ethical practice under fire: physicians’ role in...
TRANSCRIPT
Ethical Practice Under Fire:Physicians’ Role in War
Disclaimer
The views expressed in this session solely represent the views of the individual
presenters and are not to be construed in any way to represent the views of the U.S. government, the Department of Defense,
or the Department of the Army.
Agenda
• Review of medical & lay press (Jackson)• Personal overview of deployment (Collen)
Breakout into small groups: Cases (All)– Start with charge to groups (Sessums)– Small groups report back to large group
• Case & applicable law (Sessums)• Review of ethical guidance (O’Malley)• Discussion (All)
– How to teach this?

Key Goals• Highlight dilemmas confronted by
physicians in war• Outline ethical principles and laws• Identify available resources• Understand significance

“…U.S. doctors, nurses, and medics…complicit in torture in Iraq, Afghanistan,and Guantanamo Bay”
“There seems to be realtension between the physicians at Guantanamo…and the Army commanders…
“psychologists may…helpdesign coercive interrogation strategies”

The Military Physician
• Where do they come from?– Health Professions Scholarship Program– Uniformed Services University– Service academy grads, ROTC, and direct
accessions• Training
– Residency usually in military facility– Brief officer training & pre-deployment prep

Torture
• Is Common– Sanctioned by 100 governments
• Has long-term health effects for both victims and torturer– PTSD, GAD, Depression
• Doctors inadequately trained in managing victims of torture

Long History of Medical Collusion
• Nazi Germany• Soviet Union• South Africa• Chile• Mexico• Iraq (Hussein era)• Turkey
• Uruguay• Argentina• Indiana• Israel• China• Zimbabwe• Peru• Nigeria
Medical Involvement in Torture
Medieval Age– Torture was considered best evidence– Required medical certificate that subject was not
blind, mute, handicapped, pregnant, insane or ill.– Constitutio Criminalis Carolinia (1532)
• Doctor required to be present at torture• Subspecialist (Torture Physicians)
– Advised type of torture that accused would survive
– Advised when to stop torture to avoid death– Assessed whether unconsciousness was real– Treated bruises and fractures to allow torture to
continue
Examples where Doctors have made a difference
• Torture– Outlawed in Austria in 1787 due to MD– Outlawed by British in Northern Ireland
secondary to protest by police physicians

Medical Ethics• Geneva Convention
– “Medical personnel shall not be compelled to perform or carry out work contrary to the rules of medical ethics”
• American Medical Association– Physicians must oppose and must not
participate in torture for any reason– “Ethical obligations typically exceed legal
duties”

Torture (WMA)
• Deliberate, systematic, or wanton infliction of physical or mental suffering by one or more persons acting alone or on the orders of any authority, to force another person to yield information, to make a confession, or for any other reason
Reported Abuses• Beating• Burning• Asphyxiation• Shackles• Sleep/ light deprivation or
disruption• Continuous light
exposure• Exposure to high/low
temperatures• Exposure to loud noise• Prolonged forced
standing/kneeling• Hooding/blindfolding
• Chaining to the ceiling• Forced nudity• Threats • Mock burials/fake
executions• Withholding food• Withholding medical
attention for war injuries• Denying religious/cultural
needs• Prolonged isolation• Using military dogs• Waterboarding

Reported Medical Abuses
• Provided Medical Clearance
• Monitored Interrogation
• Revived interrogatees• Force fed detainees• Allowed use of
medical records by interrogators
• Helped design interrogations
• Falsified death certificates
• Failed to provide basic health care

Behavioral Science Consultation Teams
• “Biscuits”• Psychiatrist & Psychologist• Used Medical Records to help design
optimum interrogation methods

Geneva DetaineeMedical Requirement
• Access to medical care• Medical records on each detainee• Monthly Health Inspection
Potential Pressures• Provocation
– constant danger– comrades dying
• Stress of war• Prejudice against “others”
– Enemy– Different Values
• Condoned by legitimate authority– ambiguous legal
status– ambiguous illegality
• Higher Good– Prevent escalation– Useful information
• Conforming with Unit Values
• Poor training• Laxity of Command• “Okay” when no pt-client
relationship exists• Fatalism• Few “bad apples”
Recent Letters/Editorial
• Full disclosure of all medical personnel– directly – indirectly by chain of command
• Records and conduct should be reviewed by medical licensing boards in each state
• Appropriate disciplinary action should be taken

