ethiopian es 3619:2012
TRANSCRIPT
0
Secretariat
ICS:
Descriptors: Reference number:
Price based on pages DES:
ETHIOPIAN STANDARD
Specialty Center - Requirements
ES 3619:2012
First edition

Tables of ContentsACKNOWLEDGEMENT...................................................................................................... 3FOREWORD ......................................................................................................................... 4SECTION ONE: GENERAL.................................................................................................. 6
1. Scope........................................................................................................................... 62. Normative References.................................................................................................. 63. Terminologies and Definitions..................................................................................... 6
SECTION TWO: LICENSURE.............................................................................................. 92.1. General .................................................................................................................... 92.2. Application for Licensure......................................................................................... 92.3. Initial/ New Licensure ........................................................................................... 112.4. Requirements for License Renewal ........................................................................ 122.5. Removal Permits, Change of Operation and Forfeiture of License.......................... 132.6. Suspension and Revocation of a License ................................................................ 142.7. Right to Fair Hearing.............................................................................................. 162.8. Information to be disclosed .................................................................................... 16
SECTION THREE: GOVERNANCE................................................................................... 173.1. Organization and Management ............................................................................... 173.2. Chief Executive Officer (CEO) .............................................................................. 173.3. Chief Clinical Officer............................................................................................. 183.4. Management Committee ........................................................................................ 18
SECTION FOUR: PATIENT RIGHTS AND RESPONSIBILITIES .................................... 204.1. Informed Consent................................................................................................... 204.2. Patient Rights......................................................................................................... 214.3. Patient Responsibilities .......................................................................................... 24
SECTION FIVE: HUMAN RESOURCE MANAGEMENT................................................. 265.1. General Requirements ............................................................................................ 265.2. Staffing Plan .......................................................................................................... 275.3. Job Description and Orientations............................................................................ 275.4. Continuing staff Education..................................................................................... 285.5. Medical Staff.......................................................................................................... 295.6. Employee’s Health ................................................................................................. 295.7. Dress Code and Identification Badge...................................................................... 30
SECTION SIX: CROSS-CUTTING SERVICES.................................................................. 316.1. General .................................................................................................................. 316.2. Outpatient Medical Services................................................................................... 316.3. Emergency Services ............................................................................................... 346.4. Inpatient services.................................................................................................... 376.5. Nursing Services .................................................................................................... 396.6. Anesthesia Services................................................................................................ 436.7. Intensive Care (IC) Services................................................................................... 526.8. Radiological Services ............................................................................................. 576.9. Medical Laboratory Services .................................................................................. 606.10. Pharmacy Services.............................................................................................. 666.11. Medical Recording ............................................................................................. 816.12. Rehabilitation Services ....................................................................................... 85
6.13. Ambulance Service standards ............................................................................. 876.14. Health Promotion Services.................................................................................. 906.15. Morgue Services................................................................................................. 916.16. Infection Prevention............................................................................................ 936.17. Sanitation and Waste Management ..................................................................... 996.18. Food and Dietary Services ................................................................................ 1046.19. Housekeeping, Laundry and Maintenance Services........................................... 1116.20. Part-Time Health Services ................................................................................ 118
SECTION SEVEN: SPECIALTY SERVICE STANDARDS ............................................. 1197.1. Maternal & Child Health (MCH) Center .............................................................. 1197.2. Internal Medicine Center ...................................................................................... 1277.3. Surgery Center ..................................................................................................... 1327.4. Pediatric Center.................................................................................................... 1507.5. Orthopedic Center ................................................................................................ 1577.6. Cardiac Center ..................................................................................................... 1757.7. Oncology center ................................................................................................... 1897.8. Neurology Center................................................................................................. 1977.9. Gastroenterology Center....................................................................................... 2037.10. Renal Center..................................................................................................... 208
SECTION EIGHT: PHYSICAL FACILITY STANDARDS............................................... 2168.1. General ................................................................................................................ 2168.2. Site Selection Requirements ................................................................................. 2188.3. Construction Requirements .................................................................................. 2188.4. Building Space and Elements ............................................................................... 2198.5. Building Systems ................................................................................................. 2228.6. Electrical System.................................................................................................. 2238.7. Fire Protection System ......................................................................................... 2248.8. Call Systems ........................................................................................................ 2258.9. Medical Gas System............................................................................................. 2258.10. Health Facility Environment ............................................................................. 2258.11. Specific Service Areas ...................................................................................... 2258.12. Care and Treatment Areas................................................................................. 2278.13. Ancillary areas.................................................................................................. 227
ACKNOWLEDGEMENT
Ethiopian Standard Agency, ESA would like to extend its special thanks to members of
the technical working group organized by the Ethiopian Food, Medicine and Healthcare
Administration and Control Authority of Ethiopia, EFMHACA in developing the draft
health facility standards.The members of the TWG were Dr. Getahun Mengistu,
Dr.Kidane Melles, Ato Yohannes Jorge, Dr Adefris Debalke, Dr. Wondwossen Fantaye, Dr
Faris Hussein, Dr Petros Mitiku, Dr David A.conteh, Dr Ruth Lawson, Dr Birna Abdosh,
Ato Liyusew Solomon, Ato Edmealem Ejigu, Dr Solomon Tessema, Dr Endale Tefera, Ato
Yihalem Tamiru, Dr Abyou Kiflie, Ato K/mariam G/Michael, Sr Yeshialem Bekele, Ato
Wondie Alemu, W/t Raey Yohannes, Ato Ayalew Adinew, Dr Zegeye Hailemariam, Dr.
Tassew Tadesse, Dr Alem Michael, Dr. Aynalem Abraha, Dr. Mehrtu W/yes, Ato Zelalem
mesele, Ato Salehunae, Dr Daniel Admassie and Dr Tekle-ab Zaid.
In addition, the Agency would also thank all the workshop participants from the Ministry
of Health, Health Professional Associations, Universities, public and private hospitals,
private clinics, non-governmental organizations and other governmental organizations
for their commitment to enrich the draft document.
We are grateful to the USAID/PHSP-Ethiopia, MSH/SPS, Clinton Foundation and Tulane
University without whose support it would have been difficult to achieve the desired
result.
The Agency would also like to express its appreciation to FMHACA for the commitment,
effective coordination and overall leadership shown in the development of this standard.
FOREWORD
This Ethiopia Standard has been prepared under the direction of the Technical
Committee for Medical Care Practices (TC90) and published by the Ethiopian Standards
Agency (ESA).
The draft document (Working Draft, WD) has been submitted to the Secretariat by the
Ethiopian Food, Medicine & Healthcare Administration and Control Authority
(FMHACA).
A Specialty center shall provide services in accordance with this standard and shall
comply with the requirements. The standard shall enter into force starting from the day
of approval as Ethiopian Standard. This standard is approved by the convention of ………..
made on…..Application of this standard is MANDATORY with the intention to ensure the
quality and public safety of health services through standardized licensure and
inspection procedures, to promote access to quality health services and encourage
health investment.
The Ethiopian Standard Agency recommends fulfilling all the requirements stipulated
under this document. It has to be noted that the fruition of fulfilling these requirements
will ensure the quality and safety of public health services through availing appropriate
infrastructure, deployment and retention of qualified and competent health
professionals that deliver best practices and by generating innovative ideas and
methodologies to solve healthcare problems.
Finally, acknowledgement is made to the EFMHACA, Technical Working Group,
participants of national workshop and EFMHACA collaborators for their commitment
and unreserved contribution to the effort of developing Ethiopian Standards for Health
Facilities.
Ato………………W/O…………Director General, Ethiopian Standard Agency

SECTION ONE: GENERAL
1. Scope
1.1. This Ethiopian standard shall be applicable for all specialty centers new and
existing, governmental and non-governmental.
1.2. The standard covers the minimum requirements with respect to practices,
premises, professionals and products or materials put into use for specialty
centers.
1.3. Requirements of a specialty center are stipulated under section two to eight of
this standard.
2. Normative References
The latest editions of the following laws, regulations, directives and guidelines shall be
taken as part and parcel of this Ethiopian Standard.
2.1. Ethiopian Food, medicine and Healthcare Administration and Control
Proclamation No. 661/2009
2.2. Ethiopian Food, Medicine and Healthcare Administration and Control Regulation
No. 189/2010
2.3. Health Policy of Ethiopia
2.4. Drug Policy of Ethiopia
2.5. Commercial Code of Ethiopia
2.6. Criminal Code of Ethiopia
2.7. Medicines Waste Management and Disposal Directive No 2/2011
2.8. Ethiopian National Guideline for Health Waste Management, 2008
2.9. Ethiopian Building Proclamation, No. 624/2009
3. Terminologies and Definitions
3.1Appropriate Organ

Shall mean a state government organ authorized to implement food, medicine and
healthcare administration and control activities at a state level;
3.2
Authority
Shall mean the Ethiopian Food, Medicine and Healthcare Administration and Control
Authority.
3.3
Proclamation
Shall mean the Ethiopian Food, Medicine and Healthcare Administration and Control
proclamation No 661/2009.
3.4
Appropriate Law
Shall mean a law issued by a state to implement regulatory activities regarding food,
medicine and healthcare.
3.5
Person
Shall mean any physical or juridical person
3.6
Authorized Person
Shall mean any specialty center staff who is responsible for a given service
3.7
Specialty Center
Shall mean a health facility which lies in secondary or tertiary level of health care system
and provides a minimum of curative, preventive and promotion services in ambulatory
& inpatient basis as stipulated in this standard. Depending on the type of service(s), the
Specialty center shall have varying number of beds with a minimum of 10 beds for
inpatient services per specialty. The center shall have 24 hour emergency service in its
respective specialty.
3.8
Cross-Cutting Services Standards
Shall mean those standards for services which shall be rendered in all types of the
specialty centers except those services exempted under the specific specialty service
standards.
3.9
Specialty Services standards
Shall mean those standards which are specific/ peculiar to the types of the center as
described in the standard.
SECTION TWO: LICENSURE
2.1. General2.1.1 This standard provides minimum requirements for the establishment and maintenance
of specialty center in order to protect the public interest by promoting the health,
welfare, and safety of individuals.
2.1.2 No specialty center shall be built or be functional by any person without prior
permission of the appropriate organ.
2.1.3 The requirements set by this standard may not be waived unless otherwise for public
interest and there is a substantial need for waiver. There shall be an assurance that the
waiver will not create a hazard to the health and well- being of patients or others than
the public interest.
2.1.4 All health professionals shall respect & abide with the code of professional practice of
their respective profession.
2.1.5 Any information or complaint regarding this standard may be presented to the
Authority or any appropriate organ.
2.1.6 In the absence of the licensee or his /her equivalent the center shall not deliver those
services stated by the license.
2.1.7 Specialty centers shall provide services in accordance with this standard. These health
facilities shall not provide specialty services except those services stated on the license.
2.1.8 Specific public health program related services/interventions may be delivered in the
center upon approval if supported with additional trainings.
2.2. Application for Licensure2.2.1. No person shall operate a Specialty center in Ethiopia, whether governmental,
nongovernmental or private, without being licensed as required by appropriate law and this standard.
2.2.2. Any person desiring to operate a Specialty center shall: a) Complete the application form which shall contain information stated
under article 2.2.6;b) Pay the prescribed license fee; andc) Provide any information or document stated on the application form
2.2.3. A person desiring to operate a Specialty center shall consult the appropriate organ on the plant design conformity with this standard before starting newconstruction, renovation or expansion work. In case of using rental building, the applicant is responsible to make sure that the premise is in accordance with these regulatory standards before entering into any commitment.
2.2.4. An application for the initial licensure of specialty center shall be submitted to the appropriate organ no later than ninety (90) days prior to the stated date of operation. The license fee shall accompany the application.
2.2.5. The first pre-licensing inspection shall be conducted by the appropriate organ upon application without service fee. In case of failure to comply with this standard during the first pre-licensing inspection, the applicant has the right to reapply not more than two times upon paying service fee. If the applicant fails to comply with this standard for the third time, its application for licensure shall be suspended for three months.
2.2.6. The application for a Specialty center license shall state the following: a) Identification of the applicant/owner (name, citizen, address) and
evidence for ownership (if the applicant is an authorized delegate, writtendelegation letter shall be submitted);
b) Previous owner and license number for existing specialty center; c) Name and location of the specialty center;d) Surrounding area of the specialty centere) Types of services to be rendered (specialty and cross-cutting services);f) Responsible person for each service in the specialty center;g) Name, qualification, nationality and license copy of licensee;h) Staffing (Number, type, qualification, work experience & original release
and license copy of all health professionals); i) Number and type of administrative staff;j) Organizational structure;k) Name of CEO/Manager and person in charge in absence of the
CEO/Manager;l) Type of ownership: (Governmental, non- governmental, private for profit,
private for non- profit, other governmental);m) Physical facility design and its description; n) Total number of inpatient beds; o) Proposed use of idle space; p) Owner of the building; (if rental, the agreement paper shall be submitted);q) And other requirements which shall be made in close consultation with
the stakeholders and according to the rules and regulations of the region and the country as well.
2.2.7. All applicants shall demonstrate that they have the capacity to operate a Specialty center in accordance with this standard.
2.2.8. An application for a license or change in service shall be denied if the applicant cannot demonstrate that the premises, products, personnel and health care services are fit and adequate in accordance with this standard.
2.2.9. The appropriate organ shall consider an applicant's prior history in operating a health care facility either in all the regional states of the country in making licensure decision. Any evidence of licensure violations representing serious risk of harm to patients shall be considered by the appropriate organ, as well as any record of criminal convictions representing a risk of harm to the safety or welfare of patients.
2.2.10. A license issued by the appropriate organ shall not be applicable for use by any other person or at any facility other than the designated one in the license. Whenever, there is change in licensee or premises, the license shall be updated.
2.2.11. A license issued to a specialty center in a specified address can’t be used for another facility.
2.2.12. In addition, a specialty center may have a license to provide two or more specialty services in one premise (site). In such scenario, the center shall abide with all the requirements of the specialty center stipulated under section seven of this document.
2.3. Initial/ New Licensure2.3.1. Every specialty center shall have a separate license. The appropriate organ shall
issue each license in the name of the owner and chief clinical officer only for the premises and person named as applicant in the application and the license shall not be valid for use by any other person or at any place other than the designated in the license.
2.3.2. A Specialty center license shall specify the following: (a) The name, and professional license and registration number of the licensee;(b) The name and address of the Specialty center; (c) Ownership of the Specialty center;(d) Name of the owner,(e) License number, issuance and expiration dates of the license. (f) Signature and stamp of the appropriate organ and(g) Notices/reminders prepared by the appropriate organ
2.3.3. Prior to initial licensure of the specialty center, the appropriate organ shallconduct an on-site inspection to determine compliance with the applicable laws and standards governing the specialty centers.
2.3.4. The appropriate organ shall give a written report of the findings to the Specialty center upon the conclusion of the inspection.
2.3.5. A specialty center with deficiencies shall correct them and submit written proof of correction of deficiencies.
2.3.6. The appropriate organ shall conduct a follow-up inspection to determine correction of deficiencies cited within ten (10) days following the one hundred and eighty (180) day correction period or upon notification from the specialty center that the deficiencies have been corrected.
2.3.7. The appropriate organ shall deny the application for licensure to a Specialty center that has not corrected deficiencies. The applicant shall reapply for licensure when deficiencies are corrected.
2.3.8. The appropriate organ shall conduct an unannounced on-site inspection of the Specialty center shortly after the beginning of operation to assess the specialty center's continued compliance with the laws and standards governing Specialty centers.
2.3.9. The original license shall be posted in a conspicuous place at reception at all times.
2.3.10. The appropriate organ shall issue a replacement license where the originally issued license has been confirmed as lost or destroyed upon submission of an application supported by an affidavit.
2.4. Requirements for License Renewal2.4.1. A license, unless suspended or revoked or under consideration in pending case,
shall be renewable annually and the specialty center shall submit an application for license renewal to the appropriate organ no later than sixty (60) days before the expiration date of the current license.
2.4.2. Without prejudice to article 2.4.1;(a) Subsequent to submitting renewal application, the owner shall pay the
prescribed license fee
(b) License renewal shall be made during the first quarter of each fiscal
year (Hamle 1 to Nehassie 30) based on routine inspection findings
over the year
(c) In case of failure to renew license within the prescribed period, license
may be renewed upon paying penalty (50% of renewal fee) within one
month
(d) In case of failure to renew license as per article 2.4.2 (c), license shall be
considered as cancelled
2.4.3. Every applicant who needs to renew a license shall
(a) Apply to the appropriate organ filling the form prescribed by the appropriate organ ;
(b) Pay the prescribed license renewal fee; (c) Provide copies of professional licenses for all permanent and temporarily
employed health professionals of the center and(d) Provide additional information or document upon written request by the
appropriate organ.2.4.4. The appropriate organ may conduct background checks on the applicant or
licensee to determine its suitability or capability to operate or to continue operating a health care facility. Background checks shall consist of, but not be limited to, the following:
(a) Verification of licensure status; (b) Verification of educational credentials; (c) Verification of residency status; (d) Verification of solvency and (e) Contacts with federal and State government officials to determine
outstanding warrants, complaints, criminal convictions, and records of malpractice actions.
2.4.5. The appropriate organ shall renew a license for a Specialty center in substantial compliance with the applicable laws and this standard.
2.4.6. When the licensee can not avail himself for a period not more than 30 days for any reason, he/she shall assign an equivalent specialist temporarily but with prior notification to the appropriate organ. If the licensee is going to be absent for more than the stated period, he/she shall replace the license
2.5. Removal Permits, Change of Operation and Forfeiture of License2.5.1. No Specialty center or part thereof shall move from the premises for which a
license has been issued to any other premises without first having obtained a permit to move from the appropriate organ to the premises not covered by the license issued to the Specialty center.
2.5.2. Without the prejudice to article 2.5.1, permit in change of address shall indicate the special conditions governing the moving of the specialty center or part of it as the appropriate organ may find to be in the interest of the public health.
2.5.3. Without prior approval of the appropriate organ, change of licensee shall not be made.
2.5.4. The center shall notify the appropriate organ whenever there is change of owner.2.5.5. The licensee shall inform the appropriate organ any change in operation. Change
of operation means any alteration of services that is substantially different from that reported on the Specialty center's most recent license application.
2.5.6. Any transfer as to person or place without the approval of the appropriate organ shall cause the immediate forfeiture of the license. That is the license shall not be assignable or transferable and shall be immediately void if the Specialty centerceases to operate, if its ownership changes, or if it is relocated to a different site.
2.5.7. When change of ownership of a Specialty center is contemplated, the Specialty center shall notify the appropriate organ in writing and give the name and address of the proposed new owner.
2.5.8. When change of licensee of a Specialty center is contemplated, the Specialty center shall notify the appropriate organ in writing and give the name and address of the proposed new owner.
2.6. Suspension and Revocation of a License 2.6.1. The appropriate organ may suspend or revoke a license or order closure of a
service or unit within the Specialty center, cease admissions to a Specialty center, order removal of patients from a Specialty center where it finds that there has been a substantial failure to comply with this standard.
2.6.2. Without prejudice to grounds of suspension provided under relevant laws, the appropriate organ shall suspend the license for 3 to 12 months in any of the following grounds:
(a) Where the specialty center is legally suspended;
(b) Where the specialty center fails to practice medical ethics;
(c) Where the specialty center engages in rendering services which are outside the
competence of the center for which the license is obtained;
(d) Where the specialty center fails to allow inspection pursuant to the law and this
standard;
(e) When the specialty center allows a practitioner who has been suspended
by appropriate organ from practicing his profession;
(f) Members of the Governing Board or the Chief Executive Officer or other key
staff member are convicted of a serious offence involving the management or
operation of a specialty center, or which is directly related to the integrity of
the facility or the public health or safety;
(g) When the specialty center fails to implement or fulfill comments and
corrections given by the appropriate organ;
(h) When the specialty center shown any act which constitutes a threat to the
public health or safety;
(i) When the specialty center fails to observe laws relating to health services and
this standard;
(j) When the specialty center fails to submit relevant information required under
this standard.
2.6.3. Without prejudice to grounds of revocation provided under relevant laws, the appropriate organ shall revoke the specialty center license from one to two years on any of the following grounds:
(a) Where the license is proved to have been obtained by submitting false
information;
(b) Allows a practitioner who is not licensed pursuant to the appropriate law or
who has been revoked by appropriate organ from practicing his profession;
(c) Where any of its permanent health personnel is found registered/ employed
as a permanent staff in any other facility;
(d) Where the faults referred to in Article 2.6.2 have been committed for the
second time;
(e) Where the license is found transferred or rented to another person;
(f) Where the specialty center changes types of services, name, address and the
licensee without obtaining permission from the appropriate organ;
(g) Where the license is not renewed in accordance with Section 2.4 of this
standard;
(h) Where the specialty center is legally closed or ceases operation;
(i) Where the specialty center is found operating while suspended by appropriate
organ;
(j) Where the specialty center is found operating out of the scope of services
stated under this standard;
2.6.4. At least 30 days prior to voluntary surrender of its license where approved by the appropriate organ, or order of revocation, refusal to renew, or suspension of license, the specialty center must notify each patient and the patient's physician the intended closure.
2.6.5. Each license in the licensee's possession shall be the property of the appropriate organ and shall be returned to the appropriate organ immediately upon any of the following events:
(a) Suspension or revocation of the license;
(b) Refusal to renew the license;
(c) Forfeiture of a license; or
(d) Voluntary discontinuance of the operation by the licensee.
2.6.6. If the appropriate organ determines that operational or safety deficiencies exist, it may require that all admissions to the specialty center cease. This may be done simultaneously with, or in lieu of, action to revoke license and/or impose a fine. The appropriate organ shall notify to the centers in writing of such determination.
2.6.7. The appropriate organ shall order and ensure in collaboration with appropriate local health authorities the immediate removal of patients from the specialty center whenever it determines there is imminent danger to the patients’ health or safety.
2.6.8. The license shall be returned to the appropriate organ within five (5) working days from voluntary surrender, order of revocation, expiration, or suspension of license.
2.6.9. The appropriate organ shall issue to the specialty center a written notification on reasons for denial, suspension or revocation of the license.
2.7. Right to Fair Hearing 2.7.1. Any applicant made subject to action by the appropriate organ for denial or
suspension or revocation of license or who is assessed a fine under terms of this section shall have the right to a fair hearing in accordance with relevant laws.
2.7.2. Fair hearing shall be provided/ arranged by the appropriate organ whenever there is an official compliant submitted to this body and it shall be open for media.
2.8. Information to be disclosed2.8.1. Evidence based information received by the appropriate organ through inspection and
other true sources about the specialty center shall be disclosed to the public in such a
way to indicate the public a decision maker or self regulator for its own health.
2.8.2. Whenever public disclosure is necessary, the appropriate organ shall forward
inspection reports to the specialty center at least 15 days prior to public disclosure.
2.8.3. Any citizen has the right to obtain information on the official profile of services of any
licensed specialty center from the appropriate organ.
2.8.4. Anyone who is interested in establishing a specialty center shall have the right to be
provided with information concerning the standards required by the appropriate organ
at any working day.
SECTION THREE: GOVERNANCE
3.1. Organization and Management3.1.1. The Specialty center shall have organizational structure with written roles and
responsibilities of each unit.3.1.2. Unless provided by other relevant laws, the Specialty Center shall have Chief
Executive Officer, Chief Clinical Officer, Management Committee and other necessary staffs required by this standard.
3.1.3. The Center shall develop and implement a complaint procedure for patients, families, visitors, and others. The procedure shall include, at least, a system for receiving complaints, a specified response time, assurance that complaints are referred appropriately for review, development of resolutions, and follow-up action.
3.2. Chief Executive Officer (CEO)3.2.1. The manager of the specialty center formed as Charities and business
organization shall be deemed as CEO. 3.2.2. The CEO which can be the owner shall be responsible for planning, organizing,
and directing and controlling the day to day operation of the specialty centers. In case of Charities and Share Company, the CEO shall report and be directly responsible to the Board in all matters related to the maintenance, operation, and management of the center.
3.2.3. The CEO shall be responsible for the operation of the center twenty-four (24) hours per day, seven (7) days per week.
3.2.4. Without prejudice to powers and duties provided in relevant laws, the CEO shall be responsible for:
(a) Leading the development and implementation of policies and guidelines to
be used in the Center;
(b) Maintaining the Center’s compliance with all applicable laws, standards,
its policies, procedures and plans of correction;
(c) Ensuring the patients’ health, safety, and well- being;
(d) Maintaining staff appropriate to meet patient needs;
(e) Developing and implementing procedures on collecting and reporting
information on abuse, neglect and exploitation;
(f) Ensuring that investigations of suspected abuse, neglect or exploitation
are completed and appropriate steps are taken to protect patients;
(g) Ensuring appropriate response to reports from the Authority;
(h) Notifying the appropriate organ in writing where the CCO leaves for a
period not more than thirty (30) days with the equivalent substitute he
assign for that period. In case of emergency, notification shall be made
immediately.
3.3. Chief Clinical Officer 3.3.1. The Chief Clinical Officer, CCO, in whose name the license for the Specialty
Center is issued, shall be responsible for the overall management of the Specialty Center including the administration of its technical affairs.
3.3.2. The CCO shall have the following duties and responsibilities:(a) Ensure systems are in place for maintaining the quality of all services, care
and treatment provided to patients (b) Designating and defining duties and responsibilities of
department/service heads for the clinical service(c) Establish a means for effective communication and coordination among
the Center clinical and other staffs(d) Recommending the appointments to the clinical staff and scope of clinical
privileges;(e) Ensure smooth working relations exists with the appropriate regulatory
organ
3.3.3. If the CCO is not the owner of the Center, or in circumstance where the law provides for accountability of the CCO to other higher position in the organizational structure, the owner or that person shall respect the professional autonomy and independence of the CCO in accordance with this standard.
3.3.4. In case of poly specialty centers, the CCO may be chosen from one of the specialists licensed to work in the center as permanent employees.
3.4. Management Committee3.4.1. Department/ Service head shall be assigned to each of the clinical and
administrative departments. The responsibility of department/ service heads includes at least the following:
(a) Providing a written description of the services provided by the
department/service,

(b) Ensuring coordination and integration of these services with other
departments/services when relevant,
(c) Recommending space, staffing, and other resources needed to fulfill the
department’s responsibility,
(d) Defining, in coordination with the CCO, the education, skills, and education
needed by each category of employee in the department/ services,
(e) Ensuring that there is an orientation and continuing education program
for the department’s/ service’s employees,
(f) Developing and implementing a department quality improvement
program.
3.4.2. Any Specialty Center shall establish a Management Committee consisting of heads of the clinical and administrative departments/ services. The CEO shall be the chairperson of the Committee.
3.4.3. The Committee shall be an adviser of the CEO on the day to day management of the Center. In particular, the Committee shall, at least once in a quarter, review the medical care provided and the utilization of the Center resources.
3.4.4. The Committee shall meet upon regular basis. The minutes of the meeting shall be recorded and available to the appropriate organ upon request.
SECTION FOUR: PATIENT RIGHTS AND RESPONSIBILITIES
4.1. Informed Consent 4.1.1. Each Specialty center shall protect and promote every patient’s rights. This includes
the establishment and implementation of written policies and procedures for the patient right.
4.1.2. For undertaking any type of procedures and treatments an informed consent shall be required from the patient or patient’s next of kin or guardian.
4.1.3. An informed consent may not be required during emergency cases or life threatening situations where the patient is not capable of giving an informed consent and his or her next of kin or guardian is not available.
4.1.4. Unless provided by the law or this standard or by the Specialty center policies and procedures that an informed consent shall be given in written form, an informed consent of the patient can be given orally or inferred from an act. A written consent shall be needed at least for the following:
(a) Surgery and invasive procedures;(b) General anesthesia; (c) Blood transfusion; and(d) Blood or genetic testing in stigmatizing diseases.
4.1.5. The specialty center shall comply with relevant laws, national and international codes of ethics in the cases of vulnerable groups like children, women, geriatric patients etc when someone other than the patient can give consent.
4.1.6. Patient consent forms shall be available in all applicable locations like areas where surgery or invasive procedures are done or general anesthesia is used or chemotherapy is administered.
4.1.7. No photographic, audio, video or other similar identifiable recording is made of without prior informed consent of a patient.
4.1.8. A Specialty center shall establish and implement a process to provide patients and/or their designee an appropriate education to assist in understanding the identified condition and the necessary care and treatment.
4.1.9. A Specialty center shall document its assessment of every patient's ability to understand the scope and nature of the diagnosis and treatment needed.
4.1.10. A specialty center shall post list of fees & service charges for clients in a visible place.
4.2. Patient Rights Every Specialty center patient shall at least have the following rights,
4.2.1. To receive reasonable, respectful and safe access to health services by competent personnel that the Specialty center is required to provide according to this standard;
4.2.2. To receive treatment and medical services without discrimination based on race, age, color, religion, ethnicity, national or social origin, sex, sexual preferences, handicap, diagnosis, source of payment or other status;
4.2.3. To retain and exercise to the fullest extent possible all the constitutional and legal rights to which the patient is entitled by law;
4.2.4. To be informed of the names and functions of all medical practitioners and/or other clinical practitioners who are providing direct care to the patient. These people shall identify themselves by introduction or by wearing a name tag;
4.2.5. To receive an explanation of his or her complete medical condition from the patient's medical practitioner(s) or other clinical practitioner(s), recommended treatment, risk(s) of the treatment, expected results and reasonable medical alternatives in terms that the patient understands. If this information shall be detrimental to the patient's health, or if the patient is not capable of understanding the information, the explanation shall be provided to his or her next of kin or guardian and be documented in the patient's personal medical record;
4.2.6. To give informed, written consent prior to the start of specified nonemergency procedures or treatments only after a general medical practitioner or other clinical practitioner has explained specific details about the recommended procedure or treatment, the risks involved, the possible duration of incapacitation, and any reasonable medical alternatives for care and treatment in terms that the patient understands. If the patient is incapable of giving informed, written consent, consent shall be sought from the patient's next of kin or guardian or through an advance directive, to the extent authorized by law. If the patient does not give written consent, a general medical practitioner or other clinical practitioner shall enter an explanation in the patient's medical record;
4.2.7. To refuse medication and treatment and to be informed of the medical consequences of refusing treatment except conditions which are threatening to the general public health
4.2.8. To be informed if the specialty center has authorized other health care and educational institutions to participate in the patient's treatment. The patient also shall have a right to know the identity and function of these institutions, and may refuse to allow their participation in the patient's treatment;
4.2.9. To be informed by the attending medical practitioner and/or other clinical practitioner about any continuing health care requirements after the patient's discharge from the specialty center. The patient shall also have the right toreceive assistance from the general medical practitioner and/or other appropriate Specialty center staff in arranging for required follow-up care after discharge;
4.2.10. To be informed by the specialty center about any discharge appeal process to which the patient is entitled by law;
4.2.11. To be transferred to another facility only for one of the following reasons, with the reason recorded in the patient's medical record: a) The transferring specialty center is unable to provide the type or level of
medical care appropriate for the patient's needs. The Specialty center shall make an immediate effort to notify the patient's primary care general medical practitioner or other clinical practitioner and the next of kin, and document that the notifications were received; or
b) The transfer is requested by the patient, or by the patient's next of kin or guardian when the patient is mentally incapacitated or incompetent;
4.2.12. To receive from a medical practitioner or other clinical practitioner an explanation of the reasons for transferring the patient to another facility, information about alternatives to the transfer, verification of acceptance from the receiving facility, and assurance that the movement associated with the transfer will not subject the patient to substantial, unnecessary risk of deterioration of his or her medical condition. This explanation of the transfer shall be given in advance to the patient, and/or to the patient's next of kin or guardian except in a life-threatening situation where immediate transfer is necessary;
4.2.13. To be treated with courtesy, consideration, and respect for the patient's dignity and individuality i.e. the right to care that respects the patient’s personal values and beliefs;
4.2.14. To be free from physical and mental abuse, neglect, sexual harassment, sexual violence and exploitation;
4.2.15. To be free from chemical and physical restraints that are not medically necessary, unless they are authorized by attending physician or other clinical practitioner for a limited period of time to protect the patient or others from injury;
4.2.16. To have personal and physical privacy during medical treatment and personal hygiene functions, such as bathing and using the toilet, unless the patient needs assistance for his or her own safety. The patient's privacy shall also be respected during other health care procedures and when Specialty centerpersonnel are discussing the patient;
4.2.17. To get confidential treatment. Information in the patient's records shall not be released to anyone outside the specialty center except the followings;(a) If the patient has approved the request, (b) If another health care facility to which the patient was transferred
requires the information, (c) If the release of the information is required and permitted by law. (d) If the patient's identity is masked, the specialty center may release data
about the patient for studies containing aggregated statistics4.2.18. To know the price of services and procedures;4.2.19. To receive a copy of the payment rates of the specialty center, regardless of
source of payment. Upon request, the patient or responsible party shall be provided with an itemized bill and an explanation of the charges if there are further questions. The patient or responsible party has a right to appeal the charges. The Specialty center shall provide the patient or responsible party an explanation of procedures to follow in making such an appeal;
4.2.20. To have prompt access to the information contained in the patient's medical record, as per the medical record section stated under this standard, unless a treating physician or other clinical practitioner prohibits such access as detrimental to the patient's health, and explains the reason in the medical record. In that instance, the patient's next of kin or guardian shall have a right to see the record. This right continues after the patient is discharged from the Specialty center for as long as a copy of the record is kept;
4.2.21. To obtain a copy of the patient's medical record, as per the standards set under the medical record section of this standard.
4.2.22. To have access to individual storage space in the patient's room for the patient's private use. If the patient is unable to assume responsibility for his or her personal items, there shall be a system in place to safeguard the patient's personal property until the patient or next of kin is able to assume responsibility for these items;
4.2.23. To receive a medical certificate in English or Amharic or in a working language of the place where the specialty center is located;
4.2.24. To present his or her suggestion or grievances, without fear of retribution, to the specialty center staff member designated by the Specialty center to respond to questions or grievances about patient rights and to receive an answer to those grievances within a reasonable period of time without discrimination. The Specialty center shall post the names, addresses, and telephone numbers of the government agencies to which the patient can complain and ask questions.
4.2.25. To be given a summary of these patient rights, as approved by the appropriate organ, and any additional policies and procedures established by the Specialty
center involving patient rights and responsibilities. The Specialty center shall be obliged to ensure that,
(a) The patient is informed of his or her rights during the admission process;(b) This summary include the name and phone number of the Specialty center
or Specialty center staff member to whom patients can complain about possible patient rights violations;
(c) A summary of these patient rights is posted conspicuously in the patient's room and in public places throughout the Specialty center;
(d) Complete summary copies of the patient right is available at nurse stations and other patient care registration areas in the Specialty center.
4.2.26. To be informed and participate in decisions relating to their care and participates in the development and implementation of a plan of care and any changes.
4.2.27. To choose their treating physician or nurse or any other health professional if (a) there is conflict among the patient and these staff or (b) the patient has justifiable reason or (c) the center has another alternative.
4.3. Patient Responsibilities 4.3.1. The list of a patient’s responsibilities shall be posted at various places of the
specialty center premises in local languages. 4.3.2. Every patient shall have the following responsibilities:
(a) To provide, to the best of the patient’s knowledge, accurate and complete information regarding past medical history and issues related to the patient’s health, including unexpected changes, to the health professional responsible for the patient’s care;
(b) To follow the course of treatment and instructions proposed by the medical practitioner or other clinical practitioner or to accept the consequences if treatment instructions is refused;
(c) To report any changes in his/her condition or anything that appears unsafe to herself/himself or to the responsible health personnels or others;
(d) To be considerate of the rights of other patients and to respect their privacy;
(e) When his/ her condition risks the public or when in epidemic situation, the patient has the responsibility to cooperate for the control measures.
(f) To respect their caregivers; (g) To fulfill the financial obligations as promptly as possible;
(h) To keep all appointments and notify Specialty center or the appropriate person when unable to do so;
(i) To observe the specialty center policies and procedures, including those on smoking, alcohol or drug use, cellular phones, noise and visitors;
(j) Be considerate of the specialty center facilities and equipment and to use them in such a manner so as not to abuse them;
(k) Not to litter the specialty center premises; (l) To sign on “against medical advice Notice” if he/she refuses the
recommended treatment or intervention.(m) Cooperate with the clinic staff on the clinic’s policies and procedures.
SECTION FIVE: HUMAN RESOURCE MANAGEMENT
5.1. General Requirements 5.1.1 The specialty center shall have a responsible person who organizes /carries
out the major functions of Human Resource Management (HRM).5.1.2 The specialty center shall make sure each service unit shall maintain the
minimum number of staff with the qualifications, training and skills during working hours as per this standard. In addition the inpatient and emergency services of the Specialty center shall be staffed twenty-four (24) hours a day and 365 days a year.
5.1.3 The specialty center shall ensure that all health professionals recruited are licensed as per the registration and licensing requirement of the appropriate organ.
5.1.4 The specialty center shall ensure and maintain evidence of current active licensure, registration, certification or other credentials for employees and contract staff prior to letting to work and shall have procedures for verifying that the current status is maintained.
5.1.5 Whenever a licensed health-care professional is terminated as a result of a job-related incident, the specialty center shall refer a report of the incident to the appropriate organ.
5.1.6 Each person who is involved in the performance of duties involving direct patient care shall have an occupational health screening prior to entering active status and once every five (5) years thereafter. A health professional shall not conduct health examination for himself/ herself.
5.1.7 Each health screening shall include a medical history, physical examination, and any indicated laboratory work and investigations. A signed medical checkup report shall be made available.
5.1.8 The Specialty center shall keep on file the medical checkup reports of all staffand shall make available during inspection by the appropriate organ.
5.1.9 Each person who is involved in direct patient care and who has been absent from duty because of an illness caused by reportable disease or an illness that may cause a risk to the public shall, prior to returning to duty, obtain certification from a physician or other qualified health professional, as provided for in the specialty center's policies, that he or she may return to duty without apparent danger of transmitting the cause of the illness to any patient.
5.1.10 The specialty center shall regularly follow the Immunization status of all employees and all other persons who routinely come in contact with patients
or patient areas against selected communicable disease. Immunizations shall be in accordance with current guidelines developed by the MOH.
5.1.11 The specialty center shall have documentation of staff credentials, licenses and training certificates.
5.1.12 The Specialty center shall update the employment record for all staff. The record shall contain to a minimum: information on credentials, health examination (fitness for duty), work history, current job description, and evidence of orientation, in-service education / training and copies of annual evaluation.
5.1.13 All health professionals shall abide with health professionals Code of conduct and their respective scope of practice.
5.1.14 The specialty center shall have a policy or procedure for all health professionals to report any suggestive signs of child abuse, substance abuse and /or abnormal psychiatric manifestations by the patients under their care.
5.1.15 The specialty center shall notify the appropriate organ while hiring or terminating medical staff.
5.2. Staffing Plan
5.2.1. The specialty center shall avail as a minimum the staff requirements stated under this standard.
5.2.2. In addition to article 5.2.1, the staffing plan shall define the following elements:
(a) The total number and types of staff needed for the specialty center as a whole and for each service unit,
(b) The total number and types of staff currently available for the specialty center as a whole and each service unit,
(c) The required education, skills, knowledge, and experience required for each position,
(d) The process and time period for reviewing and updating the plan shall be indicated. (The plan is periodically reviewed and updated as required, but it shall be done at least every two years.)
(e) Expected/ existing workload.
5.3. Job Description and Orientations5.3.1. All staffs shall be provided with current written job descriptions and be
oriented to their specific job responsibilities at appointment.
5.3.2. The job description shall include the title and grade of the position, specific function of the job, job requirement, reporting mechanism, evaluation criteria and description of job site and work environment.
5.3.3. The orientation program for all employees shall include three levels of orientation: the facility wise, service wise and job specific.
5.3.4. Organizational and administrative structure of the specialty center shall be posted in a visible place and orientation to all staff working in the Center shall be provided by the Specialty center management.
5.3.5. Orientation to Specialty center policies, including all environmental safety programs, infection control, and quality improvement shall be provided.
5.3.6. Staff members who are not licensed to practice independently shall have their responsibilities defined in their updated job descriptions.
5.3.7. The Specialty center shall organize a system to provide & maintain evidence of an orientation program for all new staff and, as needed, for existing staff who are given new assignments. The orientation program shall include an explanation of:
(a) Job duties and responsibilities,(b) Specialty center's sanitation and infection control programs; (c) Organizational structure within the Specialty center;(d) Patient rights; (e) Patient care policies and procedures relevant to the job; (f) Personnel policies and procedures; (g) Emergency procedures; (h) Reporting requirements for abuse, neglect or exploitation(i) What to record and report.
5.4. Continuing staff Education5.4.1. The center shall ensure and facilitate that its staffs receive training in order to
perform assigned job responsibilities. 5.4.2. The professional in the specialty center shall receive ongoing Continuing
Professional Development (CPD) or continuous medical education (CME) to maintain or advance his or her skills and knowledge.
5.4.3. The CPD/ CME shall be relevant to the setting in which they work as well as to the continuing advancement of the clinic.
5.4.4. The center shall decide the type and level of training for staff in accordance with National CPD guideline and then carry out and document a program for this training and education.
5.4.5. The center shall provide and maintain evidence of CPD or CME for staff. A record shall be maintained including dates, topics, trainers and participants.
5.4.6. The center shall periodically test staff knowledge, skill and attitude through demonstration, mock events and other suitable methods. This testing shall be documented.
5.5. Medical Staff5.5.1. The medical staff shall be responsible to the governing authority for medical
care and treatment provided in the Specialty center as per this standard and shall: a) Participate in a Quality Assurance/ Performance Improvement program to
determine the status of patient care and treatment; b) Abide by Specialty center and medical staff policies; c) Establish a disciplinary process for infraction of the policies
5.5.2. The medical staff shall see that there is adequate documentation of medical events by a review of discharged patients that shall insure that medical records meet the required standards of completeness, clinical pertinence and promptness or completion of following discharge.
5.5.3. The medical staff shall actively participate in the study of nosocomial (facilityassociated) infections and infection potentials and must promote preventive and corrective programs designed to minimize their hazards.
5.5.4. There shall be regular medical staff meetings to review the clinical works & administrative duties.
5.5.5. Each patient shall be under the care of a treating physician, regardless of whether the patient is also under the care of an allied health professionallicensed to practice.
5.6. Employee’s Health 5.6.1. The specialty center shall institute systems and processes that minimize
employees’ risks; protect employees and provide access to care when needed. 5.6.2. A comprehensive Occupational Health and Safety (OHS) program shall have
the following components: a) Staff dedicated to coordinate OHS activities,b) Policies and Procedures that define components of the program,c) Training for staff on program components.
5.6.3. The standards outlined below define the core elements of an OHS program and specify minimum requirements needed to address OHS issues.a) The center shall have an occupational health and safety policy and
procedures in place to identify, assess and address identified health and
safety risks to staff and prevent those risks that will potentially compromise their health and safety.
b) The center assesses and documents safety risks through formalized, structured assessments that are done at regular intervals.
c) Interventions shall be designed and implemented to address the risks that are identified.
5.6.4. The specialty center shall have a mechanism in place to address/ protect injuries that could lead to the transmission of blood-borne diseases (needle stick and other injuries).
5.6.5. The Specialty center shall provide personal protective equipment and ensure access to prophylaxis measures to employees,
5.6.6. The Specialty center shall provide the following facilities to employees:a) Cafeteria ( access to meal for duty),b) Duty room (bed, table and chair, closet with lock),c) Adequate toilet and shower facilities.
5.7. Dress Code and Identification BadgeFor areas involving direct patient contact:
5.7.1. Footwear shall be safe, supportive, clean, and non-noise producing,5.7.2. No open toe shoes shall be worn,5.7.3. Artificial nails are prohibited. Natural nails must be kept short and no jewelry
shall be worn on fingers and wrist,5.7.4. Hair must be worn in a way that prevents contamination and does not present
a safety hazard,5.7.5. Specialty center shall avail uniforms and badges to employees and they shall
wear all the time accordingly while on duty.5.7.6. The dressing shall not interfere in any way in service provision.5.7.7. The specialty center shall specify a particular style and/or color of uniform
with different style/color code; separate for each human resource category, employee and trainees
5.7.8. The employee shall keep the uniform neat, wrinkle free and in good repair,5.7.9. The identification badge shall be worn at all times while at work and be easily
visible with name & profession.
SECTION SIX: CROSS-CUTTING SERVICES
6.1. General 6.1.1. All specialty centers shall have and fulfill all the requirements stated under the
cross cutting services section of this standard. Cross cutting services which are not applicable for a given specialty center are indicated under respective cross cutting service standards.
6.1.2. The range of treatment options and the clinical impression shall be fully described to client and/or their families and/or next of kin and shall be documented accordingly.
6.1.3. Diseases under national surveillance shall be notified to the FMOH through the proper reporting channel.
6.1.4. The center shall avail updated reference materials, treatment guidelines and manuals like National TB and leprosy, pain management, Malaria treatment, ART.
6.1.5. The center shall use standard prescriptions as per pharmacy standards and different request forms for investigation like laboratory and x-ray.
6.1.6. Medicines shall be prescribed with generic names only and dispensing shall be made according to patient choice.
6.1.7. With regard to quality assurance and transparency:(a) The specialty center shall arrange system at outpatient center to collect
feedback from clients, (b) The specialty center shall have formal administrative channel through
which clients lodge their complaints and grievances,6.1.8. The specialty center shall display the following at visible place:
(a) List of Services available in the specialty center during working hours & after working hours,
(b) List of Professionals and specialties working in the center during & after working hours,
(c) Updated list of Various fees and prices,6.1.9. All the requirements of premises, professionals and products required for each
specialty center are specified under each specialty specific services section under this standard. All specialty centers shall comply with respective standards.
6.2. Outpatient Medical Services6.2.1. Practice:6.2.1.1. The Specialty center outpatient service shall provide the following core functions:
a) Care of ambulatory patients with outpatient service,b) Examination and management of preadmission patients,c) Follow up of discharged and ambulatory patients,
d) Pharmacy service,e) Diagnostic services (Laboratory and imaging),
6.2.1.2. The outpatient services shall comply with the standards prescribed under patient rights and responsibilities section of this standard.
6.2.1.3. The outpatient service shall have policies and procedures regarding access andavailability of quality service. It shall include the following:
(a) The outpatient service shall be available for regular working hours,(b) The specialty center may have a system for providing medical services after
regular working hours. In case of this, the type of service and time schedule shall be posted at a visible place to the public,
(c) The outpatient service shall have consultation with functional intra and inter facility referral system which at least include:
Procedure for identifying cases for referral, Procedure for referring patients directly to respective services, List of potential referral sites with contact address (referral
directory), Referral forms and Documentation for referred clients, Referral tracing mechanism (linkage) and Feedback providing
mechanism, Procedure to minimize delay for referral and managing referred
patients6.2.1.4. There shall be medical assessment at outpatient services which includes at least:
(a) Comprehensive medical and social history,(b) Physical examination including at least:
Vital sign (BP, PR, RR, To), weight and pain assessment, Clinical examination pertinent to the illness,
(c) Diagnostics impression,(d) Laboratory and radiographic (roentigenographic) workups when indicated.
6.2.1.5. The outpatient service shall have clinical protocols for management of at least common disease and locally significant diseases in line with the national and/or international guidelines in absence of the national one.
6.2.2. Premises6.2.2.1. The outpatient layout shall include the following:
a) Dedicated entrance
b) Waiting area: room /lobby preferably with public telephone, TV area, drinking
fountain and gender specific toilet
c) Reception and recording area/desk
d) Dedicated patient consultation and examination rooms /cubicles for each
specialty services
e) Room for minor procedures
f) Room for providing injections
g) Store
h) Staff room (for changing cloth)
i) Cleaners room/ closet
6.2.1.1. All outpatient rooms shall have adequate light, water and ventilation
6.2.1.2. Communication system shall be connected with major functional areas
6.2.1.3. The room arrangements of outpatient services shall consider proximity between
related services
6.2.1.4. The outpatient clinical setup shall have easy access to pharmacy, laboratory and
other diagnostic services.
6.2.1.5. The outpatient clinic shall be well marked and easily accessible for disabled
clients, elderly patients, under five children and pregnant mother.
6.2.1.6. The outpatient service shall be located where access for ambulatory patients is
the easiest and where in coming client would not have to pass through other
care service outlets ( in- patient , laboratory etc )
6.2.1.7. The outpatient clinics shall have fire extinguishers placed in visible area.
6.2.2. Professionals
6.2.2.1. At least one specialist shall be available to run the respective specialized
outpatient service.
6.2.2.2. The outpatient service shall have the following professionals:
a) Specialist,b) GP as appropriate,c) Nurses,d) Cleaners,e) Runner,
6.2.2.3. The actual number of personnel shall be determined by workload analysis.
6.2.2.4. The staff shall have regular supportive supervision by senior staff or peer review
or case conferences at least every three months and it shall be documented.
6.2.3. Products
6.2.3.1. The following products shall be available for outpatient service. Products specific
to particular specialty are indicated under the specific discipline.
a) Examination Coachb) Weighing Scalec) Vital Sign and Diagnostic
Set Thermometer Stethoscope Sphygmomanometer Fundoscope Otoscope Pulseoxymeter
Reflex hammer Snellen’s chart
d) Refrigeratore) Dressing Setf) Minor Setg) Catheterization seth) Trolley i) Folding Screen j) X-Ray Film viewer
6.3. Emergency Services6.3.1. Practice6.3.1.1. The specialty center shall provide basic life support to its level of emergency care for
24hrs a day and 365 days a year which shall include but not limited to: a) Airway management and/or oxygen supply,b) Cardiopulmonary resuscitation (CPR),c) Bleeding control, d) Fluid resuscitation (shock management),e) Prevention of further damages.
6.3.1.2. On top of the above article (6.3.1.1), the specialty center shall avail advanced emergency services specific to the specialty.
6.3.1.3. There shall be written protocols for emergency services. 6.3.1.4. The Specialty center shall have protocols for the initial management of at least the
following emergency cases as appropriate:(a) Fever,(b) Shock,(c) Severe Bleeding,(d) Multiple fracture and
injuries, poly trauma,(e) Coma,(f) Burn,(g) Poisoning,(h) Tetanus,(i) Acute diarrhea (Severe
dehydration),
(j) Seizure disorder,(k) Air way obstruction,(l) Cardiac emergencies(m)Cerebrovascular accident(n) Hypertension emergencies(o) Psychiatric emergencies(p) Meningitis (q) Burn(r) Poisoning(s) Acute abdomen
6.3.1.5. Infection prevention standards shall be implemented in the emergency room as per the IP standards stated under this standard.
6.3.1.6. Every life saving emergency service shall be given to patients without any prerequisite and discrimination.
6.3.1.7. If referral is needed, it shall be done after providing initial stabilization and after confirmation of the availability of the required service in the facility where the patient is to be referred to.
35
6.3.1.8. If the patient to be referred needs to be accompanied by a physician or other health professional during the referral process, the Specialty center shall arranging an ambulance and shall assign a health personnel to accompany & assist patient.
6.3.1.9. In conditions of emergency management, all interventions, medications administered and the clinical condition shall be communicated to the patient or available family member following the emergency responses/ resuscitation measures.
6.3.1.10. The emergency service shall promote the dignity and privacy of patients.6.3.1.11. There shall be policy that facilitates support from other services for emergency
service. 6.3.1.12. The specialty center shall assign health professional to look after the emergency
service.6.3.1.13. There shall be a mechanism of quality improvement for the service at least by
collecting feedback from clients and having a formal administrative channel through which clients place their complaints and grievances.
6.3.2. Premises6.3.2.1. The emergency room shall be located in a place where it is easily recognizable to
the public and shall be labeled in bold. 6.3.2.2. The emergency premise shall be low traffic area and there shall be reserve
parking place for ambulances. 6.3.2.3. The corridor to emergency rooms shall be stretcher friendly and spacious
enough.6.3.2.4. The emergency area shall be spacious enough to provide a space for the following tasks:
(a) Triaging,
(b) Accepting, triaging and providing immediate care including emergency procedures.
(c) Admitting for a maximum of 24 hrs to provide emergency care (2 beds).
(d) Emergency medicines, supplies and equipments.
(e) Staff/duty room (shared).
(f) Toilet facilities separate for patients and staff (Male, female).
6.2.3.2. Observation beds shall be arranged as the description of inpatient beds’
arrangement.
6.2.3.3. The size of the door for the emergency room shall not be less than 1.5 meter.
6.2.3.4. The emergency premise shall allow patient dignity and privacy.
6.2.3.5. The rooms shall be arranged in such a way that the first encounter to an emergency
patient coming from outside will be the examination room or space.
6.2.3.6. The emergency room shall have the following facilities:
(a) Adequate water, light and ventilation.

36
(b) Fire extinguishers placed in visible area.
(c) Telephone
(d) Hand washing basin in each room
6.2.3.7. Waiting area for attendants and caregivers.
6.2.4. Professionals
6.2.4.1. The center shall have a specialist or GP available for emergency service.
6.2.4.2. The center shall have a policy for organizing a team for emergency service. The
emergency team for all the shifts shall contain a minimum of:
(a) specialist or GP,
(b) Nurses
(c) Cleaners
(d) Runner
6.2.4.3. After working hours, a specialist shall be available for emergency consultation on call
basis.
6.2.4.4. At least a general practitioner shall be available for emergency services at all times.
6.2.4.5. The actual number of personnel required shall be adjusted based on Workload analysis.
6.2.4.6. The center shall arrange Drill-exercise of emergency case management on regular bases
among the teams assigned in the emergency service.
6.2.5. Products
6.2.5.1. The emergency service shall have readily arranged emergency medicines and supplies
on cupboard or trolley.
6.2.5.2. There shall be at least two coaches at emergency room.
6.2.5.3. The emergency service shall have at least the following products:
(a) Examination coach(b) Stretcher with wheel(c) Wheelchair(d) IV Stand(e) EKG (shared)(f) Suction machine (g) Defibrillator(h) Tracheotomy set (i) NG tube(j) Minor surgical set
(k) Different types of splints(l) Mobile examination light(m)Hot air oven (shared)(n) Oxygen supply: oxygen,
cylinder with flow meter, trolley and nasal prongs
(o) Resuscitation set on trolley(p) Intubation set(q) Ambu bag
37
6.4. Inpatient services 6.4.1. Practice6.4.1.1. The specialty center shall make inpatient service available 24 hrs a day and 365
days a year,6.4.1.2. The specialty center shall have consultation and functional intra and inter facility
referral system.6.4.1.3. The specialty center shall include at least the following service for admitted
patients:a) Taking comprehensive medical and social history, comprehensive physical
examination and performing relevant laboratory & other medical workups upon admission and when indicated,
b) Providing 24 hours nursing care service that complies with the nursing service standard,
c) Detailed daily round/ patient evaluation by the attending physician,d) Referral service to health facilities where the service is available.
6.4.1.4. The specialty center shall have clinical protocols for management of at least common causes of admission,
6.4.1.5. The specialty center shall have a system to make follow up of patients by the same or equivalent physician,
6.4.1.6. The clinical impression, range of treatment options and treatment plans shall be communicated to patients/ clients and/or their families and/or next of kin and documented accordingly.
6.4.1.7. The inpatient service shall have quality improvement mechanisms that at least constitutes of:
a) Collecting Feedbacks from clients,b) Preparing a formal administrative channel through which clients lodge their
complaints and present their grievances,c) Conducting regular medical discussion sessions among health professionals
across all clinical disciplines, 6.4.1.8. The specialty center shall have written protocol for admission and discharge.6.4.1.9. A specialty center shall have at least ten inpatient admission beds. When two or
more specialty centers combined together the number of inpatient beds shall be a minimum of twenty.
6.4.1.10. The specialty center shall provide a clean gowns/ patient pyjamas, clean bed, bed sheet, blanket, bed spread and pillow to admitted patients.
6.4.1.11. The specialty center shall secure the properties of admitted patients in a cabinet or room with shelves.
6.4.1.12. The inpatient service shall have access to pharmacy, laboratory and imaging/diagnostic services as per their respective standards,
38
6.4.1.13. The inpatient service shall arrange the appropriate post discharge instructions and follow up.
6.4.1.14. The Specialty center shall contact the municipality or responsible body for burial service if there is no family/guardian for the deceased.
6.4.2. Premises6.4.2.1. Inpatient service of the specialty center shall have the following rooms:
a) Inpatient rooms, separate for male and female
b) Isolation room(s),c) Nursing Station d) Doctors office (consultation
room)e) Clean utility room
f) Soiled utility roomg) Store h) Toilet with shower for patient
(Male, female) i) Toilet with shower for staff
(Male, female)j) Duty room
6.4.2.2. The arrangement of rooms shall consider proximity between related services.6.4.2.3. The number of beds per room shall not exceed six (6) with the following specification:
a) Distance of bed from fixed walls shall be 0.9 m
b) Distance between beds shall be 1.2 m
c) Adult beds shall have 1m width and 2m length
d) Each bed room shall have alarm
e) The rooms shall have safe and continuous water supply, light and ventilation
6.4.2.4. There shall be washing basins for each room.
6.4.3. Professionals6.4.3.1. Specialist and/ or sub-specialist of related discipline shall be physically available during
working hours at inpatient service unit.6.4.3.2. At least one general medical practitioner shall be physically available in all the shifts in
inpatient service unit.6.4.3.3. One nurse for a maximum of six (6) patients per shift shall be available to provide nursing
care services.6.4.3.4. Support staff such as runner and cleaner shall be available all the time.6.4.3.5. Actual number of professionals shall be determined based on work load analysis.6.4.3.6. Engineer or technician for equipment maintenance and general facility maintenance shall
be available during working hours and shall be also available either on duty or on call basis during non working hours.
6.4.4. Products6.4.4.1. The following products shall be available for inpatient services. Products specific to
specialty services are indicated in respective specialty standards. Beds with wheels Bed side cabinet
39
Bed pans Urinal (Male and Female) Bed Pan carriage Bed pan Racks IV Stand Stretcher Wheel chair Safety Box Suction machine Resuscitation set
Thermometer Stethoscope
Sphygmomanometer Fundoscope Otoscope Reflex hammer Refrigerators Minor operation set Dressing Set Enema Set Lumbar puncture(LP) set Catheterization set Folding screens
X-ray Film Viewer
6.5. Nursing Services6.5.1. Practice6.5.1.1. There shall be written policies describing the responsibilities of nurses for the
nursing process in the specialty center. Such policies shall be reviewed at least once every five years.
6.5.1.2. Written copies of nursing procedure manual shall be made available to the nursing staff. The manual shall be used at least to:
(a) Provide a basis for induction of newly employed nurses,(b) Provide a ready reference on procedures for all nursing personnel,(c) Standardize procedures and practice,(d) Provide a basis for continued professional development in nursing procedures/
techniques.6.5.1.3. The Specialty center shall have established guidelines for verbal and written
communication about patient care.(a) Written communication includes proper use of clinical forms, nursing Kardex,
progress notes, and/or nursing care plan for each patient and discharge instructions.
(b) Verbal and/or written communication: reporting to treating physician(s); nurse-to-nurse reporting; communication with other service units (laboratory, pharmacy, X-Ray, social work service).
6.5.1.4. There shall be a procedure for standardized, safe and proper administration of medications by nurses or designated clinical staff.
6.5.1.5. The nursing care plan shall be initiated upon admission of the patient and shall include discharge plans as part of the long-term care provision goals.
