exercise, carbon dioxide and cystic fibrosis: a pilot study
TRANSCRIPT

Yale UniversityEliScholar – A Digital Platform for Scholarly Publishing at Yale
Yale Medicine Thesis Digital Library School of Medicine
1965
Exercise, carbon dioxide and cystic fibrosis: a pilotstudyMichael Brook MayorYale University
Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl
This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for ScholarlyPublishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A DigitalPlatform for Scholarly Publishing at Yale. For more information, please contact [email protected].
Recommended CitationMayor, Michael Brook, "Exercise, carbon dioxide and cystic fibrosis: a pilot study" (1965). Yale Medicine Thesis Digital Library. 2908.http://elischolar.library.yale.edu/ymtdl/2908

BON DIOXIDE AND S A PILOT STUDY
ROO K M A YOR
■ § s


Digitized by the Internet Archive in 2017 with funding from
The National Endowment for the Humanities and the Arcadia Fund
https://archive.org/details/exercisecarbondiOOmayo


t

EXERCISE, CARBON DIOXIDE
AND CYSTIC FIBROSIS >
A PILOT STUDY
Michael Brook Mayor, BEE.
Yale University, 1959
A thesis submitted to the faculty
of the Yale University School of
Medicine in partial fulfillment
of the requirement for the degree
of Doctor of Medicine.
Department of Pediatrics
Yale University School of Medicine
May 10, 1965

II.
c

ACKNOWLEDGE
My deepest gratitude goes to Dr. Vivian Tappan, without whom this
project would never have been initiated.
I want to extend heartfelt thanks to Dr. Guy Rivard and Katherine
Anlyan for the skill and time invested in the pulmonary function measure¬
ments, and to Dorothy Nixon for her advise and counsel over techniques
and equipment. I am indebted, also, to Dr. Norman S» Talner for the
use of his laboratory and equipment.
The final form of this paper owes a great deal to Joyce Heeley,
Elizabeth Kennard, and Barbara Dinner stein.
This Study was conducted in part under a Public Health Service
Summer Fellowship, PHS 1 SOL FR 05358-01.

«r
t a.
. .
TABLE OF CONTENTS
page
Introduction .1
Materials & Methods .. .. 6
Results . ...... 9
Discussion . 12
Summary & Conclusion.22
Bibliography
Illustrations
follows page
1. Gas Sampling Assembly...7
2. Gas Sampling Assembly.7
3. Gas Collecting Bottle.7
4. Scholander Gas Analyzer . 8
5. Summing Point .. 15
6. Schenatic Diagram .. 15
7. Schenatic Diagram: Respiratory Center.15
8. CO2 1/2 time vs. age. 22
9. CO,_ 1/2 time vs. Classification.22
10. RV/TLC vs. COz 1/2 time. 22
11. RV vs. CO^ time. 22
12. VC vs. CO2 1/2 time .. 22
13. FRC vs. CO^ 1/2 time. 22

o.
s
s o
.
. • jl O c.'iIiC' -
. ! x ax;
1 o
..
.. j • ^
. S J
. s s
s . 1 ‘ vl s
. s
\

INTRODUCTION
- 1
Cystic fibrosis is apparently an inborn error of metabolism with wide-
spread clinical and pathological effects. Its most intimate secrets, of
specific cause and detailed mechanism, are still fast. The flux in concept
of this disease had lead to a lack of definition and uniformity. The bio«
chemical changes in the exocrine glandular system are still speculative
and controversial.
Effects to clarify the genetic characteristics of the disease have lead
to the conclusion that it is probably recessive, and may or may not con¬
form to Mendelian genetic principles. Orzalesi et al, 1963, found no
significant abnormalities in sweat electrolytes, anamesis or pulmonary
function in the parents of children with cystic fibrosis.'*'
The cardio-pulmonary complications of the disease often become the
dominant determinants of its course as those with the disorder grow
2 beyond infancy. Therefore, as the disease progresses, the pulmonary
manifestations assume a critical position in the therapeutic control of
the disease.
The currently available laboratory tests of pulmonary function have not
provided unequivocal indicators of cardio-pulmonary status or of changes
3 4 5 in status 3 3 . In normals, the spirometric measurement of vital
capacity may have a range of values of as much as + 34% . Polgar &
Chernick (op. cit.) found that variations in the longitudinal study of
pulmonary functionwere generally independent of symptoms and therapy
in chronic obstructive lung disease. Cook et al (op. cit.) found the ratio

I. r. ■ i
j si i ox -
I . 3 - I.SO I poloxLJS
.
X o , S.r J5 O ■ - ■ -1
Xfi^tav'3 TSlxxbXXJSl,. OX- C -
. -X-
J i o
j xustio Isoi
- f _ Oi
,1 i JJ o
;jj ?1-. ° '
I 4J t / j g 091 L o O' ' 2i X Bi. iJOXEJ-1-1 oo "
t:.;. t.,„ . i Iqxoxci s1 -1 3C J~:ii Li‘ 00 x-J-,0-!
, ^ t , :ic .x 0..i .. \ • rrx _ i iilo- xoxidjs i- .oi.-x x
j o oil - x ixxio lo ! & nx xioxlonj
j ii; o ■ - . . - ■ ---' -.-•
i Jo OE - SjX 'U o 1. oil’1 j 1 Ml 1 i'X.liO . J'lOi l ' X J X X
< .... - j xxc d t
I ■ i. i o x i j 'x xi' i Jx; - . ii d.-x
. c. i i •
lo O _i ll jC£f X J I ■ j
m o lx., i io r. ■j j J. Ouj i J -til. -j '1 1 S’ ’>■ l-1 -1 l!
X j < is '1--OJ . ■' J 1 ■'
. -
( • jL *
(. . . . - "
of RV/TLC in patients with cystic fibrosis to have the best statistical
correlation with their clinical rating system. Mitchell et a], 1964,
analysed factors influencing prognosis in chronic obstructive broncho-
pulmonary disease . They found the RV/TLC of only "slight influence"
in predicting or correlating with mortality and disability.
In addition, significant changes occur in the performance of any
given individual on spirometric testing as a result of learning effect.
The same can be said of the values obtained by different technicians
testing the same individual, even with correction for the learning effect.
Pulmonary function testing, though a product and a tool of the science,
must constantly be interpreted with due regard for the art of the tester
and the degree of cooperation of the subject.
The purpose of this inquiry, then, is to design and evaluate a test of
cardio-pulmonary function which might provide a more sensitive measure
than current methods.
Considerable effort has been spent in an attempt to define the basic
pathophysiology of cystic fibrosis. The alterations of exocrine glandular
secretions are widespread, whatever their site of secretion in the bodies
of these patients. Certain complications of the disease can reasonably
be explained on the basis of the marked increase in the viscosity of these
secretions. These include: pancreatic enzymatic insufficiency secondary
to obstruction of the pancreatic ductules; focal biliary cirrhosis secondar
to intrahepatic biliary obstruction; recurrent pulmonary small-airway
obstruction and peri-bronchiolar inflammatory reaction, leading to
j _ i i'v - s \
- -
•xrlo ni sxaoirgotq ;r;i: n i.xi ‘xx o o l.-t- •- • J ■ -
i ; Jj OX L 1.
. J J l -
o \ r J r / ■- •
i niisl oo niloib'siq ni
. i oc ' -. i.U x <•---■ -•
_ \ . . - j — x rrxoiiqs c isx/bxvi bni
j j. .1. . o i ’ xijso . n.
OX ijf '.V O tir.j - - ni
iOo '5 . c ^ x. x ox - j . ■*- o- J-
A . ... ! .'a v-'- ~ Xi-'O -
o xxoi ixj oo: o
i , , £
. ]j >i ■ : :>c
. .. A X J - J~
n x i J-. qs xi
X
x.;. i jx.- jii ii o
.i o . v 11 i i:x v ... _ . i r>
IJ li'tx i
^ .•.!• c ‘ . • . jj 3i. Ji
_ . . j xi o
j -'-i .. x 1bIt
X J . ! . J O . - l • .
i l i: x .x g j , Jx -• <- i
_ i , j O -t J xui - X
, Ci I4 i - ij i i:c j- ci : * c,cfo

- 3
atelectasis and recurrent pulmonary infection. In the older age group,
the cardio-pulmonary problems usually far outweigh the digestive dif¬
ficulties.
The airway obstruction, inflammation and recurrent infection may
produce pulmonary hypertension and cor pulmonale and widespread des-
g
truction of lung tissue . The consensus of those studying pulmonary
function in cystic fibrosis is that there is no change in the total lung
capacity. There is a volumetric and dynamic picture consistent with
widespread airway obstruction, greater in expiration than inspiration.
A prominent early characteristic of pulmonary involvement is
9 atelectasis, which involves the right lung almost exclusively . The
net result is a loss of the normal distribution and mixing of inspired
air^. However, there is often no consequent change in the blood gas
values for CO^ and O^.
From the preceding, it comes apparent that cystic fibrosis is marked
by frequent exacerbations in the pulmonary arena, characterized early
by acute diffuse small airway obstruction, peri-bronchiolar inflammation,
bronchiolar thickening, early fibrosis and recurrent infection. Pro¬
gression and chronicity bring further fibrosis, emphysema, and inter¬
mittent hypoxemia with pulmonary hypertension. Hypercapnea and res¬
piratory acidosis, with and without compensation or complications, and
right heart failure may mark the disease.
All of the above pathological consequences could be prevented if
effective means could be found to bring the physical properties of the

