expert board - medicine.gisap.eu file1 contents n. timchenko, o. kovalska, n. timchenko, danylo...
TRANSCRIPT


Expert board:
Alexander Chiglintsev (Russia), Bakar Sudhir (India, USA), George Cruikshank (UK), Marvat Khaibullin (Kazahkstan), Shorena Vashadze (Georgia), Vasyl’ Ruden’ (Ukraine), Yuriy Lakhtin (Ukraine), Ekaterina Smetanina (Ukraine), Susanne Krause (Germany), Yelena Sharachova (Russia)
GISAP: Medical Science, Pharmacology №13 Liberal* (July, 2017)Chief Editor – J.D., Prof., Acad. V.V. PavlovCopyright © 2017 IASHE
ISSN 2053-7751ISSN 2054-0795 (Online)
Design: Alexander Stadnichenko, Anastasia Onyskiv, Inna Shekina, Yury Skoblikov
Published and printed by the International Academy of Science and Higher Education (IASHE)1 Kings Avenue, London, N21 3NA, United KingdomPhone: +442071939499, e-mail: offi [email protected], web: http://gisap.eu
! No part of this magazine, including text, illustrations or any other elements may be used or reproduced in any way without the permission of the publisher or/and the author of the appropriate article
Print journal circulation: 1000
“*Liberal – the issue belongs to the initial stage of the journal foundation, based on scientifi cally reasonable but quite liberal editorial policy of selection of materials. The next stage of the development of the journal (“Professional”) involves strict professional reviewing and admission of purely high-quality original scientifi c studies of authors from around the world”.

1
CONTENTSN. Timchenko, O. Kovalska, N. Timchenko, Danylo Halytsky Lviv National Medical University, UkraineDYNAMIC AND REGIONAL ASPECTS OF MORTALITY [І.21] DUE TO ACUTE MYOCARDIAL INFARCTION IN UKRAINE ....................................................................................................................................................................................3
V. Ruden’1, I. Koval`ska2, D. Moskviak-Lesniak3, O.-E. Vynnytskyi4, Danylo Halytsky Lviv National Medical University, Ukraine1,2,3, City Clinical Hospital of Emergency Medical Care, Ukraine4
BIBLICAL LAWS ABOUT FOOD AS THE BASIS OF HEALTHY NUTRITION OF PEOPLE.................................................11
Yu. Lakhtin1, P. Moskalenko2, L. Karpez3, Sumy State University, Ukraine1,2, Kharkiv Post-graduate Medical Academy, Ukraine3
FEATURES OF THE CYTOLOGICAL PICTURE AT MULTIFORME EXUDATIVE ERYTHEMA IN THE ORAL CAVITY................................................................................................................................................................................16
E. Romanenko1, A. Shtompel2, O. Sinkovskaya3, A. Matveeva4, N. Mirotina5, Dnipropetrovsk Medical Academy, Ukraine1,2,3,4, Dnipropetrovsk city children’s dental polyclinic No. 2, Ukraine5
CONTENT OF PROTEIN AND GLYCOPROTEINS, THEIR COMPONENTS IN THE ORAL FLUID IN CHILDREN WITH CHRONIC GASTRITIS, DUODENITIS....................................................................................................20
A. Plotnikov, Yu. Hrubnyk, Odessa National Medical University, UkraineEFFICIENCY OF LAPAROSCOPY FOR PATIENTS SUFFERING FROM POLYTRAUMA WITH PREVAILING ABDOMINAL AND CHEST INJURIES.........................................................................................................................................23
S. Konovalenko1, M. Hnatjuk2, N. Haliyash3, Kyiv International University, Ukraine1, Ternopil State Medical University named after I.Y. Gorbachevsky, Ukraine2,3
MORPHOLOGICAL CHANGES IN THE TESTICLES UNDER EXPOSURE OF THE ORGANISM TO CADMIUM CHLORIDE......................................................................................................................................................................................27
O. Prysiazhniuk, M. Blazheyevskiy, National University of Pharmacy, UkraineCOMPARATIVE STUDY OF THE ANTIBACTERIAL ACTIVITY OF OINTMENT BASED ON DIPEROXYAZELAIC AND UGRESOL 10% AND ACNE STOP 20% PREPARATIONS.................................................................................................30
O. Koval’ska, M. Blazheyevskiy, National University of Pharmacy, UkraineAPPLICATION OF THE KINETIC ENZYMATIC METHOD FOR BENZALKONIUM CHLORIDE DETERMINATION IN AEROSOL PREPARATION.......................................................................................................................................................33
2
www.iuci.eu
Promotion of international consolidation and cooperation of business structures Promotion of development of commercial businesses of various kindsAssistance in settlement of relations between businessmen with each other and with social partners in business environmentAssistance in development of optimal industrial, financial, commercial and scientific policies in different countries Promotion of favorable conditions for business in various countries Assistance in every kind of development of all types of commercial, scientific and technical ties of businessmen of different countries with foreign colleagues Promotion of international trade turnover wideningInitiation and development of scientific researches, which support the effective development of businesses and satisfy the economic needs of the societyExpert evaluation of activities in the field of settlement of commercial disputes, establishment of quality standards and defining of factual qualitative parameters of goods and servicesLegal and consulting promotion of businessEstablishment and development of activities of the international commercial arbitrationExhibition activitiesHolding of business and economic forums
Union of commercial enterprises, businessmen, scientists, public figures and politicians from different countries. The union combines the social and commercial elements of functioning.
