experiential education and public health: the potential to move america toward health
DESCRIPTION
Experiential Education and Public Health: The Potential to MOVE America toward Health. Aleta L. Meyer, Ph.D. National Institute on Drug Abuse 5 th Annual Research and Evaluation on Adventure Programs Symposium Atlanta, GA March 18, 2009. Overview. - PowerPoint PPT PresentationTRANSCRIPT
Experiential Education and Public Health: The Potential to MOVE America toward Health
Aleta L. Meyer, Ph.D.National Institute on Drug Abuse
5th Annual Research and Evaluation on Adventure Programs SymposiumAtlanta, GAMarch 18, 2009
Overview
REAP 2008 – Federal Funding to Support Research on Adventure Programs – Focus on Drug Use
Casting the Net to Other Health Areas Experiential Approaches (NIH-funded) The “State” of Best Practices Type I and Type II Translation Research Federal Funding for Research & Training Positive Risk-Taking Adventure for Thought
NIDA-funded Prevention and Prevention Services Research
National Institute on Drug Abuse (NIDA)
NIDA’s Prevention Research Branch supports a theory driven program of basic, clinical, and services research across the lifespan to reduce risks and prevent the initiation and progression of drug use to abuse and prevent drug-related HIV acquisition, transmission and progression.
Additional Outcomes of Interest Proximal problems related to substance
use (e.g., early aggression, academic failure, association with deviant peers, poor peer relationships, family conflict and poor parental management skills);
Conditions which are co-morbid with drug use (e.g., psychiatric disorder); or
Conditions which share etiology with drug use (e.g., interpersonal violence).
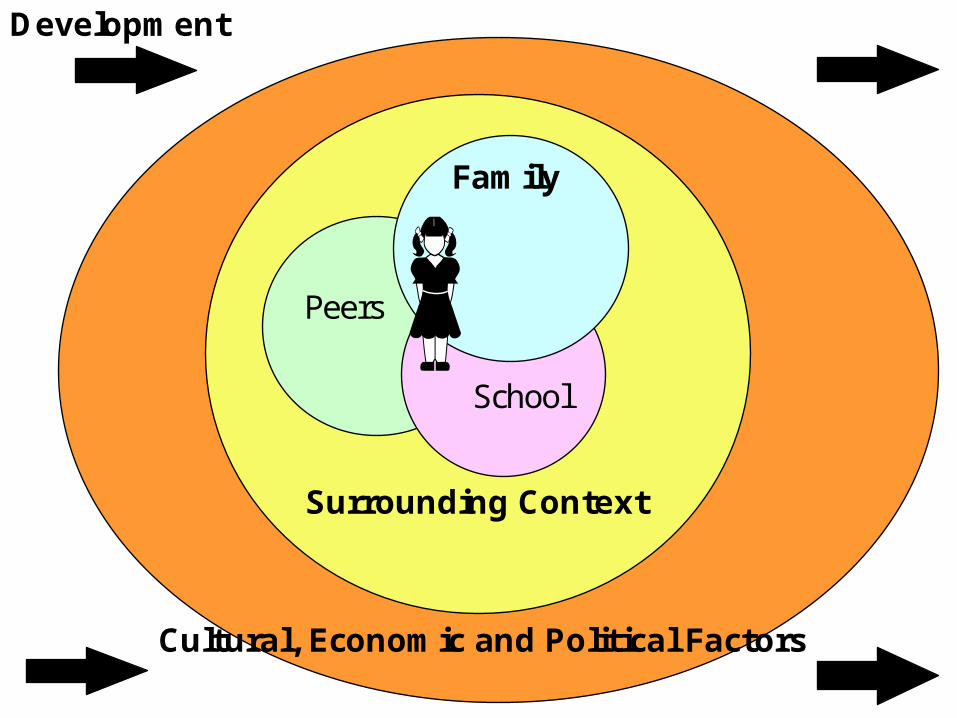
Family
Surrounding Context
Cultural, Economic and Political Factors
School
Peers
Development
Guiding Principles for Substance Use Prevention that Link to Other Health Outcomes
Development in context / Experimental etiology Intervening Early in Families
To address problematic trajectories (e.g., early aggression) To promote successful transition to school (e.g., improved regulation and
social-emotional functioning) School-Based Approaches (Universal, Selected, Indicated)
During key developmental transitions (e.g., transition into school, early adolescence)
Address risk and protective factors relevant to drug use, violence, and other outcomes
Evidence for short-term, long-term, and cross-over effects Increase Reach of Evidence-based Programs (Type 2 Translation)
Research on factors associated with the adoption and utilization of scientifically validated interventions by service systems and settings under controlled, uncontrolled or uncontrollable conditions
Impact of implementation quality on outcomes Strategies for optimal adaptation of curriculum Economic analysis of evidence-based programs Development of community coalitions and examination of impact
Behavioral Interventions that Impact Underlying Biological Processes Related to Regulation
Multidimensional Treatment Foster Care - designed to improve foster parent skills (increase reinforcement relative to discipline) (Chamberlain et al.)
