environmental health - mohp.gov.egµحة البيئة.pdf · acknowledgments this two-year...
TRANSCRIPT

Environmental Health
Prepared by
Prof. Dr. Ahmed Shoman
Professor of Public Health, Faculty of Medicine,
Ain Shams University
First Year 2019/2018

Acknowledgments
This two-year curriculum was developed through a participatory and collaborative approach between
the Academic faculty staff affiliated to Egyptian Universities as Alexandria University, Ain Shams
University, Cairo University , Mansoura University, Al-Azhar University, Tanta University, Beni Souef
University , Port Said University, Suez Canal University and MTI University and the Ministry of Health
and Population(General Directorate of Technical Health Education (THE). The design of this course
draws on rich discussions through workshops. The outcome of the workshop was course specification
with Indented learning outcomes and the course contents, which served as a guide to the initial design.
We would like to thank Prof.Sabah Al- Sharkawi the General Coordinator of General Directorate of
Technical Health Education, Dr. Azza Dosoky the Head of Central Administration of HR Development,
Dr. Seada Farghly the General Director of THE and all share persons working at General
Administration of the THE for their time and critical feedback during the development of this course.
Special thanks to the Minister of Health and Population Dr. Hala Zayed and Former Minister of
Health Prof. Ahmed Emad Edin Rady for their decision to recognize and professionalize health
education by issuing a decree to develop and strengthen the technical health education curriculum for
pre-service training within the technical health institutes.

مقشس دساسيجوصيف
المقرر بيانات -1
: الكودى الرمز : المقرر اسم Environmental Health Curriculum
: المستوى/ الفرقة Health Inspector and Health educator
: التخصص
6 عملى 3 نظرى: الدراسية الوحدات عدد
Every week: 3hs theoretical and 4hs practical for 12 weeks
:المقرر هدف -2 At the end of the course the students should know:
1-The scope of environment:
Home environment.
Work environment.
Recreation environment.
2-Different environmental stressors.
Biological stressors
Chemical stressors.
Physical stressors.
Social stressors
Psychological stressors
3-The impact of insanitary environment on health.
Immediate as infection and irritation.
Delayed as cancer.
Students of technical health institutes.
: المقرر تدريس من المستهدف -3
المعلومات. ا
: والمفاهيم
1- To recognize the epidemiological triad including the
interaction between environment, host and causative agents,
2-To recognize the different environmental stressors including:
Biological stressors
Chemical stressors.
Physical stressors.
Social stressors.
Psychological stressors.
3-To recognize the standards of sanitary environment specially:
Air:
Sulfur dioxide level.
Carbon monoxide level.

Nitrogen dioxide level.
Ozone level.
Suspended particulate level.
Carbon level.
Water:
Physical quality as turbidity, odor and color.
Chemical aspects as:
Ammonia
PH
Hydrogen sulphide
Dissolved oxygen
Organic constituents as :
Pesticides.
Aromatic hydrocarbons.
Microbial:
Virology.
Bacteriology.
Parasitology.
Radiological aspect.
Basics for Handling Food Safely
Storage
Preparation
Thawing
Cooking
Serving
Leftovers
Refreezing
Cold Storage Chart
المهارات -ب
: نيةالذه
1- To interpret air indicators and to compare with the standards.
2- To interpret water indicators and to compare with the standards.
3- To interpret food indicators and to compare with the standards.
المهنية المهارات -ج
:بالمقرر الخاصة
1- To be able to prepare and present power point slides as a material of health education.
2- To be able to communicate with people through health education sessions and counselling as tools of health education to increase awareness about the importance of environmental sanitation and to avoid the drawbacks of health hazards.
In addition

The health inspectors should have the skills of getting air and water samples and how to transmit them to the labs.
المهارات -د
: العامة
1- To have computer and net skills to contact international agencies to get the international environmental standards.
2- To have the ability to understand the different medical and environmental terminology.
:المقرر محتوى -4
Section I
General overview: 1- The epidemiological triad including the interaction
between environment, host and causative agents. The scope of environment including: home environment,
work environment and recreation environment. 2- The scope of environment including: home
environment, work environment, recreation environment.
3- Different stressors including:
Biological stressors
Chemical stressors.
Physical stressors.
Social stressors.
Psychological stressors.
Section II Air:
Air pollution.
Indicators of air pollution.
Sources of air pollution.
Effect of air pollution.
Instruments used to measure air pollution.
Section III Water:
Water quality.
Sources of water pollution.
Large scale of water purification.
Small scale of water purification.
Water related diseases.
Characteristics of water borne epidemics.
Section IV waste disposal:
Waste related health hazards.
Solid waste and methods of disposal.
Excreta disposal
Sewage system
Sewage purification
Modern sewage disposal

Section V Hospital environment:
Hospital waste disposal:
Collection.
Sorting.
Handling and transport.
Interim storage.
Final disposal.
Types of waste according to WHO.
Special precautions for different waste.
Impact on health.
Section VI Environmental changes: Green house and global warming. Ozone phenomenon.
Acid rain.
Dioxin (toxic chemicals of polychlorinated biphenyls.
It arise from uncontrolled waste incineration.
أسااية الحعليم والحعلم -5
1- Lectures including different topics. 2- Self-learning by searching through the net and
designing presentations on different topics. 3- Field visits.
أسالية الحعليم والحعلم للطالب -6
روى القذسات المحذودة
They should be submitted to simplified lectures with aids of demonstrations and pictures. The lectures should be repeated several times.
:جقويم الطالب -7
األسالية المسحخذمة -أ
a. Class work:
1. Quizzes
2. Midterm theoretical
3. Practical exam
4. Assignments
5. Participation
b. Final exam:
Written theoretical
الحوقيث -ب
a. Class work:
1. Quiz I (5th week) 5 marks
2. Attendance 5 marks
3. Midterm theoretical (7th week) 10 marks
4. Clinical work: 30 marks
b. Final exam
Practical exam (13th week) 10 marks
written theoretical exam (15th week) 90 marks
جوصيع الذسجات -ج
Case records and reports (5 marks) Quiz : 5 mark
Midterm: 10 marks
Attendance 5 marks
Clinical: 20 marks
Clinical exam:15 marks
Final written exam 90 marks.
Total percentage 150 mark
:قائمة الكحة الذساسية والمشاجع -8
اتمزكش -أ
كحة ملضمة -ب Official.
كحة مقحشحة -ج
1-Park's Textbook of Preventive and Social Medicine 2-Encyclopedia of environmental health.
...... دوسيات علمية أو نششات -د
الخ
1-American archives of environmental medicine. 2-Journal of Occupational and Environmental Medicine.

Gender and Social Norms
vi
Course Description .............................................................. vii
Chapter 1: Public Health Officer and Environment ........................ 5
Chapter 2: Epidemiological Triad Environmental sanitation ............. 9
Chapter 3: Air pollution Gases Dust Global Effect of Air pollution ..... 12
Chapter 4: Physical Agents ..................................................... 25
Chapter 5: Water Pollution ..................................................... 30
Chapter 6: Waste Disposal Solid Waste Sewage Hospital Waste ......... 37
Chapter 7: Food Sanitation ..................................................... 42
Chapter 8: Social Environment ................................................ 50
Chapter 9: Law No 4 of 1994(related to environmental Health) ....... 51
Chapter 10: Reports and exercises ........................................... 55
لوصاسة الصحة والسكان ويحزس تيع حقوق النشش والحأليف
Contents
v

7
Week Theory Practice
1st Introduction(epidemiological
triad +concept and scope of
environment)
Measurements of health trends due to environmental changed.
2nd Water:
water quality and source of
water pollution.
Skills of communication through health education and counselling.
3rd Water related
diseases.
Characteristics of
water borne
epidemics
Water samples and simple
analysis.
4th Air pollution.
Indicators of air
pollutions,
Sources of air
pollution.
air samples and simple
analysis.
5th Health effect of air
pollution.
Instruments used to
measure air
pollution.
Skills of communication
through health education
and counselling.
6th Waste disposal (solid and
sewage)
A visit to waste disposal
station.
7th Food sanitation
Presentations on sanitary
food.
Preparation
Thawing
Cooking
Serving
Leftovers
Refreezing
Cold Storage Chart
8th Hospital environment and
waste disposal
A visit to an infection
control unit in a hospital.
9th Social environment and
stress.
Training on using
different questionnaires
to evaluate strain and
stress.
10th Physical hazards: Noise ,
temperature changes and
radiation.
Training of measurement
of cooling power of air,
air temperature and
relative humidity.
11th Environmental changes.
Presentation of different
environmental changes as
greenhouse effect, global
warming and

viii
environmental disasters
12th Asphyxiant gases:
Simple.
Chemical
Irritant.
Pulmonary function tests


Gender and Social Norms
vi
Environmental Health Officers (also known as Public Health Inspectors or Environmental Health Practitioners or public health officers) are responsible for carrying out measures for protecting public health, including administering and enforcing legislation related to environmental health and providing support to minimize health and safety hazards.
Environmental Health Practitioners are multi-skilled in many areas with individuals being highly trained, usually to degree level, and often requiring additional professional training, professional competency assessment and continuing professional development in order to continue to practice in the field.
They are involved in a variety of activities, for example inspecting food facilities, investigating public health nuisances, and implementing disease control, conducting work place safety assessments and accident investigation.
Environmental health officers are focusing on prevention, consultation, investigation, and education of the community regarding health risks and maintaining a safe environment.
Environmental Health Officers (EHOs) bring to the position an understanding of microbiology, risk assessment, environmental science and technology, food science, knowledge of the built environment as well as the skills and knowledge related to the tracking and control of communicable disease, investigation of environmental health related incidents.
They therefore must also have strong investigative skills and a thorough understanding of the application of legislation related to public health, the built environment, pollution control and workplace safety. Working in partnership with Government Ministries (such as Health, Agriculture and Environment), local municipalities, businesses, community groups, other agencies and individual members of the community, the EHO plays a major role in protecting public health.
Some past/historic titles include inspector of nuisances, sanitarian, and sanitary inspector. Other titles that currently exist include environmental health specialist/practitioner/professional, public health officer, health officer, health inspector, and health official.
A Public Health Inspector (also known as an Environmental Health Officer or public health officer) investigates health hazards in a wide variety of settings, and will take action to mitigate or eliminate the hazards. Usually the public perception of a health inspector is someone who examines restaurants and ensures they maintain sanitary standards for food safety set by the regulating authority. However, public health inspectors have much broader job duties, including inspecting swimming pools, substandard housing conditions, public schools, day cares, nursing homes. Depending on their jurisdiction, Registered Environmental Health Officers often permit and inspect wells, private water systems, and individual subsurface sewage disposal (septic) systems. Other tasks include: campground inspections, tanning salon inspections, beauty salon inspections, correctional facility inspections and mobile home park inspection. The public health inspector (environmental health officer) also plays a vital role in community
Chapter 1:
Public Health Officer and Environment

Gender and Social Norms
7
projects such as those concerning health promotion, tobacco reduction, healthy built environments/healthy communities, food security, and emergency preparedness. In fact, the job description of environmental health officers is identified by the local legislation in each country.
They may also respond to complaints such as animal bites, garbage complaints, odor
complaints, or sewage overflows. Due to their educational background they can provide
information and referrals with regards to; lead, radon, mold, and emerging diseases such
as West Nile Virus and Avian Flu. And they share in surveillance system.
The essential 10 role of public health officers:
1. Monitor environmental and health status to identify community environmental health
problems.
2. Diagnose and investigate environmental health problems and health hazards in the
community.
3. Inform, educate, and empower people about environmental health issues.
4. Mobilize community partnerships to identify and solve environmental health problems.
5. Develop policies and plans that support individual and community environmental health
efforts.
6. Enforce laws and regulations that protect environmental health and ensure safety.
7. Link people to needed personal environmental health services and assure the provision
of health care when otherwise unavailable.
8. Assure a competent environmental health and personal health care workforce.
9. Evaluate effectiveness, accessibility and quality of personal and population-based
environmental health services.
10. Research for new insights and innovative solutions to environmental health problems.
COMMUNICABLE DISEASES:
Health Officers may be called upon to assist in controlling Communicable Disease as
requested during disease outbreaks. A primary role is to assist in disseminating
educational materials throughout the city or town.
EMERGENCY RESPONSE:
Health Officers should contact their local Emergency Management Director, to both
participate in the development of local Emergency Operations Plans, and discuss their
role within the community‟s existing plan.
PUBLIC EDUCATION:
Health Officers are often well positioned to take advantage of opportunities to provide
education to residents, local officials, and public health system partners. This is achieved
by disseminating materials produced by local health authority and national authority,

Gender and Social Norms
viii
sharing his expertise with individuals and groups in his community, and educating local
officials and other partners about important environmental health issues and needs.
PUBLIC HEALTH NUISANCES:
Health Officers may conduct sanitary investigations into complaints and nuisances that
may endanger public health. These may include garbage, insects, unsanitary living
conditions, rodents, and safe drinking water inspections.
SEPTIC SYSTEMS:
Health officers may inspect septic systems to determine if a system has failed and, when
necessary, coordinate with the local health department of Environmental Services to
certify septic system failure. The health officer may perform a dye test and a test of
suspected sewage to confirm system failure.
Depending on town ordinances, a health officer may also witness test pits, inspect
repaired and new system installations, and review and approve septic system design
plans.
HOUSING:
Health Officer may enforce and ensure minimum standards for housing, including: safe
drinking water, availability of hot water, garbage control, properly functioning septic
systems and that walls and roofs do not leak. This is done through visiting the house and
write a report through a checklist.
HEALTH FACILITIES:
Health Officers inspect new or modified health facilities to certify that they meet local
health codes.
These include hospitals, nursing homes, massage therapy establishments, and health club
facilities.
CHILDCARE HOMES:
Health Officers inspect\approve facilities used to provide childcare and the homes of
people serving as foster parents to assure they meet local health codes.
FOOD-BORNE ILLNESS:
Health Officers may respond to complaints and report cases of suspected food borne
diseases and food poisoning and he can design an epidemic curve to ensure the outbreak
and to identify the type and severity of this outbreak.
Food sanitation.
ealth officers may be asked to contact food service establishments in the event of a
food-borne disease outbreak.
MOSQUITO BORNE ILLESSES:
Health Officers play an important role in disseminating educational materials to the

Gender and Social Norms
9
community regarding arthropod borne disease.
RABIES:
Health Officers serve as a local resource for information on rabies and other zoonotic
diseases.
DRINKING WATER:
Health Officers may test any public\private water supply suspected of being unsafe,
depending on directions from the Department of Environmental Services.
SMOKING:
Health Officers may be asked to follow up on complaints and violations of the smoking
law. They also participate in distributing health education materials.

Gender and Social Norms
x
Epidemiology is the science dealing with distribution, determinants and dynamic of the disease.
The epidemiologic triad
It is a triangle explaining the interaction between the 3 elements for disease occurrence.
For a disease to occur a harmful agent should come into contact with a susceptible host
under specific environmental condition.
This means that there is interaction between the causative agent and the host and
the surrounding condition for a disease to occur. This triad demonstrates the importance
of the surrounding condition in causing the diseases
1) Agent factors: it may be:
Biological as:
Bacteria: Mycobacterium bacilli, Salmonella typhi and paratyphi and vibrio cholera.
Virus: Hepatitis virus(A,B<,C….), poli, measles and mumps.
Fungus: Tinea versicolor, Tinea pedis and ring worm.
Parasites: Ankylostoma and Ascaris
Other biological as spirochetes, protozoa and even insects as pediculosis.
EPIDEMIOLOGIC TRIAD
Agent
Environment Host
Chapter 2: Epidemiological Triad
And Concept of Environmental Health

Gender and Social Norms
11
Chemical as CO poisoning, metal fumes as lead and cadmium, and solvents.
Physical agents as:
-Change in temperature as too hot or too cold.
-Noise: exposure to noise above certain level cause nerve deafness. Noise
also --can be a risk factor in hypertension and cardiovascular diseases
Radiation.
-Change in pressure as in diving or climbing mountains. Examples of such
diseases are acute mountain sickness and decompression sickness.
Nutritive items: for example iron deficiency causes iron deficiency anemia, calcium
and vit D deficiency causes rickets in infants and osteomalacia in adult.
2) Host factors.
They are classified into:
A-Non modified biological traits as age, sex, ethnic group, race, and any other genetically
determined variable as the blood group. These traits are fixed and cannot be changed so
they are undependable in putting a preventive program.
B-Modified traits as the social traits that including occupation, education, marital status,
diet, smoking, and exercise and drug abuse. These traits are changeable and they play an
important role in putting a preventive program by changing the life style and behavior
attitude.
3) Environmental factors.
The environmental factors include:
A-Physical environment (climate, residency, pollution of air or water), as air pollution
precipitate to spread of droplet infection, contaminated water and food precipitate to
spread of food borne diseases.
B-Biological environment (presence of the vector of the disease as mosquitoes) as they
precipitate to spread of arthropod borne diseases as malaria, yellow fever and filariasis.
C- Socio-cultural (overcrowding, poverty,) as they may be predisposing factors for
diseases like rheumatic heart diseases, scabies and pediculosis.

Gender and Social Norms
xii
Environmental Sanitation
What are the components of environmental sanitation?
1-Sanitary planning of cities, towns, districts or villages before being established, taking
into consideration the requirements of the zone (separate industrial, commercial and
residential zones), good housing, sanitary environment and public services.
2- Housing which fulfills requirements of healthy living and needs of sound social life.
3-Air sanitation and ventilation.
4-Portable water supply.
5-Sanitary waste disposal.
6-Vector control.
7- Food sanitation.
What is the importance of environmental sanitation?
1- Prevention of health hazards including chemical, physical, biological and social
hazards.
2- Health promotion.
The most frequent accidents related to insanitary home environment:
1-Fire.
2-Gas accidents as CO poisoning.
3- Electrical shock.
4- House Fall and slippery due to bad housekeeping.
5- Chemical poisoning as by pesticides and drugs.
The different causes of insanitary housing:
Rapid growth of the population.
Urbanization.
Development of slum areas.
Crowded poor houses.
The frequent hazards due to insanitary housing:
Rheumatic heart diseases.
Respiratory tract infections.
Food borne diseases.
Vector borne diseases.
Social problems.