.
o - ‘ •
» - i. i :
j * i 0. *;r i -XJ-i <ixi ■< ' D
j X . ... il > fcn£ xtoisneJ-iiX.-v/jd (i£ c Ii pu&t
^jl : > j O- ii . i rox ..
-
, j . i o j j ^ i t 1 -•. -1 ado y is
i io . xjg x _ ~ _ i ' j Jo£ - . nommoiq
_ j. _ . ' ri,. i i - j : < i x j-
i o l.‘x ■ -iXi,J ■ j 1 . . xi x'jj io eaol £. 1 J. i ■ • n
i c
, ... O c "i
' . o t . 1 .
_ i J' < . .i •. x - j - 1 x1.
- _ . C . - . s J
. j •, . , j x jo t xx • - i" . •u;J. i:ic •
, U t X C X X ■ J ; JTx 1 i . xXt IVO X . Xioi - .
ixt, .riuD ’co xxgx x>'
• 'O'. ■ xGG X I .<'
^XVX.C. Jb • j; uJi '/• x-,.-...- O' j V JXi . ;•
_-u r, u x . , i iOjj _ .'J ' . ..
♦oessei sra \&
; x oo Is x i : vu js r .1 tc il
3XJ •. .Io ■ riJ xii [ oi xxoi (f bli og

4
viscid secretions back to normal. Many forms of therapy directed
toward this end have been deviseds on the basis of the in vitro charac«
teristics of these secretions. Their therapeutic efficiency can finally
be judged only by in vivo demonstration of effectiveness. The need for
techniques that can dependably measure changes produced by the disease
and changes produced by therapy is obvious.
Procedures for the evaluation of cardio-pulmonary function have pro¬
liferated as a result. Many of these are very precise; yet all have
their limitations. Measurement of carbon dioxide or oxygen in exhaled
air or arterial blood can be very accurately performed. Frequently,
the values in the resting state are entirely within normal limits in the
face of significant disease. The discomfort and complications attendant
on arterial puncture pose additional problems. An oxygen equilibration
3 index, devised by Demuth et al , 1962, produced too many false positives.
The complicated interplay of cardiac and pulmonary and other factors,
compensatory change in one area balancing destructive change in another,
makes the interpretation of values obtained at rest difficult and at times
misleading.
With due regard for the dangers of over-simplification, two broad
categories emerge:
1. Parameters measurably effected by disease, which are, also,
significantly influenced by factors unrelated to disease; ie., those re¬
quiring maximum patient cooperation in their measurement.
2. Parameters subject to tight homeostatic control. Compensatory
M C . • . c »i jt o s tioi '■ :
3 Uili i i 5 o <
ioi oimoqxs-rs i - ' -enci o - - : -:
.
v i rLi r»(ij.'
■£/ J.J..
; j vcr IffC i. <hsj t ••
It. . qo , . . 3 xiJ a >sj[ h xL- j
.; j,o.. - < o x ' i../ ;<'• fO • x - - xi •
- j ,/ j-toi »V -
.5 ... o j.. . I. i r. i‘J
, C j3- 3 • U . j . J2 . ii
O’ 1 OO.R '(VfV XK JU - OO It. 1.311 O J'J 3 3 U
- j i
. it. . i f ( 3 . O ^ ^ J « 13 J i 1 ^ u . ■' 3 ^ x..
Its ill . ... j. i >«oq s 3 i . ■
3 , «H (i _ ' v. ' t ' ' X
O O. Ij > ; - ■ ••: 3 _j-i )j/ x j • ill.,, x- . tiT
, z _• i • vl ' i - X cl 3 1 xx.- --G or i 1 3 - . 0- 3XI3C XXOO
i 3j i 18 -t - „ . i . 3 8 . .nljJ X C X. x - x .. J :
. j; i 3 1 ■- i X x
t J ,,._ j j. . ,t — * ^
I AX - V D
tU ' iJ , X 1 t 3 X 3 1 X J ’ * - J * -
, . i ; o . J - ••1 x
, i < . I;xX..... ’ i ' i a O )j ' •-• 3 1 x C i i -X- OH . X
.1 .03 J x ' j 3> Jj

- 5
mechanisms, cardio-pulmonary, biochemical etc., keep these parameter s
within the normal range at rest. This is particularly true of carbon
dioxide values; arterial, venous, and alveolar.
These conditions prompted a search for a test of cardio-pulmonary
function which would accurately reflect the dynamic capacities of the
system.
A number of factors led to the study of the profile of CO^ output from
the lungs in response to exercise. One of the primary functions of the
cardio-pulmonary circuit is to maintain physiologic levels of carbon
dioxide in the circulating blood. The gradient for oxygen is from with¬
out inward; that for carbon dioxide the reverse, since almost all of
it arises from endogenous metabolic processes. The amount of CO^ to
be disposed of by the lungs can be increased by increasing the rate of some
of these metabolic processes. The increased muscular activity of exer¬
cise is one of the most physiological means for achieving such an increase.
This study was based on the assumption that elimination of CO^ by
the lungs, if followed from rest, through moderate exercise, to equili¬
brium following exercise, might show a time course significantly dif¬
ferent from the normal in patients with lung damage due to cystic fibrosis.
The advantages, in addition to those enumerated above, were: an ex¬
perimental protocol involving little patient discomfort, abundant material
in exhaled gas for analysis, and accurate and proven methods for measure¬
ment of gaseous CO^.

t . 1 < - -l <
sltoi i ■ i . ■ • - i
r ^ - t J-1 ^ ■
• 1 iq anoMxLn-oo
-l
.
- r
u i ,s> a xo : a: i 1 . i fii jch-'J
' ' I
o t 1 , . . booJ _ru sbxxoi
. ■ i. , ,, i . X J { - -( ■->
i m c e i
j_ j 0 I v 0 < -
. O'. . G .' t . J
..j j.i r ", ... i_, jj C- - .< ’2 r : tj -C iJ.o ' i io
t o t -v -. i i < i i
i ; • ■ X 1 ... . j GJL. ■' ' x
ji...' i.j l . i j j . j . i_ j\i i .'Xi. ;uO > . j S'l i
j J ■ . ■ . G j j < b O
t i X j ,b J 1 / X . J • i ; . X a
... X X £ * . j- ^. ■ i j
. . O O i l.

MATERIALS AND METHODS
The experimental protocol described below was designed entirely by
the author, with the exception of the Scholander gas analysis of CO^
and
The patients participating in this study were drawn from the popu-
lation of cystic fibrosis patients under care of Dr. Vivian Tappan and
the Chest Metabolic Clinic of the Yale-New Haven Community Hospital.
They were fourteen in number, seven males from 5 —11/ 1Z to 16-5/12
years of age and seven females from 6-0/12 to 23-1/12 years of age.
Of the control group two were siblings of patients in the test, one
a 15-7/12 year old female, (B.L.), the other a 10-1/12 year old male
(D,Mt). The other four were volunteers drawn from among the pre¬
operative admissions to the Yale-New Haven Ear , Nose, and Throat
service for elective tonsil-adenoidectomies. Except for the hypertrophi
lymphoid tissue bringing them to operation they were entirely well. All
of the subjects tested had been going to school or working and came to
testing directly from their usual activities.
Each subject rested in the laboratory for at least fifteen minutes be¬
fore the first minute volume of exhaled air was collected.
The equipment used in the performance of this study was as follows:
Lanooy hyperbolic bicycle ergometer, 0-200/400 Watts
One-way 1J1 valve, 1" ID
British cloth-covered corrugated tubing, 7", 1" ID
Rubber mouth-piece & sponge-rubber nose clamp

x-xoasb Xoooio'iq -
O l1 —' i L . _ -X * -k- O i J
.
3i i i . • qxoi . -9 . ‘ ; ■
.
_ .. .x^ ~ - ■ ■
< - - .
_ _ Oj il\x-C - 1. briB t - -
i £, o s ■ i . i
A . - « X i <- - -X - -\ ~ A
- x o c. ...
- ' GXriai X
i ic i - ~j-: : i . - . i
-
1
j o I i ., i .. - i ni
ii, : j : X 7 t jxrrxrrx
\ S- < fuj Ic : lied c/t ocn
I i ( J 11 ~
: , 1 , . ' . J i ■■ ■■■>': - C ~i. .i. J i
I 1 - J - - SJO

7
Aluminum "T" shape stop-cock, 3-way tap, 3/4" ID
Neoprene latex meteorological balloons, 30 L capacity
Precision Wet Test gas meter. Precision Sci. Co., 3L/rev.
Gas collecting tubes, glass, 125 ml
Gas sampling assembly, see fig. 1_
Scholander gas analyser
Each subject was an hour or more post prandial. Each was instructed
carefully in the techniques to be employed in the test. For each minute
volume collected in the meteorological balloon, the nose clip was placed,
the mouthpiece adjusted airtight, and the patient allowed fifteen to thirty
seconds to wash out the efferent limb of the system. The three way tap
on the stopcock was then turned to conduct the exhaled air into a
previously wrung-out balloon. After the lapse of exactly one minute,
the stopcock was returned to its initial position and the neck of the
balloon was clamped with a rubber shielded Kelly clamp.
Within ten minutes of its collection, three litres of sample were fed
through the wet test meter via the special connector (fig. 2) filling the con¬
nector with sample. The rubber section was clamped and disconnected
from the meter. The vaccine bottle stopper was driven down over the
nercury-filled sampling needle (fig. 3) and 150 ml of sample gas was
admitted to the glass collecting bottle as the mercury was drained from
it. The collecting bottle stopcocks were closed, the lower first and then
the upper, to ensure that no pressure gradient existed with room air.