Fisher et al. examined its impact on HPA axis dysregulation in preschoolers
Effects of disruptions on the brain Maltreated children tend to have dysregulated cortisol rhythms
They display lower cortisol levels upon awakening and lower declines from morning to evening
Under routine conditions in regular foster care, placement changes appear to disrupt the regulation of the HPA axis resulting in less stable, more blunted HPA activity
It appears this can be mitigated by interventions that focus on providing stability, routine, nurturing, and planned transitions
Children in MTFC-P maintained a more normal diurnal rhythm during the 6 months after transition into a new placement
Fisher, Van Ryzin, & Gunnar (submitted)
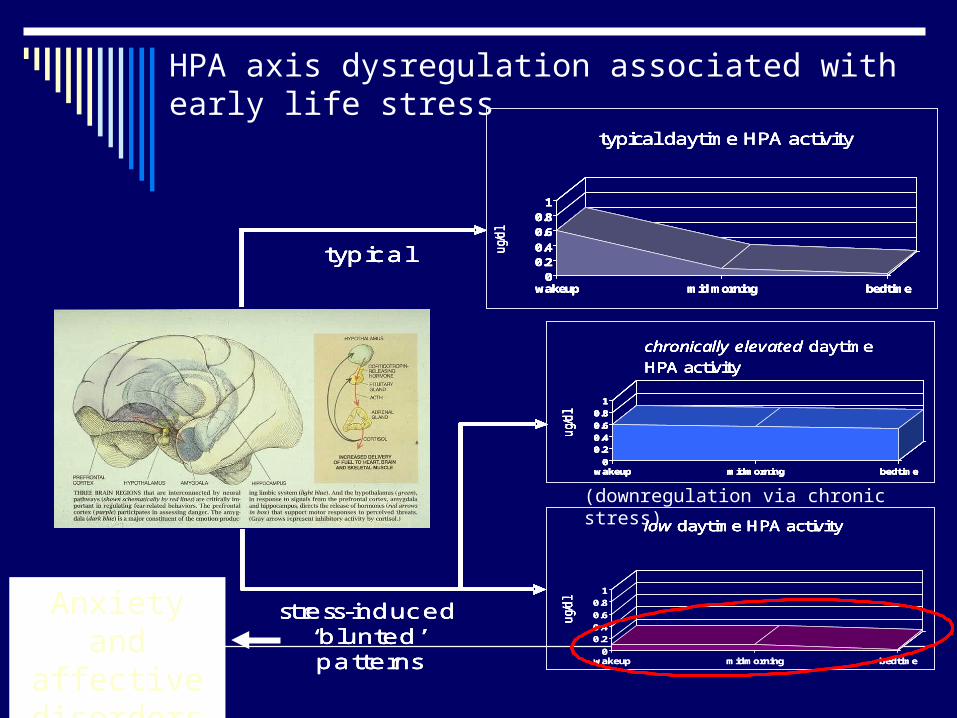
HPA axis dysregulation associated with early life stress
0
0.2
0.4
0.6
0.8
1
wakeup midmorning bedtime
00.20.4
0.60.8
1
wakeup mid morning bedtime
typical daytime HPA activity
ug/
dl
typical
low daytime HPA activity
ug/
dl
chronically elevated daytime HPA activity
ug/
dl
0
0.2
0.4
0.6
0.8
1
wakeup midmorning bedtime
stress-induced ‘blunted’patterns
0
0.2
0.4
0.6
0.8
1
wakeup midmorning bedtime
00.20.4
0.60.8
1
wakeup mid morning bedtime
typical daytime HPA activity
ug/
dl
typical
low daytime HPA activity
ug/
dl
chronically elevated daytime HPA activity
ug/
dl
0
0.2
0.4
0.6
0.8
1
wakeup midmorning bedtime
stress-induced ‘blunted’patterns
00.20.4
0.60.8
1
wakeup mid morning bedtime
typical daytime HPA activity
ug/
dl
typical
