establishing the differential diagnosis of neck lesions
TRANSCRIPT

Medicine
Establishing the differential diagnosisof neck lesions
James A. Giglio, DDS, MEdVDaniel M. Laskin. DDS. MS^
A thorough physicai examinafion of the head and neck shouid be included as part of the evaluafion ofevery denfai pafienf. Aithough fhey most often represent a seif-iimited infiammation, a benign neopiasm, ora congenitai anomaly, neck lesions can aiso be malignant. Because the pathoiogic iesions thaf can arise inthe neck are varied and diverse, the diagnostic thought process should be orderiy and inclusive so fhal areasonable differential diagnosis can be established and prompt, effecfive treatment can be rendered.(Ouintessence Int 2000:31:637-641)
Key words: oiassificafion, differentiai diagnosis, neck lesion, physical examination, tumor
Anatomically, the neck constitutes only a small per-centage of the total body area, but it contains
many vital anatomic structures and diverse tissuetypes. Consequently, the pathologic lesions tbat canarise in tbe region are equally as varied and diverse.An examination of tbe neck for lesions sbould beincluded in the evaluation of every dental patient.
Various classifications of neck lesions bave beenproposed. Some are based on anatomic location, ie,median or paramedian swellings of the neck, whileothers are based on tissue of origin. Sarnat and Sbour'differentiated between primary and secondaryswellings, while Sedgwick^ divided the swellings intotnidline, lateral, and low-lying lesions. Another classi-fication used the organ systems approach (vascular.nervous, etc).^ Park-i grouped neek lesions accordingto their etiologic origin as inftammatory, neoplastic, orcongenital. Burton and Pransky' included palpablenormal anatomic masses, such as the transverseprocess of C2, the styloid process, the mastoid tip, thegreater cornu of the hyoid bone, and the thyroid carti-lage, in their classification. Otto and Bowes^ groupedlesions by patients' age, and tMcGuirt' used an algo-rithmic approach to the diagnosis and treatment of
'Protessor, Department ot Oral and Maxillofacial Suigery, Medical Collegeof Virginia, Virginia Commonwealtti university, Sctiool of Derilistry,
Richmond, Virginia.
'Professor and Chairman, Department oí Oral and Maxiilofacial Surgery,Medical College of Virginia, Virginia Commonwealth Unwersity. School olDentislry, Richmond, Virginia
Reprint requests: Dr James A Gigiio, Professor, Department ot Oral andMaxillotacial Surgery. PO Box 980566, Medical Coiiege of Virginia, VirginiaCommonwealtti University, School of Dentistry, Richmond. Virginia 23398-0566. E-mail: [email protected]
neck masses. All classifications, however varied, areuseful in that they help the clinician to order the diag-nostic thought process and form an initial impressionof the clinical findings.
Clinical evaluation must always begin with a tho-rough history and attention to symptoms. Most diag-nostic errors occur because the history and physicalexamination are inadequate and there is an overre-liance on sophisticated imaging techniques.* Patientsat risk for serious clinical problems can often be iden-tified through tbe findings on history taking, sucb asprogressive enlargement of the mass or prolongedhoarseness." A careful history will also begin to nar-row tbe range of possible lesions and guide deductivereasoning. For example, age can be a factor. In adultsolder tban 40 years, metastatic neoplasms are strongpossibilities and should be considered. For example, anontbj,Toid neck mass in an older patient has an SO /oprobability of being neoplastic, and SO /o of these aremalignant.'" In young aduks and teenagers, inflamma-tory lesions, especially from a third molar pericoroni-tis. are common. Infectious mononucieosis and thy-roid malignancies should also be suspected in patientsin this age group. Developmental lesions, as well asthe more common lymph node response to infectionand inflammation, sbould be considered in children.
The patient's report of the duration tbat a lesionhas been present is also helpful information. A rule ofthumb states that a mass present for 7 days is inflam-matory, a mass present for 7 montbs is neoplastic, anda mass present for 7 years is congenital' Because cer-tain lesions are found in discrete anatomic locations, aknowledge of those associated with specific regions inthe neck is useful in the differential diagnosis. The fol-lowing discussion uses this approach.