_ - . q£xi 1 . A.
-
<
t ... x.'j . slloo r.£ >
t .
ij_nj - to. oxxxsIcxioC
.
t i ; .~o.. . i .
, ■-
j o" bs-n-cx/j xioxll a£V/ >.oooqo:ia 9x1 ‘ no
_ . toil: - - ■ '±
.
c .
.
c 0‘,n
.
( . ... X Hi - O ' -.
t •: . i i iJ o . b

Fig. 1: gas sampling assembly; exploded view
Fig 2: Sampling Assembly; note vacuum bottle stopper
jar


Fig. 3: Glass Collecting Bottle with Sampling Needle

- 8
The connector was lifted off the needle* returned to the wet test meter,
and the remaining gas volume was measured. This procedure was
used for all of the six gas samples taken from each subject.
Precautions were taken to prevent loss of sample volume and contam«
ination with room air, including periodic tests of the integrity of the
balloons.
Minute volume samples were taken from the subjects as follows:
1: at rest, after ten to fifteen minutes sitting quietly in the
laboratory.
2: during the last minute of a six minute period of moderate exercise
the work load being judged according to the capacities of each
subj ect.
3: during the minute immediately following cessation of exercise.
4, 5, & 6: during the one minute intevals beginning 3, 7, and 19
minutes respectively following the cessation of exercise.
The six samples thus obtained were analysed from their gas collecting
bottles on the same day. Using the transfer pipette and the Scholander
gas analyser apparatus’^, (fig- 4), the percent concentration of COg
and C>2 of each sample was measured, and the minute volume of COg cal¬
culated.

t i iJ to: > ■
rxxulc iixij 1
.f, - ii a -- i.- .£,J ' 11'-33 it ‘ • O II £ lo'±
loots 0 3 I I /oiq olj i -
i>i jd oi - ---‘t oc - ■ - -
. . OLU o'
it:o - co ; - - lov uni -
i . , 1 i o i ' ‘ I
. r u . ' . O : - i
j u x. . £.1 tti - :
oo.' r, - , f ' £oI Aio\ orli
. O ^ i d.
- '■
, o i _ . i j ■ 1- .i -
j io lylcrus cow Jj i£ c ...r i oiq.is
qi ( i ,y£b - •
. l x . .1 < 3trio £qqjs X3f ,1 li t £
t - -
I -
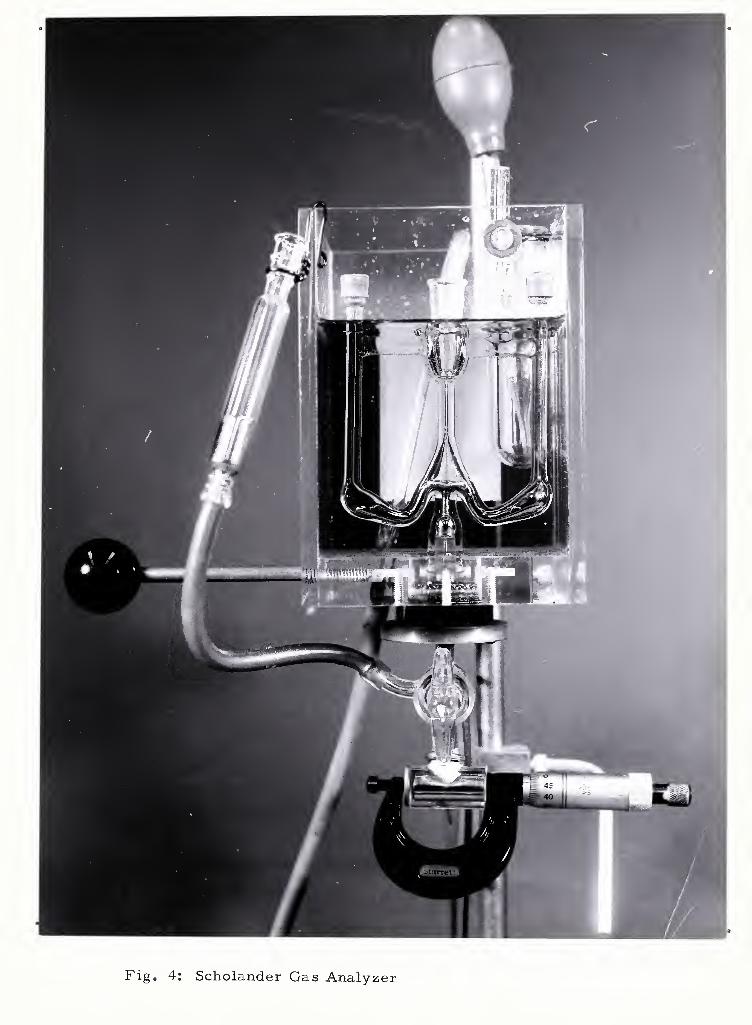
Fig. 4: Scholander Gas Analyzer

RESULTS
- 9
The protocol described above provided six values of CO^ output in
ml/min. for each subject. These values were processed to determine
e
the time in minutes required for the V to fall to halfway between
° • the steady state V of exercise and the average resting V
y co2 co2
This time determination was made graphically on semilogarithmic
ruled paper. V was plotted logarithmically on the ordinate, and coZ
the midpoint in time of the minute during which the C02 was collected
«
served as the abscissa coordinate. Three values of V were en» coz
teredo One, collected during minute 5 to minute 6 of exercise, is
the steady state value referred to above. The second is from the
minute volume collected immediately following exercise. The third
is from the minute volume collected next in sequence. This was usually
obtained starting three minutes after cessation of exercise. A best**
fitting straight line was drawn with these three values, plotted on semi-
o
logarithmic ruled paper. The resting V is the average of the minute coz
volume collected before exercise and that collected 19 minutes after
o
exercise. The V used to determine the 1/2 time was the average of
C°2 • •
the steady state exercise V and the resting V , and the 1/2 time co2 co2
was read as the time at which the best«fitting straight line defined
o
above crossed the 1/2 time V co2
It was noted that the raw real CC>2 1/2 time tended to increase with
age, necessitating some correction. In order to make the results of
testing individuals of different ages comparable, the real CO^ 1/2 times

. L' - . . i
, _j - 1 J-
o 9 j.io>qbi
c
lit o K x
i 1- -- jaxaxrix IJ otIov
ri;/ ic r
i t ido
£ C J
r iiO J • iiii'It V
■ i > . v.i • i- ■ -L • 1 bsct O0Y c:. .'ti : -i,
- , .. .,; .
, s \x „ j -■ ox
. i . . j . o • . ; • - j <
t 8-l.si/biv.rbni gniJs

