epidemiology and recent concepts in dental caries
DESCRIPTION
EPIDEMIOLOGY AND RECENT CONCEPTS IN DENTAL CARIES INCLUDING DIAGNOSIS AND PREVENTION AND MANAGEMENTTRANSCRIPT
EPIDEMIOLOGY AND RECENT CONCEPTS IN DENTAL CARIES
PRESENTED BY OMANAKUTTAN KR
CONTENTS INTRODUCTION DEFINITION PATTERN AND TRENDS GLOBAL AND INDIAN SCENARIO FACTORS INVOLVED RECENT CONCEPTS - DIAGNOSIS - PREVENTION - MANAGEMENT
DEFINITION EPIDEMIOLOGY
The study of the distribution and the determinants of health related states and events in specified population and the application of this study to control health problems ( John Last 1988.)
EPIDEMIOLOGIST A person who defines the frequency and severity of health problems in relation to such factors like age, sex, geography, nutrition, diet etc

RELEVANCE OF EPIDEMIOLOGICAL STUDIES ???
2 terms are of utmost importance in epidemiology
INCIDENCE and Point PREVELANCE Period
DURATION OF DISEASE AND INCIDENCE /PREVALANCE
……RELATION
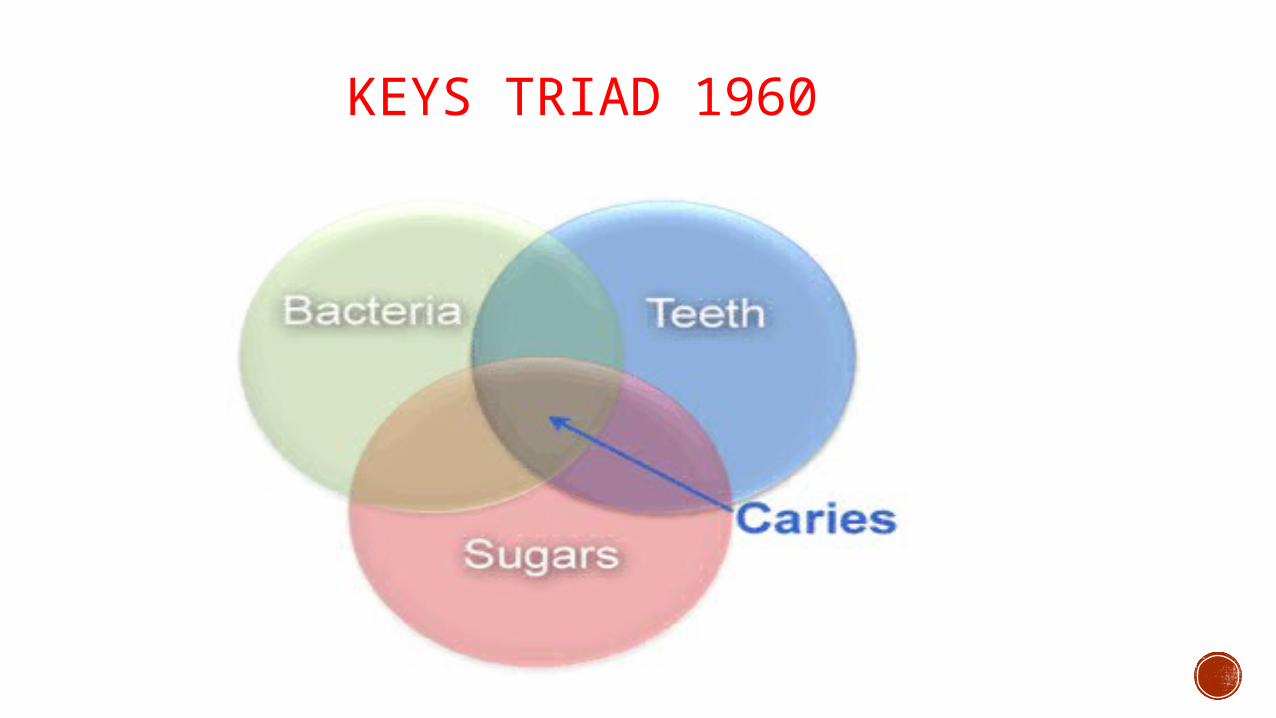
KEYS TRIAD 1960
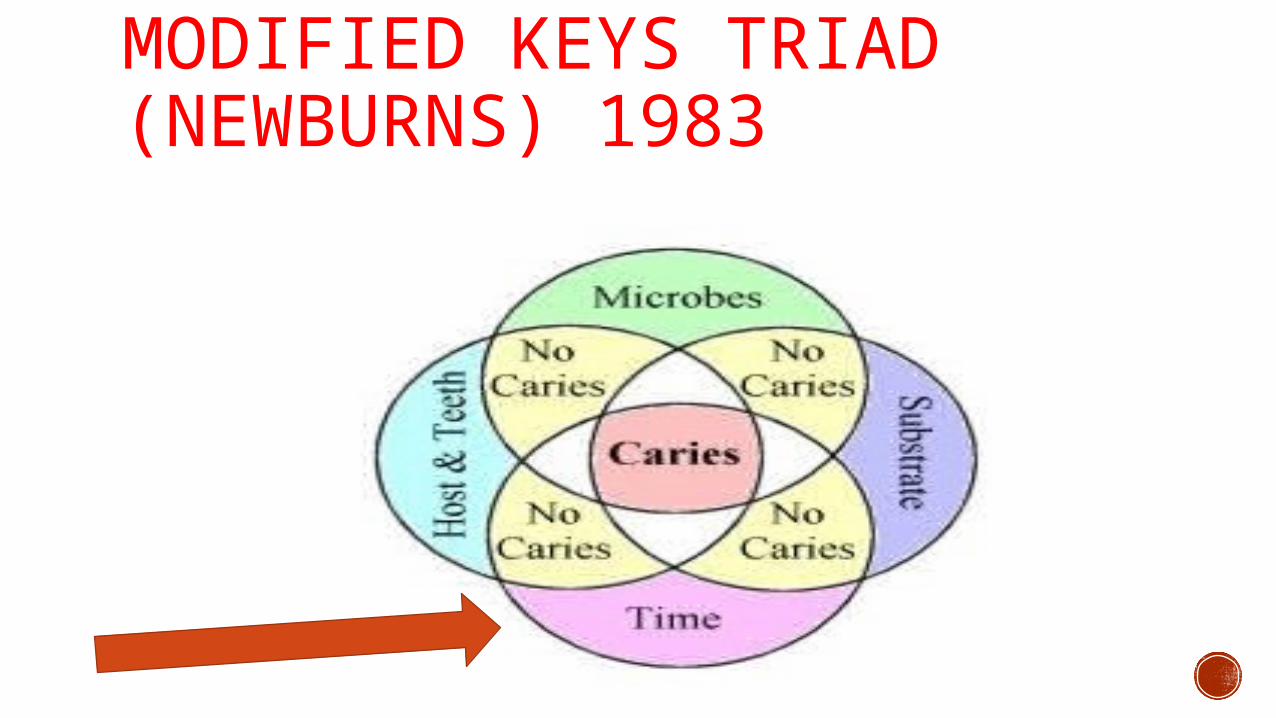
MODIFIED KEYS TRIAD (NEWBURNS) 1983
Dental Caries is an oral disease of pandemic proportion and to measure its extend and severity accurately is impossible
The closest we can assess these parameters are by epidemiological
studies that target a population which can then be generalized.
LOW CARIES INCIDENCE EXISTED IN ANCIENT MAN
LOW CARIES INCIDENCE IN THE ANCIENT MAN IS DUE TO DIET WHICH WAS :
Comparatively low in carbohydrates.
Natural (unrefined) diet.
PATTERN OF ANCIENT DENTAL CARIES
• The pattern of ancient caries was mostly cervical or root caries
PATTERN OF ANCIENT DENTAL CARIES
in the 17th century a new pattern emerged…… lesion begins in fissured surfaces and develops later on proximal surfaces.
• This pattern took place in the industrialized nations as a result of the increased use of sucrose as sugars became more available.
CURRENT GLOBAL DISTRIBUTION
During most of the 20th
century, dental cariespattern was :I. High prevalence in developed
countries & higher socioeconomic group.
II. Low prevalence in developing countries with less economic development.
Caries was referred to as “a disease of civilization.”
High level of consumption of refined carbohydrates in developed
countries
Diet low in fermentable carbohydrates in developing countries
surviving on farming lower level of cariogenic bacteria.
Explanation of this pattern is :
BY THE LATE 20TH CENTURY, CARIES PATTERN WAS CHANGING IN TWO WAYS:
1- Sharp rising in caries prevalence and severity in most developing countries especially urban areas.
2- Marked reduction among children & young adults in developed countries.
M0LLER et al.1999
The decline of caries is attributed to:
Use of fluoridated tooth paste. (Brathall et al.1996)
Fluoridation of water supplies.
The use of fissure sealants.
Implementation of preventive programs
better access to dental care
better living conditions.
GLOBAL DISTRIBUTION
Upward trend of caries in many developing countries is related to:
The absence of widespread caries preventive strategy.
Increasing consumption of sugar containing products.
Moeller et al 1999
GLOBAL SCENARIO AND CURRENT TRENDS Dental caries is still a major health problem in most industrialized countries, affecting
60-90% of school children Substantial decrease in caries prevalence in the last decades in western countries
In developing and underdeveloped countries, prevalence of caries seems to be increasing
REASONS FOR THIS CHANGE…. Increase in dental man power along with an upswing in dental health education,
more demand for dental care have resulted in decrease in dental caries experience.
INDIAN TRENDS
Caries experience is high in all age groups
percentage of subjects with caries increased as age advanced.
The percentage of subjects with caries range from about 52% in primary dentition 85% in permanent teeth in older adults(65-74 years).
Root caries prevalence was 4.5% among the 35-44 years individuals and 5.5% among the 65-74 years individuals. Prevalence of root caries was higher in rural areas than in urban areas. B S Shivakumar et.al 2002
HOST FACTORS1) Saliva Composition pH Quantity Viscosity Antibacterial factors.2) Race and ethnic groups3) Age4) Gender 5) Hereditary6) Emotional disturbances.
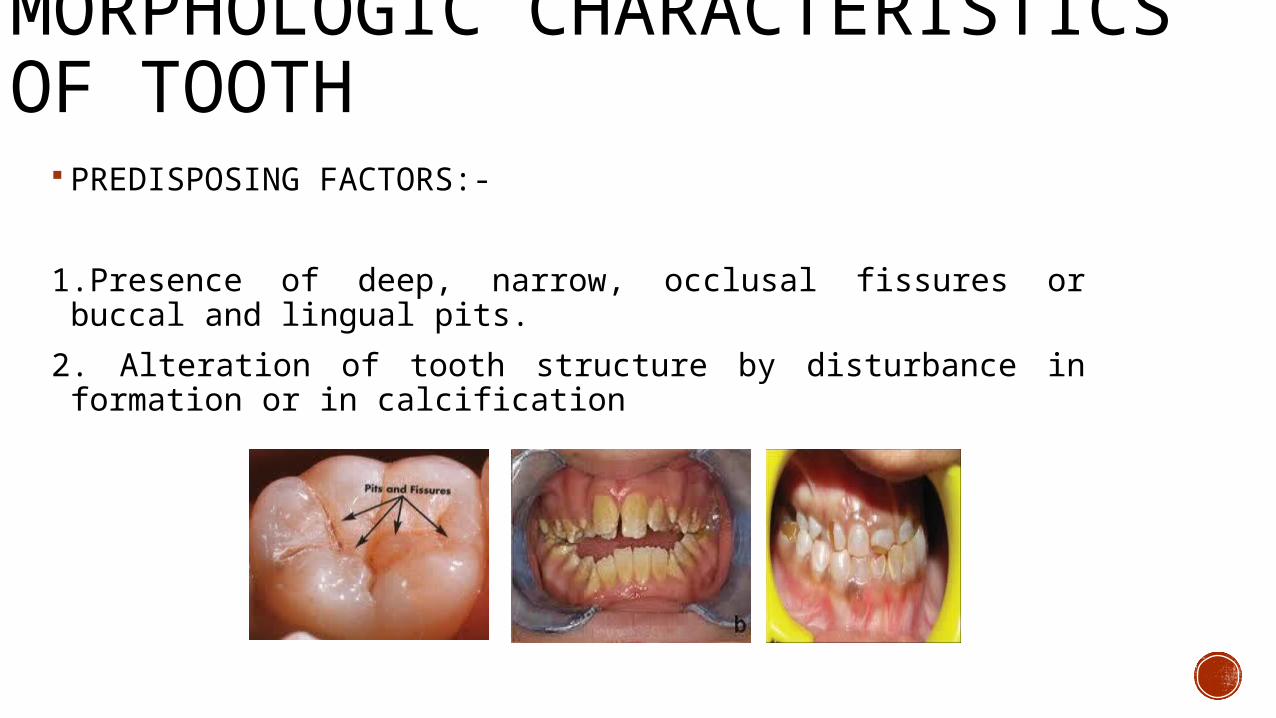
MORPHOLOGIC CHARACTERISTICS OF TOOTH
PREDISPOSING FACTORS:-
1.Presence of deep, narrow, occlusal fissures or buccal and lingual pits.
