european collaboration on dementia (eurocode)...
TRANSCRIPT

1
European Collaboration on Dementia (EuroCoDe) Technical Report (2006-2008)

Page 2 of 88
1 WP 1 – COORDINATION ........................................................................................................ 3 1.1 Aims ............................................................................................................................ 3 1.2 Results ........................................................................................................................ 3 1.3 Deliverables................................................................................................................. 3
2 WP 2 – DISSEMINATION........................................................................................................ 4 2.1 Aims ............................................................................................................................ 4 2.2 Results ........................................................................................................................ 4 2.3 Deliverables................................................................................................................. 5
3 WP 3 – EVALUATION ............................................................................................................ 6 3.1 Aims ............................................................................................................................ 6 3.2 Results ........................................................................................................................ 6 3.3 Deliverables................................................................................................................. 6
4 WP 4 - SOCIAL SUPPORT SYSTEMS ...................................................................................... 7 4.1 Introduction.................................................................................................................. 7 4.2 Methodology................................................................................................................ 7 4.3 The results/deliverables .............................................................................................. 8
5 WP5 - DIAGNOSIS AND TREATMENT....................................................................................... 9 5.1 Aims ............................................................................................................................ 9 5.2 Method ........................................................................................................................ 9 5.3 Recommendation ...................................................................................................... 14 5.4 Deliverables............................................................................................................... 15
6 WP 6 – PSYCHO-SOCIAL INTERVENTIONS ............................................................................ 16 6.1 Introduction................................................................................................................ 16 6.2 Workgroup members................................................................................................. 16 6.3 Development of guideline (progress) ........................................................................ 16 6.4 Development of quality indicators ............................................................................. 18 6.5 Deliverables............................................................................................................... 19
7 WP 7 – PREVALENCE RATES............................................................................................... 20 7.1 Aims .......................................................................................................................... 20 7.2 Workpackage Members ............................................................................................ 20 7.3 Methods..................................................................................................................... 20 7.4 Results ...................................................................................................................... 21 7.5 Deliverables............................................................................................................... 22
8 WP 8 – SOCIO-ECONOMIC IMPACT....................................................................................... 23 8.1 Introduction................................................................................................................ 23 8.2 Methods..................................................................................................................... 23 8.3 Deliverables............................................................................................................... 24
9 WP 9 - PREVENTION........................................................................................................... 25 9.1 Introduction................................................................................................................ 25 9.2 Workgroup members................................................................................................. 25 9.3 Research methodology ............................................................................................. 25 9.4 Deliverables............................................................................................................... 25
10 TECHNICAL ANNEXES ......................................................................................................... 26 10.1 Minutes of meetings organised in the framework of the project ............................... 26 10.2 Documents produced in the framework of the project .............................................. 83
Page 3 of 88
1 WP 1 – Coordination
1.1 Aims
The work package on coordination was aimed at the overall project management and the coordination of activities of the various work packages, as well as the contractual and financial administration of the project, the organisation and follow-up of meetings and the reporting to the European Commission.
Furthermore, the work package aimed at developing internal rules for conflict resolution, risk management and financial reporting.
The work package was also dedicated to the identification of third parties for consultation and endorsement of the guidelines and recommendations developed in the framework of the project.
1.2 Results
In the framework of the project, a number of activities were carried under Work Package 1 – Coordination.
Financial regulations were developed and approved by the working group members.
An inventory of organisations with an interest in dementia was done and included in the first edition of the Dementia in Europe Yearbook.
The steering committee met twice in the framework of the Alzheimer Europe conferences in Paris and in Estoril (8 May 2007) and the different work package leaders provided an update on the progress of their respective work packages
This work package was also tasked with the development of internal rules on conflict resolution. The only two issues that were identified by the steering committee were the acknowledgement of authorship of publications resulting from the project, as well as the redistribution of funds resulting from an underspent and overspent of different centres. Solutions for both these problems were proposed to the steering committee and accepted at the meeting of 8 May 2007.
Initially it was also envisaged to develop an Internet-based database for the inclusion of all the collected addresses of interested organisations and to adapt the AE Intranet to allow for a better exchange of information between project partners. After careful discussion with the project partners though, it was decided not to proceed further with these projects, but to rely on the usual communication tools for the exchange of information and the setting up of mailing lists.
At the same time, the project partners (and in particular the University of Oxford) identified the development of a database for the comparison of collected guidelines as a key objective. This development was done in collaboration with Visual Online, the company in charge of the Alzheimer Europe website and Intranet. The Internet based database allows different project partners to include data on the guidelines they have collected and will allow visitors to the Alzheimer Europe websites to compare the collected information.
1.3 Deliverables
The following deliverables were developed in the framework of Work Package 1 – Coordination:
• Financial Regulations
• Internal rules on publications
• Database tool for comparison of collected guidelines
• Interim reports to the European Commission
Page 4 of 88
2 WP 2 – Dissemination
2.1 Aims
The aim of the work package was to disseminate the results of the project to as wide an audience as possible. This should have been done through a public web site, as well as the annual conferences organised by Alzheimer Europe.
The work package also aimed at producing yearbooks with information on the contact details of the participating organisations, as well as the findings of the various work packages.
2.2 Results
2.2.1 Dissemination at meetings and conferences
The members of Alzheimer Europe were updated on the progress of the Eurocode project at the Alzheimer Europe Annual Conferences in Paris (June 2007), in Estoril (May 2007) and in Oslo (may 2008). During its Annual Conference in Brussels (May 2009), the organisation dedicated a symposium to the presentation of the Eurocode results in which all work package leaders presented the final findings of their respective work packages. The Annual Conferences of Alzheimer Europe were attended by between 300 and 600 delegates from different European counties.
Alzheimer Europe also organised a series of meetings with members of the European Alzheimer’s Alliance which is composed of Members of the European Parliament with a specific interest in dementia. Every year, the yearbooks resulting from the project were launched at presented at a meeting organised in the European Parliament.
The French Presidency conference “The fight against Alzheimer’s disease” organised in September 2008 was another opportunity for Alzheimer Europe to present the findings of the Eurocode project to an interested audience comprised of policy makers and dementia experts from all European Union Member States.
2.2.2 Dementia in Europe Yearbooks
A Dementia in Europe Yearbook was produced every year with highlights of different aspects of the project.
The 2006 Yearbook contained information on the prevalence of dementia in Europe (and calculations based on the Eurodem figures), a comparison of the availiability and reimbursement of anti-dementia drugs in Europe and a presentation and contact details of the different networks involved in EuroCoDe, as well as their national member organisations.
The 2007 Yearbook provided an overview of the social support systems in different European countries.
The 2008 Yearbook presented the results of four of the thematic work packages of the project, including:
• Recommendations and examples of good practice in the provision of social support to people with dementia and carers,
• A report on the socio-economic impact of dementia,
• A report on European guidelines on psychosocial interventions,
• A report on risk factors and prevention.
For the different yearbooks, Alzheimer Europe was able to obtain forewords to from various representatives of different European instititions, including Commissioners Markos Kyprianou, Vladimir Spidla and Androulla Vassiliou.

Page 5 of 88
2.2.3 Website
General information on the project aims and partners was included on the general website of Alzheimer Europe (www.alzheimer-europe.org). The project results were similarly included on the general website or on the AE website dedicated to public affairs in dementia (www.dementia-in-europe.eu).
Currently, Alzheimer Europe is in the process of completely reviewing its websites and integrating them into one.website in order to allow easier access to all information of the organisation and in particular the different results of the Eurocode project.
2.2.4 Other dissemination activities
Information on the Eurocode project was regularly included in the e-mail newsletter and the “Dementia in Europe” magazine produced by Alzheimer Europe.
Also, project partners presented aspects of their findings at different conferences.
Finally, the project leaders are working on submitting the project results to various scientific journals.
2.3 Deliverables
The following deliverables were developed in the framework of Work Package 2 – Dissemination:
• Presentation of project findings on AE websites: www.alzheimer-europe.org and www.dementia-in-europe.eu
• Dementia in Europe Yearbooks.
Page 6 of 88
3 WP 3 – Evaluation
3.1 Aims
The aim of the work package was to organise an evaluation of the project results by the Steering Committee and the network partners and their member organisations and centres. Also, an external evaluation of the action was to be carried out by three external experts who are independent of the various project partners.
3.2 Results
The progress and findings of the project were presented to the steering committee which met twice in the framework of the project. The steering committee supported and welcomed the findings of the project partners.
Also, the different meetings were organised in such a way that the different work package participants met together both before and after their breakout sessions which allowed for a continued involvement of all project partners in the determination of the work methodologies and analysis of research findings. This way of proceeding allowed for a participation in the different work packages of a wider group of experts than the sole members of the respective work packages.
Unfortunately, due to the delay of the different work packages and the finalisation of some of the final work package reports in 2009, it was impossible to organise the evaluation of external evaluators as initially planned.
3.3 Deliverables
Work package 3 – Evaluation did not result in any specific deliverables.

Page 7 of 88
4 WP 4 - Social Support Systems
4.1 Introduction
The overall aim of Work Package 4 was to determine the level of state support for people with dementia and their carers in each member state of the European Union (and additionally in Iceland, Turkey, Norway and Switzerland) and on the basis of the findings to draft recommendations for policy makers and provide examples of good practice. This was to be achieved my means of a working group comprised of representatives of national Alzheimer associations, all Alzheimer Europe’s member associations and external experts where necessary.
4.2 Methodology
4.2.1 The working group
The members of the working group were as follows:
• Dianne Gove Work package leader (Alzheimer Europe)
• Sirkkaliisa Heimonen Ikainst Institut (Finland)
• Hans-Jürgen Freter Deutsche Alzheimer Gesellschaft (Germany)
• Eugen Stefanut Romanian Alzheimer Association (Romania) to 11/2006
• Federico Palmermiti Fondation Alzheimer Médéric (France)
• Letitia Dobranici Romanian Alzheimer Association (Romania) from 11/2006
• Louise McCabe University of Stirling (United Kingdom)
• Maria do Rosario Zincke dos Reis APFADA (Portugal)
The following members of Alzheimer Europe also attended one or more of the project meetings:
• Sabine Henry Ligue Alzheimer (Belgium)
• Alicja Sadowka Polish Alzheimer Society (Poland)
• Julie Fraser Alzheimer Europe
Six working group meetings were held in the course of the project:
• 25-26 February 2006, Luxembourg
• 6 November 2006, Brussels
• 26 February 2007, Brussels
• 12 November 2007, Brussels
• 1 April 2008, Brussels
• 15 June 2008, Berlin
4.2.2 The survey
The survey was drafted by the members of the working group and sent out to all Alzheimer Europe’s member associations. The survey was divided into 3 sections and covered the following issues:
• Section 1: Brief background information on each country, how social support fits into the overall healthcare system, how it is organised and financed, the legislative framework surrounding the provision of social support, possible barriers to the provision or use of social support (e.g. based on age, disability, place of residence or type of disease etc.) and adequacy
Page 8 of 88
and suitability of available social support available for the specific needs of people with dementia and their carers.
• Part 2: Details about the availability of specific forms of support (i.e. specific services and benefits, who pays for it and whether there are alternative sources of support, other than from the State (e.g. from voluntary associations, religious groups and NGOs).
• Part 3: Information on the availability and reimbursement conditions for dementia drugs.
Completed questionnaires were received from 23 of Alzheimer Europe’s member associations and 5 external experts (for France, Italy, Latvia, Lithuania and Luxembourg). It was not possible to obtain responses from Turkey, Slovakia, Slovenia and Cyprus.
Members of the working group were each responsible for the follow-up of several countries. They checked the responses, asked for clarification and further information if and when necessary, translated responses in some cases, helped with the drafting of national summaries and presented the findings of the countries they were covering to the working group for discussion.
4.3 The results/deliverables
4.3.1 The national summaries and comparative report
The national summaries formed the results were presented in the form of a comparative report. The information contained in the comparative report is that which was available to the experts at the time that they completed the questionnaire (and during subsequent discussions with members of the working group). Alzheimer associations have different levels of resources and the organisation of social support is better organised in some countries than in others. For a few countries, additional information was also obtained from other sources such as publications and ministries. This report is therefore a snapshot of the situation at a particular moment in time.
The national summaries were included in the 2007 edition of the Dementia in Europe Yearbook
4.3.2 The recommendations and examples of good practice
The final version of the recommendations and examples of good practice were based on the joint work of the working group, through discussions, exchange of comments to various drafts. The section of the recommendations on the general framework for care and support (which reflected the rehabilitative approach) was mainly based on the work of Sirkkaliisa Heimonen from the Ikainst Institut, Finland and supported by an original article “Pirttilä T, Heimonen S, Granö S. (2007). The essential role of rehabilitation in dementia care. Gerontologia 21(4):320-328” (translated from Finnish).
The final report also covered ethical, legal and financial issues, suitability, accessibility and barriers to obtaining support, as well as recommendations on specific forms of support such as outpatient services, self-help, semi-residential and respite care, residential care and palliative care. These recommendations were summarized in 44 recommendations for readers who need a summary of the main points. The full reports puts these recommendations into the context of the overall framework of care and other contributing factors.
The recommendations and examples of good practice were included in the 2008 edition of the Dementia in Europe Yearbook.

Page 9 of 88
5 WP5 - Diagnosis and treatment
5.1 Aims
The aim of the EUROCODE project is to raise the profile of dementia within the EU Commission. This is being achieved through a series of EU Commission-funded syntheses of evidence and opinion. The project consists of five work packages to produce guidelines on drug treatment and diagnosis, psychosocial interventions, economics, epidemiology and prevention. This document is the output of the first of these. Recently, the Commission has agreed to develop an Alzheimer’s Action Plan. The results of EUROCODE have the potential to inform this Plan.
There is great variation in clinical practice and policy relating to dementia across Europe. This variation can leave policy makers unsure as to which clinical practices to fund and encourage. Numerous guidelines for the diagnosis and treatment of dementia have already been produced. Some of these documents include exhaustive analyses of the research literature. National guidelines frequently differ in the nuances of recommendations and occasionally, guidelines directly contradict each other.
The specific brief of this project was therefore to use existing guidelines as a basis for the development of a ‘meta-guideline’ on treatment and diagnosis of dementia, suitable for use across Europe. This is consistent with the increasing recognition that adaptation of existing guidelines can sometimes be more appropriate than re-creation of guidelines de novo.
5.2 Method
5.2.1 The WP5 working group
This work package was hosted by the Cochrane Dementia and Cognitive Improvement Group, based in Oxford UK and led by its Coordinating Editor Dr Rupert McShane, who is an old age psychiatrist.
The other 5 members of the work package were Sigurd Sparr (Norway, Alzheimer’s Europe, Geriatrician), Mario Fioravanti (Italy, experience with International Psychogeriatric Association, Psychology), Peter Tariska (Hungary, dementia specialist), Philip Scheltens (Netherlands, neurologist, neuroimaging researcher), Brigitte Grass-Kapanke (Germany, psychologist)
During the course of the project, the group’s administrator Dymphna Hermanns moved on, and was replaced by Helen Collins. Amanda Kerr was appointed on the EUROCODE grant for 16 months, starting in April 2007. She remained working on the project for a further 4 months supported by Cochrane funds.
5.2.2 Guideline identification
The starting point was to attempt a comprehensive collation of existing guidelines. This was not as simple as it might appear. First, the time frame of this project has coincided with a proliferation of new guideline creating organisations and also the maturing of some better established organisations. Second, the high level of interest in dementia as a public health problem in member states has meant that, during the timeframe of this project, there has been a continuing stream of new guidelines emerging. Third, guidelines which are the product of governmental departments are not usually published in conventional medical literature. They are therefore not accessible to the usual search techniques used by organisations which specialise in systematic reviewing of primary literature such as Cochrane.
Our cut-off point for identifying the existing guidelines which we would formally consider in developing our own was 1st quarter 2008. However, as we have become aware of new guidelines since then, we have read those too. There were no instances however, where a recommendation in the draft was altered as a result of the newer guideline since those which were identified after that point did not either add important new weight to existing controversies, or introduce new material which had not already been identified through review of the primary and secondary literature as worthy of inclusion in our guideline.

Page 10 of 88
Guidelines were ‘includable’ if they covered aspects of the drug treatment or diagnosis of dementia. We decided to limit the guideline to common neurodegenerative dementias, thus excluding dementia associated with alcohol, HIV or Huntington’s.
Guidelines were includable if they originated from a European state after 1995. Older guidelines were ignored if superseded by more recent versions. The guidelines had to be produced by government agencies, professional associations, or the voluntary sector. We did not include guidelines with a sub-national or regional remit. Recent guidelines from outside Europe were also included on the grounds that these may contribute usefully, particularly when they addressed newer findings and controversies. We restricted consideration of non-European guidelines to those in English. We also considered new literature published since 2005 which addressed emerging clinical issues or provided important new evidence to guide treatment or diagnosis but had not yet been incorporated into any existing guidelines. We excluded consideration of cognitive enhancers (which are invariably short lived ‘boosters’ of attention) or analysis of drugs with potential utility for primary prevention because prevention of dementia is the subject of another work package. However, secondary prevention of progression from minimal cognitive impairment to dementia was in scope.
We decided to ignore the differences in GDP of the countries for whom the guideline was intended not least because variations are often as great within member states as they are between them. Thus the strength of recommendations should apply across the board. However, a guiding principle as to what was includable was that treatments or diagnostic techniques should be feasible for use in routine practice not just in tertiary research centres of excellence.
5.2.3 Guideline Development
5.2.3.1 Methodological developments in guideline development
The period of this work has coincided not only with the release of many new guidelines, but also with significant developments in the technology of guideline creation. The governmental organisations which develop guidelines necessarily, as part of their mission, elaborate standard procedures for developing guidelines. Inevitably, this has meant that guidelines are produced in different forms. It is a recognised problem that there is no consensus on the way in which evidence should be graded. Similarly, there is no consensus on a grading system which should be used to describe the strength given to recommendations. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach started to be developed in 2000 but only really started to gain significant traction 2005, the year before our project began. As a method, however, it depends on assessing primary evidence, and this was clearly beyond the scope of our project.
5.2.3.2 The Adapte Framework
A very relevant framework for our project was launched too late for us to make formal use of its provisions. The Adapte Collaboration developed from two organisations, one French (Adapte) and one Canadian (Practice Guideline Evaluation and Adaptation Cycle PGEAC). The framework is a systematic approach to aid in the adaptation of guidelines produced in one setting to be used in a different cultural and/or organizational context. It is based on the following core principles:
• Respect of evidence-based principles for guideline development; • Reliable and consistent methods to ensure the quality of the adapted guideline; • Participation of key stakeholders to foster acceptance and ownership of the adapted guideline; • Explicit consideration of context to ensure relevance for local practice and policies; • Transparent reporting to promote confidence in the recommendations of the adapted guideline; • Flexible format to accommodate specific needs and circumstances; • Respect for and acknowledgement of source guidelines material.
Its founder members were oncologists and clinicians interested in the treatment of leg ulcers. The large majority of members are still from these countries and disciplines with some input from the Netherlands. The manual for guideline adaptation and evaluation study were launched in April 2007.
Potential advantages of ADAPTE
This would potentially have delivered a greater form of transparency to our decision making. It would also have had the benefit of giving a formal label to the process we used. In turn, this may have made a small difference to the credibility of the guideline.
Potential disadvantages of ADAPTE

