exercise in chronic heart failure Åsa cider med. dr, leg sjukgymnast su/sahlgrenska
TRANSCRIPT
Exercise in chronic heart failure
Åsa CiderMed. Dr, leg sjukgymnast
SU/Sahlgrenska
Chronic heart failure (CHF) a syndrom without perfect definition
Prevalence
0,3 – 2% in different populations Increase with age 10 % vid 80 år
Prognosis
Five years survival 50%
Cowie et al. Eur Heart J
1999;18:208-25

Diagnosis
Symptoms of CHF, typical are dyspnoea and fatigue at rest and during exercise
Objective signs of heart dysfunction at rest
Improved by medication
Remme, Swedberg. Eur Heart J;
2001;22: 1527-60
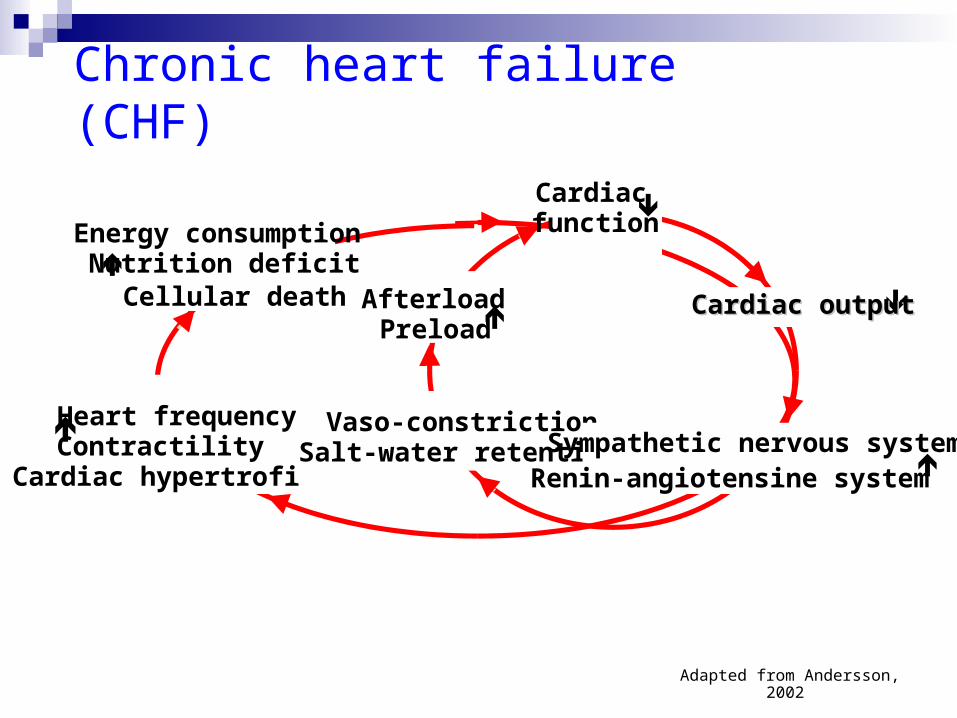
Chronic heart failure (CHF)
Adapted from Andersson, 2002
Energy consumption
Nutrition deficit Cellular death
Vaso-constrictionSalt-water retention
Heart frequencyContractility
Cardiac hypertrofi
Sympathetic nervous systemRenin-angiotensine system
Cardiacfunction
Cardiac outputCardiac outputAfterloadPreload

Why ?
Should patients with CHF exercise?
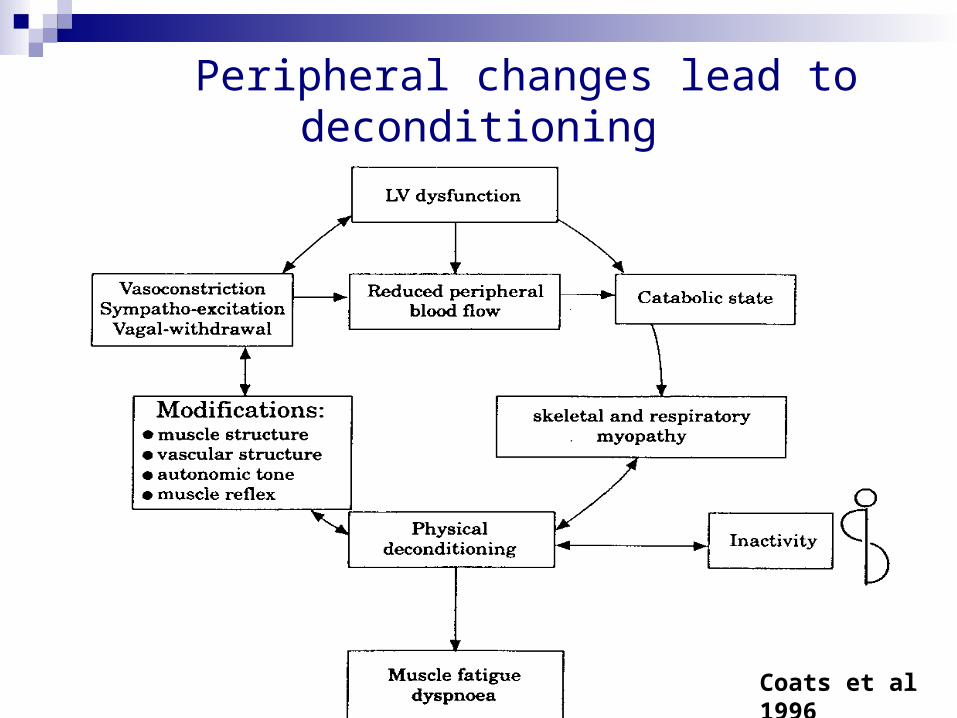
Peripheral changes lead to deconditioning
Coats et al 1996
Effects of exercise in patients with chronic heart failure Increased VO2 and work rate Increased gait velocity Increased muscle function Reduced levels of sympathetic hormones Increased endothelial function Symptom reduction and increased quality
of life
Eur Heart J 2001;22:125-35.

