exercise decreases plasma antioxidant capacity and increases urinary isoprostanes of ipf patients
TRANSCRIPT

Respiratory Medicine (2010) 104, 1919e1928
ava i lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / rmed
Exercise decreases plasma antioxidant capacity andincreases urinary isoprostanes of IPF patients
R. Jackson a,b,*, C. Ramos a, C. Gupta a, O. Gomez-Marin a,b
aResearch Service (151), Miami VAHS, 1201 NW 16th Street, Miami, FL 33125, USAbUniversity of Miami, Miami, FL 33101, USA
Received 19 February 2010; accepted 27 July 2010Available online 23 August 2010
KEYWORDSIdiopathic pulmonaryfibrosis;Oxidant stress;Exercise
* Corresponding author at: Research2687; fax: þ1 305 575 3126.
E-mail address: [email protected]
0954-6111/$ - see front matter Publisdoi:10.1016/j.rmed.2010.07.021
Summary
We tested whether markers of systemic oxidant stress were detectable in 29 typical IPFpatients, and whether these increased after low level exercise. We obtained resting plasmafor measurement of amino terminal pro brain natriuretic peptide (NT-proBNP), and plasmaand urine samples for isoprostanes and total nitrite. Total antioxidant capacity (TAC) wasmeasured in plasma, and H2O2 was measured in urine. Subjects exercised ate50 W on a semirecumbent bicycle until limited by dyspnea. Samples were obtained immediately after exer-cise for measurement of the same variables.
Plasma and urine samples were also obtained at rest from 6 normal individuals over 40 yearsof age solely to establish comparison values for NT-proBNP, nitrite, H2O2 and TAC assays.
Plasma NT-proBNP was high at rest and after exercise, suggesting pulmonary arterial hyper-tension. IPF patients’ resting NT-proBNP concentrations apparently exceeded those of normalcontrols. IPF plasma isoprostanes at rest exceeded the normals. IPF urine isoprostanesincreased significantly after exercise (P Z 0.047 by signed rank test); and, plasma TACdecreased significantly after exercise (P < 0.001 by signed rank test). Neither plasma nor urinenitrite changed significantly after exercise. H2O2 concentration was quite high after exercise insome IPF subjects’ urine.
IPF patients demonstrate systemic oxidant stress at rest detectable as increased isopros-tanes in the circulation. An increase in urine isoprostanes and a decrease in plasma TAC afterexercise suggest that reactive oxygen species (ROS) are produced during low level exercisedone by IPF patients.Published by Elsevier Ltd.
Service (151), Miami VAHS, 1201 NW 16th Street, Miami, FL 33125. Tel.: þ1 305 575 3548/305 632
du (R. Jackson).
hed by Elsevier Ltd.

1920 R. Jackson et al.
Background
Idiopathic pulmonary fibrosis (IPF) is a progressive, fibroticlung disease of unknown etiology prevalent in males over 50years of age.1,2 Patients with IPF have evidence of oxidantstress within the bronchoalveolar compartment andcirculation.3,4
Several structurally unrelated antioxidants inhibit bleo-mycin (BLM)-induced lung injury. N-acetylcysteine (N-Ac)protects rats from bleomycin-induced fibrosis.5,6 Transgenicmice that over express extracellular superoxide dismutase(EC-SOD) are protected from BLM-induced lung fibrosis.7 Acatalytic metalloporphyrin with SOD and catalase activityalso attenuates bleomycin-induced pulmonary fibrosis.8
Suppression of the transcription factor Nrf-2, which regu-lates many aspects of the antioxidant response, in miceworsens BLM-induced pulmonary fibrosis.9 Perhaps mostimportant, N-Ac has been found to minimize significantly theprogression of pulmonary function worsening in IPF patients,who were also treated with prednisone and azathioprine.10
N-Ac has been shown to prevent epithelial-mesenchymaltransition of alveolar epithelial cells while repleting cellularglutathione and decreasing reactive oxygen species (ROS)production stimulated by transforming growth factor-beta(TGF-b).11
Fluid recovered from IPF lungs by bronchoalveolarlavage (BAL) contains high concentrations of myeloperox-idase (MPO), and alveolar inflammatory cells releaseincreased quantities of superoxide anion (O2
e) and its dis-mutation product, H2O2.
12 Alveolar ELF GSH concentrationwas decreased by 77% in IPF patients compared to normalcontrols (where [GSH] Z 429 � 34 mM).13 Suppression ofoxidant stress is in part responsible for the apparent clinicaleffectiveness of N-acetylcysteine.14
Oxidative stress may trigger production or activation ofgrowth factors and cytokines and regulate matrix metal-loproteinases (MMP) that promote fibrosis.15 ROS, whichmay come from activated inflammatory cells, increaserelease of transforming growth factor-beta (TGF-b) fromepithelial cells and activate it. TGF-b activation decreasescellular glutathione, and its activation is a pivotal event inthe pathogenesis of fibrosis.16
Exercise limitation of IPF patients is also related toa combination of decreased oxygen delivery and increasedpulmonary vascular resistance. Hypoxia causes increasedO2- production by mitochondrial complex III, so H2O2 would
be anticipated to diffuse from muscle cells if scavengingmechanisms were overwhelmed. An underlying rationalefor the present study is therefore that oxidant stress maybe detected in the systemic circulation, when IPF patientsexercise at a low workload and develop hypoxemia.
We designed this pilot study to measure markers ofsystemic oxidant stress in clinically typical IPF patients whowere to be enrolled in a randomized controlled trial of silde-nafil (see http://clinicaltrials.gov/ct2/show/NCT00359736?termZipfþANDþsildenafil&rankZ4). Previous studies havenot examined well defined IPF cohorts.4 Detailed demo-graphicdataand resultsof that trial are reportedelsewhere.17
We hypothesized that classical markers of reactive oxygenspecies (ROS) in the plasma and urine, including isoprostanesand total antioxidant capacity (TAC) would demonstrate
oxidant stress at rest and be increased in IPF subjects by lowlevel exercise. We measured amino terminal pro brain natri-uretic peptide (NT-proBNP) and estimated systolic pulmonaryartery pressures (PAPsys) by echocardiography to determine ifthe subjects were at risk of pulmonary hypertension.18 Ourresults demonstrated that typical IPF patients, who oftenhave elevated NT-proBNP levels, develop hypoxemia andmildlactic acidosis that is associated with increased urinary iso-prostanes and decreased plasma total antioxidant capacityduring exercise at a low power output.