2. Alteration of tooth structure by disturbance in formation or in calcification
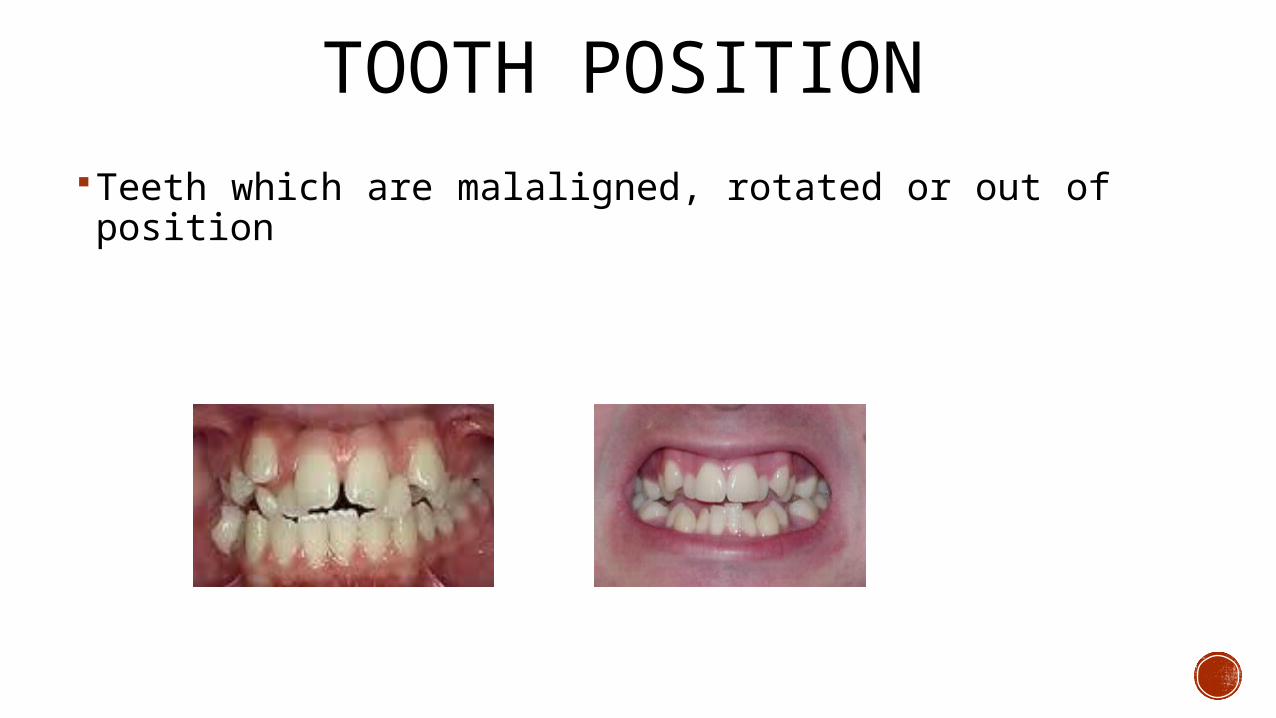
TOOTH POSITIONTeeth which are malaligned, rotated or out of position
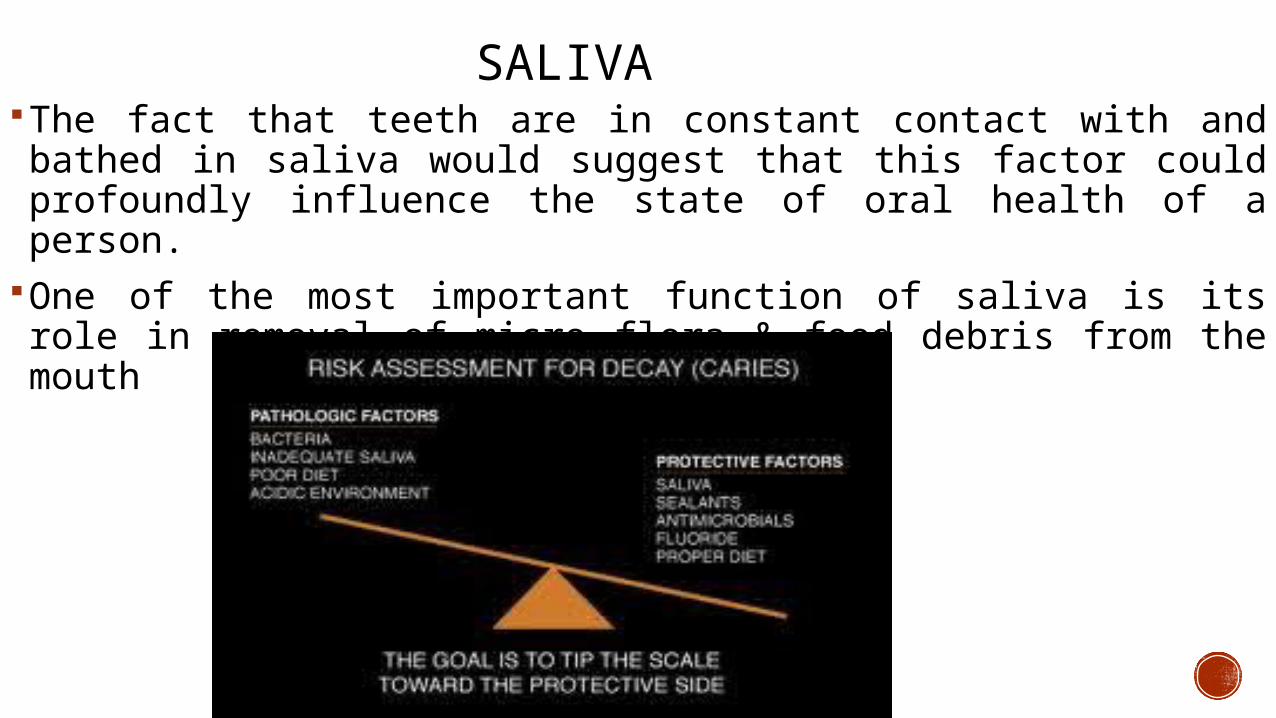
SALIVAThe fact that teeth are in constant contact with and bathed in saliva would suggest that this factor could profoundly influence the state of oral health of a person.
One of the most important function of saliva is its role in removal of micro flora & food debris from the mouth
The distribution pattern of dental caries closely follows that of plaque. Thus, the sites in the mouth which are most prone to caries are those where plaque accumulates.
DISTRIBUTION PATTERN OF CARIES
SALIVARY PH Determined mainly by the Bicarbonate concentration Salivary pH increases with flow rate Salivary buffers increase pH of saliva in the oral cavity.
Decrease pH favors caries
RACE OR ETHINC GROUPSCertain races has high degree of resistance to caries.These beliefs have faded as evidence suggests that these differences are more due to environmental factors than inherent racial attributes
Russel et al.1986
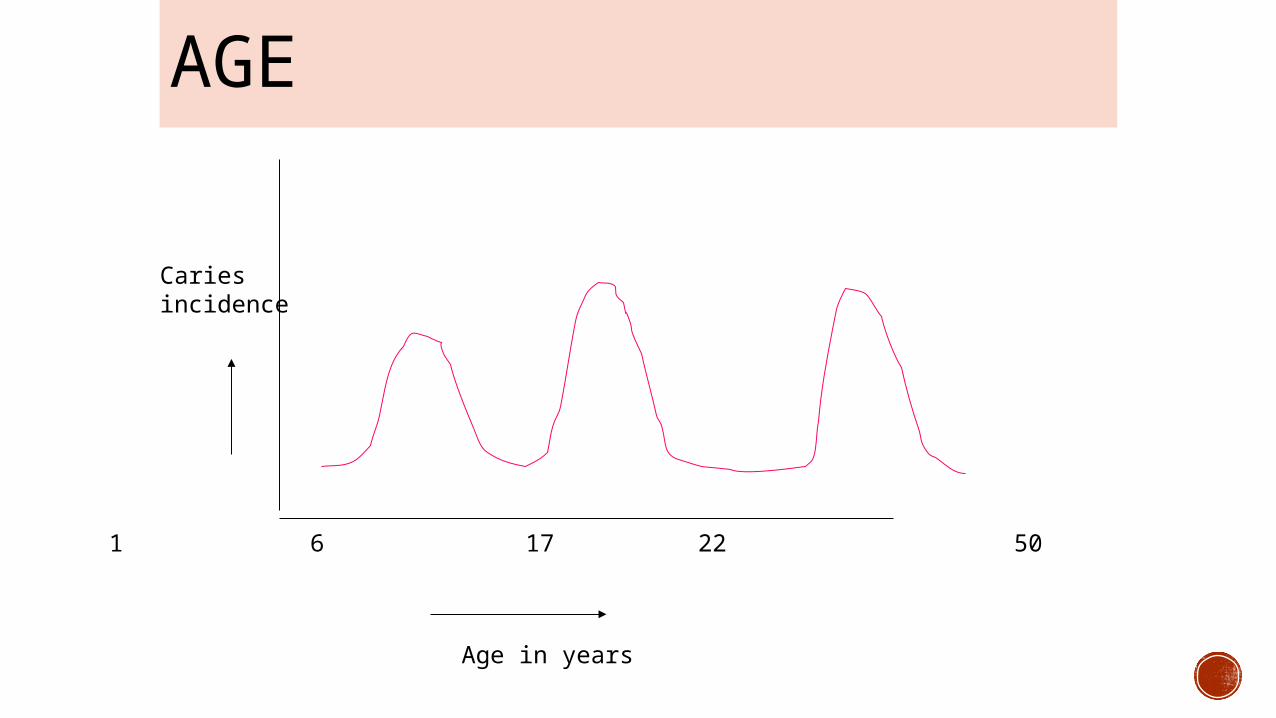
Cariesincidence
Age in years
1 6 17 22 50
AGE
GENDERhigher caries experience in girls than boys
Root caries is more prevalent in males
Increased susceptibility may be due to:1. Early eruption of teeth in females
2. Increased fondness towards sweets among girls3. Due to hormonal changes
Kaste et al 1986
FAMILIAL HEREDITY
“ GOOD OR BAD TEETH RUN IN THE FAMILY”Family studies have shown that offsprings have the same score as parents
Mansbridge (1987) found a greater resemblance in dmf score between identical twins or fraternal twins than unrelated pair of children
EMOTIONAL DISTURBANCESPeriods of stress have been associated with high caries incidence
Schizophrenics have reduced caries activity which may be attributed to increased salivation and higher pH of saliva
SOCIOECONOMIC STATUS It is difficult to correlate caries pattern with socioeconomic status due to its complexity
low SES groups have more number of decayed & missing teeth but less number of filled teeth and vice versa in high SES group
MICRO FLORAMutans Streptococcus – initiation of smooth surface caries
Lactobacillus - Initiation of pit and fissure caries, progression of smooth surface caries
Actinomyces - Root caries
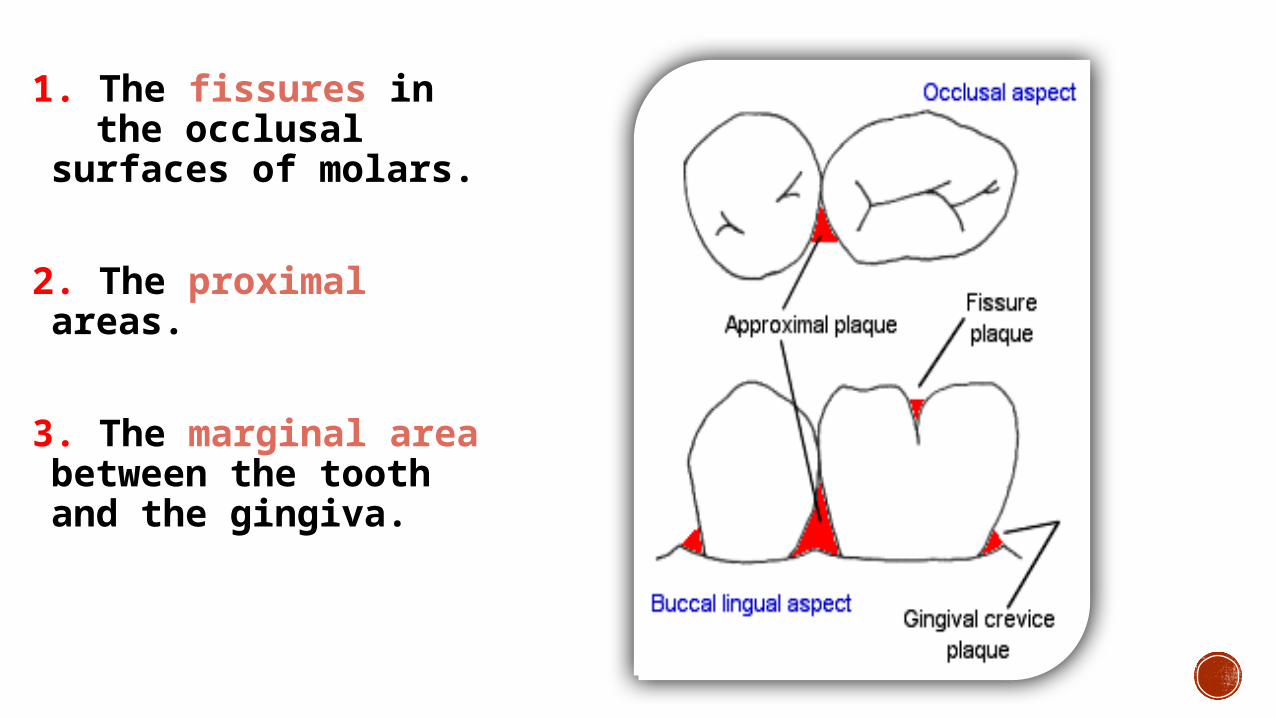
1. The fissures in the occlusal surfaces of molars.
2. The proximal areas.
3. The marginal area between the tooth and the gingiva.
SUSCEPTIBILITY OF DIFFERENT TEETH
According to the pioneering Hagerstown studies (1937), the rank order of susceptibility of teeth to caries is listed as follows:

Mandibular 1st & 2nd molars
Max. 1st & 2nd molars Mand. 2nd,max. 1st & 2nd premolars
max. central & lateral incisors.
