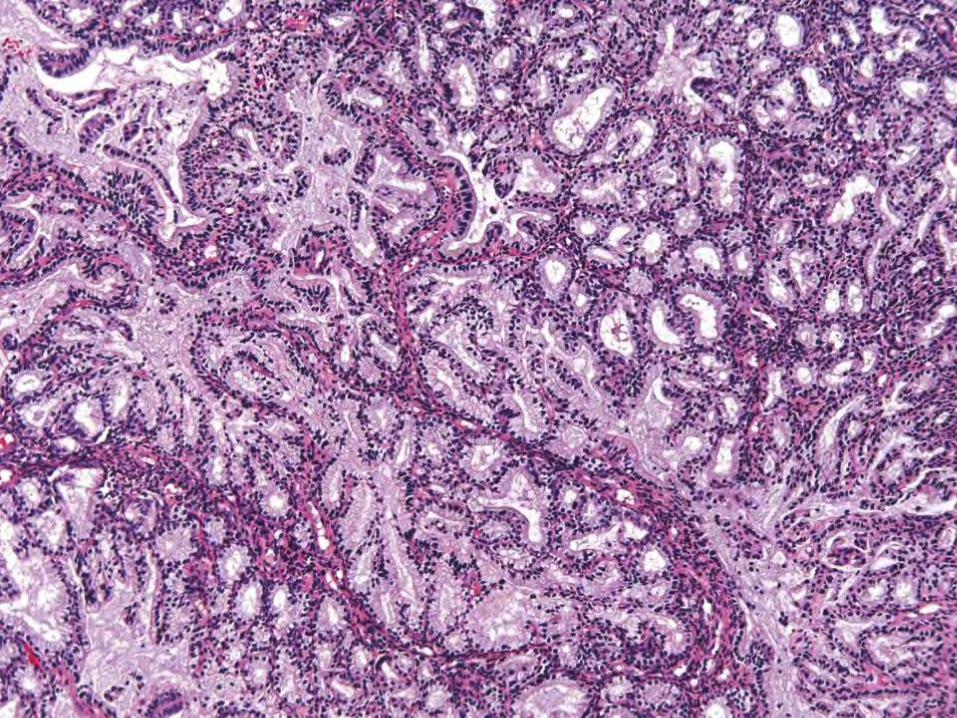
Mucinous Adenocarcinoma, Endometrial Origin
• Often deceptively bland cytology • Complex architecture may not always be
present • Copious mucin • May mimic microglandular hyperplasia or
minimal deviation adenocarcinoma • If in doubt: “complex mucinous
endometrial proliferaiton, cannot exclude carcinoma”
Endometrial vs Endocervical: All About (Predicting) Location
• Endocervical or endometrial? • Lower uterine segment? • Metastasis? • Benign or malignant?
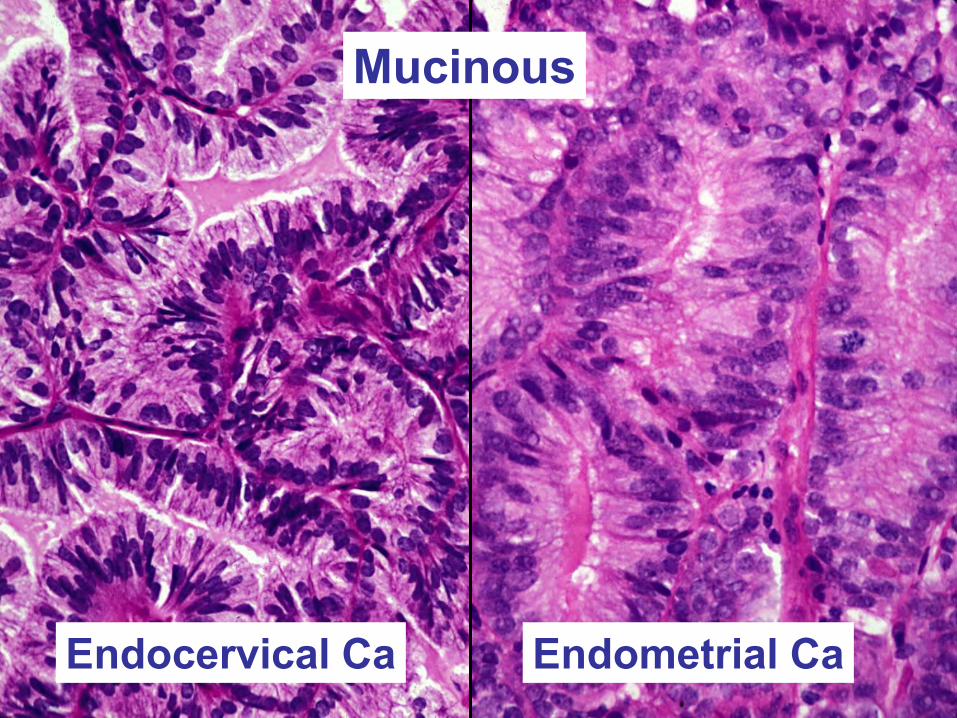
Endocervical Ca Endometrial Ca
Mucinous
