epilepsy syndromes maja ilic, md epileptologist northeast regional epilepsy group
TRANSCRIPT

Epilepsy SyndromesEpilepsy Syndromes
Maja Ilic, MDMaja Ilic, MD
EpileptologistEpileptologistNortheast Regional Epilepsy GroupNortheast Regional Epilepsy Group

What is seizure and what is What is seizure and what is epilepsy?epilepsy?
• SEIZURESEIZURE
- Physiological: Manifestation of an abnormal - Physiological: Manifestation of an abnormal and excessive synchronized discharge of a set and excessive synchronized discharge of a set of neuronsof neurons
- Clinical: Stereotypical, usually unprovoked, - Clinical: Stereotypical, usually unprovoked, disturbance of consciousness, behavior, disturbance of consciousness, behavior, emotion, motor function or sensation as a emotion, motor function or sensation as a result of the cortical neuronal dischargeresult of the cortical neuronal discharge
• EPILEPSY:EPILEPSY: 2 or more seizures 2 or more seizures

Provoked seizuresProvoked seizures
• High fever, febrile seizuresHigh fever, febrile seizures• Massive sleep deprivationMassive sleep deprivation• Excessive use of stimulantsExcessive use of stimulants• Withdrawal from sedative drugs or alcoholWithdrawal from sedative drugs or alcohol• Electrolyte disturbanceElectrolyte disturbance• HypoxiaHypoxia• Acute neurological illnessAcute neurological illness

EpidemiologyEpidemiology > 2 million people in US> 2 million people in US
125,000 new cases per 125,000 new cases per yearyear
Cumulative incidence of Cumulative incidence of epilepsy by age 80 = 3.1%epilepsy by age 80 = 3.1%
Cumulative incidence of Cumulative incidence of seizures by age 80 = 11%seizures by age 80 = 11%
Many patients outgrow Many patients outgrow their epilepsytheir epilepsy
0
10
20
30
40
50
60
70
80
90
0-9 10--19
20-39
40-59
60+
Age group (years)
Epi
leps
y ca
ses
per y
ear p
er
100,
000

Historical background:Historical background:
In an attempt to encompass a broader In an attempt to encompass a broader range of clinical features than is possible range of clinical features than is possible in a classification of seizure type – in a classification of seizure type –
ILAE published a Classifications of ILAE published a Classifications of Epilepsies and Epileptic Syndromes in Epilepsies and Epileptic Syndromes in 1985 and revised it in 19891985 and revised it in 1989

Epilepsy syndromesEpilepsy syndromes
SyndromeSyndrome is a cluster of signs and symptoms that is a cluster of signs and symptoms that occur together but unlike a disease do not have a occur together but unlike a disease do not have a single known cause or pathology.single known cause or pathology.
Epileptic syndromeEpileptic syndrome integrates all data, seizure integrates all data, seizure type, EEG findings, age of onset, cause, family type, EEG findings, age of onset, cause, family history, imaging studies, precipitating factors, etc. history, imaging studies, precipitating factors, etc. in order to make a final diagnosis of epilepsy.in order to make a final diagnosis of epilepsy.

Most Common Epilepsy Syndromes in Most Common Epilepsy Syndromes in ChildrenChildren
Childhood Absence EpilepsyChildhood Absence Epilepsy
Juvenile Absence EpilepsyJuvenile Absence Epilepsy
Juvenile Myoclonic EpilepsyJuvenile Myoclonic Epilepsy
Benign Epilepsy of Childhood with Centrotemporal Benign Epilepsy of Childhood with Centrotemporal SpikesSpikes
(Benign Rolandic Epilepsy)(Benign Rolandic Epilepsy)

Childhood Absence Childhood Absence EpilepsyEpilepsy

Absence EpilepsyAbsence Epilepsy
Generalized seizuresGeneralized seizures
Most common in the first decade, Most common in the first decade, particularly ages 5-7 years of ageparticularly ages 5-7 years of age