6.5.1.6. The nurses shall assess and document the holistic needs of admitted patients:
40
(a) formulate, implement goal-directed nursing interventions, (b) evaluate the plan of nursing care and (c) Involve patients, their relatives or next of kin in decisions about their nursing
care. 6.5.1.7. Nurses’ documentation shall include:
(a) Medication/ treatment/ other items ordered by authorized attending physician,(b) Nursing care needed,(c) Long-term goals and short-term goals,(d) Patient/ family teaching and instructional programs,(e) The psycho- social needs of the patient,(f) Preventative nursing care.
6.5.1.8. All admitted patients shall be under the supervised care of a licensed nurse at alltimes.
6.5.1.9. Implementation of infection prevention procedures and provision of information on IP practices to patients, clients, family members and other caregivers, as appropriate, shall be done by the nurses;
6.5.1.10. Nursing care shall be provided for all patients equally and without prejudice to age, sex, economic, social, political, ethnicity, religious or other status and irrespective of their personal circumstance.
6.5.1.11. Informed consent shall be sought before carrying out any procedure. 6.5.1.12. Patient discharge instructions shall be documented in the patient's medical
record and verbal instruction shall be given. 6.5.1.13. Allergies shall be listed on the front cover of the patient's chart or highlighted on
the screen in a computerized system. 6.5.1.14. There shall be a mechanism in place to ensure that assistance is provided for
patients who require assistance.6.5.1.15. There shall be a policy or procedures for nurses to report any suggestive signs of
child abuse, substance abuse and/ or abnormal psychiatric manifestations by the patients under their care.
6.5.1.16. There shall be a policy for reporting and documenting medication errors and adverse drug reactions by attending nursing personnel immediately to the prescriber and/or Pharmacist.
6.5.1.17. There shall be a policy or a protocol that state the procedure to be followed for dying patients & dead body care.
6.5.2. Premises6.5.2.1. The specialty center shall have the following premises for nursing services:
(a) Nurse’s station located in the middle of the inpatient room(s) with free access to
all rooms.
(b) Hand washing basin and toilet room at nurse station
41
(c) Procedure room for nursing procedures
(d) Nurse changing room with cabinet, chairs, cupboard
6.5.3. Professional6.5.3.1. Nursing care service at different service delivery areas shall be directed by a
licensed BSC nurse with two years of work experience.6.5.3.2. The center shall have in place a nursing workforce plan that addresses nurse staffing
requirements including, at a minimum:(a) A nurse representative in each patient care unit responsible for the operation of
the professional nursing service 24 hours per day and 365 days a year.
(b) A provision that direct patient care for 24 hours in inpatient unit be provided by
licensed nursing personnel,
(c) A method for assessing each unit’s additional nursing needs for each shift.
6.5.3.3. All nursing staff shall receive orientation, training and/or update at least annually including at least:
(a) Center’s policies and procedures,
(b) Routine nursing procedures,
(c) Emergency procedures and
(d) Infection prevention and control.
6.5.3.4. Professional Quality assurance: On-going internal institutional evaluation of outcome-based quality indicators related to nursing care shall be in place to assess and provide a safe and adequate level of patient care including at least:
(a) Patient injury rate;
(b) Medication process errors;
(c) Maintenance of skin integrity;
(d) Control of cross infections and nosocomial infection rates;
(e) Center -wide patient satisfaction with overall nursing care;
(f) Patient satisfaction with pain management.
6.5.4. Products6.5.4.1. The following products shall be available for nursing care services.
(a) Specimen collection set
(b) Rubber Sheets
(c) Restraining equipment as appropriate
(d) Patient Chart Folders
(e) Vital Sign Equipments
Trolley for vital sign monitoring,
Thermometer, BP apparatus, stethoscope, measuring tape
sphygmomanometer with stethoscope,
wrist watch/ wall clock, bedside weighing scale Pulseoxymetry
(f) Nursing procedure equipments:
Dressing trolley Dressing set, Minor set, Enema set, IV stand, Oxygen trolley, Oxygen cylinder, Oxygen regulator/gauge, Oxygen mask/ nasal catheters, Suction machine:
electrical/pedal, Waste basket,
Safety boxes, Bed screens, Kidney basin, 475ml x 5 Bed pan Urinal Mobile Examination light, Plastic apron, Drapes, Rubber sheets, Connectors, Cushion bags,
(g) Soiled utility room:
Soiled linen trolley
Bin with lid
Worktable with laminated top
Wash tub (65L)
General purpose trolley, two
trays
(h) Furniture and fixtures;
Table Chair, stackable, without
armrests Basket, waste-paper, metal Cabinet
Patient chart holder, Refrigerator, Bedside cabinet, Feeding table,
43
6.6. Anesthesia Services6.6.1. Practices 6.6.1.1. This standard are applicable to the following specialty centers
a) Surgery specialty center,
b) Orthopedics specialty center,
c) Neurology specialty center,
d) Renal specialty center and
e) Other centers which apply general or major anesthesia for surgical interventions.
6.6.1.2. There shall be a written policy about administration of regional and general anesthesia in
the specialty center,
6.6.1.3. Minor regional blocks shall be monitored in accordance with the specialty center’s policy,
6.6.1.4. Anesthesia services shall be administered in accordance with written policies and
procedures that are reviewed at least every three years, and revised more frequently as
needed. They shall include at least the following :
(a) Anesthesia care, which includes moderate and deep sedation, is planned and
documented in the patient’s record.
(b) A pre-anesthesia/sedation assessment shall be done by anesthetist or
anesthesiologist prior to the induction of anesthesia.
(c) The patient shall be reassessed immediately prior to induction of anesthesia by an
anesthesiologist or anesthetist. The plan shall be consistent with the patient
assessment and shall include the anesthesia to be used and the method of
administration.
(d) Prior to administration of any pre-anesthesia medication, a written informed consent
for the use of anesthesia shall be obtained and documented in the medical record.
(e) Each patient’s physiologic status shall be continuously monitored during anesthesia
or sedation administration and the results of the monitoring shall be documented in
the patient’s medical record on an anesthesia form, a minimum of :
Pulse rate and rhythm.
Blood pressure.
Oxygen saturation.
Respiratory rate.
(f) The anesthesia record includes:
Fluids administered.
44
Medications administered.
Blood or blood products administered.
Estimated blood loss.
The actual anesthesia used.
Any unusual events or complications of anesthesia.
The condition of the patient at the conclusion of anesthesia.
The time of start and finish of anesthesia.
Signature of the anesthesiologist/ or anesthetists.
(g) The patient shall be monitored during the post-anesthesia/surgery recovery period
and the results of monitoring shall be documented in the patient’s medical record.
(h) The time of arrival and discharge from anesthesia recovery room shall be recorded.
(i) The observation at recovery room shall be done by qualified registered nurses with
training of basic advanced cardio-pulmonary support.
(j) The decision of discharge shall be done by anesthesiologist, or anesthetist or other
qualified physician based on the documented results of monitoring during the
recovery.
(k) The discharge order from the recovery shall be documented on patients chart and
signed by anesthesiologist or anesthetist or other qualified physician before transfer.
6.6.1.5. At all times, at least one anesthetist shall be on-site or on-call and available to reach the
specialty center within 30 minutes.
6.6.1.6. The anesthetist shall visit the patient before the operation and assess the general medical
fitness of the patient, receives any medication being taken, and assess any specific
anesthesia problems.
6.6.1.7. The anesthetist shall discuss possible plans of management with the patient and explains
any options available, to enable the patient to make an informed choice.
6.6.1.8. Information on any medicines or treatments such as blood transfusion shall be discussed
with the patient.
6.6.1.9. The anesthetist shall ensure that all the necessary equipment and medicines are present
and checked before starting anesthesia.
6.6.1.10. The anesthetist shall confirm the identity of the patient before inducing anesthesia.
6.6.1.11. The anesthetist shall be present in the operating theatre around the patient throughout
the operation and shall be present on-site until the patient has been discharged from the
recovery room.
45
6.6.1.12. The conduct of the anesthesia and operation is monitored and recorded in line with the
monitoring standards and formats, to a minimum these shall contain:
a) A continuous display of the ECG,
b) Continuous pulse oximeter, and
c) A written record of the anesthetic shall be kept as a permanent record in the case
notes.
6.6.1.13. Pain shall be assessed in discussion with surgeon and/ or the patient and pain control
shall be provided.
6.6.1.14. Patients shall be managed in a recovery room, except patients requiring transfer for
intensive care in ICU, until overcome effect of anesthetic.
6.6.1.15. Written discharge criteria shall be in place, including satisfactory control of pain and
nausea, spontaneous breathing, to determine when patients can be safely discharged from
the recovery room, making it clear that the final responsibility is always with the
anaesthetist or any qualified physician for transfer.
6.6.1.16. The protocols and guidelines used for anesthesia service shall be available and well
understood by the surgical team.
6.6.1.17. Anesthetic agents administered with the purpose of creating conscious sedation, deep
sedation, major regional anesthesia, or general anesthesia shall be in accordance with
aneasthesia policies and procedures.
6.6.1.18. There shall be a written protocol to assure that surgery shall not proceed when there are
disabled alarms on the monitors,
6.6.1.19. The body temperature of each patient under general or major regional anesthesia lasting
45 minutes or more shall be continuously monitored and recorded at least every 15
minutes.
6.6.1.20. Pulse oximetry shall be performed continuously during administration of general
anesthesia, regional anesthesia, and conscious sedation at all anesthetizing locations,
unless such monitoring is not clinically feasible for the patient. Any alternative method of
measuring oxygen saturation maybe substituted for pulse oximetry if the method has been
demonstrated to have at least equivalent clinical effectiveness.
6.6.1.21. Blood pressure, pulse rate, and respiratory rates shall be determined and charted at least
every five minutes for all patients receiving anesthesia at any anesthetizing location,
except for local anesthesia and minor regional blocks.
46
6.6.1.22. The general anesthesia service shall be provided in the Operation theatre (OR), together
with the surgical services.
6.6.2. Premises
6.6.2.1. There shall be a mechanism for taking exhaust air from anesthesia machine to outside of
OR; important when performing open system for pediatric anesthesia,
6.6.2.2. There shall be central oxygen system or a system where there is a continuous supply of
charged Oxygen cylinders
6.6.2.3. Regarding the anesthesia store:
(a) It shall be well ventilated and illuminated room with shelves and cabinets,
(b) The anesthetic shall be kept on shelves and/ or cabinets, separate from medicines,
properly labeled,
(c) There shall be at least 4 electric plugs in the room,
(d) Anesthetic equipments shall be stored clean and being ready for use,
(e) Ambu bags and resuscitation kits shall be kept labeled in easily reachable place,
(f) There shall be separate place for keeping new and rechargeable Batteries and dry
cells. Used batteries and cells shall be stored and discarded properly, refer to IP
and waste disposal protocol,
6.6.2.4. Recovery Room shall be sited within the operating suit and has a minimum of:
a) two beds with side protection,
b) resuscitation equipment including a defibrillator on trolley,
c) oxygen source with face mask and or nasal catheter,
d) ensures ease of communication and access for anesthesia department staff for
close follow up,
6.6.3. Professionals
6.6.3.1. This standard allows to licensed Bsc anesthetist with a minimum of two years of
experience to lead anesthesia service for short term until the country delivers adequate
number of anesthesiologists
6.6.3.2. All anesthesia providers who administer and/or supervise the administration of general
anesthesia, major regional anesthesia, or conscious sedation anesthesia shall maintain
current training in Advanced Cardiac Life Support.

47
6.6.3.3. General or major regional anesthesia shall be administered and monitored only by the
following:
a) An anesthesiologist/ Bsc Anesthetist or
b) A registered nurse anesthetist or registered anesthetist or physician resident
(anesthesiology), a student nurse anesthetist, a student anesthetist under the
supervision of an anesthesiologist.
6.6.3.4. The supervision of general or major regional anesthesia shall be provided by a registered
anesthetist or nurse anesthetist or anesthesiologist who is immediately available. The
supervising person may concurrently be responsible for patient care, with the exception of
performing major surgery, administering general anesthesia, or major regional anesthesia.
6.6.3.5. Minor regional blocks shall be administered by the following registered professionals:
a) An Anesthesiologist/Bsc Anesthetist, or
b) A nurse anesthetist, or
c) A physician, podiatrist (foot doctor);
d) A medical intern, a physician resident, , or a student nurse anesthetist, or
student anesthetist, or a health officer, or a registered nurse, midwife, under
the supervision of at least nurse anesthetist.
6.6.4. Products
6.6.4.1. Anesthesia supplies, equipment and safety systems shall include the following:
a) All medical gas hoses and adapters shall be color-coded and labeled according to
current national standards.
b) An oxygen failure-protection device ("fail-safe" system) shall be used on all
anesthesia machines to announce a reduction in oxygen pressure, and, at lower
levels of oxygen pressure, to discontinue other gases when the pressure of supply
oxygen is reduced.
c) Vaporizer exclusion ("interlock") system shall be used to assure that only one
vaporizer, and therefore only a single agent, can be actuated on any anesthesia
machine at one time.
d) To prevent delivery of excess anesthesia during an oxygen flush, no vaporizer shall
be placed in the circuit downstream of the oxygen flush valve.
e) All anesthesia vaporizers shall be pressure-compensated in order to administer a
constant non-pulsatile output.
48
f) Accurate flow meters and controllers shall be used to prevent the delivery to a
patient of an inadequate concentration of oxygen relative to the amount of nitrous
oxide or other medical gas.
g) Alarm systems shall be in place for high (disconnect), low (sub atmospheric), and
minimum ventilator pressures in the breathing circuit for each patient under general
anesthesia.
6.6.4.2. Anesthesia supplies, equipment and patient monitoring shall include:
a) A respirometer (volumeter) measuring exhaled tidal volume shall be used whenever
the breathing circuit of a patient under general anesthesia allows.
b) A difficult airway container or trolley shall be immediately available in each
anesthesia department for handling emergencies. The following items are required
to be included in the difficult airway container or trolley:
resuscitation equipment like ambu bag, laryngoscope, defibrillator, laryngeal
mask and endotracheal tube stylet
Airway,
emergency medicines,
a laryngeal mask,
endo-tracheal tube stylet,
airway, and/or
other items of similar technical capability.
c) A precordial stethoscope or oesophageal stethoscope shall be used when indicated
on each patient receiving anesthesia. If necessary, the stethoscope may be positioned
on the posterior chest wall or tracheal area.
d) Supplemental oxygen and a delivery system appropriate to the patient's condition
shall be immediately available for patient transport from the operating room to the
post anesthesia care /recovery unit.
e) Recording and reporting forms
6.6.4.3. Equipments:
a) Time clock
b) Anesthesia machine with ventilator, 2 vaporizers, and gas cylinders
c) Adult and pediatric anesthesia circuits with filters
d) Mechanical ventilators
e) Oxygen cylinders, oxygen trolley and oxygen regulator
49
f) Worktable with laminated top
g) Resuscitation equipments; Ambu bags (adult/ pediatric/ neonates), with inflatable
bag,
h) Refrigerator,
i) Stools
j) Clips
k) Weight scale; adult & pediatric
l) Resuscitation trolley
m) Syringe pump
n) Defibrillator
o) Blood gas analyzer
p) Dust bin
q) Blankets
r) Air conditioner and heater
s) Framed boards with pencil trays
t) IV stands, infusion pumps, IV fluid pressure bags, blood warmer and IV fluid
warmer
u) Tourniquets, tongue depressors, disposable
v) Operation table with minimum of smoothly adjustable 3 sections and accessories;
Pillows, abduction
Support, head, operating table
Positioner bag, small, medium and large
Adjustable Head screen
Patient transferring Stretchers
Suction machines
w) Goggles and boots
x) Patient monitor
ECG monitor
12 leads Electrode, Monitor
Pulse oximeter
Temperature monitor
Nerve stimulator
50
Dual head stethoscope
BP apparatus with different size cuffs
y) Intubation gadgets:
Airway Guedel, pediatric & adult size
Laryngeal mask set
Mask holder
Cannula - Nasal-Oxygen,
Masks – Oxygen 40 %
Laryngoscope sets with different size blades (Mackintosh)
Magill forceps (adult & pediatrics)
Intubation stylet, adult, 15 Ch,/ Endo-tracheal tube guide
Mouth gauge
Guedel airways: size 0, 00, 3, 4 & 5
Tube, Endo-tracheal:
o disp. + connector, 3 mm, w/o balloon
o disp. + connector, 3.5 mm, w/o balloon
o disp. + connector, 4 mm, w/o balloon
o disp. + connector, 4.5 mm, w/o balloon
o disp. + connector, 5 mm, balloon
o disp. + connector, 5.5 mm, balloon
o disp. + connector, 6 mm, balloon
o disp. + connector, 6.5 mm, balloon
o disp. + connector, 7 mm, balloon
o disp. + connector, 7.5 mm, balloon
o disp. + connector, 8 mm, balloon
o disp. + connector, neonate mm, w.o balloon
o disp. + connector, balloon, 6.5mm, 7mm, 7.5mm, 8mm
Tube:
o Trachea, balloon, int.can, ster, size 6
o Trachea, balloon, int.can, ster, size 8
o Suction,CH08,L50cm, ster,disp, CH08, CH10, CH14, CH16
Extractor, mucus,20ml,ster,disp
51
Safety Pins Large & Medium
Connectors:
o Biconical, Autoclavable
o Connector, T/Y
o Connectors - Plastic – Tapered
Masks - Nebulizer/Oxygen
Other accessories/ suppleis:
Braun Splints (Arm)
Draw sheet, plastic,90x180cm
Clinical thermometer
Fridge thermometer
Tourniquet, latex rubber, 75cm
6.6.4.4. All medicines and supplies shall be available as per the national medicines list for this level
of health facility
6.6.4.5. Operating Room Linen:
a) Apron Surgical, rubber
b) Trousers, Surgical, woven; Small, Medium & Large
c) Top(shirts), Surgical, woven; Small, Medium & Large
d) Gown, Surgical, woven(Plain)
e) Caps, Surgical, woven
f) Masks, surgical, woven
g) Pillow case
h) Pillows
i) Sheet, Bed
j) Sheet, draw, white
k) Cellular Blanket
l) Organ protections,
m) Shelves
n) cabinets
52
6.7. Intensive Care (IC) Services
6.7.1. Practices
6.7.1.1. This service standard shall be applicable to the following specialty centers
a) Surgery specialty center,
b) Neurology specialty center,
c) Renal specialty center,
d) Cardiac specialty center and
e) other specialty centers (as appropriate )
6.7.1.2. The ICU is open 24 hours and 7 days a week with available medical personnel with
Advanced Life Support (ALS) training available round the clock with shift.
6.7.1.3. The ICU shall have written policies and procedures that are reviewed at least once every 3
years and implemented. They shall include at least:
(a) Criteria for admission to ICU,
(b) Criteria for discharge and transfer;
(c) A list of procedures that registered physicians, who are certified/ accredited in
intensive care, may or may not perform;
(d) Protocols for transfer and transport of patients within the specialty center or from
the center to another facility including who shall accompany the patient being
transferred or transported;
(e) Infection control procedures and/or protocols as indicated under infection
prevention standards;
(f) A visitors policy that specifies visiting hours and number which subject to the
discretion of the patient's physician or primary care nurse;
(g) A policy on the removal of a patient's life support system;
(h) A policy defining the physician, specialist and consulting physician to be called for
patient emergencies, including a response time for physicians to respond to patient
emergencies;
(i) Standing orders for patient emergencies;
(j) Policies and procedures which ensure that priority laboratory services will be
available to critical care patients at all times if medically indicated;
53
6.7.1.4. Roles and responsibilities of specialists in management of ICU patients shall be available in
written policy or protocol. All ICU patients shall be managed or co-managed by a dedicated
trained internist or independent practitioner who is exclusively responsible for patients in
one ICU.
6.7.1.5. Nursing functions shall be the responsibility of a licensed nurse and shall be accountable
to the attending ICU physician,
6.7.1.6. Complete medical records shall be kept for each patient: pertinent history, physical
examination, diagnosis, diagnostic procedures, medication administration, and treatment
to facilitate continuity of care. And the patient’s medical service record shall be integrated
with the patient's over-all specialty center’s record,
6.7.1.7. A ratio of 2 patients to 1 nurse shall be available at a general ICU.
6.7.1.8. There shall be a means of promoting harmony between critical care providers and
families. This 5-part system, known by the mnemonic VALUE, includes:
(a) valuing and appreciating what the family members communicate,
(b) acknowledging their emotions by using reflective summary systems,
(c) listening to family members,
(d) understanding who the patient is as a person by asking open-ended questions and
listening carefully to the responses, and
(e) Eliciting questions from the family more effectively than by simply asking “Any
question?’’.
6.7.1.9. There shall be portable life-support equipment for use in patient transport, both within
the center and for transfer. All ventilators in use shall be equipped with an integral
minimum ventilation pressure (disconnect) alarm. There shall be a system for obtaining
immediate emergency replacement or repair of equipment in the critical care service.
6.7.1.10. There shall be a system in the specialty center of assuring the functionality of the ICU
gadgets/ equipments at least every 3 years and labeling for the check service.
6.7.1.11. There shall be a mechanism in place for the critical care service to have access to
nutritional support services for advice on both enteral and parenteral nutritional
techniques.
6.7.1.12. There shall be a program of continuous quality improvement for the ICU service that is
integrated into the specialty center continuous quality improvement program and
includes regularly collecting and analyzing data to help identify health-service problems
54
and their extent, and recommending, implementing, and monitoring corrective actions on
the basis of these data.
6.7.2. Premises
6.7.2.1. The ICU shall be located in access restricted area of the center and well identified.
6.7.2.2. ICU room: The size of the room depends on the number of ICU beds. The ICU shall be at
least 8m x 10m in size that accommodate a maximum of 2 electrically or manually
operated ICU patient beds fitted with full range of monitors and a screen.
a) The header of beds shall be 1 m away from the wall
b) There shall be a 2m wide free traffic area by side of beds and between any of two
beds.
c) There shall be a nurse station within the ICU having a computer and a computer
point, telephone and telephone point, cabinets and shelves, and lockers for
controlled drugs.
d) There should be a separate physical area devoted to nursing management for the
care of the intermediate patient (32 sq m area including nurse station).
6.7.2.3. Nurse station in the ICU:
a) Isolated with glass, full visual access to monitor admitted patients on monitors,
b) Equipped with chairs, working laminated top tables, drawers and computers, Linen
boards, shelves, lockers
c) Telemetry monitoring for critical or post operative patients with transmitters,
d) Telephone end,
e) Medication boards, controlled drug locker,
f) Calculators,
g) Weight scale,
h) Ready to use CPR equipments with defibrillator on trolley,
i) Patient labeling for diet, allergy, etc.,
6.7.2.4. The ICU shall have easily accessible hand wash basin around the entrance-exit door.
6.7.2.5. In addition to the main ICU for critical care, the unit shall have the following spaces
(rooms): toilets, nurse room, utility room, store, duty room, cleaner’s room, staff tea room,
and spacious corridor for stretchers and wheelchairs.
6.7.2.6. Toilet: ICU shall have staff and patient toilet and shower facilities.
55
6.7.2.7. The ICU shall be access to laboratory service, or it shall be equipped with side lab,
dedicated and open for 24 hours a day and 365 days a year.
6.7.2.8. Nurse locker room: There shall be an ICU staff locker room in proximity with the ICU.
The ICU area is generally regarded as a sterile zone and there shall be shoe and cloth
change point for staff and attending families.
6.7.2.9. ICU Utility/ Sluice room: There shall be soiled utility/sluice room which acts as a storage
area for contaminated materials until they are disposed off and temporary station for
equipments until disinfected and cleaned. The soiled utility room shall have a deep bowel
sink, a hand wash basin with hot and cold water, plus cabinet and shelves.
6.7.2.10. Store room: There shall be an ICU supply room (store) at least 4m x 4m in size used for
storage of consumables and spare equipments. It shall be equipped with cabinets and
shelves. Materials shall be labeled, arranged in order, ready for use (charged) and there
shall be ventilation and enough light.
6.7.2.11. Cleaner’s room: There shall be an ICU cleaner’s / janitor’s room for an easy access to
cleaning equipments and materials or the ICU floor. If there is a mobile cleaning service it
can be optional.
6.7.2.12. Staff tea room (optional): There should be a staff tea room in close proximity to the ICU
in order to ensure the availability of staff at all times and as rest room for visitors.
6.7.3. Professionals
6.7.3.1. The specialty center ICU shall be directed by a licensed anesthesiologist or intensivist or
ICU trained internist.
6.7.3.2. The physicians working in the ICU shall be certified in either in internal medicine,
anesthesia, surgery, paediatrician or general practice and/or have completed a formal
training program in critical care approved by the licensing body in the country.
6.7.3.3. There shall be a registered professional nurse with administrative responsibility for the
ICU or combination of units who is accountable for all critical care nursing rendered in the
unit or units.
6.7.3.4. The nursing staff of each unit within the ICU service shall have special training in critical
care nursing or took on job training.
6.7.3.5. All practicing nurses in the ICU shall be trained and certified in basic cardiac life support.
6.7.3.6. Nurse assistants assigned to ICU shall be oriented and trained on basic cardiac life support
and critical care.
56
6.7.3.7. There shall be at least one registered ICU nurse in the ICU for 24 hours a day and 365 days
a year.
6.7.3.8. At least the following professionals are required:
a) One anesthesiologist and/or ICU trained internist
b) Critical care nurses
c) Cleaners
d) Porters
e) General technician
6.7.4. Products
6.7.4.1. Medicines selected for ICU services shall be available at all times
6.7.4.2. The ICU shall have the following equipment, instruments and system:
a) The ICU beds shall have removable side protections; functional wheels; shall be
easily adjustable to multipurpose positions
b) mechanical ventilator to assist breathing through an endotracheal tube or a
tracheotomy opening; at least 4; All ventilators shall be equipped with an integral
minimum ventilation pressure (disconnect) alarm.
c) Different size endotracheal tubes and tracheotomy sets, at least 4 sets,
d) monitoring equipment, equipment for the constant monitoring of bodily functions;
e) cardiac monitors including telemetry,
f) Standard 12 lead EKG machines,
g) external pacemakers (optional),
h) defibrillators; at least 2,
i) Reliable Oxygen delivery systems: Oxygen cylinder or oxygen concentrator,
j) Oxygen regulator, at least 2
k) pulse oximeter,
l) end-tidal carbon dioxide monitoring,
m) Titrated therapeutic interventions with infusion pumps,
n) A web of intravenous lines for medicines infusions, fluids or total parenteral
nutrition,
o) suction pumps,
p) infusion pump
q) Laryngoscopes with different size blades,
57
r) Ophthalmoscope,
s) Mouth gags, different size
t) Air ways, different size
u) Resuscitation trolleys,
v) Exam coaches,
w) Syringe pump,
x) Endotracheal tubes ,(different sets)
y) Wheel chair,
z) Patient transport stretcher,
aa) Sphygmomanometer, with adult and pediatric cuffs,
bb) Sthethoscopes: pediatric and adult,
cc) Electrical suction machine (at least 1 as a backup),
dd) Pedal suction machine,
ee) Nasal CPAP,
ff) Bed pan, plenty in number, different size
gg) Pacing boxes (at least 2)
hh) X-ray viewer per bed
ii) Wall clock (at least 2)
jj) Soiled cloth hampers
j) Patient screen per bed and
kk) IV stands, at least one per bed
6.8. Radiological Services 6.8.1. Practices
6.8.1.1. Basic Radiology service shall be available for specialty center, which at least
includes X-Ray & ultrasound.
6.8.1.2. The radiology service shall have written policies and procedures that are
reviewed at least once every five years and implemented. These policies and
procedures shall include at least:
a) Safety practices; b) Management of the critically ill patient; c) Infection control, including patients in isolation;
58
d) Timeliness of the availability of diagnostic imaging procedures and the results;
e) Quality control program covering the inspection, maintenance, and calibration of all equipment.
6.8.1.3. The specialty center shall make policies and procedures for radiology services available
to all staff in the radiology unit.
6.8.1.4. There shall be a written protocol for managing medical emergencies in the radiological
suite.
6.8.1.5. The radiology service of the Specialty center shall have X-Ray & Ultrasound services.
6.8.1.6. The radiology service unit shall be free of hazards to patients and personnel.
6.8.1.7. Proper safety precautions shall be maintained against fire and explosion hazards,
electrical hazards, and radiation hazards.
6.8.1.8. The Specialty center shall post/ put in easily accessible place the approval certificate
from the Ethiopian Radiation Protection Authority through periodic inspection.
6.8.1.9. There shall be documentation of the report for periodic radiation exposure dose
readings for Radiation workers by the use of exposure meters or badge tests.
6.8.1.10. Signed reports shall be filed with the patient's medical record and duplicate copies kept
in the service unit.
6.8.1.11. Requests for x-ray examination shall contain a concise statement of reason for the
examination.
6.8.1.12. X-ray films shall be labeled with minimum information such as date, name, age, sex,
right/left marks, name of institute and name of radiographer.
6.8.1.13. Reporting form shall have minimum information such as date, patient’s name, age, sex,
findings and name and signature of radiologist.
6.8.2. Premises
6.8.2.1. The radiology unit for specialty center shall fulfill the design requirements of
Ethiopian Radiation Protection Authority (ERPA) guidelines.
6.8.3. Professional
6.8.3.1. The radiology service of the center shall be directed by a licensed radiologist.
6.8.3.2. A radiologist shall be available in the center during working hours all the time or
if on call shall arrive within 30 minutes of being summoned
59
6.8.3.3. A licensed radiology technologist or radiographer shall be present in the center
at all times.
6.8.3.4. A licensed professional nurse may be available in the radiology service to
administer medications and perform other nursing care.
6.8.3.5. A receptionist, cleaners shall be available in radiology service as full time..
6.8.4. Products
6.8.4.1. All medical equipments which shall be available for radiology services at
Specialty center are indicated below:
a) Digital X-ray machine ,b) Color Duplex Ultrasound,c) X-Ray viewing boxes,d) Dark room film processing baths (if necessary),e) Drier (if necessary),f) MRI or CT scan machine depending on the type of the specialty center,g) Radiation protection equipments:
lead gloves, lead apron, lead goggle, gonad shield,
6.8.4.2. The X-Ray machine shall be regularly inspected, maintained, and calibrated; appropriate
records of maintenance shall be maintained.
6.8.4.3. Installation and un-installation of X-Ray machine shall follow the safety procedures set
by the Ethiopian Radiation Protection Authority during all procedures.
6.8.4.4. All radiation generating equipments shall be installed within a room/ building with wall
thickness that protects radiation to the surroundings, i.e., the minimum criteria set by
the Ethiopian Radiation Protection Authority /IAEA
60
6.9. Medical Laboratory Services6.9.1. Practices
6.9.1.1. The specialty center shall have a minimum of basic laboratory service working
for 24 hours a day & 365 days a year.
6.9.1.2. The specialty center laboratory service shall provide Basic Hematology,
Bacteriology, Clinical Chemistry, parasitology, urinalysis & Serology test profiles.
Based on the type of the center, complexity of the test profiles varies.
6.9.1.3. The specialty center laboratory shall have written procedures for the following:
a) Procedure manuals (Standard Operating Procedure, SOP) or guidelines for all tests and equipments,
b) Quality assurance and control processes,c) Inspection, preventive maintenance & calibration of all equipment,d) Management of reagents including availability, storage, and testing
for efficacy,e) Procedures for collecting, identifying, processing and disposing of
specimens,f) All normal ranges for all tests shall be statedg) Laboratory safety program, including infection controlh) Documentation of quality Assessment, calibration report and
refrigerator readings.6.9.1.4. The laboratory shall have procedures or (SOP) for specimen collection and/ or
transport that address specific collection requirements.
6.9.1.5. The laboratory shall follow standard operating procedures (SOP) and conduct
routine quality assessments to ensure reliable and cost-effective testing of
patient specimens.
6.9.1.6. The process of analysis shall be specified by validated written or electronic
procedures maintained in and by the laboratory. Procedures may be written by
the laboratory staff or may be adapted from previously published materials
including, but not limited to, product inserts, procedure or instrument manuals,
textbooks, journals, or international guidelines.
6.9.1.7. The Specialty center Laboratory staff shall prepare SOP or set criteria for
acceptance and rejection of clinical specimens.
6.9.1.8. The Specialty center Laboratory shall monitor the transportation of samples to
the laboratory such that they are transported, within time frame, within
temperature interval specified in the primary sample collection manual or SOP
and in a manner that ensures safety for carrier.
61
6.9.1.9. The Specialty center laboratory shall maintain a record of all samples received.
6.9.1.10. The Specialty center Laboratory shall have a procedure for storage of clinical
samples if it is not immediately examined.
6.9.1.11. Patient samples shall be stored only for as long as necessary to conduct the
designated tests (or other permitted procedure) according to fixed storage
times, and shall be destroyed safely and confidentially after storage.
6.9.1.12. Once a sample is used, remnant shall be discarded in the laboratory following
standard IP in the lab.
6.9.1.13. The laboratory for specialty center shall establish an external quality control
system with accredited agencies and shall participate nationally or
internationally in EQA at least once yearly.
6.9.1.14. The specialty center Laboratory shall produce report which shall contain the
following:
a) All laboratory test result/reports shall have reference (normal) ranges.
b) Files of reported results shall be retained by the laboratory. c) Reports shall be filed with the patient's medical record and
duplicate copies shall be filed in the laboratory in a manner which permits ready identification and accessibility and with appropriate backup.
d) In the case of laboratory tests performed by an outside laboratory, the original report from such laboratory shall be contained in the medical record.
e) Quality assured test results shall be reported on standard forms to the general medical practitioner with the following minimum information:
Patient identification (patient name, age, gender). Date and time of specimen collection. The test performed and date of report. The reference or normal range. The name and initial of the person who performed the test, and the
authorized signature of the person reviewing the report and releasing the results.
Specialty center address. f) Laboratory results shall be legible, without transcription mistakes
and reported only to persons authorized to receive them. g) The laboratory shall have policies and procedures in place to
protect the privacy of patients and integrity of patient records whether printed or electronic. Policies shall be established which
62
define who may access patient data and who is authorized to enter and change patient results.
6.9.1.15. When reports altered, the record shall show the time, date and name of the
person responsible for the change.
6.9.1.16. Safe disposal of samples shall be in line with standards prescribed under
infection prevention
6.9.1.17. No eating, drinking, smoking or other application of cosmetics in laboratory
work areas or in any area where workplace materials are handled.
6.9.1.18. No food or drink shall be stored in the laboratory.
6.9.1.19. Wearing of protective clothing of an approved design (splash proof), always
fastened, within the laboratory work area and removed before leaving the
laboratory work area.
6.9.1.20. Where services are provided by an outside laboratory (contract), the conditions,
procedures, and availability of services offered shall be in writing and available
in the Specialty center.
6.9.1.21. There shall be a policy and procedure for regular calibration and running of
control tests for laboratory equipments: semi-automated/ automated machines.
Documentation shall be maintained.
6.9.1.22. Laboratory shall have a documented and recorded programme of preventive
maintenance which at a minimum follows the manufacturer’s recommendations.
6.9.1.23. Equipment shall be maintained in a safe working condition. This shall include
examination of electrical safety, emergency stop devices. Whenever equipment
is found to be defective, it shall be taken out of service and clearly labeled.
6.9.1.24. There shall be a written safety procedure for handling hazardous chemical
reagents used in the laboratory. The procedure shall define at least the
following:
a) The storage requirements,b) Handling procedures,c) Requirements for personal protective equipment,d) Procedures following accidental contact or overexposure,
6.9.2. Premises
6.9.2.1. The specialty center shall have a well organized, adequately supervised and staffed
clinical laboratory with the necessary space, facilities and equipments.
6.9.2.2. The laboratory working environment shall be kept organized and clean, with safe
procedures for handling of specimens and waste materials.
63
6.9.2.3. The laboratory shall have adequate lighting, ventilation, water, waste and refuse
disposal.
6.9.2.4. The laboratory shall have controlled temperature of refrigerator. For which recordings
shall be documented.
6.9.2.5. Facilities shall provide a suitable environment to prevent damage, deterioration, loss or
unauthorized access.
6.9.2.6. The medical laboratory of the center shall fulfill all premises requirements described
under each specialty center.
6.9.2.7. The laboratory facilities shall meet at least the following general requirements:
a) Reliable supply of running water, b) The laboratory rooms shall have two separate sinks, one for general
laboratory use and the other reserved for hand washing, c) Continuous power supply, d) Fitted with laboratory benches, Working surface covered with
appropriate water proof, corrosive resistance materials, e) Laboratory stools for the benches. f) Laboratory furniture shall be capable of supporting anticipated loading
and uses. g) Spaces between benches, cabinets, and equipment shall be accessible for
cleaning.h) Lockable doors and cupboards. i) Closed drainage from laboratory sinks (to a septic tank or deep pit) j) Separate toilets for staff and patients.
6.9.2.8. Emergency of safety services such as deluge showers and eye-wash stations, fire
alarm systems and emergency power supplies shall be included in the laboratory
services design specifications.
6.9.3. Professionals
6.9.3.1. The laboratory service shall be directed by a licensed medical laboratory
technologist.
6.9.3.2. The specialty center shall have & maintain Job descriptions including
qualification for each lab staff.
6.9.3.3. The specialty center shall facilitate access to relevant trainings, continuing
education and assess staff competency at regular intervals.
64
6.9.3.4. Laboratory staff shall, at all times, perform their functions with adherence to the
highest ethical and professional standards of the laboratory profession.
6.9.3.5. The medical laboratory of the center shall fulfill the minimum staffing requirements
described under each specialty center.
6.9.4. Products
6.9.4.1. Specialty center medical laboratory shall have the following equipments:
a) Safety cabinet, b) Lab bench,c) Microscope, binoculard) Centrifuge, e) Autoclavef) Dry oven,g) Refrigerator with thermometer,h) Bunsen Burner,i) ESR standj) ESR tubes,,k) Water distillation apparatus,l) Incubator, m) Microhematocrit centrifuge,
n) WBC chamber,o) Differential counter,p) Hematology analyzer,q) Clinical Chemistry analyzer
(semi-automated*/ automated), r) Water bath,s) Assorted lab glass wares,t) Biohazard bag,u) Safety box, v) Glucometer,w) Hemoglobinometer,
6.9.4.2. The minimum equipments for Clinical chemistry services:
a) Autoclave b) Clinical chemistry analyzer
(Automated or semi automated) c) Glucometerd) Power surge protectors
e) Weighing balancef) Micropipettes of different volumesg) Timer with alarmh) Water bath
6.9.4.3. The minimum equipments for Parasitology & Urine, body fluid analysis &
Mycology:
a) Binocular Microscope, b) Slides
c) Staining reagents, Gram stain, Giemsa stain, AFB stain,
d) CSF analysis reagents6.9.4.4. The minimum equipment for Hematology:
a) Haemoglobinometer b) Hematology analyzer (
Automated)c) Blood roller/mixerd) Refrigerator e) Binocular microscope x10,
x40, x100 f) Haemocytometer
g) Microhematocrit centrifugeh) Microhematocrit readeri) Differential counter j) Tally counter k) Deep freezer l) Centrifugem) Timer n) Distillation unit

65
o) Shaker/ Roller
6.9.4.5. Exception: Internal medicine specialty center shall have viral load and CD4 machines.
6.9.4.6. The following minimum consumables, Lab Chemicals and solutions shall be required
a) HClb) Sulfuric Acidc) Wright staind) Giemsa staine) Formalinf) Xyleneg) Oil immersionh) Carbol fucsini) Methylene bluej) Acetonek) Crystal violetl) Gram’s iodinem) Absolute ethanoln) Methanolo) Safraninep) Glacial acetic acidq) Etherr) 75% alcohols) 0.85% NaClt) Savlone (chlorohexidine
+cetrimide)u) KOHv) Glycerolw) Urine strip of 10
parameterx) HCG Test kity) Occult blood reagentsz) Vacutainer EDTA tube of
4mlaa) Vacutainer plain tube of
10ml
bb) Vacutainer needle holdercc) Vacutainer needledd) Syringe with needle of
different sizes ee) Tourniquetff) Slide and cover slidegg) Micropipette of different
sizes (5μl -1000μl)hh) Thermometerii) Conical urine test tubesjj) Electronic pipetteskk) Disposable plastic pipettes
(1 ml-5ml)ll) Sterile urine cupsmm) Stool cupnn) Nunc tubesoo) Cryoboxespp) Pasteur pipettesqq) Test tube racksrr) Slide boxesss) Lens papertt) Disposable gloves uu) Cotton Rollvv) Applicator sticksww) Biohazard plastic bagxx) Safety Boxyy) Nunc tube racks zz) ESR rack aaa) Westergren tube bbb) Test tube racks
66
6.10. Pharmacy Services6.10.1. Practices
Dispensing and Medication Use Counseling
6.10.1.1. Standard operating procedure (SOP) for dispensing and medication use counseling shall
be established to ensure patients’ safety and correct use of medications.
6.10.1.2. Dispensers shall make sure that prescriptions are legible, written by authorized
prescriber and complete. Prescription papers shall be standardized and must contain at
least the following information and the prescriber shall complete all these information:
a) Name of patient, sex, age and medical record number,b) Diagnosis and allergy, if any, c) Name of the medicines, strength, dosage form, dose, frequency, and route of
administration, d) Duration of treatment,e) Prescriber’s name, qualification and signature,f) Prescriber’s address (name and address of Specialty center).
6.10.1.3. The pharmacist shall check the correctness of prescriptions in terms of appropriateness
for patients and of dosage, strength and drug interactions based on approved standard
treatment guidelines”
6.10.1.4. All medicines shall be dispensed with adequate and appropriate information and
counseling to patients for correct use of their medications.
6.10.1.5. The pharmacist shall make an in-depth professional judgment to make sure that each
medicines and its dosage form has all of its attributes of quality and an acceptable ratio
of safety.
6.10.1.6. The containers used for dispensing shall be appropriate for the product dispensed and
all containers intended for pharmaceuticals shall be protected and kept free from
contamination, moisture and light.
6.10.1.7. All pharmaceuticals to be dispensed shall be labeled and the labels shall be
unambiguous, clear, legible and indelible. The following minimum information shall be
indicated on the label/ sticker:
a) the generic name of the product or each active ingredient, where applicable;b) the strength, dose, frequency of administration and total quantity;c) the name of the person for whom the medicines are dispensed;d) the name of the prescriber and patient card number;
67
e) the directions for use and route of administration tailored to patient or caregiver literacy and language;
f) the name and business address of the dispenser;g) date of dispensing; andh) Special precautions as applicable
6.10.1.8. Filled prescriptions shall be signed and accountability must be accepted by the
dispensing Pharmacist.
6.10.1.9. Each Specialty center shall establish and implement policies, guidelines and procedures
for reporting any errors or any suspicion in administration or provision of prescribed
medications. Errors shall be reported to the prescriber in a timely manner upon
discovery and a written report of the error prepared and documented. Any suspicion or
error shall be communicated to the prescriber and clarified/corrected before dispensing
without affecting patient’s confidence on medical practices.
6.10.1.10. The pharmacy shall keep individualized information for patients with chronic illnesses
medication program using standardized information tracking formats and update
patient medication profile during each refill visit.
6.10.1.11. The counseling of patients or their caregivers shall be undertaken to promote the
correct and safe use of pharmaceuticals. The responsible Pharmacist must ensure that
patients are counseled before they receive pharmaceuticals that they are to self-
administer.
6.10.1.12. The Pharmacist shall assess each patient's ability to understand the information
imparted by question and answer and must be able to modify his/her approach
accordingly. Care shall be taken with counseling where understanding is likely to be a
problem.
6.10.1.13. Cautionary instructions and ancillary information about medications shall be
communicated in writing to the personnel responsible for administering medications.
Extemporaneous Pharmaceuticals Preparations (Optional):
6.10.1.14. Written procedures/SOPs for center based pharmaceutical preparations shall be
established for preventing errors, drug-drug interactions and drug contamination. This
SOP shall contain an approved Master Formula for each type of preparation that shows
the list of ingredients and their quantities required for the formulation of a specified
amount of the preparation.
6.10.1.15. Licensed pharmacists shall be responsible for the preparations of various
pharmaceutical formulations such as eye drop preparations, dosage form changes,
68
extemporaneous preparations, IV infusions and IV admixture when deemed necessary
by the center.
6.10.1.16. The center shall have a pharmacy-based intravenous infusion admixture program, which
may include services related to preparation of total parenteral nutrition, antineoplastic
agents, and large and small, continuous or intermittent volume products for infusion. A
pharmacist licensed to practice pharmacy shall prepare, sterilize if necessary, and label
parenteral medications and solutions.
6.10.1.17. The pharmacist responsible for pharmaceutical preparations shall ensure that quality is
built into the preparations of products.
6.10.1.18. Ingredients used in preparations shall have their expected identity, quality, and purity
and shall be from legally licensed sources.
6.10.1.19. Pharmaceutical preparations shall be of acceptable strength, quality and purity, with
appropriate packaging and labeling, and prepared in accordance with good
compounding practices, international standards, and relevant scientific data and
information. Labels on compounded products for individual patient shall have a
minimum of the following information:
a) Patient's nameb) Name of the compounding pharmacistc) Name and address of the compounding institutiond) A complete list of ingredients and preparation namee) Strengthf) Quantity of each ingredients and total quantityg) Directions for useh) Date of preparationi) Beyond-use datej) Storage conditionk) Batch number
6.10.1.20. Critical processes shall be validated to ensure that procedures, when used, will
consistently result in the expected qualities in the finished preparation.
6.10.1.21. Appropriate stability evaluation shall be performed or determined using international
standards for establishing reliable beyond-use date to ensure that the finished
preparations have their expected potency, purity, quality, and characteristics, at least
until the labeled beyond-use date.
6.10.1.22. Written procedures and records shall exist for investigating and correcting failures or
problems in compounding, testing, or in the preparation itself.
69
6.10.1.23. Pharmaceutical preparations compounded in the center shall be packaged in containers
meeting standard requirements mentioned under the official national or international
standards for such preparations.
Control of Drug Abuse, Toxic or Dangerous Drugs
6.10.1.24. The specialty center shall establish Policies and procedures to control the
administration of narcotic drugs and psychotropic substances with specific reference to
the duration of the order and the dosage in accordance with relevant laws.
6.10.1.25. A record of the stock on hand and of the dispensing of all these drugs shall be
maintained in such a manner that the disposition of any particular item may be readily
traced.
6.10.1.26. A licensed pharmacist shall dispense all controlled substances (narcotic and
psychotropic drugs) to the authorized health professional designated to handle
controlled substances in the specialty center. When the controlled substance is
dispensed, the following information shall be recorded into the controlled substances
(proof-of-use) record.
a) Name and signature of Pharmacist dispensing the controlled substanceb) Name and signature of designated licensed person receiving the controlled
substance.c) The date and time controlled substance is dispensed.d) The name, the strength, and quantity of controlled substance dispensed.e) The serial number assigned to that particular record, which corresponds to same
number recorded in the pharmacy's dispensing record.6.10.1.27. When the controlled substances are not in use, they shall be maintained in a securely
locked, substantially constructed cabinet or area. All controlled substance storage
cabinets shall be permanently affixed. Controlled substances removed from the
controlled substance cabinet shall not be left unattended.
6.10.1.28. The administration of all controlled substances to patients shall be carefully recorded
into the standard record for controlled substances and returned back to the Pharmacist
upon refill of controlled substances. The following information shall be recorded during
administration to patients.
a) The patient's name, card numberb) The name of the controlled substance and the dosage administered.c) The date and time the controlled substance is administered.d) The signature of the practitioner administering the controlled substancee) The wastage of any controlled substance.
70
f) The balance of controlled substances remaining after the administration of any quantity of the controlled substance
g) Day-ending or shift-evening verification of count of balances of controlled substances remaining and controlling substances administered shall be accomplished by two (2) designated licensed persons whose signatures shall be affixed to a permanent record.
6.10.1.29. All partially used quantities of controlled substances shall be licensed in to the control
substance record and returned back to the responsible Pharmacist for control
substances for disposal.
6.10.1.30. All unused and unopened quantities of controlled substances which have been removed
from the controlled substance cabinet shall be returned to the cabinet by the
practitioner at the end of each shift.
6.10.1.31. Any return of controlled substances to the pharmacy in the Specialty center shall be
documented by a licensed Pharmacist responsible for controlled substance handing in
the Specialty center.
6.10.1.32. The Specialty center shall implement procedures whereby, on a periodic basis, a
licensed Pharmacist shall reconcile quantities of controlled substances dispensed in the
Specialty center against the controlled substance record. Any discrepancies shall be
reported to the head of the center. Upon completion, all controlled substance records
shall be returned to the pharmacy by the designated responsible person.
6.10.1.33. The center shall submit regular report to the appropriate organ regarding the
consumption and stock of controlled drugs.
Clinical Pharmacy Services (optional):
6.10.1.34. The specialty center shall establish policies and procedures for the provision of clinical
pharmacy services through drug and therapeutic committee.
6.10.1.35. The pharmacist for clinical pharmacy services shall have access to patient specific
medication therapy information.
6.10.1.36. Patient-specific medication therapy information must be evaluated and a drug therapy
plan shall be developed by the pharmacist mutually with the patient, the prescriber and
nurse as appropriate.
6.10.1.37. The pharmacist shall review, monitor and propose for modification of the therapeutic
plan in case of adverse effects, patient noncompliance and evidence- based efficacy
problem and as appropriate, in consultation with the patient, prescriber and nurse.
71
6.10.1.38. Through prescription and medication history monitoring, the pharmacist shall identify
problems or opportunities for optimizing treatment and hence safeguard the patient and
ensure the optimal use of medicine
6.10.1.39. Medication education shall be delivered to patients or their caregivers upon discharge
by the pharmacist.
6.10.1.40. The pharmacist shall make sure that the patient has all supplies, information and
knowledge necessary to carry out the drug therapy plan.
6.10.1.41. As a member of the specialty center team, the pharmacist shall attend and participate at
patient visits and contribute to patient care through the provision of medicine
information, dose calculations and adjustment, assisting in the rational prescribing
decision, alternative regimens & combinations and reducing the frequency and duration
of medication errors.
6.10.1.42. The specialty center (drug and therapeutic committee) shall develop/adopt and
implement policy on antimicrobial prescribing, dispensing and usage.
Emergency Pharmacy Services
6.10.1.43. The specialty center shall have emergency pharmacy service for 24 hours a day.
6.10.1.44. The center shall have emergency medicines list and continuous availability of such
medicines shall be ensured at all times,
6.10.1.45. The center shall have the mechanism to ensure appropriate use of medicines for
emergency purposes
6.10.1.46. Orders received by words of mouth or through telephone during emergency (in case of
immediate administration is necessary, no appropriate alternative treatment is available
and when it is not reasonably possible for the physician to provide a written
prescription prior to dispensing) shall latter be endorsed by the prescriber and be
documented in writing within 24 hours. The quantity shall be limited to emergency
period only.
Adverse Drug event, ADE/ Pharmacovigilance
6.10.1.47. The pharmacy of the specialty center shall appoint an ADE (adverse drug event) focal
person responsible for the collection, compilation, analysis and communication of
adverse drug reaction, medication error and product quality defects related information
to the DTC and then to FMHACA.

72
6.10.1.48. Health professionals of the center shall be responsible to report suspected ADE cases to
the ADE focal person.
6.10.1.49. DTC shall discuss and make necessary recommendations to the center’s management for
decision on adverse drug event reported within the health facility.
6.10.1.50. The pharmacy of the center shall consistently update the safety profile of medicines
included in the formulary list for immediate medicines use decisions and consideration
during the revision of the list.
6.10.1.51. Adverse medication effects shall be noted in the patient’s medication record.
6.10.1.52. All the ADE reports, patient identity, reporters and medicine trade names shall be kept
confidential.
6.10.1.53. The reporting of ADE shall be done by the national ADE prepaid yellow form prepared
by FMHACA
Pharmaceutical Supply and Management
6.10.1.54. A drug and therapeutics committee (DTC) representing different service units of the
center shall be in place for selection of medicines and ensure proper use
6.10.1.55. The purchase of pharmaceuticals shall be the responsibility of a pharmacist who is
assigned to manage and control the supply of medicines.
6.10.1.56. The center shall have procurement policy to ensure the continuous supply of safe,
quality and effective medicines
6.10.1.57. A pharmacist shall not purchase any medicinal product where he/she has any reason to
doubt its safety, quality or efficacy and he/she should notify this to the appropriate
organ .
6.10.1.58. The pharmacist shall ensure that both the supplier and the source of any medicine
purchased are reputable and registered by the FMHACA.
6.10.1.59. The center shall introduce and maintain stock control system (manual and/or
computerized system) in the pharmacy store and dispensaries.
6.10.1.60. The center shall be responsible to make sure that pharmaceuticals promotion made by
suppliers or manufacturers in the center’s premises is made by a registered pharmacist
in accordance with the country’s laws.
6.10.1.61. The center shall be responsible to make sure that donation of pharmaceuticals has been
made in accordance with the country’s laws.
73
6.10.1.62. There shall be a responsible pharmacy personnel assigned for receiving, storage, issuing,
recording, monitoring and reporting.
6.10.1.63. The storage condition shall provide adequate protection to the medicines from all
environmental factors until the medicines are delivered to the patient.
6.10.1.64. The responsible pharmacist must ensure that all areas where pharmaceuticals are
stored are of acceptable standards (palletized or shelved, ventilated, rodent free,
temperature and moisture controlled and others) for medicines store.
6.10.1.65. The responsible pharmacist shall ensure that all medicine storage areas are inspected
regularly to ensure that:
a) pharmaceuticals are stored and handled in accordance with the pharmaceutical
manufacturer’s requirements and regulatory standards
b) expired or obsolete pharmaceuticals are stocked separately until disposition
c) pharmaceuticals requiring special environmental conditions shall be stored
accordingly
d) Temperature and humidity are maintained according to manufacturer’s
requirement
e) stock levels are adequate to ensure the continuous supply and acceptability of
pharmaceuticals at all times, including the availability of essential medicines as per
the latest edition of the medicines formulary list
f) inflammable substance are stored separately and in an appropriate manner
g) disinfectants and preparations for external use are stored separately from
pharmaceuticals for internal use
6.10.1.66. Special storage conditions shall be maintained for pharmaceuticals requiring cold chain
system, controlled substances, radiopharmaceuticals and medical gases.
6.10.1.67. Firefighting equipment or system shall be installed to pharmaceutical storage places
6.10.1.68. Distribution of pharmaceuticals within a center shall be under the direction and control
of a pharmacist and must be in accordance with the policy developed by DTC. All issuing
activities shall be made using official and serially numbered vouchers.
6.10.1.69. Written SOPs shall be provided on how supplies of stock are to be obtained from the
pharmaceuticals store. Procedures must define normal action to be taken by phar-
maceutical staff for routine stock replacement and action to be taken in the case of
incomplete documentation or other queries.
74
6.10.1.70. Written procedures shall be available for the return of expired, damaged, leftover and
empty packs from outlets to pharmaceuticals store to prevent potential misuse.
6.10.1.71. The center shall maintain stock control system (manual and/or computerized system) in
the central medical store and dispensary.
6.10.1.72. The responsible pharmacist shall ensure that adequate control procedures are in place
for all stock circulating at all outlets within the center.
6.10.1.73. Daily medicines consumption at different outlets of the center shall be recorded,
compiled, analyzed and reported.
6.10.1.74. There shall be a pharmacist assigned as medicine Supply Management Officer that is
responsible for the procurement, stock management, warehouse management,
distribution of medicines and disposal of medicine waste. There shall be also a
responsible pharmacy personnel assigned for receiving, storage, issuing, recording,
monitoring and reporting
6.10.1.75. The center pharmacist who is responsible for the management of pharmaceuticals
should conduct regular medicines use studies to ensure maximum patient benefit from
the formulary list
6.10.1.76. The DTC should be responsible for developing policies and guidelines on how to
organize and conduct medicines use studies.
Medicines Waste Management and Disposal
6.10.1.77. The disposal of medicine wastes shall be in compliance with the medicines waste
management and disposal directives issued by FMHACA.
6.10.1.78. Specialty center pharmacy shall take responsibility, through supportive policies and
procedures for the environmental and societal safety by efficiently managing the
pharmaceutical wastes.
6.10.1.79. All personnel involved in medicines waste handling shall be trained and/or well
informed about the potential risks of hazardous medicines waste and their management.
6.10.1.80. Cleaners or anybody to handle hazardous pharmaceutical wastes shall wear protective
devices like apron, plastic shoes, gloves, head gears and eye glasses when the need
arises.
6.10.1.81. General wastes shall be collected daily from the pharmacy and placed in a convenient
place outside the pharmacy to facilitate coordinated disposal by the center.
6.10.1.82. Solid wastes from the pharmacy shall be categorized as “hazardous” and ‘non-
hazardous” and shall be collected separately for proper treatment.
75
6.10.1.83. All hazardous chemicals spills shall be immediately reported to head of the pharmacy or
responsible person for safety (if available) to minimize the risk and take immediate
action.
6.10.1.84. Spillages of low toxicity shall be swept into a dust pan and placed into a suitable
container for that particular chemical and dispose accordingly.
6.10.1.85. Medicines in single dose or single use containers which are open or which have broken
seals, medicines in containers missing medicines source and exact identification (such as
lot number), and outdated medications shall be collected to the pharmacy for disposal.
6.10.1.86. The Specialty center shall form a pharmaceutical waste disposal committee to ensure
safety, accountability and transparency.
6.10.1.87. Disposal of pharmaceutical wastes shall be supported by proper documentation
including the price, batch number & expiry date of the products for audit, regulatory or
other legal requirements.
Recording
6.10.1.88. There shall be a standardized Prescription Registration Book for recording prescriptions
and dispensed medicine. A computerized dispensing and registration system with
backup can be used instead if available.
6.10.1.89. Each patient with a chronic disease shall have a separate Patients Medication Profile
Card (PMP) that should be filled appropriately with all the relevant information for each
patient. A computerized system with backup can be used instead if available.
6.10.1.90. Controlled and non-controlled prescriptions shall be documented and kept in a secure
place that is accessible only to the authorized personnel for at least five and three years
respectively.
6.10.1.91. Patient and medication related records and information shall be documented and kept
in a secure place that is easily accessible only to the authorized personnel
Billing
6.10.1.92. Pharmaceuticals shall be received and issued using standard receiving and issuing
vouchers with serial number. Issuing and receiving of pharmaceuticals has to be signed
by both the receiver and issuer and approved by an authorized Pharmacist. Receiving
and issuing vouchers shall have the following minimum information.
a) Name of medicines received and issued,
76
b) Unit of measurement, quantity and source (supplier’s or manufacturer’s name) of medicines,
c) Expiry date and batch number,d) Unit and total price,e) Date received and issued,f) Name and signature of receiver and issuer,g) Address of the Specialty center,
6.10.1.93. All medicines issued from the pharmacy dispensary shall be dispensed/ sold using
standard sales ticket with serial number. Sales tickets shall be signed and stamped.
6.10.1.94. Dispensing pharmacies shall use a standard stamp and seal for approving legal
transactions.
6.10.1.95. The consumer has the right to know the exact price of a prescription before it is filled on
sales ticket.
6.10.1.96. The Specialty center shall ensure that each customer has the right to get receipt which
has the following minimum information about medicines dispensed.
a) Name of patient,b) Name and dosage form of medicines dispensed,c) Unit of measurement and quantity,d) Unit and total price,e) Date,f) Signature of dispenser and cashier,g) Address of the Specialty center.
Organization Management and Quality Improvement
6.10.1.97. A multidisciplinary drug and therapeutic committee chaired by the medical director and
supported by a licensed pharmacist representing the center pharmaceutical services as a
secretary must be functional for the overall improvement of pharmaceutical services in
the center.
6.10.1.98. The pharmaceutical services shall be represented by a licensed senior pharmacist in
every management meetings of the center.
