expenditure tracking survey - social …saatlas.org/uploads/files/aer_pets_final_report.pdf · pets...
TRANSCRIPT

Page 0
PUBLIC EXPENDITURE TRACKING SURVEY
A STUDY OF THE SPONSORED PROGRAM NATIONAL HEALTH INSURANCE PROGRAM
(PHILIPPINES)
ACTION FOR ECONOMIC REFORMS
DECEMBER 2013
A PROJECT SUPPORTED BY US-AID IN COOPERATION WITH RESULTS FOR
DEVELOPMENT (R4D) AND THE Bandung Institute of Governance Studies (BIGS)

Page 1
Table of Contents
Acronyms ……………………………………………………………… 2
Acknowledgements ………………………………………………. 3
Introduction …………………………………………………………. 4
Study Objectives and Methodology ………………………. 9
PETS Results …………………………………………………………. 13
A. Budget Tracking at the National Level …………….. 13
B. Funding Flow from Fund Source to PhilHealth … 15
C. Funding flow on Reimbursement of Claims ……. 18
D. Survey of Beneficiaries ……………………………………. 23
Summary of Findings ……………………………………………. 29
Recommendations ………………………………………………. 31
References ………………………………………………………….. 33

Page 2
Acronyms AER Action for Economic Reforms AHA Aquino Health Agenda COA Commission on Audit DBM Department of Budget and Management DOF Department of Finance DOH Department of Health DSWD Department of Social Welfare and Development FY Fiscal Year GAA General Appropriations Act GOCC Government-Owned and Controlled Corporation HCP Health Care Provider HSRA Health Sector Reform Agenda IRR Implementing Rules and Regulations LGU Local Government Unit LHIO Local Health Insurance Office MCP Maternity Care Package MDGs Millennium Development Goals MDR Membership Data Record NBB No Balance Billing NCA Notice of Cash Allocation NDHS National Demographic and Health Survey NHIC National Health Insurance Corporation NHIP National Health Insurance Program NHTS-PR National Household Targeting System for Poverty Reduction NSCB National Statistical Coordination Board PCB Primary Care Benefit PETS Public Expenditure Tracking Survey PRO Philhealth Regional Office RA Republic Act RHU Rural Health Unit SARO Special Allotment Release Order SP Sponsored Program TB Tuberculosis

Page 3
Acknowledgements
This study is part of a three-year project of Action for Economic Reforms (AER) in cooperation with Results for Development Institute (R4D) and the Bandung Institute of Governance Studies (BIGS
). AER would like to express its deepest appreciation to all those who contributed to and supported the preparation and completion of this research.
We acknowledge the valuable contribution of colleagues from R4D and BIGS who accompanied us in this project, providing guidance and encouragement at every step of the way. We, likewise, acknowledge the input and comments of peers from partner organizations in different Southeast Asian countries who were part of this cooperation project. We note the animated discussions among colleagues and peers during the learning and sharing sessions that were organized under this project. The AER project team is grateful to the pool of consultants and advisors who offered valuable time and insights in developing the research design and in enriching the analysis. We acknowledge the assistance extended by Social Watch Philippines (SWP) and the Philippine Rural Reconstruction Movement (PRRM) in facilitating links with key national agencies and local government units. We are, likewise, thankful to the survey team who diligently reviewed relevant documents, conducted the interviews, and processed the data. The project team is especially grateful to the United States Agency for International Development (USAID) for its generous assistance extended to civil society organizations and its support to budget transparency and development initiatives in this part of the world. Finally, we express our deep gratitude to PhilHealth, the Department of Health, the Department of Finance, the City Governments of Paranaque, and the Municipal Governments of Baao, Camarines Sur, Sta. Rosa, Nueva Ecija, and Angono, Rizal. This research would not have been possible without the cooperation and assistance extended by these agencies to the project team. The AER Project Team Rene R. Raya, Ma. Luz R. Anigan and Caridad Janet R.
Carandang

Page 4
Introduction The Philippines continues to face serious challenges in improving the health situation of Filipinos, particularly the poorest among them. As of 2011, the prevalence of underweight children under 5 years of age stood at 20.2%, while under-five and infant mortality rates were recorded at 30 and 22 deaths per 1,000 live births, respectively. Maternal mortality remains high at 95-163 deaths per 100,000 (2010) while deaths associated with tuberculosis stood at 27.6 deaths per 100,000 population (2009). The latest Philippine MDG assessment noted that the country will likely miss the MDG health targets on hunger and nutrition, maternal mortality and infectious diseases, particularly tuberculosis. (NSCB, 2013) Poverty remains pervasive especially in rural communities and urban slums with consequent impact on the health situation of the poor. As of 2012, 25.2% of Filipinos were living below the poverty threshold of P52 per day or about US$1.25/day (NSCB, 2013). New vulnerabilities in health emerged as a result of series of disasters that badly hit most areas of the country in recent years. Inequities in health access and outcomes persist and are most apparent by economic status, educational level and geographical location. The latest National Demographic and Health Survey (NDHS, 2008) shows that under-five mortality rates are significantly higher in rural areas (nearly twice compared to urban areas) and among the poorest income quintile (more than 3 times compared to the richest quintile). The incidence of death of children whose mothers have no education is more than 7 times compared to those whose mothers have attended college. Similarly, the risks associated with pregnancy and childbirth are much higher among poor women. The poorest 20% are six times more likely to deliver at home and are 14 times more likely to be attended by traditional birth attendants compared to the richest 20%. The Nationwide Tuberculosis Prevalence Survey (TFDI, 2007) also noted that the lowest income groups are 1.4 times more likely to be positive for tuberculosis compared to the highest income groups. By geographical location, richer regions of the country such as the National Capital Region and the nearby regions of Central Luzon and Calabarzon have the highest number and most advanced health facilities. In comparison, the poorer regions, specifically Muslim Mindanao and Eastern Visayas, have far lesser health facilities and with fewer available health services. It is against this backdrop that the current administration of President Aquino responded to the challenge by formulating and implementing its agenda for the health sector. The (President) Aquino Health Agenda (AHA) is directed towards ensuring the achievement of Universal Health Care through better health outcomes, sustained health financing and responsive health system focusing especially on the poor and disadvantaged groups. It builds on the previous health reform strategies Health Sector Reform Agenda (HSRA) in 1999, and FOURmula One (F1) for Health in 2005. The health reform currently being implemented by the current administration shall: 1) strengthen the National Health Insurance Program (NHIP) to enhance financial risk protection especially among the poor; 2) improved access to quality hospitals and health care facilities, and; 3) attaining health-related MDGs, focusing on reducing maternal and child mortality, morbidity and mortality from TB and malaria, and the prevalence of HIV/AIDS, in addition to being prepared for emerging disease trends, and prevention and control of non-communicable diseases. The goal of universal healthcare is to provide efficient, accessible, equitable, and adequately funded health services to an informed and empowered citizenry. Thus, every Filipino, regardless of their socio-economic status, is able to get the preventive care and treatment needed with the same level of quality without discrimination. To realize this goal, health facilities and services must be accessible geographically with sufficient number of facilities and qualified health staff.

Page 5
Health financing provides the biggest challenge in achieving universal health care. The enactment of Republic Act 10351 (more popularly known as the Sin Tax Law) in December 2012 is, therefore, seen as a major breakthrough as it offers a great opportunity of having more resources available for health care from increased taxes on tobacco and alcohol. The law allocates a significant share of the incremental revenue for universal health care, specifically to fund and expand health insurance for the poor, to improve health facilities and to attain health MDGs. In 2012 and 2013, a little over Php 12 billion was allocated to the Philippine Health Insurance Corporation (PhilHealth) to support the government’s Sponsored Program which caters to the poorest 20% Filipinos. By 2014, the allocation increased substantially to Php 35.34 billion1
to expand PhilHealth’s Sponsored Program to cover the next 20% poorest Filipinos and other marginalized and vulnerable sectors of society such as persons with disabilities, and survivors of conflicts and disasters.
This study is designed to tract the funds generated from the Sin Taxes and ensure the transparency, feasibility, effectiveness and social desirability of the expanded coverage of PhilHealth’s Sponsored Program and, thus, guarantee prompt, effective and free delivery of health services to the poorest Filipino households. The Policy Environment for Universal Health Care Article XIII of the 1987 Constitution of the Republic of the Philippines declares that the State shall adopt an integrated and comprehensive approach to health development which shall endeavor to make essential goods, health and other social services available to all the people at affordable cost. Priority for the needs of the underprivileged, sick, elderly, disabled, women and children shall be recognized. Likewise, it shall be the policy of the State to provide free medical care to paupers. The National Health Insurance Program
. In 1995, Republic Act 7875 or the National Health Insurance Act was adopted by the Philippine Government and subsequently amended by Republic Act 9241. The law established the National Health Insurance Program (NHIP) as a mandatory health insurance program of the government designed to provide universal health insurance coverage for Filipino citizens. The law designates the Philippine Health Insurance Corporation (PhilHealth) to implement the program with the following objectives:
a. provide all citizens of the Philippines with the mechanism to gain financial access to health services; b. establish the NHIP to serve as the means to help the people pay for health care services; and c. prioritize and accelerate the provision of health services to all Filipinos, especially that segment of the population who cannot afford these services. The NHIP covers the following beneficiaries: employed members in the government and private sectors; individually paying members; retirees under the Lifetime member program; members of the Overseas Workers Program and indigent members covered by the Sponsored program. Also included as beneficiaries are these members’ dependents – children below 21 years old and parents over 60 years old. The Aquino Health Agenda
1 PhilHealth’s budget for the Sponsored Program is expected to further increase as taxes continue to increase annually.
. In December 2010, the new administration under President Aquino launched the “Aquino Health Agenda: Achieving Universal Health Care for All Filipinos" designed to improve, streamline and scale up reforms in the health sector with deliberate focus on the poor to
Page 6
ensure that nobody is left behind as the implementation of health reforms moves forward. The initiative seeks to address inequities in health outcomes by ensuring that all Filipinos, especially those belonging to the lowest two income quintiles, have equitable access to quality health care. It is designed to strengthen the National Health Insurance Program by improving financial risk protection of the poorest. The success of this initiative shall be measured by the progress made in preventing premature deaths, reduce maternal and newborn deaths, controlling both communicable and non-communicable diseases, improvements in access to quality health facilities and services and increasing NHIP benefit delivery rate, prioritizing the poor and the marginalized. In August 2011, the Department of Health came out with the implementation roadmap of the Aquino Health Agenda which identified three phases: 1) launching phase (August 2010-December 2011); 2) Scale-up phase (2012-2013); and, 3) sustainability phase (2014-2016). Target outputs were set for each phase and for each year with the following highlights:
- Implementation of No Balance Billing policy for indigent families - Expansion of the outpatient primary care benefits - Increase coverage of the Sponsored Program - Upgrading of rural health units and district, provincial, and DOH-retained hospitals - Attainment of all MDG health goals
The Sin Tax Law
. Republic Act 10351 or the Sin Tax Law, signed into law on December 20, 2012 by President Aquino, is designed as both a revenue and health measure. The law allocates a significant portion of the incremental revenue generated from increased excise taxes on tobacco and alcohol to fund the government’s universal healthcare agenda, while curbing the incidence of cigarette smoking especially among poor and young Filipinos.
The Department of Finance projected that in the first year of implementation, the government expects to collect P34 billion in incremental revenue from excise taxes on cigarette and alcohol products. Of this amount, about 80% is earmark for universal health care and health facilities enhancement. The bulk of the fund is allocated to fund PhilHealth’s Sponsored Program. In terms of health objectives, the Department of Health projects a substantial reduction of tobacco consumption in the Philippines which currently causes the deaths of 87,600 Filipinos annually. The Implementing Rules and Regulation (IRR) of the Sin Tax Law was approved and signed on 18 January 2014 by the heads of the five concerned agencies, including the Department of Health and PhilHealth. Under the IRR, the Department of Health was tasked to identify the annual funding requirements for financial risk protection, health programs, medical assistance and health facilities enhancement. The department is also required to submit a list of projects and programs to be implemented for the universal health care program, including funding requirements and guidelines for prioritization. The New PhilHealth Law, The National Health Insurance Act of 2013 (Republic Act 10606). The Philippine Health Insurance Corporation (PhilHealth) was established on February 14, 1995 as a Government-Owned and Controlled Corporation (GOCC) to administrate the National Health Insurance Program (NHIP). The law was amended in 2013 to incorporate the key strategies of the Aquino Health Agenda. NHIP is the compulsory health insurance program of the government that provides universal health insurance coverage and ensures affordable, acceptable, available and accessible health care services for all citizens of the Philippines (IRR of R.A. 10606).2
2 Discussions in this section on Philhealth are based on the Implementing Rules and Regulations of R.A. 10606.

Page 7
PhilHealth’s primary purpose is to ensure that all Filipinos, especially those who cannot afford the cost of health care, are given real financial risk protection. Its key functions are:
• Enrol all Filipino citizens covered under the NHIP; • Coordinate with the other government agencies, specifically DOH, DSWD and LGUs for the
enrollment and coverage of eligible indigents, sponsored members and those members in the informal economy;
• Establish a system of accreditation of health facilities and health personnel; • Establish an efficient premium collection mechanism, and maintain an updated membership
and contribution database; • Conduct information campaigns on the principles of the Program to the public and private
accredited health care providers.
PhilHealth draws its funds from three main sources: 1) premiums collected from its paying members 2) proceeds from its investments 3) allocation from the national government as enacted under the General Appropriations Act
(GAA) to fund its NHTS-PR Sponsored Program
There are currently five membership types/programs under the NHIP. These are: 1. Sponsored Program 2. Individually Paying Program 3. Employed Sector Program 4. Overseas Workers Program 5. Lifetime Member Program
A Sponsored Member is one whose contribution is being paid by the national or local government, or by a private entity according to the rules as prescribed by the Corporation. Currently, the Sponsored Program aims to cover indigents belonging to the lowest 40% (Quintiles 1 and 2) of the Philippine population, including:
1. Families listed under the National Household Targeting System for Poverty Reduction (NHTS – PR) of the Department of Social Welfare and Development (DSWD); and
2. Families identified as poor by the sponsoring Local Government Units (LGUs). PhilHealth members and their dependents are entitled to the following minimum services.
a. In-patient care: 1. Room and board; 2. Services of health care professionals; 3. Diagnostic, laboratory, and other medical examination services; 4. Use of surgical or medical equipment and facilities; 5. Prescription drugs and biologicals, subject to the limitations of the Act; and, 6. Health Education.
b. Out-patient medical and surgical care: 1. Services of health care professionals; 2. Diagnostic, laboratory and other medical services; 3. Personal preventive services; 4. Prescription drugs and biologicals, subject to the limitations of the Act; and, 5. Health Education.
c. Emergency and transfer services; d. Health Education Packages; and, e. Such other health care services that the Corporation and the DOH shall determine to be appropriate and cost-effective.