Quintessence International 637
• Giglio/Laskin
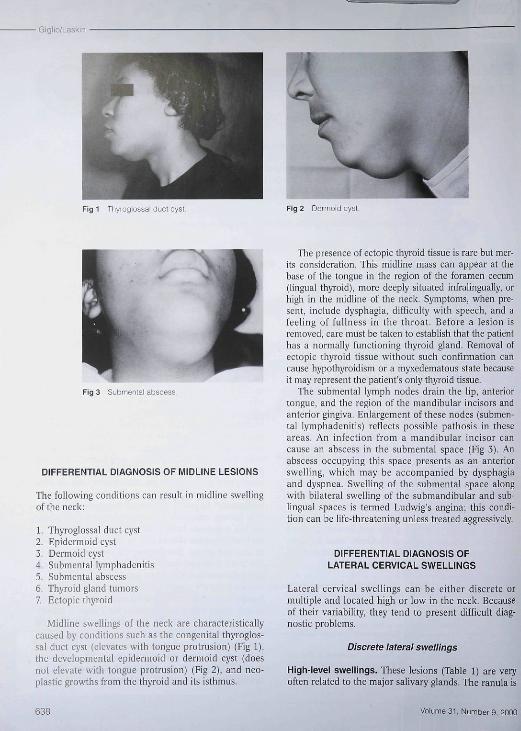
Fig 1 Thyroglossal duct cyst. Fig 2 Derrfioid cy
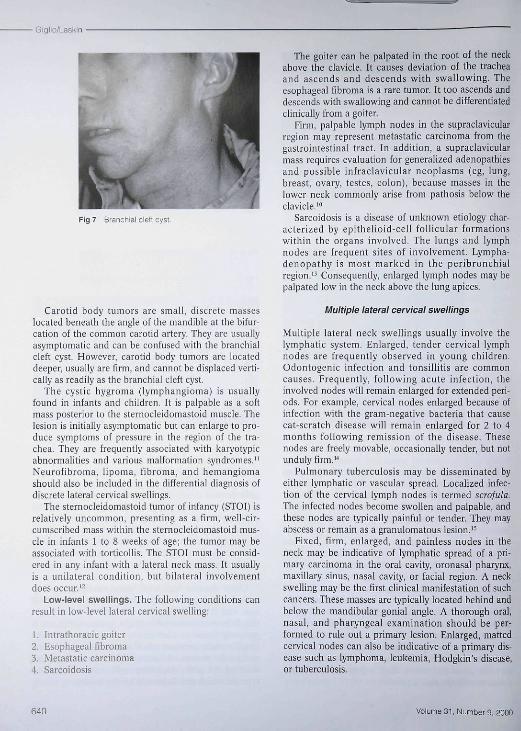
Fig 3 Submental abscess.
DIFFERENTIAL DIAGNOSIS OF MIDLINE LESIONS
Tbe following conditions ean result in midline swellingof the neek:
1. Thyroglossal duct eyst2. Epidermoid cyst3. Dermoid cyst4. Submental lymphadenitis5. Submental abscess6. Tbyroid gland tumors7. Ectopic thyroid
Midline swellings of tbe neck are characteristicallycaused by conditions sucb as tbe congenital thyroglos-sal duct cyst (elevates with tongue protrusion) (Fig 1),the developmental epidermoid or dermoiid cyst (doesnot elevate with tongue protrusion) (Fig 2), and neo-plastic growths from the thyroid and its isthmus.
The presence of eetopie thyroid tissue is rare but mer-its eonsideration. This midline mass can appear at thebase of the tongue in tbe region of tbe foramen cecum(lingual thyroid), more deeply situated infraiingually, orhigh in the midline of the neck. Symptoms, wben pre-sent, include dyspbagia, difficulty with speecb, and afeeling of fullness in the tbroat. Before a lesion isremoved, care must be taken to estabiisb that the patienthas a normally functioning thyroid gland. Removal ofeetopie thyroid tissue without sueh eonfirmation cancause bypotbyroidism or a myxedematous state becauseit may represent tbe patient's only tbyroid tissue.
