ercp: the unresolved question of endotracheal intubation
TRANSCRIPT

REVIEW
ERCP: The Unresolved Question of Endotracheal Intubation
Basavana Goudra • Preet Mohinder Singh
Received: 14 September 2013 / Accepted: 18 October 2013 / Published online: 13 November 2013
� Springer Science+Business Media New York 2013
Abstract The anesthesia community is still divided as to the
appropriate airway management in patients undergoing endo-
scopic retrograde cholangiopancreatography. Increasingly,
gastroenterologists are comfortable with deep sedation (nor-
mally propofol) without endotracheal intubation. There are no
comprehensive reviews addressing the various pros and cons of
an un-intubated airway management. It is hoped that the present
review will benefit both anesthesia providers and gastroente-
rologists. The reasons to avoid routine endotracheal intubation
and the approaches for an un-intubated anesthetic management
are discussed. The special situations where endotracheal intu-
bation is the preferred approach are mentioned. Many special
techniques to manage airway are illustrated.
Keywords ERCP � Sedation � Airway � Endoscopic
retrograde cholangiopancreatography
Background
A 59-year-old American Society of Anesthesiologists (ASA)
physical status 2 male presented for an endoscopic retrograde
cholangiopancreatography (ERCP). Past medical history was
unremarkable apart from chronic atrial fibrillation. The ven-
tricular rate was well controlled with medications. After
providing an explanation of the MAC anesthesia and associated
risks, an informed consent was obtained. The gastroenterologist
explained in detail about the ERCP and the stone extraction. As
per the standard practice, a decision was made to proceed with
deep sedation without endotracheal intubation. During the
procedure, desaturation set in that could not be treated quickly.
This was followed by sudden onset of ventricular tachycardia.
The patient was turned supine, intubated and CPR instituted.
Although effective cardiac activity and circulation could be
reestablished, the patient died a few hours later.
Horrific experiences like this are bound to affect clinical
practice of all anesthesia providers. Irrational and many times
non-evidence based decisions can be made based on either
personal experience like this one or experiences of others.
However, as experienced and trained medical professionals, it
is important that crucial practice decisions like endotracheal
intubation are made based on the available evidence rather
than a rare clinical event, however disastrous it might be. To
highlight this statement consider another example.
A 66-year-old male presented for a diagnostic upper
gastrointestinal (GI) endoscopic procedure. History inclu-
ded severe aortic stenosis (valve orifice of 0.8 cm2). Again
as per the standard practice, sedation was administered
with propofol without endotracheal intubation. Hypoxemia
(as evidenced by desaturation) led to cardiac arrest. CPR
(cardio pulmonary resuscitation) was quickly instituted;
however, the patient sustained anoxic brain injury.
Although both of these unfortunate events were heralded
by hypoxemia and possibly could have been prevented by
elective endotracheal intubation (ETT), it is unlikely that
anesthesia providers will be inclined to intubate all patients
presenting for upper GI endoscopy, as much as they are
likely to intubate all patents presenting for ERCP. In spite
of adverse outcome in both situations, the prone position-
ing necessary for ERCP segregates this entity into a
B. Goudra (&)
Clinical Anesthesiology and Critical Care, Perelman School of
Medicine, Hospital of the University of Pennsylvania,
Philadelphia, PA, USA
e-mail: [email protected]
P. M. Singh
Department of Anesthesia, Post Graduate Institute of Medical
Education and Research (PGIMER), Chandigarh, India
e-mail: [email protected]
123
Dig Dis Sci (2014) 59:513–519
DOI 10.1007/s10620-013-2931-3

separate category. It is partly due to our long-held belief
regarding the consequence of airway loss in an unintubated
patient undergoing procedure in prone position.
An important distinction has to be made regarding surgical
procedure versus endoscopic procedure conducted in prone
position. An intracranial procedure (with all its complexities in
terms of positioning) or a spine procedure is entirely different
than an ERCP, although both are conducted in prone position.