Recent Letters/Editorials
• Training should be universal– How to manage victims of Torture– What are the rights/responsibilities of
clinicians?
• Doctors working in prison: human rights and ethical dilemmas
(http://lupin-nma.net/)

Ethical Practice Under Ethical Practice Under FireFire
Introduction and Personal ExperienceIntroduction and Personal ExperienceJacob Jacob CollenCollen MDMDCPT, MC, USACPT, MC, USA
*The views expressed in this presentation are those of the autho*The views expressed in this presentation are those of the author and do not reflect the official policy of the Department of thr and do not reflect the official policy of the Department of the Army, e Army, Department of Defense, or the United States GovernmentDepartment of Defense, or the United States Government
Personal ExperiencePersonal Experience•• Assigned to 1Assigned to 1stst Infantry DivisionInfantry Division
–– Deployed to Samarra, Iraq Deployed to Samarra, Iraq –– 02/09/2004 02/09/2004 –– 02/15/200502/15/2005–– Duties Duties –– Oversaw two Battalion Aid StationsOversaw two Battalion Aid Stations
•• Sole Physician for 1000 US SoldiersSole Physician for 1000 US Soldiers•• high volume of complex trauma high volume of complex trauma •• busy sickbusy sick--call rostercall roster
–– Oversaw Brigade Detention FacilityOversaw Brigade Detention Facility