Page 11 of 88
Transparency of approach is core to the mission of Cochrane. It is relatively easy to deliver in the context of meta-analysis of primary evidence. Most of the steps in the ADAPTE framework have a rather clear way of ensuring that what has been done is open to scrutiny. However, there are is a crucial point in the framework where the basis for decisions requires judgement. This is at the point of detailed consideration of adaptation of recommendations. Whilst the toolkit suggests that justifications of any modification to the recommendations of the preferred existing guidelines are written down, it is far from certain that this commendable emphasis on documentation as part of transparency would actually make any difference to accountability. Ultimately, such modifications are a matter of judgement. What really matters is the extent to which they are either evidence based or, as is more usually the case in the absence of adequate evidence, they reflect the experience of the majority.
The ADAPTE method involves selecting no more than a few existing guidelines to ‘ADAPTE’. This would have been problematic. It would not have been constructive to select just one or two existing guidelines for adaptation because it would have led to the potential rejection of our work on the basis that it was not fully representative
Three of the 6 criteria for assessing the acceptability and applicability of recommendations were not fit for our purpose because of the large number of countries for which our guideline was intended
• The recommendation is compatible with the culture and values in the setting where it is to be used.
• There are no constraints, legislation, policies, or resources in the health care setting of use that would impede the implementation of the recommendation
• The intervention/equipment is available in the context of use
The methodology of the ‘consensus generating’ part of guideline development is not addressed in any detail. Whilst the ADAPTE framework is specifically designed for settings in which resources are limited, most consensus generating methods require substantial resources.
The Adapte framework is relatively new. Although it has excellent face validity, it has not yet been formally evaluated. Indeed, as mentioned above, the manual and toolkit were only launched in April 2007. We did not in fact became aware of its existence until 3rd quarter of 2008 which was too late for us to formally adopt and complete the manualised process.
5.2.3.3 Method used to develop EUROCODE guideline
This account and critique of ADAPTE is given because it helps to illustrate the arguments which led us to the rather simple, lean method we used to generate our draft guideline. This can be summarised as follows:
1. Identify guidelines published before 1st quarter 2008. 2. Translate relevant sections 3. Cut and paste the text of each guideline’s recommendation about a particular issue into a table 4. Load guideline into new guideline comparison website: http://guidelines.dementia-in-europe.eu/ 5. Researcher drafts provisional distillation of source recommendations 6. WP leader drafts complete new guideline which seems to best encapsulate the texts drawn
from all the parent guidelines. Make judgements to resolve differences between source guidelines on the basis of:
a. Quality of source guidelines b. Quality of evidence c. New evidence since guideline was developed d. Clinical judgement
7. Assign a rating of the ‘degree of clinical confidence’ in the draft recommendation, based on a judgement which combines
a. Strength of evidence as ascertained in parent guidelines b. Strength of recommendations in parent guidelines c. Unanimity of recommendations between parent guidelines
8. Working Group ratify draft guideline
A critique of our method, and recommendations on whether and how to generate consensus on the document are made below.
5.2.3.4 Discussion of Method
Going beyond the evidence
Page 12 of 88
The field of dementia research is, compared to some, relatively young. The number of records of randomised controlled trials in dementia which is held on the Cochrane Collaborations ‘Central’ database is smaller than many other clinical areas. The quality of these trials is routinely criticised. However, we are where we are. Rather than simply overlook areas of clinical practice because there is no evidence to inform it, the Working Group took the view that it would be better to fill in some of the gaps that exist in other dementia guidelines. This requires a degree of clinical judgement. An example of this is the approach to the drug treatment of behavioural and psychological symptoms of dementia. Clinicians require an algorithm which goes beyond first line treatment, and which, for example, differentiates between different types of agitation. There is no attempt in any existing guideline to present this in a comprehensive fashion, but we used our clinical experience to interpret the nuances of differences between guidelines to create an algorithm for first line, second line, third line… seventh line treatments. In this way, differing recommendations from source guidelines were combined in a way which seemed to us to make clinical sense. Although the justification for this would lie in whether application of this algorithm results in a better outcome than ‘care as usual’, it is rather unlikely that a clinical trial to assess this would be feasible, not least because, for many, the algorithm will be close to ‘care as usual’.
Different ratings in source documents
Some of the guidelines we identified arose from exhaustive reviews of the evidence. The differing systems for rating of the evidence means that selecting the wording of recommendations from more than one guideline would have meant selecting recommendations with differing rating systems. The large number of permutations meant that trying to document a transparent way of ‘mapping’ every one of these onto a preferred rating scale would have been a drain on resources that would not ultimately have improved the quality of our guideline, and would have been of limited validity. We decided to use the approach adopted in the American Psychiatric Association guideline because, of all the various systems which are outlined in the appendix, its simplicity best reflects what clinicians usually need from a guideline:
[I] Recommended with substantial clinical confidence
[II] Recommended with moderate clinical confidence
[III] May be recommended on the basis of individual circumstances
Guideline validation
As stated above, we did not pursue the final step in ‘validating’ the guideline. Here, we discuss the pros and cons of doing this, the various possible methods and make recommendations.
Our experience in identifying the large number of existing guidelines led us to carefully consider the merits of generating another fully validated one.
The tests of whether a further guideline would add value should be, in comparison with existing guidelines relate to process and to content:
Would this new guideline be more likely to change practice?
Would this new guideline be referred to more?
Would this new guideline be acted on more?
Are the recommendations more likely to improve outcomes?
Great effort and expense would be required to gather the evidence to answer these questions with any confidence.
Although the credibility of the source and familiarity with the guidelines do not ensure compliance, adherence to guidelines is higher when the recommendations are supported by evidence from randomized clinical trials. Guideline recommendations can lag behind appropriate changes in clinical practice because, by and large, secondary care clinicians stay up to date with the important primary evidence (1)
Therefore, an important role of guidelines is to educate trainees and non-specialists, and to consolidate clinician’s practice around the margins, rather than to change it fundamentally. Given this ‘consolidating’ effect, it is clearly important that harmful recommendations do not find their way into guidelines.
A further implication is that more frequent revisions have the potential to make guidelines more useful(1).
Page 13 of 88
The presence of a controversial recommendation in a guideline can be a useful spur to research which ultimately takes the field forward. This is particularly justifiable if the recommendation reflects common practice. The appropriate degree of confidence should be ascribed to such recommendation. It may therefore be better for the guideline to be rich in recommendations with low degree of clinical confidence, rather than to leave areas of common practice without comment.
This is the line we took.
Guidelines therefore have two competing priorities
1. Do not make recommendations which consolidate harmful practice 2. Include recommendations with a low (albeit specified) degree of confidence
The only way of resolving these lies in a validation process which depends BOTH on an understanding of the evidence and also experience.
There are two conventional approaches to securing guideline ‘validation’. The first is to send it out to preselected experts for comment. The second is to have a ‘consensus conference’ to which a large number (say 20-200) people meet together for a day or two to consider the text. Typically, the first approach is used more by government agencies where the draft was generated by experts in Evidence Based Medicine but not the subject, and the second approach is used by professional organisations who are expert in the subject – and may also be experienced in Evidenced Based Medicine.
Sending a guideline out to experts for comment is perhaps more appropriate for updates. However, no individual can be familiar with the details of literature across the whole field. Experts will therefore concentrate on their particular area of expertise.
The Consensus meeting has the advantages that face-to-face dialogue can resolve differences. To be effective, a consensus conference needs a large number of experts and clinicians. This requires long lead times, needs to be led by ‘names’, and to have the backing of influential organisations. It is expensive because it involves people flying in from across Europe usually staying overnight. The efficiency of this process is questionable, especially when existing guidelines form the starting point, as in EUROCODE, or when the purpose is to update a guideline. Furthermore, such conferences may also not always be representative of the end-users. Experts who are present at such conferences are likely to know the literature better than non-academics. In areas where there is no evidence, the anecdotal clinical experiences of non-academics may carry less weight than those of academics. The views of the writing committee carry considerable weight.
5.2.3.5 Web-based consensus generation: the route for EUROCODE WP5 validation?
Several factors led to the idea that the business of a ‘Consensus meeting’ could potentially be conducted more efficiently, and more transparently, through a web-based system. First, neither existing method of validation is entirely satisfactory from the point of transparency. In consensus meetings, those who are confident in their knowledge of the evidence may hold more sway than those who are more accurate in their understanding of it. There may be little time for those who are unsure about a new proposal to review evidence. Participants may feel under pressure to sign up even if there are elements with which they disagree. It was recognised that pressures from home institutions and economies of time mean that face to face meetings are increasingly less attractive and difficult to organise. The green imperative to minimise unnecessary flights was also recognised. In any event, we were not funded to host a consensus conference. However, we also felt uncomfortable with sending the document out to just a few experts.
Although tele- and web-based conferencing has, during the time frame of this project, become a more widely accepted feature of working life, it is not suitable for larger scale collaborations.
We were further emboldened to consider attempting a web-based system by reports of web-based Delphi consensus generation(2-6) which started to be published during the life time of this project.
5.2.3.6 Pilot study
We therefore undertook to develop a pilot of an innovative process which would enable a large number of participants to vote and comment on each of the draft recommendations.
The process was defined as follows. First, a panel of clinicians is invited. Panellists are encouraged to contact colleagues whom they think might be interested in participating. Because there are no physical limitations on the number of panellists, this snowballing, ‘viral’ approach could potentially get greater buy-in from a wider geographical constituency than is conventionally the case with consensus panels.

Page 14 of 88
Panellists log on to the website. The draft guideline is divided into small segments each of which has up to 20 statements / recommendations.
For each segment, the clinician can approve it in its entirety, or reject it with or without a comment. The clinician can also agree or disagree with the rating (I, II, III as above) for the statement.
The comments made are then incorporated into a second draft, which is generated offline. Whilst the proposed method would be likely to generate a large number of comments, the fact that one would already have an idea of the extent to which a recommendation was acceptable in its current form would actually make it easier to decide how far to revise the text on the basis of such comments. This also provides a transparent mechanism for getting consensus on the issue of the ‘degree of clinical confidence’ that should be attached to a recommendation.
The clinicians would then be contacted again and invited to comment on the changes and to vote on changed recommendations.
Following this a third draft would be prepared. The clinicians would once again contacted and asked whether they were prepared to put their name to the document.
Throughout, panellists can additionally engage in discussion with each other through a web-based forum.
An innovative aspect of this, compared to the few other web-based Delphi guideline consensus generation processes is that the system is structured so that clinicians can access all the ‘parent’ guidelines and other quoted sources of evidence which lie behind each statement. These sources of evidence could include ‘summary of findings’ tables, such as has recently been adopted in Cochrane reviews.
Advantages of web-based consensus approach
‘Evidence is international, but guidelines are local’ (Andy Oxman, Cochrane guideline guru). This observation points to a potentially fundamental barrier to the EuroCoDe guideline gaining currency. However, as public finances become increasingly constrained, the capacity of Health Technology Assessment agencies, and professional assoications of different countries to update local guidelines may be reduced. A web-based system, if it demonstrated good ‘buy-in’ from large number of clinicians from each member state, might increase the appeal of EuroCoDe in individual member states.
The ‘viral’ approach to gathering consensus participants has the advantage that a large sample of clinicians can be rapidly built. Although it is possible that interest groups supporting a particular agenda may develop, this would be readily identified.
The linkage of each statement to the underlying primary evidence would result in an invaluable educational tool. Taken to its logical conclusion, it could become the structure for a ‘tree of knowledge’ for our speciality.
By de facto incorporation of many of the principles of the ADAPTE methodology, it has the potential for more rapid, transparent and efficient updating. In an era of rapidly advancing knowledge, it may therefore improve the currency of the guideline. This is likely to increase its utility, buy-in and impact.
We recognise that the structure we developed was not specific to dementia. Indeed, if this was successful, it could be applied as a methodology for gathering consensus on any guideline.
5.2.3.7 State of pilot at end of project
As far as we have been able to ascertain, this had not been attempted before. Its outcome was therefore uncertain. We therefore took the view that the Cochrane Dementia Group should contribute support for this pilot as a way of developing experience in web-based consensus development.
The software for the project has reached an advanced state of preparation and can be viewed at http://www.eurocodeconsensuspanelwp5.org/. It has yet to be populated with the full draft guideline and we have not run the proposed process. We have done much of the work in developing the structure of the site and work-flows but the final Proof of Concept work has not been completed.
5.3 Recommendation
We judged that the web-based consensus-development tool we developed, or something similar, has the potential to form the basis of a larger, more formal project. Such a project would
Page 15 of 88
• establish consensus on the EuroCoDe guideline • establish a structure for updating the guideline • establish a peerless structure for linking evidence to a guideline • establish a structure which could be a model for other disciplines
This larger, successor project would need to formally involve people with the wider expertise and experience, including
• Guideline development – preferably to include people from outside the field of dementia • Web-based Delphi consensus generation • Business analysis • Project management • Software development • Clinical expertise • Evidence based medicine
Clinical practice guidelines are being used in many countries throughout the world to improve quality of patient care. There is a need for a common, valid and transparent approach to develop good clinical practice guidelines. The project aims to identify diagnostic instruments and guidelines for treatments for dementia used in countries within the EU in order to develop truly European and multi-disciplinary guidelines. Existing guidelines will be compared with the comparative reports on treatment and diagnosis and used to develop possible consensus guidelines.
5.4 Deliverables
The European guideline on “Diagnosis and drug treatment of dementia” is included as a separate report to the present document.
Page 16 of 88
6 WP 6 – Psycho-social interventions
6.1 Introduction
While pharmacological treatments undergo strict double-blind placebo-controlled studies, the same is very often not the case for the various non-pharmacological or psychosocial interventions used with people with dementia and their carers. Therefore, the aim of this project is to identify the available controlled studies on psychosocial interventions and consensus recommendations in order to develop European guidelines for the use of psychosocial interventions in dementia care. The building blocks of the guidelines are: a) a review of reviews on the effects of psychosocial interventions and b) an inventory on recommendations for psychosocial interventions included in dementia guidelines across Europe.
Based on these results a consensus guideline on the use of psychosocial interventions in dementia will be developed. The development and evaluation of a set of quality indicators for psychosocial interventions in dementia will be the final aim of the project.
6.2 Workgroup members
Workgroup members are involved in the Interdem (Early detection and timely intervention in dementia) network. A multi–professional network of gerontological research-practitioners who focus on psychosocial approaches to the early recognition and intervention in dementia, throughout Europe. Workgroup members are:
• Professor Myrra Vernooij-Dassen, Medical Sociologist, Director Alzheimer Centre Radboud University Medical Centre Nijmegen, The Netherlands (work package leader)
• Professor Esme Moniz-Cook, Clinical Psychologist, Director IPCRA, University of Hull, UK
• Professor Robert Woods, Clinical Psychologist, Director, DSDC, University of Wales, Bangor, UK
• Dr Manuel Angel Franco, Psychiatrist Director, INTRAS, Fundacion INTRAS, Spain
• Dr Inge Cantegreil-Kallen, Psychologist, Department of Geriatrics, Broca Hospital, Paris, France
• Dr Pascale Dorenlot, Foundation Mederic Alzheimer, Paris, France
• Sandrine Lavallé, Communication officer, Alzheimer Europe, Luxembourg
6.3 Development of guideline (progress)
At the first meeting the discussion focussed on research questions related to the development of guidelines and quality indicators on psychosocial interventions.
The following specific questions were formulated and methods proposed:
1. Will the guidelines be general? • Expert discussion.
2. What will be the structure (chapters) of the guidelines? • Research on instructions on how to construct guidelines (AGREE etc.) • Inventory of structure of national guidelines
3. Who is going to use the guidelines? • Expert decision.
4. Who are going to be the recipients of the guidelines and in which setting will the guidelines be used? • Expert decision
5. What interventions will be recommended? • Review of reviews.
6. What will be the outcomes? • Review of reviews
Page 17 of 88
7. Are we going to prepare quality indicators? • Yes, iterative consensus procedure
It was agreed that the guideline should be general rather than giving specific recommendations. The guideline should be applicable to the range of psychosocial problems and interventions. This general level is new and there is no format which can be followed. There is a need for such a general guideline since systematic reviews indicated that no specific intervention is superior.
Rather than building a guideline for a specific category of professionals, this guideline is meant for use by all stakeholders. It should be potentially helpful for a specific patient. It can be used by professional and non-professional carers.
A general guideline considering this as a starting point should indicate:
a) patients´ and carers´ needs b) potential interventions c) suggestions on how to identify needs for care and to make action plans acceptable for all those
involved
Perspectives of those involved should be pulled together. The needs to be considered relate to the domains of physical, psychological, social and spiritual aspects.
6.3.1 BUILDING BLOCKS OF GUIDELINES
6.3.1.1 Review of reviews
To gather available evidence on the effect and effectiveness of psychosocial interventions a literature search was done to identify reviews on the subject.
6.3.1.1.1 Search strategy
We searched for reviews in Pubmed and the Cochrane library using the following terms:
Dementia (MESH) AND psychosocial OR non-pharmacological OR intervention; limits: review.
Reviews found by using this strategy were used as a source for new references of reviews on the subject. The articles found were presented at the workgroup members and they agreed to only select systematic reviews and reviews that were available in the Cochrane library and not written before 1999. Also, they were asked to add any missing reviews they knew of meeting the selection criteria.
6.3.1.2 Results
The above described search strategy resulted in the selection of 17 reviews (appendix 1). Because some workgroup members are currently involved in writing a Cochrane review that would meet the search criteria, preliminary results will be considered in the development of the guideline. Also,
there seemed to be a lack of reviews focussing specifically on the use of psychosocial interventions in institutional care. Therefore, a review of the literature on this subject especially aiming at the communication between patients and nursing staff is currently been carried out. Preliminary results of this review will also be used in the development of the guideline.
6.3.1.3 Inventory guidelines on psychosocial interventions across Europe
6.3.1.3.1 Search for guidelines
To start the inventory the Interdem network was used to gather information on available guidelines on psychosocial interventions in dementia across Europe. Contacts in the following countries were sent an email with a request to gather guidelines on the subject: UK, Spain, the Netherlands, Belgium, France, Germany, Ireland, Italy, Portugal, Switzerland, Greece, Poland, Sweden, Austria, Denmark, Finland.
From contacts of Greece, Poland, and Austria no information was received. The information received from the other contacts was put together in a table (appendix 2) and is discussed hereafter.

Page 18 of 88
6.4 Development of quality indicators
6.4.1 Introduction
A quality indicator is a measurable element of practice performance, for which there is evidence available or consensus that it is capable of assessing improvement in the quality, and hence change in the quality, of care provided.
The final aim of this project is not only to develop an European guideline for the use of psychosocial interventions in dementia care, but also to develop a set of potential quality indicators that can stimulate the use of available effective psychosocial interventions, and take into account cultural differences between European countries.
6.4.2 Methods
The best method to develop quality indicators is a method which is objective, not time consuming, and uses available knowledge. The potential set of quality indicators are therefore derived from evidence-based guidelines by an iterated consensus rating procedure. This procedure combines evidence with expert opinion (Campbell et al, 2002, 2003).
It starts with selecting core recommendations from evidence-based guidelines. Then, an expert panel is used to reach consensus about the most useful recommendations. Finally, the set of potential quality indicators can be constructed from these recommendations.
6.4.3 Procedure step by step
6.4.3.1 Selection of core recommendations by workgroup
Evidence-based recommendations on psychosocial interventions that were found in European guidelines on dementia during the inventory of guidelines in Europe were gathered. During a face-to-face meeting all these recommendations were discussed by the workgroup members.
6.4.3.2 Agreement on composition and selection of expert panel in each country
The workgroup decided to only compose expert panels in countries where an Interdem member could be contacted. Also, at the Alzheimer Europe conference in Estoril (Portugal, 2007) people involved in dementia care were invited to take part in the iterated consensus rating procedure. It was agreed by the workgroup members that it was important to approach at least the opinion leaders on the subject in each country involved.
An expert in dementia care was defined as someone who is involved in dementia care, like researchers, carers or, clinicians.
6.4.3.3 First postal round
To guarantee the objectivity of the procedure and avoid time consuming face-to-face panel discussions in different countries led by different people, the experts rated the core recommendations by means of a questionnaire. In this questionnaire experts were asked to rate each core recommendation twice, based on the questions:
• Would applying this recommendation to dementia care contribute to the improvement of its quality?
2. How much priority should this recommendation be given in dementia care in your country?
Experts were also permitted to add recommendations or adjust the ones presented.
6.4.3.4 Second postal round
The creation of a reliable set of indicators requires the experts completing the questionnaire to do so a second time. This second questionnaire will be based on the results of the first postal round.
The recommendations that were adjusted or added by the experts are also presented in this second questionnaire.
Page 19 of 88
6.4.3.5 Constructing the potential set of quality indicators
Results of the second postal round are discussed in a face-to-face workgroup meeting. The potential set of quality indicators will be constructed based on an agreed cut-off point for the ratings in the second round. An other important criteria for the quality indicators is the usability in everyday practice. The potential indicator must be easy to use.
6.5 Deliverables
The work package resulted in the following deliverables:
• A report on European guidelines on psychosocial interventions
• An inventory of guidelines on psychosocial interventions across Europe
• A set of 17 key recommendations
• A set of 15 potential quality indicators for psychosocial care in Europe
All these documents were published in the 2008 edition of the Dementia in Europe Yearbook.
Page 20 of 88
7 WP 7 – Prevalence rates
7.1 Aims
The project aimed at gathering existing epidemiological studies and analysing the respective merits and shortcomings of the individual studies. Based on the report on these studies, consensual European prevalence rates were developed that will be acceptable to all partners and used as a “golden standard” within the respective organisations.
7.2 Workpackage Members
E Reynish Toulouse/ Edinburgh Toulouse University Hospital
L Fratiglioni Stockholm Karolinska Institute
M Prince London Kings Colledge
Horst Bickel Munich
Andrzej Kiejna Wroclow Medical University of Wrocław
Jean Georges (Alz Association) Luxembourg Alzheimer Europe
7.3 Methods
This project, by means of an extensive literature search using Cochrane review methodologies, has compiled a database of all European epidemiological studies in this field up to the present date.
Systematic reviews of 1) prevalence of dementia, 2) prevalence of early onset dementia and 3) prevalence of Dementia in Eastern Europe have been performed.
Data from high quality studies performed in the last 20 years looking at dementia prevalence have been pooled in a collaborative analysis. Age and sex specific prevalence rates have been calculated using this prevalence data. An outline of the components of the project are presented in Fig. 1
Figure 1
EUROCODE WP7 Components1. Systematic review and
collaborative analysis of population based studies on the prevalence of dementia in Europe
2. Systematic review of prevalence of early onset dementia
3. Systematic review of epidemiology of dementia in Eastern Europe
QUALITY

Page 21 of 88
7.4 Results
7.4.1 Systematic review and collaborative analysis: Prevalence of dementia in Europe
7.4.1.1 Methods
A Systematic review of papers reporting on the prevalence of dementia was performed. Using a Medline and Embase search we found a number of studies using the search terms “Dementia / Prevalence / Incidence / Epidemiology” or “Alzheimer’s Disease / Vascular dementia, Lewy-body disease/ Fronto-temporal dementia/ Incidence / Prevalence / Epidemiology. This was followed by hand searching these papers. A database of studies was compiled and those fulfilling predetermined quality criteria were invited to submit data for the collaborative analysis
7.4.1.2 Collaborative analysis
Inclusion criteria (Table 1) for involvement in the collaborative analysis were decided by the members of the EUROCODE prevalence working group. These were developed by consensual opinion looking at all methodological domains of this type of epidemiological study. Criteria were aimed to identify those studies of highest quality. Studies fulfilling criteria were invited to participate in the collaborative analysis. Age (by 5 year age group from 50 to >95years) and sex specific raw prevalence case numbers and underlying population were collected from all groups agreeing to participate in the collaborative analysis.
Table 1
Inclusion Criteria:-
1. Community based study 2. Minimum sample size 300 3. Study survey date including 1990 or thereafter. 4. Use of standardized diagnostic criteria 5. Participation rate over 50% 6. Available raw prevalence data
7.4.1.3 Analysis
Age (5 year age range) and sex specific raw data from participating studies was included in the analysis. Data above 95 years was combined. Below this age raw data that could not be presented in 5 year age groups was excluded from the analysis. Age and sex specific prevalence’s were calculated using the total number of prevalence cases from all studies as the numerator and total population examined as the denominator. In this way weighting was achieved by each study’s sample size.
7.4.1.4 Results
A total of 194 articles were identified from the literature search. 31 studies were identified as possible for inclusion in collaborative analysis and they were invited to submit data. Raw data was obtained from 17 studies and used in the collaborative analysis of dementia prevalence rates in Europe.
7.4.2 Systematic review: Prevalence of early onset dementia
7.4.2.1 Introduction
Dementia is often thought of as a condition of old age and although most cases are found in the elderly a significant number of people develop symptoms of dementia at a younger age. Patients with onset of symptoms below a certain age (usually set arbitrarily at 65) are said to suffer from “early onset dementia” or “presenile dementia”. The causes and classification of dementia in this age group are the

Page 22 of 88
same as in the more elderly population in that Alzheimer’s disease, vascular dementia, Lewy body dementia and frontotemporal dementia can all be recognised.
7.4.2.2 Study Design
We summarise the findings of studies reporting the prevalence of early onset dementia. We included studies that had determined prevalence rates of dementia in patients less than 65 years of age. Using a Medline and Embase search we found a number of studies using the search terms “Dementia/Prevalence/Epidemiology” or “Early onset dementia/Incidence/Prevalence/Epidemiology.” We followed this with a hand search of the references of these studies as well as any knowledge of any studies by the authors. To be included in the review studies needed to specify prevalence of dementia in subjects aged 65 or younger either looking specifically at this younger age group or as a easily identifiable subgroup of a larger study population. Papers that included the younger age groups but could not be easily determined from older ages were excluded. Those reporting only on incidence were also excluded. The initial database search produced 9 references, 5 of which were included in the review. A further 5 papers were identified by hand-searching the references of publications in the initial database search.
7.4.2.3 Results
The methodology and geography of the papers found reporting prevalence are included in a report on the prevalence of dementia which is included with the present technical report.
7.5 Deliverables
The following deliverables were produced in the framework of the work package:
• An overview of the numbers of people with dementia in the European Union based on the original Eurodem figures was included in the 2006 edition of the Dementia in Europe Yearbook.
• A report on the prevalence of dementia and a systematic review of the prevalence of early-onset dementia are published in separate reports which have been submitted together with the technical report.