Page 8
A specific provision of the new PhilHealth law provides for “No Balance Billing” (NBB) for indigent confined in public health facilities. This means that no other fee or expense shall be charged to indigent in public health care institutions subject to the guidelines issued by the PhilHealth. Local government units (LGUs) play an important role in the NHIP because they serve as the frontline agency in providing health care services to indigent families. Along this line, LGUs are enjoined to:
1. Develop policies and plans appropriate to their locality and consistent with the implementation of the national government’s health agenda
2. Mobilize and utilize local resources, PhilHealth reimbursements, user-fees, capitation fund, and other resources to organize and sustain the local health delivery system;
3. Improve the capacity of local hospitals and other public health facilities to deliver services; and
4. Establish partnership with the private sector for effective delivery of health service packages Membership, Accreditation and Benefits. In the 2012 Statistics and Charts by PhilHealth (December 31, 2012), it was reported that there is a total of 28.49 M registered members, 52.43 M dependents and 80.92 M combined. The sponsored program on the other hand has 8.29 M registered members, 28.39 M dependents and 36.68M combined. This can be broken down into 3.69 registered members, 12.56 dependents and 16.25 combined under Regular & DOH and 4.61 registered members, 15.82 dependents and 20.43M combined under NHTS-PR.3
It was also reported that there is a total of 632 level 1 hospitals (312 private and 320 government), 675 level 2 hospitals (417 private and 258 government), 252 level 3 (206 private and 46 government) hospitals and 111 level 4 hospitals (67 private and 44 government) which are PhilHealth-accredited. Philhealth’s annual report for 2012 noted that a total of 1,670 Rural Health Units (RHUs) and health centers were accredited as Primary Care Benefit (PCB) Package providers. While around 1,476 were accredited as Maternity Care Package (MCP) providers and 1,201 were accredited as TB-DOTS package providers. In addition, among the Local Government Units (LGUs) across the country, only 17% do not have a PCB provider while 55% of LGUs do not have an accredited MCP provider. In terms of benefit payments, Philhealth reported that it paid Php 47.2 billion to an estimated 4.8 million claims. Nearly half (45%) of the total number of claims for the year which amounted to 20.2 billion pesos were paid to the formal sector (Private and Government employed) followed by 24% of claims amounting to 9.6 million which were paid to the individually paying sector while 19% of claims totaling 12 billion were from the sponsored program. The Philhealth annual report for 2012 emphasized that more than a third of the total paid claims for the sponsored program were paid through the No Balance Billing Policy. The same report noted that 60% of the total claims were paid through the Case Rate Payment System. The top three medical case rates paid were for Pneumonia I, Newborn Care Package and Acute Gastroenteritis while the top three surgical case rates paid were for Hemodialysis, Normal Spontaneous Delivery Package and Caesarian section.
3 All data on membership, accreditation and benefit payments are based on the latest Statistics and Charts of PhilHealth for 2012.

Page 9
Study Objectives and Methodology This study will focus on tracking funds generated from the incremental revenue on excise taxes collected from tobacco and alcohol products under the Sin Tax Law, and appropriated for the national government’s Sponsored Program that is administered by PhilHealth. The study aims to improve public spending and service delivery in the health sector by ensuring the effectiveness, feasibility and desirability of the expanded program for universal health care in addressing the health needs of poor Filipino families. Specific Objectives 1. Develop appropriate instruments for tracking utilization of funds allocated in accordance with
the General Appropriations Act and the Sin Tax Law; 2. Identify a narrow set of health care services based on stakeholders preference to be financed by
the incremental allocation for financial risk protection; 3. Recommend specific measures to ensure transparency, effectiveness and social desirability of
the health protection and insurance for the poor. The study will seek to identify problems, issues, gaps, bottlenecks and risks in the funding flow and their impact on health services for the poor. One output of this study are recommended indicators and template instruments that can be used for continuing expenditure and performance monitoring of Philhealth’s Sponsored Program. Project Methodology Background Research
. A review of literature was conducted on the current and previous legislations related to excise taxes on tobacco and alcohol, on the National Health Insurance Program, on PhilHealth and on Universal Health Care. Additional background information were gathered from interviews of key informants, and from available studies and documents obtained from the Department of Health, PhilHealth and the National Economic Development Authority. The results of the background research enabled the project team to improve the PETS research design, finalize the set of indicators that will be monitored and draft the research instruments.
Pretest
. Preliminary instruments were drafted for hospitals/health facilities and for beneficiaries of Philhealth’s Sponsored Program. A pretest was conducted to test the appropriateness and sensitivity of the PETS instruments. The pretest was started in the last week of September 2012 and was completed by mid October 2012, covering both urban and rural provincial areas. The result of the pretest was instrumental in firming up the research design and in finalizing the survey instruments as discussed below. The pretest also highlighted the problems related to data availability and access. These were partly addressed during the actual survey. The pretest survey noted the need to obtain the formal and strong endorsement of relevant health agencies and executive offices to facilitate data access. Strategic contacts and partners within the local government units were also necessary to ensure access to relevant information at the local level.
Finalization of the survey instruments. The survey instruments were revised several times based on the background research, the results of the pretest and the discussions of the project team with the consultants. It was finalized after the interviews and focused group discussions with Philhealth officers and with local government officials. The following instruments were used for the tracking survey:

Page 10
PETS Instruments 1. Health Facility Information Sheet 2. Questionnaire for SP Beneficiaries The final versions of the questionnaires were more focused, with sharper questions and with clear targeted respondents. For health facilities, the survey focused on the funding and claims processing of service packages specifically for SP beneficiaries. For beneficiaries, the focus was on indigent families – those belonging to the poorest 20% of the population as identified through the National Household Targeting System for Poverty Reduction (NHTS-PR) of the Department of Social Work and Development (DSWD). The inclusion of SP beneficiaries of this PETS study is crucial because of the particular funding mechanism adopted by the national government to provide financial risk protection for the poor. Funds generated from Sin Taxes are transferred and allocated to finance the enrollment of identified indigent families in all cities and municipalities across the country. Allocated funds for enrollment are deemed spent or used once the target beneficiaries are enrolled as proven by their inclusion in the list of NHTS-PR/PhilHealth-SP beneficiaries; knowledge of enrolment/membership by the beneficiaries; and possession of PhilHealth ID cards and the Member Data Record (MDR). Thus, the final validation of the expenditure is made through verification of such enrolment of the target beneficiaries. The survey went further to assess the quality of such membership and the actual usage of benefits available to beneficiaries. Additional instruments were also developed to guide the data gathering and interviews of key informants from the Department of Health, Philhealth and Local Government Units. Formal links was established with Philhealth prior to the start of the survey. Interviews were made with several officers and a meeting/focused group discussion was held with key officers from the planning office and data center. A comprehensive list of data required for the study was discussed and submitted to Philhealth. Actual Conduct of PETS The tracking exercise was done at the national and local levels. At the national level, funds were tracked from the funding source to PhilHealth and how these funds flowed down to the health facilities and to the actual beneficiaries. The tracking exercise at the national level started in October 2012 and took more time than originally expected. This is because of the difficultly of obtaining the needed information for the tracking exercise. Most of the critical information was obtained only by July 2013. The required data was completed only by December 2013. At the local level, four local areas were selected for the tracking exercise – one city and 3 municipalities, covering both urban and rural areas. Two are located in the Greater Metro Manila area and the other two are in provincial areas. The local areas were selected purposively based on the following criteria:
• Mix of highly urbanized and predominantly rural areas • Significant number of Philhealth Sponsored Program beneficiaries • Presence of local partners • Willingness of LGU officials to conduct the study and provide the needed information
Two to four barangays (villages) were selected per local area. All health facilities were covered and 50 respondents were selected in each of the target local areas. The preparation for the actual survey

Page 11
was done by the second week of November 2012 which entailed negotiations with the target LGUs and the preparations of the survey package:
• Courtesy calls and orientation meetings with LGU officials • Identification and training of the local facilitators and surveyors • Production and distribution of surveyors kits, manuals and questionnaires • Endorsement letters and courtesy calls to village officials • Logistical arrangements
The actual survey started in December and was completed by the first week of February. The following areas were covered :
1. Paranaque City, Metro Manila 2. Angono, Rizal (Greater manila Area) 3. Sta. Rosa, Nueva Ecija 4. Baao, Camarines Sur
Number of health facilities covered by the survey = 25 Number of respondent-beneficiaries covered by the survey = 217
A major limitation of the PETS study is the incomplete data obtained from health facilities during the time allotted for the field work. Health facilities were not able to fill up the survey information sheet because of the lack of authority from their respective supervising agencies. Instead, information were gathered through interviews of LGU officials, health facility personnel and Philhealth staff assigned in the health facilities. The data gap was partly covered through the information gathered from the survey of beneficiaries, specifically on enrollment, membership status and usage of health facilities.
Data processing
. The project team processed the data culled from interviews and available documents from national agencies, local government units and local health facilities.
Survey data from completed questionnaires for individual beneficiaries were processed as soon as the questionnaires were checked and validated. An encoding program using the Census and Survey Processing System (CSPro) was used for this purpose. Statistical tables were generated using SPSS, a software package for statistical analysis. The encoding was started in late January 2013 and was completed by end of February 2013.
Challenges and Limitations The PETS study happened at about the same time the Sin Tax Law was enacted, signed and implemented. As such, the study is seen as important and timely because it can support the implementation during its earliest stage. At the same time, there are disadvantages because of the confusion and changes associated with the transition and implementation of a new law. In addition, there were changes at the top management level of Philhealth with the resignation of its former President in January 2013. These developments affected the agency’s data management and reporting system. Negotiations with LGUs for the conduct of the study had been very challenging, particularly given the sensitivity of government agencies over budget and financial matters. The project team had to look for influential allies and credible local partners who can facilitate links with the target local areas. But even then, negotiations with the LGUs for the conduct of the study took more time than expected and not all needed data were made available to the project team. Another factor that affected the study was the local elections scheduled in May 2013. While the survey was conducted

Page 12
several months ahead of the elections, informal campaigning had started as early as the last quarter of 2012.
As mentioned earlier, health facilities did not fill up the information sheet because of the lack of authority to do so. Moreover, hospital personnel shared that most of the data requested by the team were not available due to poor data management and lack of system of data consolidation and reporting. Most data are in raw forms and annotated in logbooks which cannot be publicly divulged even to the concerned patients and family members themselves.

Page 13
PETS Results
A. Budget Tracking at the National Level
Since the start of the new administration under President Aquino, the total National Budget of the Philippines has been increasing at a higher rate than in previous years. For the period 2011 to 2014, the total budget increased at an average rate of 15% per year. The same trend is observed for the budget of the health sector which grew at a much faster rate compared to most other sectors and to the overall national budget. In 2014, the health sector budget was allocated Php 83.7 billion from Php 51.1 billion in the previous year, or an unprecedented increase of 40% in a single year (See Table 1). Bulk of this increase is earmarked for the national government’s Sponsored Program which provides financial risk health protection for indigent families. Table 1. Budget Figures in Billions of Pesos (2011-2014)
2011 2012 2013 2014
Total National Budget
1,000.4
1,245.2
1,368.2
1,608.5
Total Health Budget
32.4
42.8
51.1
83.7
Sponsored Program Budget
3.0
12.0
12.6
35.3 Source: General Appropriations Act, 2011-2014 The graph below presents the relative magnitude of the increments of the total national budget, the health sector budget and the budget allocation for the Sponsored Program. Using 2011 as the base year (Index=1.00), it will be noted that the allocation for PhilHealth’s Sponsored Program has been increasing at a geometric pace especially for years 2012 and 2014. During the 4-year period, budget allocation for the Sponsored Program grew ten times faster compared to the total national budget. For years 2012 and 2013, the national government allocated a little over Php 12 billion to scale up the enrolment coverage of indigent families. In 2014, the huge increase was based on the projected incremental revenue that is expected to be raised for the first year of the implementation of the Sin Tax law. Figure 1. Budget Index (Base Year 2011)
Source: Basic data culled from General Appropriations Act, 2011-2014
0
2
4
6
8
10
12
14
2011 2012 2013 2014 Year
Budget Increments 2011-2014
Index 2011=1.00
Sponsored Program
Total Health
National Budget

Page 14
The huge increase in the health budget and allocation for the Sponsored Program is part of the commitment of the Aquino government to achieve universal health care. This commitment has been given a strong boost with the enactment of the Sin Tax law which allocates a significant portion of the incremental revenue from excise taxes on tobacco and alcohol products for universal health care, specifically to finance the Sponsored Program administered by PhilHealth. The Sin Tax law and its Implementing Rules and Regulations (IRR) allocate an estimated 15% of the incremental revenue from excise taxes on tobacco and alcohol products for tobacco-producing provinces and for tobacco farmers. Of the balance (of about 85%), 80% is earmarked for universal health care, specifically for financial risk protection for the poor (Sponsored Program), for health awareness, and for strengthening of preventive health programs towards attainment of health MDGs. Under the IRR, the Department of Health was tasked to identify the annual funding requirements for financial risk protection, health programs, medical assistance and health facilities enhancement. The department shall submit at the beginning of the year a list of projects and programs to be implemented for the universal health care program Adequate funds shall be allocated to enroll and continuously cover as PhilHealth members families belonging to the first and second income quintiles (Q1 and Q2) based on the list as provided by the DSWD in consultation with PhilHealth. The list shall contain families who have not been identified as poor by the NHTS-PR but are within the estimated maximum number of families that are part of Q1 and Q2. Actual excise tax collections for the first year of implementation of the Sin Tax law have exceeded previous estimates as computed by the Department of Finance (DOF). As a result of higher tax collection, the DOF now expects to generate incremental revenues of P36.34 billion from the sin tax collections throughout 2013 — 7% higher than the target of P33.96 billion set in 2012 (DOF). As mentioned, this provided a big boost for the Aquino Administration to accelerate its program on universal health care. Table 2 presents the premium contributions corresponding to the target number of family beneficiaries for the Sponsored Program using the NHTS-PR listing. From 4.61 million in 2012, the number of beneficiaries increased to and 5.06 million in 2013. For 2014, the target number of beneficiaries increased by nearly three times given the allocation of Php 35.34 billion to cover the premium contributions of 14.87 million families. Table 2. Target Number of Families and Premium Contributions for Enrollment of NHTS-PR Beneficiaries
2012 2013 2014
Target number of Families (in millions) 4.61 M 5.06 M 14.87 M
Premium Contributions (in billions of Pesos) 15.82B 16.54 B
35.34 B
Allocation from the national government (in billions of Pesos)
12.03B 12.63B 35.34 B
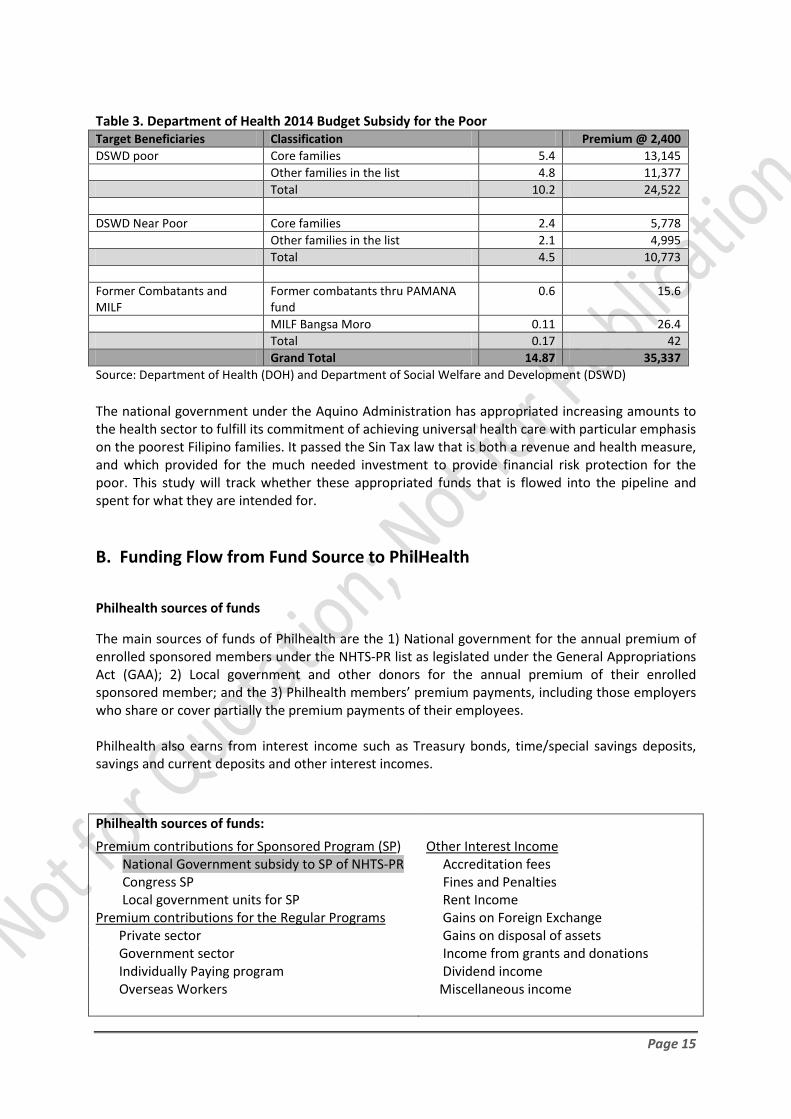
Sources: General Appropriations Act, 2011-2014; PhilHealth Annual Report 2012 Table 3 shows the breakdown of the allocation for the premium contributions of poor families under the Sponsored Program for 2014. For this particular year, the government is targeting not only those identified as poor, but also those belonging to the next poorest 20% of families which is sometimes classified as the “near poor.” Also included are former combatants of the Muslim rebel groups.
Page 15
Table 3. Department of Health 2014 Budget Subsidy for the Poor Target Beneficiaries Classification Premium @ 2,400 DSWD poor Core families 5.4 13,145 Other families in the list 4.8 11,377 Total 10.2 24,522 DSWD Near Poor Core families 2.4 5,778 Other families in the list 2.1 4,995 Total 4.5 10,773 Former Combatants and MILF
Former combatants thru PAMANA fund
0.6 15.6
MILF Bangsa Moro 0.11 26.4 Total 0.17 42 Grand Total 14.87 35,337 Source: Department of Health (DOH) and Department of Social Welfare and Development (DSWD) The national government under the Aquino Administration has appropriated increasing amounts to the health sector to fulfill its commitment of achieving universal health care with particular emphasis on the poorest Filipino families. It passed the Sin Tax law that is both a revenue and health measure, and which provided for the much needed investment to provide financial risk protection for the poor. This study will track whether these appropriated funds that is flowed into the pipeline and spent for what they are intended for. B. Funding Flow from Fund Source to PhilHealth
Philhealth sources of funds The main sources of funds of Philhealth are the 1) National government for the annual premium of enrolled sponsored members under the NHTS-PR list as legislated under the General Appropriations Act (GAA); 2) Local government and other donors for the annual premium of their enrolled sponsored member; and the 3) Philhealth members’ premium payments, including those employers who share or cover partially the premium payments of their employees. Philhealth also earns from interest income such as Treasury bonds, time/special savings deposits, savings and current deposits and other interest incomes. Philhealth sources of funds:
Premium contributions for Sponsored Program (SP) Other Interest Income National Government subsidy to SP of NHTS-PR Accreditation fees Congress SP Fines and Penalties Local government units for SP Rent Income
Gains on Foreign Exchange Premium contributions for the Regular Programs Private sector Gains on disposal of assets Government sector Income from grants and donations Individually Paying program Dividend income Overseas Workers Miscellaneous income