The submental lympb nodes drain tbe lip, anteriortongue, and the region of the mandibular incisors andanterior gingiva. Enlargement of these nodes (submen-tal lymphadenitis) reflects possible patbosis in theseareas. An infeetion from a mandibular incisor cancause an absecss in the submental space (Fig 3). Anabseess occupying tbis space presents as an anteriorswelling, which may be accompanied by dysphagiaand dyspnea. Swelling of tbe submental space alongwitb bilateral swelling of tbe submandibular and sub-lingual spaces is termed Ludwig's angina; tbis condi-tion can be life-threatening unless treated aggressively.
DIFFERENTIAL DIAGNOSIS OFLATERAL CERVICAL SWELLINGS
Lateral cervical swellings can be cither discrete ormultiple and located bigb or low in the neck. Becauseof tbeir variability, they tend to present diflicult diag-nostic problems.
Discrete lateral swellings
High-level swellings. These lesions (Table 1) are veryoften related to the major salivary glands. The ránula is
638 VoiumG3t. Nürnberg, 2000

Giglio/Laskin
TABLE 1 High-level lateral cervical swellings
Lesion
Salivary gland tumorSialoadenitisCarotid body tumorBranchiai cieft cystCyslic hyg romaNeurofibtomaFibromaHemangiomaPlunging ranuiaEnlarged nodes
Type
NeopiasticinilammatoryNeopiasticDeveiopmentalNeopiasticNeopiasticNeopiasticNeopiasticTraumaticNeopiastic /intiammatory
Fig 4 Piunging ranuia.
Fig 5 fiefi) Oöstruotive siaioactenitis.
Fig 6 (beiow) Panoramic study reveaiing calculus deposit inglanOuiar system
a form of mucous retention phenomenon that developsin association with either the sublingual or sub-martdibular gland dticts. On occasion, the ránula her-niates through the mylohyoid muscle and is stthse-quently referred to as a plunging ránula (Fig 4). Thislesion is palpable high in the neck toward the midline.
The pleomorphic adenoma is the most commonsalivary gland tumor and is typically associated withthe parotid gland; however, it can involve the sub-mandibular gland. When arising from the parotidgland, the tumor will be palpable as a firm, discrete,nonftxed mass in the region of the mandihular angle.Pleomorphic adenomas of the submandihular glandare located in the suhmandibular triangle. The massesare usually freely mobile, discrete, and not adherent tothe overlying skin. Malignant tumors of the sub-mandibular gland should be suspected if the patient isan older adult and the swelling is firm and fixed, con-tinues to enlarge, and is painful.
Sialoadenitis should be considered if the swelling isacute and painful (Fig 5). Bidigitai palpation willoften help to define the presence of calculi within theglandular or duct system. Radiographs (Fig 6) andsialography wiil confirm the diagnosis. The formingcalculus may not have calcified and, consequently,may not be evident on the radiograph. However, thecontrast medium used for the sialogratn will usuallynot flow past such an ohstruction and thus indicatesits presence.