Page 23 of 88
8 WP 8 – Socio-economic impact
8.1 Introduction
In order to describe and analyse the socio economic impact of AD, the WP 8 of EuroCoDe has 2 basic aims:
• To make an inventory and comparative report of existing studies.
• To present a consensus document on the socio-economic impact of dementia in Europe.
To fulfill these aims, the WP8 consists of several experts from different parts of the EU:
• Associate professor Anders Wimo, Karolinska Institutet (Sweden)
• Research Fellow David McDaid, London School of Economics (UK)
• Professor László Gulácsi , Corvinus University (Hungary)
• Dr Linus Jönsson, European Health Economics (UK)
• Professor Hannu Valtonen, University of Kuopio (Finland)
• Dr Paul Kenigsberg, Fondation Médéric Alzheimer (France)
• Dr Alan Jaques, Alzheimer Europe (has now retired).
8.2 Methods
8.2.1 Search strategies for the cost of illness estimates
A literature search was conducted for papers reporting data on costs of care for patients with diagnosed dementia or possible/probable Alzheimer’s disease.
Two approaches were used, the first includes bottom-up data, the second includes top-down cost-of-illness studies or similar.
The advantage with the bottom-up approach is that it allows stratification on disease severity and different cost types. This analysis is based on Jönsson-Wimo (1). For European specific studies, Medline, EMBASE and Current Contents were searched for the following terms (in any field):
(Dementia OR Alzheimer*) AND (Cost OR Economic) AND (Europe* OR Austria OR Belgium OR Cyprus OR Czech Republic OR Denmark OR Estonia OR Finland OR France OR Germany OR Greece OR Hungary OR Ireland OR Italy OR Latvia OR Lithuania OR Luxembourg OR Malta OR Netherlands OR Norway OR Poland OR Portugal OR Slovakia OR Slovenia OR Spain OR Sweden OR Switzerland OR United Kingdom)
As part of i.a the Swedish council on technology assessment in health care´s (SBU) dementia project (2), a general search including both bottom-up studies and top-down studies was conducted in PubMed/Medline, Ingenta, Cochrane Library, NHSEED/THA, HEED, PsycINFO, ERIC, Societal services abstracts and Sociological abstracts. The search terms (MESH/Subheadings when appropriate) were dementia/Alzheimer´s disease/Alzheimer disease combined with costs, economics.
More than 500 references were identified in the first rounds. Many Irrelevant papers could be removed by title reading. The abstracts of the remaining papers were then reviewed manually.
The cost of illness and burden of dementia are here presented in three ways:
• for EU 27,
• for EU27 + candidate countries (Croatia, Former Yugoslavic republic of Macedonia and Turkey) + countries in the European Economic Area (Norway, Iceland, Liechtenstein) + Switzerland,
• for the whole of Europe and regions according to the classification by United Nations (UN).
In the Alzheimer Europen Yearbook of 2008, we presented cost estimates for 2005 (3). We have now updated the figures to the situation in 2008. The prevalence figures, which are used for the cost of

Page 24 of 88
illness estimates, are now in the main option based on the new metaanalysis by Eurocode (see another section of this report) but other prevalence sources are presented in the sensitivity analysis: metaanalyses by Eurodem (4), Ferri et al (5),the Swedish health Technology assessment institute SBU (5) and Lobo et al (7) . In short, the new Eurocode prevalence figures result in a greater number of demented people, particularly of female. These age specific prevalence figures are combined with population figures from UN (8). The Eurostat provides more new and up-to-date population statistics but since it ends with the age class 85+, we regarded it as more feasible to use the UN –figures. However, the UN-figures are based on their worldwide statistics and the figures for the oldest age groups are estimates. However, we compared the UN figures for the age group 80-84 for 2008 with the available Eurostat figures for 2007. The ratio was 1.02, which with is a good agreement if a growth in the number of elderly between 2007 and 2008 is taken into consideration.
8.2.2 European cost model
Fourteen papers were finally selected as eligible for the European cost model (Table 2).
The key criterium was that direct costs and informal care costs could be identified.
For countries where no cost of illness figures were available, imputation was used. Four care patterns were identified and used for the imputation representing the relation between formal care (direct costs) and informal care in Northern (mainly formal care), Western (mix between formal and informal care), Southern (mainly informal care) and Eastern Europe (mainly informal care) (based on UN´s region classification of Europe). The imputation figures were also adjusted for differences in GDP per person between countries (9).The cost estimates are also adjusted to the year 2008 by the Eurostat HICP-Health index (Harmonized indeces for consumer prices; Health) (10).
For the countries were such HICP-figures were not available (Albania, Belarus, Bosnia and Herzegovina, Croatia, TFYR Macedonia, Moldova, Russia, Serbia and Ukraine), the CPI sfrom World Economic Outlook were used (11).
8.3 Deliverables
A report on the socio-economic impact of dementia was included in the 2008 edition of the Dementia in Europe Yearbook. The report discussed the health economical context, health economic aspects of dementia, the impact of informal care, the cost of illness and burden of dementia in Europe and presented different regional patterns with regard to the societal costs of dementia in Sweden, France, Mediterranean countries and Hungary.
The group continued to update its research findings in 2009 and a completely reviewed report is included with the present technical report to the European Commission.

Page 25 of 88
9 WP 9 - Prevention
9.1 Introduction
Dementia is a complex condition. There is no single straightforward cause, and no way of definitely preventing it. Many factors influence an individual’s risk of developing dementia. Some of these, such as age or genetics, cannot be changed. Lifestyle factors, such as physical activity, smoking, alcohol drinking or nutrition, are also linked to the risk of dementia. These factors can be changed.
The aim of this project is to develop an inventory on recommendations for a healthy lifestyle to prevent dementia. Meta-analyses will form the basis of a descriptive review of risk factors of dementia.
9.2 Workgroup members
Prof. L. Frölich Head, Division of Geriatric Psychiatry, Central Institute of Mental Health, Mannheim
K.Herold Research assistant, Division of Geriatric Psychiatry, Central Institute of Mental Health, Mannheim
Jim Jackson Alzheimer Scotland, Edinburgh Miia Kivipelto Tiia Ngandu
Associate professor, Aging Research Center, Karolinska Institutet, Stockholm, Sweden Researcher, Aging Research Center, Karolinska Institutet, Stockholm, Sweden
Istvan Degrell Heike von Lützau-Hohlbein
Frans Verhey UMC Maastricht, Maastricht
9.3 Research methodology
A literature search was done to identify reviews on the subject.
Search strategy
We searched for reviews in Pubmed using the following terms:
Relevant studies were identified by systematic search of following data
sources: MEDLINE (‘‘dementia OR Alzheimer OR Alzheimer’s disease’’[MeSH] AND (risk factor OR cohort study (age OR gender OR alcohol drinking OR smoking OR…) AND (risk OR odds-ratio))); Embase, Current contents, the Cochrane database and www.clinicaltrialresults.org for articles published from January 1966 to June 2006. Search was limited to English abstracts and human studies. We identified additional articles and studies by hand-searching referenced articles or reviews on this topic and also personal contacts with investigators.
9.4 Deliverables
A report on risk factors and prevention was included in the 2008 edition of the Dementia in Europe Yearbook. The report contains an assessment of cardiovascular risk factors, environmental and nutritional risk factors, biological non modifiable risk factors, behavioural risk factors as well as recommendations regarding lifestyle and health behaviour.
Page 26 of 88
10 Technical Annexes
10.1 Minutes of meetings organised in the framework of the project
10.1.1 Steering Committee Meetings
10.1.1.1 Minutes of the Steering Committee meeting in Paris (2 July 2006)
Present:
Steering committee members:
• Maurice O’Connell Alzheimer Europe • Jean-Pierre Bayens IAG-ER, EUGMS • Ralf Ihl EAGP • Rabih Chattat Interdem • Anthea Innes North Sea Group / Univ. of Sterling • Helen Regan Alzheimer Disease International
Work package leaders:
• Lutz Frölich CIMH Mannheim • Myrra Vernooij-Dassen Alzheimer Research Nederlands • Anders Wimo Karolinska Institute • Dianne Gove Alzheimer Europe • Emma Reynish Hôpitaux de Toulouse
Alzheimer Europe:
• Sabine Henry Ligue Alzheimer • Heike von Lützau-Hohlbein Deutsche Alzheimer Gesellschaft. • Annette Dumas Alzheimer Europe • Jean Georges Alzheimer Europe
Apologies
• Rupert McShane
Welcome
Maurice O’Connell welcomed the participants and invited them to introduce themselves.
Technical, financial and administrative questions
Jean Georges explained that the aim of the meeting was to gather the steering group and other organisations involved in the project to share progress since the meeting in Luxembourg in February 2006.
Jean Georges informed the group that the contract with the Commission was not signed yet, although this should be a matter of days.
The money will be paid out once the contract has been signed. Alzheimer Europe will receive the money and will distribute it the participating centres. Alzheimer Europe will explain how to claim expenses.

Page 27 of 88
The travel costs for this meeting will be reimbursed for the steering committee members and a per diem will be paid (according to Commission guidelines). Work package leaders will need to account for their costs in the financial accounts submitted to Alzheimer Europe.
Progress report WP4 – Social support systems - Dianne Gove
The group will look at how health and services interact through a literature search.
A questionnaire will be given to each working group member (each in charge of 5 countries). Dianne will be in charge of the rest. The questionnaire is 22-pages long (including notes and a cover letter).
A hand-out with the names of the persons responsible per country, questions on the section on anti-dementia-drugs and the topics covered by the questionnaire was distributed to the participants (attached to this report). The document also includes some definitions linked to the questionnaire on social support systems.
The draft survey has been approved and will be tested. The second stage will be a meeting in November 06, 2006 to discuss the problems faced with filling the questionnaire. In January 2007, the questionnaire will be sent to the member organisations.
The Alzheimer Europe 2006 Dementia Yearbook will use some information gathered by this WP. The Yearbook will be used towards policy makers to identify inter alia barriers to access.
A discussion followed. To the questionnaire on anti-dementia drugs, it was suggested to find out how many people take the drug in each country and to include off-label use.
To the question of price, it was suggested to know the price of a daily dose rather than the price per tablet or capsule.
It was also suggested to be more precise in the questionnaire and find out for which disease the drugs have been prescribed.
Bus passes should be included to the questionnaire section 6.5 (work/tax-related support to people with dementia).
Finally, comments were made on the length of the questionnaire.
Progress report WP6 – Psycho-social interventions – Myrra Vernooij-Dassen
The group will gather and analyse guidelines on psycho-social interventions in Europe, investigate the gaps in the availability of guidelines, build on the existing guidelines and interventions used in other European countries and disseminate the results among European countries.
The focus is on general guidelines that will be on the Internet and used in all settings.
The countries involved are the UK, France, Spain, Denmark, and Luxembourg.
The hand-out that was distributed (attached) listed the research questions, and the methodologies used.
Methodology 2: palliative care should be considered in this section. Also, it was recommended the guidelines include the professionals’ needs and consider action plans.
The suggestions made were to put in place a model that evaluates the studies, emphasize the cultural differences between the Member States, include care support programmes and support groups for people with dementia.
It was strongly recommended to have regular links with the Work Packages to discuss their respective results and avoid overlap. The importance of meetings like the meeting today was unanimously stressed.
To the question of deadlines, the group was reminded that the official publication of the EuroCoDe is end 2008 and that we should stick to this date. Interim reports will be on the Internet. It was also agreed that centres may already publish parts of their results in scientific journals. Rules for such publications would need to be developed prior to this.
An archive system must be put in place to keep track of all information that has been collected for future references.
Progress report WP 7 – Prevalence – Emma Reynish
Page 28 of 88
The group decided to be more specific in what will be achieved by this WP. They wish to be able to come up with figures that could give a realistic figure of the prevalence and incidence of Alzheimer’s disease.
The literature available is small. The next steps are to widen the range of literature search and collate data :
• do as wide a search as possible. The findings should be gathered in a database that is hoped to be hosted on Alzheimer’s Europe’s website
• carry a meta-analysis of prevalence data following a set of criteria (listed in the hand-out attached).
One of the difficulties encountered is the European diversity (different people are in charge, some populations have been studied, others not).
The question is: are there truly differences in the incidence of dementia in Europe
The participants agreed that the focus should be on Alzheimer’s disease. Of interest to AE is also early onset dementia, as Eurodem seemed to have understimated these figures.
There were discussions around MCI (mild cognitive inmpairment). The figures risk to be disappointing because too vague. It was agreed that MCI was a problem and would be skipped.
Progress report WP 8 – Socio-economic costs – Anders Wimo
The conclusions of the meeting in Luxembourg in February 2006 were handed out (attached). Anders Wimo reported that the commitments made by some participants to come up with contributions had not been fulfilled.
Under point 3, it was agreed that it was important to define the concepts. The perspective is on the cost of illness but this perspective needs to be defined.
Under point 4/5, concept about informal care : it is essential to clearly define informal care (i.e. support in activities of daily living, but also supervision activities). This will have an impact on how we estimate the cost of care. It was agreed that the easiest would be to make an estimation in hours rather than in costs. Reliable instruments and methods to validate the results are needed.
Myrra mentioned she had a report on the role of informal care givers and will send it to the WP leader.
The work this group is carrying out should take the opportunity to make a statement that the informal carer is often an elderly person. This redresses the balance when older people are considered as a burden. They in fact play a key role in society.
Point 6 : there is very little data about Eastern European countries and the group will need to focus on this issue.
Point 10: one needs to be prudent when reading the data about access to treatment. The case of Greece was given where a recent study showed that close to 100% of people with dementia are treated but the medicines actually were sold abroad (parallel imports).
It was agreed that there could be an overlap between WP4 and WP8 and that there should be close coordination between the two groups. The reference lists will be shared.
To the question about putting this WP in perspective with NICE, this was not deemed relevant as this WP does not deal with cost-effectiveness.
Report progress on WP 9 – Prevention – Lutz Frölich
A hand-out of the report of the meeting in Luxembourg on February 2006 was distributed along with a document outlining the risk factors in dementia and Alzheimer’s disease.
The WP leader reported that studies had been identified. Only treatable factors will be addressed
It is important to define what are the limitations of risk factors (definitions of the risk factors, different levels of prevention). The idea is to focus on risk reduction rather than prevention.
Many pathologies are associated to Alzheimer’s disease at 90. The risk factors are deducted from the real world. Some elements increase or decrease the risk factors. This can have an effect on other risks.
Some risk factors are independant but many interfere with one another (case of diabetes, Parkinson’s disease and Alzheimer’s disease). This reservation has to be included in the report.

Page 29 of 88
The goal of this group is to give the Commission insight leads where research should be carried out (one project rather that smaller projects that do not meet the needs).
The focus must be more on what is treatment and what is prevention.
Round up and closing
Jean Georges stated that at the end of the project, we should have been able to bring different networks together, made policy recommendations at national and European level. The focus will be on where research should be lead, what are the priorities and what is needed.
The next meeting will be in November 06, in Brussels. The meeting is organised before an Alzheimer Europe lunch in the European Parliament on November 07. The agenda of the EP lunch will be Alzheimer’s disease centenary specific policy activities (presentation of the first Dementia Yearbook and Paris Declaration).
Jean Georges invited the WP leaders to help Alzheimer Europe in approaching key opinion leaders to endorse the Declartion.
Maurice O’Connell closed the meeting by thanking all participants for their work

Page 30 of 88
10.1.1.2 Minutes of the Steering Committee meeting in Estoril (8 May 2007)
Steering Committee Members :
• Giannelli Marie, Interdem
• Ihl Ralf, European Association of Geriatric Psychiatry
• O’Connell Maurice, Alzheimer Europe
• Wortmann Marc, Alzheimer’s Disease International
Work Package Leaders :
• Gove Dianne, Alzheimer Europe, WP 4
• McShane Rupert, University of Oxford, WP 5
• Kerr Amanda, University of Oxford, WP 5
• Vernooij-Dassen Myrra, UMC St. Radboud, WP 6
• Wimo Anders, Karolinska Institutet, WP 8
Alzheimer Europe :
• Dumas Annette,
• Georges Jean.
• Guillory-Hickey Gwladys
• Laine Pekka
• Lavallé Sandrine
• Sadowska Alicja
Apologies :
• Reynish Emma, CHU Toulouse, WP 7
• Frölich Lutz, CI Mannheim, WP 9
• Baeyens Jean-Pierre, International Association of Gerontology – European Region
• Vellas Bruno, European Alzheimer’s Disease Consortium
• Waldemar Gunhild, European Federation of Neurological Societies
PROGRESS REPORTS
WP 4 – Social support systems (Dianne Gove)
Some answers to the questionnaire have already come through (11 responses). More reports are expected (10).
Nevertheless, 11 countries still have not responded. Two options were presented : either leave these countries out or AE looks for the information. Some of people present in the meeting have volunteered to help, identify contacts or contact potential participants (Marc Wortmann for The Netherlands Pekka Laine for Sweden, Amanda Kerr for Estonia). Other contact names will have to be identified for some countries like Latvia and Lithuania.
A problem identified was the difficulty for some countries to reply in English.
Next steps : national reports will be written and sent to the associations for further information or questions on unclear points.
Deadlines:
• end of questionnaire exercise : September (due to Yearbook)
• data will be used in the 2007 Dementia in Yearbook (October).
Page 31 of 88
Dianne explained that the group had concentrated on care in the community and had decided to exclude full-time residential care. However, a few members of the group felt that full-time residential care was extremely important and Anders Wimo’s group was interested in obtaining certain additional facts about such support for WP8. Dianne agreed to look into this and to discuss this issue further with Anders.
Some participants advised her to consult LSE country reports, OECD data, Eurofamcare and the EuroPharm/DIADEM project.
WP 5 – Diagnosis and treatment (Rupert McShane)
The guidelines that are being identified for the guidelines database will be European and non-European and in English. They will be from 1995 onwards.
Regional guidelines will be excluded. Also, guidelines that deal with reimbursement will not be included.
Guidelines who have a section on dementia will be included (Parkinson’s disease guidelines…). Also literature that is not couched as a guideline will be included when relevant.
Next steps :
• The guidelines will be rated using the European-funded instrument for assessing guidelines) AGREE.
• A inter-reliability study of AGREE will be carried out
• A consensus on AGREE score and quality of guidelines will be reached and input into the 2007 Dementia in Europe Yearbook.
Questions :
• Will the guidelines be in paper form ? if so, how many pages ?
• Are there any copyright issues ?
• What are the preferred options ? The US national guidelines clearing house model was suggested.
• What about the funding and maintenance (software licence) ?
Next step :
• The first draft guidelines will be based on the EFNS, SIGN, NICE, IQWIG or ANA guidelines.
• Identify way to reach a consensus on the guidelines (use DELPHI ? this proposal seems to have been dismissed).
WP 6 – Psycho-social interventions (Myrra Vernooij-Dassen)
The working group decided to use the iterative consensus procedure for the elaboration of quality indicators.
Consensus procedure for the development of quality indicators :
• Selection of core recommendations by groups
• Idenfify experts by country. Each expert will rate the core recommendations
• First postal round
• Second postal round
• Discussions in Working Group.
Countries involved in the procedure : Italy, Spain, Portugal, The Netherlands, Belgium, France, UK, Finland, Denmark and Sweden.
A translation of the questionnaires in different languages will be organised in order to ensure that the ratings are reliable.
WP 8 – Socio-economic costs (Anders Wimo)
Some discussions were held around:
• Cost description: it was decided that no comparison would be made and no outcome would be considered (bottom up approach – cost of illness).