Clinical featuresClinical features• Usual duration – 10 secondsUsual duration – 10 seconds• Ongoing activities ceaseOngoing activities cease• Motionless with a fixed blank stareMotionless with a fixed blank stare• Attack ends suddenly, activity resumesAttack ends suddenly, activity resumes
Clinical features Clinical features Occasionally – mild clonic activity of eyelids, corner of mouthOccasionally – mild clonic activity of eyelids, corner of mouth
• Automatisms – elevation of eyelids, licking, swallowing, scratching Automatisms – elevation of eyelids, licking, swallowing, scratching movements of handsmovements of hands

Absence EpilepsyAbsence Epilepsy
Most patients with typical absence have normal Most patients with typical absence have normal development and normal neurological exam development and normal neurological exam
Generalized spikes on EEG Generalized spikes on EEG
- Precipitated by hyperventilation in all untreated Precipitated by hyperventilation in all untreated patientspatients
- Photic stimulation – 15%- Photic stimulation – 15%

Absence EpilepsyAbsence Epilepsy
10% family history 10% family history
Average age when seizures stop is 10 years oldAverage age when seizures stop is 10 years old
Generally have a good prognosis – Generally have a good prognosis –
resolves in ~ 80 percent of casesresolves in ~ 80 percent of cases
Treatment:Treatment:
• EthosuximideEthosuximide• DepakoteDepakote
Suppress absence in 80%Suppress absence in 80%
• LamotrigineLamotrigine

Absence EpilepsyAbsence Epilepsy
Atypical
Complex automatisms
Slower, 2.5 Hz spike-slow wave
Focal and GTC seizures
Developmental delay
Abnormal background EEG
Typical
Simple automatisms
3 Hz spike-slow wave
No other seizure type
Normal exam
Normal background EEG
Juvenile Absence EpilepsyJuvenile Absence Epilepsy

Juvenile Absence EpilepsyJuvenile Absence Epilepsy
Age of onsetAge of onset
Near or after pubertyNear or after puberty
Between 10-17 yearsBetween 10-17 years
Normal intelligence & neurological examNormal intelligence & neurological exam
Juvenile Absence EpilepsyJuvenile Absence Epilepsy
Seizures typesSeizures types AbsencesAbsences
Generalized tonic-clonic seizures- in 80%Generalized tonic-clonic seizures- in 80% (often shortly after waking)(often shortly after waking)
Myoclonic seizures- in 15%Myoclonic seizures- in 15%
GTC and myoclonic seizure more common and most likely to GTC and myoclonic seizure more common and most likely to happen with awakeninghappen with awakening

Juvenile Absence EpilepsyJuvenile Absence Epilepsy
EEGEEG Normal backgroundNormal background Generalized spike & wave discharges (faster, 4 Hz)Generalized spike & wave discharges (faster, 4 Hz) Induced by HV, not photic stimulationInduced by HV, not photic stimulation
TreatmentTreatment DepakoteDepakote LamictalLamictal

Juvenile Absence EpilepsyJuvenile Absence Epilepsy
PrognosisPrognosis At least 80% of patients can be treated with At least 80% of patients can be treated with
Depakote aloneDepakote alone
Absences and GTC usually respond well to Absences and GTC usually respond well to pharmacotherapypharmacotherapy
Unlike CAE (in which most patients become Unlike CAE (in which most patients become seizure free) the long term evolution of JAE has seizure free) the long term evolution of JAE has not been properly characterizednot been properly characterized

Juvenile Myoclonic Juvenile Myoclonic EpilepsyEpilepsy

Juvenile Myoclonic EpilepsyJuvenile Myoclonic Epilepsy
IncidenceIncidence• 10% of all epilepsies10% of all epilepsies
Age of onsetAge of onset• 12–18 years12–18 years• Age of onset differs from age of diagnosisAge of onset differs from age of diagnosis

