evidence-based management of postpartum...
TRANSCRIPT

Michaela K. Farber MD MSDepartment of Anesthesiology, Perioperative and Pain Medicine
Brigham and Women’s HospitalBoston, MA
EVIDENCE-BASED MANAGEMENTOF
POSTPARTUM HEMORRHAGE

Objectives: Evidence-Based Management of PPH
Tailored protocols: Every unit: NPMS Hemorrhage Bundle Risk assessment prior to cesarean delivery Morbidly adherent placenta Jehovah’s Witness patients
Coagulopathy management: Fibrinogen concentrate Point-of-care (ROTEM, TEG) Tranexamic acid

www.cdc.gov

Council on Patient Safety in Women’s Health Care-National Partnership for Maternal Safety (formed in 2013)
Endorsed by: AABB, AAFP, ACNM, ACOG, AWHONN, SMFM, SOAP

13 Key Elements
4 Action Domains Readiness Recognition Response Reporting
Main EK et al. Anesth Analg 2015; 121(1): 142-8

A
8 PRBCs 4 Plasma 1 Cryo
Miller AD, personal communication

Shields LE et al. Am J Obstet Gynecol 2011; 205: 368
Key Points: • Before and after study• 4-stage protocol-guided:
• Risk assessment
• EBL measurement
• Uterotonics
• Early MD notification
• Transfusion

5813 Deliveries/16 months
Stage 1: recognition
Stage 2: >1 dose uterotonic
Stage 3: EBL >1500
Pre-protocol
Post-protocol
Stage 1 35% 82%Stage 2 53% 8%Stage 3 11% 10%
Protocol implementation:
Shorter bleeding time Lower transfusion rates Lower acuity/intervention
Shields LE et al. Am J Obstet Gynecol 2011; 205: 368

www.acog.org/About-ACOG/ACOG-Districts/District-II/Safe-Motherhood-Initiative

Pre-labor CDOdds ratio [CI]
Intrapartum CDOdds ratio [CI]
General anesthesia
22.3 [4.9-99.9] 5.4 [1.7-17.1]
Multiple pregnancies
8.0 [4.2-15.0] 3.4 [1.7-6.3]
Placenta previa
6.3 [3.4-11.8] n/a
Pre-delivery Hgb < 9.9g/dL
n/a 3.0 [1.3-6.9]
Butwick AJ et al. Anesth Analg 2017; 125:523-32.
Severe hemorrhage = EBL > 1500 mL or PRBC transfusion within 48h of delivery

Key Points
• Suspected accreta cases • 2004-2009
• N = 136; [% transfused]
• 21 accreta* [71%]• 17 increta* [82%]• 17 percreta* [82%]• 39 focal accreta [28%]• 42 no accreta [19%]
• *89% hysterectomy rate
Panigrahi AK et al. Anesth Analg 2017; 125:603-8

•884 obstetric hemorrhage cases with cell salvage collection
•Re-infusion in 189/884 = 21% of cases
Nature of Hemorrhage % Cases Re-Infusion
High-risk cesarean delivery 13Cesarean hysterectomy 76Bleeding post-cesarean delivery 69Bleeding post-vaginal delivery 53
Milne ME et al. Obstet Gynecol 2015;125(4):919-23

Key Points
• 24yo G2P1 • repeat cesarean delivery
• Atony, B-Lynch, UA ligation• Hysterectomy, 2.5L EBL
• Hemoperitoneum 3L
• CELL SALVAGE
• TEG, thrombin spray, surgicel• rFVIIa, tranexamic acid• Erythropoeitin, Vit K, IV Iron, folate
Hubbard RM et al. A A Case Rep 2017;8(12):326-9

www.acog.org/About-ACOG/ACOG-Districts/District-II/Safe-Motherhood-Initiative

Just another day on L&D…
Within 5 minutes? Plan AUncontrolled
1:1:1 ratio
Within 1 hour? Plan BControlled
ROTEM or TEG