6.10.1.99. Customer satisfaction survey on pharmaceutical services shall be conducted at least
once in a year and measures shall be taken in accordance with survey findings.
6.10.1.100. There shall be a program of continuous quality improvement for the pharmaceutical
service that is integrated into the center continuous quality improvement program and
includes regularly collecting and analyzing data to help identify pharmaceutical service
77
problems and their extent, and recommending, implementing, and monitoring corrective
actions on the basis of these data.
6.10.1.101. The pharmaceutical service shall have in effect a patient profile system for monitoring
medicine therapy. This system shall be used by the center to identify inappropriate
prescribing practices and develop interventions.
6.10.1.102. The medicines supply and management officer shall inspect all patient care areas in the
center, where medicines intended for administration to patients are stored, dispensed,
or administered at least once every two months. The pharmaceutical service shall
maintain a record of the inspections and action taken for identified problems.
6.10.1.103. A quality improvement program of the pharmaceutical service shall monitor, at a
minimum, the use of medicines, including medication errors and use of antibiotics.
Serious or consistent patterns of medication error shall be reported to the drug and
therapeutics committee or its equivalent for correction and this must be documented
6.10.2. Premises
6.10.2.1. The design and layout of the pharmacy shall permit a logical flow of work, effective
communication and supervision and ensure effective cleaning and maintenance and
must minimize the risk of errors, cross-contamination and anything else which would
have an adverse effect on the quality of medicines and service delivery.
6.10.2.2. The area(s) of counseling shall be arranged or constructed in such a manner that it
provides adequate space, have professional look and ensure reasonable privacy to the
patient at all times and eliminate background noise as much as possible.
6.10.2.3. Dispensing counter &/ or counseling area shall be designed to secure patient privacy
and confidentiality.
6.10.2.4. All parts of the pharmacy premises shall be maintained in an orderly and tidy condition.
6.10.2.5. Entrances, dispensing counters and doorways shall be accessible to persons with
disability.
6.10.2.6. The dispensing environment (dispensing counter and counseling area) shall ensure
confidentiality and allow simultaneous service delivery for multiple customers by
multiple providers.
6.10.2.7. The pharmacy premises shall be clearly demarcated and identified from the premises of
any other business or practice. The pharmacy shall be secure from theft & any other
disaster like fire & flood.
78
6.10.2.8. A procedure shall be in place to ensure access to pharmacy premises in an emergency
situation.
6.10.2.9. The ceiling height of the pharmacy store shall not be less than 2.6m. This height
requirement shall increase depending on the climatic condition of the area
6.10.2.10. The wall and floor shall be constructed to protect the safety of pharmaceuticals from
burglary, rodents, direct sunlight, moisture and others.
6.10.2.11. Medicines shall be shelved a minimum of 20cm above the floor, 1m wide between
shelves and 50cm away from the wall and ceiling. If pallets are used, there shall be 20cm
above the floor, one meter between pallets and 50cm away from the wall.
6.10.2.12. The pharmacy premises shall have the following minimum space at different service
delivery points.
a) Waiting area
b) Inpatient dispensing room, as appropriate
c) Outpatient dispensing with counseling room
d) Emergency dispensing room/lockable cabinet with shelve
e) Compounding room, as appropriate
f) Cold room, optional
g) Medicine information center room(s), as appropriate
h) Cashier room
i) Medical store intended for medicines, vaccines, lab reagents and medical
equipment storage
j) Office and duty room
k) Staff toilet (female and male)
6.10.2.13. In general, minimum standard for pharmacy premises for different specialty center shall
be as indicated in their respective standards
6.10.3. Professional
6.10.3.1. The pharmacy service shall be directed by a licensed pharmacist with a minimum of two
years work experience.
6.10.3.2. The dispensing of all prescriptions and medication use counseling shall be carried out by
licensed pharmacists.
6.10.3.3. The center shall have one additional pharmacist
6.10.3.4. In addition, the center may have additional licensed pharmacists based on workload
analysis.
79
6.10.3.5. The center shall have a pharmacy technician for the central medical store and inventory
management
6.10.3.6. The pharmacy service shall have support staff such as clerks, porters and cleaners.
6.10.4. Products
6.10.4.1. The pharmacy in Specialty center shall have medicine lists within the framework of the
national medicine list prepared by the regulatory authority.
6.10.4.2. There shall be adequate, suitable dispensing equipment in the dispensary.
6.10.4.3. The Specialty center shall have central medical store equipped with fire extinguisher,
refrigerators, deep freezers and racks/shelves.
6.10.4.4. The Specialty center pharmacy shall be provided with continuous supply of electricity,
telephone access.
6.10.4.5. In general, minimum standard for pharmacy equipment and facilities shall be as follows.
Equipment and facilities
a) Refrigerators b) Deep freezer c) Refrigerator
Thermometerd) Tablet counter e) Scientific calculator f) Table and chair
g) Scissors h) Adult weighing scalei) Room thermometer j) Balance k) Telephone line l) Access to water, toilet
and shower
6.10.4.6. In cases when the center has center based pharmaceutical preparation services, the
following additional products shall be available
a) Working bench: Level, smooth, impervious, free of cracks and crevices and non-
shedding; covered with protector sheets of plastic, rubber or absorbable paper
when appropriate
b) Mortar and pestle: 250 ml capacity or more; glass type and porcelain type
c) Water distiller: Stainless steel of 20 liter capacity or more
d) Water bath: Stainless steel of 4 openings or more
e) Electrical hotplate: Various Sizes and Features
f) Evaporating dish: Stainless steel (glazed inside) and porcelain type; with/without
handling
g) Spatula: Stainless steel and plastic type, flexible and non-flexible, different blade
lengths
80
h) Gloves: disposable, non-sterile
i) Glass rod: Different length and thicknesses
j) Wash bottle: 250ml capacity, polyethylene
k) Funnel: Glass type and plastic type (polyethylene)
l) Beakers: Glass type; different capacity
m)Volumetric flask: Glass type; different capacity
n) Balances: Prescription, torsion, manual triple beam, electronic; capacities of not less
than 300 gm; sensitivity of not less than 0.1 mg
o) Ointment tile: Glass type
p) Micropipettes: Glass type; different capacities (less than 1ml); with pipette bulb
q) Glass type; different capacities (1ml-100ml); with pipette bulb
r) Cylindrical graduate: Glass and plastic type; different capacity
s) Conical graduate: Glass and plastic type; different capacity
t) Weighing dishes: Plastic, aluminum, stainless steel type
u) Weighing paper: Normal paper; grease-proof for semisolids
81
6.11. Medical Recording 6.11.1. Practices
6.11.1.1. Medical record shall be maintained in written form for every patient seen at all
points of care.
6.11.1.2. The Specialty center shall maintain individual medical records in a manner to
ensure accuracy and easy retrieval. A patient shall have only one medical record
in the Specialty center.
6.11.1.3. If the patient received medical intervention while on ambulance, the medical
information of a patient during ambulance service including medication
administered shall be documented properly and attached into the medical
record,
6.11.1.4. The Specialty center shall establish a master patient index with a unique medical
number for each patient,
6.11.1.5. Each piece of paper or format that contains a patient medical information/
record shall carry the appropriate identification,
6.11.1.6. The Specialty center shall have a written policy and procedure which include at
least:
(a) Procedures for record completion,(b) Conditions, procedures, and fees for releasing medical information,(c) Procedures for the protection of medical record information against the loss,
tampering, alteration, destruction or unauthorized use.6.11.1.7. When a medical record is taken out until returned to the record room it shall be
documented to create a good tracking mechanism.
6.11.1.8. Any medical record shall be kept confidential, available only for use by
authorized persons or as otherwise permitted by law.
6.11.1.9. All entries in the patient's medical record shall be written legibly in permanent
ink (blue or black color), dated, and signed by the recording person.
6.11.1.10. The medical record forms shall be prepared in line with the national HMIS
guidelines.
6.11.1.11. Each medical record shall at least contain the following information:
a) Identification (name, age, sex, address),
82
b) History, physical examination, investigation results and diagnosis,c) Medication, procedure and consultation notes,d) Name and signature of treating physician, date,e) Consent form where applicable which shall be signed by the patient. In case
where someone other than the patient signs the forms, the reason for the patient's not signing it shall be indicated on the face of the form, along with the relationship of the signer to the patient.
6.11.1.12. Any consent form for medical treatment that the patient signs shall be printed in
an understandable format and the text written in clear, legible and non-technical
language.
6.11.1.13. There shall be a mechanism for medical record controlling and tracing, whenever
patients medical records are taken from and returned to the central medical
record room.
6.11.1.14. There shall be a mechanism to make medical records with appointment ready for
use and return seen cards back to the central medical record room within 24hrs.
6.11.1.15. If death happens in the center, the necessary information of the patient's death
shall be documented in the patient's medical record upon death; date, time, any
intervention, etc.,
6.11.1.16. Original medical records shall not leave Specialty center premises unless they are
under court order or in order to safeguard the record in case of a physical plant
emergency or natural disaster.
6.11.1.17. If a patient or the patient's legally authorized representative requests in writing,
a copy of the medical record shall be given.
6.11.1.18. If the patient is provided with medical certificates, copies of certificates and
other records shall be documented and/or recorded on the original medical
record.
6.11.1.19. If the patient is transferred to another facility on a non emergency basis, the
Specialty center shall maintain a transfer record reflecting the patient's
immediate needs and send a copy of this record to the receiving facility.
6.11.1.20. If the Specialty center ceases to operate, the appropriate organ shall be notified
in writing about how and where medical record will be stored at least 15 days
83
prior to cessation of operation. The patient choice on where to transfer his/her
medical record shall be respected.
6.11.1.21. The Specialty center shall establish a procedure for removal of inactive medical
records from the central medical record room.
6.11.1.22. Medical records shall be destroyed as per the law by using techniques that
assures confidentiality of the medical records. However, records which are active
for more than ten years shall not be destroyed.
6.11.1.23. There shall be procedure for data collection, compilation, processing and
reporting system.
6.11.2. Premises
6.11.2.1. The premises for medical record room shall have enough space between and
around shelves. The medical records shall be shelved a minimum 10cm above the
floor.
6.11.2.2. The medical record room shall have adequate space to accommodate the
following:
(a) Central filing space,(b) Work space,
(c) Supply/ Storage area,(d) Archive space with shelves,
6.11.2.3. The medical record room shall have adequate light and ventilation.
6.11.2.4. There shall be fire extinguisher kept in a visible and identified place in the
medical record room,
6.11.2.5. There shall be a room/ place for archiving dead files until they are permanently
destroyed
6.11.3. Professionals
6.11.3.1. There shall be full-time assigned custodian/ medical record personnel with basic
computer skill and ability to organize medical records for medical records
management.
6.11.3.2. The Specialty center shall provide basic training on medical record keeping to all
medical record unit staff.
6.11.4. Products
6.11.4.1. The Medical record room shall have:
(a) Shelves, (b) Table,
84
(c) Master patient index boxes,
(d) Log books,(e) Patient folders,(f) Computer,
(g) printer(h) Cart (i) Ladder & Fire
extinguisher
85
6.12. Rehabilitation Services 6.12.1. Practices
6.12.1.1. This standard shall be applicable to orthopedic center, cardiac center, and
neurology center. Other centers may provide this service as per this standard.
6.12.1.2. At least physical therapy/ physiotherapy services shall be available in the
Specialty center if rehabilitation service is available.
6.12.1.3. There shall be specific treatment and/or procedure protocols for each service
available and rendered in the unit,
6.12.1.4. There shall be training service for patients on copping disability. It includes
utilization of prostheses, orthoses, wheelchairs, walking aids.
6.12.1.5. There shall be a protocol or policy for safety and ethical practice of physical
therapy that complies with the six precepts for health care (safe, effective,
patient-centered, timely, efficient and equitable).
6.12.1.6. There shall be patient education on prevention of:
(a) pressure sores in clients with sensory loss,(b) contractures in clients with limb and/or trunk paralysis,(c) phantom limb pain for amputees,
6.12.2. Premises
6.12.2.1. There shall be at least one physically separated room or area for rehabilitation
and therapy.
6.12.2.2. The premises shall be friendly to disabled people and smooth pavement rail for
wheelchairs.
6.12.2.3. There shall be enough space for assistive devices and appropriate accessories.
6.12.2.4. Private area for patients and staff when they need to change clothing before and
after treatment shall be available.
6.12.2.5. The premises shall respect visual and auditory privacy of patients.
6.12.3. Professionals
6.12.3.1. The service shall be directed by a licensed physiotherapist,
6.12.3.2. Continued improvement of technical skills and knowledge shall be facilitated
through continuous medical education.
6.12.4. Products
86
6.12.4.1. Equipment shall be stored in a safe and accessible place and shall not be stored in
a public walkways and hallways.
6.12.4.2. Standard equipments and consumables which shall be available for rehabilitation
service in specialty center include:
(a) Physiotherapy mats(b) Massaging couch,(c) Splinting materials,(d) Balance boards(e) Mirror(f) Sticks(g) Crutches(h) Walking frames
(adjustable)(i) POP cutter(j) Pulley (k) Chair and table (l) Plastic apron
(m) Infrared,(n) Ultraviolet/ blue lamp,(o) Muscle stimulator,(p) Ultrasound therapy
equipment,(q) Electro-massage
apparatus for hands, legs, spine,
(r) Disposable glove(s) Cotton roll(t) POP
87
6.13. Ambulance Service standards 6.13.1. Practice
6.13.1.1. The ambulance service shall be provided to every emergency patient who needs
the service without any prerequisite and discrimination.
6.13.1.2. The ambulance service shall be available 24 hrs a day and 365 days a year,
6.13.1.3. The ambulance service shall provide the following services to patients with
urgent need of medical attention or in a medical emergency.
a) Transportation service from the Specialty center to other health facilitiesb) Clinical examinations including brief history, vital signs, very pertinent
physical examination and glucose test when needed c) Clinical life saving support that includes:
Fluid resuscitation Bleeding control Air way cleaning , oxygen administration, severe asthma management Attending labor Immobilizing a fracture Providing anti-pain Managing seizure Providing emergency medicines like adrenaline, hydralazine, glucose
etc6.13.1.4. The ambulance service shall comply with the patient rights standards stated
under this standard.
6.13.1.5. Up on arrival to the Specialty center the ambulance staff shall transfer the patient
to the emergency service. The handover of patients shall be accompanied by a
written document which at least includes identification, date, time and services
provided until arrival to the Specialty center.
6.13.1.6. If death happens on the way to a Specialty center, the dead body shall be taken to
this specialty center and death shall be confirmed. Dead body care shall be
provided as per the standards stated under the morgue service standard.
6.13.1.7. Ambulances of the Specialty center shall serve only for designated emergency
medical services
6.13.1.8. After providing a service the vehicle shall be cleaned and disinfected

88
6.13.1.9. The ambulance kit shall be checked every time after providing the service
6.13.2. Professionals
6.13.2.1. Minimum standards for personnel of the ambulance service shall include:
(a) A nurse to be pulled from emergency service unit,(b) Licensed driver,(c) Cleaner to be pooled from Emergency service for managing disinfection of the ambulance,
6.13.2.2. The nurses shall be trained on emergency medical services,
6.13.2.3. The driver shall be oriented on emergency situation management,
6.13.3. Products
6.13.3.1. The Specialty center shall avail ambulance car which shall have adequate space
for accommodating the following whenever required:
(a) A foldable stretcher(b) Ambulance Bed (couches) with security belts, fixed chair that is designed
for ambulances(c) One family attendant (d) At least one nurse(e) Medical box for items needed for providing immediate life saving support.(f) Log book (stating time of call, time of arrival, time of return)
6.13.3.2. The vehicle shall be labeled and have siren and emergency light.
6.13.3.3. The vehicle shall have adequate internal light and ventilation.
6.13.3.4. The vehicle shall fulfill requirements of road transport authority.
6.13.3.5. Ambulance kit:
(a) Medicines: Anti pains, Adrenaline inj., Hydralazine inj., IV fluids (all types),
Dextrose 40%, Diazepam inj., Phenytoin inj., Atropine inj.
(b) Supplies IV cannula, IV stand, syringe with needle, tourniquet, plaster, gauze,
bandage, spatula, antiseptic solution, catheters tourniquet
89
Personal protective devices (gown, mask, gloves, goggles)
Waste disposing containers
Support material for immobilization purpose
(c) Equipment: Minor surgical set, Oxygen supply, Ambu bag, suction machine, Stethoscope, sphygmomanometer, thermometer, Portable radio or
telephone,
Emergency tracheostomy (wide bore needle insertion),
air way, laryngeal mask, intubation set, Glucometer,
90
6.14. Health Promotion Services6.14.1. Practices
6.14.1.1. The Specialty center shall plan, schedule, coordinate, lead and monitor a
minimum of specialty center specific health promotion activities.
6.14.1.2. The Specialty center shall make sure that health promotion practice provides
unbiased and evidence based information.
6.14.1.3. Patient education shall be customer focused.
6.14.1.4. The health promotion activity of the center shall respect the national health
policy, legislations, protocols and directives.
6.14.2. Premises
6.14.2.1. The center shall have the following minimum premises requirements
a) Waiting areas suitable for health educationb) Meeting hall
6.14.3. Professionals
6.14.3.1. A health professional shall be designated to coordinate health promotion
activities.
6.14.3.2. The roles and responsibilities of the designee in relation to health promotion
shall be specified in his/her job descriptions.
6.14.3.3. Health professionals shall provide health education in their specific discipline.
6.14.4. Products
6.14.4.1. The Specialty center shall have the following health promotional materials:
a. Information desk with Printed materials (Posters, Brochures, Leaflets, News paper, Health bulletin)
b. IEC materials,c. Audio visual materials: TV,
VCD/ DVD, Radio, Tape-recorder,
d. Public health journals(Optional)
e. Internet (Optional)
91
6.15. Morgue Services 6.15.1. Practices
6.15.1.1. The Specialty center shall have written policies and procedures for dead body
care services. These policies shall delineate the responsibilities of the medical
staff and nursing staff and shall include procedures for at least the following:
a) Identification of the body, recording and labeling,b) Safe and proper handling of the body to prevent damage and this shall be
according to the patient religion and culture,c) Treatment of the dead body with formalin,d) Safeguarding personal effects of the deceased and release of personal
effects to the appropriate person,e) Proper handling of toxic chemicals by morgue and housekeeping staff, f) Infection control, including disinfection of equipment as per IP standard, g) Identifying & handling high-risk and/or infectious bodies, h) Release of the body to the family shall be as immediately as possible,
6.15.1.2. There shall be a death certificate issued by authorized medical practitioner for
each death and this shall be documented.
6.15.1.3. The specialty center shall provide the necessary care for dead body until
delivered to the relatives/ care givers.
6.15.1.4. The service shall be available for 24 hours a day and 365 days of a year.
6.15.1.5. Any dead body shall be sent to/ pass through morgue after death confirmation.
6.15.1.6. Dead body discharge shall be through the morgue exit.
6.15.2. Premises
6.15.2.1. The morgue premises at specialty center shall fulfill at least the followings:
(a) Dead body care & stay room,(b) Adequate Water supply,(c) Well ventilated, (d) Adequate supply of light,(e) Hand wash sink,(f) Secured with locks, (g) Attendant office
6.15.2.2. The morgue premises shall be secured and provided with lock.
6.15.3. Professionals
92
6.15.3.1. The morgue service shall have the following designated personnel:
(a) Morgue attendant, (b) Cleaner.
6.15.4. Products
6.15.4.1. The center shall have at least two couches (double deck if possible).
6.15.4.2. The center shall have body refrigerator which shall be maintained at
temperatures between 0° and 6.6°C (32° and 45° Fahrenheit) and shall have an
automatic alarm system that monitors the temperature.
6.15.4.3. In addition, the following products shall be available for morgue services:
(a) Plastic sheets(b) Stretcher(c) Formalin(d) Syringe with needle(e) Detergents (f) Cotton(g) Gloves(h) Aprons(i) Boots
(j) Gowns(k) Head cover(l) Goggles(m) Disinfectants(n) Plastic bags(o) White loose fabric/ clothes(p) Body table with hot and cold
water sink(q) Cupboard
93
6.16. Infection Prevention 6.16.1. Practices
6.16.1.1. All activities performed for infection prevention shall comply with the national
infection prevention guidelines.
6.16.1.2. Infection prevention and control shall be effectively and efficiently governed and
managed.
6.16.1.3. The Specialty center shall identify the procedures and processes associated with
the risk of infection and shall implement strategies to reduce infection risk.
6.16.1.4. The Specialty center shall perform the following infection risk-reduction
activities:
a) equipment cleaning and sterilization in particular invasive equipmentb) laundry and linen managementc) disposal of infectious waste and body fluidsd) handling and disposal of blood and blood componentse) kitchen sanitation and food preparation and handlingf) Operation of the mortuary and postmortem area;g) disposal of sharps and needlesh) separation of patients with communicable diseases from patients and staff
who are at greater risk due to immune-suppression or other reasonsi) management of hemorrhagic (bleeding) patients j) Engineering controls, such as positive ventilation systems, biological
hoods in laboratories and thermostats on water heaters.6.16.1.5. The following written policies and procedures shall be maintained:
a) Hand hygiene Standard precautions for hand hygiene Personal protective measures Monitoring and surveillance of hand hygiene practices
b) Transmission-based precautions Contact precautions Droplet precautions Airborne precautions
c) Post-Exposure Prophylaxis programming (PEP) for some communicable diseases like rabies, HIV, meningitis Standard precautions to follow PEP policy
94
Procedures for PEP d) Environmental infection prevention
General Specialty center hygiene Structural infection prevention Physical Specialty center organization
e) Waste management Cleaning medical instruments Implementation of a disposal system Handling medical waste Waste removal
6.16.1.6. The following specific standard precautions shall be practiced and the Specialty
center shall have its own guidelines:
a) Hand hygiene shall be performed after touching blood, body fluids, secretions, excretions, and contaminated items, both immediately after removing gloves and between patient contacts. Thorough hand washing Use disinfectants Standard procedure for using anti-septic cleaner
b) The Specialty center staff shall consider that every patient is infectious c) The Specialty center shall have personal protective equipment such as
gloves, mask, eye protection (goggles) and face shield Gloves shall be worn in the following situations but not limited to:
o When there is direct contact with exposed wounds, blood, body fluids, body organs or any type of lesion.
o When drawing blood or handling medical instruments involved with invasive procedures (catheters, IV insertion, probes, etc.).
o When there is contact with a patient who might be infectious.o When handling contaminated items.o When cleaning patient areas.
Gowns shall be worn when but not limited to:o Performing surgical procedures,o Splattering of blood or body fluids is possible,o Handling bulk soiled linen (housekeeping),o Performing waste collection for infectious waste,o Handling any type of medical waste, o Conducting Specialty center laundry washing.
Masks, goggles, or other types of face shields shall be worn when but not limited to:
o Splattering of blood or body fluids to the face is possible,
95
o Handling biohazardous and soiled linenso Performing waste collection for hazardous or non-hazardous
waste.d) Soiled patient-care equipment, textiles and laundry shall be handled
appropriately e) Any type of face shield that is apparently soiled or splattered with body
fluids shall be washed and sterilized with a disinfectant.f) Procedures shall be developed and implemented for routine care,
cleaning, and disinfecting environmental surfaces, especially frequently touched surfaces in patient care areas.
g) Used needles shall not be recapped, bent, broken, or manipulated by hand. Single handed scoop technique shall only be used when recapping is required.
h) Safety features shall be used when available and used "sharps" shall be placed in a puncture-resistant container specially designated bin for hazardous waste.
6.16.1.7. There shall be transmission-based precautions and the Specialty center shall
have its own guideline for the followings:
a) Contact precautions Shall be intended to reduce the risk of transmission through direct and
indirect contact with an infectious patient. Shall be used when a patient is known to have a specific disease that is
easily transmitted by direct contact. Shall be used for known multi-drug resistant disease, such as some
forms of TB. Shall exercise strict barrier precautions for any type of contact with the
patient and their surrounding environment. Do not share medical equipment between patients Clean surfaces near patients daily Wash linens and surfaces after patient discharge Clean medical equipment
b) Droplet precautionsc) Airborne precautions (for diseases like SARS ,TB, Swine flu, etc)
Isolation room Negative pressure in relation to surrounding areas A minimum of 6-9 air exchanges per hour Air discharged outside the building and away from intake ducts, or
through a high-efficiency filter if re-circulated Door kept closed whether or not patient is in the room
96
After discharge door kept closed until sufficient time has elapsed to allow removal of airborne organisms
Patient confined to room Room shall have toilet, hand washing and bathing facilities
6.16.1.8. Each Specialty center site shall train all staff on how to minimize exposure to
blood-borne diseases. These include:
a) Immediate first aid b) Reporting exposuresc) Assign area for starter packs 24-hours access per day d) Counseling and testing for exposed staffe) Reporting and monitoring protocols f) Evaluate PEP program
6.16.1.9. The infection prevention committee or designate shall have written protocols,
procedures and shall oversee the following activities and this shall be
documented:
a) Developing the health facility annual infection prevention and control plan with costing, budgeting and financing
b) Monitoring and evaluating the performance of the infection prevention program by assessing implementation progress as well as adherence to IPC practice
c) Conducting surveillance to monitor nosocomial infections, antimicrobial use and outbreaks of infectious diseases.
d) Formulating a system for surveillance, prevention and control of nosocomial infections.
e) Reviewing surveillance data, reporting findings to management and other staff and identifying areas for intervention
f) Assessing and promoting improved IPC practice within the Specialty center
g) Developing an IEC strategy on IP for health-care workers h) Ensuring the continuous availability of supplies and equipment for patient
care managementi) Monitoring, providing data and measuring the overall impact of
interventions on reducing infection risk6.16.1.10. The Specialty center shall provide regular training on infection prevention and
control practice to staff, patients and as appropriate, to family and caregivers
6.16.1.11. The following training guidelines shall be available
a) Prevention of the spread of infections
97
b) Improving the quality of patient carec) Promoting safe environment for both patients and staff
6.16.1.12. The Specialty center shall have procedures in place to minimize crowding and
manage the flow of visitors. This shall include
a) Patient crowd controlb) Assess urgent and non-urgent casesc) Patient sign-in d) Caregiver and visitor control.
6.16.2. Premises
6.16.2.1. The center shall have a dedicated office for IP officer,
6.16.2.2. The center shall have a room or area for temporary storage of waste containers,
6.16.2.3. The Specialty center shall have a centralized sterilization room as per the
surgical service standards.
6.16.2.4. The center shall have incinerator with ash and burial pits.
6.16.2.5. The center may have placenta pit (Mandatory for MCH center).
6.16.3. Professionals
6.16.3.1. The Specialty center shall have a designated staff to serve as IP infection
prevention and control officer.
6.16.3.2. The officer shall be a licensed infectious diseases specialist or IP trained health
professional (physician or health officer or nurse), or a public health specialist
knowledgeable of infection prevention principles and health care epidemiology.
6.16.4. Products
6.16.4.1. The Specialty center shall have the following adequate supplies and equipment
needed for infection prevention and control practice.
a) Waste management equipment and supplies: Safety boxes Garbage bins Wheelbarrows
Large garbage bin Plastic garbage bags
b) Cleaning Mop Bucket
Broom Dust mop
98
Cleaning cloth Detergent
Bleach
c) Laundry Washing machine Sink Washing basin Drying rack/line Dryers
Irons Trolley Detergent Bleach
d) Instrument processing: Autoclaves and steam
sterilizers Test strips Boiler Oven Storage shelves for the
medical equipment
Chemicals & disinfectants: 0.5% chlorine solution (diluted bleach)
Brushes (tooth brush for small items)
e) Hand hygiene Sinks (ward & other
areas) Water container with
faucet
Soap dispenser Alcohol based hand rub Personal Towels Paper Towels
f) Personal Protective Equipment Heavy duty glove Examination/ Surgical
glove Disposable glove Eye shield Goggle Visors Dust mask
Respiratory mask Other types of face mask
Plastic apron Other types Boots Nurse shoes Other protective shoes Caps Face shield
99
6.17. Sanitation and Waste Management6.17.1. Practices
6.17.1.1. Specialty center environment shall ensure the following conditions:
a) Clean sanitation and safe environment, b) Access to continuous, safe and ample water supply
6.17.1.2. There shall be written procedures to govern the use of sanitation techniques in
all areas of the Specialty center.
6.17.1.3. If the center has ground water source, there shall be a written policy and
procedures for ground water treatment,
6.17.1.4. Infectious and medical wastes shall be handled and managed according to the
recent Health Care Waste Management National Guidelines/Directives.
6.17.1.5. Infectious and non infectious medical waste contained in disposable containers
shall be placed temporarily for disposal or transport in leak proof drums, pails or
portable bins. The containment system shall be leak proof, have tight-fitting
covers and be kept clean and in good repair.
6.17.1.6. Reusable containers for infectious medical waste and general medical waste shall
be thoroughly washed and decontaminated each time emptied according to the
recent Health Care Waste Management National Guidelines/Directives
6.17.1.7. Reusable pails, drums, or bins used for containment of infectious waste shall not
be used for containment of waste to be disposed of as noninfectious waste or for
other purposes except after being decontaminated by procedures described in
the latest Health Care Waste Management National Guidelines/Directives.
6.17.1.8. Placenta disposal pit shall be available in the Specialty center where the service
is applicable. The pit shall be secured and shall be protected, secured and with
properly fitting cover.
6.17.1.9. Segregation of health care waste shall includes the following procedures:
a) Separate different types of waste as per the guideline,b) The Specialty center shall provide colored waste receptacles specifically
suited for each category of waste,c) Segregation shall take place at the source, like ward bedside, OR, laboratory
etc.
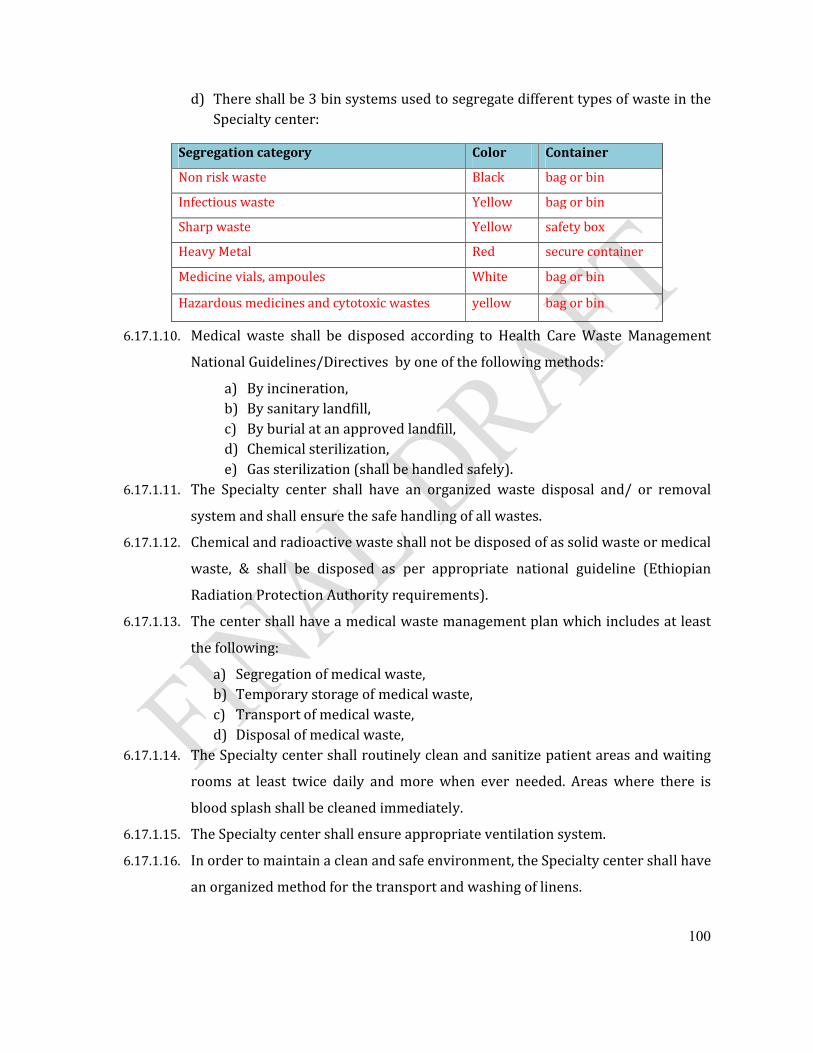
100
d) There shall be 3 bin systems used to segregate different types of waste in the Specialty center:
6.17.1.10. Medical waste shall be disposed according to Health Care Waste Management
National Guidelines/Directives by one of the following methods:
a) By incineration, b) By sanitary landfill, c) By burial at an approved landfill, d) Chemical sterilization, e) Gas sterilization (shall be handled safely).
6.17.1.11. The Specialty center shall have an organized waste disposal and/ or removal
system and shall ensure the safe handling of all wastes.
6.17.1.12. Chemical and radioactive waste shall not be disposed of as solid waste or medical
waste, & shall be disposed as per appropriate national guideline (Ethiopian
Radiation Protection Authority requirements).
6.17.1.13. The center shall have a medical waste management plan which includes at least
the following:
a) Segregation of medical waste,b) Temporary storage of medical waste,c) Transport of medical waste,d) Disposal of medical waste,
6.17.1.14. The Specialty center shall routinely clean and sanitize patient areas and waiting
rooms at least twice daily and more when ever needed. Areas where there is
blood splash shall be cleaned immediately.
6.17.1.15. The Specialty center shall ensure appropriate ventilation system.
6.17.1.16. In order to maintain a clean and safe environment, the Specialty center shall have
an organized method for the transport and washing of linens.
Segregation category Color Container
Non risk waste Black bag or bin
Infectious waste Yellow bag or bin
Sharp waste Yellow safety box
Heavy Metal Red secure container
Medicine vials, ampoules White bag or bin
Hazardous medicines and cytotoxic wastes yellow bag or bin
101
6.17.1.17. Housekeeping items shall be cleaned and sanitized regularly.
6.17.1.18. The center shall have Sewage disposal plan which shall fulfill the following
conditions (according to Health Care Waste Management National
Guidelines/Directives):
a) A functional sewerage system,b) Dispose of sanitary waste through connection to a suitable municipal
sewerage system, c) Flush toilet system,d) A designated waste storage room for solid waste &/ or a septic tank for
liquid waste,e) Written procedures defining instrument processing procedures
(disinfection and sterilization).f) All fixtures located in the kitchen, including the dishwasher, shall be
installed so as to empty into a drain which is not directly connected to the sanitary house drain.
g) Kitchen drain shall empty into a manhole or catch basin having a perforated cover with an elevation of at least 24 inches below the kitchen floor elevation, and then to the sewer.
6.17.1.19. The center shall have Plumbing system that fulfill the following conditions:
a) An approved municipal water system,b) An approved method of supplying hot water, c) Supply piping within the building shall be according to the requirements
in the standard mentioned under the physical facility, 6.17.1.20. The center shall have Catering hygiene that fulfill the following conditions:
a) There shall be a procedure for management of pest control, restriction of animal entry (eg. cats, dogs etc), posted in a visible area in the kitchen.
b) There shall be a system for regular screen and control of the health of kitchen personnel.
c) The health of kitchen personnel shall be controlled for: Personal hygiene including uniform (protective clothes), Periodical medical check-up for acute and chronic diarrhea and
other infectious diseases, Kitchen personnel with infected open skin lesions, communicable
diseases shall not be allowed to work as kitchen personnel until confirmed safe.
6.17.1.21. The Specialty center shall have the following supportive sanitation measures:
a) Clean water where there is no plumbing,
102
b) Hand hygiene practice, c) Sterilization of medical instruments,d) Isolating infectious patient in special isolation room,e) Alternatives to protective equipment.
6.17.2. Premises
6.17.2.1. Placenta disposal pit shall have a dimension of 1m X 1m and 2m deep. Lateral to
the disposal pit, the two sides shall be filled with concrete. The top shall be made
of concrete with raised opening & cover.
6.17.2.2. The Specialty center sanitary system shall have:
a) Adequate flushing toilets and hand washing basins, b) Plumbing setup stores,c) Sanitary office,d) Incinerator (if it is allowed to centers by the national waste management
and disposal directives),a) Plot of land for Safe ash pit, Burial pit, Garbage bins,e) Secured area for solid waste accumulation.
6.17.3. Professionals
6.17.3.1. Specialty center sanitation service shall be administered by environmental
health professional together with infection prevention activities.
6.17.3.2. The Specialty center shall have the following personnel to conduct sanitation
activities:
a) Housekeeping staff such as cleaners and waste handlers,b) Gardeners,
6.17.3.3. The Specialty center shall officially designate staff in charge of handling waste on
a regular basis.
6.17.3.4. The assigned staff shall be responsible for the collection and disposal of waste
products in the Specialty center.
6.17.3.5. Continuing education shall be provided to all personnel engaged in sanitation
activities on the relevant procedures.
6.17.3.6. Staff shall be oriented on personal protection methods.
6.17.4. Products
103
6.17.4.1. The Specialty center shall have equipment and supplies required for sanitation
activities. Required equipment and supplies includes:
a) Incineratorb) Safety boxes c) Leak proof containers for wasted) Trolley to transport wastee) PPE (personal protective equipments)f) Steam or dry Autoclave,g) Pressure cooker/dry oven.h) Cleaning supplies (detergents, disinfectants and other cleaning solutions
etc).i) Laundry washers,j) Laundry dryers,k) Mops and dust bins
104
6.18. Food and Dietary Services6.18.1. Practices
6.18.1.1. The Specialty center shall provide nutritionally adequate meals, supplemental
food supplies for inpatients and staffs on duty.
6.18.1.2. The dietary service shall be available for 24 hours a day and 365 days a year.
6.18.1.3. The dietary service activities shall be managed by a dietician or a catering chief.
6.18.1.4. The center shall ensure that there is good food hygiene practices along the
preparation process
6.18.1.5. The dietary service shall have written policies and procedures for all dietary
services which at least includes:
a) Purchasing, preparation and handling, b) Meal distribution, c) Handling special diet order,d) A diet manual detailing nutritional and therapeutic standards for meals and
snacks, and a nutrient analysis of menus.e) Nutritional assessment guide for patients' nutritional needs for food and
food supplements.6.18.1.6. An updated diet menu shall be available at each nurse’s station and in the dietary
service unit.
6.18.1.7. There shall be a policy to promote the participation of the dietary service in
meetings of multidisciplinary health care teams.
6.18.1.8. New admissions shall be listed for the dietary service according to the order.
6.18.1.9. The patient's diet shall be documented in the medical record. Documentation of
diet instructions shall include a description of:
a) The diet instruction provided to the patient and/or responsible person.b) Patient response, participation and understanding.c) Written instructional material provided to the patient and/or responsible
person.6.18.1.10. Diets shall be prepared in conformity with the Specialty center's dietary manual/
menu.
6.18.1.11. The dietary service shall follow the policies and procedures developed by the
drug and therapeutics committee regarding possible food/drug interactions.
105
6.18.1.12. At least three meals (breakfast, lunch and dinner) shall be served daily, and not
more than 15 hours shall elapse between dinner and breakfast.
6.18.1.13. Nourishment may be provided between meals and at night.
6.18.1.14. Food production shall be sufficient in quantity and quality to meet nutritional
needs of individual patients.
6.18.1.15. Changes in diet orders made by the treating physician shall be effected by the
next mealtime.
6.18.1.16. There shall be a mechanism for evaluating admitted patients to ensure they are
being adequately nourished.
6.18.1.17. There shall be a mechanism for the dietary service to be informed if the patient
does not receive the diet that has been ordered, or is unable to consume the diet.
6.18.1.18. There shall be a mechanism for patients and their families to interact with the
dietary service.
6.18.1.19. Dietary instruction for patients with special dietary needs from the treating
physician shall be communicated to the dietary service.
6.18.1.20. The dietitian or the catering chief shall provide diet information to the Canteen
staff for appropriate selections of food items during purchase.
6.18.1.21. The dietitian or the catering chief shall provide nutrition information as
requested by the patient, family, or treatment team which includes:
a) diet instructions,b) written instructional material, c) community dietary referrals regarding special diets, d) current diet order,e) nutritional problems,f) appetite, g) nutritional counseling, h) comprehension of diet instruction,
6.18.1.22. The dietitian or catering chief shall provide dietary information to the
discharging patient as per the treating physician instructions or as planned by
the treatment team.
6.18.1.23. Diet instructions for Inpatients or discharged patients shall include educations
involving:
106
a) therapeutic or modified dietsb) food-drug interactionsc) nutritional care for certain diagnoses/conditionsd) recommendations for changes in diet order, e) treatment plan, f) significant food allergy (lactose, wheat gluten, Soya ,egg, dairy)
6.18.1.24. Nutrition consultations:
a) Nutrition consultations shall be completed immediately after general medical practitioner’s order.
b) Nutrition consultations shall be individual or group, and may include family and/or responsible person.
c) The dietitian or Specialty center catering chief shall determine the type and frequency of follow-up care after the initial consultation. Follow-up consultation may include evaluation of nutritional care, diet education, or other nutritional concerns.
6.18.1.25. Treatment Planning: Therapeutic goals related to nutritional needs shall be
based on the following standards
a) Standard Height/Weight Tablesb) Dietary Reference Intakesc) Nutrition-related laboratory valuesd) Body Mass Index for Adults
6.18.1.26. Diet Orders and Nutritional Supplements
a) General medical practitioner/health officer diet orders shall be legible, concise and written in an understandable manner. The following information shall be included in diet orders:
Patient Name Unit Date Specific diet order; including food allergies/intolerances General medical practitioner’s / health officer signature
b) Dietary services shall receive written notification of: New diet orders Change in diet order Discontinued or canceled diet orders Unit transfers Isolation or special trays
c) All written diet orders shall be sent to dietary services immediately.
107
d) Special requests for meals or supplemental foods shall be provided as ordered to accommodate alterations in diets or meal service schedules due to new admissions, personal dietary needs, or other circumstances.
e) Diabetic and Calorie-Controlled diet orders shall include the calorie level desired.
f) The dietitian or Specialty center catering chief shall recommend appropriate nutritional supplemental foods according to general medical practitioner/health officer orders.
g) An electronic or manual spreadsheet of all diet orders shall be maintained by the dietitian or Specialty center catering chief to provide a current resource of all regular and therapeutic diets.
h) Dietary and nursing services shall be responsible to ensure dietary compliance and quality nutritional care of patients receiving general medical practitioner/health officer-ordered diets.
6.18.1.27. There shall be appropriate food safety and sanitations to ensure safe food service
for the patients.
6.18.1.28. Dry or staple food items shall be stored at least 12 inches off the floor in a
ventilated room which is not subject to sewage or waste water back-flow, or
contamination by condensation, leakage, rodents or vermin.
6.18.1.29. All perishable foods shall be refrigerated at the appropriate temperature and in
an orderly food safety manner (cold and hot holding principle).
6.18.1.30. Each refrigerator shall contain a thermometer in good working order.
6.18.1.31. Foods being displayed or transported shall be protected from contamination.
6.18.1.32. Three compartments washing procedures and techniques shall be developed and
carried out in compliance with the national hotel and catering sanitary control
guideline.
6.18.1.33. All garbage and kitchen refuse which is not disposed of mechanically shall be
kept in leak proof non-absorbent containers with close fitting covers and be
disposed of routinely in a manner that will not permit transmission of disease, a
nuisance, or a breeding place for flies.
6.18.1.34. All garbage containers shall be thoroughly cleaned inside and outside each time
emptied.
6.18.1.35. Requests for alternative food supplies shall be considered on an individual basis.
108
6.18.1.36. Foods shall be transported and served as close to preparation/re-thermalization
time as possible. Maximum cold food temperatures shall be 5°C and minimum
hot food temperatures shall be 60° C at time of service.
6.18.1.37. Dietary services shall ensure prescribed diet compliance as well as minimize
food-borne illness.
6.18.1.38. Cancellations of ordered diets shall be made as soon as possible to avoid possible
spoilage and/or waste of food items.
6.18.1.39. The specialty center may provide dietary services by one of the followings:
a) In traditional configuration where the kitchen is located in the center
premise;
b) Provide the service directly, but may prepare the bulk of the meals in a
kitchen owned by the center, located off-site; and
c) Contract out for dietary services through an off-site vendor and the contract
shall be documented. However, regardless of how the center provides the
service, the center shall ultimately be responsible for meeting the dietary
service standards.
6.18.1.40. When dietary services are provided from an off-site location, the center shall be
responsible to ensure:
a) Compliance with the quality assurance system,
b) Compliance with the infection prevention standards
c) Compliance with the dietetic policies and procedures in regards to meal
service for off hours’ admissions, late trays, food substitutions, reasonable
meal schedules, posting of current menus in the center as well as in the off-
site kitchen, tray accuracy, food handling safety practices, emergency food
supplies and deliveries, staffing and patient satisfaction,
d) The presence of a current therapeutic diet manual approved by the dietitian
and medical staff,
e) The presence of nutritional assessment indicating nutritional needs are in
accordance with recognized dietary practices as well as with orders of the
practitioners responsible for the care of the patients.
109
6.18.1.41. In cases when this service is outsourced to a contractor, the center is responsible
to ensure contractor compliance with all the standards for food and dietary
services.
6.18.1.42. Catering hygiene shall fulfill the following conditions
a) There shall be guidelines for pest control and restricting the presence of
animals (eg. cats, dogs etc) visibly posted in the kitchen.
b) There shall be a system to screen and control the health of kitchen personnel.
c) The responsible kitchen personnel health shall be controlled for:
Personal hygiene including uniform (protective clothes)
Periodical medical check-up for acute and chronic diarrhea and other
infectious diseases
Those with infected open skin lesions are not allowed to work as kitchen
personnel.
6.18.2. Premises
6.18.2.1. The following minimum facilities shall be available for dietary services:
a) Food preparation room All cooking appliances shall have ventilating hood, Washing sink with three compartments:
o Dish washing sinko Pot washing sink o Cart cleaning sinko Can washing sink
b) Storage room c) Cart storage.d) Dietitian's office.e) Janitor’s closet f) Personnel toilets with hand washing facilities and lockers convenient to but
not in the kitchen.g) Approved automatic fire extinguisher system in range hood.h) Continuous electricity (power) supplyi) safe and adequate water supply
6.18.3. Professionals
110
6.18.3.1. The Specialty center shall have an organized dietary service unit directed by a
dietitian or catering chief (who has a basic education on dietetic sciences).
6.18.3.2. In addition the Specialty center shall have the following food handlers:
(a) Meal distributors,(b) Chief cook,(c) Kitchen workers,(d) Store keeper, (e) Bakers,(f) Dishwashers,
6.18.3.3. The number of personnel, such as cooks, bakers, dishwashers and clerks shall be
adequate to perform effectively all defined functions (based on workload
analysis).
6.18.3.4. There shall be procedures to control dietary employees with infectious and open
lesions (controlling personal hygiene).
6.18.3.5. Food handlers shall meet routine health examinations according to the Ethiopian
Food Handlers’ Hygiene Guideline for food service personnel.
6.18.3.6. There shall be an in-service training program on proper handling of food and
personal grooming to dietary employees.
6.18.3.7. All kitchen workers shall wear protective kitchen clothes according to the
Ethiopian Food Handlers’ Hygiene Guideline.
6.18.3.8. A dietitian or catering chief shall be a full-time employee.
6.18.3.9. Written job descriptions for all dietary employees shall be given and
documented.
6.18.4. Products
6.18.4.1. The following products shall be available for dietary services:
a) Refrigeratorb) Kitchen utensilsc) Potsd) Jarse) Dishesf) Knivesg) Pressure cooker/ dry ovenh) Oveni) Detergents
j) Stovesk) Cartsl) Working clothes m) apron, n) boots, o) hair cover, p) gown, q) hand gloves,r) Barrel (garbage)
111
6.19. Housekeeping, Laundry and Maintenance Services6.19.1. Practices
6.19.1.1. The housekeeping service shall have the following sanitary activities.
a) Basic cleaning such as dusting, sweeping, polishing and washingb) Special cleaning of
Different types of floors Wall & ceiling Doors & windows Furniture & fixtures Venetian blinds
c) Cleaning and maintenance of toilet.d) Water treatment, filtering & purification.
6.19.1.2. In the housekeeping service, the types and sources of offensive odors shall be
identified, controlled and removed immediately
6.19.1.3. Collection, transportation and disposal of Specialty center wastes shall be
supervised and controlled
6.19.1.4. The safety of fire, electrical and natural hazards in the risk areas in the Specialty
center shall be supervised and controlled and shall work closely with Specialty
center fire brigade and safety committee.
6.19.1.5. The designee/ sanitarian shall identify, supervise and organize the control and
eradication of pests, rodents and animal nuisance in the Specialty center.
6.19.1.6. The housekeeping staffs shall create pleasant environment to patients, staffs and
visitors
6.19.1.7. The housekeeping staffs shall ensure proper lighting and ventilation in different
Specialty center areas.
6.19.1.8. The following LINEN services shall be provided in the Specialty center
a) Maintain an adequate supply of clean linens at all times b) Obtain linen from stores and laundry.c) Ensure proper storage of linen.d) Supervise washing, sterilization in the laundry.e) Maintain linen properlyf) Issues linen in service units like wards.g) Keep proper accounting of linen.
112
h) Ensure proper sorting of linen.i) Understand different color scheme.
6.19.1.9. Regular surveillance of overhead and underground tank, proper cover, regular
chlorination and cleaning shall be undertaken
6.19.1.10. The infection control measures shall be carried out in accordance with the
Specialty center infection prevention standard
6.19.1.11. There shall be reserve electrical generator for power supply for continuous 24
hours.
6.19.1.12. Potable water and electrical services shall be available 24 hours a day and 365
days a year through regular or alternate sources.
6.19.1.13. There shall be a plant safety maintenance organization as described below:
a) A multidisciplinary safety committee that develops a comprehensive center-wide
safety program and reviewed.
b) A mechanism to report all incidents, injuries and safety hazards to the safety
committee.
c) The multidisciplinary safety committee shall review all reports and be responsible
for ensuring that all reports are referred appropriately and follow-up action is
documented.
6.19.1.14. Facility maintenance services
a) The building maintenance service shall have written policies and procedures that
are reviewed for routine maintenance, preventive maintenance and
renovation maintenance.
b) The standby emergency generator shall be checked weekly, tested under load
monthly, and serviced in accordance with accepted engineering practices.
c) Floors, ceilings, and walls shall be free of cracks and holes, discoloration, residue
build-up, water stains, and other signs of disrepair.
d) Routine inspections of elevators shall be conducted.
6.19.1.15. Construction and renovation
a) Whenever construction and renovation projects are planned in and around a health
care facility, a risk assessment shall be conducted to determine the impact of the
project on patient areas, personnel, and mechanical systems.
b) The infection control program shall review areas of potential risk and populations at
risk.
113
6.19.1.16. There shall be written protocols and procedures for medical equipment maintenance
including:
a) Plan for equipment maintenance (both preventive and curative), replacements,
upgrades, and new equipments
b) Safe disposal procedures
c) An effective tracking system to monitor equipment maintenance activity.
d) A monitoring method that ensures diagnostic equipment operates with
predicted specificity and sensitivity.
6.19.1.17. The maintenance personnel including the management of the center shall take
basic trainings on the following issues and this shall be documented.
a) Building fabrics and utilities
b) Building services and economics
c) Planning maintenance demand
d) Preventive and routine maintenance practice
e) Maintenance with regard to IP and hygiene
6.19.1.18. Fire and emergency preparedness
a) The center shall comply with the National Fire Protection standard
b) All employees, including part-time employees shall be trained in procedures to be
followed in the event of a fire and instructed in the use of fire-fighting equipment
and patient evacuation of center buildings as part of their initial orientation and
shall receive printed instructions on procedures and at least annually thereafter.
c) A written evacuation diagram specific to the unit that includes evacuation
procedure, location of fire exits, alarm boxes, and fire extinguishers shall be posted
conspicuously on a wall in each patient care unit.
d) Fire extinguishers shall be visually inspected at least monthly; fully inspected at
least annually, recharged, repaired and hydro-tested as required by manufacturer's
instructions; and labeled with the date of the last inspection.
e) Fire detectors, alarm systems, and fire suppression systems shall be inspected and
tested at least twice a year by a certified testing agency. Written reports of the last
two inspections shall be kept on file.
114
f) There shall be a comprehensive, current, written preventive maintenance program
for fire detectors, alarm systems, and fire suppression systems that includes regular
visual inspection. This program shall be documented.
6.19.1.19. Housekeeping equipment or supplies used for cleaning in isolation or
contaminated areas shall not be used in any other area of the center before it has
been properly cleaned and sterilized.
6.19.1.20. All areas of the center, including the building and grounds, shall be kept clean
and orderly.
6.19.1.21. There shall be frequent cleaning of floors, walls, woodwork and windows.
6.19.1.22. The premises shall be kept free of rodent and insect infestations.
6.19.1.23. Accumulated waste material and rubbish shall be removed at frequent intervals.
6.19.1.24. No flammable cleaning agents or other flammable liquids or gases shall be stored
in any janitor's closet or other area of the center except in a properly fire rated
and properly ventilated storage area specifically designed for such storage.
6.19.1.25. If the center does not have its own housekeeping, laundry and maintenance
services; it may have a contract agreement with external organizations. The
center shall check and maintain the sanitary standards of the center regarding
the processing of its linens and shall maintain a satisfactory schedule of pickup
and delivery.
6.19.1.26. If the center contract out for housekeeping, laundry and maintenance services
there shall be documentation for a contractual agreement.
6.19.1.27. In cases when the center outsources this service to a contractor, the standards
mentioned for housekeeping, laundry and maintenance shall be adhered by the
contractor.
6.19.2. Premises
6.19.2.1. If the center maintains its own laundry, it shall have separate areas for:
a) Collection of soiled linens.
b) Washing, drying and ironing.
c) Clean linen storage and mending area.
6.19.2.2. The laundry design and operation shall comply with the manufacturer’s
requirements and/or institutional sanitation guideline
115
6.19.2.3. Clean linen storage shall be readily accessible to nurses' stations
6.19.2.4. Dirty linen storage shall be well ventilated and shall be located convenient to the
laundry or service entrance of the center. The storage of appreciable quantities of
soiled linens is discouraged.
6.19.2.5. There shall be separate space provided for the storage of housekeeping
equipment and supplies
6.19.2.6. A separate office shall be available for the maintenance and the housekeeper.
6.19.2.7. Adequate space shall be available for service specific janitor’s closets and
cleaning equipment & supplies which shall be maintained separately for the
following areas (shall not be used for cleaning in any other location):
a) Surgical suites
b) Delivery suites
c) Dietary service unit
d) Emergency service unit
e) Patient areas
f) Laboratories, pharmacy, radiology, offices, locker rooms and other areas
6.19.2.8. Exits, stairways, doors and corridors shall be kept free of obstructions.
6.19.2.9. The center shall have an alternate emergency power supply. If such emergency
power supply is a diesel emergency power generator, there shall be enough fuel
to maintain power for at least 24 hours.
6.19.3. Professionals
6.19.3.1. The housekeeping, maintenance and laundry functions of the center shall be under the
direction of a licensed environmental health professional or engineer.
6.19.3.2. The designated officer shall plan, organize, co-ordinate, control and monitor all
housekeeping, maintenance and laundry activities.
6.19.3.3. The housekeeping, maintenance and laundry personnels shall take basic
trainings on the following issues and this shall be documented in their personal
profile.
a) Basic principles of sanitation and peculiarity to center environment.
b) Basic principles of personal hygiene
116
c) Basic knowledge about different detergent and disinfectants
d) Different cleaning procedures applicable to different treatment areas
e) Basic knowledge about cleaning equipments operation techniques and
their maintenance.
f) Different processes of water treatment & purification, removing bacteria.
g) Basic principles of ventilation, composition of air, air flow, humidity and
temperature.
h) Common types of odors and their sources of origin, identification and
control.
i) Removal and control technique of different types of odors.
j) Various equipments and materials used for odor control operation.
k) Medical waste, source and generation of waste
l) Hazards of medical waste to population and community.
m) Principles of collection of different types of medical wastes
n) Operational procedures of equipments
o) Safety measures in operation
p) Center lay out, configuration work, flow of men, material and equipment
in different areas. Air, water, noise, pollution, causes of pollution and their
control and prevention in center.
6.19.3.4. In addition the center shall have electrician, plumber, painter, building
maintenance technician, diagnostic equipment maintenance technician
6.19.4. Products
6.19.4.1. There shall be appropriate tools and testing equipments for medical equipment
maintenance, calibration and validation.
6.19.4.2. The center shall have the following tools, equipment & materials for
housekeeping services.
a) Reserve electrical generatorb) Floor cleaning brush air c) Floor wiping brush d) Hockey type brush e) Counter brush.
f) Ceiling brush g) Glass cleaning / wiping
brush.h) Scrappers i) Dustbins paddles.
117
j) Waste paper basket.k) Plastic Mug l) Plastic Bucket m) Plastic drum n) Wheel barrow o) Water trolley p) Ladder q) Scraping pump r) Spraying pump s) Flit pump.t) Rate trapping cage u) Gum boots v) Gown, Masks & Gloves w) Torch x) Manual sweeping machine.
y) Floor scrubbing/polishing machine
z) Wet vacuum cleaner.aa) Dry vacuum cleaner
portable bb) Fumigation machine
(Oticare) cc) Bed pan washer.dd) Cleaning material ee) Deodorants & disinfectantff) Laundry cleaning material gg) Insecticides &
rodenticideshh) Stain removal
118
6.20. Part-Time Health Services 6.20.1 After completing the usual working hour’s duties, the specialty center may arrange
part-time service delivery limited to those services stated on the license to operate a
specialty center.
6.20.2 The practices, premises, professionals and products required for part-time specialty
services shall be similar at a minimum to those standards stipulated for such
specialties under section seven of this document.
6.20.3 All other related services available in the center and appropriate to part-time
medical services shall be delivered during the part-time service schedule
6.20.4 The specialty center shall send a copy of part-time service provider’ license to the
appropriate organ and get approval before commencement of service delivery. In
cases, when the part-time services require advanced standards for practices,
premises, products and professionals, the center shall get approval from an
appropriate organ before commencement of the service delivery.
6.20.5 The specialty center shall post the available part-time services, the name of the
professionals rendering the service & the visiting hours in a visible area.
6.20.6 The specialty center shall maintain and update profiles of professionals providing
part-time services and the profile shall contain to a minimum:
a) Copy of professional license,b) Written contract agreement between the center and service provider,c) Permission from the appropriate organ d) Credentials
6.20.7 Part-time service delivery outside the scope of the specialty center is prohibited
(For instance, a part-time neurology service is not allowed in a gastroenterology
specialty center). However, the center may provide on call consultancy services to
admitted patients.
6.20.8 The specialty center shall be accountable for all part-time services provided in the
center’s premises.
119
SECTION SEVEN: SPECIALTY SERVICE STANDARDS
7.1. Maternal & Child Health (MCH) Center7.1.1. Practices
7.1.1.1. Comprehensive emergency obstetric care shall be available 24 hours a day, 365 days a year. This includes;a) Administration of antibiotics, oxytocin and anticonvulsantsb) Manual removal of the placentac) Removal of retained products following miscarriage or abortiond) Assisted vaginal deliverye) Blood transfusionf) Caesarean sectiong) Laparatomy
7.1.1.2. There shall be delivery service available for 24 hours a day, 365 days a year.7.1.1.3. The center shall have full-fledged pediatrics services as per standards stipulated
for pediatric specialty center except that this center has optional neonatology ICU.7.1.1.4. Pediatrics & Essential newborn care shall be available including with the
following: a) Newborn resuscitation,b) Routine examination for detection of congenital anomalies,c) Routine Immunization,d) Growth monitoring & Consultation on Nutrition and infant feeding,e) Assessment and treatment of sick babies,f) PMTCT services,g) Neonatology services with optional ICU care,h) Transfer or referral of neonates to next level neonatal unit, i) Follow up of babies and children with common chronic conditions like
diabetes, asthma, congenital problems and neurological problems.7.1.1.5. Gynecological services shall be available 24 hours a day, 365 days a year. 7.1.1.6. The MCH center shall provide the following functions for pregnant women:
a) Care of women in ambulatory basis,b) Ante Natal Care (ANC) service,c) Post Natal Care (PNC) service,d) Tetanus immunization e) Family planning service,f) Infertility work up and treatment,
7.1.1.7. The center shall have blood transfusion services with proper storage facilities and delivery/ transfusion protocol.