10-
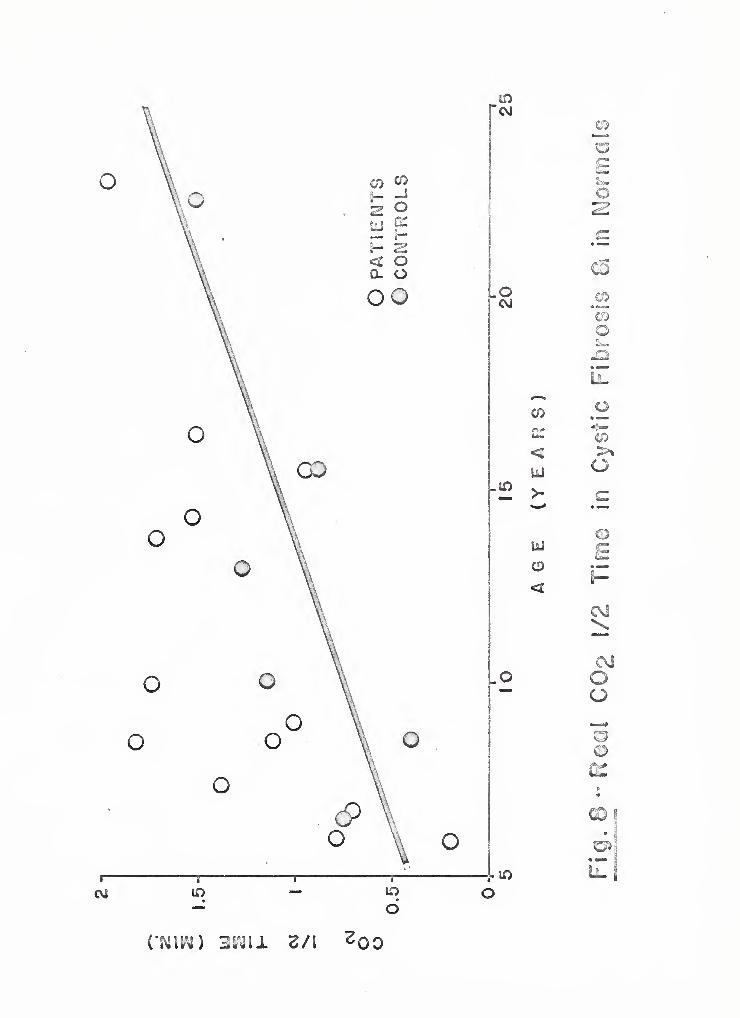
determined for the normal subjects were plotted versus age to the
nearest month. A regression line was estimated and laid on the plot.
Only after this was completed were the points representing the patients
studied also plotted, as shown in fig. 8.
The regression line so determined was used to determine the pre¬
dicted CO2 1/2 time. For all the cystic fibrosis patients, the real
1/2 time, experimentally determined, and the predicted 1/2 time for
a patient of that age, taken from the regression line, were compared
yielding the % predicted 1/2 time for each patient.
A more refined analysis of the effects of exercise would have to
establish a more rigid relationship between age and exercise load. A
plot of 1/2 time versus exercise load was tried and did not appear to
offer significant advantages.
One of the patients studied (M. L.) could not be exercised except at
the lightest of exercise loads available (10 Kw). Her CO^ response curve
was so flat that her 1/2 time could not be determined with accuracy and
she was omitted from the study. All of the other patients and all of the
normal volunteers are included in the results.
In order to test the validity of the CO^ 1/2 time as an objective
measurement, it was compared with several other available methods
of evaluation.
The first of these is shown in fig. 9. A medically qualified observer
(V.T.) with intimate and long-term aquaintance with each of the patients
sorted each of the thirteen into one of three classes. These classes

'a ii>rniof. ■ toi bs>f;irn*i--it»b
rnorr a • iso
< iJ
< -L':
( • ji
U • . .1 \J
. < s\-
, < ?. u
. \I • i-i .. xii
i
.... S \ . Jo I
, i o
.
.
rtij S\j i9rf Jj3»;j lell oe
.
■ _ic : i j l. : rru/io f i >. •• i
j o /j . ! -V J '• . j I
C
, Ol X'i.
ol hr
O d
J ( .
o

formulated on the basis of overall capacities for physical activity. In
class I were all those patients with no discernable difference from the
normal population in their reaction to physical activity. Class II con¬
tained those known to have minimal limitation} or slight dyspnea on
strenuous activity. In class III were those with moderate to severe
limitation, dyspneic on restricted activity. Fig. 9 shows a plot of the %
predicted l/Z time for each of the four groups: six controls, six
patients in class I, four in class II, and three in class III. The patient
omitted (M.L.) fell in class III. The small numbers ajoining each
point correspond to the kilowatt exercise load each individual sustained.
Comparisons were, also, made between the % predicted l/Z time
and several pulmonary function parameters. These were: RV/TLC
(fig. 10), RV (fig. 11), VC (fig. 1Z), and FRC (fig. 13). All were ex¬
pressed in terms of % of predicted value for those between age 5 and
4Z age 17, using the data of Helliesen et al . The two individuals over
17 years of age (C„ McM, a patient, and B.D., a control) were plotted
relative to the normal values for the adult cardiopulmonary laboratory
at this center.
The broken lines on figs. 9 through 13 represent the 100% levels
for the ordinate and ascissa where appropriate, to facilitate interpretation.
The units used to indicate work load are written Kw . These units
are unique to the Lanooy ergometer. They are not equivalent to
kilowatts.
. . ~ i
J G X j £,
■ i - -l
. -• '
u
It. sc exit no ot fjel^rmo'
.
txsj j oxifilifcjocj J. sin ion
V III a&J5jLo ill .'(-ivijOB -J.'C.
x : tj - i
o i o U
, < , —j . j
i rii JJ ( . .
wo-Efoi sxIj oj Jbxxoqe&'t'ioo '/.icq
c O . i t V/ iXIC •• X j iT-O
j. Ix ■ I ..
, . . r /II . ' t( _i i
x
i .ill - ■ , Ci j - j i i
t r j 3 < < i . o ' i
o . • .. Is o ‘ t o .• Xsi
. X r .X 3 bii
1 O 0
i. - • .L - brie iBnio io s x!j xot
-
.

12 -
DISCUSSION
In discussing the findings of this exercise study it may be useful to
set them against the backdrop of some of the general and specific in¬
formation available about ventilation, CC>2 output, intake and
exertion.
Foremost among the functions of the cardio-pulmonary unit are the
maintenance of physiologic levels of oxygen, carbon dioxide and hydrogen
ion concentration. In a normal young male oxygen intake is about 250 ml,
CC>2 output is approximately 200 ml for a respiratory quotient of 0.8.
In the face of severe stress, his intake may increase up to 22 times,
and his CO^ output as much as fifty times these levels. Functional
reserve of this magnitude makes it possible to maintain normal resting
values of Pq and Pqq^ i-n the arterial blood in spite of severe lung
damage due to disease. For this reason, many authors have studied
patients under some form of stress, hoping to delineate the extent of
damage more accurately.
Consideration of these studies may be facilitated by review of some of
the factors involved.
Acute hypoxia stimulates respiration only via the carotid and aortic
chemoreceptors. Hypoxia without hypercapnia will not stimulate respir¬
ation until the F^ drops to less than 14%, corresponding to an arterial
°2
Pq of less than 60 mm Hg. This is less true with chronic hypoxia.
Hypercapnia stimulates respiration both via the chemoreceptors
and acting directly on the respiratory center. Any rise in the F
TO,

: P-1 " J
i. . t i i - - r;x?.ej ax ja]
i i „ a: ■ rJ i.xxica .«_• qt'-J-»lax;d oxli uj ju - rl Pa
t < i j
j
r:cx j-. O i.j j • r.: ■ ■ < i. * / , i: -. i. . -: 'i i - - O
i < ( i I oi j i ; Iq < - . j . ■ £ fJBX
c » ~j ■ j
. . ^ .. . . f tirqSj/o q
j - . i j , : I < ■. jo -j.b < j'j
v * 1 . i - imiJ vcHil a ti rioirca bjs Si • ^ D aid
a] , 1 x j" - - i Bxn sbxrJii ax > a n
... j o • iv . ' col I si up t 5 ti i - ■- c.: ..j;xb /'.tj <■» aox/Ijsv
1 . 4 5 1 O . BP. r i O JJ
. • j < . ft . o * oa s. r; c:. / ‘ i
. /I r xi - > c-'i >ia b . B
■ i i s . i b t>: e . < . j ; P. -
.i. j u
: - i r i i j , i ; ■ . Xj rxtuJc i >< { t a ua -
^ . ■: . .. . ■ i
d _ < i. r'B c ; 1 oJ 3Cfo Ixlaxr nox
LiJ i: / ; i )
11J ■ i f r ;• d nci b it 3 *x a.* J.-dr ...i inc;Bo'X‘,q\!:
rl3 no vl io *xx : nxJo

- 13
produces a nearly linear rise in ventilation.
The inter-relationships of the 02 and C02 levels on the stimulation
of respiration are recognized but not clearly defined. Lowering the
Pq^ of the blood enchances the response to any given an<5 increases
12 the sensitivity of the respiratory center to CO^ . The respiratory
center is also sensitive to H+ concentration. The effect of CO^ may
depend on the subsequent formation of carbonic acid with the release of
+ H .
Additional studies have compared the P„„ sensitivity of adults and
13 14 infants , the capacity of man to store CO^ on an acute basis , and the
15 change in pH of the blood when the whole body is titrated with C02
The results of these inquiries have leant support to current concepts
of ventilatory chemistry,, have served to clarify and extend them, and
have provided some quantitative tools for their application. Their short¬
coming has been their failure to provide clear and precise exposition of
basic functional interrelationships.
Studies performed on man at rest have been more successful in this
regard than studies on man exercising. One difficulty has been in identifying
the specific mechanisms leading to the linear increase in ventilatory
volume at increasing levels of external work. This increase is linear
over a limited range; ie. , not exceeding 70% of the maximum six minute
work level of which the particular subject is capable^. Measurement
of arterial lactic acid, Pq^, ^CO an<^ c-*-ear^y eliminate these
parameters from any measure of control in exercise. Within 30% of

x i *iX ^6 wbotc
-
rl ^ i: fci :s, I f: . ixi^ccL.-- •: j.g noi >‘je. iqe 't io
j . . ■■■ c : - j
; j _ ./•;. .S', it .. -i r'1 / fi jT.ii.gfI3 cl ‘ -fU
j . j i j . ‘ . lj . i
j . o . iol I • ' ■ rii no bflstj
si£i io: rsi i -1 s Ibi iii
Li • . l g j < •*
| j ’ .i 7 Of) 1 i . i . '1 1 ' -I' G f •>• ' • f- X • Jj ■ ..
£xjo t-3 i'X « qxia tnjs , ■ s t a iih pxii a* dl 3 I* ® •• j 1
i X. . ; J3 I _ ’ • . slxixi&v
j i . Io o rd - . cio« i >
j. i i mi - j Ii js - i c 8 jsx gxrixxxo :
, . jj. . j j. i.;.' - ~ j i
JfflflD I -•■■■■ i - 1
, . j j . ■ i. 3 i . ■ ' ■ U ’ o ;
ni * . ■ ... x jiijBx xti oiixc
i . V J. , J. - i •
, . ; • irrtii
,
t ( iL