When Postpartum Hemorrhage Happens…
Stop the Bleeding
Address the cause and acuity!
Uterotonics
Uterine massage
Tamponade
Embolization
Surgical procedures
Help the Clotting
Packed red blood cells
Plasma
Cryoprecipitate
Platelets
Fibrinogen concentrate
Tranexamic acid
PCCs, DDAVP, rFVIIa

Low Fibrinogen Precedes Progression to Severe Postpartum Hemorrhage
Reference N Definition of progression to severe
PPH
Fibrinogen, mg/dL
Non-progressionto severe
PPH
Progression to severe
PPH
Charbit B2007
128 Hb fall >4,> 4 u RBC,
invasive procedure
440 330
Cortet M 2012
738 same 420 340
Gayat E 2011
257 Invasive procedure
265 180
De Lloyd L2012
240 > 4 U RBC or EBL >2500 mL
440 310
Collins PW 2014
346 > 4 U RBC or EBL >2500 mL
390 280
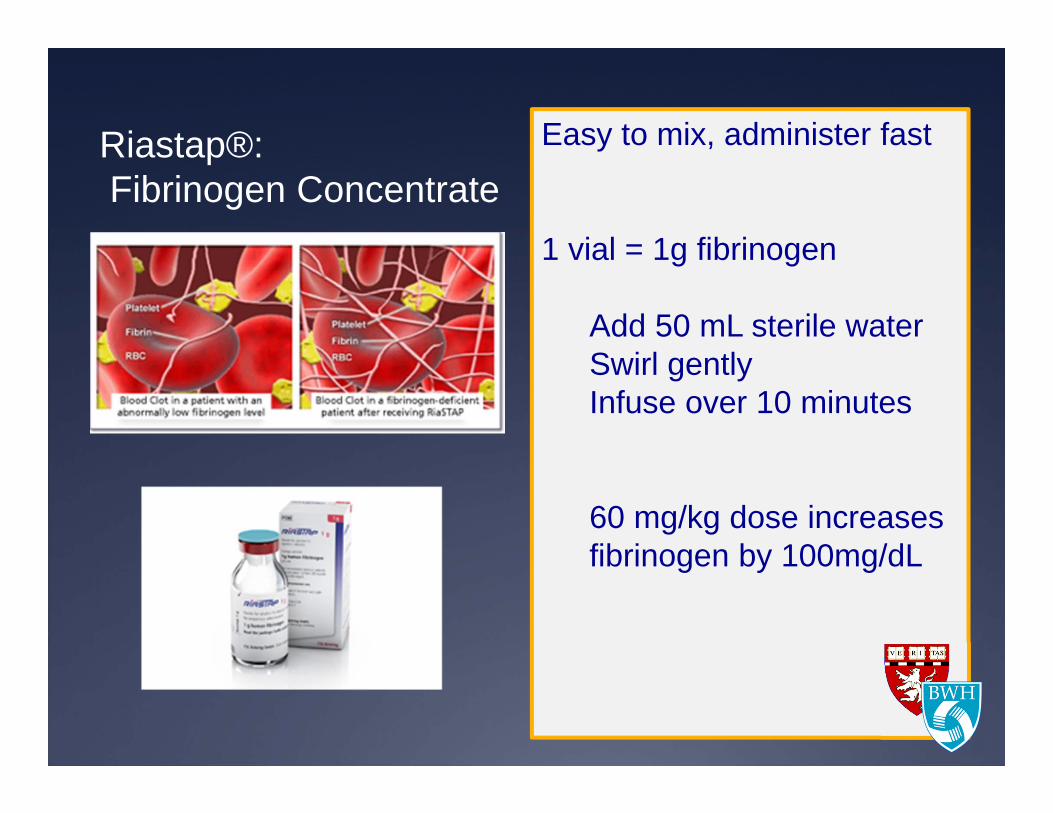
Riastap®:Fibrinogen Concentrate
Easy to mix, administer fast
1 vial = 1g fibrinogen
Add 50 mL sterile waterSwirl gentlyInfuse over 10 minutes
60 mg/kg dose increases fibrinogen by 100mg/dL