low daytime HPA activity
ug/
dl
chronically elevated daytime HPA activity
ug/
dl
0
0.2
0.4
0.6
0.8
1
wakeup midmorning bedtime
00.20.4
0.60.8
1
wakeup mid morning bedtime
typical daytime HPA activity
ug/
dl
typical
low daytime HPA activity
ug/
dl
low daytime HPA activity
ug/
dl
chronically elevated daytime HPA activity
ug/
dl
chronically elevated daytime HPA activity
ug/
dl
0
0.2
0.4
0.6
0.8
1
wakeup midmorning bedtime
stress-induced ‘blunted’patterns
(downregulation via chronic stress)
Anxiety and affective disorders
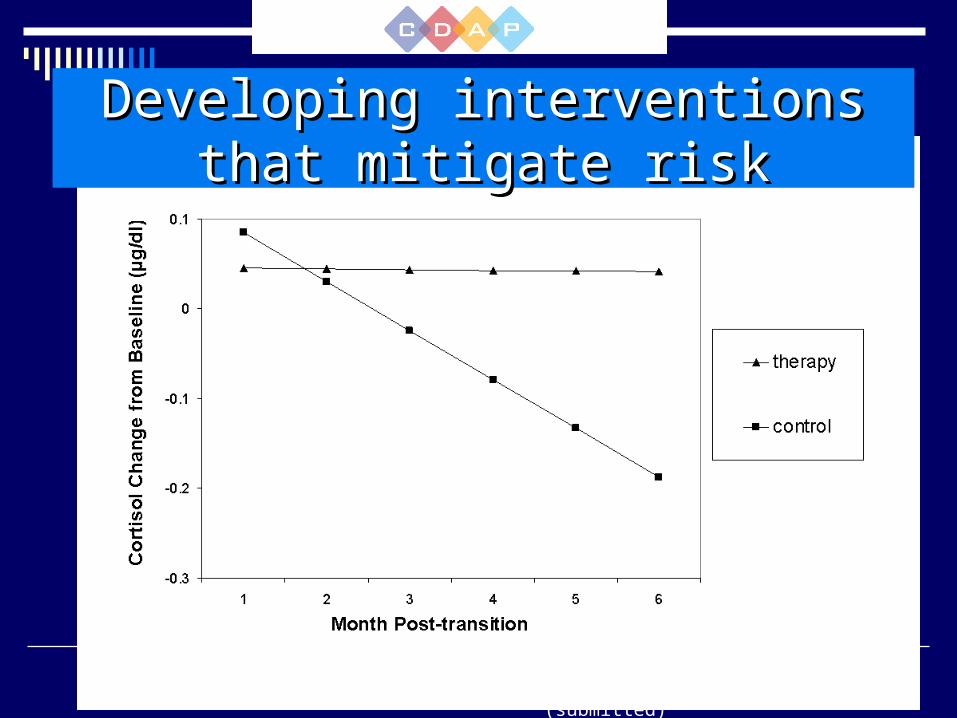
Fisher, Van Ryzin, & Gunnar (submitted)
Developing interventions that Developing interventions that mitigate riskmitigate risk
New Approach for NIDA
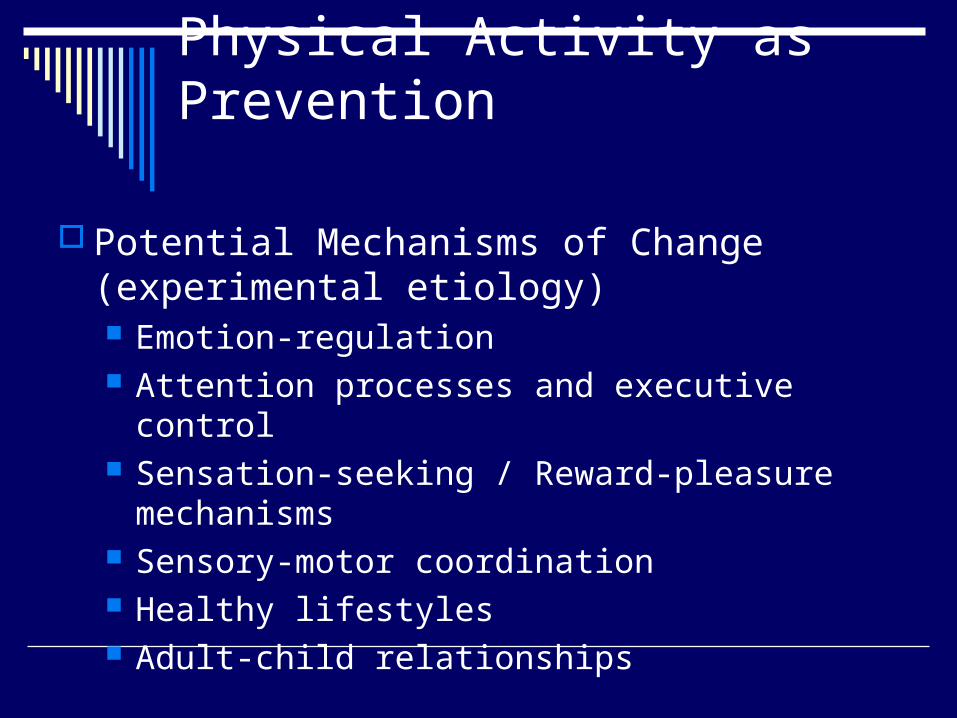
Physical Activity as Prevention
Potential Mechanisms of Change (experimental etiology) Emotion-regulation Attention processes and executive control Sensation-seeking / Reward-pleasure mechanisms Sensory-motor coordination Healthy lifestyles Adult-child relationships
Science Meeting Agenda
Panel 1: Physical Activity in Prevention Interventions
Panel 2: Technological Tools for Assessing Physical Activity
Panel 3: Informing Drug Abuse Prevention Through Research on the Epidemiology and Etiology of Physical Activity and Substance Use
Panel 4: Physical Activity and Mood — Implications for Prevention
Panel 5: The Potential Role of Physical Activity on Attention and Other Cognitive Processes — A New Paradigm for Drug Abuse Prevention?
