equipoise does not exist for revive it andrew boyle, md heart and vascular center director, florida...
TRANSCRIPT

Equipoise Does Not Equipoise Does Not Exist for REVIVE ITExist for REVIVE IT
Andrew Boyle, MDHeart and Vascular Center Director, Florida
Chairman of CardiologyMedical Director of Heart Failure, Cardiac Transplantation, and Mechanical Circulatory
SupportCleveland Clinic Florida
Weston, FL

Put Another Way:Put Another Way:
Is this the right time, with the right device, with the right
adverse event profile to move forward with REVIVE IT in a less
ill population of patients?
Relevant Financial Relationship Disclosure Statement
Equipoise with REVIVE IT
Andrew Boyle, MDI will not discuss off label use and/or investigational use of
drugs/devices
The following relevant financial relationships exist related to my role in this session:
Thoratec: Medical Advisory Board and Honoraria

Actuarial Survival vs REMATCHActuarial Survival vs REMATCH
Months
0 6 12 18 24
Per
cen
t S
urv
ival
0
10
20
30
40
50
60
70
80
90
100
CF LVAD
68%
58%55%
PF LVAD 24%
OMM REMATCH 8%
LVAD REMATCH: 23%
25%
52%
Rose E et al. NEJM 2001; 345:1435-43
Slaughter M et al. NEJM 2009; 361: 1-11.

WISL INTERMACS CategoriesWISL INTERMACS Categories

WISL INTERMACS CategoriesWISL INTERMACS Categories

Patient DemographicsPatient Demographics
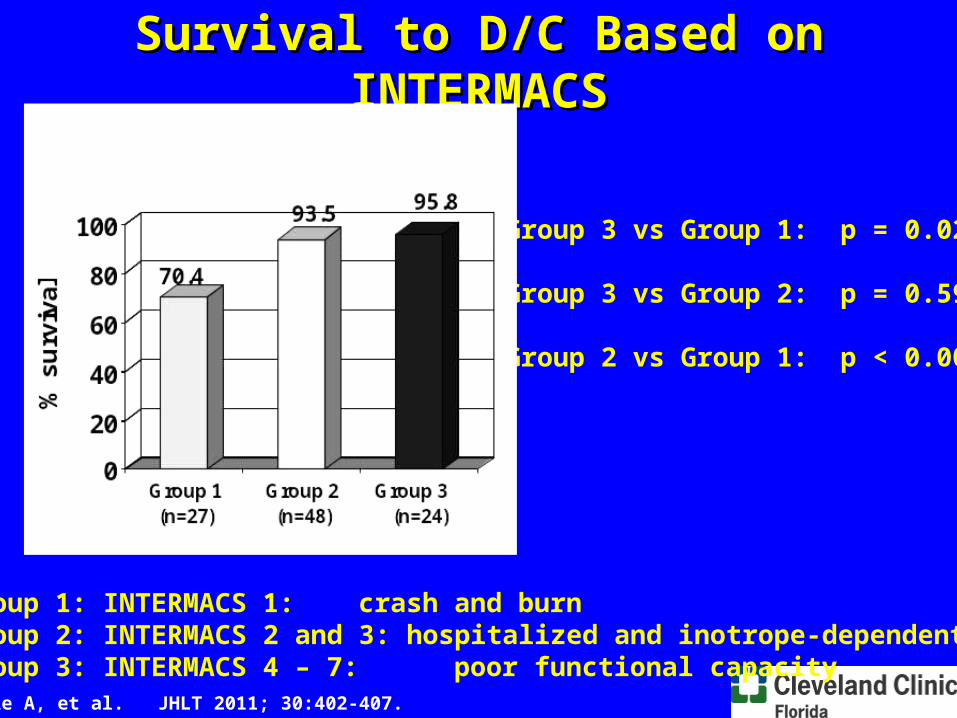
Group 1: INTERMACS 1: crash and burnGroup 2: INTERMACS 2 and 3: hospitalized and inotrope-dependentGroup 3: INTERMACS 4 – 7: poor functional capacity
Survival to D/C Based on INTERMACSSurvival to D/C Based on INTERMACS
Group 3 vs Group 1: p = 0.02 Group 3 vs Group 2: p = 0.59
Group 2 vs Group 1: p < 0.009
Boyle A, et al. JHLT 2011; 30:402-407.

