evidence-based approaches to medication … k et al: evidence-based practice in child and adolescent...
TRANSCRIPT

EvidenceEvidence--Based Approaches to Based Approaches to Medication Management in Psychiatry:Medication Management in Psychiatry:
Promises and PitfallsPromises and Pitfalls
Michael Flaum, MDMichael Flaum, MDDepartment of PsychiatryDepartment of Psychiatry
University of Iowa Carver College of MedicineUniversity of Iowa Carver College of Medicine
Director, Iowa Consortium for Mental HealthDirector, Iowa Consortium for Mental Health
April 8, 2005April 8, 2005
OutlineOutline
IntroductionIntroductionWho I am, ICMH activities around EBPWho I am, ICMH activities around EBP’’ss
EvidenceEvidence--based practicesbased practicesdefinitions and conceptsdefinitions and concepts
Why the push for EBPWhy the push for EBP’’s?s?PORT studyPORT study
Using evidenceUsing evidence--based approaches in based approaches in psychoactive prescribing psychoactive prescribing -- MedMAPMedMAP

My My Contact InfoContact Info
ee--mail: mail: [email protected]@uiowa.edu
Phone: 319Phone: 319--353353--4340 4340
Web site: Web site: www.icmentalhealth.orgwww.icmentalhealth.org
Iowa Consortium for Mental HealthIowa Consortium for Mental Health
Began in 1994Began in 1994
Mission: To enhance mutually Mission: To enhance mutually beneficial collaboration between Iowabeneficial collaboration between Iowa’’s s universities and its public mental universities and its public mental health system health system
Focus over past several years: Focus over past several years: EvidenceEvidence--based practices in mental based practices in mental healthhealth

ICMH Technical Assistance Center for ICMH Technical Assistance Center for EvidenceEvidence--Based PracticesBased Practices
Supported by:Supported by:
Iowa DHSIowa DHSCommunity Mental Health Block GrantCommunity Mental Health Block Grant
Magellan Behavior HealthMagellan Behavior HealthCommunity ReinvestmentCommunity Reinvestment
National Institute of Mental HealthNational Institute of Mental HealthOutreach Partners ProgramOutreach Partners Program
ICMH EBPICMH EBP--TAC ActivitiesTAC Activities
ICN Series: EvidenceICN Series: Evidence--Based Practices in Based Practices in Mental Health: Ready or Not Here They ComeMental Health: Ready or Not Here They Come
TA to CMHCTA to CMHC’’s on EBPs on EBP’’s as per new legislations as per new legislationSF 2288SF 2288Mandates that all CMH Block Grant money be used Mandates that all CMH Block Grant money be used for EBPfor EBP’’ss
ACT TACACT TAC
WMR TACWMR TAC

EvidenceEvidence--Based Practice in Mental Based Practice in Mental Health: Health: Ready or Not, Here They ComeReady or Not, Here They Come
ICN Site
ICN Series, Summer-Fall, 2004
Objectives of Session I: Objectives of Session I: EBP Overview, Definitions and ConceptsEBP Overview, Definitions and Concepts
Understand what is meant by the term Understand what is meant by the term ““evidence based practice(s)evidence based practice(s)””
Review the main factors driving public Review the main factors driving public mental health systems towards EBPmental health systems towards EBP’’ss
Describe the concept of Describe the concept of ““model fidelitymodel fidelity”” and and methods of its evaluationmethods of its evaluation
Recognize the limitations of the EBP Recognize the limitations of the EBP approach in mental healthapproach in mental health
Discuss barriers to implementation and Discuss barriers to implementation and strategies to overcome themstrategies to overcome them

Cautionary noteCautionary note
““As is true with any newly popularized As is true with any newly popularized term, the term term, the term ‘‘evidenceevidence--basedbased’’ has an has an almost intuitive ring of credibility to italmost intuitive ring of credibility to it……
……But thisBut this ring may be hollowring may be hollow””..
Hoagwood K et al: EvidenceHoagwood K et al: Evidence--Based Practice in Child and Adolescent Based Practice in Child and Adolescent Mental Health Services.Mental Health Services. Psychiatr Serv 52:1179Psychiatr Serv 52:1179--1189, 20011189, 2001
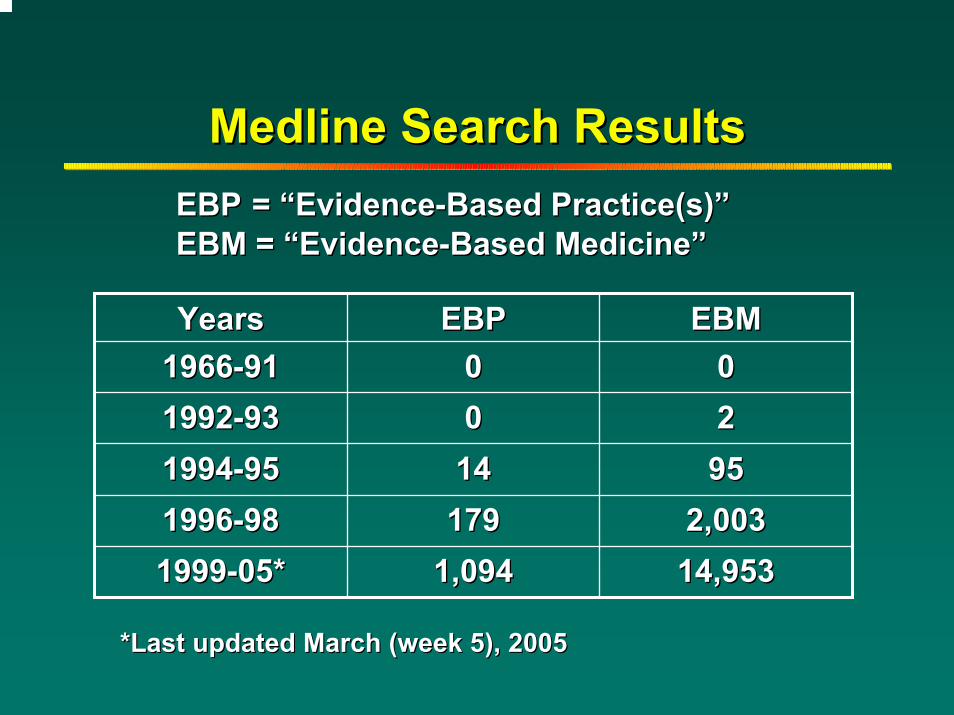
Medline Search ResultsMedline Search Results
YearsYears EBPEBP EBMEBM19661966--9191 00 0019921992--9393 00 2219941994--9595 1414 959519961996--9898 179179 2,0032,00319991999--05*05* 1,0941,094 14,95314,953
EBPEBP = = ““EvidenceEvidence--Based Practice(s)Based Practice(s)””EBM = EBM = ““EvidenceEvidence--Based MedicineBased Medicine””
*Last updated March (week 5), 2005*Last updated March (week 5), 2005
Selected DefinitionsSelected Definitions
Best PracticeBest Practice
EvidenceEvidence--Based PracticeBased Practice
Evidence Based MedicineEvidence Based Medicine
““Best PracticeBest Practice””: : Selected Generic DefinitionsSelected Generic Definitions
…… policies, principles, standards, policies, principles, standards, guidelines, and procedures that guidelines, and procedures that contribute to the highest, most contribute to the highest, most resourceresource-- effective performance of a effective performance of a discipline.discipline.
……a technique or methodology that, a technique or methodology that, through experience and research, has through experience and research, has proven to reliably lead to a desired proven to reliably lead to a desired result.result.
EvidenceEvidence--Based PracticesBased PracticesSelected Definitions (1)Selected Definitions (1)
Interventions for which there is Interventions for which there is consistent scientific evidence showing consistent scientific evidence showing that they improve client outcomes.that they improve client outcomes.
Source: Drake RE et al, Psychiatric Services, 52:179Source: Drake RE et al, Psychiatric Services, 52:179--82, 200182, 2001