Juenger et al. Heart 2002;87:235-41
QoL is reduced in Chronic heart failure (CHF)

Juenger et al. Heart 2002;87:235-41

Who?
Should all patients with CHF exercise?

Patients with CHF
Stable CHF
NYHA I-III
NYHA IV?Eur Heart J 2001;22:125-35.
Circulation 2003;107;1210-25
Cochrane;2004

How?
Should patients with chronic heart failure exercise?
Any bodily movement produced by skeletal muscles that result in energy expenditure.
A subset of physical activity that is planned, structured, repetitive, and purposeful in the sense that improvement or maintenance of physical fitness is the objective
Physical activity Exercise
Casparsen, C. Public health report. 1985
The principles of training
The principle of individuality
The principle of specificity
The principle of disuse
The principle of progressive overload
The principle of hard/easy
The principle of periodization
Wilmore and Costhill 2001
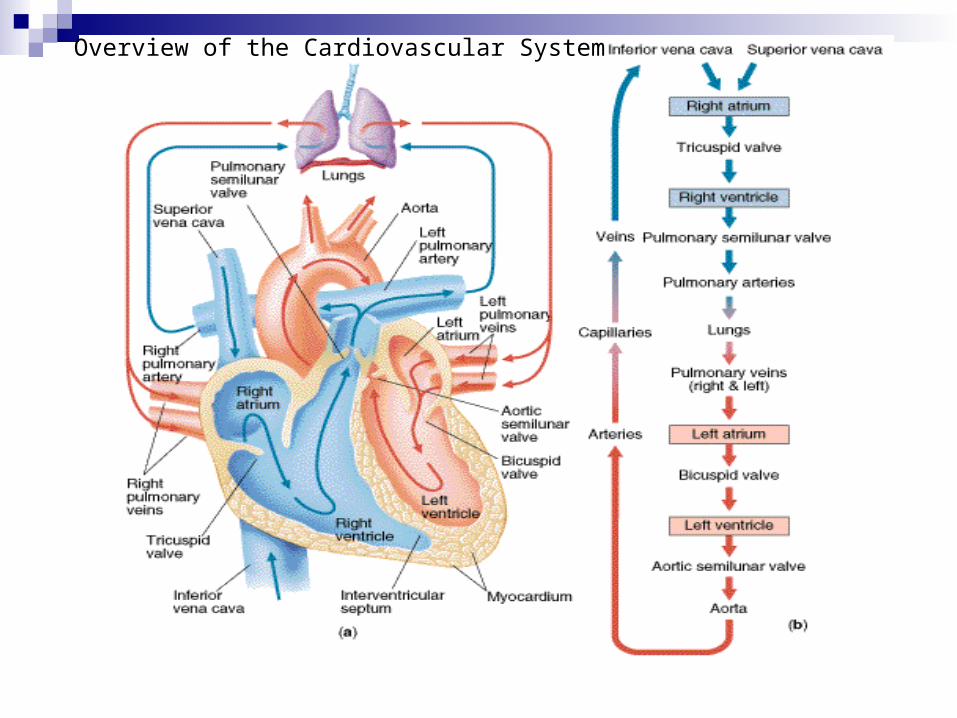
Overview of the Cardiovascular System
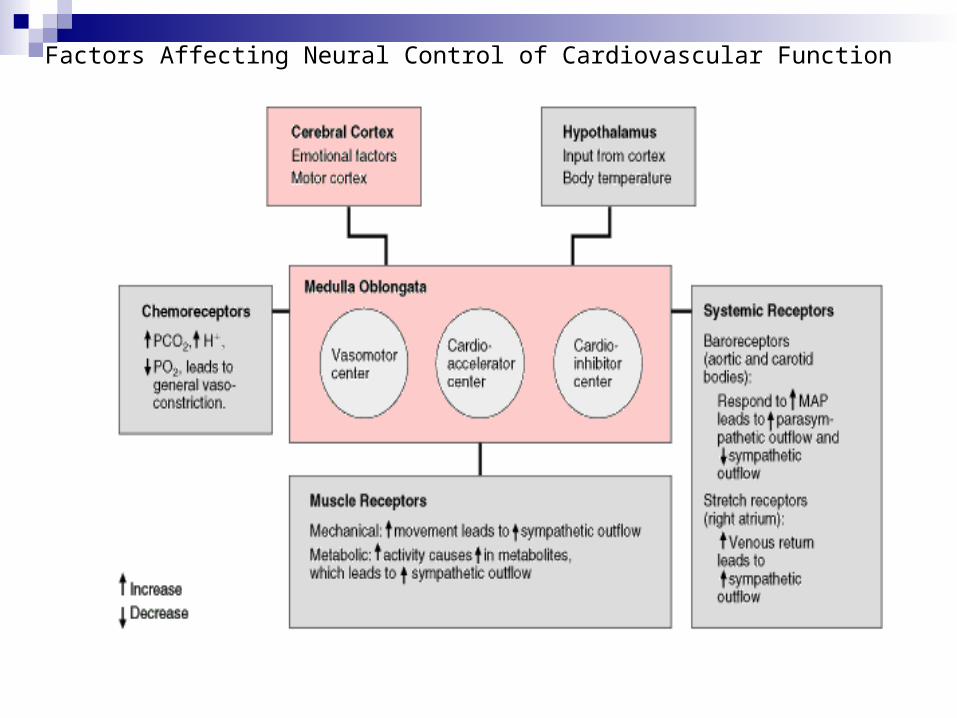
Factors Affecting Neural Control of Cardiovascular Function


