estimation of the number of people with undiagnosed hiv infection in a country andrew phillips, ucl,...
TRANSCRIPT
Estimation of the number of people with undiagnosed HIV infection in a country
Andrew Phillips, UCL, London
HIV in Europe Meeting2 November 2009, Stockholm.
Approaches to estimation of the number of people with undiagnosed HIV infection in a country
- based on prevalence surveys
- based on reported numbers of HIV diagnoses - based on reported simultaneous HIV/AIDS cases

Approaches to estimation of the number of people with undiagnosed HIV infection in a country
- based on prevalence surveys
- based on reported numbers of HIV diagnoses - based on reported simultaneous HIV/AIDS cases

Divide population into categories according to risk
MSM
IDU
AfricansMSM
Assess HIV Prevalence in the risk category
MSM
IDU
AfricansHIV prevalence
MSM

Estimate number of people in the risk category (size)
MSM
IDU
AfricansHIV prevalence x Size
MSM
Multiply to give estimated number with HIV
MSM
IDU
AfricansHIV prevalence x Size
= Number with HIV
MSM
Subtract the number with diagnosed HIV
IDU
Africans Number with HIV – Number with diagnosed HIV
MSM

….to give the number with undiagnosed HIV
IDU
Africans Number with HIV – Number with diagnosed HIV
= Number with undiagnosed HIV
MSM
Add estimates across risk categories
IDU
Africans Number with HIV – Number with diagnosed HIV
= Number with undiagnosed HIV
MSM
+
+
+

MSM
IDU
AfricansHIV prevalence x Size
= Number with HIV
MSM
Alternative Approach

Alternative Approach
MSM
IDU
AfricansUndiagnosed HIV prevalence x Size
= Number with undiagnosed HIV
MSM
Approach based on prevalence surveys
Issues to consider
What risk categories to divide population into ?
How to estimate the size of each category ?
What prevalence to assume for those not falling into any of the selected ‘risk’ categories ?
Are the prevalence surveys based on representative samples of the risk category ?