Empiric 2g fibrinogen concentrate for PPH: will it lower transfusion requirement?
Wikkelso AJ et al. Trials 2012; 13:110

PPH> 500 mL vaginal delivery > 1000 mL cesarean delivery
Empiric fibrinogen, 2g (n = 123)
Placebo Fibrinogen RR (95% CI) P value
Transfusion requirement
26 (22%) 25 (20%) 0.95 (0.58-1.54) 0.88
EBL 1700 (1500-2000)
1700 (1400-2000) 66 (-78-210) 0.37
Severe PPH 20 (40%) 24 (52%) 0.77(0.49-1.19) 0.31
Placebo (n = 121)
Wikkelso AJ et al Br J Anaesth 2015; 114(4):623-33.

Abnormal Placentation?
Uterine Rupture?
Amniotic Fluid Embolism?
Uterine Atony?
Surgical/Genital Trauma?
PLACENTA releases tissue factor, plasminogen activator
fibrinogenplasminogenfactor VIII
The Influence of the Placenta
Placental Abruption

Etiology Onset of coagulopathy
Dilutional Consumptive, local
Consumptive, DIC
Uterine atony
Late Severecases
Severe cases
Very rare
Genital or surgical trauma
Late Severecases
Severecases
Very rare
Placentalabruption
Early Severecases
Main cause Severe cases
AFE Early Most cases ----- Main cause
Uterine rupture
Early Main cause Some cases ------
Previa, accreta
Early or Late
Severecases
Some cases Rare unless infection
Identify the Cause
80%
Collis RE and Collins PW. Anaesthesia 2015; 70(1): 78-86

Consumptive Coagulopathy
VERY RARE
Amniotic fluid embolus
Severe preeclampsia/HELLP
Severe abruption
RARE
Placental bed (abruption)
Intra-uterine clots (atony)
Abnormal placentation
DISSEMINATED INTRAVASCULAR LOCALIZED (UTERUS/PLACENTA)
LOW FIBRINOGEN

ROTEM®: Hemostatic Decision-Making
CT = clotting time (initial)CFT = clot formation timeMCF = maximum clot firmnessML = maximum lysisINTEM, HEPTEMEXTEM, FIBTEM, APTEM
rotem-usa.com

FIBTEM as a Surrogate for Serum Fibrinogen
FIBRINOGEN (mg/dL) FIBTEM A5 (mm)300 15200 10100 6
Normal Term Gestation Low Fibrinogen State
Huissoud C et al. BJOG 2009; 116(8): 1097-102. Collis RE and Collins PW. Anaesthesia 2015; 70(1): 78-86