(4-6x) C.O
(2-4x) HR
20-50%SV (at least 100ml)
Frank Starling mechanism of EDV and ESV
Contractility Peripheral vasodillation
Circulatory respones due to exercise in healthy persons
Adapted fromCirculation 2003;107;1210-25
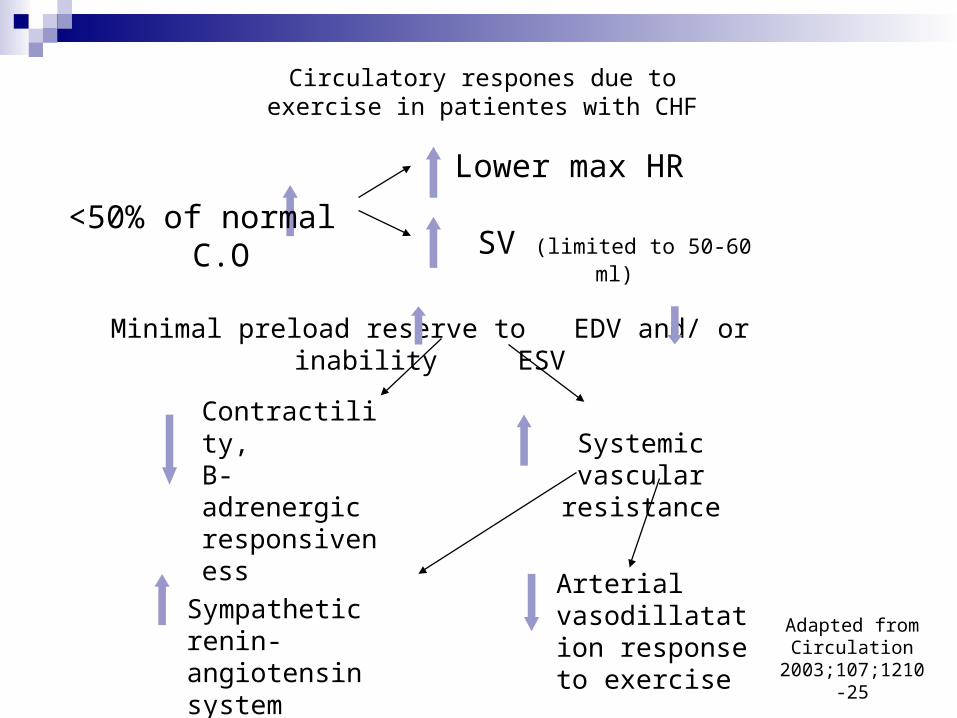
<50% of normal C.O
Lower max HR
SV (limited to 50-60 ml)
Minimal preload reserve to EDV and/ or inability ESV
Contractility,Β-adrenergic responsiveness
Systemic vascular resistance
Sympathetic renin- angiotensin system
Arterial vasodillatation response to exercise
Circulatory respones due to exercise in patientes with CHF
Adapted fromCirculation
2003;107;1210-25

CHF and 2DM
More reduced physical performance
Adapted from: Guazzi. Am J Cardiol. 2002
Control CHF CHF and 2DM
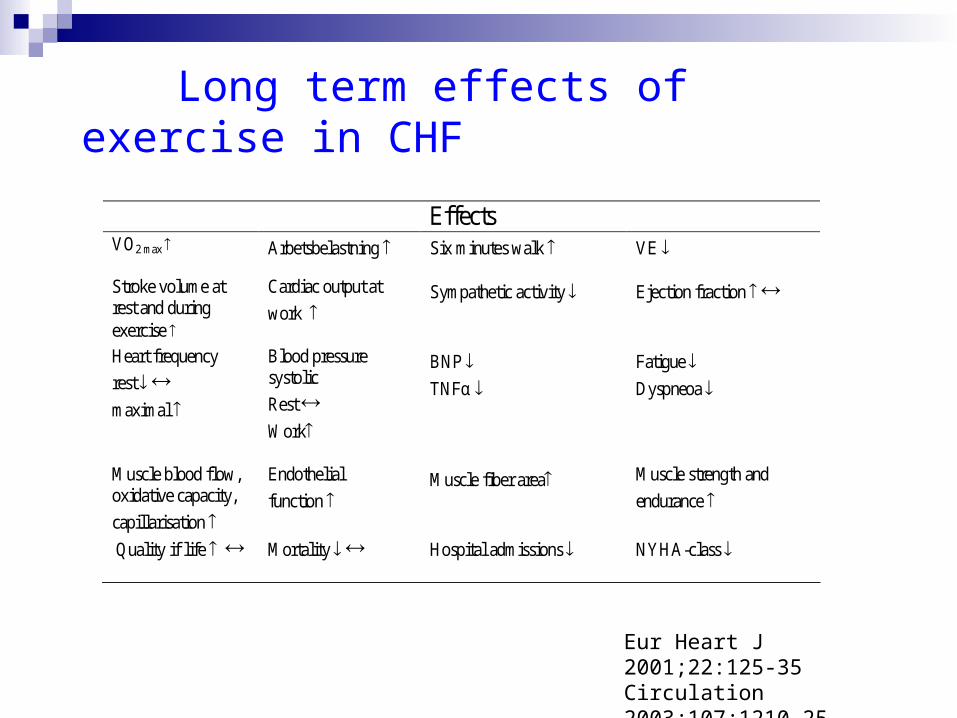
Long term effects of exercise in CHF
Eur Heart J 2001;22:125-35Circulation 2003;107;1210-25Cochrane 2004 2004(3):CD003331
Effects VO2 max
Arbetsbelastning Six minutes walk VE
Stroke volume at rest and during exercise
Cardiac output at
work
Sympathetic activity
Ejection fraction
Heart frequency
rest
maximal
Blood pressure systolic
Rest
Work
BNP
TNFα
Fatigue
Dyspneoa
Muscle blood flow, oxidative capacity,
capillarisation
Endothelial
function
Muscle fiber area Muscle strength and
endurance
Quality if life Mortality Hospital admissions NYHA-class