First, endoscopic procedures can be aborted at any notice to
facilitate airway management. The second difference, although
depth of sedation for an ERCP is similar to or even greater than
needed for a neurosurgical procedure, it is possible to titrate the
anesthetic depth to maintain spontaneous ventilation. The
intensity of stimulation for an ERCP is nowhere near a surgical
incision and, apart from the phase of gastroscope insertion, is
relatively constant. Further discussion on anesthetic approach
and airway management of patients presenting for an ERCP
will be based on these two factors.
The Intubation Dilemma
Endoscopic retrograde cholangopancreatography poses
unique challenges to both anesthesia provider and gastroen-
terologist. The last two decades have seen a phenomenal
increase in the number of ERCPS. With the expanding indi-
cations, the patient population presenting for these procedures
has also grown older and sicker. Some of the indications in our
own hospital (from a retrospective review of 653 patients) are
presented in Table 1 [1]. Although it is tempting to intubate all
ERCPS and such is the practice in many centers around the
world, the following considerations are to be borne in mind
before committing all or a majority of patients to ETT.
Why Routine ETT Anesthesia Should Be Discouraged?
How Safe is Laryngoscopy and Intubation?
Laryngoscopy and endotracheal intubation itself is not an
entirely innocuous procedure. Although the advent of video
laryngoscope is likely to change the landscape, intubation-
related injuries are common. Lip, dental and eye and other
soft tissue injuries happen with a degree of frequency [2–
4]. Although these injuries are not life threatening, they are
preventable and especially injuries to the eye can be dis-
abling. More serious injuries like bronchial rupture can
occur especially with the use of introducers [5].
Endotracheal intubation almost invariably requires
administration of skeletal muscle relaxants. Due to the
unexpected duration of this diagnostic and therapeutic
procedure, it is sensible to use succinylcholine for this
purpose. Apart from the well-known risks of muscle pain,
myoglobulinemia myoglobinuria, succinylcholine is
implicated in malignant hyperthermia [6, 7]. Depending
on the endoscopic findings, sometimes it becomes nec-
essary to administer a long acting relaxant along with the
need for reversal agents. Apart from a significant increase
in anesthesia times, use of muscle relaxants can increase
the incidence of postoperative pulmonary complications
[8, 9]. Use of reversal agents is associated with unwanted
anticholinergic effects. Use of glycopyrrolate is not uni-
versal. Use of atropine for this purpose can potentially
lead to central anticholinergic effects. Residual neuro-
muscular blockade is an important issue with nondepo-
larizing muscle relaxants [10, 11]. It can occur even 2 h
after reversal. Inadequate reversal is an additional risk
factor. It is hoped that advent of sugamedex [12] might
change the role of nondepolarizing muscle relaxants in
future.
Prone Positioning and ETT
Although all ERCP procedures involve prone positioning,
patients are asked to position themselves when ETT is not
involved. Turning prone after intubating in supine position
presents significant challenges. Endoscopy units are not as
well staffed as other surgical operating rooms. Injuries can
occur during positioning and while positioned. Accidental
extubation is risky, although can be managed either with
bag-mask or a laryngeal mask airway (LMA) [13].
Efficiency
Especially for very short procedures like change of stent,
the endotracheal anesthesia adds significant additional
time. In a retrospective study [14], we found that ‘‘anes-
thesia time’’ (total time minus procedural time) is a sig-
nificant factor contributing to overall time in ERCP
procedure. This time can be reduced by using dedicated
anesthesiologists, and decreased incidence of endotracheal
intubation is a contributing factor.
Table 1 Indications of endoscopic retrograde cholangiopancreatog-
raphy (ERCP) in an outpatient center
Indication Occurrence
Chronic pancreatitis 6.25 %
Post hepatic transplant 41.43 %
Hepatic cancer (including metastasis) 8.56 %
Cholangiocarcinoma 8.56 %
Primary sclerosing cholangitis 4.62 %
Pancreatic cancer 20.83 %
Others 9.72 %
514 Dig Dis Sci (2014) 59:513–519
123

Why Anesthesiologists Intubate the Trachea?
