exam corner - bone & joint publishing
TRANSCRIPT

Exam Corner August 2012 - Answers
The FRCS (Tr & Orth) examination has three components: MCQs, Vivas and Clinical Examination. The Vivas are further
divided into five sections comprising Basic Science, Adult Pathology, Hands, Children’s Orthopaedics and Trauma. The
Clinical Examination section is divided into upper- and lower-limb cases. The aim of this section in the Journal is to focus
specifically on the trainees preparing for the exam and to cater to all the sections of the exam every month. The vision is to
complete the cycle of all relevant exam topics (as per the syllabus) in four years.Vikas Khanduja, MSc, FRCS (Orth)
Consultant Orthopaedic
Surgeon,
Addenbrooke’s -
Cambridge University
Hospital NHS Trust,
Cambridge
CB2 0QQ, UK.
Associate Editor, the
Journal of Bone and
Joint Surgery [Br]
email: [email protected]
Contributors:
Simranjeev Johal
SpR East of England
Rotation
Karanjeev Johal
SpR, North Thames
Rotation
Mr Paul Robinson,
Specialty Registrar, East
of England Rotation
1. Which one of the following statements is false regarding septic arthritis in children?
e. An aspirate white blood cell count of > 50 000/mm3 with 75% polymorphonuclear leucocytes is diagnostic of sepsis in 60% to 70% of patients Male gender is a risk factor for septic arthritis. The knee and the hip are affected in around one third of cases each, with the lower extremity accounting for the majority of cases.1-3 An aspirate, WBC count of greater than 50 000/mm3 with 75% polymorphonuclear leucocytes is diagnostic of sepsis in 30 to 50%.
2. Which one of the following statements is true regarding the use of forest plots in systematic reviews? They:
a. Summarise treatment efficacies (risk ratio) across trials Forest plots are graphical representations of meta-analysis. They show the effect estimate and weight of each individual study as well as the overall effect estimate of combined studies. The effect measures that are commonly used include odds ratio and risk ratio amongst others. A box and a horizontal line represent each study. The mid-point of the box represents the point effect estimate of each study. The area of the box represents the weight given to each study. The width/length of the horizontal line represents the 95% confidence interval for the effect estimate of each study. A diamond represents the overall effect estimate. The width of the diamond represents the confidence interval for the overall effect estimate. There is also a vertical line, known as the line of no effect. The Forest plot also provides the summary data entered for each study. In addition, it provides the weight for each study, the effect measure, method and the model used to perform the meta-analysis, the confidence intervals used, the effect estimate from each study, the overall effect estimate and the statistical significance of the analysis. Information is also provided about the heterogeneity of the analysis.
3. Which of the following statements is false for the AAOS grades of recommendation for summaries or reviews of orthopaedic studies?
b. A systematic review of Level I studies investigating the results of treatment with inconsistent results would constitute a fair evidence study (Grade B)
AAOS Grades of Recommendation for Summaries or Reviews of Orthopaedic Surgical Studies: http://www.aaos.org/research/evidence/gradesofrec.asp
Grade Description
AGood evidence (Level I Studies with consistent finding) for or against recommending intervention.
BFair evidence (Level II or III Studies with consistent findings) for or against recommending intervention.
CPoor-quality evidence (Level IV or V) for or against recommending intervention.
D
There is insufficient or conflicting evidence not allowing a recommendation for or against intervention.
See also levels of evidence http://www.aaos.org/research/evidence/levelstables.pdf
4. All of the following have been shown to slow disease progress in osteoarthritis except:
d. Hyaluronic acid There is evidence that all of these agents have some effect on disease progression. Glucosamine (Cochraine review), Chondroitin (various studies, Cochrane review in progress), Diacetylrhein (Cochrane review), Doxycycline (Cochrane review “The symptomatic benefit of doxycycline is minimal to non-existent. The small benefit in terms of joint space narrowing is of questionable clinical relevance and outweighed by safety problems. Doxycycline should not be recommended for the treatment of osteoarthritis of the knee or hip”), Hyaluronic acid (Cochrane review on viscosupplementation does not comment on disease progression, but concludes that HA is beneficial for pain and function. Some papers quote a positive effect on disease progression).
