esiste un ruolo per il trapianto allogenico? · # conditionig regimen # transplant mortality #...
TRANSCRIPT
ESISTE UN RUOLO PER IL TRAPIANTO ALLOGENICO?
Alida Dominietto
ALLOGENEIC HSCT IN MM PTS
# WHEN AND WHO?
# PATIENT AGE
# COMORBIDITIES
# DONOR TYPE
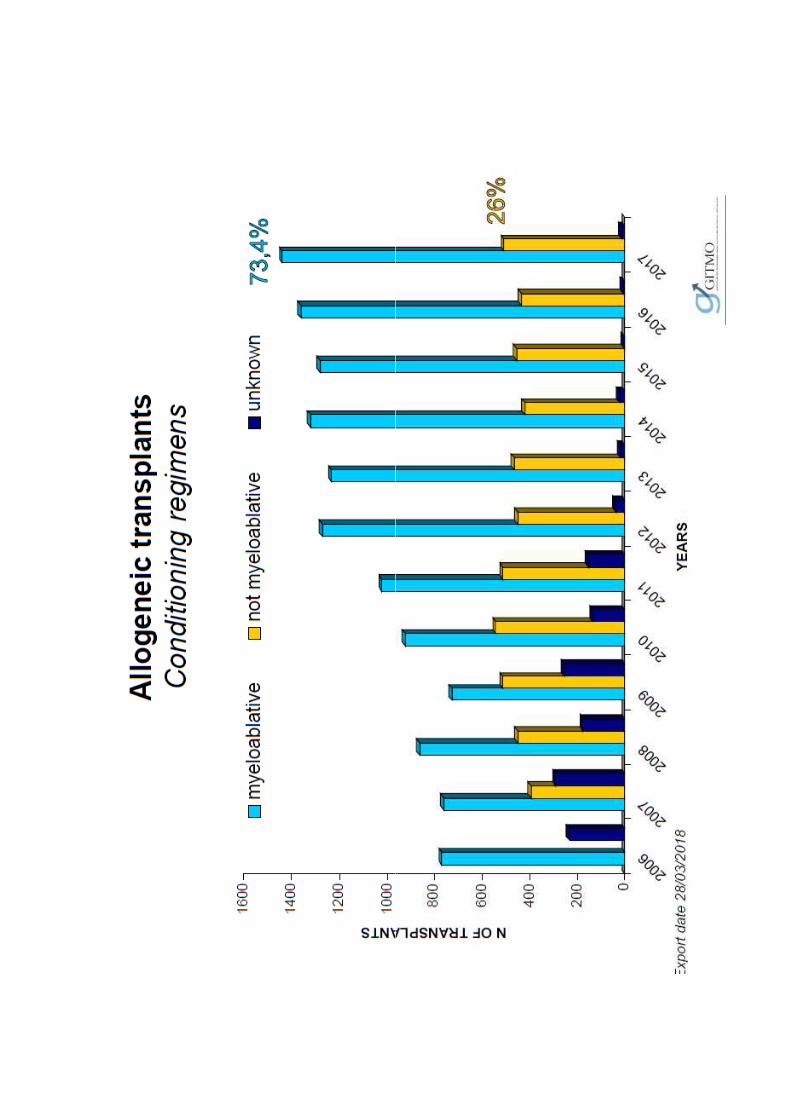
# CONDITIONIG REGIMEN
# TRANSPLANT MORTALITY
# RELAPSE

EBMT database >70000 pts
Sureda A et al. BMT 2018
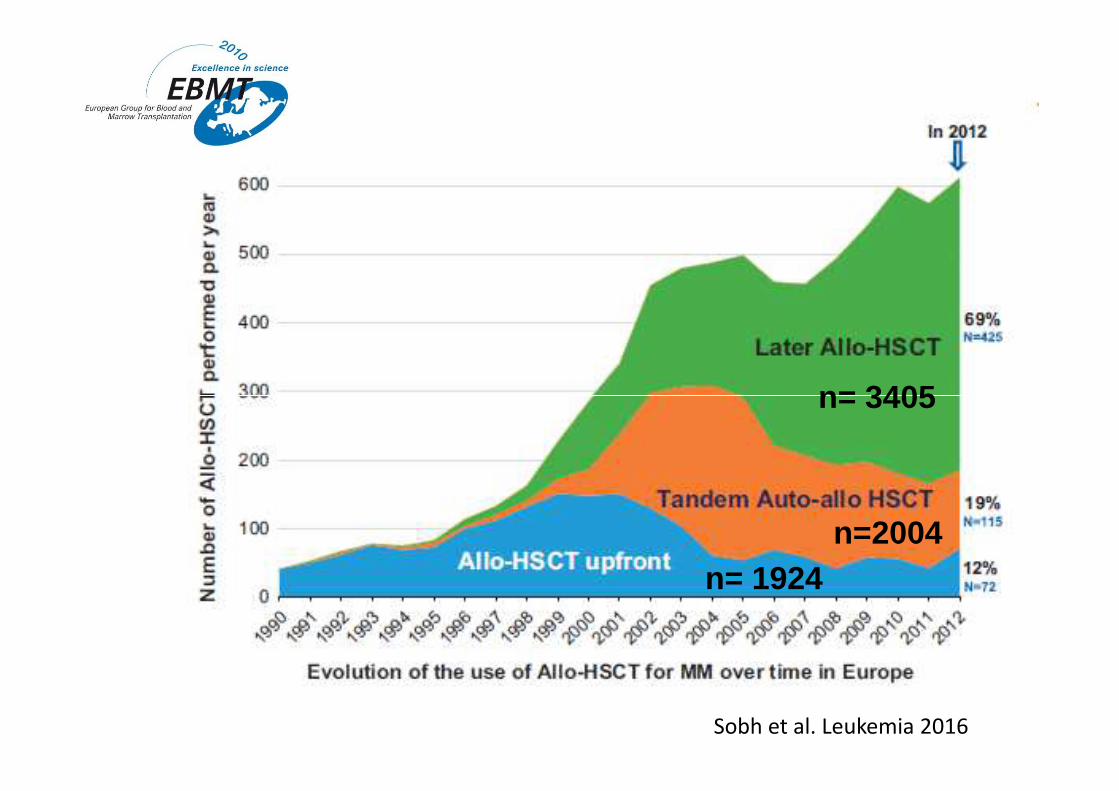
n= 3405
Sobh et al. Leukemia 2016
n= 1924n=2004
n= 3405