EvidenceEvidence--Based PracticesBased PracticesSelected Definitions (2)Selected Definitions (2)
Intervention with a body of evidence:Intervention with a body of evidence:-- rigorous research studies rigorous research studies -- specified target population specified target population -- specified client outcomesspecified client outcomes
Specific implementation criteria (e.g., Specific implementation criteria (e.g., treatment manual)treatment manual)
A track record showing that the practice can A track record showing that the practice can be implemented in different settingsbe implemented in different settings
Source: Bond G, et al, 2001Source: Bond G, et al, 2001
““ EvidenceEvidence--based medicinebased medicine””Selected definitionsSelected definitions
"Evidence"Evidence--based medicine involves based medicine involves evaluating rigorously the effectiveness of evaluating rigorously the effectiveness of healthcare interventions, disseminating the healthcare interventions, disseminating the results of evaluation and using those findings results of evaluation and using those findings to influence clinical practice.to influence clinical practice.
It can be a complex task, in which the It can be a complex task, in which the production of evidence, its dissemination to production of evidence, its dissemination to the right audiences, and the implementation the right audiences, and the implementation of change can all present problems". of change can all present problems".
Source: Appleby J, Walshe K and Ham C (1995).Source: Appleby J, Walshe K and Ham C (1995). Acting on Acting on the Evidence (NAHAT Research Paper No. 17). Birminghamthe Evidence (NAHAT Research Paper No. 17). Birmingham
Why the push for EBPWhy the push for EBP’’s? s?
Many advances in understanding and Many advances in understanding and treating mental illnesses over past few treating mental illnesses over past few decadesdecades
Limited evidence of improved Limited evidence of improved outcomesoutcomes
““Science to serviceScience to service”” gapgap

Why EBPWhy EBP’’s? Surgeon Generals? Surgeon General’’s s Report on Mental Health (1999)Report on Mental Health (1999)
““A wide variety of effective, communityA wide variety of effective, community--based based services, carefully refined through years of services, carefully refined through years of research, exist for even the most severe research, exist for even the most severe mental illnesses yet are not being translated mental illnesses yet are not being translated into community settings.into community settings.””
““Numerous explanations for the gap between Numerous explanations for the gap between what is known from research and what is what is known from research and what is practiced beg for innovative strategies to practiced beg for innovative strategies to bridge it.bridge it.””
From Ch 8: A vision for the futureFrom Ch 8: A vision for the future

Why the push for EBP's? Why the push for EBP's?
Despite extensive evidence and agreement on Despite extensive evidence and agreement on effective mental health practices for persons effective mental health practices for persons with SMI, research shows that routine mental with SMI, research shows that routine mental health programs do not provide EBPhealth programs do not provide EBP’’s to the s to the great majority of clients with these illnessesgreat majority of clients with these illnesses
This finding was a major conclusion of the This finding was a major conclusion of the surgeon generalsurgeon general’’s report (1999)s report (1999)
PORT study PORT study –– the most extensive the most extensive demonstration of the problem. demonstration of the problem.
Source: Drake RE et al, Psychiatric Services, 52:179Source: Drake RE et al, Psychiatric Services, 52:179--82, 200182, 2001

PORT Study: Patient Outcomes PORT Study: Patient Outcomes Research TeamResearch Team
Sponsors and PartnersSponsors and PartnersNIMH and AHCPR (Agency for Health Care Policy NIMH and AHCPR (Agency for Health Care Policy and Research) 1992and Research) 1992Joint effort: Hopkins, University of MarylandJoint effort: Hopkins, University of Maryland
2 major components and goals2 major components and goalsPORT 1: To develop recommendations for the PORT 1: To develop recommendations for the treatment of persons with treatment of persons with schizophreniaschizophrenia, based on , based on a synthesis of the best scientific evidence. a synthesis of the best scientific evidence. PORT 2: To quantify concurrence of actual PORT 2: To quantify concurrence of actual practice with these recommendationspractice with these recommendations
Source: Lehman et al: Schizophrenia Bulletin, Source: Lehman et al: Schizophrenia Bulletin, 24:1124:11--20, 199820, 1998
PORT 1: Generating RecommendationsPORT 1: Generating Recommendations
Literature reviewLiterature review
Strength of evidence evaluated for a Strength of evidence evaluated for a variety of interventions (A variety of interventions (A –– C)C)
30 level A recommendations generated30 level A recommendations generatedStrong evidence baseStrong evidence base
PORT PORT –– Levels of Evidence Criteria*Levels of Evidence Criteria*
Level A: Good researchLevel A: Good research--based evidence, with based evidence, with some expert opinion to support some expert opinion to support recommendationrecommendation
Level B: Fair researchLevel B: Fair research--based evidence, with based evidence, with substantial expert opinion to support substantial expert opinion to support recommendationrecommendation
Level C: Minimal researchLevel C: Minimal research--based evidence, based evidence, primarily based on expert opinion and primarily based on expert opinion and significant clinical experience to support significant clinical experience to support recommendationrecommendation
*Adapted from AHCPR Depression Guidelines*Adapted from AHCPR Depression Guidelines
PORT 1 Results: 30 Treatment PORT 1 Results: 30 Treatment Recommendations (Level A)Recommendations (Level A)
Somatic Treatments: 21Somatic Treatments: 21Pharmacotherapy: 18Pharmacotherapy: 18ECT: 3ECT: 3
Psychological Treatment: 2Psychological Treatment: 2
Family Treatment: 3Family Treatment: 3
Vocational Rehabilitation: 2Vocational Rehabilitation: 2
Service Systems: (ACT) 2Service Systems: (ACT) 2

PORT 2: Conformance StudyPORT 2: Conformance Study
Survey of a stratified random sample of 719 Survey of a stratified random sample of 719 pts with schizophrenia in 2 statespts with schizophrenia in 2 states
Public, private, VAPublic, private, VAInpatient, outpatientInpatient, outpatientDrawn from multiple communitiesDrawn from multiple communities
Looked at concurrence of practice with 12 Looked at concurrence of practice with 12 PORT treatment recommendationsPORT treatment recommendations
Dichotomous ratings (conform vs. not)Dichotomous ratings (conform vs. not)
Source: Lehman et al: Schizophrenia Bulletin, Source: Lehman et al: Schizophrenia Bulletin, 24:1124:11--20, 199820, 1998

PORT Study: Care for Schizophrenia PORT Study: Care for Schizophrenia Lags Behind ScienceLags Behind Science
Schizophrenia PORTSchizophrenia PORT ActualActualTreatment RecommendationsTreatment Recommendations Treatment Rates (%)Treatment Rates (%)
Antipsychotic medication for new orAntipsychotic medication for new orrelapsed symptomsrelapsed symptoms11 89.289.2
Appropriate dose of antipsychoticAppropriate dose of antipsychoticmedication for new or relapsed symptomsmedication for new or relapsed symptoms11 62.462.4
Antipsychotic medication on an ongoing basisAntipsychotic medication on an ongoing basis22 92.392.3
Appropriate dose of ongoing antipsychotic medicationAppropriate dose of ongoing antipsychotic medication 29.129.1
Antiparkinsonian medication for side effectsAntiparkinsonian medication for side effects 46.146.1
LongLong--lasting injections of antipsychotic medicationlasting injections of antipsychotic medication 35.035.0
1Data from inpatients studied.2Data for this box and all remaining categories are from outpatients studied.1Data from inpatients studied.2Data for this box and all remaining categories are from outpatients studied.
PORT 2 PORT 2 -- Conformance Study: Conformance Study: Sample Findings Sample Findings –– Antipsychotic DosingAntipsychotic Dosing
Acute Phase: 62.4 % receiving Acute Phase: 62.4 % receiving appropriate doses appropriate doses
15 % on a lower dose (<300 CPZ equiv.)15 % on a lower dose (<300 CPZ equiv.)
22.5 % on a higher dose (>1000 CPZ equiv.)22.5 % on a higher dose (>1000 CPZ equiv.)
Maintenance Phase: 29.1 % receiving Maintenance Phase: 29.1 % receiving appropriate dosesappropriate doses
39.1 % on a lower dose (<300 CPZ equiv.)39.1 % on a lower dose (<300 CPZ equiv.)
31.9 % on a higher dose (>600 CPZ equiv.)31.9 % on a higher dose (>600 CPZ equiv.)