5. Which of the following statements is true regarding the use of tranexamic acid in orthopaedic surgery?
c. It reduces the need for transfusion after joint replacement Tranexamic acid significantly reduces the need for allogeneic blood transfusion after joint replacement surgery. Meta-analysis of existing RCTs does not support an increased risk of thromboembolic events. However, the overall effect on mortality, DVT and PE remains uncertain
MCQs – Single Best Answer
Vivas
Adult Pathology
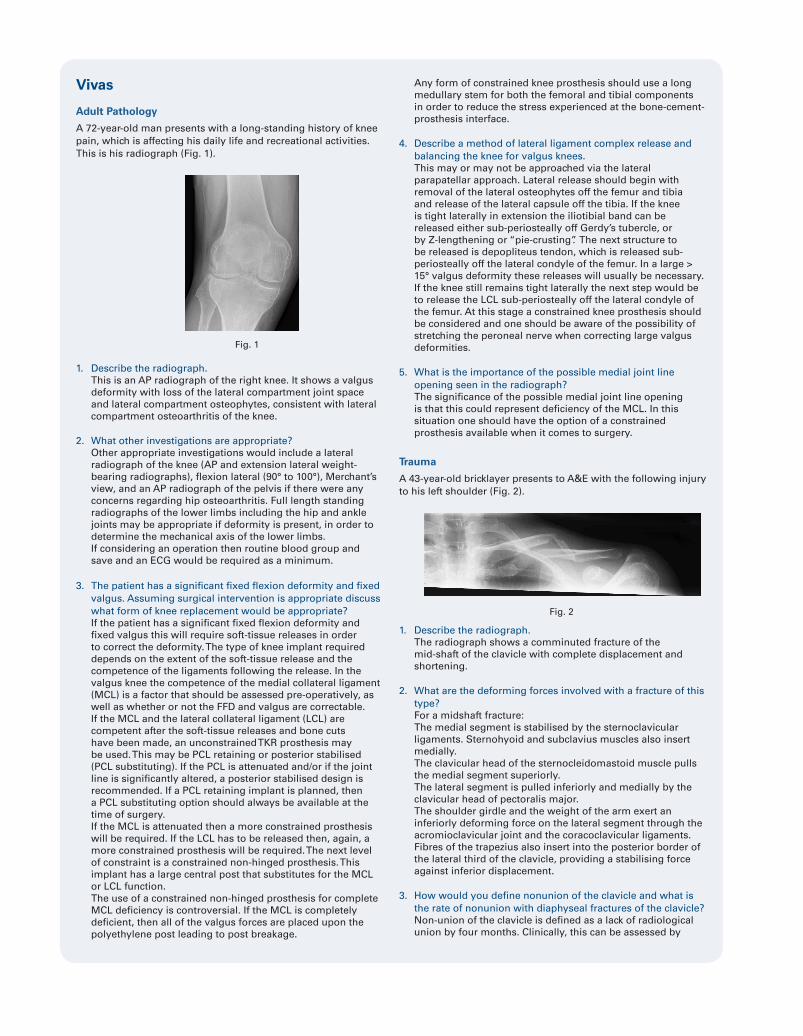
A 72-year-old man presents with a long-standing history of knee pain, which is affecting his daily life and recreational activities. This is his radiograph (Fig. 1).
1. Describe the radiograph.This is an AP radiograph of the right knee. It shows a valgus deformity with loss of the lateral compartment joint space and lateral compartment osteophytes, consistent with lateral compartment osteoarthritis of the knee.
2. What other investigations are appropriate?Other appropriate investigations would include a lateral radiograph of the knee (AP and extension lateral weight-bearing radiographs), flexion lateral (90° to 100°), Merchant’s view, and an AP radiograph of the pelvis if there were any concerns regarding hip osteoarthritis. Full length standing radiographs of the lower limbs including the hip and ankle joints may be appropriate if deformity is present, in order to determine the mechanical axis of the lower limbs. If considering an operation then routine blood group and save and an ECG would be required as a minimum.
