evaluating the responsiveness of the endometriosis health profile questionnaire: the ehp-30
TRANSCRIPT
Evaluating the responsiveness of the endometriosis health profile questionnaire:
The EHP-30
Georgina Jones1,2,3, Crispin Jenkinson2 & Stephen Kennedy11Nuffield Department of Obstetrics and Gynaecology, University of Oxford; 2Health Services Research Unit,Department of Public Health and Primary Care, University of Oxford, United Kingdom; 3Present address:Institute of General Practice and Primary Care, University of Sheffield (E-mail: [email protected])
Accepted in revised form 8 April 2003
Abstract
Objectives: To evaluate the sensitivity to change of the Endometriosis Health Profile-30 (EHP-30) ques-tionnaire. Setting: The Women’s Center, John Radcliffe Hospital, Oxford. Design: Postal survey to 66women undergoing conservative surgery for the treatment of endometriosis-associated pain. The EHP-30and the Short Form-36 (SF-36) were administered 2 weeks before the operation, and 4 months post-operatively. At T2 a transition question was included to evaluate changes in patients health status. Toevaluate responsiveness effect sizes, standardised response means, the index of responsiveness and theminimally and clinically important differences were calculated. Results: Forty (66.6%) patients returned thequestionnaires at time 1 and 2. Overall less responsive effect size scores were found for the SF-36 (0.1–0.5)compared to the EHP-30 ()0.1–1.1) for all patients who had undergone treatment. Minimally importantdifferences and the index of responsiveness were overall higher for the EHP-30 (0.4–2.0) compared to theSF-36 (0.1–1.0). Change scores for four of the five scales were significantly correlated with women’sresponses to the transition question. Conclusions: Results suggest that the EHP-30 is sensitive to change. Itsapplication in clinical trials should prove beneficial in assessing the impact of medical and surgical inter-ventions upon quality of life for women with endometriosis.
Key words: Endometriosis, Quality of Life, Questionnaires, Surgery
Abbreviations: BDI – Beck Depression Inventory; EHP-30 – Endometriosis Health Profile-30 (a disease-specific questionnaire developed to measure the health-related quality of life of women with endometriosis;EQ-5D – euro-QoL (health status measure which provides a single index score of health status); HRQoL –health-related quality of life; MOS-6A – Medical Outcomes Study 6-item general health survey (6-itemversion of the Short Form-36); MYMOP – Measure Yourself Medical Outcome Profile (patient-centredhealth status instrument); SF-MPQ – Short Form McGill Pain Questionnaire (pain specific questionnaire);SF-36 – Short Form-36 (a generic health status questionnaire); SRM – standardised response mean (a unitof measurement used to measure changes in health status)
Introduction
Traditionally, the assessment of interventions forendometriosis has relied upon clinical measureswhich have direct biological significance, e.g. bloodpressure and haemoglobin levels [1]. However, it
has recently become commonplace for quality oflife tools to be used as measures of outcome inclinical trials so that the impact of interventions onhealth-related quality of life (HRQoL) from thepatients’ perspective can be evaluated. Conse-quently, it has become important to evaluate the
Quality of Life Research 13: 705–713, 2004.� 2004 Kluwer Academic Publishers. Printed in the Netherlands.
705

responsiveness or ‘sensitivity to change’ of healthstatus instruments and the efficacy of these instru-ments at detecting and describing changes in pa-tients’ health status over time [2].
We recently reported on the development of anew disease-specific instrument designed to mea-sure the HRQoL of women with endometriosis.The results of the psychometric tests carried outindicated that the Endometriosis Health Profile-30(EHP-30) was a reliable and valid instrument [3].However, in view of the potential use of the EHP-30 in clinical trials and the application of the in-strument to evaluate the outcomes of treatment forendometriosis upon a woman’s health status, it isimportant to determine the ‘responsiveness’ of thequestionnaire.
It has been argued that the responsiveness of aninstrument should be evaluated by using a therapyof known effectiveness [4, 5]. Conservative surgicaltreatment for endometriosis is chosen if the mainoutcome is to preserve fertility. Studies haveshown the effectiveness of conservative surgery asa treatment for endometriosis, especially in theshort term [6–9] and it is generally considered to bea precise and effective treatment procedure [10,11]. The aim of this study was to evaluate whetherthe EHP-30 was sensitive to changes in healthstatus in women who had undergone conservativesurgical treatment for endometriosis. The findingswould determine whether the EHP-30 would besuitable for use in clinical settings and for detect-ing and describing clinical changes in patients’health status over time.
Methods
A postal survey was administered to a conveniencesample of 66 women with a confirmed surgicaldiagnosis of endometriosis undergoing conserva-tive surgery at the John Radcliffe Hospital, Ox-ford.
Also administered with the EHP-30 was theShort Form-36 (SF-36) [12]. It has been arguedthat there is a need for studies to be conductedwhich evaluate ‘sensitivity to change’ using differ-ent health status measures, ideally including a ge-neric and disease-specific health statusquestionnaire [13, 14]. One reason for this is thatdifferent types of health status instruments can
present different patterns of change, thereby givingthe wrong impression regarding the efficacy of anintervention upon patients’ health status [14]. TheSF-36 was chosen as the generic measure of healthstatus as it is a well-validated questionnaire and ithas been shown to be suitable for use as an out-come measure in clinical settings [15].
There are two scales in the EHP-30 and the SF-36 which measure similar attributes: the bodilypain scale of the SF-36 and the pain dimension ofthe EHP-30 core questionnaire, and the mentalhealth scale of the SF-36 and the emotional well-being dimension on the EHP-30. However, al-though the social functioning dimension of theSF-36 and the social support scale on the EHP-30sound similar, they measure different attributes.The social functioning scale measures the impactof illness on patients’ ability to continue with theirsocial activities, whereas the EHP-30 scale mea-sures the impact of endometriosis upon a woman’ssocial support network.