ALLO-UPFRONT
TANDEM AUTO-ALLO
OUTCOME ACCORDING TO TIME OF TX:
LATER ALLO HSCT
Sobh et al. Leukemia 2016

cGVHD correlates with clinical response, suggesting
the existence of a graft-versus-myeloma effect
Crawley et al. Blood 2005
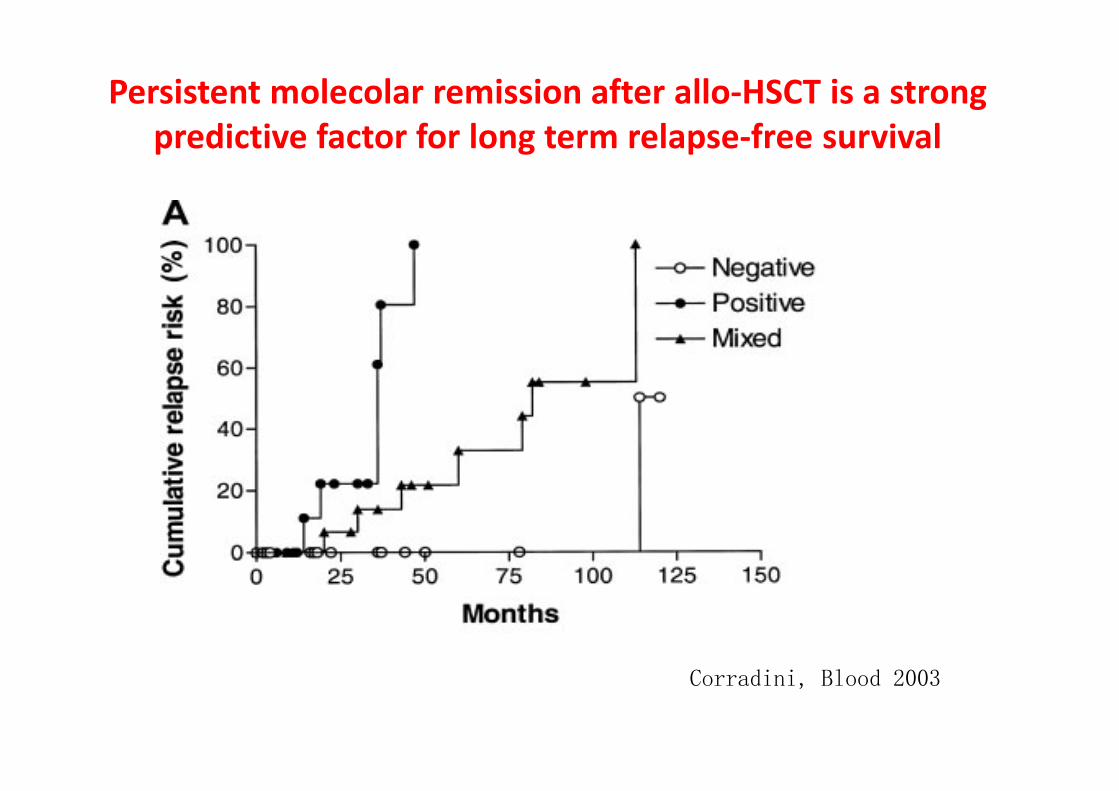
Persistent molecolar remission after allo-HSCT is a strong
predictive factor for long term relapse-free survival
Corradini, Blood 2003