Fear of Losing Airway
Fear of losing airway during the procedure is probably the
most common reason for elective endotracheal intubation
among the anesthesia providers. However, those fears are
unfounded. Many publications during recent months have
affirmed the safety of unintubated ERCP. Goudra et al.
studied 653 consecutive patients undergoing elective
ERCP in their outpatient center. Their intubation rate was
\1 % and all the indications were fear of full stomach and
history of aspiration. There were no instances of procedure
interruption or emergency endotracheal intubation. Even
while anesthetizing far sicker patients in their inpatient
endoscopy center, the incidence of endotracheal intubation
was \10 %. In a recent study, non-obese patients who
underwent ERCP needed endotracheal intubation in about
10 % procedures [15].
Risk of Hypoxemia
Many investigators have closely studied the risk of hyp-
oxemia in patients undergoing advanced endoscopic pro-
cedures and ERCP [1, 14, 16]. In the study cited above
[15], although incidence of endotracheal intubation for
ERCP was \10 %, the incidence of oxygen desaturation
was worryingly high. It is well known that hypoxemia (as
evidenced by desaturation) is the most common precursor
of more serious adverse events like cardiac arrhythmias
and asystole. Part of the reasons for a striking difference in
the intubation and desaturation rates might be the airway
management technique. In one institution, airway man-
agement was geared towards preventing hypoxemia. By
extensive use of either a nasal trumpet or an oral trumpet
(both in turn connected to a mapelson breathing system,
Figs. 1a, b, 2), one center could reduce the incidence of
desaturation to negligible levels.
However, if an anesthesia provider decides to embark on
an unintubated approach while sedating these patients,
certain precautions need to be undertaken [1]. Preoxygen-
ation and timing of propofol administration along with the
timing of endoscope insertion are all crucial. As it is well
known, once the lungs are filled with 100 % oxygen by
elective preoxygenation, it can take up to 11 min for pulse
oximeter to register a desaturation to 90 %, in spite of no
ventilation. Although, both preoxygenation for 3 min or
four vital capacity breaths can provide at least 4 min of
‘‘safety time’’ before patients start desaturating, it is
advised to use the former technique as the time available to
deal with inadequate ventilation will be longer (up to
8 min) [17]. This is due to the nature of the oxygen
desaturation curve. The arterial partial pressure of oxygen
Fig. 1 a A nasal trumpet placed in the nose and connected to a
Mapelson C breathing system with an elective endotracheal intuba-
tion (ETT) adapter. b A nasal trumpet placed in the nose and
connected to a Mapelson C breathing system, bag squeezed to assist
Fig. 2 A nasal trumpet placed in the mouth and connected to a
Mapelson C breathing system with an ETT adapter
Dig Dis Sci (2014) 59:513–519 515
123
has to fall from an initial 660 to about 90 mmHg for a fall
in oxygen saturation. The patient needs to be either apneic
or hypopneic for prolonged periods (depending on FRC
and oxygen consumption) before the pulse oximeter can
register desaturation. This period is difficult to detect
without close observation. Although ASA has recom-
mended the use of ECO2 monitoring for all patients
undergoing GI endoscopic procedure under anesthesia-
provider provided sedation [18], its efficacy in the setting
of GI endoscopy is far from satisfactory [19]. Close
observation of the chest movement and alternative, more
reliable means of ventilation (like acoustic respiratory
monitor or impedance peumograpghy) are to be
considered.