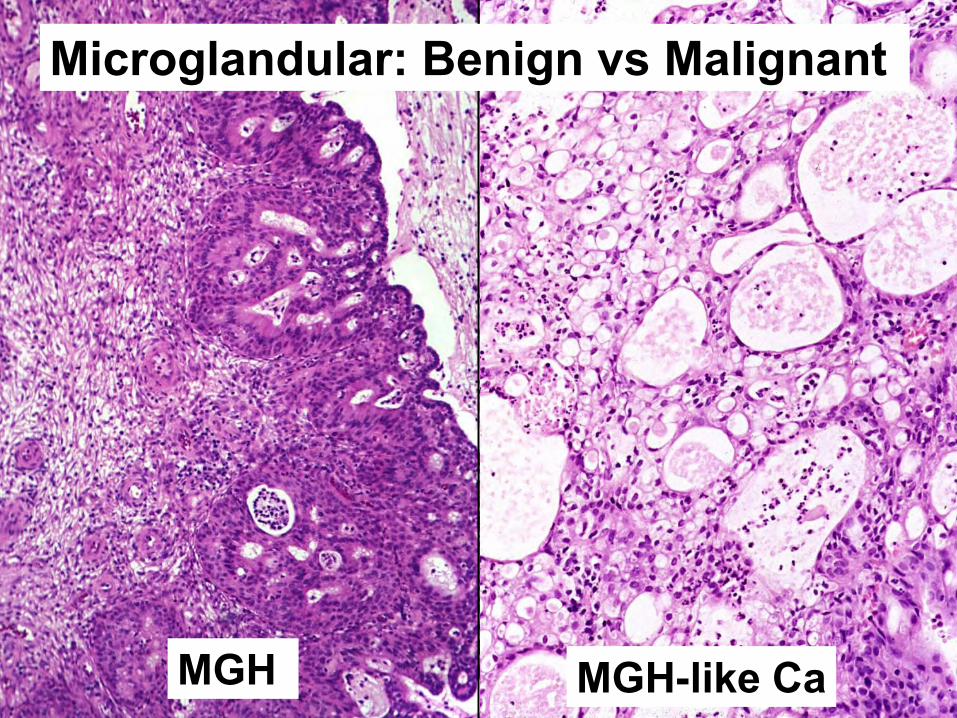
MGH MGH-like Ca
Microglandular: Benign vs Malignant
Strategies
• Physical exam • Differential or fractional curettage • Imaging studies • Histologic features • Immunohistochemical features
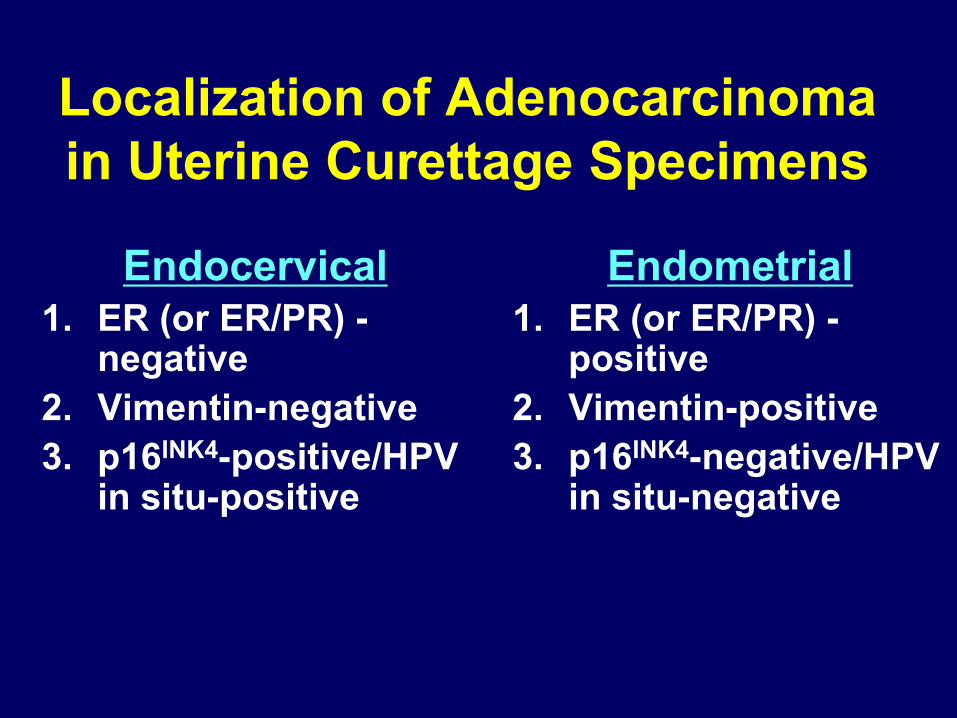
Localization of Adenocarcinoma in Uterine Curettage Specimens
Endocervical 1. ER (or ER/PR) -
negative 2. Vimentin-negative 3. p16INK4-positive/HPV
in situ-positive
Endometrial 1. ER (or ER/PR) -
positive 2. Vimentin-positive 3. p16INK4-negative/HPV
in situ-negative
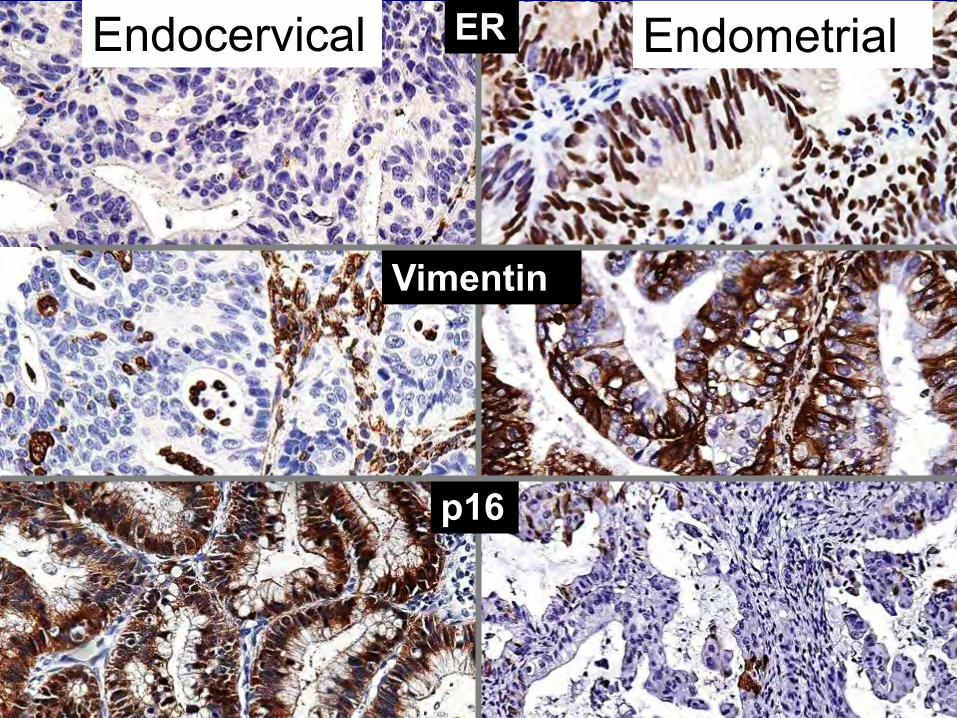