3. The patient has a significant fixed flexion deformity and fixed valgus. Assuming surgical intervention is appropriate discuss what form of knee replacement would be appropriate?If the patient has a significant fixed flexion deformity and fixed valgus this will require soft-tissue releases in order to correct the deformity. The type of knee implant required depends on the extent of the soft-tissue release and the competence of the ligaments following the release. In the valgus knee the competence of the medial collateral ligament (MCL) is a factor that should be assessed pre-operatively, as well as whether or not the FFD and valgus are correctable.If the MCL and the lateral collateral ligament (LCL) are competent after the soft-tissue releases and bone cuts have been made, an unconstrained TKR prosthesis may be used. This may be PCL retaining or posterior stabilised (PCL substituting). If the PCL is attenuated and/or if the joint line is significantly altered, a posterior stabilised design is recommended. If a PCL retaining implant is planned, then a PCL substituting option should always be available at the time of surgery. If the MCL is attenuated then a more constrained prosthesis will be required. If the LCL has to be released then, again, a more constrained prosthesis will be required. The next level of constraint is a constrained non-hinged prosthesis. This implant has a large central post that substitutes for the MCL or LCL function. The use of a constrained non-hinged prosthesis for complete MCL deficiency is controversial. If the MCL is completely deficient, then all of the valgus forces are placed upon the polyethylene post leading to post breakage.
Any form of constrained knee prosthesis should use a long medullary stem for both the femoral and tibial components in order to reduce the stress experienced at the bone-cement-prosthesis interface.
4. Describe a method of lateral ligament complex release and balancing the knee for valgus knees. This may or may not be approached via the lateral parapatellar approach. Lateral release should begin with removal of the lateral osteophytes off the femur and tibia and release of the lateral capsule off the tibia. If the knee is tight laterally in extension the iliotibial band can be released either sub-periosteally off Gerdy’s tubercle, or by Z-lengthening or “pie-crusting”. The next structure to be released is depopliteus tendon, which is released sub-periosteally off the lateral condyle of the femur. In a large > 15° valgus deformity these releases will usually be necessary. If the knee still remains tight laterally the next step would be to release the LCL sub-periosteally off the lateral condyle of the femur. At this stage a constrained knee prosthesis should be considered and one should be aware of the possibility of stretching the peroneal nerve when correcting large valgus deformities.
5. What is the importance of the possible medial joint line opening seen in the radiograph?The significance of the possible medial joint line opening is that this could represent deficiency of the MCL. In this situation one should have the option of a constrained prosthesis available when it comes to surgery.
Trauma
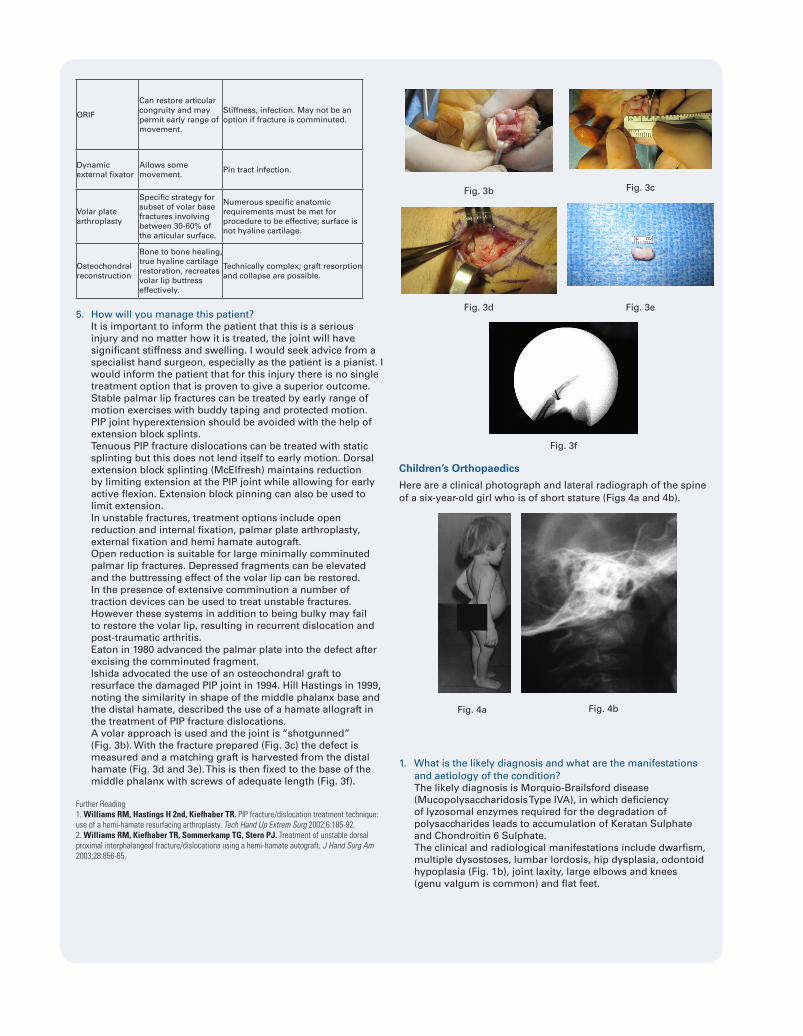
A 43-year-old bricklayer presents to A&E with the following injury to his left shoulder (Fig. 2).
1. Describe the radiograph.The radiograph shows a comminuted fracture of the mid-shaft of the clavicle with complete displacement and shortening.
