epidemic and pandemic use of antivirals introduction 15 september 2008 frederick g. hayden, m.d....
TRANSCRIPT

Epidemic and Pandemic Use of Antivirals
Introduction
15 September 2008
Frederick G. Hayden, M.D.
University of Virginia Health System
Charlottesville, Virginia, USA
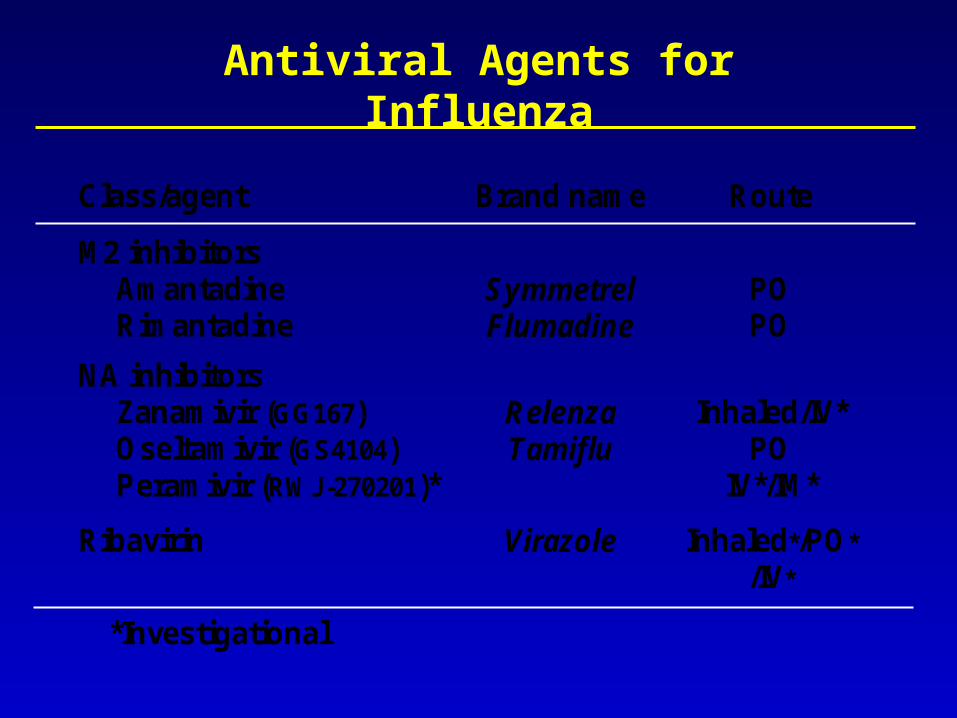
Antiviral Agents for Influenza
Class/agent Brand name Route
M2 inhibitors Amantadine Rimantadine
Symmetrel Flumadine
PO PO
NA inhibitors Zanamivir (GG167) Oseltamivir (GS4104) Peramivir (RWJ-270201)*
Relenza Tamiflu
Inhaled/IV*
PO IV*/IM*
Ribavirin
Virazole Inhaled*/PO*
/IV*
*Investigational
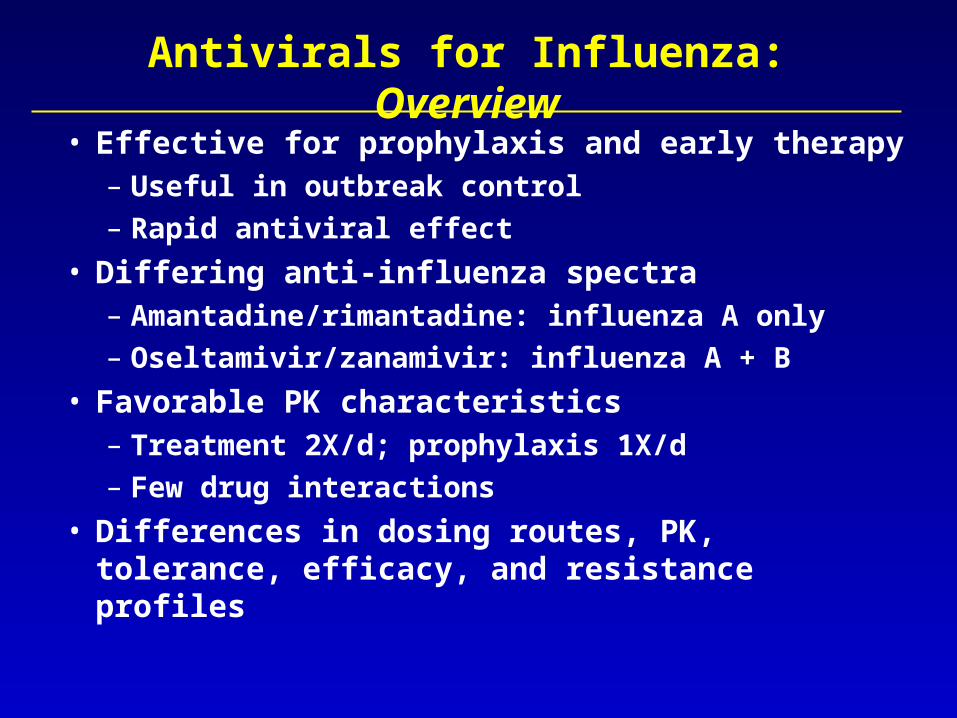
Antivirals for Influenza: Overview
• Effective for prophylaxis and early therapy– Useful in outbreak control– Rapid antiviral effect
• Differing anti-influenza spectra– Amantadine/rimantadine: influenza A only– Oseltamivir/zanamivir: influenza A + B
• Favorable PK characteristics– Treatment 2X/d; prophylaxis 1X/d– Few drug interactions
• Differences in dosing routes, PK, tolerance, efficacy, and resistance profiles