7.1.1.8. The MCH center shall have written policies and procedures that shall include:
120
a) Admission and discharge criteria for patients, b) Visitors policy that specifies the number of visitors permitted for each patient
at any time, c) Infection control specified under this standard,d) Monitoring and follow-up of patients,e) Transfer and referral of patients,
7.1.1.9. The MCH center shall avail updated reference materials, treatment guidelines and manuals,
7.1.1.10.Diseases under national surveillance shall be notified to the FMOH through the proper reporting channel.
7.1.2. Premises7.1.2.1. Labor room and delivery room shall be contiguous and shall have a means
(swinging or self-closing doors) for communication.7.1.2.2. The corridor to delivery room shall be spacious enough to allow easy transport of
laboring women with support.7.1.2.3. In addition to emergency and isolation, the specialty center shall have at least ten
inpatient beds.7.1.2.4. The nursery room shall have single entrance.7.1.2.5. Curtain tracks shall be installed around each bed, or in their absence bed screens
shall be provided.7.1.2.6. The Placental pit shall be well secured, protected from water and animals; the
outer part made of concrete; the opening shall be raised and not more than 20cmX20cm wide and provided with properly fitting cover.
7.1.2.7. The vaccination room shall organize the cold chain properly; refrigerator with monitors, cold boxes, vaccine syringes and diluents shall be kept in orderly.
7.1.2.8. The premises for MCH center shall be child friendly with play ground.7.1.2.9. The premise for MCH center shall have the following summarized rooms :
Rooms required # required
Area required
Reception, registration/ recording & waiting area
1 30sq. m
Emergency room with 2 resuscitation couches
1 16sq. m
Examination rooms with Gynecologic couch 1 12sq. m
Pediatric Examination room 1 12sq. m
Treatment/ injection room 1 12sq. m
Toilet rooms with hand washing basin 3 12sq. m
Minor OR/ Gynecologic procedure room, 1 20 sq. m
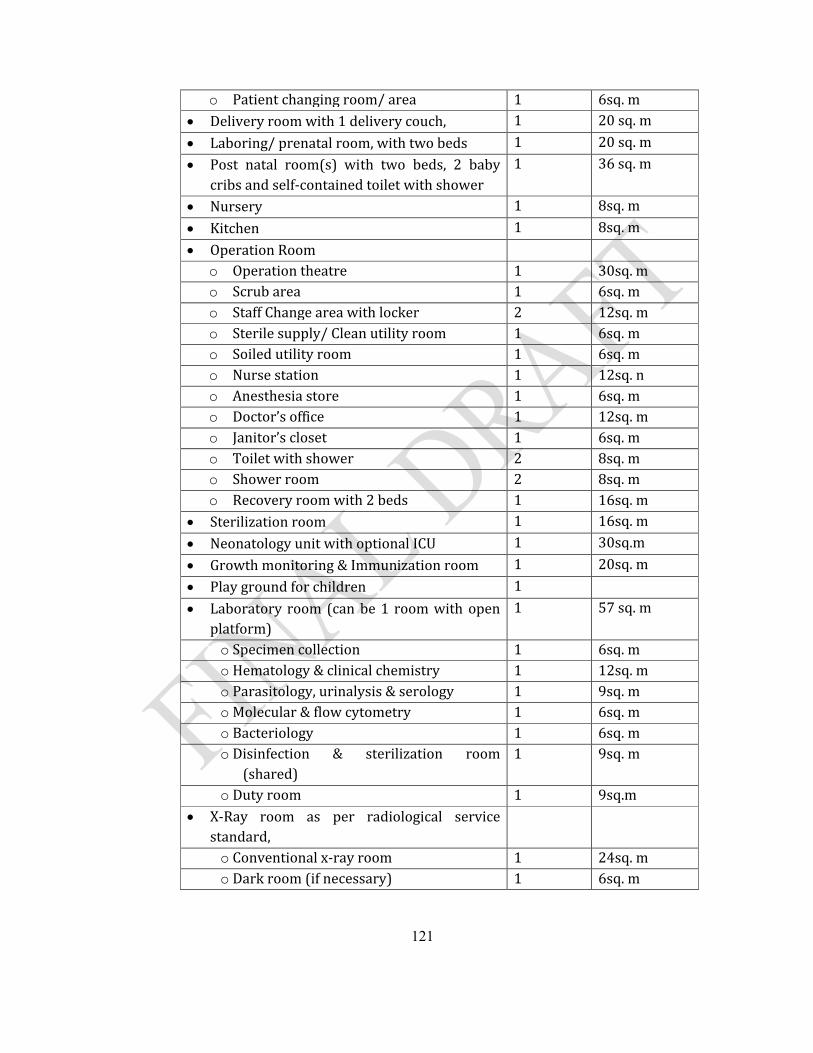
121
o Patient changing room/ area 1 6sq. m Delivery room with 1 delivery couch, 1 20 sq. m
Laboring/ prenatal room, with two beds 1 20 sq. m
Post natal room(s) with two beds, 2 baby cribs and self-contained toilet with shower
1 36 sq. m
Nursery 1 8sq. m
Kitchen 1 8sq. m
Operation Roomo Operation theatre 1 30sq. mo Scrub area 1 6sq. mo Staff Change area with locker 2 12sq. mo Sterile supply/ Clean utility room 1 6sq. mo Soiled utility room 1 6sq. mo Nurse station 1 12sq. no Anesthesia store 1 6sq. mo Doctor’s office 1 12sq. mo Janitor’s closet 1 6sq. mo Toilet with shower 2 8sq. mo Shower room 2 8sq. mo Recovery room with 2 beds 1 16sq. m
Sterilization room 1 16sq. m
Neonatology unit with optional ICU 1 30sq.m
Growth monitoring & Immunization room 1 20sq. m
Play ground for children 1
Laboratory room (can be 1 room with open platform)
1 57 sq. m
o Specimen collection 1 6sq. mo Hematology & clinical chemistry 1 12sq. mo Parasitology, urinalysis & serology 1 9sq. mo Molecular & flow cytometry 1 6sq. mo Bacteriology 1 6sq. mo Disinfection & sterilization room
(shared)1 9sq. m
o Duty room 1 9sq.m X-Ray room as per radiological service
standard, o Conventional x-ray room 1 24sq. mo Dark room (if necessary) 1 6sq. m
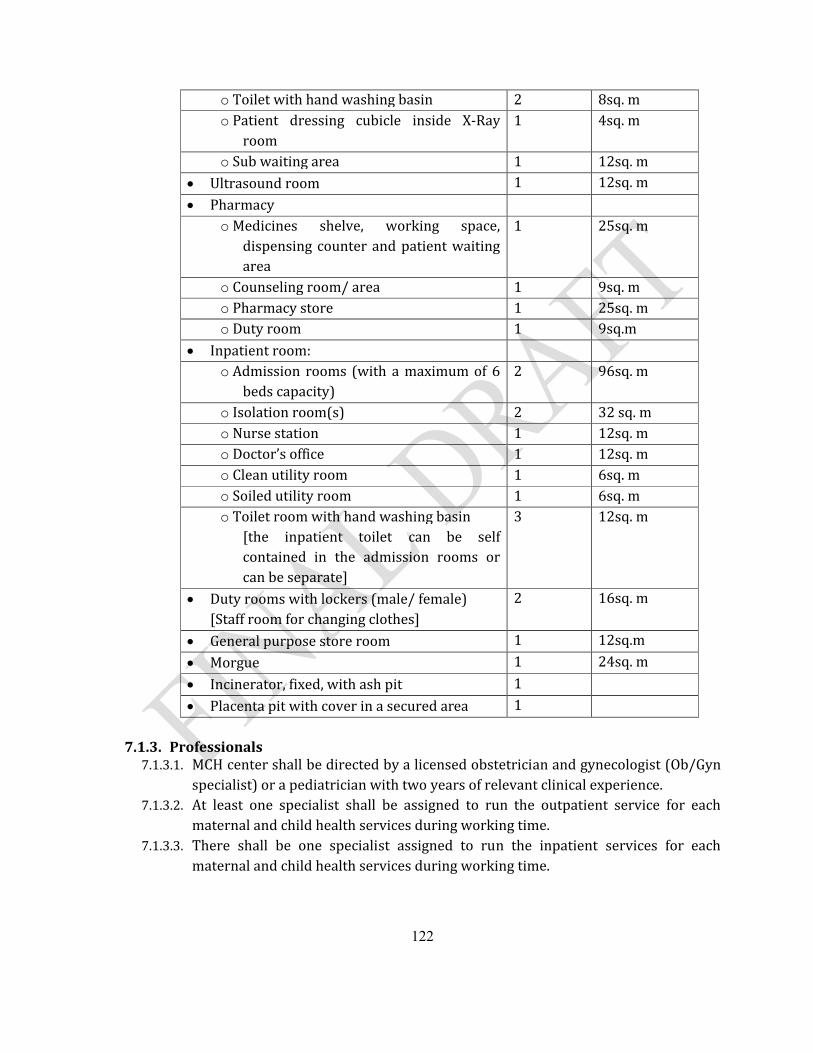
122
o Toilet with hand washing basin 2 8sq. mo Patient dressing cubicle inside X-Ray
room1 4sq. m
o Sub waiting area 1 12sq. m Ultrasound room 1 12sq. m
Pharmacyo Medicines shelve, working space,
dispensing counter and patient waiting area
1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Duty room 1 9sq.m
Inpatient room:o Admission rooms (with a maximum of 6
beds capacity)2 96sq. m
o Isolation room(s) 2 32 sq. m o Nurse station 1 12sq. mo Doctor’s office 1 12sq. mo Clean utility room 1 6sq. mo Soiled utility room 1 6sq. mo Toilet room with hand washing basin
[the inpatient toilet can be self contained in the admission rooms or can be separate]
3 12sq. m
Duty rooms with lockers (male/ female) [Staff room for changing clothes]
2 16sq. m
General purpose store room 1 12sq.m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
Placenta pit with cover in a secured area 1
7.1.3. Professionals7.1.3.1. MCH center shall be directed by a licensed obstetrician and gynecologist (Ob/Gyn
specialist) or a pediatrician with two years of relevant clinical experience.7.1.3.2. At least one specialist shall be assigned to run the outpatient service for each
maternal and child health services during working time. 7.1.3.3. There shall be one specialist assigned to run the inpatient services for each
maternal and child health services during working time.
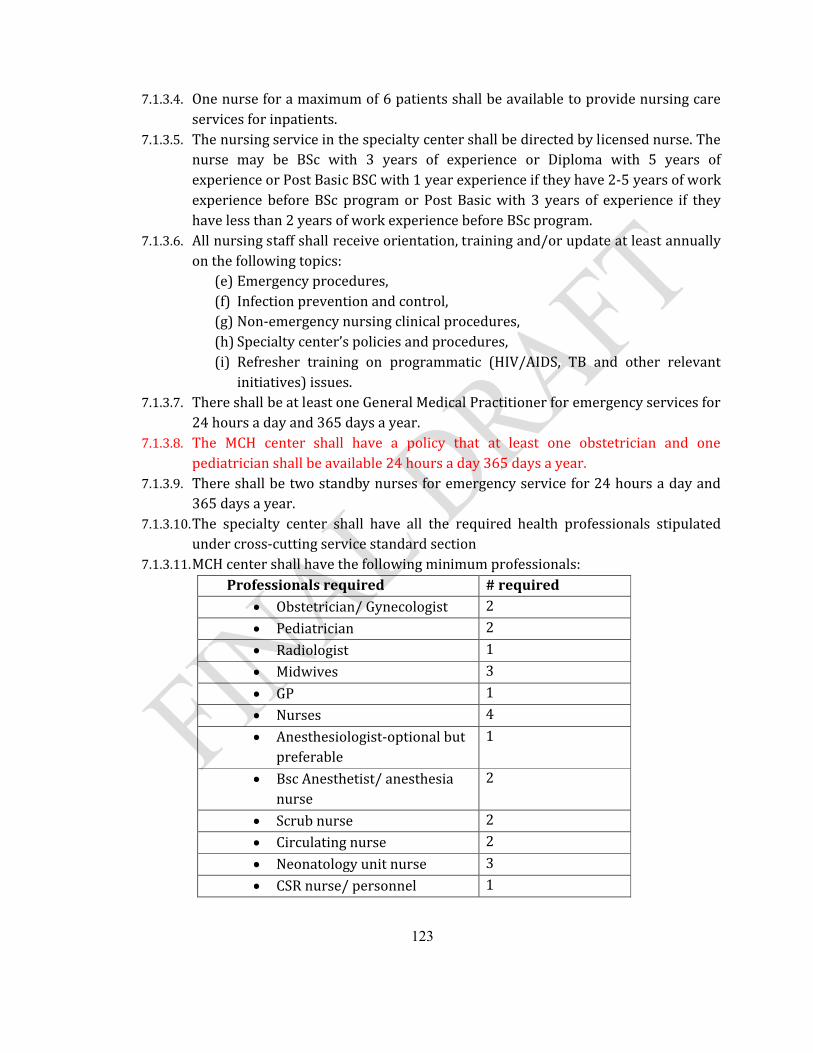
123
7.1.3.4. One nurse for a maximum of 6 patients shall be available to provide nursing care services for inpatients.
7.1.3.5. The nursing service in the specialty center shall be directed by licensed nurse. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
7.1.3.6. All nursing staff shall receive orientation, training and/or update at least annually on the following topics:
(e) Emergency procedures,(f) Infection prevention and control,(g) Non-emergency nursing clinical procedures,(h) Specialty center’s policies and procedures,(i) Refresher training on programmatic (HIV/AIDS, TB and other relevant
initiatives) issues.7.1.3.7. There shall be at least one General Medical Practitioner for emergency services for
24 hours a day and 365 days a year.7.1.3.8. The MCH center shall have a policy that at least one obstetrician and one
pediatrician shall be available 24 hours a day 365 days a year.7.1.3.9. There shall be two standby nurses for emergency service for 24 hours a day and
365 days a year.7.1.3.10.The specialty center shall have all the required health professionals stipulated
under cross-cutting service standard section7.1.3.11.MCH center shall have the following minimum professionals:
Professionals required # required Obstetrician/ Gynecologist 2
Pediatrician 2
Radiologist 1
Midwives 3
GP 1
Nurses 4
Anesthesiologist-optional but preferable
1
Bsc Anesthetist/ anesthesia nurse
2
Scrub nurse 2
Circulating nurse 2
Neonatology unit nurse 3
CSR nurse/ personnel 1
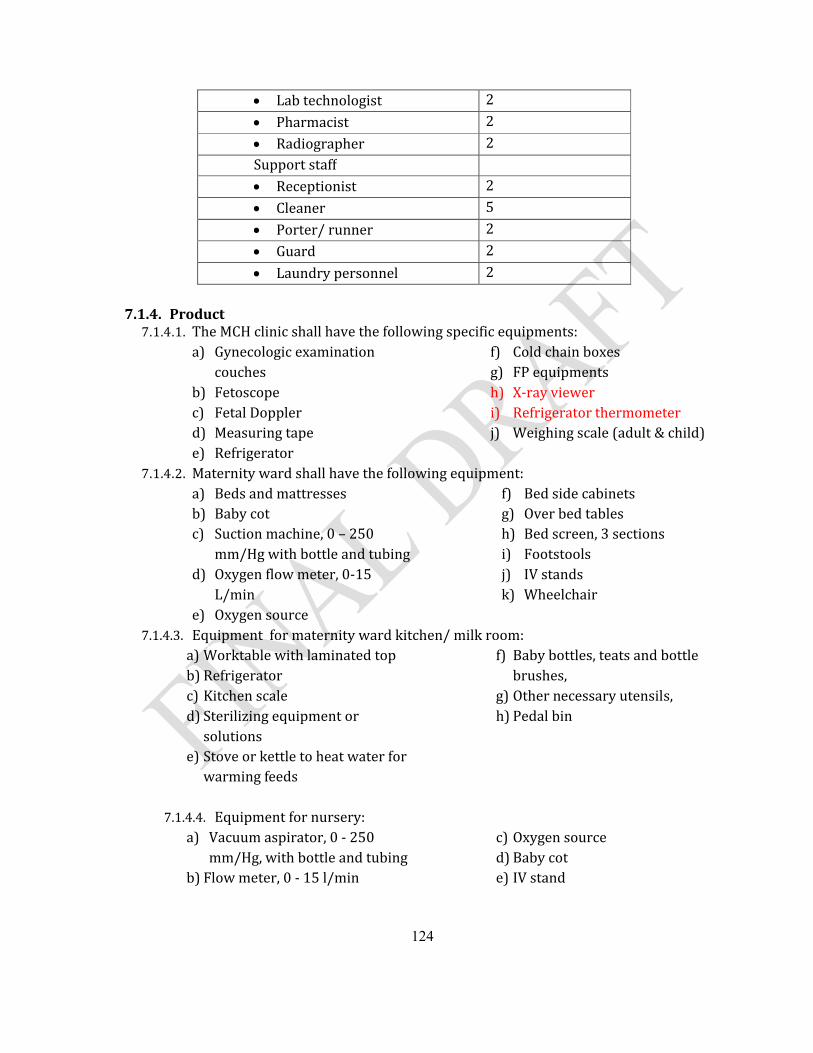
124
Lab technologist 2
Pharmacist 2
Radiographer 2Support staff Receptionist 2
Cleaner 5
Porter/ runner 2
Guard 2
Laundry personnel 2
7.1.4. Product7.1.4.1. The MCH clinic shall have the following specific equipments:
a) Gynecologic examination couches
b) Fetoscopec) Fetal Doppler d) Measuring tapee) Refrigerator
f) Cold chain boxesg) FP equipmentsh) X-ray vieweri) Refrigerator thermometerj) Weighing scale (adult & child)
7.1.4.2. Maternity ward shall have the following equipment:a) Beds and mattresses b) Baby cot c) Suction machine, 0 – 250
mm/Hg with bottle and tubingd) Oxygen flow meter, 0-15
L/mine) Oxygen source
f) Bed side cabinetsg) Over bed tablesh) Bed screen, 3 sections i) Footstoolsj) IV standsk) Wheelchair
7.1.4.3. Equipment for maternity ward kitchen/ milk room:a) Worktable with laminated topb) Refrigeratorc) Kitchen scaled) Sterilizing equipment or
solutionse) Stove or kettle to heat water for
warming feeds
f) Baby bottles, teats and bottle brushes,
g) Other necessary utensils,h) Pedal bin
7.1.4.4. Equipment for nursery:a) Vacuum aspirator, 0 - 250
mm/Hg, with bottle and tubing b) Flow meter, 0 - 15 l/min
c) Oxygen source d) Baby cot e) IV stand
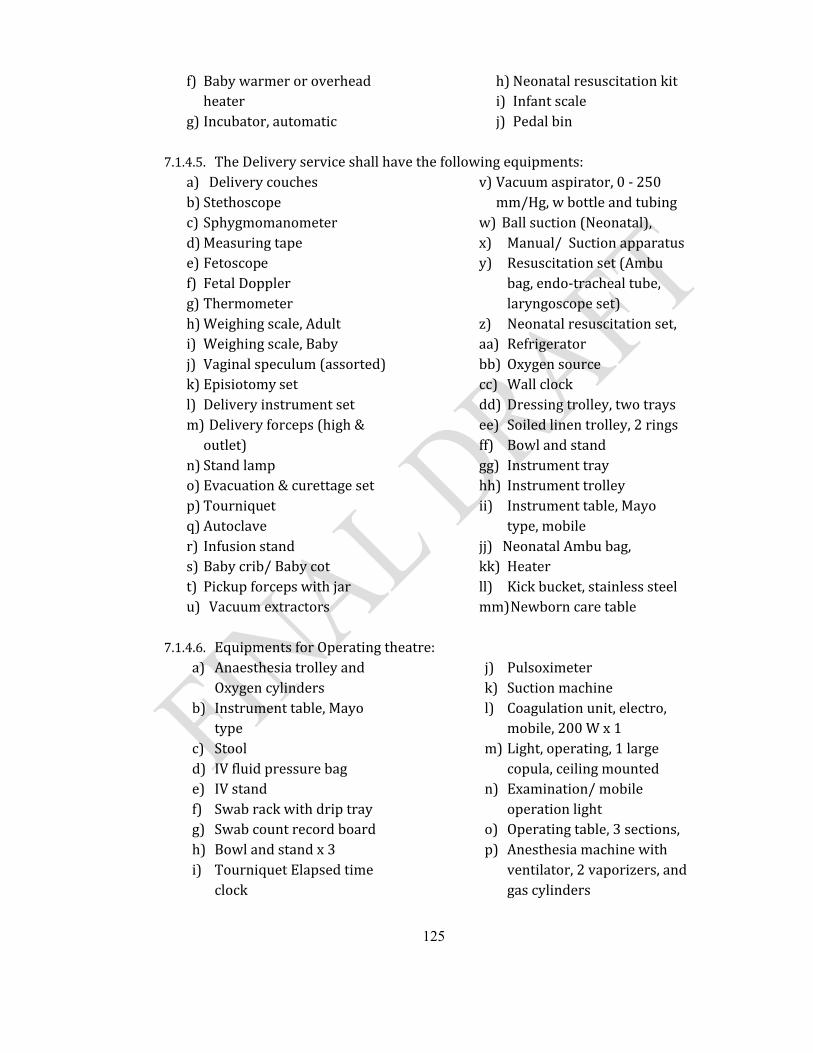
125
f) Baby warmer or overhead heater
g) Incubator, automatic
h) Neonatal resuscitation kit i) Infant scale j) Pedal bin
7.1.4.5. The Delivery service shall have the following equipments:a) Delivery couchesb) Stethoscopec) Sphygmomanometerd) Measuring tape e) Fetoscope f) Fetal Dopplerg) Thermometerh) Weighing scale, Adulti) Weighing scale, Babyj) Vaginal speculum (assorted)k) Episiotomy setl) Delivery instrument setm) Delivery forceps (high &
outlet)n) Stand lamp o) Evacuation & curettage setp) Tourniquet q) Autoclaver) Infusion stands) Baby crib/ Baby cott) Pickup forceps with jaru) Vacuum extractors
v) Vacuum aspirator, 0 - 250 mm/Hg, w bottle and tubing
w) Ball suction (Neonatal),x) Manual/ Suction apparatus y) Resuscitation set (Ambu
bag, endo-tracheal tube, laryngoscope set)
z) Neonatal resuscitation set,aa) Refrigeratorbb) Oxygen sourcecc) Wall clock dd) Dressing trolley, two trays ee) Soiled linen trolley, 2 rings ff) Bowl and stand gg) Instrument tray hh) Instrument trolley ii) Instrument table, Mayo
type, mobile jj) Neonatal Ambu bag,kk) Heater ll) Kick bucket, stainless steel mm)Newborn care table
7.1.4.6. Equipments for Operating theatre:a) Anaesthesia trolley and
Oxygen cylindersb) Instrument table, Mayo
type c) Stool d) IV fluid pressure bag e) IV stand f) Swab rack with drip tray g) Swab count record board h) Bowl and stand x 3i) Tourniquet Elapsed time
clock
j) Pulsoximeterk) Suction machine l) Coagulation unit, electro,
mobile, 200 W x 1m) Light, operating, 1 large
copula, ceiling mounted n) Examination/ mobile
operation lighto) Operating table, 3 sections, p) Anesthesia machine with
ventilator, 2 vaporizers, and gas cylinders
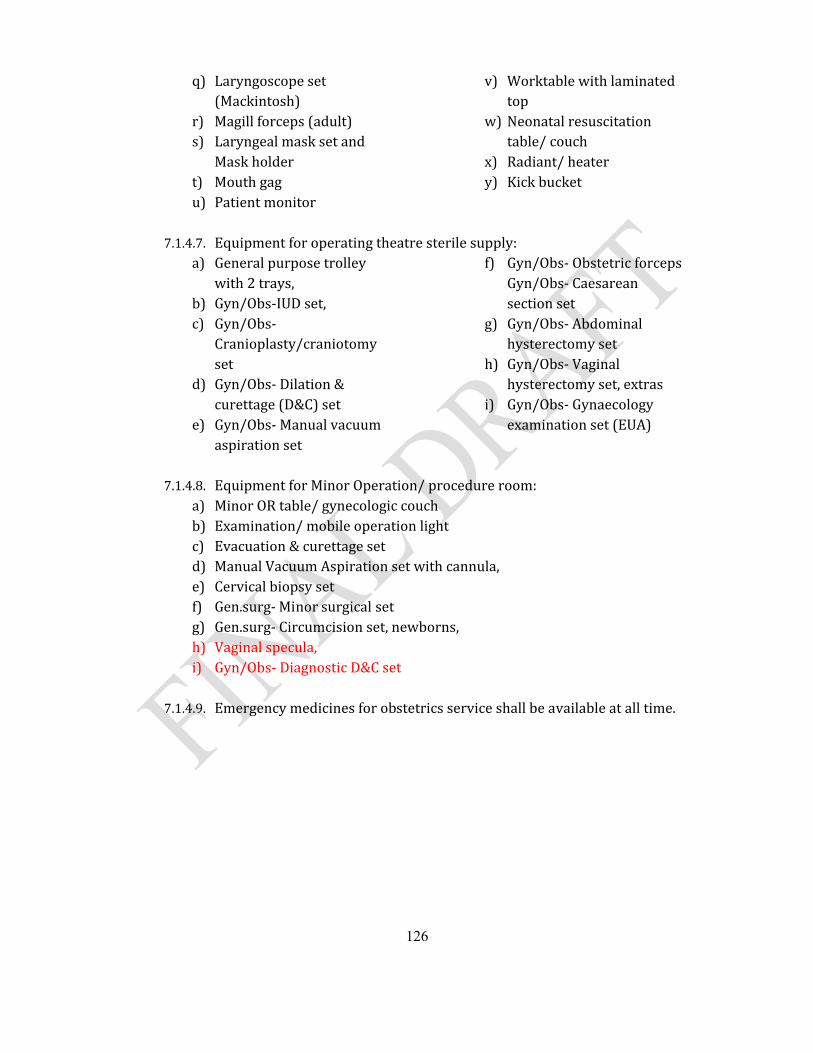
126
q) Laryngoscope set (Mackintosh)
r) Magill forceps (adult) s) Laryngeal mask set and
Mask holder t) Mouth gag u) Patient monitor
v) Worktable with laminated top
w) Neonatal resuscitation table/ couch
x) Radiant/ heater y) Kick bucket
7.1.4.7. Equipment for operating theatre sterile supply:a) General purpose trolley
with 2 trays,b) Gyn/Obs-IUD set,c) Gyn/Obs-
Cranioplasty/craniotomy set
d) Gyn/Obs- Dilation & curettage (D&C) set
e) Gyn/Obs- Manual vacuum aspiration set
f) Gyn/Obs- Obstetric forceps Gyn/Obs- Caesarean section set
g) Gyn/Obs- Abdominal hysterectomy set
h) Gyn/Obs- Vaginal hysterectomy set, extras
i) Gyn/Obs- Gynaecology examination set (EUA)
7.1.4.8. Equipment for Minor Operation/ procedure room:a) Minor OR table/ gynecologic couchb) Examination/ mobile operation lightc) Evacuation & curettage setd) Manual Vacuum Aspiration set with cannula,e) Cervical biopsy set f) Gen.surg- Minor surgical set g) Gen.surg- Circumcision set, newborns,h) Vaginal specula,i) Gyn/Obs- Diagnostic D&C set
7.1.4.9. Emergency medicines for obstetrics service shall be available at all time.
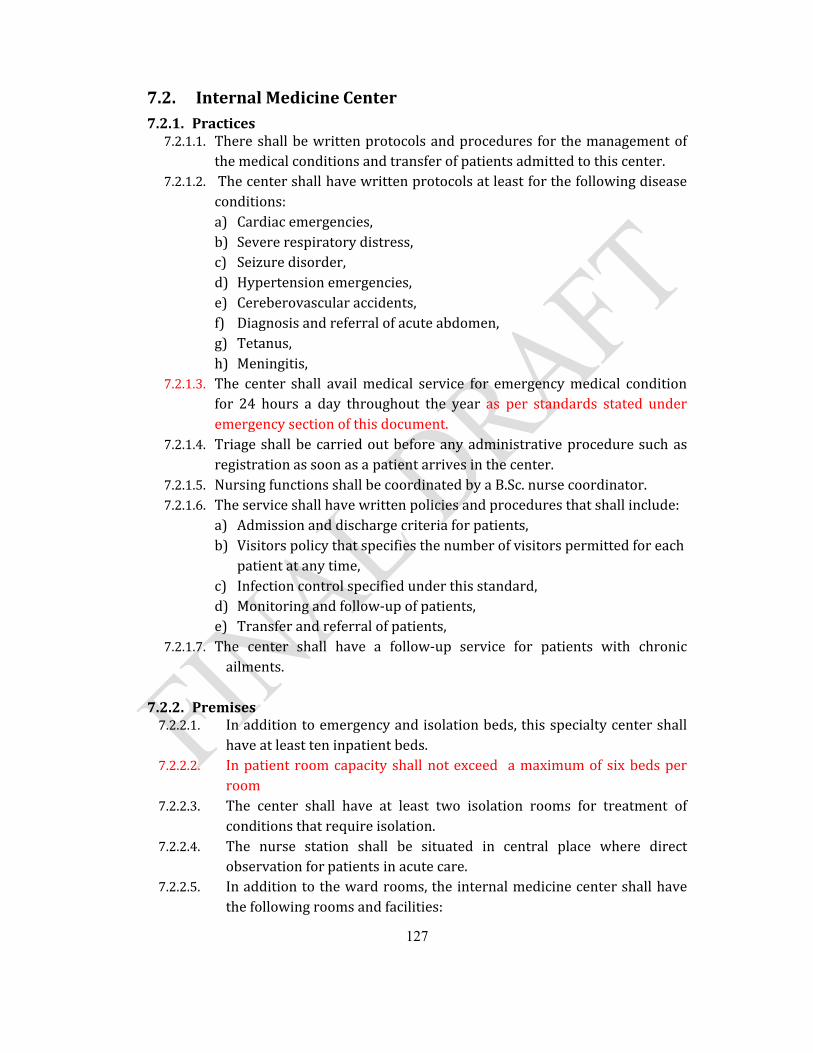
127
7.2. Internal Medicine Center 7.2.1. Practices
7.2.1.1. There shall be written protocols and procedures for the management of the medical conditions and transfer of patients admitted to this center.
7.2.1.2. The center shall have written protocols at least for the following disease conditions:a) Cardiac emergencies, b) Severe respiratory distress,c) Seizure disorder,d) Hypertension emergencies,e) Cereberovascular accidents,f) Diagnosis and referral of acute abdomen,g) Tetanus, h) Meningitis,
7.2.1.3. The center shall avail medical service for emergency medical condition for 24 hours a day throughout the year as per standards stated under emergency section of this document.
7.2.1.4. Triage shall be carried out before any administrative procedure such as registration as soon as a patient arrives in the center.
7.2.1.5. Nursing functions shall be coordinated by a B.Sc. nurse coordinator. 7.2.1.6. The service shall have written policies and procedures that shall include:
a) Admission and discharge criteria for patients,b) Visitors policy that specifies the number of visitors permitted for each
patient at any time,c) Infection control specified under this standard,d) Monitoring and follow-up of patients,e) Transfer and referral of patients,
7.2.1.7. The center shall have a follow-up service for patients with chronic ailments.
7.2.2. Premises7.2.2.1. In addition to emergency and isolation beds, this specialty center shall
have at least ten inpatient beds.7.2.2.2. In patient room capacity shall not exceed a maximum of six beds per
room7.2.2.3. The center shall have at least two isolation rooms for treatment of
conditions that require isolation.7.2.2.4. The nurse station shall be situated in central place where direct
observation for patients in acute care.7.2.2.5. In addition to the ward rooms, the internal medicine center shall have
the following rooms and facilities:
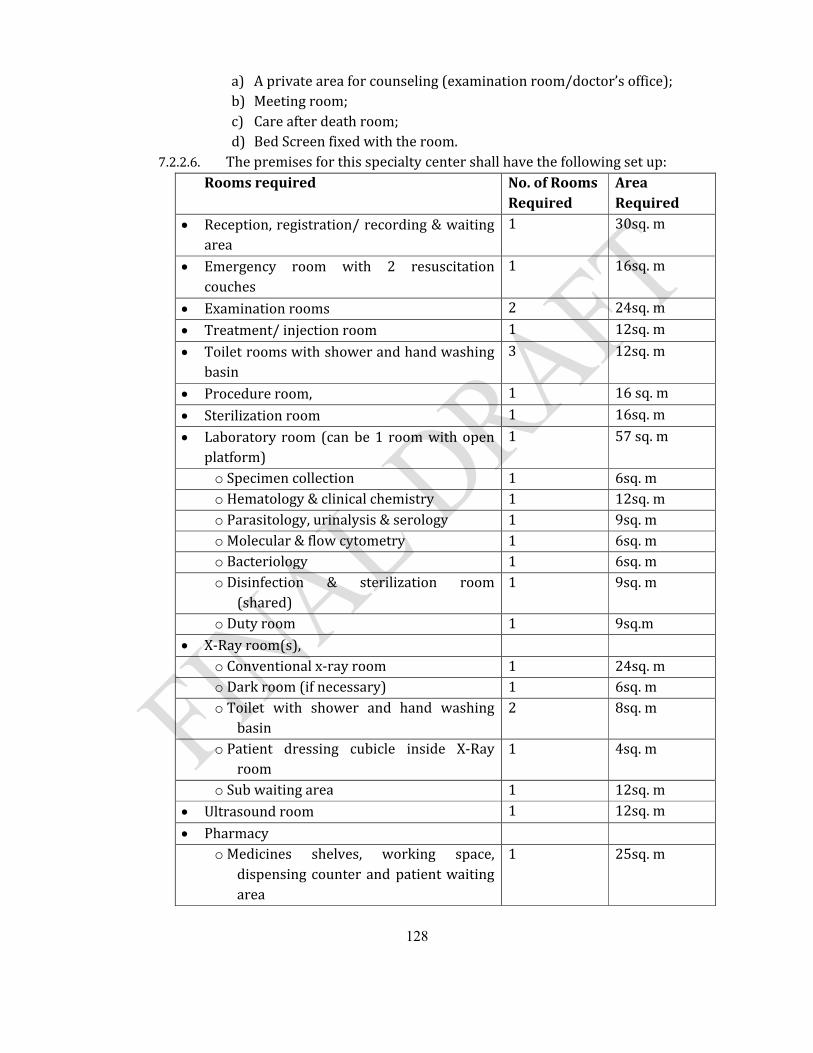
128
a) A private area for counseling (examination room/doctor’s office);b) Meeting room; c) Care after death room;d) Bed Screen fixed with the room.
7.2.2.6. The premises for this specialty center shall have the following set up:Rooms required No. of Rooms
RequiredArea Required
Reception, registration/ recording & waiting area
1 30sq. m
Emergency room with 2 resuscitation couches
1 16sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Toilet rooms with shower and hand washing basin
3 12sq. m
Procedure room, 1 16 sq. m
Sterilization room 1 16sq. m
Laboratory room (can be 1 room with open platform)
1 57 sq. m
o Specimen collection 1 6sq. mo Hematology & clinical chemistry 1 12sq. mo Parasitology, urinalysis & serology 1 9sq. mo Molecular & flow cytometry 1 6sq. mo Bacteriology 1 6sq. mo Disinfection & sterilization room
(shared)1 9sq. m
o Duty room 1 9sq.m X-Ray room(s),
o Conventional x-ray room 1 24sq. mo Dark room (if necessary) 1 6sq. mo Toilet with shower and hand washing
basin2 8sq. m
o Patient dressing cubicle inside X-Ray room
1 4sq. m
o Sub waiting area 1 12sq. m Ultrasound room 1 12sq. m
Pharmacyo Medicines shelves, working space,
dispensing counter and patient waiting area
1 25sq. m
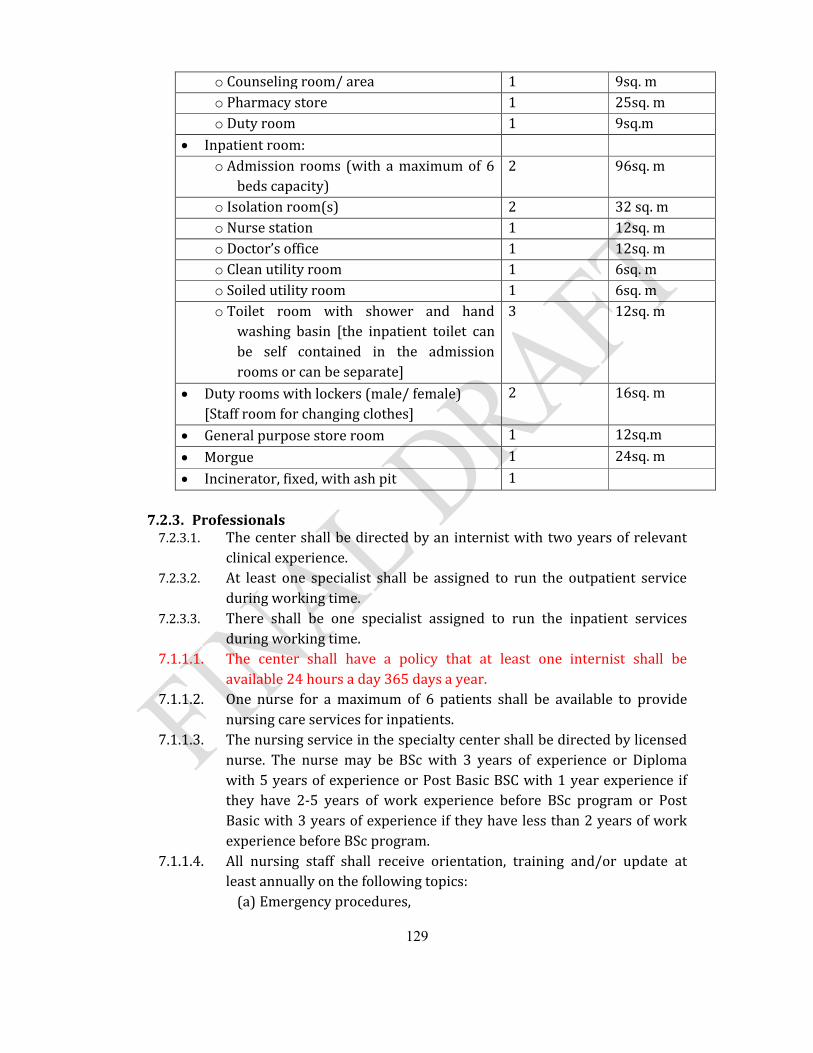
129
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Duty room 1 9sq.m
Inpatient room:o Admission rooms (with a maximum of 6
beds capacity)2 96sq. m
o Isolation room(s) 2 32 sq. m o Nurse station 1 12sq. mo Doctor’s office 1 12sq. mo Clean utility room 1 6sq. mo Soiled utility room 1 6sq. mo Toilet room with shower and hand
washing basin [the inpatient toilet can be self contained in the admission rooms or can be separate]
3 12sq. m
Duty rooms with lockers (male/ female) [Staff room for changing clothes]
2 16sq. m
General purpose store room 1 12sq.m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
7.2.3. Professionals7.2.3.1. The center shall be directed by an internist with two years of relevant
clinical experience.7.2.3.2. At least one specialist shall be assigned to run the outpatient service
during working time. 7.2.3.3. There shall be one specialist assigned to run the inpatient services
during working time.7.1.1.1. The center shall have a policy that at least one internist shall be
available 24 hours a day 365 days a year.7.1.1.2. One nurse for a maximum of 6 patients shall be available to provide
nursing care services for inpatients.7.1.1.3. The nursing service in the specialty center shall be directed by licensed
nurse. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
7.1.1.4. All nursing staff shall receive orientation, training and/or update at least annually on the following topics:
(a) Emergency procedures,
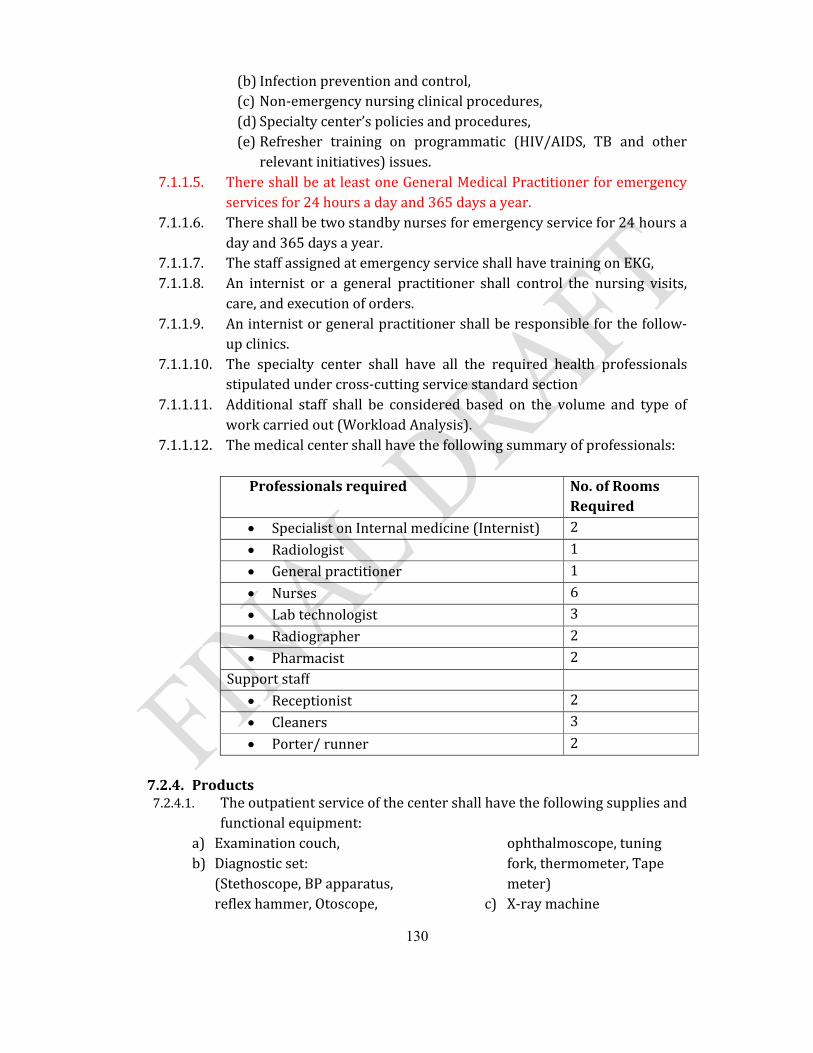
130
(b) Infection prevention and control,(c) Non-emergency nursing clinical procedures,(d) Specialty center’s policies and procedures,(e) Refresher training on programmatic (HIV/AIDS, TB and other
relevant initiatives) issues.7.1.1.5. There shall be at least one General Medical Practitioner for emergency
services for 24 hours a day and 365 days a year.7.1.1.6. There shall be two standby nurses for emergency service for 24 hours a
day and 365 days a year.7.1.1.7. The staff assigned at emergency service shall have training on EKG,7.1.1.8. An internist or a general practitioner shall control the nursing visits,
care, and execution of orders.7.1.1.9. An internist or general practitioner shall be responsible for the follow-
up clinics.7.1.1.10. The specialty center shall have all the required health professionals
stipulated under cross-cutting service standard section7.1.1.11. Additional staff shall be considered based on the volume and type of
work carried out (Workload Analysis).7.1.1.12. The medical center shall have the following summary of professionals:
Professionals required No. of Rooms Required
Specialist on Internal medicine (Internist) 2
Radiologist 1
General practitioner 1
Nurses 6
Lab technologist 3
Radiographer 2
Pharmacist 2Support staff
Receptionist 2
Cleaners 3
Porter/ runner 2
7.2.4. Products7.2.4.1. The outpatient service of the center shall have the following supplies and
functional equipment:a) Examination couch,b) Diagnostic set:
(Stethoscope, BP apparatus, reflex hammer, Otoscope,
ophthalmoscope, tuning fork, thermometer, Tape meter)
c) X-ray machine
131
d) Defibrillatore) Torch, f) Weighing scales for adults,g) Height measurement,h) Lumbar puncture, i) Bone marrow aspiration
set, j) Pleural (peritoneal) biopsy
set,
k) Cut down set, l) Pericadiocentesis set, m) Wide bore needles for
thoracentesis,n) Spatula, surgical and
disposable gloves, antiseptics, cotton, gauze
7.2.4.2. The inpatient service shall have the following supplies and functional equipments:
a) Patient beds,a) Diagnostic sets: (Torch,
Otoscope, funduscope, patella hammer etc…
b) Weighing scales,c) Vital sign set: thermometer,
BP apparatus, stethoscope etc…
d) Examination couch, e) Medicine trolley, f) Lumbar puncture set,g) Bone marrow aspiration set, h) pleural biopsy set, i) tracheotomy set, j) chest tube,k) EKG machine, l) Suction machine,m) Drip counters/Infusion
pump, n) Tourniquet,o) IV stands,p) Oxygen source/ Oxygen
cylinder, Flow-meters for oxygen,
q) Oxygen face mask,r) Nasal prongs catheters,s) Self inflating bags for
respiratory support, Masks, endotracheal tubes,
t) Laryngoscope,u) Cannulas, v) Nasogastric tubes, w) Nebulizer, x) Equipment for skin scrapings
and biopsy of dermatological lesions, bone marrow trephine needles and slides and others
y) Glucometer and glucostick,z) Pulseoximeter,aa) Wheelchair,bb)Over bed table( for feeding),cc) Bed side cabinet,dd)Curtain fixed with the ceiling,ee) Kick buckets,ff) Cup board
7.2.4.3. The center shall have emergency medicines available at all times.
132
7.3. Surgery Center7.3.1. Practices
7.3.1.1. Comprehensive emergency surgical service shall be available 24 hours a day, 365 days a year,
7.3.1.2. Services for non-emergency elective surgical cases shall be available during working time when all the necessary experts are available;
7.3.1.3. The Surgery Center shall have clear protocol for surgical procedures.7.3.1.4. There shall be a clear policy for handling emergency surgical conditions. 7.3.1.5. The preoperative diagnosis shall be recorded in the medical record for all
patients prior to surgery. 7.3.1.6. There shall be processes and procedures that ensures/ defining the
appropriateness and safety before, during and immediately after surgery, including at least the following: a) Aseptic technique, b) Disinfections and Sterilization, c) Selection of draping and gowning,
7.3.1.7. There shall be written protocols and procedures for admissions and discharges with follow up.
7.3.1.8. The admission process for emergency surgery shall be done by the emergency/ duty physician with consultation to the duty surgeon.
7.3.1.9. The admission process for elective surgery shall be done by the respective surgeon in consultation with the anesthesia department and with the other departments as needed.
7.3.1.10. For admitted patients the surgical service shall be organized in such a way that it covers all the shifts.
7.3.1.11. All surgical procedures (except in life-threatening emergencies) are performed only after appropriate history, physical examination, and indicated diagnostic tests are completed and documented in the patient’s medical record.
7.3.1.12. The preoperative diagnosis shall be recorded in the medical record for all patients prior to surgery.
7.3.1.13. The surgeon shall explain the disease condition, possible surgical intervention and outcome possibilities in clear, simple and understandable terms to the patient and/or family.
7.3.1.14. Except in life-threatening emergencies, the surgeon shall obtain an informed consent and this must be documented in the patient’s medical record. For the case with life threatening condition, consent shall be obtained from spouse, family, guardian or based on the surgeon’s clinical judgment which shall be documented properly.
133
7.3.1.15. If there is nobody to sign the consent for the patient who is in life-threatening condition, the reason for not having the signed consent shall be stated.
7.3.1.16. The nursing care of patients undergoing surgery shall be planned and documented in the medical record, directed by a trained nurse, and includes the following:
(a) Pre-operative care,(b) Type of recovery room care and monitoring needed, (c) Post-operative care and its location, (d) Pain management, (e) Patient’s understanding of discharge instructions and(f) Post operative follow up schedule.
7.3.1.17. Surgical interventions/procedures shall be written in the patient’s record and in the Operation Room (OR) register immediately after each procedure and shall include at least the following:
(a) Patient identification, (b) Preoperative Diagnosis, (c) Procedure performed, (d) Findings during surgery, (e) Post-operative diagnosis, (f) Anesthesia used, (g) Surgical specimens removed, (h) Date and time the operation done(started & ended), (i) Pain management, (j) Name of surgeon, anesthesia professional, scrub nurse and name of assistant
if any, (k) Signature of the surgeon, & the scrub nurse, (l) Immediate post-operative orders explicitly in the order sheet.
7.3.1.18. There shall be policy that leads to positively identify the patient and ensure that the correct procedure and the correct side are confirmed prior to starting the surgery.
7.3.1.19. If surgical specimen shall be sent to examination, the surgeon shall fill the pathology form and the specimen container shall be properly labeled. The container shall be filled with 10% formalin.
7.3.1.20. The specimen shall be sent to the pathology service by the OR staff. If there is no pathology service in the center, the specimen shall be sent with proper container to another facility by a family member or a relative.
7.3.1.21. There shall be a policy for preparing and availing appropriate and properly functioning supplies, equipments, and instruments for all surgeries performed in the center according to this standard.
7.3.1.22. There shall be a protocol for patient transfer from operation theatre to recovery room. This includes;
134
(a) The handover of immediate post-operative patients shall be done between the anesthesia professional who administered & followed the anesthesia and the assigned nurse in recovery room,
(b) The recovery room nurse shall immediately re-evaluate the condition of the patient in front of the anesthesia professional,
(c) The follow up of immediate post-operative patients in the recovery room shall be done by assigned nurse with relevant training until the anesthesia professional or other qualified physician makes the decision to transfer the patient from post-anesthesia care (recovery room) and this decision shall be based on the documented results of monitoring during anesthesia recovery,
(d) The transfer from recovery room shall be done after the transfer order is signed by the appropriate anesthesia professional or other qualified physician,
(e) The nurse in the recovery room shall inform the ward and the ward nurse shall transfer the patient with the signed transfer note.
7.3.1.23. The surgery center shall have an Intensive Care Unit (ICU) with all requirements stipulated under ICU standards
7.3.1.24. The surgery center shall provide anesthesia services as per the standards stipulated under anesthesia services
7.3.1.25. Post- operative patient in the wards shall get post operative care by qualified nurses. The post operative care includes to the minimum:
(a) Evaluation by the surgeon or appropriate physician and ward nurses daily or whenever needed,
(b) Follow up of vital signs and carrying out of post-operative orders as per the order specified for individual patients. (special orders-NPO, positioning, exercise, drainages, etc.,)
7.3.1.26. The operation theatre shall not be functional without the presence of a surgeon.7.3.1.27. There shall be a policy or procedure that clearly shows at least one surgeon
shall be on call/ on duty to respond for surgical requests from emergency and/ or surgical ward physician.
7.3.1.28. There shall be a mechanism that the surgeon shall be available within 30 minutes upon call.
7.3.1.29. There shall be no time left without having a physician attending the admitted surgical patients.
7.3.1.30. All admitted surgical patients shall get nursing care at all shifts.7.3.1.31. All admitted surgical patients shall be visited & evaluated by a licensed surgeon
at least once daily. 7.3.1.32. There shall be a mechanism by which the surgery center regulates provision of
board certificates in response to requests. The board shall compose of, at minimum, two surgeons and one general practitioner and one of them shall be a treating surgeon.
135
7.3.1.33. The Surgery Center shall have a copy of management protocols at least for the following:a) Acute burn management,b) pain management, c) emergency or acute trauma management,d) Emergency resuscitation (CPR). e) Infection protocol,
7.3.1.34. All surgical procedures and interventions shall be documented on medical record of the patient.
7.3.1.35. Any surgical procedure shall be performed only after appropriate history, physical examination, and indicated diagnostic tests are completed and documented in the patient’s medical record.
7.3.1.36. The surgical procedure rooms (major & minor OR) shall be kept clean at all time and it shall be cleansed thoroughly at least weekly & whenever necessary.
7.3.1.37. There shall be a written policy about administration of anesthesia in the surgery center.
7.3.1.38. For sterilization of instruments, the date of sterilization & the names of the sets/ instruments shall be written on all packs or drums of instruments after sterilization.
7.3.1.39. A written record of the anesthetic agent and outcome of the procedure shall be kept as a permanent record in the medical record of the patient.
7.3.1.40. Orientation and continuous update training shall be provided for OR support staff (cleaners) on proper handling and disposal of sharp materials and surgical wastes.
7.3.2. Premises
7.3.2.1. Operation Room /Surgical Suite: (a) The operation room shall be readily accessible to the surgical admission
wards.(b) An operating room shall have access- restricted environment where
surgical and invasive interventions are performed. It shall be organized and equipped so that OR trafficking shall be controlled and exercised over all persons and materials entering and leaving the area.
7.3.2.2. Operation Theatre: (a) The wall of the operation theatres shall be washable; the vicinity of
plumbing fixtures shall be smooth and water resistant i.e., ceramic plated up to the ceiling.
(b) The ceiling shall be monolithic, scrub-able and capable of withstanding chemicals. Cracks or perforation in these ceilings are not allowed.
(c) Floors and walls penetrated by pipes, ducts and conduits’ shall be tightly sealed.
136
(d) The floor of the theatre shall be smooth, easily cleanable, non-slippery and non-staining and it shall not be affected by water or germicidal cleaning solutions; preferably made of marble or ceramic.
(e) There shall be drainage on the floor, (f) There shall be at least six fixed electric outlets in each theatre with cover, (g) The entrance and exit doors to the theatre shall be fitted with self-closing
double doors, (h) There shall be at least one operation table in each theatre, (i) At least one ceiling operation light and one mobile operation light per
theatre shall be available (j) Glass cabinet and shelves shall be available.(k) Heater or air conditioner, based on the climate, fixed on the wall shall be
available in each theatre, 7.3.2.3. Scrub area:
(a) There shall be a scrubbing-up area outside but adjacent to the operating theatre(s). The scrub area shall be in between the two self closing doors. If there is one common scrub area for the 2 theatres, it shall be wide enough to accommodate four staff scrubbing simultaneously.
(b) This area shall have direct access to the operating room, (c) It shall be provided with multiple sinks or with wide sink and taps
for running (warm) water. The taps for running water shall be hand free, manipulated with elbow or knee joint. (e.g., long arm of valve gate to be manipulated with elbow or knee joint.)
(d) Mirror above each sink. 7.3.2.4. Nurse station:
(a) This is a room within the restricted access areas, which is so situated, constructed and equipped that it is possible for the nursing staff to observe patients directly and where necessary, to render assistance. This area need not be a room, but may form an integral part of the main patient corridor, recovery area or bed-receiving area.
(b) There shall be a corridor or allocated area for keeping charged and empty Oxygen cylinders; the empty and charged oxygen cylinders shall be labeled clearly,
7.3.2.5. Entrance/Patient Transfer Area: (a) This area shall be large enough to allow transfer of patients from a ward
bed/ stretcher to OR stretcher. (b) A line shall be clearly marked in red on the floor, beyond which no person
shall be permitted to set foot without putting on protective clothing and OR shoes.
(c) Holding bay: there shall be a space or corridor to keep and observe pre-operative patients until called to theatre.
137
7.3.2.6. Staff Change Rooms:(a) Each changing rooms shall have two doors, one entrance and the second
door accessing into the restricted access area; the entrance is from outside the restricted access area.
(b) Each changing room shall be provided with a locker to keep personal clothes and belongings.
(c) Each changing room shall be provided with shelves for Storage of clean theatre attire and inside shoes and operation theatre gum boots.
(d) Separate storage bin shall be provided for used and soiled theatre apparels/ clothes.
7.3.2.7. Set-up Area (optional): (a) Mini-Store area for suture materials and other supplies stacked on a
trolley that could be wheeled into theatre for subsequent procedure. (b) Doors into the operating room shall be big enough to wheel through the
set trolleys from the set up room into the operating room without contact with doors or non sterile surfaces.
(c) Packed instruments and other relevant materials shall be brought from the CSR and stored in this area according to the daily schedules one day prior to the scheduled operations.
(d) Mayo table and dressing trolley to set up for the next case are kept in this area.
(e) If there is no set up area the instruments can be set up within the operating theatre.
7.3.2.8. Operating Theatre Equipment Store (a) The equipment store shall be supplied with a sufficient number of
electrical plugs to keep the electrical equipments plugged in, charged and ready-to-use.
(b) Equipments shall always be stored at the same space/ location and properly labeled.
(c) There shall be enough shelves and cabinets in the store.7.3.2.9. Operating Theatre Sterile Supply room: a room for the storage of all sterile
instrument sets, swabs and sterile renewable, consumables. 7.3.2.10. Clean Utility Surgical room: a room allocated for storage of clean linen and
other sundry items. Requirements: (a) Shall be situated where OR staff have easy access to the clean utility store. (b) Metallic washable rack for storage shall be available, (c) Equipments used for special procedures like splints shall be kept here
thoroughly cleaned after use, (d) Refrigerator with thermometer shall be available for medicines requiring
cold chain.(e) Hand wash sink,
138
(f) Cabinets and shelves.7.3.2.11. Soiled Utility/Sluice room shall be available to accommodate the following
conditions & requirements:(a) Located at the back of the OR. (b) Used for keeping contaminated materials until they are disposed. (c) Sharp containers, leak proof containers with lids shall be available, used
sharps/safety boxes are to be stored here before being sent for disposal. (d) Container for temporary storage of soiled linen,(e) Hand Washing sink, (f) Drainage on the floor, (g) Trolley for soiled materials and waste human tissues,
7.3.2.12. Cleaner’s Room shall be available to accommodate the followings:(a) Cleaning equipments and materials, (b) Hand washing sink, (c) Washing sink, (d) Detergent proof shelves and cabinets.
7.3.2.13. Central Sterilization Room (CSR) shall be available with the followings;(a) Direct access to OR, (b) With a minimum of the following rooms:
Room for reception, sorting and documentation process; Room for inbuilt autoclaves; Room for storing and shelving sterile clothes and instruments as per the
guideline, properly ventilated, Cleaners’ closet.
(c) Continuous water supply with extra reservoir, 7.3.2.14. Recovery Room which shall be within the semi- restricted area of OR shall have
the following facilities:(a) A minimum of 2 beds,(b) A minimum of 1.2 meter gap between beds,(c) A minimum of two electric outlets per bed, (d) A trolley carrying functional emergency equipments,(e) Sufficient light for each bed, one head light per bed, (f) Heater or air conditioner based on the climate.
7.3.2.15. Minor Operation Room shall have the following facilities:(a) Located accessible to OPD and shall be with low traffic area, (b) Mark on the floor restricting movement of unauthorized and/or a person
without OR suit, 7.3.2.16. Surgical ward shall be available with the following facilities;
(a) In addition to emergency and isolation, the specialty center shall have at least ten inpatient beds.