Echelons of Medical Care
*Battalion Aid Station (Physician and/or Physicians Assistant)
*Combat Lifesaver/Medic“Self-Buddy Aid”
*Combat Support Hospital (Surgical Support, i.e. “MASH”)
*Landstuhl Army Regional Medical Center (Germany)
*Walter Reed or Brooke Army Medical Center(United States)
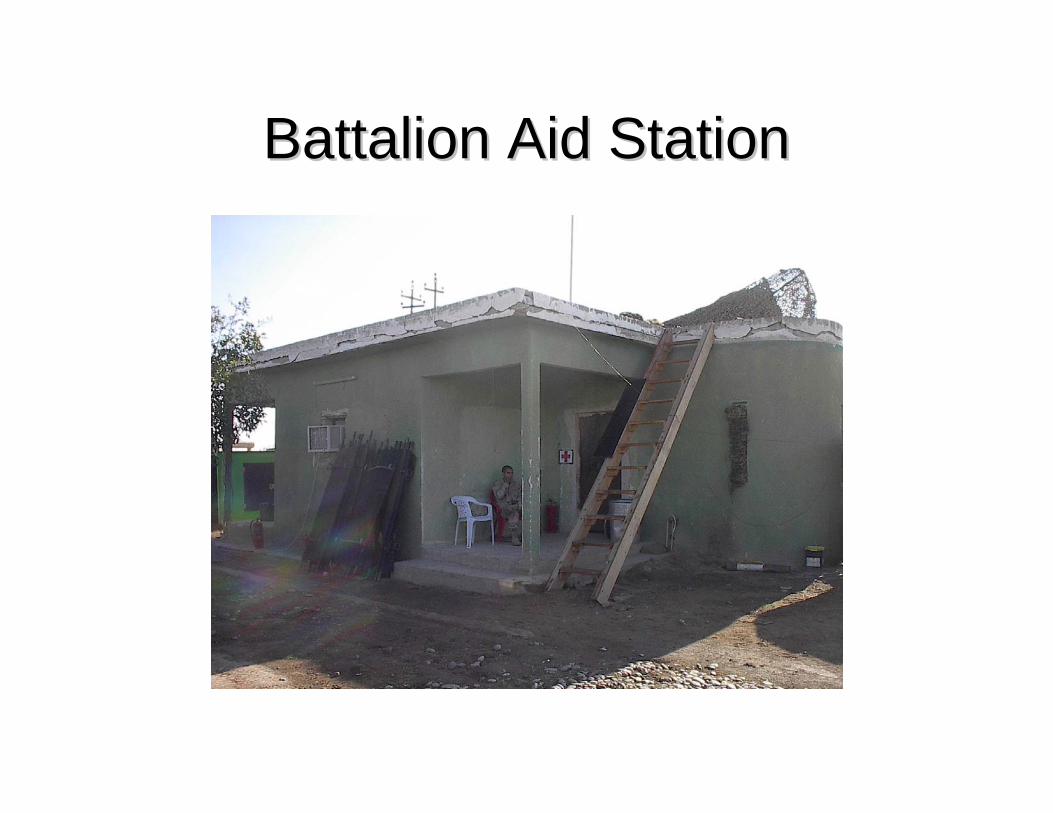
Battalion Aid StationBattalion Aid Station
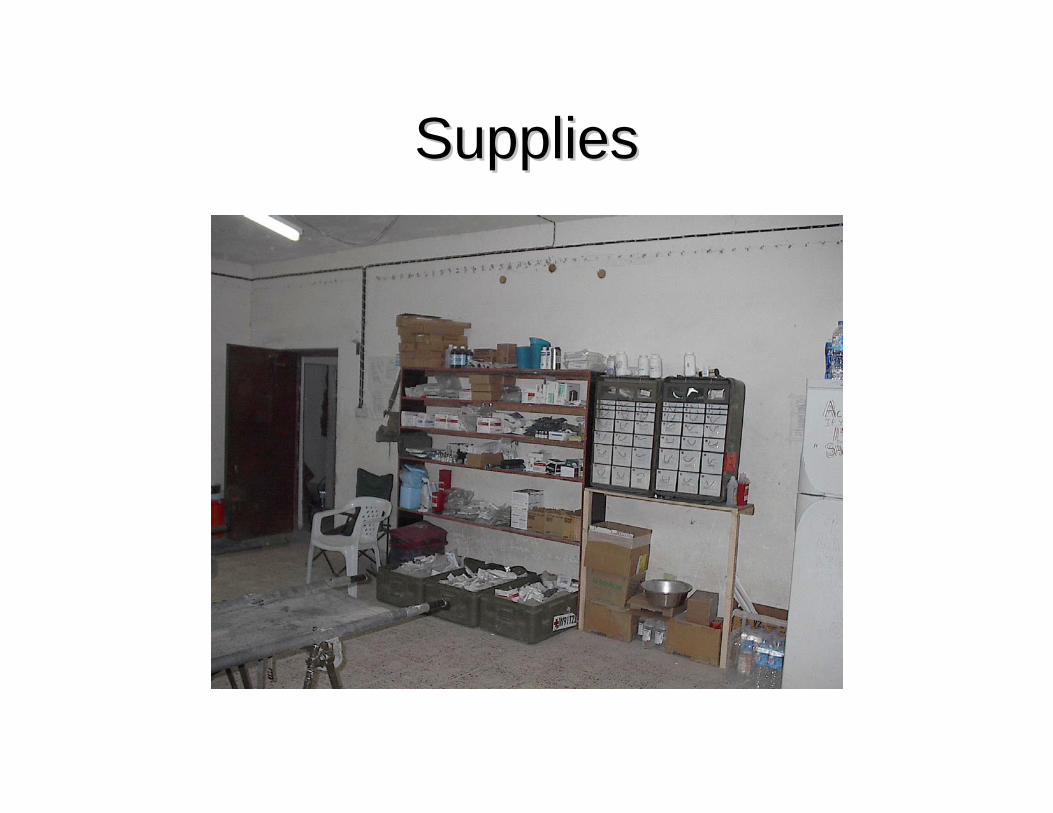
SuppliesSupplies

