experiences of dermatology services transformation julia schofield, principal lecturer university of...
TRANSCRIPT

Experiences of dermatology services transformation
Julia Schofield, Principal Lecturer University of Hertfordshire
Consultant Dermatologist, United Lincolnshire Hospitals NHS Trust

Experiences of dermatology services transformation
• What did the service look like before the redesign work?
• What changes were made and how were they made?
• What the service looks like now• Where there any barriers and how were they
overcome?• Examples of models of service from England

How best to answer these questions?

Setting the scene1997-2010
The Blair years, the NHS and Dermatology : period of unprecedented reform

Reform & modernisation: early stages
• Background of long waiting lists and poor access to services
• NHS Modernisation agency Action on Dermatology (2000-2003)
• Action on Plastic Surgery (2003-2005)• Pilot site work and Good Practice Guidance• Role of GPwSIs and extended role practitioners• Lack of good evidence for what worked


Trends in the number of dermatology patients waiting longer than 26 and 13 weeks to be seen using fourth quarter data 1999-2007, England source www.performance.doh.gov.uk/waitingtimes

So what have we learnt that is important and where is the
evidence?
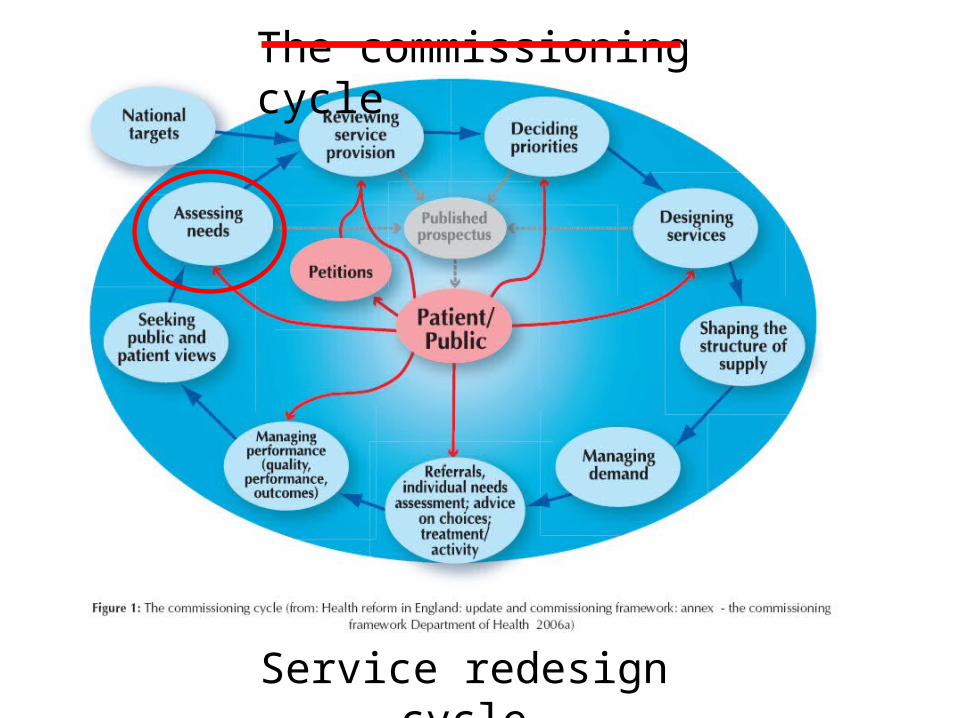
The commissioning cycle
Service redesign cycle

The 2009 Health Care Needs Assessment
• The burden of disease: how much, how expensive, impact?
• How we manage the burden: services available and their effectiveness
• Recommendations for models of care based on the EVIDENCE
http://www.nottingham.ac.uk/scs/documents/documentsdivisions/documentsdermatology/hcnaskinconditionsuk2009.pdf

Structure of the document: chapters
1. Introduction2. Burden of skin disease3. NHS reform and its impact4. Services available and their effectiveness5. Models of care and organisation of services6. Specific skin disease areas7. RecommendationsLots of references!

Linking the evidence to service redesign: ASSESSING NEED
• Coding systems poor, underestimate problem• Skin disease is very common• Lots of people self care and buy OTC products• 24% of the population seek medical advice about a
skin condition each year (12.9 million)• Commonest reason people present to a GP with a
new problem

Skin disease seen by specialists• Limited information, good scottish data*• About 6.1% of people with skin disease are referred to
see a specialist• 35-48% referrals are skin lesions, more in coastal areas• Ever increasing referrals to specialists• Eczema, acne and psoriasis commonly seen• Patients still admitted
*Benton, EC, Kerr, OA, Fisher, A, Fraser, SJ, McCormack, SKA, Tidman, MJ (2008) The changing face of dermatological practice: 25
years' experience. British Journal of Dermatology, 159, 413-8.

