evolving concepts in defining optimal strategies for management of ihd
TRANSCRIPT
Evolving Concepts in Defining Optimal
Strategies for Management of IHD
Dr. Kyaw Soe Win
Department of Cardiovascular Medicine9-Mar-15
Myanmar Medical Conference Taungyi

Angina and IHD
ANGINA is pain or discomfort in the chest
caused by inadequate blood flow through the
coronary blood vessels, is a consequence of
myocardial O2 demand exceeding supply.
It is the principle symptom of ischemic heart
disease (IHD); This is sometimes called
myocardial ischaemia
Types of Angina
Chronic stable angina also called classic, typical, or effort angina
Unstable anginaalso called preinfarction or crescendo angina
Vasospastic anginaalso called Prinzmetal’s or variant angina
9-Mar-15
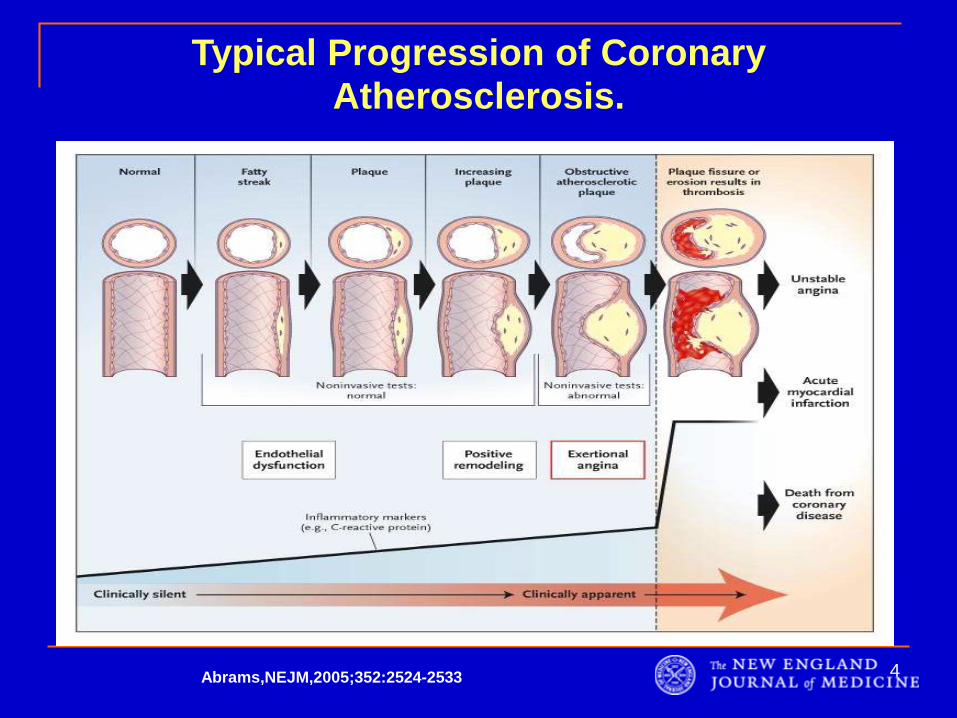
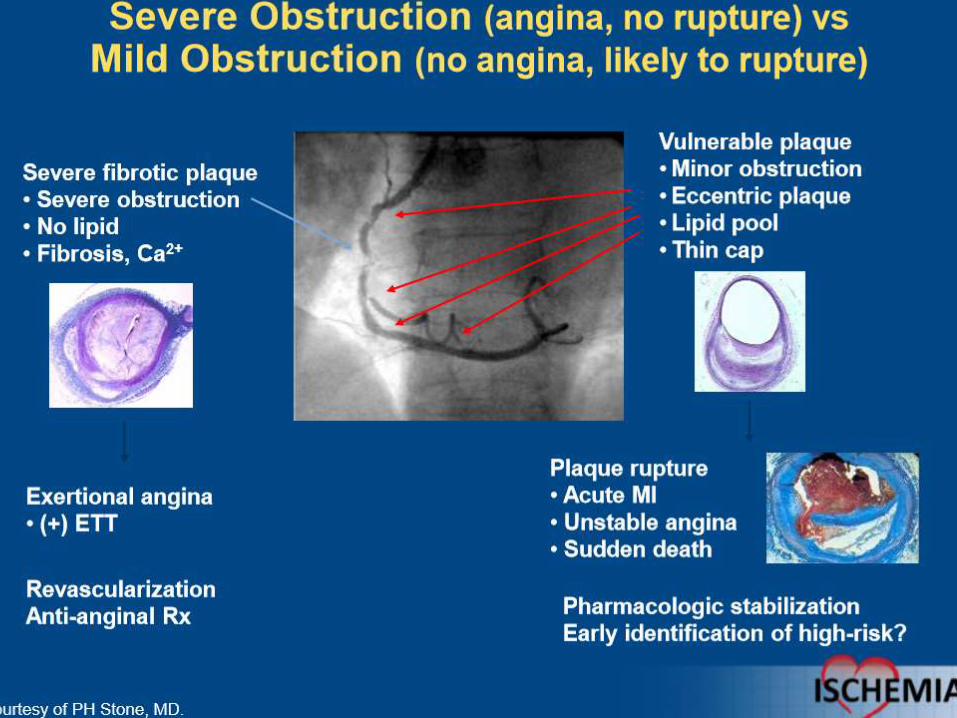
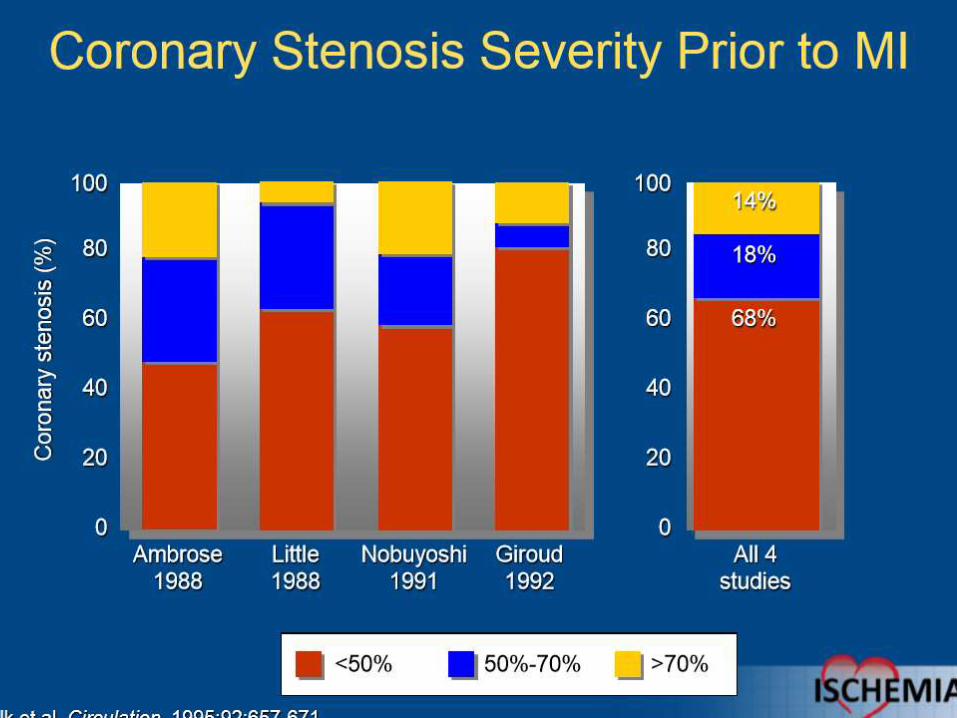
Typical Progression of Coronary Atherosclerosis.
4Abrams,NEJM,2005;352:2524-2533
Stable angina: the most common
(90%) is chest pain caused by a temporary
inadequacy of blood flow to the myocardium
• Usually lasts 1-15 minutes, and is provoked
by exercise, stress, extreme cold or heat,
heavy meals, alcohol, or smoking.
Rx: is promptly relieved by rest or
nitroglycerin (a vasodilator).
• The underlying cause is usually narrowing
of the coronary arteries by atheroma - the
narrowing of blood vessels by deposits of
fatty or fibrous material
Unstable angina
lies between stable angina and MI.
The pathology is similar to that involved in MI: a
platelet-fibrin thrombus associated with a raptured
atherosclerotic plaque, but without complete
occlusion of the blood vessel.
1. chest pains occur with increased frequency
2. precipitated by progressively less effort.
3. The symptoms are NOT relieved by rest or
nitroglycerin.
4. requires hospital admission and more aggressive
therapy to prevent death and progression to MI.
9-Mar-15