Approximately 2 weeks before the operation,the two questionnaires were sent with an accom-panying letter to the women to assess their qualityof life. All the women had been previously ap-proached at the time of their clinic appointmentand consented to participate. Four months fol-lowing the operation, the SF-36 and the EHP-30were administered again. However, a transitionquestion was also included with the question-naires. The transition question which was used toexamine changes in health status was based on theglobal health perceptions question included in theSF-36. The global question on the SF-36 requiresthe respondent to evaluate their own health statusby answering the response categories ‘much better’,‘somewhat better’, ‘about the same’, ‘somewhatworse’, or ‘much worse’. Patients in this study wereasked to choose one of these response categories todescribe how they felt their health status was at the4 month follow up. Transition questions are oftenused to examine the responsiveness of an instru-ment as they provide a simple benchmark from theperspective of the patient regarding changes inhealth status following an intervention [16, 17].
Statistical methods
For both the EHP-30 and the SF-36, scale scoresare standardised on a range from 0 to 100. For the
706

EHP-30 lower scores indicate better health status,whilst for the SF-36 a lower score indicates poorerhealth.
To examine the relationship between variables,Spearman’s non-parametric correlation was usedand the paired t-test was used to examine the sig-nificance of change scores. To interpret the re-sponsiveness of the instrument, effect sizes,standardised response means (SRMs), and an in-dex of responsiveness were calculated. However,the problem with just using these statistical meth-ods is that it is difficult to interpret what thechange scores mean. Consequently, two othermethods were used to provide some meaning ofthe change scores: the clinically important differ-ence [4–5] and the minimally important difference[18].
Effect sizes are one of the most commonly usedmethods for interpreting change in scores [19] andare an estimation of the magnitude of change inhealth status between two different times [20].They were evaluated by calculating the differencebetween the means pre-treatment and post-treat-ment and dividing by the pre-treatment SD asrecommended by Kazis et al. [1]. Changes inhealth status were then translated into a standardunit of measurement which aids the interpretationof the results. An effect size of 0.20 indicates asmall change, whereas effect sizes of 0.50 and 0.80indicate moderate and large changes respectively[21]. A small effect size implies that treatment hashad little influence on the health status of the pa-tients. The SRM is very similar to the effect size.However, to calculate the SRM it involves dividingthe mean change on a scale by the mean change inthe SD [16]. This differs to the calculation of theeffect size which involves dividing by the pre-treatment SD. The sign of the effect size and SRMare influenced by the direction of the scoring of thescale. Consequently, negative effect sizes andSRMs indicate a positive improvement on the SF-36.
An index of responsiveness as proposed byGuyatt et al. [22] was calculated by dividing themean change in score for those patients who re-ported themselves to feel ‘somewhat better’ by thestandard deviation of those patients who felt‘about the same’ as reported on the retrospectivetransition question. Although an index of re-sponsiveness statistic of 0.20 is acceptable, a value
of 1.00 or more indicates that a measure is highlyresponsive to change [17].
To evaluate the ‘clinically important difference’,comparisons were made on dimension scores be-fore and after surgery. This is a form of constructvalidity as an hypothesis was made a priori that thechange scores would be in the direction clinicallyexpected. The minimal important difference placesthe change scores in the context of the patients’subjective judgment of their change in health sta-tus. Although different methods have been postu-lated for calculating the minimal importantdifference [18] it was estimated by subtracting theamount of change experienced by those patientswho reported that they felt ‘somewhat better’ attime 2 and reporting the mean change on eachdimension.
Results
Sixty-six women with endometriosis-associatedpain were recruited into the study. A total of 58(87.8%) women completed the questionnaire attime 1. Of these 18 (31%) did not return thequestionnaire at time 2, which gave complete dataon 40 (60.6%) patients. All analyses were con-ducted on complete data only. The mean age of thepatients was 34.3 years (SD ¼ 6.0: range 22.3–60.0, n ¼ 40). The average number of years sincediagnosis was 5.6 years (SD ¼ 5.9: range 0.2–24.0,n ¼ 37). Twenty-four (60%) of the respondentswere married, 10 (25%) co-habiting, 5 (12.5%)single and 1 (2.5%) separated. Twenty-eight (70%)of the women were nulliparous, 6 (15%) had onechild and 6 (15%) had two or more children. Atthe 4 month follow up the responses to the tran-sition questions were: 2 (5.0%) reported that theirhealth was much worse, 1 (2.5%) somewhat worse,18 (45.0%) the same, 11 (27.5%) somewhat betterand 8 (20.0%) much better.