Page 16
Source: COA Audited Report on Philhealth, 2012 Figure 2. Flow of Resources In Philhealth
Other Income
(From interests, fees and
investments)
Premium Payments of
Members (EMPLOYERS & INDIVIDUALS)
LGU Budget/ Donors
Allocation for Premium of
Indigents
Nat’l Govt-DOH Budget Allocation for Premium of Indigents: NHTS-PR (As Legislated under the
GAA)
PHILHEALTH
National Office
For purposes of this study, only the allocation for the national government’s Sponsored Program which provides for the premium payments of indigents shall be covered and tracked. This is indicated in the shaded boxes in Figure 2. As mentioned in the previous section, the national government allocates a budget for the said subsidy for the particular fiscal year based on the DSWD’s NHTS-PR list of poor families as beneficiaries of the Sponsored Program. The said budget is allocated under the budget of the Department of Health and is found in the annual General Appropriations Act (GAA). Release of Funds The release of said subsidy is guided by the relevant provisions in the GAA. To facilitate the release of said subsidy, Philhealth is tasked to undertake the following:
a. Secures from DSWD the NHTS-PR list of qualified indigent households and ensures that all eligible indigents are enrolled in the NHIP. This is done in coordination with the DOH, DSWD, and the LGUs.
b. In coordination with the DOH, requests the Department of Budget for the release of the Special Allotment Release Order (SARO) and Notice of Cash Allocation (NCA).
c. Submits to DBM pertinent reports and financial statements such as i. Certification through its Chief Accountant, of the amount of applicable premium
and includes corresponding number of qualified enrollees and period of coverage
ii. Certification that Philhealth assumes full responsibility for the veracity and accuracy of the collections incorporated in the Philhealth financial statements including the list of NHTS indigents
Interest Income Treasury Bonds Time/Special savings deposits Savings and Current Deposits

Page 17
In accordance with the relevant GAA provision, and in compliance with DBM requirements, the subsidy is released to Philhealth through the Bureau of Treasury of the Philippines which deposits the funds into the government servicing banks so Philhealth can then claim the subsidy by depositing the corresponding check into its own national account. In 2012 the national government allocated a budget of Php 12.03 billion to cover said subsidy for an estimated 4.61 million families as discussed in the previous section. While processing for the requirements for the release of allocated funds, PhilHealth started the enrolment of the SP beneficiaries based on the DSWD NHTS-PR listing of indigent families. Identification Cards and the Membership Data Records (MDR) were distributed accordingly. These were checked through the survey conducted by the AER team in selected local areas as discussed in the next section. On December 21, 2012, the joint circular of DOH, DBM and Philhealth was issued to provide guidelines on the release of the subsidy in compliance with the GAA FY 2012 provision. On December 27, 2012, pertinent documents were submitted by Philhealth to facilitate the release of the subsidy, including the list of indigents under the NHTS-PR of DSWD.. Based on the released documents, the provision for the full national government subsidy on the health insurance premium of indigent families enrolled as SP beneficiaries have been released under SARO No. F-12-01426 and NCA No. F-12-0025818 both dated December 28, 2012 in the amount of P11,884,094,400 per OR# 40144236. Based on the document/accomplishment report 2012 submitted by Philhealth, the number of NHTS-PR SP beneficiaries covered by the subsidy totaled to 4.61 million members (out of 20.49 million total membership) with an estimated 15.82 million dependents. Based on the report of Philhealth on its benefit payments, claims made related to the SP beneficiaries (both NHTS-PR and LGU sponsored) totaled 931,794 or 19% of all claims processed and paid. Benefit payments made to all SP beneficiaries amounted to Php 12.09 billion or 26% of all benefits paid by Philhealth for year 2012 (PHIC 2013a). Table 4. Philhealth Registered Members and Dependents, as of December 2012
Sector Registered Members Dependents Members and
Dependents
Government-Employed 2.03 4.40 6.43 Private-Employed 9.61 9.90 19.51 Sponsored Program 8.29 28.39 36.68
LGU/Regular 3.69 12.56 16.25 NHTS-PR 4.61 15.82 20.43
Individual Paying 5.06 6.76 11.82 Lifetime Member 0.66 0.60 1.25 Overseas Worker Program 2.84 2.39 5.23 Total 28.49 52.43 80.92
Notes: 1. Figures are in millions. 2. The projected population for 2012 (95.88M) used in the estimation of enrollment rate is based on the 2010
population NSO census (medium assumption; annual growth rate = 1.9). 3. Data reported are actual counts of members and dependents registered in the database except for dependents
LGU-sponsored Program members which were estimated using the NHTS member to dependent ratio.
Source: Philhealth Stats and Charts 2012
Page 18
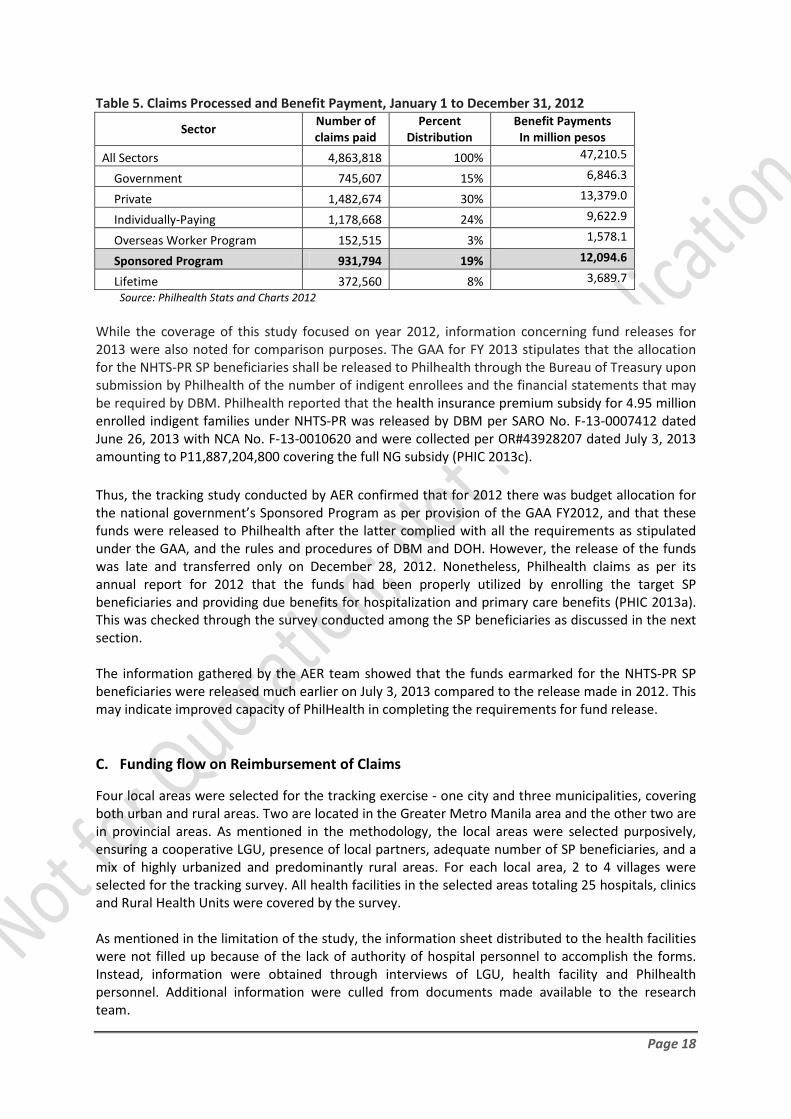
Table 5. Claims Processed and Benefit Payment, January 1 to December 31, 2012
Sector Number of claims paid
Percent Distribution
Benefit Payments In million pesos
All Sectors 4,863,818 100% 47,210.5
Government 745,607 15% 6,846.3
Private 1,482,674 30% 13,379.0
Individually-Paying 1,178,668 24% 9,622.9
Overseas Worker Program 152,515 3% 1,578.1
Sponsored Program 931,794 19% 12,094.6
Lifetime 372,560 8% 3,689.7 Source: Philhealth Stats and Charts 2012
While the coverage of this study focused on year 2012, information concerning fund releases for 2013 were also noted for comparison purposes. The GAA for FY 2013 stipulates that the allocation for the NHTS-PR SP beneficiaries shall be released to Philhealth through the Bureau of Treasury upon submission by Philhealth of the number of indigent enrollees and the financial statements that may be required by DBM. Philhealth reported that the health insurance premium subsidy for 4.95 million enrolled indigent families under NHTS-PR was released by DBM per SARO No. F-13-0007412 dated June 26, 2013 with NCA No. F-13-0010620 and were collected per OR#43928207 dated July 3, 2013 amounting to P11,887,204,800 covering the full NG subsidy (PHIC 2013c). Thus, the tracking study conducted by AER confirmed that for 2012 there was budget allocation for the national government’s Sponsored Program as per provision of the GAA FY2012, and that these funds were released to Philhealth after the latter complied with all the requirements as stipulated under the GAA, and the rules and procedures of DBM and DOH. However, the release of the funds was late and transferred only on December 28, 2012. Nonetheless, Philhealth claims as per its annual report for 2012 that the funds had been properly utilized by enrolling the target SP beneficiaries and providing due benefits for hospitalization and primary care benefits (PHIC 2013a). This was checked through the survey conducted among the SP beneficiaries as discussed in the next section. The information gathered by the AER team showed that the funds earmarked for the NHTS-PR SP beneficiaries were released much earlier on July 3, 2013 compared to the release made in 2012. This may indicate improved capacity of PhilHealth in completing the requirements for fund release.
C. Funding flow on Reimbursement of Claims
Four local areas were selected for the tracking exercise - one city and three municipalities, covering both urban and rural areas. Two are located in the Greater Metro Manila area and the other two are in provincial areas. As mentioned in the methodology, the local areas were selected purposively, ensuring a cooperative LGU, presence of local partners, adequate number of SP beneficiaries, and a mix of highly urbanized and predominantly rural areas. For each local area, 2 to 4 villages were selected for the tracking survey. All health facilities in the selected areas totaling 25 hospitals, clinics and Rural Health Units were covered by the survey. As mentioned in the limitation of the study, the information sheet distributed to the health facilities were not filled up because of the lack of authority of hospital personnel to accomplish the forms. Instead, information were obtained through interviews of LGU, health facility and Philhealth personnel. Additional information were culled from documents made available to the research team.

Page 19
The Figure below presents the flow of funds from PhilHealth to payment of claims of public health facilities which treated members of the sponsored program. For a diagram on the overall flow of funds from sources to PhilHealth and from Philhealth to payment of claims to health facilities and beneficiaries see Annex G. Figure 3. Flow of Resources from Philhealth to Health Care Providers
Philhealth accredited providers for sponsored program members are the public health facilities which are either owned by the local government units or the national government. Local government units claim benefit payments for the primary care benefit packages usually provided by their rural health units of Municipalities or health centers for cities. They also claim payments for the maternal care packages usually provided by their birthing facilities. Government hospitals claim payments through the case rate payment scheme covering 23 medical and surgical cases while other cases are still paid through the fee for service scheme.

Page 20
Reimbursement and Benefit payment process Reimbursement of claims to Philhealth follow the following general steps: 1. Health Care Provider (HCP) (Local Government Unit (LGU) hospital and other Public hospitals)
submits the properly filled claim forms 2 and claim form 3 or medical abstract, claim form 1 from the member and other documentary requirements together with the transmittal list to the Local Health Insurance Office (LHIO), (or the Philhealth Regional office (PRO), whichever is nearer the claimant.) In cases where the Local government unit claims payment for Primary Care Benefit (PCB) package services, they submit a separate set of documents but the procedure of claiming remains applicable.
2. The LHIO receives and screens claims as to the correct number and names of claimants against transmittal list. Stamps “received” on the transmittal list if there are no deficiencies in the transmittal and total number of claim; if there is/are name/s listed but no claims attached, cross-out name/s in the list and have the transmittal list initialled by the hospital representative/health care provider.
3. The LHIO returns the received copy of transmittal list to hospital representative/health care
provider and advises client that processing of claims will be done within the 60-day period.
4. The LHIO transmits the claims documents to the Philhealth Regional office.
5. The Philhealth Regional office processes the claims and if found in order prepares the cheques and advices the corresponding LHIO for pick up. PRO releases checks and documents to LHIO.
6. LHIO informs HCP of checks ready for release. Releases cheques to HCP.
In cases where HCP follows up on check releasing at the LHIO; The LHIO verifies if check is available, if not, advices the HCP of status of the check. If cheque is available, releases cheque to HCP.
7. The HCP upon receipt of cheques, counterchecks/validates cheques received then acknowledges receipt of check, affixes signature in the logbook and disbursement voucher.