2. What are the deforming forces involved with a fracture of this type?For a midshaft fracture:The medial segment is stabilised by the sternoclavicular ligaments. Sternohyoid and subclavius muscles also insert medially. The clavicular head of the sternocleidomastoid muscle pulls the medial segment superiorly.The lateral segment is pulled inferiorly and medially by the clavicular head of pectoralis major.The shoulder girdle and the weight of the arm exert an inferiorly deforming force on the lateral segment through the acromioclavicular joint and the coracoclavicular ligaments.Fibres of the trapezius also insert into the posterior border of the lateral third of the clavicle, providing a stabilising force against inferior displacement.
3. How would you define nonunion of the clavicle and what is the rate of nonunion with diaphyseal fractures of the clavicle?Non-union of the clavicle is defined as a lack of radiological union by four months. Clinically, this can be assessed by
Fig. 2
Fig. 1

the presence of pain and movement at the fracture site upon stressing. Radiologically, it can be assessed on either radiographs or a CT scan. Radiographs will show a lack of bridging callus, but these may be difficult to interpret due to the difficulty in obtaining orthogonal views. Usually the clavicle is assessed using an AP and 15° to 20° elevated AP view. An apical oblique view may also be useful. Clavicle fractures can also be assessed using an axillary view for the more lateral fractures. A CT scan will give a more reliable diagnosis of non-union. The incidence has been reported to be between 0.13% and 15% for midshaft fractures.In the paper by Robinson et al6 studying 868 clavicle fractures, the reported incidence of non-union in diaphyseal clavicle fractures was 4.5% at 24 weeks post-injury.
4. What are the risk factors for nonunion and which is the most predictive?Robinson et al6 found that following a diaphyseal clavicle fracture, advancing age, female gender, displacement of the fracture, and the presence of comminution significantly increased the risk of non-union. On multivariate analysis, all of these factors remained independently predictive of non-union, and, in their final model, the risk of non-union was increased by lack of cortical apposition.In Robinson’s study a complete fracture displacement was the most predictive of non-union. Other factors that have been found to relate to non-union include shortening > 20mm, displacement > 20 mm, increasing severity of trauma and re-fracture.Other general risk factors for non-union such as co-morbidities, smoking and medications should also be taken into account.7
5. What is the rate of dissatisfaction following these fractures and what are the possible problems with malunion?Hill et al8 found that malunion with shortening of 2 cm or more in a middle third fracture led to a poor symptomatic and functional result. 31% reported unsatisfactory results, including pain and cosmesis.There was also a recognised rate of thoracic outlet syndrome. In a RCT by the Canadian Orthopaedic Trauma Society there was a significantly higher rate of dissatisfaction with the appearance of the shoulder in the non-operative group (47%). This included a “droopy” shoulder, a bump, pain and asymmetry.9
A recent meta-analysis reported symptomatic malunions in 17 of 200 (8.5%) non-operatively treated patients after midshaft fractures of the clavicle.10
In this patient, who works as a bricklayer, one must consider whether he carries heavy loads on the injured shoulder, as a bump from a malunited clavicle fracture may be problematic.