Juvenile Myoclonic EpilepsyJuvenile Myoclonic Epilepsy
Myoclonic jerks, generalized tonic-clonic Myoclonic jerks, generalized tonic-clonic seizures, and sometimes absence seizures seizures, and sometimes absence seizures
• Myoclonic seizures Myoclonic seizures Jerks of neck, shoulder, arm or leg extensorsJerks of neck, shoulder, arm or leg extensors Usually bilaterally symmetric & synchronousUsually bilaterally symmetric & synchronous More in upper extremitiesMore in upper extremities Drop objects, interfere in morning activitiesDrop objects, interfere in morning activities

Juvenile Myoclonic EpilepsyJuvenile Myoclonic Epilepsy
Usual age at onset:Usual age at onset:
- Absence seizures is 7 -13 years; - Absence seizures is 7 -13 years;
- Myoclonic jerks, 12- 18 years; - Myoclonic jerks, 12- 18 years;
- Generalized convulsions, 13 - 20 years- Generalized convulsions, 13 - 20 years

Juvenile Myoclonic EpilepsyJuvenile Myoclonic Epilepsy More likely to have seizures with sleep deprivation and More likely to have seizures with sleep deprivation and
alcohol ingestionalcohol ingestion
Risk for seizures is lifelongRisk for seizures is lifelong Seizures recur when AEDs withdrawnSeizures recur when AEDs withdrawn
Photic stimulation often provokes a dischargePhotic stimulation often provokes a discharge
Seizures are usually well-controlled (Depakote, Lamictal)Seizures are usually well-controlled (Depakote, Lamictal)

Benign Epilepsy of Childhood with Centrotemporal Spikes Benign Epilepsy of Childhood with Centrotemporal Spikes
Benign Rolandic Epilepsy Benign Rolandic Epilepsy

BECTBECT
Age of onsetAge of onset• Range 2 – 13 yearsRange 2 – 13 years• 80% between 5 – 10 years (Peak 9 years)80% between 5 – 10 years (Peak 9 years)
Typically resolves by age 16 yearsTypically resolves by age 16 years
Normal intelligence and neurological examNormal intelligence and neurological exam
Seizures usually happen after falling asleep or Seizures usually happen after falling asleep or before awakening (75%)before awakening (75%)

BECTBECT
Most characteristic symptomsMost characteristic symptoms• Sensorimotor phenomena of faceSensorimotor phenomena of face
Oropharyngeal – Hypersalivation, guttural sounds, Oropharyngeal – Hypersalivation, guttural sounds, contraction of jaw, difficulty moving the tongue etccontraction of jaw, difficulty moving the tongue etc
Speech arrestSpeech arrest Clonic jerks at corner of mouthClonic jerks at corner of mouth Clonic jerks of one armClonic jerks of one arm
No loss of consciousnessNo loss of consciousness
Can have secondarily generalized convulsionsCan have secondarily generalized convulsions

BECTBECT
EEG: Spikes in midtemporal and central head EEG: Spikes in midtemporal and central head regionregion
More spikes in drowsiness and sleep More spikes in drowsiness and sleep
30% of cases show spikes only during sleep30% of cases show spikes only during sleep

BECTBECT
BECTS spontaneously stop with or without treatment (good BECTS spontaneously stop with or without treatment (good prognosis)prognosis)
If seizures are frequent and/or disturbing to patient and If seizures are frequent and/or disturbing to patient and family, treatment with Tegretol or Trileptal (until 14-16, family, treatment with Tegretol or Trileptal (until 14-16, response)response)• AEDs given in about 50% of casesAEDs given in about 50% of cases
• Features suggesting risk of repeated seizuresFeatures suggesting risk of repeated seizures Short interval between 1Short interval between 1stst & 2 & 2ndnd attacks attacks Early onsetEarly onset

Febrile SeizuresFebrile Seizures Up to 4% of childrenUp to 4% of children
Not epilepsyNot epilepsy
Often a family history, 10% Often a family history, 10% (chromosomes 8q, 19p)(chromosomes 8q, 19p)
Seizures only occur with fever in children age 6 Seizures only occur with fever in children age 6 months – 6 yearsmonths – 6 years

Febrile SeizuresFebrile Seizures
SimpleSimple
- 1 brief seizure (generalized)- 1 brief seizure (generalized)
ComplexComplex
– – ProlongedProlonged- More than 1More than 1- FocalFocal