Long-term clinical outcomes by molecular remission statusFollow up: 12.1 years
Ladetto et al, Leukemia 2016
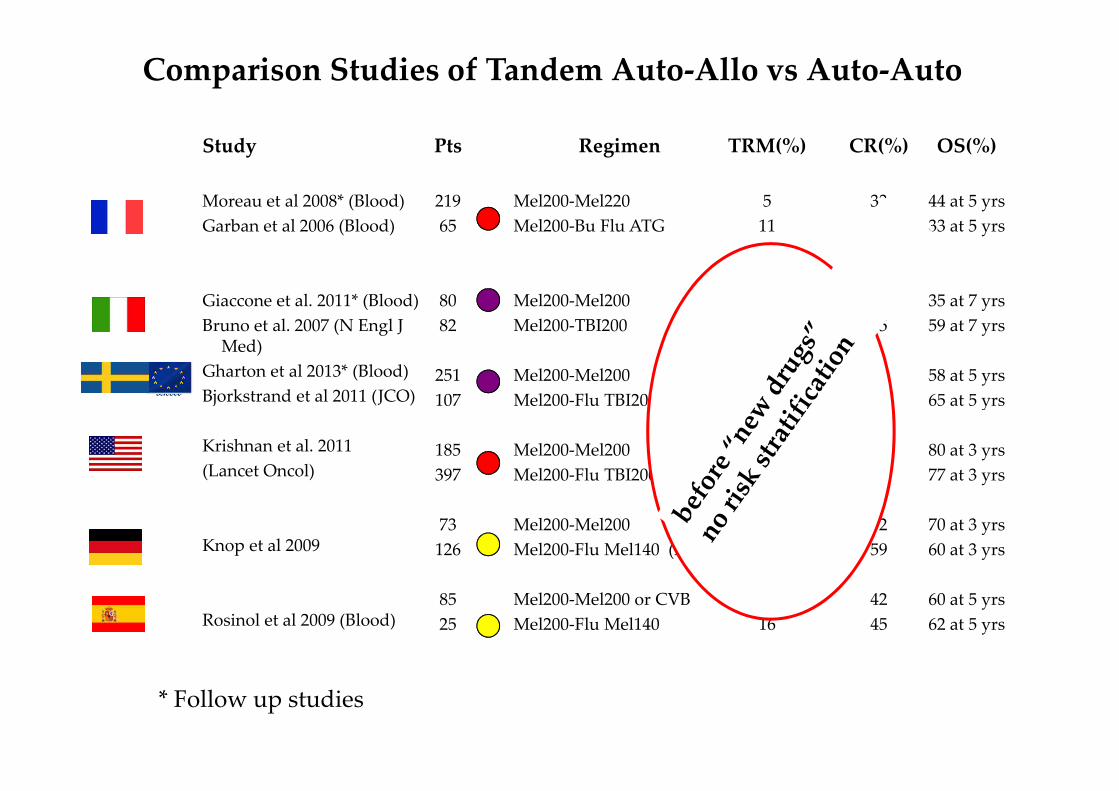
Comparison Studies of Tandem Auto-Allo vs Auto-Auto
Study
Moreau et al 2008* (Blood)
Garban et al 2006 (Blood)
Giaccone et al. 2011* (Blood)
Bruno et al. 2007 (N Engl J Med)
Gharton et al 2013* (Blood)
Bjorkstrand et al 2011 (JCO)
Pts
219
65
80
82
251
107
Regimen
Mel200-Mel220
Mel200-Bu Flu ATG
Mel200-Mel200
Mel200-TBI200
Mel200-Mel200
Mel200-Flu TBI200
TRM(%)
5
11
4
16
3 at 2 yrs
12 at 2 yrs
CR(%)
33
33
26
55
41
51
OS(%)
44 at 5 yrs
33 at 5 yrs
35 at 7 yrs
59 at 7 yrs
58 at 5 yrs
65 at 5 yrsBjorkstrand et al 2011 (JCO)
Krishnan et al. 2011