Vimentin
ER
p16
Endocervical Endometrial
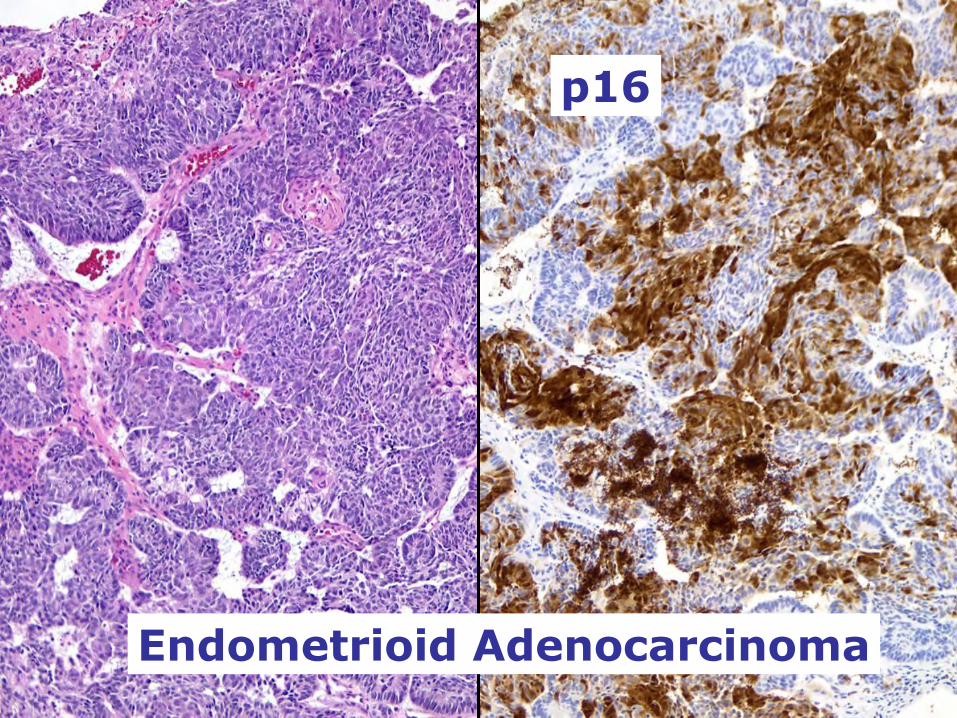
Endometrioid Adenocarcinoma
p16
p16
p16
Uterine serous carcinoma
Endometrial squamous morules
Squamous Carcinoma
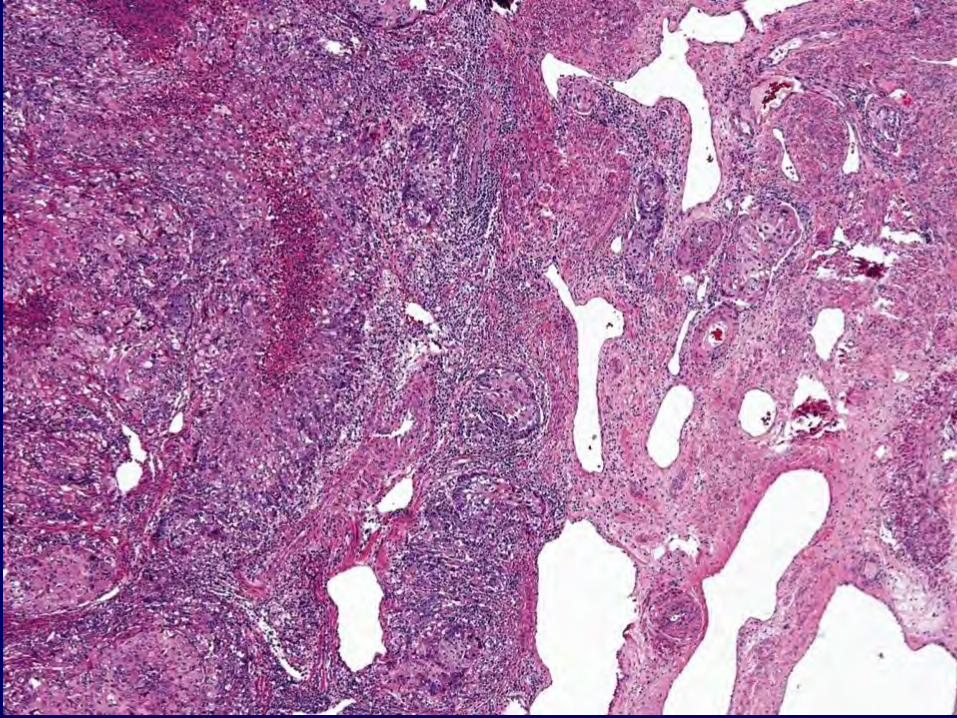
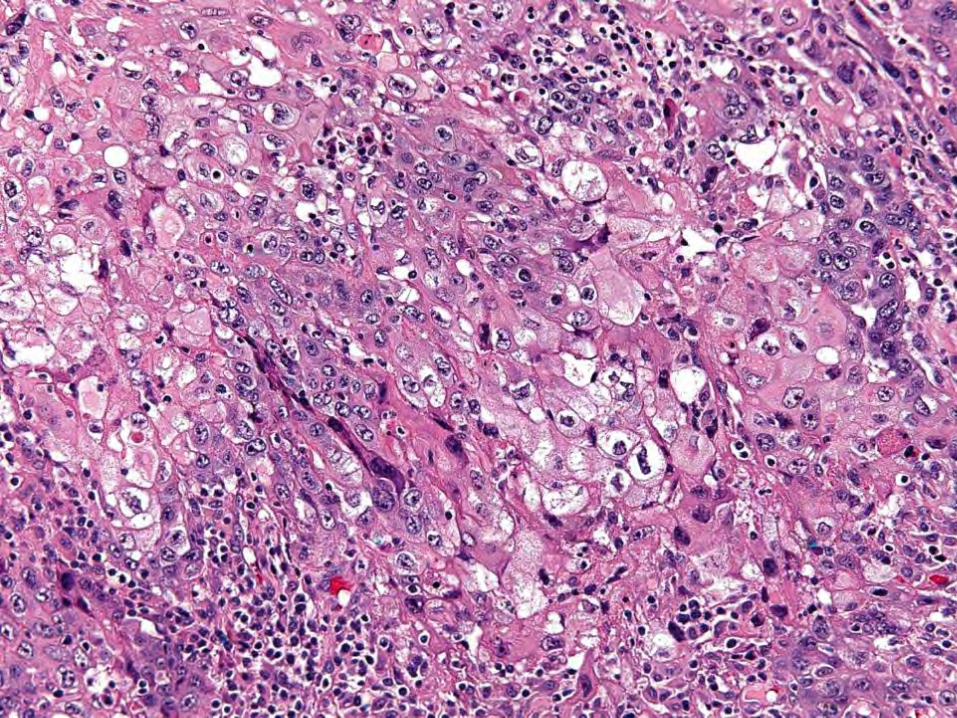
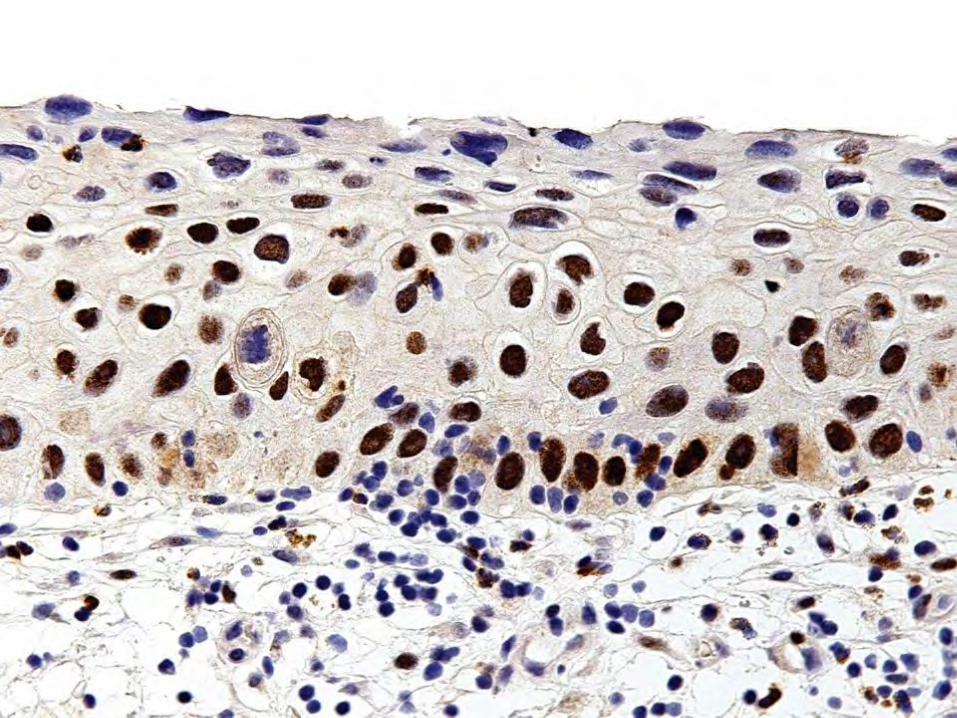
Uterine Squamous Cell Carcinoma
• Rare (less than 0.5%) • Postmenopausal • Most well to moderately differentiated • Must have no glandular component • High-risk HPV detected in rare cases
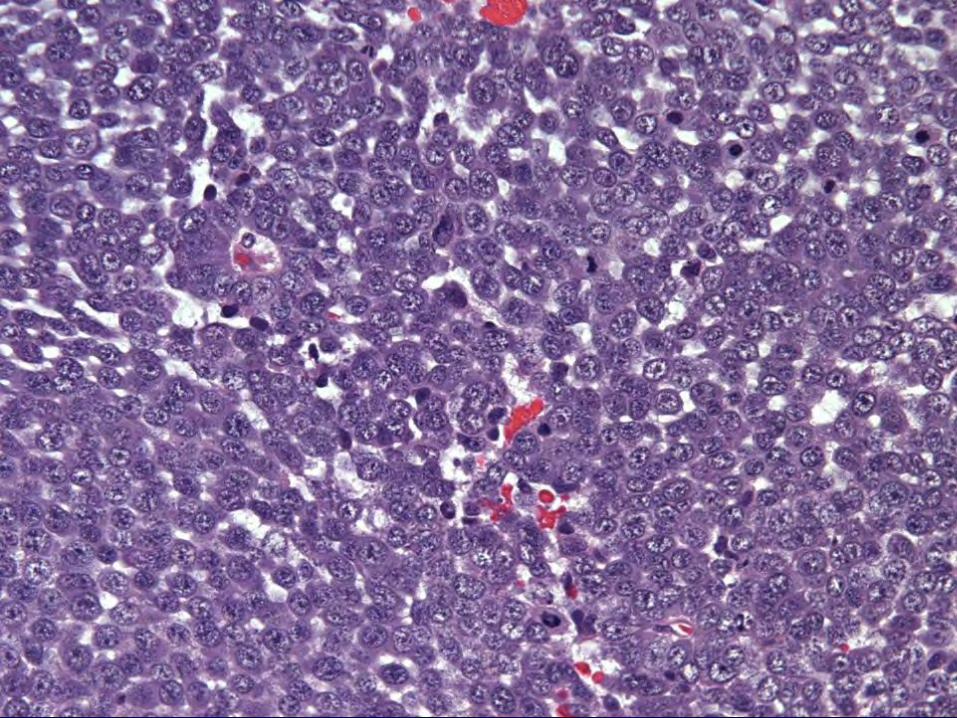
Undifferentiated Carcinoma
MSI Hypermutated