-14-
this maximum work level, rises in lactic acid and H concentration
17 contribute to but do not supplant the basic stimulus to hyperpnea „
The ventilatory responses so easily demonstrable when exogenous
18 CO;? is used are not cut of the same cloth as the ventilatory responses
to exercise,, Much work in this field has been directed toward isolating
a servomechanistic loop seeking a homeostatic set point. This wo rk
has been given added impetus by the demonstrated constancy of the
arterial P , and by the fact that manipulation of the P„„ , P,~ , C02 UUZ u2
and pH give rise to activity that tends to restore these values toward
normal. Perhaps Occam's razor has been applied here to aggressively.
It seems realistic to accept two modes of operation for the respiratory
center. One seems devoted to regulating the parameters to which de¬
tectors in the system are sensitive. The other is seemingly a higher
order of function predicated on the unique capacities made available
by the collective organized function of aggregations of nerve cells.
One of these aggregations, the respiratory center, seems to be so
organized that it responds to muscular activity, among other things,
and its response is such that significant change in the variables dependent
on ventilation are prevented. Some of the tools of the discipline of
electronic servomechanisms might be applied here with some profit. The
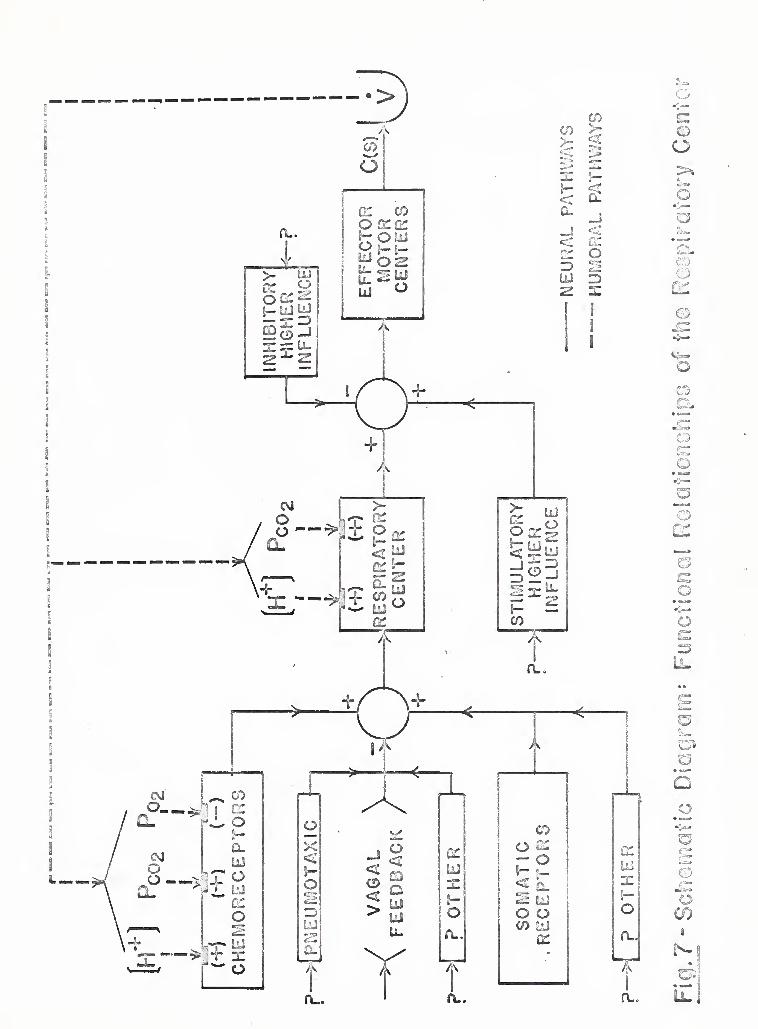
diagram showin in fig. 7 is such an application. Before elaborating on
this diagram some of the limitations imposed on formulating it must be
pointed out and emphasized.

oil i o iiu i eiifcl ±. u Z t X_ _ j — xjJ. -
c c> ^j-rd •■ jx- .ttrc j
o / <5f
OJL
-
. O __ i j i -- . J w W
,
3XIOX - /Cl X - •. - J i - ..
; cm ii ox»j « JLsj
c : l O'- x J j ■ j /,i /i-JOf. oi £<.i • evx, .'.as
vj __ 1 _ O ,1j. Cl
- -
w i O .' ^ l
o . i./ . i.I
a x ^ . ,i q j . c
i.C- O -- .. ii- . .1 _ ' ijLvi- ^
t 1 - U JS i x. i ( - ±‘ ~ J ‘ _ r OX
j _ i j . i>} 8 ■ 1 X tjE O
xi - J i i i 31 1 ’JS'.Oi X .t.
.... -
i. o mx smeii ... &e oiuo o ;
.> x. . . . 1 c J
.
. L'Xl'i i x . O .CO'

- 15
This diagram must not be interpreted as a direct translation of
the function of the respiratory center into electronic circuitry. Only
the vocabulary and symbols are to be applied, not the electronics.
Any quantitative behavior implied is intended only as a gross approx¬
imation.
This diagram is recognizably only a very crude approximation of the
components and functioning of the human respiratory system. It is
intended as a rough sketch of a very complex pattern that is at present
only dimly perceived. It is hoped that this approach will lend clearer
insights and raise clearly defined questions. Perhaps further work can
then be applied to elaborating and refining this representation to make
it even more useful.
Certain basic definitions are necessary before the diagram itself
can be discussed.
Figure 5 shows a summing point represented as an open circle. The
solid lines with directional arrows represent neural pathways. A, B,
C ....... are inputs to the summing point which act upon it, as indicated
by the associated algebraic sign, so as to produce the actuating signal
E (s) = A + B - C ............ As was pointed out above, this "sum"
should be seen as indicative of direction of effect, not as a precise,
algebraic result.
Fig. 6^ presents functional neuronal groups to visualize their response
to certain of the influences impinging on them. Increasing or decreasing
E (s) will produce an increase or decrease, respectively, in C (s), the
j .. o ■- : m xxxxsig tii aMri
-
. oi jo., i
^ k_i. O V'l xxjgoo 8 x xx
rex . J. v. . o . r.ix?.OJjxrtu) x;.i ■ loqmoo
o .. .Jo 8 - i w s.
- - - •.
. bXlGXtS - - 91- - - - xi '1
j . j . - - --
, i. _ JJ OXli ... o 9
j .. _ - -
O 9 i £1
t t . _ no ... .. i • nil biio
I o •- . . - . .
, .. . . - -90 £ .
.. •
•j < - O o. - i O - J i XI9 ^
, > - i - 1 •
_ • ■*
: x.I . j j. j ri,f. . .. i ?l 1' ni ■Ji.'.- o x.ijj - Oj
H t . .6 u : £;..~ 9. X . x - Ill

c o
«&- o
o !«• D> o> < a
■8—
_
a © dl o
• MB © «c— ——•
o tflj c
—
Ll. o tia»
8 fc» ■'
CD i 1 Q |z
o» © teas* i*s- Ll. I 1 O
*
CO
2
o <—
© o
m o
L-l
©
•w—•
o
m r^z
o <?*» 4Ks)
o
o
c» Qt
3
.2 b ©
CO a
h-
iZ