Methods
Experimental design
IPF was defined according to the American Thoracic andEuropean Respiratory Societies (ATS-ERS) clinical diagnosticcriteria.1 We studied 29 IPF patients who were to begina double blind, randomized, placebo controlled trial of sil-denafil as a potential therapy for patients with moderateimpairment of pulmonary function and mild to moderateincreases in echocardiographically estimated systolicpulmonary artery pressure (range 25e50 mm Hg). Patientswere studied in this protocol before they received theexperimental drug or placebo. Subjects did not undergo rightheart catheterization. Pulmonary function tests, includingarterial blood gases, were obtained before entry into thetrial. Patients were recruited between August 2006 andNovember 2008. All subjects and normal controls providedwritten informed consent.
We also obtained plasma and urine samples from sixvolunteers, who were laboratory employees. Two of the sixwere female. The average age was 50 � 6 (SD) years, andthe average weight was 76 � 16 (SD) kg. None of thevolunteers smoked, and none had any evident pulmonarydisease. Plasma and urine samples from the controls wereused only to standardize the assays and provide a range ofexpected values. The controls did not participate in theexercise protocol.
This study was reviewed and approved by the MiamiVAHS Institutional Review Board as protocol 4549.04.
Exercise test protocol to quantify dyspnea
Subjects underwent standardized 50-W exercise bicyclechallenges immediately before the 6-month drug inter-vention. We chose this constant low level power output totest endurance. The subjects had also completed 6-minwalk tests, which are reported elsewhere.17 Patients usedsufficient supplemental oxygen to maintain pre-exerciseoxygen saturation at 90% or greater, only if needed. Exer-cise was done in the sitting position on a semi recumbentbicycle (Life Fitness 95Ri, Life Fitness USA). It consisted ofpedaling at 50e60 revolutions/minute at a constant work-load of 50 W. This approximates an energy expenditure ofthree metabolic equivalents (MET; where 1 MET Z 3.5 mLO2/kg/minute). Exercise continued until patients werelimited by dyspnea or fatigue. O2 saturation, pulse rate,blood pressure and Borg dyspnea score were monitored andrecorded before and immediately after pedaling. Totalexercise time (seconds) was recorded.

Exercise and oxidant stress in IPF 1921
Sample collections
We collected blood and urine samples in the resting statebefore and immediately after the standardized exercise.Blood samples were collected by venipuncture in two 10 mLtubes containing sodium heparin (BD Vacutainer 366480,Franklin Lakes, NJ). Plasma was separated by centrifuga-tion (1500 � g for 10 min at 4 �C) and multiple aliquots werestored at �80 �C until analysis. Urine samples were storedin multiple aliquots at �80 �C until analysis. Samples werethawed only once before assays.
BNP assays
NT-proBNP was assayed using the automated assaydescribed in detail by Elin and Winter.19
Plasma lactate assays
The concentration of lactate in plasma samples obtainedbefore and after exercise was determined using an enzy-matic assay as described.20 Blood sampleswere placed on iceand plasma was separated as rapidly as possible. Sampleswere stored frozen at �80 �C until assays were done.
Urine creatinine assays
Urine creatinine was assayed by the clinical laboratory atthe Miami VAHS, using an automated assay.
Isoprostane measurements
We quantified F2-isoprostanes in plasma and urine usinghigh performance liquid chromatography (HPLC) tandemmass spectroscopy (MSeMS) as described in detail.21
Plasma and urine samples were stored at �80 �C untilanalysis (although isoprostanes are resistant to degrada-tion during handling). The HPLC system consisted of AgilentSeries 110 components (Agilent, Waldbronn, Germany).The HPLC system was interfaced with a triple quadrupolemass spectrometer (ADI 4000, Applied Biosystems, FosterCity, CA) run in the negative multiple reaction model. HPLCsystems and mass spectrometer were controlled by Analystsoftware (Version 1.3.1, Applied Biosystems). 500 mLsamples were injected. The assay has been validatedaccording to FDA Center for Drug Evaluation and ResearchGuidelines for bio analytical method validation.
Assays were done at the University of Colorado HealthSciences Center. Normal values for 15-F2 -isoprostanes havebeen established by this laboratory for plasma (range3e25 ng/L; n Z 16) and urine (55e348 ng/mg creatinine;n Z 16) using this technique and equipment. These valueswere used for comparison with the pre- and post-exerciseisoprostane data obtained in our subjects.
Nitrate/nitrite assays
We measured total nitrite in plasma and urine as a mar-ker of �NO production at rest and after exercise usinga nitrate/nitrite colorimetric assay (Kit No. 780001,
Cayman Chemical Company, Ann Arbor, Michigan). Nitratereductase was used to reduce all nitrate to nitrite beforemeasurement.22,23 Plasma samples were ultrafilteredthrough a 10 kDa molecular weight cut-off filter (Amicon)that had been rinsed by centrifugation with ultrapurewater. The detection limit of the assay is about 1 mMnitrite. Urine typically contains 200e2000 mM nitrite, andso urine samples were diluted before assay. Urine nitriteconcentration was expressed as nmoles/milligramcreatinine.