Hands
A 32-year-old pianist who is left-hand dominant presents after a fall from stairs, injuring his left hand. This is his radiograph (Fig. 3a).
1. Describe the radiograph.There is a comminuted intra-articular fracture at the base of the middle phalanx affecting the PIP joint. The fracture affects > 50% of the articular surface and there is subluxation of the joint.
2. What is your diagnosis?Hastings type III unstable dorsal fracture subluxation of the PIPJ. Dorsal dislocations of the PIP joint are often associated with palmar lip fractures and can be classified based on the degree of stability. When instability persists with greater than thirty degrees of flexion at the PIP joint to maintain reduction, the cup shaped geometry of the volar lip of the middle phalanx will need to be reconstructed.The amount of articular surface involvement and the resultant clinically demonstrated instability can be used to group palmar lip PIP fracture dislocations into one of three categories: stable, tenuous, and unstable. Stable fractures involve < 30% of the joint surface and maintain a congruent reduction, throughout the joint excursion. Tenuous fractures will show an involvement of 30 to 50% and are unstable injuries. Unstable injuries are those in which > 50% of the articular surface is involved. Also included in this group are fractures that remain unstable at 30° of flexion.
3. How is this injury assessed?A detailed history and examination is necessary. The history should include hand dominance, profession, hobbies / sports and to what level these are participated in (professional / amateur). The examination should include the neurovascular status of the digit and record any laceration, bruising and areas of tenderness. The alignment (coronal, sagittal and rotational) and swelling of the digit should be noted. Under a digital nerve block the range of movement and subluxation can be assessed. One should also document the status of the tendons FDS, FDP and the central slip, although the latter is more commonly injured in volar PIPJ dislocations. Radiologically the injury is assessed with an AP and true lateral radiograph of the digit. Look for the “V” sign dosally at the PIPJ on the lateral radiograph, which represents subluxation and an incongruent joint.A CT scan may give useful information about the fracture configuration if one is considering an ORIF.
4. What are the options of treatment?The joint is subluxed and incongruent, therefore the aim of treatment is to reduce the joint and hold the reduction to allow healing of the fracture in a favourable position. Early movement is desirable in order to minimise stiffness. The options of treatment are broadly operative or non-operative. Table I lists the various options with pros and cons of each. This particular injury is unstable and affects more than 50% of the joint surface; therefore, extension block splinting is unlikely to be effective. The other treatment options listed here are all possible in this patient.
Treatment Option
Pros Cons
Extension block splinting
Treatment of choice for most < 40% articular surface volar base fractures.
Requires careful assessment of congruence and follow-up, not effective in most > 40% articular surface volar base fractures. With a greater amount of joint surface involved the blocking must begin at a higher angle. May have a residual fixed flexion contracture.
Extension block pinning
Selected volar base fractures that reduce spontaneously with PIP joint flexion.
Pin tract infection.
Fig. 3a
ORIF
Can restore articular congruity and may permit early range of movement.
Stiffness, infection. May not be an option if fracture is comminuted.
Dynamic external fixator
Allows some movement.
Pin tract infection.
Volar plate arthroplasty
Specific strategy for subset of volar base fractures involving between 30-60% of the articular surface.
Numerous specific anatomic requirements must be met for procedure to be effective; surface is not hyaline cartilage.
Osteochondral reconstruction
Bone to bone healing, true hyaline cartilage restoration, recreates volar lip buttress effectively.
Technically complex; graft resorption and collapse are possible.
