evidence-based solutions for the treatment of...
TRANSCRIPT

Evidence-Based Solutions for the Treatment of
Diabetic Foot Ulcers
Shawn Cazzell, DPM
Fellow, American Professional Wound Care Association
Academy of Physicians in Wound Healing
Founder, Limb Preservation Platform
CCFMG Central California Faculty Medical Group
Fresno, California
SPONSORED BY
Michael R. Zenn, MD, MBA
Chief Medical Officer, NOVADAQ
Vice Chief of Plastic and Reconstructive Surgery
Professor of Plastic Surgery
Duke University Medical Center
Durham, North Carolina

Dr. Michael R. Zenn, MD, Professor and Vice President of Plastic
Surgery at Duke University introducing Dr. Shawn Cazzell, DPM
Evidence-Based Solutions for the Treatment of
Chronic Wounds
Illuminating Evidence-Based Wound Care Management
3/17/2016 3
Michael R. Zenn, MD, MBA Professor of Plastic
Surgery Duke University Medical Center
Durham, North Carolina
Chief Medical Officer, NOVADAQ

Introducing the NOVADAQ Wound Care Focus
Assisting clinicians in improving patient outcomes
by providing real-time, clinically relevant
information
Focusing on supporting and improving physician
and patient education in chronic wound care
diagnostics and therapies
Partnering with specialists and their teams to
improve the management of patients with acute
and chronic wounds
3/17/2016 4

3/17/2016 5
NOVADAQ Wound Care Products
Objective Assessment
Cost-Effective Solutions

Introducing DermACELL AWM® for Chronic Wounds
3/17/2016 6

A Partnership for People
3/17/2016 7
Over 7,500 Lives Saved
Millions of Lives Restored
Over 500,000 implants distributed per year
More Than 50 Utility or Design U.S. Patents

Evidence-Based Medicine
TITLE: Healing Rates in a Multicenter Assessment of a Sterile, Room Temperature, Acellular Dermal Matrix Versus Conventional Care Wound Management and an Active Comparator in the Treatment of Full-Thickness Diabetic Foot Ulcers AUTHORS: J Walters, S Cazzell, H Pham, D Vayser, A Reyzelman JOURNAL: ePlasty PUBLISHED: February 2016
3/17/2016 8
• The Largest Multicenter, Randomized Control Trial to date
for Human Acellular Dermal Matrices in Chronic Wounds
• A high-quality, rigorous study with increased emphasis on
percent reduction vs. closure rate
• Statistically significant healing rates vs. conventional care

Dr. Shawn Cazzell, DPM
A Lead Author of the recently published DermACELL AWM RCT
3/17/2016 9
Shawn Cazzell, D.P.M., specializes in Podiatry and Foot and Ankle
Surgery. Dr. Cazzell has advanced training in wound care and limb salvage
techniques. Dr. Cazzell completed his residency training through St. Mary’s
Medical Center, San Francisco. He attended California School of Podiatric
Medicine at Samuel Merritt University, Oakland, CA. His undergraduate
education was completed at UC San Diego.
Dr. Cazzell’s main areas of interest are in: advanced wound care, limb
preservation and traumatic lower extremity reconstruction.
He is a Fellow of the American Professional Wound Care Association,
Member of the Academy of Physicians in Wound Healing, and the Founder
of the Limb Preservation Platform.

DermACELL AWM Webinar Objectives:
I. Introducing Dermacell AWM for the treatment of chronic wounds
II. Results and Rigor of the Largest, Multicenter, Randomized, Controlled Trial to date for Human ADM in Chronic Wounds
III. A Changing Paradigm: Dermacell AWM, A One-Application, Cost-Effective Solution
IV. Q&A
3/17/2016 10
I. Introducing DermACELL AWM for Chronic Wounds
3/17/2016 11