Total antioxidant capacity
We determined the Trolox equivalent total antioxidantcapacity (TAC) of plasma before and after each stan-dardized exercise test. This assay quantifies the ability ofthe sample to inhibit an in vitro oxidation assay, andcompares the degree of inhibition by plasma to knownquantities of Trolox (Antioxidant Assay Kit No. 709001,Cayman Chemical Company, Ann Arbor, Michigan). It relieson the ability of low molecular weight antioxidants inplasma to inhibit oxidation of 2, 20-azino-di-[3-ethyl-benzthiasoline sulphonate] (ABTS) to ABTSþ by metmyo-globin. Inhibition of absorption at 750 nm is measured andcompared to that of the water soluble tocopherol analog,Trolox. The data therefore reflect the net antioxidantcapacity of proteins (e.g., albumin) and small molecules(e.g., GSH, vitamin E, and vitamin C) normally present inplasma.24
H2O2 assays
We assayed urine H2O2 using the xylenol orange detectionmethod for quantifying oxidation of ferrous to ferric ions byH2O2 (Urinary Hydrogen Peroxide Assay, Catalog No.706011, Cayman Chemical Company, Ann Arbor, MI).25
Catalase was added to duplicate assay wells to confirmthe specificity for H2O2. Ferric ion binds to the dye xylenolorange to form a stable colored complex. Urine sampleswith or without catalase were mixed with reagent androcked at room temperature for 60 min. Absorbance wasrecorded at 595 nm.
Statistical analyses
Data were expressed as arithmetic means � SD or medianswith [25e75th] percentiles indicated, if the distribution ofvalues were non Gaussian. Pre- and post-exercise BNP andmarkers of oxidant stress were compared using the signedrank test (i.e., pre- and post-exercise data were paired).Comparisons of IPF pre-exercise values to normal controlswere not tested statistically, because the groups were notstudied contemporaneously. Data from the control groupsare included in the figures to illustrate the distributionof the data. In post hoc exploratory analyses, Pearsonproduct moment correlations were calculated to findwhether any of the plasma or urine markers of oxidantstress correlated with the post-exercise (nadir) SaO2
or the decrease in SaO2 during exercise. Statistical calcu-lations were done using SigmaStat (Systat Software,San Jose, CA).
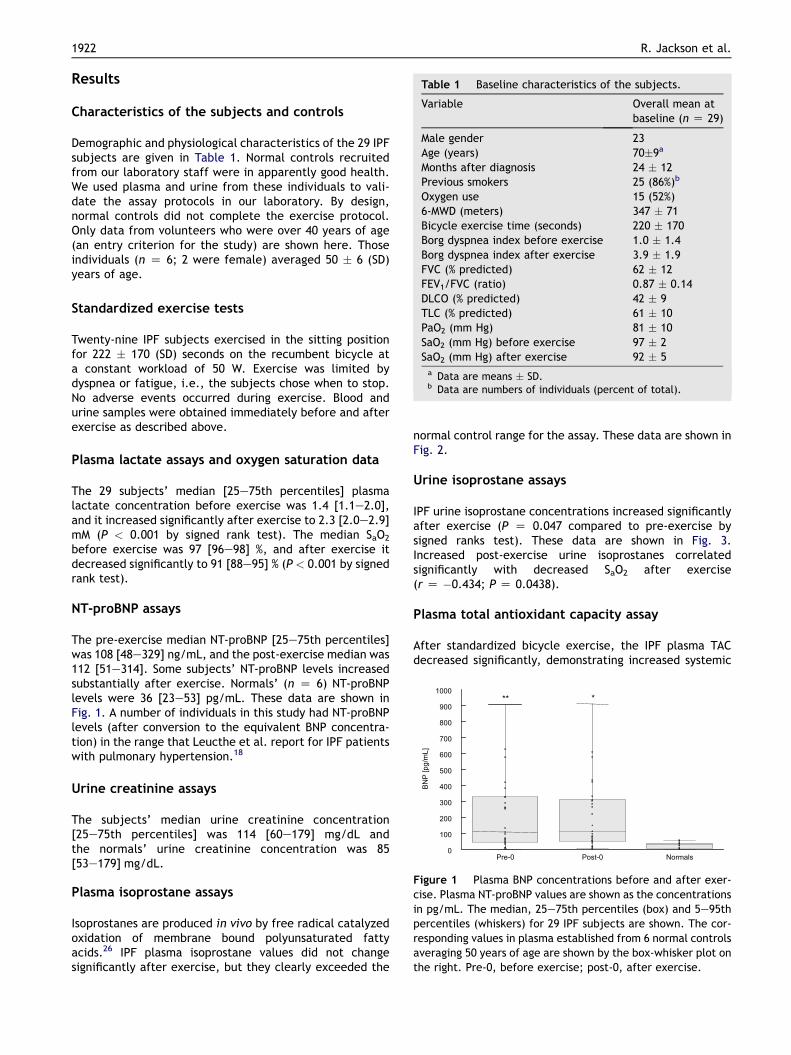
Table 1 Baseline characteristics of the subjects.
Variable Overall mean atbaseline (n Z 29)
Male gender 23Age (years) 70�9a
Months after diagnosis 24 � 12Previous smokers 25 (86%)b
Oxygen use 15 (52%)6-MWD (meters) 347 � 71Bicycle exercise time (seconds) 220 � 170Borg dyspnea index before exercise 1.0 � 1.4Borg dyspnea index after exercise 3.9 � 1.9FVC (% predicted) 62 � 12FEV1/FVC (ratio) 0.87 � 0.14DLCO (% predicted) 42 � 9TLC (% predicted) 61 � 10PaO2 (mm Hg) 81 � 10SaO2 (mm Hg) before exercise 97 � 2SaO2 (mm Hg) after exercise 92 � 5a Data are means � SD.b Data are numbers of individuals (percent of total).
Pre-0 Post-0 Normals0
100
200
300
400
500
600
700
800
900
1000
]Lm/gp[
PNB
***
Figure 1 Plasma BNP concentrations before and after exer-cise. Plasma NT-proBNP values are shown as the concentrationsin pg/mL. The median, 25e75th percentiles (box) and 5e95thpercentiles (whiskers) for 29 IPF subjects are shown. The cor-responding values in plasma established from 6 normal controlsaveraging 50 years of age are shown by the box-whisker plot onthe right. Pre-0, before exercise; post-0, after exercise.
1922 R. Jackson et al.
Results
Characteristics of the subjects and controls
Demographic and physiological characteristics of the 29 IPFsubjects are given in Table 1. Normal controls recruitedfrom our laboratory staff were in apparently good health.We used plasma and urine from these individuals to vali-date the assay protocols in our laboratory. By design,normal controls did not complete the exercise protocol.Only data from volunteers who were over 40 years of age(an entry criterion for the study) are shown here. Thoseindividuals (n Z 6; 2 were female) averaged 50 � 6 (SD)years of age.