Panel 6: Physical Activity and Reward Mechanisms — A Model for Prevention Intervention Development
Funding Opportunity Announcement
Interactions between Physical Activity and Drug AbuseRFA-DA-09-013 (R01), RFA-DA-09-014 (R03)
Receipt Date: January 29,2009
Over 70 applications
Program Officials (e.g., research cheerleaders)
Advice and GuidanceWhat’s Hot: New initiatives
Answer your scientific questions Review Issues: Dos and Don’tsDiscuss funding alternatives
In other words, send a 2-3 page concept! [email protected]
Casting the Net to Other Health Areas
Experiential Education and Public Health: The Potential to MOVE America toward Health
Scary Health Costs
In 2007, the U.S. spent over $2.2 trillion on health care, and 75 cents of every dollar went towards treating patients with one or more chronic diseases
If the prevalence of obesity was the same today as in 1987, health care spending in America would nearly be 10 % lower per person – about $200 billion less
The Preventable Behaviors that Cause Scary Health Costs
The CDC estimates that 80% of heart disease
and stroke 80% of Type 2
diabetes 40% of cancer
Could be prevented if American’s did these three things:
Stop smoking Start eating healthy Get in shape
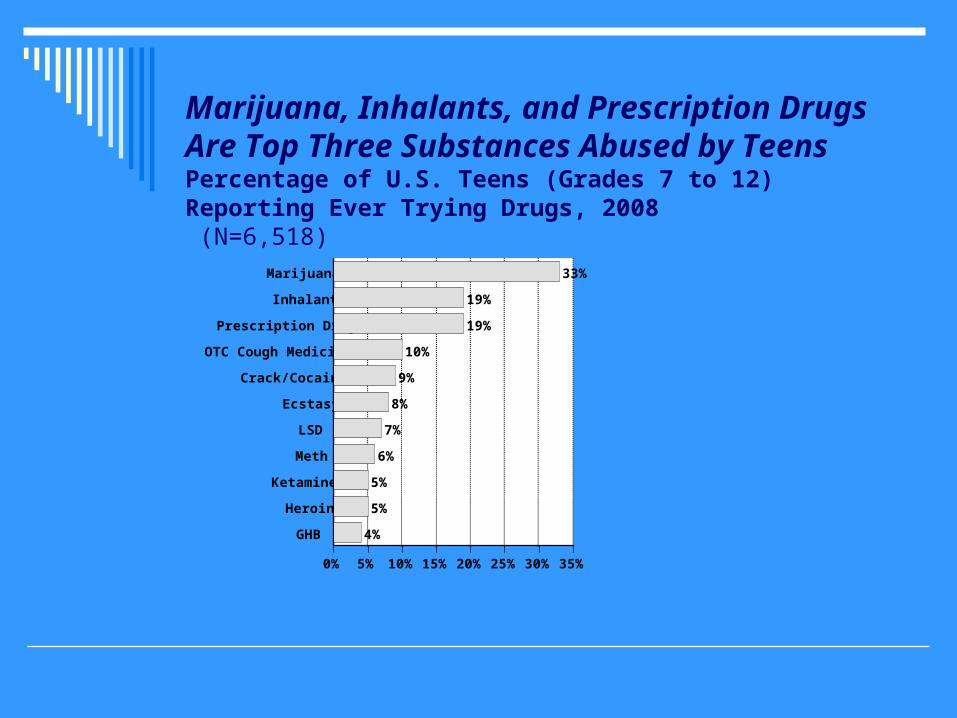
Marijuana, Inhalants, and Prescription Drugs Are Top Three Substances Abused by TeensPercentage of U.S. Teens (Grades 7 to 12) Reporting Ever Trying Drugs, 2008 (N=6,518)