PORT 2 PORT 2 -- Conformance Study: Conformance Study: Sample Findings (2)Sample Findings (2)
Urban patients more likely than rural to Urban patients more likely than rural to be out of range and to be on high dosesbe out of range and to be on high doses
Minority patients more likely to be on Minority patients more likely to be on high doseshigh doses
No evidence behind either of these trendsNo evidence behind either of these trends

PORT 2 StudyPORT 2 StudySample Findings Sample Findings -- NonNon--somatic Txsomatic Tx
InterventionIntervention Inpt. (%)Inpt. (%) Outpt. (%)Outpt. (%)
Family PsychoFamily Psycho--educationeducation 31.631.6 9.69.6
Vocational RehabilitationVocational Rehabilitation 30.430.4 22.522.5
Assertive Community Assertive Community TreatmentTreatment
8.68.6 10.110.1
% of pts with SZ % of pts with SZ receiving Txreceiving Tx

PORT PORT -- ConclusionsConclusions
Real world practice is inconsistent with Real world practice is inconsistent with practice as recommended by practice as recommended by academicsacademics
““EvidenceEvidence--based practicesbased practices”” are are markedly underutilizedmarkedly underutilized
Reasons for this need to be better Reasons for this need to be better understoodunderstood
Other strategies necessary to enhance Other strategies necessary to enhance implementation of EBPimplementation of EBP’’ss
National EvidenceNational Evidence--Based Practices Based Practices Project: SponsorsProject: Sponsors
SAMHSA SAMHSA –– Center for Mental Health ServicesCenter for Mental Health Services
Robert Wood Johnson FoundationRobert Wood Johnson Foundation
National Alliance for the Mentally IllNational Alliance for the Mentally Ill
Several state and local mental health Several state and local mental health authoritiesauthorities
New HampshireNew HampshireMarylandMarylandOhioOhioTexasTexasNorth CarolinaNorth Carolina

National EvidenceNational Evidence--Based Practices Based Practices Project: PhasesProject: Phases
Identification/selection of EBPIdentification/selection of EBP’’s (~ s (~ ‘‘98) for 98) for adults with SMIadults with SMI
6 practices selected6 practices selected
Development of initial training and evaluation Development of initial training and evaluation materials for each practice materials for each practice –– resource kits resource kits v.1.0 (v.1.0 (‘‘98 98 –– 9999’’))
Including methods to evaluate fidelity Including methods to evaluate fidelity
Piloting of EBP resource kits in multiple Piloting of EBP resource kits in multiple states with fidelity and outcome evaluation states with fidelity and outcome evaluation ((‘‘99 99 –– 0202’’))
Full development of Full development of ““implementation implementation resource kitsresource kits”” ((‘‘01 01 –– 0202’’))
National EBP Project:National EBP Project:6 Selected Practices6 Selected Practices
Assertive Community TreatmentAssertive Community Treatment
CoCo--occurring Disorders: Integrated occurring Disorders: Integrated TreatmentTreatment
Family PsychoFamily Psycho--educationeducation
Illness Management and Recovery Illness Management and Recovery
Medication Management Approaches in Medication Management Approaches in PsychiatryPsychiatry (MedMAP) (MedMAP)
Supported EmploymentSupported Employment

2001 2001 –– year long seriesyear long series
Presented rationale for emphasis on EBPPresented rationale for emphasis on EBP’’ss
Formal literature reviews on evidenceFormal literature reviews on evidence--based based practices in mental healthpractices in mental health
Introduced Introduced ““National EBP projectNational EBP project””6 6 ““blessedblessed”” practicespractices
National EBP project: Phases (2)National EBP project: Phases (2)
Demonstrate that resource kits can be used to Demonstrate that resource kits can be used to facilitate the faithful implementation of EBPfacilitate the faithful implementation of EBP’’s s in routine mental health settings and that this in routine mental health settings and that this results in improved client outcomes (results in improved client outcomes (‘‘0303-- ‘‘06)06)
Additional 7 state effectiveness studyAdditional 7 state effectiveness study
Broad dissemination of resource kitsBroad dissemination of resource kits
Dangers of EBPDangers of EBP’’ss
Dogma Dogma –– top down approachtop down approach
““CookbookCookbook”” approachapproach
OverOver--reliance on diagnostic reliance on diagnostic categoriescategories
Loss of individualityLoss of individualityProviderProviderClientClient

EvidenceEvidence--Based PracticeBased Practicess vs. vs. EvidenceEvidence--Based PracticeBased Practice
TopTop--down vs. bottom up approach down vs. bottom up approach to EBPto EBP
““BlessedBlessed”” practices vs. a practices vs. a commitment to continually use commitment to continually use outcome data to drive resource outcome data to drive resource allocation, training, etc. allocation, training, etc.
Bottom up approach to evidenceBottom up approach to evidence--based based practicepractice
Identifying desired outcomes and target Identifying desired outcomes and target population for a program or interventionpopulation for a program or intervention
Developing and implementing processes to Developing and implementing processes to assess and track those outcomes in a valid assess and track those outcomes in a valid mannermanner
Developing and implementing feedback Developing and implementing feedback processes in which outcome evaluation can processes in which outcome evaluation can and do impact programs/interventions and do impact programs/interventions (meaningful QA)(meaningful QA)
Can be organizational (e.g., CMHCCan be organizational (e.g., CMHC--wide) or wide) or specific to a programspecific to a program
Is there a problem with psychiatric Is there a problem with psychiatric prescribing patterns?prescribing patterns?
Inconsistent prescribing across providers Inconsistent prescribing across providers
Polypharmacy is rampantPolypharmacy is rampant
Costs are going through the roofCosts are going through the roof
New drugs are widely usedNew drugs are widely used
Huge influence of advertising/detailingHuge influence of advertising/detailingConsumerConsumer
ClinicianClinician
Opinion LeadersOpinion Leaders
Current Practice:Current Practice:Everyone Everyone ““Just Doing Their BestJust Doing Their Best””

One Goal of EvidenceOne Goal of Evidence--based Approach: based Approach: Aligning the ArrowsAligning the Arrows
Medication Management Approaches Medication Management Approaches in Psychiatryin Psychiatry (MedMAP) (MedMAP)
What is the goal of MedMAP in the What is the goal of MedMAP in the treatment of schizophrenia? treatment of schizophrenia?
To improve outcomes through the To improve outcomes through the optimal use of medications through optimal use of medications through implementation of the following implementation of the following principles: principles:
Utilization of a systematic approach to medication Utilization of a systematic approach to medication management management
Objective assessment of the symptoms that the Objective assessment of the symptoms that the medications are supposed to affect medications are supposed to affect
Clear, concise documentation of the treatments and Clear, concise documentation of the treatments and their outcomes their outcomes
Efforts to enhance medication adherence through Efforts to enhance medication adherence through consumer education and involvement in medication consumer education and involvement in medication decisions. decisions.

What are the core components of What are the core components of MedMAP?MedMAP?
A systematic approach to medication A systematic approach to medication managementmanagement
Guidelines and algorithmsGuidelines and algorithms
Standardized documentation Standardized documentation Identified target symptoms and quality of life goalsIdentified target symptoms and quality of life goals
Outcomes trackedOutcomes trackedSymptoms and quality of lifeSymptoms and quality of life
Consumer involvement / educationConsumer involvement / educationDecision making and symptom/outcome monitoringDecision making and symptom/outcome monitoring

DefinitionsDefinitions
GuidelinesGuidelines——Options with levels of evidence and Options with levels of evidence and principles of treatment. Suggests tactics, yet principles of treatment. Suggests tactics, yet user develops sequencesuser develops sequences
AlgorithmsAlgorithms——Specifies sequences (stages) with Specifies sequences (stages) with specific options and tactics. specific options and tactics. StepStep--byby--step flow step flow charts of best practices in medication use.charts of best practices in medication use.Recommends key decision points Recommends key decision points
““Algorithm: A step by step procedure for solving a problem Algorithm: A step by step procedure for solving a problem or accomplishing some end.or accomplishing some end.”” –– WebsterWebster’’s Dictionarys Dictionary

Guideline/Algorithm Citations for Guideline/Algorithm Citations for Treatment of SchizophreniaTreatment of Schizophrenia
Expert Consensus GuidelinesExpert Consensus GuidelinesJ. Clinical Psychiatry J. Clinical Psychiatry 6060 (Supplement 11), 1999(Supplement 11), 1999
Texas Medication Algorithm Project (TMAP)Texas Medication Algorithm Project (TMAP)J. Clinical Psychiatry, J. Clinical Psychiatry, 6565 (4); 500(4); 500--508, 2004 508, 2004
American Psychiatric AssociationAmerican Psychiatric AssociationAmerican J. Psychiatry American J. Psychiatry 161161 (Supplement), 2004(Supplement), 2004
Patient Outcomes Research Team (PORT)Patient Outcomes Research Team (PORT)Schizophrenia Bulletin Schizophrenia Bulletin 3030 (2), 193(2), 193--217, 2004217, 2004
ClarificationClarification
Guidelines and algorithms are available for Guidelines and algorithms are available for many disordersmany disorders
Tend to be diagnostically drivenTend to be diagnostically driven
““MedMapMedMap”” as currently configured is limited as currently configured is limited to Rx of Schizophreniato Rx of Schizophrenia
Principles and processes are applicable Principles and processes are applicable across conditionsacross conditions