Standardized exercise tests
Twenty-nine IPF subjects exercised in the sitting positionfor 222 � 170 (SD) seconds on the recumbent bicycle ata constant workload of 50 W. Exercise was limited bydyspnea or fatigue, i.e., the subjects chose when to stop.No adverse events occurred during exercise. Blood andurine samples were obtained immediately before and afterexercise as described above.
Plasma lactate assays and oxygen saturation data
The 29 subjects’ median [25e75th percentiles] plasmalactate concentration before exercise was 1.4 [1.1e2.0],and it increased significantly after exercise to 2.3 [2.0e2.9]mM (P < 0.001 by signed rank test). The median SaO2
before exercise was 97 [96e98] %, and after exercise itdecreased significantly to 91 [88e95] % (P < 0.001 by signedrank test).
NT-proBNP assays
The pre-exercise median NT-proBNP [25e75th percentiles]was 108 [48e329] ng/mL, and the post-exercise median was112 [51e314]. Some subjects’ NT-proBNP levels increasedsubstantially after exercise. Normals’ (n Z 6) NT-proBNPlevels were 36 [23e53] pg/mL. These data are shown inFig. 1. A number of individuals in this study had NT-proBNPlevels (after conversion to the equivalent BNP concentra-tion) in the range that Leucthe et al. report for IPF patientswith pulmonary hypertension.18
Urine creatinine assays
The subjects’ median urine creatinine concentration[25e75th percentiles] was 114 [60e179] mg/dL andthe normals’ urine creatinine concentration was 85[53e179] mg/dL.
Plasma isoprostane assays
Isoprostanes are produced in vivo by free radical catalyzedoxidation of membrane bound polyunsaturated fattyacids.26 IPF plasma isoprostane values did not changesignificantly after exercise, but they clearly exceeded the
normal control range for the assay. These data are shown inFig. 2.
Urine isoprostane assays
IPF urine isoprostane concentrations increased significantlyafter exercise (P Z 0.047 compared to pre-exercise bysigned ranks test). These data are shown in Fig. 3.Increased post-exercise urine isoprostanes correlatedsignificantly with decreased SaO2 after exercise(r Z �0.434; P Z 0.0438).
Plasma total antioxidant capacity assay
After standardized bicycle exercise, the IPF plasma TACdecreased significantly, demonstrating increased systemic

Pre-0 Post-0 Normals0
25
50
75
1002F
amsalP
-]L
m/gp[enatsorposi
**
Figure 2 Plasma isoprostane concentrations before and afterexercise. Data shown are plasma isoprostane concentrations inpg/mL. The median, 25e75th percentile (box) and 5e95thpercentiles (whiskers) for 29 IPF subjects are shown. The cor-responding values in plasma established from 16 normalcontrols described previously (see reference 20) are shown bythe box-whisker plot on the right. The plasma isoprostanevalues did not change significantly after exercise, but theyapparently exceeded the normal control range for the assay.Pre-0, before exercise; post-0, after exercise.
Pre-0 Post-0 Normals0
1
2
3
]xolorTM
m[CAT
*
Figure 4 Plasma total antioxidant capacity before and afterexercise. Data shown are plasma total antioxidant capacity inTrolox equivalents [mM]. The median, 25e75th percentile(box) and 5e95th percentiles (whiskers) for 29 IPF subjects areshown. The corresponding values in plasma established from 6normal controls averaging 50 years of age are shown by thebox-whisker plot on the right. The plasma TAC decreasedsignificantly after exercise (*, P < 0.001 post-exercisecompared to pre-exercise by signed rank test). Pre-0, beforeexercise; post-0, after exercise.
Exercise and oxidant stress in IPF 1923
oxidant stress (P < 0.001 compared to pre-exercise bysigned ranks test). As shown above, the decrease in TACwas accompanied by corresponding increases in lactate andhypoxemia after exercise. These data are shown in Fig. 4.
Nitrate/nitrite assays
IPF patients have a range of total nitrite concentrations inthe urine and blood that is easily measurable using theGriess reaction. The values are quite comparable to normalhuman data in the literature.27 These data are shown inTable 2.
pre-0 post-0 Normals0
100
200
300
400
500
600
700
800
900
1000
2Fenir
U-
]taercg/gp[
enatsorposi
*
Figure 3 Urine isoprostane concentrations before and afterexercise. Data shown are urine isoprostane concentrations inng/g creatinine. The median, 25e75th percentile (box) and5e95th percentiles (whiskers) for 29 IPF subjects are shown.The corresponding urine values established from 16 normalcontrols reported previously (see reference 20) is shown by thebox-whisker plot on the right. IPF urine isoprostane concen-tration increased significantly after exercise. Pre-0, beforeexercise; post-0, after exercise. (*, P Z 0.047 post-exercisecompared to pre-exercise by signed rank test).
Urine H2O2 assay
A wide range of H2O2 values was found; some IPF patientshave post-exercise urine H2O2 concentrations several foldabove the pre-exercise and normal values. However,because of the high variability, no significant differenceswere found. These data are shown in Fig. 5.
