evaluating neuropsychiatric risks with varenicline in ... · pdf file1 evaluating...
TRANSCRIPT

1
Evaluating neuropsychiatric risks with varenicline in patients with psychiatric
disorders
Shermaine Ngo, LMPS Pharmacy Resident 2016-2017
Psychiatry Rotation with Gillian Lagnado
October 13, 2016

Outline
• Learning Objectives
• Patient Case
• Literature Search
• Summary
• Recommendations
• Monitoring Plan
2

Learning Objectives
• Identify pharmacological options for smoking cessation in patients with psychiatric conditions
• Discuss the neuropsychiatric safety of varenicline in patients with psychiatric disorders
3

Meet the Patient
4

Patient Case: MM
5
ID 41 yo female (wt = 59kg, ht = 175cm) admitted with substance-induced psychosis on Aug 31, 2016
c/c Worsening paranoid delusions, 2o to polysubstance use
HPI 3 week history of:• Paranoid delusions of ex-boyfriend stalking her through the internet, video-taping her and trying to harm her
Allergies NKDA

Past Medical History Medications PTA
• Ongoing heroin addiction • Methadone 70mg PO daily (DWI)
• Ongoing cocaine addiction
• Ongoing nicotine addiction • Bupropion 100mg SR PO twice daily
• Depression• Generalized Anxiety Disorder
• Venlafaxine 150mg ER PO daily
• Chronic neuropathic back pain • Ibuprofen 600mg PO daily• Nabilone 2mg PO twice daily
• Hypothyroidism • Synthroid 112mcg PO daily
Social Hx:P’care coverage – Plan G Nicotine: Smokes about 1 pack per day (since 15 years old)Recreational Drugs:Intranasal use of cocaine (0.1g every 2-3 days) and heroin (0.1g every 2-3 days) Alcohol: NoneCaffeine: None
6

Current Medications (Sept 19, 2016)
Waiting for ablation appointment at BCCA for thyroid cancer
7
Medical Conditions Medications
• Substance-induced psychosis • Olanzapine 20mg PO HS
• Ongoing heroin addiction • Methadone 60mg PO daily
• Ongoing nicotine addiction • Nicotine patch 28mg/day, gum 4mg, inhaler 10mg PRN• Fagerstrom Test for Nicotine Dependence: 7• With NRT, cigarette smoking ↓ to 4-5/day(PTA: smoking 1 pack/day)
• Depression • Venlafaxine 225mg PO daily
• Anxiety • Venlafaxine 225mg PO daily• Loxapine 10-20mg PO Q1H PRN (~4x10mg daily)• Lorazepam 1mg SL Q1H PRN (~4x1mg daily)
• Chronic neuropathic back pain
• Gabapentin 300mg PO BID and 600mg PO HS• Ibuprofen 600mg PO daily
• Hypothyroidism • Levothyroxine 175mcg PO once daily

8
Review of Systems (Sept 19, 2016)
Vitals Temp 36.7oC BP 110/65 HR 100 RR 16 O2 Sat 99% RA
CNS Alert and oriented x3 GCS 15Appearance and behaviour: pleasant, groomed and cooperativeSpeech: normal pace, not pressuredMood and affect: Low (2-3/10) but euthymicThought content: Delusions are decreasing, but still thinks her ex-boyfriend is committing fraud against her and including staff in delusions, no suicidal or homicidal ideationsInsight and judgment: Some insight into her delusions and that she requires and would like help to improve her conditionCognition: No impairment in memory and attention↓ energy and ↑ in fatigue (sleeps up to 18 hours daily)
EENT ↑ in dry mouth
CVS No CP, No S3 + S4, No edema
RSP No SOB, No cough
GI ↑ in appetite (resulting in ↑ in weight of 6kg over 5 days)
GU/renalLiverEndoMSKDerm
Unremarkable

9
Relevant Labs – Sept 19, 2016
Electrolytes WNL
sCr 84 umol/L
eGFR >74 mL/min/1.73m2
TSH 49.42 mU/L
fT4 10.2 pmol/L
Total Cholesterol 4.58 mmol/L
Triglycerides 1.62 mmol/L
HDL 1.60 mmol/L
LDL 2.23 mmol/L
AST 34 U/L
ALT 33 U/L
ALP 52 U/L
GGT 10 U/L
Total bilirubin 4 umol/L
Laboratory Values

10
Diagnostics
Thyroid U/S (09/2): 2 hyperechoic lesions/modules Confirmed to be cancerous
CT Head (09/3): Unremarkable
ECG (08/31): Normal sinus rhythm. Vent rate = 65 BPM QTc = 461 msec
Diagnostics