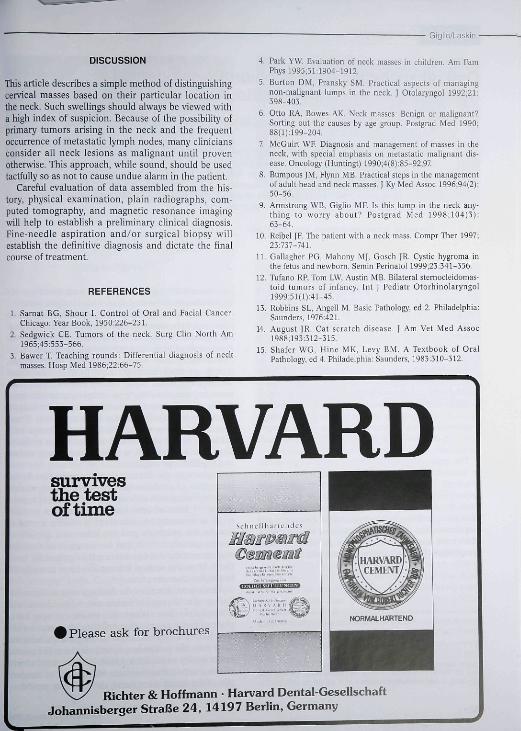
Other discrete high-level lateral cervical swellingsinclude the carotid hody tumor, the branchial eleftcyst, and the cystic hygroma. The branchial cleft cyst(Fig 7) is developmental in origin, grows slowly, and isgenerally found in adolescents and young adults. Thefreely mobile, painless lesion is usually located ante-rior to the sternoelcidomastoid muscle in the upperthird of the neck. Aspiration will reveal cholesterolcrystals, which are diagnostic for the lesion.
Quintessence international 639
• Gigüo/LaskJn
Fig 7 Branctiial clelt cyst.
Carotid body tumors are small, discrete masseslocated beneath the angle of the mandible at the bifur-cation of the common carotid artery. They are usuallyasymptomatic and can be confused with the branchialcleft cyst. However, carotid body tumors are locateddeeper, usually are firm, and cannot be displaced verti-cally as readily as the branchial cleft cyst.
The cystic hygroma (lymphangioma) is usuallyfound in infants and children. It is palpable as a softmass posterior to the sternocleidomastoid muscle. Thelesion is initially asymptomatic but can enlarge to pro-duce symptoms of pressure in the region of the tra-chea. They are frequently associated with karyotypicabnormalities and various malformation syndromes."Neurofibroma, iipoma, fibroma, and hemangicmashould also be included in the differential diagnosis ofdiscrete lateral cervical swellings.
The sternocleidomastoid tumor of infancy (STOI) isrelativeiy uncommon, presenting as a firm, well-cir-cumscrlbed mass within the sternocleidomastoid mus-cle in infants 1 to 8 weeks of age; the tumor may beassociated with torticollis. The STOI must be consid-ered in any infant with a lateral neck mass. It usuallyis a unilateral condition, but bilateral involvementdoes occur.'
Low-level swellings. Tbe following conditions canresult in low-level lateral cervical swelling:
1. Infrafhoracic goiter2, Esophageal fibroma3, Metastatic carcinoma4. Sarcoidosis
The goiter can be palpated in the root of the neckabove the clavicle. It causes deviation of the tracheaand ascends and descends with swallowing. Theesophageal fibroma is a rare tumor. It too ascends anddescends with swallowing and cannot be differentiatedclinically from a goiter.
Pirm, palpable lympb nodes in fhe supraclavicularregion may represent metastafic carcinoma from thegastrointestinal tract. In addition, a supraclavicularmass requires evaluation for generalized adenopathiesand possible infraclavicular neoplasms (eg, lung,breast, ovary, testes, colon), because masses in thelower neck commonly arise from pathosis below theclavicle,'"
Sarcoidosis is a disease of unknown etiology char-acterized by epithelioid-cell follicuiar formationswithin the organs involved. The lungs and lymphnodes are frequent sites of involvement. Lympha-denopathy is most marked in the peribronchialregion.' Consequently, enlarged lymph nodes may bepalpated low in tbe neck above the lung apices.
Multiple lateral cervical swellings
Multiple lateral neck swellings usually involve thelymphatic system. Enlarged, tender cervical lymphnodes are frequently observed in young children,Odontogenic infection and tonsillitis are commoncauses. Frequently, following acute infection, theinvolved nodes will remain enlarged for extended peri-ods. For example, cer\'ical nodes enlarged because ofinfection with the gram-negative bacteria thaf causecat-scratch disease will remain enlarged for 2 to 4months following remission of the disease. Thesenodes arc freely movable, occasionally tender, but notunduly firm."