Gender and Social Norms
13
Air pollution is change in normal air constituents by introduction of chemicals, particulates, biological materials, or other harmful materials into the Earth's atmosphere, possibly causing disease, or damage to human being and other living organisms such as food crops, or the nature.
Under ordinary conditions, the composition of outdoor air is remarkably constant. This
is brought about by certain self-cleansing conditions:
1. Wind: wind dilutes and sweeps away impurities by its movement.
2. Sunlight: it plays its role by oxidizing impurities and killing bacteria.
3. Rain: It removes the suspended and gaseous impurities.
4. Plant life: It generates oxygen.
Indicators of Air pollution:
Sulfur dioxide
Carbon monoxide
Nitrogen dioxide
Ozone
Suspended particulates
Chapter 3: Air Pollution, Related Chest
Diseases and Global Effect

Gender and Social Norms
xiv
Carbon black.
The level of such pollutants are changeable according to the season as they are
affected by air temperature and humidity.
Sources of air pollution:
Natural Sources –Volcano, forest fire, dust storms, oceans, plants and trees
Sources initiated by human beings:
1-Industrial processing, power plants, fuels combustion etc.
2-Incineration or open firing.
3-Mobile sources.
Effects of air pollution
A. Health Effects
1. Immediate or short term effect:
- Irritation to the eyes, nose and throat,
- Upper respiratory infections such as bronchitis and pneumonia.
- Other symptoms can include headaches, fatigue, nausea, and allergic reactions.
- Aggravation of the medical conditions of individuals with asthma and
emphysema.
- In the great "Smog Disaster" in London in 1952, four thousand people died in a
few days due to the high concentrations of pollution.
2. Long term effect:
- Chronic bronchitis with persistent cough and expectoration.
- Asthma due to presence of allergens.
- Kidney diseases due to inhalation of nephrotoxic fumes.
- Heart diseases secondary to increase of pulmonary pressure.
- Cancers due to presence of initiator and promoter carcinogens.
- Abortions and other reproductive hazards as congenital anomalies.
- Depression and other psychological disorders.
Measurement of air pollution:
There are many types of instruments used to measure air pollution as:
1. Absorption plates: trap pollutants on a reactive plate for a measure of air
contaminants.
2. Collecting solids on a filter paper.
3. Lasers measure pollution depending upon the amount of light reflected
Gender and Social Norms
15
4. Gas chromatography: passes air through a packed column to measure types of gaseous
contaminants.
VENTILATION IN WORK PREMISES: Aims at maintaining the concentration of pollutants below maximum permissible
limits. The provision of adequate ventilation inside work premises shall be effected in
one of two ways:
1- General ventilation
2- Local ventilation
1- GENERAL VENTILATION:
It is a suitable method for treatment of low toxicity solvent fumes. It is not suitable for
high toxicity substances, nor pollutants which are irregularly emitted or in large
quantities. It is not generally suitable for dealing with dust and fumes.
The technical engineering aspects shall be taken into consideration when
establishing the ventilation system. A specialized engineer shall supervise the
execution of this system guided by the recommendations set forth in the following
reference book: AMERICAN CONFERENCE OF GOVERNMENTAL INDUSTRIAL HYGIENISTS,
COMMITTEE ON VENTILATION, INDUSTRIAL VENTILATION. A MANUAL OF RECOMMENDED
PRACTICE, 13TH ED. AACGIH, Lansing, MI, 1974.
2- LOCAL VENTILATION:
It is more effective for controlling the different types of pollutants. It consists of a
hood, a set of pipes, a purifying apparatus to clear the air before its emission outside
the location, and a fan to circulate the air.
Whatever the design of the hood, the speed of air at the pollution point source must
be enough to remove it before it is dispersed in the work premises.
Technical and engineering aspects should be taken in consideration in designing the
local ventilation system. Execution of the system must be supervised by a specialized
engineer making use of the above mentioned reference for general ventilation.
Whenever general and local ventilation systems are used, maintenance should be
supervised periodically by a specialized engineer and efficiency should be assessed out
during periodic maintenance.

Gender and Social Norms
xvi
Role of health officer to ensure indoor air quality (IAQ):
PUBLIC HEALTH ISSUE:
Poor indoor air quality (IAQ) is caused by a number of factors and can cause a
variety of general symptoms, including headaches, eye irritation, sinus pain, and fatigue.
Poor IAQ can also exacerbate existing respiratory illness or intensify eye, ear, nose and
throat, conditions. Inappropriate air temperature or humidity levels can cause sinus
problems and general discomfort. Excessive amounts of carbon dioxide (CO2) from
inadequate ventilation (fresh air) can cause headaches and drowsiness. Although the
symptoms of poor indoor air can be debilitating, there is no current association with
cancer. Nuisance odors (e.g. septic, garbage) may not cause actual illness, but can
produce symptoms of irritation among certain sensitive individuals.
Perhaps the greatest health concerns are from exposure to carbon monoxide (CO)
poisoning, which can cause headaches, nausea, unconsciousness and, eventually, death,
as well as radon and asbestos which may pose an increased risk for cancer.
ROLE OF THE HEALTH OFFICER:
• Investigate complaints of poor indoor air quality to ensure that they are not related to
septic problems or poor sanitation.
• Encourage all symptomatic or ill persons to visit a primary care physician.
Two important areas of concern for Indoor Air Quality include ventilation control and
pollution source control.
VENTILATION/FRESH AIR:
Ventilation is a process by which outside fresh air is passed inside a building by
mechanical fans, or enters passively through open windows or doors. If enough fresh air is
not brought into a building, many sources of pollution inside can be concentrated. Air
comfort qualities such as temperature and humidity are also important concerns in
building ventilation.
The goal should be to balance the temperature in each room to accommodate all
occupants and maintain the humidity levels at a range above 30% in order to reduce the
likelihood of the occupant‟s nasal passages drying out, and below 50% in order to control
the growth of molds.
Testing of ventilation needs to be performed by a heating expert or environmental
consultant with a CO2 meter and airflow gauge.

Gender and Social Norms
17
POLLUTION SOURCES:
There are many sources of potential reservoirs for indoor air pollutants, including
polluted air being drawn into a building from outdoors. The most common sources of
indoor pollution include:
1) cleaning materials, paints and solvents;
2) new building materials and carpets;
3) allergens, such as dust mites or mold spores; and
4) faulty heating system exhausts.
The first two pollution sources can usually be discovered by discussing the recent
history of building renovations and investigating chemical storage areas for leaks or
mishandling. An environmental consultant may need to be hired to measure the air for
specific chemicals, which may be associated with the occupant‟s symptoms or a nuisance
odor.
Allergens and faulty heating systems can be less obvious and will require a trained
professional to evaluate, identify and mitigate the problems. Allergens are found in
enclosed, dark or damp areas. These allergens then spread throughout the building via
the air ventilation system. A common reservoir for dust mites is carpeting or upholstery,
which has become wet and was not dried or cleaned properly afterwards. If allergens
build up to a high level, they may create allergic rhinitis (runny nose, itchy eyes), or lead
to asthmatic attacks in sensitive individuals.
Mold spores can grow in damp fabrics, but will also grow in any standing water,
humidity drip pan, refrigerator, heater or other area where water collects. Wet areas
need to be dried and controlled with disinfectants to avoid allergen growth.
Faulty heating systems are the most dangerous of indoor air pollutants, due to the
acute toxicity (poisoning) of exhaust fumes. The primary hazard, carbon monoxide, can
cause dizziness, nausea, headaches, and drowsiness, and at high levels can lead to coma
and death. Problems can arise from leaking ovens, incomplete combustion. Carbon
monoxide can be measured with a quantitative gauge,
GASES Pollution.
Air is a mixture of gases. The normal composition of air by volume is: Nitrogen
(78.1%), Oxygen (20.93%) and Carbon dioxide (0.03%). The balance is made of other gases
which occur in traces e.g. argon, neon, krypton, xenon and helium. In addition to these
gases, air also contains water vapor, traces of ammonia and suspended matter such as

Gender and Social Norms
xviii
dust, bacteria, spores and vegetables debris. Any change in air composition causes air
pollution.
The main hazards of gases affect mainly the respiratory tract and may cause
asphyxia which is life threatening and some gases may also cause systematic
manifestations in the form of poisoning
Gases causing asphyxia are classified according to their health effects into asphyxiant as
simple, irritant and toxic gases.
A. Asphyxiant Gases
1. Simple asphyxiants:
These are inert gases that act by replacing oxygen in the air. Rapid death occurs when oxygen falls
below 10%. Examples of gases related to this group are methane, butane and helium.
Such gases can arise and pollute air in work places and at home
2. Chemical asphyxiants:
These are gases that affect the respiratory mechanism and examples of these gases: carbon
monoxide that combine with the hemoglobin giving carboxy-hemoglobin that is not suitable to carry
oxygen (hemoglobin has more than 210 times affinity to carbon monoxide than to oxygen) and so the
blood is unable to supply the tissue with enough oxygen.
The second one is hydrogen sulfide that inhibits the respiratory center and so the respiratory
mechanism is affected as the center can not control the respiratory muscles properly.
The third one is hydrogen cyanide that inhibits cytochrome oxidase that is responsible for
extraction of the oxygen from the blood by the tissue.
3-Irritant gases
Examples of these gases are ammonia and chlorine which are upper respiratory tract irritant
and nitrogen oxides that are lower respiratory tract irritants. The irritant gases act mainly by initiating
excessive mucus secretion of the respiratory tract causing block and it may also irritate the smooth
muscles fibres of the respiratory tract causing bronchospasm.
Clinical picture due to exposure to asphyxiant gases:
General clinical picture:
Dyspnea.
Blurring of vision.
Delirium, confusion and hallucination.
Arrhythmia and anginal pain.

Gender and Social Norms
19
Easy fatigability and muscle aches.
Specific clinica picture:
1-Cough, sneezing, rhinohea, lacrimation,wheeze and skin irritation specially among those exposed to
irritant gases.
2-Cyanosis except in case of CO exposure, the mucous membrane is red in colour.
First Aid of a human being suffering of asphyxia due to gas exposure:
Carry him away from the source of exposure to a well- ventilated place.
Release all the tight clothes.
Oxygen supply in case of CO exposure, oxygen supply should be under pressure.
Open the air way by removing any foreign object in the mouth and extend the neck and apply
cardio-pulmonary resuscitation if it is needed.
B-Systematic toxicant gases:
1-Arsine
It is a coloreless non irritant gas.
It is used in semiconductor industry.
It causes red blood corpuscles hemolysis.
It causes renal failure.
Clinical manifestations of exposure are in the form of triad of abdominal pain, hematuria
and jaundice.
2-Phosphine
Colorless gas with an odor of decaying fish.
It is an irritant gas.
Clinical pictures of acute poisoning: headache, vertigo, parasthesia, abdominal
pain,tenesmus,nausea,vomiting,convulsions and coma.
Air pollution by dust
Exposure to dust is mainly in the work place. Dust can be classified in different ways
1-According to its allergic effect: Dust can cause bronchial asthma (for example wood and
flowers dust) and even it can cause allergy to skin and eyes and other types of dust are
inert.
2-According to its ability to initiate fibrosis: Certain dust as silica can initiate lung fibrosis
and this group of lung disorders are named pneumoconiosis. Other type of dust as cement
Gender and Social Norms
xx
cannot initiate lung fibrosis and they are inert dust do not cause progressive lung fibrosis
and even there may be some opacities in the X rays but the lung function tests are usually
normal.
3-Dust can be classified according to its nature; inorganic dust as in case of silicosis and
organic dust as in extrinsic allergic alveolitis.
Examples of diseases caused by different types of dust exposure:
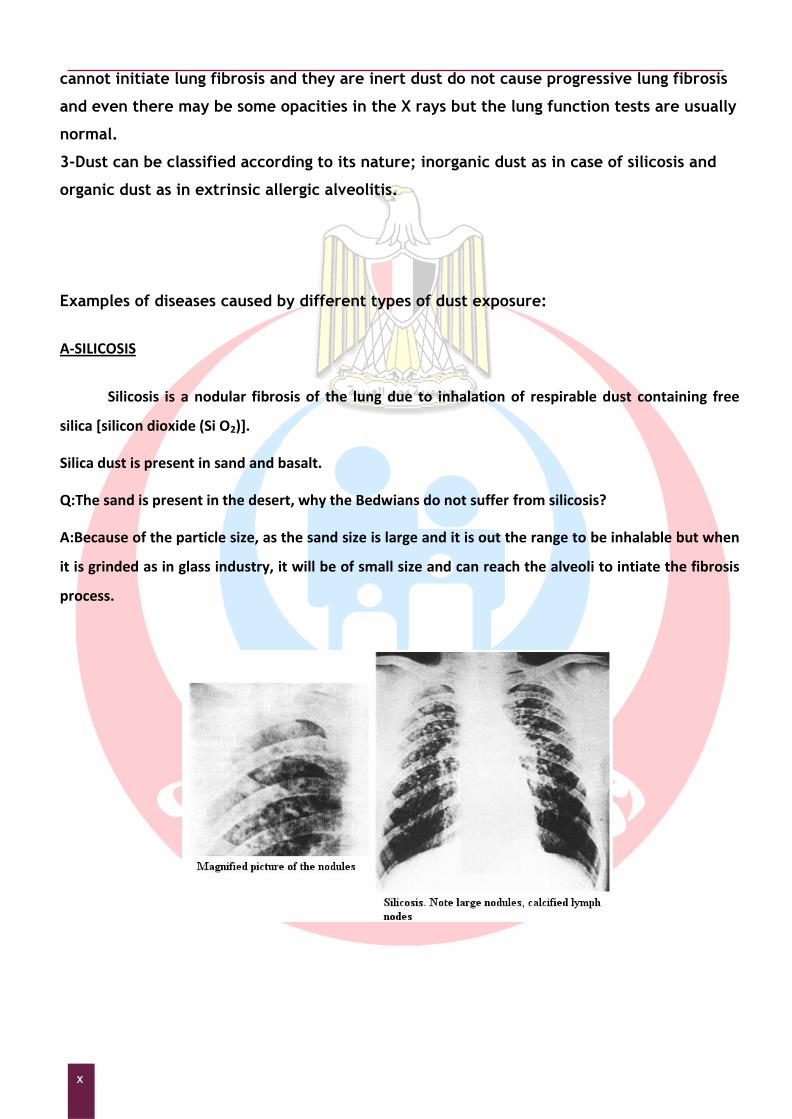
A-SILICOSIS
Silicosis is a nodular fibrosis of the lung due to inhalation of respirable dust containing free
silica [silicon dioxide (Si O2)].
Silica dust is present in sand and basalt.
Q:The sand is present in the desert, why the Bedwians do not suffer from silicosis?
A:Because of the particle size, as the sand size is large and it is out the range to be inhalable but when
it is grinded as in glass industry, it will be of small size and can reach the alveoli to intiate the fibrosis
process.

Gender and Social Norms
21
B-Diseases due to Exposure to Organic Dust
EXTRINSIC ALLERGIC ALVEOLITIS
(antigen antibody reaction at the alveoli)
Examples:
1. Farmers lung: caused by exposure to spores of the fungi (Micropolyspora faeni,
Thermoactinomyces vulgaris) found on the mouldy hay.
2. Bagassosis: caused by exposure to spores of the fungi "Thermoactinomyces sacchari" found on the
stored bagass in the wood and paper industry.
It begins by an inflammatory process in the form of granulomatous pneumonitis that occasionally
undergoes organization leading to interstitial fibrosis and thickening of the alveolo-capillary
membrane.
Clinical presentation of extrinsic allergic alveolitis:
Acute form is infrequent and it occurs in work place and rarely to occur among general
people
Chronic form:
Symptoms and signs of lung fibrosis and deficiency of gas transfer due to thickening of alveolar septa.
Usually follow repeated of subclinical attacks. This will result in dyspnoea, easy fatigaility and finger
clubbing
Diagnosed by:
1.Serology and immunology: mainly IgG precipitating antibodies against suspected antigens or by
Intradermal test.
2.Pulmonary function tests: mainly Co transfer factor is diminished.
Diagnosis of lung diseases and disorders
due to exposure to air pollution
1-History of exposure to a pollutant and this needs environmental monitoring to detect
the environmental pollutant. Frequent samples should be taken frequently at different
times and seasons. The samples are analysed for the type of the pollutant and its
concentration to see if it exceeds maximal allowable concentration and the international
Gender and Social Norms
xxii
standars. In case of dust, in addition the dust should be analysed chemically and the
particle size should be assessed to confirm if the present particle dist is inhalable or not.
These samples can be analysed in different ways one of them is through gas
chromatography and there are rapid methods to detect the presence of gas by gas tube
detector methods.
2-Clinical picture:
Symptoms: cough, expectoration, dyspnea, wheeze, fever and easily fatigability.
Examination: Inspection for any bulging or retraction and movement of chest.
Palpaction: to detect trachea centralization, tenderness……….
Percussion: to detect dulness indicating collapse or consolidation or space occupying
lesions
Aucultation: to evaluate air entry, wheeze indicating bronchospasm.
3-X ray ray of the chest: both posteranterior view and lateral view and comments on:
Centralization of the trachea.
Cardiac size and configuration.
Increase of bronchovascular markings.
Lung translucency.
Hilar lymph nodes concerning size and calcification.
Opacities, concerning distribution in the upper or the lower part part of the lung,
shape of the opacities (regular or irregular) and size of the opacities in mm.
Shape of the diaphram, if it is elevated or depressed or tenting due to traction by
fibrosis.
The pleura: If it is thickened, or encloses fluid or air or blood or pus as in case of
pleural effusion, empyema or pneumothorax.
4-Pulmonary functions:
These functions are used to detect any lung abnormalities concerning lung volumes
and air flow and cannot be used to diagnose specific diseases.
The most important disorders diagnosed by pulmonary function tests:
1-Restrictive lesions as in mass occupying lesions, pneumothorax, pleural effusion and
collapse and in this case Forced vital capacity /predicted vital capacity *100 (FVC/PVC
*100) is less than 75%.
2-Obstructive lesions as in bronchial asthma, chronic bronchitis and emphysema in which
the forced expiratory volume in 1st second/forced vital capacity*100 (FEV1/FVC*100) is
less than 75%.
Others form of pulmonary function tests:

Gender and Social Norms
23
1-CO (carbon monoxide) transfer factor is used to diagnose thickened alveolo-capillary
membrane (diffusing capacity) as in farmer‟s lung and it depends on determination of CO
in blood then allow the patient to breathe in a container in which there is certain
percentage of CO, the reevaluate CO level in blood. If the percentage in blood increases,
this means that alveolo-capillary membrane is normal allowing gas transfer across the
membrane. If the percentage does not increase it indicates thickness of the alveolo-
capillary membrane with impairment of gas exchange across the membrane.
2-Peak expiratory flow rate (PEF): it is used to diagnose obstructive lesion.
Procedure of pulmonary function tests:
The Device used to measure pulmonary function The vitalogram (the
curve from which the FEV1 and FVC can be measured)
NB: The air volume is plotted on the vertical axis while the time in seconds is plotted
on the horizontal axis.
1-Release any tight clothes.
2-Take deep inspiration.
3-Put the mouth piece and it is sealed by lips to avoid air leakage and close the nose by a
clip.
4-Expire the air into the device as fast and as strong as possible to the end.
5-You will obtain a curve as illustrated above in which the air volume in liters (vertical
axis) is plotted against the time in seconds (horizontal axis).
6-FEV1 is the volume of air on the curve expired at the end of the 1st second.
7-FVC is the maximal point on the curve.
8-PVC is obtained from special tables or charts and it depends on age, sex and height and
it represents the expected normal vital capacity for the person according to his height,
age and sex.
Gender and Social Norms
xxiv
Global effects due to air pollution
Acid rain which occurs when emissions of sulfur dioxide and nitrogen oxides in the
atmosphere react with water, oxygen, and oxidants to form acidic compounds (sulfuric
and nitric acid).The main sources of these pollutants are vehicles and industry and
power-generating machines. These compounds fall to the earth in either dry form (gas
and particles) or wet form (rain, snow, and fog).
Effects of acid rain:
1-Acid rain can damage vegetation and human structures.
2-Acid rain often falls on areas distant to the pollution source.
The greenhouse effect due to combustion of carbonic compounds causing
increase of temperature and rise of sea water level and increase of microbe
multiplication. Global warming is caused by increased concentrations of greenhouse
gases in the atmosphere, resulting from activities such as burning of fossil fuels. A
greenhouse gas is a gas in an atmosphere that traps heat and light from the sun in
the earth‟s atmosphere, which increases the temperature. The primary
greenhouse gases in the Earth's atmosphere are water vapor, carbon dioxide and
methane .
Effects of global warming resulting from greenhouse effect:
1. Global warming makes the sea rise, and when the sea rises, the water covers many low land
islands. The water covers the plants and causes some of them to die. When they die, the animals
lose a source of food.
2. Global warming causes the sea water to warm and ice in the north and south will dissolve.The
algae in the ocean may be killed causing loss of balance in the environment .
Depletion of atmospheric ozone with hazardous effect of ultraviolet rays as
the ozone layer prevent penetration and passage of large dose of harmful
ultraviolet rays with its hazards on the skin and the eyes.
Radioactive disaster: this may occur due to nuclear plant accident with release
of radioactive material. The radioactive cloud is very dangerous and permanent and
temporary evacuation of the area depends on:
1- The type of radiation as the particulate radiation is of low
penetrating power and therefore, it is enough for the man to cover
himself with a blanket, while in case of electromagnetic radiation,
there should be evacuation and covering with blanket is not enough
as this type of radiation is of high penetrating power.
Gender and Social Norms
25
2- The half-life period as if the half-life period is short, temporary
evacuation is enough as after passage of the radioactive cloud there
will be no radioactive traces because isotope will decay while if it is
long there should be permanent evacuation as the soil and water
source are polluted.
Dioxins problems:
Dioxins are a group of toxic chemicals with similar structure and variant
toxicity as polychlorinated Biphenyls and poly chlorinated dibenzo
dioxins. The main source of this group is uncontrolled incineration,
smoking, vehicle exhaust fumes and metal smelting. It is absorbed mainly
through eating animal fat where it is stored in animals. According to
WHO, the main health hazards include:
1-Damage to immune and reproductive system.
2-Diabetes mellitus.
3-Increase risk of cancer.
4-Chloracne.

Gender and Social Norms
xxvi
Heat Cooling power of air:
Definition: The ability of air to accept and to receive the continuous flow of heat loss
from the body.
The body get heat from the surrounding through:
Radiation.
Conduction.
In addition the body get heat from interior through metabolism.
The body loose heat through the following:
Radiation.
Conduction.
Sweating.
Hence the equation of heat balance is: Metabolism ±Radiation ±Conduction-Evaporation is
constant
Measurement of cooling power of air:
By Kata thermometer which is an alcohol thermometer which consists of a bulb
filled with colored alcohol and a stem with 2 markings and small upper reservoir. The bulb
is heated till the alcohol is raised to the upper reservoir. Then it is suspended in air and
the time is calculated in seconds starting from the column at the upper marking till fall to
the lower marking. A factor F is written on the stem.
The cooling power of the air is F/ the time taken in seconds= the cooling power of the air
in millicalories/cm2 /second.
The optimal cooling power of air is 5-7 millicalories/cm2 /second depending of the season.
It is 5 in summer and 7 in winter.
The factors affecting cooling power of air:
1-Air temperature and the optimal air temperature is 18o. It is measure by regular
thermometer.
2-Air movement and the optimal air velocity is 30 feet/ minute. It is measured by
Chapter 4:Physical Agents Affecting Environment

Gender and Social Norms
27
anemometer.
3-Relative humidity and the optimal relative humidity is 60% and it is measured by sling
psychrometer.
Indicators of heat strain:
1-Body temperature and it is measured per rectum or from the ear.
2-Pulse rate and it should not exceed 40 beats above the resting pulse.
3-Sweat rate: It should not exceed 1-1.5 L/hour.
Heat disorders:
1-Heat exhaustion and head syncope: they are due to excessive water and salt loss
and sever cutaneous vasodilatation with pooling of blood in the skin. In syncope there is
insufficient cerebral blood flow and the individual may fall down. In heat syncope, the
sever cutaneous vasodilatation is due to the direct effect of heat on the skin and the
reflex initiated by stimulation of nerve endings in the skin by the heat and controlled by
heat regulating center in the hypothalamus and mediated by cardiovascular center in
medulla oblongata. In exhaustion the body temperature is mostly normal and the skin is
wet as the sweating mechanism is still acting and the exhaustion is due to excessive loss
of sodium chloride and water. The treatment requires removal of the patient from
exposure to heat and fluid and electrolytes replacement.
2-Heat cramps: they are painful contraction of actively working muscles and this is
due to excessive loss of sodium chloride due to excessive sweating. The treatment is to
correct electrolytes and fluid balance, analgesics and antagonizing movement of the
affected group of muscles.
3-Sweat rash: in the form of cutaneous vesicles and papules due to occlusion and
swelling of the sweat glands ducts on the skin surface.
4-Heat stroke: It is due to failure of heat regulating center in the hypothalamus and is
characterized by hyperthermia above 40 Co, dry skin, oliguria, convulsions, arrhythmia
and heart failure. The treatment is in the form of removal of the patient from exposure to
high temperature, remove the clothes, water spray on the skin, and expose the body to
cool air current. Do not apply enforced cooling by ice as it may cause hypothermia and do
not use salicylates to lower the body temperature as such drugs are working through heat
regulating center which is fatigued.
Radiation
Radiation is classified into Non ionizing radiation and ionizing radiation.
A- Non ionizing radiation: It induces its action through heating but does not affect atom stability.
1-Infrared radiation: Occurs on exposure to extremely hot red objects. The most health

Gender and Social Norms
xxviii
hazards of exposure to infra-red radiation is the production of posterior polar cataract.
2-Ultra-violet radiation: The exposure occurs as in Photocopy machines and Photo therapy of
skin disorders. It affects skin starting from skin erythem up to skin cancer as well as it affects the
eye specially the retina.
B-Ionizing radiation: Ionizing radiation induces free radicals which attacks the cell constituents. This
induces lipid peroxidation of the unsaturated fatty acids of the endoplasmic reticulum and destruction
of the DNA of the nucleus. It is classified into:
B/1- Particulates as alpha and beta and they are characterized by high ionizing power and less
penetrating distance.
B/2-Electromagnetic as X rays used in medical diagnosis and gamma rays used in airport to inspect the
luggages. They are characterized by low ionizing power and far penetrating distance.
Health hazards of ionizing radiation:
Acute Effect:
This occurs if there is radioactive disaster.
It is due to exposure of whole body to large dose of radiation in short period.
The tissue that are mainly affected are those whose cells are characterized by rapidy
multiplication as:
1-Skin: with skin burns.
2-Mucosa of gastrointestinal tract: hyperameia and ulceration leading to GIT bleeding,
water and electrolyte loss and disturbence.
3-Bone marrow depression: decrease in RBCs number leading to anemia.
Decrease in platelets number leading to bleeding tendency.
Decrease in white blood cells leading to repeated attacks of bleeding.
Treatment is mainly by fluid and electrolyte replacement, fresh blood transfusion or packed
RBCs if there is no bleeding tendency and umberella of antibiotic.
Chronic effect:
Decrease life span.
Increase senelity feature.
Increase possibility of cancers.
Increase possibility of chromosomal aberrations and genetic malformation.
Effect on lung: interstitial fibrosis and pleurisy.

Gender and Social Norms
29
Effect on heart: pericarditis.
Effect on kidney interstitial fibrosis.
Effect on bone: bone marrow depression and periosteitis.
CNS is resistant to radiation and if it is affected, this will be through its blood supply.
Environmental monitoring for radiation
This is done by Geiger counter to measure the amount of radiation in the environment to
which the individual is exposed.
Geiger.
Noise Noise is unwanted sound irritating the human being
Sound is an energy perceived by ear due to vibrating a solid object in an elastic media creating a
series of compression and rarifaction wwaves.
Sound has to main measurements:
Frequency which is the number of complete waves in a second and measured in Hertz (Hz)
and it determines the sound pitch.
Intensity and it is measured in deciBell (dB) and it determines the sound loundness.
To measure hearing acuity of a man an audiogram is drawn in which the intensity of sound
heard by the man at different frequencies is plotted on a curve.
Audiogram on which the sound intensity Sound lever meter to monitor sound level

Gender and Social Norms
xxx
(on vertical axis) is plotted agaist
different frequencies on horizontal axis .
If the above curve or part of it is shifted downword,
this means some sort of deafness.
Health hazards of exposure to noise:
A-Auditory effect:
1-Noise induced hearing loss if the man is exposed to a noise more than 90dB for a long
time.
2-Conductive deafness due to drum rupture if the man is exposed to a very loud noise
above 130 dB.
B-Extra-auditory effect:
1-Heart rate is affected.
2-Respiratory rate is affected.
3-Peipheral vasoconstriction with hypertension.
4-Psychological disturbance as irritability, nervousness and fatigue.
Q: How to protect workers working in a noisy place for a long time?
A: this is done by using the below devices to minimize the noise.

Gender and Social Norms
31
Water pollution may affect drinking water. In many developing countries, it is usually a leading cause of death, by people drinking from polluted water sources.
Water pollution occurs when pollutants (particles, chemicals or substances that make
water contaminated) are discharged directly or indirectly into water bodies without
enough treatment to get rid of harmful compounds. Water pollution is the second most
imperative environmental concern along with air pollution.
Water pollution is defined as any change or modification in the physical, chemical and
biological properties of water that will have a detrimental consequence on living
things.
Sources of water supply (surface water as river or underground)
In cities and large town the water supply is through a pipe network and the water is
portable while in some condition the water supply is from wells and there are 2 types of
wells (deep and superficial)
Deep well Shallow well
Depth Above 20 meters Around 7 meters
Pumping Mechanically Manual
Physically My be turbid Clear
Hardness Very hard Moderate
Pollution Difficult to be polluted Can be contaminated from surface
Use Public supply in some
villages
Limited use in some private areas
Sources of water pollution:
1-Nearby latrines.
2-Nearby refuse source.
3-Infiltration from cultivated land as by pesticides.
Chapter 5:Water Pollution

Gender and Social Norms
xxxii
4-Factory waste disposal and this is a big problem in surface water. In developing
countries, 70% of industrial wastes are dumped untreated into waters where they pollute
the water supply.
5-Throw of dead animals and this is also a problem in surface water.
6-Underground storage and tube leakages:
Many liquid products (petroleum products) are stored in metal and steel tubes underground.
Other sewage systems run in underground tubes. Overtime, they rust and begin to leak. If that
happens, they contaminate the soils and the liquids in them end up in many nearby water sources.
7- Atmospheric factors play a role in air pollution by depositing the air pollutants into water. When air
is polluted with sulphur dioxide and nitrogen oxide, they mix with water particles in the air and form a
toxic substance. This falls as acid rain to the ground. The result is that water also get contaminated
and this affects animals and water organisms. Moreover, the toxic fumes coming from vehicles play a
role in water pollution. These fumes go up into the air and settle then taking up the form of soot. The
soot being heavy, is brought down to the ground and seep into the water, thus destroying the water
ecology.
How to prevent water pollution:
1. Avoid disposing waste into water.
2. Take care of the vehicles to avoid air pollution that in turn will pollute water.
3. Plant more trees. They prevent global warming as well as other forms of pollution.
4. The rules, policies and laws regarding water purification systems need to be made
strong and should not be broken down. Treatment of the waste of industry needs to be
a mandatory and not an option.
5. Use a detergent that has low phosphate levels because high phosphate levels cause
added pollution and are hazardous to the animals and plants in the water.
Steps of water purification:
1- Water intake: If water is taken from liver it should be from an area with minimal
pollution.
2- Coagulation and sedimentation: to adsorb suspended matter that is precipitated
easily.
3- To remove suspended matters and by this process a large percentage of bacteria,
parasitic ova and cysts are removed.
Gender and Social Norms
33
4- Disinfection to kill any pathogenic agents and this is done by chlorination and even
a residual chlorine is left to kill any bacterial contamination through water
distribution. In normal condition 0.6 ppm chlorine is added to filtered water and
left for a contact time of 30 minutes leaving a residual part of 0.2ppm, but in water
borne outbreak the residual chlorine is raised to 0.4ppm chlorine.
Monitoring water samples:
Problems of water sampling:
1. The sample may not be representative of the water source of interest. Many water sources vary
with time and with location. The measurement of interest may vary with distances from the water
source with overlying atmosphere and underlying or confining soil.
2. The sample taken from the water source may react with the container. Sample containers must be
made of materials with minimal reactivity with substances and pre-cleaning of sample containers
is important.
A gas chromatograph- mass spectrometer
Measures pesticides and other organic pollutants
Sanitary standards of portable water:
WHO (1993 and 1996) recommended standard for portable water. These recommendations should be
considered with respect to environmental, social, economic and cultural conditions.
A-Physical:
Colorless, odorless, clear and tasteless. Water quality is judged by its physical
characteristics.
Drinking water should be free from turbidity and color.
Gender and Social Norms
xxxiv
It should also have acceptable taste and odor that could be caused from
contamination by chemicals, or as a by-product of water treatment (e.g.
chlorination).
Hardness is defined as the soap-destroying power of water. It is classified into:
1-Carbonate “temporary” is due to the presence of calcium and magnesium
bicarbonates.
2-Non-carbonate “permanent” is due to calcium and magnesium sulphates.
B- Chemical:
The maximal allowable standards are as follow:
Item Standard
Total solids 500-1000 ppm
PH Slightly alkaline or slightly around
neutral point.
Hardness Total 20o while permanent should not
exceed 4o
Ammonia .05ppm
Organic
Albuminoid ammonia .1ppm
Nitrites Nil
Nitrates 1ppm
Metals
Zinc 15ppm
Copper 3ppm

Gender and Social Norms
35
Lead 0.1ppm
Iron 0.3ppm
B/1-Inorganic constituents:
Ammonia: Ammonia in water is an indicator of possible bacterial, sewage and
animal waste pollution.
pH : the acceptable pH is between 6.5 to 8.5,
Q: What does happen if PH is less than 6.5?
A: less pH could cause corrosion of metals of the distribution pipes (lead).
Q: What does happen if PH is above 8.5?
A: above 8.5 cause decrease in the efficiency of the chlorine disinfection process.
Hydrogen sulfide: may be noticeable in some ground water and in stagnant drinking
water in the distribution system, this is due to depletion and the subsequent
reduction of sulphate.
Dissolved oxygen: depletion of dissolved oxygen in water supplies can encourage
microbial reduction of nitrates to nitrite and sulphate to sulphide.
B/2-Organic constituents: (The following substances should be concerned as they are
carcinogenic)
Pesticides : The pesticides that are of importance in connection with water quality
include chlorinated hydrocarbons and their derivatives.
Polynuclear aromatic hydrocarbons.
C- Microbial aspect:
In general:
Total bacterial count:100 organisms /ml
Presumptive coliform: absent in 100 ml of filtered chlorinated water.
The following shows some details
C/1-Ideally drinking water should not contain any microorganisms known to be
pathogenic.
. Those at greatest risk of water - borne diseases are infants and young children,
people who are debilitated or living under insanitary conditions, the sick and the
elderly. For them the infective dose is significantly lower than for the healthy
population.
C/2-The primary bacteria is the coliform group, including both fecal and non – fecal

Gender and Social Norms
xxxvi
organisms. Typical example of the fecal group is E. coil and of the non – fecal group
klebssiella aerogens .In Drinking water: E.coli and total coliform bacteria must not be
detectable in any 100 ml sample of water.
C/3- Virological aspects:
Drinking - water should be free from any viruses infectious to man.
C/4-Parasitological aspects:
Drinking water should not contain any pathogenic intestinal protozoa. Rapid and slow
sand filtration is effective in removing a high proportion of pathogenic intestinal
protozoa.
D- Radiological Aspects
- Drinking water should be free from any source of radiation.
Indicators of water pollution:
1-Bacteriologically: E coli, Streptococcus faecalis and Closstridium welchii are normal
inhabitants of the intestine but their presence indicates contamination with fecal
materials. E coli is the type of choice for bacteriological examination. It is detected by
culture on liquid Mac-Conkey and it is detected by presence of acid and gas and the
organism is known as lactose fermenter.
2- Chemically: Nitrite test is important as nitrites are intermediate decomposition
products indicating an ongoing process of contamination.
Water fortification to avoid malnutrition:
1-Water can be fortified by iodine in endemic area of goiter, but now salt is a
more important vehicle to carry iodine.
2- Fluoridation (by adding sodium fluoride as primary prevention of dental caries
Water related diseases, health hazards and environmental
dissociation:
An insanitary water supply may be a source of many health hazards and this can be
summarized in the following points:
1-Water bore infection and in case of epidemic, the epidemic curve is in the form of
common source epidemic. People can get diseases such as hepatitis by eating seafood that
has been polluted. In many poor nations, there is always outbreak of cholera and diseases
as a result of poor drinking water treatment from contaminated waters. Every year, there
are an estimated 3–5 million cholera cases and 100,000–120,000 deaths due to cholera.
(WHO estimates that only 5–10% of cases are officially reported.