Page 32 of 88
• Cost analysis: comparators will be used/.
• Ways to evaluate the effectiveness : comparators will be used (CMA/CEA/CUA/CBA/CCA)
This work package will:
• Concentrate on the cost of dementia care
• Include the cost of indirect care (David McDaid)
• Not consider the quality/value of dementia care
• Not consider the transfer/payment system (out-of-pocket will nevertheless be considered)
• Not consider the cost effectiveness of dementia care
Any other business (Jean Georges)
The Dementia in Europe Yearbook 2007 was discussed and it was agreed to include the information on social support systems from WP4. The various work package leaders agreed to inform Alzheimer Europe by end of June at the latest, if they are able to contribute comparative information from different European countries on their respective work packages.
The participants agreed to use a standard form of acknowleding the support of the European Commission and of Alzheimer Europe in any publication resulting from the project. All members of the respective working groups will be asked to figure as co-authors of any such publication. A standard acknowledgement will be sent by Alzheimer Europe to all participants.
With regard to the financial situation, Jean informed the participants that some centres may have an underspent compared to the initial budget. It was agreed that any such underspent would be shared first between those centres of the same working group who had an overspent compared to their budget. In case, a work package has an underspent, the underspent may be used by Alzheimer Europe to cover the costs of its coordination and dissemination costs, if those resulted in an overspent.
Page 33 of 88
10.1.2 WP 4 Meetings
10.1.2.1 Minutes of the working group meeting, Luxembourg, 25-26 February 2006
Present: Dianne GOVE
Eugen STEFANUT
Federico PALERMITI
Hans-Jürgen FRETER
Jean GEORGES
Louise McCABE
Maria Do ROSARIO Dos REIS ZINCKE
Sabine HENRY
Sirkkaliisa HEIMONEN
Organisational issues
The meeting started after a plenary session involving all the participants from the various work packages. LMC was unfortunately unable to attend the first part of the WP4 meeting (i.e. on Saturday) due to problems with a flight. HJF suggested reorganising the agenda so as to start with the general issues and then have the short presentations and discussions later. This proposal was accepted.
Literature review
Participants agreed to take an active part in the search for relevant documentation. It became clear that very few had access to relevant databases (with the exception of ES) but that all could try to obtain reports from other organisations dealing with these issues, as well as from governments. It was decided that we should not limit our search to comparative reports but should also include information from single countries. Participants agreed to send summaries of relevant information in English to DG. As we will be covering a large number of countries and cannot guarantee the same degree of involvement from each Alzheimer Association, the information collected will be used in a practical way to complete the various country reports. Documents can be scanned or sent by post to DG.
Responsibility for the survey results
DG asked if each member of the group would be willing to accept responsibility for obtaining responses to the survey from 4 to 5 countries. This would mean that the surveys would be sent to all AE member associations which would then be responsible for providing the information. The role of the WP4 group members would be to make sure that the surveys are returned on time and to follow-up on any issues that seem unclear. We will ask for the surveys to be returned to the relevant group member with a copy to DG. Participants agreed to divide the countries as follows:
Dianne Gove Belgium Estonia France Latvia Lithuania Netherlands Poland Slovakia Turkey
Eugen Stefanut Bulgaria Czech Republic Hungary Romania Slovenia
Hans-Jürgen Freter Austria Germany Luxembourg Switzerland
Page 34 of 88
Louise McCabe Cyprus England and Wales Republic of Ireland Malta Scotland
Maria do Rosario Dos Reis Zincke Greece Italy Portugal Spain
Sirkkaliisa Heimonen Denmark Finland Iceland Norway Sweden
WP4 and the AE Yearbook
JG was asked which results from WP4 would be needed for the Alzheimer Europe Yearbook. He explained that only information about the reimbursement of drugs would be included in this year’s publication. We will contact our member associations for information but this will not be part of the main survey as we will need the information much sooner.
Scope of the project
After quite some discussion about the scope of the project, it was finally decided that the aim of the survey was to provide a description/explanation of the situation in each country concerning the extent to which the State supports carers and people with dementia. The information obtained will eventually be presented in the form of individual country reports, as well as a global report summarising some of the main differences between countries and containing policy recommendations and examples of best practice.
We will not be systematically measuring the actual number of services provided in each country. However, such information may be revealed in response to questions about the limitations of State support e.g. an association might report that the State supports day care if a need has been assessed but that there are only 3 day care centres in the whole country.
FP emphasised the importance of including details of the mechanisms of social protection in each country i.e. relevant legislation and the structure of the social support system. It was agreed to include this in the country reports.
It was also agreed that the relationship between health care and social care in each country needs to be understood in order to have a clear picture of how the State attempts to meet the social support needs of carers and people with dementia. It was felt that this was particularly important in view of the fact that in many countries the State has more of an obligation to provide and finance health care as opposed to social care. The point was also made that people with dementia and carers sometimes suffer the consequences of gaps in the system e.g. where neither the health care system nor the social care system has responsibility for a particular form of social support.
How general or detailed should the survey be?
The group decided not to go into too much detail but rather to ask the following kinds of questions for each form of social support:
Does the State provide support for _____ ? (e.g. respite care, home help, transport etc.)
If so, please explain how.
If not, what options are available to people?
As we want to be able to compare the situation between countries, we may decide to ask for specific details for some aspects of social support (and in order to ensure that we do not miss out important information).
It was decided to ask for a description of the services available, details of which services are lacking (according to the Alzheimer Associations) and information about any restrictions governing access to services or allowances.
Procedure for drafting the survey
Page 35 of 88
The group discussed how to go about drawing up the survey. The following procedure was decided upon:
1. DG to draw up survey on the basis of the group discussion
2. Members of the group to comment on the first draft.
3. DG to make any necessary changes.
4. Second draft to be sent to members of the working group.
5. Group members to complete the survey and report on any problems they encountered or
necessary changes which became evident.
6. Group to discuss their experience and make proposals for an improved survey (at the next
meeting in November 2006).
7. DG to draw up and circulate within the group a third draft of the survey.
8. After comment from the group and amendment of the draft, DG to send out the fourth draft to all
Alzheimer Europe’s member associations.
Second day of the meeting/plenary session
At the request of a group leader from one of the other work packages, the second day of the meeting again started with the plenary session. After two short presentations, a lengthy discussion took place in an attempt to identify and deal with possible overlap between two work packages. This was followed by short summaries of progress within the other groups.
Following these presentations, DG briefly discussed collaboration with WP8 with Anders Wimo and Dave McDaid. They suggested checking the European Commission’s DG Employment and Social Affairs work on social protection (the MISSOC website). They were interested in the WP4 group including a question in the survey about where to obtain information on the exact existence of social care provisions in each country e.g. statistics about the number of places in residential homes and day care centres. They do not need us to actually obtain such details but rather just to find out where or from whom they could obtain this kind of information.
Esme Moniz-Cook mentioned possible overlap between WP4 and WP6 (on psychosocial interventions). DG agreed to keep the group leaders of WP4 and WP6 informed of our progress so that we can ensure that we don’t duplicate work and so that we might be able to share certain information.
Reorganisation of the time schedule
Having decided to include an additional stage in the drafting of the survey, it was necessary to adapt the time schedule for completion of tasks. The following deadlines were accepted:
Timeframe Task By the end of March 2006 Complete first draft April 2006 Comments from the working group May to September 2006 Working group to complete the survey October 2006 Results to be sent to DG and circulated within the group November 2006 Meeting to discuss and improve the survey December 2006 Final amendments to be made January 2007 Survey to be sent out to Alzheimer associations February to June 2007 Alzheimer Associations to complete the survey
Content of the survey
The group then discussed the content of the survey, starting with dementia drugs and drug reimbursement systems. It was agreed to limit questions to the four main dementia drugs. Suggested questions included: when were the drugs licensed and when were reimbursement decisions made, who has the right to prescribe such drugs, what are the start and cut-off criteria for prescription, for which diseases have the drugs been approved, what is the price per tablet/capsule, how does the reimbursement system work, are there regional differences concerning access to the drugs and is bi-therapy possible?
Page 36 of 88
Other areas of social support were then considered, such as:
• Home care (e.g. bathing, taking medication, skin care, dealing with incontinence)
• Home help (e.g. housework, laundry, assistance with meals etc.)
• Occupational therapy/ergotherapy
• Home adaptation
• Day care
• Respite care
• Residential care
• Palliative care
• Legislation (relating to State obligations and specific forms of social support)
• Employment issues (time off, flexible hours, incapacity law, pension contributions)
• Government policies (State policy concerning the provision of services)
• Organisation and funding of social support (long-term care insurance, allowances)
• Tax refunds (due to incapacity, for employing home help assistants)
• Benefits (continence pads, free transport, free TV licence)
A discussion followed about certain terms used which might be confusing (e.g. the difference between allowances and benefits or between occupational therapy and ergotherapy) and about different opinions as to how to categorise certain forms of support e.g. for Romania, should personal assistants be classed as a service or as an allowance if the personal assistant is the spouse of the person with dementia and therefore receiving money for the care that they provide?
The conference in Paris
JG asked members of the group if they would like to have a workshop in Paris1 to discuss some of the issues linked to the survey. All agreed in principle but some stated that it would be necessary to check with their organisations with regard to financing. Nevertheless, they provisionally agreed to deal with the following topics:
Employment provisions Sirkkaliisa Heimonen
Drug reimbursement Maria do Rosario Dos Reis Zincke
Long-term care insurance Hans-Jürgen Freter
Assessment and legislation Louise McCabe
The system in Romania Eugen Stefanut
Each person will speak for about 10 minutes and there will be plenty of time to discuss the various issues with the people attending the workshop. Members of the group agreed to send a brief extract of their presentation to JG who will then submit the proposal to the French Alzheimer association.
Close of the meeting
DG thanked members of the working group for their work and the meeting was brought to a close. The next meeting will be held in November 2006.
Annexes
1 the 16th Annual Alzheimer Europe conference – 29 June to 1 July 2006
Page 37 of 88
A timetable of the revised work schedule is attached as a separate document. On the next page, you will find contact details for members of the group and references to some of the documents mentioned during the meeting.
Participants of WP4
Dianne GOVE Alzheimer Europe Luxembourg [email protected] Eugen STEFANUT Societatea Alzheimer
Romania Romania [email protected]
Hans-Jürgen FRETER Deutsche Alzheimer Gesellschaft
Germany [email protected]
Louise McCABE University of Stirling United Kingdom
Maria do Rosario DOS REIS ZINCKE
APFADA Portugal [email protected]
Sirkkaliisa HEIMONEN Alzheimer Keskusliitto
Finland [email protected]
Additional participants
Federico PALERMITI Fondation Medéric Alzheimer
France [email protected]
Jean GEORGES Alzheimer Europe Luxembourg [email protected] Sabine HENRY Ligue Alzheimer Belgium [email protected]
Interesting documentation
• Eurofamcare national background reports based on services for supporting family carers of elderly people in Europe, Countries covered include: AT, BE, CH, CZ, DE, DK, EL, ES, FR, HU, IRE, IT, LUX, MT, NL, NO, PL, PT, SE, SF, SLV, and UK (2002 to 2005)
• Procare reports on providing integrated health and social care for older persons, Countries covered include: AT, DE, DK, EL, FR, IT, NL, SF and UK (2003)
• Brodsky, J., Habib, J. and Mizrahi, I. (2000), A review of long-term care laws in five developed countries, Countries covered include: AT, DE and NL
• Joël, M-E and Cozette, E. (Eds.) (2002), Prise en charge de la maladie d’Alzheimer en Europe, INSERM. Countries covered include: BE, DE, DK, ES, FR, PT, SE and UK
• MISSOC comparative tables on social provision e.g. entitlement to services, certain relevant laws, reimbursement systems for medication and health services etc. Countries covered include: All EU member states, Can be accessed at: http://europa.eu.int/comm/employment_social/missoc/missoc4_en.pdf
Page 38 of 88
10.1.2.2 Minutes of the working group meeting - Brussels, 6 November 2006
Present: Dianne GOVE
Letitia DOBRANICI
Federico PALERMITI
Hans-Jürgen FRETER
Louise McCABE
Maria Do ROSARIO Dos REIS ZINCKE
Sabine HENRY
Sirkkaliisa HEIMONEN
Organisational issues
The group agreed that each person would give feedback based on their experience of filling out the draft questionnaire. Numerous pointed were raised by various members of the group, often leading to a group discussion. For this reason, the various issues raised will be recorded here in the same order as they appear in the questionnaire.
The overall structure of the questionnaire
It was decided to refer to the two sections of the questionnaire as Part 1 and Part 2 to avoid confusion when referring to the various sub-sections of Part 2. Sabine HENRY suggested rearranging the sections and the items in Part 2 in order to put questions about services and support for people with dementia before those for carers e.g. section 6 before section 5. This proposal was accepted.
Explanations and definitions
There was general agreement that the explanations and definitions currently in the appendix would be far more useful if included in the actual questionnaire at the end of each specific question. It was decided to move the definition of social support to the beginning of part 1 of the questionnaire.
Letitia DOBRANICI felt that it was unclear whether respondents should mention all existing services (irrespective of whether people with dementia can use them) or just those specifically for people with dementia. It was agreed that we would like to know about services and support that are specifically designed for people with dementia as well as more general services/support (e.g. including those for elderly, dependent and/or disabled people) provided that people with dementia can use them. An explanation will be included at the beginning of Part 2.
Part 1 of the questionnaire
Legal provisions
Hans-Jürgen FRETER pointed out that although it is interesting to know which laws exist, there is a risk that the information provided might be misleading in the sense that it might paint a rosy picture of legal provisions, which in reality, are not enforced or have little impact on the provision of support/services. Federico PALERMITI suggested asking respondents to separate laws and acts from decrees in order to separate theory from practice. This proposal was accepted. An example of how to present information on legislation and decrees will be included in the appendix.
Additional information requested
A few additional items were proposed for inclusion in Part 1 of the questionnaire such as:
• A reference to possible interaction between the State, the private sector and voluntary
associations/NGOs
• Details of government priorities linked to dementia/action plans for dementia
• Whether services are adequate and sufficiently accessible (covering issues such as people
living in rural areas, age discrimination and other barriers to access)
• The extent to which available services actually respond to the specific needs of people with
dementia

Page 39 of 88
• Whether the State supports Alzheimer associations and if so, how.
It was pointed out that the combination of a reference to the funding of the healthcare and welfare systems in question 2 and to how specific services and support are funded in question 4 could lead to confusion.
Quality of care
It was decided not to ask directly about quality of care as this is beyond the scope of our project. However, it was decided to include something about minimum standards of care and the control of services in the question about the legal framework in case there are decrees covering these issues.
Part 2 of the questionnaire
The extent and appropriateness of services provided
In the last draft of the questionnaire, we asked about the extent to which services are provided which led to some confusion. Sirkkaliisa HEIMONEN suggested taking out this question and trying to incorporate into Part 1 some reference to the main deficits of services, difficulties accessing services and the extent to which the needs of people with dementia are taken into account by the services provided. This proposal was accepted.
Whether services are funded or provided freely by the State
Some members of the group were unclear about how to answer the question about the degree of State funding for individual services (due to the either/or construction). Dianne GOVE proposed a solution which gives respondents the possibility to tick more than one box in order to indicate whether the State funds the service partly, completely or not at all, with the same options for the service user. This proposal was accepted.
The cost of care
At the request of members of WP8, a question was included in the last version of the questionnaire about the cost of each service. None of the members of the working group provided this information. The reason for this omission was discussed. Members of the working group had found it difficult to obtain such information and felt that in any case, prices varied too much from one service provider to another and from region to region. It was also felt that as the questionnaire was already very long and as the cost of care was beyond the scope of this work package, it would be unwise to cover the issue of cost. We could perhaps ask a few precise questions about the cost of certain services on behalf of WP8 once we have received most questionnaires back.
Section 1 – Types of care - Palliative care
Louise McCABE pointed out that the definition of palliative care was misleading as it did not make it sufficiently clear that we were interested in palliative care in the last stage of the disease and not throughout the whole course of the disease (which would in theory be possible due to the fact that dementia is a terminal illness). It was agreed to alter the definition.
Section 2 – Personal assistance at home
Sirkkaliisa HEIMONEN suggested taking out the question about other kinds of nursing care as the main kinds of nursing care directly linked to dementia had already been covered. This proposal was accepted.
Section 4 – Psychosocial support and training
Federico PALERMITI suggested adding a question about the existence of a general information service i.e. to inform people about services and orientate them towards specific dementia counselling services etc.
It was also agreed that there should be a question about holidays for people with dementia as there is already one about holidays for carers.
The questions on support for Alzheimer associations and training for volunteers were rejected as it was felt that whilst important issues, they are not directly about support or services for people with dementia or carers. The question on support for Alzheimer associations will nevertheless be included in Part 1 of the questionnaire.
Section 5 – Work/tax related support to carers

Page 40 of 88
It was decided to change the order of this section and section 6 in order to put people with dementia first and to add explanations about flexible working hours and free/subsidised pension contributions. The title was changed.
Section 6 – Work/tax related support to people with dementia
The title was also changed.
Section 7 – Other
An additional section was added to allow respondents to add any further information.
Responsibility for different countries
As there had been changes within the group, Dianne GOVE went through the responsibility of each member of the group for specific countries and made a small change based on the fact that we do not have a contact person for every country. The countries are now divided as follows:
Dianne Gove Belgium Estonia France Latvia Lithuania Netherlands Poland Slovenia Turkey
Letitia Dobranici Bulgaria Czech Republic Hungary Romania Slovakia
Hans-Jürgen Freter Austria Germany Luxembourg Switzerland
Louise McCabe Cyprus England and Wales Republic of Ireland Malta Scotland
Maria do Rosario Dos Reis Zincke Greece Italy Portugal Spain
Sirkkaliisa Heimonen Denmark Finland Iceland Norway Sweden
The cover letter
The group decided to make the following changes to the cover letter in order to increase the chance of member associations taking the time to fill out the rather lengthy questionnaire. The following changes were agreed upon:
• To make the first paragraph sound more friendly and straightforward.
• To add a paragraph about what the survey could bring to member associations in order to
motivate them to participate.
• To change the date for completion from 30 June to 30 March 2007.
• To delete the last paragraph and add the request for details of the contact person to the
preceding paragraph.

Page 41 of 88
Deadline for return of the questionnaires
Hans-Jürgen FRETER suggested making the deadline for the return of the questionnaires much earlier so as to avoid people putting the questionnaire on the back-burner for too long and then forgetting to do it. Letitia DOBRANICI proposed that members of the working group send out a letter introducing themselves to the associations in the countries that they are covering about one month after the questionnaire has been sent out. It is hoped that this will serve to remind them about the questionnaire and make the request more personal.
Revised work schedule
The following deadlines were set for the dispatch and completion of the questionnaires:
End of November: Completion of next draft
End of December: Comments and approval (from the working group)
Mid January 2007: Dispatch of the questionnaire (by Dianne GOVE)
Mid February 2007: Introduction and reminder from members of the working group
End of March 2007: Deadline for completion of the questionnaire
Close of the meeting
DG thanked members of the working group for their work and the meeting was brought to a close.

Page 42 of 88
10.1.2.3 Minutes of the working group meeting, 26 February 2007, Brussels
Present: Dianne GOVE
Federico PALERMITI
Hans-Jürgen FRETER
Letitia DOBRANICI
Maria Do ROSARIO Dos REIS ZINCKE
Sabine HENRY
Apologies: Louise McCABE
Sirkkaliisa HEIMONEN
Welcome
Dianne GOVE welcomed the members of the group to the meeting and explained that Louise McCABE and Sirkkaliisa HEIMONEN were unable to attend. The plenary session had been very brief so there was an extra hour for discussion in the morning.
Progress with contact details and reminders
Dianne GOVE explained that she had sent out the questionnaires to all member associations or contact people with the exception of Latvia for which Alzheimer Europe had no contact person. Later in the day, Dave McDAID from WP8 offered to supply her with a contact person for that country.
Members of the group explained that they had not sent out the reminders yet. They agreed to do this on 1 March and again on 15 March. Sabine HENRY explained that she had obtained an offer of assistance for the questionnaire for Belgium from Dr Ylieff.
Presentation of the situation in Romania
Letitia DOBRANICI gave a progress report on the completion of the questionnaire for Romania and outlined some of the main difficulties encountered. First, she explained that it was difficult deciding on just one answer from the many different ones received. She had consulted family carers of people with dementia having the severe handicap category, patients who come to her for consultation, those who come to the association, professional carers, family doctors and psychiatrists and representatives from local authorities. Their responses were very different.
She then explained that there had been a change in legislation but that the norms/regulations necessary to implement the measures contained in the new law had not yet been drawn up and this could take some time. Funds from the European Union may also have a dramatic effect on service provision so the report on Romania is likely to become quickly out of date. Dianne GOVE stated that changes to the reports, particularly from members of the working group, could be made until quite late on in the project. Sabine HENRY added that the reports resulting from the questionnaires could be seen as a kind of snapshot of the current situation in each particular country.
Letitia DOBRANICI went on to explain that it is difficult in Romania to find out about the existence of services on a local basis. Federico PALERMITI suggested consulting an official list of registered associations. Hans-Jürgen FRETER added that other countries may well have similar difficulties and that it is therefore important to have some basic background information about each country i.e. the socio-economic situation and recent developments. We could also explain that certain countries are currently in a process of transition.
Presentation of the situation in Portugal
Maria Do ROSARIO Dos REIS ZINCKE explained that the situation was quite different in Portugal. She has found a social worker who will take care of filling in the questionnaire. This person is familiar with the situation throughout the whole of Portugal and can, if necessary, contact regional branches for more information. She therefore does not envisage any major problems in completing the questionnaire.
Presentation of the situation in Germany
Hans-Jürgen FRETER gave details of the situation in Germany which is also in transition as the long-term care insurance is being reformed. The changes will come into force next year. Most are linked to the financing of the system and it is likely that people will be encouraged to take out additional private

Page 43 of 88
insurances. He emphasised the importance of background information about the different types of state involvement in the system.
With regard to legislation, there are federal laws which cover the whole of Germany and other laws which just cover the various “Länder”. The long-term care insurance is a federal law. There are also differences between the former eastern and western parts of the country. In the former East, for example, there a fewer specialised doctors and the population is currently composed of more elderly people as many younger people have moved to the former West.
National reports
Dianne GOVE stated that she would like to have a separate national report for each country containing the information from the completed questionnaire and presented in a more readable format along with the information on the availability of drugs which Jean GEORGES has already obtained. She circulated copies of a draft plan. Such reports are not required for the EuroCoDe project but would be useful to us when comparing the results from the questionnaires and may also be of interest to other people, particularly those who are just interested in one or a limited number of countries.
Letitia expressed concern about the use of tables to summarise the existence or lack of services in each country as it would not be clear from the tables how reliable or extensive the services were. In Romania, services sometimes exist for the duration of a particular project and then cease to exist when the funding runs out. Even though the tables would be followed by a detailed explanation, she felt that many people would just look at the table and then ignore the text with the result that misunderstandings could easily occur. Other members of the group agreed on the need to take out the tables and limit ourselves to a description of the findings. The actual order in which the information will be presented in each of the major sections has yet to be decided.
The national reports will be written on an ad hoc basis and will hopefully be ready for the next meeting in November (if they are returned on time).
Examples of best practice
The discussion started with a query from Hans-Jürgen FRETER about the use of the word “best practice” as we are not in a position to judge from the kind of information we will have at our disposal what best practice is. Also, we will probably not have information on the full range of support in each country. Other members of the group agreed and felt that the term “good practice” would be more appropriate.
Maria Do ROSARIO Dos REIS ZINCKE stated that we could not quote examples of good practice based simply on the existence of a particular service. Dianne GOVE explained that good practice could be understood as services or other forms of support that seem to respond to the specific needs of people with dementia and carers based on our understanding of what those needs are.
The group then discussed the possibility of writing a summary of the needs of people with dementia and carers and then fitting in selected examples from the questionnaires of support which corresponds to these needs. The idea of arranging needs according to stages was rejected so an alternative structure will have to be worked out.
Hans-Jürgen FRETER suggested checking the use of the term “needs” as it may carry negative connotations and some people argue that needs are created by society and do not reside in the individual. Federico PALERMITI agreed. Dianne GOVE stated that she would check this and in any case explain what we mean by the term if we eventually use it.
The recommendations
The group briefly discussed the recommendations. Dianne GOVE explained that the recommendations were intended for policy makers according to the project proposal. A few issues were suggested (linked to the earlier discussion on needs and good practice) e.g. services and benefits that are flexible, accessible, widely available and adapted to the needs of people with dementia and their carers, specially trained personnel, services for people with different types of dementia and from different sub-groups, support for Alzheimer associations etc. More in-depth discussions will be held in November 2007.
Planned documents and working schedule
The group discussed the different documents that will be produced and how the work could be organised. It was agreed that Dianne GOVE would write the national reports and eventually find some background information on how the health care system fits into the overall system within each country (just a paragraph or two to explain the context).

Page 44 of 88
Members of the group will send out reminders, chase up responses, ask for clarification if needed, propose examples of good practice and recommendations and comment on the various draft reports.
Maria Do ROSARIO Dos REIS ZINCKE said that it was important for her to seek additional information on the legal provisions in the countries she is handling in order to make sense of the information received. Although other members of the group will not necessarily be able to do this as they do not all have the legal expertise necessary, Dianne GOVE thanked Rosarió for this offer and added that any assistance from members of the group with texts, documents and background information would be welcome.
Federico PALERMITI suggested having an example of a completed questionnaire as organisations might find this useful. As Letitia DOBRANICI has completed hers already, I attach this for information and also as a possible example for other organisations. Members of the group should feel free to ask Letitia any questions concerning the questionnaire and it would be helpful if they included the group as “copy” in the email.
Dianne GOVE will draft either a list or a short document to serve as a basis on which to develop a text on the needs of people with dementia and their carers. Examples of good practice will later be incorporated into this document. The recommendations could also be included in this document unless we later decide to keep them separate.
Additional meetings
The group felt that November was a little late for the next meeting and that a short meeting in Portugal in May would be useful. Hans-Jürgen FRETER will not be attending the conference in Portugal. The other members of the group will probably all be present. Dianne GOVE said that she would check with Louise McCABE2 and Sirkkaliisa HEIMONEN who were not at the meeting. Anders WIMO from WP8 asked if we could meet on 10 May in Estoril for a short discussion about helping each other with certain issues.
Close of the meeting
DG thanked members of the working group for their work and the meeting was brought to a close.
Annex - Revised working plan
Tasks (2006) F M A M J J A S O N D Kick-off meeting/determine research methodology X Carry out literature search X X X X X X X X Prepare and send out survey: DG to prepare first draft X Group to send comments X DG to send out second draft to the group X Group to complete the survey X X X X X Completed surveys to be circulated in the group X Meeting to discuss changes to the survey X DG to make final changes and send final draft to the group X
Group to approve final draft X
Tasks (2007) J F M A M J J A S O N D Ongoing search for information X X X X X X X X X X X X DG to send out survey to all member associations X Group members to send introduction and reminder X Member associations to complete survey X X X DG to draft country reports X X X X X X X X Group to discuss the results and clarify various responses X X X Group to seek additional information if needed X X X X
Work on recommendations and best practice X X
Tasks (2008) J F M A M J J A S O N D
2 Louise has since informed me that she will not be able to attend a meeting in May.