Self reported/ self managed skin disease
0.75 million people with skin disease referred for NHS
specialist care, 1.5%
50% population approx 25 million
24% population, 12.9 million seeking Primary Care (England and Wales)
Need: summary of key messages
3752 deaths due to skin disease

Linking the evidence: SERVICE PROVISION
• We MUST define the level of care and the location• Confusion about terms• Primary care means ‘first point of contact care’• Secondary care means ‘specialist care’• Too much talk of ‘shift’ without understanding the
meaning

Define LEVELS of care: self care, generalist, specialist, supra-specialist
From Skin conditions in the UK: a Health Care Needs Assessment Schofield et al 2009

Linking the evidence: service provision
Generalist care• Patients like to be treated by their GP• GP diagnostic skills for skin lesions are not great• Standards for GP skin surgery need to be
improved• Up-skilling of Practice Nurses limited benefit• Community specialist outreach nursing services
effective for chronic skin disease

Linking the evidence: service provision
Specialist care• Dermatologists should be diagnosing the skin
lesions: they are good at it• Dermatologists can prevent hospital admissions
for some conditions• If GPwSIs are to be used, they need to be
accredited• Specialist nurse services for prediagnosed
conditions are effective

Services available: who sees what and where?
Primary careSkin infections
Specialist careSkin lesions 45-60%
WHY?
31-59% are for diagnosis – skin lesions even higher

Service provision: the diagnostic bottleneck
Patients with skin disease requiring diagnosis and
management
Specialist opinion, diagnostic service
Treatment
Surgery
CORRECT DIAGNOSIS=
CORRECT MANAGEMENT

Linking the evidence: DECIDING PRIORITIES
MUST do’s• NICE guidance includes skin cancer, biologics for
psoriasis, atopic eczema• DH access targets 31/62 days for cancer• 18 week patient journey• Choose and Book• Care Closer to Home recommendations

Linking the evidence: deciding priorities
Inequity of access need vs demand• Variable low priority frameworks across
England• Skin surgery• Lymphoedema services• Botulinum toxin services for sweating • ‘One pot spent well’• Decisions should be based on the evidence base

What is need?Need is ‘the ability to benefit from care’Williams HC. J Roy Coll Physicians 1997;31:261-2
The use of the biological agents to treat psoriasis
The use of isotretinoin to treat acne

Demand and supply
Demand = “that which is asked for”
Supply = “that which is provided for”
Williams, HC. J Roy Coll Physicians 1997;31:261-2
Seborrhoeic keratoses – demand or need?

How to save a billion (part II)• Up to £700m could be saved if PCTs decommissioned some
procedures:
“relatively ineffective” Max potential reduction in procedures (%)
Max potential savings (£m)
Tonsillectomy 90 45
Back pain injections & infusion 90 24
Grommets 90 21
Knee washouts 90 20
“Potentially cosmetic”
Aesthetic breast surgery 80 18
Varicose veins 80 18
Inguinal, umbilical & femoral hernias 50 50
Minor skin surgery for non cancerous lesions
25 74