~ 16 ~
controlled variable. Nothing more than that is implied. The dotted
lines with directional arrows indicate non«neural, humoral pathways.
M, N, P o . represent measurable humoral parameters, and
their site of action on the "transducer neurons" of the nervous system
is indicated by the dark bars, and the algebraic signs beneath each
indicates the direction of effect on C (s) produced by increasing M, N,
P, etc.
Having thus defined the basic vocabulary, the respiratory center
can be diagrammed with its important functional relationships, as in
Fig. 7. Only those pathways particularly pertinent to respiration
and physical work have been made explicit. Additional factors, known
and unknown, are acknowledged but not elaborated.
Using this diagram, it becomes easy to point out that the motor nerve
activity C (s) which drives the muscles of respiration to produce a given
Q
ventilation, V, is the result of a multitude of controlling factors. The
interplay of these factors is well described by the diagram to support
the contention that it is unnecessary to insist that a humoral factor be
the principle regulator of respiration in exertion.
However, it has been very difficult to accept that the oxygen and carbon
dioxide levels in the milieu interne might have no controlling influence on
respiration during exercise. Since the cardinal function of respiration is
to acquire oxygen and dispose of carbon dioxide, it would be very rash
to propose some completely unrelated mechanism to regulate respiration
without first searching for some role for carbon dioxide and/or oxygen.
Obviously, it is important to search for humoral factors which may
. .
-X_ r_i o os J
. • * <.
i 1 rxc oi Jojb to 9 j
it . J ; ...Jt t £■ ■ Yc 'x *
< ( no )dcj o xioxJdsi xb . soibx
t oc oi - xij xix niv£
- -
xX . .
j-i. • . • ,d o Ieoh. c. hi
-i 5 - *
o t • .
vxnb fioirfvv (a) D "<{ixviiD£
i < ' < x.
x--.'.. Xi; X • ' c o.s'1 a oxii io vriq-iSJUi
x - 'i Xbx nox :xj TiOD rL'
O x 3 CX . - V’ OH
. i X l . is .1 -Oi
. x , - - .x . oi. o
i , £i i u ‘; c x. rx xi- yj o u
o o
J L. L *_• \' »: 'j II r O .i
* y J. - l i •' o o

- 17 -
effect changes in respiration, and which may act at any point of influence.
Thus, it has been demonstrated that raising the hydrogen ion con¬
centration or the P„„ will increase the output of the respiratory center co2
19 by direct effect . It has been shown that the aortic and carotid chemo-
20 receptors are sensitive to pH, P__ , and P . The feedback loop co2 <J2
o
from V is closed via these sensors.
However, it may now be timely to formulate and investigate more
fully the alternative pathways for stimulation of respiration.
The many investigations already reported would seem to point to a
capacity built in to the system, whose characteristics enable an anti¬
cipatory adjustment of ventilation to prevent any change in oxygen
or carbon dioxide levels in the circulating blood. Such an extraordinary
wisdom cannot be asserted for the body without careful and difficult
investigation. It does seem timely to propose it, and to employ the cd n~ t.
cepts and vocabulary of electronic technology more extensively in in¬
vestigating it.
W.O. Fenn has speculated on this mode of operation for the respiratory
center in the face of exercise, calling it a 5behavioristic approach1 to
21 its function . None of this speculation should be construed as minimizing
the importance of the chemosensitive mechanisms in homeostasis. In
the face of exercise in the intact animal and man these simpler chemical
22 23 24 25 drives seem not to play a dominant role in regulating respiration 5 3 *
A few other details pertinent to humans in exercise are relevant here.
Cronin Macintosh, 1962, found that muscular efficiency was measurably

. t . tOi - - • ■
Xi J. < ■■ c
-t. js S llx-A „ _ *3 0 X . -
A L> i Y*
S ft, < . ^ c L X., ftS . C 33-i
. V- - J - j - - - I ' r
- L - <
; ■ . ■ _ j i O /lj - JX > -I
i .1 - < J oi ai J-iiud ySiz&q&s
> Ji i _ noj.-ixjx. J - • J t • : *o;(r
. JO J J J _ X - i x Xol t A. 'J o o
- -
t . ^ _ o 0. . , 0G:. .ft L x J
.
. j 1-Xj
.
i J C - 3 - X
JLS oj - _ x jl - rx . . jj .
c
A . - ' x; , i < 0-* -
- 18
greater under conditions of induced hypoxia . This may be related to the
increased contractility of actinomyosin in an acid medium. Pulmonary
blood volume drops in normal subjects by a mean of 6% during supine
exercise for three minutes at 112. 5 Kg«M/min . Pulmonary diffusing
capacity increases when normals are subjected to moderate to severe
degrees of exercise; at mild exercise levels the diffusing capacity may
not change. In the face of chronic lung disease, the rise is less, and
Z 8 in most individuals, there was seen to be no change or a fall . Both
ventilation and perfusion are greater in the more dependent areas of
the lungs, with a higher ventilation to perfusion ratio in the upper lung
fields. These findings were not significantly changed in normals by
29 exercise . Oxygen consumption, pulse rate and work load are closely
related. The pulse rate may be misleading in those in poor physical
30 training
Working capacity, defined by pulse rate limits of 170/minute, has been
studied. This has been shown to increase linearly with age and to be
32, 33 consistently greater in males than females . Whereas, studies of
i i • 34 the pulse rates m recovery from exercise have not been rewarding ,
several other measurements of exercise in heart disease have been
35, 36 fruitful
The development of exercise tests in the evaluation of pulmonary
disease has been more limited. Jones et al, 1963, measured the change
in FEV produced by exercise and Gandevia, 1963, observed the response
37 38 of minute ventilation in the last minute of a four minute exercise test ’

:
.. .. .. tc . - -
,c 1-, ' . -;OC i; - JO ooIJ
. . g j i ■ ■ i \ri j r o .
tljJXTt _* Ji ii r . • • <.G 5 i v' /'• JBCJ.SO
I L- \ -
ISJi_- 3 0 3 ttl . -I X- il
■ j. <: i-ii-' x . ’Om ni
• . oi. i.’ "i > ■ j.. tx ro; • • ■ x >v
, • . . ri i t ., ; j-x o ■i
... .
_.: ■. , ,■ X/ . ji ■ ;• { cC . • - •
. . - • '• . . ' '
-y t- • » r- 4 . IJ.-X iJ
. ii q y i - < - i, -- . o
■ ■. •.. .
xusri ni > SfJ n - • -
. i ■ . J. voo'j’i x:i - . • - s>x!3
S ;xo I9X •<. U869U C&jrfio IjSISV
.
S' j - X: ,3'lOv.' if TiCOif1 . 3t' ->
j.. , . -. :ix xl 9'xoxrx nsscl esri qsjb - J
, . • • ; • ; . O’- - ’I xii
. .. . . Jfcl - r • - r , ...... - ■' ijLrnix.x Ac
- 19
Of more specific interest in terms of the present study are the reports
39 40 41 of Berg, 1947, Erikson, 1957, and Refsum, 1964 ’ 5 . These
investigations were concerned with the response to acute exercise,
with measurement of oxygen and carbon dioxide curves during the re¬
covery phase. These studies used short exercise regimens of one minute
under a moderate to large work load. Results showed a small but
definite difference in the different groups under consideration. The
overlap with the normal population in all these measurements was consid¬
erable. Only 2/3 of Refsum1s group of cases fell outside the normal
range.
The objectives of this particular study are limited. First it provides
a preliminary evaluation of the efficacy of this type of exercise stress
test in the study of cardio-pulmonary disease. Second, it can serve,
as a pilot study, as a nucleus around which improved a refined exercise
tests may develop.
In the face of the paucity of experimental regimens available for the
conduct of a test of this kind, it is the purpose of this inquiry to provide
a first, gross evaluation of the usefulness of such a test in children with
cystic fibrosis . It is hoped that such an effort will help to determine
whether or not attempts to polish and refine and perfect such tests might
be fruitful in the investigation and treatment of pulmonary disease.
Formal statistical analysis was not brought to bear on the data of
the present study, because of the small sample size, because of the
inherent coarseness in this context of minute volume measurements.

.• . . i . !. i .. . i i : ■ ji i - j . .
1 ' , , i 1 < .i t <
J39*X . . no: . -.'I ; ' :
j df"£9 brrs as%\ o . i
. . a . . •
x . .. j 9 boi
. u . . . .. ril ni • •. 3 i
x ! , Hi i < ijjsli :joq i 3j iiox ri; < ^Xgy
'
. . iJ <j: •£ J iv. x o a- vi
i . n< io. j. Isv$• v-ixini.ail: iq 6
, i . x .. x: - . o \ r t
i . o . <
.... _ . ■ .
j i i . \\i . : j x * q . x _x. ,3
,j xi . , ■ . i j ,r ^ x j / .. ' O .' P, 1 S ^ Xx.. 1 v
x , J j O X.. X ’ -x jx. J. / O < o • I
J .. I . x r. xX . i: x ,
c;& xlc< , ,'i. - x s 11e Jon -iu tadiedw
JK x. i /£ x i i x ix • J
\ t O.i U X • J X'Xi X1 X . x i .. J1 1 x *. XO
, s. x ix . x. i < ■■ n-i q
> i - nor j -j i . ! x-Eoo ir j j/ix i

~ 20
and because of the large scatter resulting. Carefully designed and
executed visual displays of data, described above, are adequate for this
purpose.
In all of figures 8 through 13, though a very broad correlation between
the presence of pulmonary disease and an elevation in the CO^ half time
can be visualized, it is also apparent that the degree of overlap be¬
tween the diseased and the normal population is considerable. The low¬
est 1/2 time was shown by one of the patients (G.A.). He was, also,
the youngest individual tested at 5-11/12 years, but his exercise level,
20 Kw, was equal to the work done by the oldest patient in the group
(C. McM.), 23-1/12 years old.
For this reason only the very broadest of generalizations can be
made regarding the results of this study.
From figures 8 and 9j it is apparent that none of the normals showed
half times over 150% of predicted. Among the patients, six of the thir¬
teen plotted fall above 150% of predicted half time. In addition the minimal
half time of each of the patient groups is greater the more marked the
involvement by disease, though less significance can be attached to such
an observation. It is of interest to note that none of the class III 1/2 times
fell below 100%.
4 Cook et al studied 64 patients with cystic fibrosis, age 6 to 25 years .
70% showed an increase, outside of the normal range, of the ratio RV/TLC.
Only 46% showed an elevated RV. 34% showed a fall in VC, and 21% an
increase in FRC.