Discussion
Summary
An underlying rationale for the present study was thepreviously reported oxidative and nitrosative stress in bothepithelial lining fluid and circulation of IPF patients.4,28,29
We reasoned that exercise would exacerbate systemicoxidant stress in IPF patients, perhaps related to impairedoxygenation and resulting cellular hypoxia as in COPD.30,31
We studied patients selected for enrollment ina randomized clinical trial of sildenafil, a pulmonary vaso-dilator, for IPF.17 Enrolled patients were quite typical of IPFpatients followed in the outpatient clinic, and their diag-noses were based on the presently accepted ATS-ERS casedefinition.1,2
Plasma NT-proBNP is elevated in IPF patients
Despite the modest increase in pulmonary artery systolicpressure (estimated echocardiographically in the midthirties) required for entry into the trial, we found that IPFpatients had plasma NT-proBNP levels clearly above the sixnormals, as shown in Fig. 1. Elevated brain natriureticpeptide (BNP) levels correlate well with significant pulmo-nary hypertension in patients with chronic lung diseases,including idiopathic pulmonary fibrosis.18 None of oursubjects had clinically or echocardiographically evident left

Table 2 Plasma and urine nitrite concentrations.a
Pre-exercise Post-exercise Controls Pb
Plasma total nitrite [mM] 12 [8e15] 10 [7e14] 7 [4e11] 0.314Urine total nitrite [mmol/g creatinine] 216 [156e341] 218 [133e353] 293 [190e542] 0.509a Data from 29 subjects and 6 controls are medians with the [25e75th] percentiles shown. Total nitrite represents the sum of nitrite
and nitrate after reduction in vitro with nitrate reductase.b Pre-exercise compared to post-exercise value by signed rank test.
1924 R. Jackson et al.
ventricular failure, confirming that high NT-proBNP levelswere likely related to the increase in pulmonary arterypressure that typifies IPF. The range and median of post-exercise NT-proBNP values appeared similar to the pre-exercise values as shown in Fig. 1. Nineteen of 29 individualsubjects had detectable increases in their NT-proBNPvalues after exercise. While some individual patients hadboth high post-exercise NT-proBNP and elevated systolicpulmonary artery pressure (RVSP) by echocardiography, nosignificant statistical correlation could be found by regres-sion analysis. The lack of correlation was due to individualvariability and the small number of subjects in the trial.Increased pulmonary vascular resistance and impaired rightventricular pressure appear to be key factors in exerciselimitation of IPF patients.
Oxidant stress is an important mechanism in IPF
Oxidative stress in IPF is detectable using various biomarkers(e.g., protein carbonyls, antioxidant capacity, thio-barbituric reactive substances) in bronchoalveolar lavagefluid (BALF) and plasma.4,28 For example, 8-isoprostanes(i.e., F2-isoprostanes), a product of non enzymatic, radicalcatalyzed lipid peroxidation are found in BALF of patients
007
008
005
006
crea
tinin
e]
004
005
[nm
oles
/mg
002
003
Urin
e H
[
slamroN0-tsoP0-erP0
001
U
Figure 5 Urine hydrogen peroxide concentration. Datashown are urine H2O2 concentrations in nmol/mg creatinine.The median, 25e75th percentile (box) and 5e95th percentiles(whiskers) for 29 IPF subjects are shown. The correspondingvalues in urine established from 6 normal controls averaging 50years of age is shown by the box-whisker plot on the right. Arange of values was found; some IPF patients have post-exer-cise urine H2O2 concentrations several fold above the pre-0 andnormal values. However, because of the variability, no signifi-cant differences were found. Pre-0, before exercise; post-0,after exercise.
with interstitial and other chronic lung diseases.26 Depletionof lung GSH is relevant to the pathogenesis of IPF,32,33 as isimplied by a recent clinical trial. Deterioration of vitalcapacity (VC) and diffusing capacity (DLCO) were delayedsignificantly in the N-acetylcysteine group.10
Plasma and urine isoprostanes indicate systemicoxidant stress in IPF
F2-isoprostanes are prostaglandin-like compounds, derivedfrom esterified arachidonic acid by non enzymatic, freeradical catalyzed reactions. They have provided evidence ofoxidative stress in a number of disease states includingatherosclerosis, chronic obstructive pulmonary disease andneurodegenerative conditions (for review, see reference 26).
We detected significantly increased urine isoprostanesafter low level exercise. Elevated urine isoprostanes reflectrapid renal clearance of lipid peroxidation products fromthe circulation. While we cannot eliminate renal produc-tion of isoprostanes as the source, the kidney presumablyremains well perfused during exercise and well oxygenatedcompared to skeletal muscle.
Plasma isoprostane levels in IPF patients are several foldhigher than those in controls’ plasma, as shown in Fig. 2.We did not detect an increase after exercise, perhapsbecause of the already high levels. While we and others21,26 take this to represent convincing evidence of oxidantstress, the potent vasoconstrictor activities F2-isoprostanesare also plausibly related to the increase in pulmonaryartery pressure found on echocardiography. Isoprostanesare potent vasoactive thromboxane receptor agonists,demonstrating also a potential pathophysiological role asmediators of pulmonary hypertension.26 Thus, findingincreased isoprostanes is mechanistically relevant to exer-cise induced increase in pulmonary vascular resistance andassociated right ventricular dysfunction.