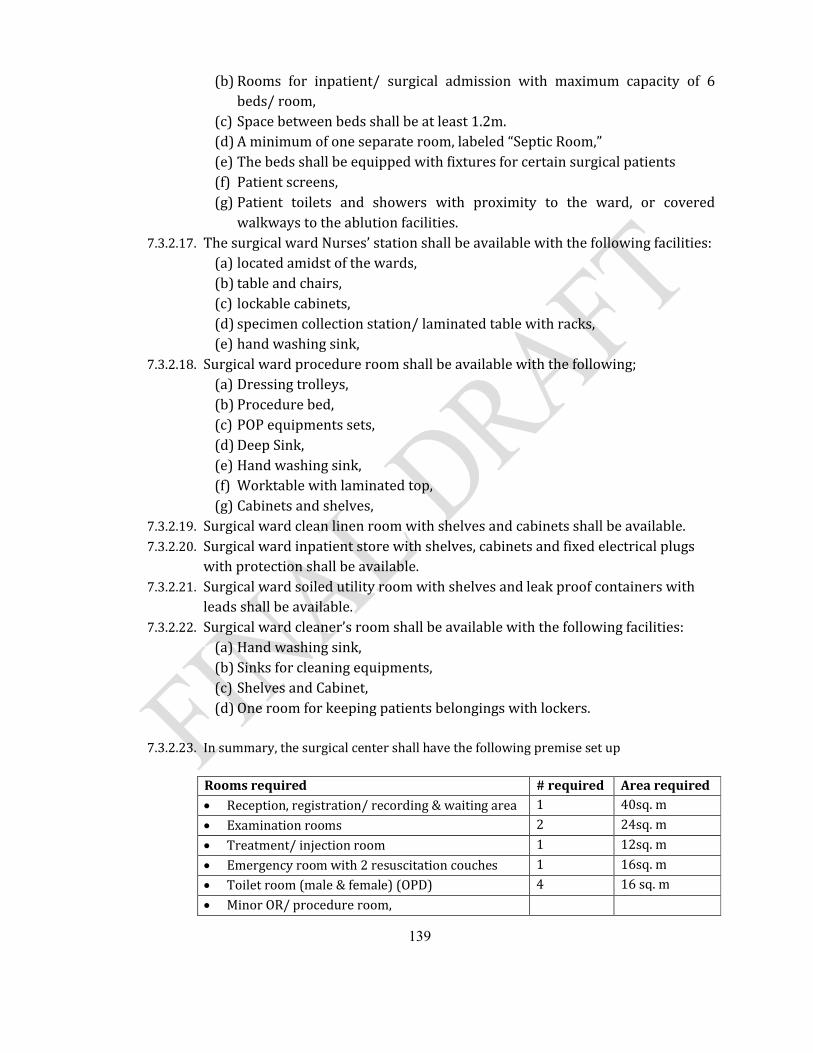
139
(b) Rooms for inpatient/ surgical admission with maximum capacity of 6 beds/ room,
(c) Space between beds shall be at least 1.2m.(d) A minimum of one separate room, labeled “Septic Room,” (e) The beds shall be equipped with fixtures for certain surgical patients(f) Patient screens, (g) Patient toilets and showers with proximity to the ward, or covered
walkways to the ablution facilities. 7.3.2.17. The surgical ward Nurses’ station shall be available with the following facilities:
(a) located amidst of the wards,(b) table and chairs,(c) lockable cabinets, (d) specimen collection station/ laminated table with racks,(e) hand washing sink,
7.3.2.18. Surgical ward procedure room shall be available with the following;(a) Dressing trolleys,(b) Procedure bed,(c) POP equipments sets, (d) Deep Sink, (e) Hand washing sink, (f) Worktable with laminated top, (g) Cabinets and shelves,
7.3.2.19. Surgical ward clean linen room with shelves and cabinets shall be available.7.3.2.20. Surgical ward inpatient store with shelves, cabinets and fixed electrical plugs
with protection shall be available.7.3.2.21. Surgical ward soiled utility room with shelves and leak proof containers with
leads shall be available.7.3.2.22. Surgical ward cleaner’s room shall be available with the following facilities:
(a) Hand washing sink, (b) Sinks for cleaning equipments, (c) Shelves and Cabinet, (d) One room for keeping patients belongings with lockers.
7.3.2.23. In summary, the surgical center shall have the following premise set up
Rooms required # required Area required Reception, registration/ recording & waiting area 1 40sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Emergency room with 2 resuscitation couches 1 16sq. m
Toilet room (male & female) (OPD) 4 16 sq. m
Minor OR/ procedure room,
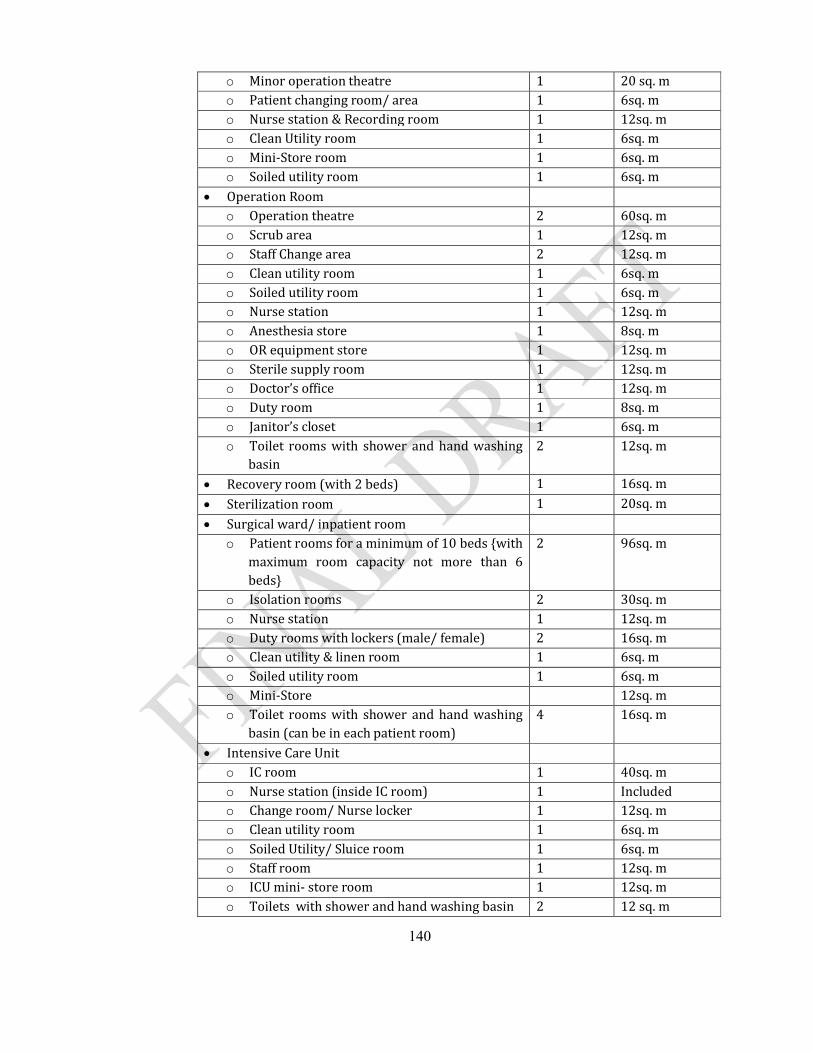
140
o Minor operation theatre 1 20 sq. mo Patient changing room/ area 1 6sq. mo Nurse station & Recording room 1 12sq. mo Clean Utility room 1 6sq. mo Mini-Store room 1 6sq. mo Soiled utility room 1 6sq. m
Operation Roomo Operation theatre 2 60sq. mo Scrub area 1 12sq. mo Staff Change area 2 12sq. mo Clean utility room 1 6sq. mo Soiled utility room 1 6sq. mo Nurse station 1 12sq. mo Anesthesia store 1 8sq. mo OR equipment store 1 12sq. mo Sterile supply room 1 12sq. mo Doctor’s office 1 12sq. mo Duty room 1 8sq. mo Janitor’s closet 1 6sq. mo Toilet rooms with shower and hand washing
basin2 12sq. m
Recovery room (with 2 beds) 1 16sq. m
Sterilization room 1 20sq. m
Surgical ward/ inpatient roomo Patient rooms for a minimum of 10 beds {with
maximum room capacity not more than 6 beds}
2 96sq. m
o Isolation rooms 2 30sq. mo Nurse station 1 12sq. mo Duty rooms with lockers (male/ female) 2 16sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 12sq. mo Toilet rooms with shower and hand washing
basin (can be in each patient room)4 16sq. m
Intensive Care Unito IC room 1 40sq. mo Nurse station (inside IC room) 1 Included o Change room/ Nurse locker 1 12sq. mo Clean utility room 1 6sq. mo Soiled Utility/ Sluice room 1 6sq. mo Staff room 1 12sq. mo ICU mini- store room 1 12sq. mo Toilets with shower and hand washing basin 2 12 sq. m
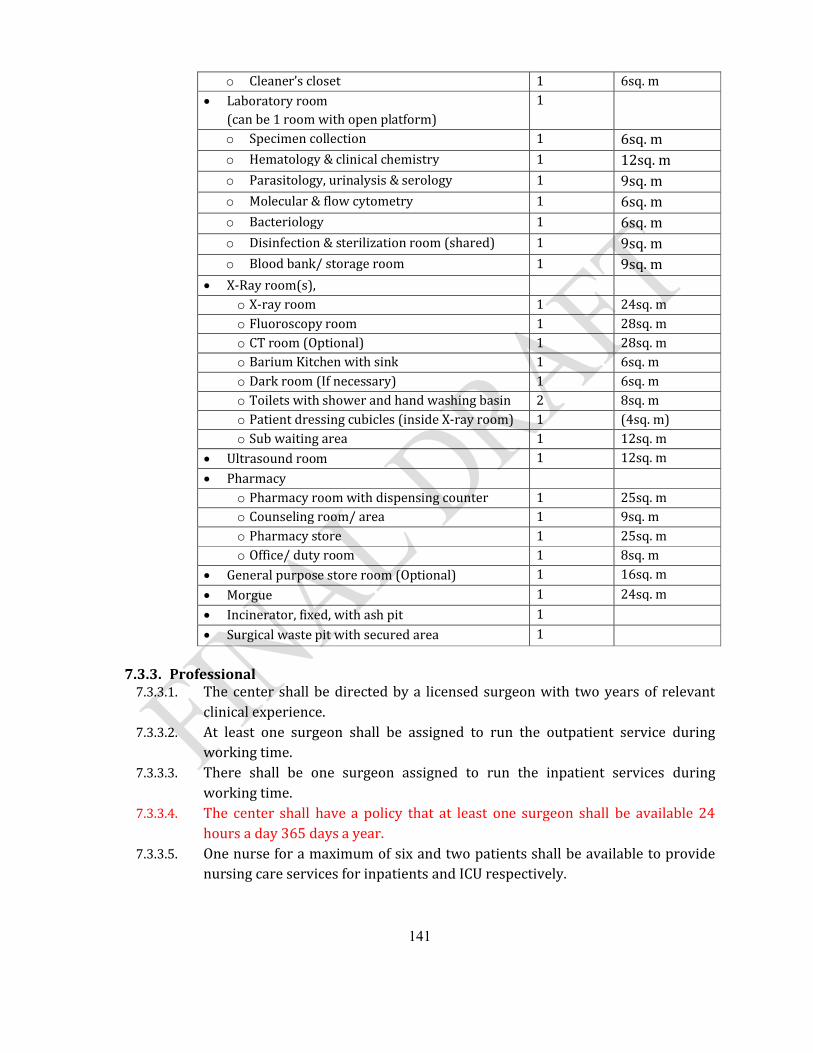
141
o Cleaner’s closet 1 6sq. m Laboratory room
(can be 1 room with open platform)1
o Specimen collection 1 6sq. mo Hematology & clinical chemistry 1 12sq. mo Parasitology, urinalysis & serology 1 9sq. mo Molecular & flow cytometry 1 6sq. mo Bacteriology 1 6sq. mo Disinfection & sterilization room (shared) 1 9sq. mo Blood bank/ storage room 1 9sq. m
X-Ray room(s), o X-ray room 1 24sq. mo Fluoroscopy room 1 28sq. mo CT room (Optional) 1 28sq. mo Barium Kitchen with sink 1 6sq. mo Dark room (If necessary) 1 6sq. mo Toilets with shower and hand washing basin 2 8sq. mo Patient dressing cubicles (inside X-ray room) 1 (4sq. m)o Sub waiting area 1 12sq. m
Ultrasound room 1 12sq. m
Pharmacyo Pharmacy room with dispensing counter 1 25sq. mo Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 8sq. m
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
Surgical waste pit with secured area 1
7.3.3. Professional 7.3.3.1. The center shall be directed by a licensed surgeon with two years of relevant
clinical experience. 7.3.3.2. At least one surgeon shall be assigned to run the outpatient service during
working time. 7.3.3.3. There shall be one surgeon assigned to run the inpatient services during
working time.7.3.3.4. The center shall have a policy that at least one surgeon shall be available 24
hours a day 365 days a year.7.3.3.5. One nurse for a maximum of six and two patients shall be available to provide
nursing care services for inpatients and ICU respectively.
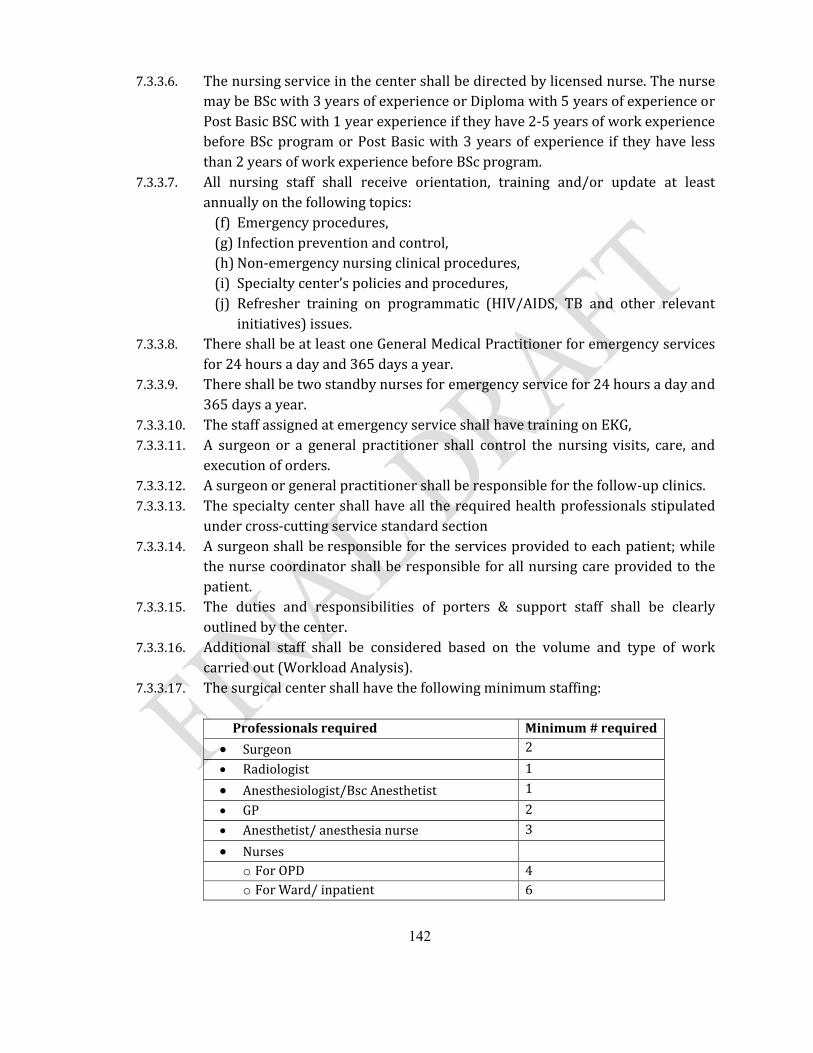
142
7.3.3.6. The nursing service in the center shall be directed by licensed nurse. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
7.3.3.7. All nursing staff shall receive orientation, training and/or update at least annually on the following topics:
(f) Emergency procedures,(g) Infection prevention and control,(h) Non-emergency nursing clinical procedures,(i) Specialty center’s policies and procedures,(j) Refresher training on programmatic (HIV/AIDS, TB and other relevant
initiatives) issues.7.3.3.8. There shall be at least one General Medical Practitioner for emergency services
for 24 hours a day and 365 days a year.7.3.3.9. There shall be two standby nurses for emergency service for 24 hours a day and
365 days a year.7.3.3.10. The staff assigned at emergency service shall have training on EKG,7.3.3.11. A surgeon or a general practitioner shall control the nursing visits, care, and
execution of orders.7.3.3.12. A surgeon or general practitioner shall be responsible for the follow-up clinics.7.3.3.13. The specialty center shall have all the required health professionals stipulated
under cross-cutting service standard section7.3.3.14. A surgeon shall be responsible for the services provided to each patient; while
the nurse coordinator shall be responsible for all nursing care provided to the patient.
7.3.3.15. The duties and responsibilities of porters & support staff shall be clearly outlined by the center.
7.3.3.16. Additional staff shall be considered based on the volume and type of work carried out (Workload Analysis).
7.3.3.17. The surgical center shall have the following minimum staffing:
Professionals required Minimum # required
Surgeon 2
Radiologist 1
Anesthesiologist/Bsc Anesthetist 1
GP 2
Anesthetist/ anesthesia nurse 3
Nurseso For OPD 4o For Ward/ inpatient 6
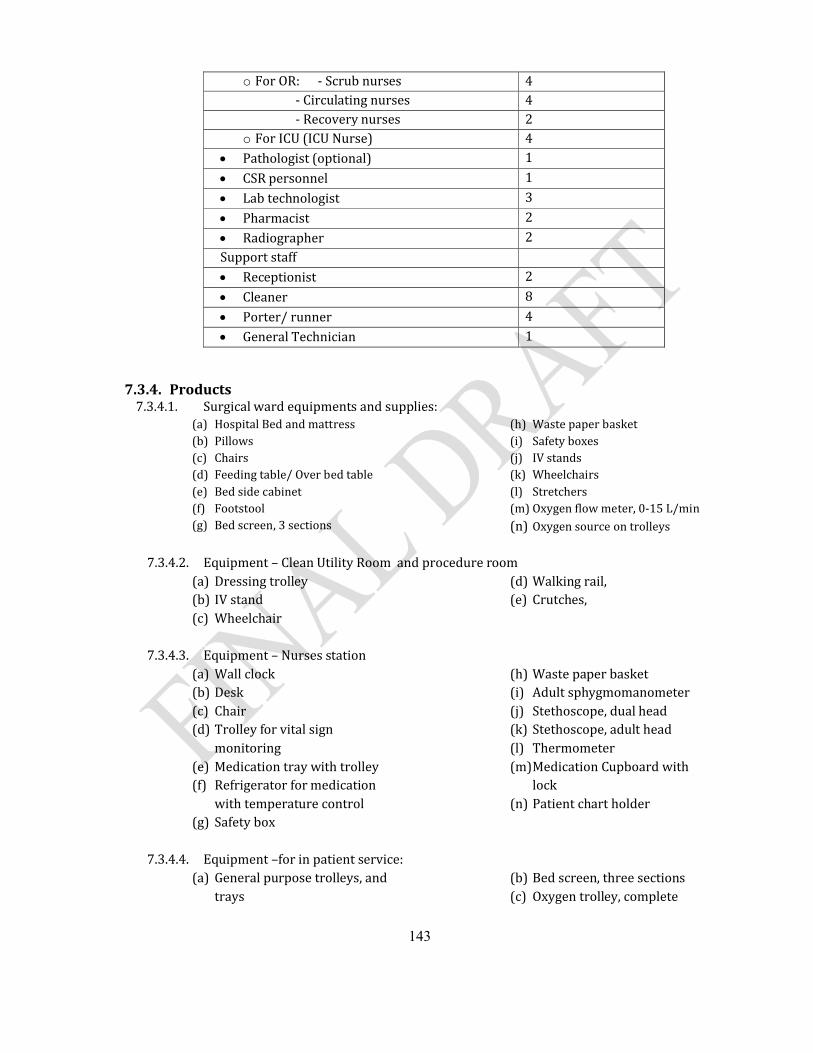
143
o For OR: - Scrub nurses 4 - Circulating nurses 4 - Recovery nurses 2
o For ICU (ICU Nurse) 4 Pathologist (optional) 1
CSR personnel 1
Lab technologist 3
Pharmacist 2
Radiographer 2Support staff Receptionist 2
Cleaner 8
Porter/ runner 4
General Technician 1
7.3.4. Products 7.3.4.1. Surgical ward equipments and supplies:
(a) Hospital Bed and mattress (b) Pillows (c) Chairs (d) Feeding table/ Over bed table (e) Bed side cabinet (f) Footstool (g) Bed screen, 3 sections
(h) Waste paper basket (i) Safety boxes (j) IV stands (k) Wheelchairs (l) Stretchers (m) Oxygen flow meter, 0-15 L/min (n) Oxygen source on trolleys
7.3.4.2. Equipment – Clean Utility Room and procedure room(a) Dressing trolley (b) IV stand (c) Wheelchair
(d) Walking rail, (e) Crutches,
7.3.4.3. Equipment – Nurses station(a) Wall clock (b) Desk (c) Chair (d) Trolley for vital sign
monitoring (e) Medication tray with trolley(f) Refrigerator for medication
with temperature control (g) Safety box
(h) Waste paper basket (i) Adult sphygmomanometer (j) Stethoscope, dual head(k) Stethoscope, adult head (l) Thermometer (m)Medication Cupboard with
lock(n) Patient chart holder
7.3.4.4. Equipment –for in patient service:(a) General purpose trolleys, and
trays (b) Bed screen, three sections(c) Oxygen trolley, complete
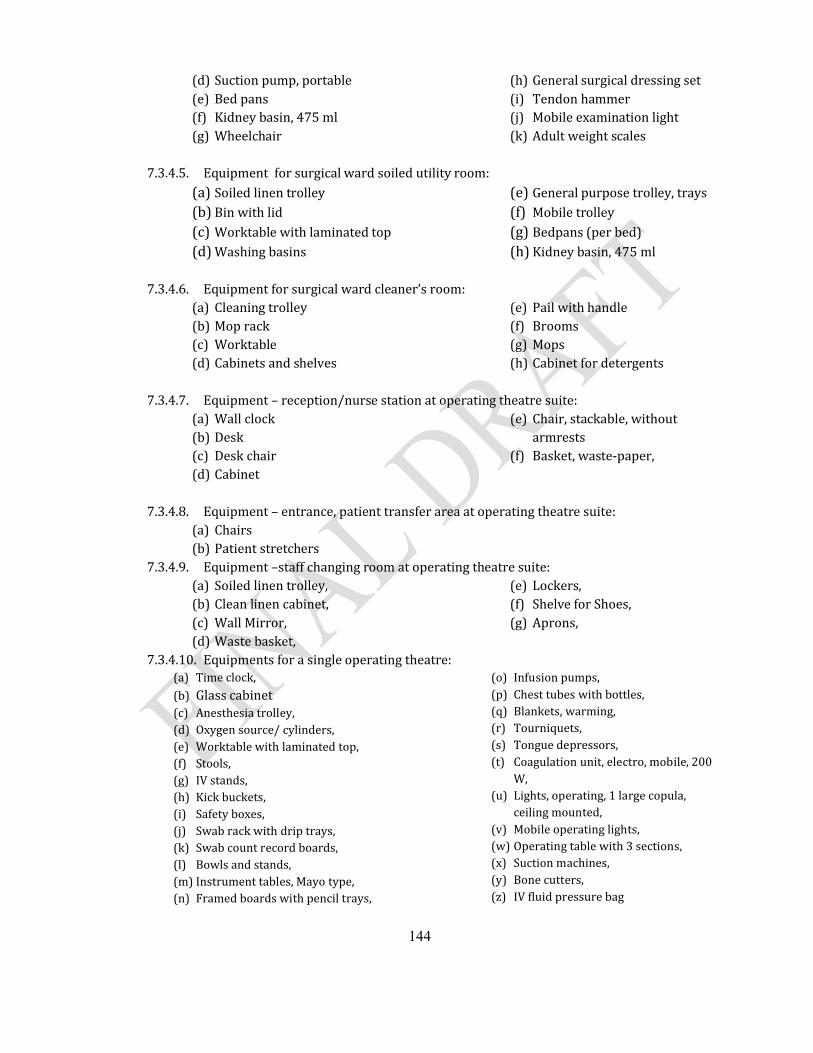
144
(d) Suction pump, portable(e) Bed pans (f) Kidney basin, 475 ml (g) Wheelchair
(h) General surgical dressing set(i) Tendon hammer (j) Mobile examination light (k) Adult weight scales
7.3.4.5. Equipment for surgical ward soiled utility room:(a) Soiled linen trolley (b) Bin with lid (c) Worktable with laminated top (d) Washing basins
(e) General purpose trolley, trays (f) Mobile trolley(g) Bedpans (per bed)(h) Kidney basin, 475 ml
7.3.4.6. Equipment for surgical ward cleaner’s room:(a) Cleaning trolley (b) Mop rack (c) Worktable (d) Cabinets and shelves
(e) Pail with handle (f) Brooms (g) Mops (h) Cabinet for detergents
7.3.4.7. Equipment – reception/nurse station at operating theatre suite:(a) Wall clock (b) Desk (c) Desk chair (d) Cabinet
(e) Chair, stackable, without armrests
(f) Basket, waste-paper,
7.3.4.8. Equipment – entrance, patient transfer area at operating theatre suite:(a) Chairs(b) Patient stretchers
7.3.4.9. Equipment –staff changing room at operating theatre suite:(a) Soiled linen trolley,(b) Clean linen cabinet,(c) Wall Mirror,(d) Waste basket,
(e) Lockers,(f) Shelve for Shoes,(g) Aprons,
7.3.4.10. Equipments for a single operating theatre:(a) Time clock,(b) Glass cabinet(c) Anesthesia trolley,(d) Oxygen source/ cylinders,(e) Worktable with laminated top,(f) Stools,(g) IV stands,(h) Kick buckets,(i) Safety boxes,(j) Swab rack with drip trays,(k) Swab count record boards,(l) Bowls and stands,(m) Instrument tables, Mayo type,(n) Framed boards with pencil trays,
(o) Infusion pumps,(p) Chest tubes with bottles,(q) Blankets, warming,(r) Tourniquets,(s) Tongue depressors,(t) Coagulation unit, electro, mobile, 200
W,(u) Lights, operating, 1 large copula,
ceiling mounted,(v) Mobile operating lights,(w) Operating table with 3 sections,(x) Suction machines,(y) Bone cutters,(z) IV fluid pressure bag
145
(aa)Anesthesia machine with ventilator, 2 vaporizers, and gas cylinders
(bb) Laryngoscope, set (Mackintosh) (cc) Magill forceps (adult & pediatrics) (dd) Laryngeal mask set
(ee)Mask holder (ff) Mouth gag(gg)Patient monitor (hh) Dual head stethoscope
7.3.4.11. Equipment for set up area:(a) Worktable with laminated top,(b) Cabinets and shelves,(c) Dressing trolley,
(d) Instrument table, Mayo type,(e) Blood warmer,(f) IV fluid warmer
7.3.4.12. Equipment – operating theatre store(a) Patient transfer, stretchers,(b) General purpose trolleys,(c) IV stands,(d) Hygrometer, humidity and
temperature,(e) Pillows, abduction,
(f) Support, head, operating table,(g) Positioner, bag (small,
medium, large),(h) Apron, protective (small,
medium, large),
7.3.4.13. Equipment at operating theatre sterile supply room:(a) General purpose trolleys,
trays (b) General surgery-Suture set(c) General surgery- Basic surgery
set (d) Orthopedic set (e) Thyroidectomy set (f) Cholecystectomy set (g) Thoracotomy set
(h) General surgery- Laparotomy set
(i) General surgery- Small dissection set
(j) General surgery- Minor surgical set
(k) General surgery- Suprapubic puncture set
7.3.4.14. Equipment at surgical clean utility room:(a) General purpose trolley, trays (b) Worktable, laminated top (c) Refrigerator
(d) Shelves (e) cabinets
7.3.4.15. Equipments at operating theatre sluice room(a) Soiled linen trolley (b) General purpose trolley, trays (c) Bin with lid (d) Worktable with laminated top
(e) Wash basins (f) Bedpans (g) Kidney basin, 475 ml
7.3.4.16. Equipment – cleaners’ room, operating theatre:(a) Cleaning trolley (b) Mop rack (c) Worktable
(d) Pail with handle (e) Brooms (f) Mops
7.3.4.17. In addition to products mentioned under radiological services, the surgical center shall have
(a) Ultrasound(b) CT (optional)(c) Floroscopy(d) X-ray machine
146
7.3.4.18. Consumables for surgical unit:(a) Guedel airways: size 0, 00, 3, 4 &
5 (b) Disposable aprons (c) Aqua-packs Oxygen humidifier (d) Bags - Refuse - All Colors and
Sizes (e) Bags – Urine (f) Bandage - Crepe (g) Batteries - Medical & General (h) Blood Administration Sets (i) Blood Sampling:
Needles, disposable, sterile, 20 G, 21 G, 23 G
Tube, Vacuum 5ml (Vacutainer)
Tube, Vacuum EDTA 5ml (Vacutainer)
Tube, Vacuum Heparinised 5ml (Vacutainer)
Vacutainer Holder
Vacutainer needle(j) Bottles - Suction - Glass/Plastic (k) Braun Splints (Arm) (l) Cannula - Nasal-Oxygen (m) Cannula, IV short, ster, disp, 18G,
20 G, 22 G, 24 G (n) Caps - Mop/Bonnet Type (o) Catheter - Jacques (p) Chest, Electrode, Monitor (q) Combur Tests,(r) Connectors/ reducers:
Biconical Autoclavable,
Connector, T/Y,
Connectors - Plastic – Tapered,(s) Container, Sample, urine, plastic,
non-sterile, 60 ml (t) Cotton
Cotton Buds
Cotton Wool Balls - Sterile/Non-Sterile
Cotton Wool Rolls (u) POP (v) Covers - PVC - Mattress/Bed
Wedge (w) Cytological Fixative Spray (x) Drawsheet,plastic,90x180cm (y) Face Mask Water Repellent
(z) Foley Catheters – Latex/Silicone Size 10, 12 and 14
(aa)Gauze Absorbent Ribbon (bb) Gloves:
Household Large & Medium
Surgical Size 6, 6 ½, 7, 7 ½, 8
Exam, latex, disp, large, medium, small
(cc) Hand wash Antiseptic Liquid (Hibiscrub)
(dd) Hand wash Povidone (Betadine)
(ee)Hot Packs (ff) I.V. Sets :
I.V. Administration Sets – 15 Drop
I.V. Administration Sets - 60 Drop
I.V. Set, Infusion “Y”, Luer lock, air inlet
(gg)Incontinence Sheets (hh) Intubation stylet, adult,
15 Ch (ii) IV Infusion set Buretrol (jj) K.Y. Jelly (kk) IV stands (ll) Drums (mm) Latex Tubing (nn) Linen Savers (oo) Masks -
Nebulizer/Oxygen (pp) Masks – Oxygen 40 % (qq) Nail Brushes -
Autoclavable/Disposable (rr) Needles:
Spinal disp, (0.9x90mm),sterile, 20G, 22G, 24G
Disp,15G, 18G, 21G, 22G, 23G, 25G
Butterfly 23G (ss) Oxygen T Pieces (tt) Oxygen Tubing (uu) Face Masks (vv)Razor Medical - Disposable -
Single Edge (tt) Rubber Bath Mat - Non-Slip
147
(uu) Specific Gravitiy Meter (Urine Meters)
(yy)Safety Pins, Large & Medium (zz) Sharps Containers (Safety
Box/used syringes and needles) (aaa) Shroud (bbb) Spatulas – Tongue depressor(ccc) Spigot Large, Medium and
Small (ddd) Spray Bottles - Plunger
Operated (eee) Surgical Splints (fff) Suture absorbable (Chromic,
vicryl) for episiotomy and perinea tears
(ggg) Syringes:
Volume: 2ml, 5ml, 10ml, 20ml
Syringes 50 ml Conical Tip
Syringes 50 ml Luer Lock
Syringes Insulin (hhh) Tape:
Elastic Adhesive Plaster - White 5cm and 10 cm
Micropore tape
Surgical Adhesive Hypo-Allergenic
Adhesive, zinc oxide, perforated,10cmx5m
Adhesive, zinc oxide, 2.5cmx5m (iii) Clinical thermometer:(jjj) Fridge thermometer:(kkk) Tourniquet, latex rubber,75cm (lll) Tubes:
Endo-tracheal, disp. + connector, neonate mm, withoutballoon
Endo-tracheal, disp. + connector, balloon, 6.5mm, 7mm, 7.5mm, 8mm
Suction, L125cm,ster,disp, CH10, CH12, CH16
7.3.4.19. Operating Suite Renewable/Consumables:(a) Airway Guedel, pediatric & adult
size (b) Plastic, reusable aprons (c) Urine bags, collecting, 2000 ml (d) 012 Band, Esmarch, 6 cm x 5 m (e) Survival blanketl,220x140cm (f) Blood Sampling:
Needle, disposable, sterile, 20G, 21G
Tube, Vacuum 5ml (Vacutainer)
Tube, Vacuum EDTA 5ml (Vacutainer)
Tube, Vacuum Heparinised 5ml (Vacutainer)
Vacutainer holder
Vacutainer needles, 18-24G (g) Bouffant Nurse Cap (h) Bubble Tubing (i) Cannula, IV short, ster, disp, 18G,
20G, 22G, 24G (j) Catheters:
Sup-Pubic, CH 10, 1.65 cm, ster, disp adult with trocar
Ureteral, CH5, ster, disp
Urethral, CH6, ster, disp
Urethral, CH7, ster, disp
Foley, ster, disp, CH10, CH12, CH14
Three way foley catheter(k) Compresses:
Abdominal compress, 40 x 40 cm
Compress, Swab, 20x 20 cm
Compress, gauze,10x10cm,n/ster/PAC-100
Compress, gauze,10x10cm,ster/PAC-5
Compress, paraffin,10x10cm,ster/BOX-10
(l) Connector, biconical, OD 7-11-7mm
(m) Cotton wool,500g,roll,non-ster (n) Diathermy pencil/ball/blade (o) Disposable, dispersive,
electrode(Diathermy pad) (p) Drain, corrugated sheet, 3 cm x
25 cm (q) 063 Drain, wound, CH 12, ster,
disp, CH12, CH16, CH6 (r) Drawsheet,plastic,90x180cm (s) Elastoplasts, 10 cm x 3 m (t) Electrode, Chest, Monitor
148
(u) Extractor,mucus,20ml,ster,disp (v) Gauze:
Ball, Large (sterile)
Ball, Large (un-sterile)
Ball, Peanut (sterile)
Swabs RAYTEX® 10 X 10 cm
Swabs, Un-sterile (Green)
Roll,90cmx100m,non-ster
Vaseline gauze (w) Gloves,exam,latex,disp, large,
medium & small (x) Gloves,surg,disp, 6.0, 6.5, 7.0, 7.5,
8, 8.5 (y) Gum elastic bougie, CH 15, 60 cm (z) Intubation stylet, adult, 15 Ch (aa)Lancet,blood,ster,disp/PAC-200 (bb) Mask, Clinical, Disposable
(non-woven) (cc) Mask, Protection, High Filtration(dd) Needle, spinal,
0.9x90mm),ster,disp, 20G, 22G, 24G
(ee)Oxygen mask, adult (ff) Oxygen, nasal cannula (gg)Reusable, Diathermy, Cable (hh) Safety box for .used syrgs/ndls (ii) Set, Infusion “Y”, Luer lock, air
inlet (jj) Scalpel blade,ster,disp,no.10, no.
11, no. 15, no. 22, no. 23 (kk) Shoe cover, disposable (ll) Silicone Rubber Tubing (mm) Surgeon's Cap, Easy-Tie (nn) Suturing materials:
Abs,DEC1,need 1/2,18mm,round/BOX-36
Abs,DEC2,need 3/8 18mm,round/
Abs,DEC2,need 3/8,26mm,tri
Abs,DEC3,need 1/2 30mm,round
Abs,DEC3,need 3/8 50mm,round
Abs,DEC3,spool
Abs,DEC4,need 3/8 36mm,tri
Nonabs,DEC2,need 3/8 13mm,tri
Nonabs,DEC3,need 3/8 30mm,tri
(oo) Syringe,dispos, 2ml, 5ml, 10ml, 20ml
(pp) Tape,adhesive,Z.O,perforated,10cmx5m
(qq) Tape,adhesive,Z.O.,2.5cmx5m (rr) Telfa, dressing (Various Sizes) (ss) Tourniquet,latex rubber,75cm (tt) Tubes:
Endo-tracheal, disp. + connector, 3 mm, w/o balloon
Endo-tracheal, disp. + connector, 3.5 mm, w/o balloon
Endo-tracheal, disp. + connector, 4 mm, w/o balloon
Endo-tracheal, disp. + connector, 4.5 mm, w/o balloon
Endo-tracheal, disp. + connector, 5 mm, balloon
Endo-tracheal, disp. + connector, 5.5 mm, balloon
Endo-tracheal, disp. + connector, 6 mm, balloon
Endo-tracheal, disp. + connector, 6.5 mm, balloon
Endo-tracheal, disp. + connector, 7 mm, balloon
Endo-tracheal, disp. + connector, 7.5 mm, balloon
Endo-tracheal, disp. + connector, 8 mm, balloon
Trachea, balloon, int.can, ster, size 6
Trachea, balloon, int.can, ster, size 8
suction,CH08,L50cm,ster,disp, CH08, CH10, CH14, CH16
N.G Tubes 12, 14, 16
7.3.4.20. Operating Room Linen:(a) Apron Surgical, rubber (b) Trousers, Surgical, woven, Small,
Medium & Large
149
(c) Top(shirts), Surgical, woven, Small, Medium & Large
(d) Gown, Surgical, woven(Plain) (e) Cap, Surgical, woven (f) Masks, surgical, woven (g) Drape:
Surgical, woven(1 x 1 m)
Surgical, woven(1 x 1.5 m)
Surgical, woven(1.5 x 1.5 m)(fenestrated
Surgical, woven(45 cm x 70 cm)(fenestrated)
Surgical woven (2 x 1.5 m)(h) Pillow case (i) Pillows (j) Sheet, Bed (k) Sheet, draw, white (l) Cellular Blanket (m) Mayo cover (n) Towel Bath (o) Towel Hand
7.3.4.21. Equipment recovery room:(a) Vacuum aspirator,(b) Pulse oximeter (c) Oxygen Flow meter, 0 - 15 l/min (d) Oxygen source (O2 cylinder or
Oxygen concentrator)(e) Patient transfer, (stretcher/
wheelchair) (f) Dressing trolley, trays (g) Recovery beds with flexible
side protections,(h) Bed with mattress
(i) Stools (j) IV stands (k) Bed screen, 3 sections, mobile (l) Pedal bin (m) Oxygen trolley, complete (n) Resuscitator, hand operated (o) Defibrillator(p) Suction machines (q) Mobile examination light (r) Dual head stethoscope
7.3.4.22. Equipment-Central sterilization room(a) Inbuilt Auto claves ;big (b) Autoclaves ;small (c) Drums
(d) Metallic shelves (e) Cabinets
7.3.4.23. The Surgery center shall avail emergency medicines at all times7.3.4.24. The center shall have equipments and supplies in accordance with the standards
stipulated under intensive care unit services.
150
7.4. Pediatric Center7.4.1. Practices
7.4.1.1. Emergency care with a qualified staff shall be available 24 hours a day and 365 days a year.
7.4.1.2. Triage shall be carried out by a general practitioner/professional nurse as soon as a sick child arrives in the center, well before any administrative procedure such as registration
7.4.1.3. The pediatric services shall have a plan to deal with emergency conditionssuch as the arrival of one or more seriously injured pediatric patients
7.4.1.4. Pediatric services shall have at least inpatient and outpatient plus immunization and well child services.
7.4.1.5. For non-emergency pediatric patients, the service shall be available during regular working hours
7.4.1.6. The pediatrics unit shall have a follow-up service for patients with chronic ailments
7.4.1.7. Admitted patients shall receive services for 24 hours a day and 365 days a year.
7.4.1.8. The service shall have written policies and procedures that shall includea) The age below which all patients must be admitted to a pediatric
service; b) Admission and discharge criteria specific to the service; c) A visitors policy regarding what is allowed and not allowed for visitors; d) Infection prevention and control as per the standard prescribed under
IP standardse) Transfer and referral of patients f) Safety measures for the purpose of preventing electrical and bodily
injury to pediatric patients.g) Monitoring and follow-up of pediatric patients at outpatient level
7.4.1.9. The nursing assessment and care of each pediatric patient shall consider the patients developmental needs
7.4.1.10. The parents or guardians of pediatric patients shall be included in the development of the nursing plan for patient care;
7.4.1.11. Immunization services shall be available in the pediatric unit during regular working hours;
7.4.1.12. All children seeking service in the center shall be checked for their immunization status & managed accordingly;
7.4.1.13. Medical records shall be kept in line with medical record standards
151
7.4.1.14. Information contained in the medical record shall be complete and sufficiently detailed relative to the patient's history, physical examination, diagnosis, diagnostic procedures, medication administration, and treatment.
7.4.1.15. Growth monitoring activities and nutritional advice shall be available.
7.4.2. Premises7.4.2.1. In addition to emergency and isolation beds, the specialty center shall have
at least ten inpatient beds.7.4.2.2. The capacity of inpatient rooms shall be not more than six beds per room.7.4.2.3. The pediatric premises shall include at least emergency unit, outpatient,
and inpatient 7.4.2.4. The pediatric outpatient shall have a functional oral rehydration therapy
corner7.4.2.5. In addition to admission beds, the center shall have a minimum of two
separate isolation rooms. 7.4.2.6. The number and size of the rooms shall be adequate in relation to the
volume and nature of the activity in the unit (work load analysis).7.4.2.7. Patients in acute care shall be under direct observation in a room near the
nurse’s station.7.4.2.8. The paediatric OPD shall have at least the following rooms:
A room for reception and registration Patient waiting area. Two rooms for outpatient examination follow up A Procedure room A room for treatment/injection A room for nurse station Mini-store Separate toilets for patients and staff
7.4.2.9. The paediatric inpatient shall have at least the following rooms: Rooms for inpatient care Procedure room Room for severely malnourished patients (Nutrition Rehabilitation
Center) Nutritional supplement preparation room Nurses station Staff toilet and bath Toilet and bath for patients and care takers Mini-store store room
152
Office for physicians7.4.2.10. The pediatrics emergency shall have at least the following rooms:
a) Space for patient triagingb) Examination roomc) A room with two observation beds for management of patients
7.4.2.11. In addition to the rooms in the units mentioned above pediatrics services shall have the following rooms:a) Counselling roomb) Duty room at inpatient and emergency service unitsc) Meeting hall
7.4.2.12. The premises requirement is summarized in the following table
Rooms required # required Area required Reception, registration/ recording & waiting area 1 40sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Emergency room with 2 resuscitation couches 1 16sq. m
Toilet room (male & female) (OPD) with shower and hand washing basin
4 16 sq. m
Procedure room 1 20 sq. m
Sterilization room 1 20sq. m
Pediatric ICU- as per ICU standard (Optional) 1
Pediatric Ward/Inpatient roomo Inpatient rooms for a minimum of 10 beds {with
maximum room capacity not more than 6 beds} 2 96sq. m
o Isolation rooms 2 30sq. mo Nurse station 1 12sq. mo Milk preparation room 1 6sq.mo Duty rooms with lockers (male/ female) 2 16sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 12sq. mo Toilet rooms (can be in each patient room) with
shower and hand washing basin4 16sq. m
Laboratory room (can be 1 room with open platform) 1o Specimen collection 1 6sq. mo Hematology & clinical chemistry 1 12sq. mo Parasitology, urinalysis & serology 1 9sq. mo Molecular & flow cytometry 1 6sq. mo Bacteriology 1 6sq. m
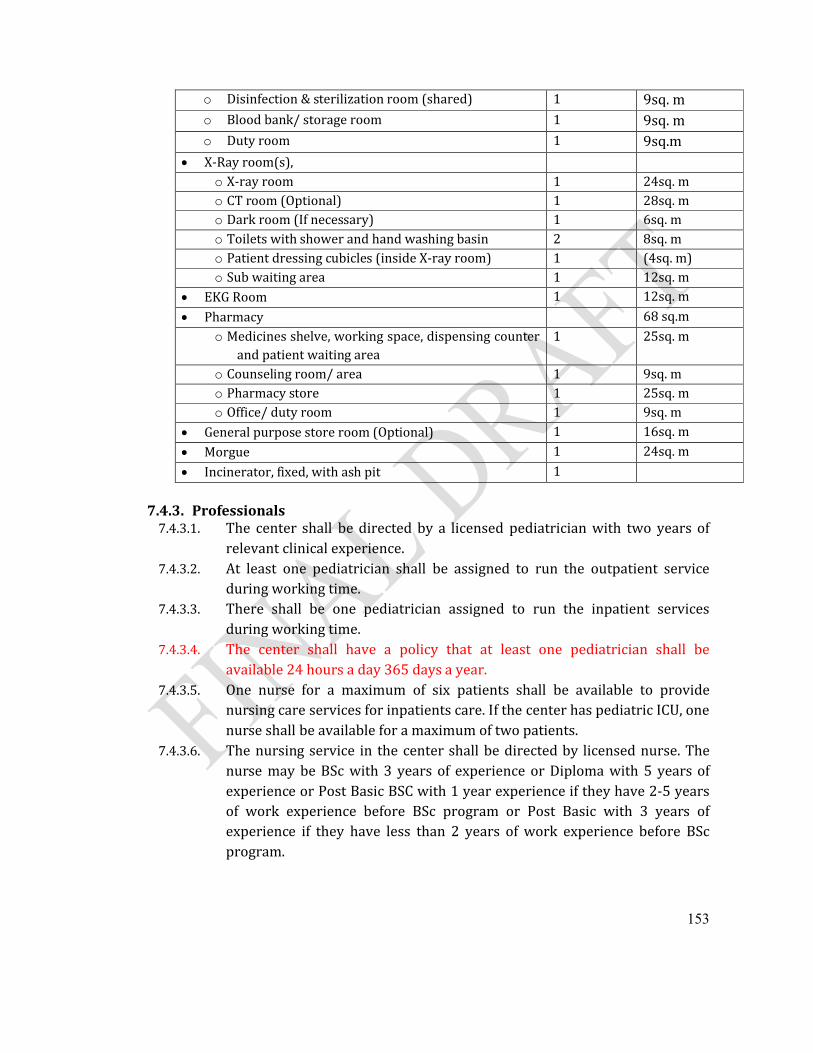
153
o Disinfection & sterilization room (shared) 1 9sq. mo Blood bank/ storage room 1 9sq. mo Duty room 1 9sq.m
X-Ray room(s), o X-ray room 1 24sq. mo CT room (Optional) 1 28sq. mo Dark room (If necessary) 1 6sq. mo Toilets with shower and hand washing basin 2 8sq. mo Patient dressing cubicles (inside X-ray room) 1 (4sq. m)o Sub waiting area 1 12sq. m
EKG Room 1 12sq. m
Pharmacy 68 sq.mo Medicines shelve, working space, dispensing counter
and patient waiting area1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 9sq. m
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
7.4.3. Professionals7.4.3.1. The center shall be directed by a licensed pediatrician with two years of
relevant clinical experience. 7.4.3.2. At least one pediatrician shall be assigned to run the outpatient service
during working time. 7.4.3.3. There shall be one pediatrician assigned to run the inpatient services
during working time.7.4.3.4. The center shall have a policy that at least one pediatrician shall be
available 24 hours a day 365 days a year.7.4.3.5. One nurse for a maximum of six patients shall be available to provide
nursing care services for inpatients care. If the center has pediatric ICU, one nurse shall be available for a maximum of two patients.
7.4.3.6. The nursing service in the center shall be directed by licensed nurse. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
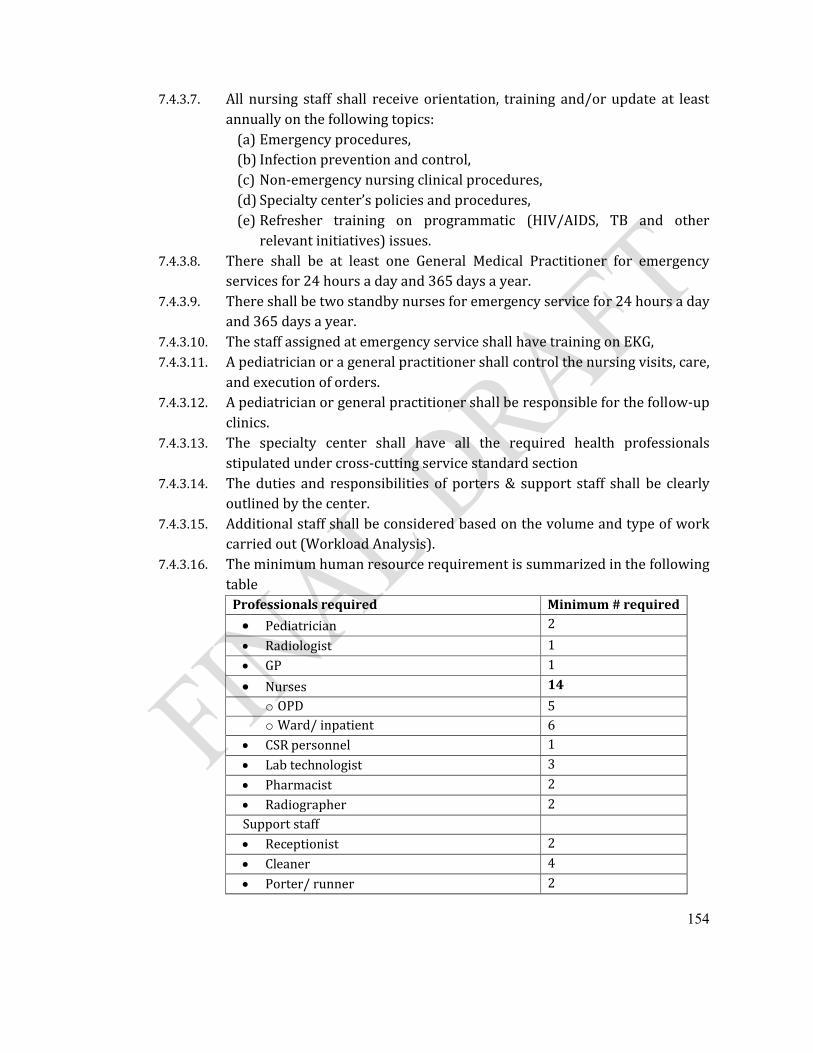
154
7.4.3.7. All nursing staff shall receive orientation, training and/or update at least annually on the following topics:
(a) Emergency procedures,(b) Infection prevention and control,(c) Non-emergency nursing clinical procedures,(d) Specialty center’s policies and procedures,(e) Refresher training on programmatic (HIV/AIDS, TB and other
relevant initiatives) issues.7.4.3.8. There shall be at least one General Medical Practitioner for emergency
services for 24 hours a day and 365 days a year.7.4.3.9. There shall be two standby nurses for emergency service for 24 hours a day
and 365 days a year.7.4.3.10. The staff assigned at emergency service shall have training on EKG,7.4.3.11. A pediatrician or a general practitioner shall control the nursing visits, care,
and execution of orders.7.4.3.12. A pediatrician or general practitioner shall be responsible for the follow-up
clinics.7.4.3.13. The specialty center shall have all the required health professionals
stipulated under cross-cutting service standard section7.4.3.14. The duties and responsibilities of porters & support staff shall be clearly
outlined by the center. 7.4.3.15. Additional staff shall be considered based on the volume and type of work
carried out (Workload Analysis).7.4.3.16. The minimum human resource requirement is summarized in the following
tableProfessionals required Minimum # required
Pediatrician 2
Radiologist 1
GP 1
Nurses 14
o OPD 5o Ward/ inpatient 6
CSR personnel 1
Lab technologist 3
Pharmacist 2
Radiographer 2Support staff Receptionist 2
Cleaner 4
Porter/ runner 2
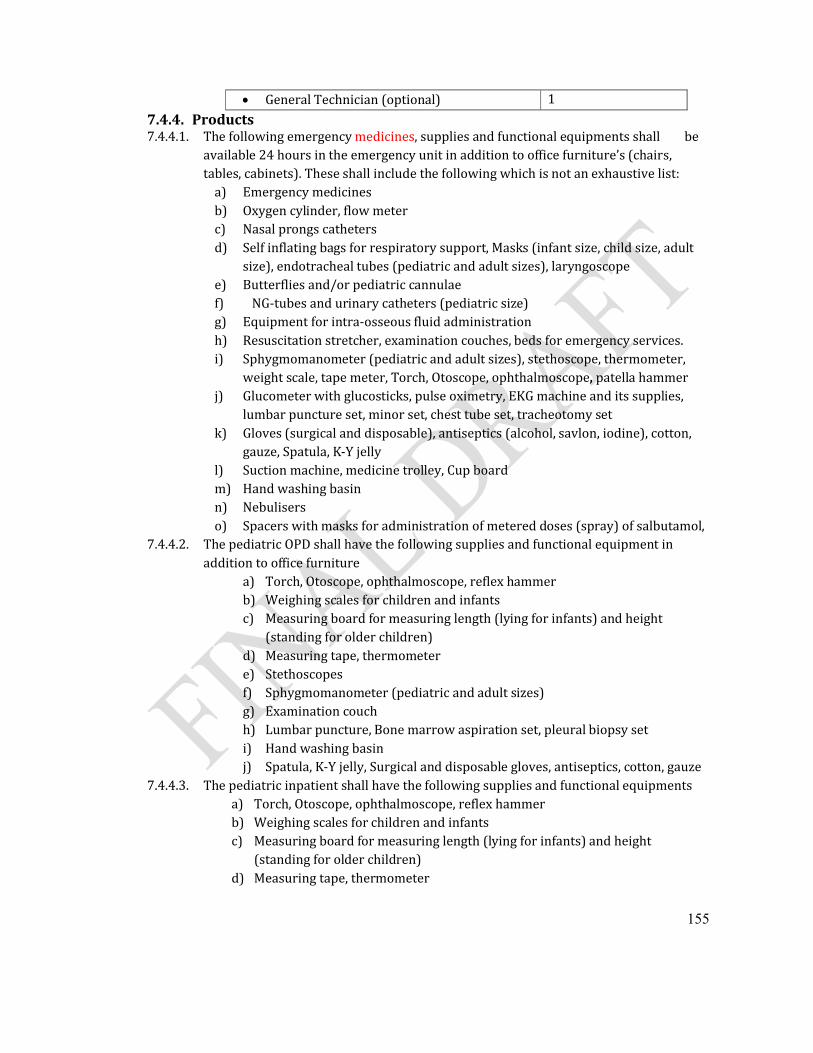
155
General Technician (optional) 1
7.4.4. Products7.4.4.1. The following emergency medicines, supplies and functional equipments shall be
available 24 hours in the emergency unit in addition to office furniture’s (chairs, tables, cabinets). These shall include the following which is not an exhaustive list:
a) Emergency medicinesb) Oxygen cylinder, flow meter c) Nasal prongs catheters d) Self inflating bags for respiratory support, Masks (infant size, child size, adult
size), endotracheal tubes (pediatric and adult sizes), laryngoscope e) Butterflies and/or pediatric cannulae f) NG-tubes and urinary catheters (pediatric size) g) Equipment for intra-osseous fluid administrationh) Resuscitation stretcher, examination couches, beds for emergency services.i) Sphygmomanometer (pediatric and adult sizes), stethoscope, thermometer,
weight scale, tape meter, Torch, Otoscope, ophthalmoscope, patella hammerj) Glucometer with glucosticks, pulse oximetry, EKG machine and its supplies,
lumbar puncture set, minor set, chest tube set, tracheotomy setk) Gloves (surgical and disposable), antiseptics (alcohol, savlon, iodine), cotton,
gauze, Spatula, K-Y jellyl) Suction machine, medicine trolley, Cup boardm) Hand washing basinn) Nebulisers o) Spacers with masks for administration of metered doses (spray) of salbutamol,
7.4.4.2. The pediatric OPD shall have the following supplies and functional equipment in addition to office furniture
a) Torch, Otoscope, ophthalmoscope, reflex hammerb) Weighing scales for children and infantsc) Measuring board for measuring length (lying for infants) and height
(standing for older children) d) Measuring tape, thermometere) Stethoscopesf) Sphygmomanometer (pediatric and adult sizes)g) Examination couchh) Lumbar puncture, Bone marrow aspiration set, pleural biopsy seti) Hand washing basinj) Spatula, K-Y jelly, Surgical and disposable gloves, antiseptics, cotton, gauze
7.4.4.3. The pediatric inpatient shall have the following supplies and functional equipmentsa) Torch, Otoscope, ophthalmoscope, reflex hammerb) Weighing scales for children and infantsc) Measuring board for measuring length (lying for infants) and height
(standing for older children) d) Measuring tape, thermometer
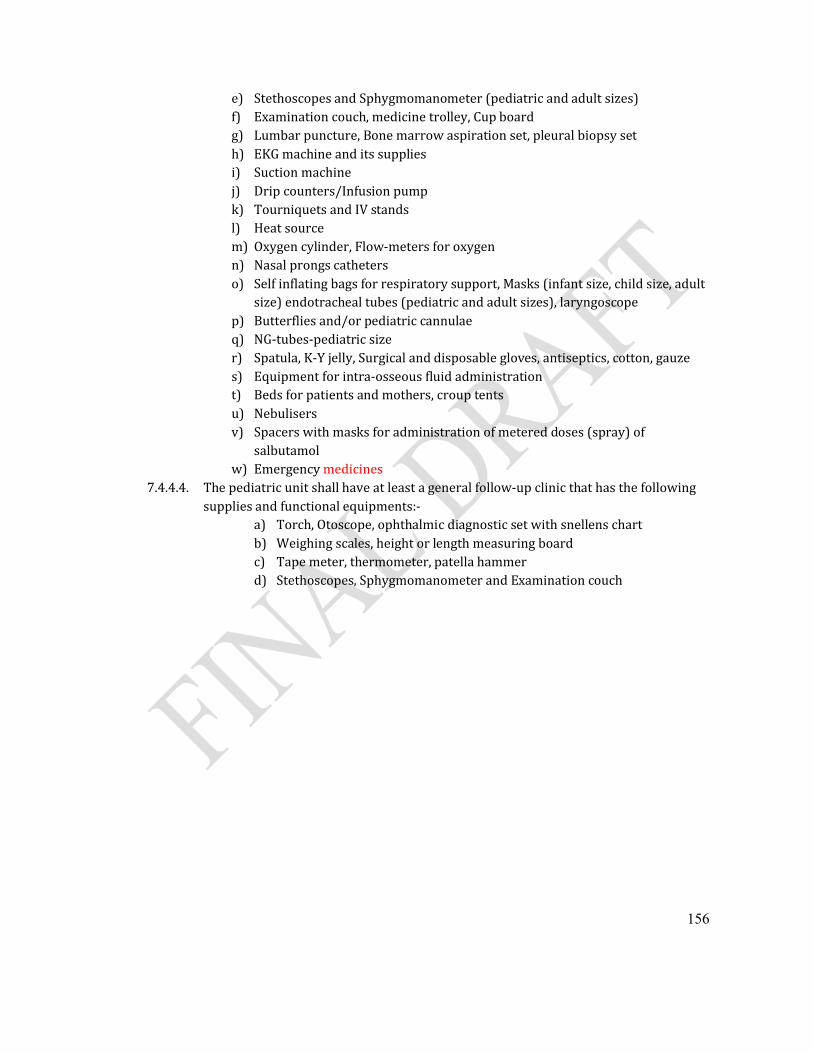
156
e) Stethoscopes and Sphygmomanometer (pediatric and adult sizes)f) Examination couch, medicine trolley, Cup boardg) Lumbar puncture, Bone marrow aspiration set, pleural biopsy seth) EKG machine and its suppliesi) Suction machinej) Drip counters/Infusion pumpk) Tourniquets and IV standsl) Heat sourcem) Oxygen cylinder, Flow-meters for oxygenn) Nasal prongs catheters o) Self inflating bags for respiratory support, Masks (infant size, child size, adult
size) endotracheal tubes (pediatric and adult sizes), laryngoscope p) Butterflies and/or pediatric cannulae q) NG-tubes-pediatric size r) Spatula, K-Y jelly, Surgical and disposable gloves, antiseptics, cotton, gauzes) Equipment for intra-osseous fluid administrationt) Beds for patients and mothers, croup tents u) Nebulisers v) Spacers with masks for administration of metered doses (spray) of
salbutamolw) Emergency medicines
7.4.4.4. The pediatric unit shall have at least a general follow-up clinic that has the following supplies and functional equipments:-
a) Torch, Otoscope, ophthalmic diagnostic set with snellens chartb) Weighing scales, height or length measuring board c) Tape meter, thermometer, patella hammerd) Stethoscopes, Sphygmomanometer and Examination couch
157
7.5. Orthopedic Center7.5.1. Practices7.5.1.1. Orthopedic surgical service shall be available 24 hours a day, 365 days a year, 7.5.1.2. Services for non-emergency elective orthopedic surgical cases shall be available only
when all the necessary experts are available; 7.5.1.3. There shall be written protocols and procedures for admissions and discharges with
follow up.7.5.1.4. There shall be protocols for the management of the orthopedic surgical conditions in
the unit. 7.5.1.5. There shall be protocols for consultation and transfer of patients admitted to this unit.7.5.1.6. There shall be a clear policy for handling emergency orthopedic surgical conditions. 7.5.1.7. The Center shall make sure the emergency orthopedic surgical services is available,
staffed with the necessary technical staff, equipped with all the necessary facilities including emergency transfusion, transportation, and electric back up.