INTERNATIONAL
UNION OF COMMERCE
AND INDUSTRY
3
http://dx.doi.org/10.18007/gisap:msp.v0i13.1651
Formulation of the problem in general
Mortality rate of the population of the country due to diseases is а generally recognized indicator of the nation’s health and the main criterion of evaluation of success of the country’s social and economic development [14], which shows the ability of the society to transform the existing economic resources into the most important product – health of the nation [9].
The mortality of the population due to acute myocardial infarction (AMI) is not an exception. It is one of the main causes of mortality of patients with diseases of the cardiovascular system [1, 12], which makes it relevant to study the different aspects of mortality from this pathology.
Analysis of the researches and publications of recent years
Insufficient attention was paid to the study of the problem of mortality due to AMI among the population of Ukraine. The mentioned problem in different periods was partially studied by such researchers as: V.V. Babushkin (2007) – in the age-related context of senile persons and elderly people; О.О. Kvasha (2009) – assessment of the contribution of risk factors to the mortality rate; К.М. Sokol (2011) – a social and medical research in the regional context; N.Y. Fedchyshyn (2013) – hospital lethality in the aspect of the regional medical institution;
V.М. Kovalenko and V.М. Kornatskyi (2013) – in the context of age and gender groups of Ukraine.
Highlights of previously unsolved aspects of the general problem
It should be noted that the AMI mortality among the population of Ukraine needs the identifi cation and scientifi c substantiation of epidemiological and regional peculiarities. This will allow to optimize the existing problems as to prevention, organization of diagnostics and treatment, as well as rehabilitation processes in relation to AMI by implementing the modern highly effective medical technologies in clinical practice.
Aim of the study
The aim was to examine the peculiarities of dynamics and the regional aspect of mortality among the
population of Ukraine due to AMI for the period of 2002-2013.
Materials and methods of the research
We have analysed the offi cial statistical data of the State Statistics Service of Ukraine [10], Ministry of Health Care of Ukraine for 2000, 2005, 2010 and 2013 concerning the AMI mortality [8] according to the International Statistical Classifi cation of Diseases and Related Health Problems, 10th revision [3] with use of retrospective, medical and statistical, medical and geographical, cartographic methods of research and also methods of structural and logical analysis as well as deductive awareness based on the principles of systems approach and systems analysis. The statistical data was processed and analysed by the automated method using the PC and the software Microsoft Offi ce
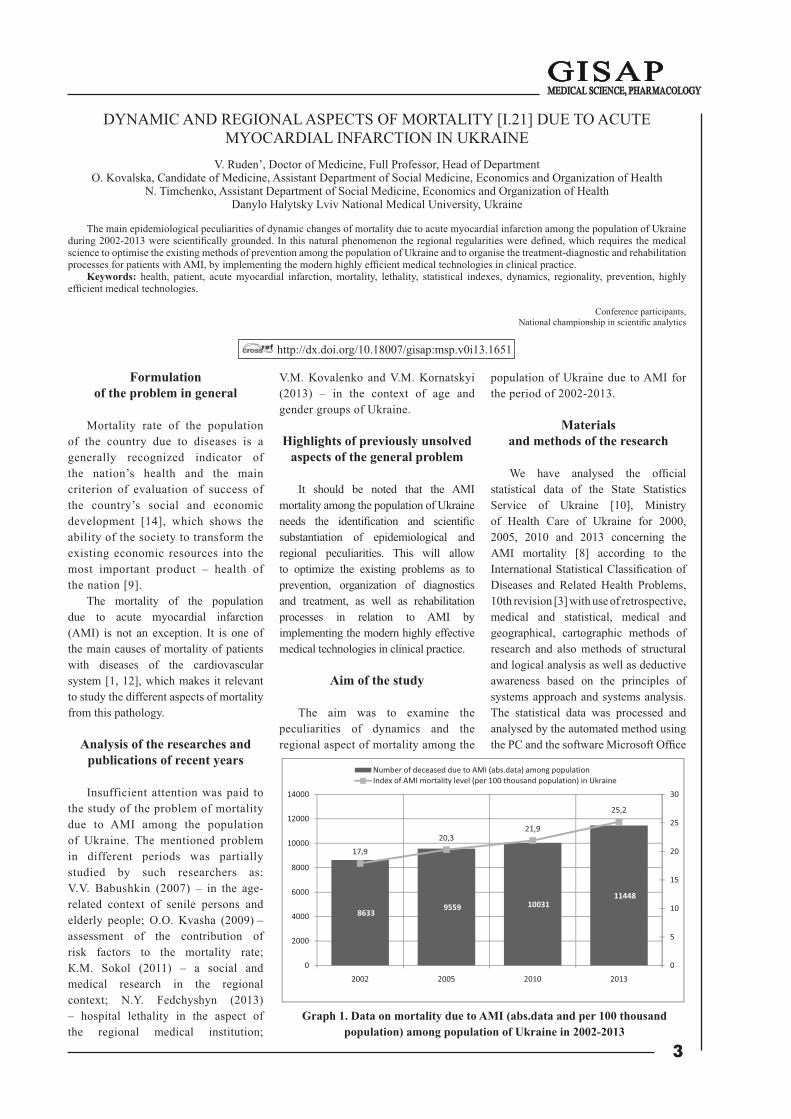
Graph 1. Data on mortality due to AMI (abs.data and per 100 thousand population) among population of Ukraine in 2002-2013
86339559 10031
11448
17,920,3
21,9
25,2
0
5
10
15
20
25
30
0
2000
4000
6000
8000
10000
12000
14000
2002 2005 2010 2013
Number of deceased due to AMI (abs.data) among populationIndex of AMI mortality level (per 100 thousand population) in Ukraine
DYNAMIC AND REGIONAL ASPECTS OF MORTALITY [І.21] DUE TO ACUTE MYOCARDIAL INFARCTION IN UKRAINE
V. Ruden’, Doctor of Medicine, Full Professor, Head of Department O. Kovalska, Candidate of Medicine, Assistant Department of Social Medicine, Economics and Organization of Health
N. Timchenko, Assistant Department of Social Medicine, Economics and Organization of Health Danylo Halytsky Lviv National Medical University, Ukraine
The main epidemiological peculiarities of dynamic changes of mortality due to acute myocardial infarction among the population of Ukraine during 2002-2013 were scientifi cally grounded. In this natural phenomenon the regional regularities were defi ned, which requires the medical science to optimise the existing methods of prevention among the population of Ukraine and to organise the treatment-diagnostic and rehabilitation processes for patients with AMI, by implementing the modern highly effi cient medical technologies in clinical practice.