M2 Inhibitor Prophylaxis During Pandemic Influenza
Protective efficacy
Pandemic Influenza A illness
Seroconversion
1968 H3N2
1977 H1N1
59-100%
31-71%
28-52%
19-39%
Hayden. J Infect Dis 176:S56, 1997
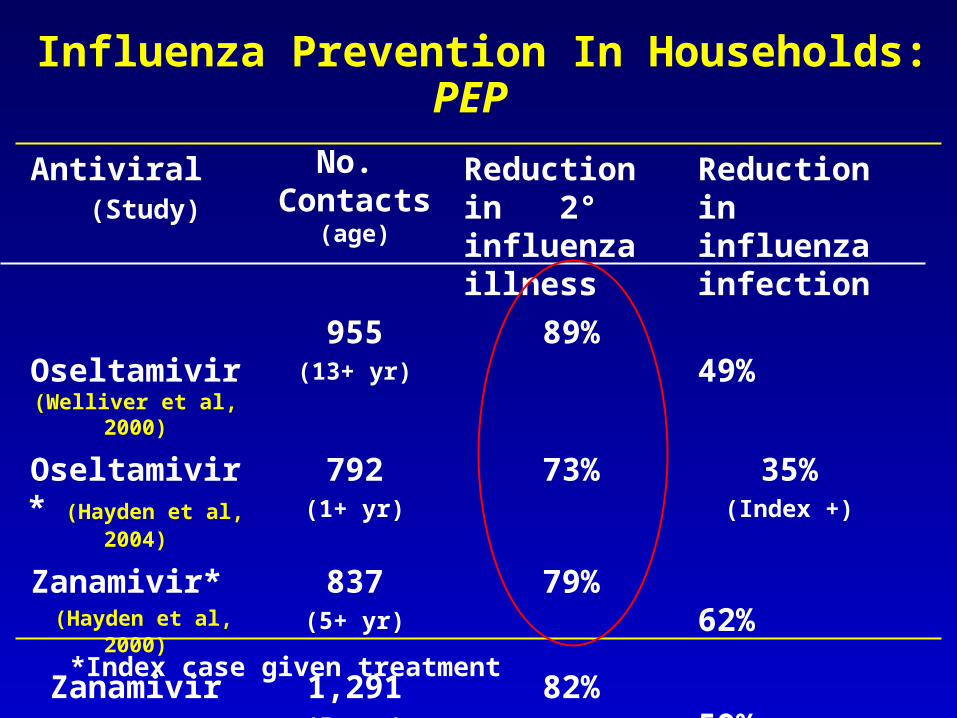
Influenza Prevention In Households: PEP
Antiviral (Study)
No. Contacts
(age)
Reduction in 2° influenza illness
Reduction in influenza infection
Oseltamivir (Welliver et al, 2000)
955(13+ yr)
89% 49%
Oseltamivir* (Hayden et al, 2004)
792(1+ yr)
73% 35%(Index +)
Zanamivir* (Hayden et al, 2000)
837(5+ yr)
79% 62%
Zanamivir (Monto et al, 2002)
1,291(5+ yr)
82% 59%
*Index case given treatment
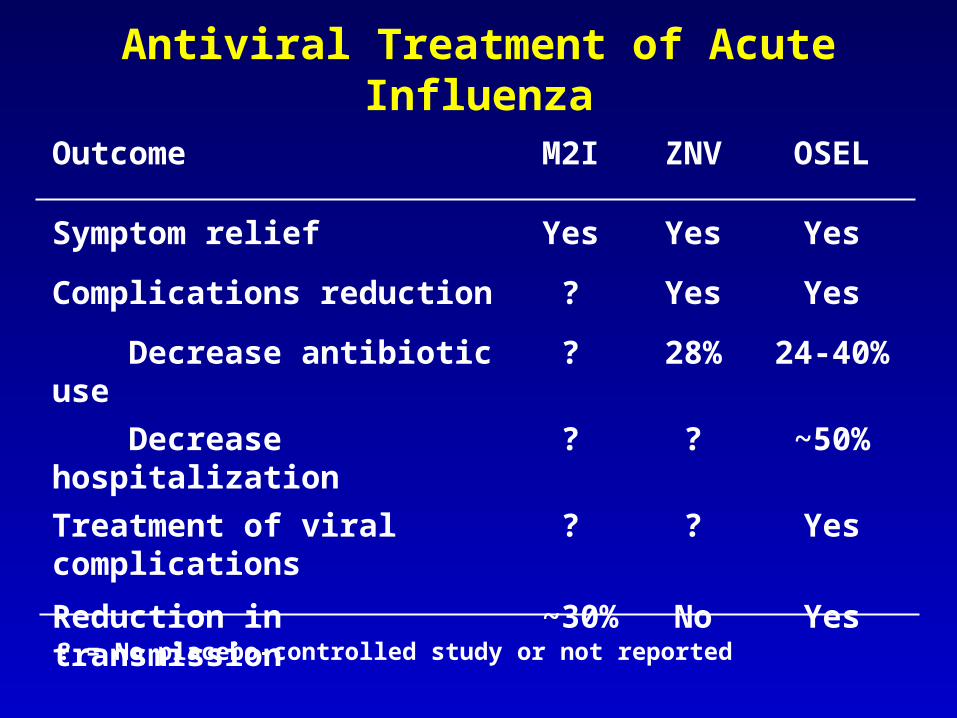
Antiviral Treatment of Acute Influenza
