epilepsy and memory david m. treiman, m.d. barrow neurological institute phoenix, arizona
TRANSCRIPT
EPILEPSY AND MEMORY
David M. Treiman, M.D.
Barrow Neurological InstitutePhoenix, Arizona
“. . . The commonest failure is loss of memory and that this, if regarded in all degrees, is more frequent than the integrity of that faculty.”
- J. Russell Reynolds, 1861 Epilepsy: its symptoms, treatment and relation to other chronic convulsive diseases. London: John Churchill
Epilepsy
A neurological disorder characterized by recurrent non-provoked epileptic seizures.
Epileptic Seizure
A clinical manifestation of a transient, usually hypersynchronous, abnormal electrical discharge in the brain, consisting of sudden and transitory abnormal behavioral phenomena (alterations of consciousness, motor, sensory, autonomic, or psychic events).
Epileptic SeizureGeneric description
• Abrupt onset
• Impaired consciousness during event
• Amnesia for the event and part of the post-ictal period
• Post-ictal depressed consciousness, with gradual recovery
Epilepsy & MemoryIssues for consideration
• Ictal amnesia & fugue states
• Post-ictal amnesia
• Inter-ictal memory deficits
Hx. of Concepts of Memory
• Unitary memory
• Multiple memory systems– Franz Joseph Gall & phrenology
– Maine de Biran» Representative memory - recollection of ideas & events
» Mechanical memory - acquisition of habits & skills
» Sensitive memory - memory for feelings
– 19th C neurologists - memory centers
• 1st half of 20th C - back to unitary memory
• Post WWII - multiple memory systems again– Much of renewed interest stimulated by case of H.M.
Case of H.M.• 27 yo motor winder, hs grad, szs since age 10
• Possible TBI age 9, nl PEG x2, EEGs non-focal
• 9/53 bilateral MT resections, posterior to 8 cm
• Post-op no neuro deficit, except memory:– little ability to retain & recollect new information
across a delay
– no difficulty with immediate or short term retention
– could learn new motor skills
– remote memories retained
– FSIQ 112 (vs 104 pre-op)
• Szs persisted, but much less severe & frequent
Scoville & Milner, J Neurol Neurosurg Psychiat 20:11, 1957
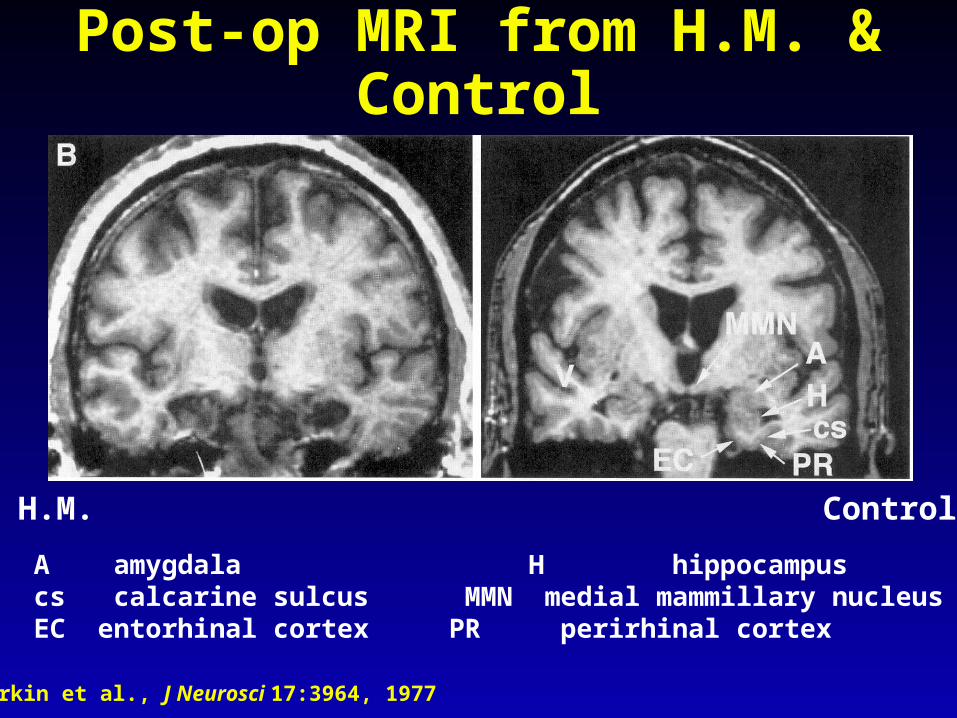
Post-op MRI from H.M. & Control
Corkin et al., J Neurosci 17:3964, 1977
H.M. Control
A amygdala H hippocampuscs calcarine sulcus MMN medial mammillary nucleusEC entorhinal cortex PR perirhinal cortex
Human Memory SystemsDeclarative or explicit memory: recall
• Episodic memory (remembering)– the explicit recollection of incidents that occurred at
a particular time and place in one’s personal past
– mesial TL damage: impairs new acquisition
– prefrontal cortex: impairment of recall of temporal order and of source (when, where)
• Semantic memory (knowing)– general knowledge, not linked to time or place
– mesial TL damage: impairs new acquisition
Human Memory Systems Nondeclarative or implicit memory:
unconscious, no active recall
• Perceptual Representation System– Identification of words and objects based on their
form and structure, but not their meaning.
– Presemantic - not involved in associative or conceptual information, i.e., meaning or function.