Keywords: health, patient, acute myocardial infarction, mortality, lethality, statistical indexes, dynamics, regionality, prevention, highly effi cient medical technologies.
Conference participants,National championship in scientifi c analytics

4
Excel 2010 and cartographic editor ГІС Data Graf.
Results of study and discussion
It was established (graph 1) that the number of deaths due to AMI among the population of Ukraine for the period of 2002-2013, according to index of growth rate, had increased by +24.6% (n=2815) and in 2013 there were 11448 cases of deaths, while the index of accumulation of natural phenomenon in 2005 had increased by +1.11, in 2010 – by +1.05 and in 2013 – by +1,.14. It should be
mentioned that the number of residents of Ukraine for the analysed period, according to the absolute growth rate, has decreased by -2904055 persons (-6.4%) and in 2013 – by 45553047 persons [6].
By analysing the value of the integral index of mortality level among the population of Ukraine due to AMI we have determined its tendency to rapid growth in public health of population of the country. In 2005 it has increased by +13.4% as compared to the data of 2002; in 2010 it has increased by +7.9% as compared to the data of 2005; in 2013 it has increased by +15.1% as compared
to the data of 2010. Therefore, in general, the mortality level in 2013, according to the index growth rate, has increased by +40.7% as compared to 2002 – 17.9 cases per 100 thousand persons. As for the gender structure of the index of mortality of Ukrainian population due to AMI, it was determined that during the analysed years the specifi c weight of men prevailed by 15.2±4.7% as compared to females. The index was 55,2±0,46% – 59,2±0,5%, whereas among the women who passed away because of the studied phenomenon the index was within 40,8±0,5% – 44,8±0,46%.
In the context of the above-mentioned it was determined that the level of mortality due to AMI among men in Ukraine in 2013, as compared to 2002, had increased by +33.8% and had reached 30.1 deceased per 100 thousand male persons (graph 2).
As to the coeffi cient of level of mortality among women due to the given pathology, it was established that the researched index in 2013 (21.0 cases of deaths per 100 thousand women) also had shown the tendency to increase by +50.0%, which confi rmed the data of index rate growth as compared to the data of 2002 (14.0 cases of deceased per 100 thousand females).
Moreover, it was determined that the index of correlation between mortality of women and men due to AMI during the studied period had the following numerical expression, namely: in 2002 per 100 deceased women there were 139 deceased men; in 2005 – 100:145; in 2010 – 100:138 and in 2013 – 100:123. This confi rmed the existing tendency to equalization of the number of cases of deaths due to AMI among men and women.
In the course of scientifi c inquiry it was proved that in the structure of mortality due to AMI (graph 3) according to the place of residence the specifi c weight of urban residents was 4.6 times higher (82,0±0,4%) than that among the rural residents, where the given index was 18,0±0,4%.
It was clarifi ed that the coeffi cient of correlation among the dead rural and urban residents due to AMI in 2002 was 1:5.1; in 2005 – 1:4.8; in 2010 – 1:4.6, whereas in 2013 that index had the numeric expression of 1:4.0. This
Graph 2. Data concerning mortality due to AMI (abs. data; per 100 thousand population of corresponding gender) among men and women of Ukraine in
2002-2013
Graph 3. Data on mortality state among the urban / rural residents due to AMIduring 2002-2013 in Ukraine (per 100 thousand residents of the city/village)
5016 5663 5819 6316
3617 3896 42125132
22,5
26,027,6
30,1
14,015,4
17,1
21,0
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
0
1000
2000
3000
4000
5000
6000
7000
2002 2005 2010 2013
Number of men died due to AMI (abs. data)
Number of women died due to AMI (abs. data)
Prevalence of mortality due to AMI among men (per 100 thousand men)
Level of mortality due to AMI among women (per 100 thousand women)
7222
79348194
9167
1411 1625 1837 2281
22,4
2526,2
29,5
8,810,6
12,7
16
0
5
10
15
20
25
30
35
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
2002 2005 2010 2013
Number of deceased due toAMI among the urbanresidents (abs. data)
Number of deceased due toAMI among the ruralpopulation (abs. data)
Level of mortality due toAMI among the urbanresidents (per 100 thousandurban population)
Prevalence of mortality dueto AMI among the ruralpopulation (per 100thousand rural residents)
5
confi rmed the growth of the number of persons who passed away because of that pathology in rural areas by 38.1% (n=870), in spite of the growth of the number of the deceased – +21.2% (n=1945) urban residents.