Max. canines & mand. 1st premolars
Mand. Central& lateral Incisors & canines.
1
2
3
4
5 Hagerstown studies (1937)
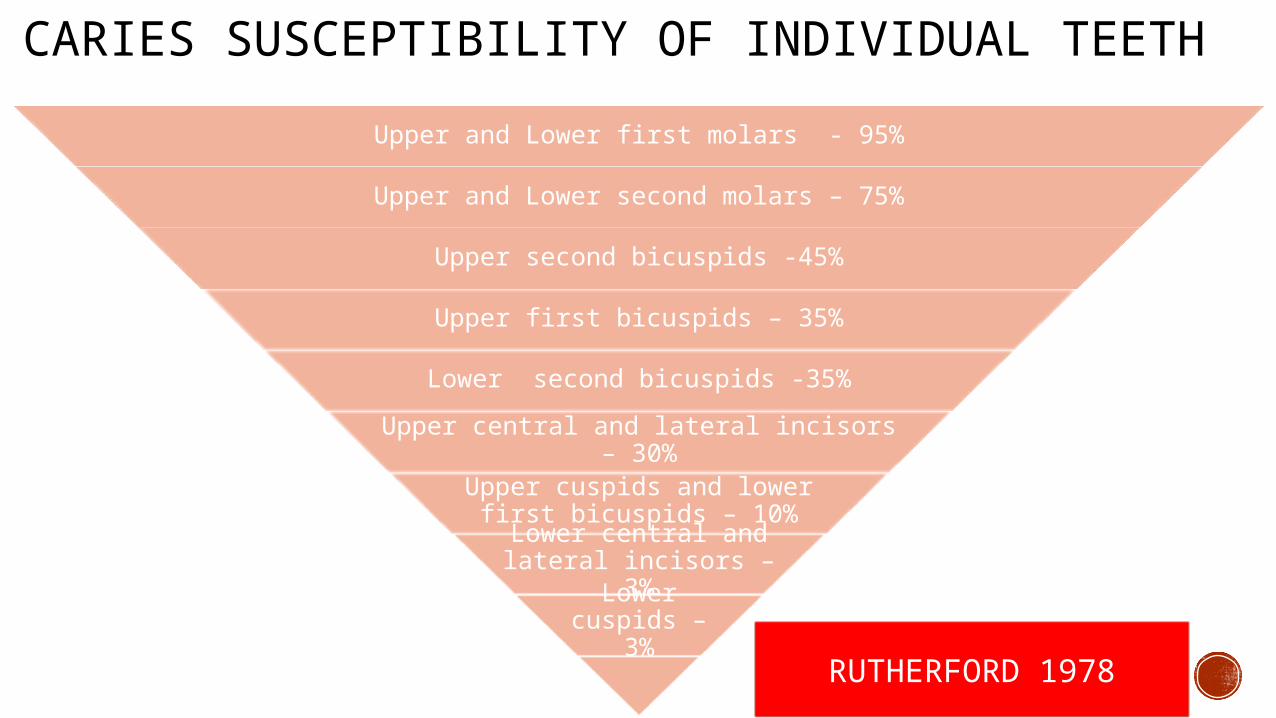
CARIES SUSCEPTIBILITY OF INDIVIDUAL TEETHUpper and Lower first molars - 95%
Upper and Lower second molars – 75%
Upper second bicuspids -45%
Upper first bicuspids – 35%
Lower second bicuspids -35%
Upper central and lateral incisors – 30%Upper cuspids and lower first
bicuspids – 10%Lower central and
lateral incisors – 3%Lower cuspids –
3% RUTHERFORD 1978
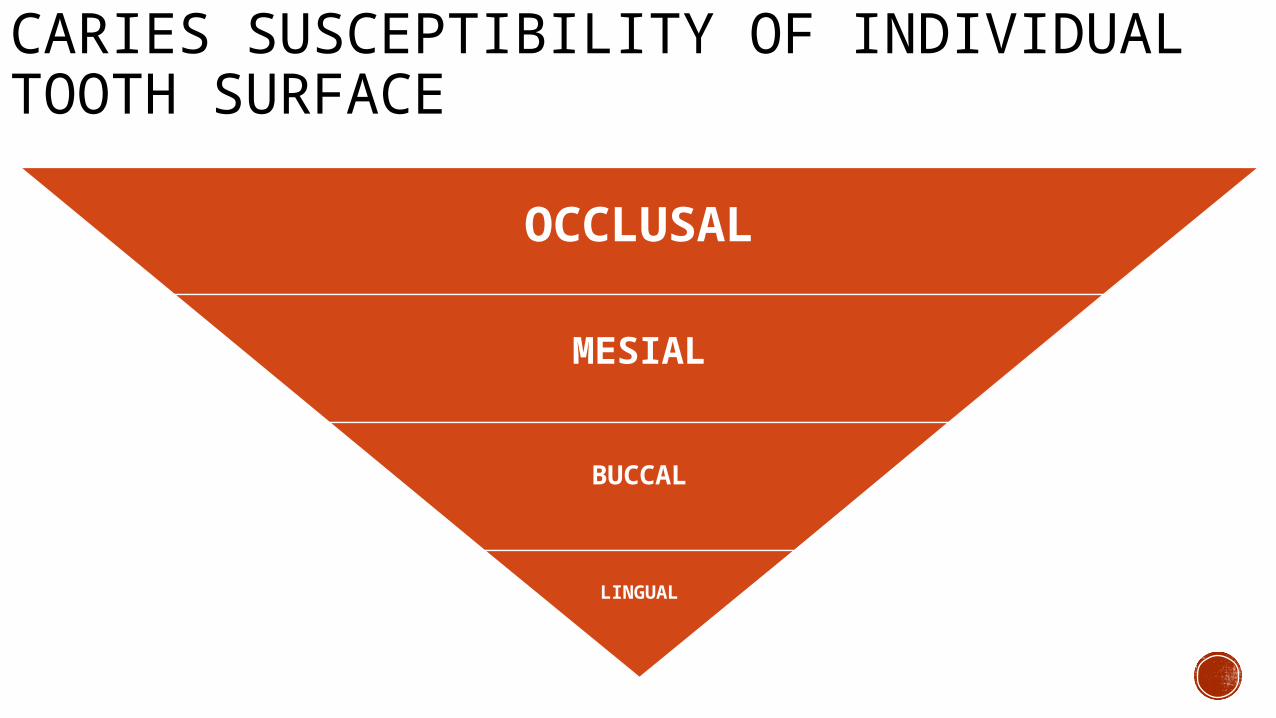
CARIES SUSCEPTIBILITY OF INDIVIDUAL TOOTH SURFACE
OCCLUSAL
MESIAL
BUCCAL
LINGUAL
RECENT CONCEPTS IN DENTAL CARIES
Scientific advances in cariology have led to the understanding that
dental caries is a chronic, dietomicrobial , site-specific disease caused by a shift from protective factors favoring tooth remineralization to destructive factors leading to demineralization. JADA 2009;140(9 suppl):25S-34S.
From antient times there has been multiple theories involving the
initiation of dental caries
THEORIES OF DENTAL CARIES
THEORIES Legend of Worm Humoral Theory Chemical Theory Vital Theory Parasitic Theory Acidogenic Theory Proteolytic Theory Proteolytic Chelation Theory
DIAGNOSIS – RECENT CONCEPT
44
WHAT IS DIAGNOSIS?
Defined as utilization of scientific knowledge for identifying a disease process and to differentiate it from other disease process.
CARIES DIAGNOSIS
IMPORTANCE OF DIAGNOSISTo identify etiological factors
Determine nature of the disease involved
To determine treatment planning
To access prognosis 45
46
ADVANCES IN VISUAL METHODINTERNATIONAL and CARIES DETECTION ASSESSMENT
SYSTEM (ICDAS)
Created in 2002 based on visual examination aided by a WHO PROBE
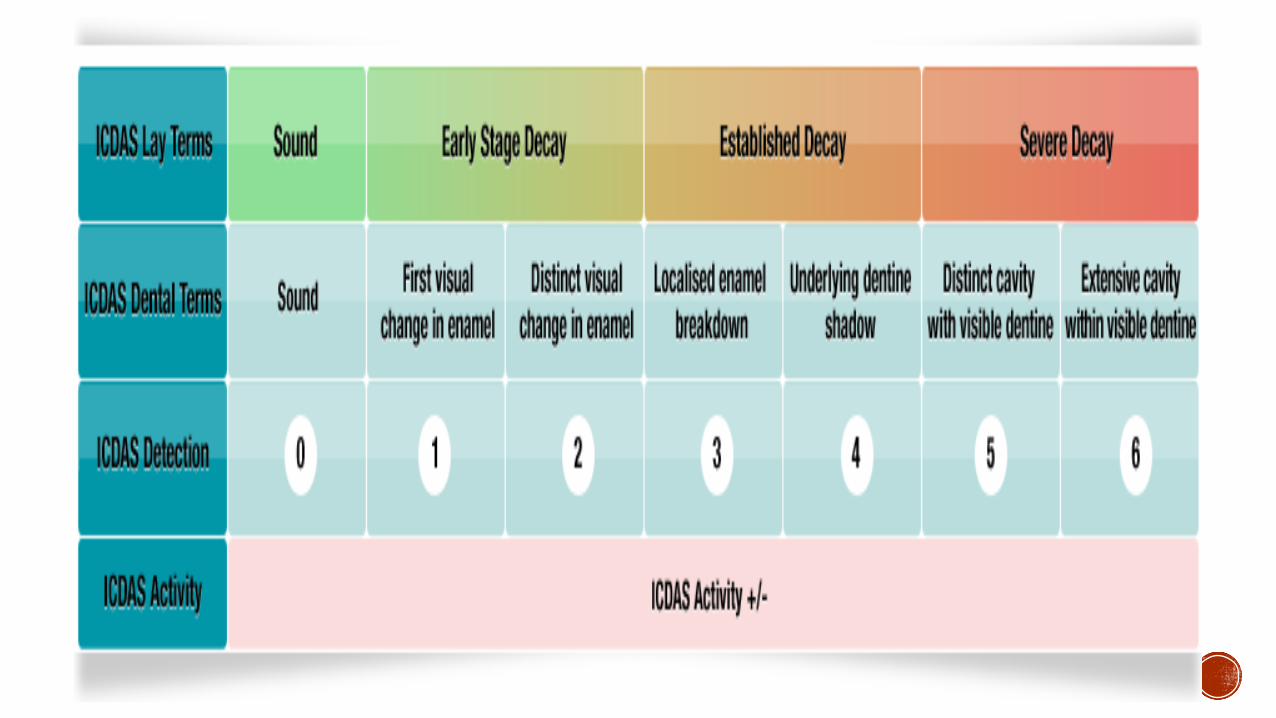
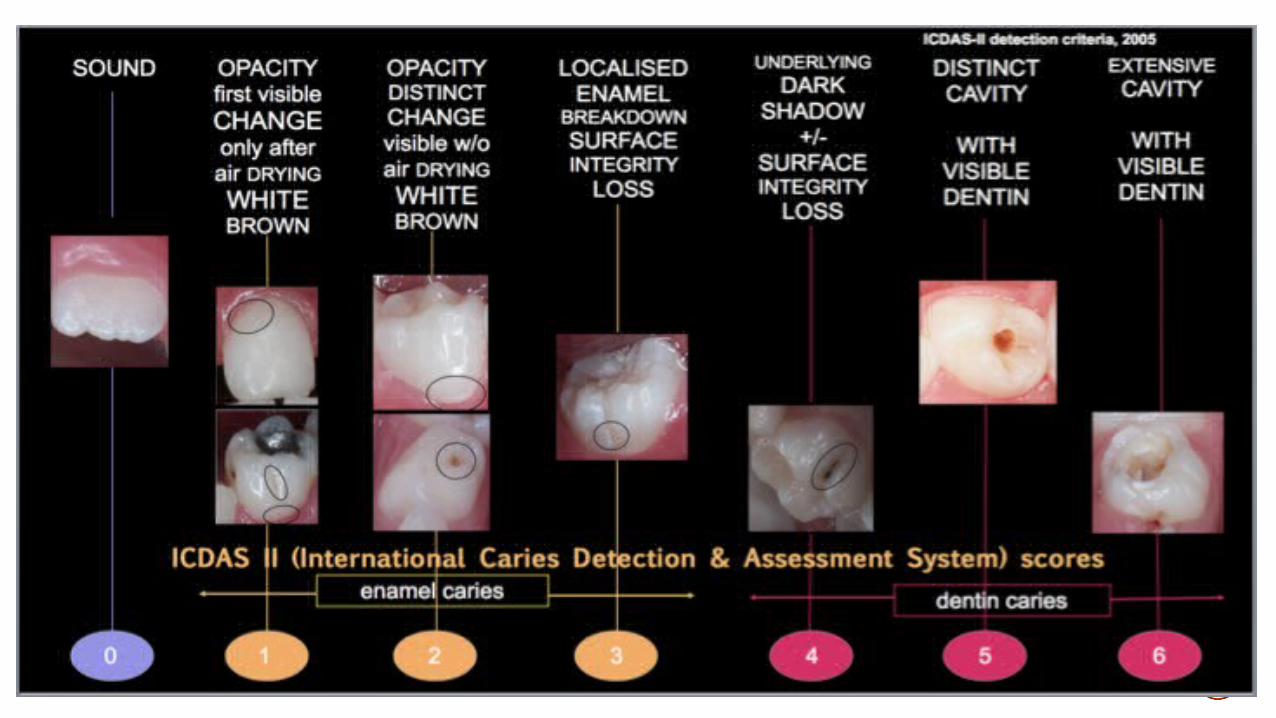
2 digit system (x-y)Scoring system of 0,1,2,3,4,5,6 with respective criterias
NYVAD’S SYSTEM
For activity assessment of non cavitated and cavitated lesions
Scores of 0,1,2,3,4,5,6,7,8,9 assigned
CLASSIFIES A LESION AS ACTIVE OR INACTIVE

52
ADVANCES IN X RAYS:Xeroradiography
Digital radiography
Computer aided radiography
Digital subtraction radiography
Tuned aperture computed tomography
XERO RADIOGRAPHY Technique simulates that of photo-copying Image recorded on aluminium plate with a layer of
selenium particles
Xerographic films to record the images produced by X-rays
These are a given a uniform electrostatic charge
X-rays-passes through film-causes the discharge of particles producing a latent image-converted in a processing unit.