(Lancet Oncol)
Knop et al 2009
Rosinol et al 2009 (Blood)
107
185
397
73
126
85
25
Mel200-Flu TBI200
Mel200-Mel200
Mel200-Flu TBI200
Mel200-Mel200
Mel200-Flu Mel140 (ATG)
Mel200-Mel200 or CVB
Mel200-Flu Mel140
12 at 2 yrs
-
-
NR
16
5
16
51
45
58
32
59
42
45
65 at 5 yrs
80 at 3 yrs
77 at 3 yrs
70 at 3 yrs
60 at 3 yrs
60 at 5 yrs
62 at 5 yrs
* Follow up studies
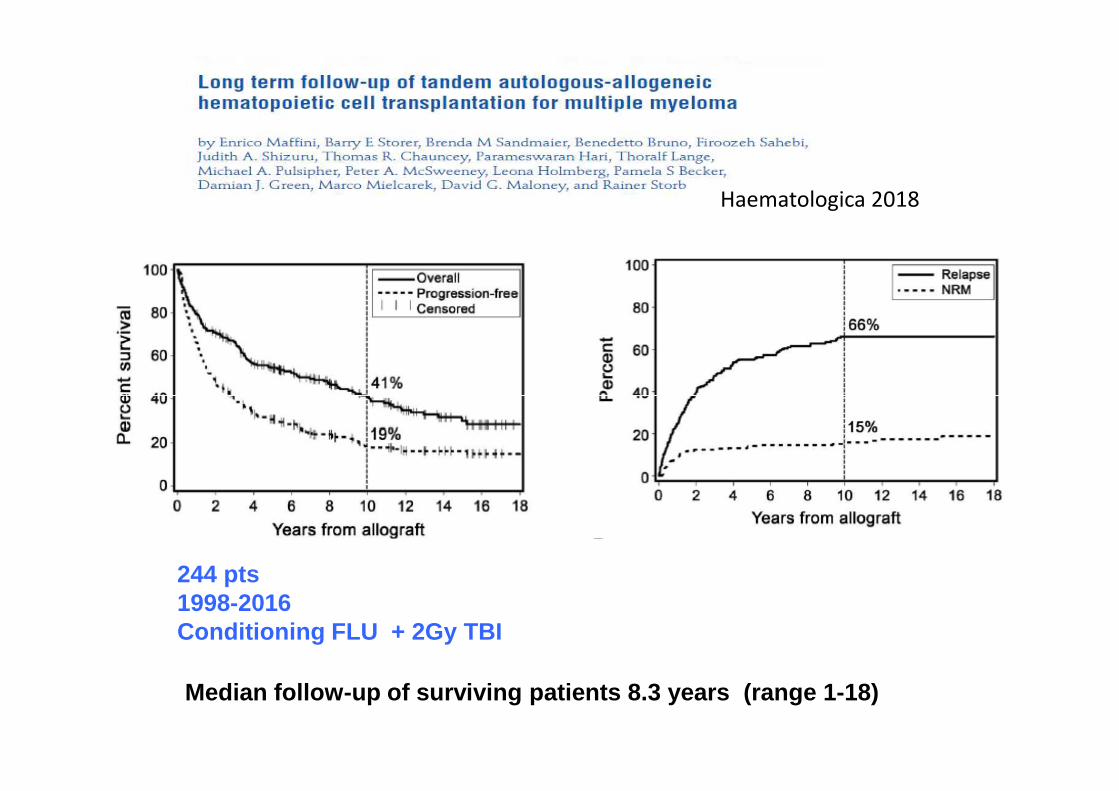
Haematologica 2018
244 pts1998-2016Conditioning FLU + 2Gy TBI
Median follow-up of surviving patients 8.3 years ( range 1-18)
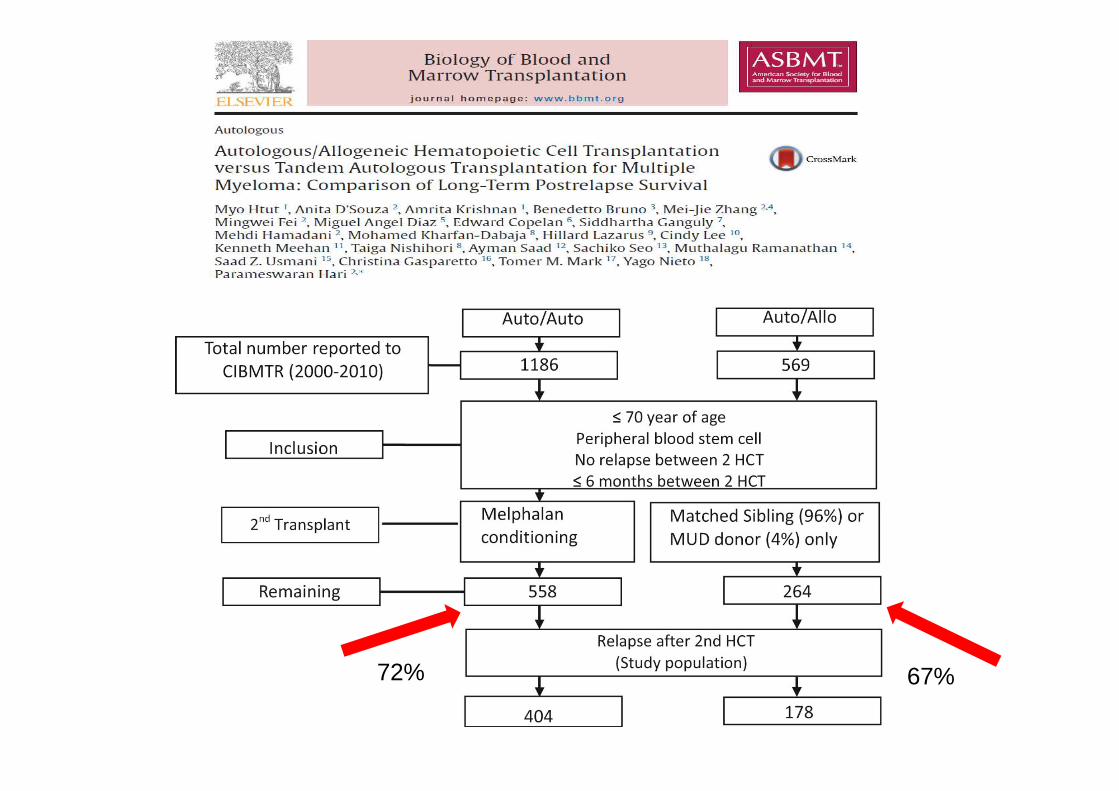
72% 67%
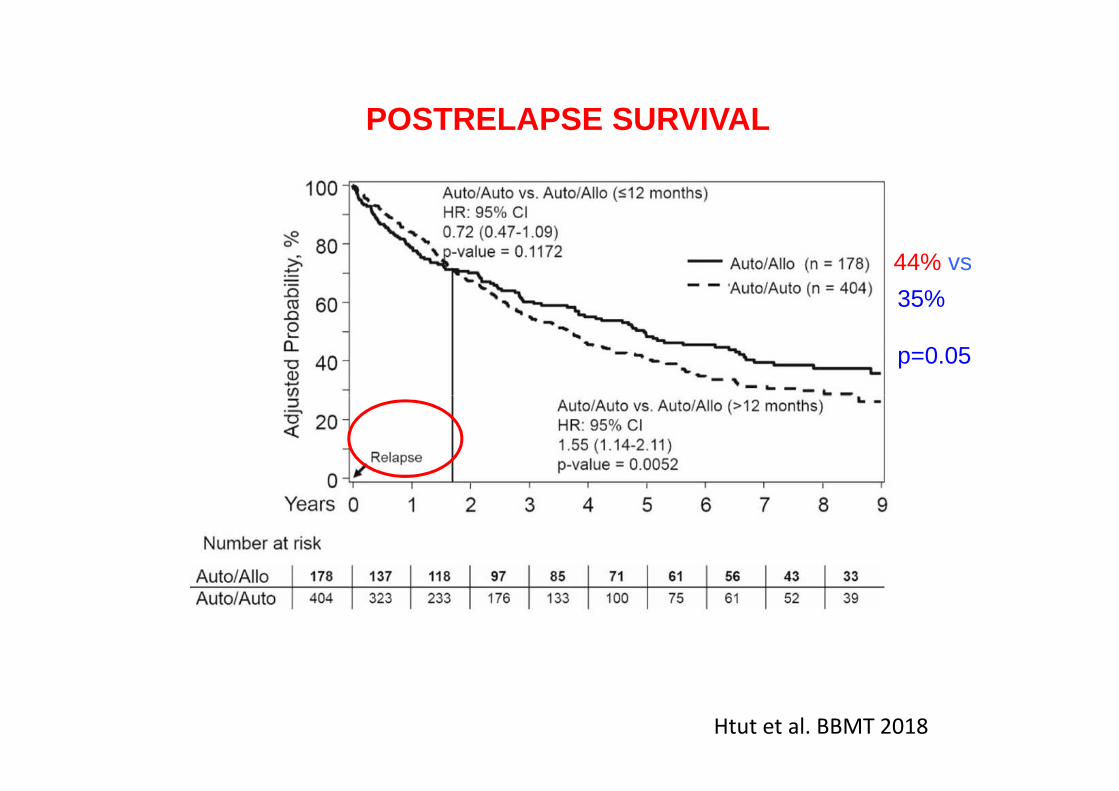
POSTRELAPSE SURVIVAL
44% vs
35%
p=0.05
Htut et al. BBMT 2018