0% 5% 10% 15% 20% 25% 30% 35%
Marijuana
Inhalants
Prescription Drugs
OTC Cough Medicine
Crack/Cocaine
Ecstasy
LSD
Meth
Ketamine
Heroin
GHB
33%
19%
19%
10%
9%
8%
7%
6%
5%
5%
4%
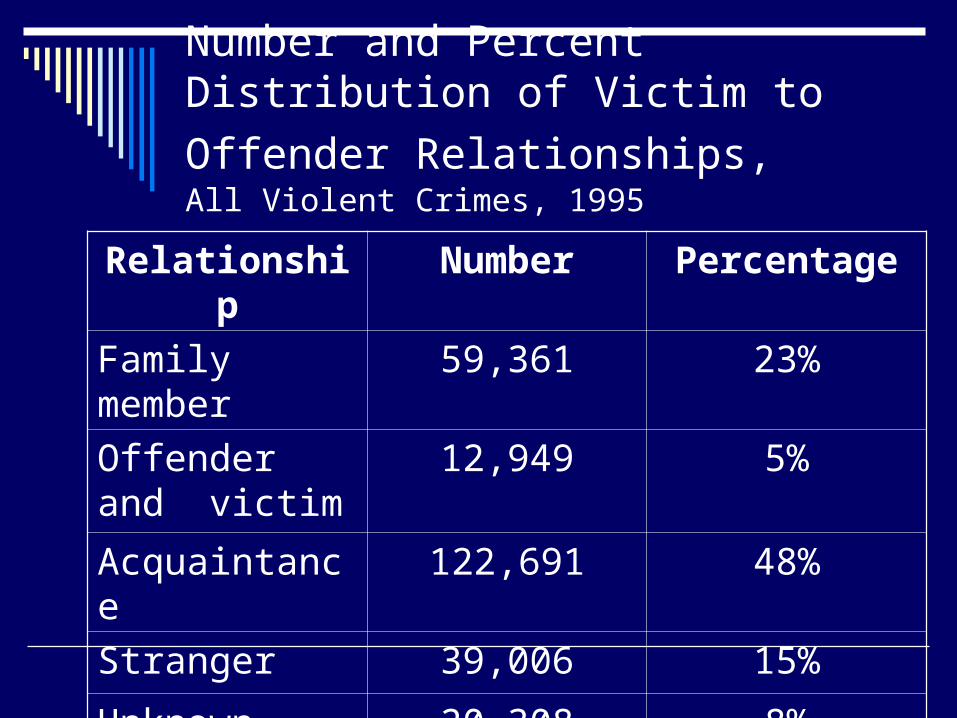
Number and Percent Distribution of
Victim to Offender Relationships, All Violent Crimes, 1995
Relationship Number Percentage
Family member 59,361 23%
Offender and victim
12,949 5%
Acquaintance 122,691 48%
Stranger 39,006 15%
Unknown Relationship
20,308 8%
Universal, School-Based Violence Prevention as an Example
Failure of educational and attitude-only programs to sustain behavior change
Skills and small group interaction based approaches
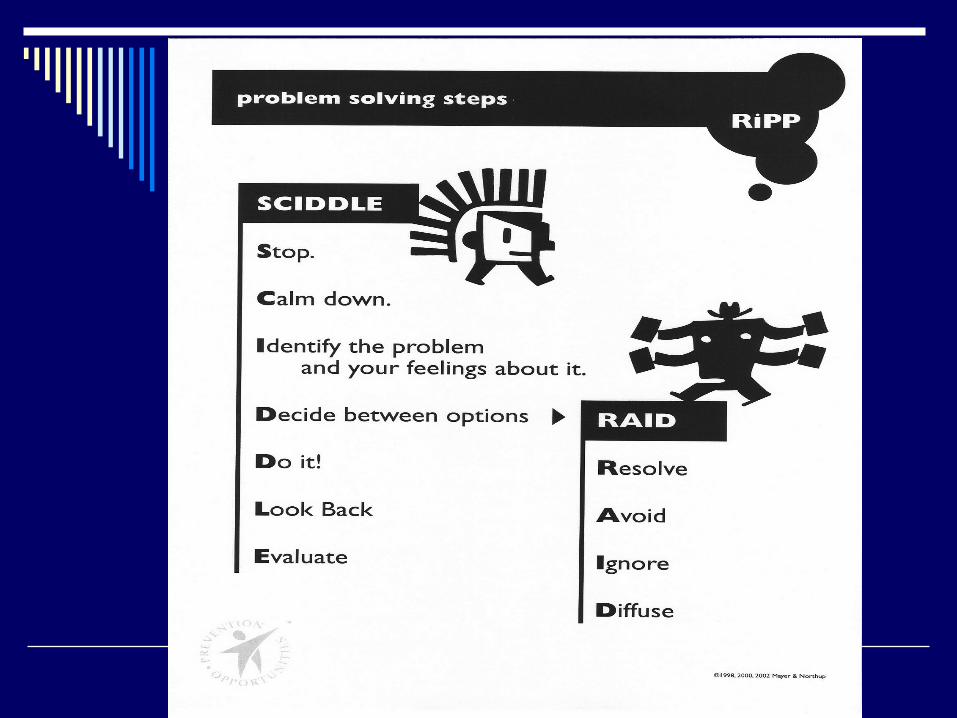
Responding in Peaceful and Positive Ways
Appeal of Experiential Approaches
Four categories of adventure programs (Priest, Gass & Gillis, 2000/2003) Recreational feelings Educational thinking and feelings Developmental social behaviors, thinking, and
feelings Treatment or therapy decreasing dysfunctional
behaviors and improving functional behaviors, social behaviors, thinking and feeling

Active approaches that are fun
How to teach diffuse? Tenkan
Appeal of moving beyond fun activities to intentional, experiential approaches “…simply going camping with juvenile offenders may produce youth more capable of living in the wilderness, but not necessarily youth more capable of succeeding in society.”