53
Advantages-
-edge enhancement -less radiation -economical
Disadvantages -
electrical charge may cause discomfort to patients exposure time varies with thickness of film process of development cannot be delayed more than 15min 54
DIGITAL IMAGINGPrinciple: works on a CCD which is electronically connected
to computer
CCD-is a semi-conductor made of metal oxide silicon coated with x-ray sensitive photons
55
Advantage no dark room processing greater exposure latitude reduced radiation dose capability of teletransmission image manipulation ability to enlarge specific area
Disadvantage high cost of the system life expectancy is not fixed
56
57
Digital radiography
Direct: Indirect
DIGITAL IMAGINGVariety of multiple well established digitalsensors are available
1. Charge couple device based sensors (CCD)
2. Complimentary metal oxide semiconductors (CMOS)
3. Photo stimulable phosphor plates (PSP)
58
59
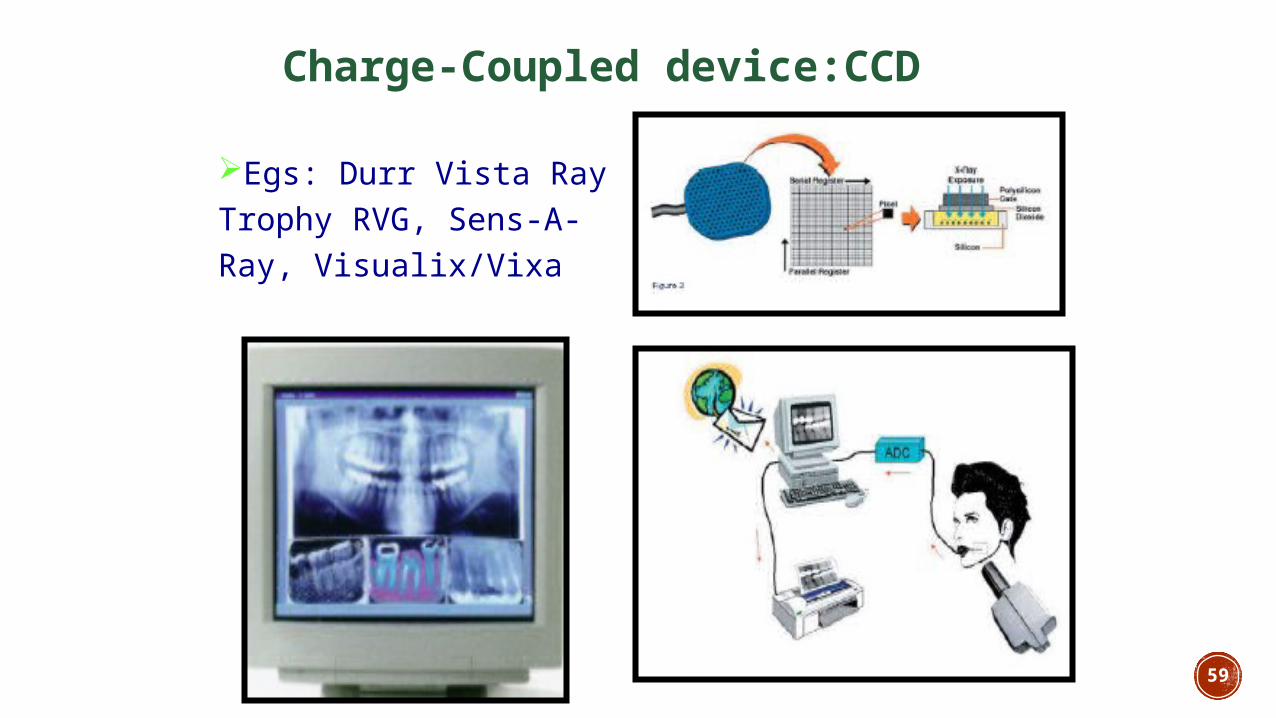
Charge-Coupled device:CCD
Egs: Durr Vista Ray Trophy RVG, Sens-A-Ray, Visualix/Vixa
60
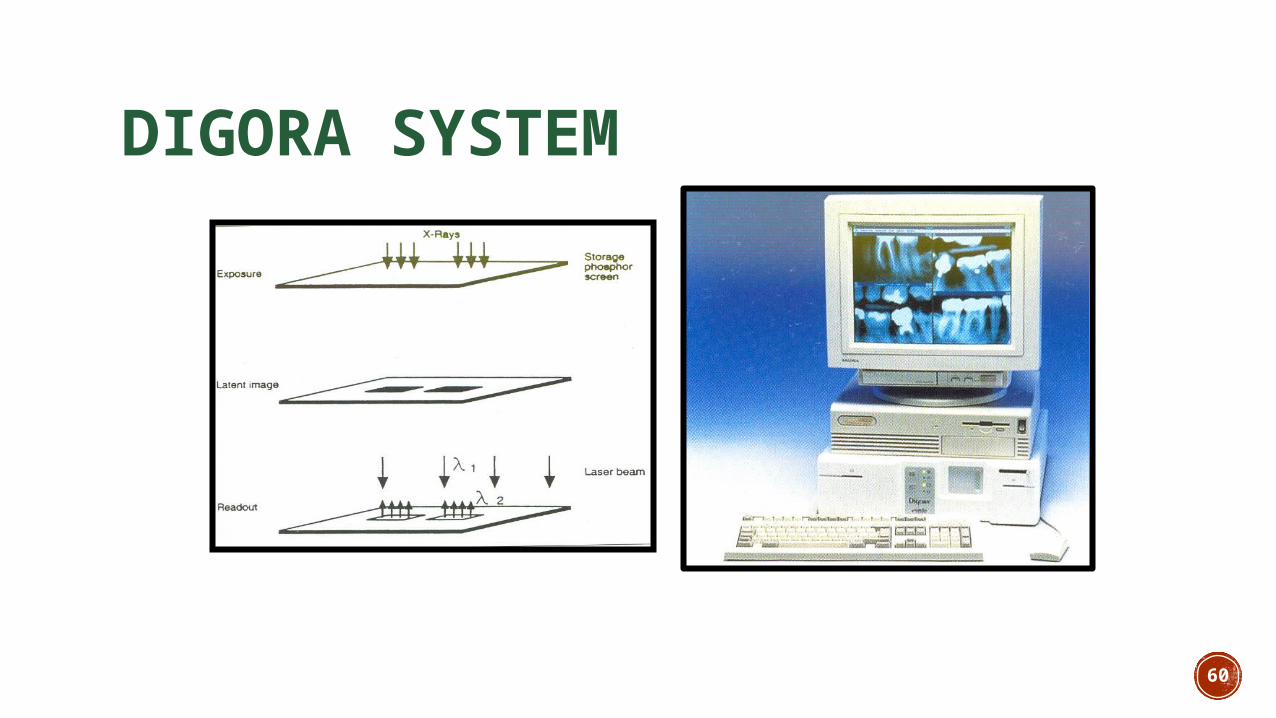
DIGORA SYSTEM
61
According to Kantor et al ( J. Dent. Aug 2005) who compared the conventional radiography with digital radiography and found no statistically significant difference in diagnosis of proximal caries
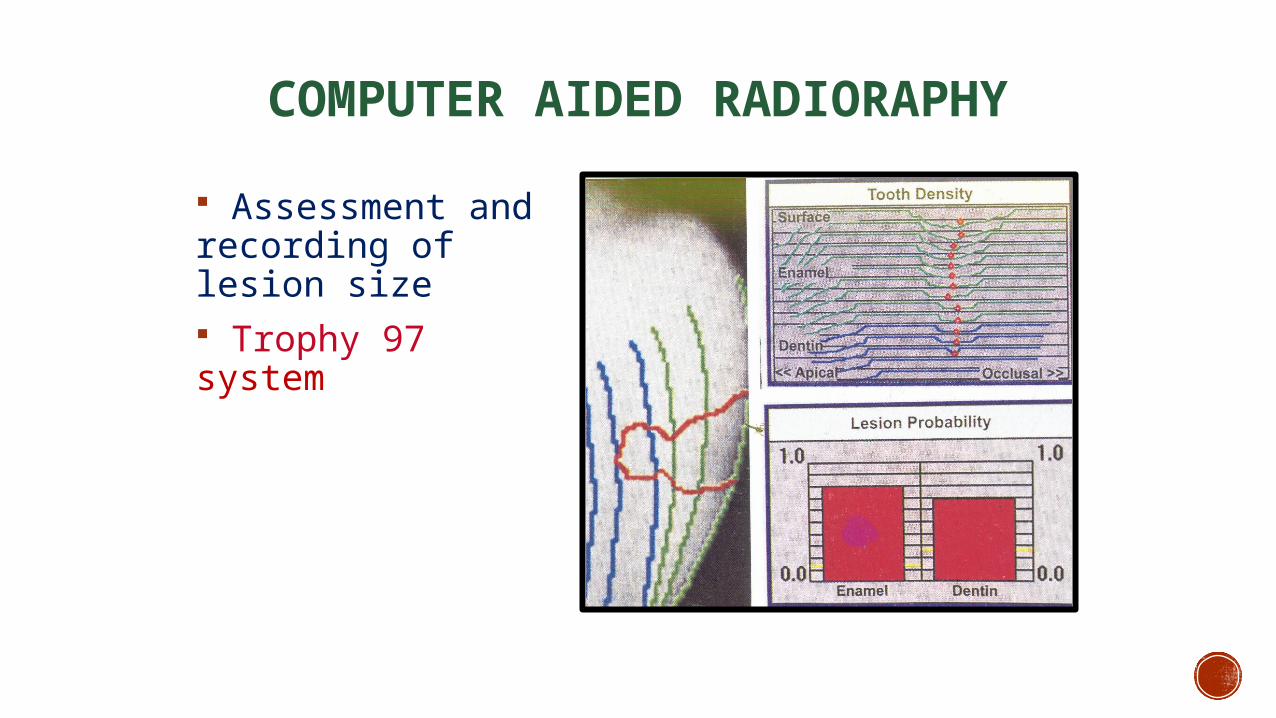
COMPUTER AIDED RADIORAPHY
Assessment and recording of lesion size Trophy 97 system
DIGITAL SUBSTRACTION RADIOGRAPHY
Principle:Optimally, all unchanged anatomical background structures will cancel, and unchanged areas will be displayed in a neutral grey shade in the subtraction image.