5. How will you manage this patient?It is important to inform the patient that this is a serious injury and no matter how it is treated, the joint will have significant stiffness and swelling. I would seek advice from a specialist hand surgeon, especially as the patient is a pianist. I would inform the patient that for this injury there is no single treatment option that is proven to give a superior outcome.Stable palmar lip fractures can be treated by early range of motion exercises with buddy taping and protected motion. PIP joint hyperextension should be avoided with the help of extension block splints.Tenuous PIP fracture dislocations can be treated with static splinting but this does not lend itself to early motion. Dorsal extension block splinting (McElfresh) maintains reduction by limiting extension at the PIP joint while allowing for early active flexion. Extension block pinning can also be used to limit extension.In unstable fractures, treatment options include open reduction and internal fixation, palmar plate arthroplasty, external fixation and hemi hamate autograft.Open reduction is suitable for large minimally comminuted palmar lip fractures. Depressed fragments can be elevated and the buttressing effect of the volar lip can be restored.In the presence of extensive comminution a number of traction devices can be used to treat unstable fractures. However these systems in addition to being bulky may fail to restore the volar lip, resulting in recurrent dislocation and post-traumatic arthritis. Eaton in 1980 advanced the palmar plate into the defect after excising the comminuted fragment.Ishida advocated the use of an osteochondral graft to resurface the damaged PIP joint in 1994. Hill Hastings in 1999, noting the similarity in shape of the middle phalanx base and the distal hamate, described the use of a hamate allograft in the treatment of PIP fracture dislocations.A volar approach is used and the joint is “shotgunned” (Fig. 3b). With the fracture prepared (Fig. 3c) the defect is measured and a matching graft is harvested from the distal hamate (Fig. 3d and 3e). This is then fixed to the base of the middle phalanx with screws of adequate length (Fig. 3f).
Further Reading1. Williams RM, Hastings H 2nd, Kiefhaber TR. PIP fracture/dislocation treatment technique: use of a hemi-hamate resurfacing arthroplasty. Tech Hand Up Extrem Surg 2002;6:185-92.2. Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am 2003;28:856-65.
Children’s Orthopaedics
Here are a clinical photograph and lateral radiograph of the spine of a six-year-old girl who is of short stature (Figs 4a and 4b).
1. What is the likely diagnosis and what are the manifestations and aetiology of the condition?The likely diagnosis is Morquio-Brailsford disease (Mucopolysaccharidosis Type IVA), in which deficiency of lyzosomal enzymes required for the degradation of polysaccharides leads to accumulation of Keratan Sulphate and Chondroitin 6 Sulphate.The clinical and radiological manifestations include dwarfism, multiple dysostoses, lumbar lordosis, hip dysplasia, odontoid hypoplasia (Fig. 1b), joint laxity, large elbows and knees (genu valgum is common) and flat feet.
Fig. 4a Fig. 4b
Fig. 3b Fig. 3c
Fig. 3d Fig. 3e
Fig. 3f

This 12-year-old boy is about to undergo an operation because of progressive valgus of the left elbow and early symptoms of ulnar neuritis (Figs 5a and 5b).
2. What is the condition and what operation would you undertake?The diagnosis is nonunion of a minimally displaced fracture of the lateral condyle of the humerus sustained seven years earlier.Flynn11 outlined 3 criteria for surgical treatment of an established nonunion:1. A large metaphyseal fragment2. Displacement of less than 1 cm from the joint surface3. An open, viable lateral condylar physisIt was thought that reconstruction of the elbow was inadvisable because it was unlikely that joint congruency could be restored and major stiffness would ensue.The operation undertaken was a supracondylar closing-wedge osteotomy with transposition of the ulnar nerve.One year later the boy was symptom-free with full movements and the osteotomy had united (Figs 5c, 5d and 5e).
Basic Science
1. While designing a new theatre complex, what are the different zones that one has to bear in mind and why?
Operating theatre zones:An outer, or general access zone for patient reception area and general office.A clean, or limited access zone between the reception bay and theatre suite, and dispersal areas, corridors and staff rest room.Restricted access zone, for those properly clothed personnel engaged in operating theatre activities, including anaesthetic room, utility and “scrub up” rooms.An aseptic operating zone – the operating theatre. This keeps the number of people moving through the operating zone to a minimum, as the bacteriological count is related to the number of persons and their movement. This also allows the operating zone to be separate and to enable control of ventilation, air filtration and temperature, humidity and light.Disposal zone.