Assessment of physical function
Exercise test
Six minute walk6MWT Submaximalt test Guyatt Can Med Assoc J 1985;132:919-23. Lipkin BMJ 1986;292:653-5 Korrelerar väl med V02 och överlevnad. Cahalin 1996;110:325-32. Reproducerbarheten varierar i olika studier. ”Takeffekt”
Referensekvation finns för friska Enright Am J Resp Crit Care 1998;158:1384-7.
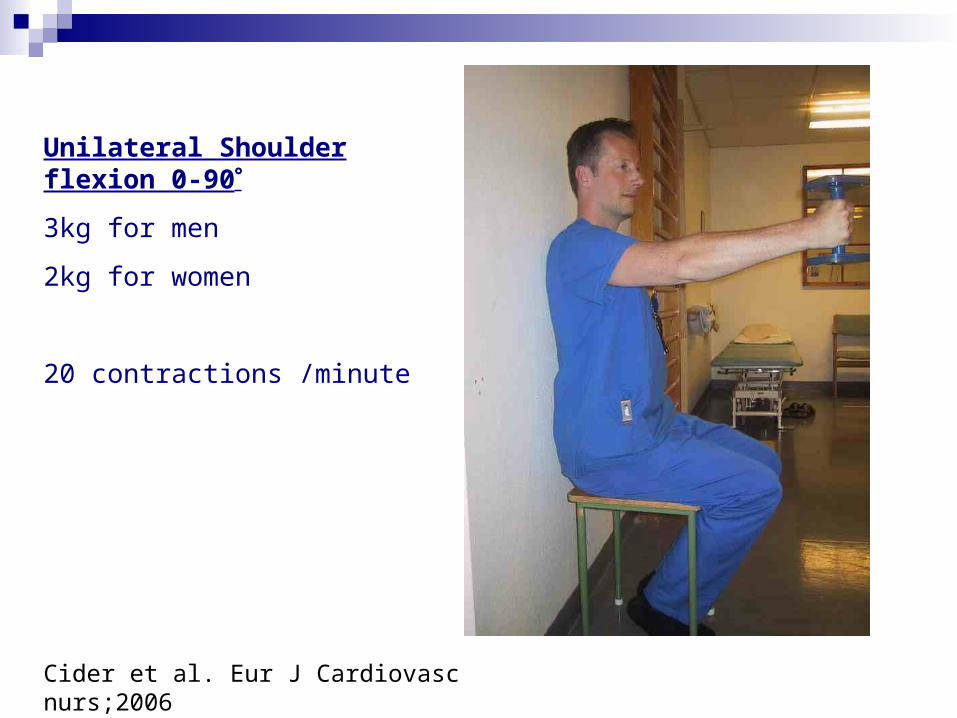
Unilateral Shoulder flexion 0-90
3kg for men
2kg for women
20 contractions /minute
Cider et al. Eur J Cardiovasc nurs;2006

Isotonic unilateral heel lift
10 tilted wedge
head should meet the length measurer arm
30 lifts/minute