Accordingly, the accumulation index of persons who died because of the AMI among the rural residents in 2005, as compared to 2002, was +1,15; in 2010 – +1,13, and in 2013 – +1,24; whereas among the persons who died because of that pathology in the cities the analysed index had the following expression: in 2005 – +1,1; in 2010 – +1,1 and in 2013– +1,1. This data again proved the direction to more rapid growth of the number of deaths among the rural residents, as compared to mortality among the urban residents, which confi rmed the steady upward trend of the researched phenomenon.
Besides, it was determined that prevalence index of AMI mortality for that period among the urban residents, according to the index of growth rate, also had the steady upward trend - by +31,7% in 2013 (29.5 deaths per 100 thousand urban residents), as compared to the data of 2002 (22.4/100 thousand); in 2005 it gradually increased by +11,6%; in 2010 – by + 4,8%, in 2013 – by +12,6%.
Despite the lower level of the average value of coeffi cient of mortality level due to AMI among the population of rural areas (M=12,03/100 thousand) - 53,34±0,33% less than the same index among the urban residents (M=25,78/100 thousand), the fi rst index was characterized by the gradual numerical growth: in 2005 – +20,4%; in 2010 – +19,8%, in 2013 – +26% In 2013 its growth for the whole studied period according to the index growth rate was +81,8%, which was 16 dead persons per 100 thousand rural residents.
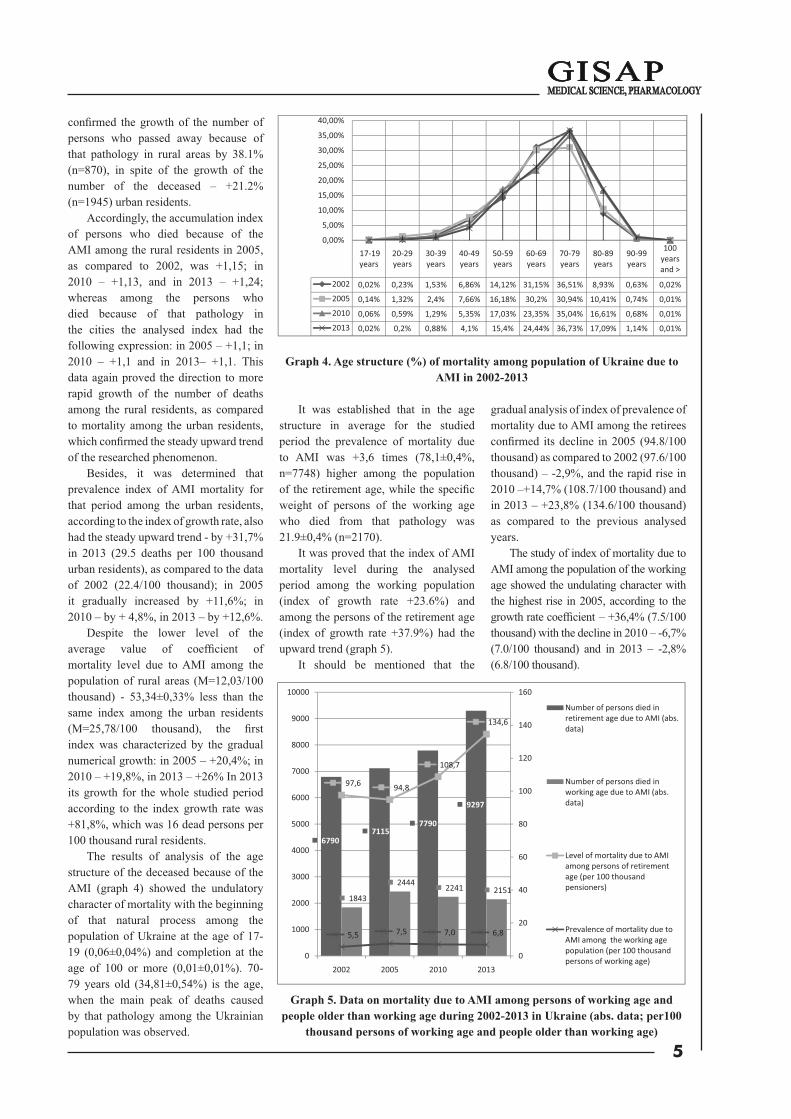
The results of analysis of the age structure of the deceased because of the AMI (graph 4) showed the undulatory character of mortality with the beginning of that natural process among the population of Ukraine at the age of 17-19 (0,06±0,04%) and completion at the age of 100 or more (0,01±0,01%). 70-79 years old (34,81±0,54%) is the age, when the main peak of deaths caused by that pathology among the Ukrainian population was observed.
It was established that in the age structure in average for the studied period the prevalence of mortality due to AMI was +3,6 times (78,1±0,4%, n=7748) higher among the population of the retirement age, while the specifi c weight of persons of the working age who died from that pathology was 21.9±0,4% (n=2170).
It was proved that the index of AMI mortality level during the analysed period among the working population (index of growth rate +23.6%) and among the persons of the retirement age (index of growth rate +37.9%) had the upward trend (graph 5).