The responsiveness of the EHP-30 was evaluat-ed by calculating effect sizes for all patients whohad undergone treatment (Table 1). These resultswere then compared with the effect size scoresgained for the SF-36 (Table 2). The results indi-cated that the EHP-30 was more responsive. Largeeffect sizes were found for two dimensions (controland powerlessness, and pain). Three dimensionsdemonstrated a moderate change (emotional well-
707
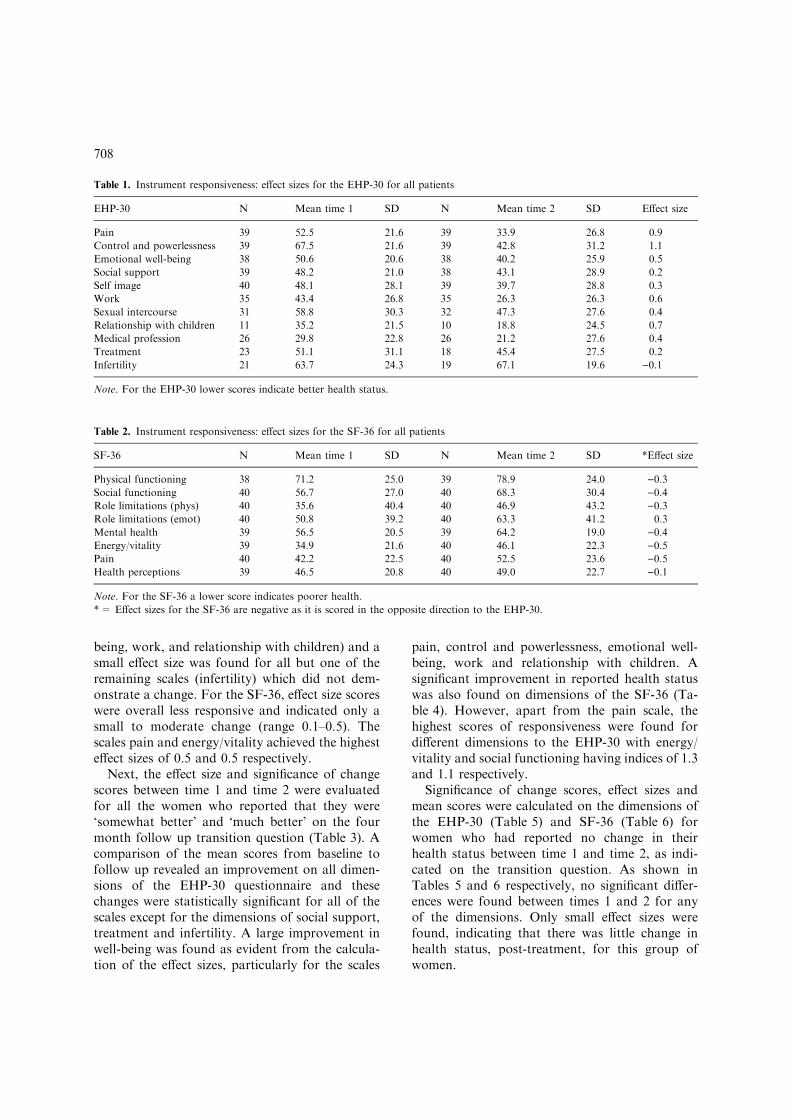
being, work, and relationship with children) and asmall effect size was found for all but one of theremaining scales (infertility) which did not dem-onstrate a change. For the SF-36, effect size scoreswere overall less responsive and indicated only asmall to moderate change (range 0.1–0.5). Thescales pain and energy/vitality achieved the highesteffect sizes of 0.5 and 0.5 respectively.
Next, the effect size and significance of changescores between time 1 and time 2 were evaluatedfor all the women who reported that they were‘somewhat better’ and ‘much better’ on the fourmonth follow up transition question (Table 3). Acomparison of the mean scores from baseline tofollow up revealed an improvement on all dimen-sions of the EHP-30 questionnaire and thesechanges were statistically significant for all of thescales except for the dimensions of social support,treatment and infertility. A large improvement inwell-being was found as evident from the calcula-tion of the effect sizes, particularly for the scales
pain, control and powerlessness, emotional well-being, work and relationship with children. Asignificant improvement in reported health statuswas also found on dimensions of the SF-36 (Ta-ble 4). However, apart from the pain scale, thehighest scores of responsiveness were found fordifferent dimensions to the EHP-30 with energy/vitality and social functioning having indices of 1.3and 1.1 respectively.
Significance of change scores, effect sizes andmean scores were calculated on the dimensions ofthe EHP-30 (Table 5) and SF-36 (Table 6) forwomen who had reported no change in theirhealth status between time 1 and time 2, as indi-cated on the transition question. As shown inTables 5 and 6 respectively, no significant differ-ences were found between times 1 and 2 for anyof the dimensions. Only small effect sizes werefound, indicating that there was little change inhealth status, post-treatment, for this group ofwomen.
Table 1. Instrument responsiveness: effect sizes for the EHP-30 for all patients
EHP-30 N Mean time 1 SD N Mean time 2 SD Effect size
Pain 39 52.5 21.6 39 33.9 26.8 0.9
Control and powerlessness 39 67.5 21.6 39 42.8 31.2 1.1
Emotional well-being 38 50.6 20.6 38 40.2 25.9 0.5
Social support 39 48.2 21.0 38 43.1 28.9 0.2
Self image 40 48.1 28.1 39 39.7 28.8 0.3
Work 35 43.4 26.8 35 26.3 26.3 0.6
Sexual intercourse 31 58.8 30.3 32 47.3 27.6 0.4
Relationship with children 11 35.2 21.5 10 18.8 24.5 0.7
Medical profession 26 29.8 22.8 26 21.2 27.6 0.4
Treatment 23 51.1 31.1 18 45.4 27.5 0.2
Infertility 21 63.7 24.3 19 67.1 19.6 )0.1
Note. For the EHP-30 lower scores indicate better health status.
Table 2. Instrument responsiveness: effect sizes for the SF-36 for all patients
SF-36 N Mean time 1 SD N Mean time 2 SD *Effect size
Physical functioning 38 71.2 25.0 39 78.9 24.0 )0.3Social functioning 40 56.7 27.0 40 68.3 30.4 )0.4Role limitations (phys) 40 35.6 40.4 40 46.9 43.2 )0.3Role limitations (emot) 40 50.8 39.2 40 63.3 41.2 0.3
Mental health 39 56.5 20.5 39 64.2 19.0 )0.4Energy/vitality 39 34.9 21.6 40 46.1 22.3 )0.5Pain 40 42.2 22.5 40 52.5 23.6 )0.5Health perceptions 39 46.5 20.8 40 49.0 22.7 )0.1
Note. For the SF-36 a lower score indicates poorer health.
*= Effect sizes for the SF-36 are negative as it is scored in the opposite direction to the EHP-30.