2. What are the sources of contamination in an operating theatre?Sources of contamination:Internal; from the patient themselves e.g. the skin of the patient and bacteraemia.External;Airborne pathogens – airborne particles mainly from theatre personnel.Human – theatre personnel, other than airborne pathogens e.g. direct contact or transfer via inanimate object.Instruments / equipment / protheses – both disposable / single use and re-usable.Theatre fixtures and fittings.
3. How is the risk of this contamination reduced?In order to reduce the risk of contamination British Orthopaedic Association guidelines recommend:12
1. The level of sterile precautions required to perform orthopaedic surgery safely are higher than those for surgery involving the bowel, infected body cavities, contaminated wounds and other soft-tissue surgery.2. The following measures must be enforced when material is implanted in bone, major joints are opened or bone is exposed.3. The use of clean air theatres, installed, maintained and checked according to NHS standards is considered essential for orthopaedic surgery.4. All staff in the operating theatre suite, including the anaesthetic room and corridor, must adhere to existing high standards of theatre discipline and follow established procedures which include: -a. All hair to be kept covered at all times.b. Masks to be worn at all times within the operating theatre and lay-up room.c. Street clothes and clothes worn outside the operating theatre suite, including shoes, must not be worn within the theatre suite.d. Staff may only enter or leave the operating theatre through clearly identified doors so that air within the operating theatre is not disturbed needlessly.e. The number of people within the operating theatre must be kept to the minimum required to function safely.f. Traffic from dirty areas and within the lay-up room must be rigidly controlled.g. Drapes and gowns must be made of impervious material. Thin cotton drapes and gowns have no place in orthopaedic surgery.In addition to these guidelines, the use of ultraclean air and prophylactic antibiotics greatly reduces infection rates. Lidwell et al13 in the MRC trial reported the lowest incidence of deep infection (0.06%) was achieved using ultra-clean air, body exhaust systems and prophylactic antibiotics. Further measures to reduce contamination include:14
• Screening and eradication of MRSA• Day of surgery admission onto specific wards
Fig. 5a
Fig. 5c Fig. 5d
Fig. 5e
Fig. 5b

• Body exhaust systems• Double-gloving• Effective surgeon scrubbing and use of skin antiseptics
e.g. Chlorhexidine gluconate 4% • Patient skin preparation with antiseptics• If the operative site is to be shaved, this should be
performed as close to the operation as possible• Equipment cleaning, disinfection and sterilisation• Surgical technique; e.g. shorter operative time
4. What are the types of ventilation system that you are aware of? Describe each in detail.Types of ventilation system;Source of air for ventilation; air is usually taken in at the roof level of the theatre suite. It is drawn by a series of fans through filters capable of removing bacteria carrying particles. It is also humidified and warmed or cooled. High-efficiency particulate air (HEPA) filters are employed. These are capable of filtering particles of 0.5 microns in size with 99.97% efficiency. Generally operating theatres are equipped with positive pressure (plenum) ventilation systems. In this system the pressure inside the theatre is greater than outside. Clean air is fed via wall or ceiling diffusers and let out of vents placed just above floor level. Air also passes out around doors and other openings. The opening of doors and the movement of personnel make this system less efficient. Standard positive pressure ventilated operating theatres deliver around 15 to 25 air changes per hour.Laminar airflow; see answer 5.