• ARID5B
• KRAS
• Frameshift deletions in RPL22
• Most with MLH1 promoter hypermethylation
• 10-fold increased mutation frequency
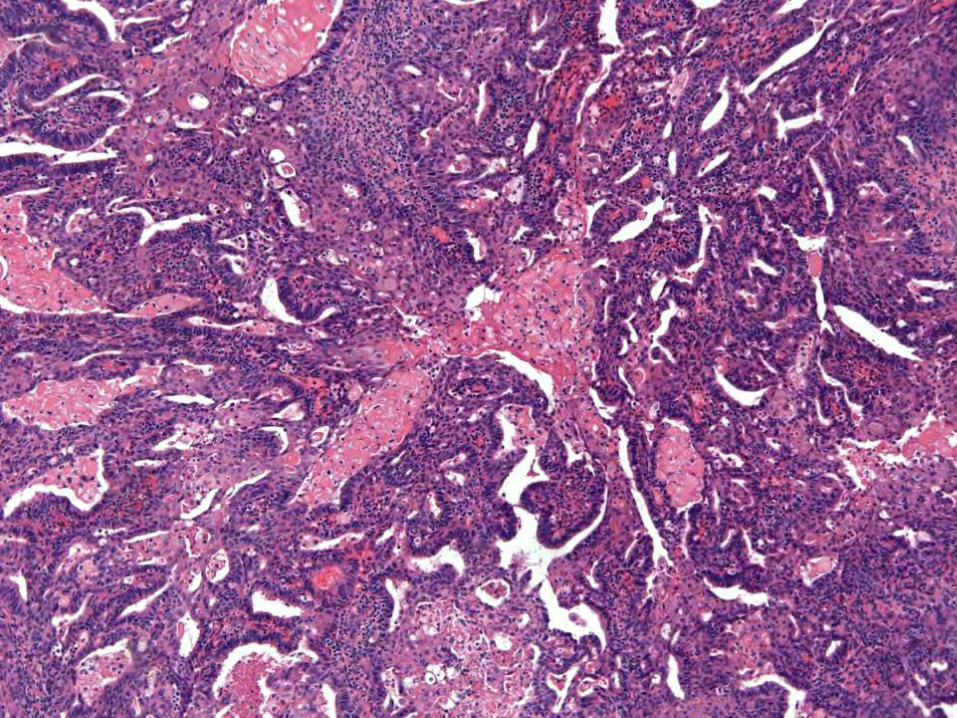
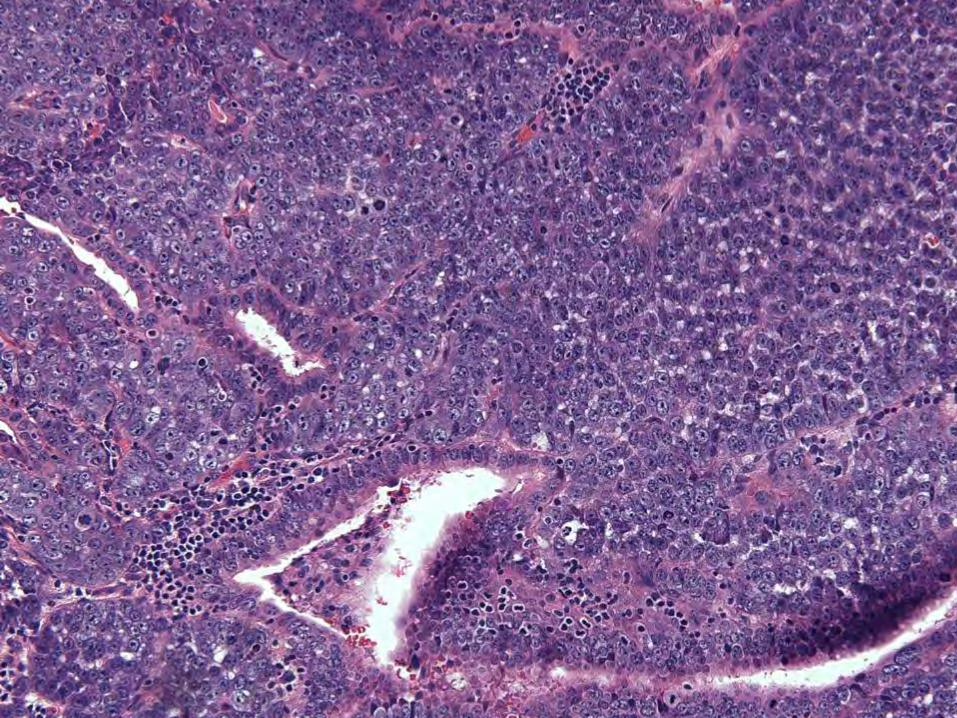
“Dedifferentiated” Endometrioid Carcinoma
• Low grade component with well-formed glands
• Undifferentiated component • Typically abrupt transition • Poor prognosis • Subset assoc. with mismatch repair
protein defects & Lynch syndrome
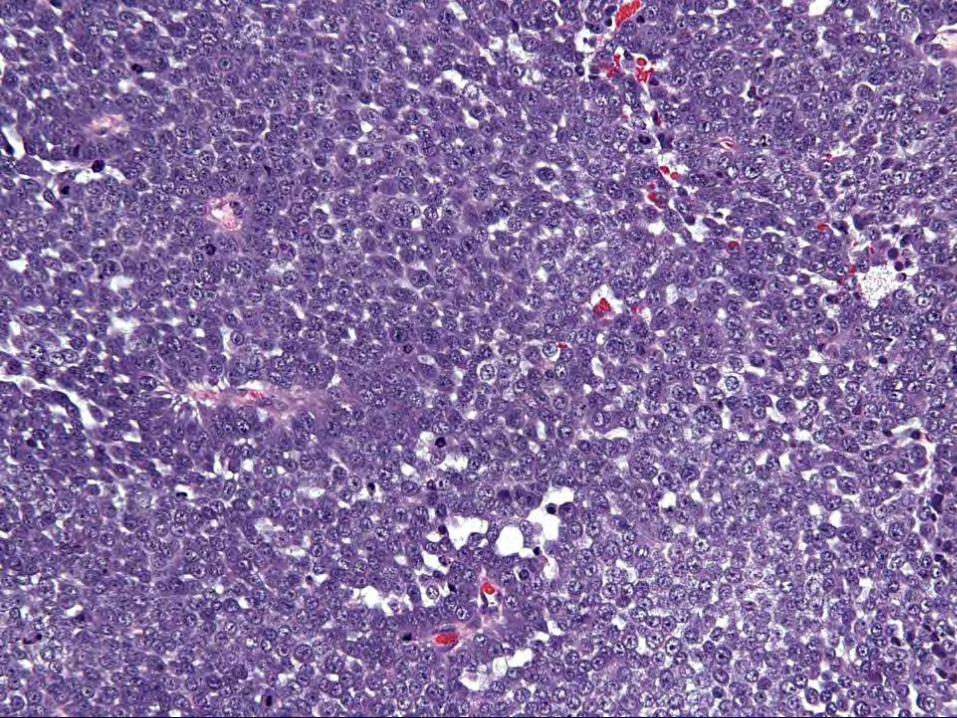
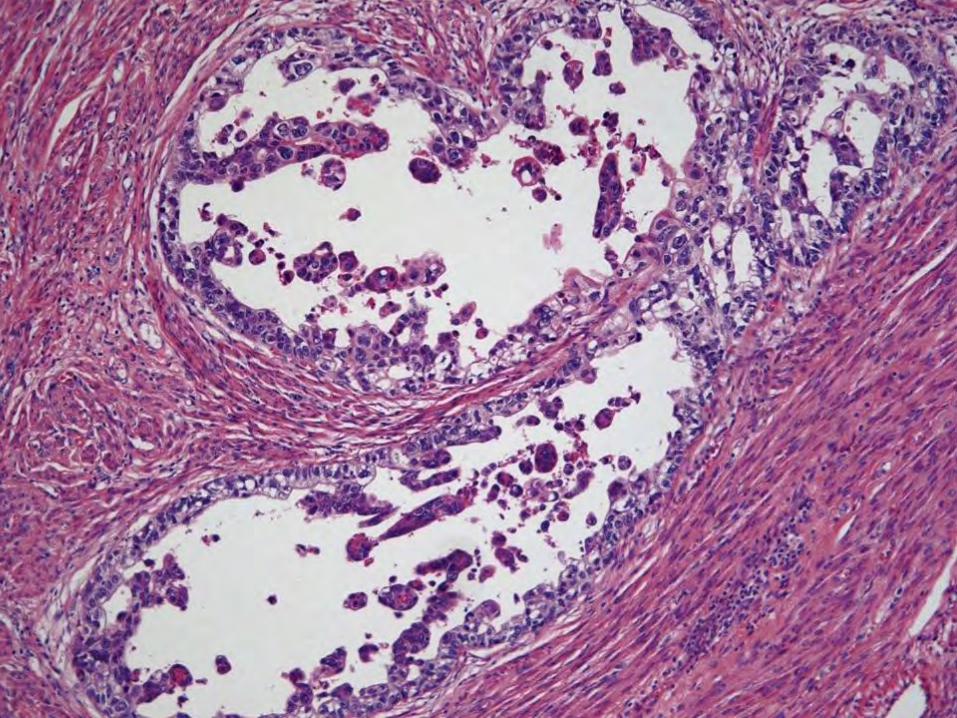
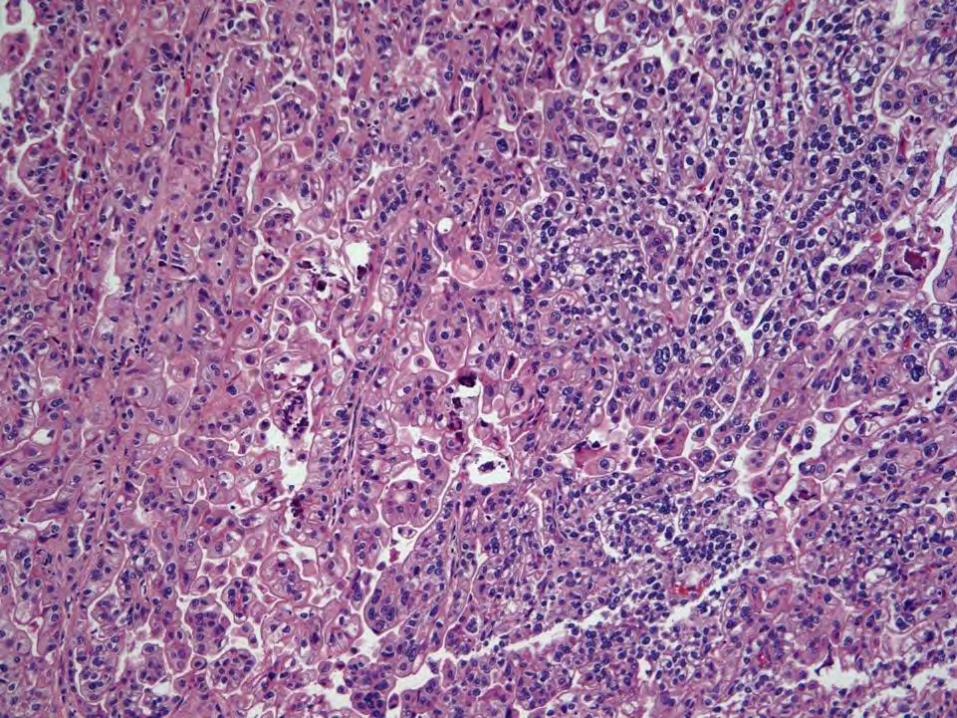