Linking the evidence: DESIGNING SERVICES
• Emphasis on rapid access to diagnosis• Right place, right person, first time• Range of national guidance about models of care• Integrated care• Local specialist services with links to regional and national
specialist services• Services for sick patients in hospital• Day treatment OP phototherapy services• Patients must be involved in the design of services
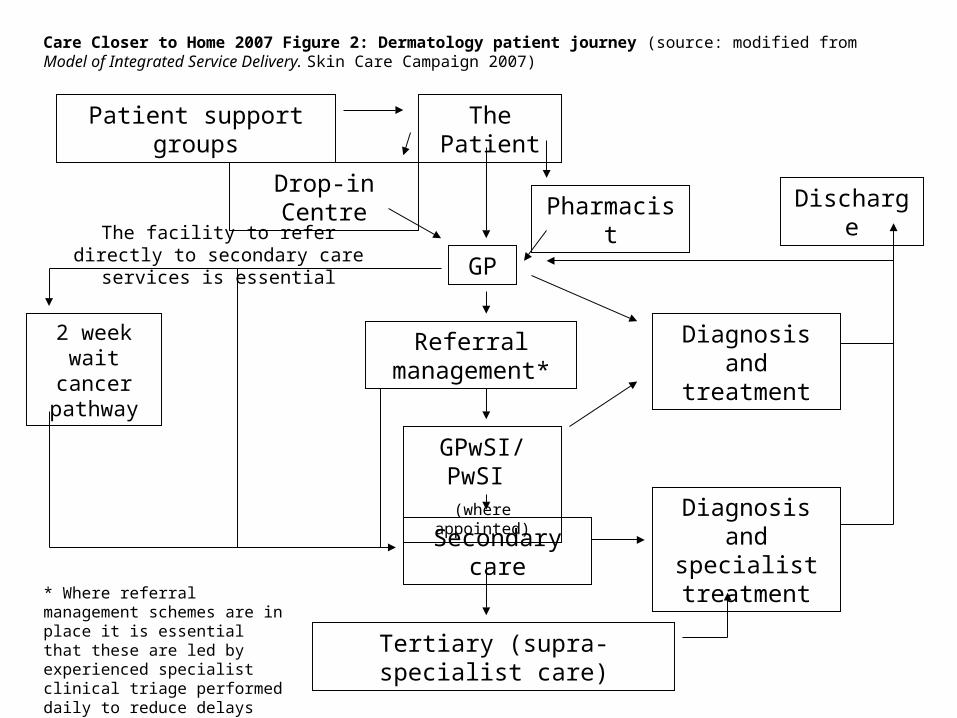
The PatientPatient support groups
Care Closer to Home 2007 Figure 2: Dermatology patient journey (source: modified from Model of Integrated Service Delivery. Skin Care Campaign 2007)
GP
GPwSI/PwSI (where appointed)
Secondary care
Tertiary (supra-specialist care)
Drop-in CentrePharmacist
Referral management*
Diagnosis and treatment
Diagnosis and specialist treatment
Discharge
2 week wait cancer
pathway
* Where referral management schemes are in place it is essential that these are led by experienced specialist clinical triage performed daily to reduce delays
The facility to refer directly to secondary care services is essential
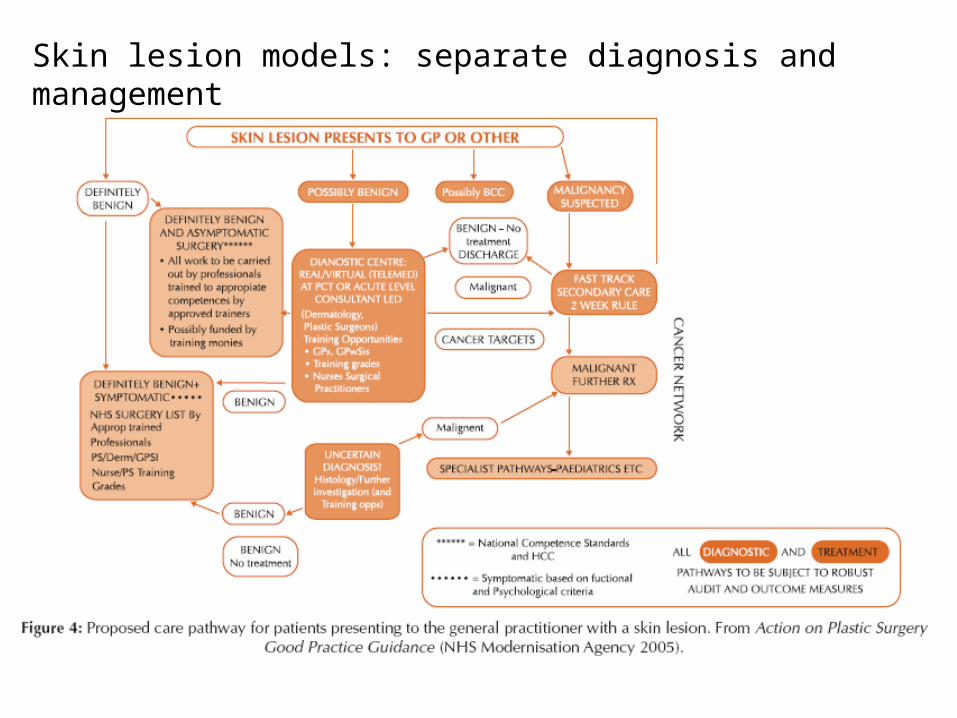
Skin lesion models: separate diagnosis and management

18 week skin lesion pathway
Linking the evidence: designing services
• Shifting care to community settings does not necessarily reduce activity or cost
• There is a link between a reduction in wait times and increased referral rates
• National standards and review are in place for skin cancer services

Linking the evidence: designing services
• GPwSI services improve access but do not reduce cost
• Specialist nurses working with specialist teams are effective
• Specialty and Associate Specialist doctors are interested in working in new models of care

Linking the evidence: designing services
• Teledermatology useful for remote areas• ‘Store and forward’ digital image and referral
useful• Clinically-led guidelines may be helpful but a
lot of work!• Referral management services (RMS) evidence
free zones*. ? Role of Tier 2 services/ Clinical Assessment and Treatment services
Davies, M, Elwyn, G (2006) Referral management centres: promising innovations or Trojan horses? BMJ, 332, 844-6.