Drug Therapy Problems• MM is at risk of cardiovascular disease,
ischemic heart disease, smoking-related cancers and mortality, secondary to continued use of cigarettes. She would benefit from a reassessment of therapy.
• MM is experiencing adverse effects (↑ appetite, weight gain, dry mouth), secondary to receiving olanzapine.
• MM is experiencing paranoid delusions which have partially improved with therapeutic doses of olanzapine.
• MM is experiencing ongoing and unresolved anxiety and is requiring several PRN doses of antipsychotics and anxiolytics.
11

Goals of Therapy
• Achieve complete and sustained remission from tobacco use disorder
• Support smokers in the pre-contemplative and contemplative stages of change to move to preparation and then action stages.
• Support smokers who successfully quit to achieve long-term abstinence
• Minimize adverse reactions
12

Background
13

Pharmacologic Options for Smoking Cessation
1st Line Options:
• Nicotine Replacement Therapy
• Bupropion
• Varenicline
2nd Line Options:
• Clonidine
• Nortriptyline
14

Intervention Odds Ratio (95% CI)a No. of Studies
Placebo 1 267
Nicotine gum 1.68 (1.51–1.88) 56
Nicotine patch 1.91 (1.71–2.14) 43
Nicotine inhaler, lozenge or spray
2.04 (1.75–2.38) 16
Bupropion 1.85 (1.63–2.1) 6
Nicotine patch plus as-needed inhaler, gum or spray
2.73 (2.07–3.65) 2
Varenicline 2.89 (2.4–3.48) 15
e-Therapeutics: Smoking Cessation
15
a Odds ratios were derived from comparisons with placebo.
Odds Ratio of Quitting

Varenicline
MOA α4β2-nicotinic receptor partial agonist• prevents nicotine stimulation of mesolimbic dopamine system• stimulates dopamine activity (smaller degree than nicotine) to help decrease craving and withdrawal symptoms
Doses Days 1 to 3: 0.5 mg once dailyDays 4 to 7: 0.5 mg twice dailyMaintenance (≥ Day 8): 1 mg twice daily for 11 weeks• Set quit date 1-2 weeks after starting• If still smoking 4 weeks after starting, reassess therapy; can be continued for an additional 12 weeks if patient has benefited
16

Champix® Monograph
http://www.pfizer.ca/products/champix-varenicline-tartrate-tablets
17

Clinical Question
P 41 yo female with substance-induced psychosis (medically and clinically unstable)
I Varenicline
C BupropionNicotine replacement therapyPlacebo
O • Neuropsychiatric adverse events• Achievement of abstinence during treatment• Sustained abstinence after treatment completion
18

Search StrategyDatabases Medline, PubMed
Search Terms “varenicline” AND“neuropsychiatric” OR “psychiatric” OR “psychosis” OR “mania” OR “depression
Inclusion Humans, Adults, English
Results • 5 systematic reviews/meta-analysis • 1 systematic review• 4 meta-analysis• 14 RCTs • 6 reviews • 20 case reports • 9 retrospective studies • 1 prospective studies
19

Lancet 2016; 387:2507-20
20

EAGLES
Design Double-blind, triple-dummy, placebo-controlled, active-controlled RCT (Nov/11-Jan/15)
P N = 4116 in psychiatric cohort (4074 included in the safety analysis)N = 4028 in non-psychiatric cohort (3984 included in the safety analysis)
Inclusion: 18-75 years old motivated-to-quit smokers• smoked an average of > 10 cigs/day • exhaled carbon monoxide concentration > 10 ppm at screening Additional Inclusional critiera for psychiatric cohort:• Met DSM-IV-TR criteria currently (during last 30 days) and/or past for:Mood disorders (MDD, bipolar disorder) Anxiety disorders (panic disorder, PTSD, OCD, social phobia, GAD) Psychotic disorder (schizophrenia, schizoaffective disorder) Personality disorders, limited to past history of borderline personality disorder • Clinically stable: no exacerbation in the preceding 6 monthson stable medication and dose for at least 3 months with no treatment change anticipated during the study In the opinion of the investigator, not at high risk of self injury or suicidal behaviour
21