– Three major subsystems:» visual word form
» auditory word form
» structural description - relations between parts that determines global structure (what it is).
– Not mediated by mesial temporal lobe
Human Memory SystemsImplicit
• Procedural memory – Acquisition of skills and habits (knowing how)
– Acquired gradually through repetitive practice (e.g., athletes, musicians
– Not dependent on mesial temporal structures
– Cortical striate system critical (HD patients poor at learning new motor skills, altho intact explicit mem.)
– Cerebellum necessary for sequences of movements
Human Memory Systems
• Working memory– short term retention over a period of seconds
– way of holding information on-line in service of comprehending, reasoning, problem solving
– Three components:» phonological loop - allows recycling of speech-based
information - left parietal supramarginal gyrus
» visuaospatial sketch pad - short-term retention of visual and spatial information - several sites right hemisphere
» central executive or limited capacity work space - prefrontal cortex
Summary of Memory
• Explicit memory systems (both episodic and semantic memory) require intact temporal lobe, and thus are at risk in temporal lobe epilepsy.
• Implicit memory systems (perceptual representation system, procedural memory, working memory) are localized outside of the mesial temporal lobe, and thus not at risk in temporal lobe epilepsy.
What is the evidence for memory impairment in temporal lobe epilepsy?
Interictal memory deficits
• Physician impression– Russell Reynolds’ observation (1861)
– Lennox (1942): “…the patient finds it hard to recall events and names, especially those learned recently.”