Areas with mineral loss appear in darker shades of grey, and areas of gain appear lighter than the background.
63

64
TUNED APERTURE COMPUTED TOMOGRAPHY
It constructs radiographic slices, cross sections, through teeth-viewed for radiolucencies
Images brought to a 3D image- known as pseudohologram
Used in early caries and recurrent caries detection
65
66
ADDITIONAL DIAGNOSTIC METHODS:
67
Based on light:
DIFOTI- DIGITAL FIBRE OPTIC TRANSILLUMINATION
Quantitative laser light fluorescence
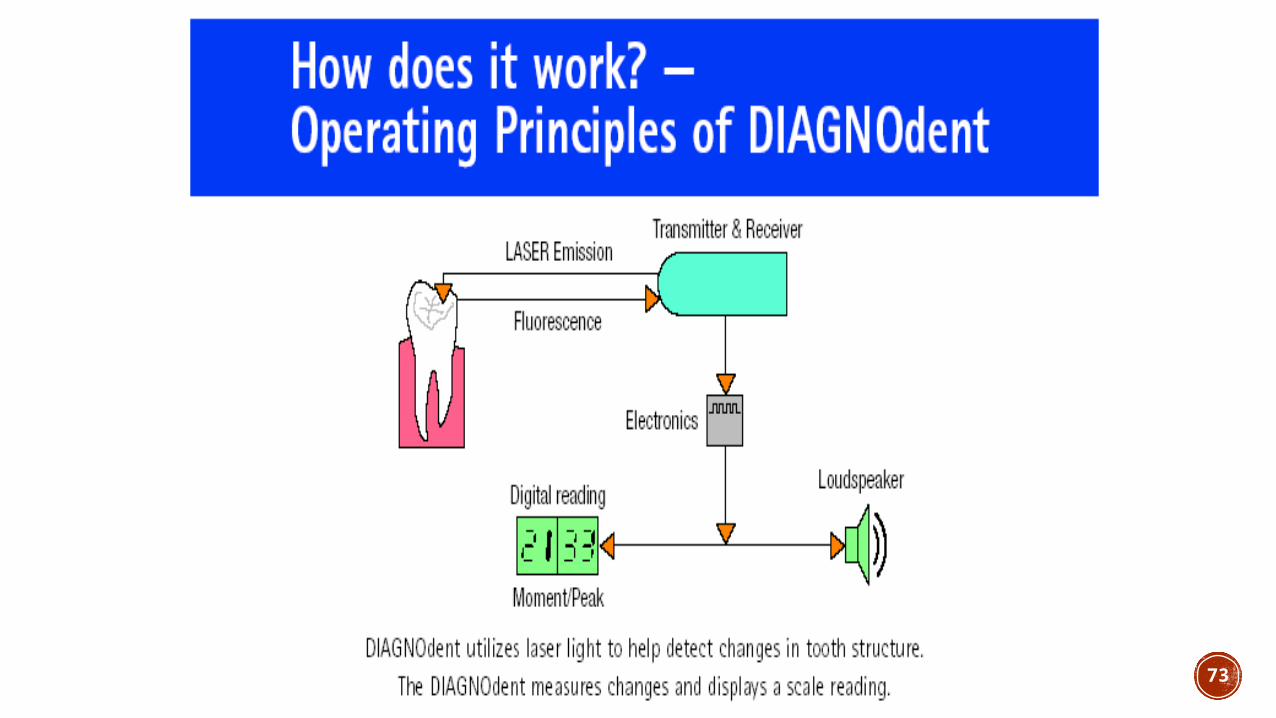
Diagnodent
FLUORESCENCE
A phenomenon by which the wavelength of the emitted light is changed into a larger wavelength as it travels back.
68
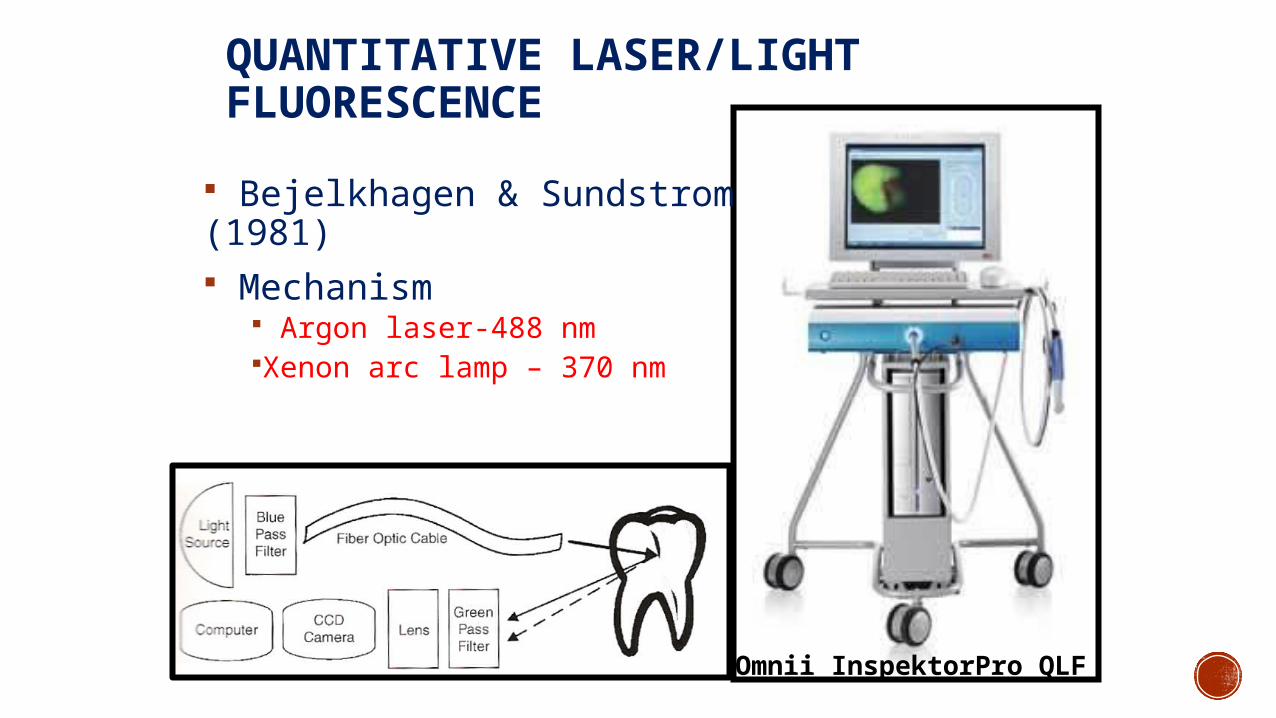
Omnii InspektorPro QLF
QUANTITATIVE LASER/LIGHT FLUORESCENCE
Bejelkhagen & Sundstrom (1981) Mechanism
Argon laser-488 nmXenon arc lamp – 370 nm
70
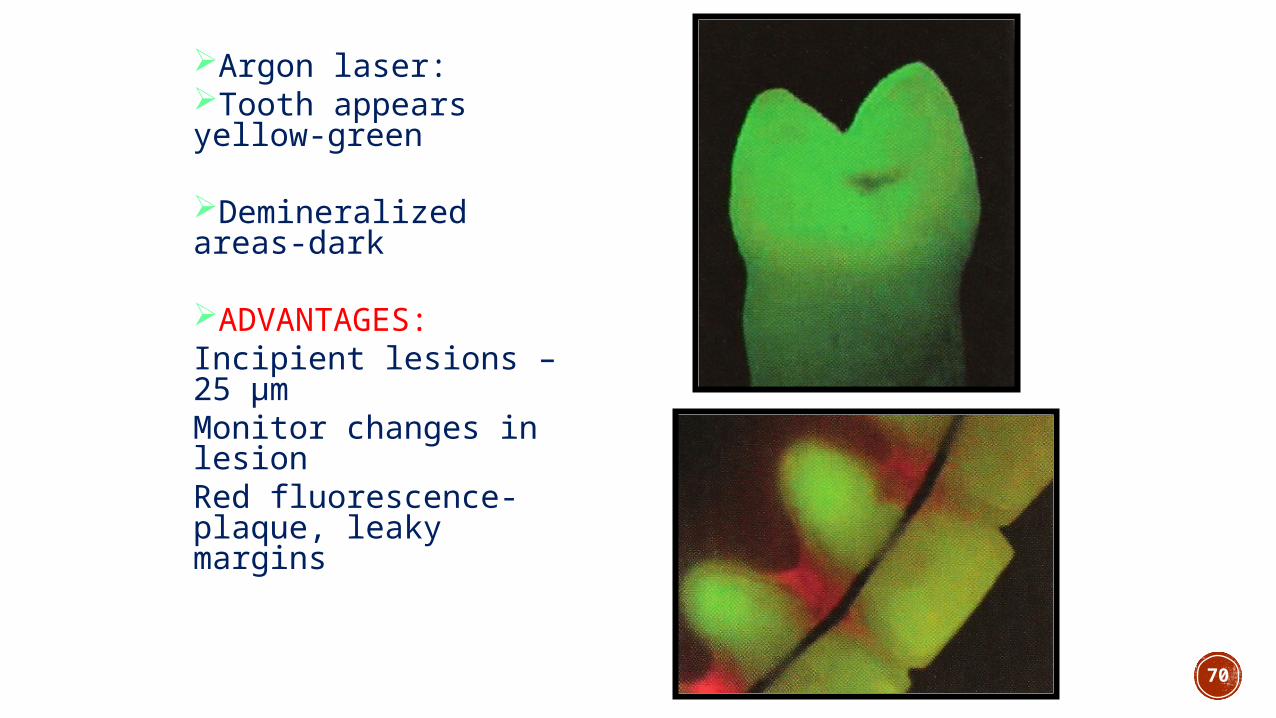
Argon laser:Tooth appears yellow-green
Demineralized areas-dark
ADVANTAGES: Incipient lesions – 25 μm Monitor changes in lesionRed fluorescence-plaque, leaky margins
71
LIMITATIONS:
• On accessible smooth surfaces only• Cant discriminate between enamel & dentin
lesions• Cant differentiate between decay , hypoplasia

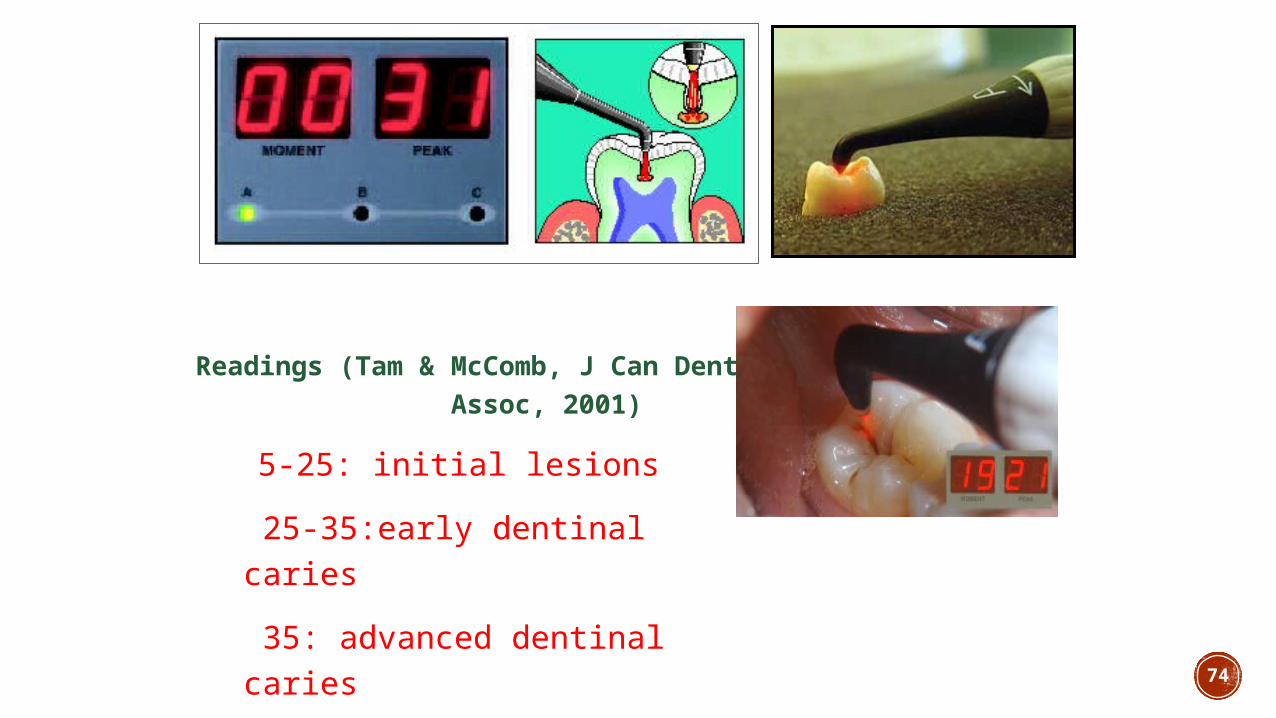
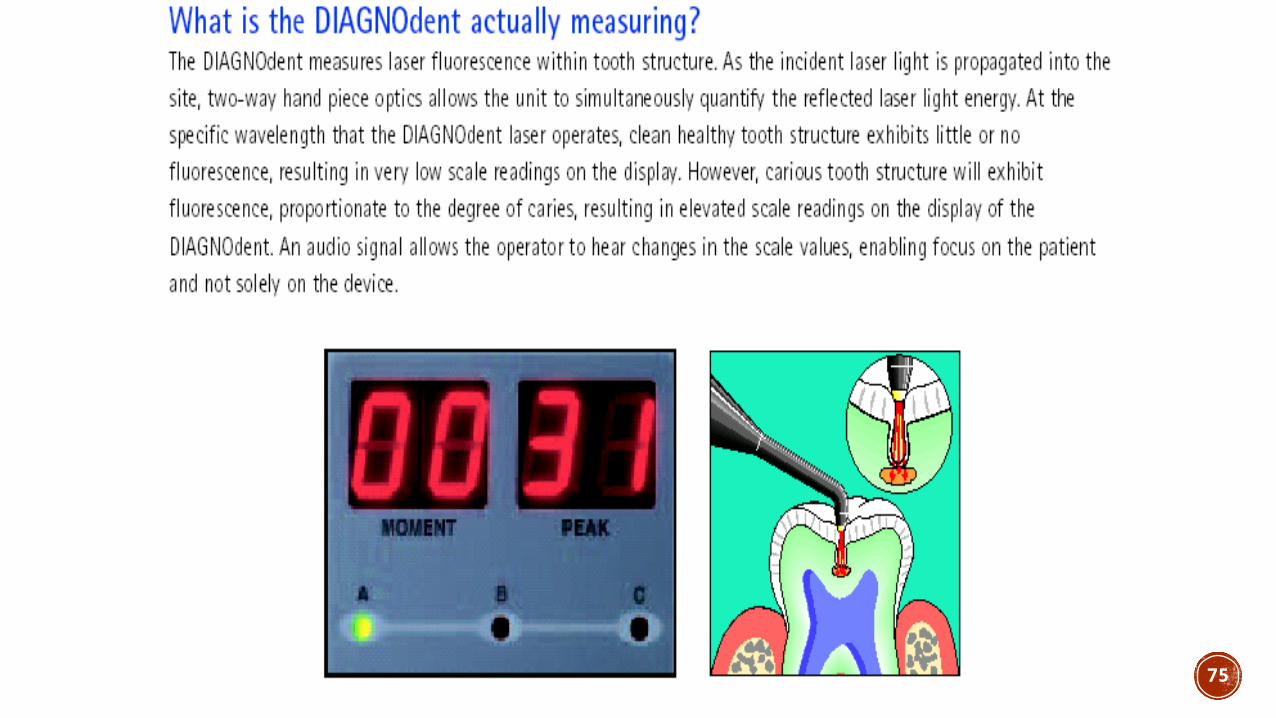
Diagnodent
72
73
74
Readings (Tam & McComb, J Can Dent Assoc, 2001)
5-25: initial lesions 25-35:early dentinal caries 35: advanced dentinal caries
75
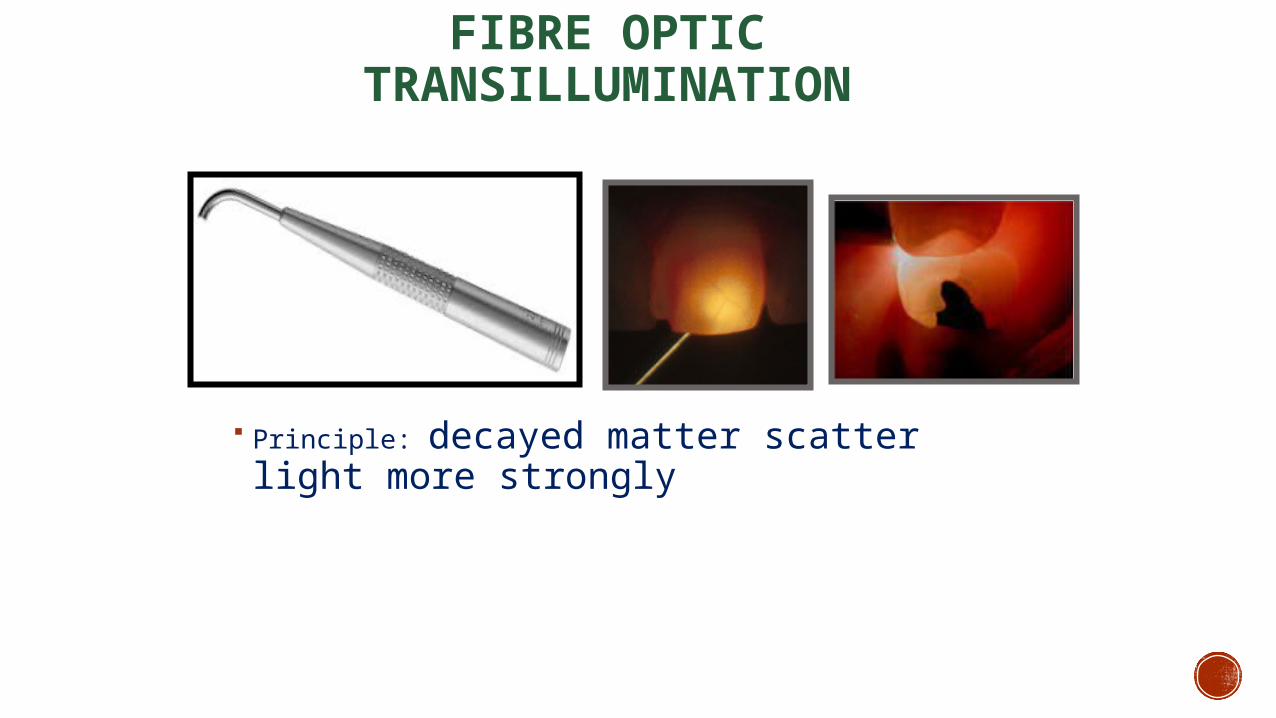
FIBRE OPTIC TRANSILLUMINATION
Principle: decayed matter scatter light more strongly
76
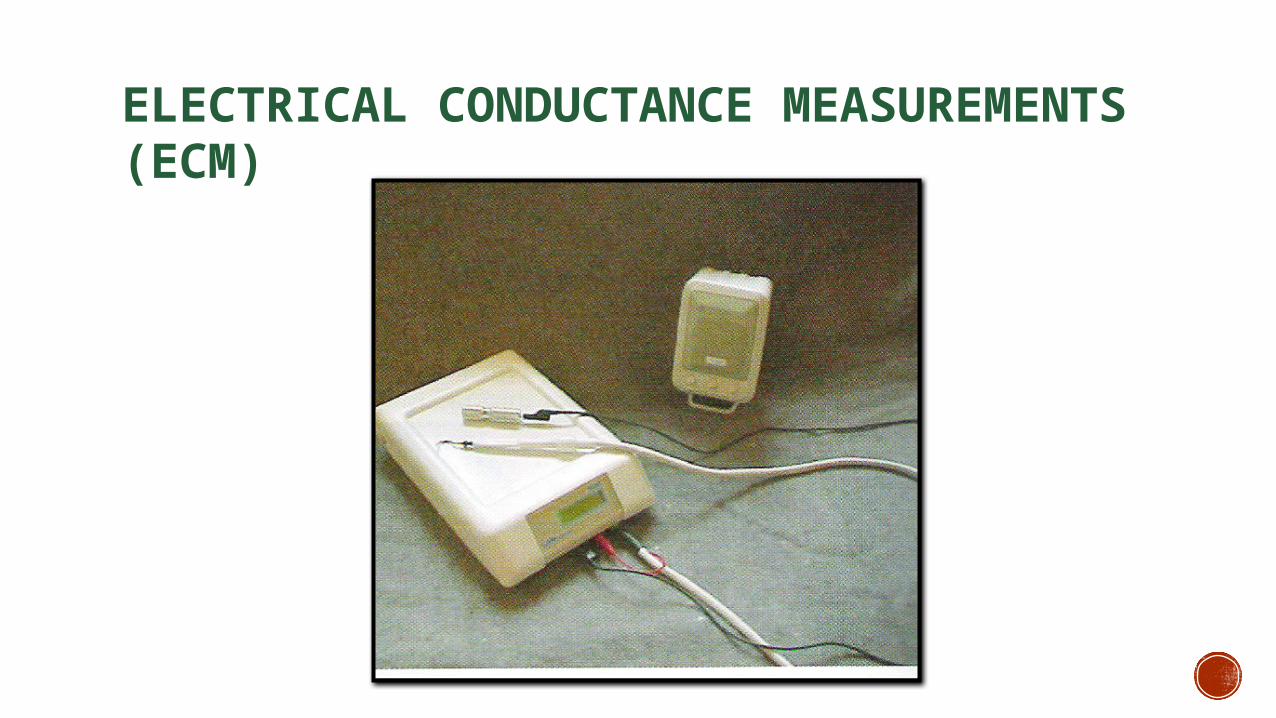
ELECTRICAL CONDUCTANCE MEASUREMENTS (ECM)
77
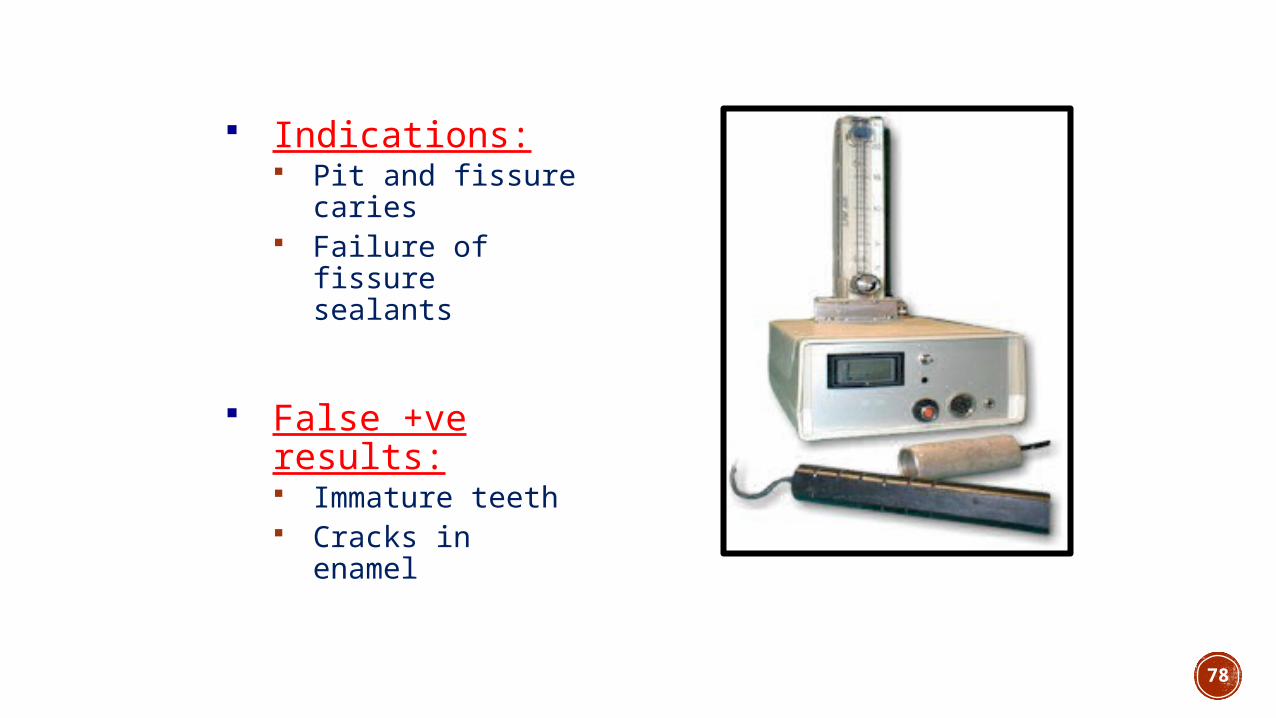
78
Indications: Pit and fissure
caries Failure of fissure
sealants
False +ve results: Immature teeth Cracks in enamel
MANAGEMENT AND PREVENTION – RECENT CONCEPTS
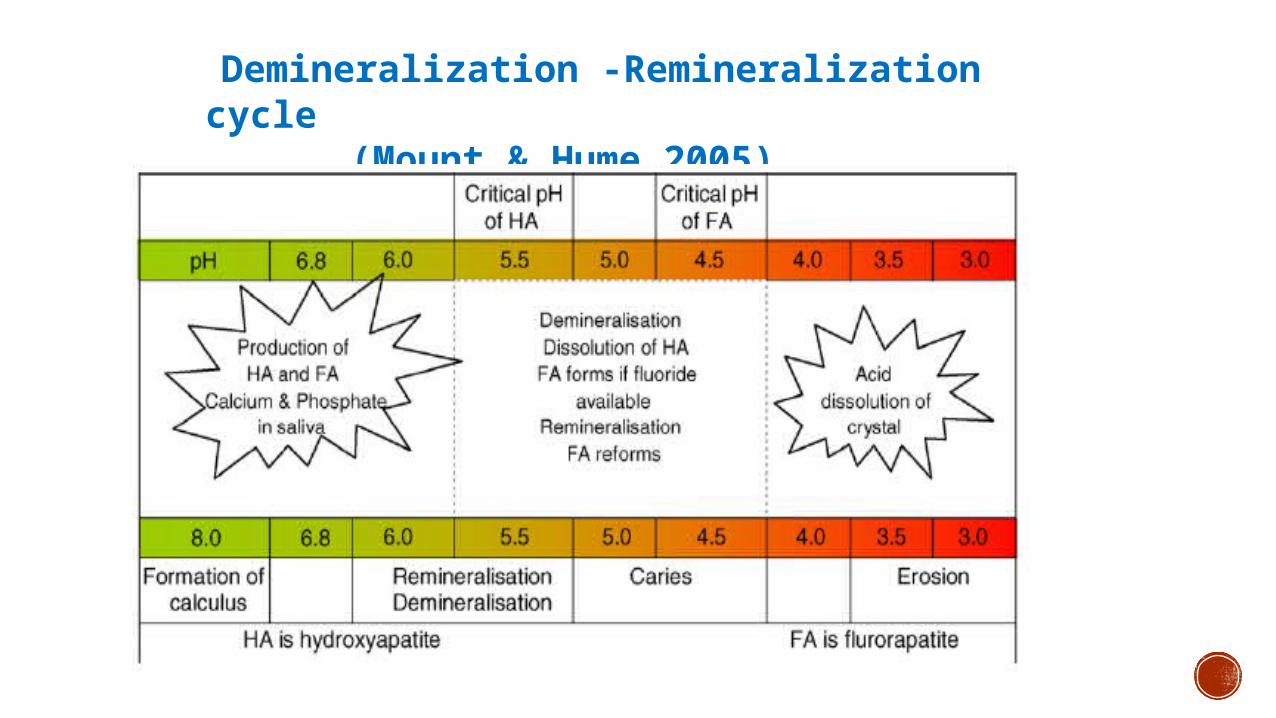
Demineralization-Remineralization cycle
Demineralization -Remineralization cycle (Mount & Hume
2005)
PREVENTION- RECENT CONCEPTS
CARIES MANAGEMENT BY RISK ASSESSMENT (CAMBRA)
CARIOGRAM
TOOTH MOUSSE (CCP-ACP)
CAMBRABuilt on the understanding that dental caries is a dynamic disease