The second issue is to have a means of assisting venti-
lation if (and when) hypoventilation is detected. Obviously,
any airway obstruction needs to be corrected by
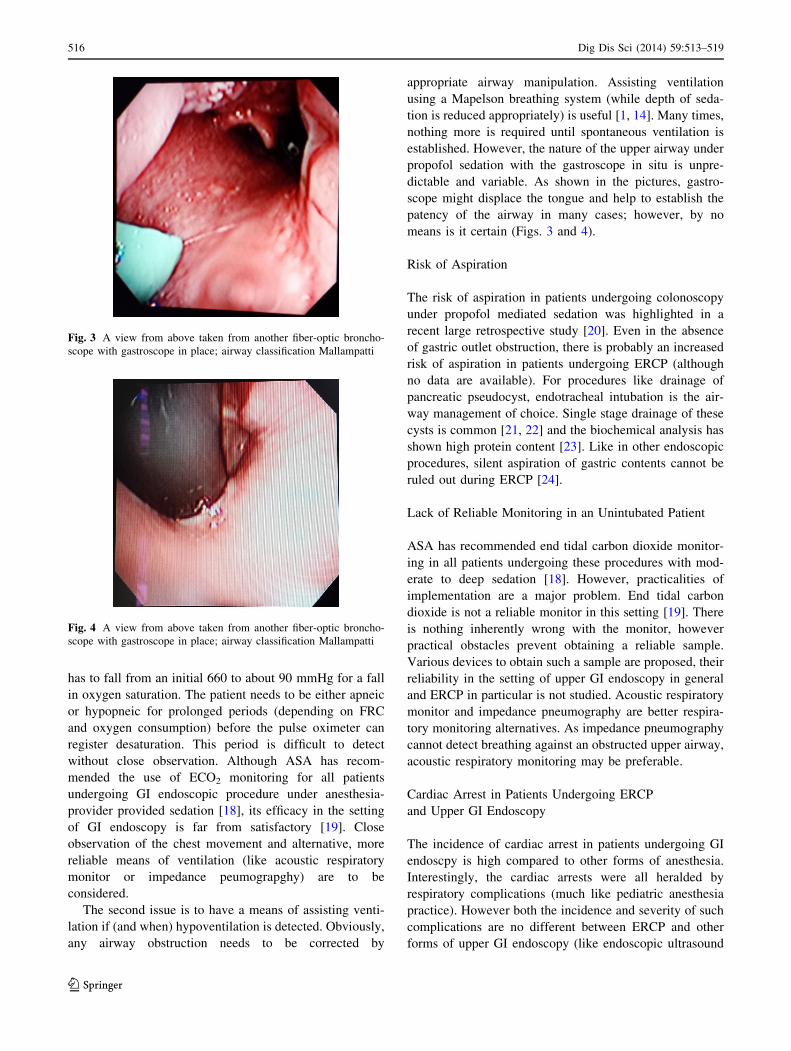
appropriate airway manipulation. Assisting ventilation
using a Mapelson breathing system (while depth of seda-
tion is reduced appropriately) is useful [1, 14]. Many times,
nothing more is required until spontaneous ventilation is
established. However, the nature of the upper airway under
propofol sedation with the gastroscope in situ is unpre-
dictable and variable. As shown in the pictures, gastro-
scope might displace the tongue and help to establish the
patency of the airway in many cases; however, by no
means is it certain (Figs. 3 and 4).
Risk of Aspiration
The risk of aspiration in patients undergoing colonoscopy
under propofol mediated sedation was highlighted in a
recent large retrospective study [20]. Even in the absence
of gastric outlet obstruction, there is probably an increased
risk of aspiration in patients undergoing ERCP (although
no data are available). For procedures like drainage of
pancreatic pseudocyst, endotracheal intubation is the air-
way management of choice. Single stage drainage of these
cysts is common [21, 22] and the biochemical analysis has
shown high protein content [23]. Like in other endoscopic
procedures, silent aspiration of gastric contents cannot be
ruled out during ERCP [24].
Lack of Reliable Monitoring in an Unintubated Patient
ASA has recommended end tidal carbon dioxide monitor-
ing in all patients undergoing these procedures with mod-
erate to deep sedation [18]. However, practicalities of
implementation are a major problem. End tidal carbon
dioxide is not a reliable monitor in this setting [19]. There
is nothing inherently wrong with the monitor, however
practical obstacles prevent obtaining a reliable sample.
Various devices to obtain such a sample are proposed, their
reliability in the setting of upper GI endoscopy in general
and ERCP in particular is not studied. Acoustic respiratory
monitor and impedance pneumography are better respira-
tory monitoring alternatives. As impedance pneumography
cannot detect breathing against an obstructed upper airway,
acoustic respiratory monitoring may be preferable.
Cardiac Arrest in Patients Undergoing ERCP
and Upper GI Endoscopy
The incidence of cardiac arrest in patients undergoing GI
endoscpy is high compared to other forms of anesthesia.