Patriarca et al. BBMT 2018 UPDATE

LONG TERM PFS IN DONOR GROUP 0.
500.
751.
00P
roba
bilit
y
PFS
p<0.0001
p<0.0001
Donor 7 y PFS : 18%
0.00
0.25
0.50
Pro
babi
lity
0 20 40 60 80months
donor no_donor
Median follow-up of surviving patients 110 months ( range 38-180)
Donor 2 y PFS : 42%
No donor 2 y PFS 18%
No donor 7 y PFS 0
Patriarca et al. BBMT 2018 UPDATE

RIC , n=33
50%
DFS for 51 MM pts 2001-2018: Genova data
27%
MAC , n=18

CONCLUSION 1
# Most of the available data on allogeneic HSCT upfront inMM pts are before the era of the novel agents, are notstratified for risk and the results are discordant.
# Even thouth the evidence of a graft versus myeloma effectis associated with a long term disease control, a consistentsurvival benefit is not clearly demonstrated.survival benefit is not clearly demonstrated.
# Allo-HSCT should be considered AT DIAGNOSIS foryoung ultra high/high-risk patients only in clinical trilas andin EARLY RELAPSE (18 mm) from first-line treatmentwith/wo high-risk features according to IMWG/EMN/NCCNrecommendations.

ALLOGENEIC HSCT IN MM PTS
# WHEN AND WHO?
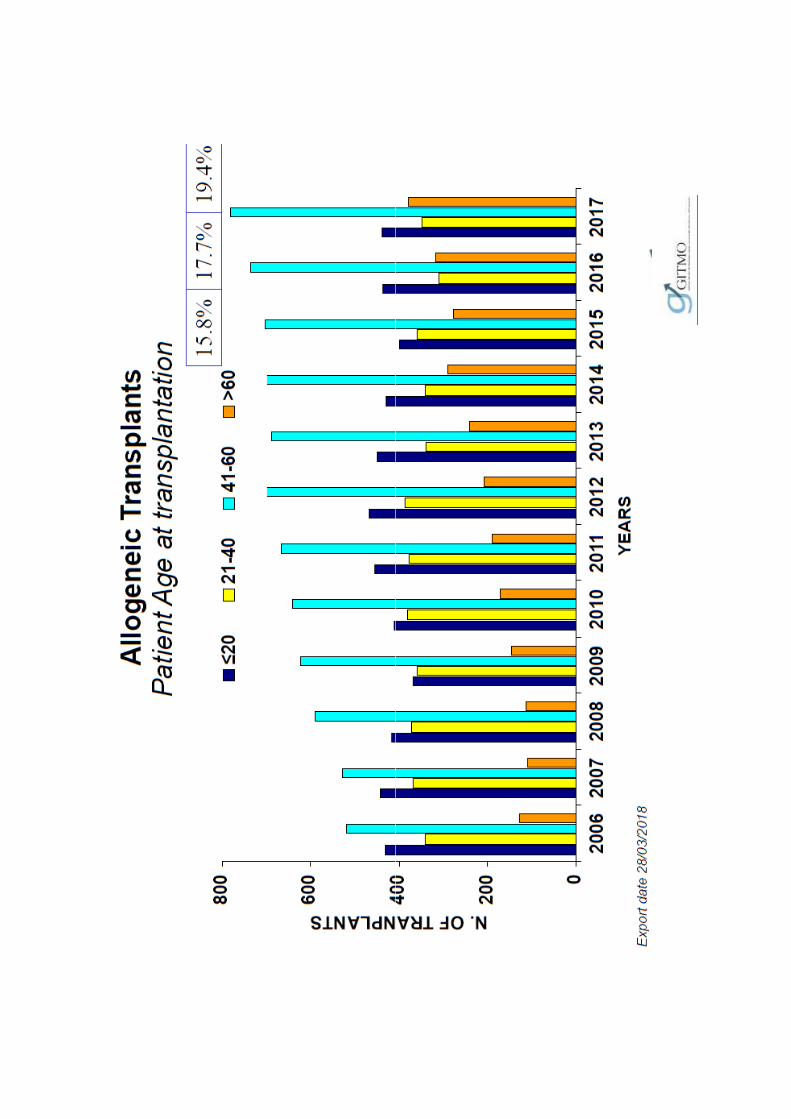
# PATIENT AGE
# COMORBIDITIES
# DONOR TYPE
# CONDITIONIG REGIMEN
# TRANSPLANT MORTALITY
# RELAPSE
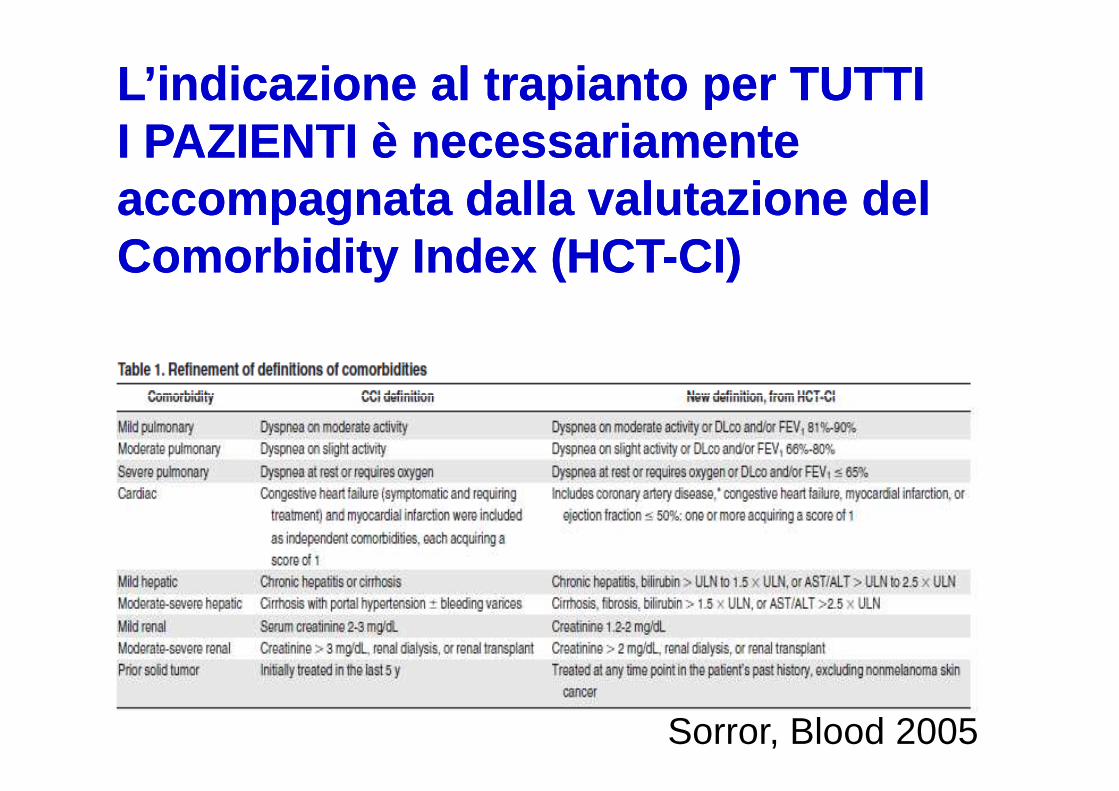
L’indicazioneL’indicazione al trapianto per TUTTI al trapianto per TUTTI I PAZIENTI è I PAZIENTI è necessariamentenecessariamenteaccompagnataaccompagnata dalladalla valutazionevalutazione del del Comorbidity Index (HCTComorbidity Index (HCT --CI)CI)
Sorror, Blood 2005
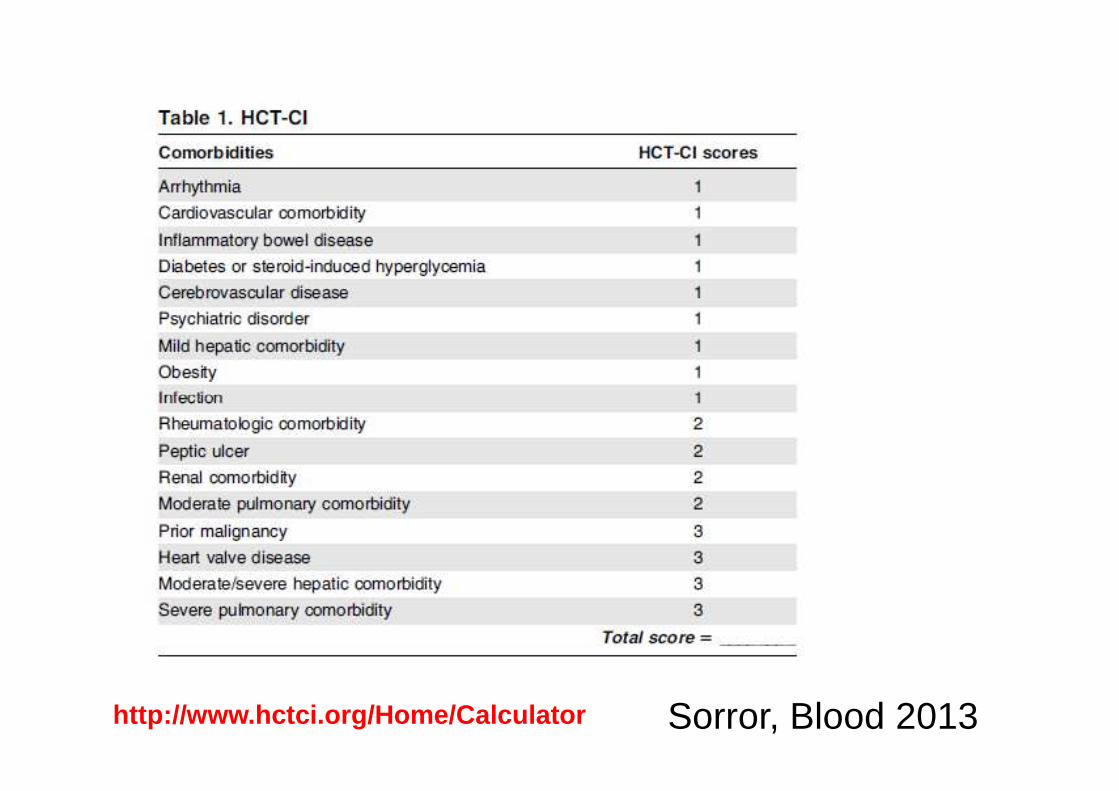
http://www.hctci.org/Home/Calculator Sorror, Blood 2013

CI-INDEX AND OUTCOME
Barba et al. BBMT 2014442 pts BMT 1998-2008 only RIC

ALLOGENEIC HSCT IN MM PTS
# WHEN AND WHO?
# PATIENT AGE
# COMORBIDITIES
# DONOR TYPE
# CONDITIONIG REGIMEN
# TRANSPLANT MORTALITY
# RELAPSE