Triage/Treatment AreaTriage/Treatment Area
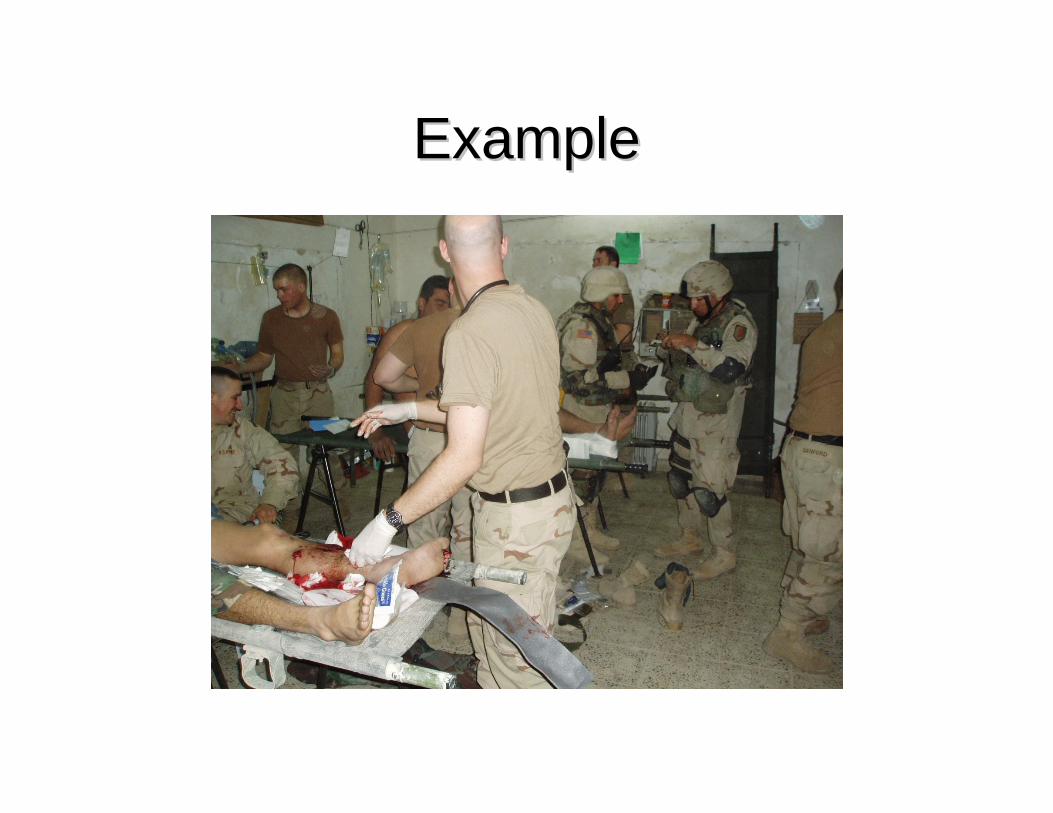
ExampleExample
ExpectationsExpectations•• Battalion Surgeon:Battalion Surgeon:
–– Battalion Staff OfficerBattalion Staff Officer–– Physician for all soldiers in the BattalionPhysician for all soldiers in the Battalion–– Oversee medical care of Detainees and Local Oversee medical care of Detainees and Local
NationalsNationals–– Oversee medical care of Iraqi ArmyOversee medical care of Iraqi Army–– Preventive MedicinePreventive Medicine–– Civil AffairsCivil Affairs
MedicalProfession
MilitaryProfession
Ethical Issues FacedEthical Issues Faced
What is the proper balance?

Tale of Two WorldsTale of Two Worlds
•• Infantry Battalion PreparationInfantry Battalion Preparation–– Advance notice on deployment dateAdvance notice on deployment date–– Advance PlanningAdvance Planning
•• Order suppliesOrder supplies•• attend briefings with downrange counterparts attend briefings with downrange counterparts
–– Field Training ExercisesField Training Exercises•• Vary from a few weeks to two months in field Vary from a few weeks to two months in field •• Practice with equipmentPractice with equipment
–– WeaponsWeapons–– Vehicles Vehicles –– Communications systemsCommunications systems

Physician PreparationPhysician Preparation
•• Frequently little advance noticeFrequently little advance notice•• Not formally trained in what they will Not formally trained in what they will
encounter encounter •• Usually have not worked with their unitUsually have not worked with their unit•• Few resources to facilitate field trainingFew resources to facilitate field training•• May be seen as an May be seen as an ““outsideroutsider””

Ethical Dilemmas FacedEthical Dilemmas Faced
•• Two dead insurgents are dropped off at the Aid Two dead insurgents are dropped off at the Aid StationStation–– Cuffed and no evidence of medical Cuffed and no evidence of medical
interventionsinterventions•• Corruption in Civil Affairs missionCorruption in Civil Affairs mission
–– Grant money likely funneled to insurgencyGrant money likely funneled to insurgency•• Medical Care for informationMedical Care for information
–– BombBomb--makermaker’’s whereabouts for treatment of a s whereabouts for treatment of a neck abscessneck abscess