Isometric bilateral 90 shoulder abduction
with a one kg dumbell in each hand

Central circulatory traning
Peripheral muscle traning
Combined peripheral and central circulatory training
Respiratory-muscle traning
Land Water Eur Heart J 2001;22:125-35Circulation 2003;107;1210-25 Cochrane 2004(3):CD003331
Tai Chi
Electric stimulation
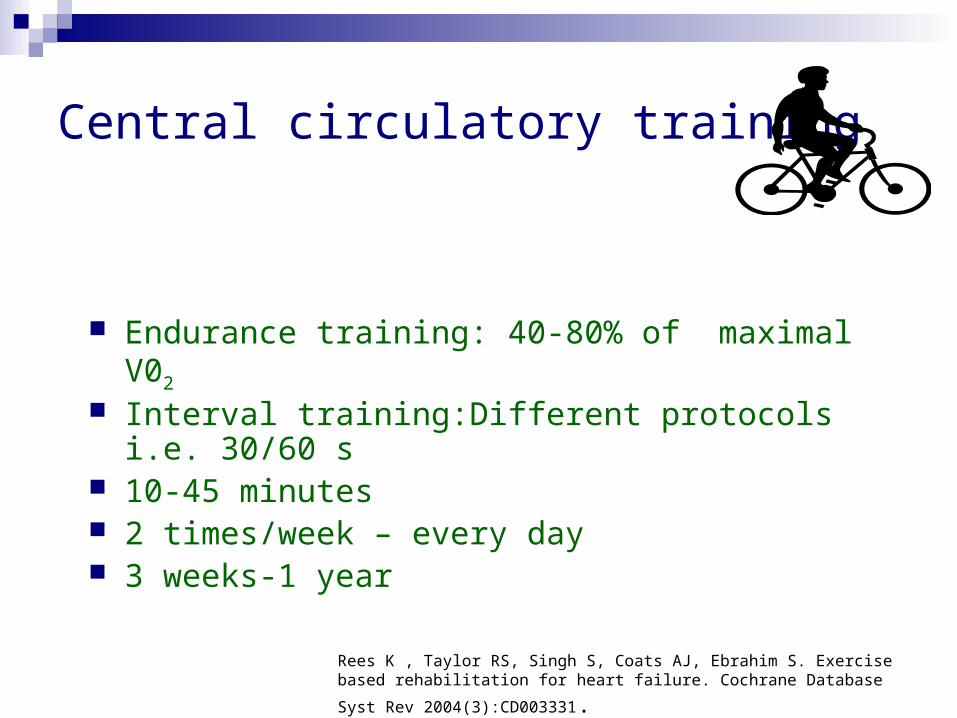
Central circulatory training
Endurance training: 40-80% of maximal V02
Interval training:Different protocols i.e. 30/60 s 10-45 minutes 2 times/week – every day 3 weeks-1 year
Rees K , Taylor RS, Singh S, Coats AJ, Ebrahim S. Exercise based rehabilitation
for heart failure. Cochrane Database Syst Rev 2004(3):CD003331.
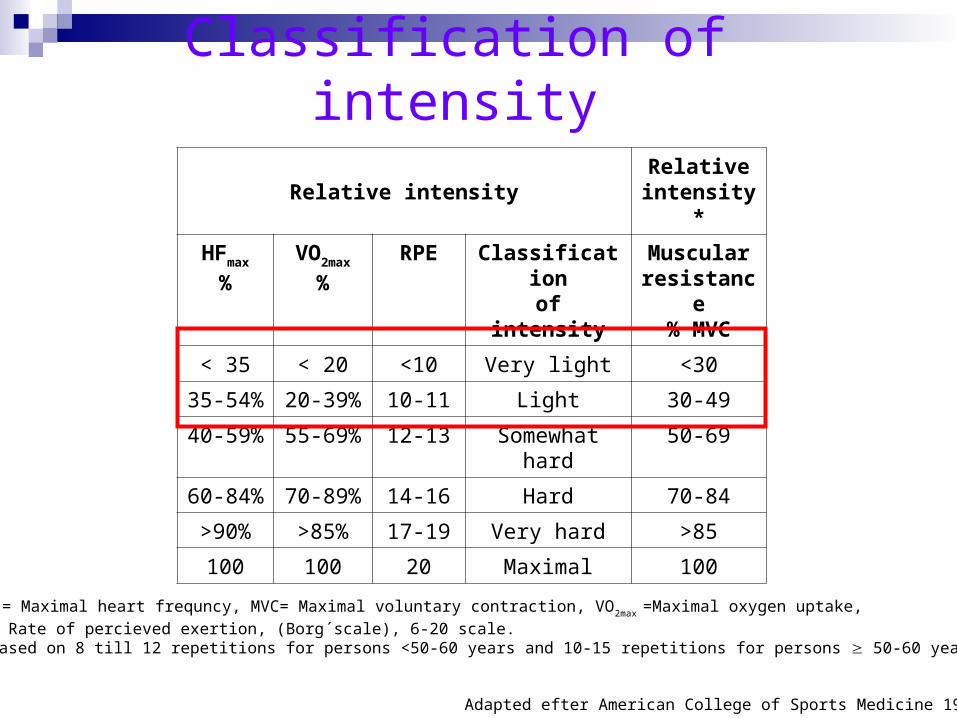
Classification of intensity
Adapted efter American College of Sports Medicine 1998
Relative intensityRelative
intensity*
HFmax
%
VO2max
%
RPE Classificationof intensity
Muscular resistance
% MVC
< 35 < 20 <10 Very light <30
35-54% 20-39% 10-11 Light 30-49
40-59% 55-69% 12-13 Somewhat hard
50-69
60-84% 70-89% 14-16 Hard 70-84
>90% >85% 17-19 Very hard >85
100 100 20 Maximal 100
HFmax = Maximal heart frequncy, MVC= Maximal voluntary contraction, VO2max =Maximal oxygen uptake,
RPE= Rate of percieved exertion, (Borg´scale), 6-20 scale.*= Based on 8 till 12 repetitions for persons <50-60 years and 10-15 repetitions for persons 50-60 years.
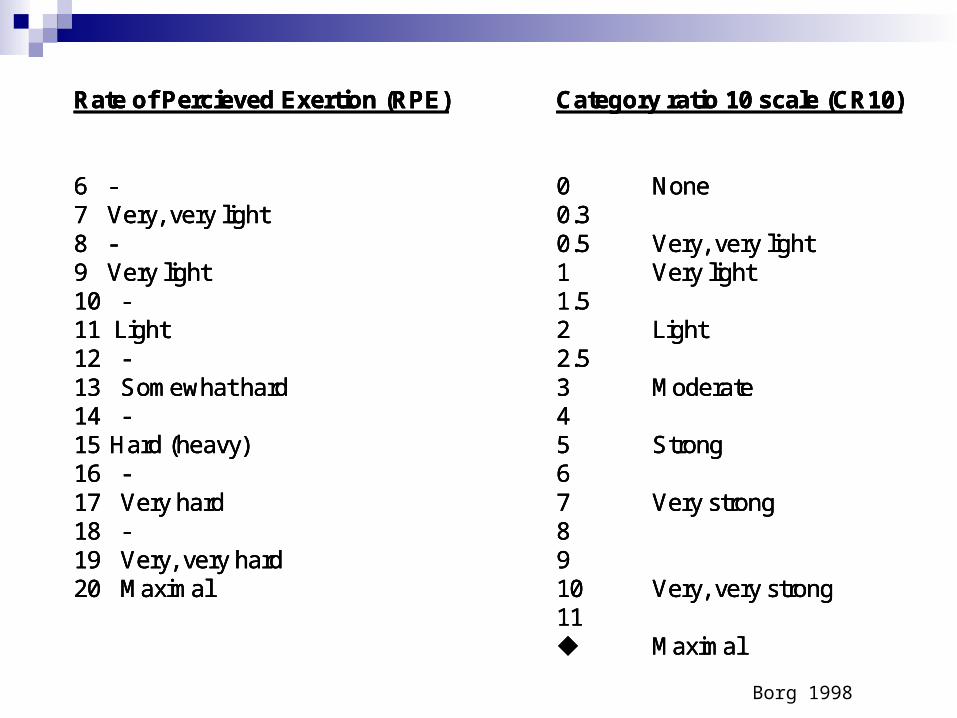
Rate of Percieved Exertion (RPE)
6 -7 Very, very light8 -9 Very light10 -11 Light12 -13 Somewhat hard14 -15 Hard (heavy)16 -17 Very hard18 -19 Very, very hard20 Maximal