Page 21
The procedure for claims and benefit payment is illustrated in Figure 4. Figure 4. Reimbursement Flow Chart Source: Modified from Process Flowchart in Citizen’s Charter 2013, Philhealth 2013 The following issues and bottlenecks in the funding flow were shared to the research team by key LGU, health facility and beneficiary informants in implementing and utilizing the benefit packages of sponsored program members.
• Varying turn-around-time. A common complaint among hospitals is the more often long waiting time before there are able to claim their reimbursements. While others admit that some Philhealth reimbursements take around 30 days to claim, for most other cases, it usually takes three months before they are able to claim their reimbursements. This limits their capacity to purchase other medical needs of the health facility.
• No systematic paper tracking system. The long waiting time for reimbursements is worsened by the lack of ways in updating the status of claims. Hospital personnel do not know what happened to the papers they have submitted nor where the papers are.
•
• Lack of documentation. Hospitals have difficulty keeping track of sponsored program members accessing the services of the health facility. The difficulty arises from a lack of system to document entry and usage of sponsored program member/dependent-patients. Only a logbook is kept but the data/content is not translated into usable information on the sponsored program member/dependent-patient. Hospitals also could not cite data on expected claims (both in amount or tally) for the sponsored program. They rely on Philhealth’s utilization reports which are usually delayed.

Page 22
• Poor documentation of the list of National Household Targeting System for Poverty Reduction (NHTS-PR) members and dependent. The NHTS-PR list of DSWD and Philhealth do not have exact addresses or locators. The list is also not updated as many sponsored program members have relocated due to work or entire areas displaced by floods/landslides/calamities. Sponsored program members sometimes do not have their Philhealth IDs or Membership data record (MDR). Sometimes the dependents are not listed in the MDR.
•
• Non-implementation of the No Balance Billing (NBB) policy. The NBB policy is not being implemented in many public hospitals such that sponsored program members still had to cover some of the charges for their hospitalization. The NBB policy means no other fees or expenses shall be charged to or be paid for by the member-patient above and beyond the packaged rate covered by the case rate payment scheme.
•
In addition, NBB is only applied to selected medical conditions or surgeries and not for all cases. In complicated cases where patients have more than one medical condition covered by case rate package in one confinement, only one case rate package can be charged to Philhealth. Case rate refers to fixed rate or amount that Philhealth will reimburse for a specific illness/case. Guidelines are still needed in the actual implementation of the NBB while some hospitals prepare the NBB or Philhealth Bed or wards.
•
• The Philhealth Pilot study (March 2013) of NBB implementation in 6 public hospitals showed some problems along the way. These difficulties include complaints by hospitals like: some were denied claims by Philhealth because documents of sponsored program member were incomplete or names were misspelled; some hospitals excluded coverage of deliveries after the fourth baby who under the new law should have been covered; hospitals complained that it took too long before they were reimbursed the much needed funds to purchase other medical needs.
•
• Case rate amounts are low. A particular hospital covered by the study was not keen on shouldering the fees beyond the packaged rate of Philhealth because the case rate amounts are too low to cover the actual cost of service.
•
• Lack of medicines and supplies. The lack of medicines and supplies remains a perennial problem of public health facilities and it pushed Philhealth member-patients to pay advances, or at least replace what they used.
•
• Health facility not yet Philhealth accredited. Several public health units/center and lying-in clinics have not yet satisfied Philhealth requirements for accreditation. Some have yet to build the facility in accordance with Philhealth standards as well as purchase the necessary equipments. Some have not yet signed the Memorandum of agreement (MOA) or performance commitments of LGUs. Others did not want to pay the fines/penalties for late accreditation. Several lying in clinics covered by the study were already accommodating deliveries but could not claim these from Philhealth because they were not yet accredited.
•
• Non-monitoring of capitation/Per Family Payment Rate (PFPR) fund. Philhealth is tasked to guide and monitor the disposition of the capitation fund or currently the PFPR fund. However, Philhealth is faced with challenges as LGUs decide on how to use said funds.
•
• Transparency for audit. Hospitals complained of not knowing the reasons for denied claims by Philhealth while COA audit report for 2012 cites huge amounts of unclaimed benefits totaling around 250 million pesos. Costs of hospital/medical services are not clear to beneficiaries as well as the costs charged to Philhealth.
Page 23
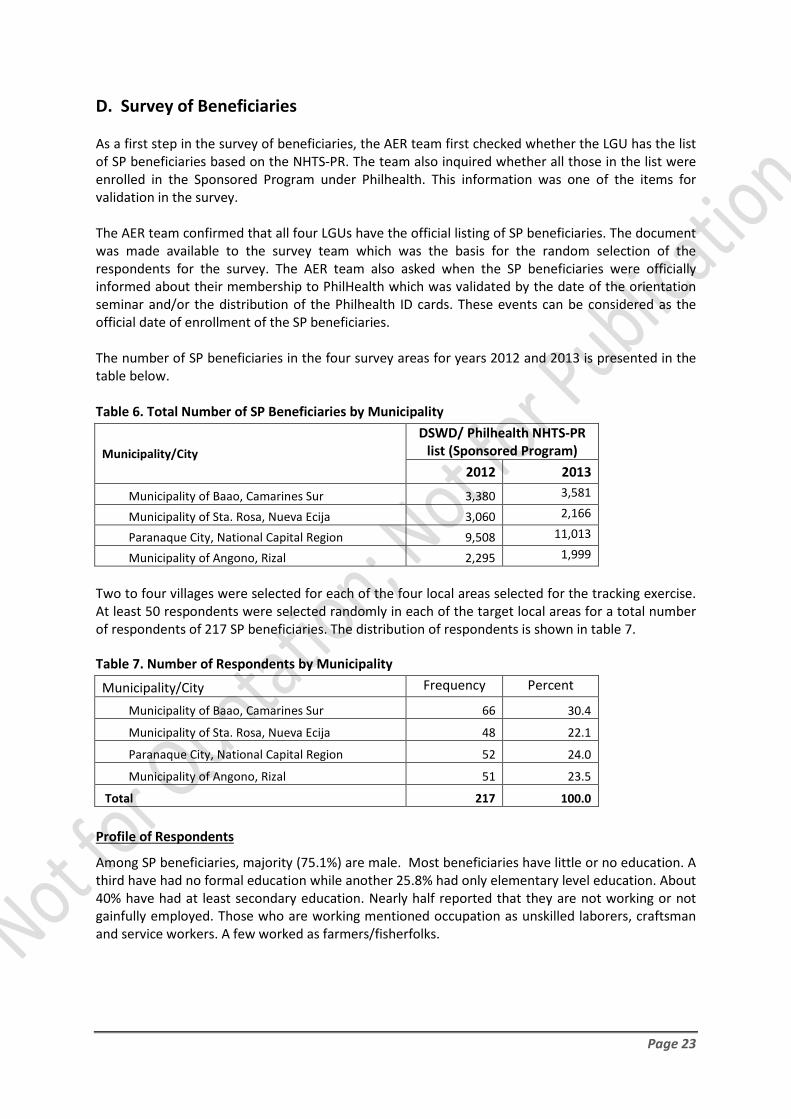
D. Survey of Beneficiaries As a first step in the survey of beneficiaries, the AER team first checked whether the LGU has the list of SP beneficiaries based on the NHTS-PR. The team also inquired whether all those in the list were enrolled in the Sponsored Program under Philhealth. This information was one of the items for validation in the survey. The AER team confirmed that all four LGUs have the official listing of SP beneficiaries. The document was made available to the survey team which was the basis for the random selection of the respondents for the survey. The AER team also asked when the SP beneficiaries were officially informed about their membership to PhilHealth which was validated by the date of the orientation seminar and/or the distribution of the Philhealth ID cards. These events can be considered as the official date of enrollment of the SP beneficiaries. The number of SP beneficiaries in the four survey areas for years 2012 and 2013 is presented in the table below. Table 6. Total Number of SP Beneficiaries by Municipality
Municipality/City DSWD/ Philhealth NHTS-PR
list (Sponsored Program) 2012 2013
Municipality of Baao, Camarines Sur 3,380 3,581
Municipality of Sta. Rosa, Nueva Ecija 3,060 2,166
Paranaque City, National Capital Region 9,508 11,013
Municipality of Angono, Rizal 2,295 1,999 Two to four villages were selected for each of the four local areas selected for the tracking exercise. At least 50 respondents were selected randomly in each of the target local areas for a total number of respondents of 217 SP beneficiaries. The distribution of respondents is shown in table 7.
Table 7. Number of Respondents by Municipality
Municipality/City Frequency Percent
Municipality of Baao, Camarines Sur 66 30.4
Municipality of Sta. Rosa, Nueva Ecija 48 22.1
Paranaque City, National Capital Region 52 24.0
Municipality of Angono, Rizal 51 23.5
Total 217 100.0
Profile of Respondents
Among SP beneficiaries, majority (75.1%) are male. Most beneficiaries have little or no education. A third have had no formal education while another 25.8% had only elementary level education. About 40% have had at least secondary education. Nearly half reported that they are not working or not gainfully employed. Those who are working mentioned occupation as unskilled laborers, craftsman and service workers. A few worked as farmers/fisherfolks.

Page 24
Table 8. Profile of Respondents
Frequency Percent
Sex
Male 163 75.1
Female 54 24.9 Level of Education
No Grade 72 33.2 Elementary 56 25.8 High School 80 36.9 College 7 3.2 No Response 2 0.9
Occupation
Laborer and unskilled workers (Construction workers, vendors, helpers) 43 19.8
Trades & related worker (Drivers, Carpenters) 39 18.0 Farmers and fisherfolks 14 6.5
Service workers/ shop and market sales workers (Security Guard, Manicurist) 14 6.5 Others 4 1.8 None/No occupation 103 47.5 Total 217 100.0
Philhealth Membership
Some 79.3% of the respondents have Philhealth cards of which 3 in 5 were able to show the cards when asked to. This is a good indication of their formal membership status and awareness about the sponsorship program. A lower percentage of respondents (66.8%) said they have their Member Data Record (MDR) which is a basic required document to claim for Philhealth benefits. Of these, 5 of 10 were able to show the MDR. A few of the respondents said they applied to be enrolled for Philhealth membership through the local MSWD office or local Barangay (Village) Chief. These are the ones who are not covered by the NHTS-PR program. This is a continuing issue in targeting which LGUs assert that they are in a better position to identify the poor in their localities.
Table 9. Possession of ID Cards and MDR Frequency Percent
With PhilHealth Identification card (Philhealth ID Shown to surveyor)
172 (136)
79.3 (62.7 )
With Membership Data Record (MDR) (MDR Shown to surveyor)
145 (113)
66.8 ( 52.1)
Awareness on Philhealth Sponsored Program
Nearly two-thirds of the respondents were aware that they got their enrolment card because they were sponsored under the NHTS-PR program or sponsored by the LGU. A significant number (30.0%) were not aware about the source of the sponsorship while another 9.6% thought that the LGU

Page 25
sponsored their Philhealth membership. A little over two-thirds (71.9%) were aware that their membership card is good for one year, so it will be expiring by the end of the 2013. Table 10. Awareness about Sponsorship
Frequency Percent Knows National Government/ DSWD NHTS (or 4Ps) as Sponsor
131 60.4
Not aware or misinformed about NHTS Sponsorship
69 39.6
Knows expiration date of Sponsorship
156 71.9
When asked about the benefits provided for under the sponsored program, the respondents are generally not familiar with the benefit packages as sponsored members. While over half (53.0%) were aware about the No Balance Billing (NBB) policy as one of the benefits of the Philhealth sponsored program, very few were aware about the other benefits, such as the Case Rate Packages, the Primary Care Benefits and the Childcare benefit (Garantisadong Pambata), among others. Table 11. Awareness about Benefits
Benefit Package Frequency Percent No Balance Billing (NBB) policy /Free hospitalization
115 53.0
Case rate payment 39 18.0 Case rate package 27 12.4 Non-case rate confinement 8 3.7 Primary Care Benefit Package 10 4.6 Garantisadong Pambata (Health-care benefits for children 0-14)
8 3.7
Benefit Utilization
Among the respondents who were confined, more than half were in health facilities which were outside their area of residence. In the case of both Baao and Sta. Rosa, public hospitals are a town away or in another city. It is important to note, however, that Sta. Rosa has a lying in clinic (Panganakang bayan), but the facility has not yet been accredited by Philhealth. Almost half were confined in private health facilities. In the case of Baao, there is no public hospital within the municipality. Very few (only 3) went to a non-Philhealth accredited health facility. Table 12. Hospital Confinement
Frequency Percent Public Health Facility 48 52.2 PhilHealth Accredited 87 94.6 Confinement included in Case Rate Package 52 56.5
Patient assigned to a No Balance Billing (NBB) bed
33 35.9
Patient asked to buy medicine and other medical supplies
64 69.6
Patient paid something at the billing station 39 42.4