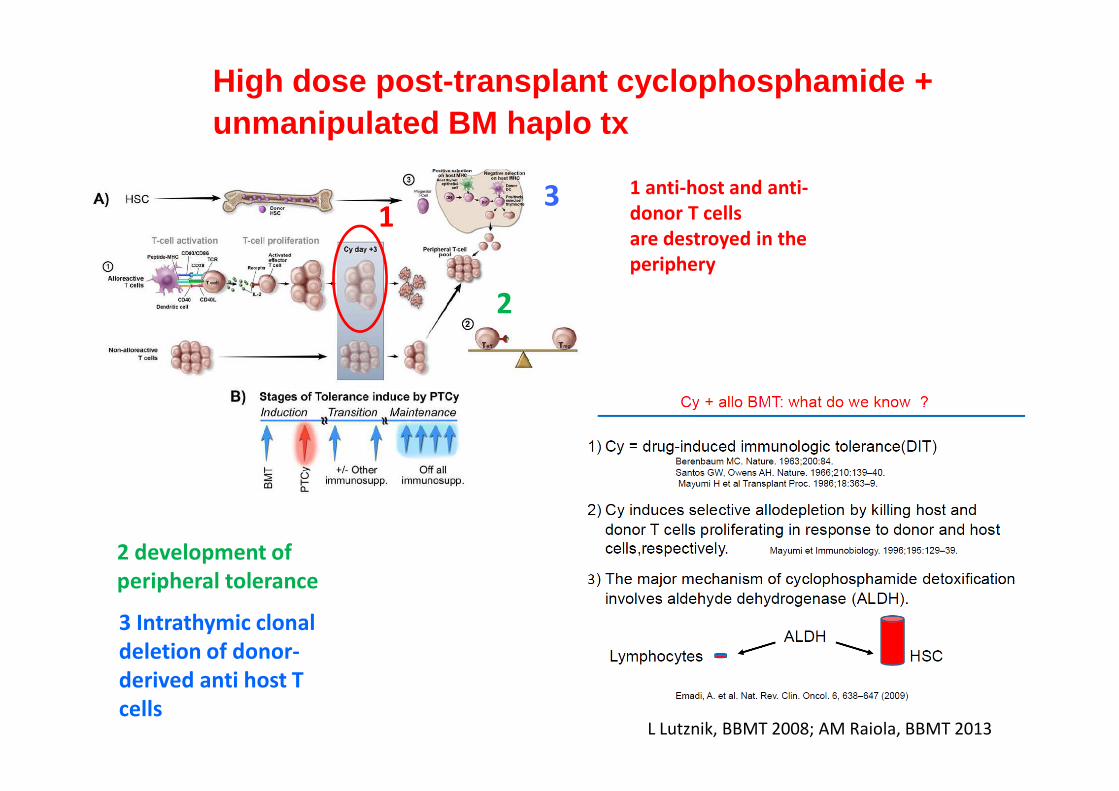
High dose post-transplant cyclophosphamide + unmanipulated BM haplo tx
1 anti-host and anti-
donor T cells
are destroyed in the
periphery
1
2
3
L Lutznik, BBMT 2008; AM Raiola, BBMT 2013
2 development of
peripheral tolerance
3 Intrathymic clonal
deletion of donor-
derived anti host T
cells
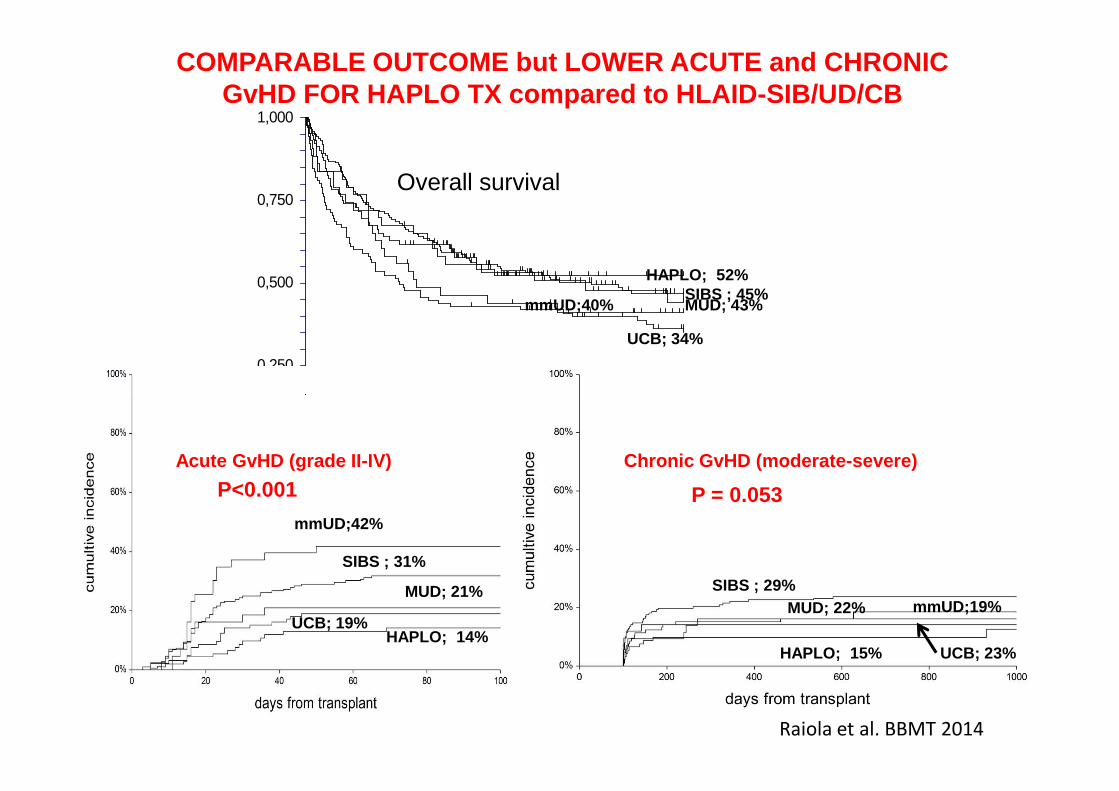
COMPARABLE OUTCOME but LOWER ACUTE and CHRONIC GvHD FOR HAPLO TX compared to HLAID-SIB/UD/CB
0,250
0,500
0,750
1,000
UCB; 34%
SIBS ; 45%HAPLO; 52%
mmUD;40% MUD; 43%
Overall survival
0,0000,0 266,7 533,3 800,0 1066,7 1333,3 1600,0
days from transplant
p=0.11
Acute GvHD (grade II-IV)
UCB; 19%
SIBS ; 31%
HAPLO; 14%
mmUD;42%
P<0.001
MUD; 21%
Chronic GvHD (moderate-severe)
MUD; 22%
UCB; 23%HAPLO; 15%
SIBS ; 29%
P = 0.053
mmUD;19%
Raiola et al. BBMT 2014

CONCLUSION 2
# Patient age at transplant is increased during thelast decade, due to better control of transplantrelated complications.
# It is mandatory the evaluation of the comorbiditiesin order to assess the risk of mortality at transplant.in order to assess the risk of mortality at transplant.
# The Sorror HCT-CI is simple and it is a veryuseful prognostic indicator.
# Haplo transplant is a valid alternative option, witha comparable outcome to the other donors and witha lower a/c GvHD.

ALLOGENEIC HSCT IN MM PTS
# WHEN AND WHO?
# PATIENT AGE
# COMORBIDITIES
# DONOR TYPE
# CONDITIONIG REGIMEN
# TRANSPLANT MORTALITY
# RELAPSE