Outcome M2I ZNV OSEL
Symptom relief Yes Yes Yes
Complications reduction ? Yes Yes
Decrease antibiotic use ? 28% 24-40%
Decrease hospitalization ? ? ~50%
Treatment of viral complications
? ? Yes
Reduction in transmission ~30% No Yes
? = No placebo-controlled study or not reported
7
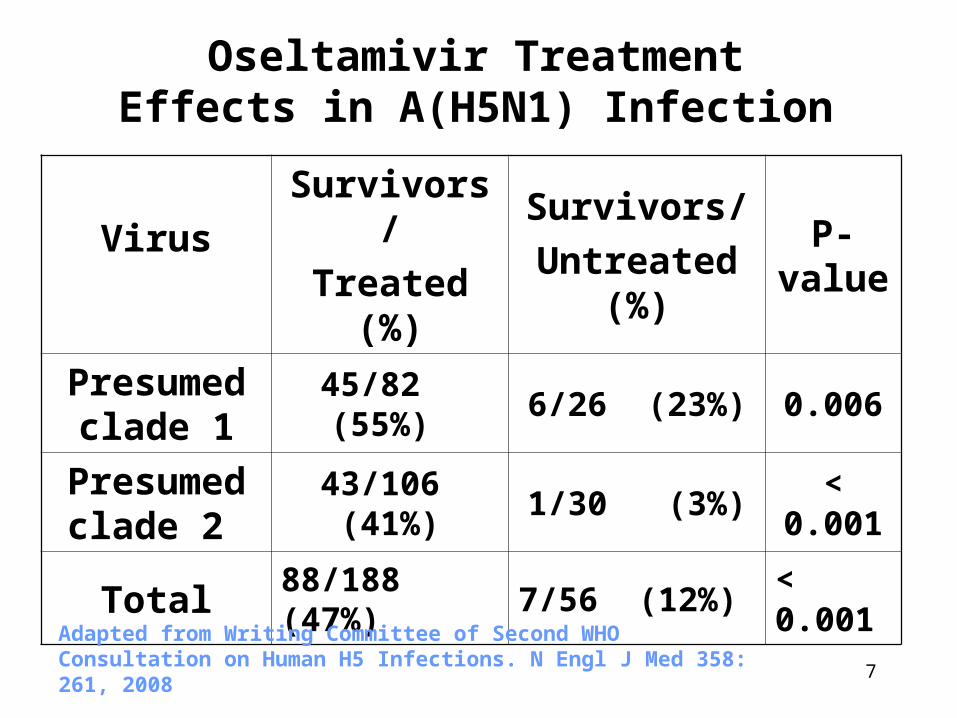
Oseltamivir Treatment Effects in A(H5N1) Infection
VirusSurvivors/
Treated (%)
Survivors/
Untreated (%)
P-value
Presumed clade 1
45/82 (55%) 6/26 (23%) 0.006
Presumed clade 2
43/106 (41%) 1/30 (3%) < 0.001
Total 88/188 (47%) 7/56 (12%) < 0.001
Adapted from Writing Committee of Second WHO Consultation on Human H5 Infections. N Engl J Med 358: 261, 2008