Lengths of Stay Based on INTERMACSLengths of Stay Based on INTERMACS
Group 1: INTERMACS 1: crash and burnGroup 2: INTERMACS 2 and 3: hospitalized and inotrope-dependentGroup 3: INTERMACS 4 – 7: poor functional capacity
Group 3 vs Group 1: p < 0.001
Group 3 vs Group 2: p < 0.001
Group 2 vs Group 1: p = 0.62
Boyle A, et al. JHLT 2011; 30:402-407.

0
20
40
60
80
100S
urv
iva
l (%
)
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Months post-LVAD
Group 1 Group 2 Group 3
Overall SurvivalActuarial Survival on MCSActuarial Survival on MCS
Group 3 vs 1: p = 0.011Group 3 vs 2: p = 0.065Group 2 vs 1: p = 0.18
Boyle A, et al. JHLT 2011; 30:402-407.

60
70
80
90
100
0 60 120 180 240 300 360
Days Post Implant
% S
urv
ival
Event: Death (censored at transplant or recovery)
ITT Population
Heartware BTT Secondary Outcome: SurvivalHeartware BTT Secondary Outcome: Survival
Days Post Implant
Treatment Control
30 98.6% 96.6%
90 95.6% 93.6%
180 93.9% 90.2%
360 90.6% 85.7%
p = .39
HVAD
Control
Presented at AHA 2010 by K. Aaronson et al.


Have We Truly Shifted to a Have We Truly Shifted to a Less Sick Population?Less Sick Population?

The “LVAD Triad” for Successful The “LVAD Triad” for Successful Widespread AdoptionWidespread Adoption
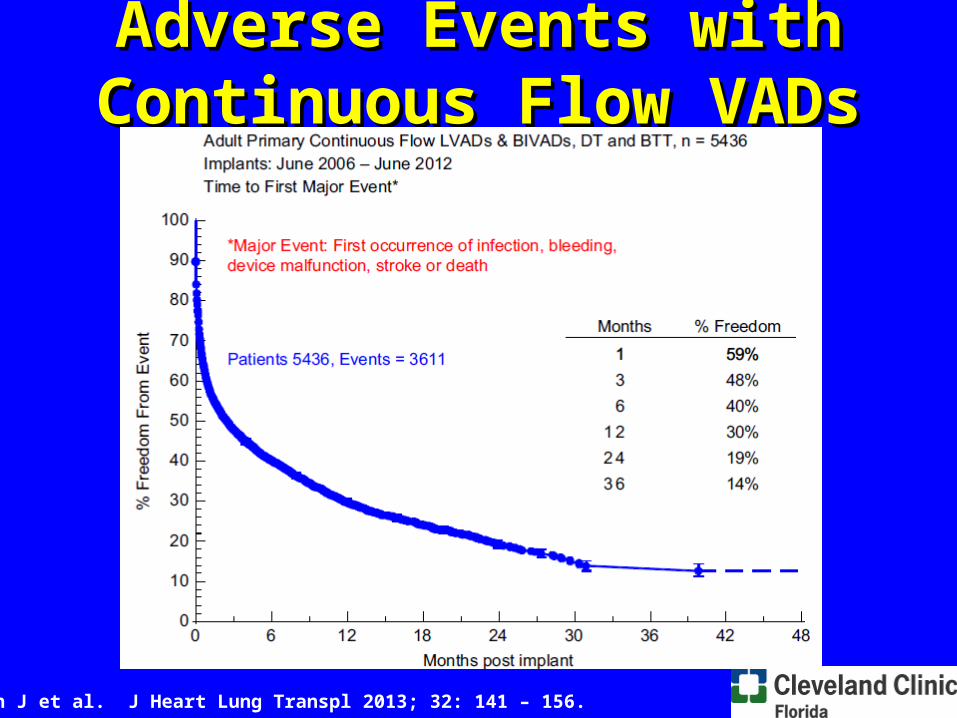
Adverse Events with Adverse Events with Continuous Flow VADsContinuous Flow VADs
Kirklin J et al. J Heart Lung Transpl 2013; 32: 141 – 156.