DermACELL AWM Clinical Applications
Dermacell AWM is a technologically advanced Acellular Dermal Matrix (ADM) that is used to treat diabetic foot ulcers and
other chronic non-healing wounds. Dermacell AWM is processed using Matracell® technology, which is a validated and patented process which renders the Dermacell AWM graft acellular, without compromising the biomechanical or desired biochemical properties of the graft. This process is gentle, yet robust enough to ensure the native scaffold, vascular channels, growth factors and proteins are preserved to assist in the healing of the wound.3
Chronic wounds often have an excess of MMPs (Matrix Metalloproteinases) and reduced growth factor activity. Together, these result in the degradation of the native ECM (extracellular matrix). For wound healing to occur, the balance between protease and growth factor activity has to be adjusted. Pre-clinical information available about the mode of action of an acellular matrix (such as Dermacell AWM) shows that it may assist in the following ways:
» Acts as a scaffold to support cell in-growth and angiogenesis
» Has receptors that permit fibroblasts to attach to the scaffold
» Tissue granulation
» Contains certain growth factors2
3/17/2016 12
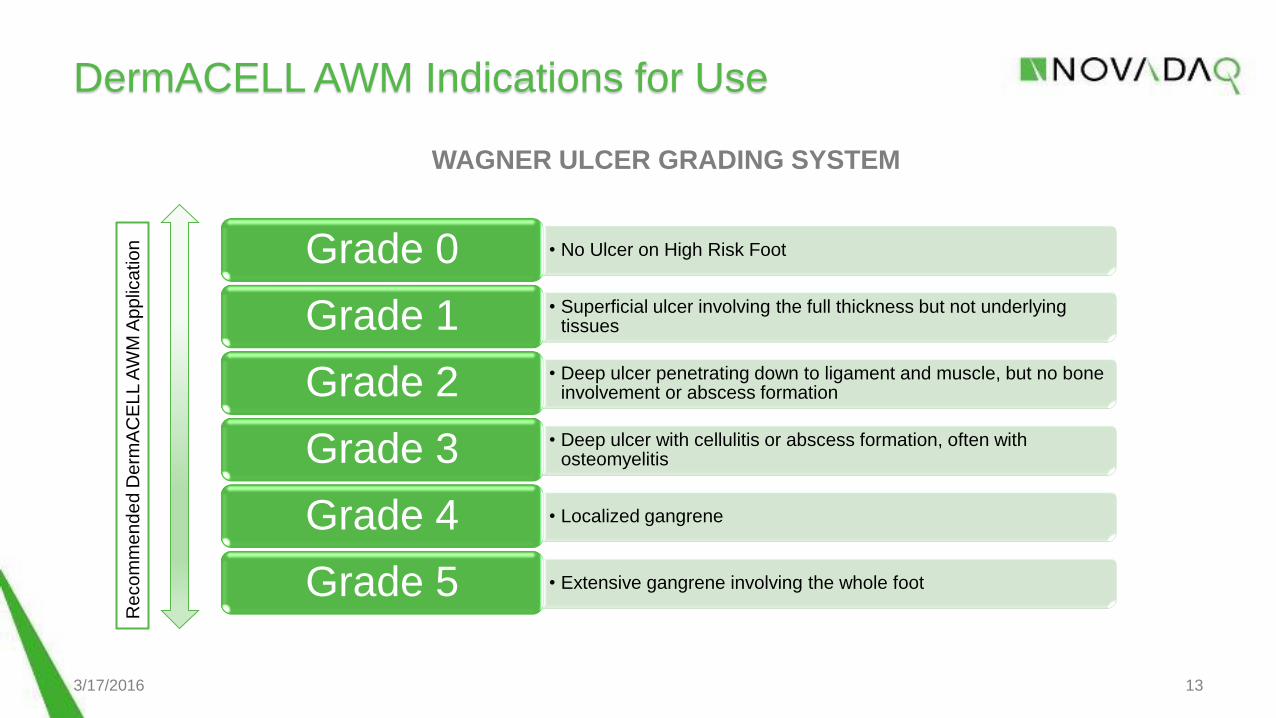
DermACELL AWM Indications for Use
3/17/2016 13
• No Ulcer on High Risk Foot Grade 0 • Superficial ulcer involving the full thickness but not underlying
tissues Grade 1 • Deep ulcer penetrating down to ligament and muscle, but no bone
involvement or abscess formation Grade 2 • Deep ulcer with cellulitis or abscess formation, often with
osteomyelitis Grade 3
• Localized gangrene Grade 4
• Extensive gangrene involving the whole foot Grade 5
Re
co
mm
en
de
d D
erm
AC
EL
L A
WM
Ap
plic
atio
n
WAGNER ULCER GRADING SYSTEM