Resistance to M2 Inhibitors (S31N) in Community Isolates of A/H3N2, 2000-07
0
10
20
30
40
50
60
70
80
90
100
2000/1 2001/2 2002/3 2003/4 2004/5 2005/6 2006/7
China
Hong Kong
Australia
Japan
Europe
USA
%
Bright et al. Lancet 2005, JAMA 2006; Klimov et al. CDC unpublished; Barr et al. Antiviral Res 2006; R Saito, Niigata Univ, unpublished

Oseltamivir Resistance in H1N1 (H274Y)
• Rare in community H1N1 isolates, 1996-2007– 0 to <1% in most surveys– 2.2% in Japan in 2005-6 (but not in 2006-7 or
early in 2007-8)• High prevalence in Europe and globally, 2007-8
– Patients without known oseltamivir use or exposure to those on drug
– Generally no obvious epidemiologic links• Household contacts, several apparent clusters
– Typical influenza illness; some fatalities• Efficient person-to-person transmission
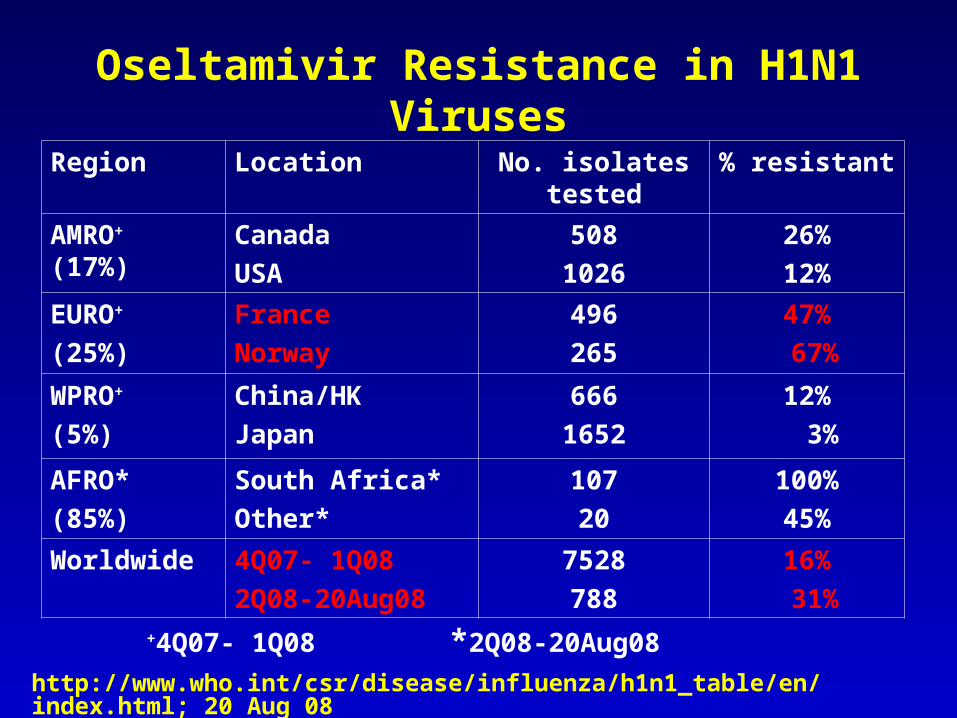
Oseltamivir Resistance in H1N1 Viruses
+4Q07- 1Q08 *2Q08-20Aug08
http://www.who.int/csr/disease/influenza/h1n1_table/en/index.html; 20 Aug 08
Region Location No. isolates tested
% resistant
AMRO+ (17%)
Canada
USA
508
1026
26%
12%
EURO+
(25%)
France
Norway
496
265
47%
67%
WPRO+
(5%)
China/HK
Japan
666
1652
12%
3%
AFRO*
(85%)
South Africa*
Other*
107
20
100%
45%
Worldwide 4Q07- 1Q08
2Q08-20Aug08
7528
788
16%
31%

Antivirals for Seasonal, A(H5N1), and Pandemic Influenza: Efficacy, Resistance,
and New Agents
15 September 2008
Frederick G. Hayden, M.D.
University of Virginia Health System
Charlottesville, Virginia, USA

Do We Need New Anti-Influenza Agents?
• Antiviral resistance– Global spread of M2 inhibitor resistance in
H3N2 > H1N1
– New emergence of oseltamivir-resistant H1N1
– Dual M2 and NAI resistance in IC hosts
• Antiviral efficacy incomplete in H5N1 disease– Oseltamivir resistance emergence
• Safety/efficacy ? in risk populations: infants < 1 yr, pregnancy, hospitalized, IC hosts
• Lack of parenteral agents

Viral Loads and Antiviral Treatments in Immunocompromised Host with Fatal
Oseltamivir-Resistant H1N1 Illness
• 67 yo male with CLL + recent chemoRx neutropenia
• Fever, cough, SOB acute respiratory failure
Oseltamivir resistance (H274Y)
Amantadine resistance (L26F)
Van der vries et al. NEJM 359:1074, 2008
Re
-intu
ba
tion
Ex
tub
atio
n
Intu
ba
tion

Medical Needs for Anti-Influenza Antivirals
• Greater antiviral efficacy greater clinical benefit
• Safety and efficacy in special risk populations: infants < 1 yr, pregnancy, hospitalized, immuno-compromised
• Reliable drug delivery in seriously ill patients• Manage antiviral resistance • Combinations

Influenza Virus Replication and Sites for Antiviral Inhibition
De Clercq. Nature Reviews- Drug Discovery 5:1015, 2006