Category ratio 10 scale (CR10)
0 None0.30.5 Very, very light1 Very light1.52 Light2.53 Moderate45 Strong67 Very strong8910 Very, very strong11 Maximal
Rate of Percieved Exertion (RPE)
6 -7 Very, very light8 -9 Very light10 -11 Light12 -13 Somewhat hard14 -15 Hard (heavy)16 -17 Very hard18 -19 Very, very hard20 Maximal
Category ratio 10 scale (CR10)
0 None0.30.5 Very, very light1 Very light1.52 Light2.53 Moderate45 Strong67 Very strong8910 Very, very strong11 Maximal
Rate of Percieved Exertion (RPE)
6 -7 Very, very light8 -9 Very light10 -11 Light12 -13 Somewhat hard14 -15 Hard (heavy)16 -17 Very hard18 -19 Very, very hard20 Maximal
Category ratio 10 scale (CR10)
0 None0.30.5 Very, very light1 Very light1.52 Light2.53 Moderate45 Strong67 Very strong8910 Very, very strong11 Maximal
Borg 1998
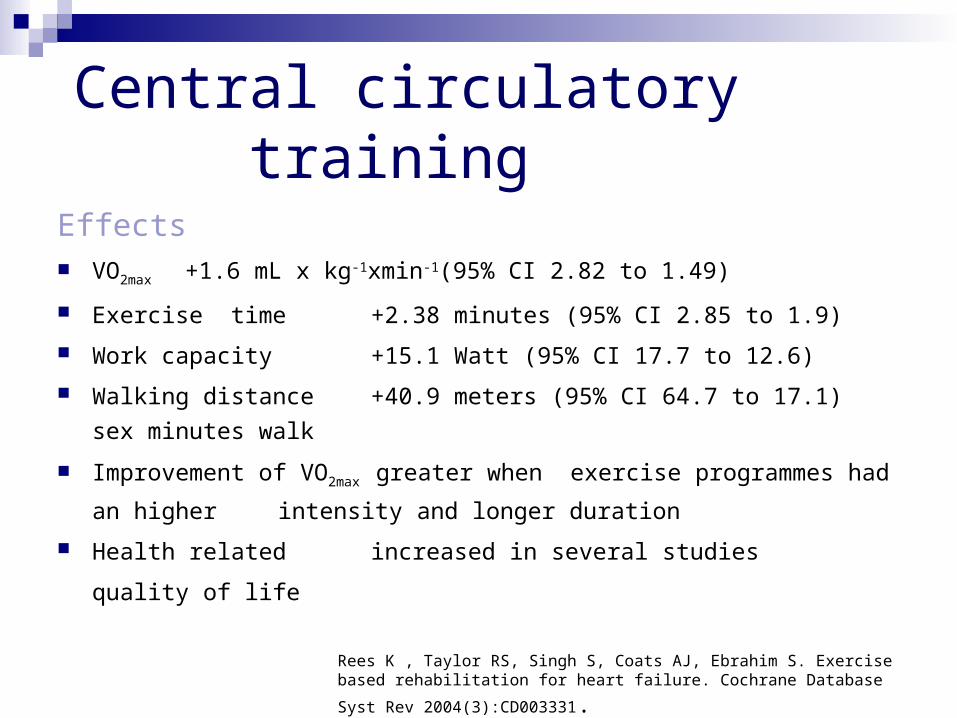
Central circulatory training
Effects VO2max +1.6 mL x kg-1xmin-1(95% CI 2.82 to 1.49)
Exercise time +2.38 minutes (95% CI 2.85 to 1.9)
Work capacity +15.1 Watt (95% CI 17.7 to 12.6)
Walking distance +40.9 meters (95% CI 64.7 to 17.1)
sex minutes walk
Improvement of VO2max greater when exercise programmes had an higher
intensity and longer duration
Health related increased in several studies
quality of life
Rees K , Taylor RS, Singh S, Coats AJ, Ebrahim S. Exercise based rehabilitation
for heart failure. Cochrane Database Syst Rev 2004(3):CD003331.
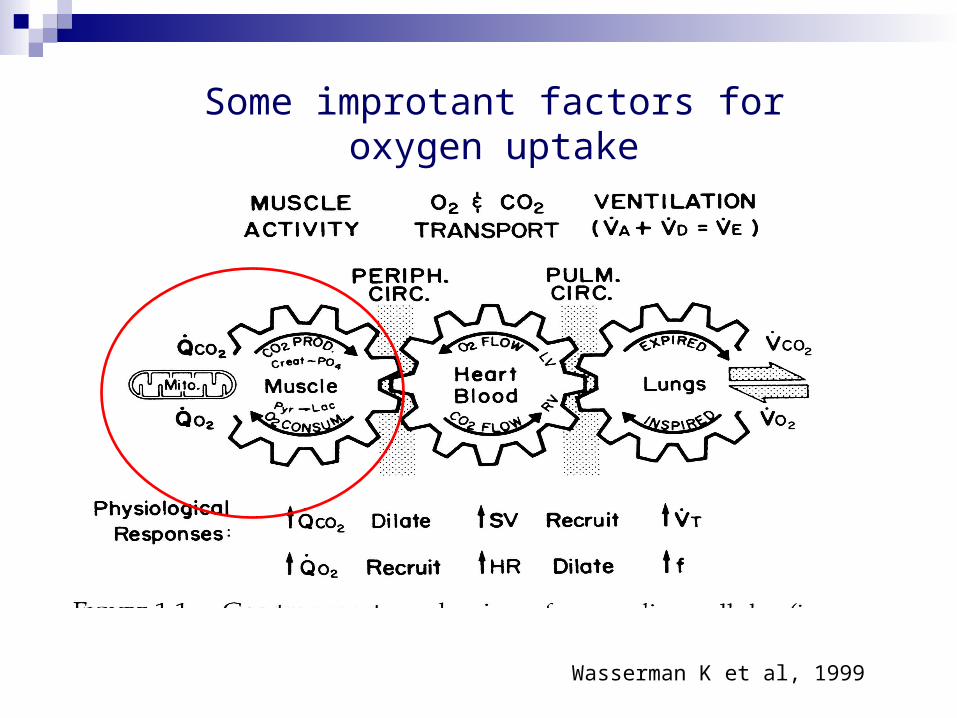
Wasserman K et al, 1999
Some improtant factors for oxygen uptake