– Loiseau et al. (1988): “…memory deficits in epileptic patients merit special attention since they seek help for these more frequently than for other mental impairments.”
• Self-reports of patients
• Neuropsychological testing of memory– Many reports, especially in TLE
Factors that may increase riskSummary of older studies
• Identified etiology (risk from underlying disorder)
• Seizure type (TLE for reasons already cited)
• Age of onset/duration of epilepsy
• Frequency and severity of seizures
• “Ictal time”
• Highly disordered EEG
• Antiepileptic drugs
Is neuronal damage progressive in chronic intractable epilepsy?
Impairment of hippocampal-dependent spatial memory after SE
• Abundant evidence from experimental studies– Scoville & Milner 1957, Morris et al. 1982, Holmes et
al. 1988, Stafstrom et al. 1993, Nissinen et al 2000
• Rutten et al 2002 studied development of SE-induced cognitive dysfunction in immature rats
– SE induced by Li/pilo age P20
– Water maze performance at P22,P25, P30,P50
– P50 rats exposed to nonenriched or enriched envir.
– Water maze performance compared between control and SE rats and in SE rats between environments
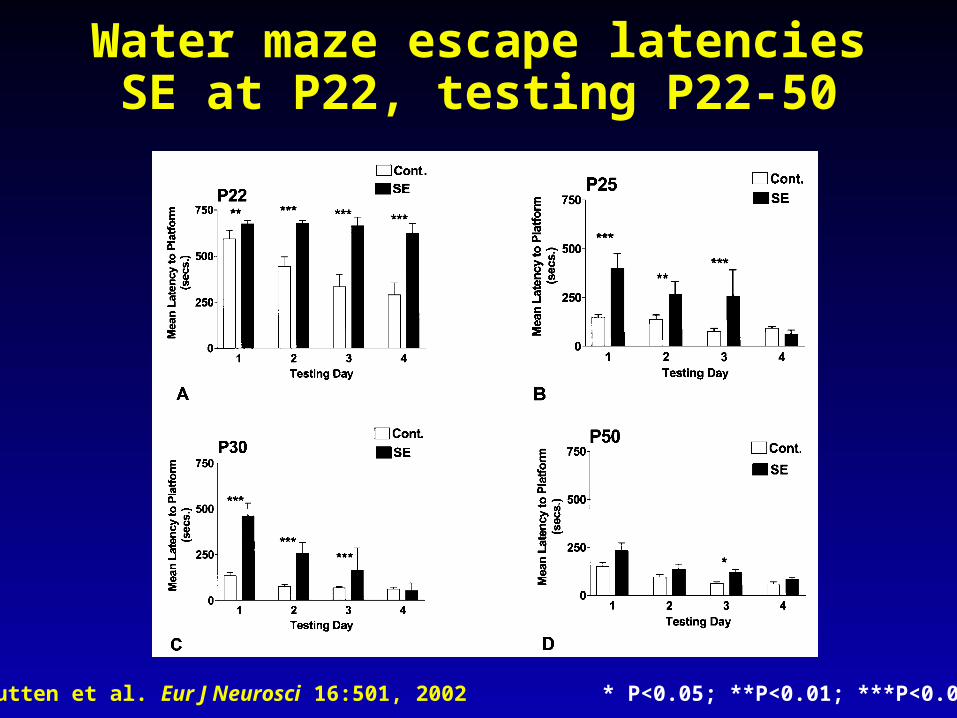
Water maze escape latenciesSE at P22, testing P22-50
Rutten et al. Eur J Neurosci 16:501, 2002 * P<0.05; **P<0.01; ***P<0.001

Enriched EnvironmentToys, moving objects, classical music
Rutten et al. Eur J Neurosci 16:501, 2002
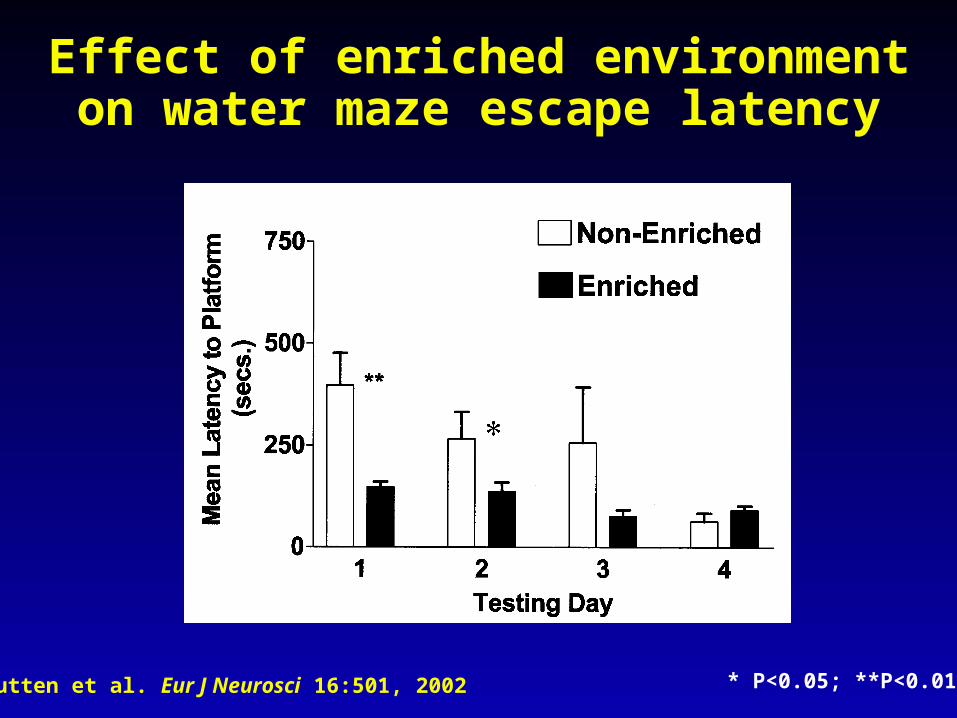
Effect of enriched environment on water maze escape latency
Rutten et al. Eur J Neurosci 16:501, 2002 * P<0.05; **P<0.01
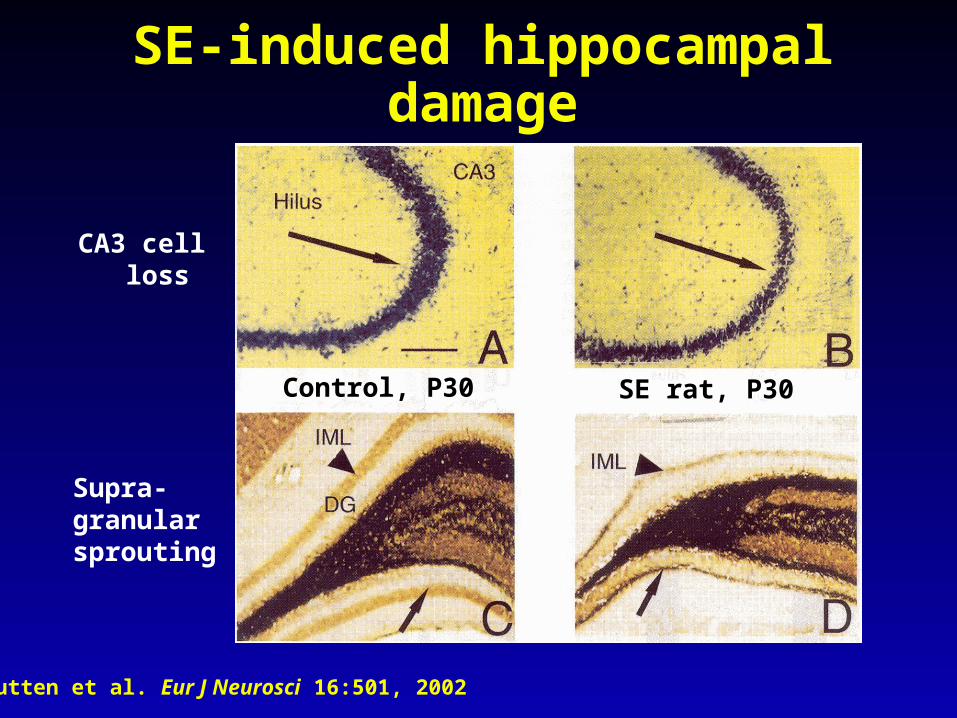
SE-induced hippocampal damage
Rutten et al. Eur J Neurosci 16:501, 2002
Control, P30 SE rat, P30
CA3 cell loss
Supra-granularsprouting
To what extent is memory task- specific in the MT lobes?