Mallaiah S et al. Anaesthesia 2015; 70(2): 166-75
plasma
Fibrinogen
platelets

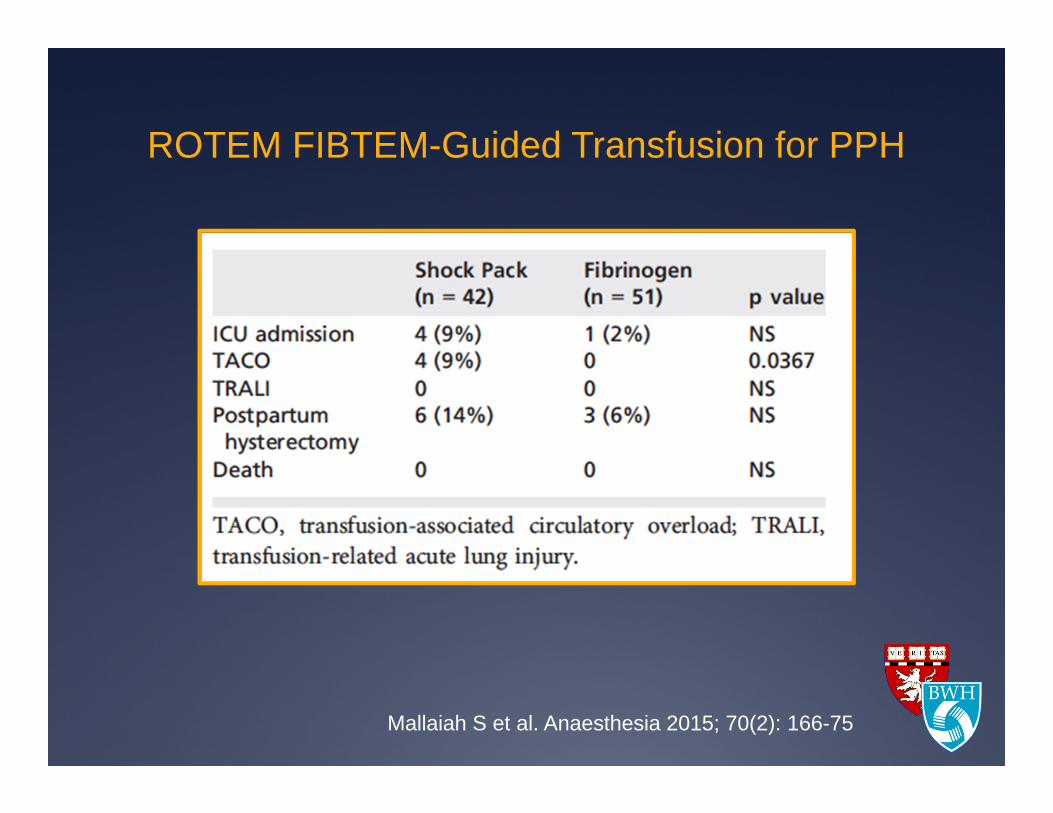
ROTEM FIBTEM-Guided Transfusion for PPH
Mallaiah S et al. Anaesthesia 2015; 70(2): 166-75
ROTEM FIBTEM-Guided Transfusion for PPH
Mallaiah S et al. Anaesthesia 2015; 70(2): 166-75

PPH> 500 mL vaginal delivery > 1000 mL cesarean delivery
ROTEM FIBTEM A5 < 15 mm
Fibrinogen (n = 28)[23-Fibtem A5 x IBW/140]
Placebo (n = 28)
1o outcome: # PRBCs, plasma, cryoprecipitate, platelets transfused
Collins PW et al. Br J Anaesth 2017; 119(3): 411-21

Collins PW et al. Br J Anaesth 2017; 119(3): 411-21
Transfusion rate Placebo Fibrinogen Treatment effect (95% CI) P value
PRBCs 1.32(38 U)
1.41(37 U)
0.94 (0.44-2.02) 0.87
Plasma 1.22 0.64 0.53 (0.13-2.16) 0.37
# transfused, n (%)
Cryoprecipitate 26 (96.3) 27 (9643) NA
Early infusion of fibrinogen during PPH with a Fibtem A5 < 15mm did not lowertransfusion requirement or blood loss.*Threshold effect may be A5 < 12mm.

Tranexamic Acid

Tranexamic Acid

APTEM: No Fibrinolysis
APTEM: Fibrinolysis Confirmed
When Tranexamic Acid would Really Help:
rotem-usa.com

Ducloy-Bouthors AS et al. Crit Care 2011
• PPH after vaginal delivery:
• > 800 mL EBL
• TXA 4g/1h then 1g/h for 6h
• EBL at T2 (30min), to T4 (6h)Lower EBL, shorter
duration, less severe PPH
221 vs. 173 mL!!