708
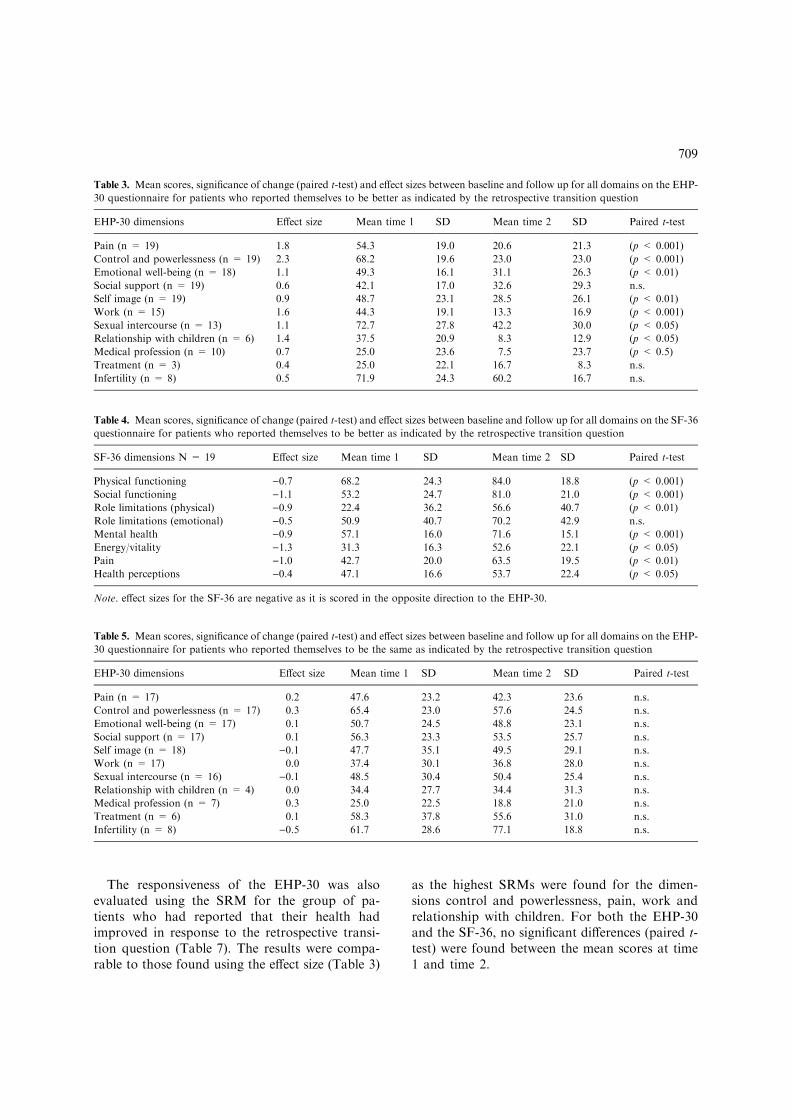
The responsiveness of the EHP-30 was alsoevaluated using the SRM for the group of pa-tients who had reported that their health hadimproved in response to the retrospective transi-tion question (Table 7). The results were compa-rable to those found using the effect size (Table 3)
as the highest SRMs were found for the dimen-sions control and powerlessness, pain, work andrelationship with children. For both the EHP-30and the SF-36, no significant differences (paired t-test) were found between the mean scores at time1 and time 2.
Table 3. Mean scores, significance of change (paired t-test) and effect sizes between baseline and follow up for all domains on the EHP-
30 questionnaire for patients who reported themselves to be better as indicated by the retrospective transition question
EHP-30 dimensions Effect size Mean time 1 SD Mean time 2 SD Paired t-test
Pain (n = 19) 1.8 54.3 19.0 20.6 21.3 (p < 0.001)
Control and powerlessness (n = 19) 2.3 68.2 19.6 23.0 23.0 (p < 0.001)
Emotional well-being (n = 18) 1.1 49.3 16.1 31.1 26.3 (p < 0.01)
Social support (n = 19) 0.6 42.1 17.0 32.6 29.3 n.s.
Self image (n = 19) 0.9 48.7 23.1 28.5 26.1 (p < 0.01)
Work (n = 15) 1.6 44.3 19.1 13.3 16.9 (p < 0.001)
Sexual intercourse (n = 13) 1.1 72.7 27.8 42.2 30.0 (p < 0.05)
Relationship with children (n = 6) 1.4 37.5 20.9 8.3 12.9 (p < 0.05)
Medical profession (n = 10) 0.7 25.0 23.6 7.5 23.7 (p < 0.5)
Treatment (n = 3) 0.4 25.0 22.1 16.7 8.3 n.s.
Infertility (n = 8) 0.5 71.9 24.3 60.2 16.7 n.s.
Table 4. Mean scores, significance of change (paired t-test) and effect sizes between baseline and follow up for all domains on the SF-36
questionnaire for patients who reported themselves to be better as indicated by the retrospective transition question
SF-36 dimensions N = 19 Effect size Mean time 1 SD Mean time 2 SD Paired t-test
Physical functioning )0.7 68.2 24.3 84.0 18.8 (p < 0.001)
Social functioning )1.1 53.2 24.7 81.0 21.0 (p < 0.001)
Role limitations (physical) )0.9 22.4 36.2 56.6 40.7 (p < 0.01)
Role limitations (emotional) )0.5 50.9 40.7 70.2 42.9 n.s.
Mental health )0.9 57.1 16.0 71.6 15.1 (p < 0.001)
Energy/vitality )1.3 31.3 16.3 52.6 22.1 (p < 0.05)
Pain )1.0 42.7 20.0 63.5 19.5 (p < 0.01)
Health perceptions )0.4 47.1 16.6 53.7 22.4 (p < 0.05)
Note. effect sizes for the SF-36 are negative as it is scored in the opposite direction to the EHP-30.