Febrile seizuresFebrile seizures
13% incidence of epilepsy if at least 2 factors:13% incidence of epilepsy if at least 2 factors:
- History of non-febrile seizureHistory of non-febrile seizure- Abnormal neurological exam or developmentAbnormal neurological exam or development- Prolonged febrile seizure Prolonged febrile seizure - Focal febrile seizure Focal febrile seizure

Febrile seizuresFebrile seizures
Recurrence risk:Recurrence risk:- Children with simple FS 30%Children with simple FS 30%- Children with complex FS 50%Children with complex FS 50%
Risk of epilepsy:Risk of epilepsy:
- With history of simple FS 2-4%- With history of simple FS 2-4%
- With history of complex FS 6%- With history of complex FS 6%

Febrile SeizuresFebrile Seizures
Increase risk of recurrence if 1Increase risk of recurrence if 1stst before 18 months before 18 months or lower temperatureor lower temperature
Focal need MRI, EEGFocal need MRI, EEG
Testing unnecessary with simpleTesting unnecessary with simple Treatment usually not necessaryTreatment usually not necessary

Epilepsy Prognosis:Epilepsy Prognosis:
Depends on seizure type:Depends on seizure type:
Typical Absence – 80% resolveTypical Absence – 80% resolve
JME- respond well to treatment but need JME- respond well to treatment but need meds for lifemeds for life
Neurologically abnormal often difficult to control seizuresNeurologically abnormal often difficult to control seizures
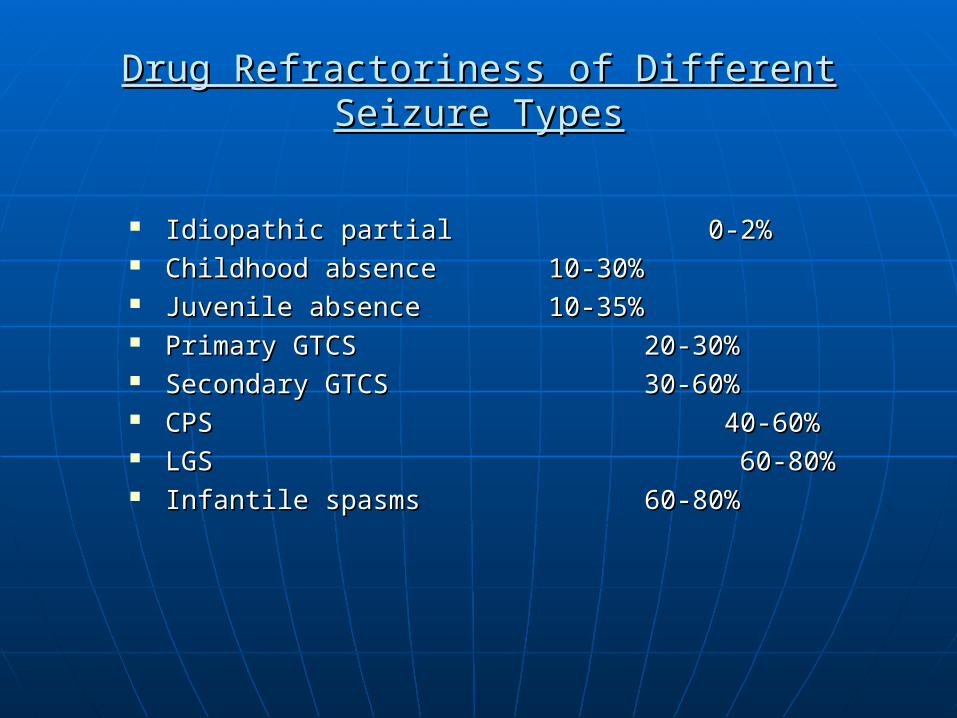
Drug Refractoriness of Different Seizure TypesDrug Refractoriness of Different Seizure Types
Idiopathic partial 0-2%Idiopathic partial 0-2% Childhood absence Childhood absence 10-30%10-30% Juvenile absence Juvenile absence 10-35%10-35% Primary GTCS Primary GTCS 20-30%20-30% Secondary GTCS Secondary GTCS 30-60%30-60% CPS 40-60%CPS 40-60% LGS LGS 60-80%60-80% Infantile spasms 60-80%Infantile spasms 60-80%