Gender and Social Norms
37
2- Lead poisoning is a common problems where lead pipes or connection are used in the
pipes network. This may lead to plumbism.
3- Health hazards of radioactive effect if the water is contaminated by radioactive
materials.
4- Dental caries if the fluoride content of water is less than 0.1ppm. If the fluoride
content is more than1.5 ppm it may cause fluorosis.
5-Methemoglobinemia in young infants if there excessive nitrates more than 20 ppm.
6- Animals, including water animals die when water is poisoned for various reasons. Other
animals are stressed and their populations are endangered.
7-Disruption of food-chains: Pollution disrupts the natural food chain as well. Pollutants
such as lead and cadmium are eaten by tiny animals. Later, these animals are consumed
by fish and shellfish, and the food chain continues to be disrupted at all higher levels.
There is a historical story in Japan concerning this, as a factory was discharging its waste
containing cadmium into a lake from where the people were getting their drinking water.
This water was used in irrigating rice crops. So cadmium reached to people and deposited
in their bones causing osteomalacia with severe pain and multiple fractures. Another
story a waste containing mercury was discharged into water. Mercury was stored in fish
bodies and reached to human causing mercury toxicity.

Gender and Social Norms
xxxvi
Waste Disposal
Definition of waste:
Waste can be defined as something which the owner no longer wants it at given
place and time.
Refuse is the solid waste materials originating from houses, hospitals and factories and in some references the liquid waste is called sewage.
The hospital waste should be disposed with special care and this will be discussed later. The factories waste should be treated perfectly before disposal to avoid the chemical health hazards.
Solid Refuse Disposal Health hazards of insanitary domestic solid waste disposal:
1-Infection.
2-Flies and different insect breeding.
3-Rodents breeding.
4-Irritation and allergy.
5-Fire.
6-Source of chemicals and radiation hazards.
Waste is a source of spreading infection through the following:
1-Airborne dust contaminated with microorganisms causing droplet infection as in
tuberculosis. It can also cause wound contamination through contact mode of infection as
in tetanus.
2-Flies breeding causing spreading of infection as the flies transmit the organisms
mechanically from one place to another.
3-Rodents breeding as they are sources for many diseases as plaque and salmonella
transmission.
4-pollution of subsoil water that may pollute underground water.
5-Animals infection that will transmit diseases to human beings (Zoonosis).
6-Hand contamination that will transmit the infection to eyes, contaminate food or
contact wound causing wound infection.
Chapter 6 : Waste Disposal
Solid Waste Sewage
Hospital Waste

Gender and Social Norms
39
Different methods of sanitary solid waste disposal:
1-Incineration which is suitable for hospital waste disposal but not suitable to manage
large amount of waste.
2-Controlled dumping:
The waste is put in the dump and covered by about 20 cm of earth and left to settle down
before putting another layer of waste and the land may be used as playing yards till
complete settlement when it can be used for building.
Sewage
It is a combination of the different liquid wastes arising from different activities of
human life
Effect of insanitary waste disposal:
1-Infection.
2-Flies breeding.
3-Mosquitoes breeding on water collection.
4-Offensive odor.
5-Rodents breeding.
6-Pollution of subsoil water that may pollute underground water.
7-Chemical poisoning by polluting the underground water.
Different methods of final sewage disposal:
1-Disposal at sea but this method requires certain precautions under strict condition.
2-Sedimentation and filtration: It is in the form of screening by grit chambers, then
sedimentation and finally it is divided into 3 layers: sludge at the bottom, scum at the top
and crude effluent in between. The sludge may be digested, and the crude effluent may
be used in farm irrigation.
3- Activated sludge: In the form of screening then the sludge is activated in certain tanks
by adding activated sludge to give aerobic bacteria and exposed to compressed air. Then
it pass to settlement tanks to be separated into sludge (returned to new process) and
clear effluent (used in farm irrigation).

Gender and Social Norms
xl
It is clear that insanitary solid waste or sewage disposal result in insect
breeding that will be summarized in the following table:
The insect The disease
House flies Food borne diseases.
Eye infection.
Wound infection.
Cockroaches Food borne diseases.
Mosquitoes Anopheles: malaria.
Culex: Filaria and west Nile fever.
Aedes: Yellow fever.
Sanflies Leishmaniasis
Ticks Q fever
Relapsing fever.
Hospital Waste
Improper hospital waste disposal may cause several hazardous effect.
Definition of hospital waste:
Medical waste is defined as materials generated as a result of patient diagnosis or
treatment.
Infectious waste is defined as the portion of medical waste that could transmit an
infections.
According to the World Health Organization recommendations, hospital waste is
classified into eight main categories:
1. General waste: is any substance that do not need a special handling.
2. Pathological waste: consists of any tissue or fluid of the body.
3. Radioactive waste: includes any waste contaminated with radioactive materials.
4. Infectious waste contains pathogens in sufficient concentration or quantity causing
infections.
5. Chemical waste comprises any chemical substance. It may be hazardous (as toxic,
flammable and genotoxic substances) and non-hazardous chemical waste ( as some
amino acids, organic and inorganic salts)
6. Pharmaceutical waste: It includes drugs.
7. Pressurized containers: such as aerosol cans.

Gender and Social Norms
41
Hospital Waste management
A waste management plan should address four components of waste management:
1. Sorting:
Sorting is separating waste by type (e.g., infectious waste, pharmaceutical
waste) into color coded bags at the place where it is generated. Never discard
needles and sharps in soft waste bags, as the housekeeping staff might get
injured. Medical waste containers should be cleaned.
2. Handling:
Handle medical waste as little as possible. Medical waste and sharps
containers should be discarded when they are three quarters full or at least once
per day. Never put hands into a container of medical waste.
3. Temporary storage:
Never store medical waste in open containers. Never throw waste into an
open pile.
4. Final disposal:
The following precautions should be concerned
1. There must be special trolley or any transportation method that is assigned
specially for waste with regular cleaning.
2. Incineration is the preferred methods for hazardous waste.
3. Radio-active waste must be kept in special containers (lead) and put under
control of the governmental agency
4. General waste: once segregation had been carried out no need for incineration
and managed as any domestic waste.
5. Recycling is preferred for general waste or pressurized containers which are not
infectious.
6. Pharmaceutical waste must return to the pharmacy in the hospital to deal with.
Impact on Health
The hazards of hospital waste arise if not hygienically managed:
A. To the patient: may cause nosocomial infection.
B. To the workers in the hospitals: nosocomial infection may occur also among health
care workers.
C. To the environment there is a risk of contamination of air and soil in and outside
hospital environment.

Gender and Social Norms
xlii
Legislation for Egypt
In Egypt we have a law from Egyptian Environmental Affairs Agency in 1994 that
stresses the prevention of handling of dangerous waste without a license from the
responsible administrative area. This law must be put into action with good supervision.

Gender and Social Norms
43
Food is liable to be contaminated during production, distribution, cooking and storage.
Food is a potential source for infection, poisoning, allergy and other special
diseases and food sanitation aims at prevention of food borne diseases and
poisoning.
Food borne diseases
Classification according to causative
agent
Diseases
Viral Gastroenteritis and viral hepatitis
Parasitic Amoebic dysentery, Ascaris, Tinea
soleum, Tinea saginata
Bacteria Salmonella (Typhoid and para typhoid),
bacillary dysentery, Brucella, E coli
diarrhea, Food poisoning
Food allergy Eggs, banana and milk may cause allergy
Food poisoning It may be chemical or of bacterial origin
Special condition Favism which is a hemolytic disorder
Food adulteration:
This may be done by addition of some substances, substitution and
abstraction.
1- Example of addition is starch addition to milk and this can be detected by iodine
that produce blue color.
Chapter 7:Food Sanitation
Gender and Social Norms
xliv
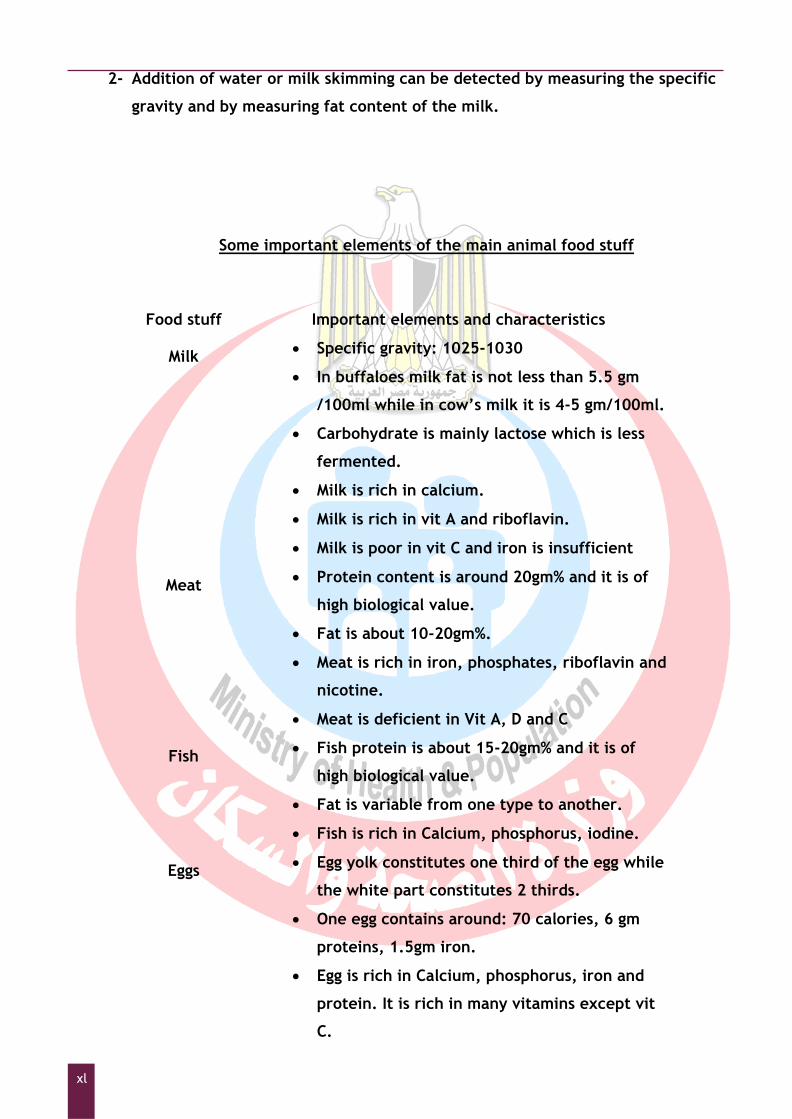
2- Addition of water or milk skimming can be detected by measuring the specific
gravity and by measuring fat content of the milk.
Some important elements of the main animal food stuff
Food stuff Important elements and characteristics
Milk Specific gravity: 1025-1030
In buffaloes milk fat is not less than 5.5 gm
/100ml while in cow‟s milk it is 4-5 gm/100ml.
Carbohydrate is mainly lactose which is less
fermented.
Milk is rich in calcium.
Milk is rich in vit A and riboflavin.
Milk is poor in vit C and iron is insufficient
Meat Protein content is around 20gm% and it is of
high biological value.
Fat is about 10-20gm%.
Meat is rich in iron, phosphates, riboflavin and
nicotine.
Meat is deficient in Vit A, D and C
Fish Fish protein is about 15-20gm% and it is of
high biological value.
Fat is variable from one type to another.
Fish is rich in Calcium, phosphorus, iodine.
Eggs Egg yolk constitutes one third of the egg while
the white part constitutes 2 thirds.
One egg contains around: 70 calories, 6 gm
proteins, 1.5gm iron.
Egg is rich in Calcium, phosphorus, iron and
protein. It is rich in many vitamins except vit
C.

Gender and Social Norms
45
Disease transmitted through different food staff under insanitary condition:
1-Milk borne diseases:
Tuberculosis, brucellosis, salmonellosis, Staphylococcal, streptococcal and
intestinal anthrax.
2-Cattle meat:
Tuberculosis, salmonellosis, brucellosis and taenia saginata.
3- Pigs meat:
Tuberculosis, salmonellosis, brucellosis , taenia solium and trichinosis
4-Poultry:
Salmonellosis.
5-Fish:
Heterophyes heterophyes and Diphyllobothrium latum.
5-Eggs:
Samonellosis
Any food service providers must fulfill the following criteria:
1. Comply with all applicable local standards and regulations.
2. Ensure that food establishment managers are trained and certified as food service managers.
3. Report all foodborne illness complaints promptly to the local health authority.
Food service employees must: Report to the Food Services Manager any information about their health and
activities as they relate to diseases transmissible through food, including:
o diarrhea, vomiting, or other acute gastrointestinal illness
o jaundice
o infected wound, boil, or other lesion containing pus on the hands, wrists, or exposed portions of the arms.
o Salmonella, Shigella, Escherichia coli (E. coli), or other enteric bacterial pathogen
o Hepatitis A virus.
Food service managers must:
1. Fulfill the requirements of local law to obtain Food Service Manager.
2. Provide proof of certification.

Gender and Social Norms
xlvi
3. Notify local health authority of any food employee reporting any of the symptoms or illnesses covered above.
4. Maintain a record of all employee reports of illness, which must be available for review by local health authority.
5. Participate in training, continuing education and/or re-certification, as needed, and regulated by local health authority.
Emergency Closure of Food Service Facility If following an on-site inspection, it was recommended that closure of a food facility is
required in order to protect environmental or public health, local health authority will order the immediate closure of the facility in writing. The order will:
Identify the food type.
Describe the specific reasons why emergency closure is needed.
List the corrections which are necessary before the establishment can be re-opened.
The person receiving the order must close the facility and request all customers to vacate. The facility will remain closed until local health authority end the order for emergency closure.
Food poisoning
Definition
Consumption of contaminated food may cause food poisoning including heavy metal
intoxication, poison of plant origin like ergot alkaloids, poison of animal and toxins of
bacterial origin.
Frequent causes of foodborne illnesses are:
1) Toxins elaborated by bacterial growth in the food before consumption (Clostridium
botulinum, Staphylococcus aureus and Bacillus cereus; or in the intestines (Clostridium
perfringens).
2) Toxins produced by harmful algal species (ciguatera fish poisoning, paralytic,
neurotoxic, diarrheic or amnesic shellfish poisoning) or present in specific species (puffer
fish poisoning).
Prevention of food poisoning
Principles:
avoiding food contamination.
destroying or denaturing contaminants.
preventing further spread or multiplication of these contaminants.