Page 26
Only 35.9% claimed to have been assigned to a no balance billing bed. More than two thirds (69.6%) of those confined were asked to buy medicines and other medical supplies. This should not be the case since the benefit package includes all the needed supplies and prescribed medicines. Some 42.4% of those confined claimed they paid something at the billing station prior to being discharged. Half of those who paid spent between 1,000 and 10,000 pesos. Two SP members paid more than 30,000 pesos while the rest paid less than 1,000. When asked what items they paid for, most frequently cited items were medicines, laboratory/x-ray, doctor’s fee and donation. This should have been covered under the No Balance Billing Policy.
Assistance in Settling Philhealth Requirements
Half of those confined in health facilities had been assisted regarding their Philhealth transactions. Some 73.9 % claimed that there was a Philhealth staff at the billing station. When asked if the Philhealth staff was helpful, 65.2% agreed that said Philhealth staff was helpful. Nearly another half (46.7%) claimed that there were other personnel in the hospital who helped with the Philhealth transactions. Among those confined, 55.4% claims that they had all the requirements needed to avail of Philhealth benefits when they were admitted to the hospital. A higher percentage, 78.6% claimed they had all the requirements needed for the Philhealth benefits before that got discharged. Nearly one third (28.3%) of those confined said they needed to go out of the hospital to get the Philhealth requirements. The most frequently cited documents which required them to go out of the hospital to obtain these were birth certificates (of child dependents), the Member data record and marriage contract. Among those who had to go out of the hospital to obtain Philhealth required documents, about half of them already have these documents with them at home while the rest had to either go to the civil registry/national statistics office or at Philhealth local offices. Over half of those who had to go out of the hospital to obtain the documents did it in a day or less. Table 13. Fulfilling Philhealth Requirements
Frequency Percent Patient assisted in completing forms
46 50.0
PhilHealth staff present in hospital billing station
68 73.9
Philhealth staff in the hospital helpful
60 65.2
Other personnel helped with the PhilHealth
43 46.7
Patient had all requirements for PhilHealth upon admission
51 55.4
Patient had all requirements for PhilHealth upon discharge
72 78.6
Patient relative/s needed to go out of the hospital to secure required documents
26 28.3
Page 27
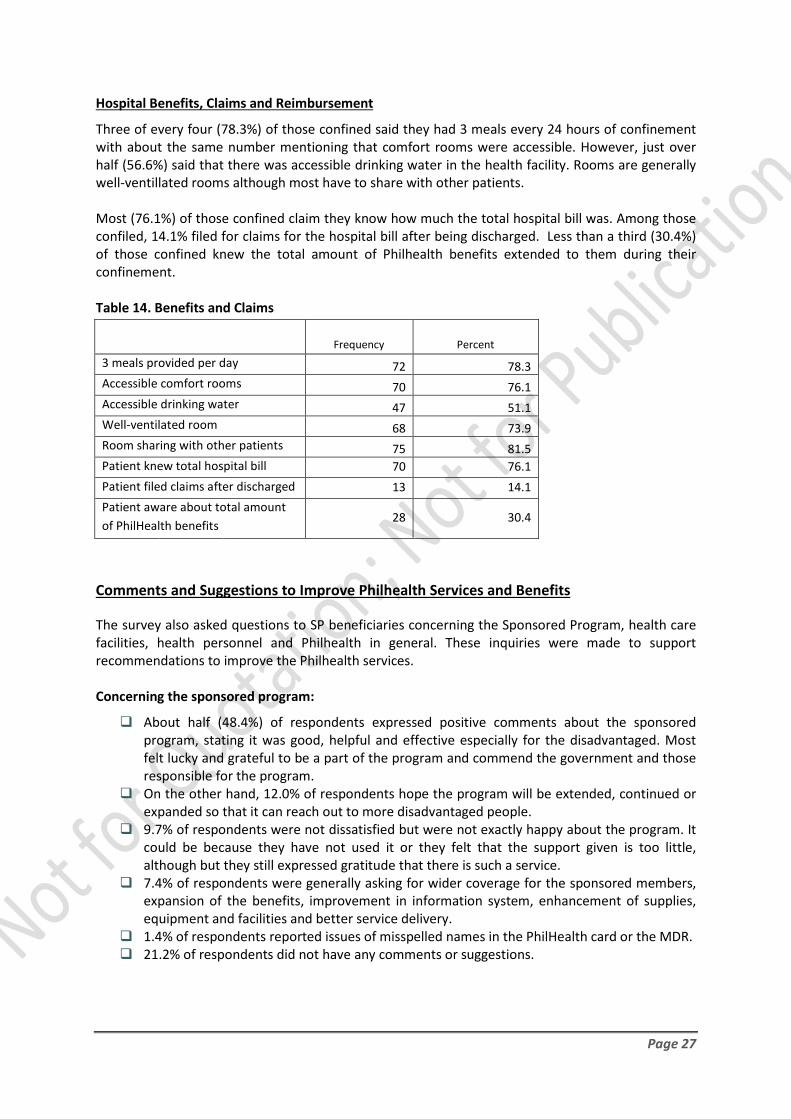
Hospital Benefits, Claims and Reimbursement
Three of every four (78.3%) of those confined said they had 3 meals every 24 hours of confinement with about the same number mentioning that comfort rooms were accessible. However, just over half (56.6%) said that there was accessible drinking water in the health facility. Rooms are generally well-ventillated rooms although most have to share with other patients. Most (76.1%) of those confined claim they know how much the total hospital bill was. Among those confiled, 14.1% filed for claims for the hospital bill after being discharged. Less than a third (30.4%) of those confined knew the total amount of Philhealth benefits extended to them during their confinement. Table 14. Benefits and Claims
Frequency Percent
3 meals provided per day 72 78.3 Accessible comfort rooms 70 76.1 Accessible drinking water 47 51.1 Well-ventilated room 68 73.9 Room sharing with other patients 75 81.5 Patient knew total hospital bill 70 76.1 Patient filed claims after discharged 13 14.1 Patient aware about total amount of PhilHealth benefits 28 30.4
Comments and Suggestions to Improve Philhealth Services and Benefits
The survey also asked questions to SP beneficiaries concerning the Sponsored Program, health care facilities, health personnel and Philhealth in general. These inquiries were made to support recommendations to improve the Philhealth services. Concerning the sponsored program:
About half (48.4%) of respondents expressed positive comments about the sponsored program, stating it was good, helpful and effective especially for the disadvantaged. Most felt lucky and grateful to be a part of the program and commend the government and those responsible for the program.
On the other hand, 12.0% of respondents hope the program will be extended, continued or expanded so that it can reach out to more disadvantaged people.
9.7% of respondents were not dissatisfied but were not exactly happy about the program. It could be because they have not used it or they felt that the support given is too little, although but they still expressed gratitude that there is such a service.
7.4% of respondents were generally asking for wider coverage for the sponsored members, expansion of the benefits, improvement in information system, enhancement of supplies, equipment and facilities and better service delivery.
1.4% of respondents reported issues of misspelled names in the PhilHealth card or the MDR. 21.2% of respondents did not have any comments or suggestions.
Page 28
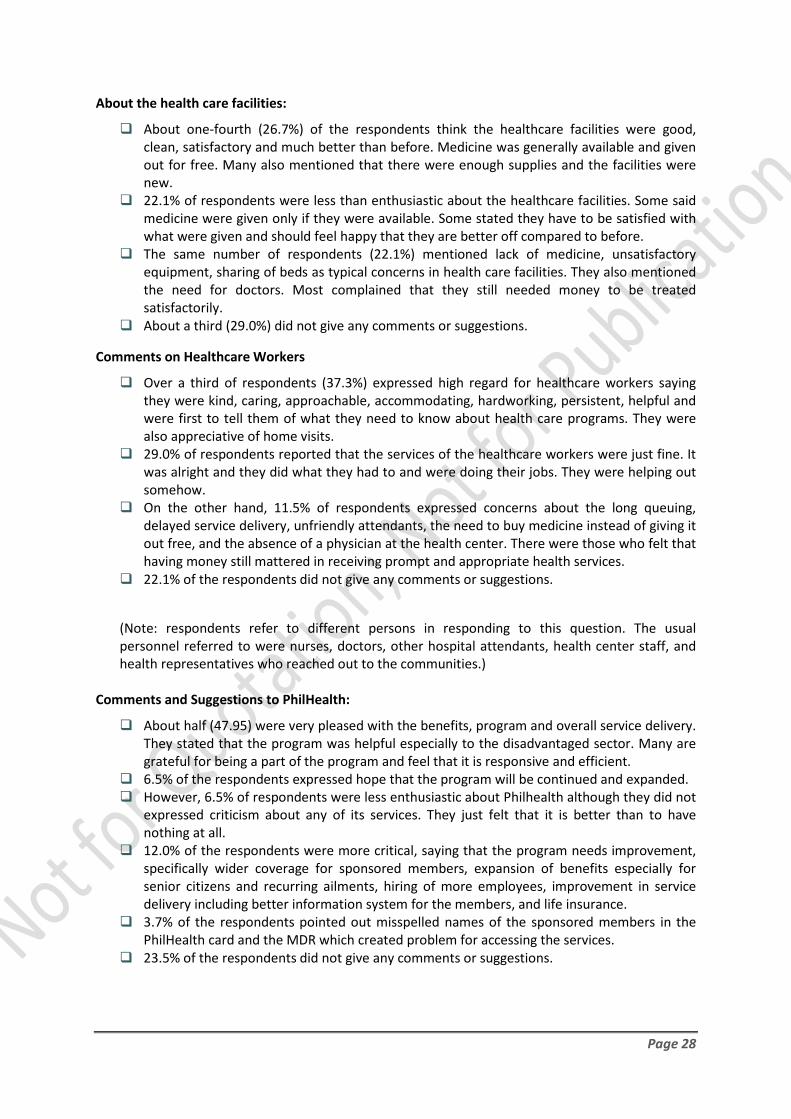
About the health care facilities:
About one-fourth (26.7%) of the respondents think the healthcare facilities were good, clean, satisfactory and much better than before. Medicine was generally available and given out for free. Many also mentioned that there were enough supplies and the facilities were new.
22.1% of respondents were less than enthusiastic about the healthcare facilities. Some said medicine were given only if they were available. Some stated they have to be satisfied with what were given and should feel happy that they are better off compared to before.
The same number of respondents (22.1%) mentioned lack of medicine, unsatisfactory equipment, sharing of beds as typical concerns in health care facilities. They also mentioned the need for doctors. Most complained that they still needed money to be treated satisfactorily.
About a third (29.0%) did not give any comments or suggestions.
Comments on Healthcare Workers
Over a third of respondents (37.3%) expressed high regard for healthcare workers saying they were kind, caring, approachable, accommodating, hardworking, persistent, helpful and were first to tell them of what they need to know about health care programs. They were also appreciative of home visits.
29.0% of respondents reported that the services of the healthcare workers were just fine. It was alright and they did what they had to and were doing their jobs. They were helping out somehow.
On the other hand, 11.5% of respondents expressed concerns about the long queuing, delayed service delivery, unfriendly attendants, the need to buy medicine instead of giving it out free, and the absence of a physician at the health center. There were those who felt that having money still mattered in receiving prompt and appropriate health services.
22.1% of the respondents did not give any comments or suggestions.
(Note: respondents refer to different persons in responding to this question. The usual personnel referred to were nurses, doctors, other hospital attendants, health center staff, and health representatives who reached out to the communities.)
Comments and Suggestions to PhilHealth:
About half (47.95) were very pleased with the benefits, program and overall service delivery. They stated that the program was helpful especially to the disadvantaged sector. Many are grateful for being a part of the program and feel that it is responsive and efficient.
6.5% of the respondents expressed hope that the program will be continued and expanded. However, 6.5% of respondents were less enthusiastic about Philhealth although they did not
expressed criticism about any of its services. They just felt that it is better than to have nothing at all.
12.0% of the respondents were more critical, saying that the program needs improvement, specifically wider coverage for sponsored members, expansion of benefits especially for senior citizens and recurring ailments, hiring of more employees, improvement in service delivery including better information system for the members, and life insurance.
3.7% of the respondents pointed out misspelled names of the sponsored members in the PhilHealth card and the MDR which created problem for accessing the services.
23.5% of the respondents did not give any comments or suggestions.

Page 29
Summary of Findings The first key research finding is that the national government under the Aquino presidency has appropriated increasing amounts to the health sector, specifically to the Sponsored Program (SP) administered by PhilHealth. The huge budgetary increment allocated to the health sector is designed to fulfill the government’s commitment of achieving universal health care with particular emphasis on the poorest Filipino families. For year 2012, the national government appropriated Php 12.03 billion for Philhealth’s SP. The tracking study confirmed that these funds were released to Philhealth after the latter complied with all the requirements as stipulated under the approved national budget of 2012. While the release of the funds was late, Philhealth was able to utilize the funds by enrolling the target SP beneficiaries and providing due benefits for hospitalization and primary care benefits. Thus, the funding allocation for 2012 has been essentially disbursed with the enrollment of the 4.61 million indigent families as identified by the NHTS-PR of DSWD. The premium payment of Php 1,200 per beneficiary for one year will amount to about 50% of the allocated amount for 2012. The other half is reserve for the expected increase of the premium payments from Php 1,200 to Php 1,800 and eventually to Php 2,400 per beneficiary per year. The increase in the premium payment is intended for the expansion of the coverage and benefits of the health insurance program for paying and sponsored members.
The SP beneficiaries have been identified and enrolled in Philhealth based on the available documents and interviews with key informants from LGUs and health facilities. This is also validated based on the survey of beneficiaries in the four local areas covered by the study. Proof of membership was further confirmed by the significant percent of respondents who reported having a Philhealth ID Card and a Member Data Record. For 2013, about the same allocation was approved for and disbursed by Philhealth which provided premium payments to 5.06 million indigent families. The earmarked funds were released much earlier in July 2013 which may indicate improved capacity of PhilHealth in completing the requirements for fund release. While the allocation has been essentially disbursed to the intended beneficiaries, there were problems and issues related to the enrolment process, the utilization of Philhealth benefits, and the actual benefits received by the SP beneficiaries.
1. There were delays in the enrolment of the target beneficiaries, specifically the distribution of ID Cards and MDR, and the orientation of the SP beneficiaries. These were completed only in the second half or latter part of 2012.
2. The orientation and information drive about the program need much improvement to explain the different benefits provided and to encourage usage of the Philhealth benefits. Thus, the quality of membership is affected because of the lack of knowledge about the benefit package as SP beneficiaries.
3. Access to and enjoyment of Philhealth benefits have been constrained because of access to public health facilities. The concerned LGUs, DOH and Philhealth have not campaigned more aggressively to promote utilization of preventive health care and hospitalization benefits provided for under the Sponsored Program. These and related issues are elaborated further below.

Page 30
The tracking study identified important issues related to the coverage of the sponsorship program:
1. Children of single parents as well as orphaned children and partners who are not married were all not part of the sponsored members and therefore cannot avail any of the features of the sponsored program even if they belonged to the poorest 20%.
2. A significant percentage of beneficiaries were not able to enjoy the full benefits for lack of
awareness, specifically about the No Balance Billing policy, the case rate packages, the primary care benefits, the childcare benefit package, and the provision of all needed medicines and supplies during confinement.
3. There is underutilization of Philhealth benefits among indigent families covered under the
program for the following reasons: - Lack of proper documents - Lack of awareness/knowledge about the benefit package - Delays in the enrolment/receipt of the ID cards and MDR - Accessibility of accredited public health facilities - Gender blind targeting of Philhealth beneficiaries (not a few women were not covered
because they were not married to the Philhealth member) - Poor health practices and persisting cultural beliefs (preference for home deliveries,
does not want to consult health professionals, prefer home remedies/traditional healers)
The low utilization of PhilHealth benefits is also related to accessibility to Philhealth-accredited public health facilities. A significant percentage of those confined were hospitalized in private hospitals which are not covered by the No Balance Billing policy. In fact, only half of all municipalities in the country have accredited public health facilities. LGUs, on their part, cited the following problems related to accreditation:
- Accreditation process is taking too long; - Strict requirements/standards for accreditation (facilities/equipment) are unduly imposed; - Lack of pro-active support from both DoH and Philhealth to assist and expedite the
accreditation process.
There is also limited capacity of local health facilities to respond to the demand for quality health care and services. Poor facilities and lack of equipment, supplies and medicines are limitations in delivering health services. In addition, not all illnesses that are frequently experienced by the poor are covered by the case rate packages. The information system of LGUs, health facilities and Philhealth are inefficient by design and actual operation. While data aggregated at the national level are usually available, disaggregated data by province, municipality and health facility is almost always not available and could not be generated. Transparency, particularly related to financial matters, is a critical issue that must be addressed to ensure proper budget and performance monitoring. This is compounded by complacency and negative attitude of most government agencies and officials to provide information to the public. Given the current system, it is difficult to track enrolment, utilization and benefits derived by Philhealth SP beneficiaries and Philhealth members in general.