Consider the cumulative effects of inactivity, quick fix orientation to discomfort, and negative interactions with those we care about….
What can Adventure teach U.S. about…
Physical activity? Healthful eating? Natural highs? Social support? Coping with stress? Conflict resolution?
Adventure as Prevention or Treatment?
Potential Mechanisms of Change (experimental etiology) Emotion-regulation Attention processes and executive control Sensation-seeking / Reward-pleasure mechanisms Sensory-motor coordination Healthy lifestyles Adult-child relationships
Experiential Intervention Processes
Immediate feedback (e.g., reinforcement and consequences)
Skill development (e.g., behavioral enactment and rehearsal)
Emotion-affect link to real-life experiences (e.g., building a personal history of experience)
Social interaction Development of specific competencies Becoming teachable and coachable
Experiential Approaches Funded by NIH
Across NIH institutes
Different funding mechanisms R03 R21 R34 R01 P and U mechanisms K’s and supplements
HealthWise South Africa: Life Skills for
Young Adults
Funded by National Institute on Drug Abuse
Promoting healthy development and reducing risky behavior at a crucial developmental time point: early to middle adolescence
Examined the impact of the HealthWise school-based curriculum on substance use, violence, and sexual risk behaviors among low-income 8th and 9th grade students in South Africa.
The HealthWise program builds upon Botvin’s Life Skills Training and is designed: To help youth understand the benefits of leisure To avoid boredom and develop interests To teach youth leisure skills (such as how to plan for leisure and
overcome constraints) To encourage youth to take personal responsibility around making
healthy, meaningful, and developmentally productive choices in one’s free time.
Reduce risk behaviors by increasing the influence of protective factors
Comprehensive intervention In-school curriculum After school strategy
Targeted risk behaviors -- substance use, sexual risk behavior, and enacting violence
12 lessons in grade 8 3 50-min. classes per
lesson 6 booster lessons in grade 9
2-3 50-min classes per lesson
Implemented by trained teachers
Linkages with recreation and health providers
Skills to make leisure more positive and meaningful
Self-management skills (e.g., reduce anger, anxiety, stress)
Negotiating relationships Identifying and avoiding risky
situations Learning facts about sexual
risk behavior and substance misuse
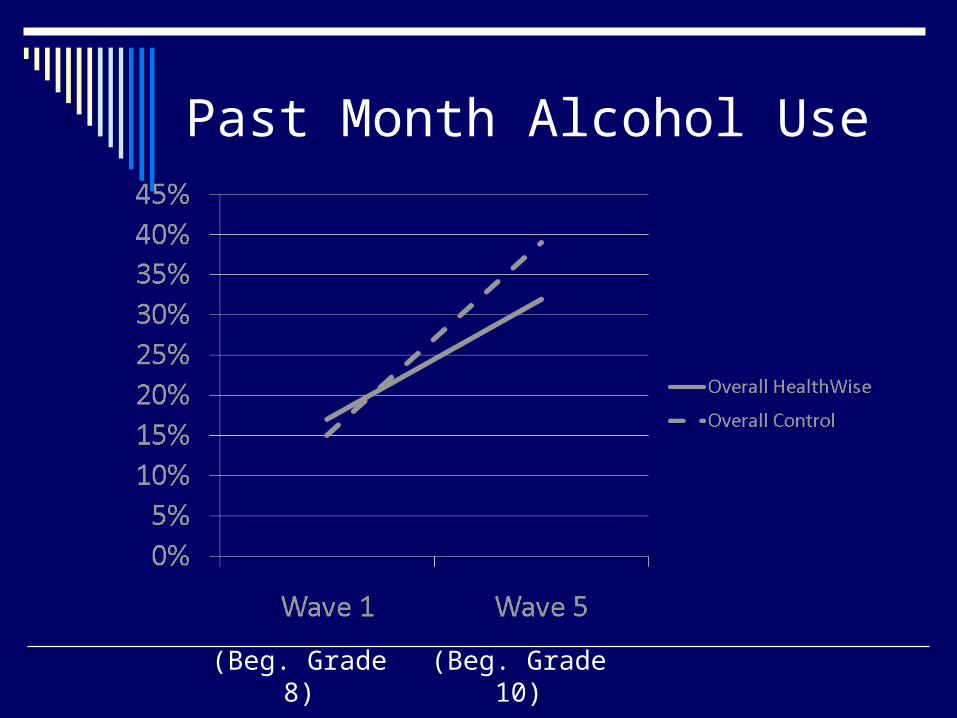
Past Month Alcohol Use
(Beg. Grade 8) (Beg. Grade 10)
Results of HealthWise in South Africa
Positive effects on cigarette and alcohol use (and condom use self-efficacy) are very encouraging and indicate the program is a potentially promising efficacious program that may be helpful in reducing some risk behaviors among low-income adolescents in South African and elsewhere.