Gender and Social Norms
47
educating food handlers about proper practices in cooking and storage of food.
personal hygiene.
WHO document concerning food sanitation:
1. Keep Clean.
2. Separate raw and cooked.
3. Cook thoroughly.
4. Keep food at safe temperatures.
5. Use safe water and raw materials.
Staphylococcal Food Intoxication
It is intoxication characterized by sudden onset of severe nausea, cramps, vomiting,
diarrhea sometimes with subnormal temperature and lowered blood pressure, it
may extend for one or two days.
Several enterotoxins of staphylococcus aureus. They are produced by the organism
which multiplies in food. The toxins are stable at boiling temperature, (heat-
resistance enterotoxins).
Reservoir of infection is man: the organism is found in nose, throat, or septic skin
lesion, infected udders of animal which leads to milk contamination.
Mode of transmission is by ingestion of food products containing staphylococcus
enterotoxin, food is contaminated during handling followed by inadequate heating
or refrigeration such as pastries, custards, creams, and salad. Food remains at room
temperature for several hours before being eaten so the staphylococcus multiplies
and produces the heat stable toxin.
Incubation Period is from 30 minutes to 8 hours usually 2-4 hours.
Salmonella Food Poisoning
It is enterocolitis of sudden onset of headache, abdominal pain, diarrhea, nausea
and fever is always present.
It is caused by Salmonella typhi murium and Salmonella enteritidis.
Reservoir of infection and contamination are Poultry, cattle, rodents, turtles,
chicks, dogs, human cases or carriers.
Mode of Transmission is by ingestion of inadequately cooked meat from infected
animal, ingestion of eggs, or milk contaminated by organism from man or animal.
There is a chance for person to person transmission.
Gender and Social Norms
xlviii
Incubation Period is from 12-36 hours.
Clostridium Perfringens Food Intoxication
It is a mild disease of short duration with sudden onset of colic, abdominal cramps,
diarrhea, nausea and vomiting, fever is usually absent.
It is caused by type A strain of Clostridium perfringens (C. welchii) which is an
anaerobic organism. The disease is caused by elaboration of toxins from spores.
The spores are present in soil and gastrointestinal tract of healthy persons and
animals.
Mode of transmission is by ingestion of food that was contaminated by soil or faeces
of man or animal and held on condition that permit multiplication of the organism,
this occurs with inadequate heating of the meat and poultry, the spores survive and
germinate through gradual slow cooling.
Incubation Period is 10 –12 hours.
Botulism
It is severe intoxication from preformed toxins present in contaminated food. The
illness is characterized by acute bilateral cranial nerve impairment and descending
weakness or paralysis, visual disturbance and dysphasia vomiting and diarrhea may
be present before neurological manifestations. Fever is absent. It is diagnosed by
the presence of toxin from incriminated food or from stool, serum or gastric
aspirate of infected persons.
Infectious agent and its characteristics:
1. Toxin of clostridium botulinum is produced by a spore forming anaerobic bacillus.
2. Toxin is produced in improperly canned low acid and alkaline foods.
3. Toxin is destroyed by boiling, inactivation and destruction of spores require a
higher temperature (116°C).
4. Resistance of spores to heat sterilization is reduced at a low PH.
Reservoir: Spores are present in the soil and intestinal tract of animal.
Mode of transmission is through ingestion of food in which toxin has been formed,
enhanced by inadequate heating during canning or inadequate cooking.
Incubation Period: neurological manifestation appears within 12-36 hours may
extend to days. The shorter the incubation period the more severe the disease.
Gender and Social Norms
49
1. In classic botulism, the GIT tract should be emptied of still unabsorbed toxins by
emesis or gastric lavage.
Ten golden rules for safe food preparation:
1. Choose foods processed for safety.
2. Cook food thoroughly.
3. Eat cooked food immediately.
4. Store cooked foods carefully.
5. Reheat cooked food thoroughly.
6. Avoid contact between raw food and cooked food.
7. Wash hands repeatedly.
8. Keep all kitchen surfaces strictly clean.
9. Protect food from insects, rodents and other animals.
10. Use safe water.
Control measures for food poisoning:
1. Discard incriminated food in a sanitary manner.
2. Concurrent disinfection of all surfaces and served utensils.
3. Specific treatment with fluid replacement and proper medication for cases.
Milk sanitation:
There are three pillars for milk sanitation:
1-The animal itself as the cattle may be a source of tuberculosis or brucellosis.
2-The containers in which the milk is received.
3-The human-being who is milking the animal and he may be the source of infection if he
is suffering from hand infection or upper respiratory tract infection.
Milk sterilization:
1-By boiling through raising the temperature to 100o or above for about 5 minutes. This
method will kill all the bacteria but it destroys some food items and decreases its nutritive
value.
2-Pasteurization which will kill most of the bacteria including heat resistant bacteria. It
preserves the nutritive value of milk.
Characteristics of milk borne epidemic
1-Wide spread and explosive especially among middle class.
2-Affects infants, pregnant mothers and old age as they are the vulnerable groups
consuming milk.
3-Affect families consuming milk from the same source.

Gender and Social Norms
l
4-The infections usually have shorter incubation period.
5-The epidemic will decrease and disappear by well control of the milk source.

Gender and Social Norms
51
The surrounding social events, at home and workplace and even in the street, affect the human physically, emotionally and psychologically
When the human is under stress the body response by secreting adrenaline and increasing cholesterol and sugar levels in the bloodstream. The response to environmental stress is related to:
a) Individual vulnerability:
Personality structure.
Age.
Previous experience.
Health status of the individual.
b) Social factors:
Family life: as his relation with his family members and his responsibilities.
Social support outside. If there is a support from his friends, family members or
colleagues, this will help him to cope with the stress situations.
If the individual fails to cope with stress factors this will be manifested as follows:
Health Effects of environmental Stress
1- Early Warning Signs of environmental Stress:
Headache, Sleep disturbances, Difficulty in concentration and Low morale 2- Long Term effects of environmental Stress:
A. Physical effect
Coronary artery disease as well as hypertension, and strokes
Gastrointestinal Disease as peptic ulcer, ulcerative colitis and Spastic
colon.
Other diseases as Diabetes, Headaches and Asthma.
B. Psychological effects
The psychological effects of stress range from mild subjective symptoms to psychiatric disease.
C. Behavioral changes
Behavioral changes may also occur in response to environmental stress as: Diminished participation in family or social activities.
Tobacco consumption.
Alcohol & substance abuse.
Alterations in appetite and eating behavior.
Chapter 8:Social Environment
Gender and Social Norms
lii
Definitions related to environmental health and formulated from the above mentioned law
Article 1: In the application of the provisions of this Law, the following words and expressions shall have the meanings hereby assigned to them: 1. Environment:
The biosphere which encompasses living organisms together with the substances it contains and the air, water and soil that surround it, as well as the establishments set up by man.
2. Air: The mixture of gases constituting air in its known percentages and natural properties, and in the provisions of this Law, it is the ambient air, air within the work places, and air in closed or semi-closed public places.
3. The Convention: The International Convention for the Prevention of Marine Pollution from Ships (1973-1978), and international conventions, to which the Arab Republic of Egypt adheres, in the area of the protection of the marine environment from pollution and compensation for pollution accidents.
4. Public Place: A place equipped to receive people or a specific category of people for any purpose.
5. Closed Public Place: A public place which is in the form of an integrated building that receives no incoming air except from designated inlets. Vehicles for public transport are considered closed public places.
6. Semi-closed Public Place: A public place which is in the form of a non-integrated building with direct access to the ambient air and which cannot be completely closed.
7. Environmental Pollution: Any change in environmental properties which may result directly or indirectly in harming living organisms or establishments or in affecting the ability of people to lead a normal life.
8. Environmental Degradation: Effect on the environment that reduces its value, or changes its nature, depletes its resources or harms living organisms or monuments.
9. Environmental Protection: Protecting and promoting the components of the environment and preventing or reducing their degradation or pollution. These components encompass air, seas, internal waters, including the river Nile, lakes and subterranean water, land, natural protectorates, and other natural resources.
10. Air Pollution: Any change in the properties or specifications of the natural air which causes hazards to human health or to the environment, whether resulting from natural
Chapter 9: LAW NUMBER 4 OF 1994
PROMULGATING THE ENVIRONMENT LAW, Egypt

Gender and Social Norms
53
factors or human activities, including noise. 11. Rapid Transport Vehicles:
Motor cars, tractors, motorcycles and other machines designed for use on public roads.
12. Water Pollution: The introduction of any substance or energy into the water environment, whether intentionally or unintentionally, directly or indirectly, which causes damage to living or non-living resources, poses a threat to human health or hinders water activities, fishing and tourist activities or impairs the quality of sea water so as to render it unfit for use, diminish the enjoyment thereof or alter its properties.
13. Polluting Substances and Factors: Any solid, liquid or gaseous substances, noise, radiation, heat, or vibrations arising from acts of man that lead directly or indirectly to environmental pollution or degradation.
14. Water Polluting Substances: Any substance whose discharge into the water environment, intentionally or unintentionally, leads to a change in its properties, or contributes to such change directly or indirectly to an extent that can harm man, natural resources, sea water or marine tourist areas, or which interferes with other legitimate uses of the sea. These substances include: A- Oil or oily mixtures. B- Harmful and dangerous wastes as determined in the international conventions to
which the Arab Republic of Egypt adheres. C- Any other substance (solid, liquid or gaseous) as determined in the executive
regulations of this law. D- Untreated industrial waste or effluents from industrial establishments. E- Toxic military containers. F- Substances listed in the Convention and its annexes.
15. Oil: Crude oil and its products in all forms, including any kind of liquid hydrocarbons, lubricating oil, fuel oil, refined oil, furnace oil, tar and other petroleum derivatives or waste.
16. Oily Mixtures: Any mixture containing oil in a ratio of more than 15: 1,000,000.
17. Unclean Balancing Water (Unclean Ballast Water): Water in ship-borne tanks if its oil content is greater than 15:1,000,000.
18. Hazardous Substances: Substances having dangerous properties which are hazardous to human health, or which adversely affect the environment, such as contagious, toxic, explosive or flammable substances or those with ionizing radiation.
19. Hazardous Waste: Waste of activities and processes or its ashes which retain the properties of hazardous substances and have no subsequent original or alternative uses, like clinical waste from medical treatments or the waste resulting from the manufacture of any pharmaceutical products, drugs, organic solvents, printing fluid, dyes and painting materials.
20. Substance Handling: Anything that leads to the displacement of substances for the purpose of assembling, transporting, storing, treating, or using them.
21. Waste Management: Collecting, transporting, recycling and disposing of waste.
22. Waste Disposal: Processes which do not extract or recycle waste such as composting, deep

Gender and Social Norms
liv
subterranean injection, discharge to surface water, biological treatment, physio-chemical treatment, permanent storage or incineration.
23. Waste Recycling: Processes which allow the extraction or recycling of waste, such as using it as fuel, or extracting metals and organic materials or soil treatment or oil re-refining.
24. Liquid Substances Harmful to the Water Environment: The substances listed in the International Convention of 1973/1978.
25. Reception Facilities: Installations, equipment and basins designed to receive, filter, treat and dispose of
contaminated substances or ballast water, as well as installations provided by companies working in the field of shipping and unloading petroleum products; or other administrative agencies supervising ports and waterways.
26. Discharge: Any leakage, effusion, emission, draining or disposal of any kind of pollutants into the
waters of the territorial sea, the exclusive economic zone, the sea, the river Nile and the waterways, taking into consideration the levels determined for certain substances in the executive regulations.
27. Dumping: A- Any deliberate disposal of polluting substances or waste from ships, planes,
platforms or other industrial establishments and land-based sources into the territorial sea, the exclusive economic zone or the sea.
B- Any deliberate dumping by ships or industrial or other establishments into the territorial sea, the exclusive economic zone or the sea.
28. Compensation: Means compensation for the damage resulting from pollution accidents in accordance
with the application of the provisions of the Civil Code and the provisions of the International Convention on Civil Liability to which the Arab Republic of Egypt adheres or to which it will adhere in future, including the International Convention on Civil Liability for Damage Caused by Oil Pollution Accidents signed in Brussels in 1969, or any other pollution accidents mentioned in the executive regulations of this Law.
29. Means of Oil Transport: Every pipeline used in transporting oil and any other equipment used in loading,
unloading or transporting oil, as well as pumps or other equipment required for the use of these pipes.
30. Ship: Any floating marine vessel of any type, vessels which move over hydrofoil cushions or
underwater establishments. Also, any fixed or mobile establishment constructed along the coasts or on surface water for the purpose of conducting commercial, industrial, touristic or scientific activities.
31. War Ship: Any ship that belongs to the armed forces of a state, carrying its distinct external insignia, under the command of an officer officially appointed by the government of such state and operated by a crew governed by the rules of military discipline of that state.
32. Government Ship: A ship owned by the state and operated or used for governmental and non-commercial
purposes. 33. Harmful Materials Carrier:
A ship constructed originally or redesigned for the purpose of carrying cargoes of harmful liquid substances in bulk, including oil tankers when fully or partially loaded with harmful liquid substances not packed in accordance with the provisions stated in Chapter One, Part Three of this Law.

Gender and Social Norms
55
34. Establishment: Establishment means the following: - Industrial establishments subject to the provisions of Law No. 21 of 1958 and Law No.
55 of 1977. - Tourist establishments subject to the provisions of Law No. 1 of 1973 and Law No. 1
of 1992. - Establishments used for electrical power generation and production which are under
the provisions of laws Nos. 145/1948, 63/1974, 12/1976, 13/1976, 27/1976, and 103/1986.
- Mines, quarries and establishments operating in the field of oil exploration, drilling, transportation and usage which are subject to the provisions of laws Nos. 66/1953, 86/1956, 61/1958 and 4/1988.
- All infrastructure projects. - Any other establishment, activity or project which may have a noticeable impact on
the environment . These shall be determined by a decision issued by the Environmental Affairs Agency in agreement with the competent administrative authority.
35. Environmental Monitoring Networks: Agencies which undertake, within their spheres of competence and through their
stations and work units, to monitor the components and pollutants of the environment and relay their results and data to the competent authorities periodically.
36. Environmental Impact Assessment: Studying and analyzing the environmental feasibility of proposed projects, whose
construction or activities might affect the safety of the environment in order to protect it.
37. Environmental Disaster: An accident resulting from natural factors or human action which causes severe
damage to the environment and requires resources beyond the local means. 38. The competent Administrative Agency Concerned with the Protection of the Water Environment:
Any of the following agencies, each within its field of competence: A- The Environmental Affairs Agency (EEAA) B- The Department of Ports and Lighthouses. C- The Suez Canal Authority. D- Port Authorities in ARE. E- The General Egyptian Organization for the Protection of the Coast. F- Egyptian General Petroleum Corporation. (EGPC).
G- General Department of Surface Water Police. H- Tourism Development Authority. I- Other agencies designated by a Prime Ministerial Decree.

Gender and Social Norms
lvi
ANNEX (5)
MAXIMUM LIMITS OF OUTDOOR AIR POLLUTANTS
(MICROGRAM PER CUBIC METER)
POLLUTANT
MAXIMUM LIMIT EXPOSURE PERIOD
Sulphur Dioxide
350
150
60
1 hr
24 hrs
1 year
Carbon Monoxide
30 Milligrams/cubic
meter
10 Milligrams/cubic
meter
1 hr
8 hr
Nitrogen Dioxide
400
150
1 hr
24 hrs
Ozone
200
120
1 hr
8 hr
Suspended
Particles Measured
as Black Smokes
150
60
24 hrs
1 year
Total Suspended
Particles (TSP)
230
90
24 hrs
1 year
Respirable Particles
(Pm 10)
70 24 hrs
Lead 1 year
1 1 year
Chapter 10:Reports and exercises
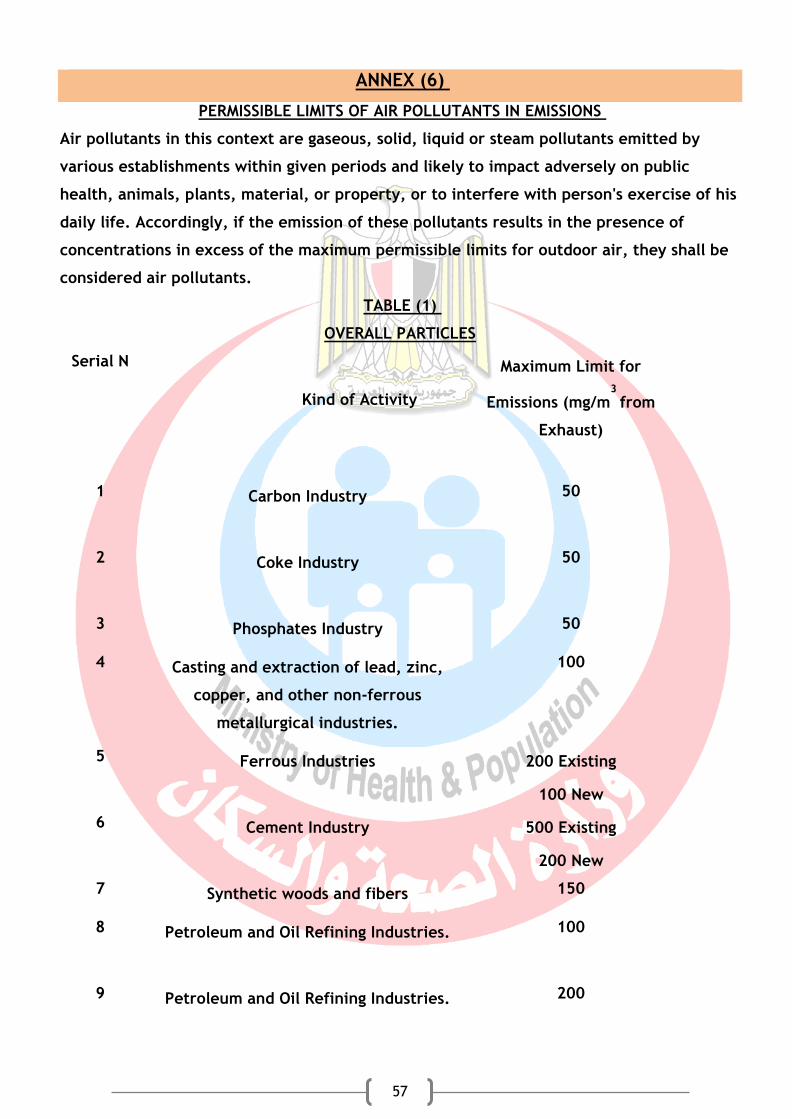
Gender and Social Norms
57
ANNEX (6)
PERMISSIBLE LIMITS OF AIR POLLUTANTS IN EMISSIONS
Air pollutants in this context are gaseous, solid, liquid or steam pollutants emitted by
various establishments within given periods and likely to impact adversely on public
health, animals, plants, material, or property, or to interfere with person's exercise of his
daily life. Accordingly, if the emission of these pollutants results in the presence of
concentrations in excess of the maximum permissible limits for outdoor air, they shall be
considered air pollutants.
TABLE (1)
OVERALL PARTICLES
Serial N
Kind of Activity
Maximum Limit for
Emissions (mg/m3
from
Exhaust)
1 Carbon Industry
50
2 Coke Industry
50
3 Phosphates Industry 50
4 Casting and extraction of lead, zinc,
copper, and other non-ferrous
metallurgical industries.
100
5 Ferrous Industries 200 Existing
100 New
6 Cement Industry 500 Existing
200 New
7 Synthetic woods and fibers 150
8 Petroleum and Oil Refining Industries.
100
9 Petroleum and Oil Refining Industries.
200

Gender and Social Norms
lviii
THRESHOLD LIMITS OF
EXPOSURE TO MINERAL DUSTS
1- SILICA - SILICON DIOXIDE:
A- CRYSTALLIZED:
Quartz: Threshold limits (million particles per cubic foot)
300
= ______________________________________
Percentage of Quartz Concentration in dust + 10
Threshold limits of Inhalable dusts (LESS THAN 5 MICRONS) (mg/m3
)
10 mg/m3
= __________________________________________
Percentage of Quartz Concentration in dust + 2
Threshold limits of total dust (mg/m3
)
30 mg/m3
= ___________________________________________
Percentage of Quartz Concentration in dust + 3
CRISTOBALITE AND CRI STOBALITE AND TRIDYMITE : Half the value calculated for Quartz shall be used.
B- UNCRYSTALLIZED SILICA
Threshold limits
20 Million particles per
cubic foot
2- ASBESTOS: Asbestos dusts with fibers lengths of more than 5 microns.
AMOSITE 0.5 of fibers per cm3
of air
CROCIDOLITE 0.2 of fibers per cm3
of air
OTHER KINDS 2 of the fibers per
cm3 of air
3- TALC: FIBROUS TYPE: 2 fibers per cm3 of air
NON FIBROUS TYPE: 20 million particles
per cubic foot of air
4-MICA: 20 million particles per cubic foot of air

Gender and Social Norms
59
ANNEX (7)
PERMISSIBLE LIMITS OF SOUND INTENSITY
AND PERIODS OF SAFE EXPOSURE
TABLE (1)
Intensity of sound inside the work place
and closed places: *
Maximum permissible noise levels inside places
of productive activities:
No TYPE OF PLACE AND
ACTIVITY
MAXIMUM PERMISSIBLE
NOISE [level equivalent
to decibel (A)]
1. Work place with up to 8
hour shifts and aiming to
limit noise hazards on
sense of hearing
90
2. Work place where
acoustic signals and good
audibility are required
80
3. Work rooms for the
follow up, measurement
and adjustment of high
performance operations
65
4. Work rooms for
computers, typewriters
or similar equipment
70
5. Work rooms for activities
requiring routine mental
concentration
60
Maximum permissible period for exposure to noise in the work place (factories and
workshops):
* The value given hereafter is indicated on the basis of not affecting the sense of hearing.
- Intensity of noise shall not exceed 90 decibels (A) during a daily 8-hour work shift.