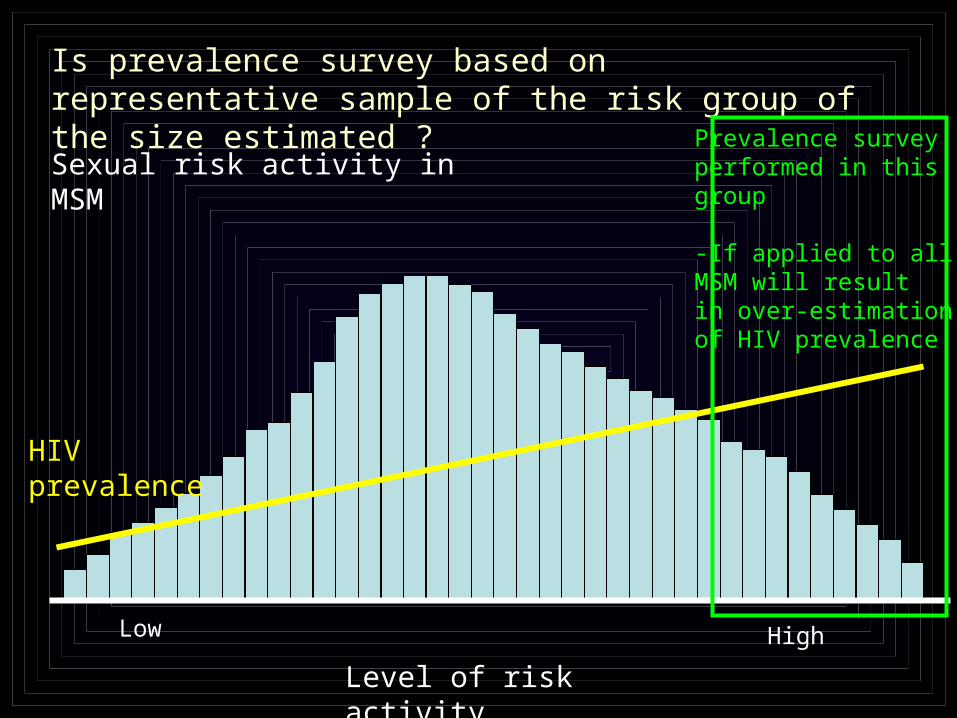
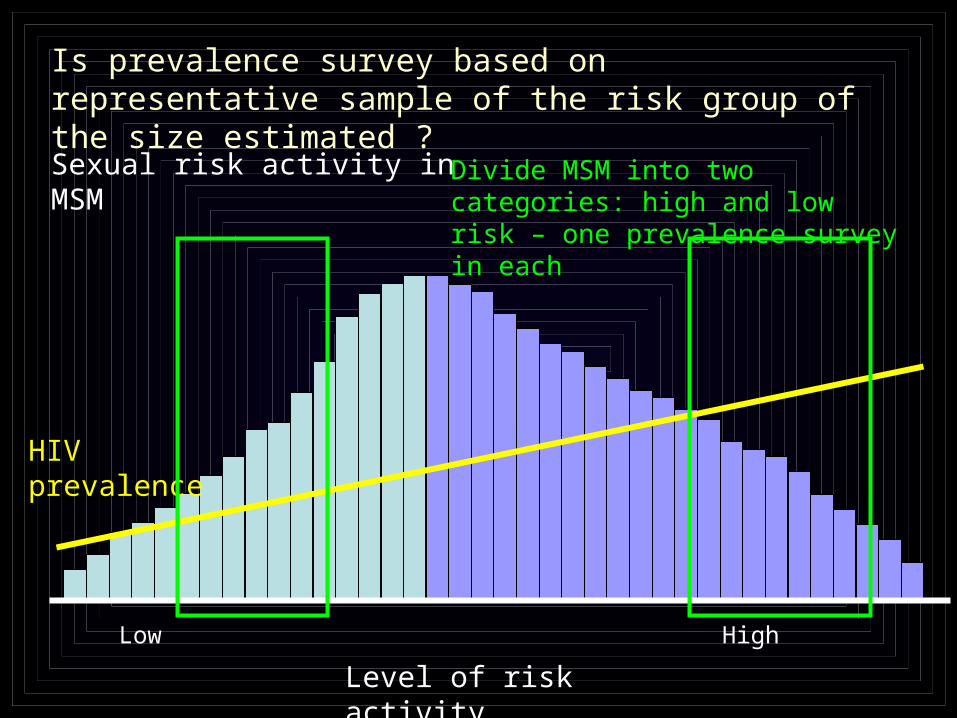
Is prevalence survey based on representative sample of the risk group of the size estimated ?
Level of risk activity
HighLow
Sexual risk activity in MSM
HIV prevalence
Is prevalence survey based on representative sample of the risk group of the size estimated ?
Level of risk activity
HighLow
Prevalence surveyperformed in this group
-If applied to all MSM will result in over-estimationof HIV prevalence
HIV prevalence
Sexual risk activity in MSM
Is prevalence survey based on representative sample of the risk group of the size estimated ?
Level of risk activity
HighLow
Sexual risk activity in MSM
HIV prevalence
Divide MSM into two categories: high and low risk – one prevalence survey in each

Approach based on prevalence surveys
Advantages
- Assumptions are explicit and effect of changing them can be investigated
- Can provide up-to-date estimates
- Avoids assumptions involved in other methods
Approaches to estimation of the number of people with undiagnosed HIV infection in a country
- based on prevalence surveys
- based on reported numbers of HIV diagnoses - based on reported simultaneous HIV/AIDS cases

Original “back-calculation” approach, before availability of treatment
Calendar year
Number of AIDScases diagnosed

Original “back-calculation” approach, before availability of treatment
Calendar year
What can this tell usabout how many peoplewere infected and whenthey were infected ?
Observed number of AIDS cases diagnosed

Curve linking infection to AIDS, without treatment
Expected number of new AIDS cases per year after 1000 people infected - illustration
Number of new AIDS cases per year
2 3 10 25 40 65 80 90 100 100 100 90 80 70 55 30 25 15 10 5 5
Years from infection0 5 10 15 20
Curve known from seroconverter cohorts