Plasma antioxidant capacity decreases afterexercise
IPF patients at rest had plasma antioxidant capacity (TAC)comparable to or higher than normal controls. This resultobviously differs from the findings of Rahman et al., whoreported that IPF patients had diminished TAC at rest.4 Overone-half of the subjects in their study were current cigarettesmokers (while none of our subjects were active smokers),and this may represent the greatest difference between ourstudy populations. Our patients were strictly classified usingcontemporary criteria 1,2 and none were treated withcorticosteroids or experimental therapy at the time of these

Exercise and oxidant stress in IPF 1925
measurements, so the patient population we studieddiffered significantly from that described by Rahman et al.4
IPF patients developed a large and significant decreasein plasma TAC after exercise as shown in Fig. 4, reminiscentof exercise induced oxidant stress described in chronicobstructive pulmonary disease (COPD) patients.29 Thisoxidant stress is accompanied by hypoxemia and lactateproduction, indicating that low level exercise has signifi-cant metabolic effects in IPF subjects. TAC represents thecapacity of plasma to inhibit an in vitro oxidation reaction.It is a nonspecific functional assay and likely reflects theavailability of reduced sulfhydryl groups on albumin inaddition to low molecular weight antioxidants such asnonprotein sulfhydryls, ascorbic acid, tocopherol andmembrane lipids that compete as targets of oxidation.24
Changes in TAC after exercise are not specific for IPF butrather represent a general indication of oxidant stress thatmay occur in various disease states. For example, asthmapatients are found to have significantly decreased totalantioxidant status during acute exacerbations.34 Similarly,TAC is lower than normal in COPD patients’ plasma, and itcorrelates with the severity of airway obstruction.35 TAC isdecreased in a number of other pathologies, includingsevere sepsis.36
Urinary hydrogen peroxide as a marker of oxidantstress
While we found no significant increase in urinary H2O2 afterexercise, some individual post-exercise values were highcompared to those at rest and to the normal controls asshown in Fig. 5. Because not all urine samples containedmeasurable H2O2, exploratory analysis was limited to thosesamples in which we could measure H2O2. The urinaryconcentration of hydrogen peroxide is increased in patientswith malignancies, where it correlates with increasedplasma hydrogen peroxide and erythrocyte malondialde-hyde.37 Although auto oxidation reactions in urine couldgenerate H2O2,
25 elevated urinary H2O2 is regarded asa marker of systemic oxidant stress in malignancies.37
Nitrosative stress in IPF
Reactive nitrogen species (RNS), which interact with ROS,also contribute importantly to epithelial injury in IPF.Myeloperoxidase (MPO) and nitrotyrosine (NT) co-localize ina number of inflammatory lesions.38 Finding MPO and NTtogether suggests that NO2
� (the major end product of �NOmetabolism) and HOCl react to produce NO2, whichaccounts for tyrosine nitration. Lung sections from IPFpatients stain strongly positive for nitrotyrosine (NT) andinducible nitric oxide synthase (iNOS) in alveolar macro-phages, neutrophils and alveolar epithelium.29
Although nitrosative stress is evident in IPF lungsections,29 we found no increase in IPF plasma total nitriteconcentration compared to controls as shown in Table 2.We likewise found no differences in urine nitrite concen-tration after exercise. This observation reflects restrictionof the well described nitrosative stress found in IPF patientsto alveolar compartment.
Systemic oxidant stress and exercise in IPF andother chronic lung disease
We found a significant increase in urine isoprostaneconcentration after low level exercise as shown in Fig. 3,confirming our hypothesis that low level exercise wouldexacerbate oxidant stress in IPF patients. Since urine iso-prostanes were negatively correlated with post-exerciseSaO2, the observed increase in isoprostanes is associatedwith evidence for hypoxemia.
We found a significant decrease in hemoglobin oxygensaturation and a small but significant increase in lactateafter low level exercise, suggesting that some subjectsexercised at near maximal capacity. Lactate productionreflects the integration of ATP production and its cellularutilization, so that efficient lactate uptake may result inrelatively low circulating concentrations that reflectadaptation to hypoxia. Plasma lactate may not reflectanaerobic glycolysis in muscles, as aerobic overproductionof pyruvate may occur early during maximal exercise.39
IPF patients we studied developed hypoxemia as shownby decreased SaO2 and increased lactate concentrations,along with increases in oxidant stress after exercise. Whilean increase in lactic acid production is typical of severeexercise, it occurred here at a rather low level of exertion(50 W). The increase in lactate may have been bluntedbecause of the subjects’ exercise limitation due to increasedpulmonary vascular resistance and right ventriculardysfunction.
Exercise as well as hypoxia per se imposes oxidativestress on skeletal muscle.40,41 Increases in myocardial andskeletal muscle free radical concentration confirm thatexcess ROS produced during exercise precede fatigue.41
While the source of ROS produced by muscle cells is notentirely clear, it is likely that mitochondria, enzymes andactivated phagocytes all contribute.42 Significant musclecell hypoxia may occur during exercise in patients withimpaired gas exchange and systemic hypoxemia.30 Hypoxiaincreases production of ROS by mitochondria, yet indirectevidence from manganese-containing superoxide dismutaseheterozygous knockout mice indicates that mitochondriamay not be the only source of O2
�.42
Glutathione metabolism is also clearly affected byexercise. Prolonged submaximal exercise by humans causesa decrease in reduced glutathione and a concomitantincrease in GSSG.43 Allopurinol inhibited the increase inGSSG/GSH and lipid peroxidation, otherwise observed inexercising COPD patients.44 Changes in exercise capacitywere not measured, although inhibition of ROS production,e.g., with allopurinol, would conceivably prevent skeletalmuscle dysfunction and increase exercise capacity.
Redox signaling may also be required for adaptation toexercise. Endurance exercise training can reduce oxidativestress after exhaustive exercise and may permit increasedfunctional capacity.45,46 Exercise training increases CuZn-containing superoxide dismutase and decreases p67phox,ERK phosphorylation and malondialdehyde production.40
Although we obtained novel and valuable data from thisstudy, we recognize several intrinsic limitations in its designand execution. The study population was small, as would beexpected in a single center trial. By design, each subject

NO nitric oxide radicalNT nitrotyrosineNT-proBNP amino terminal pro brain natriuretic
peptidePAPsys systolic pulmonary arterial pressurePDE5 phosphodiesterase fivePAH pulmonary arterial hypertensionO2- superoxide anion
RCT randomized controlled trialRVESP right ventricular end systolic pressureSaO2 arterial oxygen saturationSD standard deviationSOD superoxide dismutaseTAC total antioxidant capacity (of plasma)TGF-b transforming growth factor-beta
1926 R. Jackson et al.
served as his or her own control, so we did not compareresponses of IPF patients to those of disease controls (e.g.,COPD or sarcoid) or to normals. We chose rather to assessendurance at a low, constant workload as the stimulus tooxidant stress. Maximum oxygen consumption was notmeasured, although it is likely that protocol would haveprovoked a greater degree of oxidative stress. The controlsdid not participate in the exercise protocol because of theplanned, paired nature of the design. The controls tendedto be younger and healthier than the IPF patients westudied in the exercise protocol. Despite these limitations,which themselves raise testable hypotheses, the paireddesign effectively allowed us to detect significant intra-group differences after exercise.
Conclusions
A number of important new observations came from thistrial. Finding that NT-proBNP is elevated in typical IPFpatients and that two markers of oxidant stress, decreasedplasma TAC and increased urine isoprostanes occur afterlow level exercise and are associated with hypoxemia, isimportant. Such observations could lead to testing thehypotheses that systemic oxidant stress may be due tocellular hypoxia and that oxidant stress during exercise maybe a factor that limits endurance of IPF patients. Takentogether, these results show that IPF patients develophypoxemia and oxidant stress at low levels of exercise andsuggest that isoprostanes could therein contribute toincreased pulmonary vascular resistance.