Aims of drug treatment for stable
Angina
Relieve symptoms
Minimize the frequency, duration and
intensity of attacks.
Improve the patient’s functional capacity with
as few side effects as possible
Stop and regression of the disease process
Prevent or delay the worst possible outcome,
MI & death
9-Mar-15
To reduce the cardiac workload and
metabolic demand
To increase the perfusion of the heart
muscle
To prevent myocardial infarction
Therapeutic goals

To reduce the cardiac workload and metabolic demand
To increase the perfusion of the heart muscle
To prevent myocardial infarction
Ca2+ antagonists, β-adrenoreceptor antagonists,
Ivabradine, Trimetazidine, Ranolazine
Lipid lowering drugs, particularly statins, can be given if
elevated plasma cholesterol levels are detected
Antiplatelet drugs, especially low-dose (75mg) aspirin to
reduce the possibility of thrombosis.
Therapeutic goals
Nitrates, Nicorandil, PCI, CABG
Treatment of Chronic Stable Angina
MedicalRevascularization
PCI CABG
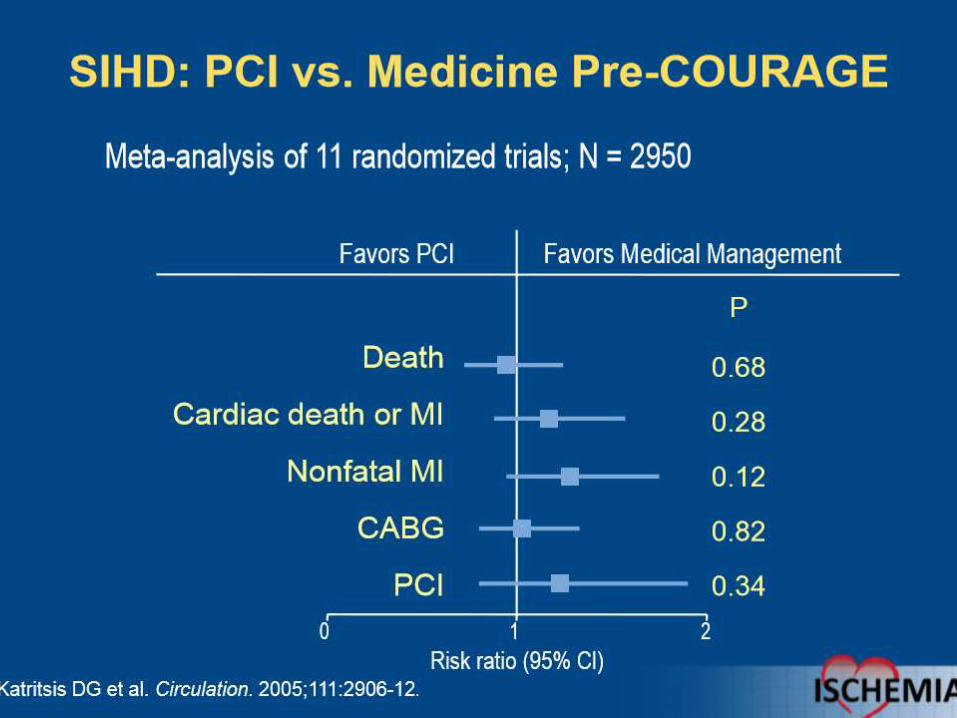
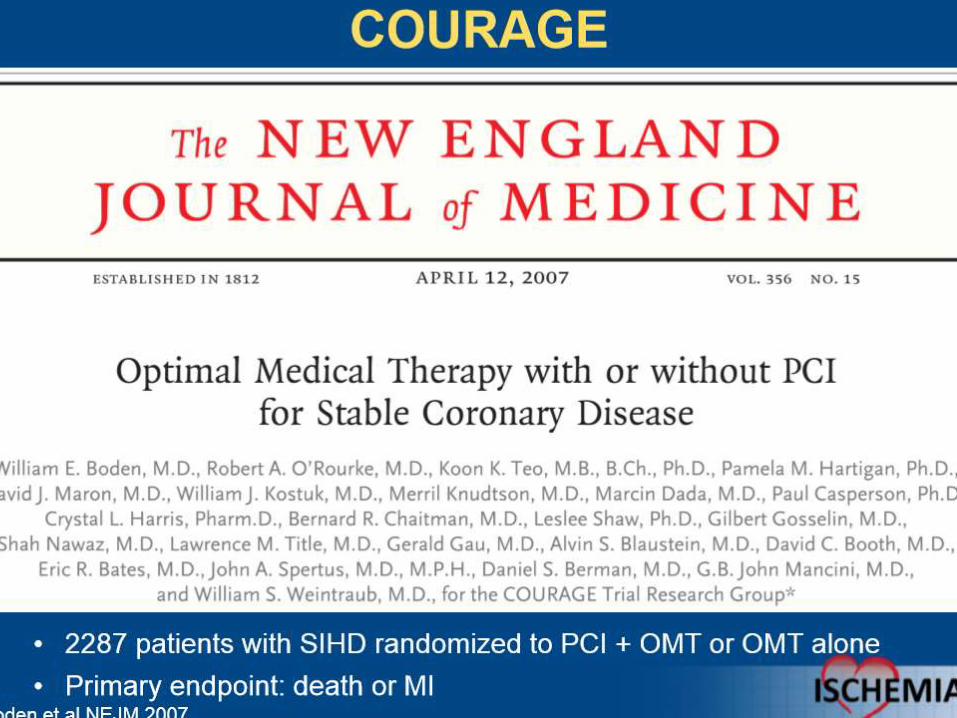
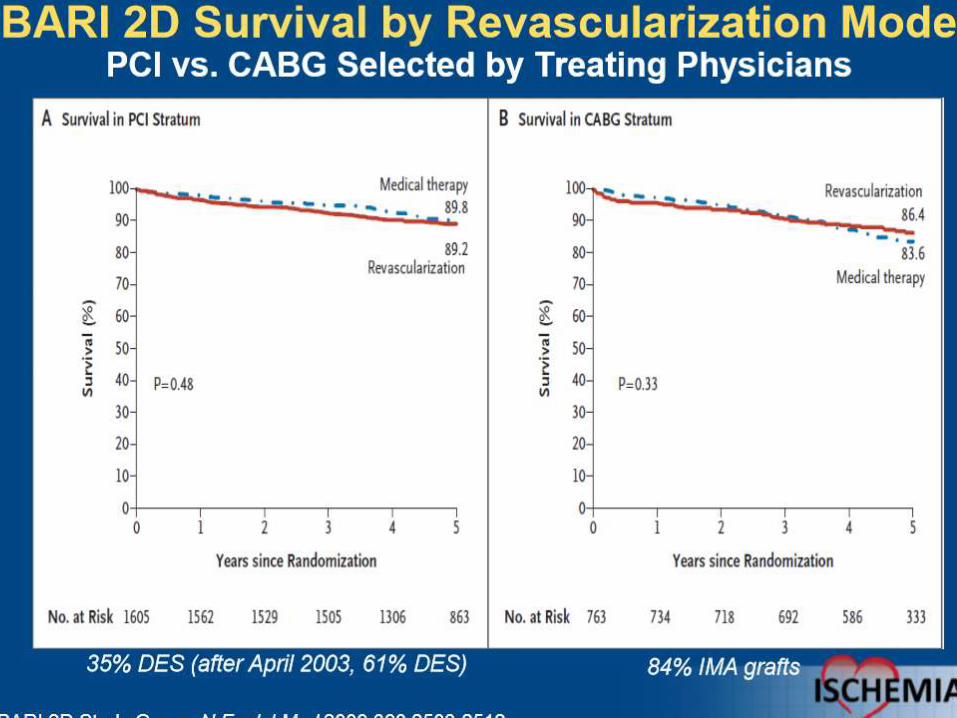
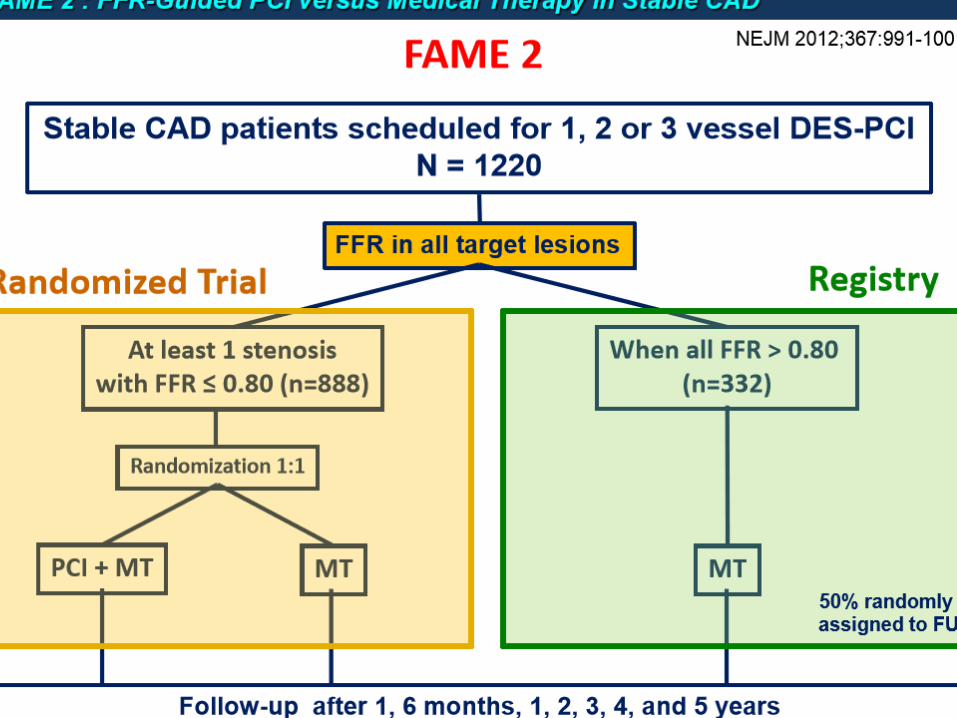
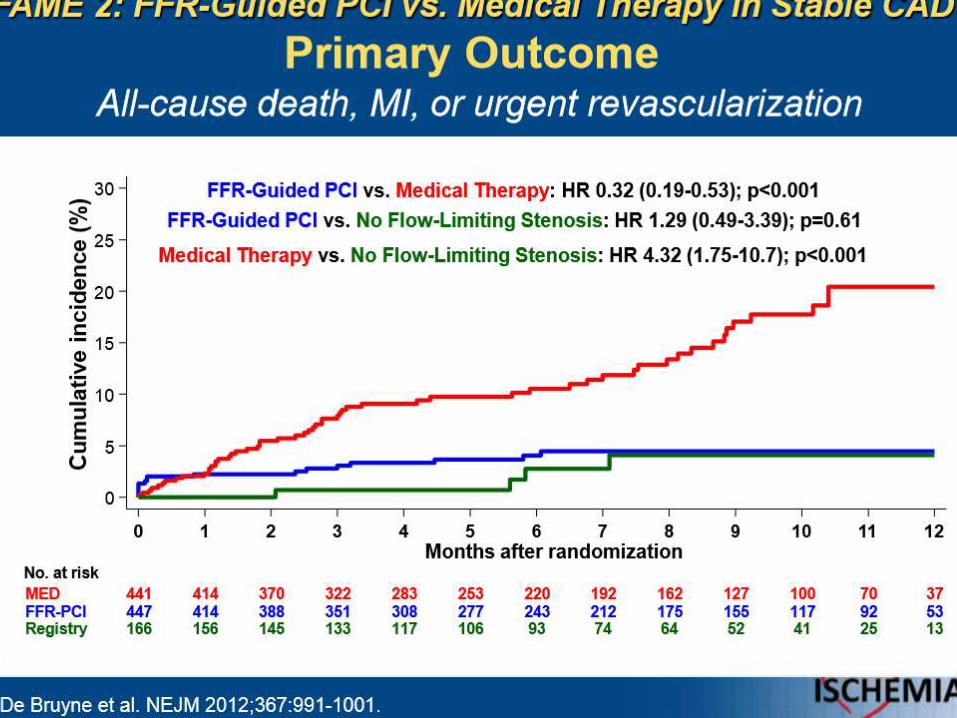
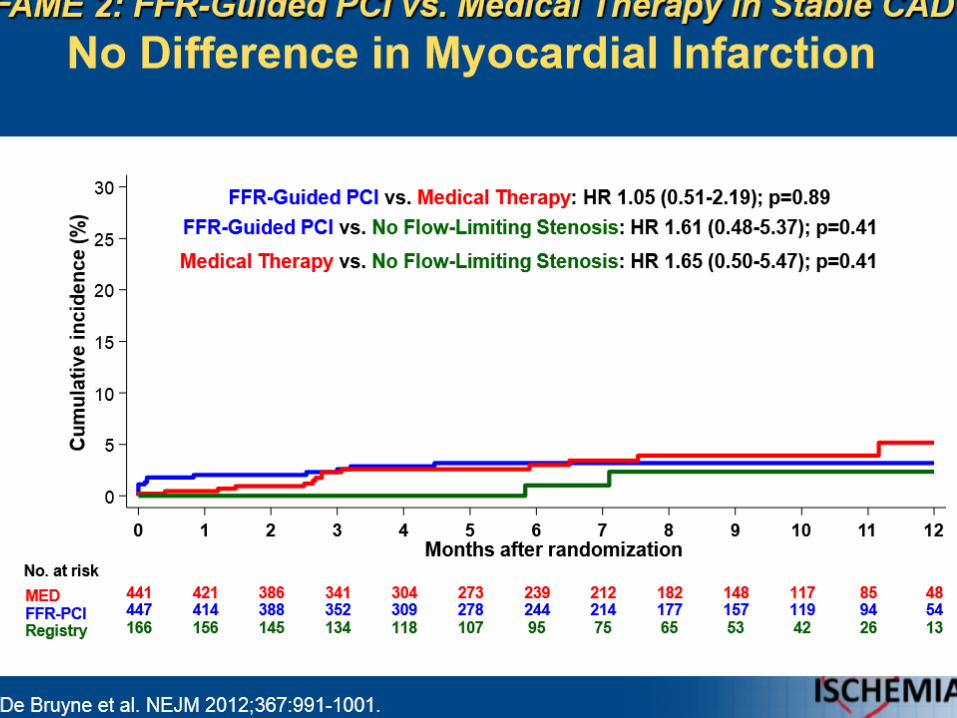
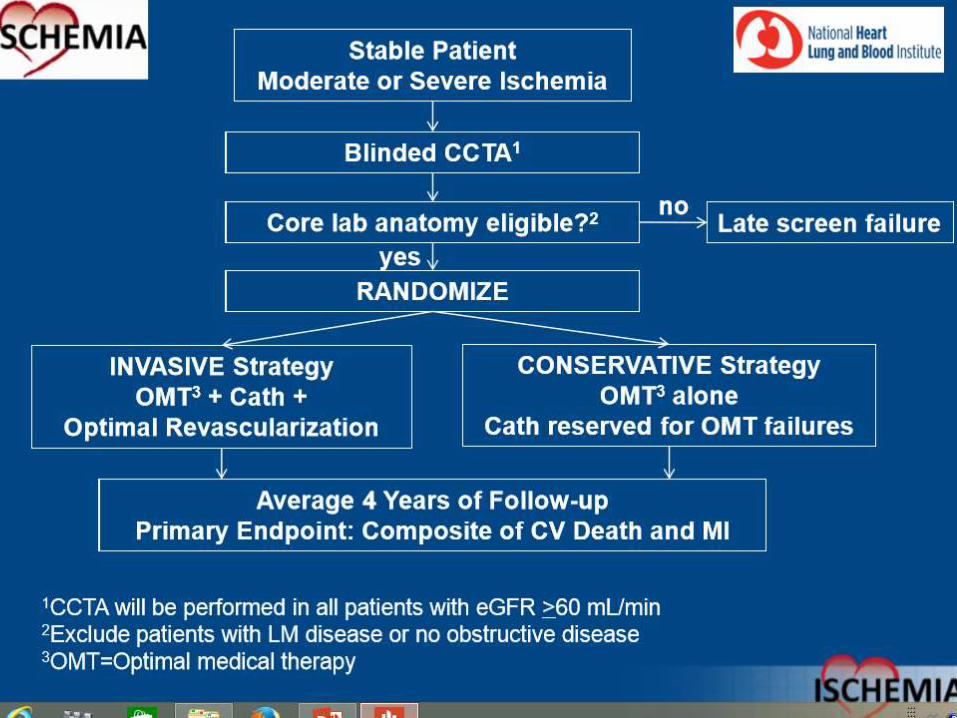
Does Revascularization improve
Prognosis in Stable IHD ie;
Reduction of and MI and death?
9-Mar-15