EAGLESP Exclusion:
Subjects presenting with any of the following past or current conditions:• destabilizing psychiatric conditions•schizophreniform disorder, delusion disorder, psychotic disorder not otherwise specified• all delirium, dementia and amnestic and other cognitive disorders• all factitious disorders, dissociative disorders, impulse control disorders• all substance-induced disorders (other than nicotine)• evidence of severe substance abuse/misuse or dependence• subjects need to be in sustained full remission for the last 12 months, and not taking opioidagonists or partial opioid agonists. • Severe anti-social, schizotypal or other personality disorder
Subjects with a past history of a condition listed above could be included in the study and placed in the psychiatric cohort, only if concurrently diagnosed with an inclusionary Axis I or II diagnosis and able to comply with study requirements.
•Suicidal ideation associated with the actual intent and/or plan in the past year•Previous suicidal behaviour in the past year• Subjects who have taken varenicline, bupropion, NRT or investigational drug within 30 days prior to baseline visit• Subjects with risk of seizure (e.g. Current or history of seizures, abrupt discontinuation of alcohol or seizures, anorexia or bulimia nervosa, use of MAOIs within the past 14 days, use of desipramine, nortriptyline, type 1C antiarrhythmic, thioridazine)
22

EAGLES
I Varenicline 1mg twice daily for 12 weeks
C Bupropion 150mg twice daily for 12 weeksNicotine patch 21mg per day with taper for 12 weeks Matched placebo daily for 12 weeks
23
• Target quit date: 1 week after randomization
• End of titration for varenicline and bupropion
• Initiation of nicotine patch
• At each study visit: pill and patch counts were done to measure compliance

EAGLESO 1o efficacy endpoint: continuous abstinence rate for weeks 9-12
Self-reported abstinence and no exhaled CO concentration > 10 ppm• If lost to follow-up: considered to be smokers
1o composite safety endpoint (during treatment or within 30 days of discontinuation):based on post-marketing reports of neuropsychiatric AEs in smokers taking varenicline and bupropion
• >1 “severe” adverse event of: anxiety, depression, feeling abnormal, hostility AND/OR• >1 “moderate” or “severe” adverse event of: agitation, aggression, delusions, hallucinations, homicidal ideation, mania, panic, paranoia, psychosis, suicidal ideation, suicidal behaviour, completed suicide
2o safety endpoints:• subset of all neuropsychiatric adverse events that were rated severe and the occurrence of each of the individual components• all adverse events
24

Psychiatric Cohort• Gender
– 40% male
– 60% female
• Region:
– 58% USA
– 29% Western Europe and other countries
• Smoking
– FTCD score: 6 (High)
– 28 years of smoking
– 20 cigarettes/day
– 3.5 previous quit attempts
25

Psychiatric Cohort• Psychiatric disorders
– 70% unipolar and bipolar mood disorders
– 19% anxiety disorders
– 9% psychotic disorders
– <1% personality disorders
– 50% on psychotropic meds• 31-37% antidepressants
• 2% mood stabilisers
• 16% antipsychotics
• HADS score: 8.2-8.7– Anxiety score: 5 (3.9)
– Depression score: 3.3 (3.3)
• C-SSRS:– History of ideation: 34%
– History of behaviour: 13%
26

Results – Efficacy
Comparator Bupropion Nicotine Patch Placebo
Varenicline (Wk 9-12) 1.74 (1.14-2.14)P < 0.0001
1.62 (1.32-1.99)P < 0.0001
3.24 (2.56-4.11)P < 0.0001
Varenicline (Wk 9-24) 1.41 (1.11-1.79)P = 0.0047
1.51 (1.19-1.93)P = 0.0008
2.50 (1.90-3.29) P < 0.0001
27
Odds Ratio (95% CI):