2 3 10 25 40 65 80 90 100 100 100 90 80 70 55 30
2 3 10 25 40 65 80 90 100 100 100 90 80 70
2 3 10 25 40 65 80 90 100 100 100
2 3 12 28 50 92 123 165 205 230 265 270 270 260 235 200
t0t0t2t0 t1
Numbers of AIDS cases expected over time if 1000 people infected at t0, t1 and t2
Assume a certain number of people infected in each year, and calculate the expected number of AIDS cases by year - how close is this to the observed number ?
Adjust the assumed number infected in each year to give the best fit to the observed number of AIDS cases
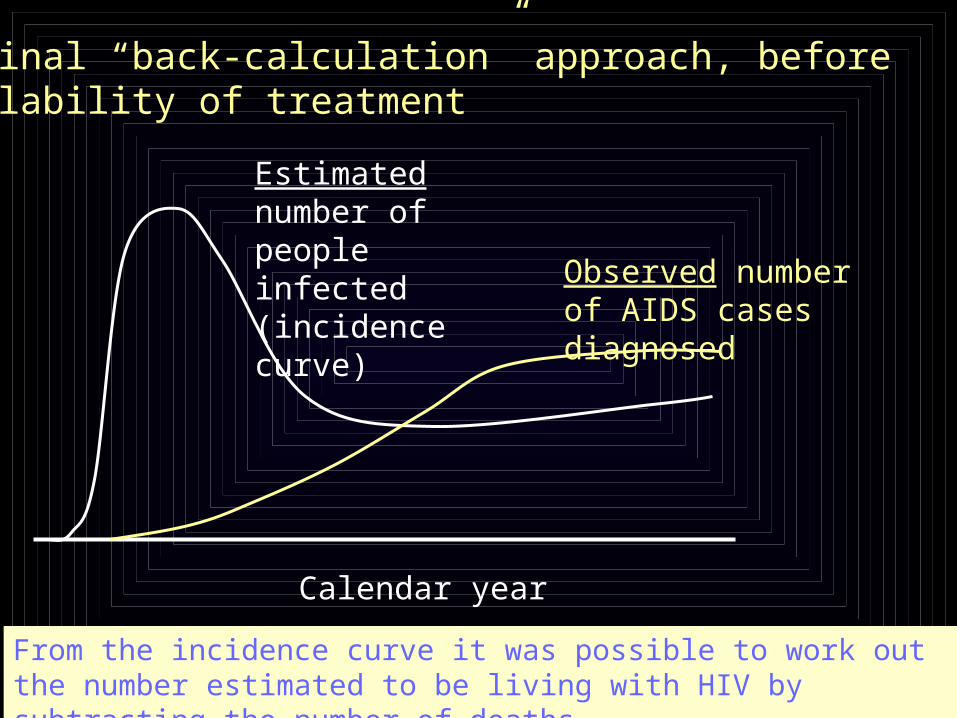
Original “back-calculation” approach, before availability of treatment
Estimated number of people infected (incidence curve)
Observed number of AIDS cases diagnosed
Calendar year
From the incidence curve it was possible to work out the number estimated to be living with HIV by subtracting the number of deaths