Pulmonary tuberculosis may be disseminated byeither lymphatic or vascular spread. Localized infec-tion of the cervical lymph nodes is termed scrofula.The infected nodes hecome swollen and palpable, andthese nodes are typically painful or tender. They mayabscess or remain as a granulomatous lesion,'^
Fixed, firm, enlarged, and painless nodes in theneck may be indicative of lymphatic spread of a pri-mary carcinoma in the oral cavity, oronasal pharynx,maxillary sinus, nasal cavity, or facial region. A neckswelling may be the first clinical manifestation oí suchcancers. These masses are typically located behind andbelow fhe mandibular gonial angle. A thorough oral,nasal, and pharyngeal examinafion should be per-formed to rule out a primary lesion. Enlarged, mattedcervical nodes can also be indicative of a primary dis-ease such as lymphoma, leukemia, Hodgkin's disease,or tuberculosis.
640 Volume 31, Number 9. 2Q00
Giglio/Laskin •
DISCUSSION
This article describes a simple method of distinguishingcervical masses hased on their particular location inthe neck. Such swellings should always he viewed witha high index of suspicion. Because of the possibility ofprimary tumors arising in the neck and the frequentoccurrence of metastatic lymph nodes, many cliniciansconsider all neck lesions as malignant until provenotherwise. This approach, while sound, should be usedtactfully so as not to cause undue alarm in the patient.
Careful evaluation of data assembled from the his-tory, physical examination, plain radiographs, com-puted tomography, and magnetic resonance imagingwill help to establish a preliminary clinical diagnosis.Fine-needle aspiration and/or surgical biopsy willestablish the definitive diagnosis and dictate the finalcourse of treatment.
REFERENCES
1. Sarnat BG, Shour I. Controi of Oral and Facial Cancer.Chicago; Year Book, 1950:226-231.
2. Sedgwicit CE Tumors of the neck. Surg Clin North Am
5. Bawer T. Teaching rounds: Differential diagnosis of neckmasses. Hosp Med 1986:22 66-75.
4. Park YW. Evaluation of neck masses in children. Am FamPhysl995;5!:1904-1912.
5. Burton DM, Pransky SM. Practical aspects of managingnon-malignant lumps in the neck. J Otoiaryngol 1992;21:398-403.
6. Otto RA, Bowes AK. Nt;c:k masses: Benign or malignant?Sorting out the causes by age group. Postgrad Med 1990;88(l);199-204.
7. McGuirt WF. Diagnosis and management of masses in theneck, with special emphasis on metastatic malignant dis-ease. Oncology (Huntingt] 1990 ;4(S):85-92,97
8. Bunipous |M, Fiynn MB Practical steps in the managementof aduit head and neck masses. J Ky Med Assoc 1996;94(2):50-56.
9. Armstrong WB, Giglio MF. Is this lump in the neck any-thing to worry about? Postgrad Med 1998;104(3).63-64
10 Reibel JP. The patient with a neck mass. Compr Ther 1997;23:737-741.
11. Gallagher PG, Mahony MJ, Gosch |R. Cystic hygroma inthe fetus and newborn. Semin Perinatol 1999;23:341-356.
12. Tufano RP, Tom LW, Austin MB Bilateral sternocleidomas-toid tumors of infancy. lnl ] Pediatr Otorhinolaryngol1999;5111):41-45
13. Robbins SL, Angelí M. Basic Pathology, ed 2. Philadelphia:Saunders, 1976:421.
14. August JR. Cat scratch disease. J Am Vet Med Assoc1988:193:312-315.
15. Shafer WG. Hine MK, Levy BM A Textbook of OralPathology, cd 4. Philadeipiiia: Saunders, 1983.310-312.
HARVARDsurvivesthe testof time
I Please ask for brochures
^ Richter & Hoffmann • Harvard Dental-GesellschaftJohannisberger Straße 24, 14197 Berlin, Germany