DermACELL AWM Processing
• Biocompatible* Cells and > 97% DNA
Removed
• Retains native growth factors, collagen and elastin** Intact Acellular
Framework
• Excellent handling. Minimal Prep Time Room Temperature
Storage***
• Pull-out strength and load to failure are comparable to existing allograft products** Strength
• Maximized safety for patients Sterile (10-6 Sterility
Assurance Level)
3/17/2016 14
Optimal Decellularization. Safely and efficiently removes donor cells and DNA without
sacrificing the biomechanical or biochemical properties.
* ISO 10993-5 (Testing Results on File)
** Data on file at LifeNet Health, Virginia Beach, VA.
*** 15° – 30° C

DermACELL AWM Application
3/17/2016 15
Debridement • Remove the obvious
necrotic tissue, excessive bacterial burden and cellular burden of dead and senescent cells
Application • Apply Dermacell AWM
over the wound bed using sterile technique, with the reticular (dermal) side facing against the wound.
Fixation • Dermacell AWM should
be secured to the wound bed.
• Secure Dermacell AWM using Staples, Steri-strips® or Sutures

II. Results & Rigor of the Largest, Multicenter, Randomized,
Controlled Trial to date for Human Acellular Dermal Matrices
in Chronic Wounds
3/17/2016 16

A Clinical Trial of DermACELL AWM for Diabetic Foot Ulcers
3/17/2016 17
• Title:
Healing Rates in a Multicenter Assessment of a Sterile, Room Temperature,
Acellular Dermal Matrix Versus Conventional Care Wound Management and
an Active Comparator in the Treatment of Full-Thickness Diabetic Foot
Ulcers
• Published February 2016 in ePlasty
• Authors:
Jodi Walters, DPM – Southern Arizona VA Health Care System
Shawn Cazzell, DPM - Limb Preservation Platform, Valley Vascular Surgical Assoc.
Hau Pham, DPM – Boston Univ. School of Medicine, Boston Medical Center
Dean Vayser, DPM, FACFAS – ILD Research Center, San Diego CA
Alexander Reyzelman, DPM, FACFAS – UCSF Center for Limb Preservation

Study Design Endpoints
Primary Endpoint:
Assessment of complete re-epithelialization with no drainage or dressing requirements up to 16
weeks.
In further stringency, an assessment of wound closure required confirmation at 2 consecutive
study visits performed 2 weeks apart.
The healing rate of wounds at 16 weeks and the percentage of reduction in wound size from
baseline up to 16 weeks were also analyzed.
3/17/2016 18
Rigor of Study: It is important to note that the study reported here uses a more rigorous
healed ulcer criteria than other reports and as outlined in the FDA guidance on skin
substitutes and the 2011 report from the AHRQ on the design of products to assist with
wound healing. This study required that an ulcer must demonstrate complete healing on 2
consecutive visits to be considered healed rather than being considered healed at the first
instance of wound closure.

Study Objective:
Objective: The purpose of this 16-week, multicenter, randomized, controlled trial was to assess the
healed ulcer rate of a human acellular dermal matrix, Dermacell AWM, compared with conventional
care and a second acellular dermal matrix, GraftJacket, in the treatment of full-thickness diabetic
foot ulcers.
Three treatment arms:
3/17/2016 19
Conventional Care GraftJacket
(Conv Care) (D-ADM) (GJ – ADM)

Study Methods:
Methods: One hundred sixty-eight patients were randomized into Dermacell AWM, conventional
care, and GraftJacket treatment arms in a 2:2:1 ratio. Patients in the acellular dermal matrix groups
received either 1 or 2 applications of the graft at the discretion of the investigator. A second
application was allowed to be administered no fewer than 3 weeks but no longer that 12 weeks
(weeks 3-12) after the first application. Weekly follow-up visits were conducted until the ulcer healed
or the endpoint was reached.
3/17/2016 20
• 2:2:1 Ratio
• 1 or 2 applications
• Weekly follow-up