Gender and Social Norms
lx
- In case of increasing noise level intensity over 90 dB (A), the period of exposure must be
reduced according to the following table:
Noise intensity level decibel
95 100 105 110 115
Period of exposure (hour)
4 2 1 1/2 1/4
- In case of exposure to different noise intensity levels of over 90 decibels:
(1) For intermittent periods during a shift, the result must not exceed:
(A1 + A2 + ....) over the integer one
B1 B2
whereas:
A the period of exposure to a specific level of noise (hour).
B the permissible period of exposure at the same noise level (hour)
- In case of exposure to intermittent noise emanating from sledgehammers:
Depends on the exposure period (number of impacts during the daily shift) according to
noise intensity as per the following table:
Noise intensity (Decibel)
Number of permissible impacts during
the daily working hours
135 300
130 1000
125 3000
120 10000
115 30000
Noise issuing from sledgehammers shall be considered intermittent if the period
between impacts is one second or more. If the period is less, the noise shall be considered
continuous and subject to the preceding items.
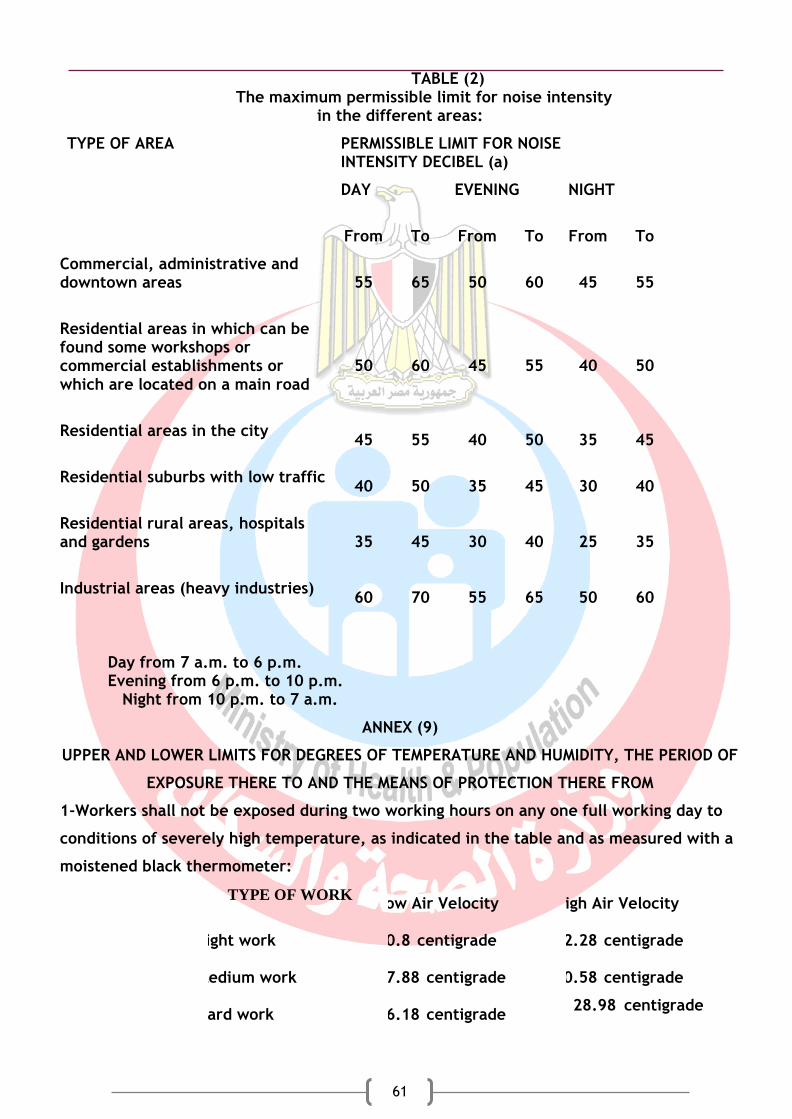
Gender and Social Norms
61
TABLE (2) The maximum permissible limit for noise intensity
in the different areas:
TYPE OF AREA
PERMISSIBLE LIMIT FOR NOISE INTENSITY DECIBEL (a)
DAY
EVENING NIGHT
From To From To From To
Commercial, administrative and downtown areas
55 65 50 60 45 55
Residential areas in which can be found some workshops or commercial establishments or which are located on a main road
50 60 45 55 40 50
Residential areas in the city
45 55 40 50 35 45
Residential suburbs with low traffic
40 50 35 45 30 40
Residential rural areas, hospitals and gardens
35 45 30 40 25 35
Industrial areas (heavy industries)
60 70 55 65 50 60
Day from 7 a.m. to 6 p.m. Evening from 6 p.m. to 10 p.m.
Night from 10 p.m. to 7 a.m.
ANNEX (9)
UPPER AND LOWER LIMITS FOR DEGREES OF TEMPERATURE AND HUMIDITY, THE PERIOD OF
EXPOSURE THERE TO AND THE MEANS OF PROTECTION THERE FROM
1-Workers shall not be exposed during two working hours on any one full working day to
conditions of severely high temperature, as indicated in the table and as measured with a
moistened black thermometer:
TYPE OF WORK Low Air Velocity High Air Velocity
Light work 30.8 centigrade 32.28 centigrade
Medium work 27.88 centigrade 30.58 centigrade
Hard work 26.18 centigrade 28.98 centigrade

Gender and Social Norms
lxii
2-A worker may not be allowed to work without precautionary supervision when exposed
to high temperature levels.
3- If any worker is exposed for a period of one continuous or intermittent hour during
two working hours to working conditions of extreme temperature in excess of 26.18
centigrade for men and 24.58 centigrade for women, one or more of the following
methods shall be used to ensure that the worker's internal temperature does not rise.
(A) Acclimatizing the worker to the temperature over a period of six days by
exposing him/her to 5% of the daily exposure period on the first working day
then increasing the period of exposure by 10% a day until it reaches 100% on
the sixth day.
(B) A worker who is absent for a period of nine days or more after the
acclimatization process or who falls ill for a period of four consecutive days
must be re-acclimatized over a period of four days by being exposed to 50%
of the daily exposure period on the first day and an additional 20% a day
thereafter so as to reach 100% exposure on the fourth day.
4- Organizing working hours to reduce the physiological stress on the worker and enable
him to get adequate rest between the working hours.
5- Distributing the total period of work evenly on the same day.
6- Scheduling work so that jobs exposed to high temperatures are shifted to the coolest
periods of the day.
7- Scheduling short rest breaks at least once every hour to enable workers to drink a
saline solution. Each worker shall be given a minimum of 2 litres of potable water in
which 0.1% salt is dissolved (without giving salt pills), and the water supply must
not be far than 60 meters from the workers.
8- Providing and using suitable protective clothing and equipment.
MEDICALLY:
- Conducting medical examinations on workers exposed to high temperatures to ascertain
their tolerance levels, checking in particular their cardio -vascular, respiratory and
urinary systems, [liver, endocrine glands, skin and medical history, especially in regard to
heat-related diseases.
- Conducting periodic check-ups every two years for workers under the age of 46 who are
exposed to high temperature and every year for older workers.
- Presence of a trained health worker to observe and confront cases and diseases resulting
from heat during work, in addition to the availability of first aid facilities.
TRAINING:

Gender and Social Norms
63
Workers who are exposed to high temperatures must be informed of the following:
1- Importance of drinking water during work.
2- Importance of taking salts.
3- Importance of daily weighing of the body before starting work and at the end of duty.
4- The symptoms of the main diseases connected with heat exposure, e.g. dehydration,
drowsiness, exhaustion and cramps resulting from heat.
5- Dangers of any toxic substances or other physical hazards to which the worker is
exposed.
6- The importance of heat acclimatization (while recording the data concerning each
worker in a special file easily accessible to the worker).
Monitoring:
1- Placing a wet bulb thermometer (ordinary mercury thermometer with the mercury
reservoir wrapped in moistened gauze) in hot work places.
2- Using the black GLOB thermometer (mercury thermometer with the mercury reservoir
wrapped in black metal) in addition to the wet thermometer.
3-Waiting for half an hour before taking the reading of each thermometer.
4-Determining the black wet temperature degree from the equation:
Black wet thermometer temperature degree = 0.7 x reading of wet thermometer + 0.3 x
reading of GLOB thermometer

Gender and Social Norms
lxiv
Exercise 1 Source (exercise 1-6): Book of Department of Community, Environmental and Occupational Medicine, Faculty of Medicine, Ain Shams University. National Library Deposit No 20569/2010 K. Park Textbook of Preventive and Social Medicine. M/S Banarsidas Bhanot (India). 23ed.
The main role of the public health officer (health inspector) is to investigate an outbreak such as food poisoning or infectious disease.
Design a program to investigate an outbreak. The following handout can be used as guidelines:
Investigation of an Outbreak
An epidemic exists when there are more cases of a particular disease than expected in a given area, or among a specific group of people, over a particular period of time. When an epidemic occurs suddenly in a relatively limited geographical area, it is termed as “Outbreak”. In an outbreak or epidemic, the cases are usually related to one another or that they have a common cause.
The development and maintenance of a disease outbreak typically requires each of the following three characteristics:
1. The presence of a pathogen in sufficient quantities to affect multiple persons.
2. An appropriate mode of transmitting the pathogen to susceptible persons.
3. An adequate pool of susceptible persons who are exposed to the pathogen.
Public health officer must distinguish between two primary modes of transmission in acute outbreaks of diseases.
1- Person to person spread: occurs when the causal agent is transmitted from one
person to another e.g. Typhoid fever.
2- Common source exposure: occurs when the causal agent is transmitted to the
affected individuals by some shared features in the environment. e.g. consumption of
contaminated water or milk
Objectives of outbreak investigations
To control ongoing outbreaks.
To prevent future outbreaks.
To collect data about a disease.
Steps of an Outbreak Investigation:
1. Prepare for field work.
2. Verify the diagnosis.
3. Establish the existence of an outbreak.
4. Define and identify cases.
5. Describe and orient the data in terms of time, place, and person.
6. Develop hypotheses.
7. Evaluate hypotheses.
8. Refine hypotheses and carry out additional studies.
9. Implement control and prevention measures.
10. Communicate findings.

Gender and Social Norms
65
The steps are presented here in conceptual order. In practice, however, several may be done at the same time, or they may be done in a different order. For example, control measures should be implemented as soon as the source and mode of transmission are known, which may be early or late in any particular outbreak investigation.
Step 1: Prepare for Field Work
Review literature.
Prepare the supplies and equipment.
Consult laboratory staff.
Arrange for portable computer, camera.
Consult local staff.
Step 2: Verify the Diagnosis
Goal is to rule out misdiagnosis and laboratory error.
Examine case-patient(s) Visit and interview several people who became ill.
Review medical records Review clinical findings and laboratory results.
Confirm laboratory findings.
Step 3: Establish the Existence of an Outbreak
If current number of reported cases exceeds expected number, by comparing the current number of cases with the number from the previous few weeks or months, or from a comparable period during the previous few years.
The sources of these data vary:
For a notifiable disease use health department surveillance records.
For other diseases and conditions, find data from local sources such as hospital
discharge records, death (mortality) records, and cancer registries.
Many factors affect changes in total number of cases reported (pseudo-outbreak). Change in reporting procedures or case definition.
Increased local interest or public awareness.
Improved diagnostic procedures.
Changes in population size.
Step 4: Define and Identify Cases
a) Establish a case definition.
A case definition usually includes 4 components:
1. clinical information about the disease,
2. characteristics about the people who are affected,
3. information about the location or place, and
4. specify time during which the outbreak occurred.
Case finding through passive surveillance; or active surveillance
Ideally, case definition should be broad enough to include most, if not all, of the actual cases, without capturing what are called "false-positive" cases (when the case definition is met, but the person actually does not have the disease in question).

Gender and Social Norms
lxvi
Investigators often classify cases as one of the following:
Confirmed: usually has clinical & laboratory verification.
Probable: usually has clinical features without lab verification.
Possible: usually has fewer of typical clinical features.
b) Identify and count cases " to determine the true size and geographic extent of the problem".
Regardless of the particular disease you are investigating, the following types of information about every person affected should be collected:
Identifying information: This may include name, address, and telephone number
and allows you and other investigators to contact patients for additional questions
and to notify them of laboratory results and the outcome of the investigation.
Addresses also allow you to map the geographic extent of the problem.
Demographic information: This may include age, sex, race, and occupation to
characterize the population at risk.
Clinical information: This information allows you to verify that the case definition
has been met. Date of onset allows you to create a graph of the outbreak. Also,
clinical information may include whether the person was hospitalized or died to
describe the spectrum of illness.
Risk factor information: Information about risk factors as: Specific exposures, and
immunity status. For example, in an investigation of hepatitis A, ask about
exposure to food and water sources.
Traditionally, data collection through a standard case report form, questionnaire, or data abstraction form then abstract selected critical items in a table called a "line listing." In a line listing, each column represents an important variable, such as name or identification number, age, sex, and case classification, while each row represents a different case, by number. New cases are added to a line listing as they are identified.
Step 5: Describe and Orient the Data in Terms of Time, Place, and Person.
Characterize the outbreak by time, place, and person (descriptive epidemiology)
a) Characterizing by time
By drawing a graph of the number of cases by their date of onset. This graph, called an epidemic curve, or "epi curve" for short, gives a simple visual display of the outbreak's magnitude and time trend.
An epidemic curve is a line graph plotted during an epidemic describing the cumulative number of affected people in relation to the time of onset of clinical symptoms.
It is helpful in identification of the incubation period of illness and consequently identification of the causal agent, since different agents have characteristic incubation periods.
The overall shape of the epi curve can reveal the type of outbreak (the pattern of spread)
1- Common source
Continuous
Point source
Gender and Social Norms
67
2- Propagated
b) Characterizing by place Assessment of an outbreak by place provides information on the geographic extent of a problem and may also show clusters or patterns that provide clues to the identity and origins of the problem. A simple and useful technique for looking at geographic patterns is to plot, on a "spot map" of the area, where the affected people live, work, or may have been exposed.
c) Characterizing by person You determine what populations are at risk for the disease by characterizing an outbreak by person. We usually define such populations by personal characteristics (e.g., age, race, sex, or medical status) or by exposures (e.g., occupation, activities, use of medications, tobacco, drugs). These factors are important because they may be related to susceptibility to the disease and to opportunities for exposure.
Summarizing by time, place, and person After characterizing an outbreak by time, place, and person (descriptive epidemiology), investigator need to summarize what they know to see whether their initial hypotheses are on track.
Step 6: Develop Hypotheses
After describing the outbreak by time, place, and person, a hypotheses will be generated. The hypotheses should address the source of the agent, the mode of transmission, and the exposures that caused the disease.
Hypotheses may be based on:
Descriptive epidemiology - person, place and time
Interviews with affected people
Consultation with health officials in community
Step 7: Evaluate Hypotheses
By using analytic epidemiology to test hypotheses by using a comparison group to quantify
relationships between various exposures and the disease.
There are two types of analytic studies: cohort studies and case-control studies. Cohort studies compare groups of people who have been exposed to suspected risk factors with groups who have not been exposed. Case-control studies compare people with a disease (case-patients) with a group of people without the disease (controls). The nature of the outbreak determines which of these studies you will use.
a) Cohort studies
A cohort study is the best technique for analyzing an outbreak in a small, well-defined population.
The followings are the rates obtained by cohort study: Attack rate & relative risk
In cohort study you start by 2 groups. One group is exposed to the risk and the 2nd group not exposed and you follow them up to detect those who become diseased in each group.
1) Data needed:

Gender and Social Norms
lxviii
1. number of diseased among exposed,
2. number of no diseased among exposed,
3. number of diseased among not exposed,
4. number of non diseased among not exposed.
2) Make 2x2 table using these data- comparison groups are in rows
Diseased Not Diseased Totals
Exposed a b a+b
Not Exposed c d c+d
Total a+c b+d a+b+c+d
3) Calculate attack rates AR
1. AR exposed = a/(a+b)
2. AR not exposed = c/(c+d)
4) Calculate relative risk= RR
RR= AR exposed/ AR not exposed
RR= a/(a+b)
c/(c+d)
b) Case-control studies
In most outbreaks the population is not well defined, and so cohort studies are not
applicable. In these instances, you would use the case-control study design. In a case-
control study, you ask both case-patients and controls about their exposures.
In case control study you start by 2 groups. One group is diseased and the 2nd group is non
diseased and you ask about the history of exposure in each group.
The following is the rate obtained by case control study Odds ratio
1) Data needed:
1. number of exposed among diseased (cases)
2. number of not exposed among diseased (cases)
3. number of exposed among non-diseased(controls)
4. number of not exposed among non-diseased (controls)
2) Make 2x2 table using these data: comparison groups are in columns
diseased (cases) Non diseased (controls)
Totals
Exposed a b a+b
Not Exposed c d c+b
Total a+c b+d a+c+b+d
C) Calculate odds of exposure for each group
1. Odds for cases = a/c
Gender and Social Norms
69
2. Odds for controls= b/d
D) Calculate odds ratios (OR)
OR= odds of exposure for cases/ odds of exposure for controls
OR= a/c
b/d
OR= ad
bc (cross-product)
Testing statistical significance
Determine how likely the study results could have occurred by chance
Called testing for “statistical significance”
Steps to testing “statistical significance”
State null hypothesis – no association between exposure and outcome
Calculate chi-square test
Look up corresponding p-value in table of chi-squares.
The common cutoff point is .05 If the p-value is below the cutoff point, the finding is
considered “statistically significant” and the null hypothesis is rejected
The smaller the p-value, the stronger the evidence is for statistical significance
Q1 Which is study is more accurate?
A1 Cohort is more accurate.
Q2 Which study is more practical?
A2 Case control study is more practical.
Step 8: Refine Hypotheses and Carry out Additional Studies
When analytic epidemiological studies do not confirm the hypotheses, Laboratory and
environmental studies are needed to test the hypotheses.
Step 9: Implementing Control and Prevention Measures.
Control measures, which can be implemented early, should be aimed at specific
links in the chain of infection, the agent, the source, or the reservoir
Control measures are directed at interrupting transmission
Control strategies fall into four major categories of activity.
1. Prevention of exposure: the source of infection is reduced to prevent the disease
spreading to other members of the community.
2. Prevention of infection: susceptible groups are protected by vaccination.
3. Prevention of disease: high-risk groups are offered chemoprophylaxis.