9-Mar-15

9-Mar-15
9-Mar-15
9-Mar-15

9-Mar-15

9-Mar-15

9-Mar-15
9-Mar-15
9-Mar-15
9-Mar-15

9-Mar-15
9-Mar-15

9-Mar-15
9-Mar-15

9-Mar-15

9-Mar-15

9-Mar-15

9-Mar-15

9-Mar-15
9-Mar-15
9-Mar-15
9-Mar-15

9-Mar-15
9-Mar-15

9-Mar-15
9-Mar-15
Does Revascularization improve
Prognosis in Stable IHD ie;
Reduction of and MI and death ?
9-Mar-15
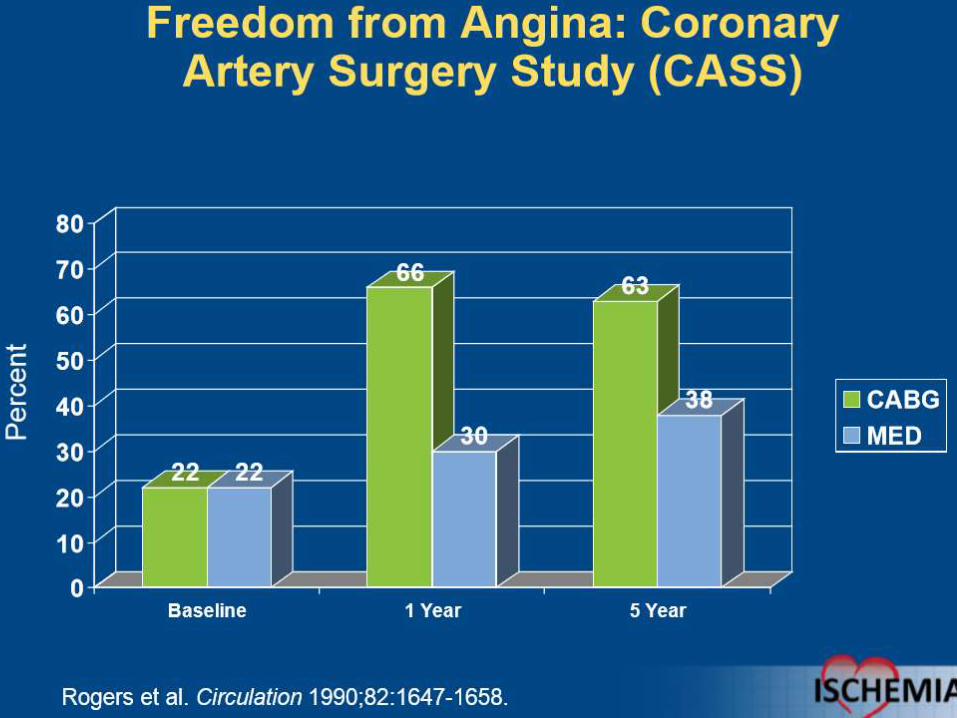
Does Revascularization improve
symptom ?
No
Yes

Optimal Medical Therapy for Stable
Coronary Artery Disease.
39
1.Non-pharmacologic therapy
2.Vasculoprotective therapy
3.Anti-anginal therapy
40
1.Lifestyle Modification
1. Regular aerobic activity
2. Weight reduction and maintainence
3. Diet
4. Tobacco abstinence and avoidance
of passive smoke
2.Optimize non cardiac comorbidities
Non Pharmacologic Therapy
9-Mar-15

9-Mar-15
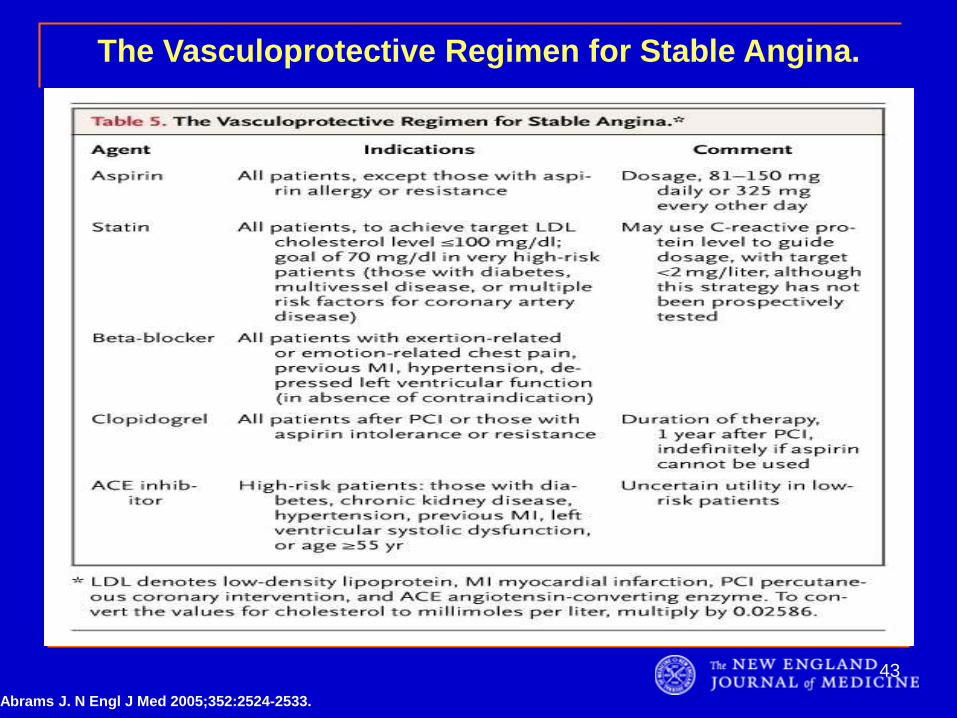
The Vasculoprotective Regimen for Stable Angina.
Abrams J. N Engl J Med 2005;352:2524-2533.
43
Antianginal Drugs
Nitrates : sublingual, transcutaneous, oral
Beta Blockers
Calcium Channel Blockers
Nicorandil
9-Mar-15