Revised back-calculation approach
Question changes…
How many people must be infected, and when must they have been infected, in order to produce the numbers of new AIDS we have observed ?
How many people must be infected, and when must they have been infected, and what must the probability of getting diagnosed have been, in order to produce the numbers of new HIV diagnoses we have observed ?
infection AIDS
infection HIV diagnosis
from:
to:
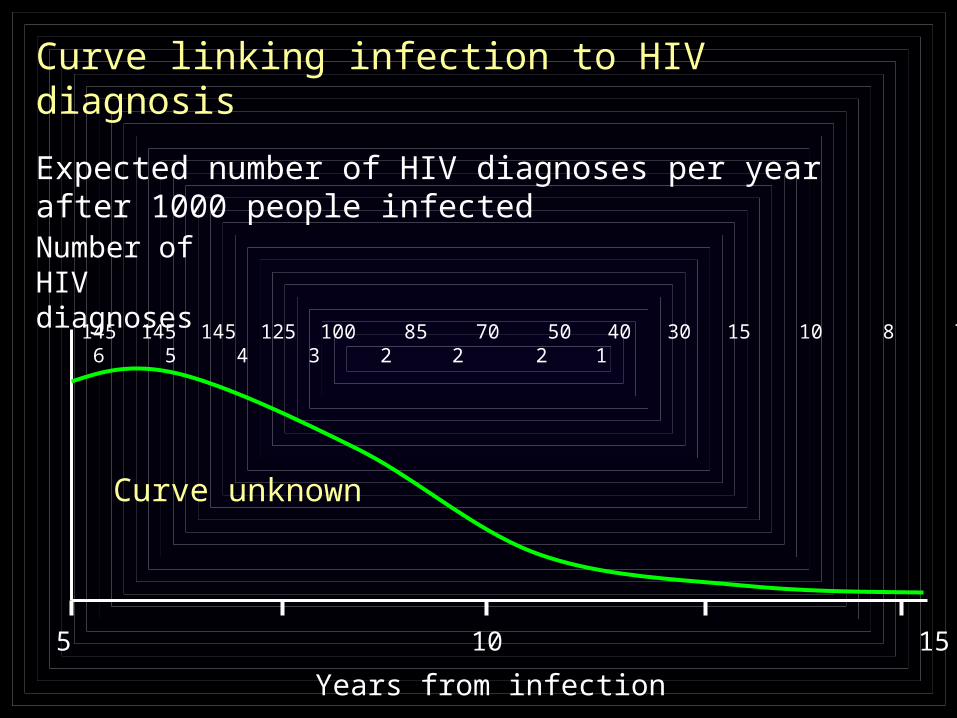
Curve linking infection to HIV diagnosis
Expected number of HIV diagnoses per year after 1000 people infected
Number of HIV diagnoses
Years from infection
0 5 10 15 20
145 145 145 125 100 85 70 50 40 30 15 10 8 7 6 5 4 3 2 2 2 1
Curve unknown
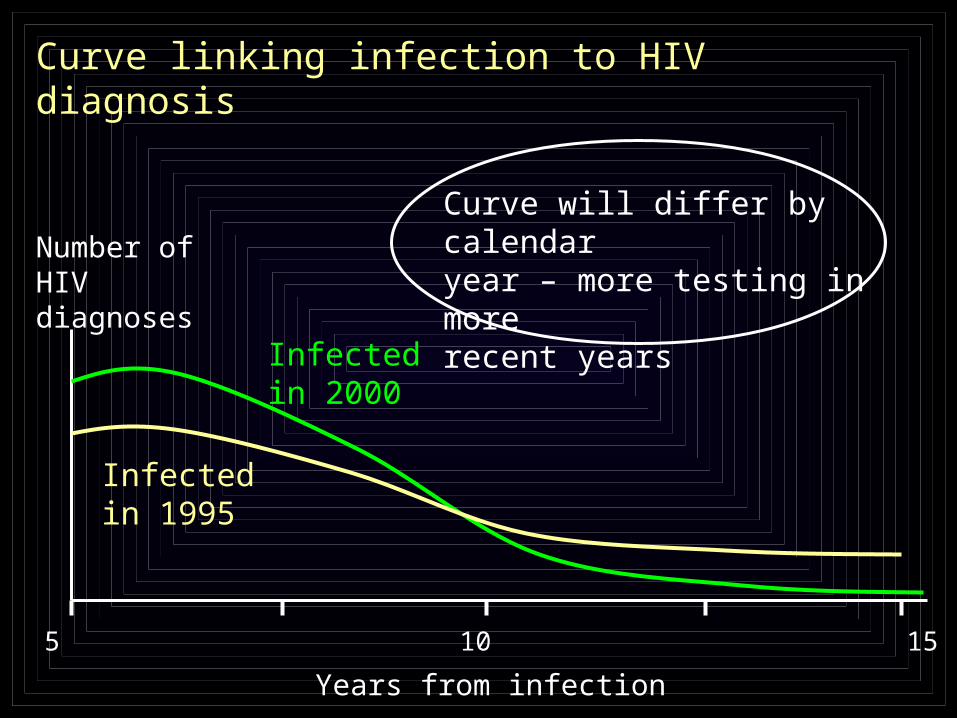