Referral management services
Referral management centres• Paper/electronic process• Count referrals• Assess quality and reduce inappropriate
referrals• Redirect referrals to appropriate service• May lack clinical input

Referral management services
DH guidance 2006• Must not lengthen patient journey• Must carry clinical support• Should confer real diagnostic or treatment
benefit• Not be imposed without agreement• In England largely financially driven

Experience of a Clinical Assessment and Treatment Service in Hertfordshire
• Specialist led, GPwSIs, consultant outreach, specialist nurses
• Specialist triage• Community settings• Routine, straightforward dermatology• Patients happy, good service• Robust governance and quality

Urgent
ROUTINE
Pre-diagnosedN/L eczema
N/L psoriasis
N/L leg ulcer
GPwSI
Consultant outreach
Consultant appointment
ROUTINE
Needs specialist services
OUTCOME
Discharge or follow up
2 week wait
Consultant/Associate Specialist triage
Dermatology Service from September 2007
Referral to CATS service Other referrals
Triage CHOICE
CHOICE
CHOICE
Wellswood House
Borehamwood
Skin surgery

Impact on secondary care referral rates
0
50
100
150
200
250
300
350
400
Sept Oct Nov Dec Jan Feb Mar Apr May June July Aug
Pre-CATS CATS period

BUT: total referral activity including CATS referrals increased
0
100
200
300
400
500
600
Sept Oct Nov Dec Jan Feb Mar Apr May June July Aug
Pre-CATS CATS period TOTAL
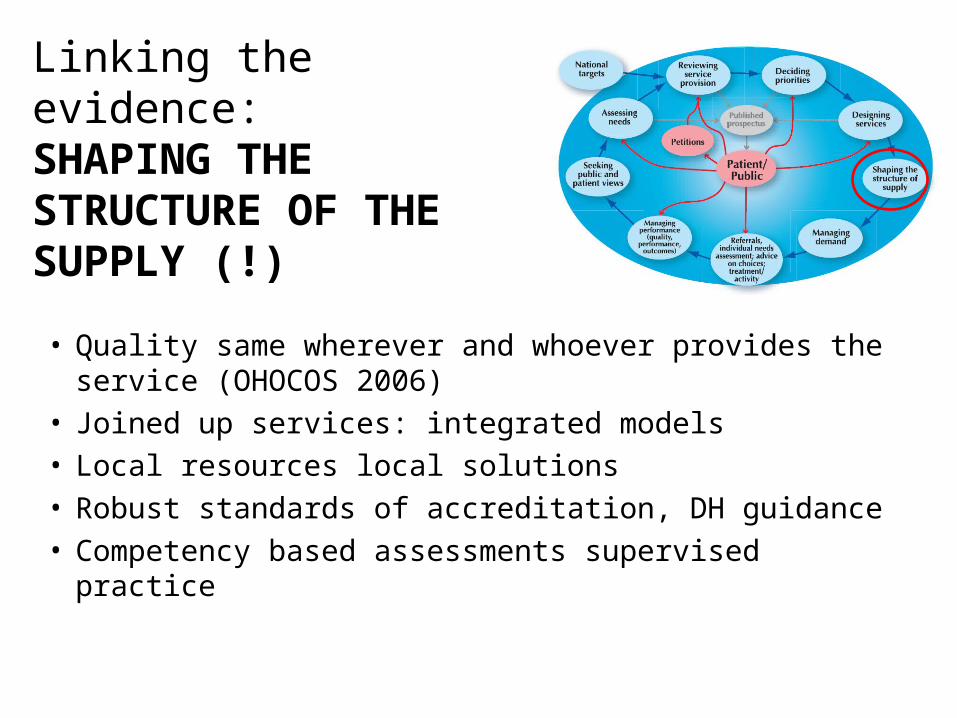
Linking the evidence: SHAPING THE STRUCTURE OF THE SUPPLY (!)
• Quality same wherever and whoever provides the service (OHOCOS 2006)
• Joined up services: integrated models• Local resources local solutions• Robust standards of accreditation, DH guidance• Competency based assessments supervised practice

Linking the evidence: MANAGING THE DEMAND
• General Practitioner will remain the gatekeeper• Resources are finite and demand will need to be
managed• No evidence that strategies to date are effective• Priority setting may be the key• Need vs demand increasingly an issue

GP as gatekeeper: education and training• Limited undergraduate training• Postgraduate training not compulsory• GP curriculum could map better to what is
seen in practice• Training and education important• Not a short term solution

18% more patients seen5.6% more new patients seenFewer people waiting
24% rise in consultant numbers
The final piece of evidence to think on

Implementing the 18 week target
Presented the evidence• Service redesign cycle• Needs Assessment• Burden of skin disease• Service provision• Models of care• Referral management
No magic wand!

THANK YOU
The HCNA is available free at:http://www.nottingham.ac.uk/scs/documents/documentsdivisions/documentsdermatology/hcnaskinconditionsuk2009.pdf
Hard copies can be purchased from the Centre of Evidence based Dermatology for a nominal sum from [email protected]