NEWER ANTIANGINAL DRUGS
Metabolic modulators, eg, ranolazine,
trimetazidine
Direct bradycardic agents, eg, ivabradine
Potassium channel activators, eg, nicorandil
9-Mar-15
European guidelines onthe management of
stable coronary artery disease
Key points&
new position for Ivabradine and Trimetazidine
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
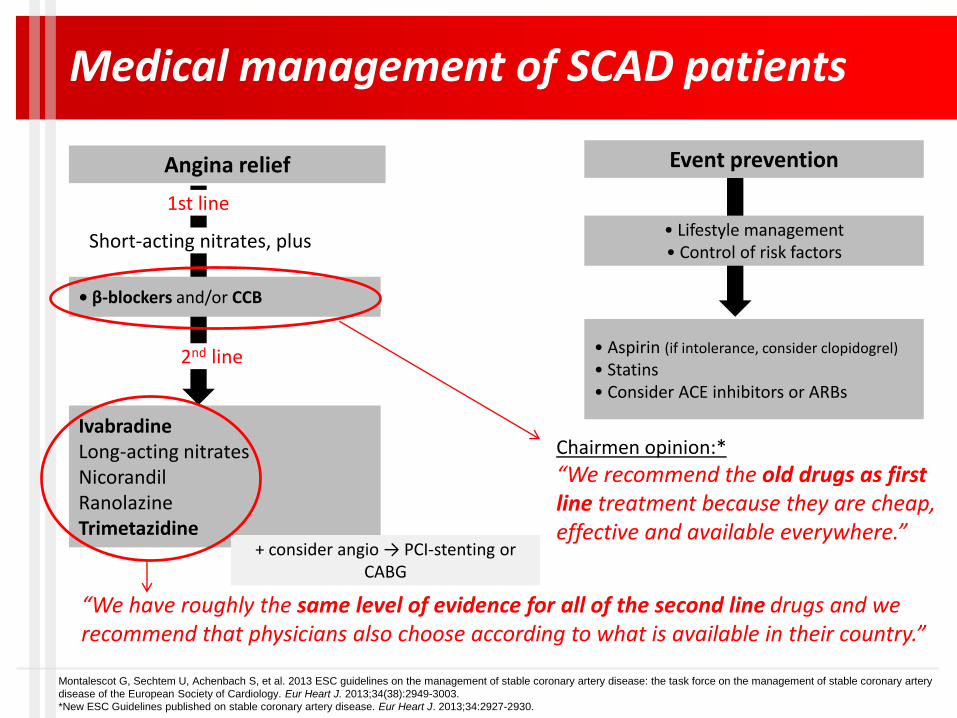
Medical management of SCAD patients
“We recommend the old drugs as first line treatment because they are cheap, effective and available everywhere.”
“We have roughly the same level of evidence for all of the second line drugs and we recommend that physicians also choose according to what is available in their country.”
Chairmen opinion:*
Angina relief Event prevention
• β-blockers and/or CCB
IvabradineLong-acting nitratesNicorandilRanolazineTrimetazidine
• Lifestyle management• Control of risk factors
• Aspirin (if intolerance, consider clopidogrel)
• Statins• Consider ACE inhibitors or ARBs
+ consider angio → PCI-stenting or CABG
Short-acting nitrates, plus
1st line
2nd line
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
*New ESC Guidelines published on stable coronary artery disease. Eur Heart J. 2013;34:2927-2930.
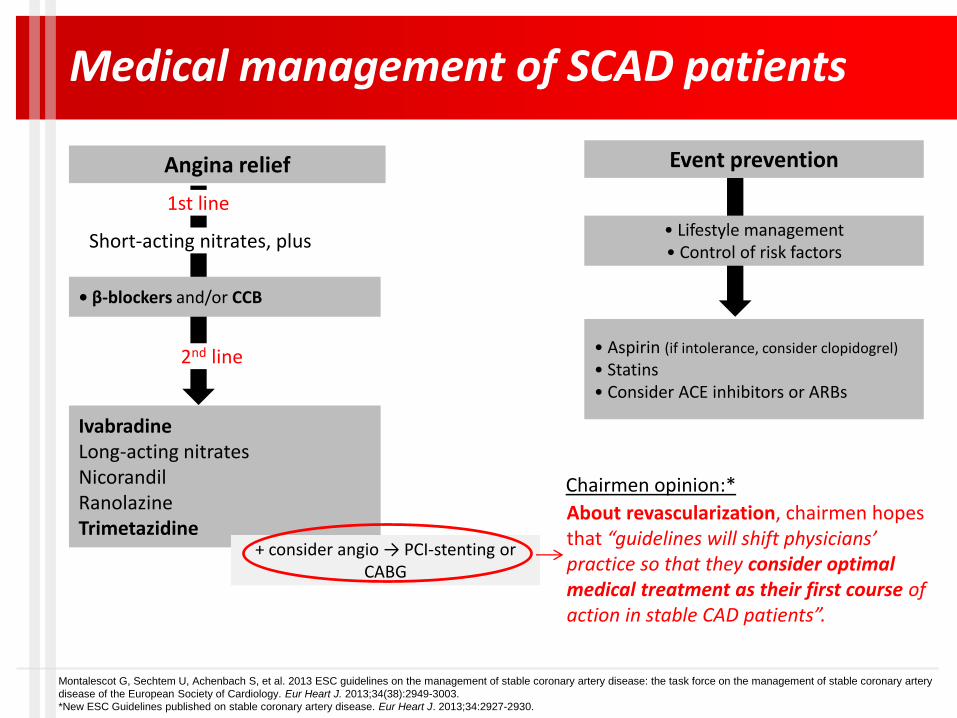
Medical management of SCAD patients
Chairmen opinion:*
Angina relief Event prevention
• β-blockers and/or CCB
IvabradineLong-acting nitratesNicorandilRanolazineTrimetazidine
• Lifestyle management• Control of risk factors
• Aspirin (if intolerance, consider clopidogrel)
• Statins• Consider ACE inhibitors or ARBs
+ consider angio → PCI-stenting or CABG
Short-acting nitrates, plus
1st line
2nd line
About revascularization, chairmen hopes that “guidelines will shift physicians’ practice so that they consider optimal medical treatment as their first course of action in stable CAD patients”.
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
*New ESC Guidelines published on stable coronary artery disease. Eur Heart J. 2013;34:2927-2930.