Curve will differ by calendar year – more testing in more recent years
Number of HIV diagnoses
Years from infection
0 5 10 15 20
Infected in 2000
Infected in 1995
Curve linking infection to HIV diagnosis
0
500
1000
1500
2000
2500
3000
3500
4000
2003 2004 2005 2006 2007 2008
0
0.1
0.2
0.3
0.4
0.5
0.6
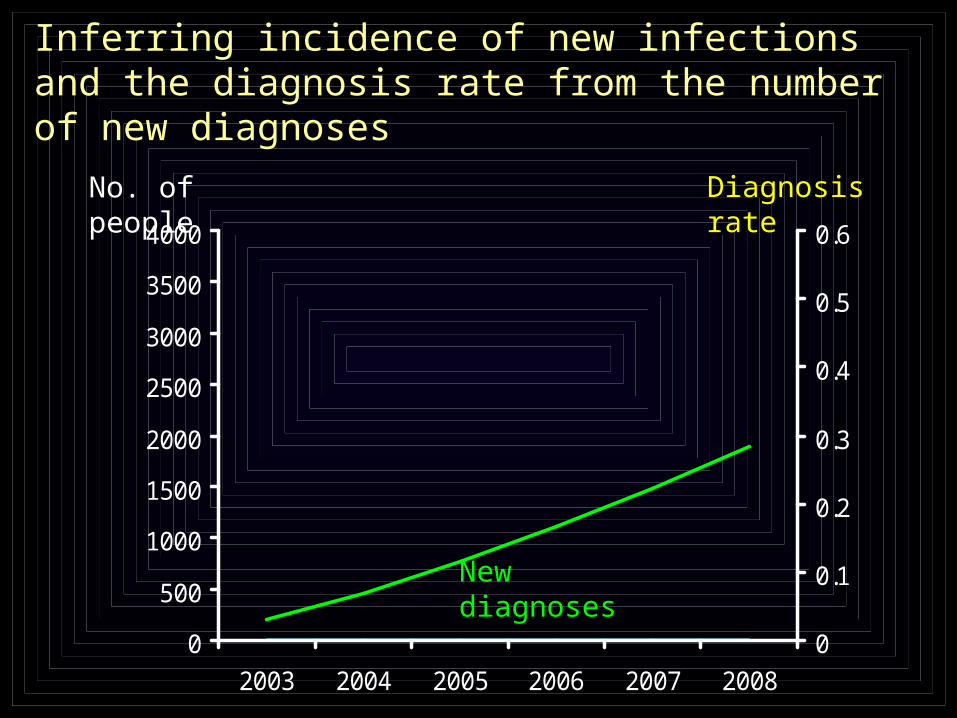
No. of people
New diagnoses
Inferring incidence of new infections and the diagnosis rate from the number of new diagnoses
Diagnosis rate
0
500
1000
1500
2000
2500
3000
3500
4000
2003 2004 2005 2006 2007 2008
0
0.1
0.2
0.3
0.4
0.5
0.6
Diagnosisrate
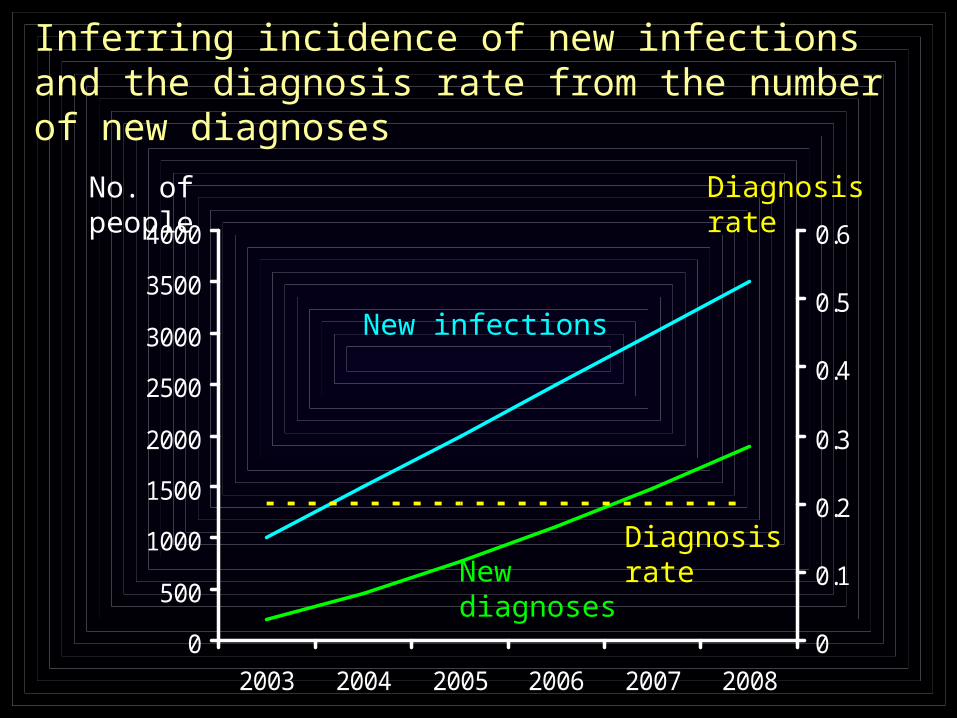
New infections
No. of people
New diagnoses
Inferring incidence of new infections and the diagnosis rate from the number of new diagnoses
Diagnosis rate