Correlations with task specific declarative memory (L > R)
• Hippocampal sclerosis
• Hippocampal neuronal density
• Hippocampal volume
• Hippocampal N-acetylaspartate/creatine ratios
• NAA/Cr better correlated than volume

Sawrie et al., Epilepsia 42:1403, 2002
MRI, Cr/NAA, Verbal Memory
LM% - logical memory percentage retention Cr - creatineNAA - N-acetylaspartate
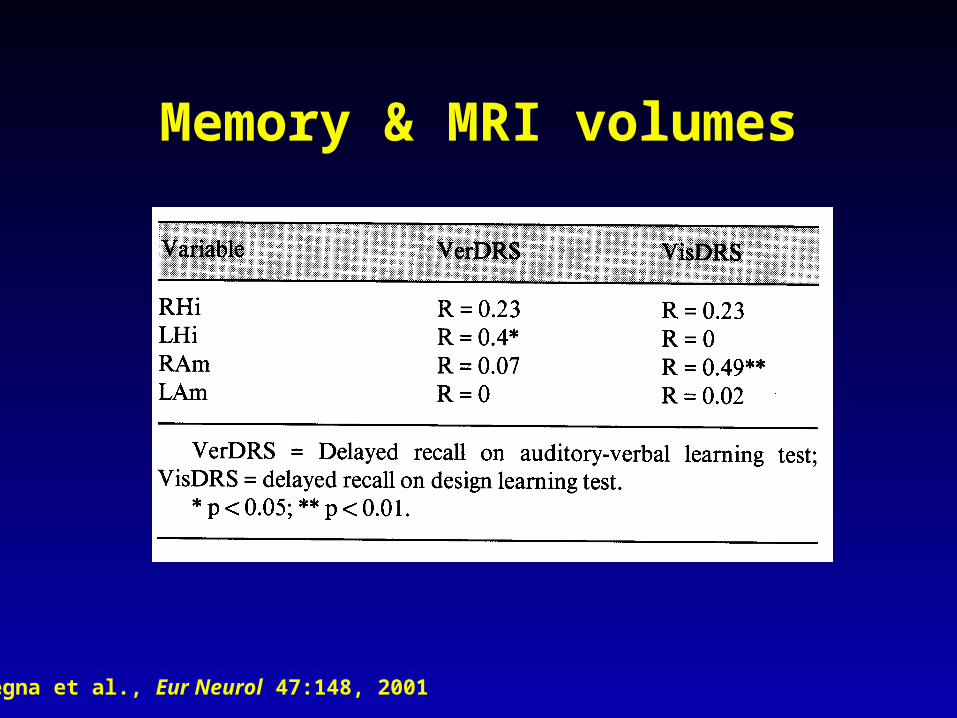
Pegna et al., Eur Neurol 47:148, 2001
Memory & MRI volumes
Surgical Treatment of Epilepsy
• Types of procedures:– ATL; selective amygdalohippocampectomy
» 70% to 90% seizure free
– Focal cortical resections
– Corpus Callosotomy
– Hemispherectomy
• Evaluation:– Scalp vido-EEG monitoring to localize seizure onset
– Invasive monitoring» depth wire electrodes
» intracranial grid electrodes
Risk of TL Surgery to memory
• Case of H.M. (cited 1744 times through 2001)
• Two cases w/ right MTL EEG s and amnesia after LT lobectomy w/ lg hippocampal removal
– Penfield & Milner, 1958