Determines and deals with multiple factors that cause the expression of
the disease and helps take corrective actions
An evidence based approach for prevention of dental caries
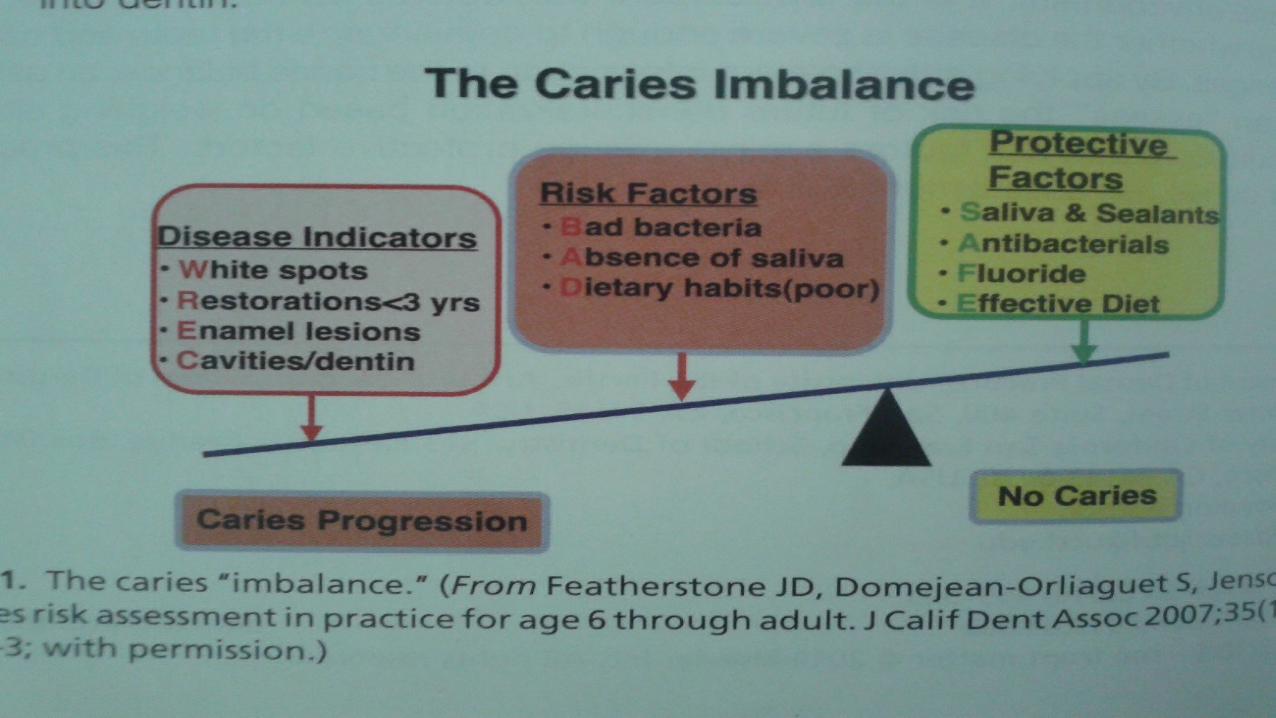
THE CARIES BALANCE/IMBALANCE MODEL
A visual representation of the multifactorial nature of the disease
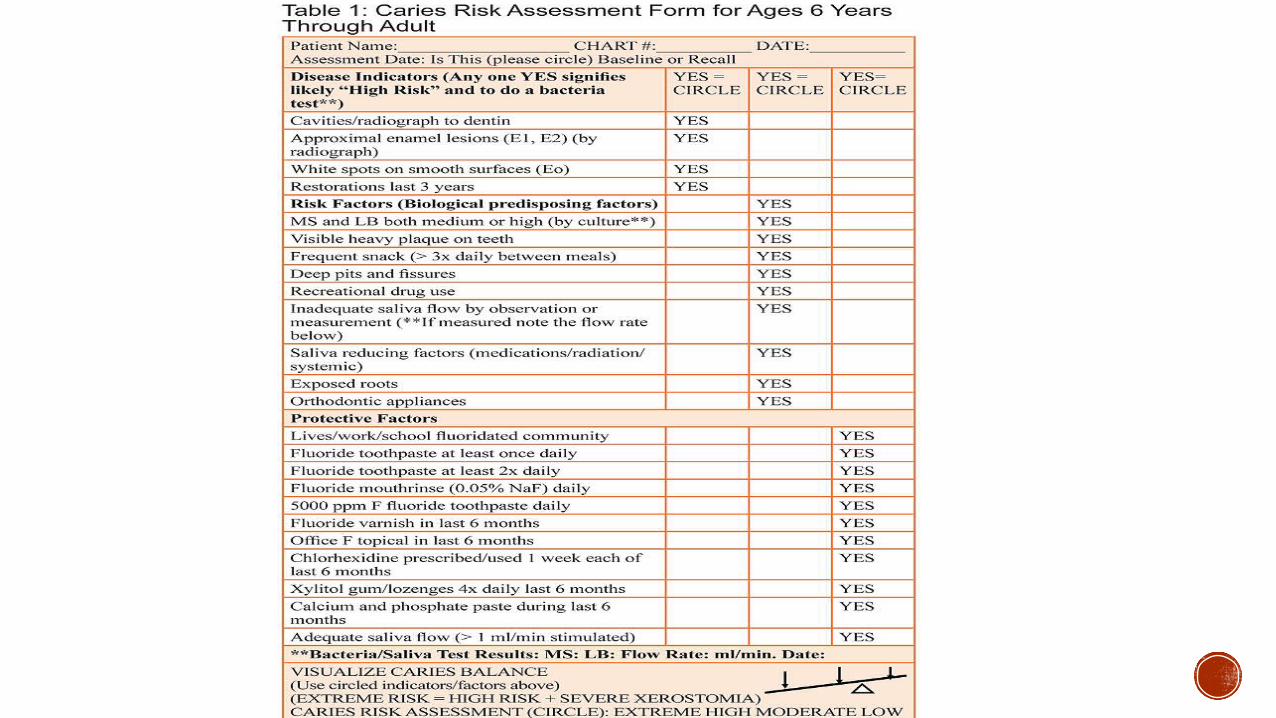
Risk of demineralization can be assessed by weighing all the disease
indicators and risk factors against protective factors
CARIES RISK ASSESSMENT
CARIOGRAMA graphical illustration of the caries risk profile of an individual.
Includes factors directly and indirectly involved in biochemical
events on the tooth surface
ILLUSTRATES AN OVERALL RISK SCENARIO
DATA NEEDEDCARIES EXPERIENCERELATED DISEASEDIET- CONTENTS AND FREQUENCYPLAQUE LEVELMUTANS STREPTOCOCCIFLUORIDE EXPOSURESALIVA SECRETIONSALIVARY BUFFER TEST
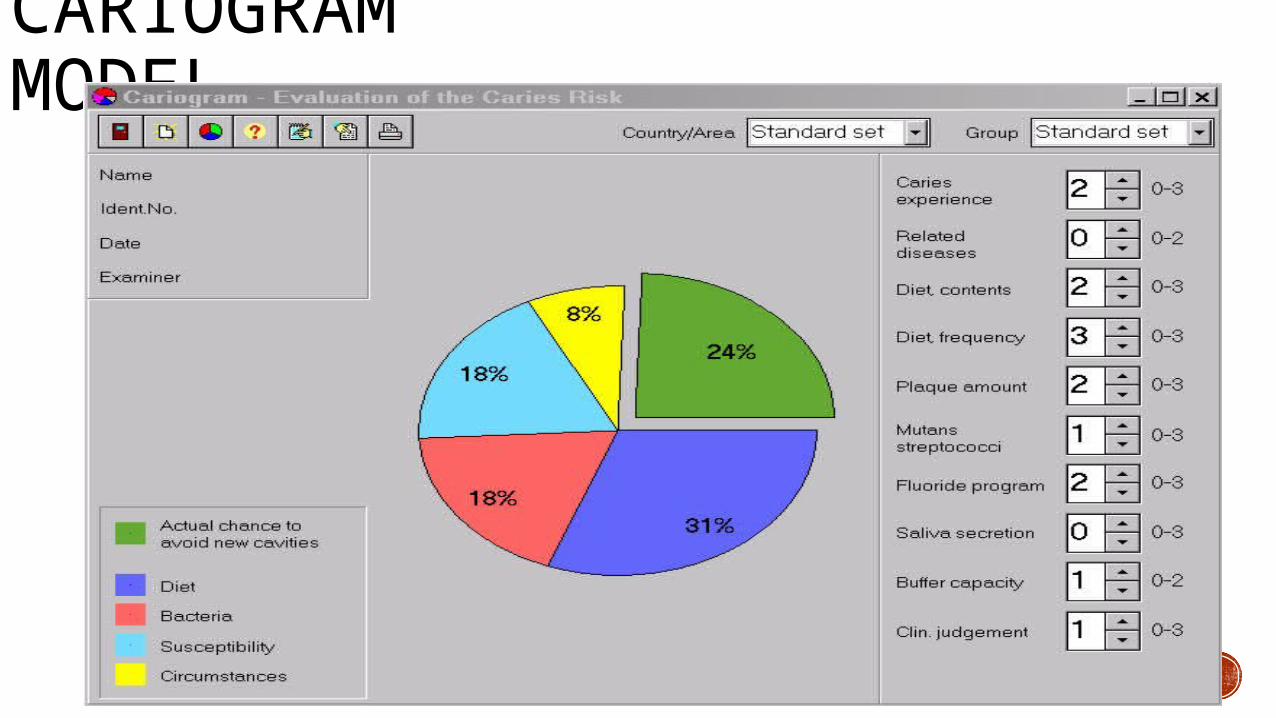
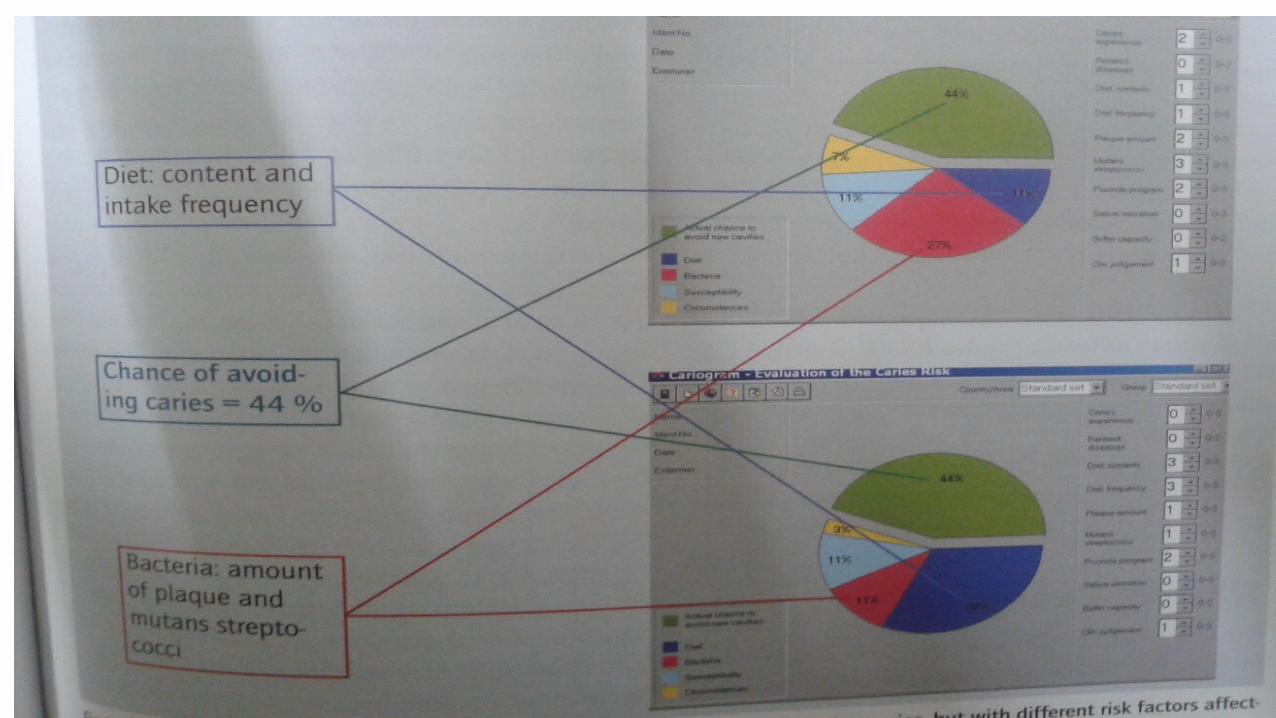
CARIOGRAM MODEL
CASEIN PHOSPHOPEPTIDE AMORPHOUS CALCIUM PHOSPHATE COMPLEXES - CPP-ACPBIOACTIVE PEPTIDE
HAS SPECIFIC PHOSPHORYLATED ELEMENTS CAPABLE OF CALCIUM BINDING