Page 31
Recommendations On Monitoring and Reporting
a) Develop an effective, transparent, and participatory monitoring system to track the flow of funds generated from the Sin Taxes to PhilHealth and to health facilities, local governments, and Sponsored Program beneficiaries and Philhealth members.
b) Identify a set of indicators which can be aggregated and disaggregated at regional, provincial, municipality and health facility levels to facilitate easy tracking and validation check. In this way, outliers among claimants, health facilities, health personnel and LGUs can be checked for potential leakages. Nature of illnesses, geographical location and medical services provided can be tracked to assess the responsiveness of Philhealth services and benefit packages. For this purpose, the key items covered by the PETS questionnaire can be considered for inclusion in the set of indicators. If feasible, the Benefit Delivery Rate should also be generated at regional, provincial and municipal levels.
c) Philhealth, DOH, LGUs and health facilities should prepare quarterly and annual monitoring reports on the key indicators related to membership, information dissemination, awareness program, accreditation, claims, reimbursements, and benefit payments. The same report should also contain information on funding, income and revenues generated, and disbursements. Such reports should be made available to concerned agencies, the oversight committee of the legislature, interested parties and the general public.
d) Pertinent documents related to the utilization of the earmarked funds shall also be made available by concerned agencies and the general public to ensure transparency and accountability in the use of funds.
Identification of Beneficiaries and Coverage of the Sponsored Program
a) Strengthen the NHTS-PR for better targeting and coverage of the poorest families, allowing LGU and CSO to participate in the survey design, training of enumerators and evaluation of the survey process.
b) Ensure the enrollment of indigent families/individuals who have not been selected through the NHTS-PR system.
c) Implement a credible system for reviewing the list of selected NHTS-PR beneficiaries with participation from LGUs and CSOs.
d) Provide all relevant data to the concerned LGUs, including the complete roster of Philhealth members in the local areas.
e) Conduct periodic review to assess coverage of the target beneficiaries through broad consultations with concerned agencies and stakeholders.
f) Expand coverage of the Sponsored Program to fully utilize the earmarked funds generated from the Sin Taxes to include the following: - Persons with disabilities (PWDs) - Under-five children - Senior citizens - Survivors of disasters, wars, armed conflicts and human rights abuses - Ex-prisoners/detainees during the first two years of release or until they are able to find
gainful employment - Displaced Overseas Filipino Workers (OFW) who were repatriated due to disasters, wars,
trafficking, and human rights abuses (free coverage for the first two year after repatriation or until they are able to find gainful employment
- Consider the enrolment of pregnant and lactating women as priority target for the Sponsored Program

Page 32
Information Dissemination and Awareness-Building
a) Implement an effective information, education and communications (IEC) program to improve awareness and knowledge of SP beneficiaries on Philhealth services and benefit package.
b) The DOH, Philhealth and LGUs should take a pro-active role to sustain the IEC initiatives with concrete results, specifically in terms of improved health practices and increased utilization of Philhealth benefits.
Accreditation of Health Facilities
a) Ensure the accreditation of all national and local health facilities, including Rural Health Units and lying-in clinics. A clear timeline should be targeted for the accreditation of such facilities.
b) The DOH and Philhealth should rationalize its accreditation system, ensuring a unified and standardized system of accreditation.
c) Hasten the process of accreditation by providing the needed assistance to LGU and local health facilities. The DOH and Philhealth should take a pro-active stance to fast-track the accreditation of all public health facilities. Both agencies, along with the concerned LGUs, should be jointly liable for problems and delays in the accreditation process.
d) Improve access to health services by Increasing the number of LGU/DoH accredited health facilities able to provide primary care benefit package, TB-dots, health MDGs and hospitalization benefits for common and critical illnesses.
Expansion of Benefit Package
a) Develop more benefit packages (case rate packages) to cover the most common illnesses of indigents to ensure responsiveness to the health needs of the poorest.
b) Increase in Philhealth investment in primary health care, specifically by increasing the “capitation” fund and improving the monitoring of the utilization of the fund by PCB providers.
c) Conduct periodic review with the participation of LGUs, CSOs and other stakeholders to assess and improve the benefit packages, case rate payments and allocation for PCB.
Inter-Agency Coordination
a) Conduct regular continuing consultations among concerned government agencies, including LGUs, DOH, Philhealth, CSOs and other stakeholders.
b) Hold regular dialogues between concerned government agencies and Philhealth members/SP beneficiaries.
Information Management System
a) Install a sound system for recording, processing, retrieval and management of all relevant information and data related to Philhealth services, performance and financial transactions.
b) Establish clear guidelines to improve recording, encoding, and management of data for all PhilHealth services and benefits.
c) Consolidate/interface existing databases, specifically Philhealth, DSWD’s NHTS-PR; NSO, DOH, LGU administrative data and DILG’s CBMS.
d) Ensure easy access and retrieval of disaggregated information related to Philhealth membership, claims, and benefit payments. For this purpose, the Philhealth information sheet used in this tracking study may be used as one of the references.
Page 33
References Commission on Audit (COA). (2013). Annual Audit Report on the Philippine Health Insurance
Corporation, for the year ended December 31, 2012. Retrieved from http://www.coa.gov.ph/2012_AAR/GOCCs/Zipfiles/PHIC_aar2012.zip
Department of Budget and Management (DBM), Department of Health (DOH), Philippine Health
Insurance Corporation (NHIC). (2012). Joint Circular No. 2012-0424. Guidelines on the Implementation of Special Provision (SP) No. 15 on the National Health Insurance Program (NHIP) for Indigents, Department of Health (DOH) under Republic Act (RA) No. 10155, the FY 2012 General Appropriations Act. Retrieved from http://www.philhealth.gov.ph/joint_circulars/2012/jc2012-0424.pdf
Department of Health (DOH). (2010). Administrative Order No. 2010-0036. The Aquino Health
Agenda: Achieving Universal Health Care for All Filipinos. Retrieved from http://www.doh.gov.ph/sites/default/files/Aquino%20Health%20Agenda%20-%20Universal%
Department of Health (DOH). (2010). Toward Financial Risk Protection, Health Care Financing
Strategy of the Philippines 2010-2020. Health Sector Reform Agenda Monograph No. 10. Manila: DOH. Retrieved from http://www.scribd.com/doc/35105401/Health-Care-Financing-Strategy 2010-2020-Philippines
Department of Health (DOH). (2011). Department Order No. 2011-0188. Kalusugan Pangkalahatan
Execution Plan and Implementation Arrangements. Retrieved from http://www.doh.gov.ph/sites/default/files/Kalusugan%20Pangkalahatan.pdf
Department of Health (DOH). (2012). National Objectives for Health Philippines, 2011-2016 Health
Sector Reform Agenda Monograph No. 12. July 2012. Manila: DOH. Retrieved from http://www.doh.gov.ph/content/national-objectives-health-2011-2016.html
National Statistics Office (NSO) [Philippines], and ICF Macro. (2009). National Demographic and
Health Survey 2008. Calverton, Maryland: National Statistics Office and ICF Macro. National Statistical Coordination Board (NSCB). (2013). NSCB website for data on poverty and the
MDGs retrieved from http://www.nscb.gov.ph Philippine Health Insurance Corporation (PHIC). (2013a). 2012 Annual report, Arangkada Tungo sa
Pangkalahatang Kalusugan. Retrieved from http://www.philhealth.gov.ph/about_us /annual_report/ar2012.pdf
Philippine Health Insurance Corporation (PHIC). (2013b). 2012 Stats and Charts. Retrieved from
http://www.philhealth.gov.ph/about_us/statsncharts/snc2012.pdf Philippine Health Insurance Corporation (PHIC). (2013c). Financial Statements as of September 30,
2013. Retrieved from http://www.philhealth.gov.ph/about_us/annual_report/ PhilHealth_FS_2013September.pdf

Page 34
Philippine Health Insurance Corporation (PHIC). (2013d). Philhealth Citizen’s Charter 2013. (Revised November 2013). Retrieved from http://www.philhealth.gov.ph/news /updates/2013/Citizens_Charter_2013_Revised.pdf
Philippine Health Insurance Corporation (PHIC). (2013e). Strategic Initiatives Profile. Retrieved from
http://www.philhealth.gov.ph/about_us/transparency/ major_programs_projects/PhilHealth_Strategic_Initiative_Profile_PES2_090213.pdf
Philippine Health Insurance Corporation (PHIC). (2013f). Table on Distribution of Philhealth members
by Province and membership category. (Table in letter of PHIC submitted to the Department of Health dated February 28, 2013). Retrieved from http://www.philhealth.gov.ph/about_us/ transparency/accomplishment_report/2012_PhilHealth_Corporate_Accomplishment_Report.pdf
Philippine Health Insurance Corporation (PHIC). (2013g). Table on Distribution of Philhealth members
by Province and membership category with count of Dependents as of September 2013. Retrieved from http://www.philhealth.gov.ph/about_us/transparency /accomplishment_report/ PHIC_Enrollment_September2013.pdf
Republic Act No. 10606. National Health Insurance Act of 2013. Retrieved from
http://www.philhealth.gov.ph/about_us/ra10606.pdf Republic Act No. 10606 and its Implementing Rules and Regulations. Retrieved from
http://www.philhealth.gov.ph/about_us/ra7875_as_Amended_NHIActof2013.pdf Republic Act No. 10155. General Appropriations Act Fiscal Year 2012 (Philippine National Budget for
2012). Retrieved from http://www.dbm.gov.ph/?page_id=775. Republic Act No. 10352. General Appropriations Act Fiscal Year 2013 (Philippine National Budget for
2013). Retrieved from http://www.dbm.gov.ph/?page_id=5280. Republic Act No. 10633. General Appropriations Act Fiscal Year 2014 (Philippine National Budget for
2014). Retrieved from http://www.dbm.gov.ph/?page_id=7906 Tropical Disease Foundation Inc. (TDFI). (2007). Nationwide Tuberculosis Prevalence Survey 2007.

ANNEXES
ANNEX A Philhealth Information Sheet
ANNEX B Health facility questionnaire – Hospital
ANNEX C Health facility questionnaire – Birthing facility
ANNEX D Health facility questionnaire – Rural Health Unit or Health Center
ANNEX E Questionnaire for Individual Philhealth Member under the Sponsored Program (NHTS-PR)
ANNEX F Information culled from LGU and Health facility, Four Local Areas
ANNEX G Overall Flow of Resources in Philhealth

Page | 1
ANNEX A Philhealth Info Sheet: Data Requirements for AER Study on NHIP
Sponsored Program Table 1: Membership type and Coverage (National and By Province, City and Municipality) Registered
members Average number of dependents
Government-employed Private-employed Individually-paying Sponsored Program
• Regular and DOH • NHTS-PR
Lifetime Members Overseas Workers Program Table 2: Membership Type and Claims Summary Report (National and By Province, City and Municipality)
Mem
bers
and
de
pend
ents
File
d cl
aim
s
Paid
cla
ims
Amou
nt o
f pai
d cl
aim
s
Pend
ing
clai
ms
Amou
nt o
f pen
ding
cl
aim
s
deni
ed c
laim
s
Amou
nt o
f den
ied
clai
ms
Government-employed
Private-employed Individually-paying Sponsored Program
• Regular and DOH
• NHTS-PR
Lifetime Members Overseas Workers Program

Page | 2
Table 3: Facility Type and Claims Report Summary (National and By Province, City and Municipality) Fi
led
cla
ims
Paid
cla
ims
Amou
nt o
f pa
id c
laim
s
Pend
ing
clai
ms
Amou
nt o
f pe
ndin
g cl
aim
s
deni
ed c
laim
s
Amou
nt o
f de
nied
cla
ims
Hospitals Ambulatory Clinics Rural Health Units Authorized Hospitals Free Standing Dialysis Clinics
TB-DOTS centers Maternity Care Clinics

Page | 3
Table 4: Claims Report Summary for all 23 Illnesses (Case Rate Payment) (National and By Province, City and Municipality)
All 2
3 ca
se
rate
s
File
d cl
aim
s
Paid
cla
ims
Amou
nt o
f pa
id c
laim
s
Pend
ing
clai
ms
Amou
nt o
f pe
ndin
g cl
aim
s
deni
ed c
laim
s
Amou
nt o
f de
nied
cla
ims
Pneumonia I (Moderate Risk) Pneumonia II (High Risk) Dengue I (Dengue Fever and DHF Grades I & II)
Dengue II (DHF Grades III & IV),
Acute Gastroenteritis (AGE) Maternity Care Package (MCP)
NSD Package in Level 1 Hospitals
NSD Package in Levels 2 to 4 Hospitals
Caesarian Section Package Newborn Care Package Asthma Typhoid Essential hypertension Cerebral infraction (CVAI) Cerebral-vascular accident (CVAII) Hemorrhage
Appendectomy Cholecystectomy Dilatation and Curettage Thyroidectomy Herniorrhaphy Mastectomy Hysterectomy Cataract Surgery

Page | 4
Table 5: Facility Type and Sponsored Members (Regular and DOH and NHTS-PR) Availment
Sponsored Members Claims
Regular and DOH Claims
NHTS-PR Claims
Hospitals Ambulatory Clinics Rural Health Units Authorized Hospitals Free Standing Dialysis Clinics
TB-DOTS centers Maternity Care Clinics
Health Facility Data Requirement Table 6: Facility Type and Claims Report Summary
File
d c
laim
s
Paid
cla
ims
Amou
nt o
f pa
id c
laim
s
Pend
ing
clai
ms
Amou
nt o
f pe
ndin
g cl
aim
s
deni
ed c
laim
s
Amou
nt o
f de
nied
cla
ims
Provincial and District Hospitals
Rural Health Units
Maternity Care Clinics; Birthing Homes; Lying-ins

Page | 1
Name of Healthcare Facility: Location: (Region, Province, City, Municipality, District/Barangay)
Please check one: __ Hospital __ RHU __Other health facilities
If hospital, what level? __ Level 1 __ Level 2 __ Level 3 If not a hospital, which is it among the following?
__ Primary Care Facility __ Diagnostic/Therapeutic Facility __ Specialized Out-Patient Facility
When did the facility receive its DOH license? When did the facility receive PhilHealth accreditation? Accredited as a (check all that apply) Accredited on (date) o Freestanding Dialysis Clinic o Primary Care Benefit Provider o Maternity Package Benefit Provider o Anti TB-DOTS Package Provider o Malaria Package Provider o HIV-AIDS o Other package provider (Please Specify) Medical Personnel: How many doctors work in the facility? Of these, # of PhilHealth accredited? How many surgeons work in health facility? Of these, # of PhilHealth accredited? How many nurses work in the facility? How many midwives work in the facility? PhilHealth Personnel: How many Philhealth staff in all work in hospital? _____________________ Is there PhilHealth staff in the billing station? How many? ______________ Is there PhilHealth CARES in the premises? How many? ________________
Facility: Bed capacity: _____________ Occupancy rate: ___________ Are there specified accommodations for Sponsored members? ______________ How many NBB beds does the facility have? _____________________________ How many beds in the charity ward of the facility? ________________________
HEALTH FACILITY QUESTIONNAIRE- Hospital
Tracking Coverage and Effectiveness of the National Health Insurance Program (NHIP)
Action for Economic Reforms (AER)
ANNEX B