Acknowledgments
The authors thank Chhavi Gupta, PhD and Rolando Garcia-Rojas for technical assistance; and, Dr. Rafael Valenzuelaand Miguel Roman for the lactate and NT-proBNPmeasurements.
Abbreviations
ATS American Thoracic SocietyBLM bleomycinBNP brain natriuretic peptideCOPD chronic obstructive pulmonary diseaseCuZn-SOD copper-zinc superoxide dismutaseEC-SOD extracellular superoxide dismutaseELF epithelial lining fluidGSH reduced glutathioneGSSG glutathione disulfideHOCl hypochlorous acidcGMP cyclic guanosine monophosphateERS European Respiratory SocietyIPF idiopathic pulmonary fibrosisILD interstitial lung diseaseIPAH idiopathic pulmonary arterial hypertensionMMP matrix metalloproteinaseMPO myeloperoxidaseN-Ac N-acetylcysteine
Authors’ contributions
RJ designed the study, obtained funding, directed allclinical trial procedures and wrote the manuscript incollaboration with the biostatistician. CR served asstudy coordinator, recruited subjects, did all clinicaltrial procedures and collected primary data. CGacquired samples and completed assays of the oxidantstress markers. OG served as biostatistician, assistedin study design and co-wrote the manuscript. Allauthors read and approved the final manuscript.
Conflict of interest statement
The authors declare that they have no conflicting interests.
References
1. American thoracic society/European respiratory society inter-national multidisciplinary consensus classification of the idio-pathic interstitial pneumonias. Am J Respir Crit Care Med2002;165:277e304.
2. Wells A, Hirani N. Interstitial lung disease guideline: the britishthoracic society in collaboration with the thoracic society ofAustralia and New Zealand and the Irish thoracic society.Thorax 2008;63:v1e58.
3. Kinnula V. Redox imbalance and lung fibrosis. Antioxid RedoxSignal 2008;10:249e52.
4. Rahman I, Skwarska E, Henry M, Davis M, O’Connor C,FitzGerald M, et al. Systemic and pulmonary oxidative stress inidiopathic pulmonary fibrosis. Free Radic Biol Med 1999;27:60e8.
5. Yildrim Z, Kotuk M, Iraz M, Kuku I, Ulu R, et al. Attenuation ofbleomycin-induced lung fibrosis by oral sulfhydryl containingantioxidants in rats: erdosteine and N-acetylcysteine. PulmPharmacol Ther 2005;18:367e73.
6. Serrano-Mollar A, Closa D, Prats N, Blesa S, et al. In vivoantioxidant treatment protects against bleomycin-inducedlung damage in rats. Br J Pharmacol 2003;138:1037e48.
7. Bowler R, Nicks M, Warnick K, Crapo J. Role of extracelluarsuperoxide dismutase in bleomycin-induced pulmonaryfibrosis. Am J Physiol Lung Cell Mol Physiol 2002;282:L719e26.
Exercise and oxidant stress in IPF 1927
8. Day B. Antioxidants as potential therapeutics for lung fibrosis.Antioxid Redox Signal 2008;10:355e70.
9. Hye-Young C, Reddy S, Yamamoto M, Kleeberger S. The tran-scription factor Nrf2 protects against pulmonary fibrosis. FASEBJ 2004;18:1258e60.
10. Demedts M, Behr J, Buhl R, Constable U, Dekhuijzen R,Jansen H, et al. High-dose acetylcysteine in idiopathicpulmonary fibrosis. N Engl J Med 2005;353:2229e42.
11. Felton V, Borok Z, Willis B. N-acetylcysteine inhibits alveolarepithelial-mesenchymal transition. Am J Physiol Lung CellMolec Physiol 2009;297:L805e12.
12. Cantin A, North S, Fells G, Hubbard R, Crystal R. Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis.J Clin Invest 1987;79:1665e73.
13. Cantin A, Hubbard R, Crystal R. Glutathione deficiency in theepithelial lining fluid of lower respiratory tract in idiopathicpulmonary fibrosis. Am Rev Respir Dis 1988;139:370e2.
14. Behr J, Maier K, Degenkob B, Krombach F, Vogelmeier C.Antioxidative and clinical effects of high-dose N-acetylcys-teine in fibrosing alveolitis. Am J Respir Crit Care Med 1997;156:1897e901.
15. Fu X, Kassim S, Parks W, Heinecke J. Hypochlorous acidgenerated by myeloperoxidase modifies adjacent tryptophanand glycine residues in the catalytic domain of matrix metal-loproteinase-7 (matrilysin). An oxidative mechanism forrestraining proteolytic activity during inflammation. J BiolChem 2003;278:28403e9.
16. Kinnula V, Fattman C, Tan R, Oury T. Oxidative stress inpulmonary fibrosis. A possible role for redox modulatorytherapy. Am J Respir Crit Care Med 2005;172:417e22.
17. Jackson R, Ramos C, Glassberg M, Bejarano P, Gomez-Marin O.Vasodilator therapy and exercise tolerance in idiopathicpulmonary fibrosis: A randomized, placebo controlled trial ofsildenafil. Lung 2010;188:115e23.
18. Leuchte H, Neurohr C, Baumgartner R, Holzapfel M, Giehrl W,Vogeser M, et al. Brain natriuretic peptide and exercisecapacity in lung fibrosis and pulmonary hypertension. Am JResp Crit Care Med 2004;170:360e5.
19. Elin R, Winter W. Laboratory and clinical aspects of b-typenatriuretic peptides. Arch Pathol Lab Med 2004;128:697e9.
20. Lundholm L, Mohme-Lundholm E, Vamos N. Lactic acid assaywith L(þ) lactic acid dehydrogenase from rabbit muscle. ActaPhysiol Scand 1963;58:243e9.