Smith, E., Palen, L., Caldwell, L., Flisher, A., Graham, J., Mathews, C., Wegner, L., & Vergnani,T. (2008). Prevention Science e pub.
Physical Activity in Adults and Early Adolescence
Improving Safety and Access for Physical Activity – D. Wilson (R01-NIDDK)
Self-Determination for Increasing Physical Activity – D. Wilson (R01-NICHD)
Experiential Approaches for Normative Transitions
Community Partnership to Affect Cherokee Adolescent Substance Abuse – J. Lowe (R01 – NIDA)
The Senior Odyssey: A Test of the Engagement Hypothesis of Cognitive Aging Stine-Morrow R01-NIA
Early Childhood
The CIA (Children in Action) Program – T. Nicklas R21-NICHD
Measuring Physical Activity Affordances in Preschool Outdoor Environments R. Moore R21-ES
Stress and Trauma
Stress Reduction: Impact on BP in African American Youth F-Treiber R01-NHLBI
Mindful Awareness in Body-Oriented Therapy for Women's Substance Abuse Treatment C. Price R21-NIDA
A First-Line Community-Based Mindfulness Trauma Intervention M. Dutton R34 - NIMH
Cessation and Relapse Prevention
Group Therapy for Nicotine Dependence D. Wetter R01-NIDA
Experiential Avoidance and Substance Use Relapse N. Chawla F31-NIDA
The State of “Best Practices”
Although there has been tremendous progress in the area of evidence-based practices, prevention and treatment efforts to sustain health behavior change have not had the hoped for impact on public health.
A Familiar Story
Despite great outcomes in efficacy and effectiveness trials, dissemination and sustainability not happening.
NIDA and SAMSHA efforts
Steve Aos at University of Washington
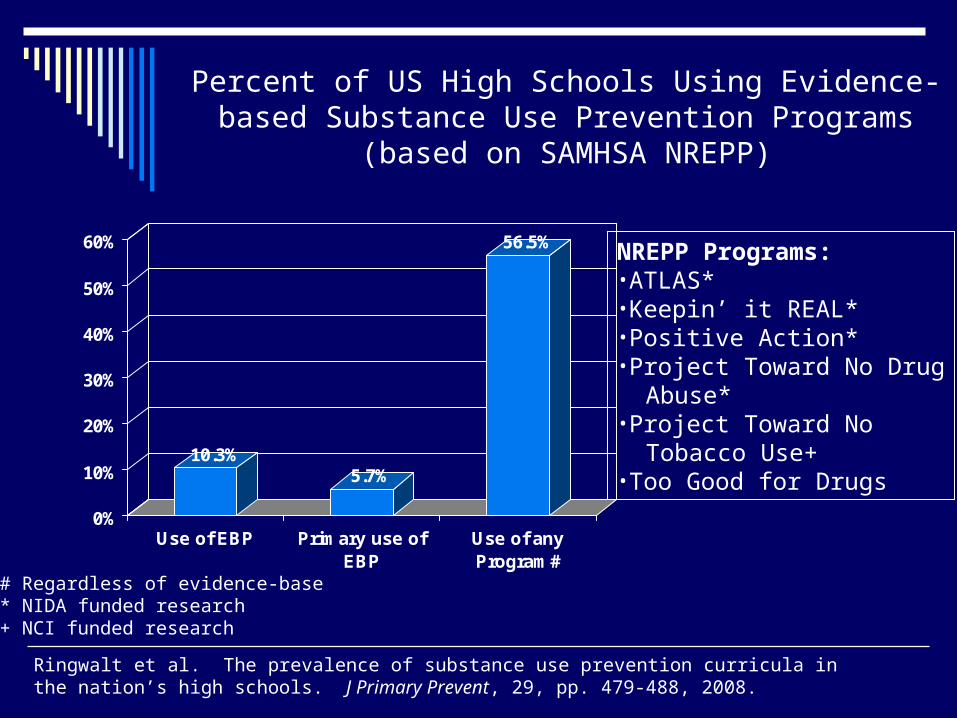
10.3%5.7%
56.5%
0%
10%
20%
30%
40%
50%
60%
Use of EBP Primary use ofEBP
Use of anyProgram#
NREPP Programs:•ATLAS*•Keepin’ it REAL*•Positive Action*•Project Toward No Drug Abuse*•Project Toward No Tobacco Use+•Too Good for Drugs
Ringwalt et al. The prevalence of substance use prevention curricula in the nation’s high schools. J Primary Prevent, 29, pp. 479-488, 2008.