Heartware Adverse Event ProfileHeartware Adverse Event Profile
Presented by Maltais S et al at ISHLT 2014.

Starling RC et al. N Engl J Med 2014;370:33-40.
Overall Occurrence of Confirmed Pump Thrombosis Overall Occurrence of Confirmed Pump Thrombosis at 3 Months after HM II Implantationat 3 Months after HM II Implantation

Occurrence and Incidence of Confirmed Pump Thrombosis Occurrence and Incidence of Confirmed Pump Thrombosis Stratified According to Implantation Date.Stratified According to Implantation Date.
Starling RC et al. N Engl J Med 2014;370:33-40.

LVAD Pump ThrombosisLVAD Pump Thrombosis

ROADMAP: Thoratec Initiated Post-marketing StudyROADMAP: Thoratec Initiated Post-marketing StudyREVIVE-IT: Thoratec Supported NHLBI Trial REVIVE-IT: Thoratec Supported NHLBI Trial
Title Acronym Objective Status
Risk Assessment and Comparative Effectiveness Of Left Ventricular Assist Device and Medical Management in Ambulatory Heart Failure Patients
ROADMAP Compare the effectiveness of HM II versus optimal medical management (OMM) in ambulatory non-inotrope dependent NYHA Class IIIB / IV patients
Enrolled 200/200 pts (@ 37 sites)
Randomized Evaluation of LVAD Intervention Before Inotropic Therapy
REVIVE-IT Compare the effectiveness of HeartMate II versus OMM in NYHA Class III patients with illness not severe enough to qualify for transplant or permanent LVAD therapy based on current guidelines
Enrolled 0/100 pts (randomized study)0/2500 pts (screening registry)
0/14 sites

1 1 2 2 3 3
ROADMAP and REVIVE-ITROADMAP and REVIVE-ITComplementary Studies Exploring HeartMate II in Earlier-Stage HFComplementary Studies Exploring HeartMate II in Earlier-Stage HF
4 4 5 5 6 6 7 7INTERMACS
Profiles
CMS Coverage: Class IVCMS Coverage: Class IV
FDA Approval: Class IIIB / IVFDA Approval: Class IIIB / IV
NYHA Class III
Class IIIB
Class IV (Ambulatory
)
Class IV(On
Inotropes)
Currently Not Approved Limited Adoption Growing Acceptance
And How Representative are And How Representative are These Patients Anyways?These Patients Anyways?
• Anticipating 2500 screening failures in the registry to find 100 eligible patients for the study
• How meaningful is that to my clinical practice?

Who Are the Patients Who Would Who Are the Patients Who Would Consent to Such a Study?Consent to Such a Study?
• Have to agree to be randomized to a VAD
• Therefore will be a selected population of patients who are already interested in a VAD
• Being randomized to OMM arm is not a benign event for these patients: remember patients assigned to the XVE arm of the HM II DT trial?

ConclusionsConclusions• We should be moving to a less sick population
which is the ambulatory Class IV patient• Data will be needed to convince MD’s to refer for
MCS in IM 4 and 5 patients let alone IM 6 and 7• The devices currently commercially available do
not have a favorable adverse event profile that would justify moving to a Class III population
• We will not get a DO OVER. If this is done poorly MCS will forever be banished to the inotrope dependent patient. We better do it right the first time.