It should be mentioned that the
gradual analysis of index of prevalence of mortality due to AMI among the retirees confi rmed its decline in 2005 (94.8/100 thousand) as compared to 2002 (97.6/100 thousand) – -2,9%, and the rapid rise in 2010 –+14,7% (108.7/100 thousand) and in 2013 – +23,8% (134.6/100 thousand) as compared to the previous analysed years.
The study of index of mortality due to AMI among the population of the working age showed the undulating character with the highest rise in 2005, according to the growth rate coeffi cient – +36,4% (7.5/100 thousand) with the decline in 2010 – -6,7% (7.0/100 thousand) and in 2013 – -2,8% (6.8/100 thousand).
Graph 5. Data on mortality due to AMI among persons of working age and people older than working age during 2002-2013 in Ukraine (abs. data; per100
thousand persons of working age and people older than working age)
Graph 4. Age structure (%) of mortality among population of Ukraine due to AMI in 2002-2013
17 19years
20 29years
30 39years
40 49years
50 59years
60 69years
70 79years
80 89years
90 99years
100yearsand >
2002 0,02% 0,23% 1,53% 6,86% 14,12% 31,15% 36,51% 8,93% 0,63% 0,02%2005 0,14% 1,32% 2,4% 7,66% 16,18% 30,2% 30,94% 10,41% 0,74% 0,01%2010 0,06% 0,59% 1,29% 5,35% 17,03% 23,35% 35,04% 16,61% 0,68% 0,01%2013 0,02% 0,2% 0,88% 4,1% 15,4% 24,44% 36,73% 17,09% 1,14% 0,01%
0,00%
5,00%
10,00%
15,00%
20,00%
25,00%
30,00%
35,00%
40,00%
67907115
7790
9297
1843
2444 2241 2151
97,6 94,8
108,7
134,6
5,5 7,5 7,0 6,8
0
20
40
60
80
100
120
140
160
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
2002 2005 2010 2013
Number of persons died inretirement age due to AMI (abs.data)
Number of persons died inworking age due to AMI (abs.data)
Level of mortality due to AMIamong persons of retirementage (per 100 thousandpensioners)
Prevalence of mortality due toAMI among the working agepopulation (per 100 thousandpersons of working age)

6
In the context of analysis of mortality of the population of Ukraine due to AMI the investigated data and mortality of patients in the in-patient departments of medical institutions should be regarded as indicators of effectiveness of timely appeal for medical aid, term and completeness of hospitalization, beginning of treatment, effectiveness of methods, technologies of treatment and rehabilitation measures [13], quality of care for patients and organisation of work of structural specialized subdivisions of medical institutions, and medical and
preventive treatment is institutions in general.
It was confi rmed (graph 6) that in the specialized in-patient departments of medical institutions of Ukraine in 2002 69.5±0,89% (n=5998) patients of the total number of deceased (n=8633) died due to AMI; in 2005 – 63,5±0,82% (accordingly=6068 to n=9559); in 2010 – 65,3±0,81% (accordingly n=6549 to n=10031), whereas in 2013 the specifi c weight of persons who passed away because of the AMI in specialized inpatient departments was 65,5±0,76% (accordingly=7496 to
n=11448), demonstrating the increasing number of deaths in cardiology in-patient departments of medical institutions of Ukraine for the analysed period by +25% or n=1498 cases.
It was established that the index of hospital lethality in average for the analysed years was 13.19±0.19%. The above-mentioned index insignifi cantly declined (-1%) in 2005 (12.87%) as compared to data of 2002 (12.99%), while in 2010 it increased by +1.1% as compared to 2005 – 13.0%. However, in 2013 the index of hospital lethality due to AMI was characterized by the rapid growth +6.8%. Deaths in cardiology in-patient departments due to AMI amounted up to 13.88% of the total number of those discharged and deceased.
During the research we have analysed the places of death of patients with AMI. As a result it was determined that from the total number of persons who died because of the AMI 65.9±0.4% died in the in-patient departments of medical institutions, whereas 3.5±0.4% of persons died in the process of providing pre-hospital medical care and transportation by teams of emergency medical services.
The paradoxical fact is that 30.6±0.4% of patients (n=3390) died out of institutions of the health care system. It was proved that the correlation index among those deceased in the in-patient departments and out of them was the highest in 2002 – 228:100; it was the lowest in 2005 – 174:100. In the following years there was the upgoing trend of hospital mortality: 2010 – 188:100, 2013 – 190:100. It confi rms in most cases the late appeal of patients for medical care at occurrence of cardiac pain [11].
During the research we have examined such component of mortality as pathoanatomical autopsies of the deceased due to AMI, conducted to determine the causes and mechanisms of death of patients [7]. It was the objective criteria for assessing the fi nal results of activity of attending physicians / structural subdivisions and medical and preventive treatment institutions in general [5].