. '
t 5 . i
. o; /
< 1 il io U
'( O- h c. 10
^ i i• k:
:- s aoi ;xdi:qoc XfiOT'xon orfJ Du* b- c.c^ex'- rf t x<s
( j . i 1 \ \. t • \ t •
\ !. - . J • ' i .< i C _
io j Oi i.£J £ t
. .. J - J. -
• e r! J /j io i o .j ■ i axril o .
I . O J. . ' L , 1 3 - -
i < : ' •: ■ i ^
; t n ‘ „ ■ rv- o j ^ i jZ
.
CJ_ ; • ... i i _• . J--■ ■* ii«
. i
S v < . . . ^ i ■/:/ O i i J
. x i.
i ^ _ t j i i. c _ o o v_'
t i ..X U J - ' ' <
- 21 -
In the group of patients studied here, only 46% had elevated RV/TLC.
46%, also, had a % predicted half time of over 150%, but only 33% had
both an elevated RV/TLC and an elevated 1/2 time.
In figures 10 through 13, both ordinate and abscissa are plotted
linear~linear in percentage deviation from the predicted value concerned.
If there were no significant relationship between the disease and the values
of the ordinate and abscissa coordinates, the points as plotted should
group themselves at random. They would show radical symmetry around
the intersection of the ordinate and abscissa 100% lines. If the disease
effected only the ordinate quantity, the plot would show an axis of symmetry
around the 100% line arising from the abscissa. If both the ordinate and
abscissa values were significantly effected by the disease, the points
plotted should tend to segregate in one of the quadrants formed by the
100% lines.
In all of these figures, the disease seems to have tended to raise the
1/2 time above that predicted for that age. In fig. 10, the disease tends
to elevate the RV/TLC, and the points tend to fall in the upper-right
quadrant.
In fig. 11, the disease tends to raise the RV, and the points tend to
fall in the upper-right quadrant.
In fig. 12, the vital capacity is decreased in most, and the points
tend to fall in the lower-right quadrant.
In fig. 13, the functional residual capacity is decreased in most, and
the points tend to fall in the lower-right quadrant.

t£
, ' ' <
c-i.tn-Di.oq j - -
, sniirioo .
'
< - m ' - me mi:
X
o > f-' - Xjjoi. be iJclq
r.il • i
■i t ‘ • I j : ‘ lit tO 1j S:
. . u • : svou omit S\I
t
. I . .• 31
, . • . ,11 .
- ■■•i j ■' -
. ^ Ijb.i , - • - x•’
. i.... . j! ..i Hi - i
x • rn: , J. . i 1--
i rtnioq > fi J

~ 22
SUMMARY k CONCLUSION
It should be emphasized again in closings that the skew seen here
may well be produced by factors other than the pathologic pulmonary
forces in cystic fibrosis. The size of the normal group is insufficient
to ensure that they are in fact completely reliable to represent the
normal population with any exactness. The results shown above are
not inconsistent with the initial hypothesis that pulmonary disease,
and cystic fibrosis in particular, will prolong the time required for the
elimination of excess CO^ resulting from exercise.
The test in its present form is inadequate to provide a definitive
and clinically useful laboratory test of pulmonary function. However,
it does provide additional evidence that there may be some promise in
further development and refinement of the study of the diseased lung
under stress.

r ■ - <3
si3 ariT . .i- I . ■
jj ildjsiloi yi oo lorf j - mm oi
. . ■ i itox
4 ill w ,‘iEXjyoiJi^q DidiX . May • |«Ml
5 - •
i 4 i
'
.

OVERALL SUMMARY
Twenty subjects, fourteen patients with cystic fibrosis and six normal
individuals, were moderately exercised on a bicycle ergometer.
Collections of minute volumes of expired air before, during and follow¬
ing exercise were made.
The times required for the carbon dioxide output to fall half way to
the level at rest were calculated.
These times, for cystic fibrosis patients, were compared with the
times for normals and with selected objective tests of pulmonary function.

< Y ; ’ 1
< •
t - (_ : i;io • i •- '•£ £ lioO
, ■ i r
' . >1
t i J <
.
(MUM) 3iMll S/1 z00
CD
CO
*co o
- ,
E
o
fl ST-
<\! \
CM O
o
0
CD
OS
I


o o O CD <fr o OJ 04 OJ
o <D
O OJ
o o
o
>s
■f r.tum
o
<
o
o <6. Cwoa*
o
r~
CL
O
O r*
•5
o o
o
0^0 u"> £! rO
ooo O lO
o o OJ
O o o
CO j —5
6
CO
o
o
!
r-
O o oo
-T—
o <r 04
O o OJ
5
o CO
o 04
T“
O CO
o
W”‘
g *
imi Z/\ G310!Q3^!d %


200-1
o CO
6
o
o
O
« S I o o o CO O Si"
011/ AU 03 lOIGB^d


21
0 -
o
o
!' O
o o o
o o o
n o Qj>
I o UO
o 00
AU G 3 10 IQ 3 Ud %
PR
ED
ICT
ED
1/2
TIM
E


o
o i 0
O
o
i
i
I O 1 I
O o
o
o
CO
'r o
1 l 1 2
o o
o
B k 0
o o o O O w i*-
OA Q3101Q3U6 CP/
JO
r
o CD eg
O
eg UJ
O o eg 04 s evil
o ti
il 091
b 5
IL. I
fbj
jL O co
i o V
o to


APPENDIX
Tabulated Data
Patient Age Height^ 2
Work load CO y time"" 2
rv/tic
Gr « A . 5 11/12 110 20 0.20 .31
L.L. 6 0/l2 128 10 0.78 .42
■ if R.M. 6 8/l2 118 10 0.70 • 25
M.M. 7 4/12 116 25 1.38 .24
E.S. 8 5/12 123 10 1.82 .51
-n N.C. 8 7/12 129 15 1.12 .28
S.M. 9 0/l2 130 40 1.00 .22
M.Ii. 9 l/l2 127 10 3o50 .44
1.1. 10 0/12 121 10 1»73 o35
D.D. 1310/12 138 50 1.71 - »37
D.R. 14 4/12 161 50 lo 51 .26
«j • D o 15 7/12 149 50 0.94 .31
H J.McN « 16 5/l2 161 40 1.50 »49
C.McM. 23 l/l2 163 20 1.95 .30
Normal Age Height’*' 2
Work load C0^ y time^ 2
rv/tlc
D.R. 6 6/12 107 15 0.73 J • .A, • 8 7/12 121 20 0.39 D.M. 10 l/l2 144 50 1.13 A. Gr. 13 0/l2 158 30 1.27 B.L. 15 7/12 153 40 0.88
B «D. 22 7/12 162 50 1.50
1: centimeters 2 s Kw» see text 3s minutes

BIBLIOGRAPHY
1. MM Orzalesi, D Kohner, CD Cook, H Shwachman; Anamnesis,
Sweat Electrolytes and Pulmonary Function Studies in Parents
with Cystic Fibrosis of the Pancreas. Acta. Paed. Scand. 52:
267, May *63.
2. SW Royce; Cardiac & Pulmonary Complications in Fibrocystic
Disease of the Pancreas. Ross Ped. Research Conf 18: 7% 1956.
3. GR Demuthj WF Howatt and NS Talner; Intrapulmonary Gas Dis¬
tribution in Cystic Fibrosis. Am. J. Dis. of Children 103: 129,
1962. 4. CD Cook, PJ Helliesen, L Kulczycki, H Barrie, L Friedlander,
S Agathon, GBC Harris,,. H Shwachman; Studies of Respiratory
Physiology in Children 11; Lung Volumes and Mechanics of Res¬
piration in 64 patients with Cystic Fibrosis of the Pancreas. Ped.
24: 181, 1959.
5. G Polgar, W Chernick and RM Toft; Longitudinal Studies of
Pulmonary Function in Children with Cystic Fibrosis (abstr.).
Am. Rev. Resp. Dis. 88: 123, 1963.
6. JH Comroe, RE Forster, AB DuBois, WA Briscoe, E Carlsen;
The Lung 2nd ed. Year Book Med. Pub., Inc. Chicago, 1962.
7. RS Mitchell, NC W ejob, GF Filley; Chronic Obstructive Broncho¬
pulmonary Disease fiT; Factors Influencing Prognosis. Am. Rev.
Resp. Dis. 89: 878, 1964.
8. RM Goldring, AP Fishman, CM Turino, HF Cohen, CR Denning,
DH Andersen; Pulmonary Hypertension and Cor Pulmonale in Cystic
Fibrosis of the Pancreas. J. of Ped. 65(4): 501, Oct r64„
9. PA di SanPAgnese; Bronchial Obstruction with Lobar Atelectasis
and Emphysema in Cystic Fibres is of the Pancreas. Ped. 12:
178, 1953.
10. JR West, PA di SanPAgnese; Studies of Pulmonary Function in
Cystic Fibrosis of the Pancreas. J. Dis. Childhood 86: 496,
1953.
11. PF Scholander; Analyzer for Accurate Estimation of Respiratory
Gases in One-Half cubic Centimeter Scruples. J. of Biol. Chem.
167(1): 235, 1947.