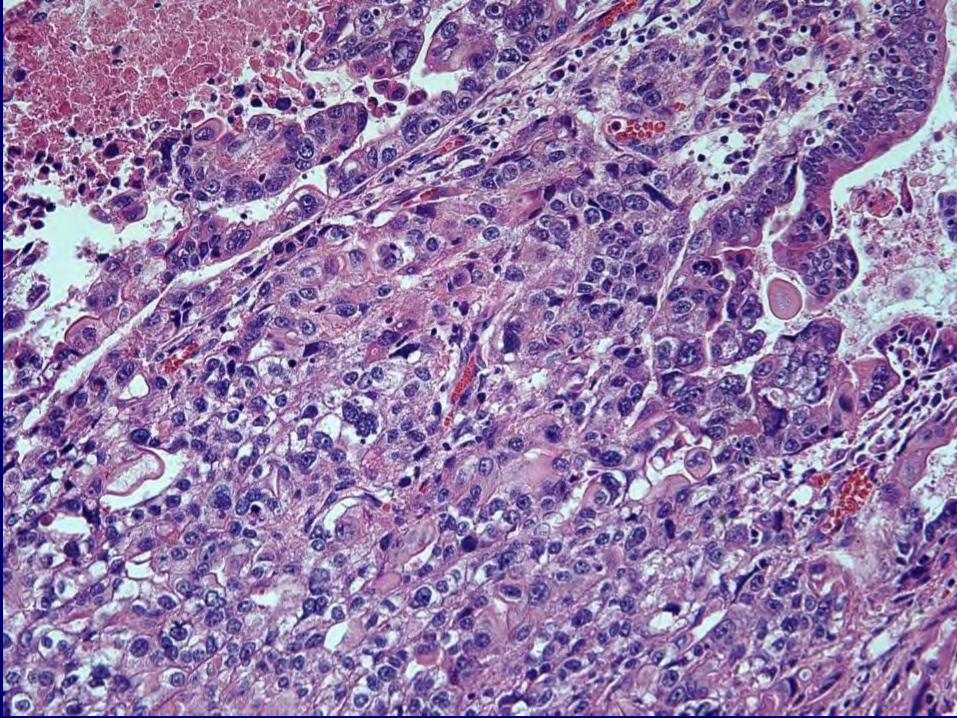
Carcinoma with Yolk Sac Differentiation
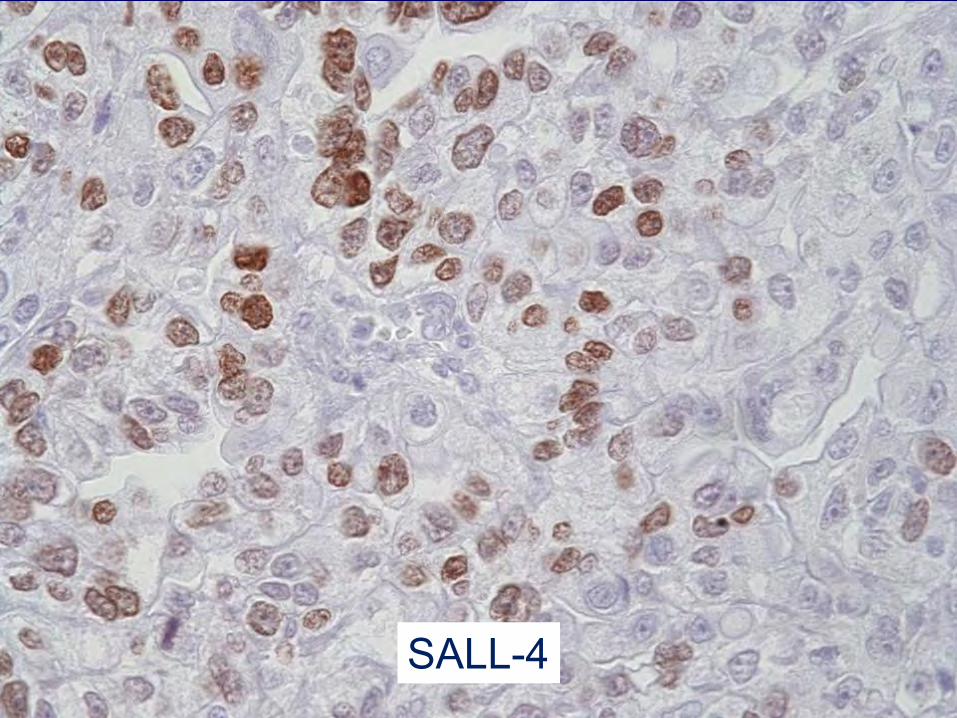
SALL-4
Carcinoma with Yolk Sac Differentiation
• High-grade endometrioid or serous • May have elevated serum AFP • May present in recurrent tumor,
suggesting transformation • Few cases, so best treatment not clear
Mesonephric Carcinoma
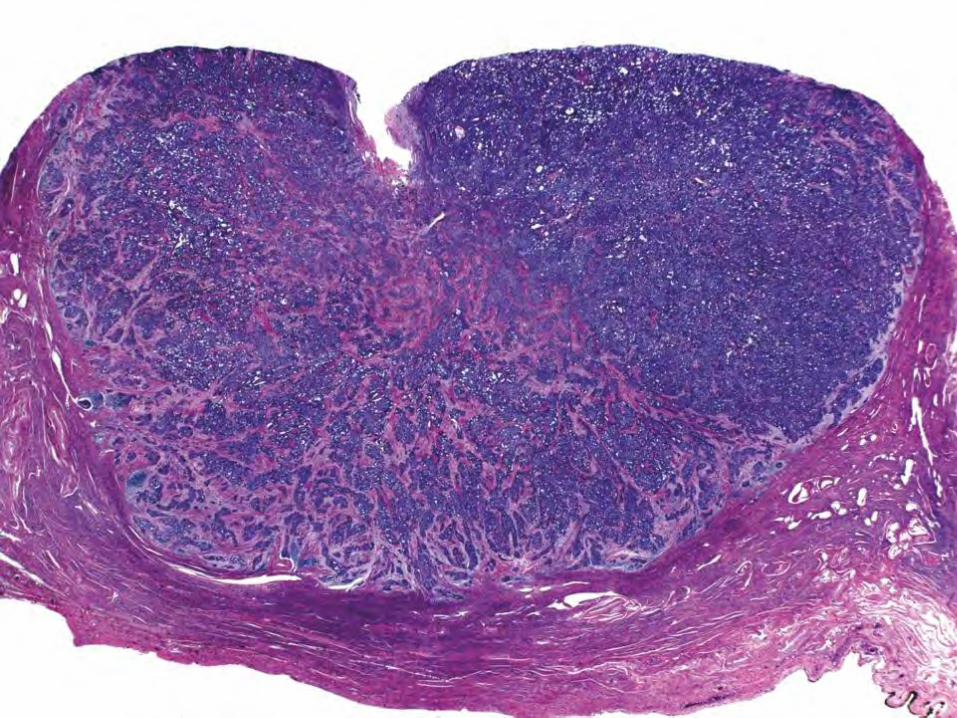
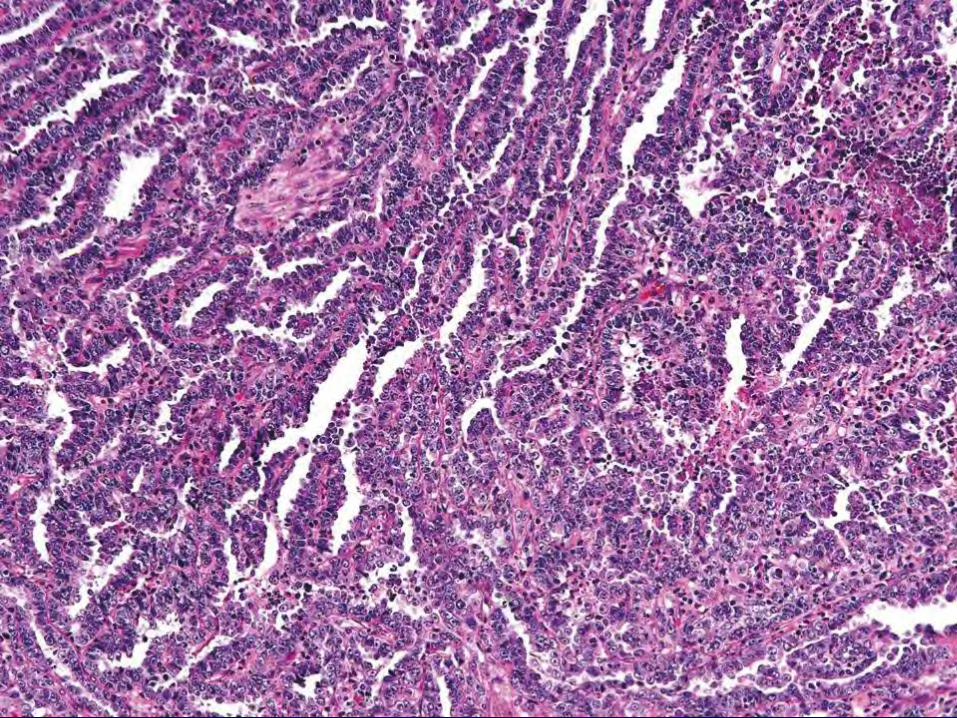
Mesonephric Adenocarcinoma
• Rare – often no surface component • Wide age range • Not linked to HPV • Can have ductal, retiform, tubular, solid,