Algorithm/Guideline DevelopmentAlgorithm/Guideline Development
Sponsoring Group/ProjectSponsoring Group/Project Abv.Abv. YearYearPatient Outcome Research TeamPatient Outcome Research Team PORTPORT ‘‘94, 94, ‘‘0404
TMAPTMAP
ExpertExpert
APAAPAVAVA
CPACPACanadian Psychiatric AssociationCanadian Psychiatric Association ‘‘9898
Texas Medication Algorithm Texas Medication Algorithm ProjectProject
‘‘96, 96, ‘‘99, 99, ‘‘0404
Expert Consensus Guidelines for Expert Consensus Guidelines for the Treatment of Schizophreniathe Treatment of Schizophrenia
‘‘96, 96, ‘‘9999
American Psychiatric Association American Psychiatric Association ‘‘97, 97, ‘‘0404Department of Veterans AffairsDepartment of Veterans Affairs ‘‘9797
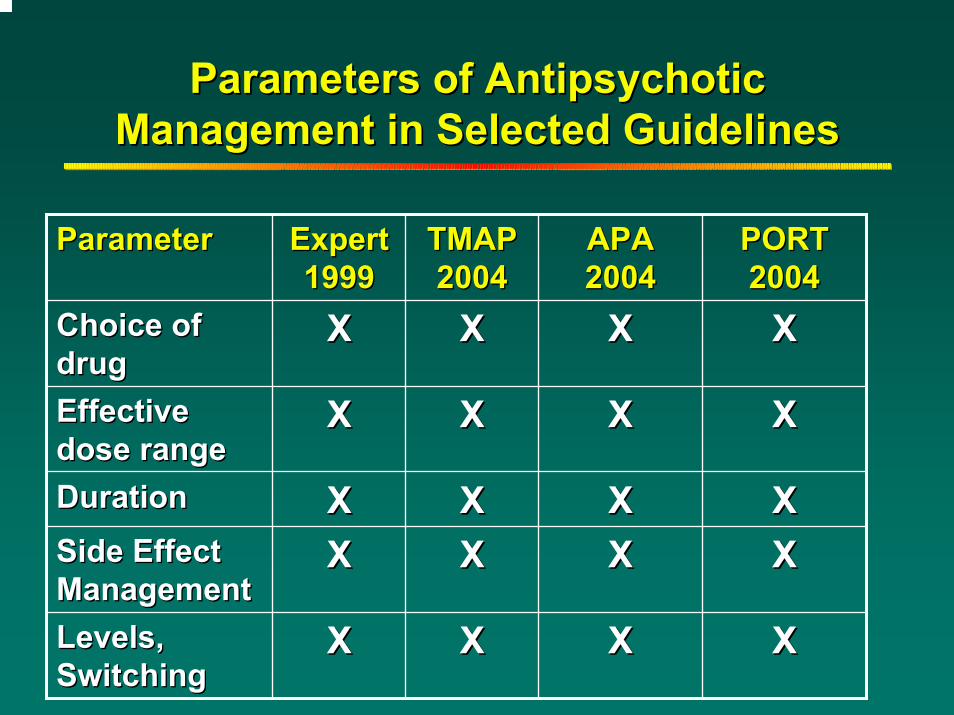
Parameters of Antipsychotic Parameters of Antipsychotic Management in Selected GuidelinesManagement in Selected Guidelines
ParameterParameter ExpertExpert19991999
TMAP TMAP 20042004
APA APA 20042004
PORT PORT 20042004
Choice of Choice of drug drug
XX XX XX XX
Effective Effective dose rangedose range
XX XX XX XX
Duration Duration XX XX XX XXSide Effect Side Effect ManagementManagement
XX XX XX XX
Levels, Levels, SwitchingSwitching
XX XX XX XX
Choosing and Antipsychotic by Choosing and Antipsychotic by Sequence and StageSequence and Stage
First episodeFirst episode
First failureFirst failure
Number of failures before clozapineNumber of failures before clozapine
Clozapine failureClozapine failure
Clozapine augmentationClozapine augmentation
Combination antipsychoticsCombination antipsychotics

Example of Algorithm from
Texas Medication Algorithm Project
(TMAP)

Expert TMAPExpert TMAP VAVA APA CPAAPA CPA19961996 1996 19971996 1997 1997 19981997 1998
First episode First episode A,TA,T A,TA,T A,TA,T A,TA,T A A
Second choice Second choice A,TA,T A,TA,T A,TA,T A,T,C A,TA,T,C A,T
Third choice Third choice CC AA CC C CC C
Fourth choice Fourth choice –– CC –– –– ––
Fifth choice Fifth choice –– –– –– –– ––
Combinations Combinations –– –– –– –– ––
Key: A=Atypicals T=Typicals C=Clozapine C+=Clozapine Augmentation CF=Clozapine Failure
Schizophrenia Guideline/Algorithm Schizophrenia Guideline/Algorithm Recommendations: 1Recommendations: 1stst WaveWave
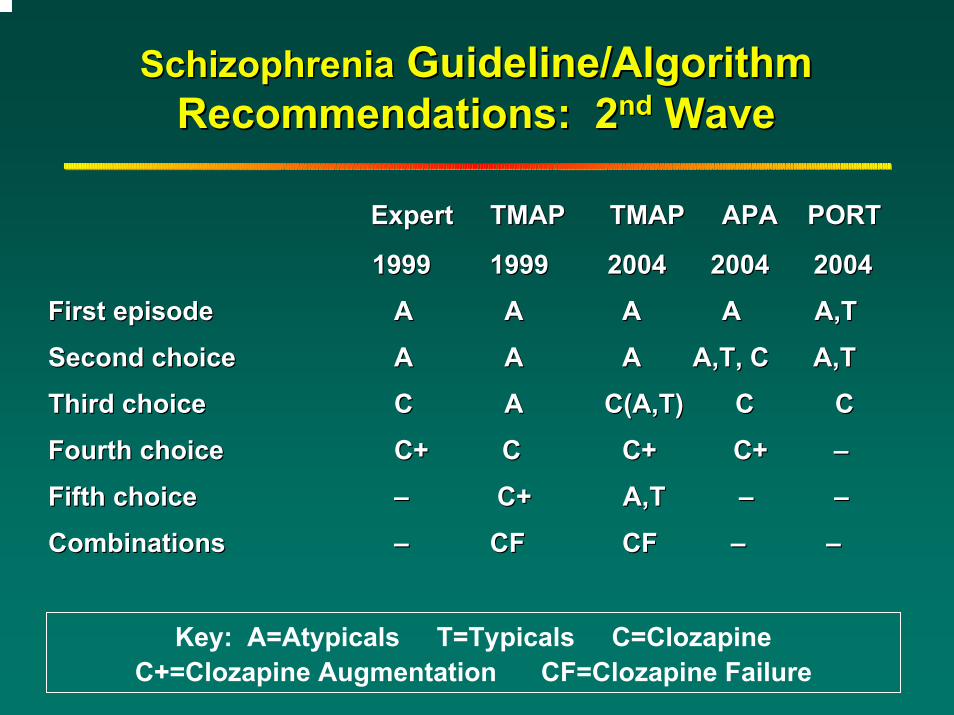
SchizophreniaSchizophrenia Guideline/Algorithm Guideline/Algorithm Recommendations: 2Recommendations: 2ndnd WaveWave
Expert TMAP TMAP APA PORTExpert TMAP TMAP APA PORT
1999 1999 2004 2004 20041999 1999 2004 2004 2004
First episode First episode AA AA A A A,TA A A,T
Second choiceSecond choice AA AA A A,T, C A,TA A,T, C A,T
Third choiceThird choice CC A C(A,T) C C A C(A,T) C C
Fourth choiceFourth choice C+ CC+ C C+ C+ C+ C+ ––
Fifth choiceFifth choice –– C+C+ A,T A,T –– ––
CombinationsCombinations –– CFCF CF CF –– ––
Key: A=Atypicals T=Typicals C=Clozapine C+=Clozapine Augmentation CF=Clozapine Failure