• Women Women more frequently have CAD with stable angina and no obstructive
coronary disease.
Women are more likely to have complications from revascularization.
• Diabetic patients Need different risk factor management.
• Older patients High-risk group with higher mortality and higher rates of myocardial infarction.
Usually undertreated, receiving less drugs.
Difficult diagnosis due to atypical symptoms.
Higher risk of complications during and after coronary revascularization.
• Comorbidities/intolerance Depending on comorbidities/tolerance, it is indicated to use second-line therapies
as first-line treatment in selected patients.
Specific patient profiles
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.

Therapy to prevent MI and death
Aspirin
Low-dose aspirin is the drug of choice in most cases and clopidogrel
may be considered for some patients.
Statin
Target LDL-C: <1.8 mmol/L and/or >50% reduction if the target level
cannot be reached.
Renin-angiotensin-aldosterone system blockers
ACE inhibitors are recommended for the treatment of patients with
SCAD, especially with coexisting hypertension, LVEF ≤40%, diabetes,
or chronic kidney disease, unless contra-indicated.
ARBs are recommended as an alternative therapy for patients with
SCAD when ACE inhibition is indicated but not tolerated.
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
“Adding ivabradine 7.5 mg twice daily to atenolol therapy gave better control of heart rate and
anginal symptoms.”
“In 1507 patients with prior angina enrolled in the Morbidity-Mortality Evaluation of the If Inhibitor
Ivabradine in Patients With Coronary Artery Disease and Left Ventricular Dysfunction
(BEAUTIFUL) trial, ivabradine reduced the composite primary end point of CV death,
hospitalization with MI and HF, and reduced hospitalization for MI. The effect was
predominant in patients with a heart rate 70 bpm.”
“Ivabradine is thus an effective anti-anginal agent, alone or in combination with β-blockers.”
New ESC guidelines and Ivabradine
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.

New ESC guidelines and Trimetazidine
“Trimetazidine is an anti-ischemic metabolic modulator, with similar anti-
anginal efficacy to propranolol in doses of 20 mg thrice daily.”
“Trimetazidine (35 mg twice daily) added to β-blockade (atenolol)
improved effort-induced myocardial ischemia, as reviewed by the EMA in
June 2012.”
In diabetic persons, Trimetazidine improved HbA1c and glycemia, while
increasing forearm glucose uptake.”
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.

Conclusion
ESC Guidelines highlighted two aims for the pharmacological management
of stable CAD patients: obtain relief of symptoms and prevent cardiovascular
events.
CAD patients should all receive aspirin and a statin, plus an ACE inhibitor
in case of comorbidities.
-blockers or CCBs should be prescribed as first-line treatment to reduce
angina.
Ivabradine and Trimetazidine (as well as long-acting nitrates, nicorandil and
ranolazine) are recommended second-line, in combination with first-line
treatment, in patients remaining symptomatic.
Physicians should consider optimal medical treatment before
revascularization procedures.
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery
disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.

54
Lifestyle modification and management of non-
cardiac comorbidities is important.
It needs to be understood that coronary artery
disease is a chronic condition, which is
manageable but not curable.
Conclusions
Vasculoprotective therapy is important
including antiplatelet agents such as aspirin
and clopidogrel, statins, and ACEI
Antianginal drugs should be prescribed to
relieve symptoms. Beta blockers should be
used unless contraindicated or not tolerated.
Under most circumstances, optimal medical
therapy is primary approach and
revascularization should be considered as
needed or for special coronary anatomy.
Conclusions

What is the role of revascularization
in unstable IHD ie; Acute Coronary
Syndrome?
9-Mar-15

Thank you
9-Mar-15