• Right MTL pathology verified at autopsy– Penfield & Mathieson, 1974
• Subsequent reports by others of memory deficits after unilateral TL lobectomy with contralateral pathology
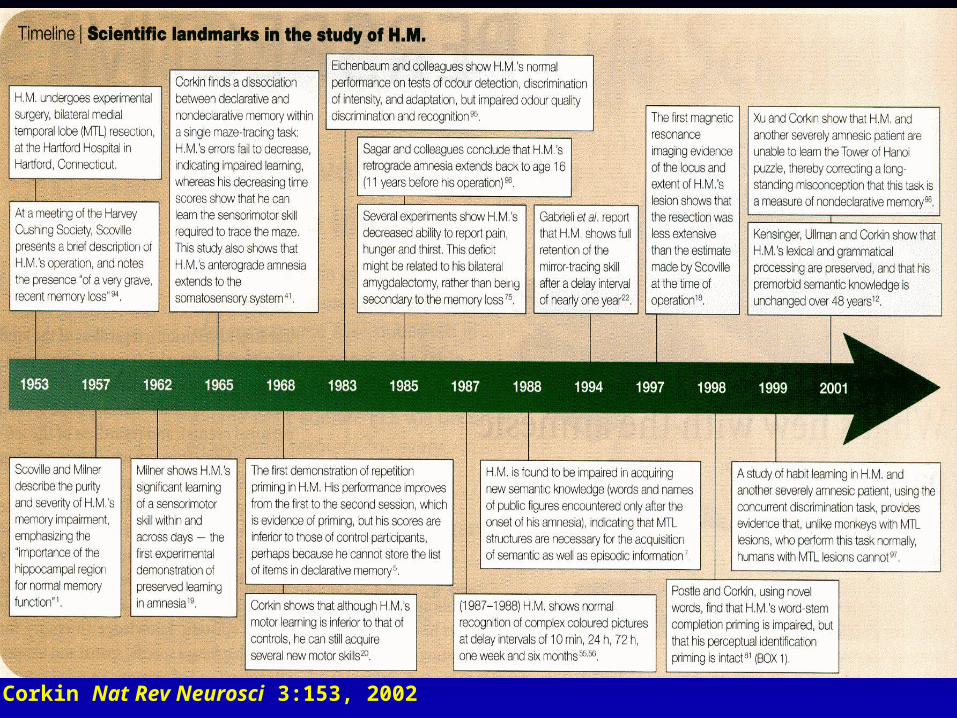
Corkin Nat Rev Neurosci 3:153, 2002
Intracarotid Na+ AmobarbitalWada Test
• Wada (1949) used intracarotid Amytal to assess lateralization of speech dominance
• Milner et al. (1962) modified Wada test to study memory competence
• Now used routinely for pre-operative assessment of patients in whom TL lobectomy or selective amygdalo-hippocampectomy is planned
IAP Protocol
• Transfemoral cerebral angiogram to evaluate vascular anatomy/degree of cross-flow
• Arms are elevated, patient counts backward from 20
• Amytal injected by hand (usually 100-125 mg) until contralateral arm drops and slowing is seen on EEG
• Memory items presented and patient asked to name them to assess language
• Memory tested after drug effect is gone, assessed by normalization of behavior & EEG
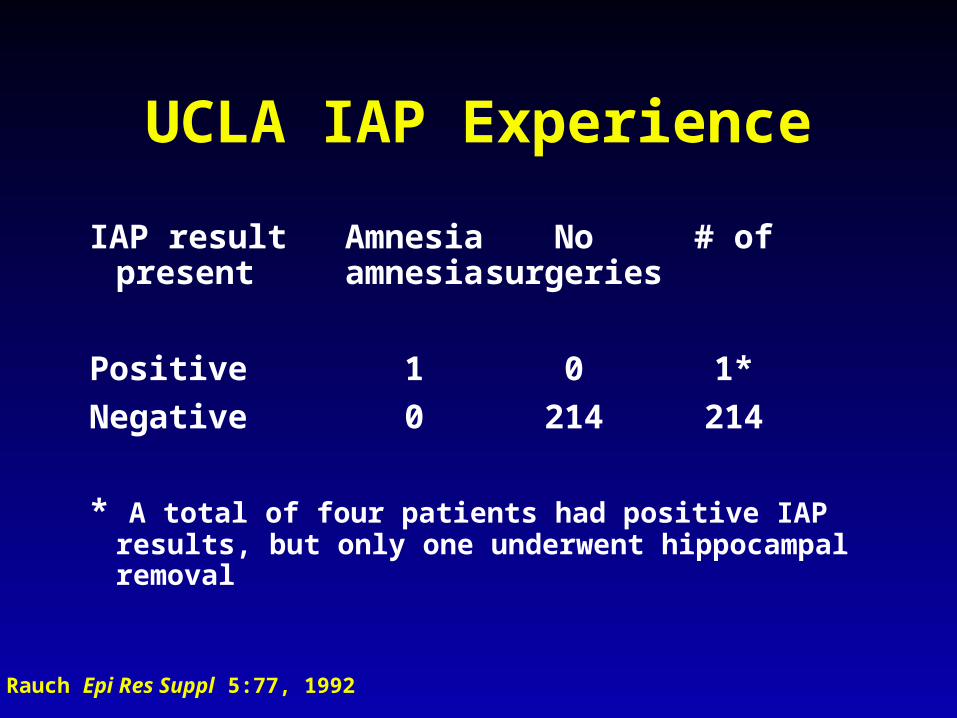
UCLA IAP Experience