GUSItf
J Si ' W i
t.l ' i
-
' 1 i ■' I
u rail
:
< -J <<
i ; iXIXi JJX>v
J J
- u -
T' J.I
x o Jns. x
t o
t. V
■ c l .. is yi
i noi
i , i c x :
: - , i:
£ io
.• J
t - jO.
« — * 1 J , - J
, 3 ' O
, j >
*1.
/ x ^xomix. c]
. .
• l o .
XIX i c.1
JjX.iU. J.J
v_ '• i PO ■
.
lij O Si o
j ox
- i c ■’
1 r I
1 < x \ X
, !
O - J" o - J - I-
‘ 0 I • iorJoc
il'J w -i-
X

12. CA Keele and E Neil; Samson WrighPs Applied Physiology,
10th ed. Oxford Univ. Press, London, 1961.
13. ME Avery, V Cherwick, RE Dutton, S Permutt; Ventilatory
Response to Inspired Carbon Dioxide in Infants and Adults.
J0 App. Physiol. 18(5): 895 Sept, 1963.
14. ASE Fowle, EJM Campbell; The Immediate Carbon Dioxide
Storage Capacity of Man. Clin. Sci. Z7: 41, 1964.
15. NC Brackett, JJ Cohen, WB Schwartz; The Carbon Dioxide
Titrution Curve of Normal Man. N. E.J.M. 272: 6, 1965.
16. MB Mcllroy; The Respiratory Response to Exercise. Ped.
(Suppl) 3£: 680, 1963.
17. MB Mcllroy & A Holmgren; Arterial Blood Gas Tensions During
Exercise in Normal Subjects. Fed. Proc. 20: 423, 1961.
18. WO Fenn, AB Craig; The Effect of Carbon Dioxide on Respiration
Using a New Method of Administering CO . J. App. Physiol.
_18_(15): 1023, 1963.
19. RA Mitchell, HH Loeschcke, JW Severinghaus, BW Richardson,
WH Massion. Regions of Respiratory Chem o sensitivity on
the Surface of the Medulla. Ann. N. Y„ Acad. Sci. 109(2):
661, 1963.
20. P Dejours; Control of Respiration by Arterial Chemoreceptors
Ann. N. Y. Acad Sci. 109(2): 682, 1963.
21. WO Fenn; Introductory Remarks. Ann. N. Y. Acad. Sci. 109(2):
415, 1963.
22. FF Kao, CC Michel, SS Mei, WK Li; Somatic Influence on Respir¬
ation. Ann. N„ Y, Acad. Sci. 109(2): 696, 1963.
23. WF Storey, J Butler; Evidence that the P,-,0 of Mixed Venous U 'y
Blood is not a Regulator of Ventilation During* Exercise. J.
App. Physiol. 18(2): 345, 1963.
E Asmussen, M Nielsen; Experiments on Nervous Factors Controlling
Respiration During Exercise Employing Blocking of the Blood Flow.
Acta. Physiol. Scand. 60: 103, 1964.
7 A L* •

; i .
. I
j. t : [oi t . ■
< i o
j > w ~
. J
C 0 i
l /Olllc • -
- < 8 :_
- • j
c ■ .* B xc
; • < i ■ -HI
ojd J '
< J. :( J-±l.
.. • •
i ,no i s f
iii d io - •!-< r, d
. - j. rI f
:(
C - 0 . .
. -
. i; l, i : ; : '•
. n < j
j.GJCA i < : ■ c. . S
jon ex r-ooia
j. .. - .
tx
xj j i jjCI xioriBi j o 3 9 HI

25. E Asmussen, SH Johansen, M Jorgensen, M Nielsen; The
Neurogenic Factors in the Regulation of Respiration & Circulatory
during Muscular Exercise. Acta. Physiol. Scand. 59 (Suppl 213):
19, 1963.
26. RFP Cronin & DJ Macintosh; The Effect of Induced Hypoxia on
C>2> Uptake during Muscular Exercise in Normal Subjects. Cam.
J„ of Bioch. and Physiol. 40: 717, 1962.
27. WR Chaffee, H Smulyan, JF Keighley, RH Eich; The Effect of
Exercise on Pulmonary Blood Volume. Amer. Heart J. 66:
657, 1963.
28. GN Bedell, RW Adams; Pulmonary Diffusing Capacity during
Rest and Exercise; A Study of Normals and Persons with Atrial
Septal Defect, Pregnancy, and Pulmonary Disease. J.C.I. 41:
1908, 1962.
29. AC Bryan, LG Bentinoglio, F Beerel, H MacLeish, A Zidulka,
DV Bates; Factors Affecting the Regional Distribution of Venti¬
lation and Perfusion in the Lung. J. of App. Physiol. 19(3):
395, 1964.
30. GR Gumming & R Danzinger; Bicycle Ergometer Studies in
Children II; Correlation of Pulse Rate with Oxygen Consumption.
Ped. 32_: 202, 1963
31. MS Malhotra, J Sen Gupta,, RM Rai; Pulse Count as a Measure
of Energy Expenditure. J. App. Physiol. 18(5): 994, 1963.
32. E Bengtsson; The Working Capacity in Normal Children, Evaluated
by Submaximal Exercise on the Bicycle Ergometer and Compared
to Adults. Acta. Med. Scand. 154: 91, 1956.
33. GR Gumming, PM Cumming; The Working Capacity of Normal
Children. Cam. Med. Assoc. J. 88: 351, 1963.
34. JD Kramer, PR Lurie; Maximal Exercise Tests in Children.
Amer. J. Dis. Children 108: 283, 1964.
35. RM Harvey, WM Smith, JO Parker, MI Ferrer; The Response
of the Abnormal Heart to Exercise. Circ. 26: 341, 1962.
AG Bicklemann, EJ Lippschutz, L Weinstein; The Response of
the Normal and Abnormal Heart to Exercise; A Functional Eval¬
uation. Circ. 28: 238, 1963.
36.
a v m A
37. RS Jones, MJ Wharton, MH Buston; The Place of Physical Ex¬
ercise and Bronchodilator Drugs in the Assessment of the Asthmatic
Child. Arch. Dis. in Childhood 38: 539, 1963.
38. B Gandevia; Ventilatory Response to Exercise and the Results of
a Standard Exercise Test in Chronic Obstructive Lung Disease.
Amer. Rev. Resp. Dis. 88: 406, 1963.
39. WE Berg; Individual Differences in Respiratory Gas Exchange
during Recovery from Moderate Exercise. Amer. J. Physiol.
149 (3): 597, 1947.
40. H Erikson; The Respiratory Response to Acute Exercise of
Eskimos and White. Acta. Physiol. Scand. 41: 1, 1957.
41. HE Refsum; Evaluation of Cardio Pulmonary Function by Studying
the Recovery of the Gaseous Exchange after Exercise of
Short Duration. Scand. J. Clin. & Lab. Invest. (Supp) 15: 76,
1964.
42. P.J. Helliesen, CD Cook, L Friedlander, S Agathon; Studies
of Respiratory Physiology in Children, I; Mechanics of Respiration
and Lung Volumes in 85 Normal Children 5 to 17 years of Age.
Ped. 22: 80, 1958.

(.* •f-Iihoi'-Djcio
: _ . . - •
;
. . • .
- - , :(
. . i
.
, x ■ J
;i
X
« - .
- - - C ' A loY gin
I t o :




YALE MEDICAL LIBRARY
Manuscript Theses
Unpublished theses submitted for the Master's and Doctor's degrees and
deposited in the Yale Medical Library are to be used only with due regard to the
rights of the authors. Bibliographical references may be noted, but passages
must not be copied without permission of the authors, and without proper credit
being given in subsequent written or published work.
This thesis by has been
used by the following persons, whose signatures attest their acceptance of the
above restrictions.
NAME AND ADDRESS
SD
/- 3
t?, £ 3
DATE
f \/(o 7