Page | 2
For Year 2011 (January to December)
Please fill in the following tables based on the facility’s records from January – December 2011. What is the total number of confinements? _____________
Of these, how many are PhilHealth members? ___________ How many are Sponsored Program Members? ___________
NHTS ______ LGU _______ Others _______ (Specify)
How many are non-members? _________ PhilHealth Members
# o
f Cas
es o
f Co
nfin
emen
t
# of
Cla
ims
File
d
Tota
l Am
ount
of
Cla
ims F
iled
# of
Pai
d Cl
aim
s (R
eim
burs
ed)
Tota
l Am
ount
of
Pai
d Cl
aim
s (R
eim
burs
ed)
#
of P
endi
ng
Clai
ms
Tota
l Am
ount
of
Pen
ding
Cl
aim
s #
of D
enie
d Cl
aim
s To
tal A
mou
nt
of D
enie
d Cl
aim
s
Total confinement cases
All 23 case rates
Sponsored Program Members
# o
f Cas
es o
f Co
nfin
emen
t
# of
Cla
ims F
iled
Tota
l Am
ount
of
Clai
ms F
iled
# of
Pai
d Cl
aim
s (R
eim
burs
ed)
Tota
l Am
ount
of
Paid
Cla
ims
(Rei
mbu
rsed
)
# of
Pen
ding
Cl
aim
s
Tota
l Am
ount
of
Pend
ing
Clai
ms
# of
Den
ied
Clai
ms
Tota
l Am
ount
of
Deni
ed C
laim
s
Total confinement cases
All 23 case rates
Special Packages: (Sponsored Members Only) How many availed of TB-DOTS? ___________ How many availed of Malaria Treatment package? ___________ How many availed of HIV-AIDS Treatment package? ___________ How many availed of Animal Bite Treatment package? ___________ Primary Care Benefits: (Sponsored Members Only) How many availed of Primary Preventive Services? ___________ How many underwent Diagnostic Examinations? ___________ How many availed of any of the Drugs and Medicines packages? ___________

Page | 3
For Year 2012 (January - September 2012)
Please fill in the following tables based on the facility’s records from January - September 2012. What is the total number of confinements? _____________
Of these, how many are PhilHealth members? ___________ How many are Sponsored Program Members? ___________
NHTS ______ LGU _______ Others _______ (Specify)
How many are non-members? _________ PhilHealth Members
# o
f Cas
es o
f Co
nfin
emen
t
# of
Cla
ims
File
d
Tota
l Am
ount
of
Cla
ims F
iled
# of
Pai
d Cl
aim
s (R
eim
burs
ed)
Tota
l Am
ount
of
Pai
d Cl
aim
s (R
eim
burs
ed)
#
of P
endi
ng
Clai
ms
Tota
l Am
ount
of
Pen
ding
Cl
aim
s #
of D
enie
d Cl
aim
s To
tal A
mou
nt
of D
enie
d Cl
aim
s
Total confinement cases
All 23 case rates
Sponsored Program Members
# o
f Cas
es o
f Co
nfin
emen
t
# of
Cla
ims F
iled
Tota
l Am
ount
of
Clai
ms F
iled
# of
Pai
d Cl
aim
s (R
eim
burs
ed)
Tota
l Am
ount
of
Paid
Cla
ims
(Rei
mbu
rsed
)
# of
Pen
ding
Cl
aim
s
Tota
l Am
ount
of
Pend
ing
Clai
ms
# of
Den
ied
Clai
ms
Tota
l Am
ount
of
Deni
ed C
laim
s
Total confinement cases
All 23 case rates
No Balance Billing Policy: (Sponsored Members Only) Total number of
cases Cases free of hospital charges
With automatic deductions but with additional out-of-pocket fees
Total number of cases without deductions
Case Rate Payments:
Non-Case Rate Payment Confinement

Page | 4
Special Packages: (Sponsored Members Only) How many availed of TB-DOTS? ___________ How many availed of Malaria Treatment package? ___________ How many availed of HIV-AIDS Treatment package? ___________ How many availed of Animal Bite Treatment package? ___________ Primary Care Benefits: (Sponsored Members Only) How many availed of Primary Preventive Services? ___________ How many underwent Diagnostic Examinations? ___________ How many availed of any of the Drugs and Medicines packages? ___________ Sponsored Members:
# o
f Cas
es o
f Co
nfin
emen
t
# of
Cla
ims F
iled
Tota
l Am
ount
of
Clai
ms F
iled
# of
Pai
d Cl
aim
s (R
eim
burs
ed)
Tota
l Am
ount
of
Paid
Cla
ims
(Rei
mbu
rsed
)
# of
Pen
ding
Cla
ims
Tota
l Am
ount
of
Pend
ing
Clai
ms
# of
Den
ied
Clai
ms
Tota
l Am
ount
of
Deni
ed C
laim
s
Total confinement cases
All 23 case rates
Pneumonia I (Moderate Risk)
Pneumonia II (High Risk)
Dengue I (Dengue Fever and DHF Grades I & II)
Dengue II (DHF Grades III & IV),
Acute Gastroenteritis (AGE)
Maternity Care Package (MCP)
NSD Package in Level 1 Hospitals
NSD Package in Levels 2 to 4 Hospitals
Caesarian Section Package
Newborn Care Package

Page | 5
For year 2011, what is the average number of days before claims are reimbursed? ___________ For year 2012, what is the average number of days before claims are reimbursed? ___________ What are the most common reasons for a beneficiary to be denied of claims? (Please elaborate)
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
What are the common problems of the facility encountered in filing for claims? (Pls. elaborate) ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Are there reports required to be submitted to any of the PhilHealth offices in relation to its members and their benefits? What are these? (Please elaborate) ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Are there other concerns in relation to the beneficiary or the facility regarding PhilHealth members’ benefits availment and claims processing? ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
THANK YOU! Name: ___________________________________ Date Completed: __________________

Page | 1
Name of Healthcare Facility: Location: (Region, Province, City, Municipality, District/Barangay)
When did the facility receive its DOH license? When did the facility receive PhilHealth accreditation? Accredited as a (check all that apply) Accredited on (date) o Primary Care Benefit Provider o Maternity Care Package Benefit Provider o Anti TB-DOTS Package Provider o Other package provider (Please Specify) Medical Personnel: How many doctors work in the facility? Of these, # of PhilHealth accredited? How many surgeons work in health facility? Of these, # of PhilHealth accredited? How many nurses work in the facility? How many midwives work in the facility? PhilHealth Personnel: How many Philhealth staff in all work in the facility? _____________________ Is there PhilHealth staff in the billing station? How many? ______________ Is there PhilHealth CARES in the premises? How many? ________________ Facility: Bed capacity: _____________ Occupancy rate: ___________ Are there specified accommodations for Sponsored members? ______________ How many NBB beds does the facility have? _____________________________ How many beds in the charity ward of the facility? ________________________
Deliveries:
Total number of deliveries performed by the facility for 2012: ____________________
Deliveries attended by Doctors: ________, Nurses: _________, Midwives: __________
How many availed the Maternal Care Package (MCP)? ______________
How many are Philhealth members/Dependents?_____________________
How many are SP-NHTS members/dependents? ______________________
HEALTH FACILITY QUESTIONNAIRE – Birthing facility
Tracking Coverage and Effectiveness of the National Health Insurance Program (NHIP)
Action for Economic Reforms (AER)
ANNEX C

Page | 2
What services are included in the MCP (check all that applies) Delivery Supplies and other ancillary procedures Postpartum care Labor, delivery and recovery rooms Counseling for reproductive health, breast feeding and newborn screening
Other medically necessary charges for delivery and postpartum care
Room and board Professional fee Drugs and medicines Others (Specify): Laboratory
Total number of newborn managed by the facility in 2012: ________________
How many availed the Newborn Care Package (NCP)? _______________
How many are Philhealth members/Dependents?_____________________
How many are SP-NHTS members/dependents? ______________________
What services are included in the NCP Package (check all that applies) Immediate drying of the newborn Weighing of the newborn Early skin-to-skin contact BCG vaccination Cord clamping First dose of Hepatitis B immunization Non-separation of mother-baby for early breastfeeding initiation
Newborn Screening Test
Eye prophylaxis Newborn Hearing Test Vitamin K administration Pofessional fee Estimated number and amount of MCP claims under NHTS-PR __________________________
Estimated number and amount of MCP claims from Philhealth __________________________
Actual MCP claims received for 2012 under NHTS-PR __________________________________
Actual MCP claims received for 2012 for all Philhealth members _________________________
Estimated number and amount of NCP claims under NHTS-PR __________________________
Estimated number and amount of NCP claims from Philhealth __________________________
Actual NCP claims received for 2012 under NHTS-PR __________________________________
Actual NCP claims received for 2012 for all Philhealth members _________________________
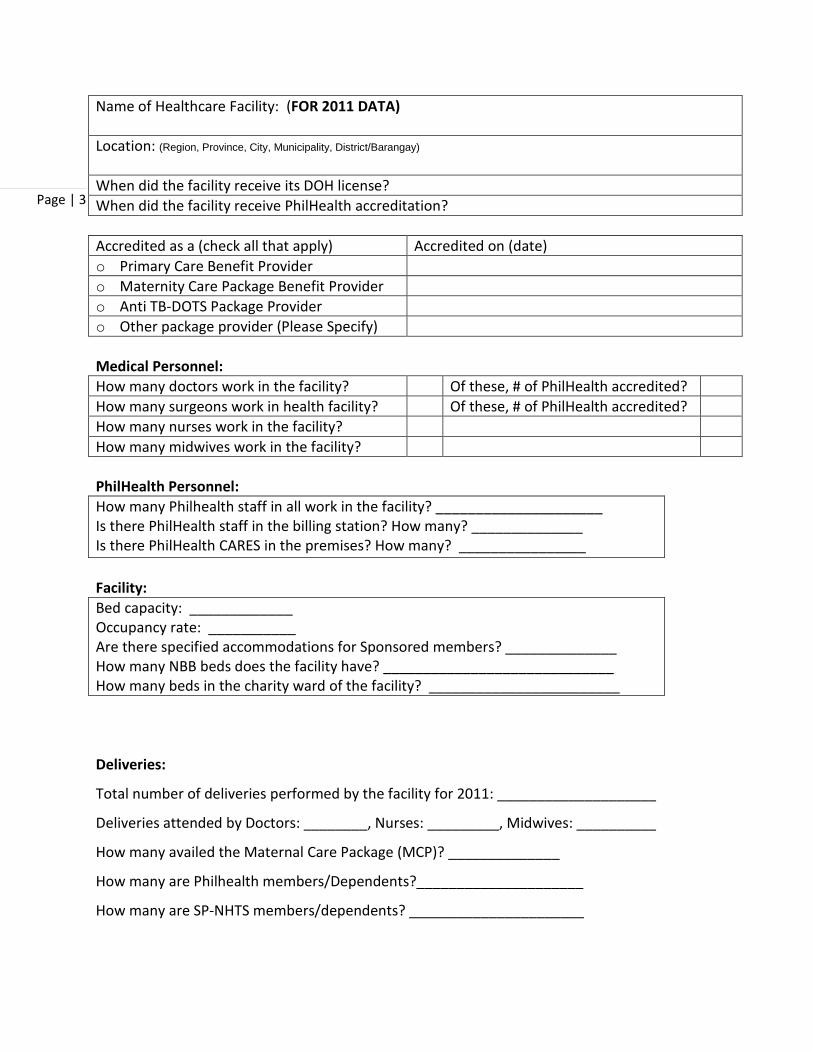
Page | 3
Name of Healthcare Facility: (FOR 2011 DATA) Location: (Region, Province, City, Municipality, District/Barangay)
When did the facility receive its DOH license? When did the facility receive PhilHealth accreditation? Accredited as a (check all that apply) Accredited on (date) o Primary Care Benefit Provider o Maternity Care Package Benefit Provider o Anti TB-DOTS Package Provider o Other package provider (Please Specify) Medical Personnel: How many doctors work in the facility? Of these, # of PhilHealth accredited? How many surgeons work in health facility? Of these, # of PhilHealth accredited? How many nurses work in the facility? How many midwives work in the facility? PhilHealth Personnel: How many Philhealth staff in all work in the facility? _____________________ Is there PhilHealth staff in the billing station? How many? ______________ Is there PhilHealth CARES in the premises? How many? ________________ Facility: Bed capacity: _____________ Occupancy rate: ___________ Are there specified accommodations for Sponsored members? ______________ How many NBB beds does the facility have? _____________________________ How many beds in the charity ward of the facility? ________________________
Deliveries:
Total number of deliveries performed by the facility for 2011: ____________________
Deliveries attended by Doctors: ________, Nurses: _________, Midwives: __________
How many availed the Maternal Care Package (MCP)? ______________
How many are Philhealth members/Dependents?_____________________
How many are SP-NHTS members/dependents? ______________________

Page | 4
What services are included in the MCP (check all that applies) Delivery Supplies and other ancillary procedures Postpartum care Labor, delivery and recovery rooms Counseling for reproductive health, breast feeding and newborn screening
Other medically necessary charges for delivery and postpartum care
Room and board Professional fee Drugs and medicines Others (Specify): Laboratory
Total number of newborn managed by the facility in 2011: ________________
How many availed the Newborn Care Package (NCP)? _______________
How many are Philhealth members/Dependents?_____________________
How many are SP-NHTS members/dependents? ______________________
What services are included in the NCP Package (check all that applies) Immediate drying of the newborn Weighing of the newborn Early skin-to-skin contact BCG vaccination Cord clamping First dose of Hepatitis B immunization Non-separation of mother-baby for early breastfeeding initiation
Newborn Screening Test
Eye prophylaxis Newborn Hearing Test Vitamin K administration Pofessional fee Estimated number and amount of MCP claims under NHTS-PR __________________________
Estimated number and amount of MCP claims from Philhealth __________________________
Actual MCP claims received for 2011 under NHTS-PR __________________________________
Actual MCP claims received for 2011 for all Philhealth members _________________________
Estimated number and amount of NCP claims under NHTS-PR __________________________
Estimated number and amount of NCP claims from Philhealth __________________________
Actual NCP claims received for 2011 under NHTS-PR __________________________________
Actual NCP claims received for 2011 for all Philhealth members _________________________

Page | 5
For year 2011, what is the average number of days before claims are reimbursed? ___________ For year 2012, what is the average number of days before claims are reimbursed? ___________ What are the most common reasons for a beneficiary to be denied of claims? (Please elaborate)
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
What are the common problems of the facility encountered in filing for claims? (Pls. elaborate) ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Are there reports required to be submitted to any of the PhilHealth offices in relation to its members and their benefits? What are these? (Please elaborate) ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Are there other concerns in relation to the beneficiary or the facility regarding PhilHealth members’ benefits availment and claims processing? ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
THANK YOU! Name: ___________________________________ Date Completed: __________________

Page | 1
Name of Healthcare Facility: Location: (Region, Province, City, Municipality, District/Barangay)
When did the facility receive its DOH license? When did the facility receive PhilHealth accreditation? Accredited as a (check all that apply) Accredited on (date) o Primary Care Benefit Provider o Maternity Package Benefit Provider o Anti TB-DOTS Package Provider o Malaria Package Provider o HIV-AIDS o Freestanding Dialysis Clinic o Other package provider (Please Specify) Medical Personnel: How many doctors work in the facility? Of these, # of PhilHealth accredited? How many surgeons work in health facility? Of these, # of PhilHealth accredited? How many nurses work in the facility? How many midwives work in the facility? PhilHealth Personnel: How many Philhealth staff in all work in the facility? _____________________ Is there PhilHealth staff in the billing station? How many? ______________ Is there PhilHealth CARES in the premises? How many? ________________ AS PCB PROVIDER Type of membership of family Number of assigned families Number of Families served SP-NHTS SP-LGU Other SP members Other PHIC members (OG & OFW) Non-PHIC members TOTAL Primary Care Benefits: (NHTS Sponsored Members Only) How many availed of Primary Preventive Services? ___________ How many underwent Diagnostic Examinations? ___________ How many availed of any of the Drugs and Medicines packages? ___________
HEALTH FACILITY QUESTIONNAIRE – Health Unit/Center
Tracking Coverage and Effectiveness of the National Health Insurance Program (NHIP)
Action for Economic Reforms (AER)
ANNEX D