IAP result Amnesia No # ofpresent amnesia surgeries
Positive 1 0 1*
Negative 0 214 214
* A total of four patients had positive IAP results, but only one underwent hippocampal removal
Rauch Epi Res Suppl 5:77, 1992
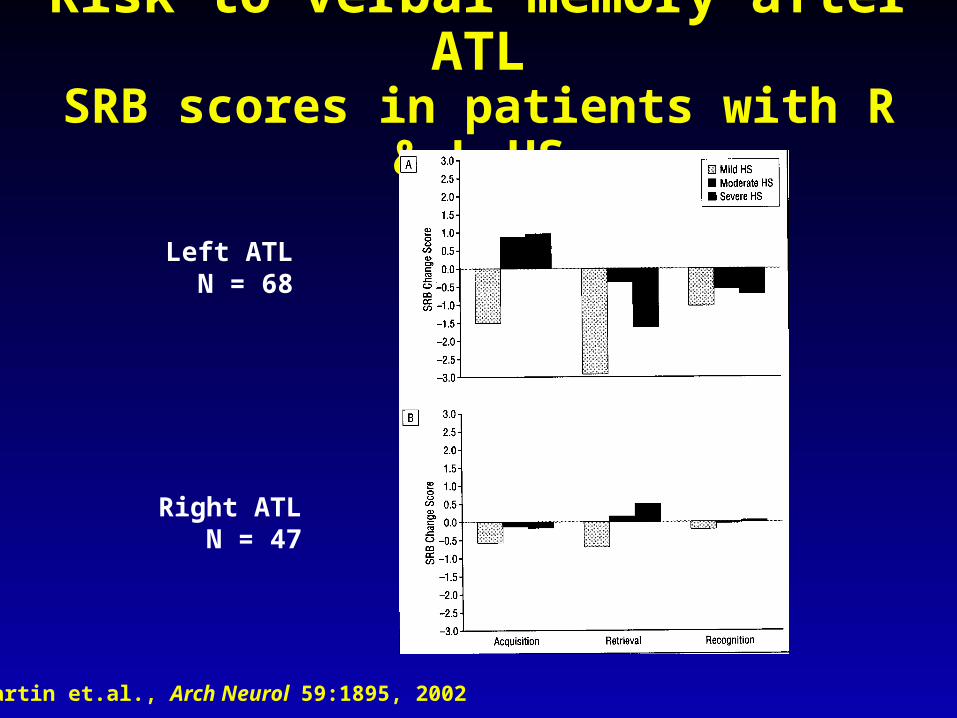
Risk to verbal memory after ATLSRB scores in patients with R & L HS
Martin et.al., Arch Neurol 59:1895, 2002
Left ATL N = 68
Right ATL N = 47
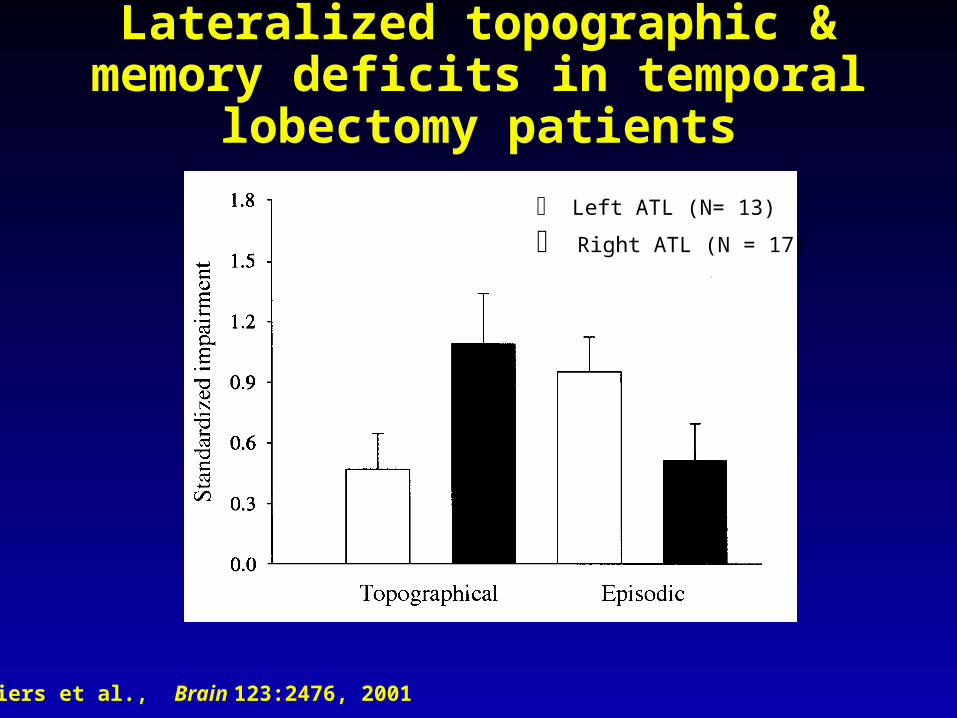
Lateralized topographic & memory deficits in temporal lobectomy patients
Spiers et al., Brain 123:2476, 2001
Left ATL (N= 13)
Right ATL (N = 17)
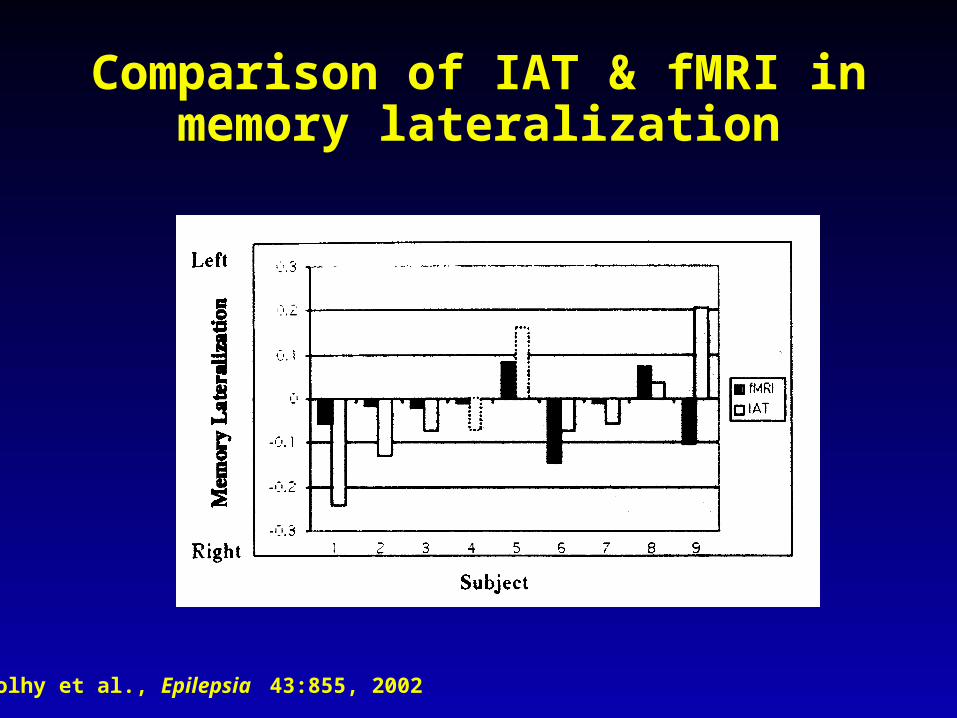
Comparison of IAT & fMRI in memory lateralization
Golhy et al., Epilepsia 43:855, 2002
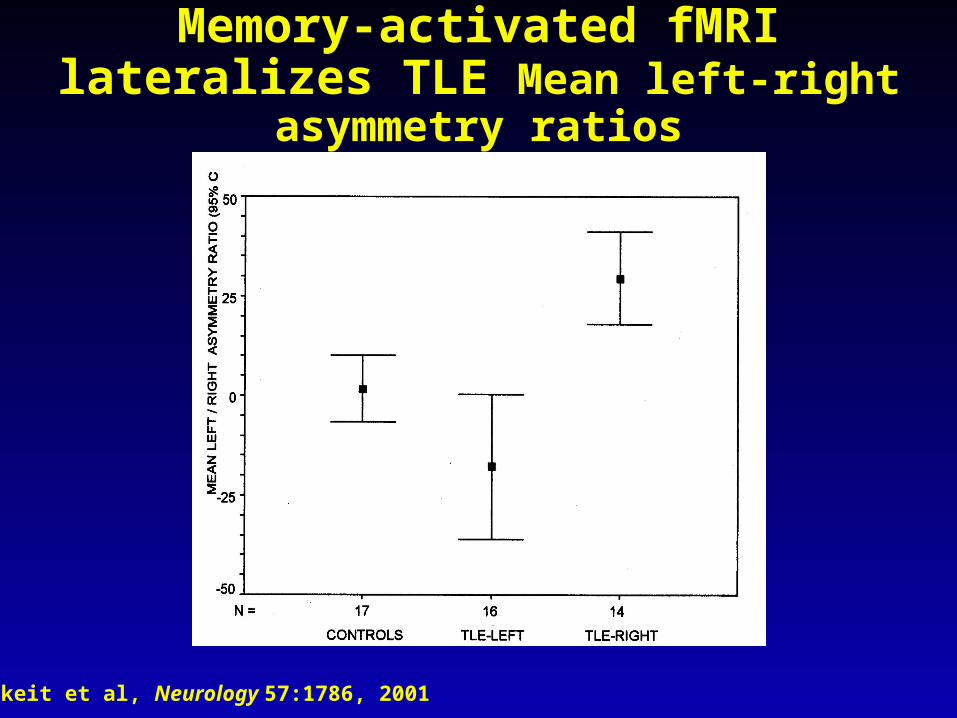
Memory-activated fMRI lateralizes TLE Mean left-right asymmetry ratios
Jokeit et al, Neurology 57:1786, 2001
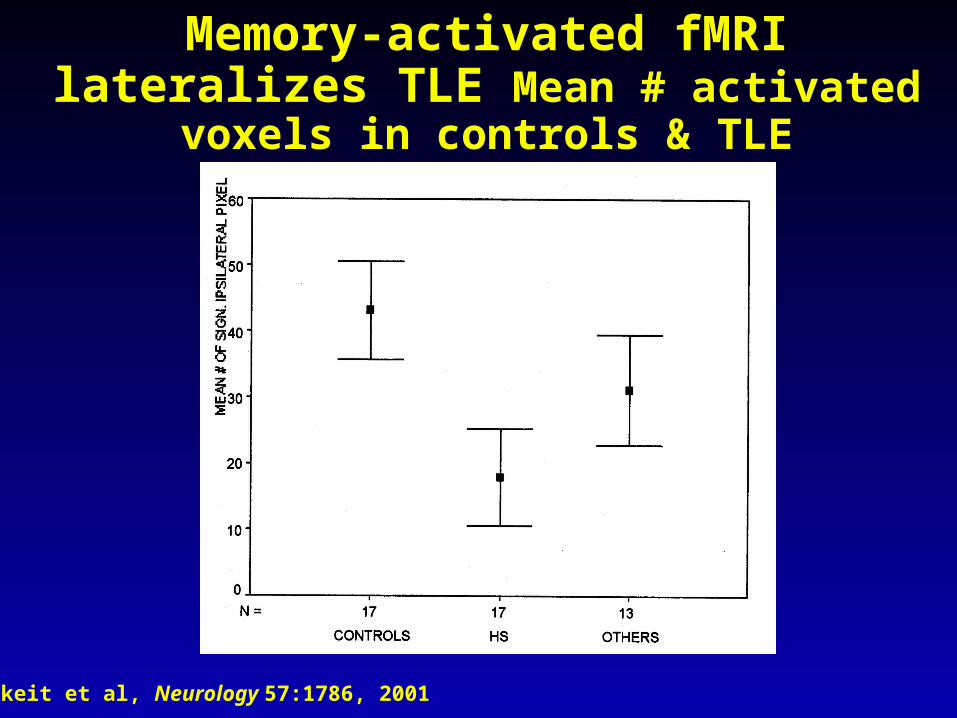
Memory-activated fMRI lateralizes TLE Mean # activated voxels in controls & TLE
Jokeit et al, Neurology 57:1786, 2001