Investigational Anti-Influenza Agents
• Neuraminidase (NA) inhibitors- Zanamivir (IV), peramivir (IV/IM), A-315675 (oral)
• Long-acting NA inhibitors (LANI)
–CS8958/R-118958 (topical), Flunet (topical)
• Conjugated sialidase- DAS181 (topical)
• HA inhibitors- cyanovirin-N, sialyl-glycopolymer, arbidol
• Polymerase inhibitors- ribavirin; viramidine; siRNA; T-705
• Protease inhibitors- aprotinin
• Biologics- antibodies, interferons

Investigational Agents in Clinical Development
Agent Target Sponsor Route Development phase
Zanamivir NA GSK IV Phase 1, 2a
Peramivir NA Biocryst IV, IM Phase 2
CS8958 NA Sankyo, Biota
Topical Phase 2
T-705 Polymerase Toyama Oral Phase 2
DAS181 HA receptor Nexbio Topical Phase 1

Neuraminidase Inhibitors
Peramivir

NA Inhibitor Resistance Profiles
NA mutation
NA type/ subtype
Susceptibility in the NAI assay (fold )
Oselt Zana Peram A-315675
E119V A/N2 R (>50->1000)
S (1) S (1) S (1-2)
R292K A/N2 R (>1000) S (4-25) R (40-80) S (8-13)
H274Y A/N1 R (>700) S (1) R (40-100) S (3)
R152K B R (>30-750)
R (10-100) R (>400) R (150)
Mishin et al. AAC 49:4516, 2005; Wetherall et al. AAC 41:742, 2003; Abed et al. Antiviral Res 77: 163, 2008
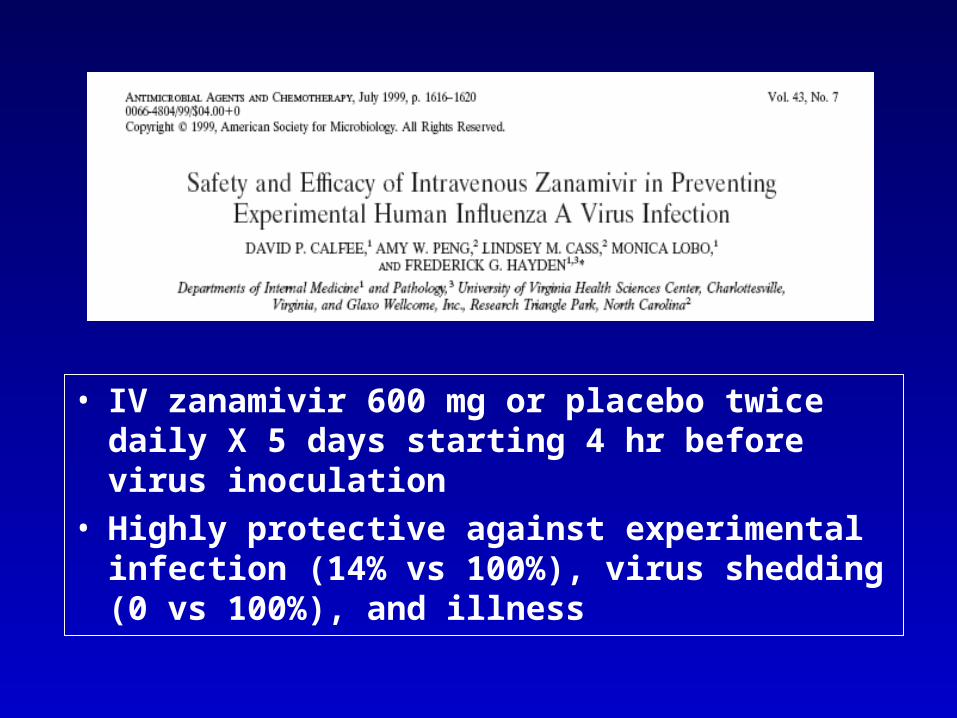
• IV zanamivir 600 mg or placebo twice daily X 5 days starting 4 hr before virus inoculation
• Highly protective against experimental infection (14% vs 100%), virus shedding (0 vs 100%), and illness

21
Pharmacokinetic Profiles of Intravenous and Intramuscular Peramivir
Kilpatrick JM, et al. Pharmacokinetics and Safety of Peramivir by Intramuscular Administration, Options for the Control of Influenza VI, Toronto, 2007
Intravenous Intramuscular
• Linear PK; prolonged plasma T1/2elim (18 – 20 hr)

IM Peramivir: Time to Alleviation of Illness
J Alexander, BioCryst Pharmaceuticals, unpublished data