Inclusion Criteria
Inclusion criteria included:
– The patient having a single, full-thickness target DFU with a Wagner ulcer classification grade of 1 or 2
– A wound area of 1 cm2 or greater and less than 25 cm2
– A wound depth of 9 mm or less
– Adequate circulation to the affected area, defined as having at least one of the following criteria within the past 60
days:
• Transcutaneous oxygen measurement at the dorsum of the foot 30 mm Hg or more
• Ankle-brachial index ranging from 0.8 to 1.2
• Or at least biphasic Doppler arterial waveforms at the dorsalispedis and posterior tibial arteries
3/17/2016 21

Exclusion Criteria
Exclusion criteria included:
– Circulating hemoglobin A1c exceeding 12% within 90 days of the screening visit
– Serum creatinine concentrations of 3.0 mg/dL or greater within 30 days before screening
– Having had wound treatments involving biomedical or topical growth factors within 30 days before
screening
– Having undergone a revascularization procedure aimed at increasing blood flow in the target limb
– Or receiving a living skin equivalent within 4 weeks before screening
3/17/2016 22

3/17/2016 23
Patient Population

Approved Dressings
3/17/2016 24

Combined Study Results: Summary
Results:
At 16 weeks, the Dermacell AWM arm had:
– A significantly higher proportion of completely healed ulcers than the conventional care arm
• 67.9% vs 48.1%; P = .0385
– A non-significantly higher proportion than the GraftJacket arm
• 67.9% vs 47.8%; P = .1149
The Dermacell AWM arm also exhibited a greater average percent reduction in wound area than:
– The conventional care arm
• 91.4% vs 80.3%; P = .0791
– The GraftJacket arm
• 91.4% vs 73.5%; P = .0762
The proportion of severe adverse events and the proportion of overall early withdrawals were similar among the 3 groups based on relative population size (P ≥ .05).
3/17/2016 25

Combined Results: Complete Healing at 16 weeks
3/17/2016 26
Sta
tis
tic
ally S
ign
ific
an
t
Tre
nd
ing
to
wa
rd S
ign
ific
an
ce
At 16 Weeks, the Dermacell
AWM arm had:
- A statistically significant
higher proportion of
completely healed ulcers than
the conventional care arm
(67.9% vs 48.1%; P = .0385)
- A non-significantly higher
proportion than the
GraftJacket arm (67.9% vs
47.8%; P = .1149)

Combined Results: Percent (%) Wound Reduction
3/17/2016 27
At 16 weeks, the Dermacell AWM
arm exhibited a greater average
percent (%) reduction in wound
area than:
- The conventional care arm
(91.4% vs 80.3%; P = .0791)
- And the GraftJacket arm (91.4%
vs 73.5%; P = .0762).
Significance of % Wound Reduction
D-ADM–treated ulcers demonstrated a greater reduction in wound size than both the
conventional care and GJ-ADM arms at 12 weeks and 16 weeks
Early prediction of wound healing
Reversal of ulcer gradation using the Wagner scale
Improvement in performance on foot pressure tests.7-9
Higher healed ulcer rates are critical to reducing the escalating cost of treating DFUs faced
by both patients and the health care system.11 Amputation and hospitalization expenses
averaged $18,084 for a minor procedure and $13,258 per stay,12 respectively, making early
and effective treatment important to avoid spiraling costs.
3/17/2016 28

One-Application Data
3/17/2016 29
DermACELL AWM
# of
patients 12 Week Wound Closure 16 Week Wound Closure Healing Rates
1-application 40
Statistically significant
higher rates of closure than
conventional care and higher
closure rate than 1-app GJ-
ADM
Statistically significant
higher rates of closure than
conventional care and
strong but nonsignificant
over GJ-ADM
The difference in %
average wound area
reduction was
significant at weeks
3 and 6-15 vs. conv
care

One Application Data – 12 Weeks
One & Done
A Cost-Effective, One Application Solution
Complete Healing at 12 Weeks
– Dermacell AWM (40 Patients): 65%
– Conventional Care (56 Patients): 41.1%
– GraftJacket (16 Patients): 56.3%
Percent (%) Wound Reduction
– Dermacell AWM (40 Patients): 94.6%
– Conventional Care (56 Patients): 71.6%
– GraftJacket (16 Patients): 88%
3/17/2016 30
A single application of Dermacell AWM
demonstrated Statistical Significance
over the Conventional Care arm in both
Complete Healing (P=0.0203) and
% Wound Reduction (P=0.0004)
at 12 Weeks