It was proved (graph 7) that the specifi c weight of pathoanatomical investigations during the studied years
Graph 6. Data onmortality in the inpatientdepartments of medical and preventive treatment institutions (abs. data; %) due to AMI among population
of Ukraine in 2002-2013
8633 955910031 11448
5998 6068 6549 7496
12,99%12,87%
13,00%
13,88%
12,20%
12,40%
12,60%
12,80%
13,00%
13,20%
13,40%
13,60%
13,80%
14,00%
0
2000
4000
6000
8000
10000
12000
14000
2002 2005 2010 2013
Number of persons (abs. data) died due to AMI among population of Ukraine
Number of deceased (abs. data) due to AMI in the inpatient departments of medical andpreventive treatment institutionsIndex of hospital lethality (%) due to AMI
Graph 7. Data on the results of pathoanatomical autopsies (abs. data; %) in Ukraine among persons died due to AMI in 2002-2013
8633 9559 10031 11448
73477967
856010126
85,4%
83,3%
85,3%
88,4%
80,0%
81,0%
82,0%
83,0%
84,0%
85,0%
86,0%
87,0%
88,0%
89,0%
0
2000
4000
6000
8000
10000
12000
14000
2002 2005 2010 2013
Number of persons died due to AMI (abs. data)Number of autopsies of deceased due to AMI (abs. data)% pathoanatomical autopsies of deceased due to AMI

7
was characterized by the decline in 2005 – -2.5% (83.8%) as compared to 2002 (85.4%), by growth (+2.4%) in 2010 (85.3%) as compared to 2005, and by rapid growth in 2013: +3.6% (88.4%) as compared to pathoanatomical autopsies of dead bodies (due to AMI) in 2010.
Thus, despite the high indexes of diagnoses of AMI confi rmed by the
pathoanatomical studies, still there were a signifi cant number of deceased whose diagnoses of AMI were not confi rmed posthumously [4]: in 1286 dead persons in 2002 or in 14.6% of all cases of deaths for that reason; in 1592 deceased (16.7%) in 2005; in 1471 dead persons (14.7%) in 2010 and in 1322 deceased in 2013 (11.6%).
The analysed state of mortality among the population of Ukraine due to AMI in the context of the existing administrative territorial units [2] clearly showed (table 1) that the population of the Eastern region was in the fi rst rating place in the regional peculiarities of the natural process of the given pathology with the index at 31.1 cases per
Tab. 1.The regional peculiarities of AMI morbidity among the population of Ukraine in 2013
Name of regions ofUkraine
Names ofregions and cities under
central authority
Level of morbidity due to AMI (I.21)
All population (cases per 100 thousand population)
including, amongthe urban population (per 100
thousandurban residents)
the rural population(per 100 thousand
rural residents)
Wes
tern
regi
on
Lviv region 26,6 32,8 17,1Ivano-Frankivsk reg. 12,5 13,1 12,1
Ternopil region 21,5 28,7 15,9Volyn region 13,2 17,0 9,2Rivne region 12,1 14,1 10,4
Chernivtsi region 18,3 29,2 10,3Zakarpattia region 20,9 28,0 16,8
Level ofthe Western region
Scope = 12,1 - 26,6 13,1-32,8 9,2-17,117,9 23,3 13,1
Rating place V V V
East
ern
regi
on
Kharkiv region 36,0 39,9 20,6Donetsk region 31,8 32,8 22,0Luhansk region 25,4 26,2 20,4
Level ofthe Eastern region
Scope = 25,4–36,0 26,2-39,9 20,4-22,031,1 33,0 21,0
Rating place I І І
Sout
hern
regi
on
Zaporizhia region 37,0 41,8 21,3Kherson region 18,2 21,2 13,6Odessa region 24,2 28,9 14,9
Mykolaiv region 22,3 27,6 11,1AR of Crimea 25,2 29,0 19,0
Sevastopol 32,2 33,3 16,8Level of
the Southern regionScope = 18,2–37,0 21,2-41,8 11,1-21,3
26,5 30,3 16,1Rating place II ІІ ІІІ
Nor
ther
n re
gion
Zhytomyr region 16,2 19,0 12,4Kyiv region 28,6 30,2 26,0
Chernihiv region 21,7 25,1 16,0Sumy region 20,2 23,2 14,1
Kyiv 35,7 35,7 -Level of
the Northern regionScope = 16,2–35,7 19,0-35,7 12,4-26,0
24,5 26,6 17,1Rating place IІІ ІІІ ІІ
Cen
tral r
egio
n
Vinnytsia region 16,4 20,1 12,8Dnipropetrovsk reg. 28,3 30,0 20,1Kirovohrad region 16,9 19,0 13,4
Poltava region 28,1 32,4 21,4Cherkasy region 16,9 20,0 13,0
Khmelnytsky region 20,1 22,9 16,7Level of
the Central regionScope = 16,4–28,3 19,0-32,4 12,8-21,4
21,1 24,1 16,2Rating place IV IV IV
8
100 thousand persons (including: the urban population – 33.0/100 thousand and the rural residents – 21.0/100 thousand). The situation with the AMI mortality in the Eastern region of the country was 1.74 times higher than that of the Western region, where the index of mortality was 17.9 cases per 100 thousand persons. Western region took the last fi fth place in the rating across the entire population: urban (23.3/100 thousand) and rural (13.1/100 thousand) residents.
The Southern region of the country was in the second place in the ranking. Here the index of prevalence of AMI mortality was 26.5 cases per 100 thousand persons. However, among the residents of cities the analysed coeffi cient was 30.3/100 thousand, while among the village residents –16.1/100 thousand.
The Northern region (24.5/100 thousand in the region; 26.6/100 thousand – the urban residents and 17.1/100 thousand – the rural residents) was in the third place in the rating by value of index of mortality level due to AMI among the population. The Central Region was in the fourth place in the rating (21.1/100 thousand for the entire population; 24/100 thousand – in cities and 16.2/100 thousand – in rural areas).
It was discovered that the coeffi cient of correlation among the residents of villages and cities, who died due to AMI in the aspect of regions of the country,
was the highest in the Southern and the Western regions: 188 rural residents and 178 urban residents – per 100 deaths from that pathology. Whereas in other regions (Eastern, Northern and Central) those indexes were much lower: 100:157, 100:155, 100:149 respectively.