Table 5. Mean scores, significance of change (paired t-test) and effect sizes between baseline and follow up for all domains on the EHP-
30 questionnaire for patients who reported themselves to be the same as indicated by the retrospective transition question
EHP-30 dimensions Effect size Mean time 1 SD Mean time 2 SD Paired t-test
Pain (n = 17) 0.2 47.6 23.2 42.3 23.6 n.s.
Control and powerlessness (n = 17) 0.3 65.4 23.0 57.6 24.5 n.s.
Emotional well-being (n = 17) 0.1 50.7 24.5 48.8 23.1 n.s.
Social support (n = 17) 0.1 56.3 23.3 53.5 25.7 n.s.
Self image (n = 18) )0.1 47.7 35.1 49.5 29.1 n.s.
Work (n = 17) 0.0 37.4 30.1 36.8 28.0 n.s.
Sexual intercourse (n = 16) )0.1 48.5 30.4 50.4 25.4 n.s.
Relationship with children (n = 4) 0.0 34.4 27.7 34.4 31.3 n.s.
Medical profession (n = 7) 0.3 25.0 22.5 18.8 21.0 n.s.
Treatment (n = 6) 0.1 58.3 37.8 55.6 31.0 n.s.
Infertility (n = 8) )0.5 61.7 28.6 77.1 18.8 n.s.
709
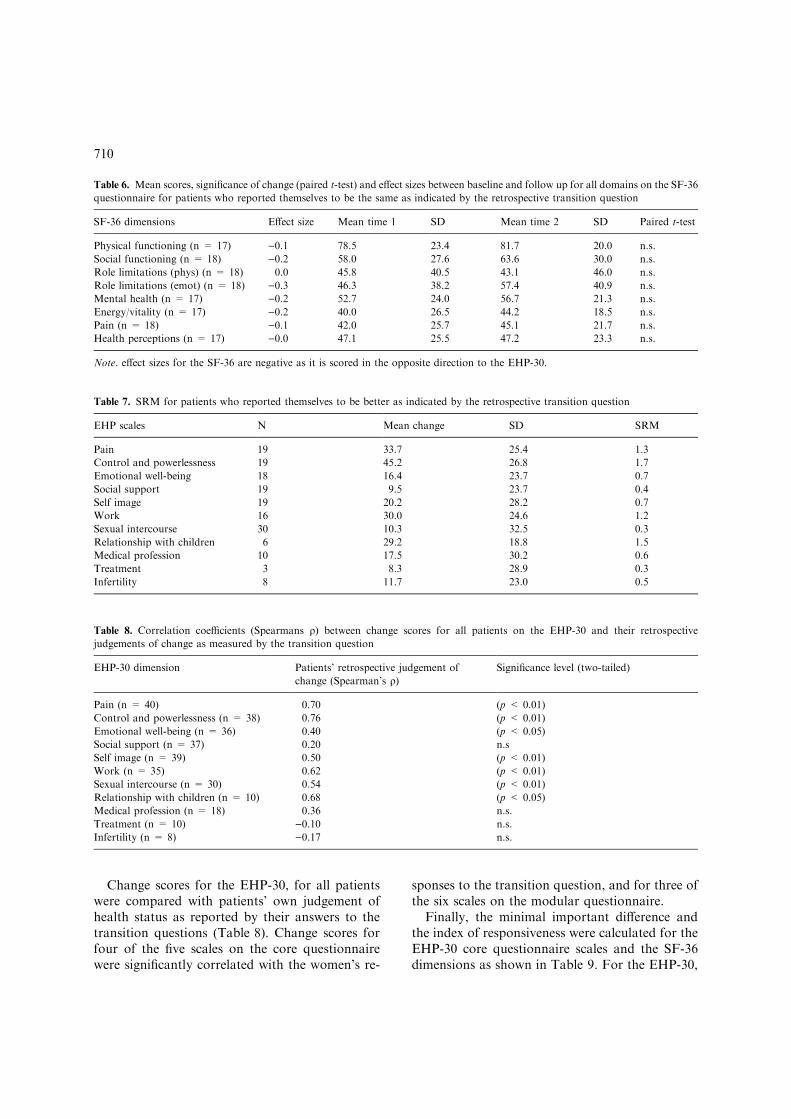
Change scores for the EHP-30, for all patientswere compared with patients’ own judgement ofhealth status as reported by their answers to thetransition questions (Table 8). Change scores forfour of the five scales on the core questionnairewere significantly correlated with the women’s re-
sponses to the transition question, and for three ofthe six scales on the modular questionnaire.
Finally, the minimal important difference andthe index of responsiveness were calculated for theEHP-30 core questionnaire scales and the SF-36dimensions as shown in Table 9. For the EHP-30,
Table 6. Mean scores, significance of change (paired t-test) and effect sizes between baseline and follow up for all domains on the SF-36
questionnaire for patients who reported themselves to be the same as indicated by the retrospective transition question
SF-36 dimensions Effect size Mean time 1 SD Mean time 2 SD Paired t-test
Physical functioning (n = 17) )0.1 78.5 23.4 81.7 20.0 n.s.
Social functioning (n = 18) )0.2 58.0 27.6 63.6 30.0 n.s.
Role limitations (phys) (n = 18) 0.0 45.8 40.5 43.1 46.0 n.s.
Role limitations (emot) (n = 18) )0.3 46.3 38.2 57.4 40.9 n.s.
Mental health (n = 17) )0.2 52.7 24.0 56.7 21.3 n.s.
Energy/vitality (n = 17) )0.2 40.0 26.5 44.2 18.5 n.s.
Pain (n = 18) )0.1 42.0 25.7 45.1 21.7 n.s.
Health perceptions (n = 17) )0.0 47.1 25.5 47.2 23.3 n.s.