Peripheral muscle traning
A high relative load on individual muscle groups while maintaining low central circulatory stress levels
Gaffney et al 1982
Pulley exercise
Exercise with dumb- bells
Exercise in Quadriceps table

Repetitions Maximum (RM)
Repetitions, Repetitions, resistanceresistance and expected effectand expected effect
RepetitionsRepetitions 1 2 3 51 2 3 5 77 1010 2525 5050
Resistance inResistance in 100 95 90 85 80100 95 90 85 80 7070 5050 3030% of 1 RM% of 1 RM
EffectEffect maximal strengthmaximal strength muscle growthmuscle growth enduranceendurance
coordinationcoordination
Adapted from: Karlsson J, Thommé R et al 1998
Repetition Maximum
Repetitions, Repetitions, resistanceresistance and expected effectand expected effect
RepetitionsRepetitions 1 2 3 51 2 3 5 77 1010 2525 5050
Resistance inResistance in 100 95 90 85 80100 95 90 85 80 7070 5050 3030% of 1 RM% of 1 RM
EffectEffect maximal strengthmaximal strength muscle growthmuscle growth enduranceendurance
coordinationcoordination
Adapted from: Karlsson J, Thommé R et al 1998
Repetition Maximum

Peripheral muscle traning
35 -80% of one Repetition Maximum (1 RM) 2-7 times/week 15-60 minutes 8 weeks – 5 months
Delagardelle C, Feiereisen P. Eura Medicophys 2005;41(1):57-65.
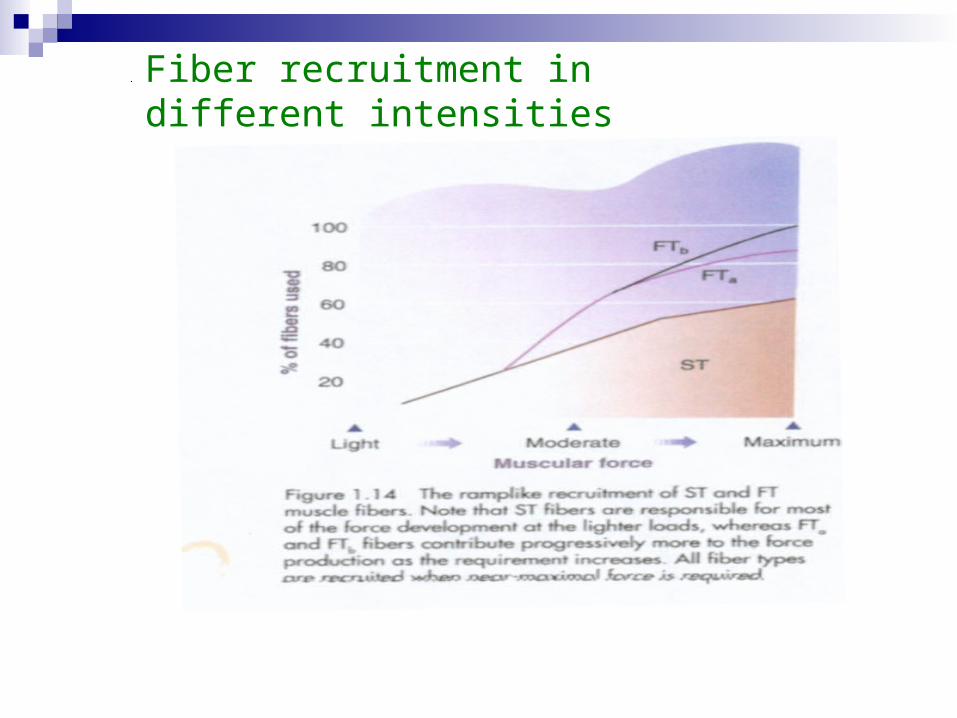
Fiber recruitment in different intensities