21. Haschke M, Zhang YL, Kahle C, Klawitter J, Korecka M, Shaw L,et al. HPLC-atmospheric pressure chemical ionization MS/MSfor quantification of 15-F2t-isoprostane in human urine andplasma. Clin Chem 2007;53:489e97.
22. Tsikas D. Analysis of nitrite and nitrate in biological fluids byassays based on the Griess reaction: appraisal of the Griessreaction in the L-arginine/nitric oxide area of research. JChromatogr 2007;851:51e70.
23. de Andrade J, Crow J, Viera L, Alexander C, Young K,McGiffin D, et al. Protein nitration, metabolites of reactivenitrogen species, and inflammation in lung allografts. Am JRespir Crit Care Med 2000;161:2035e42.
24. Frei B, Stocker R, Ames B. Antioxidant defenses and lipidperoxidation in human blood plasma. Proc Natl Acad Sci 1988;85:9748e52.
25. Long L, Evan P, Halliwell B. Hydrogen peroxide in human urine:implications for antioxidant defense and redox regulation.Biochem Biophys Res Commun 1999;262:605e9.
26. Basu S. F2-Isoprostanes in human health and diseases: frommolecular mechanisms to clinical implications. Antioxid RedoxSignal 2008;10:1405e34.
27. Becker A, Uckert S, Tsikas D, Noack H, Stief C, Frolich J, et al.Determination of nitric oxide metabolites by means of theGriess assay and gas chromatography-mass spectrometry in thecavernous and systemic blood of healthy males and patients
with erectile dysfunction during different functional conditionsof the penis. Urol Res 2000;28:364e9.
28. Markart P, Luboeinski T, Korfei M, Schmidt R, Wygrecka M,Mahavida P, et al. Alveolar oxidative stress is associated withelevated levels of nonenzymatic low-molecular weight anti-oxidants in patients with different forms of chronic fibrosinginterstitial lung disease. Antioxid Redox Signal 2009;11:227e40.
29. Saleh D, Barnes P, Giaid A. Increased production of the potentoxidant peroxynitrite in the lungs of patients with idiopathicpulmonary fibrosis. Am J Respir Crit Care Med 1997;155:1763e9.
30. Koechlin C, Maltais F, Saey D, Michaud A, LeBlanc P, Hayot M,et al. Hypoxemia enhances peripheral muscle oxidative stressin chronic obstructive pulmonary disease. Thorax 2005;60:834e41.
31. Richardson R, Duteil S, Wary D, Wray D, Hoff J, Carlier P.Human skeletal muscle intracellular oxygenation: theimpact of ambient oxygen availability. J Physiol 2006;571:415e24.
32. Meyer A, Buhl R, Magnussen H. The effect of oral N-ace-tylcysteine on lung glutathione levels in idiopathic pulmonaryfibrosis. Eur Respir J 1994;7:431e6.
33. Meyer A, Buhl R, Kampf S, Magnussen H. Intravenous N-ace-tylcysteine and lung glutathione of patients with pulmonaryfibrosis and normals. Am J Respir Crit Care Med 1995;152:1055e60.
34. Katsoulis K, Kontakiotis T, Leonardopoulos I, Kotsovili A,Legakis I, Patakas D. Serum total antioxidant status in severeexacerbation of asthma: correlation with the severity of thedisease. J Asthma 2003;40:847e54.
35. Nadeem A, Raj H, Chhabra S. Increased oxidative stress andaltered levels of antioxidants in chronic obstructive pulmonarydisease. Inflammation 2005;29:23e32.
36. Cowley H, Bacon P, Pamela J, Goode H, Webster N, Jones G,et al. Plasma antioxidant potential in severe sepsis:a comparison of survivors and nonsurvivors. Crit Care Med1996;24:1179e83.
37. Banerfjee D, Madhusoodanan U, Nayak S, Jacob J. Urinaryhydrogen peroxide: a probable marker of oxidative stress inmalignancy. Clin Chim Acta 2009;334:205e9.
38. Baldus S, Eiserich J, Jackson R, Alexander C, Freeman B.Spatial mapping of nitrotyrosine in vascular and pulmonaryinflammatory diseases reveals a pivotal role for myeloperox-idase as a catalyst for tyrosine nitration in vivo. Free Radic BiolMed 2002;33:1010e9.
39. Cerretelli P, Samaja M. Acid-base balance at exercise in nor-moxia and in chronic hypoxia. Revisiting the "lactateparadox.". Eur J Appl Physiol 2003;90:431e48.
40. Rush J, Turk J, Laughlin M. Exercise training regulates SOD-1and oxidative stress in porcine aortic endothelium. AmJ Physiol Circ Physiol 2003;284:H1378e87.
41. Sen C. Oxidants and antioxidants in exercise. J Appl Phys 1995;79:675e86.
42. McArdle A, van der Meulen J, Close G, Pattwell D, VanRemmen H, Huang T, et al. Role of mitochondrial superoxidedismutase in contraction-induced generation of reactiveoxygen species in skeletal muscle extracellular space. AmJ Physiol, Cell Physiol 2004;286:C1152e8.
43. Vina J, Servera E, Asensi M, Sastre J, Pallardo F, Ferrero J,et al. Exercise causes blood glutathione oxidation in chronicobstructive pulmonary disease: prevention by O2 therapy.J Appl Phys 1996;81:2199e202.
44. Heunks L, Vina J, Van Herwaaden C, Folgering T, Gimeno A,Dekhuijzen R. Xanthine oxidase is involved in exercise-inducedoxidative stress in chronic obstructive pulmonary disease. AmJ Phys 1999;277:R1697e704 (Regulatory Integrative CompPhysiol 46).

1928 R. Jackson et al.
45. McArdle F, Spiers S, Aldemir H, Vasilaki A, Beaver A,Iwanejko L, et al. Preconditioning of skeletal muscle againstcontraction-induced damage: the role of adaptations tooxidants in mice. J Physiol 2004;561:233e44.
46. Mercken E, Hageman G, Schols A, Akkermans M, Bast A,Wouters E. Rehabilitation decreases exercise-induced oxida-tive stress in chronic obstructive pulmonary disease. AmJ Respir Crit Care Med 2005;172:994e1001.