spindle patterns • May arise in corpus
Mesonephric Adenocarcinoma
• Cytokeratin positive • CK7 negative or weak positive • Calretinin positive • CD10 positive
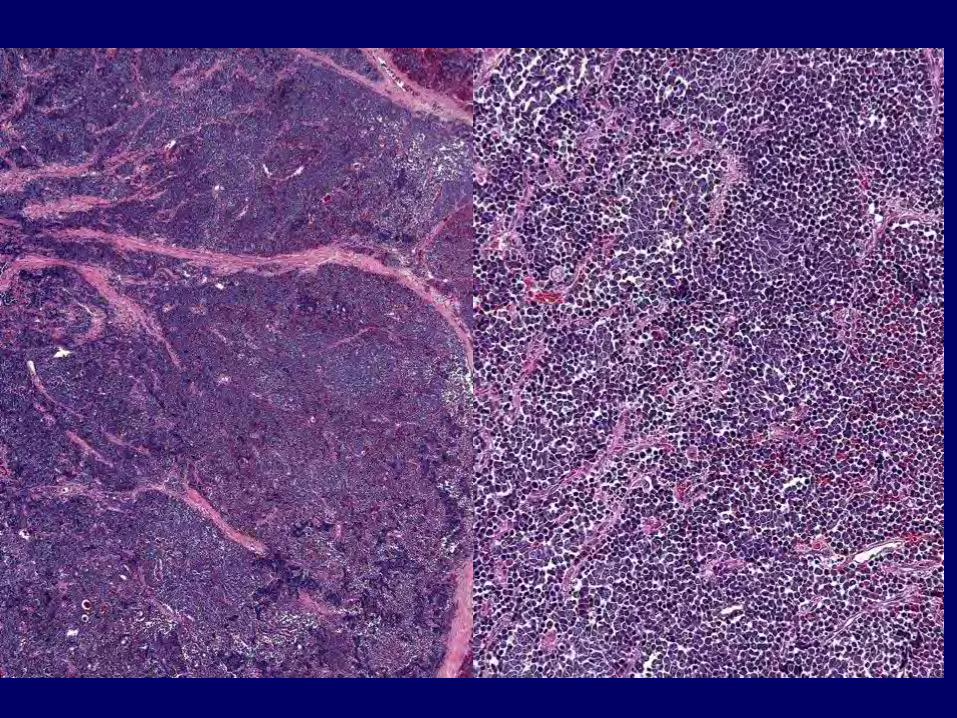
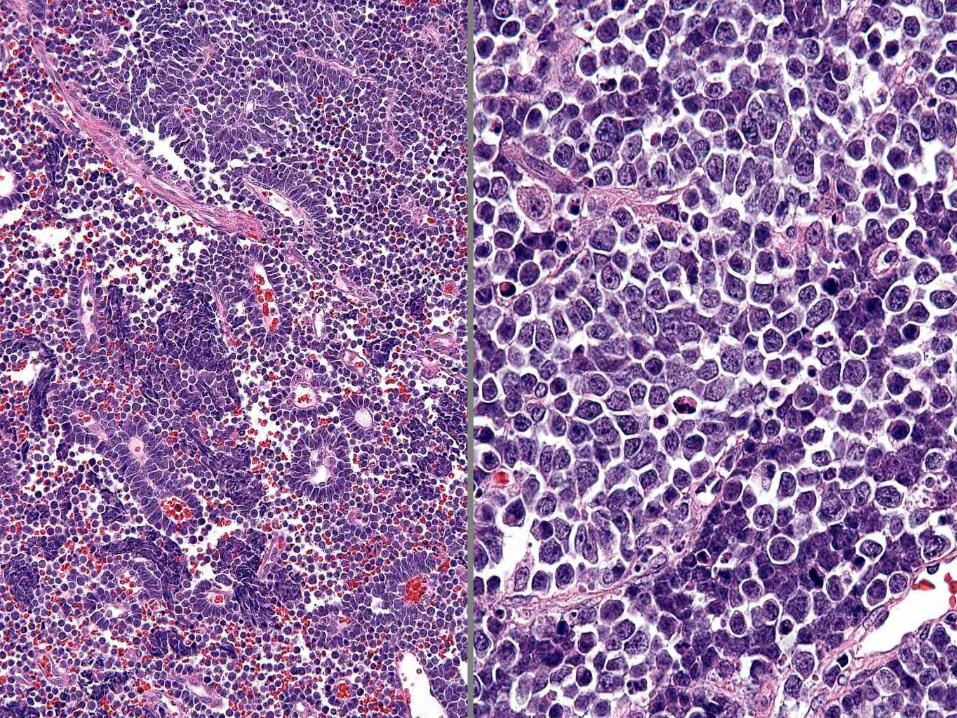
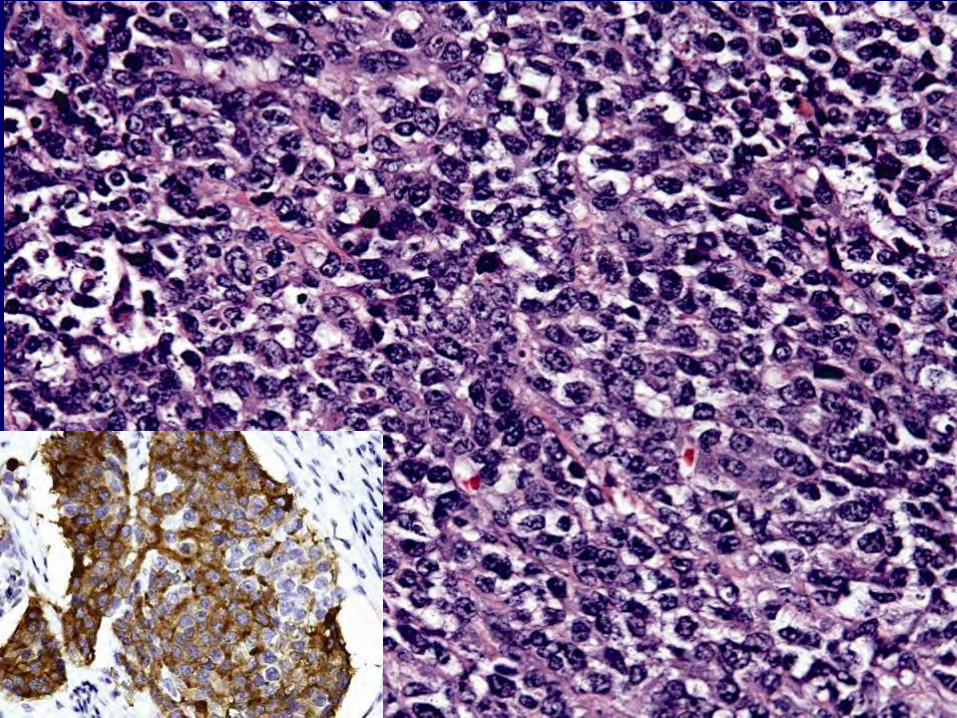
Neuroendocrine Carcinoma
GYN: Low-Grade Neuroendocrine • Well differentiated, grade 1 (“carcinoid”)
have a low Ki-67 index (≤2%) and low mitotic count (< 2 per 10 high power fields)
• Well differentiated, grade 2 tumors (“atypical carcinoid”) have increased Ki-67 index (3-20%) and increased mitotic