Page 45 of 88
Work on recommendations and best practices X X X Work on country profiles and comparative report X X X X X X X X X X Endorsement and presentation X X X

Page 46 of 88
10.1.2.4 Minutes of the working group meeting, Brussels, 12 November 2007
Present: Dianne GOVE
Federico PALERMITI
Hans-Jürgen FRETER
Letitia DOBRANICI
Louise McCABE
Maria Do ROSARIO Dos REIS ZINCKE
Sirkkaliisa HEIMONEN
Sabine HENRY (for part of the meeting)
Alicja SADOWSKA (guest participant)
Gwladys GUILLORY (guest participant)
Organisational issues
The first half of the meeting was dedicated to sharing information obtained from the survey and the second part to making preparations for the drafting of the recommendations.
But first, the members of the group discussed the Dementia in Europe Yearbook 2007. They were impressed with the result and pleased that the country reports had been published. However, there was some concern that the information would quickly become out-of-date. Dianne Gove explained that the reports would eventually be made available on the Alzheimer Europe website and that it would then be very easy to update them whenever necessary.
The situation in Romania
Letitia then gave some additional information about Law 448 which regulates the rights and obligations of handicapped people in order to promote their social inclusion and integration. She explained that not all forms of dementia are recognised as a handicap (just Alzheimer’s disease, senile dementia and mixed dementia – not other forms of dementia). In order to apply for handicap status, it is necessary to submit a file, be admitted to hospital, be evaluated by a psychiatrist and psychologist and have a scan. The scan is free of cost provided that the applicant is in hospital and that the scan has been recommended by a specialist. Younger people with dementia cannot get an assessment. The necessity to obtain disability status acts as a barrier to obtaining support.
Those who qualify for disability status are entitled to an allocation plus personal assistance. The allocation is quite high (i.e. EUR 250/month) so at local level, attempts are being made (unofficially) to reduce the number of people entitled to it. Even specialists readily adopt unofficial guidelines out of fear of being questioned by the audit commission. There is corruption within the system and bribing doctors is quite common. This is a further unofficial barrier to accessing services and support.
The situation in Scotland and Malta
Louise spoke about the situation in Scotland where the focus is on needs and where social support is dependent on an assessment. Services are free at the point of delivery and means tested but this does not extend to the income of people’s children. Personal care is free and is based on a long-winded definition which differs from one local authority to the next. There is a wide range of services. The emphasis is on community care but residential care is also sometimes considered as community care. Daytime opportunities for socialisation are not common but there has been a massive investment in telecare and AT. Carers also receive an assessment but there is no budget for services behind this assessment. The voluntary sector provides good services but its funding is not very sure.
She then described the situation in Malta where there seems to be a good range of services provided through the healthcare system which are free at the point of delivery. There are 13 day care centres and a good telecare system but only 4 hours’ assistance (home help) is provided per week which is not a lot in the case of dementia.
The situation in Finland
Sirkkaliisa described the situation in Finland. She explained that the Finnish government is committed to promoting the functional capacity of elderly people and is therefore supportive of home care services.
Page 47 of 88
The use of AT is very important too. However, there are a number of projects which have run for 3 years and then stopped so there is clearly a problem with continuity.
Furthermore, although each municipality must have a care strategy and provide services, there are no official quality criteria. There are, however, guidelines and recommendations. For example, there will be new “quality recommendations for care and services for older people (2001)” by the end of the year and there is a “Roadmap for a good old age. Policy definitions for good care and services for older people (2015)”. Sirkkaliisa kindly offered to translate this and circulate the translated version amongst the group.
In Finland, like in many other countries, there is a problem providing services in rural areas. However, they have adopted a novel approach which is a memory bus and nurse, which visits the rural areas. An expert group is currently making guidelines to assess the functional ability of elderly people. The group will consider different assessment tools as well as the ethics of assessment.
The situation in Portugal and Spain
Rosário explained that in Portugal there is no specific department responsible for providing support to people with dementia and that services for the elderly are not necessarily suitable for people with dementia. Services and support are funded through general taxation and National Health Services fees. APFADA is the sole provider of psychosocial support. People with dementia may be entitled to a monthly payment of between EUR 80 and EUR 150 depending on their degree of dependency. However, the definition of dependency is very physically orientated rather than towards mental disease.
She then went on to provide brief details about the systems in Spain and Greece. She pointed out that in Spain taxation does not cover social care which is means tested and that Spain has an information system which is completely funded by the State as well as free medication for people over 65 years of age with insufficient means. In Greece, the emphasis is on social support rather than financial assistance and services are designed to try to keep people at home for as long as possible.
The situation in Germany
Hans-Jürgen provided information about the reform of the long-term care system. He explained that there is a 200 page proposal which will be presented to the parliament in December and that changes should normally be introduced on 1 July 2008. Some of the possible changes are as follows: an increase from 1.7% to 1.95% for the LTCI contribution with a further increase of 0.25% for people with no children; an increase in the allowance, especially for ambulance services; the introduction of the “Pflegestutzpunkt” which is a base where people can apply for services; managed care/file management which provides for someone to take care of applications for money from the care allowance; and more money for low level interventions such as “Betreuungs” groups and volunteer training.
He also described a certain kind of living arrangement called a “Wohngemeinschaft”. On the surface, it seems like a good idea in that people with dementia live together in the same building. This provides something in between living completely independently and going into residential care because it is like living at home but there are other people who live there too and some kind of assistance if needed. However, he pointed out that there is no state control of these communities and consequently, no guarantee of quality.
The situation in France
Federico told the group about an Alzheimer Commission which had been set up and whose role was to propose measures to the President. This is not the same thing as the “Alzheimer Plan”. It will be available in January and Federico has kindly offered to translate the major points and send the summary to members of the group. He explained that the Fondation Méderic Alzheimer had been involved in the expert meetings and outlined some of the proposed changes:
• Promotion of the use of advance directives and ethical committees; guidelines on good practice for professionals and simple information for families.
• Big investment in medical research and development of psychosocial research. • Creation of a legal status for carers. • Development of memory centres and of information and counselling services. • Development of palliative care for people with dementia (specially trained staff). • Development of home care services, AT and home adaptations. • Possible creation of case management.
There is no planned revolution in the provision of services except that more effort will be made concerning rural areas and details about how all the proposed changes are to be financed are missing.

Page 48 of 88
The recommendations and the criteria for good practice
It was agreed that we must define what we mean by good practice in the recommendations. The necessity to write in a concise manner and to keep the text simple was also stressed. Letititia suggested including case studies and Hans-Jürgen suggested including graphics, a series of steps progressing from initial counselling to the need for residential care and on to palliative care. Letitia mentioned that she had a series of statements about needs and services made by carers based on the 10 most serious problems encountered and that she could send these so that they could be used as quotations. Hans-Jürgen proposed that all members of the group look for examples of statements made by carers and people with dementia about service provision and support.
Dianne suggested having a document which introduces different topics, offers recommendations and supports the recommendations with examples of “good practice” taken from the survey results (or elsewhere if we find others). The graphics, case studies and quotations could be carefully woven into the text.
The group discussed how to identify good practice. It was decided that good practice should not be understood as referring to the actual quality of specific services (e.g. whether good quality day care is provided in Luxembourg) as we did not have access to that kind of information, but rather to the extent that specific services or ranges of services are provided and respond to the needs of people with dementia. The following criteria were considered appropriate:
• care that is appropriate for people with dementia and corresponds to the different stages of the disease
• care which focuses on specific needs within dementia e.g. people living alone, younger people, people with learning disabilities and people with co-morbidity, people in rural areas etc.
• services which are accessible • services which offer choice and flexibility • a seamless care chain/integrated care • support to carers • 24 hour care • person-centred care and a holistic approach
The above ideas can be further developed in the coming months.
A few issues which might eventually make up part of the recommendations were discussed in detail. For example, it was agreed that:
• quality of life must be balanced with a certain degree of risk (so as to enhance autonomy) • people with dementia should be able to live in their own homes which means they must be
provided with the services that will enable them to do so. • people with dementia and carers should be involved in the planning of services as early as
possible. • in rural areas, services should be available which are adapted to the needs of people in those
areas. The memory bus was considered an example of good practice. • successful project-based services provided by NGOs should receive continued support so as to
ensure continuity of services. • an integrated care approach should be pursued but it must nevertheless be clear at all times,
who has responsibility. Someone needs to take the lead. • the possibility of respite care in the home should be offered so as to avoid unnecessary
upheaval and stress for the person with dementia. • local authorities should be able to provide a list of the services that are available locally. • a wider range of services is needed. • a proper assessment should be carried out. • the rehabilitative aims of support and services should be emphasized.
The comparative report
As the comparative report has be ready by the end of January and the next meeting is set for the end of March, Dianne suggested writing the report in December so that it can be submitted along with the next interim report but pointed out that it would be possible to carry on working on it after that date.
Plan for the completion of the work
Different members of the group agreed to work on various issues in preparation for the drafting of the recommendations and in order to have a basis for more in-depth discussion at the next meeting. They agreed to prepare ideas for recommendations and look for examples of good practice to support their

Page 49 of 88
arguments wherever possible. Dianne agreed to prepare a list of contact details of all the Alzheimer associations and experts responsible for the writing of the reports (please see Annex).
Preparatory work to be carried out by members of the group Sirkkaliisa Rehabilitation, flexibility of service structures and appropriateness to needs Rosário Carer support Louise Choice and the work force Hans-Jürgen The steps from counselling to nursing home/palliative care Dianne Home care services
Close of the meeting
DG thanked members of the working group for their work and the meeting was brought to a close.
Annex – Contact details of Alzheimer Associations and external experts Austria Antonia Croy and Roswitha Bartsch from
the Austrian Alzheimer Association [email protected]
Belgium Sabine Henry from Ligue Nationale Alzheimer Liga and Dr. Michel Ylieff
Czech Republic Iva Holmerová, M.D., Ph.D. from the Czech Alzheimer Society
Denmark Merete Jensen from the Danish Alzheimer Association
England, Wales and Northern Ireland
Clive Evers from the Alzheimer’s Society, with the assistance of Louise Lakey and Samantha Sharp
Estonia Eve Võrk from the Estonian Association of Alzheimer’s Disease
Finland Sirpa Granö from the Alzheimer Society of Finland
France Federico Palermiti and the team from Fondation Médéric Alzheimer
Germany Hans-Jürgen Freter of the Deutsche Alzheimer Gesellschaft
Greece Fotini Kounti from the Greek Association of Alzheimer’s Disease and Related Disorders
Hungary Eva Himmer from the Hungarian Alzheimer Society
Iceland Helgi Johann Hauksson from Alzheimer Iceland (F.A.A.S)
Ireland Samantha Taylor from the Alzheimer Society of Ireland
Italy Marie V. Gianelli from Scuola provinciale per le Professioni Sociali BOLZANO (BOZEN) and Andrea Fabbo (MD)
Latvia Docent Māris Taube, MD from the Public Health Agency in Latvia
Lithuania Liuba Murauskiene from “MTVC” - Training, Research and Development Center
Luxembourg Dianne Gove from Alzheimer Europe (on behalf of Luxembourg)
Malta Dr Charles Scerri and Dr Stephen Abela from the Malta Dementia Society
Netherlands Marco Blom from the Dutch Alzheimer Association
Norway Maija Juva from the Norwegian Alzheimer Association
Poland Mirka Wojciechowska from the Polish Alzheimer Association
Portugal Rui Barros de Abreu on behalf of the Portuguese Alzheimer Association (APFADA)
Romania Letitia Dobranici from the Romanian Alzheimer Association
Scotland Kate Fearnley from Alzheimer Scotland [email protected] Spain Ms Ines Quiroga and the Fondation
Alzheimer España [email protected] (only speaks Spanish)
Sweden Lennart Garney from the Demensförbundet
Switzerland Marianne Wolfensberger from the Swiss Alzheimer Association

Page 50 of 88
10.1.3 WP 5 Meetings
10.1.3.1 Minutes of the meeting held in Luxemburg on 25-26 February 2005
Present: Mario Fioravanti, Brigitte Grass-Kapanke, Dymphna Hermans, Rupert McShane
Absent: Peter Tariska and Philip Scheltens
Rupert welcomed everybody and introductions were made.
The first milestone in WP2 is month 2 when discussion regarding the research methodology should be finalized. Obviously, as contracts have not been signed yet, no progress has been made with this at all. We decided it would be important to try to make a start with this during our stay in Luxemburg. Other issues Rupert thought we should discuss at this stage were structure of communications and conflict resolution.
Conflict resolution could be done using the DELPHI model but as this is in fact part of the Alzheimer Europe’s WP (D3 – Internal rules for conflict resolution, risk management and financial administration and reporting) which should be delivered in month 6, it was decided to leave that for now and see what has happened on that at the meeting in Paris at the beginning of July (only WP leaders will be expected to attend that meeting).
Rupert: to ensure that this gets discussed at the Paris meeting
Communications: it was decided that it will be valuable to have regular teleconferences with all members of WP5. Skype provides free telecommunications via computers and we agreed it would be ideal if all members could set up Skype on their computers.
Dymphna: to inform all WP members on where to find Skype, how to download it and set it up; also to send out reminders regarding teleconferences
Dymphna and Mario: to test Skype between them by end of March 2006
The first test round will take place on Wednesday 5 April at 12.00h UK time/13.00h Europe time; the call will be organized by Dymphna from Oxford.
The first WP5 teleconference will take place on Wednesday 24 May at 12.00h UK time/13.00h Europe time; the call will be organized by Dymphna from Oxford.
A call for agenda items will be sent out by Dymphna in early May; the agenda and associated papers will be send out a week before the teleconference.
Research methodology: we discussed a number of issues.
Who is our audience?
For diagnosis as well as treatment it was thought that we should focus on clinicians.
What diseases are included under ‘dementia’
We should cover AD, VD, PDD, DLB, MCI, FTD and (after discussion with main group) alcohol related dementia. However, we agreed that the WP looking at ‘Prevention’ would deal with alcohol, and we would deal with treatment of ‘MCI’.
What treatments are included in our WP?
Treatment should be anything that gets into the bloodstream.
How far back should we look for guidelines and what geographical areas should we cover
We decided that only literature from the last 5 years should be included and that we should look at all existing guidelines (the whole world)
It was decided that it would be highly desirable to have a draft/template consensus guideline ready for both diagnosis and treatment for discussion at the Paris meeting in early July. Even if this has to undergo subsequent changes it will be very useful to have a framework to work to.
Rupert: to develop draft consensus guideline and circulate to WP5 members for discussion at the 24 May teleconference
We looked at a few guidelines in detail to get some idea of the kinds of information we would want to extract and put in our guidelines database.
Page 51 of 88
• Looking at the Scottish BPSD guidelines for example we noted that it will be useful to record the date of the guideline, the date of the next update, level of evidence and grade of recommendation.
• Other fields that were flagged up looking at several other guidelines: o Contact details o Channel for comments and criticisms o People involved/panel selection o Development process of guidelines o Type of intervention o Remit of guideline/mission statement o What treatments o Do treatment guidelines decide on other issues like consent o Does it have a recommendation section o Method of generating guidelines (e.g. systematic review) o Does it have a summary table o Who initiated guideline o Statement of method of creating consensus o Practice recommendation of a diagnosis (distinction between dementia and sub
etiologies? o Sensitivity &specificity section? o Accuracy and laboratory testing o Screening/types of investigations you do o Diagnosis communication – how is it done o Anything on driving? o Anything on financial matters? o Capacity for treatment decisions (advanced directives) o Structure of services (team work) o Evidence base (type of searches and information sources o Quorum approach? o Evidence tables?
No decision was taken as to how to develop this further for the moment.
The next face to face meeting of WP5 (and all other work packages) will be in Brussels on 14-15-16 November (dates to be confirmed by Jean Georges).
Page 52 of 88
10.1.3.2 Minutes of EUROCODE WP5 meeting in Brussels 06.11.06
Present: Rupert McShane, Brigitte Grass-Kapanke, Peter Tariska, and Sigurd Sparr
Apologies: Dymphna Hermans, Philip Scheltens, Mario Fioravanti
The main work was to
• define what guidelines should be included and excluded
• define the data items to be collected in the database of guidelines
• define the structure of the document/guideline we are to produce
• identify possible barriers to successful delivery
As well as general discussion, we each considered a separate guideline as a way of helping us to identify issues we would need to address. The texts we looked at were:
• Italian guideline
• SIGN guideline on BPSD
• ANA Practice parameter on vascular
• Canadian guideline on stroke
The next WP5 meeting is 26th February in Brussels
We agreed this would be preceded by an email in mid January (12th), reporting progress on
• List of guideline
• Preliminary database fields
• Recruitment of research worker
and a teleconference shortly after that (date to be arranged).
A draft report on the database is required for presentation at the Steering Group (WP leaders only) in Lisbon on 8th May.
Summary of conclusions
Database of guidelines
The first part of the project is to collate a database of existing guidelines. The data to be collected about each guideline, and recorded in database is to be based on the AGREE schedule for assessment of guidelines. An AGREE score is to be recorded for each guideline.
Guidelines to be included
1. Nationality • European • Non-European (English language only) • International = English language
2. Organization • Government • Professional • Voluntary sector • Commercial? Guidelines which are for insurance purposes only are not to be included
3. Currency – since 1995 or last one (European countries only). • Current • Superceded – ignore these
Page 53 of 88
• In development – do not ignore these if there is something concrete to review. But keep distinct in the database.
4. List of diagnoses covered • AD (include Downs), • VD, • PDD,DLB • Dementia NOS • MCI • Reversible dementias exclusion
5. Treatments to be covered • Anything which gets into the blood stream • Our remit does not include wider management such as Driving, finances, capacity etc
6. Populations • MCI • Mild • Moderate • Severe
7. Method for development of database • Systematic review of literature
i. Search strategy reported ii. What sort of literature: Published literature or beyond iii. QUORUM data will be reported
• Evidence rated according to quality using AGREE
Diagnosis-specific issues to be recorded in database
Considers definition of dementia
Considers definition of MCI
Educational bias issue
Distinguishes screening and diagnosis separately
Differentiation from normal and differential diagnosis
Data on specificities, sensitivities and accuracy are reported
Guidance on delivery of diagnosis included
Incremental benefit
History, Examination, Investigations
This is as far as we got. It is recognized that this is a very partial list of the issues relating to diagnosis that we would expect to be covered in the ideal guideline.
Overall objective specifically described:
Clinical questions covered specifically described
Health benefits, side-effects and risks have been considered in formulating the recommendations
Explicit link between recommendations and supporting evidence
Treatment-specific issues
Side effects and treatment effects
Effects on major domains as per Cochrane reviews
• Global, • Cognition, • ADL, • Behaviour, • QOL, • Pharmacoeconomics
Summary/composite meta-guideline

Page 54 of 88
We acknowledged that it would be counterproductive, impossible and outside our remit to replicate the literature reviews that have already been done in developing existing guidelines. Our aim is to construct a database of existing guidelines, report on their strengths and weaknesses, recommend the strong ones, and draw up a composite guideline based on the strongest aspects of each. The risk of plagiarism and copyright issues needs to be addressed by AE.
The AGREE structure for assessing guidelines is to be the frame for assessing others, and defining the structure of our own.
Proposed structure of the meta-guideline we will produce:
1. EUROCODE Meta-data a. Provenance
i. EUROCODE 1. AE 2. Panel selection : Not formal representative, but designed to include
wide variety of interested parties, including associations, professions, nationalities
b. Process i. Statement of method of developing consensus on AGREE score, and
description in database • 2 per paper: worker+group member. • Consensus discussion between the two • Disagreements come to the group. Consensus • EUROCODE • ?external experts for opinion especially where lack of consensus within
5 ?process for selection of these. ii. Channel for comments and criticisms
1. ?AE web site iii. Revision - mechanism
c. Definition i. Audience
1. Comprehensible to lay audience a. lay summary b. Ask AE about mechanism and timing of lay review of guideline
2. Clinicians a. Psychiatrists, Geriatricians, Neurologists, Psychologists,
Specialists nurses b. GPs
i. Screening – details of accuracy ii. When to refer
ii. Population 2. The database 3. Which guidelines do we recommend?
o Diagnosis Research Clinical Epidemiology / Screening
o Treatment o Weblinks?
3. The précis of recommendations we draw from our recommended guidelines a. Clinical Question Statement
i. Diagnostic criteria reliable? ii. Accurate for differential diagnosis
1. Neuropsych differentiation 2. Commentary: Special tests for special circumstances
a. Language/culture-free tests b. Downs
iii. Do lab tests improve accuracy 1. Structural 2. Quantitative structural 3. Functional

Page 55 of 88
4. CSF 5. Genetic biomarkers
iv. Comorbidities to be evaluated at initial assessment eg 1. Depression 2. B12, folate, syphilis
4. Treatment a. Dementia NOS b. MCI c. AD d. VD e. PDD/DLB
Page 56 of 88
10.1.3.3 Minutes of the working group meeting of 12 Movember 2007 in Brussels
Attendees: Rupert McShane, Amanda Kerr, Sigurd Sparr, Mario Fioravanti, Peter Tariska
Apologies: Brigitte Grass-Kapanke, Philip Scheltens
Eurocode Guideline Background
Discussion
RMc updated on progress so far.
• Description of guideline database,
• discussion of scope of project (to include all European and non-european guidelines from 2002-
2007, include only guidelines where dementia is the focus, include literature since 2005),
• discussion of quality rating of guidelines using AGREE tool (volunteers to rate guidelines to be
requested)
• discussion of possibly poor rating of EuroCoDe guideline using AGREE (due to limited nature of
membership of WP5, need consultation with wider group of stakeholders)
• discussion of peer review/consultation process, how to deal with conflicting views, how to reach
consensus, who should review
• presentation of potential rating schemes (see attachment). 2 basic types EFNS style (grade A,
grade B etc) AAN style (Standard, Guideline, Practice option). WP5 conclude to use AAN style
rating scheme for EuroCoDe guideline
• discussion of issues not covered in most guidelines
o drug holidays
o review periods
o stop rules
• discussion of format for guideline. RMc suggests recommendation followed by commentary to
cover conflicting guidelines, country specific issues, new research and other issues.
Action Items
• Suggestions requested for potential peer reviewers and external stakeholders (organizations
and individuals). WP5 to send suggestions to AK
• Volunteers and nominations to rate quality of guidelines using AGREE tool
Eurocode recommendations
Discussion
RMc and AK presented draft recommendations for discussion.
• Discussion of the following recommendations o 2.1.2.1.1 Cholinesterase Inhibitors for AD - recommendation approved o 2.1.2.1.2 Memantine for AD - recommendation approved discussion of memantine for
mild AD (WP5 state no), discussion of memantine in combination with cholinesterase inhibitors (no conclusion)
o 2.1.2.1.3 Other treatments for AD - recommendation should be split into treatment and prevention. RMc idenitifed new evidence that statins may be effective
Page 57 of 88
o 2.1.3 General Management of BPSD – update recommendation to stress need to front-line non-drug treatment with drug treatment for risky/dangerous situations. Myrra Vernooij joined to discuss Psychosocial Interventions WP. WP5 conclude to briefly refer to psychosocial interventions then refer users to Psychosocial Interventions work package for further information.
o 1.1.13 Blood Tests – update recommendation to include blood tests for lipids. Add that the primary care physician may order the blood tests prior to referral. Add as a practice option that syphilis, HIV and CJD tests may be ordered if there are specific indications
o 1.1.14 Neuroimaging - update recommendation to remove ‘subtype’ o 1.1.14.1 Structural imaging – update recommendation to remove ‘subtype’. General
discussion of benefits of CT and MRI. CT scan should be done as routine o 1.1.14.2 SPECT and PET – recommendation approved o 1.1.14.3 EEG – update recommendation specific indications (CJd, seizure disorders,
focal neurological deficits, encephalitis) o 1.1.15 CSF analysis – update recommendation, CSF analysis is not recommended as
part of the routine diagnostic work-up. If CJD or NPH is suspected then CSF analysis may be done.
o 1.1.16 Genetic testing – update recommendation. Genotyping is not recommended as part of the routine diagnostic work-up in dementia. If there is a clear family history (eg 2 family members with pre-senile dementia) then genotyping may be of value
Action items
AK to forward draft recommendations to WP5 for review
Peer review
Discussion
RMc call for suggestions on peer reviewers.
• Should reviewers be experts or generalists? – WP suggest some of both • Should reviewers review the whole document or sections – WP5 suggest overview the whole
document, focus review on specific sections
Call for suggestions of individuals and organizations to act as peer reviewers
Action Items
WP5 to nominate peer reviewers
Page 58 of 88
10.1.4 WP 7 Meetings
10.1.4.1 Working group meeting in Luxembourg (25-26 February, 2006)
Participants: Naja Skovgaard, Manuel Franco, Moniga, Esme Moniz-Cook, Sandrine Lavalle, Myrra Vernooij-Dassen. WP 6 members not present: Bob Woods, Anne-Sophie Rigaud
Research questions
The discussion focussed on research questions related to the development of guidelines and quality indicators on psycho-social interventions. The following questions were formulated:
• What is a psycho-social intervention? • Will the guidelines be general or will guidelines be made for specific intervention? • What will be the structure of the guidelines? • Who is going to use the guidelines? • Who are going to be the recipients of the guidelines and in which settings will the guidelines be
used? • Which interventions will be recommended? • What will be the recommended outcomes? • Are we going to prepare quality indicators? • What will be the dissemination plan?
Methodology
The proposed methodology to address these research questions is:
1. What is a psycho-social intervention? a. A literature research will be done on definitions used to describe psycho-social
intervention b. Expert discussion on description of psycho-social interventions
2. Will the guidelines be general? Expert discussion. 3. What will be the structure (chapters) of the guidelines?
a. Research on instructions on how to construct guidelines (AGREE etc.) b. Inventory of structure of national guidelines
4. Who is going to use the guidelines? Expert decision. 5. Who are going to be the recipients of the guidelines and in which setting will the guidelines be
used? Expert decision 6. What interventions will be recommended? Review of reviews. 7. What will be the outcomes? Review of reviews 8. Are we going to prepare quality indicators? Yes, methodology to be decided 9. What will be the dissemination plan? Yes, methodology to be decided
Preliminary results
• Decision: focus on general guidelines applicable to range of psycho-social interventions.
• Users of guidelines will be health care and social care workers.
• The recipients of the guidelines will be persons with dementia and their informal carers. Guidelines will be used in all settings.
Time schedule and division of tasks:
• A literature research on definitions used to describe psycho-social intervention: Researcher WP 6, July 2006
• Selection and study of existing guidelines. Deadline May 1 2006: o Naja Skovgaard: Finland, Sweden Denmark. o Esme Moniz-Cook: UK o Manuel Franco: Spain and Portugal o Sandrine Lavalle: France, Belgium. Network Alzheimer Europe o Myrra Vernooij-Dassen: The Netherlands, France
10.1.4.2 Working group meeting in Hull (24-25 March 2006)
Participants: Manuel Franco, Esme Moniz-Cook, Bob Woods, Myrra Vernooij-Dassen
Page 59 of 88
Aim of meeting: to clarify how to define general guidelines
It was agreed in Luxembourg that the guidelines should be general rather than giving specific recommendations. The guideline should be applicable to the range of psycho-social problems and interventions. This general level is new and there is no format which can be followed. There is a need for such a general guideline since systematic reviews indicated that no intervention is superior. Reviews suggest that psychosocial interventions should be directed at patients´ and carers´ specific problems and needs for care.
A general guideline considering this as a point of departure should indicate a) patients´ and carers´ needs; b) potential interventions; c) suggestions on how to identify needs for care and to make action plans acceptable for all those involved. Perspectives of those involved should be pulled together.
The needs to be considered relate to the domains of physical, psychological, social and spiritual aspects.
The interventions presented in the national guidelines can be judged using the indication for the level of evidence as used in Sign (see www. sign.ac.uk : guideline 86 on management of dementia patients and sign 50 on forming guideline recommendations, chapter 6 checklist).
Rather than building a guideline for a specific category of professionals, this guideline
is meant for use by all stakeholders. It should be potentially helpful for a specific patient. It can be used by professional and non-professional carers. It can empower people via the website.
The European perspective is gather and analyse guidelines in European countries and to find gaps in the availability of interventions per country.
10.1.4.3 Working group meeting in Paris (29 June 2006)
Participants
Bob Woods, Inge Cantegreil, Esme Moniz-Cook, Emmelyne Vasse, Rabih Chattat
Emmelyne Vasse is the researcher on this project.
Tasks
Guidelines
The guidelines should be gathered by the participants as agreed at the Luxembourg meeting.
The interest is the section on psychosocial interventions. This section should be translated into English, except for the German and the French guidelines.
In order to proceed the request, workpackage members are first asked to send the titles of the guidelines to Myrra Vernooij within one month and to send the translated parts before september 1.
• Selection and study of existing guidelines. o Naja Skovgaard: Finland, Sweden Denmark. o Esme Moniz-Cook: UK o Manuel Franco: Spain and Portugal o Sandrine Lavalle: France, Belgium. Network Alzheimer Europe o Myrra Vernooij-Dassen: The Netherlands o Inge Cantegreil, France and Germany
Literature reviews
Emmelyne started the literature study with a review on psychosocial interventions related to communication. The first results have been presented at the Alzheimer Europe conference. Reviews on reviews on carer and combined patient carer interventions will follow, as well as interventions aimed at staff.
Emmelyne will do a literature review on definitions of psychosocial interventions. Esme will send the relevant papers to Emmelyne or Myrra. (APA definition and related articles)
Theoretical models
• Reviews of theoretical models used in intervention studies. Emmelyne