7.5.1.8. The admission process for emergency orthopedic surgery shall be done by the emergency/ duty physician with consultation to the duty orthopedic surgeon.
7.5.1.9. The admission process for elective orthopedic surgery shall be done by the respective orthopedic surgeon in consultation with the anesthesia department and with the other departments as needed.
7.5.1.10. For admitted patients the orthopedic surgical service shall be organized in such a way that it covers all the shifts.
7.5.1.11. The orthopedic center shall be directed by a licensed orthopedic surgeon. 7.5.1.12. There shall be a mechanism of interdepartmental consultations with orthopedic
center for which the orthopedic surgeon on duty shall be responsible. 7.5.1.13. Adequate orthopedic center records shall be kept for each patient and the patient’s.7.5.1.14. All orthopedic surgical procedures (except in life-threatening emergencies) are
performed only after appropriate history, physical examination, and indicated diagnostic tests are completed and documented in the patient’s medical record.
7.5.1.15. The preoperative diagnosis shall be recorded in the medical record for all patients prior to orthopedic surgery.
7.5.1.16. The orthopedic surgeon shall explain the disease condition, possible orthopedic surgical intervention and outcome possibilities in clear, simple and understandable terms to the patient and/or family.
7.5.1.17. Except in life-threatening emergencies, the orthopedic surgeon shall obtain an informed consent and this must be documented in the patient’s medical record. For the case with life threatening condition, consent shall be obtained from spouse, family, guardian or based on the orthopedic surgeon’s clinical judgment.
7.5.1.18. If there is no body to sign the consent for the patient who is in life-threatening condition, the reason for not having the consent shall be stated.
158
7.5.1.19. The nursing care of patients undergoing orthopedic surgery shall be planned and documented in the medical record, directed by a trained nurse, and includes the following:
(a) Pre-operative care,(b) Location of post-operative care, (c)Type of post-operative care and monitoring needed, (d) Pain management, and (e) Patient’s understanding of discharge instructions.
7.5.1.20. Operative reports shall be written in the patient’s record and in the OR registration book immediately after orthopedic surgery and include at least the following:
(a) Patient identification, (b) Pre-operative diagnosis, (c) The procedure performed, (d) Findings during orthopedic surgery, (e) Post-operative diagnosis, (f) Orthopedic surgical specimens removed, (g) Date and time operation started and ended, (h) Name of orthopedic surgeon, anesthesiologist/anesthetist, scrub nurse, and
any assistants, (i) Signature of the orthopedic surgeon, and the scrub nurse (j) Immediate post-operative orders explicitly in the order sheet.
7.5.1.21. There shall be policy that leads to positively identify the patient and ensure that the correct procedure and the correct side are confirmed prior to starting the orthopedic surgery.
7.5.1.22. There shall be processes and policies defining the appropriate safety before, during and immediately after orthopedic surgery, including at least the following:
(a) The orthopedic surgeon shall fill the pathology form and the specimen container shall be properly labeled. The container shall be filled with 10% formalin.
(b) The specimen shall be sent to the pathology department by the OR staff. It there no pathology department in the same center, the specimen shall be sent to another facility by a family member or a relative.
Aseptic technique,
Sterilization and disinfections,
Selection of draping and gowning,
Counting of sponges, instruments, and needles, 7.5.1.23. There shall be a protocol for patient transfer from operation theatre to recovery room.
This includes; (a) The handover and/or transfer of immediate post-operative patients shall be
done between the anesthetist or anesthesiologist who administered the anesthesia and the registered nurse in recovery room,
(b) The nurse in the recovery room shall immediately re-evaluate the condition of the patient in front of the anesthesiologist or anesthetist,
159
(c) The follow up of immediate post-operative patients in the recovery room shall be done by registered nurse with special training or similar experience until the anesthesiologist, anesthetist or other qualified physician makes the decision to transfer the patient from post-anesthesia care and this decision shall be based on the documented results of monitoring during anesthesia recovery,
(d) The transfer from recovery room shall be done after the transfer order is signed by the appropriate anesthetist, anesthesiologist, or other qualified physician,
(e) The nurse in the recovery room shall inform the ward and the ward nurse shall transfer the patient with the signed transfer note.
7.5.1.24. Post- operative patient in the wards shall get post operative care by qualified nurses.The post operative care includes to the minimum:
(a) Evaluation by the orthopedic surgeon or appropriate physician and ward nurses daily or whenever needed,
(b) Follow up of vital signs and carrying out of post-operative orders shall be done as per the order specified for individual patients. (special orders-NPO, positioning, exercise, drainages, etc.,)
7.5.1.25. The center shall have an Intensive Care Unit (ICU) with all requirements stipulated under ICU standards
7.5.1.26. The center shall provide anesthesia services as per the standards stipulated under the anesthesia services
7.5.1.27. The Center shall have clear protocol for orthopedic surgical activities to be done at outpatients level, orthopedic surgical referral clinics, follow up clinics, minor operations and orthopedic procedures
7.5.1.28. There shall be no time left without having general orthopedic surgeon or physician attending the orthopedic Center.
7.5.1.29. There shall be a policy or procedure that clearly shows at least one orthopedic surgeon shall be on call/ on duty to respond for orthopedic surgical requests from emergency and/ or orthopedic ward physician.
7.5.1.30. There shall be a mechanism that the orthopedic surgeon shall be available within 30 minutes upon call.
7.5.1.31. All patients in orthopedic center shall be attended by registered nurse all the time with supervision by duty physician.
7.5.2. Premises 7.5.2.1. The orthopedic Center shall include orthopedic wards, operation room, recovery
room, the central sterilization room (CSR), toilet rooms, showers and changing rooms with lockers, offices, store rooms, clean and dirty utility rooms, duty rooms and cleaners room.
7.5.2.2. The operation room shall be readily accessible to the orthopedic wards. 7.5.2.3. Orthopedics Operation Room / Suite:
160
(a) The operation room shall have three operation theatres of which one is for septic procedures, one nurse station, four staff toilets, six shower stands, four changing rooms with lockers, one rest room, anesthesia store, nurse store, one general store.
(b) An operating room shall have access- restricted environment where orthopedic surgical and invasive interventions are performed. It shall be organized and equipped so that OR trafficking shall be controlled and exercised over all persons and materials entering and leaving the area.
7.5.2.4. Operation Theatre:(a) At least one standard size operation theatre and one septic operation theatre shall
be available (b) The wall of the operation theatres shall be washable; the vicinity of plumbing
fixtures shall be smooth and water resistant i.e., ceramic plated up to the ceiling. (c) The ceiling shall be monolithic, scrub-able and capable of withstanding chemicals.
Cracks or perforation in these ceilings are not allowed. (d) Floors and walls penetrated by pipes, ducts and conduits’ shall be tightly sealed. (e) The floor of the theatre shall be smooth, easily cleanable, non-slippery and non-
staining and it shall not be affected by water or germicidal cleaning solutions; preferably made of marble or ceramic.
(f) There shall be drainage on the floor, (g) There shall be at least six fixed electric outlets in each theatre with cover, (h) The entrance and exit doors to the theatre shall be fitted with self-closing double
doors, (i) There shall be at least one operation table in each theatre, (j) At least one ceiling operation light and one mobile operation light per theatre shall
be available (k) Glass cabinet and shelves shall be available(l) The OR shall be thoroughly cleansed weekly. (m)Heater fixed on the wall shall be available in each theatre,
7.5.2.5. Scrub area:(a) There shall be a scrubbing-up area outside but adjacent to the operating
theatre(s). The scrub area shall be in between the two self closing doors. If there is one common scrub area for the four theatres, it shall be wide enough to accommodate four staff scrubbing simultaneously.
(b) This area shall have direct access to the operating room, (c) It shall be provided with multiple sinks or with wide sink and taps for running
(warm) water. The taps for running water for scrubbing shall be hand free to be manipulated with elbow or knee joint. (e.g., long arm of valve gate to be manipulated with elbow or knee joint.)
7.5.2.6. Nurse station:(a) This is a room within the restricted access areas, which is so situated,
constructed and equipped that it is possible for the nursing staff to observe patients directly and where necessary, to render assistance. This area need not
161
be a room, but may form an integral part of the main patient corridor, recovery area or bed-receiving area.
(b) There shall be a corridor or allocated area for keeping charged and empty Oxygen cylinders; the empty and charged oxygen cylinders shall be labeled clearly,
7.5.2.7. Entrance/Patient Transfer Area:(a) This area shall be large enough to allow for the transfer of patients from a bed to
OR stretcher. (b) A line shall be clearly marked in red on the floor, beyond which no person shall
be permitted to set foot without putting on protective clothing and OR shoes. (c) Holding bay: there shall be a space or corridor to keep and observe pre-operative
patients until called to theatre. 7.5.2.8. Staff Change Rooms
(a) Suitable two separate changing room facilities shall be available and clearly labeled for male and female,
(b) Each changing rooms shall have two doors, one entrance and the second door accessing into the restricted access area; the entrance is from outside the restricted access area.
(c) Each changing room shall be provided with a locker for a minimum of 10 staff to keep personal clothes and belongings.
(d) Each changing room shall be provided with shelves for Storage of clean theatre attire and inside shoes and operation theatre gum boots.
(e) Separate storage bin shall be provided for used and soiled theatre apparels. (f) Wash hand basins: Toilets, showers,
7.5.2.9. Set-up Area (optional): (a) Store area for suture materials and other supplies from where necessary
consumables could be stacked on a trolley that could be wheeled into theatre for subsequent procedure.
(b) Doors into the operating room shall be big enough to wheel through the set trolleys from the set up room into the operating room without contact with doors or non sterile surfaces.
(c) Packed instruments and other relevant materials shall be brought from the CSR and stored in this area according to the daily schedules one day prior to the scheduled operations.
(d) Mayo table and dressing trolley to set up for the next case are kept in this area. (e) If there is no set up area the instruments can be set up within the operating
theatre 7.5.2.10. Operating Theatre Equipment Store
(a) There shall be equipment store area in the operating room that shall be supplied with a sufficient number of electrical plugs to keep the electrical equipments plugged in, charged and in case of power failure to work as back up electrical supply / or emergency electrical supply.
(b) Equipments shall always be stored at the same space/location and properly labeled.
162
(c) Shelves and cabinets 7.5.2.11. Operating Theatre Sterile Supply Store: This shall be a room which is used for the
storage of all sterile instrument sets, swabs and sterile renewable, consumables and it requires shelves.
7.5.2.12. Clean Utility, Orthopedic surgical Suite: There shall be a room allocated for storage of IV fluids, clean linen, medicines and other sundry items. Requirements: (a) Shall be situated where OR staff have easy access to the clean utility store. (b) Metallic washable rack for storage shall be available, (c) Equipments used for special procedures like splints shall be kept here thoroughly
cleaned after use, (d) Refrigerator with thermometer shall be available for medicines requiring a
temperature range of 4 to 8 °C. (e) Sink, cabinets and shelves
7.5.2.13. Soiled Utility/Sluice room shall be available with the followings:(a) This room shall be located at the back of the OR. (b) This room shall be for keeping contaminated materials until they are disposed. (c) Sharp containers, leak proof containers with lids shall be available, used
sharps/safety boxes are to be stored here before being sent for incineration. (d) Container for temporary storage point for soiled linen, (e) Hand Washing basin, (f) Drainage on the floor, (g) Trolley for soiled materials and waste human tissues,
7.5.2.14. Cleaner’s Room shall be available with the followings:(a) A room provided with 2 sets of cleaning equipments and materials, (b) Hand washing Basin, (c) Washing sink, (d) Detergent proof shelves and cabinets.
7.5.2.15. Central sterilization room shall be available with followings:(a) Direct access to OR, (b) Needs a minimum of needs rooms:
One for reception, sorting of equipments; or clothes and documentation process;
One for inbuilt autoclaves;
One separate properly ventilated room for storing and shelving sterile clothes and instruments as per the guideline,
One staff room and
One cleaners’ room (c) Shall have at least two inbuilt autoclaves, with small one as backup, (d) Continuous water supply with extra reservoir, (e) Shelves shall be washable ,corrosive free and metallic racks as per the guideline, (f) The date of sterilization & the name of the instruments shall be written after
sterilization. (g) Staff toilets,
163
7.5.2.16. Recovery facilities shall be available with the followings:(a) It shall be close to OR, and shall be within the semi- restricted area. (b) A minimum of four beds shall be available, (c) There shall be a minimum of 1.2 meter gap between beds for patient
transferring stretcher, (d) Recovery beds shall have flexible side protections, (e) A minimum of two electric outlets shall be available for each bed, (f) A trolley carrying functional emergency equipments shall be available in the
recovery room, (g) A minimum of four bed pans (h) A minimum of four patient screens shall be available, (i) There shall be sufficient light for each bed, one head light per bed, (j) There shall be a heater,
7.5.2.17. Minor operation theatre shall be available with the followings:(a) It shall hall be located accessible to OPD, and shall be with low or no traffic area. (b) There shall be one operation room with two theatres, (c) There shall be two glass cabinets for orthopedic surgical consumables in the OR, (d) There shall be two patient changing rooms, (e) There shall be mark on the floor restricting movement of unauthorized and/or
person without OR suit, (f) Rest room (g) Utility room, (h) Store with shelves and cabinets, (i) Nurse station with table and chairs, (j) Toilet rooms for male female, (k) Cleaners room,
7.5.2.18. Orthopedic ward shall be available with the followings;(a) It shall be part of the inpatient service, (b) In addition to emergency and isolation beds, the specialty center shall have at
least ten inpatient beds.(c) The beds shall be flexible and orthopedic beds, (d) In third class, space between beds shall be at least 1.2m. (e) There shall be a minimum of one separate room, labeled “Septic Room” for septic
patients, (f) The beds shall be equipped with fixtures for certain orthopedic surgical patients-
orthopedic cases (g) Patient screens, (h) Patient toilets and showers with proximity to the ward, or covered walkways to
the ablution facilities. 7.5.2.19. Orthopedics ward Nurses’ station shall be available with the following;
(a) located amidst of the wards (b) shall have table and chairs (c) shall have lockable cabinets,
164
(d) shall have specimen collection station/ laminated table with racks (e) shall have hand washing basin,
7.5.2.20. Orthopedic ward clean utility room (procedure room) shall be available with the following;(a) Dressing trolleys ,beds (b) POP equipments sets, (c) Deep Sink, (d) Hand washing basin, (e) Worktable with laminated top, (f) Cabinets and shelves,
7.5.2.21. Orthopedic ward clean linen room with shelves and cabinets shall be available 7.5.2.22. Orthopedic ward in patient store with shelves, cabinets and fixed electrical plugs
with protection shall be available7.5.2.23. Orthopedic ward soiled utility room with shelves and leak proof containers with
leads shall be available 7.5.2.24. Orthopedic ward cleaner’s room shall be available with the following
(a) Hand washing basin, (b) Sinks and cleaning equipments, (c) Shelves and Cabinet, (d) One room for keeping patients belongings with lockers.
7.5.2.25. The premises requirement is summarized in the following table.Rooms required #
requiredArea required
Reception, registration/ recording & waiting area 1 40sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Emergency room with 2 resuscitation couches 1 16sq. m
Toilet room (male & female) (OPD) 4 16 sq. m
Minor OR/ procedure room,o Minor operation theatre 1 20 sq. mo Patient changing room/ area 1 6sq. mo Nurse station & Recording room 1 12sq. mo Clean Utility room 1 6sq. mo Mini-Store room 1 6sq. mo Soiled utility room 1 6sq. m
Operation Roomo Operation theatre 2 60sq. mo Scrub area 1 12sq. mo Staff Change area 2 12sq. mo Clean utility room 1 6sq. mo Soiled utility room 1 6sq. mo Nurse station 1 12sq. m

165
o Anesthesia store 1 8sq. mo OR equipment store 1 12sq. mo Sterile supply room 1 12sq. mo Doctor’s office 1 12sq. mo Duty room 1 8sq. mo Janitor’s closet 1 6sq. mo Toilet rooms 2 8sq. mo Shower rooms 2 8sq. m
Recovery room (with 2 beds) 1 16sq. m
Sterilization room 1 20sq. m
Physiotherapy room 1 16sq.m
Surgical ward/ inpatient roomo Patient rooms for a minimum of 10 orthopedic
beds {with maximum room capacity not more than 6 beds}
2 96sq. m
o Isolation rooms 2 30sq. mo Nurse station 1 12sq. mo Duty rooms with lockers (male/ female) 2 16sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 12sq. mo Toilet rooms (can be in each patient room) 4 16sq. m
Intensive Care Unit (Optional)o IC room 1 40sq. mo Nurse station (inside IC room) 1 Included o Change room/ Nurse locker 1 12sq. mo Clean utility room 1 6sq. mo Soiled Utility/ Sluice room 1 6sq. mo Staff room 1 12sq. mo ICU mini- store room 1 12sq. mo Toilets 2 8sq. mo Cleaner’s closet 1 6sq. m
Laboratory room (can be 1 room with open platform)
1
o Specimen collection 1 6sq. mo Hematology & Clinical chemistry 1 12sq. mo Parasitology, urinalysis & serology 1 9sq. mo Disinfection & sterilization room (shared) 1 9sq. mo Blood bank/ storage room 1 9sq. mo Duty room 1 9sq.m
CT or MRI room (Optional) 1 28sq. m
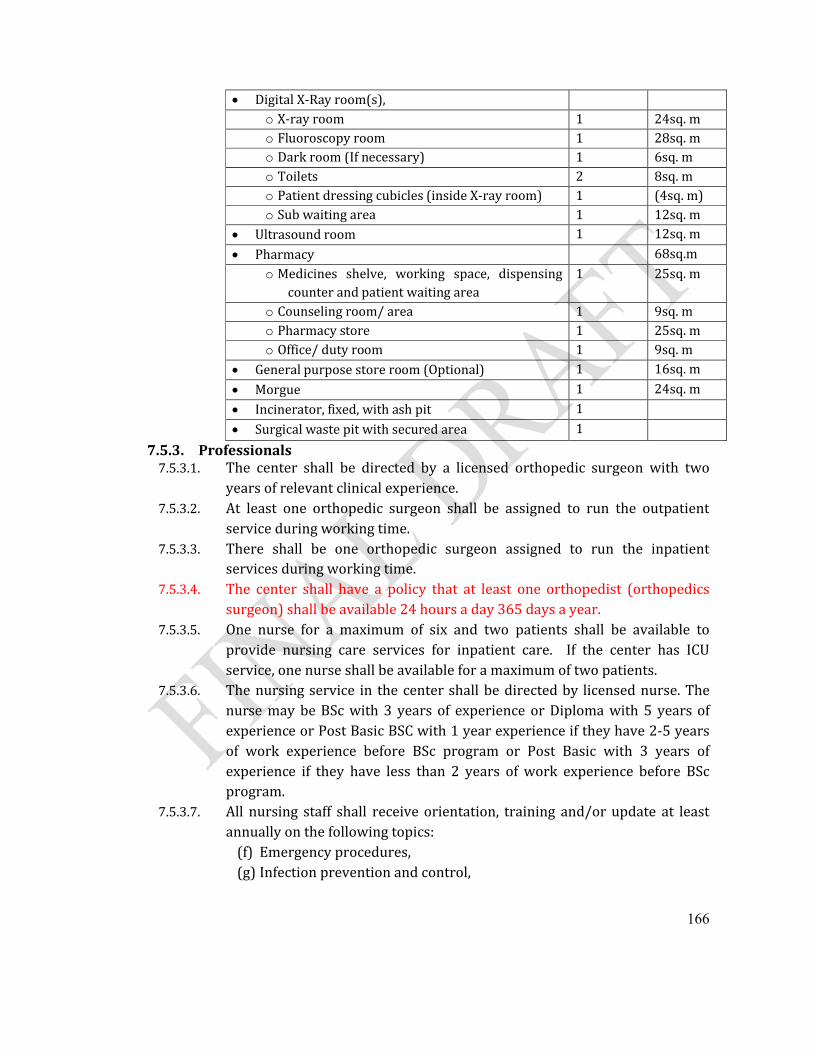
166
Digital X-Ray room(s),o X-ray room 1 24sq. mo Fluoroscopy room 1 28sq. mo Dark room (If necessary) 1 6sq. mo Toilets 2 8sq. mo Patient dressing cubicles (inside X-ray room) 1 (4sq. m)o Sub waiting area 1 12sq. m
Ultrasound room 1 12sq. m
Pharmacy 68sq.mo Medicines shelve, working space, dispensing
counter and patient waiting area1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 9sq. m
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
Surgical waste pit with secured area 1
7.5.3. Professionals 7.5.3.1. The center shall be directed by a licensed orthopedic surgeon with two
years of relevant clinical experience. 7.5.3.2. At least one orthopedic surgeon shall be assigned to run the outpatient
service during working time. 7.5.3.3. There shall be one orthopedic surgeon assigned to run the inpatient
services during working time.7.5.3.4. The center shall have a policy that at least one orthopedist (orthopedics
surgeon) shall be available 24 hours a day 365 days a year.7.5.3.5. One nurse for a maximum of six and two patients shall be available to
provide nursing care services for inpatient care. If the center has ICU service, one nurse shall be available for a maximum of two patients.
7.5.3.6. The nursing service in the center shall be directed by licensed nurse. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
7.5.3.7. All nursing staff shall receive orientation, training and/or update at least annually on the following topics:
(f) Emergency procedures,(g) Infection prevention and control,
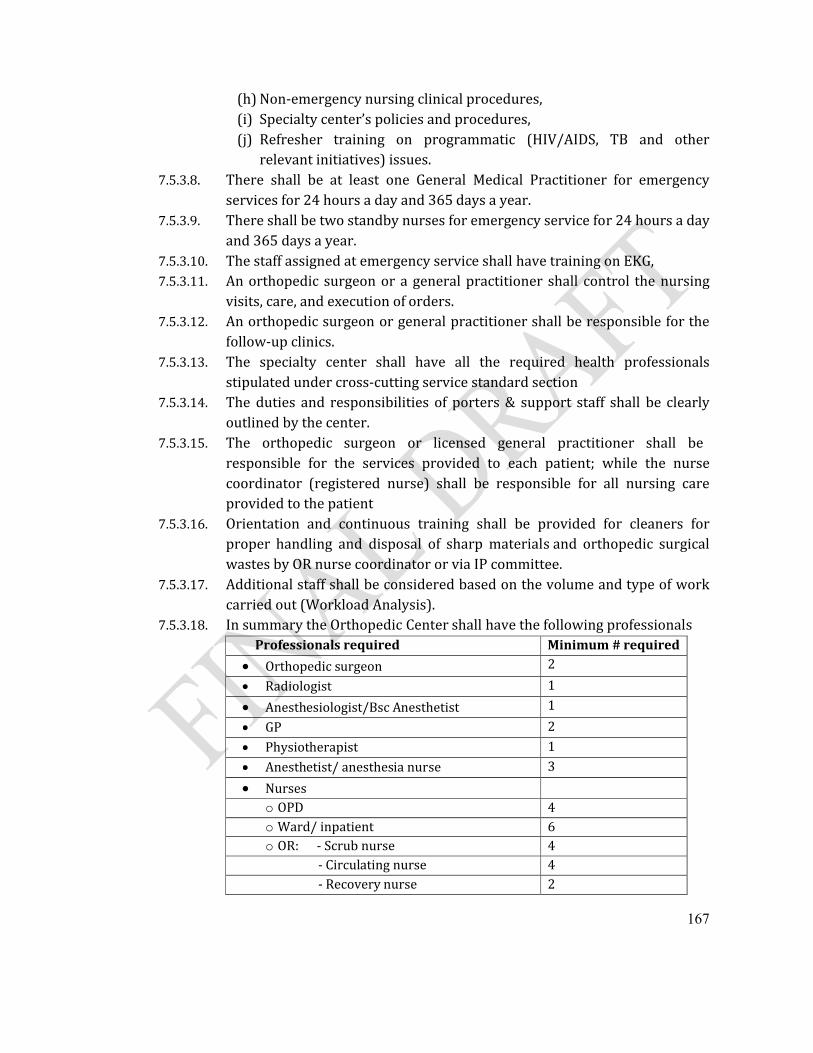
167
(h) Non-emergency nursing clinical procedures,(i) Specialty center’s policies and procedures,(j) Refresher training on programmatic (HIV/AIDS, TB and other
relevant initiatives) issues.7.5.3.8. There shall be at least one General Medical Practitioner for emergency
services for 24 hours a day and 365 days a year.7.5.3.9. There shall be two standby nurses for emergency service for 24 hours a day
and 365 days a year.7.5.3.10. The staff assigned at emergency service shall have training on EKG,7.5.3.11. An orthopedic surgeon or a general practitioner shall control the nursing
visits, care, and execution of orders.7.5.3.12. An orthopedic surgeon or general practitioner shall be responsible for the
follow-up clinics.7.5.3.13. The specialty center shall have all the required health professionals
stipulated under cross-cutting service standard section7.5.3.14. The duties and responsibilities of porters & support staff shall be clearly
outlined by the center. 7.5.3.15. The orthopedic surgeon or licensed general practitioner shall be
responsible for the services provided to each patient; while the nurse coordinator (registered nurse) shall be responsible for all nursing care provided to the patient
7.5.3.16. Orientation and continuous training shall be provided for cleaners for proper handling and disposal of sharp materials and orthopedic surgical wastes by OR nurse coordinator or via IP committee.
7.5.3.17. Additional staff shall be considered based on the volume and type of work carried out (Workload Analysis).
7.5.3.18. In summary the Orthopedic Center shall have the following professionalsProfessionals required Minimum # required
Orthopedic surgeon 2
Radiologist 1
Anesthesiologist/Bsc Anesthetist 1
GP 2
Physiotherapist 1
Anesthetist/ anesthesia nurse 3
Nurseso OPD 4o Ward/ inpatient 6o OR: - Scrub nurse 4
- Circulating nurse 4 - Recovery nurse 2
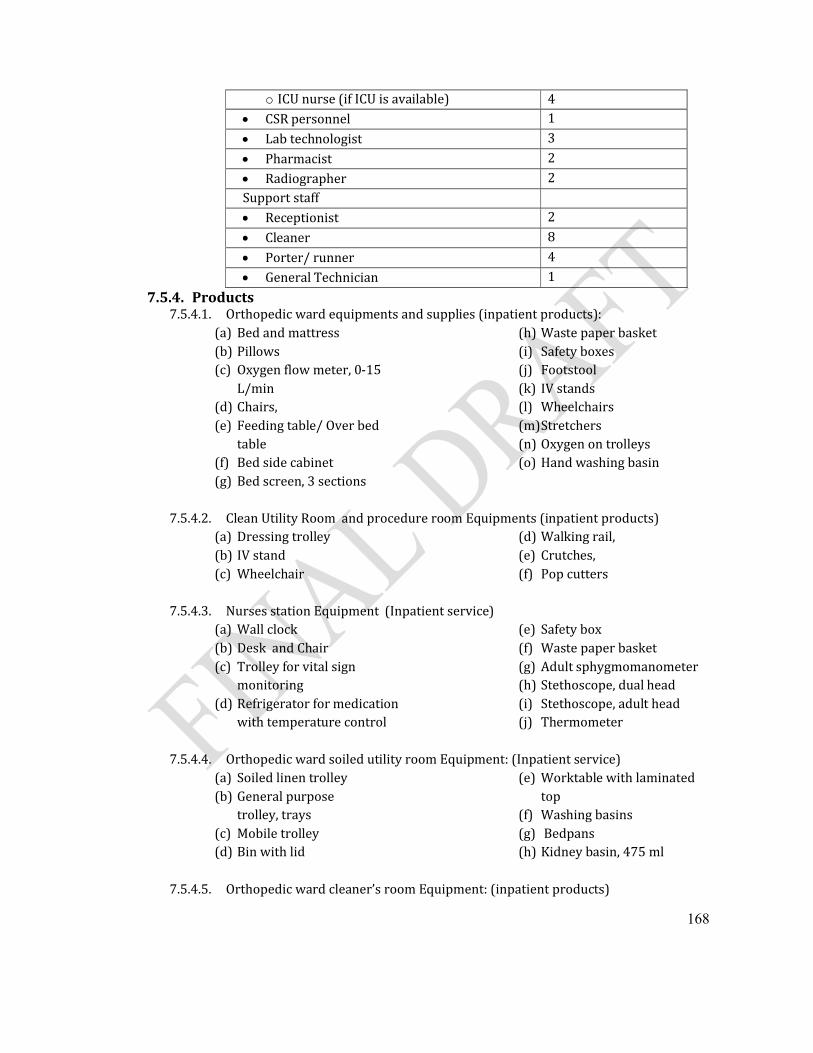
168
o ICU nurse (if ICU is available) 4 CSR personnel 1
Lab technologist 3
Pharmacist 2
Radiographer 2Support staff Receptionist 2
Cleaner 8
Porter/ runner 4
General Technician 1
7.5.4. Products 7.5.4.1. Orthopedic ward equipments and supplies (inpatient products):
(a) Bed and mattress (b) Pillows (c) Oxygen flow meter, 0-15
L/min (d) Chairs, (e) Feeding table/ Over bed
table (f) Bed side cabinet (g) Bed screen, 3 sections
(h) Waste paper basket (i) Safety boxes (j) Footstool (k) IV stands (l) Wheelchairs (m)Stretchers (n) Oxygen on trolleys (o) Hand washing basin
7.5.4.2. Clean Utility Room and procedure room Equipments (inpatient products)(a) Dressing trolley (b) IV stand (c) Wheelchair
(d) Walking rail, (e) Crutches, (f) Pop cutters
7.5.4.3. Nurses station Equipment (Inpatient service)(a) Wall clock (b) Desk and Chair (c) Trolley for vital sign
monitoring (d) Refrigerator for medication
with temperature control
(e) Safety box (f) Waste paper basket (g) Adult sphygmomanometer (h) Stethoscope, dual head(i) Stethoscope, adult head (j) Thermometer
7.5.4.4. Orthopedic ward soiled utility room Equipment: (Inpatient service)(a) Soiled linen trolley (b) General purpose
trolley, trays (c) Mobile trolley(d) Bin with lid
(e) Worktable with laminated top
(f) Washing basins (g) Bedpans (h) Kidney basin, 475 ml
7.5.4.5. Orthopedic ward cleaner’s room Equipment: (inpatient products)
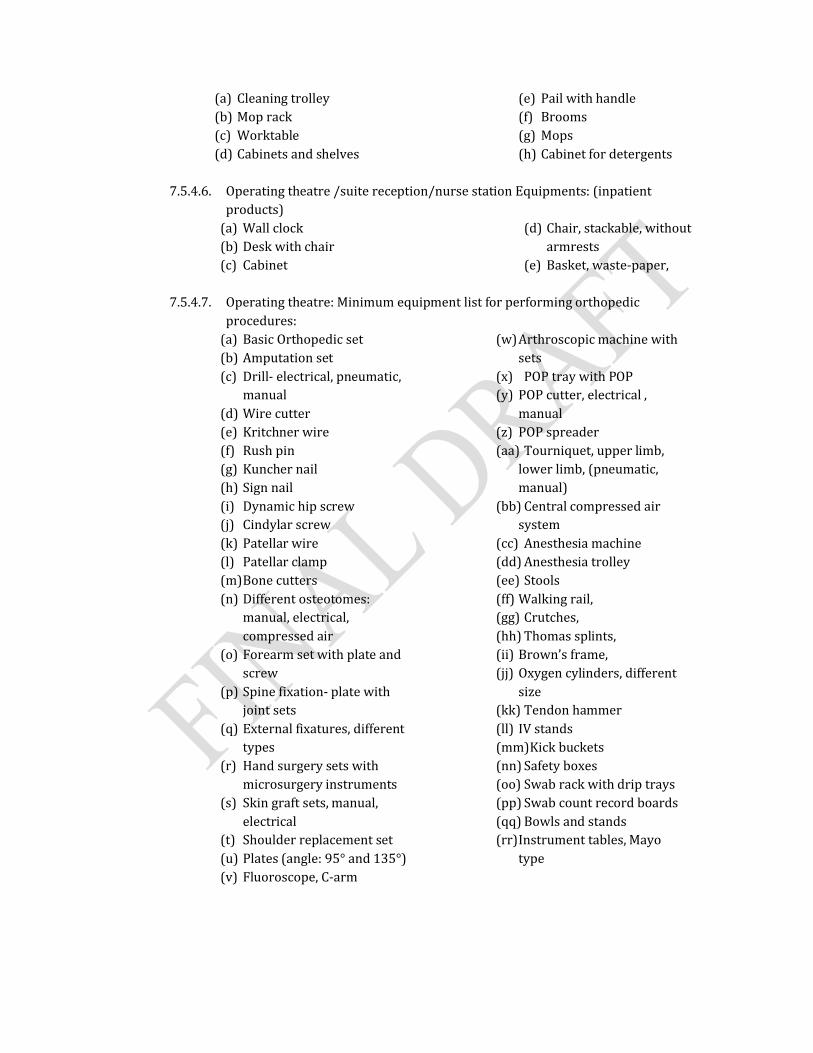
(a) Cleaning trolley (b) Mop rack (c) Worktable (d) Cabinets and shelves
(e) Pail with handle (f) Brooms (g) Mops (h) Cabinet for detergents
7.5.4.6. Operating theatre /suite reception/nurse station Equipments: (inpatient products)
(a) Wall clock (b) Desk with chair (c) Cabinet
(d) Chair, stackable, without armrests
(e) Basket, waste-paper,
7.5.4.7. Operating theatre: Minimum equipment list for performing orthopedic procedures:
(a) Basic Orthopedic set (b) Amputation set(c) Drill- electrical, pneumatic,
manual (d) Wire cutter(e) Kritchner wire(f) Rush pin(g) Kuncher nail(h) Sign nail(i) Dynamic hip screw(j) Cindylar screw(k) Patellar wire(l) Patellar clamp(m)Bone cutters(n) Different osteotomes:
manual, electrical, compressed air
(o) Forearm set with plate and screw
(p) Spine fixation- plate with joint sets
(q) External fixatures, different types
(r) Hand surgery sets with microsurgery instruments
(s) Skin graft sets, manual, electrical
(t) Shoulder replacement set(u) Plates (angle: 95° and 135°)(v) Fluoroscope, C-arm
(w)Arthroscopic machine with sets
(x) POP tray with POP(y) POP cutter, electrical ,
manual(z) POP spreader(aa) Tourniquet, upper limb,
lower limb, (pneumatic, manual)
(bb) Central compressed air system
(cc) Anesthesia machine(dd) Anesthesia trolley (ee) Stools (ff) Walking rail, (gg) Crutches, (hh) Thomas splints, (ii) Brown’s frame, (jj) Oxygen cylinders, different
size (kk) Tendon hammer (ll) IV stands (mm)Kick buckets (nn) Safety boxes (oo) Swab rack with drip trays (pp) Swab count record boards (qq) Bowls and stands (rr)Instrument tables, Mayo
type
170
(ss)Framed boards with pencil trays
(tt) Blankets, warming (uu) Coagulation unit, electro-
cauthery, mobile, 200 W (vv) Lights, operating, 1 large
copula, ceiling mounted (ww) Mobile operating lights (xx) Operating table, 3 sections
(yy) Suction machines (zz) Hip spica tables (aaa) Anesthesia machine with
ventilator, 2 vaporizers, and gas cylinders
(bbb) Apron, protective,
7.5.4.8. In addition to equipments mentioned under radiological services, the center shall have
(a) Digital X-ray machine(b) Fluoroscopy
(c) CT/MRI (optional)(d) Ultrasound
7.5.4.9. The center shall have physiotherapy facilities7.5.4.10. Surgery Equipment – OR sterile supply store:
(a) General purpose trolleys, trays
(b) General surgery-Suture set(c) Minor set
7.5.4.11. Renewable/Consumables for orthopedic surgical service: (as per the surgical service standard)
(a) Tongue depressors(b) Guedel airways: size 0,
00, 3, 4 & 5 (c) Disposable aprons (d) Bags - Refuse - All Colors
and Sizes (e) Bags – Urine (f) Bandage -(g) Batteries - Medical &
General (h) Bedpan Covers (i) Blood Administration
Sets (j) Blood Sampling
Needles, disposable, sterile, 20 G, 21 G, 23 G
Tube, Vacuum 5ml (Vacutainer)
Tube, Vacuum EDTA 5ml (Vacutainer)
Tube, Vacuum Heparinised 5ml (Vacutainer)
Vacutainer Holder
Vacutainer needle
(k) Bottles - Suction -Glass/Plastic
(l) Braun Splints (Arm) (m)Bubble tubing box (n) Cannula - Nasal-Oxygen (o) Cannula, IV short, ster,
disp, 18G, 20 G, 22 G, 24 G
(p) Caps - Mop/Bonnet Type (q) Catheter - Jacques (r) Chest, Electrode, Monitor (s) Cleansing Swabs – Sterile (t) Cleansing Swabs Non-
Sterile (u) Cold/Hot Packs (v) Connector,
Biconical Autoclavable
Connector, T/Y
Connectors - Plastic –Tapered
(w)Container, Sample, urine, plastic, non-sterile, 60 ml
(x) Cotton
Cotton Buds
171
Cotton Wool Balls -Sterile/Non-Sterile
Cotton Wool Rolls (y) POP (z) Covers - PVC -
Mattress/Bed Wedge (aa) CVP – Cannulae (bb) Drawsheet,plastic,90x1
80cm (cc) Foley Catheters –
Latex/Silicone Size 10, 12 and 14
(dd) Gauze Absorbent Ribbon (ee) Gloves:
Household Large & Medium
Orthopedic surgical Size 6, 6 ½, 7, 7 ½, 8
Exam, latex, disp, large, medium, small
(ff) Hand wash Antiseptic Liquid (Hibiscrub)
(gg) Hand wash Povidone (Betadine)
(hh) Hot Packs (ii) I.V. Sets :
I.V. Administration Sets –15 Drop
I.V. Administration Sets -60 Drop
I.V. Set, Infusion “Y”, Luer lock, air inlet
(jj) Intubation stylet, adult, 15 Ch
(kk) IV Infusion set Buretrol (ll) K.Y. Jelly (mm) IV stands (nn) Drums (oo) Latex Tubing (pp) Linen Savers (qq) Nail Brushes -
Autoclavable/Disposable
(rr)Needles:
Spinal disp, (0.9x90mm),sterile, 20G, 22G, 24G
Disp,15G, 18G, 21G, 22G, 23G, 25G
Butterfly 23G (ss)Oxygen T Pieces (tt) Oxygen Tubing (uu) Face Masks (vv) Razor Medical -
Disposable - Single Edge (ww) Safety Pins Large &
Medium (xx) Sharps Containers
(Safety Box/used syringes and needles)
(yy) Shrouds (zz) Soap,toilet,bar,approx.1
10g,wrapped (aaa) Spigots Large, Medium
and Small (bbb)Spray Bottles - Plunger
Operated (ccc) Orthopedic surgical
Splints (ddd)Syringes:
Volume: 2ml, 5ml, 10ml, 20ml
Syringes 50 ml Conical Tip
Syringes 50 ml Luer Lock
Syringes Insulin (eee) Tape:
Elastic Adhesive Plaster - White 5cm and 10 cm
Micropore tape
Orthopedic surgical Adhesive Hypo-Allergenic
172
Adhesive, zinc oxide, perforated,10cmx5m
Adhesive, zinc oxide, 2.5cmx5m
(fff) Tourniquet, latex rubber,75cm
(ggg) Tourniquet, pneumatic (hhh)Tubes:
Endo-tracheal, disp. + connector, neonate mm, w.o balloon
Endo-tracheal, disp. + connector, balloon, 6.5mm, 7mm, 7.5mm, 8mm
Suction, L125cm,ster,disp, CH10, CH12, CH16
7.5.4.12. Operating Suite Renewable/Consumables:(a) Airway Guedel, pediatric &
adult size (b) Plastic, reusable aprons (c) Urine bags, collecting, 2000
ml (d) 012 Band, Esmarch, 6 cm x
5 m (e) Survival blanket,
220x140cm (f) Blood Sampling:
Needle, disposable, sterile, 20G, 21G
Tube, Vacuum 5ml (Vacutainer)
Tube, Vacuum EDTA 5ml (Vacutainer)
Tube, Vacuum Heparinised 5ml (Vacutainer)
Vacutainer holder
Vacutainer needles, 18-24G (g) Bouffant Nurse Cap (h) Cannula, IV short, ster, disp,
18G, 20G, 22G, 24G (i) Catheters:
Sup-Pubic, CH 10, 1.65 cm, ster, disp adult with trocar
Urethral, CH6, ster, disp
Urethral, CH7, ster, disp
Foley, ster, disp, CH10, CH12, CH14
(j) Compresses:
Abdominal compress, 40 x 40 cm
Compress, Swab, 20x 20 cm
Compress, gauze,10x10cm,n/ster/PAC-100
Compress, gauze,10x10cm,ster/PAC-5
Compress, paraffin,10x10cm,ster/BOX-10
(k) Connector, biconical, OD 7-11-7mm
(l) Cotton wool,500g,roll,non-ster
(m) Diathermy pencil/ball/blade
(n) Disposable, dispersive, electrode(Diathermy pad)
(o) Drain, corrugated sheet, 3 cm x 25 cm
(p) Drain, wound, CH 12, ster, disp, CH12, CH16, CH6
(q) Drawsheet,plastic,90x180cm
(r) Elastoplasts, 10 cm x 3 m (s) Electrode, Chest, Monitor (t) Gauze:
Ball, Large (sterile)
Ball, Large (un-sterile)
Ball, Peanut (sterile)
173
Swabs RAYTEX® 10 X 10 cm
Swabs, Un-sterile (Green)
Roll,90cmx100m,non-ster
Vaseline gauze (u) Gloves,exam,latex,disp,
large, medium & small (v) Gloves,surg,disp, 6.0, 6.5,
7.0, 7.5, 8, 8.5 (w) Gum elastic bougie, CH 15,
60 cm (x) Intubation stylet, adult, 15
Ch (y) Mask, Clinical, Disposable
(non-woven) (z) Mask, Protection, High
Filtration (aa)Needle, spinal,
0.9x90mm),ster,disp, 20G, 22G, 24G
(bb)Oxygen mask, adult (cc) Oxygen, nasal cannula (dd)Reusable, Diathermy, Cable (ee)Safety box for .used
syrgs/ndls (ff) Set, Infusion “Y”, Luer lock,
air inlet (gg)Scalpel
blade,ster,disp,no.10, no. 11, no. 15, no. 22, no. 23
(hh)Shoe cover, disposable (ii) Silicone Rubber Tubing (jj) Orthopedic surgeon's Cap,
Easy-Tie (kk) Suturing materials:
Abs,DEC1,need 1/2,18mm,round/BOX-36
Abs,DEC2,need 3/8 18mm,round/
Abs,DEC2,need 3/8,26mm,tri
Abs,DEC3,need 1/2 30mm,round
Abs,DEC3,need 3/8 50mm,round
Abs,DEC3,spool
Abs,DEC4,need 3/8 36mm,tri
Nonabs, DEC2,need 3/8 13mm,tri
Nonabs, DEC3,need 3/8 30mm,tri
Wires, different size/thickness
Plates and screws, different size and shape
Implants, different types and size
(ll) Tape,adhesive,Z.O,perforated,10cmx5m
(mm) Tape,adhesive,Z.O.,2.5cmx5m
(nn) Tubes:
Endo-tracheal, disp. + connector, 3 mm, w/o balloon
Endo-tracheal, disp. + connector, 3.5 mm, w/o balloon
Endo-tracheal, disp. + connector, 4 mm, w/o balloon
Endo-tracheal, disp. + connector, 4.5 mm, w/o balloon
Endo-tracheal, disp. +connector, 5 mm, balloon
Endo-tracheal, disp. + connector, 5.5 mm, balloon
Endo-tracheal, disp. + connector, 6 mm, balloon
Endo-tracheal, disp. + connector, 6.5 mm, balloon
Endo-tracheal, disp. + connector, 7 mm, balloon
Endo-tracheal, disp. + connector, 7.5 mm, balloon
174
Endo-tracheal, disp. + connector, 8 mm, balloon
suction,CH08,L50cm,ster,disp, CH08, CH10, CH14, CH16
N.G Tubes 12, 14, 16
7.5.4.13. Operating Room Linen:(a) Apron Orthopedic surgical, rubber (b) Trousers, Orthopedic surgical, woven,
Small, Medium & Large (c) Top(shirts), Orthopedic surgical,
woven, Small, Medium & Large (d) Gown, Orthopedic surgical,
woven(Plain) (e) Cap, Orthopedic surgical, woven (f) Masks, orthopedic surgical, woven (g) Drape:
Orthopedic surgical, woven(1 x 1 m)
Orthopedic surgical, woven(1 x 1.5 m)
Orthopedic surgical, woven(1.5 x 1.5 m)(fenestrated
Orthopedic surgical, woven(45 cm x 70 cm)(fenestrated)
Orthopedic surgical woven (2 x 1.5 m)(h) Pillow case (i) Pillows (j) Sheet, Bed (k) Sheet, draw, white (l) Cellular Blanket (m) Mayo cover (n) Towel Bath (o) Towel Hand
7.5.4.14. Equipment recovery area:(a) Vacuum aspirator (b) Oxygen Flow meter, 0 - 15
l/min (c) Oxygen (one cylinder per
bed) (d) Oxygen concentrater (e) Patient transfer, (stretchers) (f) Dressing trolley, trays (g) Bed with mattress (h) Stools
(i) IV stands (j) Bed screen, 3 sections, mobile (k) Pedal bin (l) Oxygen trolley, complete (m)Pulse oximeter (n) Resuscitator, hand operated (o) Suction machines (p) Mobile examination light (q) Dual head stethoscope
7.5.4.15. Equipment-Central sterilization room(a) Auto claves, big and small(b) Drums, metallic shelves, cabinets, tables and chairs
7.5.4.16. If the center has ICU, products shall be available as per the ICU standards stated under this document
175
7.6. Cardiac Center7.6.1. Practices
7.6.1.1. Outpatient services (a) Emergency services listed below shall be available 24 hours a day and 365
days a year.
Resuscitation of patients with sudden cardiac events like cardiac arrest and malignant ventricular arrhythmia.
Treatment, including defibrillation or cardioversion for patients with sudden life threatening rhythm disturbances
Resuscitation of patients with cardiogenic shock and severe hemodynamic instability
Resuscitation of newborns with life threatening congenital heart disease.
Resuscitation and management of sudden cardiac arrest in children with congenital or acquired cardiac lesions.
(b) Regular outpatient service listed below shall be available during working hours.
Acceptance and evaluation of patients with heart diseases
Follow-up care for patients on whom cardiac surgery or interventional catheterization has been performed
Follow-up of patients on whom medical or conservative management has been decided
(c) Stress testing(d) Echocardiography
7.6.1.2. The center shall be responsible for admission of patients on emergency basis for care and management of cardiac related conditions
7.6.1.3. The center shall have an Intensive Care Unit (ICU) with all requirements stipulated under ICU standards
7.6.1.4. The center shall provide anesthesia services as per the standards stipulated under the anesthesia services if the center provides cardiac surgery services.
7.6.1.5. The center may have Operating Theatre and Catheterization Laboratory.Centers having such cardiac facility shall provide the following services:
(a) Open heart surgery for patients with acquired or congenital cardiac diseases(b) Closed heart operations for different types of heart diseases in a child or an
adult (c) Insertion of chest tubes, drainage of pericardial effusions, insertion of
permanent pacemakers etc.(d) Diagnostic cardiac catheterization for purpose of cardiac anatomy and
function (e) Interventional cardiac catheterization for coronary angiography and
Percutaneous Coronary Intervention (PCI)
176
(f) Interventional cardiac catheterization for different types of congenital and acquired heart diseases
(g) Cardiac catheterization for the purpose of electrophysiological studies and transcatheter radiofrequency ablation.
7.6.2. Premises7.6.2.1. Out Patient: The outpatient service shall have the following space with
specified requirements(a) The regular outpatient area
Two rooms with adequate space, good lighting and ventilation windows:(at least 20 sq.m each)
It shall be provided with a working laminated top table, at least three chairs and a hand washing sink plus a hand maneuvered patient examination couch.
General waiting area/room: 30sq.m(b) The emergency resuscitation room
The emergency resuscitation room shall at least be 50 sq.m square meters wide with a good lighting and ventilation windows.
There shall be at least two resuscitation couches, cupboards and shelves, a wheelchair and patient transporter.
(c) Stress testing room:
The size of the room shall be at least 20 sq.m with good lighting and ventilation.
There shall be a Treadmill or a bicycle ergo meter, the stress test recording panel and at least a chair.
There shall be a resuscitation trolley and a defibrillator available for immediate use.
7.6.2.2. Ward: The clinical ward shall fulfill the followings: (a) At least ten beds with no more than two beds in one room. (b) Each room shall be at least 20 sq.m with a distance of not less than two
meters between the two beds. (c) There shall be staff toilet, shower and changing facilities(d) Nursing stations with telephone and telephone terminals, computer and
computer points, chairs and working laminated top tables.(e) Patient toilet and shower facilities. (f) Clean utility room used for storage of supplies both clean and sterile
consumables and linen, preparing and storing dressing trolleys, the storage, preparation and assembly of items or equipment for diagnostic and therapeutic procedures
7.6.2.3. The center shall have an Intensive Care Unit as per the requirements stipulated under ICU standards.
7.6.2.4. Operating Theatre (Optional): The operating zone shall be sterile and demarcations shall be clear beyond which one cannot cross without scrub shoes on. The operating area shall consist of the operating theatre, scrub
177
room, the heart lung machine supply room, the OR supply room, the staff locker rooms, and a soiled utility/sluice room with the following requirements:
(a) The theatre room:
The theatre room size shall be at least 63 sq. m and shall accommodate all the equipments mentioned under the section ‘OR equipments’.
There shall be enough space for the surgical team (surgeon, surgeon assistant, anesthetist, Transesophageal echocardiographer, perfusionist, theatre nurse and circulating nurse).
(b) The scrub room:
The scrub room shall be in close proximity with the theatre room and no more than one door crossed after scrubbing.
The room size shall at least be 8 sq.m.
The scrub room shall be able to accommodate at least two professionals scrubbing simultaneously.
(c) The OR supply room (12 sq. m):
The OR supply room shall be in proximity / continuity with the theatre room and is used for storage of consumable and small sized equipments for all theatre, anesthesia and perfusion purposes.
There shall be separate staff locker rooms for ladies and gentlemen used for staff changing facilities, placement of scrub suits and scrub shoes.
There shall be separate staff toilets and shower facilities for ladies and gentlemen in proximity with the locker rooms.
(d) Staff locker room (12 sq.m):
There shall be separate locker rooms for ladies and gentlemen located in proximity with the procedure room.
There shall be toilet, shower facilities and hand wash sinks either in or in proximity with the locker rooms.
(e) Soiled utility / sluice rooms:
The room shall be at least 12 sq. m in size shall have the facility for storage of contaminated materials until they are disposed off as well as cleaning of contaminated equipments.
There shall be adequate supply of clean gloves and heavy duty gloves for those working in the soiled utility area.
7.6.2.5. CAT Lab (Optional): Whenever the center has established such facility, it shall consist of the cath room itself, the control room, the scrub room and the cath lab supply room.
(a) Cath room / procedure room:
The procedure room shall be at least 36 sq. m and accommodate all the equipments mentioned under ‘cath lab equipments’.
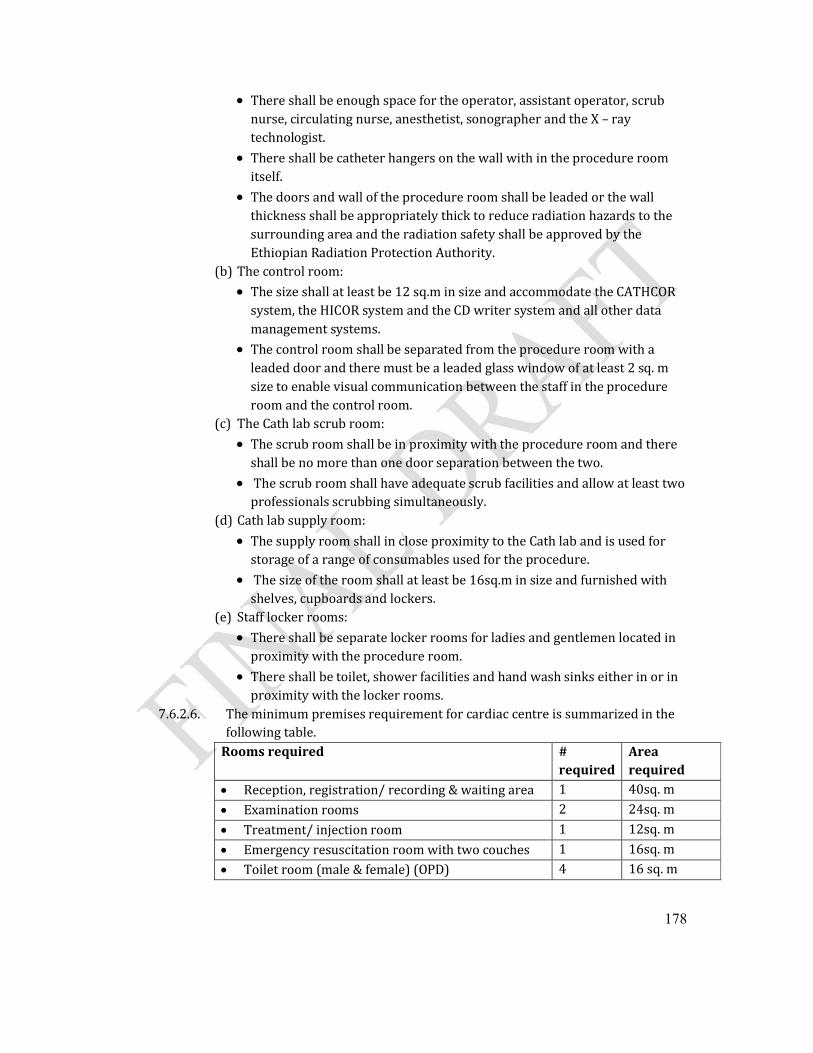
178
There shall be enough space for the operator, assistant operator, scrub nurse, circulating nurse, anesthetist, sonographer and the X – ray technologist.
There shall be catheter hangers on the wall with in the procedure room itself.
The doors and wall of the procedure room shall be leaded or the wall thickness shall be appropriately thick to reduce radiation hazards to the surrounding area and the radiation safety shall be approved by the Ethiopian Radiation Protection Authority.
(b) The control room:
The size shall at least be 12 sq.m in size and accommodate the CATHCOR system, the HICOR system and the CD writer system and all other data management systems.
The control room shall be separated from the procedure room with a leaded door and there must be a leaded glass window of at least 2 sq. msize to enable visual communication between the staff in the procedure room and the control room.
(c) The Cath lab scrub room:
The scrub room shall be in proximity with the procedure room and there shall be no more than one door separation between the two.
The scrub room shall have adequate scrub facilities and allow at least two professionals scrubbing simultaneously.
(d) Cath lab supply room:
The supply room shall in close proximity to the Cath lab and is used for storage of a range of consumables used for the procedure.
The size of the room shall at least be 16sq.m in size and furnished with shelves, cupboards and lockers.
(e) Staff locker rooms:
There shall be separate locker rooms for ladies and gentlemen located in proximity with the procedure room.
There shall be toilet, shower facilities and hand wash sinks either in or in proximity with the locker rooms.