23
COMMERCIAL IN CONFIDENCE
Long Acting Neuraminidase Inhibitors (LANI)- 2 Strategies
O
NH
O
NHO
O
OH
NH
NH2
OHOH
O
NH
O
NH
O
NHO
O
OH
NH
NH2
OHOH
O
NH
X
OCH3(CH2)6
O
NH
O CO2H
NHNH
OH
NH2O
OMe
OH
NH
O CO2H
NHNH
OH
NH2O
OMe
CS-8958 FLUNET
DimerPreclinical
Pro-drugClinical
R-125489
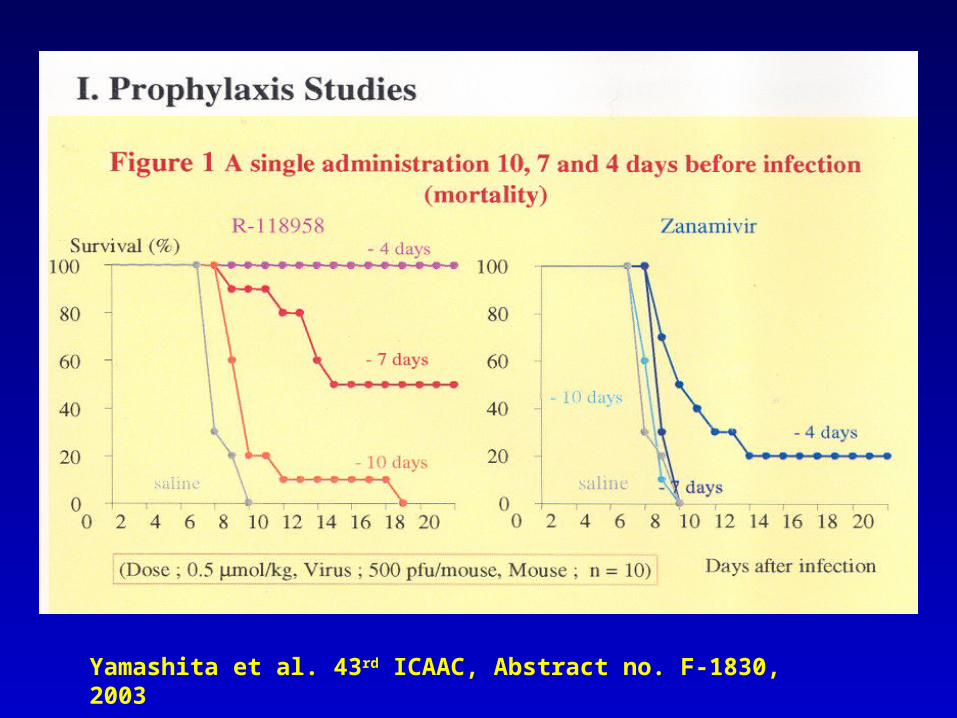
Yamashita et al. 43rd ICAAC, Abstract no. F-1830, 2003

• Double-blinded trial found that inhaled CS-8958 administered once only was not statistically different than standard oseltamivir regimen.
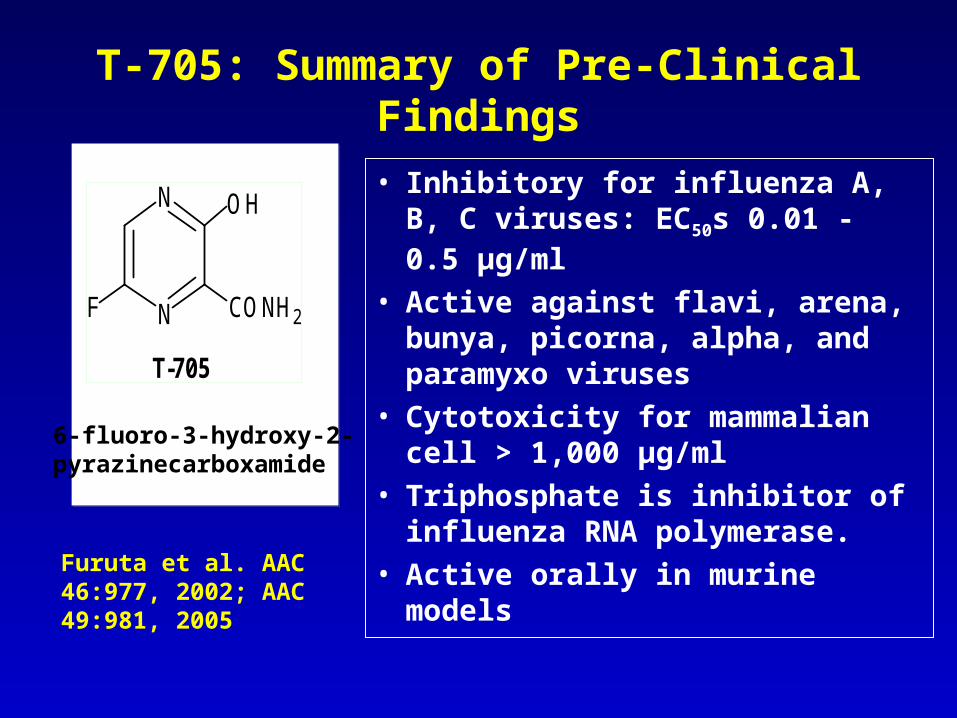
T-705: Summary of Pre-Clinical Findings
• Inhibitory for influenza A, B, C viruses: EC50s 0.01 - 0.5 µg/ml
• Active against flavi, arena, bunya, picorna, alpha, and paramyxo viruses
• Cytotoxicity for mammalian cell > 1,000 µg/ml
• Triphosphate is inhibitor of influenza RNA polymerase.
• Active orally in murine models
N
NF
OH
CONH2
T-705
6-fluoro-3-hydroxy-2-pyrazinecarboxamide
Furuta et al. AAC 46:977, 2002; AAC 49:981, 2005

T-705: In Vitro Activity vs Ribavirin
Compound
IC50(μM) ± SD
(A PR/8/34 H1N1 influenza)
CC50(μM) ± SD
(MDCK cells)
T-705 1.0 ± 0.9 > 6,370
Ribavirin 31.6 ± 9.2 94.3 ± 47.6
Furuta Y, et al. Antimicrob Agents Chemother. 2005;49:981-986.