Page 60 of 88
• Selection and very short description of theoretical models used by Interdem members, to start with the Eurocode group. All workpackage members. Submitting to Myrra before september 1.
Suggestion made in steering group meeting to add a special chapter on methodology. The steering group also underlines the importance of cultural differences among countries,. This confirms our ambitions.
Cultural background
Interdem members will be asked to respond on the cultural barriers and facilitators of the interventions selected for use.
Methodology
The limitations of the methodology used and a critical appraisal of current methodology (randomised controlled trial) will be presented in a special chapter as well as suggestions on how to adapt the methodology for use in dementia care studies.
Next meeting in november
• Preparation of a list of potential articles and responsibilities • Discusssion on results of review of reviews • Preliminary results on guideline study
Page 61 of 88
10.1.4.4 Working group meeting in Brussels (6 November 2006)
Participants present: Manuel Franco, Bob Woods, Esme Moniz-Cook, Myrra Vernooij-Dassen, Inge Cantegreil, Sandrine Lavallé, Pascale Dorenlot, Emmelyne Vasse
Guidelines across Europe, inventory results
All Interdem contacts across Europe were sent a request for searching guidelines on dementia in their country. Answers and/or guidelines were received from Finland, Denmark, UK, Netherlands, Germany, Belgium, France, Switzerland, Spain, Portugal, and Italy.
Pascale Dorenlot will do a last search for guidelines in Sweden, Italy, and Switzerland to complete the inventory.
The collected guidelines will be presented in a table that indicates if guidelines are policy driven or evidence-based and recommendations on psychosocial interventions will be compared with recommendations of systematic reviews.
Also, attention should be given to differences between European countries in the reimbursement of costs for implementing guidelines.
Theoretical models
A chapter of the final document will be dedicated to theoretical models for psychosocial interventions. Participants were asked to describe their “favourite” theoretical model in psychosocial research.
Bob Woods: Kitwood, rehabilitation concept
Esme Moniz-Cook: Stress coping adaptation models caregivers
Pascale Dorenlot: Not every intervention has a theory behind it. Practice based evidence also important
Manuel Franco: Multicomponent/multidisciplinair approach. Individualized interventions.
Inge Cantegreil: Stress coping model Psychotherapy after disclosure of diagnosis
Sandrine Lavallé: Importance of matching theory/model with environment of patient.
Myrra Vernooij: Family crisis/support model, Personal disease management needs patient
Milestones/Quality indicators
Besides European guidelines on psychosocial interventions it would be good to also add quality indicators based on the recommendations done in the guidelines. Manuel explained his work already done on the subject. It was agreed that the guidelines as well as the indicators should be general rather than recommending specific interventions. It was suggested to use the AGREE instrument for the appraisal of the final guidelines/quality indicators.
The process of developing the quality indicators will be explained in more detail at the next meeting.
Review of reviews
It was agreed to only use systematic reviews for the review of reviews. A document with systematic reviews found in Pubmed and Cochrane Library was handed out. No reviews were added/missed.
The next step will be to compare recommendations done in these reviews and compare these with recommendations done in the guidelines across Europe.
Bob suggested using the same strategy as Margaret Gatz did in her review.
Outcomes
Besides the outcomes that will be recommended by the Interdem outcomes workgroup, it is also important to focus on social and environmental outcomes.

Page 62 of 88
10.1.4.5 Minutes of the meeting of 26 February 2007 in Brussels
Participants: Myrra Vernooij-Dassen, Esme Moniz-Cook, Bob Woods, Sandrine Lavallé, Manuel Franco, Pablo Gomez, Pascalle Dorenlot, Martha De Sant’Anna, Emmelyne Vasse
Special guest Maurice O’Connell
Procedure development quality indicators
It was proposed to use the iterative consensus procedure for constructing quality indicators.
It was agreed to follow this procedure instead of the Rand modified Delphi because of its better fit to the time and possibilities we have within this project:
• two postal rounds of rating recommendations instead of face-to-face discussions • avoiding the organisation of face-to-face discussions in different European countries • using already gathered guidelines/recommendations as much as possible
Expert panels
It is important that we approach the opinion leaders in on the subject in each country involved. The experts will be asked to rate the recommendations on importance to European guidelines on psychosocial interventions.
Probably we can use the Interdem web page for the rating of core recommendations by experts. We should try to make an online version of the questionnaire to avoid paper work. Also, we could hand out questionnaires at the European Alzheimer congres in Portugal next May.
A set up of the questionnaire will be made and send to all members of the work group before May for corrections.
Countries involved in the procedure
Italy, Spain, Portugal, The Netherlands, Belgium, France, UK, Finland, Denmark, Sweden.
It will be tried to translate the questionnaire in the language of each country to be sure the ratings are reliable.
Discussion on core elements review of reviews
Brodaty: Caregivers, patient and carer, more intensive and ongoing.
Chung: conclusions already mentioned in recommendations
Clare: Woods: update of the review and the conclusion is still the same. Cognitive training is not effective. Cognitive rehabilitation no evidence available from RCT’s.
Cooke: social and cognitive components, multi-component is important.
Forbes: no evidence, not every intervention is suitable for every patient.
Heyn: some recommendation on physical activity (term to use)
Lee: depends on the quality of respite care and fits to the needs. No conclusion from RCT’s
So recommendation on expert consensus/discussion.
Livingston: methodology is not very good but it can be concluded that behavioural management are generally successful and staff training/caregiver training seem also successful. Individual approaches, recommendations on how to communicate with dementia patients for staff/caregivers.
Neal: no evidence so far.
Pusey: Individualized Psychosocial Interventions
Price: no evidence, environmental problems
Sorensen: multicomponent approaches
Teri: individualized
Thorgrimsen: not sure if the aromatherapy or the attention of the staff added to the effect.
Verkaik: no evidence available yet

Page 63 of 88
Vink: no conclusion can be drawn. Maybe promising because of five positive studies. But probably used in a tailored way.
Woods: despite the positive RCT’s no evidence because the poor quality of the studies. We have to look into it in more detail.
Discussion on core recommendations
Some important core recommendations for psychosocial care in dementia could be overlapping with the area of the WP on social support (e.g., case management, organisation of care). The meeting offered the possibility to immediately contact the WP group. There proved to be no overlap.
It was proposed that the structure in which the recommendations will be presented to the experts should be in outcome domains.
It is important to be clear about and agree on definitions of psychosocial terms used in recommendations. The definition for cognitive stimulation will be:
engagement in a range of activities and discussions (usually in a group) aimed at general enhancement of cognitive and social functioning. This is the definition is used in the Cochrane protocol for a review on “Cognitive stimulation to improve cognitive functioning in people with dementia” (Woods et al, 2005).

Page 64 of 88
10.1.4.6 Minutes of the meeting of 12 November in Brussels
Participants: Manuel Franco, Myrra Vernooij-Dassen , Pascale Dorenlot, Esme Moniz-Cook, Inge Cantegreil-Kallen, Bob Woods, Emmelyne Vasse
Today’s plan
During our workgroup sessions we are going to rate the quality of the SIGN and Italian guidelines with the AGREE instrument. Afterwards we will discuss and reach consensus on each item.
Rating other guidelines with AGREE
Guidelines that are not written in English will also be rated with AGREE. In case there are several guidelines available in a country, the most recent ones should be choosen. Also, the guidelines should give broad attention to psychosocial interventions.
Spanish guidelines raters: Manuel, Marisol (Alzheimer Centre Nijmegen)
German guidelines raters: Inge, Pascale, Raymond (Alzheimer Centre Nijmegen)
NICE guideline raters: Esme, Pascale
Dutch guideline raters: Emmelyne, Myrra
Quality consensus discussion
The ratings will be solely based on the sections on psychosocial interventions. Other sections in the guidelines were not considered during the consensus procedure, except for the more general quality questions like stakeholder involvement.
SIGN
Scope and purpose (1-3)
1. The remit to guideline, very brief not very specified. This is an update of earlier
guideline. Manuel scores 4, Pascale 3: Overall objective is clear but short. Depends on the purpose of use. No overall clear specific aim for psychosocial interventions.
Look at overall objective if not mentioned than look at chapter which mentions the psychosocial
interventions. (2)
2. To general in clinical way and to general for application to caregiving. Some items are quite specific but others are not very clear and specific. Its varying. The recommendations were developed the wrong way around. They do not start with a clinical question but start from the evidence from literature.
Overall: real outcome benefits are not mentioned. The question is not clear enough for the psychosocial interventions part. (2)
3. There is not a clear statement on age but they make a statement about all stages and all types of dementia. They describe and define different kinds of dementia. (4)
Stakeholder involvement (4-7)
4. There were a lot of medical doctors in the group. No representative of social aspects of care. Lack of social influences. (3)
5. Nothing found about that. It is not explicitly mentioned, it is not stated. (1)
Mentioned in the introduction of development group but that’s it.
6. Not explicitly mentioned, it is assumed but not mentioned. (1)
7. Because of previous arguments (1)
Rigour of development (8-14)
8. Agreement (4)
9. Agreement (4). It is on the website.
10. There is confusion within the workgroup about the evidence or the criteria for level of evidence grades. No specific statements on how difficulties in the development group were solved. The criteria
Page 65 of 88
for selecting evidence are clear but how it actually worked out in the development group is not mentioned at all. We know how they planned to do it but are not sure if consensus was reached according to plan in the group process (2) 11. It is mentioned but not very specific. In general they considered it (3)
12. Agreement (4)
13. Not any patient representatives and not clear what happened with the comments, no description on methodology. (3)
14. Agreement (4), section 1.6
Clarity and presentation (15-18)
15. Most of the time to general. Not pinned down to setting or group of dementia patients. Not clear for who it was for. (3)
16. They did not make recommendations on specific issues but on interventions.
Confusion about the question interpretation. It is not focused on problems but mentions only options. It is not clear when these options should be used. There is no hierarchie in the chapter for psychosocial interventions. The original question is to vague so they mention options but are not clear enough about
specific groups (3)
17. Agreement (4)
18. Nothing on psychosocial interventions especially (1)
Applicability (19-21)
19. Introduction on general application, implementation (2)
20. Some things are mentioned in general. About psychosocial interventions there is not very specific information (2)
21. In section 6.3 it is mentioned, no consensus was reached some rated (3), others (2)
Editorial independence (22-23)
22. Many people involved but NHS directors are also involved (2)
23. It is stated that declarations of interest were made. Agreement (4).
Overall: Recommend.
It is not enough specified for specific groups of dementia patients and settings. Psychosocial interventions are not ignored but could be mentioned in context of certain groups of dementia patients or certain specific settings.
Italian guidelines
Scope and purpose (1-3)
1. Psychosocial perspective: broad about treatment but not a clear aim. (2)
2. In the introduction it was adressed but not detailed enough. (3)
3. Not very explicit/specific but it is mentioned. Attention is given to different types of dementia and possible interventions, table 3. (3)
Stakeholder involvement (4-7)
4. No social people. Not all relevant professional groups are presented. Not clear who the authors are. (2)
5. Alzheimer association has reviewed it but nothing more is mentioned about it (2).
6. Agreement (4)
7. Not mentioned at all (1)
Rigour of development (8-14)
8. A systematic procedure is mentioned but this is not very detailed. Methodology is clear but not how they have used the method (3)
9. Agreement on (4) although real details are lacking.

Page 66 of 88
10. Not clear how consensus in group was reached (2)
11. Agreement (1)
12. Agreement (4)
13. Approved by steering committee but this is not a very good process of reviewing (2).
14. Agreement (1)
Clarity and presentation (15-18)
15. Same as SIGN, no specific groups or settings are mentioned. (3)
16. It is to general (2)
17. They are in a table but not very easy to find in the text. (3)
18. Agreement (1)
Applicability (19-21)
19. Something mentioned about it but not sufficient (2)
20. Not mentioned (1)
21. Nothing mentioned, agreement (1)
Editorial independence (22-23)
22. Unconditional grant was mentioned, still a bit suspicious (3)
23. Agreement (1)
Overall: Would not recommend
This is because the psychosocial part is not as broad enough as the pharmacological part of the guideline. There is more evidence available but this was not included at all in the guideline. It is therefore biased for pharamcological interventions.
Discussion on proposed articles
Guideline inventory: National differences might not be very good to focus on because the focus of the guidelines also depends on the writers/developers and not of differences between countries. Everyone probably uses the same literature and research.
It is a good idea to start with abstracts and set-up of the articles. Everyone can see which data is going to be used in which articles. All workgroup members can then choose to which articles they want to contribute.
Consensus workgroup meetings are needed for:
• Comparison guidelines national differences • Delphi procedure: Consensus for recommendations based on results expert questionnaires
Consensus on quality indicators based on the recommendations
Page 67 of 88
10.1.5 WP 8 Meetings
10.1.5.1 Conclusions from the group meeting of WP8, Luxembourg Feb 25
and work that should be started before the next group meeting in November later this year.
Participants: Anders Wimo, Hannu Valtonen, David McDaid, Krisztian Karpati, Alan Jacques, Annette Dumas.
Absent: Linus Jönsson, Laszlo Gulacsi.
1. Anders Wimo and Linus Jönsson will present a methodological background to COI-studies.
2. Anders Wimo and Linus Jönsson will have the main responsibility for the literature review of what is written about the cost of illness of dementia/AD with a focus on European studies. The presented costs in the studies will, if possible be divided into cost categories (e.g. direct medical costs, direct non-medical costs, indirect costs-informal care etc). AW and LJ will distribute the literature list to the other members of the WP. If it is OK from the Swedish HTA organisation SBU, AW will distribute the section of COI and cost-effectiveness to the group members (and to Rupert McShane in WP5).
Since WP4 will describe available resources for dementia care in the different EU countries, AW will have contact with the WP leader of this group.
3. Hannu Valtonen will present a background of welfare theory, utilization of resources occur in care systems including a theoretical discussion in terms of the relation between demands and supplies of care and needs of care and how resources are allocated. Our task is not to analyse cost-effectiveness studies, but we can discuss how much welfare that can be produced, given the resources. Hannu will also present a background theory for costing (opportunity costs, cost categories (e.g. in terms of direct medical resources, direct non medical resources, indirect costs, informal care.)
4. David McDaid will review informal care (quantification, costing), both in methodological terms and what is written about it in dementia care.
5. David will send an internet reference to a report (from WHO?) where the number of health care resources and long term institutional care is described in most European countries. The focus will be not only on present EU members states but also on potential new members. The information about community services is probably more limited. The next step, to identify to what extent resources are utilized by demented is more difficult. Population based studies may be a source. David also has a source in a project he was involved in where expenditures on mental disorders in official terms can be contrasted to the calculated economical burden.
David also has another source: European services mapping schedule, contact person: Louis Salvador. This source describes different resources for the mentally handicapped in Europe, unclear whether dementia is included.
6. Krisztian Karpati will discuss further details with Laszlo Gulacsi about the planned questionnaire, where data about resource utilization of demented in Hungary will be collected. If possible, a staging of the patents in terms of dementia severity would be an advantage. It would probably be difficult to identify the proportion of demented in Hungarian nursing homes. Krisztian and Laszlo will also contact collegues in other parts of Eastern Europe regarding resource utilization/cost studies of dementia/AD in these countries.
7. We also discussed the possibilities to present data that could be of value for policy discussions in Alzheimer Europe and with EU. Alan Jaques and Annette Dumas from AE stressed the need for information about the socioeconomic impact of younger people with dementia (both on the demented persons themselves and the nexts of kin). They also stressed the need for projections of future costs and the need for information of how many demented that live alone in different parts of Europe. Another important topic is alcohol related dementia even if it is difficult to get any figures of the economic impact.
Other issues are that a description of available resources for dementia care (such as day care, long term institutional care, special living arrangements for dementia, diagnostic resources) in the EU and how they are utilized (not necessarily costed). There are probably utilized in different ways in Europe and the relation between different formal resources and informal care is different to highlight. Even if it is not WP8:s task to present recommendations, the highlighting of differences are important. It is also of interest to present information to what extent resources are paid by the state/the public system and out of pocket by patients and nexts of kin. David has such information (?).

Page 68 of 88
8. If it is judged as important to make investments in some kind of care in a country where this resource is limited/lacking, a special infrastructure for this resource (in its wide context: education-competence, buildings tec) may be needed with an investment cost, that need to be considered.
It was also considered as interesting to highlight the consequences of changes in transfer systems. With a societal perspective and with an opportunity cost approach, the net effect of transfers is zero, but it may be of interest for policy makers to have information on the effects on different parts of the care system.
9. Some new approaches were interesting, such as a system of vouchers to patients/caregivers (corresponding to 2/3 or 100% of residential care) in the Netherland (and UK??).
10. Alan Jacques from AE will write a short text about “what is unique with dementia in terms of use of resources”. Alan will also check whether AE has information of the sellings and perhaps use (in terms of e g Defined daily doses DDDs) of the “antidementia drugs” (cholinesterase inhibitors, memantine) in the different EU countries. Otherwise AW will try to get this information, perhaps via EMEA. Alan J will also send an e-mail through the AE network in EU and ask for local and national studies (not available in Medline/Pubmed or similar) regarding dementia studies of costs, resource utilization and perhaps care organisation. If these studies are in the local languages, there is such competence in the group (Hannu in German, Krisztian in German, Annette Dumas in French, David in Spanish etc).
11. We do not know to what extent people with dementia are diagnosed in Europe. One option could be to present the content of a basic diagnostic investigation of suspected dementia and if it then is assumed that, say, 80% of the incident cases would be identified, what is the cost for this in different countries (with country specific costs) of Europe. This approach assumes that country specific incidence data are available in EU. It also assumes that time use and use of other resources are similar (there are probably local-national-inter national variations in the effectiveness of the diagnostic process). AW will first communicate with WP5 regarding the diagnostic approach and then circulate it in our WP8. One policy approach could be to compare the estimate of diagnostic costs with the estimated total societal costs of dementia.
10.1.5.2 Conclusion from the EuroCoDe meeting in Brussels, WP8, Socio-economic impact, Nov 6, 2006.
Participants: Anders Wimo, David McDaid, Hannu Valtonen, Anders Gustavson (replacing Linus Jönsson), Alan Jaques, Paul Kenigsberg (new working member of the group)
Absent: Laszlo Gulacsi
The work in WP8 is proceeding well and as reported on the meeting, we will succeed in keeping the deadlines and deliverables. WP is also in need for later collaboration with particularly WP 4 (social support systems) and WP 7 (prevalence rates).
Specific tasks for group members
1. ALL: deadlines
a. Financial report: to Jean Georges
Jan 31 2007
Jan 31 2008
Feb 28 2009
The period for the first economic report is Jan 1, 2006 to December 31, 2006. This means that ASAP when the new year begins, you should start to prepare the report to Jean. I refer to the document that was presented by Jean Georges at the meeting.
b. Activity report: to Anders Wimo
The period for the first activity report is Jan 1, 2006 to December 31, 2006. Send activity report to Anders Wimo, who will edit it and send it to Jean Georges who needs it before Jan 31, 2007. This means that you should send it to Anders Wimo as early as possible in January 2007. It should include a brief report of what you have done so far , including the results of literature review (including references of papers, if possible with Endnote format).
Deliverable 1. 18 months from start Jan 1, 2006. In spring 2007: send 1st report of results of work.
Jan 31 2008
Page 69 of 88
Feb 28 2009
2. Specific task for group members as discussed on the meeting
Anders Wimo, Linus Jönsson, Anders Gutavsson:
Present a definition of socioeconomic impact as defined in application and also definition(s) of cost of illness.
Present estimates of cost of illness of dementia in Europe, based on costing models, such as EBC, DWCD but also an update of published COI studies.
Send the EBC report to members of WP8.
Send references about informal care from the Swedish SBU report´s database to David McDaid (with cc to others).
Present available results regarding differences in costs of different types of dementia, such as AD, VaD, PDD.
Present costs of dementia diagnostics from two levels: basic diagnostics and extended diagnostics at the specialist level.
Reflect whether forecasts of cost of illness figures should be presented, based on demographic changes and assumptions of e.g similar cost patterns in the whole Europe as in the country with the highest COI per case.
Hannu Valtonen:
Classifie European countries health care and social care systems such as “Nordic welfare system”, “Family based systems (Germany?)”, “Market oriented systems” or something similar.
Comment on especially David´s work on informal care
David McDaid
Literature search with an update on informal care
Send us Search strategy in MESH terms
Describe costing methods of informal care
Discuss “new” components of informal care such as immigrants from eg Eastern Europe, Philippines, North Africa and real “black market” carers vs traditional carers such as spouses, children.
Describe a coming(?) voucher system in the UK?
Paper by Richard Harvey about the consequences of early onset dementia.
Quantitative data on informal care should be presented, but reflect whether costs for informal care should be calculated or not and if yes: how such data will be presented.
Alan Jacques
Use Alzheimer Europe´s network to describe care organisation for dementia in the different European countries
Describe the consequences for early onset of dementia for the families: lost income, costs of care etc.
Discuss the most important care activity if priorities must be set: early diagnostics? Quality of care?
Paul Kenigsberg
Send short CV to Anders Wimo
Make search in French databases regarding the socio-economic impact of dementia.
Organise translations of papers in French, but also Geerman and Italian.
Describe French system with taxation relief if private staff is employed to do social care (not nursing).
Make database search regarding differences in dementia care due to rural/urban living but also due to different socioeconomic status of patients and caregivers. Discuss search strategy with David.
Discuss the influence of disability and economic allowance from society due to that.
Present a simple figure for theory of change (based on hypothesis, identification of problems etc)