Interestingly, the cardiac arrests were all heralded by
respiratory complications (much like pediatric anesthesia
practice). However both the incidence and severity of such
complications are no different between ERCP and other
forms of upper GI endoscopy (like endoscopic ultrasound
Fig. 3 A view from above taken from another fiber-optic broncho-
scope with gastroscope in place; airway classification Mallampatti
Fig. 4 A view from above taken from another fiber-optic broncho-
scope with gastroscope in place; airway classification Mallampatti
516 Dig Dis Sci (2014) 59:513–519
123

or therapeutic endoscopy). The incidence during colonos-
copy was zero during the same period.
Airway Management for Prone ERCP
As mentioned earlier, the oxygen dissociation curve is not
an anesthesia provider’s friend. Due to the steep portion of
the curve, it is very important (while anesthetizing any
unintubated, spontaneously ventilating patient) to have a
low threshold for endoscope withdrawal. Corrective airway
maneuvers need to be instituted in anticipation of hypox-
emia rather than as a response to hypoxemia. Waiting for
pulse oximeter to display a saturation of 90–95 to respond
might be too late. To facilitate such an approach, a
patient’s ventilatory efforts need to be observed very clo-
sely. If the attending anesthesiologist (supervising the case)
is doubtful of the abilities of his assistant, intubation might
be a safer option. These skills can be easily taught and
learnt. Especially in the initial stages of the procedure
(endoscope insertion and recommencement of effective
ventilation), documentation needs to be ignored and
attention paid to monitor the patient. Inadequate levels of
sedation can equally lead to severe cough and sometimes
laryngospasm. In the absence of effective preoxygenation,
hypoxemia can set in very quickly. As ERCP scopes have a
side camera (rather than at the tip) insertion difficulties can
lead to inadvertent stimulation of vocal cords triggering
violent cough. Immediate endoscope withdrawal and
deepening sedation is important. An anesthesia provider
should not hesitate to express his concerns and request for a
more experienced endoscopist to do the insertion. If the
difficulties continue, it is prudent to reevaluate the plan and
effect an endotracheal intubation after turning supine.
At times, after commencement of the procedure, airway
manipulations, insertion of nasal trumpet or bagging with
the oral/nasal trumpet are insufficient to prevent hypox-
emia. In such cases, withdrawal of the scope and bagging
with a face mask to reoxygente is required. In the absence
of any other difficulties, after appropriate adjustment of the
depth of sedation, endoscope reinsertion can be permitted.
There is increasing evidence as to the safety of LMA
both as a primary airway in prone position and as a rescue
method [13, 25, 26].
Although, a nasal trumpet connected to a Mapelson C
breathing system (Fig. 1a, b) has been used as a standard in
our hospital, it can also be used as a rescue measure.
Another way to administer oxygen is by use of a modified
nasal airway inserted into the mouth next to bite block and
connected to a Mapelson C breathing system (Fig. 2).
Both gastrolaryngeal tube (Fig. 5) and endoscopy mask
(Fig. 6) could be used as support and possible ventilation
during ERCP procedures [27]. However there is little
published literature with either of these airways during
these procedures. Absence of a suction port is an obvious
disadvantage with an endoscopy mask.
Studies documenting the use of LMA for ERCP are
lacking, but its use in prone position to administer anes-
thesia for other surgical procedures are plenty.
Who Should Provide Anesthesia for ERCP?
Another way to increase both the safety and efficiency in
ERCP sedation is to have a team of dedicated anesthesia
providers. This approach is known to decrease desatura-
tions and reduce the anesthesia time [14]. In this recently
published study, a comparison was made between two
naturally divided groups of anesthesia providers. Apart
from an incidence of desaturation, a comparison was also
made between the ‘‘anesthesia time’’ in the two groups. As
a group, non-dedicated anesthesia providers took more
time than dedicated providers. Moreover this amounted to
an increase in the cost of anesthesia by about 760,000 US$
Fig. 5 Gastrolaryngeal tube
Fig. 6 Endoscopy mask
Dig Dis Sci (2014) 59:513–519 517
123

in one hospital alone. Although no special fellowships and
certifications are currently necessary, out-of-OR anesthesia
might soon become frequent and complicated enough to
require additional training. At the hospital of the University
of Pennsylvania, dedicated out-of-operating-room resident
anesthesia rotations are already in place to address this
aspect of training. It is hoped that ASA and ABA will
notice this expanding field of anesthesia and make appro-
priate provisions in the residency training curriculum.