Lessons LearnedLessons Learned1.1. Effective communication criticalEffective communication critical2.2. Work to build battalion trust Work to build battalion trust 3.3. CommandCommand’’s perspective: s perspective:
•• Preserve the health of the US soldiersPreserve the health of the US soldiers4.4. Not a command priority:Not a command priority:
•• Detainees, Iraqis, Civil AffairsDetainees, Iraqis, Civil Affairs

Who Do You Report To?
• “Go up the military chain of command”

Chain of Command
Squad9-10 soldiers
Sergeant
Platoon4-6 squads (40-60 soldiers)
Lieutenant/ NCO (Sergeant)
Company3-5 platoons (60-190 soldiers)
Captain/ First Sergeant
Battalion4-6 Companies (300-1000 soldiers)
Lt COL/ CSM
Brigade2-5 Battalions (3-5000 soldiers)
COL/ NCO (Sergeant)
Division3 Brigades (15000 soldiers)
Maj Gen/ CSM
Battalion Surgeon
Brigade Surgeon
Division Surgeon
ConclusionConclusion•• Was a rewarding and unique experienceWas a rewarding and unique experience•• Ethical conflicts are often subtleEthical conflicts are often subtle
–– Occur in a stressful environmentOccur in a stressful environment–– Occur in realOccur in real--timetime–– Frequently unrecognized until afterwardsFrequently unrecognized until afterwards–– Rarely criminalRarely criminal
•• Constant balancing actConstant balancing act

Ethical Practice Under Fire:
The Law of War
Laura L. Sessums, JD, MDWalter Reed Army Medical Center


You triage the most severe who might surviveUS soldiers and Iraqi civilians are woundedYou begin to treat an Iraqi civilian firstYou are a military surgeon, overwhelmed
Us versus Them
Your superior officer says:– “Leave those civilians alone; there are dying
soldiers all around you. I’ll court martial you if you touch a wounded civilian.”
What do you do?

Good news and Bad news
• Legal precepts exist to guide your actions– Even in the most difficult circumstances– Sometimes with straightforward answers
• You may have to stand up to superior officers
• Clear answers do not mean easy action

What I’m going to tell you
• Physician’s role in war– Solely to carry out a humanitarian mission– This special mission brings special protection – Actions outside of this special mission put the
special protection at risk• Care of the wounded and sick
– Protected and entitled to care if under DoD control– Regardless of their categorization
• This mission may conflict with that of a physician’s unit
The Law Can Provide Answers
• Hierarchy of legal guidance*:
1. Geneva Conventions2. U.S. Code3. Dept of Defense Instruction4. Dept of Defense Directive5. Army Regulation6. Army Field Manual or Pamphlet
* In descending order of priority
Where to find the Law• Geneva Conventions • Detainee Treatment Act of 2005
– Public Law 109-163, Sections 1401-06
• U.S. Code Title 18, Part I – Chapter 113C, Section 2340
• Instruction on DoD Medical Program Support for Detainee Ops – No. 2310.08E, 6 Jun 2006
• Directive on DoD Detainee Program – No. 2310.01E, 5 Sept 2006
• Army Field Manual 27-10: The Law of Land Warfare– 18 Jul 1956, as changed 15 Jul 1976

Lawful or unlawful order?
• If superior officer’s order is lawful– You must obey it
• If it is unlawful and you obey it– You may be committing a breach of the
Geneva Conventions– You could be court-martialed

1st: In War, what is your mission?
No!!No!!
A physicianA physician’’s role is humanitarian*s role is humanitarian*
*Geneva Convention; The Law of Land Warfare, p. 28.*Geneva Convention; The Law of Land Warfare, p. 28.
To care for the wounded and the sick. To care for the wounded and the sick. This mission gives physicians and medical units in war special pThis mission gives physicians and medical units in war special protection from harmrotection from harmChaplains are the only other group given these protections.Chaplains are the only other group given these protections.
To “conserve the fighting strength”, right?
2nd: In War, who are your patients?
• U.S. soldiers in preference to any wounded civilians or detainees under DoDcontrol?
• No!!!• The wounded and sick must be collected
and cared for.*• Detainees are entitled to adequate
medical care.*** Common Article 3 to the Geneva Conventions**DoD Instruction No. 2310.08E

3rd: Who to Treat First?• Between 2 persons both within your mission to
treat:– The only basis on which to treat one in preference to
another is “urgent medical reasons.”*
• The wounded must in all circumstances be treated humanely without any adverse distinction founded on race, color, religion or faith, sex, birth or wealth, or any other similar criteria.*
*The Law of Land Warfare FM 27-10, pp 84-85.