Page 70 of 88
Lazslo Gulasci (Absent on meeting)
Present Eastern Europe patterns of dementia care.
LATER:
ALL: discuss methodological issues (informal care, comorbidity, younger demented, different care systems, rural/urban areas, Eastern Europe, diagnostics, migration)
ALL: discuss policy implications for presented figures : differences between countries/regions vs how care is organised. Recommendations for future research.
ALL: discuss with other WPs, particularly WP 4 and 7.
10.1.5.3 Minutes of the meeting of 26 February 2007 in Brussels
Participants: Anders Wimo, David McDaid, Alan Jaques, Paul Kenigsberg
Absent: Laszlo Gulacsi, Linus Jönsson, Hannu Valtonen
The work in WP8 is proceeding well and the deadline for first activity report was held successfully.
WP is also in need for later collaboration with particularly WP 4 (social support systems) and WP 7 (prevalence rates). Preliminary we plan to meet in Portugal in May.
Anders will check the dates for the next delivery deadline.
An outline for the final report of WP8 was discussed:
• Background, aims for the work of WP8: Anders Wimo
• General methodological introduction – economics, health economics, care systems: Hannu Valtonen
• Overview of specific methodological issues regarding cost of illness and dementia in Europé (e.g. informal care, comorbidity, younger demented, different care systems, rural/urban areas, Eastern Europé and other regional differences, diagnostics): ALL
• Informal care: David McDaid
• Demograhics and migration (coordinate with WP4)
• Specific country/region presentations: Eastern Europe: László Gulácsi,
France: Paul Kenigsberg. Sweden: Anders Wimo. UK/England?: David McDaid. Scotland? Alan J. Finland: Hannu Valtonen ,
• Urban vs rural /health geography areas. Paul Kenigsberg ? David? (may be problematic)
• Younger demented: Alan Jaques?
• Cost of illness of dementia in Europe: Anders Wimo, Linus Jönsson
• Impact of results: methodological and in policy terms, discuss policy implications for presented figures : differences between countries/regions vs how care is organised, early diagnostics? Recommendations for future research: all’
• Coordination: WP4 (social support systems) and WP7 (prevalence)
“Europe” needs clarification. EU 25/27? Whole continent of Europe? Candidate countries for EU? Countries with association agreements with EU?
We will try to get country specific data regarding some basic issues. We need to coordinate this with WP 4 but David and Linus are also members of a group, Mental health economics Europe where the following issues may be raised:
How is long term care paid?
Out of pocket share for different kinds of care?
Carer allowance payment to informal carers?
Number of institutional beds per e.g. 1000 65+?
Dementia share in institutions?
Page 71 of 88
Tax systems and financing?
Something about barriers for care??
The major cost drivers in dementia care are costs of institutional care (by the way, what is an institution?) and informal care and the interaction and trade offs between these two components. One crucial issue is the situation when a decision about institutionalisation or not under discussion. Important aspects are the discussions about ”freedom to choose” where to live and where to be cared for, of course the situation for the demented person (cognition, ADLs, behaviour) and the carer(exhaustion etc), the availability of institutional beds (numbers, decision rules, legal aspects), the out of pocket proportion and who is paying for care, how are the institutions run (public, private etc), what happens if incentives change on a country level? etc etc
Regarding informal care, a new aspect is the migration of informal hidden “black market paid” carers from e.g. Eastern Europe.
Another migration issue is that many retired people move to other countries and stay there for long periods. Who has the responsibility of care for these people?
Since WP8 has representatives from several European countries (Sweden, Finland, France, Hungary, UK) there are opportunities for deeper presentations of resource use and costing issues from these countries in the final report.
Another EU project is dealing with institutional care (lead by Jim Mansell from Kent ) Comparative cost analysis……… It will perhaps be possible to get information about institutional care costs (e.g. per day) from different countries. David will check the link to the report.
Cost of diagnostics will be overviewed. Anders will check the guidelines from the EFNS regarding diagnostics and some costing examples, based on key countries, will be presented. The cost effectiveness of diagnostics (costs per true positive case and perhaps costs per missed true case) will not be possible to analyse, but the issue may be highlighted. It should also be clarified that this part has nothing to do with the mass-screening issue.
The influence of comorbidities on the costs will need to be discussed in terms of gross and net costs.
Although not the task for WP8, since dementia shortens life, the effects of potential interventions on prevalence and costs will be discussed. Will a potential life prolonging (as a result of an intervention) appear in the early phase of dementia (when the patient lives at home) or in the endstage, when most patients are institutionalized. David knows about a modelling paper from the LSE where effects of treatment of AD is built in (in terms of costs of institutional care)
Anders Wimo and Linus Jönsson will contact Laszlo Gulacsi to discuss the Eastern Europe part of WP8.
Anders Wimo and Linus Jönsson will also continue with the review of European COI papers. (including also papers on costs of different levels of dementia severity). The following cost classification will be used: Direct medical costs, direct non medical costs, costs of informal care, indirect costs (production losses of patients). If possible, out of pocket issues will be highlighted. Otherwise it was regarded as problematic to cover the care financing/reimbursement/transfer issues from a European perspective (discuss with WP4).
Alan Jaques will write a section about the socio economic impact regarding younger persons with dementia.
We was also informed about a forthcoming report from Marin Knapp et al regarding the COI of dementia in the UK that will be presented within a few days.
Alan stressed the need to include costs for repeated assessments needs evaluations during the course of dementia.
Alan also reported that he had sent questions about “hidden” or “unknown” studies to the European network, but nothing of value was found.
Paul raised the question whether mental disability/cognitive decline is taken into account when decisions about allowance/remuneration or similar are made.
The issue of technical progress (e.g. telemedicine? Monitoring devises in homes? GPS, alarms etc?) was raised. Although this probably will have a great potential for the future (better “freedom” for patients, less staff need etc) there are hardly any costing or cost effectiveness studies so far, but Anders W will at least make a Pubmed search.

Page 72 of 88
10.1.5.4 Minutes of the meeting of 12 November 2007 in Brussels
Participants: Anders Wimo, David McDaid, Paul Kenigsberg, Laszlo Gulacsi, Krisztian Karpati
Absent:, Linus Jönsson, Hannu Valtonen
Alan Jaques has retired(many thanks for his work in the group)
The work in WP8 is proceeding well and the first interim report was approved.
1. Deadlines etc
The next deadline for financial reporting is January 31, 2008. Each center reports directly to Jean Georges.
For the 2nd interim report, the deadline is the same, Jan 31, 2008. To make it possible for the WP8 leader Anders Wimo to edit the interim report, each WP8 center must send their reports no later than January 15 to Anders Wimo.
The deadline for final consensus report is February 28, 2009. For practical reasons it is strongly recommended that each WP finalize their work no later than Dec 31, 2008.
For WP 8 it is strongly recommended that the 1st manuscript drafts for the WP8 centers contributions are sent to Anders Wimo no later than June 23, 2008.
The next meeting for WP8 will be on March 31, 2008 in Brussels.
The next steering committee meeting will be on May 25, 2008 in Oslo.
The final presentation of the results of the whole project will be on December 9, 2008 in Brussels.
2. WP8 progress
The meeting focused on the 2nd interim report. There is an outline for the final report and the 2nd interim report will be based on this outline. The comprehensive literature search for the 1st interim report will be updated.
Although there should be an internal review and feed-back discussions for the separate parts of the WP8 report, there are designated key persons for each part of the outline (underlined).
Outline for the final WP8 report (somewhat edited).
1. Background, aims (Anders Wimo)
2. General methodological introduction – economics, health economics, health and social care systems (Hannu Valtonen)
3. Overview of specific methodological issues regarding cost of illness (COI) and dementia in Europe (Anders Wimo, Linus Jönsson)
4. Methodological issues and available results regarding the major cost drivers: Informal care (David McDaid) and long term institutional care (Anders Wimo)
5. Specific country/region presentations: Eastern Europé (Laszlo Gulacsi, Krisztian Karpati) and Southern Europe/France (Paul Kenigsberg, David McDaid)
6. Estimates of the costs of illness of dementia in EU (Anders Wimo, Linus Jönsson)
7. Impact of results: Methodological and in policy terms. Recommendations for future research. Policy making issues on EU level and country level (all)
Comments:
2. Hannu Valtonen will be addressed whether the overview also includes social care systems and not only health care systems. The group stressed the need also to include aspects on social care systems since a great part of dementia care is taking part there. David McDaid may give some input here.
3. Despite general issues of cost of illness, such as bottom up/ top down approaches, prevalence/incidence based designs, different cost items that are important for the COI of dementia will be discussed, such as prevalence figures. The overview will also highlight, although not systematically review or include, the possibility also to include aspects of burden of illness and not only cost of illness. Burden of illness may e.g. include the QALY and DALY concepts. Another issue is costs of diagnostic

Page 73 of 88
activities. The AE network (via Dianne Grove) will be addressed questions about e.g. the proportion of incident cases of dementia that undergo diagnostic procedures.
4. This section will i.a. review the current literature on informal care in terms of quantitative figures (e.g. hours per day) but also highlight the methodological issues regarding quantification and costing of informal care. Anders Wimo will highlight the conceptual issues regarding institutional care. He has had a fruitful communication with Dianne Grove in WP4 regarding the estimated proportion of demented in institutional care and costs of institutional care in different EU countries. Another issue is the number of institutional beds in different EU countries.
5. There is a Hungarian project ongoing with a cooperation will representatives from the Ministry of Health and also a questionnaire to GPs. This will probably end up in a comprehensive report regarding resource use of demented in hospitals and in family practice as well as regarding informal care. There is also a cooperation with the University of Vienna (prof Auguste Oesterie ?) and there is hope also to get information from Romania and some other countries in Eastern Europe. There will also be a general presentation of care patterns in Eastern Europe.
Besides the focus on France, Paul K will also together with David McDaid briefly highlight care patterns in Southern Europe, such as family oriented care.
6. The COI estimates will be presented from different methodological viewpoints (e.g literature based review with bottom up and top down figures, modelling approaches).
Cost estimates will be presented for the whole EU, Europe, regions and specific countries.
7. A general discussion/summary of the methodological issues as well as the need for different research activities will be included. Which costs of dementia can be avoidable by prevention (life style, treatment etc). This is similar to the discussion of how much the prevalence of dementia that can be postponed/prevented by treatment actions. Different effect on different types of dementia? Another issue to discuss whether there may be prevention effects on carers in monetary terms. Another issue to be highlighted is the different costing perspectives from a EU perspective.
Since cost effectiveness NOT was on the agenda for this group, such results will not be presented. However, in the discussion there may be references to such reviews, e.g. by the Swedish SBU or NICE in the UK with a brief presentation of results (this point was suggested to me during the plenary discussion after the group meeting).
Page 74 of 88
10.1.6 WP 9 Meetings
10.1.6.1 Minutes of EuroCode WP9 meeting in Luxemburg 25 – 26.02.2006
1. Present: Jim Jackson, Tiia Ngandu, Lutz Frölich
2. Absent: Istvan Degrell, Heike von Lützau-Hohlbein, Frans Verhey
Month 1:
According to our milestones, we have finalized the research methodology and have detailed the content of the literature search.
Month 1: Methodology finalization at meeting:
We will screen world-wide studies not only European and we will search public databases, e.g. PubMed. We will draw on textbooks for identification of risk factors, and include data from reports which are available to WP members (e.g. SBU report from Miia Kivipelto).
We will restrict ourselves to a detailed report on “Treatable” risk factors and only mention briefly “Non-treatable” risk factors. This means that we will review the data only on those risk factors amenable to intervention and in the second part, will review the intervention studies on those risk factors. A brief table will be devoted to non-treatable risk factors.
As a first step, we have identified the following potential risk factors (list not complete):
Alcohol / smoking / occupation-dependent risk factors / physiological / pathophysiological risk factors / Activity dependent risk factors / Nutrition dependent risk factors
It was decided that several points are to be explained:
Definitions: Risk factors and prevention (primary, secondary, tertiary prevention).
We will deal only with primary and sexondary prevention intervention studies (diagnosis, methodology). Specific methodological problems of intervention studies in dementia shall be made clear. Level of evidence for intervnetion studies. Specific problems of outcome criteria.
Explanation of efficacy of intervnetions: “attributable risk” (ANDREAS SEIDLER as consulatant)
Alcohol as a risk factor / protective factor in dementia and the diagnosis of alcohol-dementia (ISTVAN?)
The problem of MCI will be dealt with by the WP on diagnosis/treatment, not by our WP.

Page 75 of 88
10.1.6.2 Minutes of WP 9 meeting in Brussels on 6/11/2’’6
Present: Frans Verhey, Jim Jackson, Heike von Lützau-Holbein
The following comments were made on the individual slides:
• Incident and prevalence increase with age up to age 85 (slide 6), if there is a levelling off at this
age, this will have implications for the Prevention WP
• Familial aggregation (slide 7), need to explain very clearly that this is increased risk and not
inevitable, we would also add that genetic testing should not be routinely offered because it is
difficult for people to use the revealed information, also noted that there is no simple test to
assess risk.
• Diabetes (slide 8), this is a rapidly changing field, therefore there is a particular need to keep up
with the latest information, should risk factors for diabetes be listed as risk factors for dementia?
Does well regulated diabetes reduce risk for dementia?
• Hypertension (slide 8), is there any evidence for intervention studies?
• Cardiovascular disease – also need to cover cerebrovascular illness (see the Rotterdam study)
• Folate/vitaminB12 (slide9), needs explanation as in Good for you, good for your brain.
• Inflammatory factors (slide 10), needs cross reference to later statement that side effects made
this not suitable for treatment
• Aluminium (slide 10), it could state that no evidence has been found of this effect, it was an
artifact in the original study
• Obesity and nutrition (slide 11), needs to keep in touch with the latest studies
• Smoking (slide11), more could be said including the link with cerebrovascualar disease
• Occupational exposure (slide 12), add pesticides
• Low level occupation etc (slide12), cross reference to higher education (slide 14), also consider
social-economic explanations
• NSAIDs (slide 13), we felt the statement may be too positive, one trial discontinued because of
side-effects, also the reference mentioned may not be the right one
• Under pharmacological factors (slide13), there also ought to be statements about lithium and
cortisone, both would not be recommended as dementia therapies
• Alcohol (slide14) , need to explain light/moderate drinking – be more specific about the number
of glasses
• Leisure time activities (slide 14) could be expanded to include mental stimulation and social
activities
• Summary (slide 15), need to explain that it is worthwhile following the recommendations even
though the evidence is only moderately strong

Page 76 of 88
• Some doubts about omega-3 oil and fish because although good for you, the dementia
evidence is not strong.
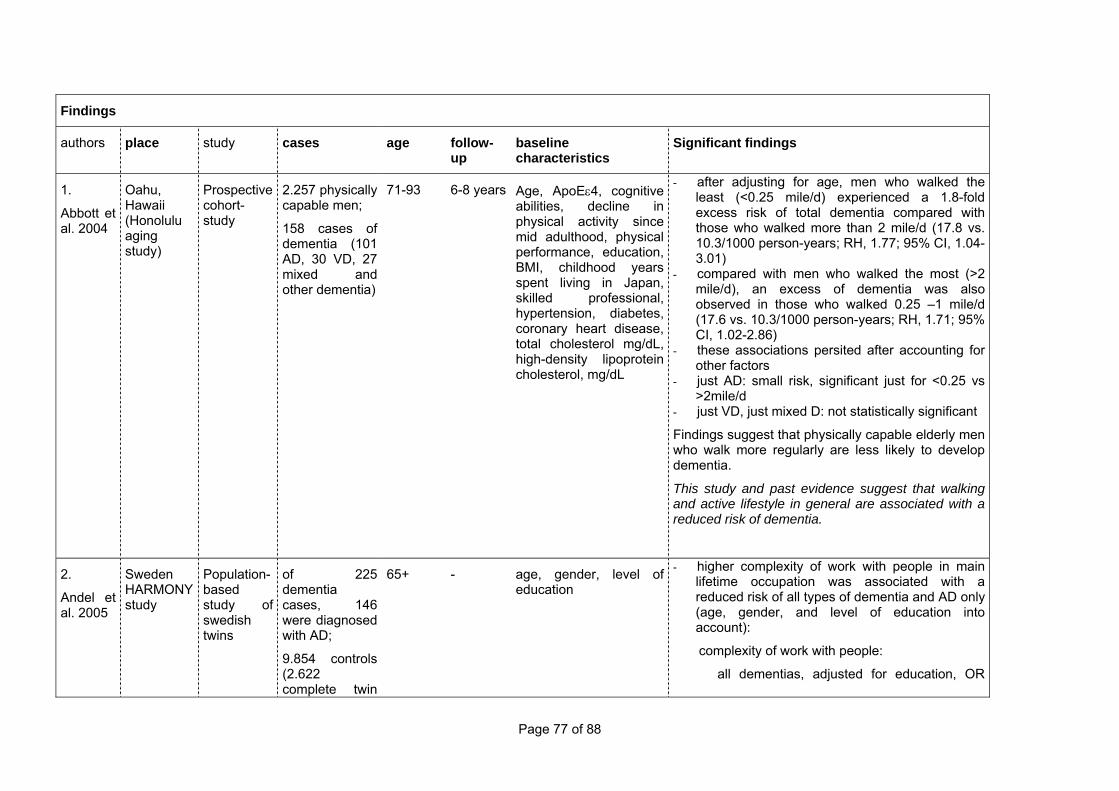
Page 77 of 88
Findings
authors place study cases age follow-up
baseline characteristics
Significant findings
1.
Abbott et al. 2004
Oahu, Hawaii (Honolulu aging study)
Prospective cohort-study
2.257 physically capable men;
158 cases of dementia (101 AD, 30 VD, 27 mixed and other dementia)
71-93 6-8 years Age, ApoEε4, cognitive abilities, decline in physical activity since mid adulthood, physical performance, education, BMI, childhood years spent living in Japan, skilled professional, hypertension, diabetes, coronary heart disease, total cholesterol mg/dL, high-density lipoprotein cholesterol, mg/dL
- after adjusting for age, men who walked the least (<0.25 mile/d) experienced a 1.8-fold excess risk of total dementia compared with those who walked more than 2 mile/d (17.8 vs. 10.3/1000 person-years; RH, 1.77; 95% CI, 1.04-3.01)
- compared with men who walked the most (>2 mile/d), an excess of dementia was also observed in those who walked 0.25 –1 mile/d (17.6 vs. 10.3/1000 person-years; RH, 1.71; 95% CI, 1.02-2.86)
- these associations persited after accounting for other factors
- just AD: small risk, significant just for <0.25 vs >2mile/d
- just VD, just mixed D: not statistically significant
Findings suggest that physically capable elderly men who walk more regularly are less likely to develop dementia.
This study and past evidence suggest that walking and active lifestyle in general are associated with a reduced risk of dementia.
2.
Andel et al. 2005
Sweden HARMONY study
Population-based study of swedish twins
of 225 dementia cases, 146 were diagnosed with AD;
9.854 controls (2.622 complete twin
65+ - age, gender, level of education
- higher complexity of work with people in main lifetime occupation was associated with a reduced risk of all types of dementia and AD only (age, gender, and level of education into account):
complexity of work with people:
all dementias, adjusted for education, OR