count (2-20 per 10 high power fields). Necrosis may be present in the “atypical carcinoid” tumors.
GYN: High-grade Neuroendocrine
• Neuroendocrine carcinoma (small cell or large cell type).
• Neuroendocrine carcinoma is considered grade 3;
• High Ki-67 index (>20%) and high mitotic counts (>20 per 10 high power fields).
• Multifocal necrosis is common.
Molecular Classification (TCGA Data)
• POLE ultramutated • Microsatellite instability hypermutated • Copy number low • Copy number high
POLE Ultramutated
• Mutations in exonuclease domain of POLE
• Increased C to A transversion • PTEN
• PIK3R1
• PIK3CA
• KRAS
• Improved progression-free survival
MSI Hypermutated
• ARID5B
• KRAS
• Frameshift deletions in RPL22
• Most with MLH1 promoter hypermethylation
• 10-fold increased mutation frequency
Low Single Copy Number Abnormalities
• CTNNB1
• KRAS
• SOX17
Mutually exclusive, so different mechanisms activating WNT signaling
High Single Copy Number Abnormalities
• Serous (94%) • Mixed histology (62%) • Endometrioid (12%)
– 24% Gr 3 & 5% Gr 1-2
High Single Copy Number Abnormalities • TP53
• MYC
• ERBB2
• CCNE1
• FGFR3
• SOX17
Stanford University
Thank you