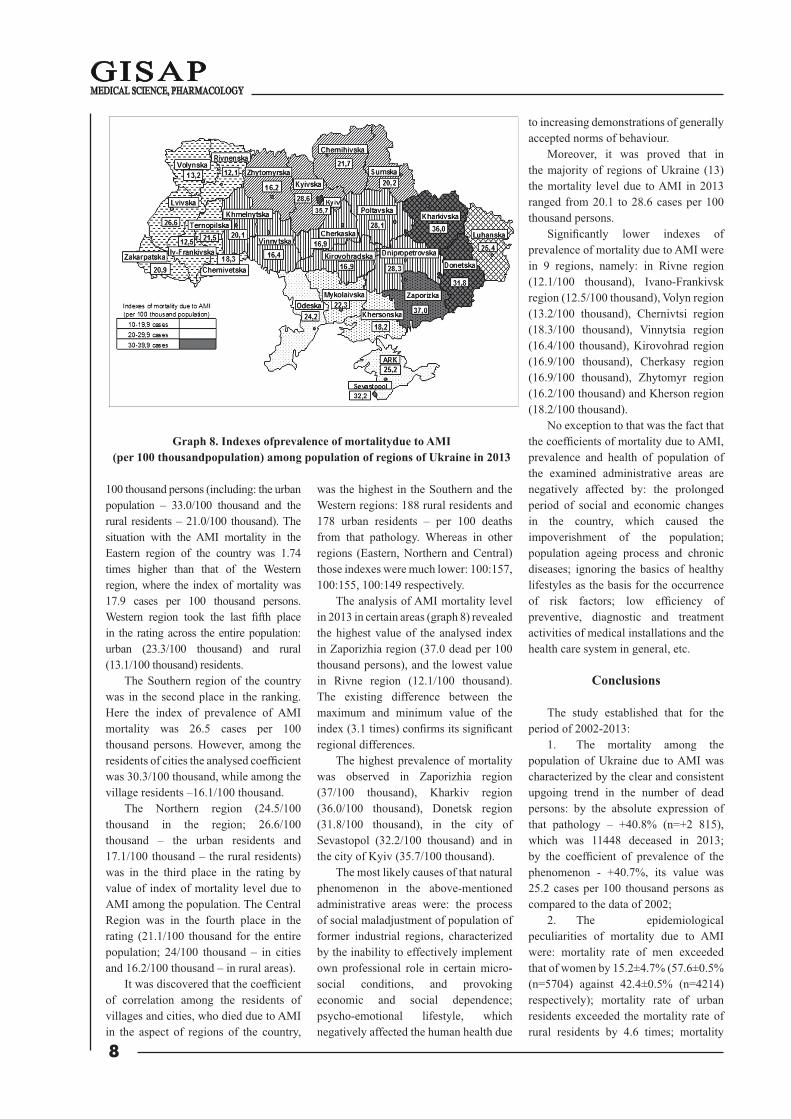
The analysis of AMI mortality level in 2013 in certain areas (graph 8) revealed the highest value of the analysed index in Zaporizhia region (37.0 dead per 100 thousand persons), and the lowest value in Rivne region (12.1/100 thousand). The existing difference between the maximum and minimum value of the index (3.1 times) confi rms its signifi cant regional differences.
The highest prevalence of mortality was observed in Zaporizhia region (37/100 thousand), Kharkiv region (36.0/100 thousand), Donetsk region (31.8/100 thousand), in the city of Sevastopol (32.2/100 thousand) and in the city of Kyiv (35.7/100 thousand).
The most likely causes of that natural phenomenon in the above-mentioned administrative areas were: the process of social maladjustment of population of former industrial regions, characterized by the inability to effectively implement own professional role in certain micro-social conditions, and provoking economic and social dependence; psycho-emotional lifestyle, which negatively affected the human health due
to increasing demonstrations of generally accepted norms of behaviour.
Moreover, it was proved that in the majority of regions of Ukraine (13) the mortality level due to AMI in 2013 ranged from 20.1 to 28.6 cases per 100 thousand persons.
Signifi cantly lower indexes of prevalence of mortality due to AMI were in 9 regions, namely: in Rivne region (12.1/100 thousand), Ivano-Frankivsk region (12.5/100 thousand), Volyn region (13.2/100 thousand), Chernivtsi region (18.3/100 thousand), Vinnytsia region (16.4/100 thousand), Kirovohrad region (16.9/100 thousand), Cherkasy region (16.9/100 thousand), Zhytomyr region (16.2/100 thousand) and Kherson region (18.2/100 thousand).
No exception to that was the fact that the coeffi cients of mortality due to AMI, prevalence and health of population of the examined administrative areas are negatively affected by: the prolonged period of social and economic changes in the country, which caused the impoverishment of the population; population ageing process and chronic diseases; ignoring the basics of healthy lifestyles as the basis for the occurrence of risk factors; low effi ciency of preventive, diagnostic and treatment activities of medical installations and the health care system in general, etc.