Back to the CaseClear answers → Difficult action
• Completely in accordance with the law of war.
• Difficult for your superior officer: your mission differs from his.
• Act on your best medical judgment • Attempt to explain that you care for all the
wounded
Lessons Learned
• Understand your mission and responsibilities– Early on in deployment process– Review this often– Anticipate questions under emergency
circumstances• Educate others in your unit
– Commander, other key personnel– About your role as a physician
• Know where to go to learn more and for help
Ethical GuidanceWhile Under Fire
Hippocrates, AMA, ACP, Military
Disclaimer: Not to be construed as the official views of the Dept of Army or the DoD

Sources of Ethical Guidance
• Hippocratic oath
• AMA (Code of Medical Ethics)
• ACP (Ethics Manual)
• Military medical leadership
HIPPOCRATES
Hippocratic Oath
• Loyalty to the profession– Practice with uprightness and honor
• Hold oneself aloof from wrong• Practice solely for “cure” of patients• Confidentiality• If faithful, good repute; if not, the opposite
AMA

American Medical Association
• Code of Medical Ethics (2003)– 1847, 1903, 1912, 1947, 1994, 2001
• Basis: Social contract with humanity
AMA (2001)Principles of Medical Ethics
I. Competent care w/ compassion and respect for human dignity and rights
II. Uphold professionalism-- Be honest-- Report deficient physicians
III. Respect rights, and safeguard confidences
VIII. Regard responsibility to the patient as paramount
Preamble: Responsibility to patients first and foremost; to society, to other health professionals, and to self
Special Circumstances - AMA
• Filming patients – Must consent• Life Sustaining treatment
– Relieve pain/suffering; Pt preference prevails• Torture – Must oppose• Capital punishment – Cannot participate

Other topical areas
• Confidentiality• Industry-employed• Management
positions• Medical Directors• Neglect of patient• Termination of Phys-
Patient relationship
• Reporting Impaired, incompetent, unethical colleagues
• Caring for the poor• Medical testimony• Patient-Physician
relationship
ACP

American College of Physicians (2005)Ethics Manual
• Obligations of Physicians to Society– Parallels obligations to patients– Should merit respect of the community
• Violation of human rights– Harmful consequences for the individual and
the community
ACP Ethics Manual 2005
Relation of Physician to Government
• Speak out against torture/abuses• Must not be instrument to weaken the
physical/mental health of a human being• Prisoner Care – Advocate for:
– Timely treatment– Independent judgment about appropriate care
ACP Ethics Manual 2005

Military Medical LeadershipMedical Command (MEDCOM)

Dual Agency
• Military Medical Professional: – Concurrent obligation to two clients– Two solemn commitments (“sacred oaths”)– Which one trumps the other if conflicted?

The Military Professional
Is bound to do the following:
1. Defend the Constitution • Against all enemies (foreign and domestic)
2. Obey every lawful order3. Place the mission first4. Take care of those under command5. Refuse to obey any unlawful order
The Medical ProfessionalIs bound to do the following:
1. Act in the patient’s best interest2. Patient’s needs come first3. Personhood and autonomy of the patient4. Avoid unnecessary harm to the patient.5. Distribute care and resources justly.

The Army Values
• Loyalty• Duty• Respect• Selfless Service• Honor• Integrity• Personal Courage

The Army Values
• Loyalty• Duty• Respect• Selfless Service• Honor• Integrity• Personal Courage

Integrity for the Army Physician
• Be true to both professions• Your obligations to one may trump the other
Conclusions
• Unique dual professional roles– Military and Medical
• War brings out potential conflicts• There are resources to serve as guidance
– Hippocrates, MEDCOM, AMA, ACP• Personal Integrity is final guide
– Periodic self-reflection is warranted• Systematic preparation pre-deployment?