Page | 2
OBLIGATED SERVICES Number of NHTS families served
Total number of families served
Primary preventive services 1. BP measurement Hypertensive Nonhypertensive 2. Periodic clinical breast cancer examination 3. Visual inspection with acetic acid
Benefits/Services Provided No. of members/dependents Given Referred
Primary Preventive Services M D M D 1. Consultation 2. Visual Inspection with acetic acid 3. Regular BP measurements 4. Breastfeeding program education 5. Periodic clinical breast examinations 6. Counselling for lifestyle modification 7. Counselling for smoking cessation 8. Body measurements 9. Digital rectal examination Diagnostic Examinations 1. Complete blood count (CBC) 2. Urinalysis 3. Fecalysis 4. Sputum microscopy 5. Fasting blood sugar (FBS) 6. Lipid profile 7. Chest X-Ray
Medicines Given Number of : Members Dependents
1. Asthma 2. AGE with no or mild dehydration 3. URTI/Pneumonia (Minimal & low risk) 4. UTI 5. Nebulisation services

Page | 3
Estimated number and amount of PFPR claims under NHTS-PR __________________________ Estimated number and amount of PFPR claims on total sponsored program ________________ Actual PFPR received for 2012 under NHTS-PR _______________________________________ Actual PFPR received for 2012 for all sponsored program members ______________________ ============================================================================= TUBERCULOSIS CONTROL PROGRAM Does the health center have a Tuberculosis control program? ___ YES ____NO Number of Tuberculosis cases covered by the program in 2012: ____________________ Is the health center accredited as a Philhealth TB-DOTS Package provider? ____ YES ____NO
If YES, proceed to the questions on as TB-DOTS Package provider If NO, explain why NOT ___________________________________________________ Does the center want to become a philhealth TB DOTS provider? ____ YES ____NO Does the center plan to become a philhealth TB DOTS provider? ____ YES ____ NO
AS TB-DOTS PACKAGE PROVIDER Type of membership of family Number of assigned
families Number of Families served
SP-NHTS SP-LGU Other SP members Other PHIC members (OG & OFW) Non-PHIC members TOTAL Number of NHTS assigned
families served Total Number of families served (availed)
TB-DOTS PACKAGE Estimated number and amount of TB-DOTS claims under NHTS-PR _______________________ Estimated number and amount of TB-DOTS claims on total sponsored program ____________ Actual TB-DOTS claims received for 2012 under NHTS-PR ______________________________ Actual TB-DOTS claims received for 2012 for all sponsored program members ______________

Page | 4
For year 2011, what is the average number of days before claims are reimbursed? ___________ For year 2012, what is the average number of days before claims are reimbursed? ___________ What are the most common reasons for a beneficiary to be denied of claims? (Please elaborate)
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
What are the common problems of the facility encountered in filing for claims? (Pls. elaborate) ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Are there reports required to be submitted to any of the PhilHealth offices in relation to its members and their benefits? What are these? (Please elaborate) ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Are there other concerns in relation to the beneficiary or the facility regarding PhilHealth members’ benefits availment and claims processing? ____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
THANK YOU! Name: ___________________________________ Date Completed: __________________

Questionnaire: Individual Philhealth Members Sponsored Program Beneficiaries (NHTS-PR)
Target Respondent: Sponsored member, spouse/partner, or household member 21 years old and above with adequate knowledge of the sponsored family’s health situation. Background of Sponsored Member: Name: Sex: Age: Occupation/Employment: Educational Attainment:
Barangay: PPP beneficiary: YES, Since when _____________ NO Please enumerate family members of the Sponsored Member (Spouse/partner, children & parents)
NAME SEX AGE RELATIONSHIP TO THE SPONSORED MEMBER
CHECK IF LEGAL DEPENDENT
1
2
3
4
5
6
7
8
9
10
Use another sheet as needed Are there other people who live in the household?
Siblings ____ Grandchildren ____ Grandparents ____ Parents-in-Law ____ Other Relatives ____ Caregivers/Helpers ____ Other Persons ____ None
Who is the head of the household? _____________________________ Relationship to the Sponsored Member? _________________________
Are there other Philhealth Members in the Household? Yes No Relationship to the Sponsored Member? _________________________
Membership Status:
Do you (Does the sponsored member) have a PhilHealth card? (Request respondent if the card can be shown) Yes None (Card shown? Yes No)
Do you (Does the sponsored member) have the Member Data Record (MDR)? (Request respondent if the MDR can be shown) Yes None (MDR shown? Yes No)
ANNEX E

Page 2
How did you get the card? (How did the Sponsored member get the card; Do you know that you are a part of the NHTS-PR)?
� part of NHTS-PR � sponsored by LGU � sponsored by National Government Agency/other public officials � sponsored by private sector � don’t know
Did you apply to be a Sponsored member? (Did the Sponsored member apply to be a member?)
Yes No
How did you apply? (How did the Sponsored member apply?) _____________________________
____________________________________________________________________________________
Since when have (you/he/she) been a sponsored member? (Date) _______________________
Until when is the Sponsored member’s PhilHealth card valid? (Date) _____________________
Where did (you/he/she) get the PhilHealth Card? MSWD/CSWD PhilHealth office Barangay Health Station/Unit Household visit Neighborhood Governor Mayor Others _________
Knowledge:
What are the benefits of being a sponsored member? � NBB policy (mention of free hospitalization) � Case rate payment (mention of per case payment reimbursement) � Case rate packages (mention of any of the case rate packages even without figures) � Non-case rate confinement (mention of benefits for any 24-hour confinement outside of case rates) � Primary Care Benefit (outpatient benefits, preventive measures) � Garantisadong Pambata (mention of healthcare benefits of children 0-14)
Have you (the sponsored member) attended an orientation about the membership? Yes No Where did you (the sponsored member) get information about the sponsored program?
� Household visit by health worker � fliers/posters/brochures � Philhealth branch/Philhealth staff � media/news/radio/newspaper � Philhealth staff in Hospital
� hospital staff � workplace � family/relatives � friends/neighbors � others
Have you (the sponsored member) attended an orientation on reproductive health? Yes No
Has this household been visited by RNheals? Yes No
What was the purpose of the visit? __________________________________________________
____________________________________________________________________________________
Has this household been visited by CHTs and/or other health workers? Yes No
What was the purpose of the visit? __________________________________________________
____________________________________________________________________________________

Page 3
Family Health:
Please accomplish the table for health services availed of during the past 12 months Family Members Has ____ visited
RHUs or other health facilities for primary care services (PCB)?
Has ____ visited RHUs or other health facilities for pre-natal services?
Has ____ consulted a healthcare worker/doctor due to sickness or injury?
Has ____ been confined in a hospital or health facility? (incl. deliveries)
1 2 3 4 5 6 7 8 9 10 Before proceeding to the evaluation below, please accomplish one form for every
confinement of Sponsored Members and legal dependents.
********** Evaluation:
Do you have any comments/suggestions on the sponsored program? _______________________ ____________________________________________________________________________________ ____________________________________________________________________________________
Do you have any comments/suggestions on the healthcare workers? _______________________ ____________________________________________________________________________________ ____________________________________________________________________________________
Do you have any comments/suggestions on the healthcare facilities? _______________________ ____________________________________________________________________________________ ____________________________________________________________________________________
Do you have any comments/suggestions for PhilHealth? __________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________
Are you satisfied with PhilHealth benefits and services? Very Satisfied Satisfied Not Satisfied Don’t Know/No Basis
***************************** THANK YOU

Page 4
Supplementary Questions for Confined Philhealth Members or Dependents Please accomplish one form for every confinement of any of the sponsored member/legal dependents. Name of confined member/dependent: Name of the healthcare facility:
Location: ______________________________________________________________________ City/Municipality: _____________________________________ Private Public: PhilHealth Accredited: Yes No Is the reason for confinement included in the case rate packages? (aided by the enumerator)
Yes No
Which case rate package is applicable? If not a case rate, please indicate the ailment or injury? (aided by the enumerator) ______________________________________________________ Admission and Confinement: Did anyone request for the Sponsored Member’s PhilHealth ID?.............. Yes No
Did anyone request for the Member Data Record (MDR)? ........................ Yes No
Did anyone assist the patient or the member regarding their benefits? ... Yes No
Was the patient assigned to a Philhealth accredited doctor right away?... Yes No
Was the patient assigned to a No Balance Billing (NBB) bed? .................... Yes No
Was the patient asked to buy medicine and other medical supplies? ……. Yes No
How long was the patient confined? ______Days Philhealth Transactions:
Was there a PhilHealth staff in the billing station in the hospital? …………. Yes No
Was the Philhealth staff in the billing station of the hospital helpful? ……. Yes No
Were there other personnel who helped with the PhilHealth transactions? ……… Yes No
Did you have all the requirements needed for the PhilHealth benefits when you got admitted to the hospital? Yes No
Did you have all the requirements needed for the PhilHealth benefits before getting discharged? Yes No
Did you need to go out of the hospital to get PhilHealth’s required documents (e.g. marriage certificate, birth certificate, etc.)? Yes No

Page 5
What was/were these required documents?
Where did you go to get the required documents? (Dswd, Philhealth, employer, house others)
How long did you wait before you were able to get hold of these documents?
Billing, Costs, Claims: Do you know how much the total bill was? Yes No If YES, How much? ……………………..…. Did you pay for anything at the billing station prior to being discharged?.. Yes No If YES, How much did you pay? P_______________
What did you pay for? Please itemize. _____________________________ P_______________ _____________________________ P_______________ _____________________________ P_______________ _____________________________ P_______________ _____________________________ P_______________
Did you file for claims for the hospital bill after being discharged?............. Yes No
If YES, How much was reimbursed? P_______________
Did you file for claims for medicine and other medical supplies?................ Yes No
If YES, How much was reimbursed? P_______________
Do you know how much the total amount of PhilHealth benefits is for the confinement?
Yes No If Yes, How much? P_______________ Room and Board Evaluation:
Did the patient have 3 meals every 24 hours of confinement?................ Yes No (Or the doctor declared the patient was under a special diet?................ Yes No)
Was there accessible drinking water? .................. Yes No
Were there accessible comfort rooms? ................ Yes No
Was the room well-ventilated? ………….................. Yes No
Did the patient share the room with other patients? Yes No
***************************** THANK YOU
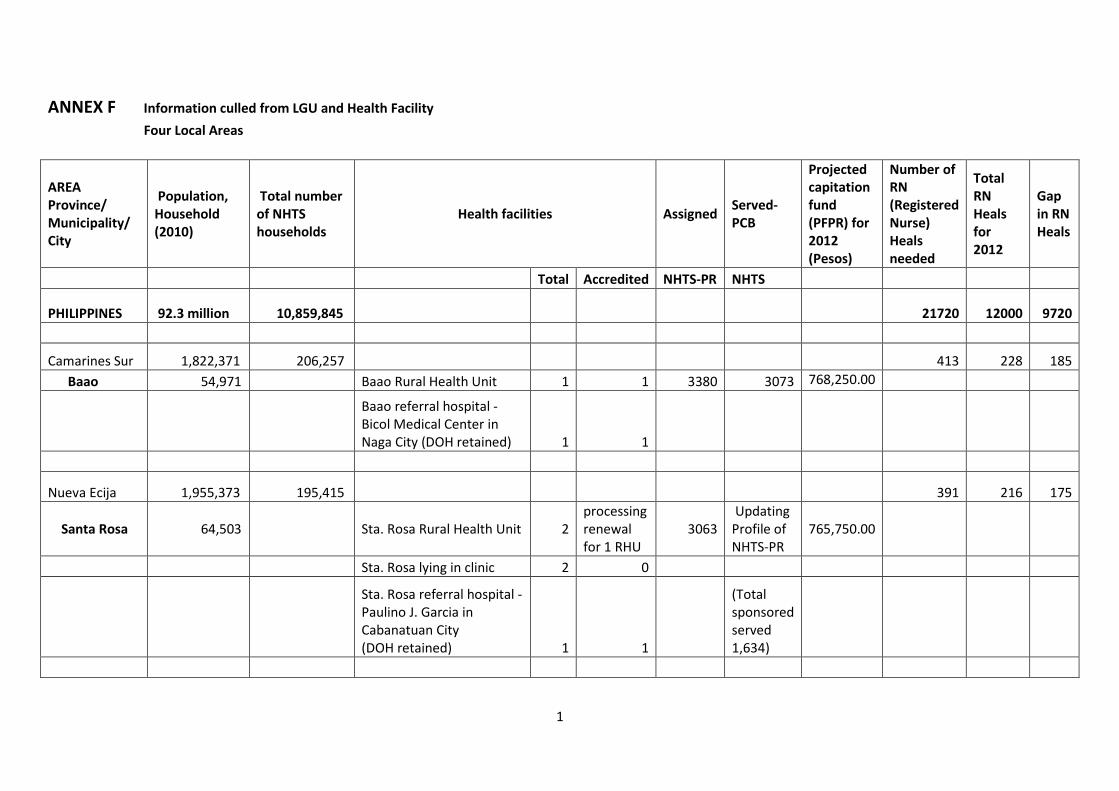
1
ANNEX F Information culled from LGU and Health Facility Four Local Areas
AREA Province/ Municipality/ City
Population, Household (2010)
Total number of NHTS households
Health facilities Assigned Served-PCB
Projected capitation fund (PFPR) for 2012 (Pesos)
Number of RN (Registered Nurse) Heals needed
Total RN Heals for 2012
Gap in RN Heals
Total Accredited NHTS-PR NHTS
PHILIPPINES 92.3 million 10,859,845
21720 12000 9720
Camarines Sur 1,822,371 206,257 413 228 185 Baao 54,971 Baao Rural Health Unit 1 1 3380 3073 768,250.00
Baao referral hospital - Bicol Medical Center in Naga City (DOH retained) 1 1
Nueva Ecija 1,955,373 195,415
391 216 175
Santa Rosa 64,503 Sta. Rosa Rural Health Unit 2 processing renewal for 1 RHU
3063 Updating Profile of NHTS-PR
765,750.00
Sta. Rosa lying in clinic 2 0
Sta. Rosa referral hospital - Paulino J. Garcia in Cabanatuan City (DOH retained) 1 1
(Total sponsored served 1,634)

2
AREA Province/ Municipality/ City
Population, Household (2010)
Total number of NHTS households
Health facilities Assigned Served-PCB
Projected capitation fund (PFPR) for 2012 (Pesos)
Number of RN (Registered Nurse) Heals needed
Total RN Heals for 2012
Gap in RN Heals
Total Accredited NHTS-PR NHTS
Rizal 2,484,840 87,874
176 97 79
Angono 102,407 Angono Rural Health Unit 1 Processing 2295 573,750.00
Angono General hospital - Managed by Rizal Provincial government 1 1
Paranaque City 588,126 24,509 Paranaque city health office 9,508
49 27 32
Barangay health centers (14) 8 8 3131 2908 727,000.00
Lying in clinics (9) 6 0
Barangay health centers-TB-DOTS provider 1 1
Bernabe hospital - Paranaque City managed hospital 1 1

ANNEX G OVERALL FLOW OF RESOURCES IN PHILHEALTH, 2012
Source: Source. Modified from Figure 1 Health Financing Flows in the Philippines, Department of Health, 2010
Households/
Companies USERS
Taxes
DBM
Donors
Budget Allocation – National subsidy to NHTS-PR premium
Other income - fees, penalties, forex
Premiums DOH
PHILHEALTH
Budget- premium of indigent
Income from investment
Rural Health Units (RHU)
Investments
Private health facilities
Benefit Payments
LGU
LGU Hospitals
Other LGU health facilities
Other public hospitals
Public specialty hospitals