Effect of a T-705 Treatment in Mice Exposed to Lethal A/Duck/N/1525/81
(H5N1) Virus
Sidwell RW, et al. Antimicrob Agent Chemother. 2007;51:845-851.
0
20
40
60
80
100
4 12 24 48 60
Control T-705, 300 mg/kg T-705, 600 mg/kg
Delay before starting treatment following viral exposure, hours
Sur
viva
l (%
)
* *
* *
*
*
* *
*P < .01 relative to control

Pharmacokinetics of Oral T-705
• Bioavailability > 97% in mouse
• Rapid absorption in humans (Tmax < 1 hr)
• Plasma T1/2elim from 1.3 to 3.9 hr– Mainly excreted as T-
705M1 in urine
• Single doses up to 1,600 mg or multiple up to 400 mg tid for 7 days well tolerated
0.001
0.01
0.1
1
10
100
0 3 6 9 12 15 18 21 24
Time after dose (hr)T-
705 P
lasm
a Con
cent
ratio
n (μ
g/mL)
30 mg (n=6)
90 mg (n=6)
200 mg (n=6)
400 mg (n=6)
800 mg (n=6)
1600 mg (n=6)
Single oral doses of T-705 over a range of 30 to 1600 mg
Toyama Chemical Co, unpublished

Molecular Model of DAS181 (Fludase®)
• Fusion construct with
catalytic domain of A.
viscosus sialidase and
an epithelium-
anchoring domain
(human amphiregulin)
– Active against both α2,6-
and α2,3-linked sialic
acid receptorsMalakhov et al. AAC 50:1470, 2006

Preclinical Features of DAS181
• Inhibitory for range of influenza A and B viruses – In vitro EC90 values: 1-14 nM– Epithelial tag increases activity 5-30 fold– Pretreatment (24 hr) effective
• Intranasal dosing shows– Prophylactic and therapeutic activities in mice– Antiviral effects with reduced inflammatory
responses in ferrets
Malakhov et al. Antimicrob Agent Chemother 50:1470, 2006

Effect of DAS181 on S. pneumo Binding to Human Airway Epithelium (HAE) Cells
• DAS181 treatment had no significant effect on adherence.
Nicholls et al. J Antimicrob Chemother 62:426, 2008

DAS181 Treatment in Mice with H5N1
• Dose of 1 mg/kg/d for 7-8 d
• Inoculum of 3 MLD50
• Time-to-treatment effects on survival and lung titers on day 3 and 6.
Belser et al. JID 196:1439, 2007

Potential Role of Combination Antiviral Therapy in Influenza Treatment
• Combinations evaluated in animal models– Amantadine + interferon– M2 inhibitors + ribavirin– M2 inhibitors + oseltamivir– Oseltamivir + ribavirin
• Combinations evaluated in humans– Oral rimantadine + nebulized zanamivir
• Future considerations– Dual NAIs– Triple therapy: M2 inhibitor + ribavirin (or other transcriptase inhibitor) + IFN-α or NAI– Inclusion of other novel agents
Ong and Hayden. J Infect Dis 196:181, 2007; Hayden FG. Antivir Res 71:372, 2006

CASG* Trial of Nebulized Zanamivir + Rimantadine in Hospitalized Adults
Measure Zanamivir + Rimantadine
Rimantadine alone P value
No or mild cough, day 3
15/16 (94%) 11/20 (55%) .01
Days of hospitalization 4.7 ± 2.3 5.2 ± 2.3 .52
Frequency of rimantadine resistance
0 3 ND
Ison et al. Antiviral Ther. 2003;8:183-190.
*CASG = Collaborative Antiviral Study Group.

39
Survival of mice inoculated with rg VN-1203/04 –Survival of mice inoculated with rg VN-1203/04 –Amantadine susceptibleAmantadine susceptible
0
0.25
0.5
0.75
1
0 5 10 15 20
0
0.25
0.5
0.75
1
0 5 10 15 20
Days after inoculationDays after inoculation Days after inoculationDays after inoculation
Su
rviv
al d
istr
ibu
tio
n f
un
ctio
nS
urv
iva
l dis
trib
uti
on
fu
nct
ion
Su
rviv
al d
istr
ibu
tio
n f
un
ctio
nS
urv
iva
l dis
trib
uti
on
fu
nct
ion
AM 30AM 30
AM 15AM 15
AS 1.5AS 1.5
OS 10OS 10
ControlControl ControlControlOS 1OS 1
AM 30 + OS 10AM 30 + OS 10
AM 15 + OS 10AM 15 + OS 10
Single-drug therapySingle-drug therapy Combination therapyCombination therapy
Ilyushina et al. Antiviral Therapy 12;363, 2007