STABILIZES CALCIUM PHOSPHATE AS AMORPHOUS CALCIUM PHOSPHATE
CPP + ACP
SUPERSATURATION
MANAGEMENT - RECENT CONCEPTSCALCIUM SODIUM PHOSPHOSILICATE (BIOACTIVE GLASS) – NOVAMIN
AIR ABRASION
POLYMER CUTTING INSTRUMENTS
CALCIUM SODIUM PHOSPHOSILICATE (BIOACTIVE GLASS) – NOVAMIN
A ceramic material used for remineralization
Combines with water to release calcium, phosphorous , sodium , and silicon
ions and results in hydrocarbonate crystal formation (HCA)
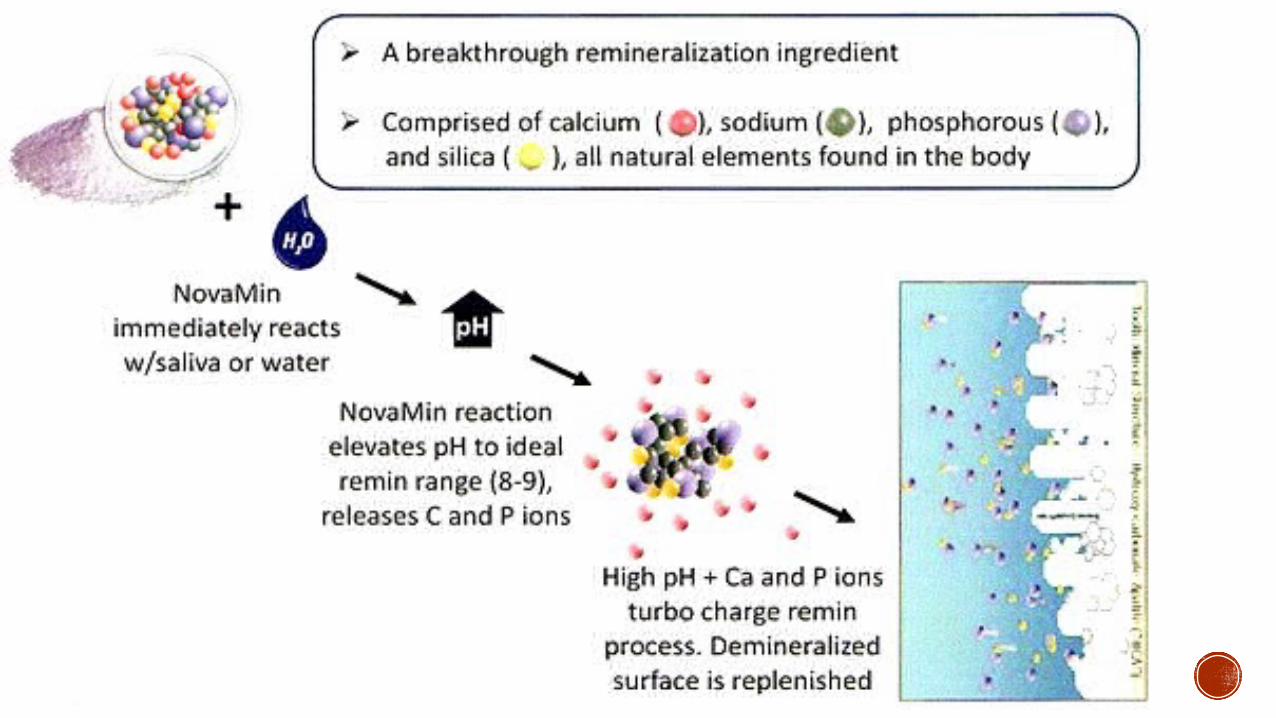
ions
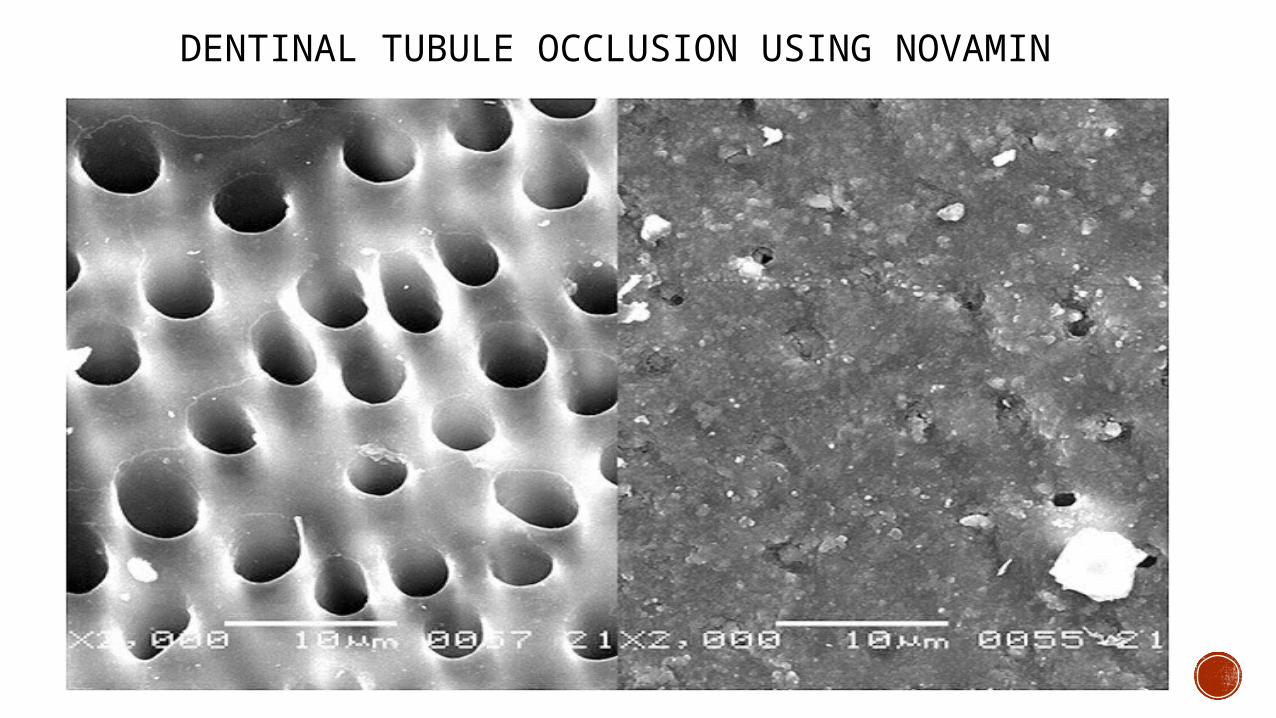
DENTINAL TUBULE OCCLUSION USING NOVAMIN
AIR ABRASION
PSEUDO MECHANICAL, NON- ROTARY METHOD OF CUTTING AND TISSUE
REMOVAL
PRINCIPLE ACTION IS OF END CUTTING TYPE
DESSICATED ABRASIVE PARTICLES ASSIST CUTTING
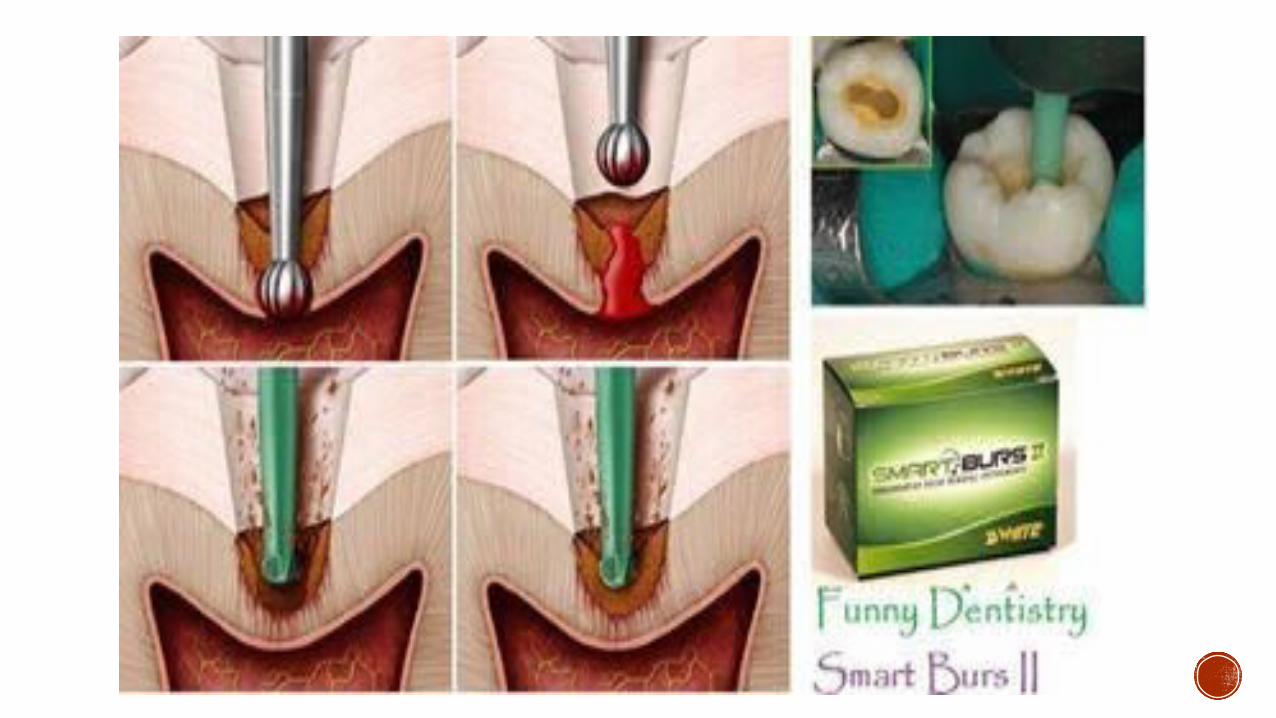
POLYMER CUTTING INSTRUMENTS
DIFFERENTIATE BETWEEN DECAYED AND HEALTHY DENTINE
REMOVES CARIOUS DENTINE NOT SOUND DENTINE
DESIGN IS BASED ON THE DIFFERENTIAL HARDNESS OF TOOTH TISSUE
DOESN’T EXPOSE VITAL ODONTOBLASTS AND HENCE LIMITED PATIENT DISCOMFORT
SINGLE USE DISPOSABLE BURS

THANK YOU