7.6.2.6. The minimum premises requirement for cardiac centre is summarized in the following table.
Rooms required # required
Area required
Reception, registration/ recording & waiting area 1 40sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Emergency resuscitation room with two couches 1 16sq. m
Toilet room (male & female) (OPD) 4 16 sq. m
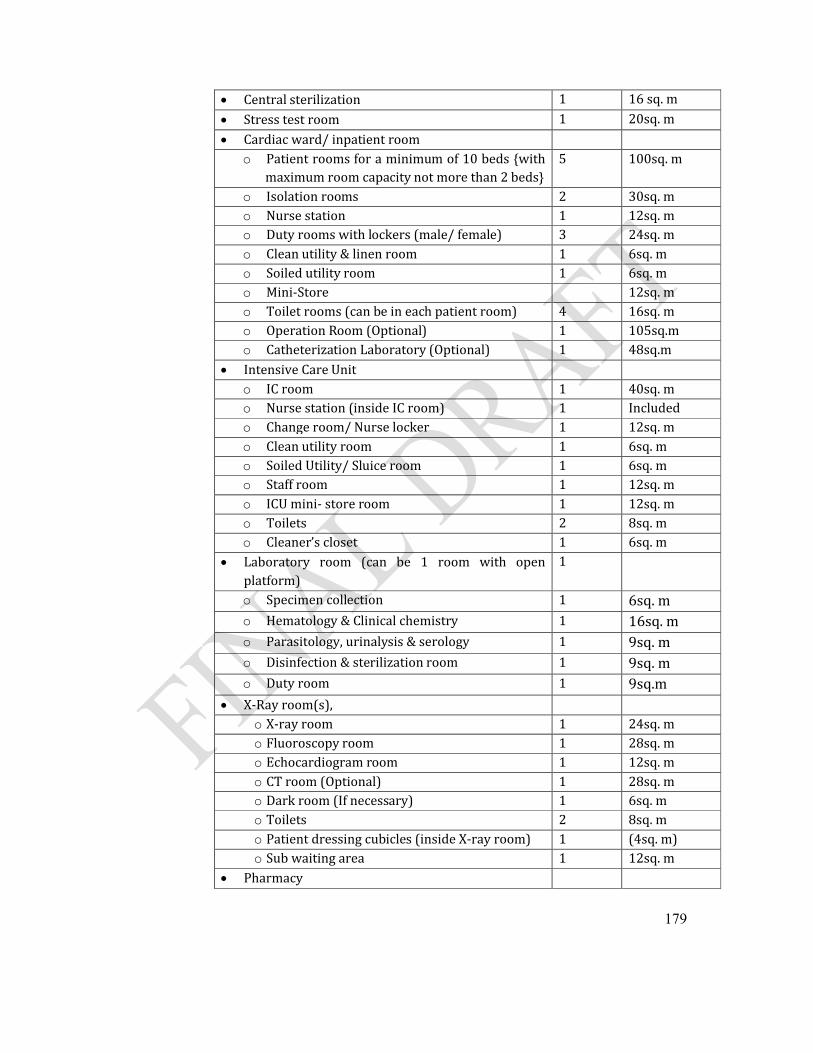
179
Central sterilization 1 16 sq. m
Stress test room 1 20sq. m
Cardiac ward/ inpatient roomo Patient rooms for a minimum of 10 beds {with
maximum room capacity not more than 2 beds} 5 100sq. m
o Isolation rooms 2 30sq. mo Nurse station 1 12sq. mo Duty rooms with lockers (male/ female) 3 24sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 12sq. mo Toilet rooms (can be in each patient room) 4 16sq. mo Operation Room (Optional) 1 105sq.mo Catheterization Laboratory (Optional) 1 48sq.m
Intensive Care Unito IC room 1 40sq. mo Nurse station (inside IC room) 1 Included o Change room/ Nurse locker 1 12sq. mo Clean utility room 1 6sq. mo Soiled Utility/ Sluice room 1 6sq. mo Staff room 1 12sq. mo ICU mini- store room 1 12sq. mo Toilets 2 8sq. mo Cleaner’s closet 1 6sq. m
Laboratory room (can be 1 room with open platform)
1
o Specimen collection 1 6sq. mo Hematology & Clinical chemistry 1 16sq. mo Parasitology, urinalysis & serology 1 9sq. mo Disinfection & sterilization room 1 9sq. mo Duty room 1 9sq.m
X-Ray room(s), o X-ray room 1 24sq. mo Fluoroscopy room 1 28sq. mo Echocardiogram room 1 12sq. mo CT room (Optional) 1 28sq. mo Dark room (If necessary) 1 6sq. mo Toilets 2 8sq. mo Patient dressing cubicles (inside X-ray room) 1 (4sq. m)o Sub waiting area 1 12sq. m
Pharmacy
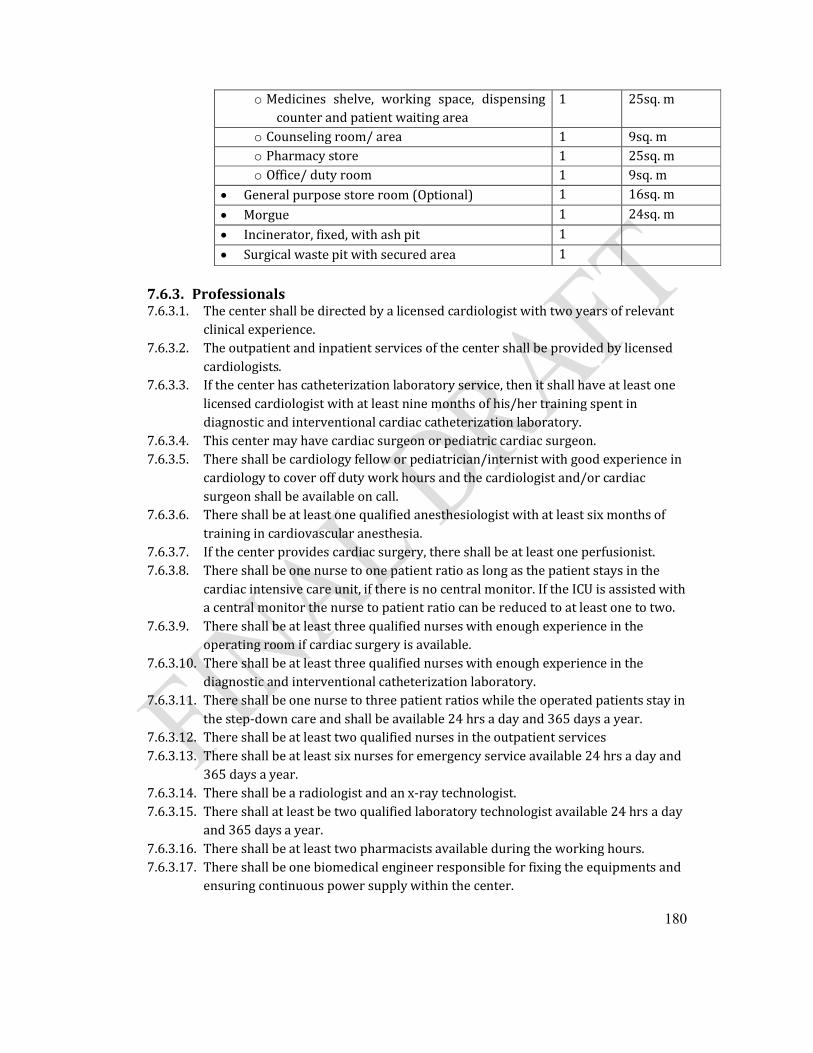
180
o Medicines shelve, working space, dispensing counter and patient waiting area
1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 9sq. m
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
Surgical waste pit with secured area 1
7.6.3. Professionals7.6.3.1. The center shall be directed by a licensed cardiologist with two years of relevant
clinical experience. 7.6.3.2. The outpatient and inpatient services of the center shall be provided by licensed
cardiologists.7.6.3.3. If the center has catheterization laboratory service, then it shall have at least one
licensed cardiologist with at least nine months of his/her training spent in diagnostic and interventional cardiac catheterization laboratory.
7.6.3.4. This center may have cardiac surgeon or pediatric cardiac surgeon.7.6.3.5. There shall be cardiology fellow or pediatrician/internist with good experience in
cardiology to cover off duty work hours and the cardiologist and/or cardiac surgeon shall be available on call.
7.6.3.6. There shall be at least one qualified anesthesiologist with at least six months of training in cardiovascular anesthesia.
7.6.3.7. If the center provides cardiac surgery, there shall be at least one perfusionist.7.6.3.8. There shall be one nurse to one patient ratio as long as the patient stays in the
cardiac intensive care unit, if there is no central monitor. If the ICU is assisted with a central monitor the nurse to patient ratio can be reduced to at least one to two.
7.6.3.9. There shall be at least three qualified nurses with enough experience in the operating room if cardiac surgery is available.
7.6.3.10. There shall be at least three qualified nurses with enough experience in the diagnostic and interventional catheterization laboratory.
7.6.3.11. There shall be one nurse to three patient ratios while the operated patients stay in the step-down care and shall be available 24 hrs a day and 365 days a year.
7.6.3.12. There shall be at least two qualified nurses in the outpatient services7.6.3.13. There shall be at least six nurses for emergency service available 24 hrs a day and
365 days a year.7.6.3.14. There shall be a radiologist and an x-ray technologist.7.6.3.15. There shall at least be two qualified laboratory technologist available 24 hrs a day
and 365 days a year.7.6.3.16. There shall be at least two pharmacists available during the working hours.7.6.3.17. There shall be one biomedical engineer responsible for fixing the equipments and
ensuring continuous power supply within the center.
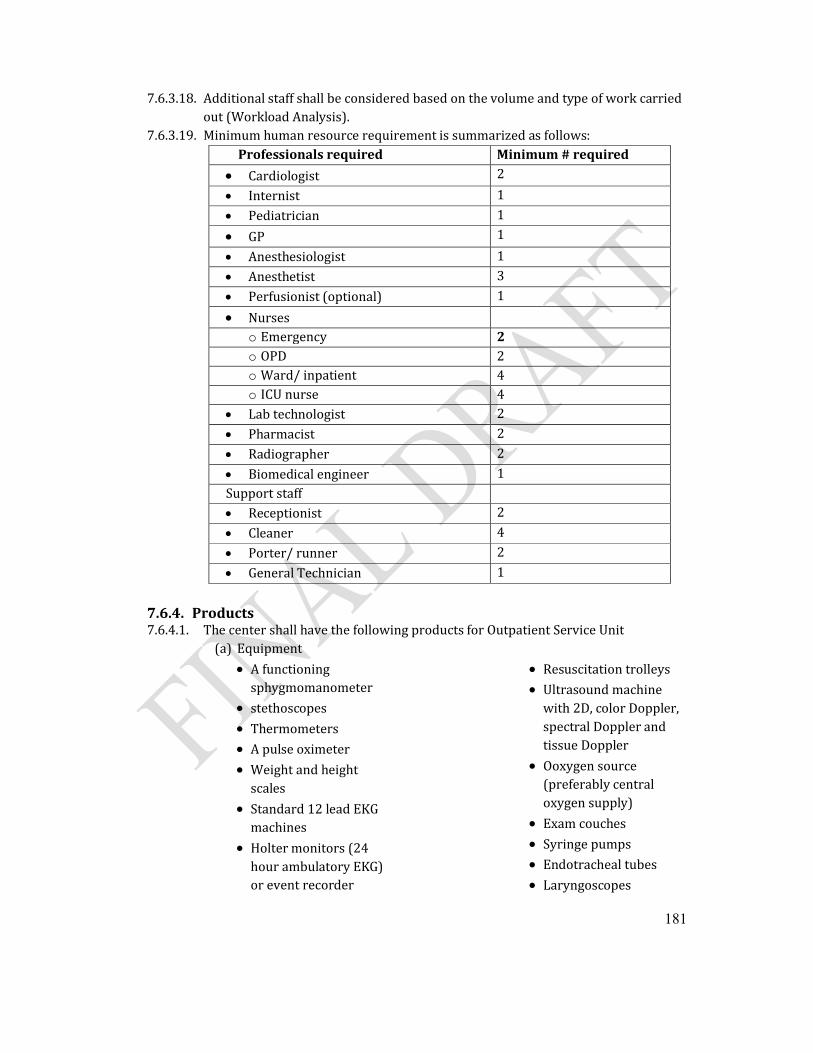
181
7.6.3.18. Additional staff shall be considered based on the volume and type of work carried out (Workload Analysis).
7.6.3.19. Minimum human resource requirement is summarized as follows:Professionals required Minimum # required
Cardiologist 2
Internist 1
Pediatrician 1
GP 1
Anesthesiologist 1
Anesthetist 3
Perfusionist (optional) 1
Nurseso Emergency 2o OPD 2o Ward/ inpatient 4o ICU nurse 4
Lab technologist 2
Pharmacist 2
Radiographer 2
Biomedical engineer 1Support staff Receptionist 2
Cleaner 4
Porter/ runner 2
General Technician 1
7.6.4. Products7.6.4.1. The center shall have the following products for Outpatient Service Unit
(a) Equipment
A functioning sphygmomanometer
stethoscopes
Thermometers
A pulse oximeter
Weight and height scales
Standard 12 lead EKG machines
Holter monitors (24 hour ambulatory EKG) or event recorder
Resuscitation trolleys
Ultrasound machine with 2D, color Doppler, spectral Doppler and tissue Doppler
Ooxygen source (preferably central oxygen supply)
Exam couches
Syringe pumps
Endotracheal tubes
Laryngoscopes
182
Defibrillators
Wheel chair
Patient transport stretcher
(b) Emergency medicines as per the national medicines list of Ethiopia specific to cardiac center
7.6.4.2. Clinical wards (a) Equipments
Patient beds fitted with non-invasive monitors and mounting rails behind all beds
Chairs (one per bed)
Drip stands
Medical gas ports
Telephone terminals
Working laminated top table
Nurse trolleys
Resuscitation trolleys
Reliable oxygen source
Syringe pump
Endotracheal tubes ofdifferent sizes
Laryngoscopes
Defibrillators
Dressing sets
Bed pans
Kidney dishes
Scissors
Surgical blade holders
Lockers and cupboards
shelves
Telemetry monitoring for post operative patients with transmitters for step down care and selected patients in the ward.
Nurse stations with chairs and computers plus computer points.
(b) Consumables
Disposable gloves
Sterile surgical gloves
Foley catheters of different sizes
Sterile gauze
Needles and syringes of different sizes
Venous cannulae of different sizes
Transfusion sets
Surgical blades
Patient cards/charts
7.6.4.3. Cardiac operating room (Optional)(a) Equipments
Scrub room with a scrub facility (at least 4x2m)
Surgical instrument cabinet
Endoscope cabinets
Sterile instruments cabinet
Electrically maneuvered operating tables
Anesthesia machine designed and dedicated for cardiovascular anesthesia
Laryngoscope
183
Backup cylinder ports for oxygen/air
Heart lung machine with all its accessories
Standard OR lights (at least 3)
Surgeons head light
Headlight source
Cardiac monitors with screens (fitted with all invasive monitors)
Surgeon’s goggles
Surgeon’s sitting and standing stools
Scrub shoes
Tubing clump and Tubing scissors
Drip stands (minimum 3)
Drums (at least 5)
kidney dishes (at least 12)
Vacuum/electrical suctions (at least 3 terminals)
Medical gas supply (ports for oxygen, atmospheric air and nitrous oxide)
Diathermy (at least 2)
Theatre trolleys (at least 2)
Anesthetic trolley (at least 2)
Perfusionist’s trolley
Bowl trolley
Sterilized device and cloth trolley
Medication trolley
Medical waste trolley
Laundry collection trolley
Mayo stand
Sharp container’s (at least 4)
Wall white board (at least 2 each at least 80x50cm)
Digitally operated air conditioner
Autoclaves (Tabletop steam sterilizer at least 1)
Wall sockets (minimum 12)
Open heart surgical set (at least 2)
Closed heart surgical set (at least 2)
Electric / pneumatic saw
Defibrillator with internal paddles
Echo machine with pediatric and adult Transesophageal facilities
Heater/cooler
Patient warmer with electric blanket
Heating cabinet to warm patient fluid
Balloon pump
Pressure transducers (at least 3)
Syringe pumps (at least 2)
Pressure bags (at least 5)
Stainless steel bowls (at least 2)
Racks (at least 2)
Blood gas analyzer
Transport monitor
Transport oxygen cylinder (at least 1)
Activated Clotting time Testing machine (ACT machine)
Temporary pacing boxes
Refrigerators (at least 2 each 180 liters each)
Sharp/blunt sterile scissors
Oxygen saturation probes (newborn, infant pediatric)
Patient transport stretcher (at least 1)
(b) Consumables
Scrub brushes with soap and iodine
Antiseptics
Angled perfusion cannullae of different sizes
IV cannullae of different sizes
Pressure domes
Oxygenator and venous reservoir
Cardioplegia set
Cardiovascular set
Hear exchanger
Disposable connectors
Arterial for perfusion (range of sizes)
Left heart vent catheters
Blood transfusion filters for perfusion
Arterial Cannullae of different sizes
Coated, braided polyester sutures (1/0, 2/0, 3/0, 4/0, 5/0, 6/0)
ECG electrodes
Diathermy pencils
Gore-Tex stretch graft suture
Gore-Tex large diameter stretch graft
Gore-Tex stretch graft
Quadrilumen CVC sets
Triplelumen CVC sets
ACT cartridges
Pediatric multi-lumen Central Venous Catheterization sets of different sizes
Swan-Ganz pulmonaryartery wedge catheters of different sizes
Uncuffed Endotracheal tubes of different sizes
Cuffed Endotracheal tubes of different sizes
I-STAT cartridges
Temporary pacing wires
Blood burettes
Clear fluid burettes
Chest tube set
Urine bags with urinary catheters and urine meter
Intraosseous infusion needle
Nasal cannula
Oxygen face mask (infant, pediatric, adult)
Nebulisers
Micropore tape
IV site dressing
Blood transfusion set
Hypodermic needles (orange, blue, white, green)
Connecting 3-way stopcocks
Bladder syringes
Luer-lock syringes
Luer-Slip syringes
Sterile suction tubing
Non-sterile examination gloves
Sterile surgical gloves of different sizes
Tender tip suction catheter of different sizes
Wound care packs
185
Sterile oral hygiene packs
Non-woven swabs
X-ray detectable gauze swabs
Pre-injection swabs
Nasogastric tubes of different sizes
Silk stitches
Sterile drapes
Scrub suits
Ambubag
Snapper plate
Haemofilters
Balloon tipped silicon coronary artery ostial cannula of different sizes
Foley catheter of different sizes
Steel wires
Surgical gowns of different sizes
Chest drainage bottles
Powder free latex sterile gloves of different sizes
Surgical blades of different sizes
Thoracic catheter of different sizes
7.6.4.4. Cardiac Intensive Care Unit shall have the following products(a) Equipment
Electrically maneuvered pediatric and adult beds fitted with monitors and screens
Invasive pressure transducers (1 per bed)
Ventilators with accompanying accessories
Feeding tables (per bed)
Ports for oxygen, atmospheric air and vacuum (1 of each per bed)
Electrical suction machine (at least 1 as a backup)
Drip stands (2 per bed)
Infusion pumps (1per bed)
Syringe pump (3 per bed)
Incubators and radiant warmers
Refrigerator (at least 1)
Nasal CPAP
Bed pan (1 per bed)
Pacing boxes (at least 2)
Device trolleys (1 per bed)
Pharmacy trolley (at least 1)
Resuscitation trolley (at least 1) Refrigerator
Defibrillator (at least 1)
Electrical sockets on the nurse station desk (at least 12-16)
2 meter long mounting rails behind all beds
10 main sockets behind each bed
Portable x-ray machine with protective lead apron and lead curtain
X-ray viewer
Echocardiography machine with 2D, color, spectral Doppler and tissue Doppler.
Nurse stations equipped with chairs, tables,
186
drawers and computers, shelves, lockers
Linen boards
Screen and curtain (for privacy)
Water supply and sink facility with soap
Paper towel dispenser
Telephone and telephone point
Arterial pressure bags
Blood gas analyzer
A 12 – lead standard ECG machine
Medication boards
Controlled drug locker
Calculators
Weight scale
Wall clock (at least 2)
Soiled cloth hampers
Manual sphygmomanometers with infant, pediatric and adult cuffs.
Thermometers
Stethoscope
Intubation set
(b) Consumables
Non-sterile examination gloves
Sterile surgical gloves
Chest drainage bottles
Foley catheters with urine bags
Adhesive plasters
Cannullae of different sizes
Needles
A range of crystalloid and colloid IV fluids
Patient charts/cards (case summary, order sheet, nurses monitoring sheet etc.) and other stationeries.
7.6.4.5. Diagnostic and interventional cardiac catheterization laboratory (Optional)(a) Equipments
At least a single C-arm angiography machine with a movable angiography table
Angiography and RGB monitoring screens
A well functioning CATHCOR system
CD recorder
Digitally operated air conditioner
At least a stand alone pressure injector system
A pressure amplifier box
Pressure transducer cables
ECG monitor system
Syringe pump (at least 2)
Infusion pump (at least 1)
An anesthesia machine
Laryngoscope
Gas ports for oxygen, medical air and nitrous oxide
187
Echocardiogram with pediatric and adult Transesophageal facilities
An Ambubag
A control room with chairs
Scrub room with scrub facilities
Drip stands (at least 2)
Light source
Lead aprons and thyroid shield for every member of staff working in the cath lab
A telephone and telephone point
Catheter and wire rinsing basins
Drums at least 4
Galipot at least 8
At least 4 kidney dishes
Scissors
Artery forceps
Surgical blade holders
Sponge forceps
Blood gas analyzer
Nurse trolleys (at least 1)
Device trolley (at least 1)
Resuscitation trolley
Defibrillators
Computer and computer network terminal
Patient transport couches
Pulse oximeter
Vital sign tray
Waste baskets for soiled and dry linen
Sharp disposal containers
Catheter hangers
Apron hangers
(b) Consumables
Local anesthetics (Lidocaine, Bupivacaine, Xylocaine, etc)
Contrast injector syringes
3, 5 and 10ml syringes
Puncture needles
Surgical blades
Disinfectants
Sterile gauze
Small guide wires (J-guide wires)
Valved introducers with dilators (with a range of sizes)
Multipurpose catheters (a range of sizes)
NIH catheters (with a range of sizes)
Pigtail catheters (a range of sizes)
Balloon tipped flow guided catheters (a range of sizes)
Left and right coronary catheters (a range of sizes)
Soft tipped guide wires (a range of sizes)
Exchange range guide wires (a range of sizes)
Super stiff guide wires (a range of sizes)
Contrast agents (Omnipac, Iopamiron)
Balloon angiocatheters of different types ( with a range of sizes)
188
Coronary stents with associated delivery systems (a range of sizes)
Vascular stents with associated delivery systems (a range of sizes)
Duct occluders with associated delivery systems (a range of sizes)
Septal occluders with associated delivery systems (a range of sizes)
Face mask
IV cannullae (a range of sizes)
Butterfly needles
Patient drapes
Scrub suits (single use or fabric)
Pressure domes and connectors
Injector connecting tubes
Endotracheal tubes of different sizes
Cidex solution for probe cleaning
Probe covers
Lubricant and transmission gel & suction tubes
Adult and pediatric ECG electrodes
Non sterile examination gloves
Sterile surgical gloves of different sizes and
189
7.7. Oncology center7.7.1. Practices7.7.1.1. The oncology outpatient services shall include:
(a) New patient services, (b) Follow-up services,(c) Radiotherapy planning services, (d) Radiotherapy treatment sessions,(e) Weekly Radiotherapy treatment checks,(f) Chemotherapy sessions,(g) Oncologic emergency services including emergency procedures, (h) Health education on cancer related topics(i) Pain clinics if possible, (j) Radiological and pathology services
7.7.1.2. The oncology inpatient services shall include:(a) Delivering chemotherapy sessions,(b) Nursing care according to individual patients’ needs (c) Brach therapy (Low dose rate or high dose rate, preferably high dose rate sources)
7.7.1.3. There shall be a multidisciplinary cancer committee, chaired by a physician for a defined period that is responsible for at least the development of oncology policies and procedures, tumor review, and tumor registry.
7.7.1.4. The multidisciplinary team shall consist of clinical oncologist designated leader, surgeon who deals with the respective tumor type, pathologist, radiologist, nuclear medicine physician depending on the type of malignancy, oncology nurse and there shall be meetingson a regular basis.
7.7.1.5. The center may have an Intensive Care Unit (ICU) with all requirements stipulated under ICU standards
7.7.1.6. If the center provides surgical services, it shall comply with the standards stipulated under surgical and anesthesia services.
7.7.1.7. The Center shall have written policies and procedures that are reviewed at least once every five years, revised more frequently as needed, and implemented. They shall include at least:
a) Criteria for admission b) Guidelines for mixing chemotherapy, when performed on the unit, c) Guidelines for administering chemotherapy d) Training of nursing and housekeeping staff in the disposal of chemotherapeutic
agents; e) Use, handling, storage, and disposal of specific chemicals, agents, and body wastes; f) Assuring informed consents to chemotherapy; and g) Psychological/social and spiritual aspects of patient care.
7.7.1.8. There shall be a formal mechanism for communication between the oncology service and each of the following clinical areas: nursing, dietary, social work, nuclear medicine,laboratory, pathology and pharmacy.
190
7.7.1.9. All patients with cancer shall be managed by a multidisciplinary process. It includes diagnosis and all aspects of treatment and care, including symptom management and end-of-life care. It considers each individual patient’s need and preference for care and treatment. The multidisciplinary process shall include the followings:
a) There shall be a multidisciplinary management protocols covering systems for referral (including to medical, surgical, oncology and palliative care services), investigation, diagnostics, staging for treatment, treatment, follow-up and end-of-life care for patients with cancer.
b) All patients shall have access to palliative and supportive care appropriate to their needs
c) There shall be written local protocols for discharge planning, which includes details for pre-discharge, actual discharge and post-discharge arrangements.
d) All patients with cancer shall have individualized care plans, developed jointly and agreed between the patient and members of the multidisciplinary care team, documenting clinical and non-clinical issues and the proposed action to address such issues.
e) A comprehensive, single care plan shall be available to the patient and members of the multidisciplinary care team including health professionals
7.7.1.10. Care, support and services for cancer shall be provided in partnership with patients and care givers. There shall be a clear record of what the patient or care givers has been told about the condition, treatment and care options, outcomes, risks and side-effects.
7.7.1.11. Patients with cancer shall be enabled and supported to make decisions throughout their care experience. All patients with cancer shall have access to a healthcare worker with experience and knowledge of their current care needs and the skills to facilitate informed decision-making.
7.7.1.12. Patient and family teaching shall be provided in any case where the patient and family are in need of and able to receive instruction.
7.7.1.13. Criteria shall be developed in consultation with the social work department for identifying patients in need of social work services and/or discharge planning and making referrals as needed.
7.7.1.14. There shall be a system to refer patients and family and direct staff to in-house and community support groups and services.
7.7.1.15. There shall be a program of continuous quality improvement for oncology that is integrated into the center continuous quality improvement program and includes regularly collecting and analyzing data to help identify health-service problems and their extent, and recommending, implementing, and monitoring corrective actions on the basis of these data.
7.7.1.16. There shall be a pain clinic and patients shall be managed according to the national pain management guidelines.
7.7.1.17. Pain shall be considered as a 5th vital sign. The Oncology nurse shall utilize appropriate pain assessment tools and will encourage the patient “self-report” of pain.
7.7.1.18. Principles of pain management including non-pharmacological methods of pain management may be taught.
7.7.1.19. The oncology nurse shall document pain assessment and interventions.
191
7.7.1.20. The patient will be protected from infection and cross contamination according to infection prevention standards mentioned in this document. Nursing personnel shall institute specific precautions to prevent infection in patients with an absolute neutrophil count (ANC) of less than 1,000
7.7.1.21. Medications shall be administered per written policies and procedures.a) Chemotherapy shall be administered as per written procedures.b) The pharmacist and nursing staff shall wear protective gloves and approved
chemotherapy gowns when compounding/preparing and administering chemotherapy to patients
c) Licensed nurses shall take necessary steps to prevent and treat extravasations of chemotherapeutic agents so that the patient will have minimum complications
d) Treatments, medications, and IV’s ordered by the physician shall be instituted 7.7.1.22. Patients shall be admitted to patient care areas according to their physical and psychosocial
needs, unit admission criteria, and bed availability.7.7.1.23. The patient shall be oriented to the room, service unit and to their assigned nurse upon
arrival.7.7.1.24. Identified patient needs and subsequent nursing interventions shall be evaluated and
documented in the Integrated Notes.a) The nursing staff shall provide assessment and care during every shift to the patient
with mucositis, an inflammatory response to chemotherapeutic agents. Patient education will be provided.
b) The nursing staff shall initiate and teach appropriate precautions for the patient with myelosuppression
c) The nursing staff shall provide assessment, care, and evaluation of interventions to the patient receiving chemotherapy with high emetogenic potential.
7.7.1.25. Patient teaching shall begin during the admission process and shall be ongoing. Documentation shall include the teaching plan and patient response.
7.7.1.26. Nursing personnel shall provide information to patients regarding administered chemotherapeutic agents
7.7.1.27. Nursing staff shall seek input from the patient and other health care professionals to plan and implement care. Oncology nursing staff shall utilize the nursing process to provide for the physical, emotional, and spiritual needs of oncology patients and make referrals as appropriate.
7.7.1.28. The nurse shall utilize available resources to facilitate an optimal transition between health care settings. The patient or family who is complex, unable to cope, or being discharged which requires coordination by the multidisciplinary team will be followed by Integrated Case Management.
7.7.1.29. Patient’s comfort level shall be assessed and comfort measures/pain management will be provided to meet patient needs.
7.7.1.30. The Oncology patients shall be provided with a bath or shower for personal hygiene daily or as per need. Daily morning care shall include offering mouth care, a wet washcloth, and repositioning the patient for breakfast.
7.7.1.31. Consent for procedure and patient understanding shall be verified prior to implementation.
192
7.7.1.32. Additional information regarding advance directives shall be provided as requested by patient.
7.7.1.33. Patient’s spiritual and cultural beliefs shall be considered when planning and implementing care. The nursing staff shall utilize the nursing process to assess the patient and family’s ability to cope with his/her diagnosis and treatment of disease. Interventions shall be congruent with the patient/family belief system.
7.7.1.34. Available resources shall be utilized to maximize patient’s support and care giver as needs are identified. Patients who are assessed by oncology staff as unable to cope shall be referred to the social worker or appropriate support group.
7.7.1.35. Chemotherapya) All chemotherapy regimens shall be given according to the treatment guidelines
Staff dealing with cytotoxic medicines shall follow the safety guidelines;
Vertical Laminar Air Flow Hood shall be used during the preparation of all chemotherapy on the unit.
Goggles, masks, gloves shall be worn when dealing with chemotherapy.
Office of Occupational Medicine shall be used to develop procedures for preparing chemotherapy. Example using Fume hood for chemotherapy mixing
b) Inpatient chemotherapy shall only be given in wards where it is agreed as the whole of, the wards allowed activities.
c) Out-patient chemotherapy shall only be given in outpatient areas where it is agreed as part of, or the whole of, that areas allowed activity.
d) While out-patient chemotherapy is being given the area shall only be used for this purpose and other aseptic treatments and procedures on cancer patients.
e) Oncology nurse administers parentheral chemotherapy as prescribed by the oncologist in the presence of oncologist or other trained physician
7.7.1.36. Radiotherapy (Optional service)a) The safety standards of radiotherapy shall be according to the Ethiopian National
Radiation Protection Authority (ENRPA) /IAEA standardsb) The radiotherapy technician can deliver Radiation in the presence of a radiation
oncologistc) Both acceptance and commissioning test should be done by experienced medical
physicist for Barchytherapy and teletherapy machine before being used for patients’ treatment.
7.7.1.37. There shall be one oncologist available during working hours and on call basis at all times for consultation.
7.7.1.38. As the patient’s condition or nursing interventions warrant, the bed will be kept in the low position with the wheels locked and upper side rails in the up position and call light within reach of patient. Oncology nursing staff will implement thrombocytopenic precautions for patients with platelets less than or equal to 20,000
7.7.1.39. An allergy label shall be placed on the front of each patient’s chart with “Allergies” or “No Known Allergies” listed as appropriate. Allergies” or “No Known Allergies” will be entered into the patient’s medical record (Care vision) during the admission process and updated as appropriate
193
7.7.1.40. Vital signs shall be completed, unit routine, physician order, or as patient condition warrants.
a) Patients receiving blood or blood products shall have vital signs monitored b) Patients with neutropenia shall have vital signs taken
7.7.1.41. Psychological and psychiatric services shall be available in the premises 7.7.1.42. Chaplin or related religious counseling may be facilitated upon patient request
7.7.2. Premises7.7.2.1. Buildings and rooming styles shall generally be in accordance with the Ethiopian national
radiation Protection authority/ International Atomic Energy Associations ENRPA/IAEA standards
7.7.2.2. One of the examination room shall be fitted with Gynecology examination and procedure couch,
7.7.2.3. In addition to emergency and isolation, the specialty center shall have at least ten inpatient beds.
7.7.2.4. Minimum requirements for inpatient section:(a) Isolation rooms or single bedrooms shall be available to accommodate patients with
neutropenia, or critically ill patient or septic patients that needs wound care(b) All patients will be provided with an environment conducive to rest/recovery.
7.7.2.5. The minimum premises requirements for oncology centre are summarized as follows.Rooms required # required Area required Reception, registration/ recording & waiting area 1 40sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Emergency room with 2 resuscitation couches 1 16sq. m
Toilet room (male & female) (OPD) 4 16 sq. m
Central sterilization 1 16 sq. m
Oncology ward/ inpatient roomo Patient rooms for a minimum of 10 beds {with
maximum room capacity not more than 6 beds} 2 96sq. m
o Isolation rooms 2 30sq. mo Isolation room, septic 1 12sq.mo Nurse station 1 12sq. mo Duty rooms with lockers (male/ female) 2 16sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 12sq. mo Toilet rooms (can be in each patient room) 4 16sq. m
Intensive Care Unit (Optional)o IC room 1 40sq. mo Nurse station (inside IC room) 1 Included o Change room/ Nurse locker 1 12sq. m
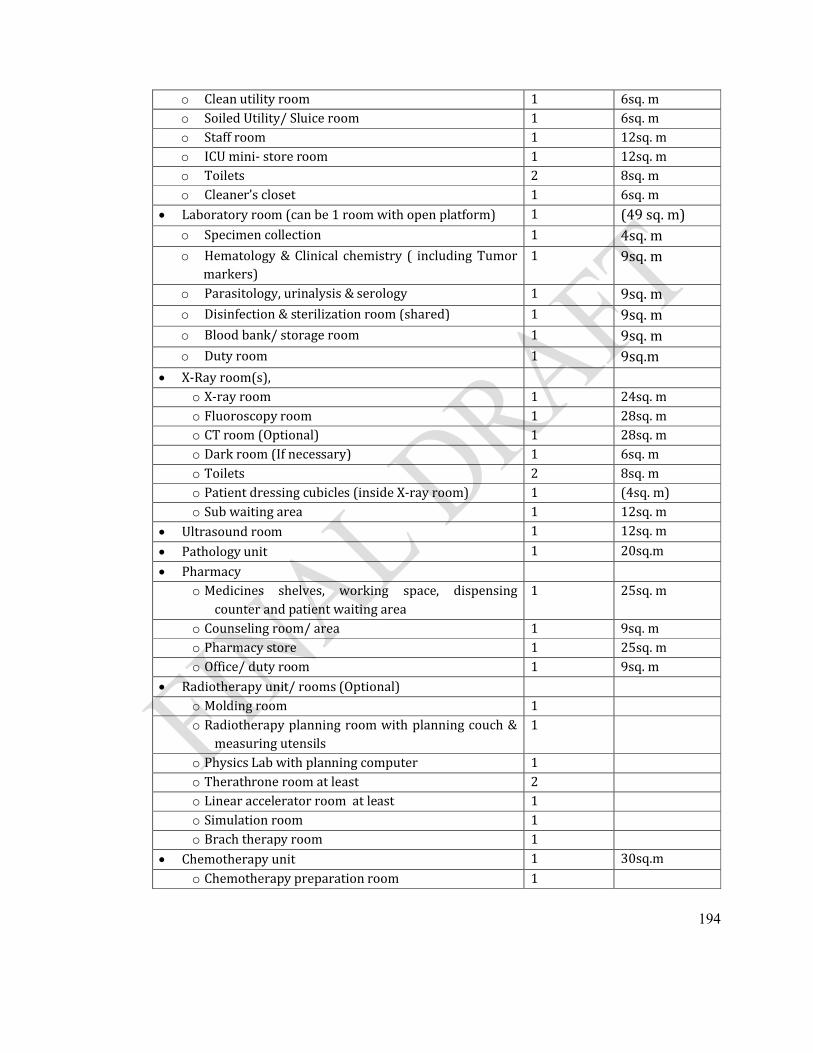
194
o Clean utility room 1 6sq. mo Soiled Utility/ Sluice room 1 6sq. mo Staff room 1 12sq. mo ICU mini- store room 1 12sq. mo Toilets 2 8sq. mo Cleaner’s closet 1 6sq. m
Laboratory room (can be 1 room with open platform) 1 (49 sq. m)o Specimen collection 1 4sq. mo Hematology & Clinical chemistry ( including Tumor
markers)1 9sq. m
o Parasitology, urinalysis & serology 1 9sq. mo Disinfection & sterilization room (shared) 1 9sq. mo Blood bank/ storage room 1 9sq. mo Duty room 1 9sq.m
X-Ray room(s), o X-ray room 1 24sq. mo Fluoroscopy room 1 28sq. mo CT room (Optional) 1 28sq. mo Dark room (If necessary) 1 6sq. mo Toilets 2 8sq. mo Patient dressing cubicles (inside X-ray room) 1 (4sq. m)o Sub waiting area 1 12sq. m
Ultrasound room 1 12sq. m
Pathology unit 1 20sq.m
Pharmacyo Medicines shelves, working space, dispensing
counter and patient waiting area1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 9sq. m
Radiotherapy unit/ rooms (Optional) o Molding room 1o Radiotherapy planning room with planning couch &
measuring utensils1
o Physics Lab with planning computer 1o Therathrone room at least 2o Linear accelerator room at least 1o Simulation room 1o Brach therapy room 1
Chemotherapy unit 1 30sq.mo Chemotherapy preparation room 1
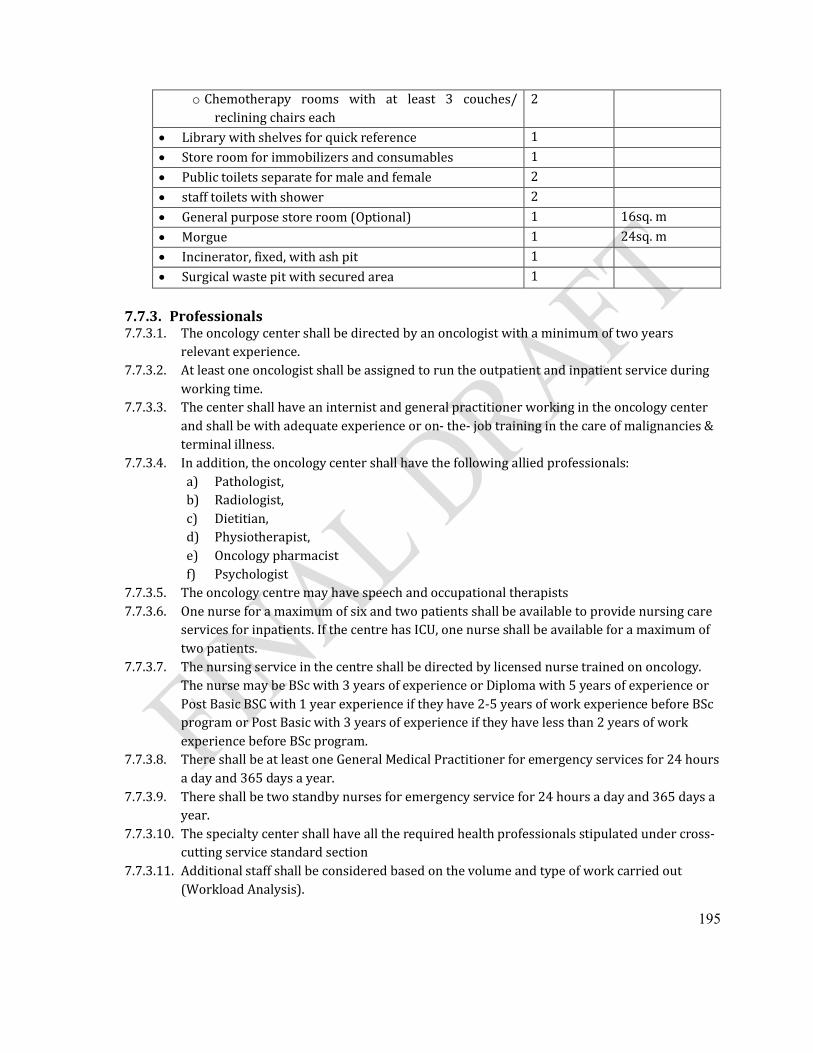
195
o Chemotherapy rooms with at least 3 couches/ reclining chairs each
2
Library with shelves for quick reference 1
Store room for immobilizers and consumables 1
Public toilets separate for male and female 2
staff toilets with shower 2
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
Surgical waste pit with secured area 1
7.7.3. Professionals7.7.3.1. The oncology center shall be directed by an oncologist with a minimum of two years
relevant experience.7.7.3.2. At least one oncologist shall be assigned to run the outpatient and inpatient service during
working time. 7.7.3.3. The center shall have an internist and general practitioner working in the oncology center
and shall be with adequate experience or on- the- job training in the care of malignancies & terminal illness.
7.7.3.4. In addition, the oncology center shall have the following allied professionals:a) Pathologist,b) Radiologist,c) Dietitian, d) Physiotherapist,e) Oncology pharmacistf) Psychologist
7.7.3.5. The oncology centre may have speech and occupational therapists7.7.3.6. One nurse for a maximum of six and two patients shall be available to provide nursing care
services for inpatients. If the centre has ICU, one nurse shall be available for a maximum of two patients.
7.7.3.7. The nursing service in the centre shall be directed by licensed nurse trained on oncology. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
7.7.3.8. There shall be at least one General Medical Practitioner for emergency services for 24 hours a day and 365 days a year.
7.7.3.9. There shall be two standby nurses for emergency service for 24 hours a day and 365 days a year.
7.7.3.10. The specialty center shall have all the required health professionals stipulated under cross-cutting service standard section
7.7.3.11. Additional staff shall be considered based on the volume and type of work carried out (Workload Analysis).
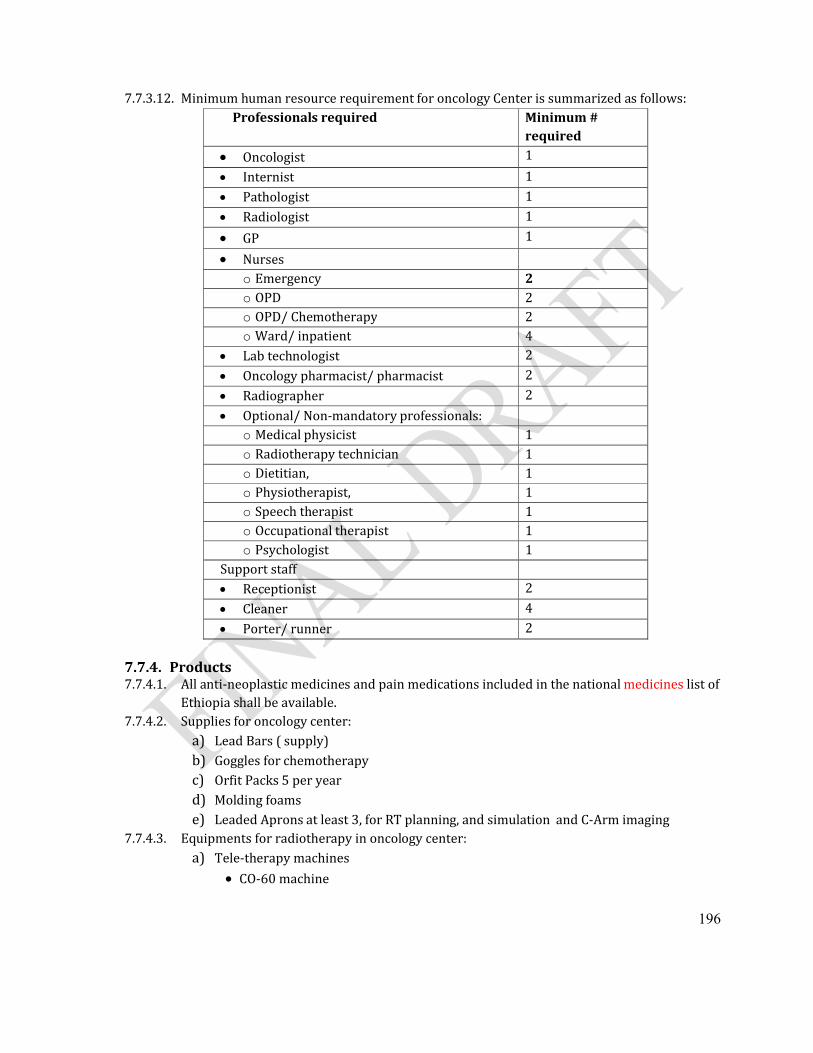
196
7.7.3.12. Minimum human resource requirement for oncology Center is summarized as follows:Professionals required Minimum #
required
Oncologist 1
Internist 1
Pathologist 1
Radiologist 1
GP 1
Nurseso Emergency 2o OPD 2o OPD/ Chemotherapy 2o Ward/ inpatient 4
Lab technologist 2
Oncology pharmacist/ pharmacist 2
Radiographer 2
Optional/ Non-mandatory professionals:o Medical physicist 1o Radiotherapy technician 1o Dietitian, 1o Physiotherapist, 1o Speech therapist 1o Occupational therapist 1o Psychologist 1
Support staff Receptionist 2
Cleaner 4
Porter/ runner 2
7.7.4. Products 7.7.4.1. All anti-neoplastic medicines and pain medications included in the national medicines list of
Ethiopia shall be available.7.7.4.2. Supplies for oncology center:
a) Lead Bars ( supply) b) Goggles for chemotherapy c) Orfit Packs 5 per yeard) Molding foamse) Leaded Aprons at least 3, for RT planning, and simulation and C-Arm imaging
7.7.4.3. Equipments for radiotherapy in oncology center:a) Tele-therapy machines
CO-60 machine
197
Linear Accelerator b) Orthovoltage X-Ray 100KvP c) Brach therapy machine accessories:
High dose rate source of CO-60 or low dose rate Cesium source
Fume hood for chemotherapy mixing d) One brachy therapy machinee) Simulation equipment : one CT simulator and C-Arm x-ray unitf) Mold room equipments:
Molding Machine( cutter)
Alloy melting pot
Lead Melting machine
Steriofoam cutter
Boiler for orfit preparation
Couchg) Dosimeter equipment:
Farmer dosimeter
Electrometer
Personal dosimeter
Survey meter
Appropriate Ion chambers to radiotherapy machines used
Water phantom
Barometer
Digital thermometerh) Treatment planning system
Computers with printer
Treatment planning software
Digitizeri) Immobilizers
Breast Board Minimum,
thermoplastic head casts, head and neck uniframe immobilizer set,
Plastic head rests ( with size A, B, C, D, E, F)
Head and Neck uniframe immobilizers
Pelvi-meter
Flexi curve ruler
Orfit packs as requiredj) Chemotherapy equipment: One fume hood and two perfuser for chemotherapy
7.8. Neurology Center7.8.1. Practice7.8.1.1. The Neurology center shall have the following services:
198
(a) outpatient service,(b) follow-up clinic, (c) neurologic consultations,(d) Neurosurgery with ICU services(e) referral services to respective facilities,(f) Emergency neurological and/ or care for stroke,(g) Inpatient neurologic care for different diseases,(h) headache and pain management,
7.8.1.2. There shall be written protocols and procedures for management of common neurological conditions in the center as well as consultation and transfer of admitted patients to other services.
7.8.1.3. The center shall have an Intensive Care Unit (ICU) with all requirements stipulated underICU standards
7.8.1.4. The center shall provide anesthesia services as per the standards stipulated for anesthesia services.
7.8.1.5. The center shall avail neurological service for emergency neurological conditions for 24 hours a day throughout the year,
7.8.1.6. For non-emergency condition the neurological service shall be available during the regular working hours.
7.8.1.7. The neurological service shall be organized to cover all the shifts for admitted patients (24 hours of the day and seven days of the week),
7.8.1.8. Nursing functions for each shift shall be carried out by the nurse responsible for the shift, 7.8.1.9. The service shall have written policies and procedures that shall include:
(a) Admission and discharge criteria specific to the service; (b) A visitors policy that allows for 24 hour visitation by designated visitors and specifies
the number of visitors permitted for each patient at any one time(c) Infection control as per National and or center IP guideline(d) Transfer and Referral of patients (e) Monitoring and follow-up of patients
7.8.1.10. The administrative functions shall be a responsibility of the center’s administration,7.8.1.11. Every neurological records shall be kept for each patient 7.8.1.12. Information contained in the neurological record shall be complete and sufficiently detailed
relative to the patient's history, physical examination, diagnosis, diagnostic procedures, medication administration, and treatment.
7.8.1.13. The center shall use standard Prescription & different request forms for investigation like laboratory, x-ray, etc.
7.8.1.14. The center shall have a system for involving patients, family members &/ or caretakers in the process of care & treatment.
7.8.1.15. There shall be chronic care follow up service for certain prevalent neurological conditions in the center.
7.8.2. Premises7.8.2.1. In addition to emergency and isolation beds, the specialty center shall have at least ten
inpatient beds.
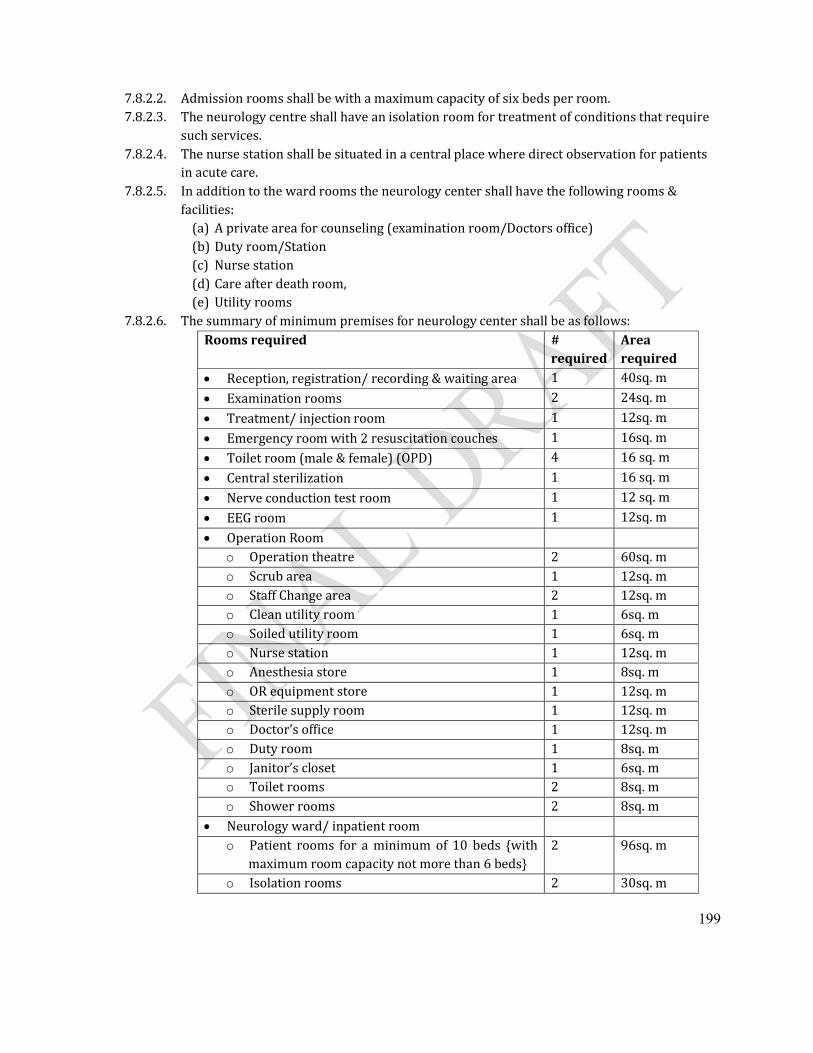
199
7.8.2.2. Admission rooms shall be with a maximum capacity of six beds per room.7.8.2.3. The neurology centre shall have an isolation room for treatment of conditions that require
such services. 7.8.2.4. The nurse station shall be situated in a central place where direct observation for patients
in acute care.7.8.2.5. In addition to the ward rooms the neurology center shall have the following rooms &
facilities:(a) A private area for counseling (examination room/Doctors office)(b) Duty room/Station(c) Nurse station(d) Care after death room,(e) Utility rooms
7.8.2.6. The summary of minimum premises for neurology center shall be as follows:Rooms required #
requiredArea required
Reception, registration/ recording & waiting area 1 40sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Emergency room with 2 resuscitation couches 1 16sq. m
Toilet room (male & female) (OPD) 4 16 sq. m
Central sterilization 1 16 sq. m
Nerve conduction test room 1 12 sq. m
EEG room 1 12sq. m
Operation Roomo Operation theatre 2 60sq. mo Scrub area 1 12sq. mo Staff Change area 2 12sq. mo Clean utility room 1 6sq. mo Soiled utility room 1 6sq. mo Nurse station 1 12sq. mo Anesthesia store 1 8sq. mo OR equipment store 1 12sq. mo Sterile supply room 1 12sq. mo Doctor’s office 1 12sq. mo Duty room 1 8sq. mo Janitor’s closet 1 6sq. mo Toilet rooms 2 8sq. mo Shower rooms 2 8sq. m
Neurology ward/ inpatient roomo Patient rooms for a minimum of 10 beds {with
maximum room capacity not more than 6 beds} 2 96sq. m
o Isolation rooms 2 30sq. m
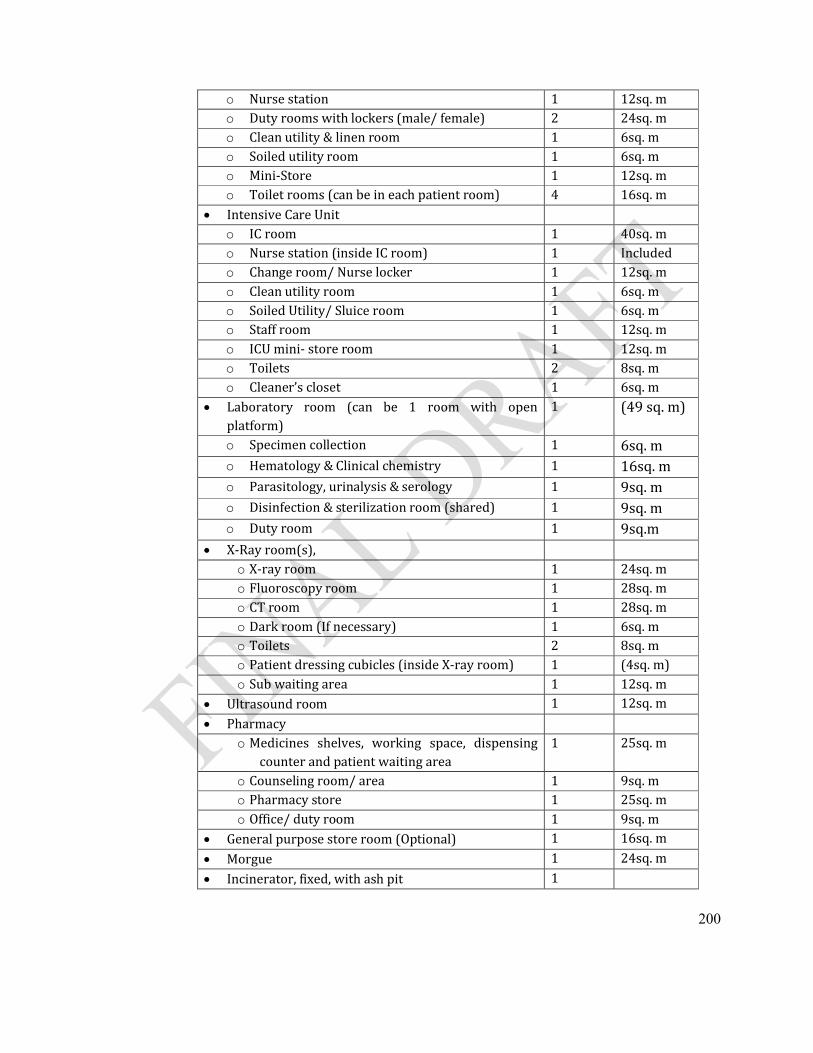
200
o Nurse station 1 12sq. mo Duty rooms with lockers (male/ female) 2 24sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 1 12sq. mo Toilet rooms (can be in each patient room) 4 16sq. m
Intensive Care Unit o IC room 1 40sq. mo Nurse station (inside IC room) 1 Included o Change room/ Nurse locker 1 12sq. mo Clean utility room 1 6sq. mo Soiled Utility/ Sluice room 1 6sq. mo Staff room 1 12sq. mo ICU mini- store room 1 12sq. mo Toilets 2 8sq. mo Cleaner’s closet 1 6sq. m
Laboratory room (can be 1 room with open platform)
1 (49 sq. m)
o Specimen collection 1 6sq. mo Hematology & Clinical chemistry 1 16sq. mo Parasitology, urinalysis & serology 1 9sq. mo Disinfection & sterilization room (shared) 1 9sq. mo Duty room 1 9sq.m
X-Ray room(s), o X-ray room 1 24sq. mo Fluoroscopy room 1 28sq. mo CT room 1 28sq. mo Dark room (If necessary) 1 6sq. mo Toilets 2 8sq. mo Patient dressing cubicles (inside X-ray room) 1 (4sq. m)o Sub waiting area 1 12sq. m
Ultrasound room 1 12sq. m
Pharmacyo Medicines shelves, working space, dispensing
counter and patient waiting area1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 9sq. m
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
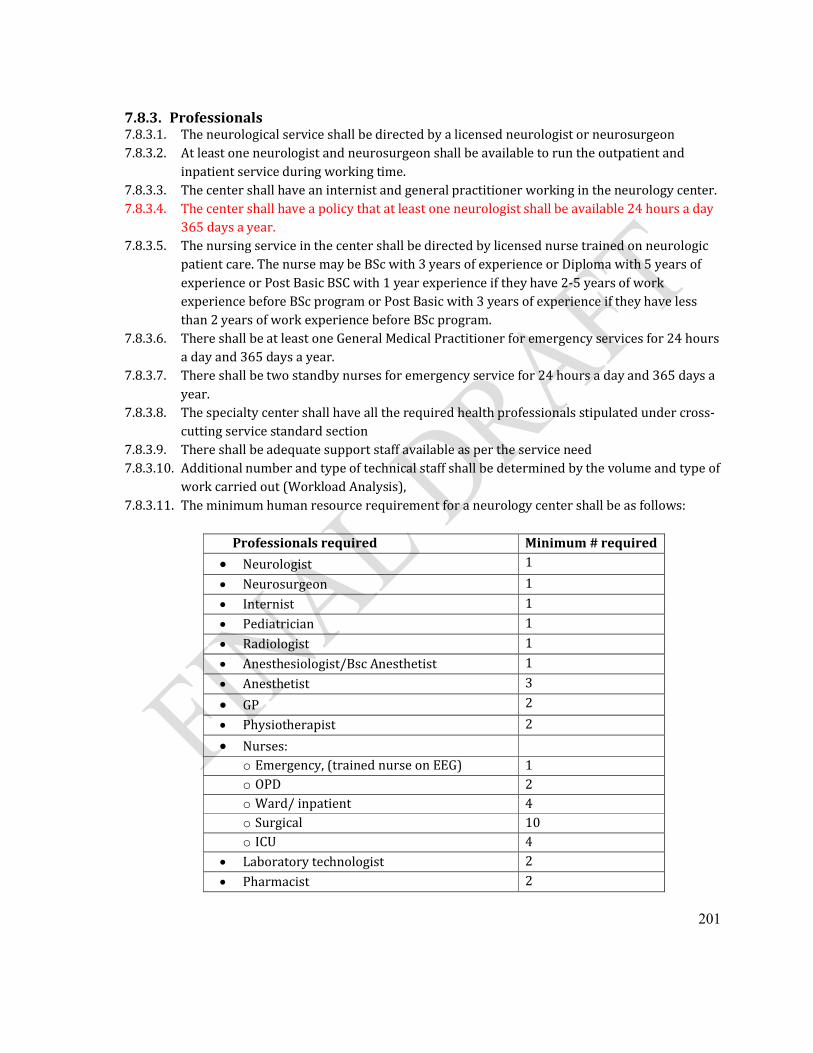
201
7.8.3. Professionals7.8.3.1. The neurological service shall be directed by a licensed neurologist or neurosurgeon7.8.3.2. At least one neurologist and neurosurgeon shall be available to run the outpatient and
inpatient service during working time. 7.8.3.3. The center shall have an internist and general practitioner working in the neurology center. 7.8.3.4. The center shall have a policy that at least one neurologist shall be available 24 hours a day
365 days a year.7.8.3.5. The nursing service in the center shall be directed by licensed nurse trained on neurologic
patient care. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
7.8.3.6. There shall be at least one General Medical Practitioner for emergency services for 24 hours a day and 365 days a year.