• Comparison of monotherapy with i.p. zanamivir (ZNV), celecoxib, mesalazine, or gemfibrizol to triple regimen of ZNV + celecoxib + mesalazine in mice– High inoculum of A/Vietnam/1194/04 (103 LD50)
– Therapy initiated at 48 hrs post-inoculation
– No survival benefit of early therapy (4 hrs) with single agents except ZNV
Zheng et al. PNAS, on line 6/2008

survival with ZNV + celecoxib + mesalazine
• 2/8 surviving mice in triple therapy group had detectable titers at day 21.
Antiviral + Immunomodulator Therapy for H5N1 in Mice

Influenza Antivirals: Future Directions• Goal: Rapid inhibition of influenza viral
replication at all affected sites• Near-term: parenteral NAIs
– IV zanamivir or IV/IM peramivir
• Next: antiviral combinations – NAI plus M2 inhibitors, polymerase inhibitor
(T-705 or ribavirin), or neutralizing antibodies
• Longer-term: – Antivirals with immunomodulators
– Host function-targeted agents
44
Forthcoming Book from ASM Press
• Third edition• Updates 2002
version• Available first
quarter 2009

Back-up Slides

• Pre-clinical assessment of arbidol toxicity and antiviral activity– Ethyl-6-bromo-4-[(dimethylamino)-methyl]-5-
hydroxy-1-methyl-2-[(phenylthio)methyl]-indole-3-carboxylate hydrochloride monohydrate
– Previous reports of activity for influenza, hepatitis B and C viruses
Shi et al. Arch Virol 152:1447, 2007

• Influenza testing by CPE inhibition in MDCK cells
• Arbidol causes overt cytotoxicity at >16 ug/ml
• Broad spectrum; narrow therapeutic index
Shi et al. Arch Virol 152:1447, 2007

In Vivo Activity of Arbidol
• Murine model of A/PR/8/34(H1N1)
• Drugs by oral gavage X 6 d starting 24 hr pre-virus
• Up to ~3 log10 lung virus titers
• LD50 of 314 mg/kg/d for arbidol
• Narrow TI
Shi et al. Arch Virol 152:1447, 2007
• Kinetic analysis of NA (sialidase) activity
– Whole virus suspensions of isolates from 2007-8 and prior seasons
• Vm (reflecting enzyme activity) similar in susceptible and resistant isolates from 2007-8 but both ~3X than in earlier H1N1 viruses
• Km (reflects substrate affinity) ~2X in susceptible H1N1 from 2007-8 than earlier; intermediate for oseltamivir-resistant isolates
Rameix-Welti et al. PLoS Pathogens 4:e1000103, 2008

Growth of H1N1 Viruses from 2007-8 in MDCK SIAT-1 Cells
• Replication of oseltamivir-resistant H1N1 (H274Y) isolates not impaired in vitro compared to susceptible H1N1 viruses from 2007-8 or earlier.
S
SR
R
Rameix-Welti et al. PLoS Pathogens 4:e1000103, 2008

NA Gene Phylogeny
• NA substitutions found in majority of H1N1 from 2007-8 include 3 near catalytic site (222, 249, 344).
NA affinity for substrate and NAIs may have altered HA-NA balance to fitness ?
Rameix-Welti et al. PLoS Pathogens 4:e1000103, 2008

Clinical Experience Suggests No Role for Corticosteroids in A(H5N1) Treatment
•Vietnam Survival
Steroid Rx No steroids P-value
Hanoia 12/29 (41%) 29/38 (76%) 0.008
Published casesb
3/19 (16%) 10/15 (66%) 0.007
a Cao T, Liem NT. N Engl J Med 2008; 358: 261b Emerg Infect Dis 2005; 11: 201; N Engl J Med 2004; 350: 1179; N Engl J Med 2006; 355: 2186-94.

Convalescent Plasma Therapy in H5N1 Disease
• Case report of 31 yo male who presented with 4 day Hx of fever, cough, and sputum– CXR on day 6 showed LLL pneumonia– Tracheal aspirate + H5N1 by RT-PCR and
culture– Oseltamivir 150 mg bid started day 9 of
illness but progressive bilateral pneumonia– Convalescent plasma infusions from H5
survivor (200 ml X 3) on days 12-13• Plasma neutralizing ab titer of 1:80
– Hospital discharge on day 30
Zhou et al. NEJM 357:1450, 2007

Convalescent Plasma Therapy in H5N1 Disease
• Relative contributions of exogenous plasma, endogenous immune responses, and oseltamivir ?
Zhou et al. NEJM 357:1450, 2007
• H5N1 hyperinduces COX-2 and proinflam-matory cytokine RNAs in macrophages but not type 2 alveolar epi cells, compared to H1N1.
• COX-2 expressed in epithelial cells of autopsy lung tissue of H5N1 patients