Gender and Social Norms
lxx
4. Prevention of death: through prompt diagnosis and management of cases.
Step 10: Communicate Findings
The final task in an investigation is to communicate the findings to others through:
Oral briefings
Meetings
Written reports
The report should be as the following way:
Background of disease.
Historical data.
Methodology of investigation.
Analysis of data.
Control measures.
Exercise 2
There is an epidemic of air-borne disease like meningitis. Put a program to control such
epidemic.
You can use the following guideline:
1-Follow the general steps to confirm the presence of an outbreak.
2-You can be guided by the following points as epidemic measure to control air-borne
disease.
a-Isolation of cases (at home or hospital) and give treatment
b-Appropriate surveillance system for early case detection and prompt treatment.
c-Some control measures towards contacts are directed at reducing susceptibility,
such as immunizations,(active or passive) or chemoprophylaxis
d-Health education (Proper ventilation, spacing and prevention of over-crowding.)
NB: The are measures taken for:
1- The cases.
2- The contacts.
3- The environment.

Gender and Social Norms
71
Exercise 3
There is an epidemic of food-borne disease like typhoid. You detected that there is
a common source of infection which is water source. Put a program to control such
epidemic.
You can use the following guideline:
Epidemic measures for food-borne diseases
1. Super-chlorination of water supply, sanitary disposal of wastes, strict food and milk
sanitation.
2. Health education of the public for preventive measures.
3. Vaccination of population at risk.
4. Epidemiologic study, to trace the source (s) and methods of infection .
NB: In this case the measures are focusing on:
1- The environment which is water in this case.
2- The general population.
Exercise 4
In the above mentioned outbreaks, you have detected the cases. Now you can plot your
cases to design the epidemic curve.
You can use the following guideline to learn how to plot and interpret the curve then you
can design similar curves.
Epidemic curve
It is a histogram (a type of curves) that shows the course of a disease
outbreak or epidemic by plotting the number of cases by time of onset.
At the end you should learn the following characteristics of an outbreak:
1. Pattern of spread (is it common source pattern or propagating
pattern).
2. Magnitude of the epidemic.
3. Time trend (is there an increase or decrease of the case in addition,
it gives the date of 1st and last cases and the number of cases in
between.).
4. Exposure and/or disease incubation period.
5.
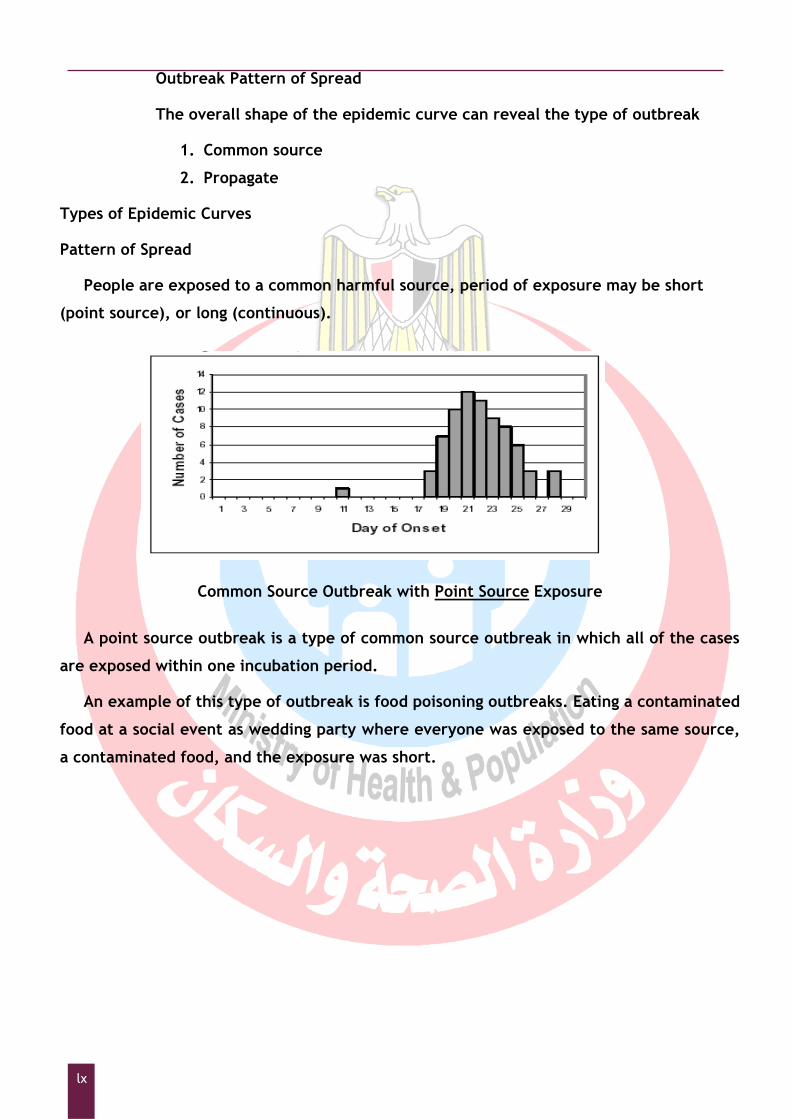
Gender and Social Norms
lxxii
Outbreak Pattern of Spread
The overall shape of the epidemic curve can reveal the type of outbreak
1. Common source
2. Propagate
Types of Epidemic Curves
Pattern of Spread
People are exposed to a common harmful source, period of exposure may be short
(point source), or long (continuous).
Common Source Outbreak with Point Source Exposure
A point source outbreak is a type of common source outbreak in which all of the cases
are exposed within one incubation period.
An example of this type of outbreak is food poisoning outbreaks. Eating a contaminated
food at a social event as wedding party where everyone was exposed to the same source,
a contaminated food, and the exposure was short.

Gender and Social Norms
73
Common Source Outbreak with Continuous Exposure
This graph shows an example of an epidemic curve for a common source outbreak with
continuous exposure. In this type of outbreak, the duration of exposure is relatively long
and often cases will rise gradually. It may occur over more than one incubation period.
An example of this type of outbreak could be a contaminated well used for drinking
water
Propagated Outbreak
This graph shows an example of an epidemic curve for “A propagated outbreak”. It
occurs when there is person-to-person spread.
This type of outbreak could occur, for example, with a disease such as Measles, in
which one infected person transmits the disease to several other people who, in turn,
infect even more people.
1. Outbreak Magnitude
– By counting the number of cases in certain period.

Gender and Social Norms
lxxiv
2. Outbreak Time Trend
An epidemic curve can provide:
1. Date of illness' onset for the first case.
2. Date when the outbreak peaked.
3. Date of illness onset for the last case.
3. Exposure and/or disease incubation period.
This can be calculated from point source epidemic.
a-Determining the timing of the exposure, If the incubation period of the disease is
known, epidemic curves can be used to estimate the timing of the exposure by:
– Counting back the median incubation period from the peak of the epidemic.
– Identifying last case and counting back maximum incubation period.
– Identifying first case and counting back minimum incubation period.
B-Determining the incubation Period
If the timing of the exposure is known, epidemic curves can be used to estimate the
incubation period of the disease. The time between the exposure and the peak of the
epidemic curve represents the median incubation period.
Exercise 5
Egypt has succeeded to be free from poliomyelitis and nowadays the strong program
to eradicate measles and rubella. Such programs depends mainly on 2 pillars:
1-Mass vaccination by potent vaccine.
2-Strong surveillance system.
Now, you are asked to design a surveillance system to be free from measles:
The following is a guide for surveillance system in general.
Surveillance System
Surveillance is a tool of epidemiological practices. It is defined as the ongoing systematic
collection, analysis and interpretation of health data. These data are essential for
planning, implementation and evaluation of public health practices. This is followed by
dissemination of data to the data collectors and health policy makers for feedback. From
that definition, it is clear that there is a link between surveillance and prevention and
control efforts. This is called the surveillance cycle, which is a continuous process that

Gender and Social Norms
75
rarely ends, e.g., when the Smallpox is eradicated.
Definition of terms used in case classification:
Case: A person who meets the case definition.
Case definition: A set of diagnostic criteria that must be fulfilled to be regarded as a case
of a particular disease. Case definitions can be based on clinical criteria, laboratory
criteria, or a combination of the two.
Suspect case: A case that is classified as suspected usually on a clinical basis, for reporting
purposes.
Probable case: A case that is classified as probable on clinical plus either epidemiologic or
laboratory criteria for reporting purposes.
Confirmed case: A case that is classified as confirmed usually on a laboratory basis for
reporting purposes.
Sources of surveillance data:
Vital statistics regarding mortality, fertility, marriage and divorce.
Health reports regarding morbidity data for notifiable diseases from hospitals,
private clinics and laboratories.
Hospital records.
Registries which may be:
a) Population-based registries having information about all the cases of a
disease in a geographical area, which is most useful for epidemic purposes.
b) Disease case-registry which is a hospital or health facility based.
Health surveys
Epidemiological studies (active surveillance).
Data collection is done by one of three approaches:
1. Active surveillance in an ongoing process where data collectors go and collect data
from its sources.
2. Passive surveillance where data collectors wait to receive data from the source.
3. Sentinel approach where special units are made at the place of occurrence of the
disease.

Gender and Social Norms
lxxvi
Communicable diseases under surveillance in Egypt
The communicable diseases are classified into 3 groups according to the time needed for
notification.
Notifiable Communicable diseases in Egypt
GROUP A:IMMEDIATE REPORTING REQUIRED
1 Meningitis
2 Acute Flaccid Paralysis/ Poliomyelitis
3 HIV/AIDS
4 Rabies/ Animal bite
5 Diphteria
6 Malaria
7 Plaque
8 Tetanus(Neonatal)
9 Acute Food Poisoning
10 Viral Hemorrhagic Fever
11 Rift Valley Fever
12 Botulism
13 Cholera
14 Others
GROUP B:WEEKLY REPORTING REQUIRED
1 Typhoid
2 Brucellosis
3 TB
4 Measles
5 Pertussis
6 Bloody diarrhea(dysentery)
GROUP C:MONTHLY REPORTING REQUIRED
1 Viral hepatitis
2 Mumps
3 Rubella
4 Shistosomiasis
5 Leprosy
6 Fasciola
7 Filaria
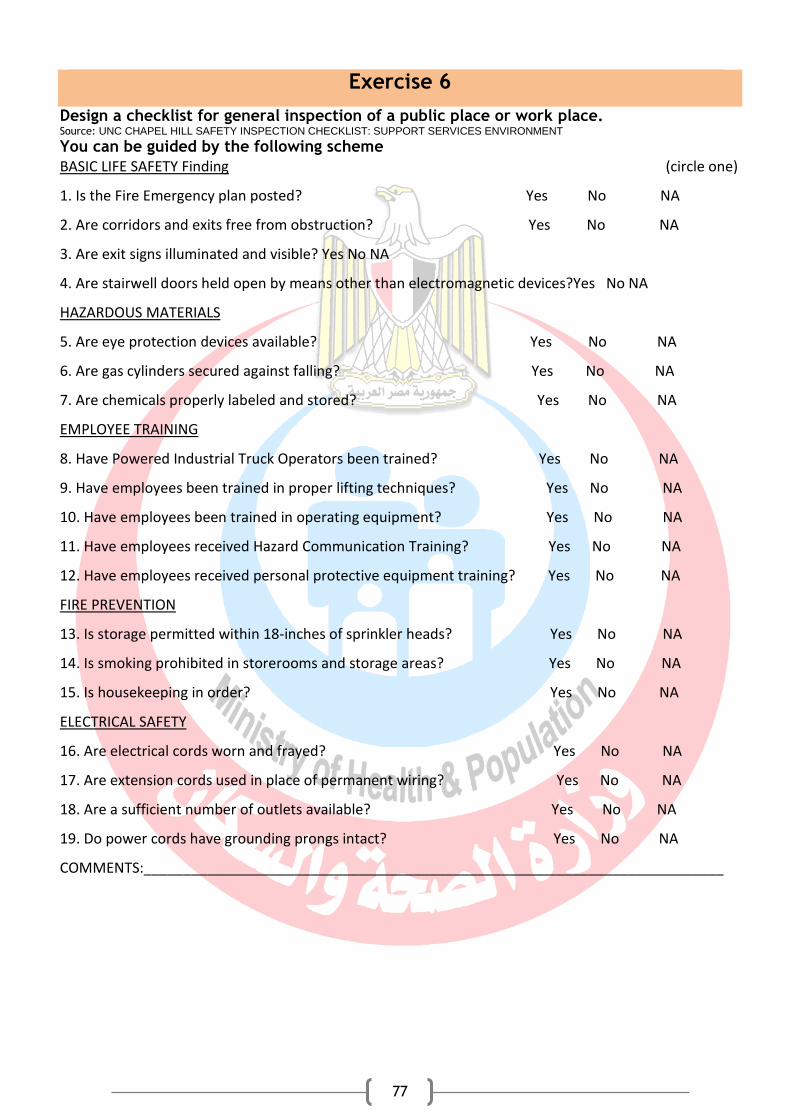
Gender and Social Norms
77
Exercise 6
Design a checklist for general inspection of a public place or work place. Source: UNC CHAPEL HILL SAFETY INSPECTION CHECKLIST: SUPPORT SERVICES ENVIRONMENT
You can be guided by the following scheme
BASIC LIFE SAFETY Finding (circle one)
1. Is the Fire Emergency plan posted? Yes No NA
2. Are corridors and exits free from obstruction? Yes No NA
3. Are exit signs illuminated and visible? Yes No NA
4. Are stairwell doors held open by means other than electromagnetic devices?Yes No NA
HAZARDOUS MATERIALS
5. Are eye protection devices available? Yes No NA
6. Are gas cylinders secured against falling? Yes No NA
7. Are chemicals properly labeled and stored? Yes No NA
EMPLOYEE TRAINING
8. Have Powered Industrial Truck Operators been trained? Yes No NA
9. Have employees been trained in proper lifting techniques? Yes No NA
10. Have employees been trained in operating equipment? Yes No NA
11. Have employees received Hazard Communication Training? Yes No NA
12. Have employees received personal protective equipment training? Yes No NA
FIRE PREVENTION
13. Is storage permitted within 18‐inches of sprinkler heads? Yes No NA
14. Is smoking prohibited in storerooms and storage areas? Yes No NA
15. Is housekeeping in order? Yes No NA
ELECTRICAL SAFETY
16. Are electrical cords worn and frayed? Yes No NA
17. Are extension cords used in place of permanent wiring? Yes No NA
18. Are a sufficient number of outlets available? Yes No NA
19. Do power cords have grounding prongs intact? Yes No NA
COMMENTS:_________________________________________________________________________

Gender and Social Norms
lxxviii
Exercise 7
You are asked to write a report on indoor air quality in a certain building: Source: NH DHHS, Division of Public Health Services September 2011,Air Quality-Indoor Health Officers Manual Page 2 of 3, NH Department of
Environmental Services. Some modifications were done to cope with Egyptian environment
You can be guided by the following points:
A CHECKLIST FOR HEALTH OFFICERS
� Obtain a description of the building condition (age, design, problems, etc.), and type of
ventilation.
� Obtain a description of any symptoms or odors experienced by the occupants.
� Interview occupants who are concerned about IAQ (indoor air quality) to determine how their
concerns or symptoms may be linked to the building air or other causes such as job type, personal
behaviors, etc.
� Determine the last date when the heating, ventilation and air conditioning (HVAC) system was
serviced.
� Inspect the ventilation system to see if the filters are in good working order.
� Identify from where fresh air is being drawn into the building.
� Inspect the building for signs of mold, or excess dust on the floors, carpets or upholstery.
� Inspect the building for toxic pollution sources such as chemical storage, use of solvents, paints,
glues, adhesives, fuels, cleaning supplies or other materials that may produce noxious vapors.
Exercise 8
You are asked to inspect a house and to write a report on the house environment:
Source: The guide was written after Sample-Housing Complaint Investigation Form Health Officers Manual, NH DHHS, Division of Public Health Services September 2011, some modifications were done to cope with Egyptian law and surrounding condition.
You can be guided by the following points:
Are the premises infected by insects and rodents and the landlord is not conducting a periodic inspection and eradication program.
• Is there defective internal plumbing or a back up of sewage caused by a faulty septic or
sewage system.
• Are there exposed wires, improper connectors, defective switches, outlets or other
conditions that create a danger of electrical shock or fire?
• Does the roof or walls leak consistently?
• Is the plaster falling or has fallen from the walls or ceilings?
• The floors, walls or ceiling contain substantial holes that seriously reduce their function
or render them dangerous to the inhabitants.
• Is there an accumulation of garbage or rubbish in common areas?
• Is there an inadequate supply of sanitary water?
• Are there leaks in any gas lines?
• Measure the temperature inside the house.