The Evidence PyramidThe Evidence Pyramid
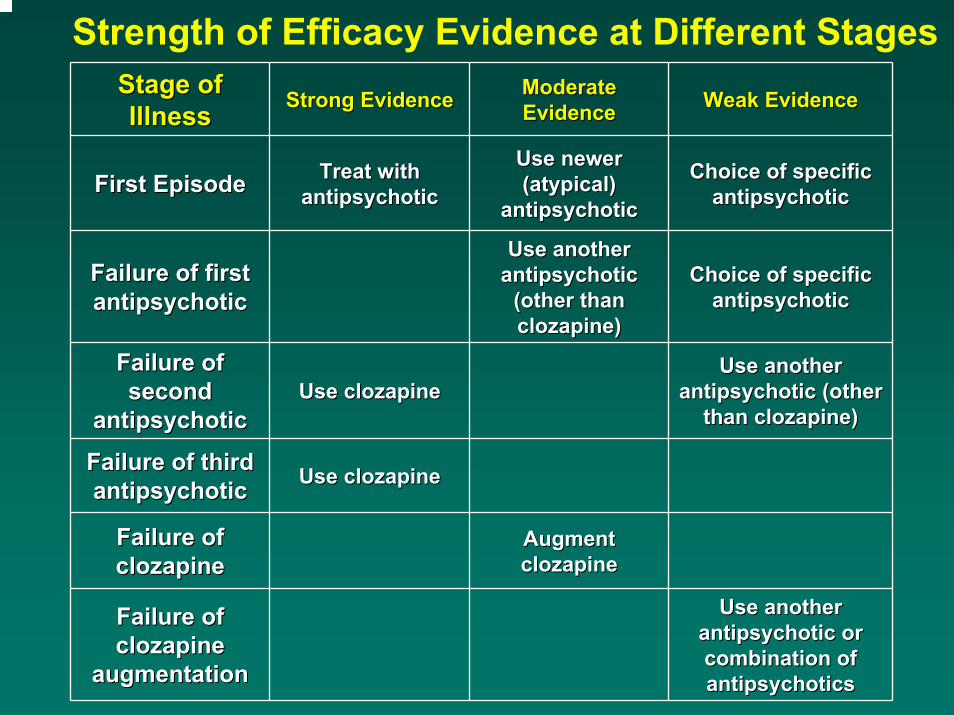
Strength of Efficacy Evidence at Different StagesStage of Stage of IllnessIllness Strong EvidenceStrong Evidence Moderate Moderate
EvidenceEvidence Weak EvidenceWeak Evidence
First EpisodeFirst Episode Treat with Treat with antipsychoticantipsychotic
Use newer Use newer (atypical) (atypical)
antipsychoticantipsychotic
Choice of specific Choice of specific antipsychoticantipsychotic
Failure of first Failure of first antipsychoticantipsychotic
Use another Use another antipsychotic antipsychotic
(other than (other than clozapine)clozapine)
Choice of specific Choice of specific antipsychoticantipsychotic
Failure of Failure of second second
antipsychoticantipsychoticUse clozapineUse clozapine
Use another Use another antipsychotic (other antipsychotic (other
than clozapine)than clozapine)
Failure of third Failure of third antipsychoticantipsychotic Use clozapineUse clozapine
Failure of Failure of clozapineclozapine
Augment Augment clozapineclozapine
Failure of Failure of clozapine clozapine
augmentationaugmentation
Use another Use another antipsychotic or antipsychotic or combination of combination of antipsychoticsantipsychotics
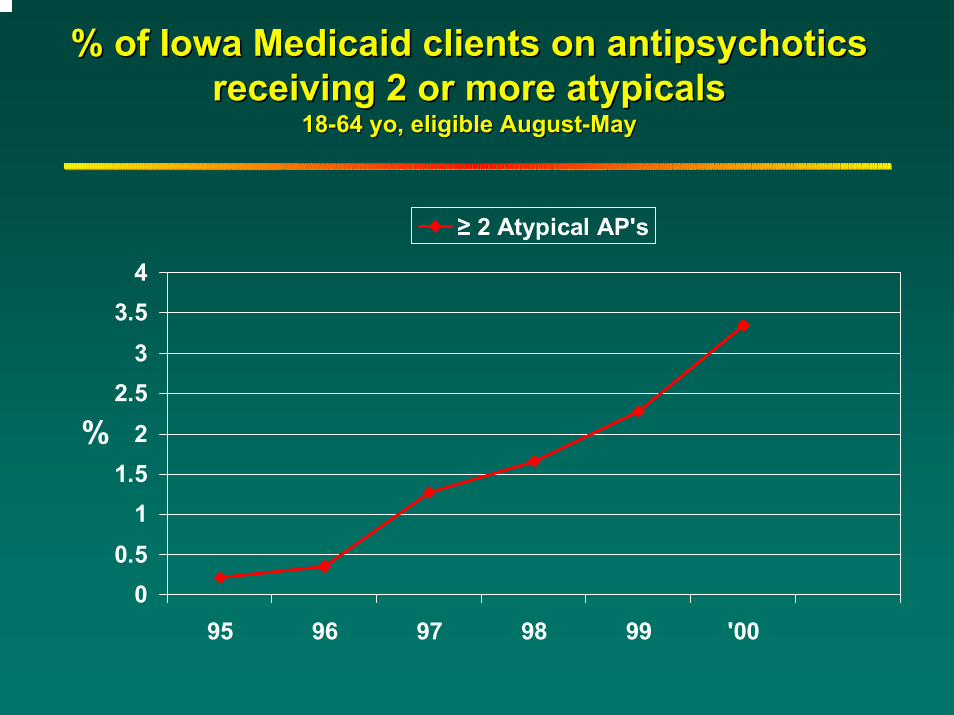
% of Iowa Medicaid clients on % of Iowa Medicaid clients on antipsychoticsantipsychoticsreceiving 2 or more receiving 2 or more atypicalsatypicals
1818--64 yo, eligible August64 yo, eligible August--MayMay
00.5
11.5
22.5
33.5
4
95 96 97 98 99 '00
%
≥ 2 Atypical AP's
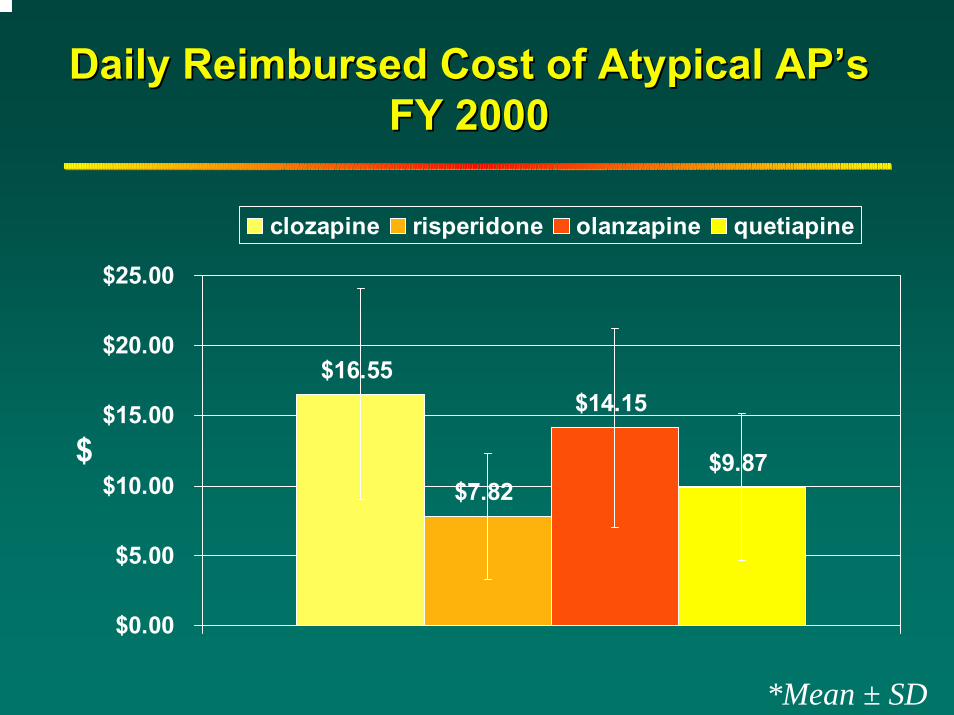
Daily Reimbursed Cost of Atypical APDaily Reimbursed Cost of Atypical AP’’ssFY 2000FY 2000
$16.55
$7.82
$14.15
$9.87
$0.00
$5.00
$10.00
$15.00
$20.00
$25.00
$
clozapine risperidone olanzapine quetiapine
*Mean ± SD