Note. effect sizes for the SF-36 are negative as it is scored in the opposite direction to the EHP-30.
Table 7. SRM for patients who reported themselves to be better as indicated by the retrospective transition question
EHP scales N Mean change SD SRM
Pain 19 33.7 25.4 1.3
Control and powerlessness 19 45.2 26.8 1.7
Emotional well-being 18 16.4 23.7 0.7
Social support 19 9.5 23.7 0.4
Self image 19 20.2 28.2 0.7
Work 16 30.0 24.6 1.2
Sexual intercourse 30 10.3 32.5 0.3
Relationship with children 6 29.2 18.8 1.5
Medical profession 10 17.5 30.2 0.6
Treatment 3 8.3 28.9 0.3
Infertility 8 11.7 23.0 0.5
Table 8. Correlation coefficients (Spearmans q) between change scores for all patients on the EHP-30 and their retrospective
judgements of change as measured by the transition question
EHP-30 dimension Patients’ retrospective judgement of
change (Spearman’s q)Significance level (two-tailed)
Pain (n = 40) 0.70 (p < 0.01)
Control and powerlessness (n = 38) 0.76 (p < 0.01)
Emotional well-being (n = 36) 0.40 (p < 0.05)
Social support (n = 37) 0.20 n.s
Self image (n = 39) 0.50 (p < 0.01)
Work (n = 35) 0.62 (p < 0.01)
Sexual intercourse (n = 30) 0.54 (p < 0.01)
Relationship with children (n = 10) 0.68 (p < 0.05)
Medical profession (n = 18) 0.36 n.s.
Treatment (n = 10) )0.10 n.s.
Infertility (n = 8) )0.17 n.s.
710
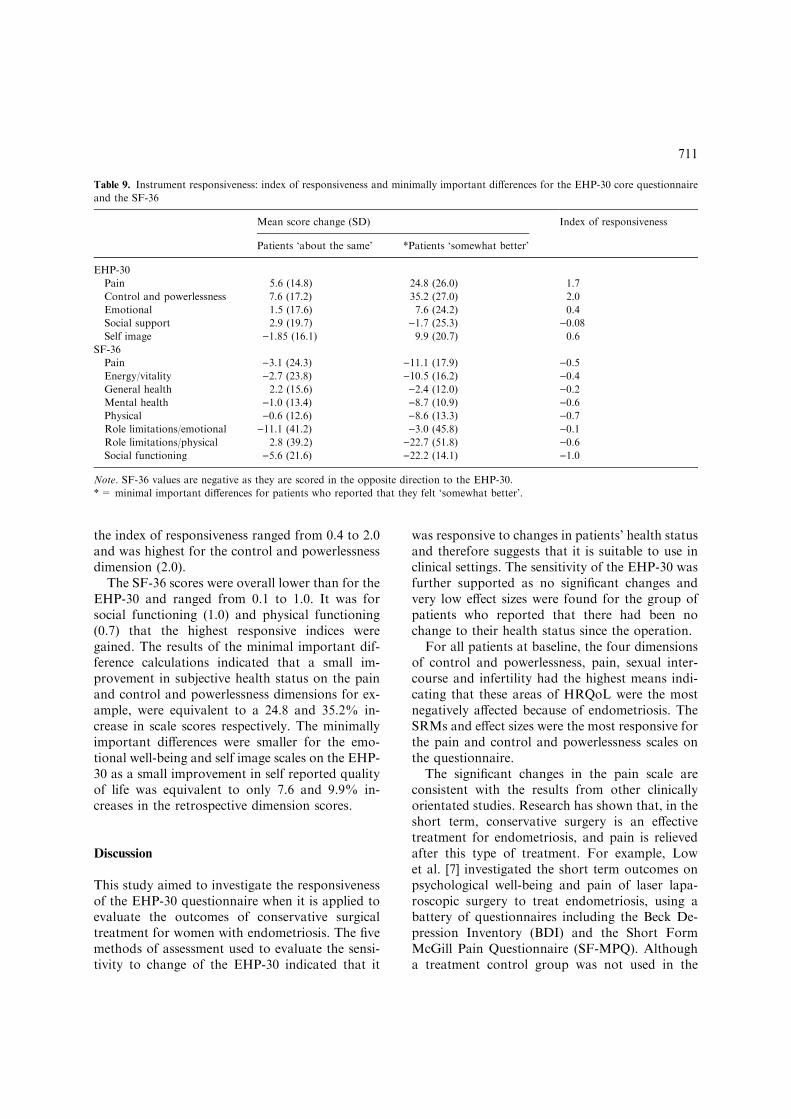
the index of responsiveness ranged from 0.4 to 2.0and was highest for the control and powerlessnessdimension (2.0).
The SF-36 scores were overall lower than for theEHP-30 and ranged from 0.1 to 1.0. It was forsocial functioning (1.0) and physical functioning(0.7) that the highest responsive indices weregained. The results of the minimal important dif-ference calculations indicated that a small im-provement in subjective health status on the painand control and powerlessness dimensions for ex-ample, were equivalent to a 24.8 and 35.2% in-crease in scale scores respectively. The minimallyimportant differences were smaller for the emo-tional well-being and self image scales on the EHP-30 as a small improvement in self reported qualityof life was equivalent to only 7.6 and 9.9% in-creases in the retrospective dimension scores.
Discussion
This study aimed to investigate the responsivenessof the EHP-30 questionnaire when it is applied toevaluate the outcomes of conservative surgicaltreatment for women with endometriosis. The fivemethods of assessment used to evaluate the sensi-tivity to change of the EHP-30 indicated that it
was responsive to changes in patients’ health statusand therefore suggests that it is suitable to use inclinical settings. The sensitivity of the EHP-30 wasfurther supported as no significant changes andvery low effect sizes were found for the group ofpatients who reported that there had been nochange to their health status since the operation.