Combined central circulatory andperipheral training
Ergometer and peripheral muscle training
3 times a week 60 minutes 3 months
Dellagarede 1999, Hare 1999, Maiorana 2001, Dellagarde 2002, Senden 2005
Hydrotherapy
Could it be incorporated in the rehabilitation of patients with chronic heart failure?
Cider et al Eur J Heart Fail.2003;5(4):527-35.Cider et al. Clin Physiol Funct Imaging. 2005;25(6):313-7.Cider et al. Eur J Heart Fail. 2006 May;8(3):308-13
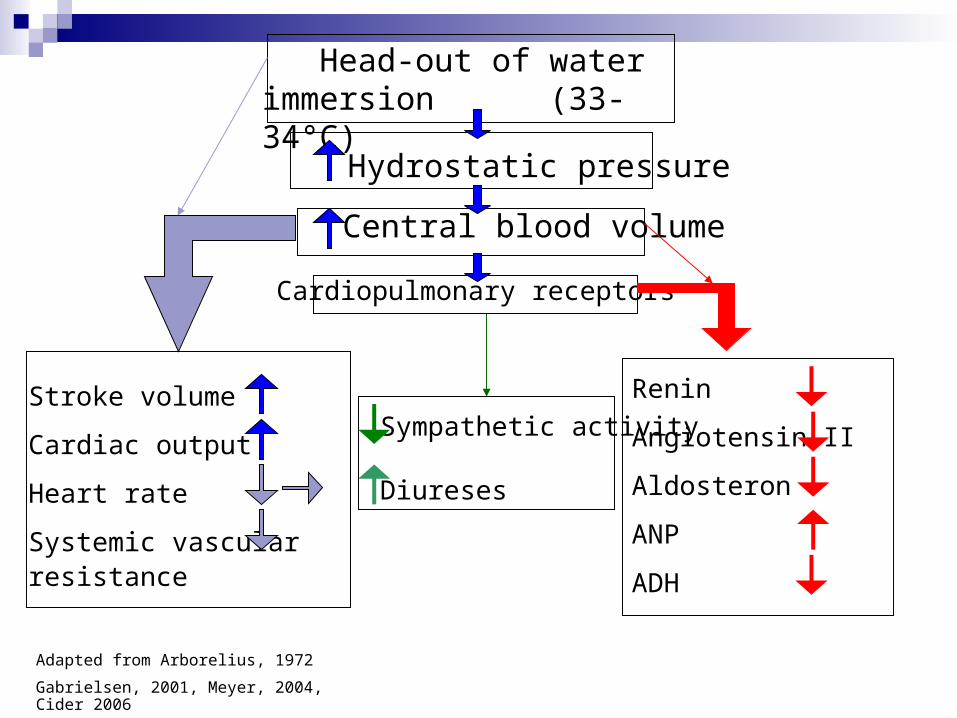
Head-out of water immersion (33-34°C)
Central blood volume
Hydrostatic pressure
Adapted from Arborelius, 1972
Gabrielsen, 2001, Meyer, 2004, Cider 2006
Stroke volume
Cardiac output
Heart rate
Systemic vascular resistance
Cardiopulmonary receptors
Renin
Angiotensin II
Aldosteron
ANP
ADH
Sympathetic activity
Diureses

Respiratory muscle exercises
Inspiration and/or expiration exercises Duration/exercise occasion:15-30
minutes Frequency:6 times/day- 3 times/week Long term duration:6 weeks -3 months
Mancini 1995, Johnsson 1998, Martinez 2001, Laoutaris 2004, Dall‘Ago P 2006.
Other training modalities
Tai Chi Electric stimulation
Conclusion Exercise should be incoperated in the
medical treatment in CHF.
Central circulatory training improves VO2.
Peripheral muscle training improve sceletal muscle function.
Hydrotherapy improves VO2 as well as sceletal muscle function

Patient cases
Athens 2006

Svea 82 years
Ischemic heart diease 1995 ( myocardial infarction) CHF 1998, EF 40% Diabets type 2 1999 Polyneuropathy, problems with gait Depressed mood Exercise -ECG 40 w, need to stop due to dyspneoa and
leg fatigue

Olle, 44 years Cardiomyopathy 2005 EF 20% Used to be healthy Exercised occasionally the last 10 years, mostly
jogging and floorball
Exercise-ECG 200 w, no signs of ischemia, HFmax 130, BPmax 185/-. Discontinue due to leg fatigue

Leif 72 years
Ischemic heart disease since 20 years back, CHF since 4 years back PCI x 5 and CABG x 2 Suffering from angina while exercising Inoperable Exercise-ECG, Pronounced ST-changes at
50 w, HF 88, BP 140/-
Metabolic equivalent (MET)
1MET=1.0kcal(4.184kJ)/kg/h eller
3.5 mLO2 x kg-1x min-1
Lätt fysisk aktivitet:<3METs Moderat fysisk aktivitet: 3-6 METs Kraftig Fysisk aktivitet>6 METs
Ainsworth BE et al. Med Sci Sports Exerc 2002;32(Suppl):S498-S516.

<2METs
2METs
3METs
4Mets
5Mets
Resting EatingMoving in bedSitting on the edge of the bed
Adapted from: Woods Cardiac nursing; 2004
Standing and transfering to chairChair exercises
Self care Walking in room
Walking 3km/h indoors
Climbing a flight of stairs

Functional class
O2 cost mLO2 x kg-1x min-1
METS Bicycle Ergometer
watt
56.0 16 52.5 15 49.0 14 45.5 13
250
42.0 12 38.5 11 200 35.0 10 31.5 9 28.0 8
150
24.5 7
Normal and
functional- class I
21.0 6 100 2 17.5 5 75
14.0 4 10.5 3
3
7.0 2
50 25
4 3.5 1