Daily Cost of Antipsychotics: Mono Daily Cost of Antipsychotics: Mono vs. vs. PolytherapyPolytherapy, FY 2000, FY 2000
$10.88
$17.57
$26.32
$0.00
$5.00
$10.00
$15.00
$20.00
$25.00
$30.00
$35.00
$40.00
$
AP monotherapy any AP polytherapy atypical polytherapy
*Mean ± SD

Clinical Reasons for Clinical Reasons for Algorithms/GuidelinesAlgorithms/Guidelines
Improve quality of careImprove quality of care
Facilitate clinical decisionFacilitate clinical decision--makingmaking
Make treatment plans consistent Make treatment plans consistent across sites and physiciansacross sites and physicians
Decrease influence of advertising, Decrease influence of advertising, commercial detailing, samples etc. commercial detailing, samples etc.
Administrative Reasons for Administrative Reasons for Algorithms/GuidelinesAlgorithms/Guidelines
Consistent documentation and outcomes Consistent documentation and outcomes across sites and providersacross sites and providers
Improve quality monitoringImprove quality monitoring
Provide a rational process for introducing Provide a rational process for introducing new treatmentsnew treatments
Improve cost efficiency Improve cost efficiency Define costs related to specific treatments or Define costs related to specific treatments or outcomesoutcomes
Make costs more predictableMake costs more predictable

What Do We Know About Clinical What Do We Know About Clinical Adherence to Guidelines?Adherence to Guidelines?
CME is ineffective*CME is ineffective*CME plus academic detailing is helpfulCME plus academic detailing is helpfulPrompts are more effective than audit/Prompts are more effective than audit/feedbackfeedbackCME plus audit/feedback is helpfulCME plus audit/feedback is helpfulPatients influence providersPatients influence providersChart reviews reveal low likelihood Chart reviews reveal low likelihood (<50%) of interpretable information by (<50%) of interpretable information by which to gauge adherencewhich to gauge adherence
*Davis DA, et al. JAMA 1995;274:700-705.

Components of MedMAP Resource KitComponents of MedMAP Resource Kit
Information for StakeholdersInformation for Stakeholders
Implementation Tips for Mental Health Implementation Tips for Mental Health Program LeadersProgram Leaders
Implementation Tips for Public Mental Health Implementation Tips for Public Mental Health AuthoritiesAuthorities
Fidelity ScaleFidelity Scale
Monitoring Client OutcomesMonitoring Client Outcomes
Manual for Practitioners and Provider Manual for Practitioners and Provider OrganizationsOrganizations

MedMap ElementsMedMap Elements
Guideline for medication treatments, with Guideline for medication treatments, with strategy and tacticsstrategy and tactics
Systematic documentation of medicationSystematic documentation of medication--related informationrelated information
Measurement of outcomesMeasurement of outcomes
PatientPatient--oriented approach to adherenceoriented approach to adherence
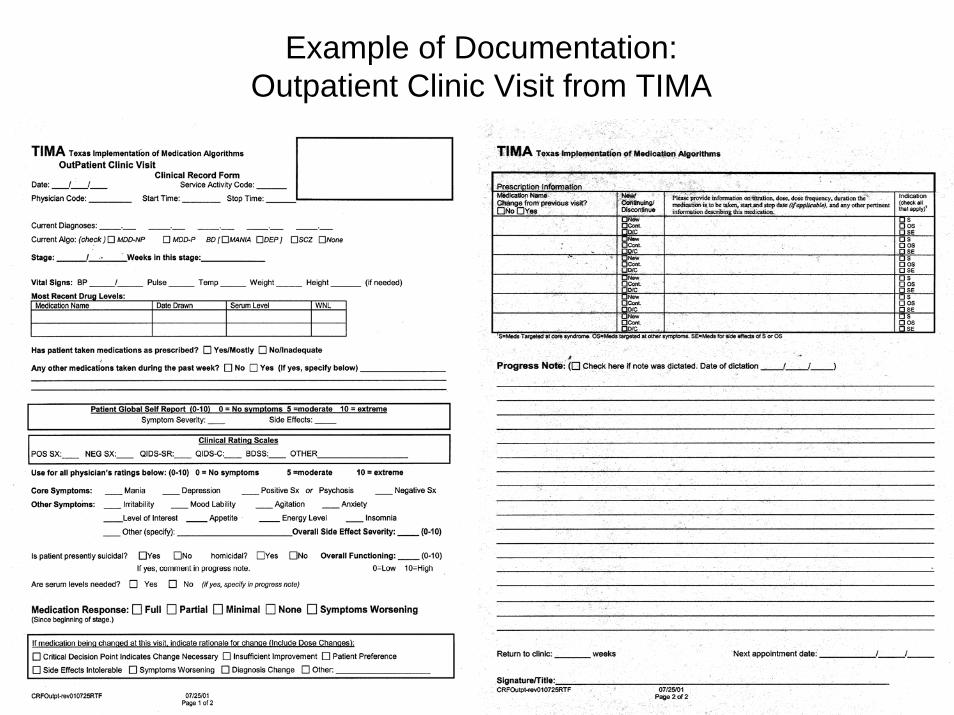
Example of Documentation:Outpatient Clinic Visit from TIMA
Documentation and Outcomes: Documentation and Outcomes: Use of clinical rating scalesUse of clinical rating scales
Specific algorithm clinical rating scalesSpecific algorithm clinical rating scales
General symptom Likert scalesGeneral symptom Likert scales
Patient rated scalesPatient rated scales
Clinician defined Likert scalesClinician defined Likert scales
Clinical global scalesClinical global scales
The patient’s progress as shown in symptoms and side effects are measured with the use of clinical rating scales in accordance with TIMA guidelines. Use of scales includes the following sub-elements that apply to primary and secondary diagnoses:

OUTCOMES ASSESSMENTSOUTCOMES ASSESSMENTS
Outcome Outcome ParameterParameter
Expert Expert 19991999
TMAP TMAP 20042004
APA APA 20042004
PORT PORT 20042004
Symptom Symptom DomainDomain
PositivePositive
NegativeNegative
PositivePositive
NegativeNegative
PositivePositive PositivePositive
Specific Specific MeasuresMeasures
NoNo YesYes NoNo NoNo
Failure CriteriaFailure Criteria NoNo YesYes NoNo NoNo
Documentation Documentation FormsForms
NoNo YesYes NoNo NoNo
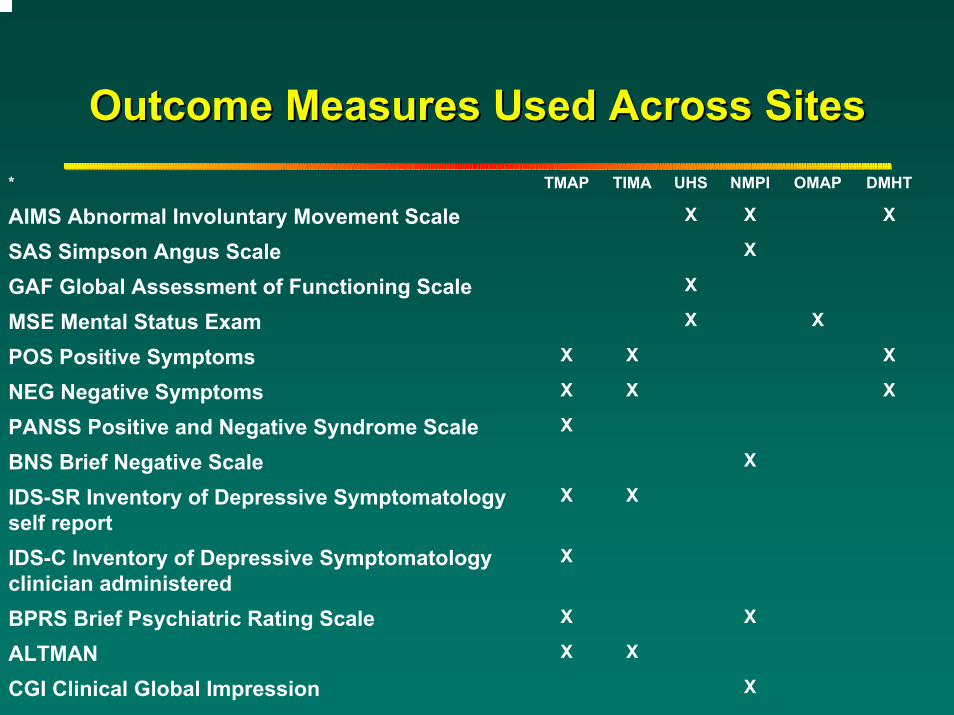
Outcome Measures Used Across SitesOutcome Measures Used Across Sites* TMAP TIMA UHS NMPI OMAP DMHT
AIMS Abnormal Involuntary Movement Scale X X X
SAS Simpson Angus Scale X
GAF Global Assessment of Functioning Scale X
MSE Mental Status Exam X X
POS Positive Symptoms X X X
NEG Negative Symptoms X X X
PANSS Positive and Negative Syndrome Scale X
BNS Brief Negative Scale X
IDS-SR Inventory of Depressive Symptomatology self report
X X
IDS-C Inventory of Depressive Symptomatology clinician administered
X
BPRS Brief Psychiatric Rating Scale X X
ALTMAN X X
CGI Clinical Global Impression X
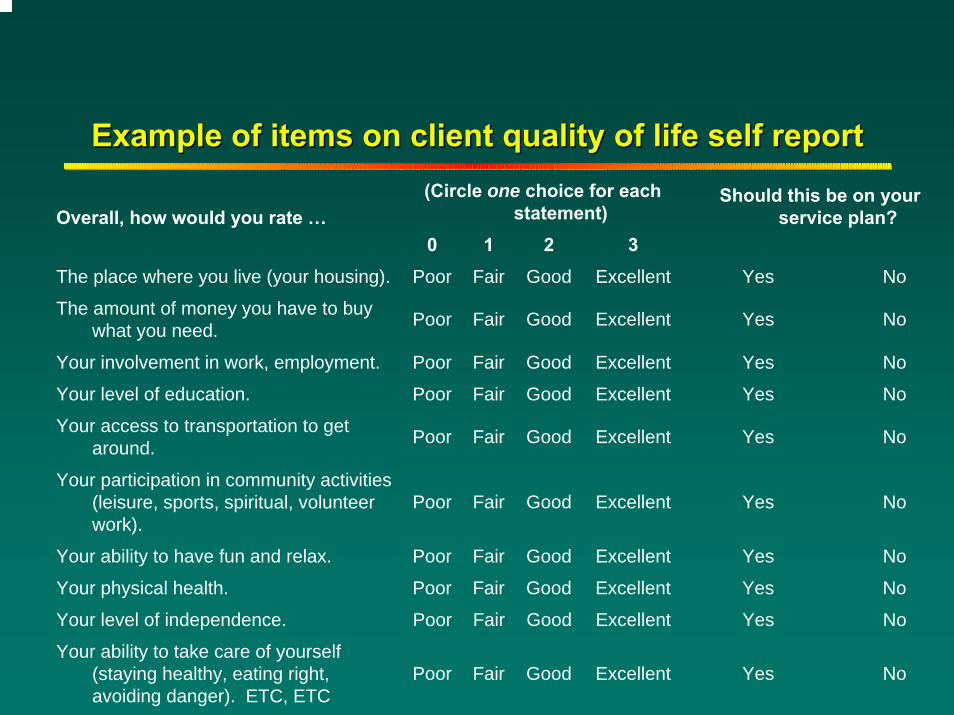
Example of items on client quality of life self reportExample of items on client quality of life self report(Circle one choice for each
statement)Overall, how would you rate …0 1 2 3
The place where you live (your housing). Poor Fair Good Excellent Yes No
The amount of money you have to buy what you need. Poor Fair Good Excellent Yes No
Your involvement in work, employment. Poor Fair Good Excellent Yes No
Your level of education. Poor Fair Good Excellent Yes No
Your access to transportation to get around. Poor Fair Good Excellent Yes No
Your participation in community activities (leisure, sports, spiritual, volunteer work).
Poor Fair Good Excellent Yes No
Your ability to have fun and relax. Poor Fair Good Excellent Yes No
Your physical health. Poor Fair Good Excellent Yes No
Your level of independence. Poor Fair Good Excellent Yes No
Your ability to take care of yourself (staying healthy, eating right, avoiding danger). ETC, ETC
Poor Fair Good Excellent Yes No
Should this be on your service plan?
Patient/Family EducationPatient/Family Education
Education PromotesEducation PromotesTreatment AdherenceTreatment Adherence
Partnership/Therapeutic AlliancePartnership/Therapeutic Alliance
Better Clinical DecisionsBetter Clinical Decisions
Better SelfBetter Self--carecare
Better symptom and relapse recognitionBetter symptom and relapse recognition
Better OutcomesBetter Outcomes
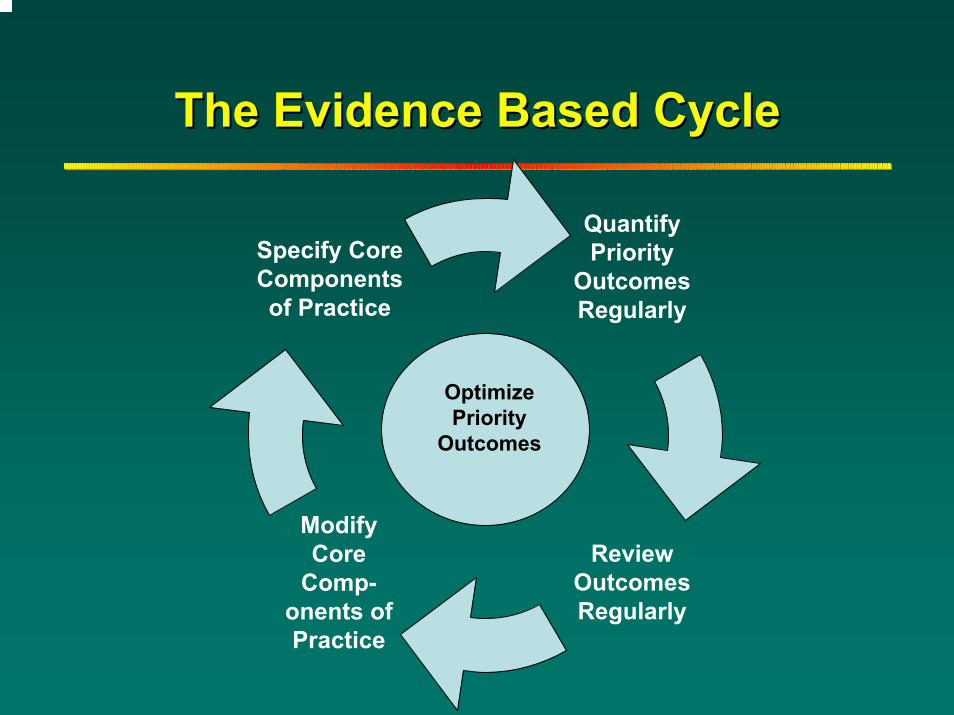
The Evidence Based CycleThe Evidence Based Cycle
Quantify Priority
OutcomesRegularly
Modify Core
Comp-onents of Practice
Review OutcomesRegularly
Specify Core Components of Practice
Optimize Priority
Outcomes

““FidelityFidelity””
The degree to which the actual The degree to which the actual implementation of a practice is consistent implementation of a practice is consistent with the intent of the modelwith the intent of the model
Must guard against Must guard against ““changing the sign on the changing the sign on the doordoor””
Research on Assertive Community Treatment Research on Assertive Community Treatment (ACT) shows that degree of fidelity to the (ACT) shows that degree of fidelity to the original model is correlated with outcomesoriginal model is correlated with outcomes
Much effort now in developing, evaluating and Much effort now in developing, evaluating and implementing methods to assess fidelityimplementing methods to assess fidelity
Fidelity Evaluation: Fidelity Evaluation: MedMAP Fidelity ScaleMedMAP Fidelity Scale
2 overall levels of assessment2 overall levels of assessment
Prescriber Level of AssessmentPrescriber Level of Assessment
Organizational Level of AssessmentOrganizational Level of Assessment