Page 78 of 88
pairs, 4.835 individuals)
0.86,
95%, CI, 0.76-0.98
AD, adjusted for education, OR 0.83, 95%, CI,
0.70-0.98 (same for twins: complexity with people:
all dementias OR 0.47, 95%, CI, 0.25-0.88; AD only
OR 0.05, 95%, CI, 0.01-0.35)
- other complexity dimensions, like complexity of work with data, showed no significant associations
Findings suggest that greater complexity of work, and paricularly complex work with people, may reduce the risk of AD.
3.
Bäckman et al. 2003
Stockholm Sweden, Kungsholmen
Prospective cohort-study
230 non-demented at baseline, diagnosed with AD at a 3-year follow-up
75+ 3 years Predictor variables:
age, sex, years of education, previous and recent diseases, ApoE status, blood pressure, depression, vitamin B12, social network, substance use
- significant change in MMSE score between baseline and follow-up (t(229)=18.28 and p < .001)
- mean MMSE score was 25.20 (SD=2.87) at baseline and 19.32 (SD=5.27) at follow-up
- only number of diseases resulting in hospital admission during the follow-up period made an independent contribution to rate of MMSE change (p<.001)
- increasing age and number of disease resulting in hospital admission between baseline and follow-up were associated with a more rapid rate of cognitive decline
- number of recent diseases was related to rate of cognitive decline independent of age, whereas the reverse was not true
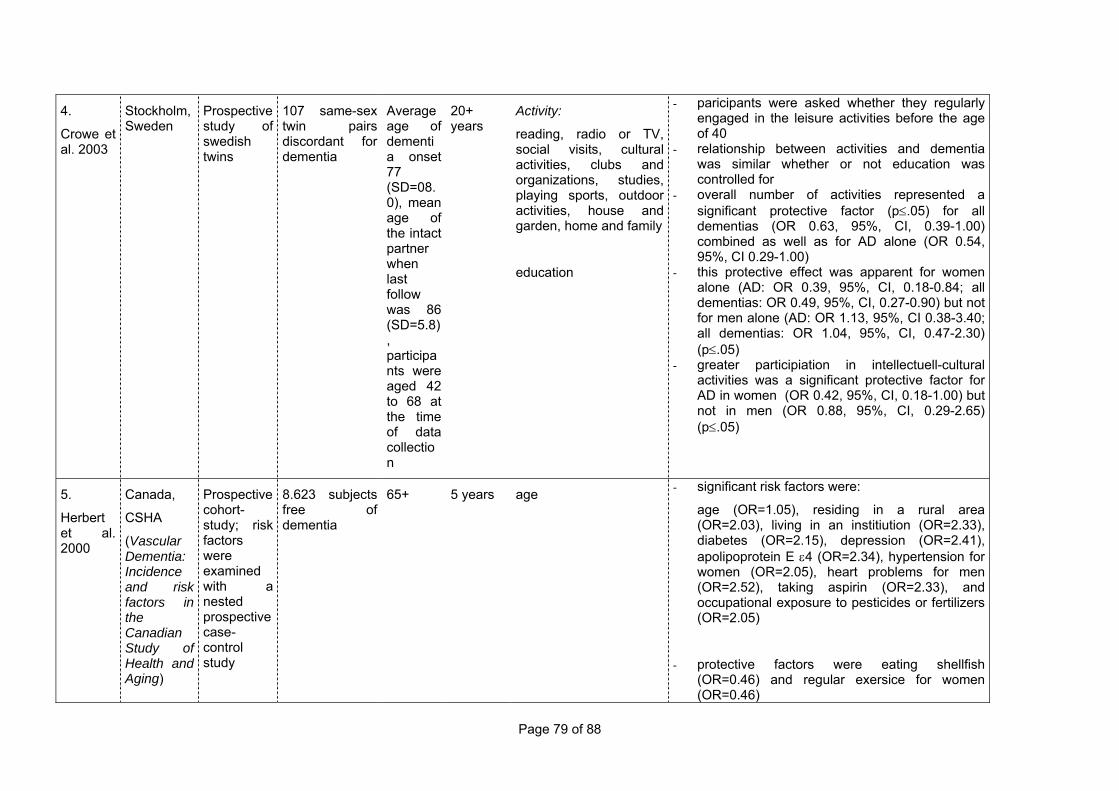
Page 79 of 88
4.
Crowe et al. 2003
Stockholm, Sweden
Prospective study of swedish twins
107 same-sex twin pairs discordant for dementia
Average age of dementia onset 77 (SD=08.0), mean age of the intact partner when last follow was 86 (SD=5.8), participants were aged 42 to 68 at the time of data collection
20+ years
Activity:
reading, radio or TV, social visits, cultural activities, clubs and organizations, studies, playing sports, outdoor activities, house and garden, home and family
education
- paricipants were asked whether they regularly engaged in the leisure activities before the age of 40
- relationship between activities and dementia was similar whether or not education was controlled for
- overall number of activities represented a significant protective factor (p≤.05) for all dementias (OR 0.63, 95%, CI, 0.39-1.00) combined as well as for AD alone (OR 0.54, 95%, CI 0.29-1.00)
- this protective effect was apparent for women alone (AD: OR 0.39, 95%, CI, 0.18-0.84; all dementias: OR 0.49, 95%, CI, 0.27-0.90) but not for men alone (AD: OR 1.13, 95%, CI 0.38-3.40; all dementias: OR 1.04, 95%, CI, 0.47-2.30) (p≤.05)
- greater participiation in intellectuell-cultural activities was a significant protective factor for AD in women (OR 0.42, 95%, CI, 0.18-1.00) but not in men (OR 0.88, 95%, CI, 0.29-2.65) (p≤.05)
5.
Herbert et al. 2000
Canada,
CSHA
(Vascular Dementia: Incidence and risk factors in the Canadian Study of Health and Aging)
Prospective cohort-study; risk factors were examined with a nested prospective case-control study
8.623 subjects free of dementia
65+ 5 years age - significant risk factors were:
age (OR=1.05), residing in a rural area (OR=2.03), living in an institiution (OR=2.33), diabetes (OR=2.15), depression (OR=2.41), apolipoprotein E ε4 (OR=2.34), hypertension for women (OR=2.05), heart problems for men (OR=2.52), taking aspirin (OR=2.33), and occupational exposure to pesticides or fertilizers (OR=2.05)
- protective factors were eating shellfish (OR=0.46) and regular exersice for women (OR=0.46)
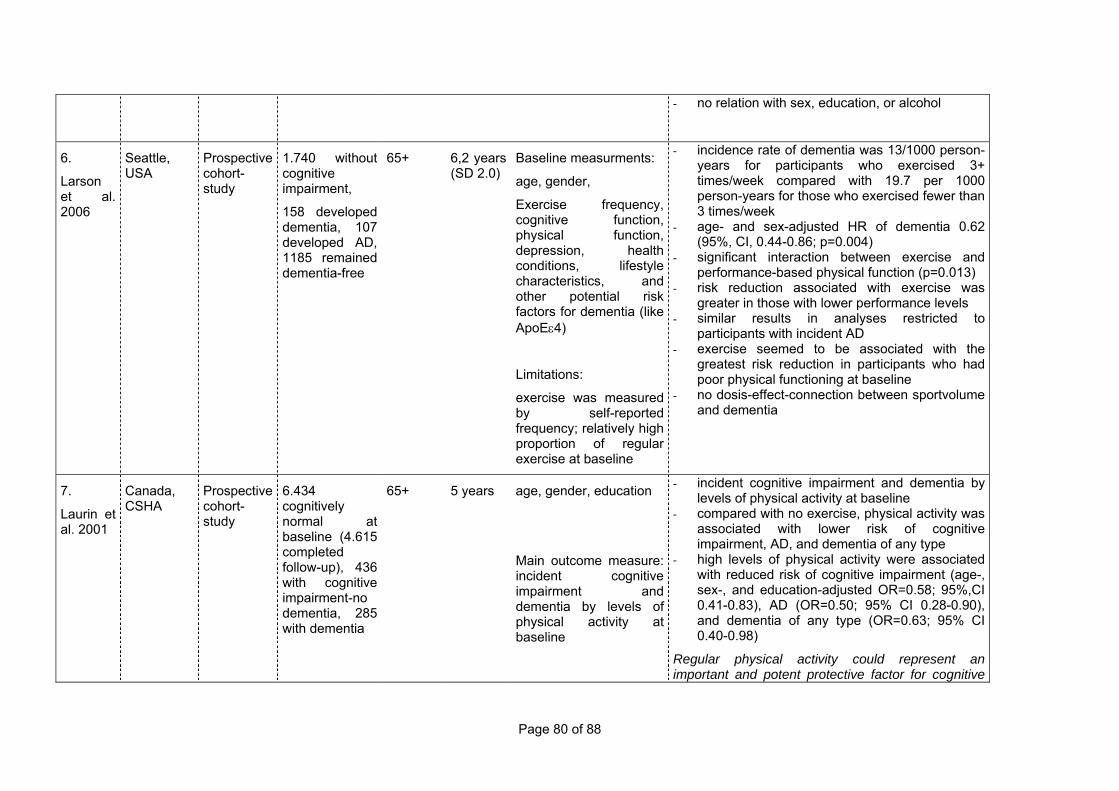
Page 80 of 88
- no relation with sex, education, or alcohol
6.
Larson et al. 2006
Seattle, USA
Prospective cohort-study
1.740 without cognitive impairment,
158 developed dementia, 107 developed AD, 1185 remained dementia-free
65+ 6,2 years (SD 2.0)
Baseline measurments:
age, gender,
Exercise frequency, cognitive function, physical function, depression, health conditions, lifestyle characteristics, and other potential risk factors for dementia (like ApoEε4)
Limitations:
exercise was measured by self-reported frequency; relatively high proportion of regular exercise at baseline
- incidence rate of dementia was 13/1000 person-years for participants who exercised 3+ times/week compared with 19.7 per 1000 person-years for those who exercised fewer than 3 times/week
- age- and sex-adjusted HR of dementia 0.62 (95%, CI, 0.44-0.86; p=0.004)
- significant interaction between exercise and performance-based physical function (p=0.013)
- risk reduction associated with exercise was greater in those with lower performance levels
- similar results in analyses restricted to participants with incident AD
- exercise seemed to be associated with the greatest risk reduction in participants who had poor physical functioning at baseline
- no dosis-effect-connection between sportvolume and dementia
7.
Laurin et al. 2001
Canada, CSHA
Prospective cohort-study
6.434 cognitively normal at baseline (4.615 completed follow-up), 436 with cognitive impairment-no dementia, 285 with dementia
65+ 5 years age, gender, education
Main outcome measure: incident cognitive impairment and dementia by levels of physical activity at baseline
- incident cognitive impairment and dementia by levels of physical activity at baseline
- compared with no exercise, physical activity was associated with lower risk of cognitive impairment, AD, and dementia of any type
- high levels of physical activity were associated with reduced risk of cognitive impairment (age-, sex-, and education-adjusted OR=0.58; 95%,CI 0.41-0.83), AD (OR=0.50; 95% CI 0.28-0.90), and dementia of any type (OR=0.63; 95% CI 0.40-0.98)
Regular physical activity could represent an important and potent protective factor for cognitive

Page 81 of 88
decline and dementia in elderly persons.
8.
Podewills
et al. 2005
USA
(Cardiovascular Health Cognition Study CHS)
Population-based, prospective cohort study
3.375 people free of dementia at baseline; 480 incident cases of dementia
65+ 5,4 years Variables like:
age, gender, race, education, BMI, MMSE, APOE ε4, Comorbid condition like stroke, diabetes…, ADL,
- after multivariate adjustment, participants in the highest quartile of physical energy expenditure had a relative risk of dementia of 0.85 (95% CI 0.61-1.19) compared with those in the lowest quartile, and participants engaging in ≥ 4 acitivities had a relative risk of dementia of 0.51, 95% CI 0.33-0.79 compared with those engaging in 0-1 activity
- these associations were absent in apolipoprotein E genotype (APOE) ε4 allele carriers
9. Scarmeas et al. 2003
USA , northern Manhattan
Prospective cohort-study
1.772 nondemented individuals; 207 became demented
65+ 2,9 years
Adjusting for age, ethnic group, education, and occupation, were used to estimate the relative risk (RR) of incident dementia associated with high leisure activities
- risk of AD was decreased in subjects with high leisure activities (RR=0.62; 95%, CI=0.46-0.83) vs. low leisure activities
- when factors such as ethnic group, education, and occupation were controlled for, subjects with high leisure activity had 38% less risk of developing dementia
- reading, visiting friends or relatives, going to movies or restaurants, and walking for pleasure or going for an excursion were most strongly associated with a reduced risk of incident dementia
- the absence of social and intellectual engagements may not be risk factors themselves but may be related to some unknown causal risk factor cannot be completely excluded
Findings suggest a relation between the degree of
leisure activity and the risk of developing AD.

Page 82 of 88
10. Verghese et al. 2003
New York, Bronx Aging Study
Prospective cohort-study
469 subjects (124 developed dementia (61 AD, 30 VD, 8 other types of dementia))
75+ 5,1 years Adjustment for age, sex, educational level, presence or absence of chronic medical illness, and base-line cognitive status
- leisure activities, reading, playing board games, playing musical instruments, and dancing were associated with a reduced risk of dementia
- the physical-activity score was not significantly associated with dementia: >16 vs. <9 (RR=1.27; 95%, CI=0.78-2.06)
- cognitive activity score >11 vs. <8 (RR=0.37; 95%, CI=0.23-0.61)
- significant association between a higher level of participation in leisure activities at base-line and a decreased risk of dementia- both for AD and for VA
11.
Rovio et al. 2005
Finland Population-based cohort
117 persons with dementia, 76 with AD
65-79 mean follow-up, 21 years
age, follow-up time, education, gender, ApoE ε4 carriers, systolic, diastolic blood pressure, BMI, total serum cholesterol, history of locomotor disorders
- leisure-time physical activity at midlife at least twice a week was associated with a reduced risk of dementia and AD (OR 0.48, 95%, CI 0.25-0.91 and 0.38 (0.17-0.85) respectively), even after adjustments for age, sex, education, follow-up time, locomotor disorder, APOE genotype, vascular disorder, smoking and alcohol drinking
- gular physical activity may reduce the risk or delay the onset of dementia and AD, especially among gentically susceptible individuals
10.2 Documents produced in the framework of the project3
10.2.1 Financial regulations
Introduction
These financial regulations provide information to the different project partners on their financial reporting duties to Alzheimer Europe and the European Commission. They should be read in conjunction with the financial provisions contained in the contract from the European Commission, of which each centre received a copy by e-mail.
Payment procedures
Bank information
Each centre shall provide full banking details to Alzheimer Europe, which will use this information for the payment of grants to the different centres.
Initial payment
After the contract has been signed by all contract partners and the European Commission, a first payment of 30% of the overall grant will be made to Alzheimer Europe. Alzheimer Europe will provide each participating centre with 30% of their respective grant.
Second payment
As specified in the financial provisions of the Commission contract, Alzheimer Europe will be paid a further 20% of the total grant after receipt and acceptance by the European Commission of the first interim report and first financial report. These reports should be sent to the Commission no later than 1 March 2007.
To allow Alzheimer Europe to prepare the global financial report, each centre shall provide Alzheimer Europe with a detailed breakdown of all expenditure and will do so no later than 31 January 2007.
Failure to so by the deadline of 31 January 2007 will result in the missing centre not receiving the second payment of its total grant and payment will be deferred until the next reporting period. Similarly, centres having used up less than 70% of their initial grant payment will not be paid their second instalment until the next reporting period.
Centres having complied with these regulations and having used up at least 70% of their initial grant payment will be paid a further 20% of their grant after receipt of the second instalment from the European Commission.
Third payment
A further 20% of the total grant will be paid to Alzheimer Europe after receipt and acceptance by the European Commission of the second interim report and second financial report. These reports should be sent to the European Commission no later than 1 March 2008.
To allow Alzheimer Europe to prepare the global financial report, each centre shall provide Alzheimer Europe with a detailed breakdown of all expenditure and will do so no later than 31 January 2008.
Failure to so by the deadline of 31 January 2008 will result in the missing centre not receiving the third payment of its total grant and payment will be deferred until the next reporting period. Similarly, centres having used up less than 70% of their previous grant payments will not be paid their third instalment until the next reporting period.
Centres having complied with these regulations and having used up at least 70% of their previous grant payments will be paid a further 20% of their grant after receipt of the third instalment from the European Commission.
3 Only those documents are included here which were not produced separately or as part of a Dementia in Europe Yearbook
Page 84 of 88
Payment of the grant balance
The grant balance will be paid to Alzheimer Europe after acceptance by the Commission of the final report and final financial report.
Alzheimer Europe will transfer these funds to the different project partners immediately after receipt of the final payment by the European Commission.
Payments to be made to project partners will not exceed the amounts for Community contribution included in the Commission Contract.
Calculation of final Commission grant
The final grant of the European Commission may not exceed €843,019 for the total of the project, nor can it exceed 59.23% of the total cost of the project. Should the total cost of the project be less than €1,423,190, the final grant of the Commission will be reduced proportionately.
The same rules apply to the different budgets of the project partners in that the grant will be reduced if the total expenditure of a project partner is below the total expenditure budgeted for the centre.
At the same time, should the total expenditure of a centre exceed the total amount of the budgeted expenditure, the grant may not be increased proportionately.
Financial Reporting
Each centre is responsible for the management of its budget and shall provide Alzheimer Europe with yearly financial reports of all costs incurred by the centre for the project. Alzheimer Europe will collect the financial reports of the different partners and present global financial reports to the European Commission for the totality of the project.
Deadlines for financial reporting
In line with the requirements of the European Commission, project partners are required to submit their financial reports at least one month before the deadline for submission of the global financial report to the European Commission.
• For the first financial report (covering the period of 1 January 2006 to 31 December 2006), the deadline is 31 January 2007
• For the second financial report (covering the period of 1 January 2007 to 31 December 2007), the deadline is 31 January 2008
• For the first financial report (covering the period of 1 January 2008 to 31 December 2008), the deadline is 28 February 2009.
Structure of financial report
Each centre shall include the following information on its financial report which will need to be printed on the headed letter paper of the participating centre and signed by a representative of the centre. A model financial report is enclosed in the annex.
Declaration of honour
The financial report shall be preceded by the following mention:
The undersigned, NAME AND FUNCTION, acting on behalf of NAME OF CENTRE hereby certifies that the following constitutes a fair and true presentation of the expenditure occurred by NAME OF CENTRE for the carrying out of activities of the project “European Collaboration on Dementia – Agreement Number 2005108” for the year YEAR.
Staff costs
Staff costs should be presented as follows:
NAME OF STAFF MEMBER: NUMBER OF DAYS x DAILY RATE = TOTAL
Supporting evidence: Each centre will be required to send in to Alzheimer Europe the filled in time sheets (See Annex) for the days spent by staff of the centre on the project

Page 85 of 88
For the calculation of costs, you can use the following formulas (either total monthly staff costs including all costs to the employer divided by 20 OR total yearly staff costs including all costs to the employer divided by 220).
Travel costs
Travel costs should be presented as follows:
1. NAME OF STAFF MEMBER
2. REASON FOR TRAVEL (i.e. Working group or steering committee or other project linked meeting)
3. ORIGIN OF TRAVEL TO PLACE OF MEETING
4. METHOD OF TRAVEL (i.e. PLANE, TRAIN, VAR)
5. COST
Supporting evidence: Each centre will be required to send in to Alzheimer Europe a copy of the ticket or invoice together with the financial report.
Subsistence allowances
Subsistence costs should be presented as follows:
1. NAME OF STAFF MEMBER
2. MEETING (i.e. Working group or steering committee or other project linked meeting)
3. PLACE OF MEETING
4. COST = NUMBER OF DAYS OF MEETING x DAILY RATE = TOTAL
Supporting evidence: No supporting evidence will be required from the different centres. The centres are obliged to use the daily per diems fixed by the European Commission (See in Annex).
Each centre will be required to send in to Alzheimer Europe a copy of the ticket or invoice together with the financial report.
Consumables and supplies (ONLY work package leaders)
Work package leaders have a budget of €2,000 for literature searches and for purchases of publications
The work package leaders therefore need to provide a detailed breakdown for the costs incurred under this heading.
Supporting evidence: The work package leaders should include copies of the various invoices with their financial report.
Other costs (ONLY University of Oxford)
The University of Oxford has a budget of €3,000 for the translation of existing guidelines. When reporting these costs, it needs to provide a detailed breakdown of these costs.
For each translated document, it will need to specify the language from which the document was translated, the number of words or pages of the document, the cost per word or page and the total cost per translated document.
Supporting evidence: Invoices for the different translations need to be included with the financial reports.
Overheads
Each centre can include 7% overheads to the total of its expenditure.
Budget adjustments
When presenting their financial reports, centres should stay as close as possible to the original budget. Nevertheless, it is possible for centres to adjust the estimated budget by
Page 86 of 88
making transfers between different lines of expenditure. These adjustments may not exceed 10% (See Article I.3.4. of the Commission contract for full details).
Other reporting
The different workpackage leaders should prepare progress reports on the different working groups and submit them by the same deadline as that for the financial reports.
The following documents should be included with the different reports:
1. For the first interim report: A brief progress report together with the minutes of the different meetings, as well as a bibliography for the collected literature on the subject.
2. For the second interim report: A brief progress report together with the minutes of the different meetings, as well as a comparative report on the findings of the literature search.
3. For the final report: A detailed progress report together with the minutes of the different meetings, as well as the new consensus documents or recommendations.

Page 87 of 88
Annex I: Model Financial Report
The undersigned, NAME AND FUNCTION, acting on behalf of NAME OF CENTRE hereby certifies that the following constitutes a fair and true presentation of the expenditure occurred by NAME OF CENTRE for the carrying out of activities of the project “European Collaboration on Dementia – Agreement Number 2005108” for the year YEAR.
1. Staff costs Staff member Number of days
worked on project Daily Rate Total
TOTAL:
2.1. Travel costs Staff member Reason for travel
and date From … to … Method of travel Cost
TOTAL:
2.2. Subsistence costs Staff
member Reason for
travel and date Meeting
Place Number of
Days Daily per diem Cost
TOTAL:
3. Consumables and supplies (Work package leaders ONLY) Description of expense Cost
TOTAL:
4. Other costs (University of Oxford ONLY) Name of document From
language to language
Number of pages/words
Cost per page/word
Cost
TOTAL:
OVERVIEW Total eligible costs 1+2+3+4
Overheads 7% TOTAL COSTS 1+2+3+4+7%
Commission grant Percentage of TOTAL COSTS as per contract
Applicant’s contribution TOTAL COSTS – Commission grant
TOTAL INCOME Same as total costs
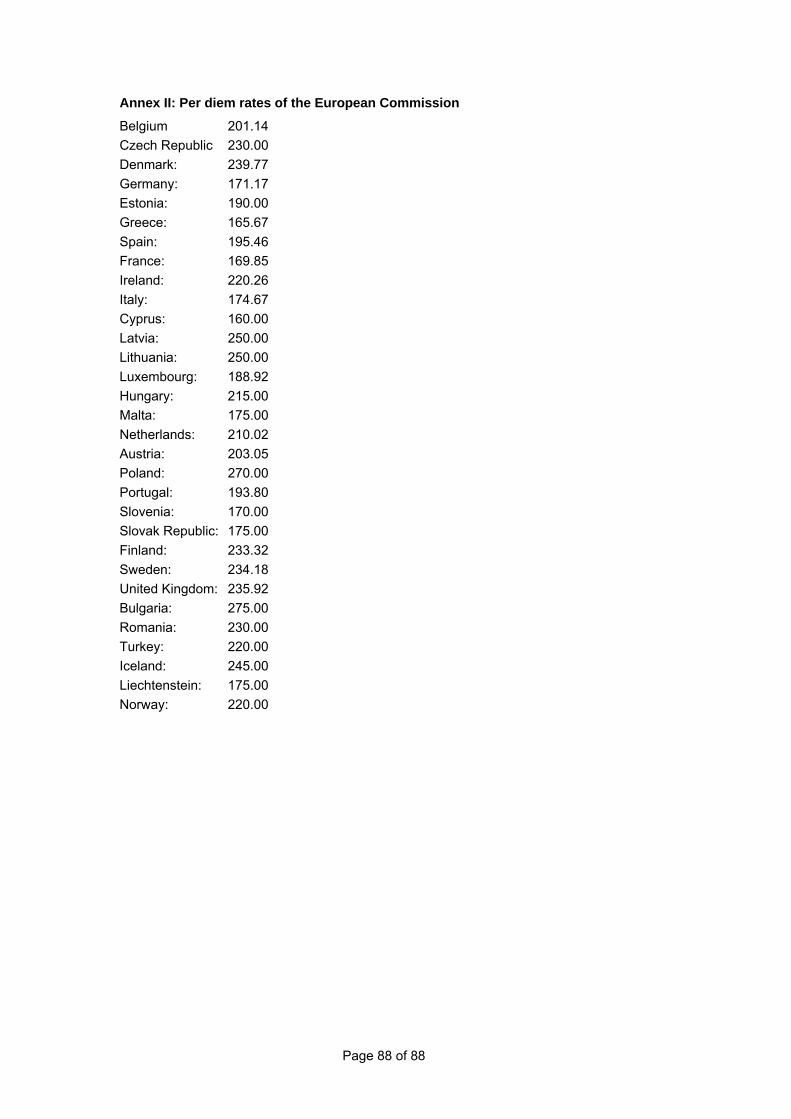
Page 88 of 88
Annex II: Per diem rates of the European Commission
Belgium 201.14 Czech Republic 230.00 Denmark: 239.77 Germany: 171.17 Estonia: 190.00 Greece: 165.67 Spain: 195.46 France: 169.85 Ireland: 220.26 Italy: 174.67 Cyprus: 160.00 Latvia: 250.00 Lithuania: 250.00 Luxembourg: 188.92 Hungary: 215.00 Malta: 175.00 Netherlands: 210.02 Austria: 203.05 Poland: 270.00 Portugal: 193.80 Slovenia: 170.00 Slovak Republic: 175.00 Finland: 233.32 Sweden: 234.18 United Kingdom: 235.92 Bulgaria: 275.00 Romania: 230.00 Turkey: 220.00 Iceland: 245.00 Liechtenstein: 175.00 Norway: 220.00

This report was produced by a contractor for Health & Consumer Protection Directorate General and represents the views of thecontractor or author. These views have not been adopted or in any way approved by the Commission and do not necessarilyrepresent the view of the Commission or the Directorate General for Health and Consumer Protection. The EuropeanCommission does not guarantee the accuracy of the data included in this study, nor does it accept responsibility for any use madethereof.