For all patients at baseline, the four dimensionsof control and powerlessness, pain, sexual inter-course and infertility had the highest means indi-cating that these areas of HRQoL were the mostnegatively affected because of endometriosis. TheSRMs and effect sizes were the most responsive forthe pain and control and powerlessness scales onthe questionnaire.
The significant changes in the pain scale areconsistent with the results from other clinicallyorientated studies. Research has shown that, in theshort term, conservative surgery is an effectivetreatment for endometriosis, and pain is relievedafter this type of treatment. For example, Lowet al. [7] investigated the short term outcomes onpsychological well-being and pain of laser lapa-roscopic surgery to treat endometriosis, using abattery of questionnaires including the Beck De-pression Inventory (BDI) and the Short FormMcGill Pain Questionnaire (SF-MPQ). Althougha treatment control group was not used in the
Table 9. Instrument responsiveness: index of responsiveness and minimally important differences for the EHP-30 core questionnaire
and the SF-36
Mean score change (SD) Index of responsiveness
Patients ‘about the same’ *Patients ‘somewhat better’
EHP-30
Pain 5.6 (14.8) 24.8 (26.0) 1.7
Control and powerlessness 7.6 (17.2) 35.2 (27.0) 2.0
Emotional 1.5 (17.6) 7.6 (24.2) 0.4
Social support 2.9 (19.7) )1.7 (25.3) )0.08Self image )1.85 (16.1) 9.9 (20.7) 0.6
SF-36
Pain )3.1 (24.3) )11.1 (17.9) )0.5Energy/vitality )2.7 (23.8) )10.5 (16.2) )0.4General health 2.2 (15.6) )2.4 (12.0) )0.2Mental health )1.0 (13.4) )8.7 (10.9) )0.6Physical )0.6 (12.6) )8.6 (13.3) )0.7Role limitations/emotional )11.1 (41.2) )3.0 (45.8) )0.1Role limitations/physical 2.8 (39.2) )22.7 (51.8) )0.6Social functioning )5.6 (21.6) )22.2 (14.1) )1.0
Note. SF-36 values are negative as they are scored in the opposite direction to the EHP-30.
*= minimal important differences for patients who reported that they felt ‘somewhat better’.
711
study, a statistically significant change in scoresfrom the initial assessment to the 3 month followup in both pain and psychological state was found.
The results from other studies which havemeasured the sensitivity to change of existing en-dometriosis-specific questionnaires have alsofound a marked improvement in the short term inrelation to pain outcomes. For example, Bodneret al. [23] used the SRM to evaluate the respon-siveness of their endometriosis-specific instrumentin two groups of patients: those who receivedtreatment (n ¼ 52) and those who did not (n ¼ 62)over a 6 month period. Small changes were found(e.g. between 0.2 and 0.5) on all dimensions of thequestionnaire except for the pain scale which hadmoderate to large SRMs. Similarly, Colwell et al.[17] found that on their endometriosis-specificquestionnaire many of the scales were moderatelyto highly sensitive to change for women who hadreported an improvement in their endometriosis-associated pain. The most highly sensitive tochange scales were physical functioning, rolefunctioning/physical and bodily pain.
Only one scale on the EHP-30 core question-naire failed to demonstrate any responsiveness(social support), possibly because the items on thequestionnaire are too broad to detect subtlechanges or because too many items on the in-strument are not relevant to the clinical trial [24].However, significant improvements were found onthe social functioning dimension of the SF-36.This dimension measures the impact of illness onpatients’ ability to continue with their social ac-tivities. This is in contrast to the EHP-30 scalewhich measures the impact of endometriosis upona woman’s social support network. The findingsfrom this study therefore suggest that conservativesurgical treatment for endometriosis has a greaterpositive impact on a woman’s ability to resume hersocial activities, which is perhaps not surprisinggiven the significant improvements found on thepain scale.
Overall, the EHP-30 demonstrated greater re-sponsiveness than the SF-36. For example, theEHP-30 pain scale was more responsive than theSF-36 bodily pain scale. In addition, all the scalesof the EHP-30 core questionnaire, except the so-cial support scale, demonstrated high responsive-ness and overall were greater than those found onthe SF-36. This was in the direction expected given
that the items on the questionnaire were areas ofHRQoL identified to be of most concern towomen with endometriosis. This finding is con-sistent with other research which has foundincreased responsiveness of disease-specific instru-ments compared to generic questionnaires [14, 23,25]. For example, Paterson et al. [25] found thatthe Measure Yourself Medical Outcome Profile(MYMOP) was more sensitive to change than thegeneric Medical Outcomes Study 6-item generalhealth survey (MOS-6A) and the EQ-5D whenused to measure treatment outcomes for patientswith acute exacerbations of chronic bronchitis.
Overall, the majority of the women who un-derwent conservative surgery had laser laparo-scopic treatment for their endometriosis. At thefour month follow up, 47.5% (n ¼ 19) of thesewomen who had laser surgery for their endo-metriosis reported a short term improvement intheir health status after the treatment. This was inthe direction clinically expected as positive findingshave been found with laser laparoscopy in theshort term [6]. This finding also supports a previ-ous study which measured the short term impactof conservative surgery on HRQoL in 57 patientsundergoing laparoscopic excision of endometrioticdeposits [26]. Positive short term improvementswere found at the four month follow up as mea-sured by the SF-12.
One possible criticism of this study is the smalldata set which was used. However, it has beensuggested that only relatively small data sets arerequired to examine the responsiveness of instru-ments [27]. For example, to determine the minimalimportant difference for an asthma quality of lifequestionnaire, complete data were only availablefor 37 subjects [27].