Prescriber ScalePrescriber Scale
16 items, scored 116 items, scored 1--55
1 = poor, 3 = satisfactory, 5 = excellent1 = poor, 3 = satisfactory, 5 = excellent
Covers multiple aspects of medication Covers multiple aspects of medication management and coordination with other management and coordination with other providers and aspects of treatmentproviders and aspects of treatment
Domains of Prescriber ScaleDomains of Prescriber Scale
Adequate information about diagnosis and treatment?Adequate information about diagnosis and treatment?
Measurement and use of outcomes?Measurement and use of outcomes?
Reduce medication burden and side effects?Reduce medication burden and side effects?
Dosing, monitoring okay?Dosing, monitoring okay?
Failures identified?Failures identified?
Patient and family involved in decisions, adherence Patient and family involved in decisions, adherence strategies?strategies?
Coordination with treatment team?Coordination with treatment team?
Organization ScaleOrganization Scale
13 items, scored 113 items, scored 1--55
1 = poor, 3 = satisfactory, 5 = excellent1 = poor, 3 = satisfactory, 5 = excellent
Rates organization on administrative support Rates organization on administrative support for prescribers, provision of materials to for prescribers, provision of materials to patients and prescribers, monitoring of patients and prescribers, monitoring of prescribersprescribers
Domains of Organization ScaleDomains of Organization Scale
Useful standardized Useful standardized forms?forms?
Rapid and reliable Rapid and reliable information access?information access?
Medications readily Medications readily available?available?
Failures identified?Failures identified?
Quality control?Quality control?
Materials for patient Materials for patient education?education?
Materials for Materials for guideline guideline implementation?implementation?
Scheduling Scheduling flexibility?flexibility?
Integration of Integration of servicesservices
Staff training?Staff training?

Use of Fidelity Scale in MedMAPUse of Fidelity Scale in MedMAPBaseline measurements of prescribers, Baseline measurements of prescribers, organizationorganization
Analyze results, identify strengths and Analyze results, identify strengths and weaknessesweaknesses
Design and implement changesDesign and implement changes
ReRe--do fidelity scale assessmentsdo fidelity scale assessments
Analyze results, identify effects of changesAnalyze results, identify effects of changes
ReRe--design implementation strategiesdesign implementation strategies

Limitations of Algorithms/GuidelinesLimitations of Algorithms/Guidelines
Tend to be diagnostically drivenTend to be diagnostically drivenDx categories likely to be heterogeneous Dx categories likely to be heterogeneous with respect to pathophysiology and with respect to pathophysiology and treatment responsetreatment responseMust adapt to individual patientMust adapt to individual patient
Evolve with new treatmentsEvolve with new treatmentsEfficacy versus effectivenessEfficacy versus effectivenessScience versus clinical wisdomScience versus clinical wisdom
Resistance to the overall approachResistance to the overall approach
““Cookbook medicineCookbook medicine””
Unique or different Unique or different –– ““more ill, rural, more ill, rural, urban, real world vs University, etcurban, real world vs University, etc””
Information collected (rating scales) Information collected (rating scales) not clinically usefulnot clinically useful
Data is collected for research purposesData is collected for research purposes
Based on University research and has Based on University research and has no relevance to the real worldno relevance to the real world
Resistance (cont.)Resistance (cont.)
Takes more timeTakes more time
Adds more paperworkAdds more paperwork
Costs more moneyCosts more money
Old way is better Old way is better –– ““if it ainif it ain’’t broke, t broke, dondon’’t fix itt fix it””
No one else is doing itNo one else is doing it
““Fad that will go away eventuallyFad that will go away eventually””

Leading the Implementation Leading the Implementation
MedMAP is more likely to be MedMAP is more likely to be successfully implemented if a clearly successfully implemented if a clearly identified person is responsible for identified person is responsible for leading the initiative. leading the initiative.
The identified person is most likely to succeed if he The identified person is most likely to succeed if he or she is a senior administrator or clinician or has or she is a senior administrator or clinician or has the backing of executive level staff and decisionthe backing of executive level staff and decision--making authority. making authority.
Clearly, the likelihood of success is greatly Clearly, the likelihood of success is greatly enhanced if this person has the respect of the onenhanced if this person has the respect of the on--line staff and fully understands the operation of the line staff and fully understands the operation of the facility/agency. facility/agency.
Readiness for EBPReadiness for EBP’’s?s?
ResearchResearchClinicalClinicalServicesServices
Administrative Administrative Data Data infrastructureinfrastructureFinancingFinancingCredentialingCredentialing
ClinicalClinical
EducationalEducationalCMECME’’ss
TraineesTrainees
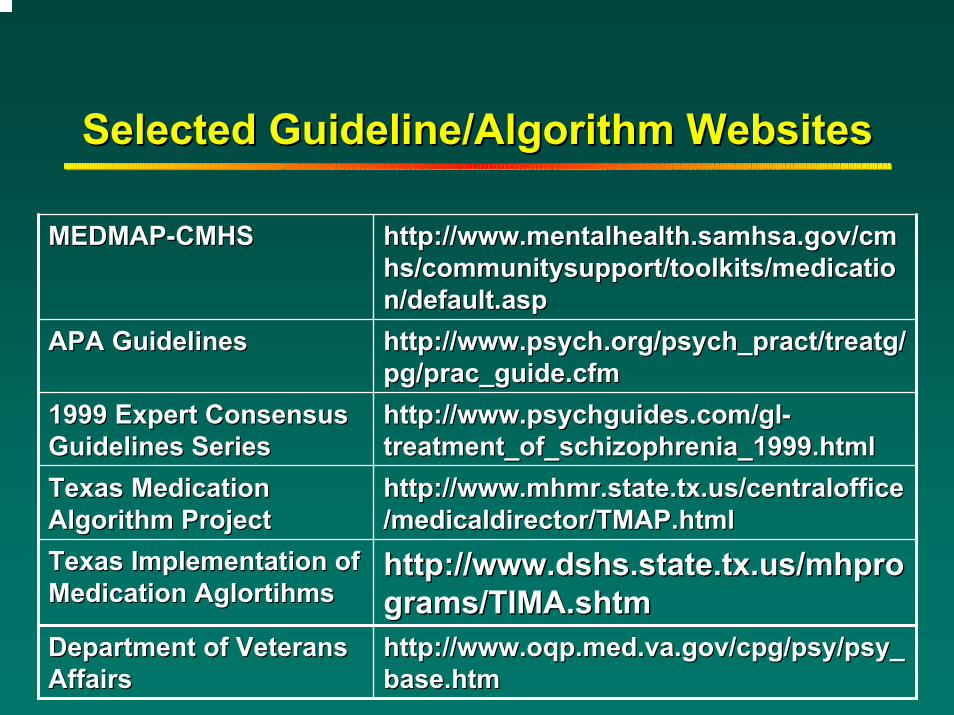
Selected Guideline/Algorithm WebsitesSelected Guideline/Algorithm Websites
MEDMAPMEDMAP--CMHSCMHS http://www.mentalhealth.samhsa.gov/cmhttp://www.mentalhealth.samhsa.gov/cmhs/communitysupport/toolkits/medicatiohs/communitysupport/toolkits/medication/default.aspn/default.asp
APA GuidelinesAPA Guidelines http://http://www.psych.org/psych_pract/treatg/www.psych.org/psych_pract/treatg/pg/prac_guide.cfmpg/prac_guide.cfm
1999 Expert Consensus 1999 Expert Consensus Guidelines SeriesGuidelines Series
http://www.psychguides.com/glhttp://www.psychguides.com/gl--treatment_of_schizophrenia_1999.htmltreatment_of_schizophrenia_1999.html
Texas Medication Texas Medication Algorithm ProjectAlgorithm Project
http://www.mhmr.state.tx.us/centralofficehttp://www.mhmr.state.tx.us/centraloffice/medicaldirector/TMAP.html/medicaldirector/TMAP.html
Texas Implementation of Texas Implementation of Medication Medication AglortihmsAglortihms
http://http://www.dshs.state.tx.us/mhprowww.dshs.state.tx.us/mhprograms/TIMA.shtmgrams/TIMA.shtm
Department of Veterans Department of Veterans Affairs Affairs
http://http://www.oqp.med.va.gov/cpg/psy/psy_www.oqp.med.va.gov/cpg/psy/psy_base.htmbase.htm
My My Contact InfoContact Info
ee--mail: mail: [email protected]@uiowa.edu
Phone: 319Phone: 319--353353--4340 4340
Web site: Web site: www.icmentalhealth.orgwww.icmentalhealth.org