RCT
PPH after vaginal or cesarean delivery
192 hospitals, 21 countries
20,000 women
Tranexamic acid 1g (10,051) vs. placebo (10,009)
Re-dosed if bleeding after 30 minutes
Primary endpoint: death from bleedingLancet 2017; 389: 2105-16

191(1.9%)
127(1.7%)
Tranexamic acid
155 (1.5%)
89(1.2%)
DEATH from Postpartum Hemorrhage:
If TXA received within 3h of PPH…
Control
Lancet 2017; 389: 2105-16
Vs.

“TXA reduces death due to bleeding in women with PPH with no adverse effects.”
Lancet 2017; 389: 2105-16

Correspondence…“TXA could save the lives of 1 in 3 mothers who would otherwise
bleed to death after childbirth”
“We believe such statements seem to misrepresent the data.”Letson HL and Dobson GP, Lancet 2017
“It is reasonable to add TXA, a cheap medication, widely available and convenient to use, in the early steps of PPH protocols” Ducloy-Bouthers AS, Godier A Anaesth Crit Care Pain Med 2017
“Results not generalizable to high income countries” Dennis AT and Griffiths JD, Lancet 2017

http://womantrial.lshtm.ac.uk/
Australian cohort 11 PPH deaths in 5 years 1.5 million deliveries NNT = 35,587 women
WOMAN cohort 346 PPH deaths in 6 years 20,060 deliveries NNT = 250 women
Dennis AT and Griffiths JD, Lancet 2017
WOMAN: External Validity?
“ Although the absence of thrombotic complications is reassuring, on the basis of the NNT anddifferent contexts with which this study was done, TXA should not be routinely used for obstetric
hemorrhage in women from high-income countries.”

Tranexamic Acid: Safety Low-dose (1g IV, repeated x1 if needed)
no increased risk of:-venous thromboembolic events-seizures -???-renal complications
Drug error: spinal injection of tranexamic acid
death or major neurologic injury
WOMAN Trial Collaborators, Lancet 2017Yeh HM et al. Anaesthesia 2003Garcia PS et al. Anesth Analg 2007

Tranexamic Acid Research
TRAAP: TXA (Sentilhes L et al)
WOMAN – ETAPlaT (Dallaku K et al)
WOMAN – ETAC (Shakur H et al)
TAPPH-1 (Alam A et al)
NICHD MFM-U (Pacheco LD et al)

Anticipate Coagulopathy/Use Point-of-Care
Fibrinogen Concentrate Tranexamic Acid
Ongoing Bleeding?
Secondary Uterotonic Surgical maneuvers
Address the Underlying CAUSE
Atony: Uterotonics Trauma: Repair
Postpartum Hemorrhage Diagnosis

Postpartum Hemorrhage: What I Do• Oxytocin 1-3U slow bolus then infusion• Fundal massage• Measure blood loss (gravimetry, other)
Atony Management(All Patients)
• 2 large-bore IVs• CBC, PT, aPTT, fibrinogen, POCT: TEG or ROTEM• 100% oxygen by face mask• Carboprost, methylergonovine secondary uterotonics
Stage 1: > 500 mL vaginal
>1000 mL cesarean
• Activate your MTP, start transfusion• Move to OR if vaginal PPH; inspect for lacerations• Consider: arterial line for ABGs• Consider TXA: 1g IV/10 min; repeat x1 over 2-3 h• Consider fibrinogen: 4 vials = 1 dose of
cryoprecipitate• Surgical: broad ligaments, tamponade, embolization
Stage 2:<1500 mL but ongoing
• Uncontrolled: 1:1:1, POCT• Controlled: use POCT, goal-directed therapy• Fluid warming, watch acidosis, high K+, low Ca2+
• Surgical: B-Lynch, hysterectomy, UA ligation
Stage 3: > 1500 mL

Conclusions
Protocol-driven PPH management is justified, for every unit, and for specific at-risk populations
Coagulopathy is rare in obstetric bleeding, but more common during severe hemorrhage
Use of fibrinogen, point-of-care, and tranexamic acid may lower morbidity or mortality from severe hemorrhage