Results – Safety
• More neuropsychiatric adverse events in psychiatric cohort
– Psychiatric: 5.8% vs. Non-psychiatric: 2.1% (p<0.0001)
• Psychiatric cohort: no significant pairwise treatment differences
– 95% confidence interval included zero
– Non-psychiatric cohort: varenicline was significantly lower than placebo
28
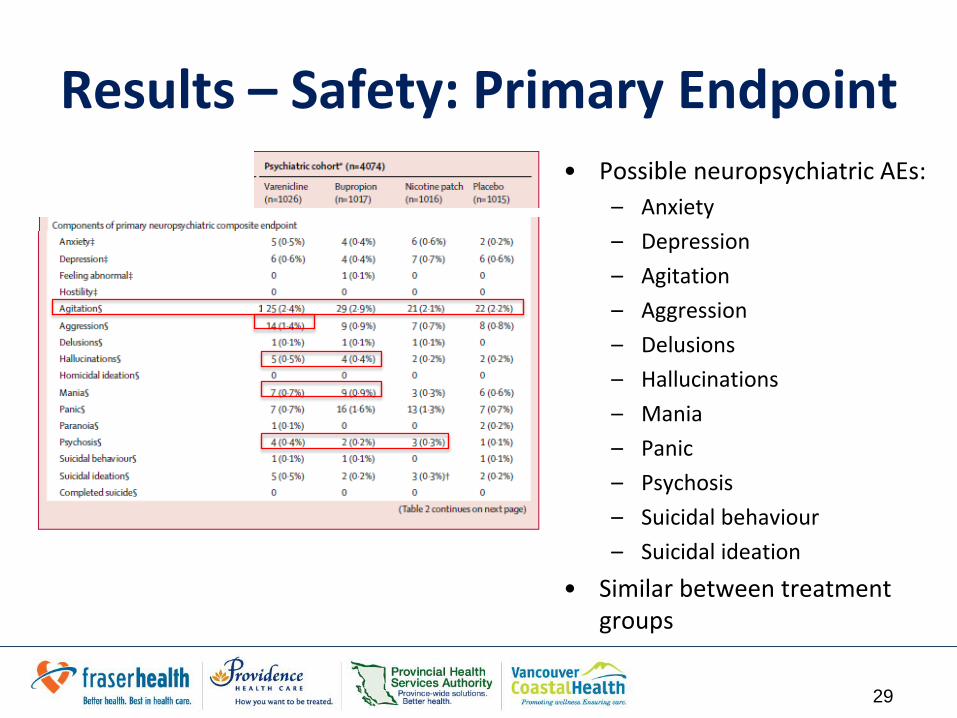
Results – Safety: Primary Endpoint • Possible neuropsychiatric AEs:
– Anxiety
– Depression
– Agitation
– Aggression
– Delusions
– Hallucinations
– Mania
– Panic
– Psychosis
– Suicidal behaviour
– Suicidal ideation
• Similar between treatment groups
29

Results – Safety: Neuropsychiatric AEs
• Incidence is relatively similar between treatment arms
• Most common for varenicline:
– Psychiatric disorders 39%
– Abnormal dreams 12%
– Insomnia 9%
– Anxiety 8%
– Depression 5%
– Irritability 5%
30

Results – Safety: Suicide Risk
• Greater suicidal risk in the psychiatric cohort
– Non-psychiatric: suicidal behaviour/ideation <1%
Varenicline:
• Suicidal behaviour:– No patients during treatment
– <1% after last dose to end of study
• Suicidal ideation:– 3% during treatment
– 2% after last dose to end of study
• Slightly greater than other treatments
31

Results – Safety: General
32
Varenicline Bupropion Nicotine Patch
Abnormal dreams
12% Abnormaldreams
8% Abnormal dreams
14%
Anxiety 8.4% Anxiety 10.3% Anxiety 9.2%
Insomnia 9% Insomnia 12% Insomnia 10%
Depressed 4.6% Depressed 4.6% Depressed 5.1%
Nausea 26.1% Dry mouth 7.5% Pruritus 5.7%
Headache 12.6% Headache 9.7% Headache 10.2%
Fatigue 8.6%

Strengths
• Methodology
– Triple-dummy, double-blinded, placebo-controlled, active-controlled and multi-center RCT
– Relatively large sample size • required 2000 per arm to estimate a 75% ↑ in neuropsychiatric
adverse event rate within +1.59% or -1.59%
– Long-term follow-up (12 weeks)
• Clinically
– Overall treatment compliance: 80%
– Relevant efficacy and safety outcomes
33

Limitations• Methodology
– Population: Out-patients with stable and treated psychiatric conditions that were in remission and motivated to quit smokers
• Majority: unipolar and bipolar mood disorders
• Extensive exclusion criteria
• Clinically
– Purpose of NAEI: starting point to identify concerning side effects
• Most sites used it as a checklist...often no additional information provided to give context into the severity assigned
• Some narratives were inconsistent with investigator’s rating of severity
– ~ 50% required psychotropic medication at baseline
– ~ 16% required antipsychotic
• ?Generalizability of results to general psychiatric population
34

Study’s Bottom Line
Efficacy:“Varenicline was more effective than placebo, nicotine patch and bupropion in helping smokers achieve abstinence, whereas, bupropion and nicotine patch were more effective than placebo”
Safety:“did not show a significant increase in neuropsychiatric adverse events attributable to varenicline or bupropion, relative to nicotine patch or placebo”
35

Wu, Qi et al. Addiction(2016).
Roberts, Emmert et al. Addiction (2016).
36

Systematic Reviews & Meta-Analyses
• Patient Population:
– Severe Mental Illness (SMI): any non-organic disorder with psychotic features that result in a substantial disability, including schizophrenia or other types of schizophrenia-like psychosis (e.g. schizophreniform and schizoaffective disorders), bipolar disorder, delusional disorder, depressive psychoses
37