In conclusion, for women undergoing conser-vative surgery as a treatment for their endo-metriosis, it appears that health status improvesat least in the short term. However, it is recom-mended that more studies which have longerfollow up times be conducted to further deter-mine the impact that the different medical andsurgical interventions for endometriosis have up-on the health status of the patient. The findingsfrom this study have indicated that the EHP-30 issensitive to change and suggests that it may be anappropriate instrument to use in such futurestudies.
712

Acknowledgements
The authors thank Pharmacia Corporation, USfor funding this research.
References
1. Kazis LE, Anderson JJ, Meenan RF. Effect sizes for in-
terpreting changes in health status. Med Care 1989; 27:
S178–S189.
2. Streiner DL, Norman G. Health Measurement Scales: A
Practical Guide to their Development and Use. 2nd ed.
Oxford: Oxford University Press, 1995.
3. Jones G, Kennedy S, Barnard A, Wong J, Jenkinson C.
Development of an endometriosis quality-of-life instru-
ment: The Endometriosis Health Profile-30. Obstet Gynecol
2001; 98: 258–264.
4. Guyatt G, Walter S, Norman G. Measuring change over
time: Assessing the usefulness of evaluative instruments. J
Chron Dis 1987; 40: 171–178.
5. Fayers PM, Machin D. Quality of Life: Assessment,
Analysis and Interpretation. Chichester: John Wiley &
Sons, 2000.
6. Sutton CJG, Hill D. Laser laparoscopy in the treatment of
endometriosis: A 5-year study. Br J Obstet Gynaecol 1990;
97: 181–185.
7. Low YL, Edelmann RJ, Sutton C. A psychological profile
of endometriosis patients in comparison to patients with
pelvic pain of other origins. J Psychosom Res 1993; 37:
111–116.
8. Daniell JF. Laser laparoscopy for endometriosis. Colpos-
copy Gynecol Laser Surg 1984; 1: 185–192.
9. Donnez J. Today’s treatments: Medical, surgical and in
partnership. Int J Gynecol Obstet 1999; 1: S5–S13.
10. Adamson GD, Hurd SJ, Pasta DJ, Rodriguez BD. Lapa-
roscopic endometriosis treatment: Is it better? Fertil Steril
1993; 59: 35–44.
11. Sutton CJ. What can we expect from the surgical man-
agement of endometriosis? Br J Clin Pract Suppl 1991; 72:
33–42.
12. Ware JE, Sherbourne EC. The MOS 36-Item Short Form
Health Survey 1: Conceptual Framework and Item Selec-
tion. Med Care 1992; 30: 473–483.
13. Liang MH, Fossel AH, Larson MG. Comparisons of five
health status instruments for orthopedic evaluation. Med
Care 1990; 28: 263–642.
14. Fitzpatrick R, Ziebland S, Jenkinson C, Mowat A, Mowat
A. A comparison of the sensitivity to change of several
health status instruments in rheumatoid arthritis. J Rheu-
matol 1993; 20: 429–436.
15. Kosinski M, Keller SD, Hatoum HT, Kong SX, Ware JE.
The SF-36 Health Survey as a generic outcome measure in
clinical trials of patients with osteoarthritis and rheumatoid
arthritis: Tests of data quality, scaling assumptions and
score reliability. Med Care 1999; 37: MS10–MS22.
16. Jenkinson C. Measuring Health and Medical Outcomes.
London: UCL Press, 1994.
17. Colwell H, Mathias SD, Pasta DJ, Henning JM, Steege JF.
A health-related quality of life instrument for symptomatic
patients with endometriosis: A validation study. Am J
Obstet Gynecol 1998; 179: 47–55.
18. Guyatt GH, Feeny D, Patrick D. Proceedings of the in-
ternational conference on the measurement of quality of life
as an outcome in clinical trials: Postscript. Controlled Clin
Trials 1991; 12: 266s–269s.
19. Lydick E, Epstein RS. Interpretation of quality of life
changes. Qual Life Res 1993; 2: 221–226.
20. Lohr KN, Aaronson NK, Alonso J, Burnam MA, Patrick
DL, Perin EB. Evaluating quality of life and health status
instruments: Development of scientific review criteria. Clin
Ther 1996; 18: 979–992.
21. Cohen J. Statistical Power Analysis for the Behaviourial
Sciences. New York: Academic Press, 1977.
22. Guyatt GH, Eagle DJ, Sackett B. Measuring quality of life
in the frail elderly. J Clin Epidemiol 1993; 46: 1433–1444.
23. Bodner C, Garratt AM, Ratcliffe J, Macdonald LM, Pen-
ney GC. Measuring health-related quality of life outcomes
in women with endometriosis: Results of the gynaecology
audit project in Scotland. Health Bull (Edinb) 1997; 55:
109–117.
24. Fitzpatrick R. Applications of health status measures. In:
Jenkinson, C (ed.), Measuring Health and Medical Out-
comes, London: UCL Press, 1994: 27–41.
25. Paterson C, Langan CE, McKaig GA, et al. Assessing pa-
tient outcomes in acute exacerbations of chronic bronchitis:
The measure your medical outcome profile (MYMOP),
medical outcomes study 6-item general health survey
(MOS-6A) and EuroQol (EQ-5D). Qual Life Res 2000; 9:
521–527.
26. Garry R, Clayton R, Hawe J. The effect of endometriosis
and its radical laparoscopic excision on quality of life in-
dicators. Br J Obstet Gynaecol 2000; 107: 44–54.
27. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determin-
ing a minimal important change in a disease-specific quality
of life questionnaire. J Clin Epidemiol 1994; 47: 81–87.
Address for correspondence: Georgina Jones, Institute of Gen-
eral Practice and Primary Care, Community Sciences Centre,
Northern General Hospital, Herries Road, Sheffield S5 7AU,
UK
Phone: +44-114-2715929
E-mail: [email protected]
713