7.8.3.7. There shall be two standby nurses for emergency service for 24 hours a day and 365 days a year.
7.8.3.8. The specialty center shall have all the required health professionals stipulated under cross-cutting service standard section
7.8.3.9. There shall be adequate support staff available as per the service need7.8.3.10. Additional number and type of technical staff shall be determined by the volume and type of
work carried out (Workload Analysis),7.8.3.11. The minimum human resource requirement for a neurology center shall be as follows:
Professionals required Minimum # required
Neurologist 1
Neurosurgeon 1
Internist 1
Pediatrician 1
Radiologist 1
Anesthesiologist/Bsc Anesthetist 1
Anesthetist 3
GP 2
Physiotherapist 2
Nurses: o Emergency, (trained nurse on EEG) 1o OPD 2o Ward/ inpatient 4o Surgical 10o ICU 4
Laboratory technologist 2
Pharmacist 2
202
Radiographer 2Support staff Receptionist 2
Cleaner 4
Porter/ runner 2
7.8.4. Products7.8.4.1. The outpatient service of the center shall have the following equipment & supplies:
(a) Examination couches,(b) Examination light,(c) MRI or CT(d) Diagnostic sets:
reflex hammers ophthalmoscope thermometer sphygmomanometer Snellen’s chart Tuning fork
(e) Weighing scale,(f) Height measurement,(g) EEG machine,(h) Nerve
conduction/electromyography machine,
(i) Doppler ultrasound(j) Lumbar puncture set with
manometer
7.8.4.2. The inpatient service shall have the following equipments & supplies:(a) Patient beds,(b) Diagnostic sets: (Torch,
Otoscope, funduscope, patella hammer etc…
(c) Weighing scales, (d) Vital sign set: thermometer, BP
apparatus, stethoscope etc… (e) Examination couch, (f) Medicine trolley, (g) Lumbar puncture set,(h) EKG machine, (i) Suction machine,(j) Drip counters/Infusion pump, (k) Tourniquet,(l) IV stands,(m)Oxygen source/ Oxygen
cylinder, Flow-meters for oxygen,
(n) Oxygen face mask,(o) Nebulizer, (p) Nasal prongs catheters,
(q) Self inflating bags for respiratory support, Masks, endotracheal tubes,
(r) Laryngoscope,(s) Cannulas, (t) Nasogastric tubes, (u) Glucometer and glucostick,(v) Pulseoximeter,(w)Wheelchair,(x) Over bed table(for feeding),(y) Bed side cabinet,(z) Curtain fixed with the ceiling,(aa) Kick buckets,(bb) Cup board, (cc) Wall clock (dd) Trolley for vital sign
monitoring(ee) Refrigerator with
temperature control for medication
(ff) Medication Cupboard with lock(gg) Patient chart holder
7.8.4.3. The neurology service unit shall have all medicines at all times specific to this center as per the national medicine list of Ethiopia
203
7.9. Gastroenterology Center7.9.1. Practices7.9.1.1. The Gastroenterology center shall have the following services:
(a) outpatient service,(b) follow-up clinic, (c) referral services to respective facilities,(d) Emergency gastroenterology and/ or care for GI bleedings, (e) Inpatient care for different gastroenterology diseases, (f) Investigation & interventions with endoscopies.
7.9.1.2. There shall be written protocols/ procedures for the consultation and management of cases that shall include:
(a) Identifying critical cases,(b) Handling of Emergency & critically ill patients,(c) Infection control specified under this standard and National IP guideline,(d) Procedures, interventions and special investigations like Endoscopy,
sigmoidoscopy, proctoscopy, etc. ,(e) Referral of patients, (f) Monitoring and follow-up of patients.(g) Inpatient Gastroenterology Service.
7.9.1.3. The center shall avail medical service for emergency conditions for 24 hours throughout the year.
7.9.1.4. Information contained in the medical record shall be complete and sufficiently detailed relative to the patient's history, physical examination, diagnosis, diagnostic procedures, medication administration, and treatment. Refer to the medical record section of this standard.
7.9.1.5. The Gastroenterology center shall have a follow-up service for patients with chronic ailments.
7.9.1.6. Diseases under national surveillance shall be reported to FMOH through the proper channel.
7.9.1.7. The Gastroenterology center shall avail updated reference materials, treatment guidelines and manuals within the scope of practice (e.g. National TB and leprosy, pain management, Malaria treatment, ART, etc)
7.9.1.8. The center shall use standard prescriptions and different request forms for investigation like laboratory, x-ray, etc.
7.9.1.9. The center shall have a system for involving patients, family members &/ or caretakers in the process of care & treatment.
7.9.1.10. There shall be chronic care follow up service for certain prevalent neurological conditions in the center.
7.9.1.11. There shall be a protocol for instrument processing & sterilization.

204
7.9.2. Premises7.9.2.1. In addition to emergency and isolation beds, the specialty center shall have at least
ten inpatient admission beds.7.9.2.2. Admission rooms shall be with a maximum capacity of six beds per room.7.9.2.3. The Gastroenterology centre shall have an isolation room for treatment of
conditions that require such services. 7.9.2.4. The nurse station shall be situated in a central place where direct observation for
patients in acute care.7.9.2.5. In addition to the ward rooms the Gastroenterology center shall have the following
rooms & facilities:(a) A private area for counseling (examination room/Doctors office)(b) Duty room/Station(c) Nurse station(d) Care after death room,(e) Utility rooms
7.9.2.6. The summary of minimum premises for Gastroenterology center shall be as follows:Rooms required #
requiredArea required
Reception, registration/ recording & waiting area 1 40sq. m
Examination rooms 2 24sq. m
Treatment/ injection room 1 12sq. m
Emergency room with 2 resuscitation couches 1 16sq. m
Toilet room (male & female) (OPD) 4 16 sq. m
Central sterilization 1 16 sq. m
Endoscopy room 1 12 sq. m
Gastroenterology ward/ inpatient roomo Patient rooms for a minimum of 10 beds {with
maximum room capacity not more than 6 beds} 2 96sq. m
o Isolation rooms 2 30sq. mo Nurse station 1 12sq. mo Duty rooms with lockers (male/ female) 2 24sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 1 12sq. mo Toilet rooms (can be in each patient room) 4 16sq. m
Laboratory room (can be 1 room with open platform)
1 (40 sq. m)
o Specimen collection 1 6sq. m

205
o Hematology & Clinical chemistry 1 16sq. mo Parasitology, urinalysis & serology 1 9sq. mo Disinfection & sterilization room (shared) 1 9sq. mo Duty room 1 9sq.m
X-Ray room(s), o X-ray room 1 24sq. mo Fluoroscopy room 1 28sq. mo CT room (Optional) 1 28sq. mo Barium kitchen with sink 1 6sq. mo Dark room (If necessary) 1 6sq. mo Toilets 2 8sq. mo Patient dressing cubicles (inside X-ray rooms) 1 (4sq. m)o Sub waiting area 1 12sq. m
Ultrasound room 1 12sq. m
Pharmacyo Medicines shelves, working space, dispensing
counter and patient waiting area1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 9sq. m
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
7.9.3. Professionals7.9.3.1. The Gastroenterology center shall be directed by a gastroenterologist with a
minimum of two years related experience. 7.9.3.2. At least one gastroenterologist shall be available to run the outpatient and inpatient
service during working time. 7.9.3.3. The center shall have an internist and general practitioner working in the
gastroenterology center. 7.9.3.4. The center shall have a policy that at least one gasteroenterologist shall be available 24
hours a day 365 days a year.7.9.3.5. The nursing service in the center shall be directed by licensed nurse trained on
gastroenterology patient care. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
206
7.9.3.6. There shall be at least one General Medical Practitioner for emergency services for 24 hours a day and 365 days a year.
7.9.3.7. There shall be two standby nurses for emergency service for 24 hours a day and 365 days a year.
7.9.3.8. The specialty center shall have all the required health professionals stipulated under cross-cutting service standard section
7.9.3.9. There shall be adequate support staff available as per the service need7.9.3.10. Additional number and type of technical staff shall be determined by the volume
and type of work carried out (Workload Analysis)7.9.3.11. There shall be adequate support staff available as per the service need.7.9.3.12. The Gastroenterology center shall have at least the following professionals:
Professionals required Minimum # required Gastroenterologist 1
Internist 1
Radiologist 1
GP 1
Nurses: o Emergency 1o OPD 2o Ward/ inpatient 3
Lab technologist 2
Pharmacist 2
Radiographer 2Support staff Receptionist 2
Cleaner 4
Porter/ runner 2
7.9.4. Products7.9.4.1. The gastroenterology center shall have the following supplies and functional
equipments at OPD:a) Diagnostic Equipments:
Stethoscope, Sphygmomanometer, Weighing scales for adults, Height Measurement, Tape meter, Thermometer, Reflex/patellar hammer,
b) X-ray viewer,c) Examination couch,d) Examination light,e) Biopsy set, f) Cut down set, g) Endoscope,h) Proctoscope,i) Laryngoscope (optional),
j) Resuscitation kits: Ambu bag, air ways,
k) Oxygen cylinder, Flow-meters for oxygen, Nasal prongs/ catheters,
l) Plastic bowels for chemical disinfection,
7.9.4.2. The inpatient service of Gastroenterology center shall have the following supplies and functional equipments:
a) Examination couch, b) Patient beds,c) Diagnostic sets: (Torch,
Otoscope, funduscope, patella hammer etc…
d) Weighing scales, e) Vital sign set: thermometer,
BP apparatus, stethoscope etc…
f) Medicine trolley, g) Suction machine, h) IV stands,i) Oxygen source/ Oxygen
cylinder, Flow-meters for oxygen,
j) Oxygen face mask,
k) Nasal prongs catheters, l) Self inflating bags for
respiratory support, Masks, endotracheal tubes,
m) Laryngoscope,n) Cannulas, o) Nasogastric tubes, p) Glucometer and glucostick,q) Pulseoximeter,r) Wheelchair,s) Over bed table( for feeding),t) Bed side cabinet,u) Curtain fixed with the ceiling,v) Kick buckets,w) Cup board
7.9.4.3. The center shall have the following emergency medicines and supplies at all times.a) Emergency medicines:
a. Esomprazole inj.,b. Adrenaline,c. Diazepam,d. Pethidine,e. Hydrocortisone,
f. Lidocaine,g. Sclerosing agents, inj.,h. KCl,i. Calcium Gluconate,j. IV fluids, of all types,
b) Spatula, K-Y jelly, surgical and disposable gloves, antiseptics, cotton, gauzec) Glucometer and glucosticks,
208
7.10. Renal Center 7.10.1. Practice7.10.1.1. The Renal center shall provide both medical & surgical services (i.e., Nephrology &
Urology) with the following modalities:(a) outpatient service,(b) follow-up clinic,(c) referral services to respective facilities,(d) Emergency service for kidney & related problems, (e) Inpatient care for related diseases,
7.10.1.2. There shall be written protocols and procedures for medical & surgical management of common genito- urinary & kidney conditions.
7.10.1.3. The center shall avail both nephrology & urology services for emergency renal conditions for 24 hours a day throughout the year,
7.10.1.4. The center shall have an Intensive Care Unit (ICU) with all requirements stipulated under ICU standards
7.10.1.5. The center shall provide anesthesia services as per the standards stipulated for anesthesia services.
7.10.1.6. For non-emergency condition the nephrology & urology services shall be available during the regular working hours.
7.10.1.7. The nephrology & urology services shall be organized to cover all the shifts for admitted patients (24 hours of the day and seven days of the week),
7.10.1.8. Nursing functions for each shift shall be carried out by the nurse responsible for the shift,
7.10.1.9. The service shall have written policies and procedures that shall include:(a) Admission and discharge criteria specific to the service; (b) A visitors policy,(c) Infection control as per National and or IP guideline of the center,(d) Transfer and Referral of patients,(e) Monitoring and follow-up of patients,
7.10.1.10. The urology unit of the renal center shall have the following services:(a) Urethroscopy,(b) Extracorporal Shock Wave Lithotripsy,(c) Percutaneous lithotripsy,(d) Insertion of stents,(e) Transurethral diagnostic procedures &/ or lithotripsy(f) And other related services
7.10.1.11. The nephrology unit of the renal center shall have the following services:(a) Medical treatment,
209
(b) Dialysis,7.10.1.12. The center shall develop & implement operational policies addressing at least the
following concerns:(a) Lithotripsy:
Maximum number of shocks &/ or voltage allowable, Post ESWL follow-up, Contraindicated medication, Pre-admission testing requirements, Pediatric cases, Criteria for: - treatment; cancelation; retreatment; General safety protocols, Inspection of lithotripter by qualified person; with documentation of all
preventive maintenances,(b) Hemodialysis:
Admission criteria that includes acceptance of patients who have communicable or transmittable diseases,
Orientation of new patients to the unit, Contraindications, Pre-admission testing requirements, Criteria for: - treatment; cancelation; retreatment; General safety protocols, Infection control protocol & dialysis waste management, Specific facility response to medical & non-medical emergencies including, for
e.g., equipment failure & water supply problems, Regular inspection of hemodialysis machine by qualified person; with
documentation of all preventive maintenances, There shall be proper written and verbal instruction for patients about dialysis
process and the machine used.7.10.1.13. There shall be a red alarm light and an audible beep on the machine.7.10.1.14. The set up for hemodialysis is to the level of intensive care, there shall be isolation
and restriction of traffic. 7.10.1.15. The patient or guardian or care giver shall be oriented, explained about the machine
and its part before and during the dialysis process.7.10.1.16. The administrative functions shall be a responsibility of the center administration,7.10.1.17. All medical records & lab investigations with plan shall be documented on each
patient’s record. 7.10.1.18. Information contained in the medical record shall be complete and sufficiently
detailed relative to the patient's history, physical examination, diagnosis, diagnostic procedures, medication administration, and treatment.
7.10.1.19. The center shall use standard prescription & different request forms for investigation like laboratory, x-ray, etc.
7.10.1.20. The center shall have a system for involving patients, family members &/ or caretakers in the process of care & treatment.
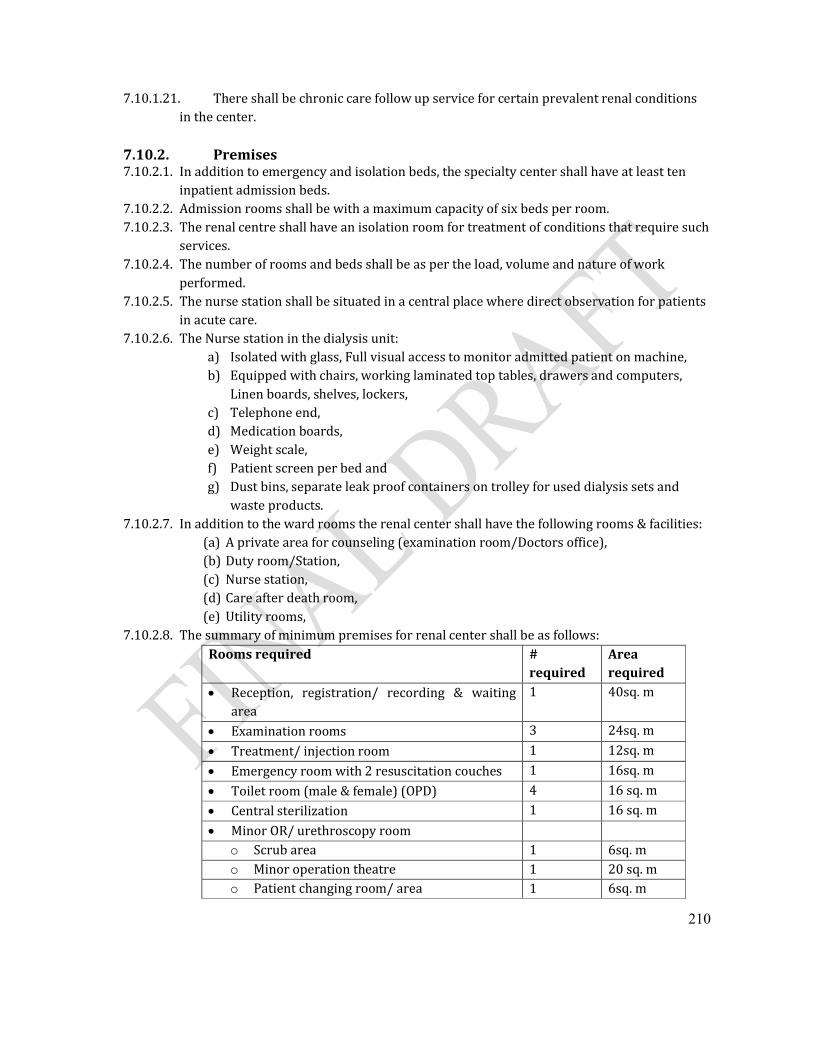
210
7.10.1.21. There shall be chronic care follow up service for certain prevalent renal conditions in the center.
7.10.2. Premises7.10.2.1. In addition to emergency and isolation beds, the specialty center shall have at least ten
inpatient admission beds.7.10.2.2. Admission rooms shall be with a maximum capacity of six beds per room.7.10.2.3. The renal centre shall have an isolation room for treatment of conditions that require such
services. 7.10.2.4. The number of rooms and beds shall be as per the load, volume and nature of work
performed.7.10.2.5. The nurse station shall be situated in a central place where direct observation for patients
in acute care.7.10.2.6. The Nurse station in the dialysis unit:
a) Isolated with glass, Full visual access to monitor admitted patient on machine,b) Equipped with chairs, working laminated top tables, drawers and computers,
Linen boards, shelves, lockers,c) Telephone end,d) Medication boards, e) Weight scale,f) Patient screen per bed and g) Dust bins, separate leak proof containers on trolley for used dialysis sets and
waste products.7.10.2.7. In addition to the ward rooms the renal center shall have the following rooms & facilities:
(a) A private area for counseling (examination room/Doctors office),(b) Duty room/Station,(c) Nurse station,(d) Care after death room,(e) Utility rooms,
7.10.2.8. The summary of minimum premises for renal center shall be as follows:Rooms required #
requiredArea required
Reception, registration/ recording & waiting area
1 40sq. m
Examination rooms 3 24sq. m
Treatment/ injection room 1 12sq. m
Emergency room with 2 resuscitation couches 1 16sq. m
Toilet room (male & female) (OPD) 4 16 sq. m
Central sterilization 1 16 sq. m
Minor OR/ urethroscopy roomo Scrub area 1 6sq. mo Minor operation theatre 1 20 sq. mo Patient changing room/ area 1 6sq. m
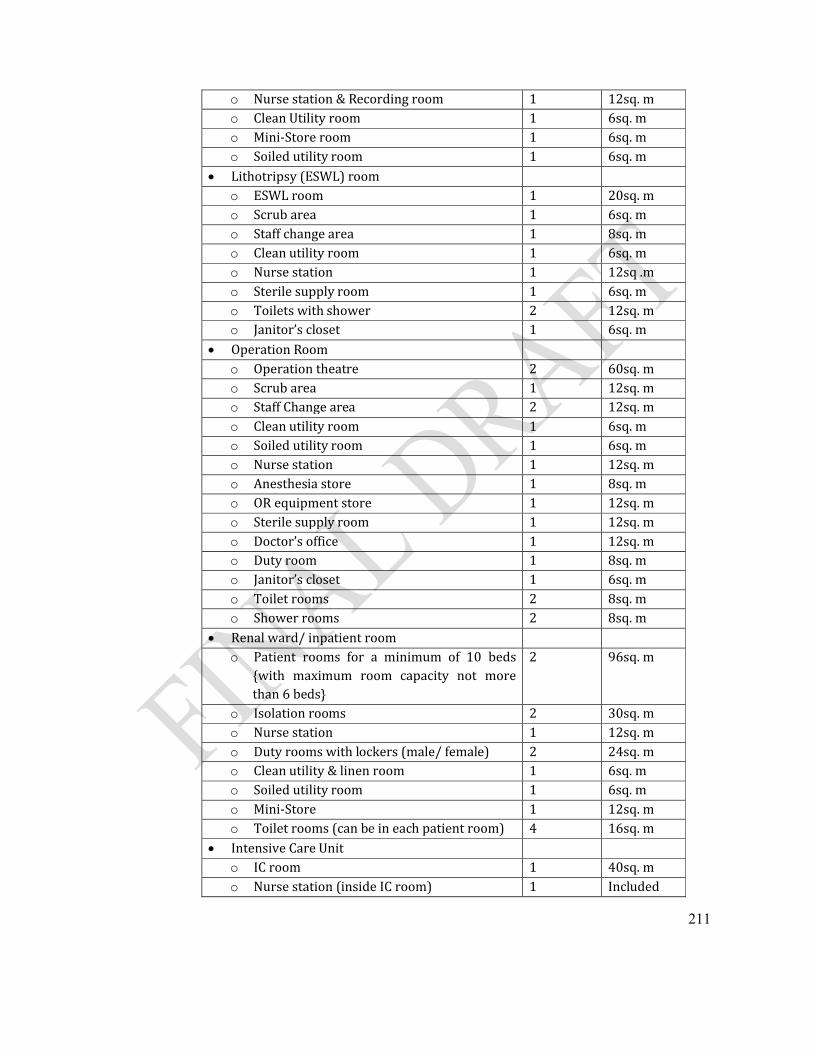
211
o Nurse station & Recording room 1 12sq. mo Clean Utility room 1 6sq. mo Mini-Store room 1 6sq. mo Soiled utility room 1 6sq. m
Lithotripsy (ESWL) roomo ESWL room 1 20sq. mo Scrub area 1 6sq. mo Staff change area 1 8sq. mo Clean utility room 1 6sq. mo Nurse station 1 12sq .mo Sterile supply room 1 6sq. mo Toilets with shower 2 12sq. mo Janitor’s closet 1 6sq. m
Operation Roomo Operation theatre 2 60sq. mo Scrub area 1 12sq. mo Staff Change area 2 12sq. mo Clean utility room 1 6sq. mo Soiled utility room 1 6sq. mo Nurse station 1 12sq. mo Anesthesia store 1 8sq. mo OR equipment store 1 12sq. mo Sterile supply room 1 12sq. mo Doctor’s office 1 12sq. mo Duty room 1 8sq. mo Janitor’s closet 1 6sq. mo Toilet rooms 2 8sq. mo Shower rooms 2 8sq. m
Renal ward/ inpatient roomo Patient rooms for a minimum of 10 beds
{with maximum room capacity not more than 6 beds}
2 96sq. m
o Isolation rooms 2 30sq. mo Nurse station 1 12sq. mo Duty rooms with lockers (male/ female) 2 24sq. mo Clean utility & linen room 1 6sq. mo Soiled utility room 1 6sq. mo Mini-Store 1 12sq. mo Toilet rooms (can be in each patient room) 4 16sq. m
Intensive Care Unit o IC room 1 40sq. mo Nurse station (inside IC room) 1 Included
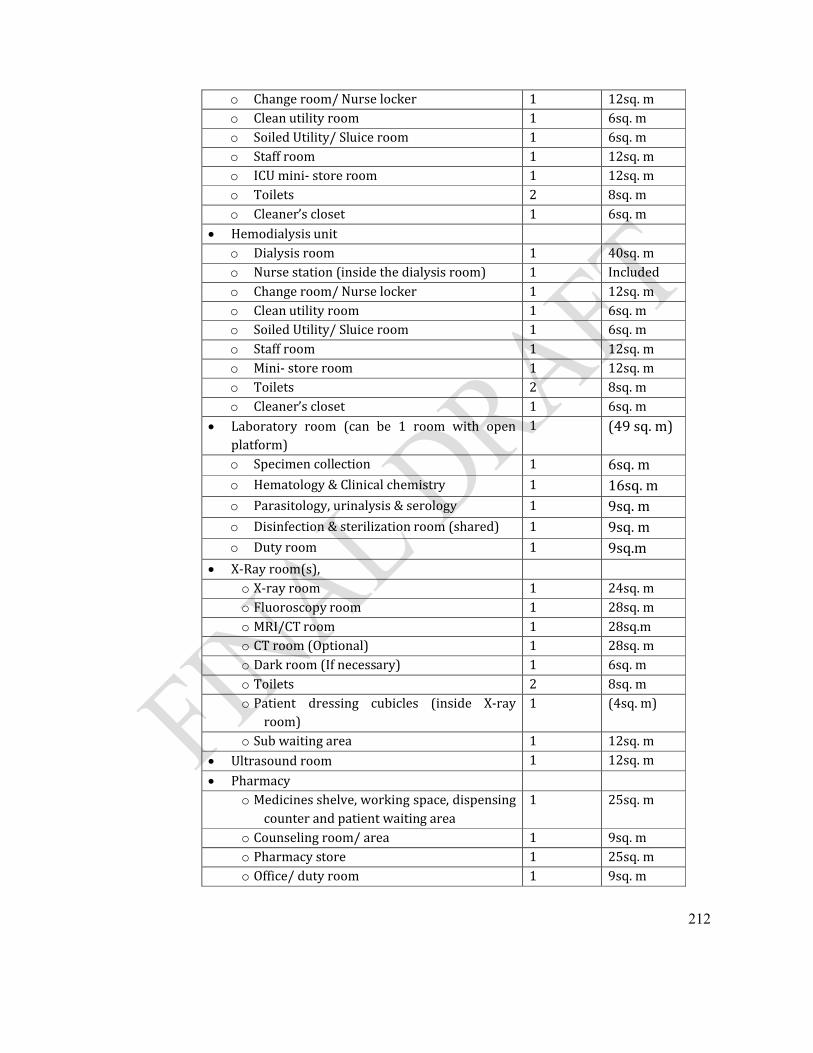
212
o Change room/ Nurse locker 1 12sq. mo Clean utility room 1 6sq. mo Soiled Utility/ Sluice room 1 6sq. mo Staff room 1 12sq. mo ICU mini- store room 1 12sq. mo Toilets 2 8sq. mo Cleaner’s closet 1 6sq. m
Hemodialysis unito Dialysis room 1 40sq. mo Nurse station (inside the dialysis room) 1 Included o Change room/ Nurse locker 1 12sq. mo Clean utility room 1 6sq. mo Soiled Utility/ Sluice room 1 6sq. mo Staff room 1 12sq. mo Mini- store room 1 12sq. mo Toilets 2 8sq. mo Cleaner’s closet 1 6sq. m
Laboratory room (can be 1 room with open platform)
1 (49 sq. m)
o Specimen collection 1 6sq. mo Hematology & Clinical chemistry 1 16sq. mo Parasitology, urinalysis & serology 1 9sq. mo Disinfection & sterilization room (shared) 1 9sq. mo Duty room 1 9sq.m
X-Ray room(s), o X-ray room 1 24sq. mo Fluoroscopy room 1 28sq. mo MRI/CT room 1 28sq.mo CT room (Optional) 1 28sq. mo Dark room (If necessary) 1 6sq. mo Toilets 2 8sq. mo Patient dressing cubicles (inside X-ray
room)1 (4sq. m)
o Sub waiting area 1 12sq. m Ultrasound room 1 12sq. m
Pharmacyo Medicines shelve, working space, dispensing
counter and patient waiting area1 25sq. m
o Counseling room/ area 1 9sq. mo Pharmacy store 1 25sq. mo Office/ duty room 1 9sq. m

213
General purpose store room (Optional) 1 16sq. m
Morgue 1 24sq. m
Incinerator, fixed, with ash pit 1
7.10.3. Professionals7.10.3.1. The renal center shall be directed by a licensed nephrologist or urologist/ urosurgeon7.10.3.2. At least one nephrologist and urologist shall be available to run the outpatient and
inpatient service during working time. 7.10.3.3. The nephrologist shall be responsible for:
(a) Medical services provided to each patient; while the licensed nurse shall be responsible for all nursing care provided to the patient, nursing visits, care, carry out and execution of the orders
(b) Control of the hemodialysis service,(c) Being available (physically present) during working time, and on call basis during
after hours, (d) While on duty or on call, the specialist shall be able to present at the center in a
period of time not to exceed thirty (30) minutes.7.10.3.4. The urologist shall be responsible for:
(a) Surgical services provided to patients; -tripsy, -scopy, (b) Being available (physically present) during working time, and on call basis during
after working hours, (c) While on duty or on call, the specialist shall be able to present at the center in a
period of time not to exceed thirty (30) minutes.7.10.3.5. The center shall have an internist and general practitioner working in the renal center. 7.10.3.6. The nursing service in the center shall be directed by licensed nurse trained on renal
patient care. The nurse may be BSc with 3 years of experience or Diploma with 5 years of experience or Post Basic BSC with 1 year experience if they have 2-5 years of work experience before BSc program or Post Basic with 3 years of experience if they have less than 2 years of work experience before BSc program.
7.10.3.7. There shall be at least one General Medical Practitioner for emergency services for 24 hours a day and 365 days a year and specialist(s) on call basis.
7.10.3.8. There shall be two standby nurses for emergency service for 24 hours a day and 365 days a year.
7.10.3.9. There shall be one to one ratio among nurses and dialysis machines at all times.7.10.3.10. The dialysis machine shall be attended & checked all the time by appropriate
technician or engineer.7.10.3.11. The specialty center shall have all the required health professionals stipulated under
cross-cutting service standard section7.10.3.12. There shall be adequate support staff available as per the service need7.10.3.13. Additional number and type of technical staff shall be determined by the volume and
type of work carried out (Workload Analysis),7.10.3.14. The renal center shall have the following minimum professionals as summary:
Professionals required Minimum # required
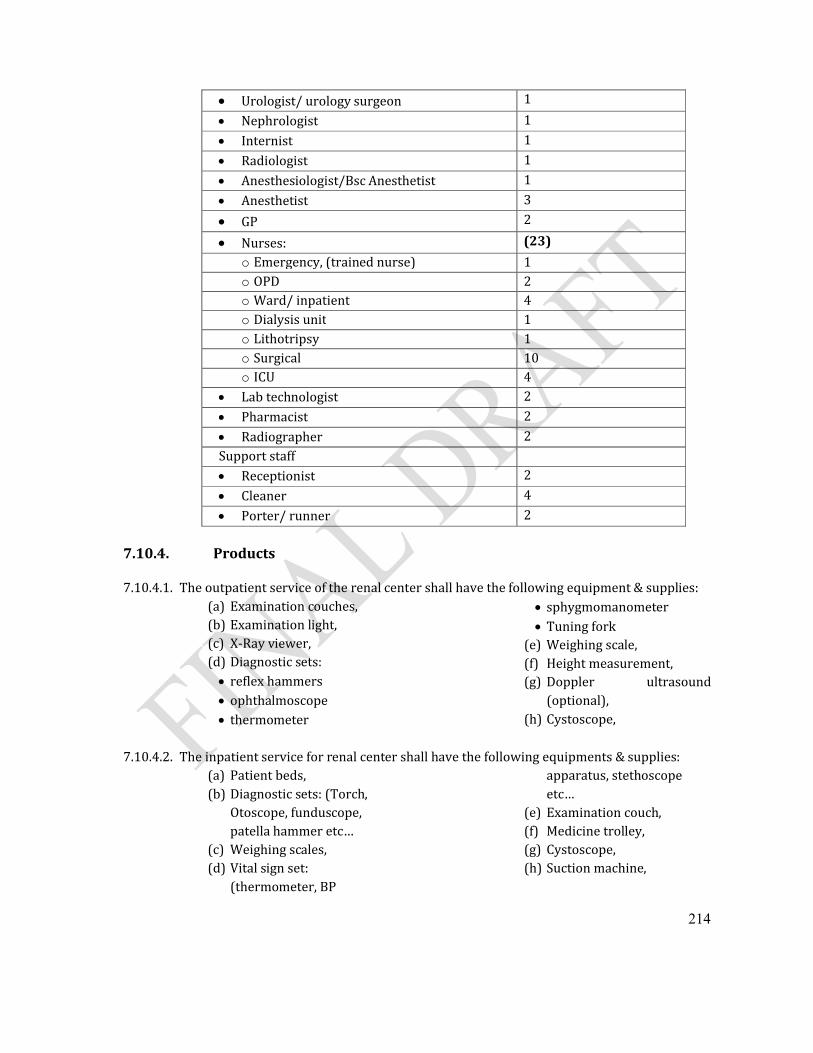
214
Urologist/ urology surgeon 1
Nephrologist 1
Internist 1
Radiologist 1
Anesthesiologist/Bsc Anesthetist 1
Anesthetist 3
GP 2
Nurses: (23)
o Emergency, (trained nurse) 1o OPD 2o Ward/ inpatient 4o Dialysis unit 1o Lithotripsy 1o Surgical 10o ICU 4
Lab technologist 2
Pharmacist 2
Radiographer 2Support staff Receptionist 2
Cleaner 4
Porter/ runner 2
7.10.4. Products
7.10.4.1. The outpatient service of the renal center shall have the following equipment & supplies:(a) Examination couches,(b) Examination light,(c) X-Ray viewer,(d) Diagnostic sets: reflex hammers ophthalmoscope thermometer
sphygmomanometer Tuning fork
(e) Weighing scale,(f) Height measurement,(g) Doppler ultrasound
(optional),(h) Cystoscope,
7.10.4.2. The inpatient service for renal center shall have the following equipments & supplies:(a) Patient beds,(b) Diagnostic sets: (Torch,
Otoscope, funduscope, patella hammer etc…
(c) Weighing scales, (d) Vital sign set:
(thermometer, BP
apparatus, stethoscope etc…
(e) Examination couch, (f) Medicine trolley, (g) Cystoscope,(h) Suction machine,
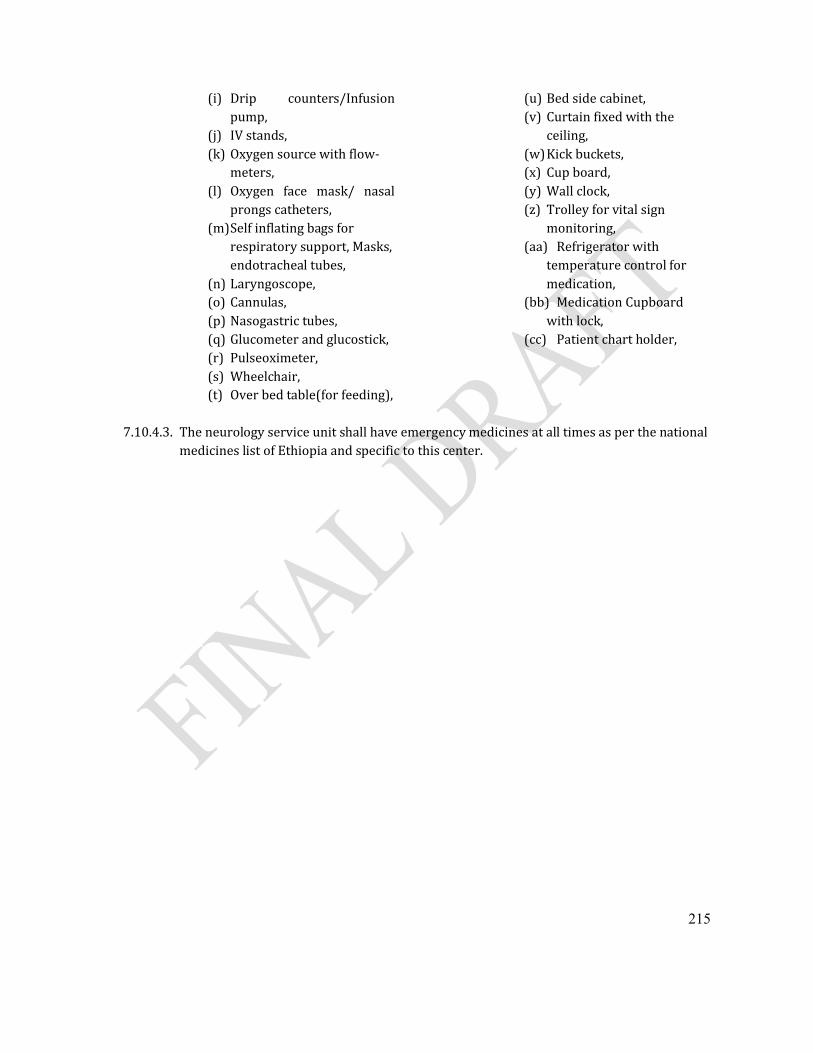
215
(i) Drip counters/Infusion pump,
(j) IV stands,(k) Oxygen source with flow-
meters, (l) Oxygen face mask/ nasal
prongs catheters, (m)Self inflating bags for
respiratory support, Masks, endotracheal tubes,
(n) Laryngoscope,(o) Cannulas, (p) Nasogastric tubes, (q) Glucometer and glucostick,(r) Pulseoximeter,(s) Wheelchair,(t) Over bed table(for feeding),
(u) Bed side cabinet,(v) Curtain fixed with the
ceiling,(w)Kick buckets,(x) Cup board, (y) Wall clock,(z) Trolley for vital sign
monitoring,(aa) Refrigerator with
temperature control for medication,
(bb) Medication Cupboard with lock,
(cc) Patient chart holder,
7.10.4.3. The neurology service unit shall have emergency medicines at all times as per the national medicines list of Ethiopia and specific to this center.
216
SECTION EIGHT: PHYSICAL FACILITY STANDARDS
8.1. General8.1.1. A Specialty center shall fulfill the minimum required standards for the building
which contains the facilities required to render the services contemplated in the application for license. The term "safe" used in this Section shall be interpreted in the light of compliance with the requirements of the latest country building codes presently in effect.
8.1.2. The Specialty center premises shall have dedicated territory/ compound with entrances.
8.1.3. All rooms shall have adequate light and ventilation.8.1.4. All rooms for patient care shall promote patient dignity and privacy. 8.1.5. All patient care rooms shall be provided with running water supply & functional
hand washing basin.8.1.6. The arrangement of rooms shall consider proximity between related services.8.1.7. Glass doors shall be marked to avoid accidental collision. 8.1.8. Potential source of accidents shall be identified and acted upon like slippery
floors, misfit in doorways and footsteps.8.1.9. The specialty center facilities shall be well marked and easily accessible for
persons with disability.8.1.10. The specialty center shall have fire extinguisher placed in visible area. 8.1.11. The office layout shall be arranged in a way that ensures patient independence
and comfort by label and service proximity.8.1.12. The premises of specialty center shall have ceilings.8.1.13. The Internal surfaces of the center (floors, walls, and ceilings) shall be:
a) Smooth, impervious, free from cracks, recesses, projecting ledges and other features that could harbor dust or spillage,
b) Easy to clean and decontaminate effectively,
c) Constructed of materials that are non-combustible or have high fire-resistance and low flame-spread characteristics.
8.1.14. The specialty center shall have a mechanism to have uninterrupted access to ambulance services and it shall have a designated parking area.
8.1.15. The corridor to examination rooms shall be spacious enough to allow easy transport of emergency patients or patients with support.

217
8.1.16. There shall be a waste disposal mechanism for all categories of wastes generated by the specialty center.
8.1.17. The Specialty center shall have a minor operation room which shall have:a) Standard size, with layout of change area, scrub area, operating/ procedure
area when viewed from entrance.b) Washable walls; crack free and of scrub-able Ceiling.c) Vicinity of plumbing fixtures, floors and walls penetrated by pipes shall be
sealed & smoothened, d) Floor shall be smooth, easily cleanable and non-slippery, preferably made
of marble or ceramic. e) Fitted with at least 2 fixed electric outlets, f) A line shall be clearly marked in red or green on the floor, beyond which no
person shall be permitted to set foot without changing shoes or applying shoes cover.
g) The scrub area which shall be provided with wide sink and taps for running water. The taps for running water shall be hand free, manipulated with elbow or knee. (e.g., long arm valve gate).
8.1.18. In addition to emergency and isolation, the specialty center shall have at least ten inpatient beds.
8.1.19. The room used for admission shall have an area calculated using the following table and specifications unless otherwise stated in a specific service of this standard:
a) Distance of bed from fixed walls shall be 0.9 m,
b) Distance between beds shall be 1.2 m (Conventionally inpatient beds have width of 0.9m and length of 2m),
c) In case of multiple beds, area per bed shall be 8.6 m2,
d) In case of single bed room, area shall be 9 m2
8.1.20. The maximum room capacity shall be 6 patients (beds) per room.8.1.21. Depending on the size of the room, each inpatient room shall have at least one
window. 8.1.22. All inpatient rooms shall have easy access to a bath room and toilet.8.1.23. The inpatient rooms shall provide call bells at each bed.8.1.24. The specialty center shall have an emergency room which shall be easily
recognizable to the public and shall be labeled in bold. 8.1.25. The emergency premises shall be low traffic area and there shall be reserve
parking place for ambulances.
218
8.1.26. The emergency area shall be spacious enough to provide a space for the following tasks:(g) Accepting patients and providing immediate care including emergency
procedures,(h) Admitting for a maximum of 24 hrs to provide resuscitation,(i) Access to emergency medicines, supplies and equipments.
8.1.27. Resuscitation couches shall be arranged in a way 90cm away from walls and 1.2m gap.
8.1.28. At emergency room there shall be sub waiting area for attendants and caregivers.
8.2. Site Selection Requirements 8.2.1. The entrance to the specialty center shall be clear, easy to road access,8.2.2. The entrance to the specialty center shall be away from highways, railways,
construction areas, 8.2.3. There shall be secured boundaries, no access for animals, 8.2.4. The specialty center shall be located away from unordinary conditions of undue
noises, smoke, dust or foul odors, and shall not be located adjacent to railroads, freight yards, grinding mills, chemical industries, gas depot and waste disposal sites.
8.2.5. Specialty center shall be provided with road access, water supply, electric city and communication facilities.
8.2.6. Specialty center shall be well landscaped, therapeutic, appealing scenery, attractive with green areas/beautiful trees and possible outdoor recreation facilities.
8.3. Construction Requirements 8.3.1. The Authority shall be consulted before commencement of any physical
development planned for new health facility; or remodeling of existing building for conformity to the standards.
8.3.2. Plans and specifications for construction or remodeling shall comply with Ethiopian Building Code.
8.3.3. The authority may be consulted on construction processes and milestones for conformity to the standards.
8.3.4. Upon completion of construction the authority shall inspect and issue an approval for operation of the specialty center if all the findings are in conformity to the standards.
8.3.5. There shall be approval from the authority when buildings constructed for other purposes are used for the operation of specialty center.
219
8.3.6. The construction shall comply with the following codes and guidelines to provide a safe and accessible environment:
a) The Ethiopian Building Proclamation 624/2009; b) The Ethiopian Standard Building Code;c) Life Safety Code (National Fire Protection Code); d) National Electrical Design Code;e) The Ethiopian Disability Code; f) Other codes –Sanitation codes, environmental protection laws, water codes
8.3.7. Ways, paths and corridors to and between Specialty center buildings shall be well paved, smooth and friendly for people with disability.
8.3.8. Selected construction materials shall be used for special services in conformity to the Ethiopian Building Code.
8.4. Building Space and Elements
8.4.1. The specialty center shall have secured compound with dedicated entrance. If the specialty center is situated in multipurpose multi stair building all service units shall be together and accessible horizontally.
8.4.2. All horizontal and vertical circulation areas that include stairs, doors, windows, corridors, exits and entrances of the center shall be kept clear and free of obstructions.
8.4.3. Size of rooms and space allocation shall consider room loadings based on the number of staff and clients involved, usable medical equipments available, available furniture and applicable functions.
8.4.4. Corridors: 8.4.5. Patient serving corridors shall not be less than 240cm wide, 8.4.6. The openings to the corridor shall be designed to allow easy movement of
stretchers/ couches and be equipped with safety and all assistive devices (door stopper, protecting girders, alarms, self opening electronic devices, etc).
8.4.7. The circulation ways and sub corridors shall be a minimum 2m wide.8.4.8. Doors: Doors shall be able easy to open and close, 8.4.9. Doors swing into corridors shall be avoided.8.4.10. Patient rooms: Each patient room shall meet the following requirements:
a) Floor Area: Floor area shall be 9.20m2 (100ft2) for a single bedroom and 7.50m2 (80ft2) per bed in multi-bedrooms.
b) Ceiling Height: Ceiling height needs to be determined based on the climate, the functional requirements considering air space, technical requirements, room size proportions and number of occupants. The ceiling height of the regular rooms shall not be less than 240cm,
220
c) Ceiling height of operation theater and X-Ray room shall be 320 cm, room requiring interstitial floor needs to be more than 520cms)
d) Windows: All rooms housing patients shall have access to natural light and ventilation, or prove the availability of artificial ventilation and light at all times.
e) Total area of windows shall be 1to 8 proportion of the floor area. f) The window sill shall not be higher than 91cm above the floor. For toilets
and washing rooms, over desk laboratory tables, laundry and kitchen utensils, the height can be modified accordingly).
g) Windows shall not have any obstruction to vision (wall, cooling tower, etc.) within 1.52m as measured perpendicular to the plane of the window.
h) Storage: Each admitted patient shall be provided with a hanging storage space of not less than 40.cm x 60.cm x 130cm (16" x 24" x 52") for his personal belongings.
i) Furnishings: The furniture shall be hygienic (washable, dust and bacteria protective and resistant for cleansing reagents) durable that can control vandalism and avoid accidents.
j) Curtains: rooms shall be equipped with curtains or blinds at windows. All curtains shall have a flame spread of 25 or less or as per the national fire protection code. And all as per the national infection prevention guidelines requirements.
k) Cubicle curtains or equivalent built-in devices for privacy in all multi-bed rooms shall be provided. They shall have a flame spread of 25 or less or as per the national fire protection code.
l) Finishing Walls and ceilings of all rooms (procedure, minor OR, isolation,
laboratory, sterile processing rooms) shall be suitable for easy washing. Floors of the specialty center shall be easily cleanable, smooth, non-
adsorptive, non-slippery. Scrub-able room finishes provided in operating rooms and isolation
rooms shall have smooth, non-adsorptive, non-perforated surfaces that are not physically affected by harsh germicidal cleaning solutions and methods.
All walls and ceiling finishing materials used shall have a 1-hour fire rating (One hour rated products offer more than "one hour's" worth of fire protection).
m) Sanitary Finishing Toilet rooms shall be fitted with functional flush.
221
Toilet rooms shall have floors, walls and ceilings fitted with washable finishing materials.
Floors and walls penetrated by pipes, ducts, siphons and conduits shall be tightly sealed & smooth.
n) Electrical Finishing Patient bed light shall be controlled by the patients. Room light luminescence shall be bright enough for staff activities but
needs to be controlled not to disturb the patients. All electrical fixtures inlets, outlets, appiances shall fulfill Ethiopia
Electrical Safety requirements and if applicable fitted with safety guards,
For psychiatry service area light fixtures, sprinkler heads and other apparatus shall be of a temper resistant type.
8.4.11. Outdoor Areas: the outdoor area shall be equipped and situated to allow safe movement/ flow of patients, care givers, staff and visitors. a) The landscape shall be designed with patient room visual access,b) Walkways, connection roads and elevation differences shall be designed to
allow movements of couches/stretchers and persons with disabilities. c) The outdoor traffic arrangement shall not cross each other.
8.4.12. Windows: windows shall comply with LUX requirements of room space without compromising room temperature and ventilation. a) Windows shall be a minimum of 50 cm wide x 100cm high. However,
dimension shall be adjusted for the climate and bed capacity of the room.b) Windows for specialty center shall be fitted to swing/ open to outside. In
areas where security/ safety grids applied or wire mesh fitted, opening to the room can be allowed.
c) Windows for specialty center shall have open, fitted with wire mesh, at top portion for cross ventilation & uninterrupted circulation of air. Advanced technology can be used that maintain the air circulation.
d) Safety glass, tempered glass or plastic glass materials shall be used for pediatrics and psychiatric service units to avoid possible injuries.
8.4.13. Vertical Circulation: All functioning rooms shall be accessible horizontally.a) Specialty center where functional units are at different floor shall have a
mechanism of accessing all the functioning rooms horizontally- either by stairs, ramp or elevator.
b) Stairs: All stairways and ramps shall have handrails and their minimum width shall be 120cm.
c) All stairways shall be fitted with non slippery finishing materials
222
d) All stair threads, risers and flights shall comply with the Ethiopia Building proclamation.
e) Elevators (optional): Minimum cab dimensions required for elevator is 195cm x 130cm inside clear measurements and minimum width for hatchway and cab doors shall be 100cm.
f) Ramp (Optional): Ramps shall be designed with a slope of 6 to 9 percent, minimum width of 120 cm and the landing floor of 240cm wide on both sides.
8.4.14. Fire Safety Considerations: a) One-Story Building: Wall, ceiling and roof construction shall be of 1-hour fire
resistive construction as defined by National Fire Code. Floor systems shall be of non-combustible construction.
b) Multi-Story Buildings: Must be of two-hour fire resistive construction as defined in National Fire Code.
8.4.15. Parking areas: a) The specialty center shall have reserved parking spaces for ambulance. b) Parking space shall have a clear mark for Staff, Patients and Visitors with
separate 10% of it for person with disability parking all as per Ethiopia Building Proclamation and building code.
c) General services of the specialty center that require loading unloading docks, heavier truck movement and temporary truck parking place shall be available.
d) The parking space shall not cross pedestrian walkways, if it is mandatory to cross, proper precaution measures such as Zebra cross, Speed Breaker, guiding notice and traffic stopping culverts or signals shall be provided.
8.5. Building Systems Specialty center shall have building systems that are designed, installed and operated in such a manner as to provide safety, comfort and well being of the patient. 8.5.1. Water supply and plumbing:
a) Specialty center connected to municipal water system shall maintain the patency of the system, whenever there is any repair or modification to the underground lines and to the elevated tank or to the well or pump.
b) Specialty center connected to its own separate water supply system shall have certificate for safety by the concerned body.
c) Water reserves used in specialty center shall be protected from external contamination, cleaned and washed every 6month.
d) Supply piping within the building shall be in accordance with plumbing standards. Special care must be taken to avoid use of any device or installation which might cause contamination of the supply through back-
223
siphonage or cross connections or the water distribution system shall be protected with anti-siphon devices, and air-gaps to prevent potable water system and equipment contamination.
8.5.2. Sewerage and Waste Processing Systems a) The specialty center shall maintain a sanitary and functioning sewage
system in accordance with the national healthcare waste management guidelines and Ethiopian building code.
b) In addition, the health facility shall fulfill the following requirements; The specialty center shall dispose all sanitary wastes produced in the
center through connection to a suitable municipal sewerage system. septic tank,
Waste segregation shall be done for hazardous wastes before it is released to the municipal or private sewage system.
The specialty center shall provide secluded secured area to collect, contain, process, and dispose of medical and general waste produced.
The specialty center shall have incinerator with combustion level over 600 °C as recommended by the national healthcare waste management guidelines.
8.5.3. Ventilating and Air-Conditioning Systems: a) Airflow shall move from clean to soiled locations. Air movement shall be
designed to reduce the potential of contamination of clean areas. b) Specialty center shall provide adequate ventilation and/or clean air to
prevent the concentrations of contaminants which impair health or cause discomfort to patients and employees.
c) There shall be a mechanical exhaust ventilation system for windowless toilets, baths, laundry rooms, housekeeping rooms, kitchens and similar rooms at ten air changes per hour.
d) If mechanical ventilation system(s) is applied, the air changes per hour (hereafter "ACH") shall be as follows: Care and treatment areas: five (5) ACH; Procedure and airborne isolation areas: fifteen (15) ACH; & Operating rooms: twenty (20) ACH.
e) Toilets, janitors’ closets, soiled linen and similar areas shall have six (6) air changes per hour.
f) Areas occupied by patients shall have two (2) air changes per hour.
8.6. Electrical System 8.6.1. All facilities shall provide the minimum average illumination levels as follows or
as per the Ethiopian Electrical Design Code:
224
a) General purpose areas: five (5) foot candles; b) General corridors: ten (10) foot candles; c) Personal care and dining areas: twenty (20) foot candles; d) Reading and activity areas: thirty (30) foot candles; e) Food preparation areas: forty (40) foot candles; f) Hazardous work surfaces: fifty (50) foot candles; g) Care and treatment locations: seventy (70) foot candles; h) Examination task lighting: one hundred (100) foot candles; i) Procedure task lighting: two hundred (200) foot candles; j) Surgery task lighting: one thousand (1000) foot candles; and k) Reduced night lighting in patient rooms and corridors. l) Three hours Emergency light shall be provided in exit, entry and in all
landing of staircase.8.6.2. Essential Power System:
a) The electric installation in the specialty center shall fulfill the criteria set by ELPA,
b) The electric outlets shall be up to the safety standard of the country,c) The specialty center shall have functional generator with fuel and
assigned attendant.d) Solar panels can also be used as backup power option where appropriate..
8.7. Fire Protection System 8.7.1. The specialty center shall comply with the National Fire Protection "Life Safety
Code”.8.7.2. All employees, including part-time and contract or temporary employees shall be
trained in procedures to be followed in the event of a fire and instructed in the use of fire-fighting equipment and patient evacuation of center’s buildings as part of their initial orientation and at least annually thereafter.
8.7.3. All employees, including part-time and contract or temporary employees shall receive printed instructions on procedures to be followed in case of emergency, including patient evacuation of the buildings.
8.7.4. A written evacuation diagram specific to the unit that includes evacuation procedure, location of fire exits, alarm boxes, and fire extinguishers shall be posted conspicuously on a wall in each patient care unit.
8.7.5. Fire extinguishers shall be visually inspected at least monthly; fully inspected at least annually, recharged, repaired and hydro-tested as required by manufacturer's instructions; and labeled with the date of the last inspection.
225
8.8. Call Systems8.8.1. Call systems shall be operable from all patient private spaces. Such us from
patient beds, procedure and operating rooms, and recovery bed, bathing and toilet locations.
8.8.2. In locations where patients are unable to activate the call, a dedicated staff assists or code call device shall promptly summon other staff for assistance or continuous visual connection to supper attending staff should be provided.
8.9. Medical Gas System8.9.1. The specialty center shall maintain the safety of medical gas and vacuum if
provided centrally installed system or by means of portable equipment.8.9.2. The installation, testing, and certification of nonflammable medical gas, clinical
vacuum, and air systems shall comply with the requirements of the Life Safety Code (National Fire Protection agency proclamation).
8.9.3. The specialty center shall identify portable and system components, and periodically test and approve all medical gas piping, alarms, valves, and equipment for patient care and treatment. The specialty centers shall document such approvals for review and reference.
8.10. Health Facility Environment
8.10.1. The specialty center shall provide and maintain a safe environment for patients and the public.
8.10.2. Existing and new facilities shall comply with the physical facility standards contained in this chapter.
8.11. Specific Service Areas8.11.1. Bathing and Toilet Rooms:
a) The specialty center shall provide a bathing room consisting of a tub and/or shower adjacent to each bedroom or provide a central bathing room around inpatient rooms. Tubs and showers regardless of location shall be equipped with hand grips or other assistive devices as needed or desired by the bathing patient.
b) In case of common bathing and toilet room, one toilet and bath shall be dedicated for a maximum of six patients at all times.
c) The specialty center shall provide toilet rooms with hand-washing sinks for patient and staffs separately in each service units. In addition the following requirements shall be ensured. Flush toilets shall be available throughout the workplace.
226
Posted signs (written and/or visual messages) shall be indicated describing which is for ladies and gents.
Indicating arrows shall be located on the corridors. At least one toilet room shall be designated for patients with
disability with all assisted services. At least one sitting toilet shall be available for seriously ill patients
8.11.2. Patient Rooms: the specialty center patient rooms shall:a) allow the provision of medical intervention,b) space for sleeping, c) afford privacy, d) provide access to furniture and belongings, and e) Accommodate inpatient care and treatment. f) Patient rooms shall be arranged to maximize staff supervision and nursing
assistances.g) No patient room shall be located away from nursing stations without proper
covered gangway.h) Patient rooms shall be provided with a window with minimum size of 8
square feet or 0.743 sq. m per patient on the outside wall of the rooms.i) If there are multiple beds in a room, there shall be 1.2m gap between beds,
8.11.3. Isolation Rooms: a) The isolation room shall have adjoining bath and toilet room, b) Shall be equipped with hand-washing and gown changing facilities at the
entrance of the room.c) Air circulation and traffic shall be arranged to be not into the corridor,
8.11.4. Observation Areas: If the specialty center provides medical observation or behavior intervention methods, there shall be one appropriately equipped room for patients needing close supervision. Each room shall:
a) Have appropriate temperature control, ventilation and lighting; b) Avoid unsafe wall or ceiling fixtures and sharp edges; c) Have a way to observe the patient,d) Minimize the potential of the patient's escape, injury, suicide or hiding of
restricted substances. e) Be provided with proper safety communication systems and emergency
signaling.8.11.5. Cubicles: Patient care and treatment cubicles shall have a minimum floor area of
7.2 square meters (2.4m x 3m) with at least 90 cm between bedsides and adjacent side walls.
8.11.6. Examination Rooms: Each examination room shall have a minimum floor area of 24 square meters (4.5m x 5m) and a minimum of 90 cm clear dimension around three sides of the examination table or chair.
227
8.11.7. Treatment Rooms: Treatment room for procedures performed under topical, local, or regional anesthesia without pre-operative sedation shall have a minimum floor area of 10.8 square meters (2.7m x 4m or 3m x 3.6m) and a minimum of 3 meter clear dimension.
8.11.8. Procedure Rooms: Procedure rooms for invasive and minor surgical procedures performed in conjunction with oral, parenteral, or intravenous sedation or under analgesic or dissociative medicines shall have a minimum floor area of 18 square meters and a minimum of 4 meter clear dimension.
8.12. Care and Treatment Areas
8.12.1. The specialty center shall not share care and treatment areas for those services which require dedicated space,
8.12.2. The specialty center shall not provide services in detached structures unless the way of service delivery dictates or proper building configuration established.
8.13. Ancillary areas 8.13.1. Dietary: If the specialty center prepares food for its inpatient services by its own,
it shall dedicate space and equipment for the preparation of meals and separate washing room (dishes and other food preparation equipments), refrigerated and non-refrigerated storage areas in accordance with the standards mentioned under the Food and dietary services of this health facility. If the center prefers contractual services for its dietary services, it shall have areas for immediate storage spaces, cleaning and disposal spaces and responsible to make sure that the contractor is delivering food according to the standard stipulated for food and dietary services.
8.13.2. Laundry: The specialty center shall provide laundry service. a) On-site: If on-site services are provided, the specialty centers shall
have areas dedicated to laundry in accordance with the following requirements: The laundry areas shall have designated area for sorting, sink/
wash tubs, rinsing, drying and ironing. Supplied with equipments: washer and dryer (Optional), The laundry area shall be divided into separate soiled (sort and
wash areas) and clean (drying, folding, and mending areas) rooms.
A separate soaking and hand-washing sinks and housekeeping room shall be provided in the laundry area.
228
Separate clean linen supply storage facilities shall be conveniently located in each care and treatment location.
8.13.3. Administrative Areas: Administrative Offices shall be located separately from care and treatment areas and shall be clearly labeled. It includes;
a) Administration office.b) Finance and business office c) Staff room(s) with toilet separate for male and femaled) Staff cafeteria (optional)e) Visitors cafeteria (Optional)
8.13.4. General Storage areas. There shall be a two hour fire rated lockable room large enough to store.
8.13.5. Maintenance Area: Sufficient area for performing routine maintenance activities shall be provided and shall include office for maintenance engineer.
8.13.6. Incinerator: The specialty center shall have functional incinerator with dedicated ash pit. The incinerator area shall be secured with fence and gate.
8.13.7. Janitor rooms: The specialty center shall have a separate room/ cubicle for janitors in Outpatient and inpatient areas.
8.13.8. Green area: The specialty center shall dedicate at least 10% of the total compound for green area.