ResultsWu et al. (N=8) Robert et al. (N=14)
Inclusion RCTs on smokers with SMI without language restriction
RCTs on motivated to quit smokers with SMI in English
Trials • Clinically stable• majority: schizophrenia or schizoaffective disorder• Varenicline vs. Placebo• Average: 20 cigs/day
• Exclude: unipolar depression, 1o dx of ETOH or substance abuse• majority: schizophrenia or schizoaffective disorder
Smoking cessation in terms of quit rate
At end of treatment:RR= 4.33 (1.96-9.56)
v. Placebo: OR = 5.17 (1.78-15.06)v. Bup: OR = 1.15 (0.24–5.45)
Smoking reduction - 6.39 cigs/day, (2.22-10.56)
Safety Relative RiskDepression: 1.45 (0.45-4.64)Anxiety: 0.77 (0.28-2.17)Suicidal ideation: 1.06 (0.4-2.82)
Discontinuation due to AEs:v. Placebo: OR = 1.30 (0.50-3.37)v. Bup: OR = 1.21 (0.28–5.19)
38

Journal of clinical psychopharmacology 33.1 (2013): 55-62.
39

Search Strategy
Design and Aim Systematic review of published case reports of neuropsychiatric adverse events ascribed to varenicline and to determine potential risk factors for these adverse events
Databases MEDLINE, the Cochrane Library, EMBASE, and PsychInfo database
Search Terms ‘‘varenicline case report’’, ‘‘varenicline and depression’’, ‘‘varenicline and suicide’’, ‘‘varenicline and psychosis’’, ‘‘varenicline and mania’’, ‘‘varenicline and schizophrenia’’, ‘‘varenicline and neuropsychiatric adverse events’’, ‘‘champixneuropsychiatric adverse events’’, ‘‘champix case report’’, ‘‘chantix neuropsychiatric adverse events’’, and ‘‘chantix case report’’.
Inclusion case reports about the neuropsychiatric adverse events of varenicline published in English from 2006 (approval year by theFDA and the EMA) to January 1, 2012
40

Results
• 25 case reports
– Most required admission to hospital due to severity of neuropsychiatric adverse events
• Population:
– Average age: 46.4 years (range, 24-75 years)
– Males: 56%
– Psychiatric history: 68%
41

Results• Neuropsychiatric Adverse Events:
– Onset ranged from 2 days to 3 months after the initiation of varenicline
– In 2 reports: symptoms occurred after discontinuation
– 84% of cases resolved after discontinuation
42
Neuropsychiatic Adverse Event % of Case Reports
Mania 40%
Psychosis (including hallucinations and delirium) 36%
Suicidal Ideation (including completed suicide) 28%
Sleep disturbance/abnormal dreams 12%
Anxiety 8%

Summary• Varenicline: highest efficacy for smoking cessation
• Applicability of EAGLES:
– Clinically stable psychiatric conditions
– Specific patient population (mood disorders)
– Strength of evidence regarding safety
• Current or history of psychiatric conditions should not preclude the use of varenicline
– Consider: • Nicotine dependence
• Motivation to quit
• Clinical stability
• Ability to monitor the patient
43

Recommendations1. Optimize Nicotine Replacement Therapy
– Encourage use of PRN gums and inhaler
– Educate on non-drug measures
• Online Quit Program by Smoker’s Helpline
• Quit Coach by Smoker’s Helpline
• Connecting with community pharmacy
– Set a target quit date
2. Consider re-trial of bupropion
– Efficacy of bupropion and NRT is greater than either alone
– Bupropion: also used for depression and anxiety
3. Consider trial of varenicline if:
– Adequate trials of 1st line failed
– Clinically stable
– Able to closely monitor MM
44

Monitoring – Efficacy
45
Monitoring Parameters By Who? Expected ∆? When?
Cravings Patient NursePhysicianPharmacist
Decrease/Absence Daily
Withdrawal Symptoms (e.g. agitation, irritability, low mood, insomnia)
Decrease/Absence Daily
Number of cigarettes per day
Decrease/Absence Daily

Monitoring – Safety
46
Monitoring Parameters By Who? Expected ∆? When?
CNS Headache, abnormal dreams,insomnia, drowsiness, confusion, extrapyramidalreaction, diaphoresis
PatientNursePhysicianPharmacist
Presence Daily in hospital
HEENT Mild local irritation (throatirritation), hiccups, jaw pain and orodental problems, dry mouth, dyspepsia, constipation
RESP Cough, rhinitis
CVS Prolonged QT, tachycardia
GI ↑ appetite, nausea, dyspepsia
DERM Skin sensitivity and irritation
METAB ↑ weight gain (~4-5kg at 12 mos)

Thank you!
Questions?
47