Single Application Study Comparison – Integra IDRT
Integra IDRT – Founder Study*
3/17/2016 31
0%
10%
20%
30%
40%
50%
60%
70%
80%
DermACELL AWM - Combined
Integra IDRT
16 Week Healing Rates
• It should also be noted that of the 53 D-ADM
patients, 40 patients received 1 application
and 13 patients received 2 applications of D-
ADM
• In contrast, Integra IDRT patients received as
many as 15 applications.
*Driver VR, Lavery LA, Reyzelman AM, et al. A clinical trial of
Integra® template for diabetic foot ulcer treatment. Wound Repair
Regen. 2015;23(6):891-900.

Study Rigor
This study required that an ulcer must demonstrate complete healing on 2 consecutive visits
to be considered healed rather than being considered healed at the first instance of wound
closure
While this analysis likewise relied on the disposition by the respective principal investigators of
whether a wound was healed, we also sought the opinion of a blinded third-party adjudicator.
At the 12-week primary endpoint, more than 87% agreement in assessment of complete healing
was obtained between the blinded adjudicator and the principal investigator.
The more stringent healed ulcer criteria should be taken into account when comparing the healing
rates of this study with others that have been published, especially those before 2011. Several
ulcers in this study had 100% wound size reduction at a given week but were not considered
healed because of these criteria.
3/17/2016 32

3/17/2016 33
Preoperative diabetic foot ulcer at
baseline with an area of 6.4 cm2 after
debridement.
Wound was completely closed
at 12 weeks following treatment
with a single application of D-ADM.

III. A Changing Paradigm: DermACELL AWM as a One-Application,
Cost-Effective Solution
3/17/2016 34

As a leader in the Wound Care field, your ultimate goal is to provide evidence
based, high-quality and fiscally responsible treatments to your patients.
3/17/2016 35
Dermacell AWM provides a cost-effective, one-application treatment solution for
patients with chronic lower extremity ulcerations. In the largest and most rigorous
randomized, controlled trial (RCT) to date for human ADM products in chronic
wounds, Dermacell AWM demonstrated superior rates of healing and wound
closure in Diabetic Foot Ulcers than conventional care and an active comparator.
Unlike many other human tissue products, Dermacell AWM can be stored for up to
4 years in ambient temperature, does not require special handling and is fast and
easy to apply.
• One Application
• Cost-Effective
• Rigorous Level I Clinical Data

Putting It All Together
3/17/2016 36
The Future of Wound Care Management
LUNA Case Manager
Dermacell AWM
The Mission of NOVADAQ Wound Care

References
1. LNH Sterile Decellularized Dermis IFU 63-0050-01
2. Acellular Matrices For The Treatment Of Wounds; International Consensus; Wounds International Enterprise House; 2011
3. DermACELL Application Instructions 68-40-148.00
4. DermACELL Application Guide 68-50-237 .01
5. Guidelines for the Treatment of Diabetic Ulcers. David L. Steed, MD, et. al. Wound Repair and Regeneration; 2006 by the Wound Healing Society
6. http://www.ethicon360.com
7. Snyder RJ, Cardinal M, Dauphin´ee DM, Stavosky J. A post-hoc analysis of reduction in diabetic foot ulcersize at 4 weeks as a predictor of healing by 12 weeks. Ostomy Wound Manage. 2010;56(3):44-50.
8. Sheehan P, Jones P, Caselli A, Giurini JM, Veves A. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care. 2003;26(6):1879-82.
9. Bashmakov YK, Assaad-Khalil SH, Seif MA, et al. Resveratrol promotes foot ulcer size reduction in type 2 diabetes patients. ISRN Endocrinol. 2014;2014:1-8.
10. Hicks CW, Selvarajah S, Mathioudakis N, et al. Trends and determinants of costs associated with the inpatient care of diabetic foot ulcers. J Vasc Surg. 2014;60(5):1247-54.
11. Rice JB, Desai U, Cummings AK. Burden of diabetic foot ulcers for Medicare and private insurers. Diabetes Care. 2014;37(3):651-8.
12. Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. A meta-analysis. Diabetes Care. 1999;22(5):692-5.
3/17/2016 37