5. What do you understand by the term ‘laminar air flow’?Laminar airflow; this involves the entire body of air within a designated space moving with uniform velocity in a single direction along parallel flow lines.There are three main types of theatre airflow:Horizontal laminar flowVertical laminar flowEx-flow or exponential flow (Howorth enclosures)Theatres are usually designed with a vertical downward airflow concept. The flow of air is around 0.3 m/s.Horizontal laminar flow; HEPA filters form a wall, or part of a wall. The positioning of potential objects to the laminar flow is important in order to avoid obstructions (e.g. theatre personnel, image intensifiers).Vertical laminar flow; air is passed through HEPA filters in the ceiling and directed downwards towards the operative field in a vertical direction. The area of HEPA filters on the ceiling is enclosed by panels extending towards the floor (should extend to within 2 m of the floor). Objects such as theatre lights form obstacles and create turbulence. Also, personnel standing under the edge of the enclosure deflect the vertical airflow inwards (peripheral entrainment), also deflecting contaminated air inwards towards the operative site. Ex-flow or exponential flow (Howorth enclosures); this describes the flow of clean air downwards and outwards in the shape of an inverted trumpet. This eliminates the problem of peripheral entrainment. This system is in theory more efficient than laminar flow, and requires fewer changes of air per hour.
6. What is the effect of laminar air flow on the risk of infection in joint replacements?In the MRC trial, Lidwell et al13found that ultra-clean air reduced the risk of deep joint sepsis in arthroplasty by a factor of 2.6 compared with controls. When all groups in the trial were considered together the analysis showed deep sepsis after 63 out of 4133 operations in the control group (1.5%) and after 23 out of 3922 operations in the ultraclean-air groups (0.6%) (Ratio 2.6, 95% confidence limits 1.6-4.2; p < 0.001). Fitzgerald et al15 found the incidence of deep sepsis after 5,865 total hip arthroplasties performed in four centres varied from 0.5% to 2.3%.Procedures performed in a conventional operating room were associated with the highest incidence of deep sepsis (1.3%). The use of a vertical, unidirectional airflow system with a helmet aspirator suite was associated with the lowest incidence of deep sepsis (0.6%).
References1. Goergens ED, McEvoy A, Watson M, Barrett IR. Acute osteomyelitis and septic arthritis in children. J Paediatr Child Health 2005;41:59-62.2. McCarthy JJ, Dormans JP, Kozin SH, Pizzutillo PD. Musculoskeletal infections in children: basic treatment principles and recent advancements. Instr Course Lect 2005;54:515-28.3. Kang SN, Sanghera T, Mangwani J, Paterson JM, Ramachandran M. The management of septic arthritis in children: systematic review of the English language literature. J Bone Joint Surg [Br] 2009;91-B:1127-33.4. Sukeik M, Alshryda S, Haddad FS, Mason JM. Systematic review and meta-analysis of the use of tranexamic acid in total hip replacement. J Bone Joint Surg [Br] 2011;93-B:39-46.5. Alshryda S, Sarda P, Sukeik M, et al. Tranexamic acid in total knee replacement: a systematic review and meta-analysis. J Bone Joint Surg [Br] 2011;93-B:1577-85.6. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg [Am] 2004;86-A:1359-65.7. Gaston MS, Simpson AH. Inhibition of fracture healing. J Bone Joint Surg [Br] 2007;89-B:1553-60.8. Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg [Br] 1997;79-B:537-9.9. No authors listed. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures: a multicenter, randomized clinical trial. J Bone Joint Surg [Am] 2007;89-A:1-10.10. McKee RC, Whelan DB, Schemitsch EH, McKee MD. Operative versus nonoperative care of displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. J Bone Joint Surg [Am] 2012;94-A:675-84.11. Flynn JC. Nonunion of slightly displaced fractures of the lateral humeral condyle in children: an update. J Pediatr Orthop 1989;9:691-6.12. No authors listed. British Orthopaedic Association. Recommendations on sterile procedures in operating theatres, 1999.13. Lidwell OM, Lowbury EJ, Whyte W, et al. Effect of ultraclean air in operating rooms on deep sepsis in the joint after total hip or knee replacement: a randomised study. Br Med J (Clin Res Ed) 1982;285:10-14.14. Hughes SP, Anderson FM. Infection in the operating room. J Bone Joint Surg [Br] 1999;81-B:754-5.15. Fitzgerald RH Jr, Bechtol CO, Eftekhar N, Nelson JP. Reduction of deep sepsis after total hip arthroplasty. Arch Surg 1979;114:803-4.