0
500
1000
1500
2000
2500
3000
3500
4000
2003 2004 2005 2006 2007 2008
0
0.1
0.2
0.3
0.4
0.5
0.6
Diagnosisrate
New infections
No. of people
New diagnoses
Inferring incidence of new infections and the diagnosis rate from the number of new diagnoses
Diagnosis rate
Approaches based on reported numbers of HIV diagnoses and AIDS cases
Advantages
- Based on routine case reporting data only – does not require prevalence studies
- Can tell us about the predicted time from infection of those undiagnosed

Approaches to estimation of the number of people with undiagnosed HIV infection in a country
- based on prevalence surveys
- based on reported numbers of HIV diagnoses - based on reported simultaneous HIV/AIDS cases

CD4 count Distribution of CD4 count
Incidence of AIDS (/year)
Expected no. of simultaneous HIV/AIDS diagnoses per year
0-49 0.03 1.00 n × 0.03 × 1.00
50-199 0.15 0.20 n × 0.15 × 0.20
200-349 0.22 0.05 n × 0.22 × 0.05
350-499 0.25 0.02 n × 0.25 × 0.02
500-649 0.20 0.015 n × 0.20 × 0.015
650- 0.15 0.008 n × 0.15 × 0.008
Total - 1.00 n × 0.080
n = number of people with undiagnosed HIV
Approach based on reported simultaneous HIV/AIDS cases
Observed number of simultaneous HIV/AIDS diagnoses = n x 0.080
Issues to consider
- Distribution of CD4 count in undiagnosed
- Under-diagnosis and under-reporting of AIDS
Approach based on reported simultaneous HIV/AIDS cases

Advantages
- Uses information on CD4 count at diagnosis
- Particularly well suited to estimating number of undiagnosed people with low CD4 count
See poster: Lodwick et al PE 18.1/5
Approach based on reported simultaneous HIV/AIDS cases
Summary and Conclusions
Countries need to know the number of people living with HIV in various risk groups as a starting point for planning prevention measures and clinical care needs.
This requires estimation of the number with undiagnosed HIV.
At least three different types of approach exist. Each has advantages and disadvantages. Since they use different data they should provide independent estimates. If it is possible to use all approaches this will provide the greatest insight.
Simple guidance is needed for countries on how to use the various approaches.

How to implement ? - Dynamic iterative approach
- produce document on guidance for countries on methods for estimating prevalence of undiagnosed infection, given current state of the field
- through ECDC, try to enourage countries to implement estimation
- this should help to stimulate more complete collection of surveillance data
- this process will be part of an ongoing process of evaluating the relative value of alternative approaches
- the guidance document on methods will evolve to include more extensive data modelling approaches
Acknowledgements
Useful discussions with
Daniela de AngelisPaul BirrellValerie DelpechMatthew LawCaroline SabinJens LundgrenColette SmithAlison RodgerRebecca LodwickGeoff Garnett
Lodwick et al - poster PE 18.1/5, EACS, Cologne