Beginning in 1991
Classic Myeloablative conditioning
Median FU=26 months
40% at 76 months
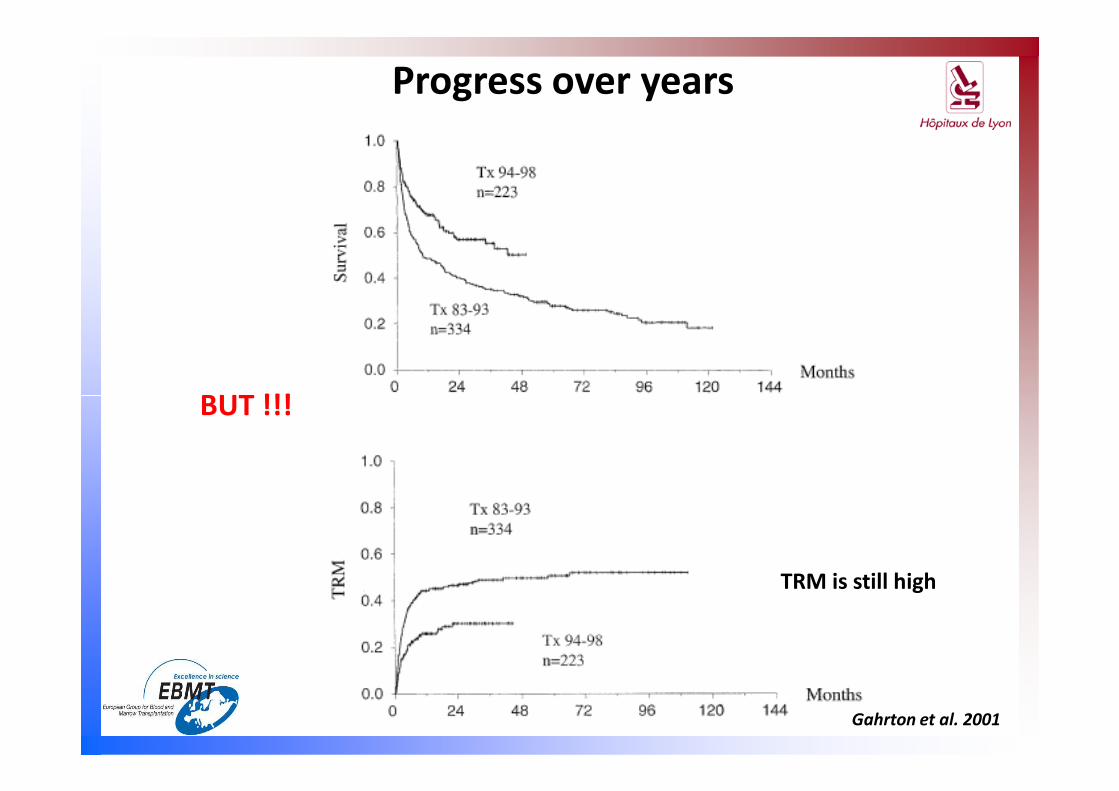
Progress over years
BUT !!!BUT !!!
TRM is still high
Gahrton et al. 2001

After 2000
Reduced Intensity Conditioning
NMA = fludarabine + TBI 2Gy
50% 50%20%40%
MA with reduced toxixity (RIC)=Fludarabine + melphalan 140 mg/m 2
(as alternative FLU+CY/BU+FLU)

N=196
N=320

BM
Conditioning regimen for allo-HSCT in MM pts in Genoa
CY CY
FOR HAPLO TX
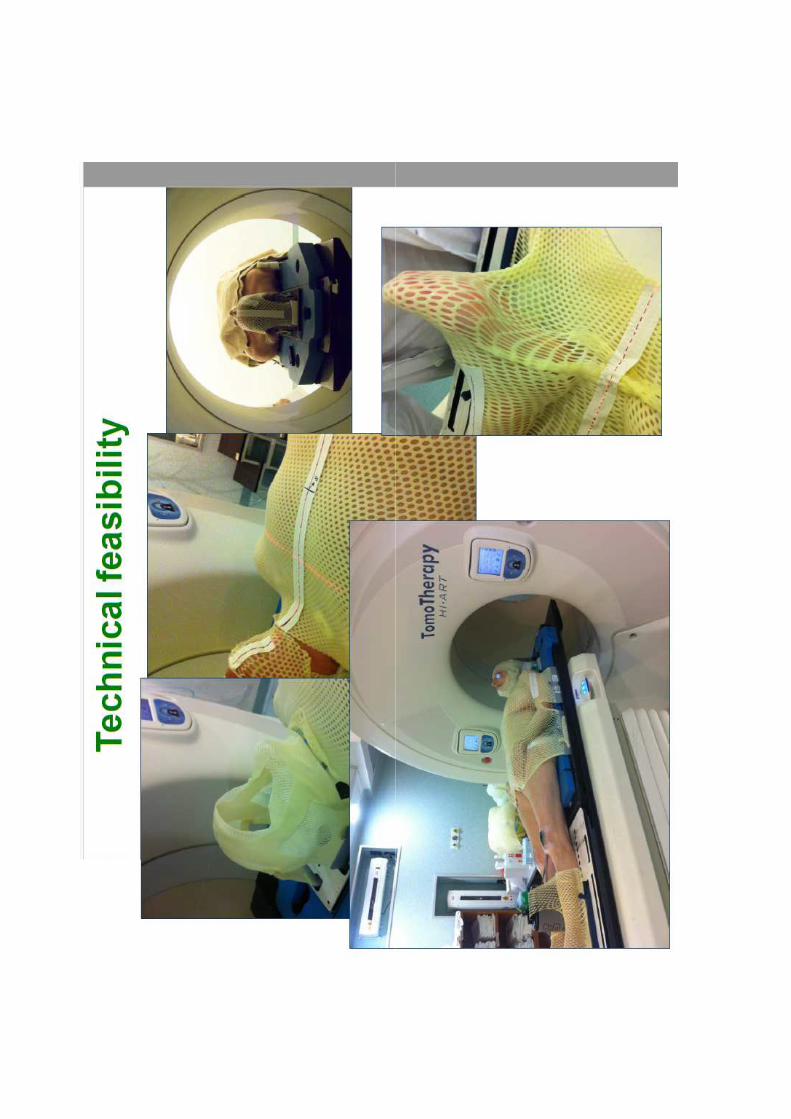
-9 -8 -7 -6 -5 -4 -3 -2 -1 0 +3 +4 +5
Thiotepa 10 mg/Kg day -6Fludarabine 50 mg/m^2 day -5-4-3Melphalan 140 mg/mq day -2
TMI 4 Gy day -9-8-7+boost tomotherapy on PET + bone lesions