Frequently, the question arises about the nomenclature
of sedation technique used for these procedures. Gast-
roenterologists are always competing with anesthesia pro-
viders to administer propofol. As observed in our
institution, although the patients presenting for upper
endoscopy (including ERCP) are told (and consented) that
they will have moderate to deep sedation, 96 % of these
patients were under deep general anesthesia as measured
by brain function monitor (SEDLne). As a result, it is only
appropriate that ‘‘sedation’’ for these procedures is pro-
vided by anesthesia providers.
Having discussed the pros and cons of endotracheal
intubation for ERCP, a low threshold to intubate is advised
in the following subset of patients.
Obesity
As stated earlier, emergency expert help in turning the
patient supine to secure an airway may not be easy in an
endoscopic suite. In a morbidly obese patient, such heroics
could be fraught with dangers. With an already compro-
mised FRC and increased oxygen consumption, time
available to reestablish effective ventilation will be very
limited. ETT is the preferred method of airway manage-
ment, especially in the inexperienced.
Risk of Aspiration
Suspicion of gastric outlet obstruction, full stomach and
drainage of pseudocyst of pancreas are probably managed
better with an ETT.
Anticipated Difficult Ventilation
Although anticipated difficult intubation may not be an
indication for elective ETT, anticipated difficult ventilation
should be.
Additionally, other institution-specific factors like
availability of anesthesia provider with experience in
endoscopy anesthesia, location and size of the room, type
and extent of help are important in this decision making.
Conclusions
Patients presenting for an ERCP can be safely and effec-
tively sedated without the need for an elective endotracheal
intubation. Close respiratory monitoring, ready availability
of means of establishing ventilation and experience are
important. Various airway techniques and adjuncts
described can help in preventing and treating hypoxemia.
Conflict of interest None.
References
1. Goudra B, Singh P, Sinha A. Outpatient endoscopic retrograde
cholangiopancreatography: safety and efficacy of anesthetic
management with a natural airway in 653 consecutive proce-
dures. Saudi J Anaesth. 2013;7:259.
2. Newland MC, Ellis SJ, Peters KR, et al. Dental injury associated
with anesthesia: a report of 161,687 anesthetics given over
14 years. J Clin Anesth. 2007;19:339–345.
3. Vogel J, Stubinger S, Kaufmann M, Krastl G, Filippi A. Dental
injuries resulting from tracheal intubation—a retrospective study.
Dent Traumatol. 2009;25:73–77.
4. Yu H-D, Chou A-H, Yang M-W, Chang C-J. An analysis of
perioperative eye injuries after nonocular surgery. Acta Anaes-
thesiol Taiwanica Off J Taiwan Soc Anesth. 2010;48:122–129.
5. Sahin M, Anglade D, Buchberger M, Jankowski A, Albaladejo P,
Ferretti GR. Case reports: Iatrogenic bronchial rupture following
the use of endotracheal tube introducers. Can J Anaesth J Can
Anesth. 2012;59:963–967.
6. Dexter F, Epstein RH, Wachtel RE, Rosenberg H. Estimate of the
relative risk of succinylcholine for triggering malignant hyper-
thermia. Anesth Analg. 2013;116:118–122.
7. Hopkins PM. Malignant hyperthermia: pharmacology of trig-
gering. Br J Anaesth. 2011;107:48–56.
8. Tejada Artigas A, Bello Dronda S, Chacon Valles E, et al. Risk
factors for nosocomial pneumonia in critically ill trauma patients.
Crit Care Med. 2001;29:304–309.
9. Berg H, Roed J, Viby-Mogensen J, et al. Residual neuromuscular
block is a risk factor for postoperative pulmonary complications.
A prospective, randomised, and blinded study of postoperative
pulmonary complications after atracurium, vecuronium and
pancuronium. Acta Anaesthesiol Scand. 1997;41:1095–1103.