Percent of US High Schools Using Evidence-based Substance Use Prevention Programs (based on SAMHSA
NREPP)
# Regardless of evidence-base* NIDA funded research+ NCI funded research
Type One and Type Two Translation Research
Type One Applies basic science discoveries to the development of interventions for the prevention and treatment of drug abuse, i.e., clinical research. Usually called “bench to bedside.”
Families that have dinner together…. Link this to Russell’s concurrent model… Role of bursts of exercise on academic performance Role of motivation in physical activity (Presidential
Guidelines) Drug preferences change….natural highs??
Type One and Type Two Translation Research
Type Two Research on factors associated with the adoption and utilization of scientifically validated interventions by service systems under controlled, uncontrolled or uncontrollable conditions, i.e., services research. CLINICAL PROCESSES IN DRUG ABUSE PREVENTION –
D. Coatsworth R01-NIDA Implementation of Adventure Programs
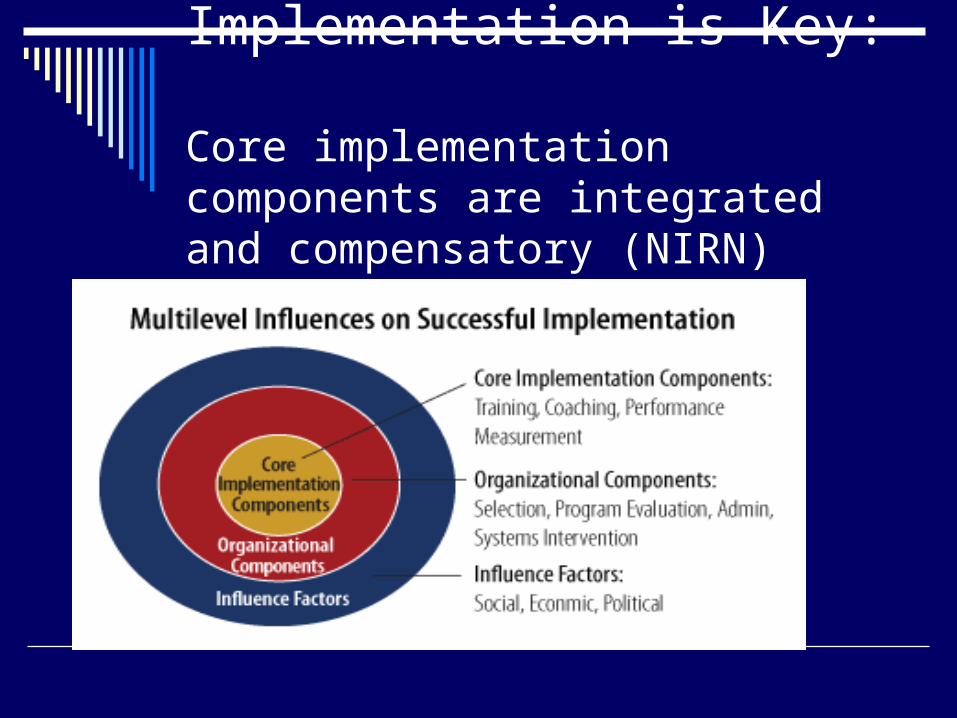
Implementation is Key: Core implementation components are integrated and compensatory (NIRN)
Center Tests
NIH Funding Opportunities
American Recovery Act (ARRA) Challenge Grants Additional RFA’s
Existing Program Announcements Drug Abuse Prevention Intervention Research
PA-08-217 (R01), PA-08-218 (R21), PA-08-219 (R03) Reducing Risk Behaviors by Promoting Positive Youth
Development PA-08-241 (R01), PA-08-242 (R03)
Training Opportunities Diversity Supplements Transition Awards
Educators, Scientists and Contemplatives Dialogue on Cultivating a Healthy Mind, Brain, and Heart
Because experiences can effect individuals on all levels…
Physiological Emotional Cognitive Psychological Social Historical
…the experiential approach has tremendous potential to sustain behavior change over time
Compared to didactic, skills-based, and educational modalities…
Experiential modalities…
Have naturally-occurring behavioral reinforcement built-in
Can provide metaphors to promote transfer of learning
Offer a learning style favored by many