Most patients (>70%) will have excellent seizure Most patients (>70%) will have excellent seizure control with medicationscontrol with medications
Some patients will continue to have seizures Some patients will continue to have seizures despite good medical therapydespite good medical therapy
• Ketogenic dietKetogenic diet• Vagal nerve stimulatorVagal nerve stimulator• Epilepsy surgeryEpilepsy surgery

Treatment GoalsTreatment Goals
Prevent recurrence of seizuresPrevent recurrence of seizures Avoid side effects from AEDsAvoid side effects from AEDs Attain “therapeutic levels”Attain “therapeutic levels” Ensure complianceEnsure compliance

General Guidelines for Use of AEDsGeneral Guidelines for Use of AEDs
Select AED specific for seizure type and EEG Select AED specific for seizure type and EEG findingsfindings
Start with single drugStart with single drug
Optimize AEDOptimize AED• Balance seizure control vs. toxicityBalance seizure control vs. toxicity
Add second drug if first failsAdd second drug if first fails
Anticipate medication interactionsAnticipate medication interactions

When to Treat After Single Seizure?When to Treat After Single Seizure?
DefinitelyDefinitely With structural lesionWith structural lesion
• Brain tumorBrain tumor• Arteriovenous Arteriovenous
malformationmalformation• Infection, such as abscess, Infection, such as abscess,
herpes encephalitisherpes encephalitis
Without structural lesionWithout structural lesion• EEG with definite epileptic EEG with definite epileptic
patternpattern• History of previous seizure History of previous seizure • History of previous brain History of previous brain
injuryinjury• Status epilepticus at onsetStatus epilepticus at onset
PossiblyPossibly Unprovoked seizureUnprovoked seizure
Probably notProbably not (although short- (although short-term therapy may be used)term therapy may be used)
Alcohol withdrawalAlcohol withdrawal Drug abuseDrug abuse Seizure in context of acute Seizure in context of acute
illness illness Postimpact seizure Postimpact seizure Specific benign epilepsy Specific benign epilepsy
syndromesyndrome Seizure provoked by Seizure provoked by
excessive sleep deprivationexcessive sleep deprivation

MedicationsMedications
Trileptal, Tegretol, Keppra, Depakote, Trileptal, Tegretol, Keppra, Depakote,
Lamictal, Phenobarbital,Topamax, Lamictal, Phenobarbital,Topamax, Ethosuximide…Ethosuximide…
Choice based on type of seizures, EEG Choice based on type of seizures, EEG findings, side effects, age and sexfindings, side effects, age and sex
22ndnd AED may be added if seizures not AED may be added if seizures not controlledcontrolled

Newer antiepiletic medications:Newer antiepiletic medications:
Lacosamide (Vimpat)Lacosamide (Vimpat)
Vigabatrin (Sabril)Vigabatrin (Sabril)
Rufinamide (Banzel)Rufinamide (Banzel)
Perampanel (Fycompa)Perampanel (Fycompa)

Conclusion:Conclusion:
Seizure type and diagnosis are only one element Seizure type and diagnosis are only one element of a more comprehensive patient assessment of a more comprehensive patient assessment that should result in a precise epilepsy syndrome that should result in a precise epilepsy syndrome diagnosisdiagnosis
Only an accurate diagnosis of a specific epilepsy Only an accurate diagnosis of a specific epilepsy syndrome allows patients and physicians to syndrome allows patients and physicians to examine all treatment optionsexamine all treatment options

www.epilepsyfoundation.orgwww.epilepsyfoundation.org www.epilepsyadvocate.comwww.epilepsyadvocate.com www.paceusa.orgwww.paceusa.org www.epilepsy.comwww.epilepsy.com