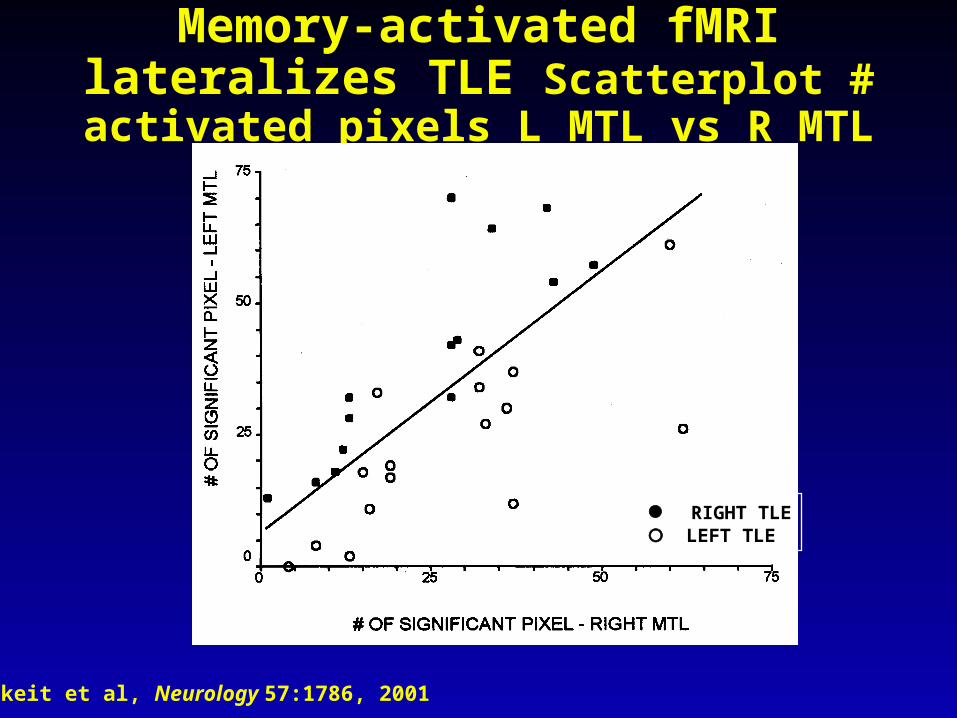
Memory-activated fMRI lateralizes TLE Scatterplot # activated pixels L MTL vs R MTL
Jokeit et al, Neurology 57:1786, 2001
RIGHT TLE LEFT TLE
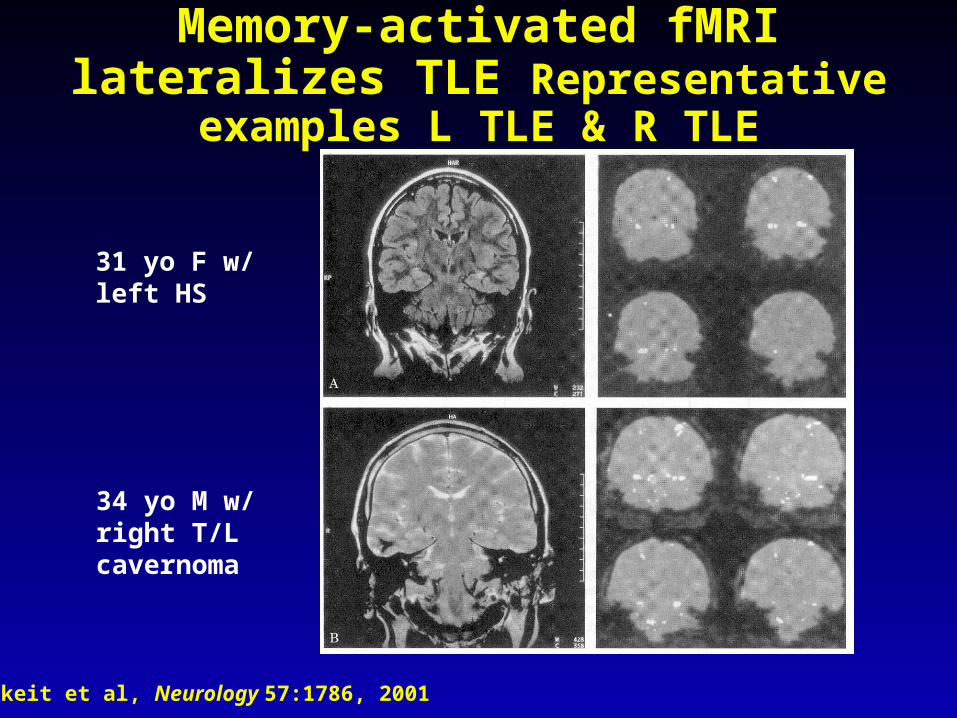
Memory-activated fMRI lateralizes TLE Representative examples L TLE & R TLE
Jokeit et al, Neurology 57:1786, 2001
31 yo F w/left HS
34 yo M w/right T/Lcavernoma
Follow-up on HM• Now 76 years old
• Continues to be unable to acquire new memories
• Intelligence normal and no deficits in perception, abstract thinking, reasoning
• Language ok: can repeat & transform sentences with complex syntax, get the point of jokes, even those turning on semantic ambiguity
• Social behavior appropriate & courteous
• Original 1957 paper cited 1744 times thru 2002
• Physically still in good health, except mobility markedly reduced from osteoporosis as a complication of chronic long-term PHT
• Brain will be examined when H.M. dies
SUMMARY
• Memory problems associated with epilepsy have been recognized for > 150 years
• Unitary vs multiple memory systems considered; case of HM renewed interest in multiple memory systems
• Current thinking:
– Explicit memory systems (both episodic and semantic memory) require intact temporal lobe, and thus are at risk in temporal lobe epilepsy.
– Implicit memory systems (perceptual representation system, procedural memory, working memory) are localized outside of the mesial temporal lobe, and thus not at risk in temporal lobe epilepsy.
SUMMARY
• Many reports of memory deficits in TLE
• Suggestion of progressive deficits, but evidence is limited
• Abundant animal data, especially from SE studies
• Memory deficits may be at least partially task-specific
• Unilateral temporal lobectomy 70% - 90% success, but need to avoid disasters of memory impairment
• Wada test useful in lateralizing language, memory
• fMRI shows promise to replace Wada test (IAT)
• Suggestion of progressive deficits emphasize importance of early consideration for TL, if TLE is refractory to AEDs