Gender and Social Norms
79
Inspect the drainage system.
Assess the ventilation inside the building.
Exercise 9
Write a report concerning the role and duties of public officer concerning communicable disease. Source: Health Officers Manual Page 1 of 3 January 2017 Source: NH DHHS, Division of Public Health, Infectious Disease Program. Some modifications were done to cope with Egyptian conditions
You can use the following guide in writing your report:
PUBLIC HEALTH background
A communicable or infectious disease is one which spread from one person to another or from
an animal to a person. These diseases can spread via the air, blood, intestinal tract, or by direct
contact. The control and prevention of communicable diseases is a major focus of the Infectious
Disease Control Program. Access to health care and education are two important issues in the control
of communicable diseases. The local health officers support this vital public health role with the
provision of current information about the occurrence, transmission, and prevention of communicable
diseases in their catchment area.
ROLE OF THE HEALTH OFFICER:
health officers should follow the case with notification to the local health office about the
progress of the case and should notify if the case died.
age to the community to control and prevent the spread of
the disease.
REPORTING OF COMMUNICABLE DISEASE
According to the law (as mentioned above), any physician or other health care provider who assesses,
diagnoses, or treats a person believed by him to be a case or suspect case of a reportable disease shall
immediately report to the local health authority according to the tables mentioned above.
Local office of Health shall report immediately to the ministry Communicable Disease Control Program
those cases or suspect cases of reportable diseases of which they have knowledge. The report should
contains the full name, age, sex, race, ethnicity, address, telephone number, occupation, and place of
occupation of the patient; the name of the disease; the date of onset; and, the name of the person
reporting.
ISOLATION AND QUARANTINE
Certain terms, such as isolation and quarantine are clearly defined.
Isolation is defined as: “the separation, for the period of communicability, of infected persons from

Gender and Social Norms
lxxx
others in such places and under such conditions as to prevent or limit the direct or indirect
transmission of the infectious agent from those infected to those who are susceptible or who may
spread the agent to others.”
Quarantine is defined in the law as: “the restriction of activities of well persons who have been
exposed to a case of communicable disease, during its period of communicability, to prevent disease
transmission during the incubation period if infection should occur.”
COMMUNICATION WITH PUBLIC HEALTH
While the Infectious Disease Control Program makes every effort to keep the Health Officer informed
when it comes to illness in their town, it is typically not necessary to inform a Health Officer regarding
a single case of a communicable disease. Decisions about whether or not to inform the Health Officer
about individual cases are made on a case-by-case basis depending upon the seriousness of the case.
A Health Officer may be notified in situations that involve an outbreak or cluster of illness.
Exercise 10
You are asked to inspect a lab. And to write a report. Source: Laboratory Safety Manual – the University of North Carolina at Chapel Hill after some modification to cope with Egyptian conditions
You can be guided by the following points: 1. DOCUMENTATION & TRAINING
Lab entrance signs with current contacts & emergency numbers posted.
Lab Safety Manual accessible.
Lab Safety Plan accessible and up-to-date.
Other required manuals (Biological Safety Manual, Radiation Safety Manual, Laser
Safety Manual) accessible and up-to-date.
Chemical inventory has undergone annual review/update.
All laboratory personnel are registered (Lab Worker Registration Form).
Lab personnel know where and how to obtain Material Safety Data Sheets (MSDS).
Initial and annual Lab Safety Plan training for ALL lab members.
General Lab Safety/Managing Hazardous Waste training for ALL lab members.
Lab specific policies (Working Alone, Standard Operating Procedures, Lab Accident
Protocols, etc.).
2. EMERGENCY EQUIPMENT
Fire extinguisher available
a. Unobstructed & mounted at designated location.
b. Extinguisher has annual inspection, sealed, and charged.
Gender and Social Norms
81
c. Appropriate extinguisher for hazard (Class A, B, C, or D).
Safety shower present
a. Unobstructed.
b. Checked/tested by Facilities Services.
Eyewash present
a. Unobstructed.
b. Checked/tested by lab within past month.
3. PERSONAL PROTECTIVE EQUIPMENT (PPE)
PPE (eyewear, gloves, lab coats) available and used in lab.
Proper eye protection use (safety glasses/goggles/face shield).
Visitor glasses readily available (if visitors permitted).
Proper chemical resistant/heat resistant/cryogenic gloves.
Long pants and closed shoes (no open toe or canvas shoes) worn.
Rubber apron available (if concentrated acid/base use).
PPE (personal protective equipment) not used in food areas, elevators, opening doors,
etc.
4. GENERAL HAZARDS
Corridors & exit doors unobstructed
Adequate lighting for tasks.
Excess trash, boxes, & paper removed promptly.
No eating/drinking/food storage in lab (except in designated areas).
Hand washing facility (with liquid soap) available.
Proper disposal of needles and sharp objects (plastic red for biohazards, plastic white for
non-hazardous).
Proper disposal of broken glass waste (lined cardboard box) - No cardboard boxes are
greater than ¾ full.
Exercise 11
You are requested to write a report on the role of public officer concerning water sanitation. Source: NH DHHS, Division of Public Health Services September 2011 after some modifications to cope Egyptian environment
You can use the following points as a guide: PUBLIC HEALTH ISSUE:
Ensuring the quality and availability of drinking water is one of the oldest and most
critical public health efforts. The bacterial quality of drinking water is the single most
important water quality test as disease-causing organisms are a major health concern.
One glass containing just a few microorganisms can cause illness in anyone ingesting the
Gender and Social Norms
lxxxii
water. In contrast, contamination by chemicals such as petroleum by-products, or a
naturally occurring element such as arsenic or radon, usually requires a long period of
exposure to cause measurable health risks.
Populations at higher risk for adverse health effects from contaminated water include
children, the elderly, pregnant women, and persons who are immunocompromised from
infection with HIV, those undergoing chemotherapy, or have auto-immune illnesses.
ROLE OF THE LOCAL HEALTH OFFICER:
1. Testing of water supplies: If a health officer suspects, or is made aware of, a public or
private water supply that may be contaminated, they may be able to offer suggestions on
having the water supply tested.
2. If the water samples do not fulfill the standard, the public officer should inform the
local health authority.
3. Boil orders: When the water in a public water system is contaminated with fecal
Coliform or Escherichia (E. coli) bacteria, the system owners are required to make a
public announcement to boil all water from the system used for human or animal
consumption. Local health authority sends health officers a copy of all boil orders. If a
municipality owns the water system, then the health officer might be actively involved in
public notice and issuing the boil order. If the town is served by a public water system not
owned by the town, the health officer is not formally or legally obliged to issue orders.
The local health officer in such cases should be an important local resource for the
community by keeping the community and consumers informed as to the status of the
water supply. The health officer may also request additional public information or notice
from the water system owner.
NB: In Egypt the owner is the government and the community.
4. Local resource on questions of water quality: The local health officer may be contacted
for information on water quality issues such as arsenic, lead, copper, giardiasis,
cryptosporidium, radon, chemical contamination. Health officers should become familiar
with the information on these topics.
COLIFORM BACTERIA:
Coliform bacteria belong to the family Enterobacteriaceae - which includes aerobic
and facultative anaerobic, gram negative, rod-shaped, non-spore forming bacteria.
Coliform include the genera Escherichia (E. coli), Klebsiella, Citrobacter and
Enterobacter. They are found in the intestines of warm-blooded animals and man, and
therefore occur in sewage. Some coliform, with the exception of E. coli, are naturally
occurring in soils and vegetation. To determine if these bacteria are present in a water
supply, one needs to do a coliform analysis. The best indicator of fecal coliform activity-

Gender and Social Norms
83
and probable contamination from human and animal waste is E. coli. The coliform test is
the standard test for determining bacterial quality of drinking water. The organisms in the
coliform group are considered indicator organisms. When present, they indicate that
there is a possibility of disease organisms also being present in the water. Normally
coliform bacteria themselves are not believed to cause disease when ingested although
some strains of E. coli are capable of producing diseases. Examples of water-borne
diseases include cholera, typhoid fever, dysentery and giardiasis. The coliform test is easy
to perform, inexpensive.
TOTAL COLIFORM:
These organisms are prolific in the soil and their presence does not necessarily
imply contamination with human or animal wastes. The presence of only total coliform
generally does not imply an imminent health risk but does require an examination of the
system to determine how these organisms gained entry.
FECAL COLIFORM:
Fecal coliform is a much smaller sub-group of the coliform family. Fecal coliform
bacteria generally originate in the intestines of warm-blooded animals including birds.
Fecal coliform have a relatively short life span compared to environmental coliform. Their
presence is of greater concern because it indicates the possibility of recent pollution by
human or animal waste. In a Public Water System, immediate Public notice is required in
view of the higher potential risk of disease presence. The predominant organism of this
group is Escherichia coli (E. coli). Ninety-nine percent of fecal coliform samples are E. coli
positive.
ESCHERICHA COLI:
E. coli is species of microorganism within the coliform group. They originate only in
the intestines of warm-blooded animals including birds and humans. Their presence
indicates a strong likelihood that human or animal wastes are entering the water supply
source. As with fecal coliform, immediate public notice is required in Public Water
Systems.
CAUSES OF BACTERIA IN WATER SAMPLES
Total and fecal coliform bacteria reside in the intestinal tracts of man and other
animals, including birds. Outside of the animal host, bacteria die off quickly, typically
within 30 days or less. Therefore, if coliform bacteria are detected in a water system over
a long period of time, this indicates that new bacteria are constantly entering the well,

Gender and Social Norms
lxxxiv
aquifer or distribution system. Poor well construction is the most common explanation for
bacteria in water samples from wells.
GIARDIASIS:
Giardia lamblia is an intestinal parasite, which can cause a diarrheal illness in
humans and animals, called giardiasis. The parasite occurs naturally in warm-blooded
animals such as humans and other forms of wildlife. The only way to confirm a Giardia
infection is by laboratory analysis of stool samples. Giardiasis is usually not life
threatening to otherwise healthy persons. Medication can normally cure giardiasis in
approximately ten days. Giardiasis often affects many members of the same family.
Reinfection from hand to mouth behaviors is often a problem among young children.
Exercise 12
You are asked to inspect a school environment and to write a report.
You can be guided by the following points: Source: NH DHHS, Health Officer Manual May 2018 after modification to cope Egyptian environment
1. School Information: Enter data to identify the school being inspected concerning name address and level. 2. Inspection Information: Enter the name and contact information of the health officer,
or
Whoever is doing the inspection.
3. Information/Instructions: Read the brief directions on completing the form. The form is
set up as a checklist; however, a Health Officer may include notes on the form, take
photos, or add attachments. Remember, the inspection form is used to describe the
facility on that particular day, although you can make notes about any obvious past
repairs, stains, or odors that reflect ongoing issues.
If needed, request and attach the following to the school health inspection form:
- If a septic system Sewage system) is on site, tank-pumping service reports.
- If animals (for agriculture school) are on site, animal vaccination certificates for dogs,
cats, and ferrets, etc.
- If a pool (in some private school) is present, swimming pool testing records.
- If on well water, water testing records for hazards.
- If food is prepared on site, a food service license.
- A floorplan of the school with bathrooms noted.
- Summary table of hot water locations & test results.
- Summary table of drinking water fixtures, locations.
In your responses to the questions below, you can check off either „Yes‟, „No‟, or
Gender and Social Norms
85
„Unknown‟.
_ If „YES‟ or „NO‟, include any helpful notes, corrective actions, and a date the correction
should be made.
_ If the response is „Unknown‟, make a note as to why.
_ If the response is „Not Applicable‟, then make a note as to why.
4. Sanitary Investigation: Inspect all areas and enter data.
Q: Is there a presence of garbage, insects, rodents, or other unsanitary conditions?
Document the conditions with photos and note this on the form.
5. Restrooms: Inspect all areas and enter data.
Q: Are all restrooms clean and in working order?
If not, please describe the location with a problem. Document with photos if needed.
Q: Do all restrooms have hot water, dispensed soap, toilet paper & dispensed paper towels
or heated air dryers?
Note: Test at least one (1) hot water tap in each restroom with a thermometer, and
record the average temperature, and time it took to reach temperature. Inspect and note
any missing dispensers for soap, paper or dryers.
Q: Is there at least one toilet fixture for every 50 people?
Note: Document the number of toilet fixtures and divide by the number of occupants in
that building. If the ratio is less than 1:50, make a note.
6. Food preparation, dining areas, sinks & water fountains: Inspect and enter data for the
following items.
Q: If food is prepared on-site, is a current license from the municipality or local health
licensing authority posted?
If yes, note expiration date. Document with a photo if needed.
Q: Are toxic materials clearly labeled and properly stored away from food?
Inspect to ensure any toxics or cleaners are labeled, and stored in a way that there is no
risk of contaminating food.
Q: Is hot water available for cleansing, laundry and building maintenance?
Note: Test hot water tap in each food preparatory area with a thermometer, record the
average temperature, and time it took to reach temperature.
Q: Are all the water fountains clean with sufficient water pressure?
If not, describe the location of the problem area.
7. Septic and water supply systems: Inspect and enter data.
Q: Is there a pump schedule for the septic system?
If available, view or document the pump receipts.
Q: Is there a reason to suspect the septic system has a system failure?

Gender and Social Norms
lxxxvi
Evidence of failure may include backup into sinks, or odor of septic waste, or waste water
on or near the leach field. If so, please describe the condition.
Q: Is the well (in case the water supply is from a well) registered and tested as required?
8. Environmental hazards (mold, lead paint,): Inspect and enter data.
Q: Moisture damage or mold.
_ Is there a presence of water leaks in the ceiling, walls, or internal plumbing?
If so, please describe the condition and location.
_ Is there any mildew or mold present?
If so, describe the condition and location:
_ Note any evidence of „visible mold‟ (e.g., signs of wet or dry mold or stains, mildew or
mold on walls, ceiling, or floors).
_ Note any conditions that may indicate „hidden mold‟ (e.g., musty odors, damp
conditions, water damage, history of water infiltration, etc.)
_ Remember, almost every mold problem is a moisture problem. Focus on helping schools
to identify and fix moisture problems, as well as, documenting any potential for mold
growth.
9. Smoking: Inspect and enter data.
Q: Are there any signs of smoking in or near the building?
-Note if you find any cigarette butts or active smoking.
Q: Are signs posted noting the prohibition of smoking on the school‟s grounds?
10. Animals on school property: Inspect and enter data. This may be important in
agriculture schools.
Q: Are all animals enclosed by appropriate and lockable cages/stalls?
- Do all animals have a current certificate of good health from a licensed veterinarian?
Q: Does it appear that animal fecal material is adequately cleaned from the cage/stall?
Q: Is a handwashing station available nearby with hot water and soap for those
students or staff handling the animals or cleaning the cages?
11. Additional remarks: Reflect on the inspection process, and add in any other notes you
feel would be relevant to health issues, especially indoor air quality.

Gender and Social Norms
87
Exercise 13
A worker in a factory where air is highly polluted by isocyanate. He complained of
chest tightness. He was submitted to pulmonary function test. His predicted forced vital
capacity was 4 liters. His Forced vital capacity was 3.25 liters and his forced expiratory
volume in 1st second was 2 liters. Answer the following questions:
1- What is the most probable lesion in the lung?
2- Design a checklist to inspect the work place.
3- Put a preventive program for such problem.
Exercise 13
A worker in a factory where air is highly polluted by silica dust. He complained of
chest tightness. He was submitted to pulmonary function test. His predicted forced vital
capacity was 4 liters. His Forced vital capacity was 2 liters and his forced expiratory
volume in 1st second was 1.75liters. Answer the following questions:
1- What is the most probable lesion in the lung?
2- What are the investigations to be done?
3- Design a checklist to inspect the work place.
4- Put a preventive program for such problem.

Gender and Social Norms
lxxxvi
Source: The Encyclopedia of Environmental Studies: William Ashworth ...,https://www.amazon.com/Encyclopedia-Environmental-Studies-
William.../081601531
Encyclopedia of Environmental Science - John F. Mongillo, Linda ...,,https://books.google.com ›
Environmental science | Britannica.com, https://www.britannica.com/science/environmental-science
Encyclopedia of environmental health (eBook, 2011) [WorldCat.org] www.worldcat.org/title/encyclopedia-of-environmental-health/oclc/771922842
K. Park .Textbook of Preventive and Social Medicine. M/S Banarsidas Bhanot (India). 23ed.
Book of Department of Community, Environmental and Occupational Medicine, Faculty of Medicine, Ain Shams University. National Library Deposit No 20569/2010
. K. Park .Textbook of Preventive and Social Medicine. M/S Banarsidas Bhanot (India). 23ed.
Encyclopedias/Handbooks - Occupational Health and Safety ... ecu.au.libguides.com/c.php?g=410557&p=2796102
Fundamentals of Air Pollution - 5th Edition - Elsevier https://www.elsevier.com/books/fundamentals-of-air-pollution/vallero/978-0-12-401733-7Purchase
Josef la Duo, Occupational and Environmental Medicine. 4th
ed. Prentice Hall International. Inc
Book of Department of Community, Environmental and Occupational Medicine, Faculty of Medicine, Ain Shams University. National Library Deposit No 20569/2010
K. Park .Textbook of Preventive and Social Medicine. M/S Banarsidas Bhanot (India). 23ed.
Hand Book of Environmental Sociology edited by Riley E. Dunlap and William Michelson. Greenwood Press. Wetport, Connecticut. London
Textbook of Preventive and Social Medicine. K. Park. M/S Banarsidas Bhanot (India). 23ed.
Bok Coordinator
Mostafa Fathallah
General Directorate of Technical Education for Health
هيحزس تيعولوصاسة الصحة والسكان حقوق النشش والحأليف

5