10. Debaene B, Plaud B, Dilly M-P, Donati F. Residual paralysis in
the PACU after a single intubating dose of nondepolarizing
muscle relaxant with an intermediate duration of action. Anes-
thesiology. 2003;98:1042–1048.
11. Varposhti MR, Heidari SM, Safavi M, Honarmand A, Raeesi S.
Postoperative residual block in postanesthesia care unit more than
two hours after the administration of a single intubating dose of
atracurium. J Res Med Sci Off J Isfahan Univ Med Sci.
2011;16:651–657.
12. Sokoł-Kobielska E. Sugammadex—indications and clinical use.
Anaesthesiol Intensive Ther. 2013;45:106–110.
13. Raphael J, Rosenthal-Ganon T, Gozal Y. Emergency airway
management with a laryngeal mask airway in a patient placed in
the prone position. J Clin Anesth. 2004;16:560–561.
14. Goudra BG, Singh PM, Sinha AC. Anesthesia for ERCP: impact
of anesthesiologist’s experience on outcome and cost. Anesth Res
Pract. 2013;2013:570518.
518 Dig Dis Sci (2014) 59:513–519
123

15. Barnett SR, Berzin T, Sanaka S, Pleskow D, Sawhney M,
Chuttani R. Deep sedation without intubation for ERCP is
appropriate in healthier, non-obese patients. Dig Dis Sci. (Epub
ahead of print). doi:10.1007/s10620-013-2783-x.
16. Berzin TM, Sanaka S, Barnett SR, et al. A prospective assessment
of sedation-related adverse events and patient and endoscopist
satisfaction in ERCP with anesthesiologist-administered sedation.
Gastrointest Endosc. 2011;73:710–717.
17. Gambee AM, Hertzka RE, Fisher DM. Preoxygenation tech-
niques: comparison of three minutes and four breaths. Anesth
Analg. 1987;66:468–470.
18. Weaver J. The latest ASA mandate: CO2 monitoring for moderate
and deep sedation. Anesth Prog. 2011;58:111–112.
19. Goudra BG. Comparison of acoustic respiration rate, impedance
pneumography and capnometry monitors for respiration rate
accuracy and apnea detection during GI endoscopy anesthesia.
Open J Anesth. 2013;03:74–79.
20. Cooper GS, Kou TD, Rex DK. Complications following colon-
oscopy with anesthesia assistance: a population-based analysis.
JAMA Intern Med. 2013;173:551–556.
21. Ahlawat SK, Charabaty-Pishvaian A, Jackson PG, Haddad NG.
Single-step EUS-guided pancreatic pseudocyst drainage using a
large channel linear array echoendoscope and cystotome: results
in 11 patients. JOP J Pancreas. 2006;7:616–624.
22. Ahn JY, Seo DW, Eum J, et al. Single-step EUS-guided trans-
mural drainage of pancreatic pseudocysts: analysis of technical
feasibility, efficacy, and safety. Gut Liver. 2010;4:524–529.
23. Monkemuller KE, Harewood GC, Curioso WH, et al. Biochem-
ical analysis of pancreatic fluid collections predicts bacterial
infection. J Gastroenterol Hepatol. 2005;20:1667–1673.
24. Raksakietisak M. Unrecognised aspiration pneumonitis during
enteroscopy: two cases report. J Med Assoc Thail Chotmaihet
Thangphaet. 2009;92:869–871.
25. Abrishami A, Zilberman P, Chung F. Brief review: airway rescue
with insertion of laryngeal mask airway devices with patients in
the prone position. Can J Anaesth J Can Anesth. 2010;57:
1014–1020.
26. Osborn IP, Cohen J, Soper RJ, Roth LA. Laryngeal mask air-
way—a novel method of airway protection during ERCP: com-
parison with endotracheal intubation. Gastrointest Endosc.
2002;56:122–128.
27. Fabbri C, Luigiano C, Cennamo V, et al. The gastro-laryngeal
tube for interventional endoscopic biliopancreatic procedures in
anesthetized patients. Endoscopy. 2012;44:1051–1054.
Dig Dis Sci (2014) 59:513–519 519
123