ALLOGENEIC HSCT IN MM PTS
# WHEN AND WHO?
# PATIENT AGE
# COMORBIDITIES
# DONOR TYPE
# CONDITIONIG REGIMEN
# TRANSPLANT MORTALITY
# RELAPSE
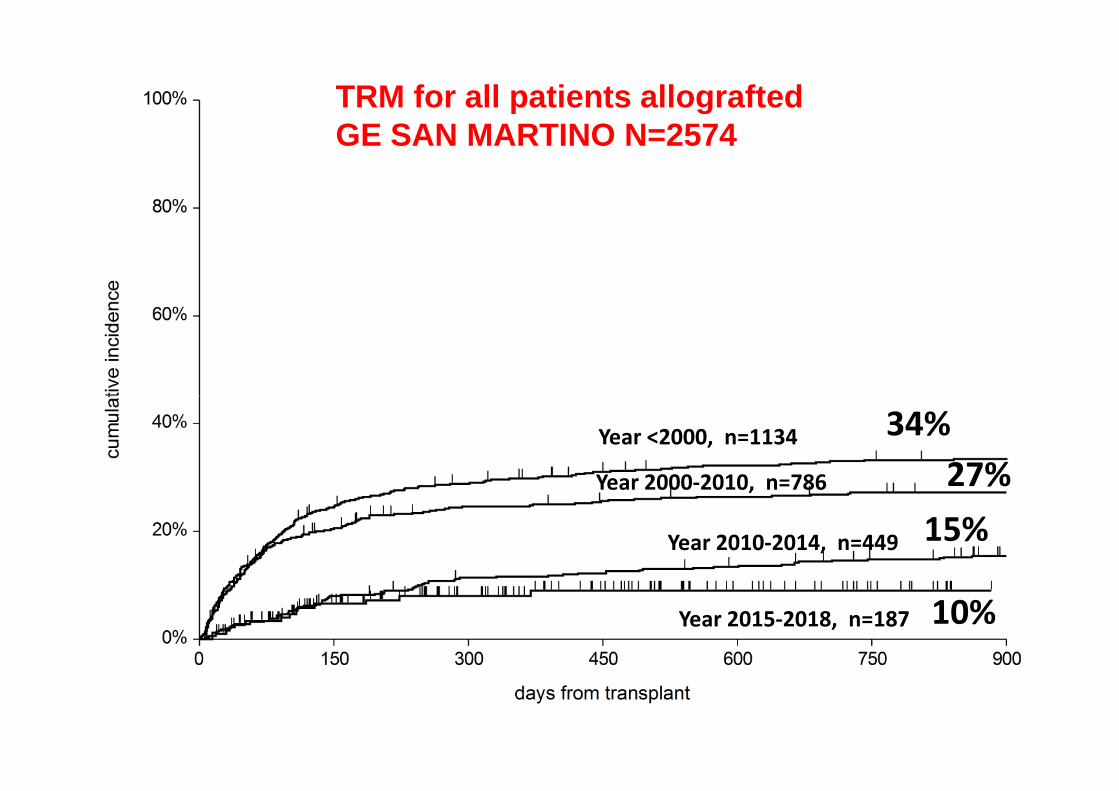
TRM for all patients allografted GE SAN MARTINO N=2574
34%
27%
15%
10%Year 2015-2018, n=187
Year 2010-2014, n=449
Year 2000-2010, n=786
Year <2000, n=1134
ALLOGENEIC HSCT IN MM PTS
# WHEN AND WHO?
# PATIENT AGE
# COMORBIDITIES
# DONOR TYPE
# CONDITIONIG REGIMEN
# TRANSPLANT MORTALITY
# RELAPSE
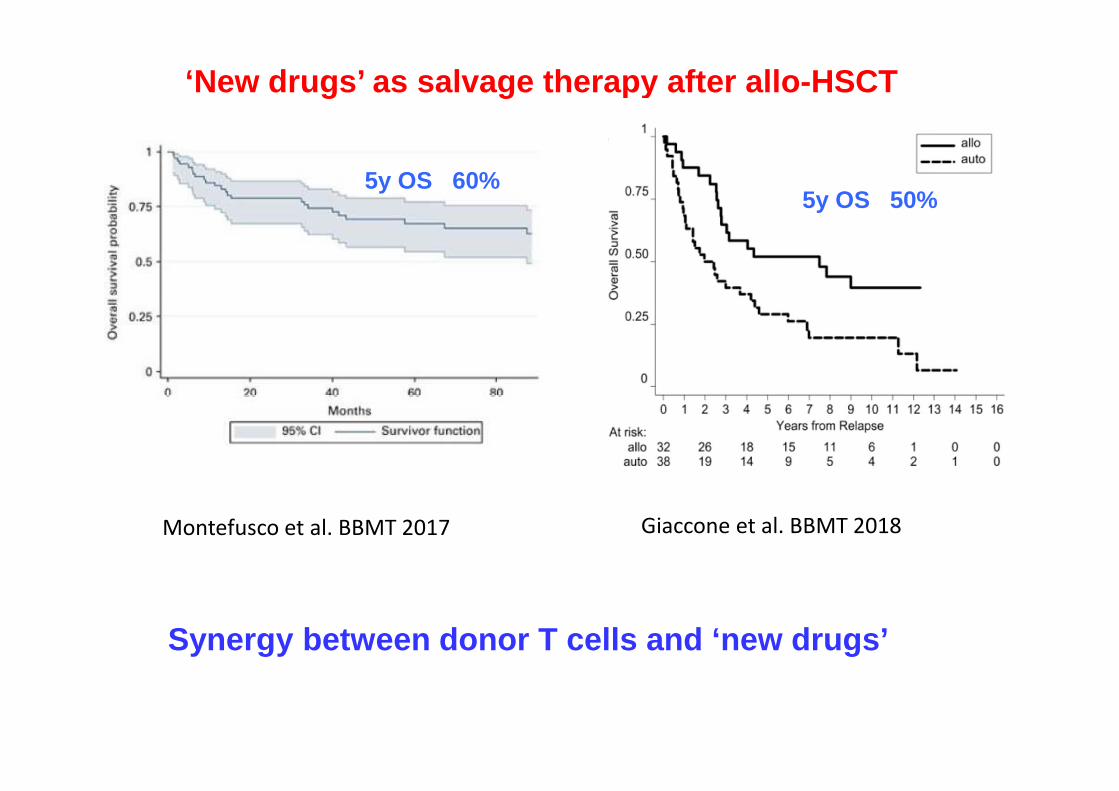
‘New drugs’ as salvage therapy after allo-HSCT
5y OS 60%5y OS 50%
Montefusco et al. BBMT 2017 Giaccone et al. BBMT 2018
Synergy between donor T cells and ‘new drugs’

Mobilization of PBSC
NDMM risk-analysis(Tp53 bi-allelic mutation, 1q amp and GEP70 signature)
ALLOGENIC TRANSPLANTATION (HCT)
INDUCTION TREATMENT
UP-FRONT THERAPYASCT
New proposal for high risk MM pts
ALLOGENIC TRANSPLANTATION (HCT)
ARM A
Maintenance with ixazomib
ARM B
Observation
Ultra-high RISK
MRD assessment at CR
SINGLE-AGENT IXAZOMIB MAINTENANCE AFTER ALLO-HSCT FOR
DOUBLE-HIT MM PATIENTS to reduce the risk of relapse

CONCLUSION 3
# Myeloablative reduced toxicity conditioning regimen (melphalanbased) is preferred to NMA for allo-HSCT in MM pts.
# Adding TMI to the standard conditioning regimen can be an option toreduce the risk of relapse w/o toxicity
# New drugs are synergic to donor T lymphocytes in relapsed patients# New drugs are synergic to donor T lymphocytes in relapsed patientsafter allo-HSCT with long term survival
# The incorporation of the proteasoma inhibitors (ixazomib) after allo-HSCT in high risk patients can be a new strategy in upfront setting.

R-ISSHAEMATOLO
BMT
U
HARVESTHARVEST
CONDITIONING CONDITIONING
CSE
OGY
DEPT
UNIT
CSE
Haematology Dept
A Ghiso
C Ghiggi
S. Nati
S Aquino
AM Congiu
A Ibatici
G Beltrami
E Angelucci
BMT Unit
C di Grazia
R Varaldo
M T Van Lint
S Bregante
AM Raiola
T Lamparelli
F Gualandi
Stem Cell Lab
S Geroldi
S Lucchetti
A Bo
Data Managers
M Daneri
G.Conti
B Bruno (GITMO)
Immunology
C Mingari
D Pende
R Meazza
Nursing team
Infect Dis Unit
C Viscoli
M Mikulska
Radiotherapy Unit
S Vagge
R Corvò