Conclusions
The study established that for the period of 2002-2013:
1. The mortality among the population of Ukraine due to AMI was characterized by the clear and consistent upgoing trend in the number of dead persons: by the absolute expression of that pathology – +40.8% (n=+2 815), which was 11448 deceased in 2013; by the coeffi cient of prevalence of the phenomenon - +40.7%, its value was 25.2 cases per 100 thousand persons as compared to the data of 2002;
2. The epidemiological peculiarities of mortality due to AMI were: mortality rate of men exceeded that of women by 15.2±4.7% (57.6±0.5% (n=5704) against 42.4±0.5% (n=4214) respectively); mortality rate of urban residents exceeded the mortality rate of rural residents by 4.6 times; mortality
Graph 8. Indexes ofprevalence of mortalitydue to AMI(per 100 thousandpopulation) among population of regions of Ukraine in 2013

9
rate of elderly persons exceeded the mortality rate of persons of the working age by +3.6 times (78.1±0.4% (n=7748) against 21.9±0.4% (n=2170) respectively); the majority of the deceased Ukrainian citizens were in the age group of 70-79 (34.81±0.54%), but this natural process began in the age group of 17-19 (0.06±0.04%) and ended in the age group of 100+ (0.01±0.01%); the number of deaths in cardiology in-patient departments increased by +25% (n=+1498) cases against the decrease of the average length of stay of patients by -24%, while 34.5% (n=3952) died out of health care institutions and in 11.6% (n=1322) cases the diagnosis of AMI was not confi rmed posthumously; in the Eastern region (31.1/100 thousand) the mortality was 2 times higher than in the Western region (17.9/100 thousand), and as for the the administrative areas: Zaporizhia region (37/100 thousand), Kharkiv region (36.0/100 thousand), Donetsk region (31.8/100 thousand), the city of Sevastopol (32.2/100 thousand) and the city of Kyiv (35.7/100 thousand).
3. Areas of work to reduce the level of mortality due to AMI among residents of Ukraine: activation of prevention work at the national level and that performed by individual doctors of primary level of medical provision through informing the population regarding the bases of formation, preservation and promotion of healthy lifestyle; identifi cation of patients with high risk of cardiovascular pathology; effective and high-quality implementation in clinical practice of the modern medical technologies - antithrombotic therapy, timely coronary artery bypass surgery, primary percutaneous coronary intervention / fi brinolysis and other types of invasive researches and methods of revascularization, which would positively affect the health of the nation.
References:
1. Desjat' vedushhih prichin smerti v mire. Informacionnyj bjulleten' VOZ No. 310 Maj 2014 [Ten leading causes of death in the world. WHO news bulletin No. 310, May 2014. Russian]., Access mode: http://www.who.int/ mediacentre/factsheets/fs310/ru/.
2. Konstitucіja Ukraїni. Stattja
133. Zakon VR Ukraїni vіd 28.06.1996 r. za No. 254k/96-VR [Constitution of Ukraine. Article 133. The Law of VR of Ukraine of 28/06/1996, No. 254k/96-VR.Ukrainian]., Access mode: http://zakon2.rada.gov.ua.
3. Mіzhnarodnij klasifіkator hvorob MKH-10 [International Classifi cation of Diseases ICD-10. Ukrainian]., Access mode: http://www.medukr.com/problems/details/760/.
4. Nakaz MVS Ukraїni, MOZ Ukraїni, General'na prokuratura Ukraїni vіd 28.11.2012 r. za № 1095/955/119 «Pro zatverdzhennja Porjadku vzaєmodії mіzh organami vnutrіshnіh sprav, zakladami ohoroni zdorov’ja ta prokuraturi Ukraїni pri vstanovlennі faktu smertі ljudini» [Order of the MIA of Ukraine, MoH of Ukraine, General Prosecutor of Ukraine of 28/11/2012, No. 1095/955/119 "On approval of the interaction between bodies of internal affairs, health care institutions and the Prosecutor’s Offi ce of Ukraine in establishing the fact of death of a person". Ukrainian]., Access mode: http://zakon3.rada.gov.ua/laws/show/z2106-12.
5. Nakaz MOZ Ukraїni «Pro rozvitok ta udoskonalennja patologoanatomіchnoї sluzhbi v Ukraїnі» vіd 12.05.1992 roku za No. 81 (іz zmіnami) [Order of the MoH of Ukraine "On the development and improvement of pathoanatomical service in Ukraine" of 12/05/1992, No. 81 (with changes). Ukrainian]., Access mode: http://www.uazakon.com/.
6. Naselennja Ukraїni za 2013 rіk. Demografіchnij shhorіchnik [The population of Ukraine for 2013. Demographic Yearbook]. – Kyiv., Derzhavna sluzhba statystyky Ukrayiny [State Statistics Service of Ukraine]., 2014., Р. 19., Access mode: ht tp: / /database.ukrcensus.gov.ua/PXWEB2007/.
7. Osnovi zakonodavstva Ukraїni pro ohoronu zdorov'ja. Stattja 72. Patologoanatomіchnі roztini. Verhovna Rada Ukraїni; Zakon vіd 19.11.1992, No. 2801-XII (іz zmіnami) [Fundamentals of Legislation of Ukraine on Health Care. Article 72. Pathoanatomical autopsies. Verkhovna Rada of Ukraine; Law dated 19/11/1992, No. 2801-XII (with changes)]., Access mode: http://zakon0.rada.gov.ua/.
8. Pokazniki zdorov'ja naselennja ta vikoristannja resursіv ohoroni zdorov'ja v Ukraїnі za 2000-2013 roki. Centr medichnoї statistiki MOZ Ukraїni [Indexes of health of population and use of health care resources in Ukraine for 2000-2013. Medical Statistics Centre of the Ministry of Health of Ukraine]. – Кiev., 2001-2014.
9. Polishchuk M.Ye., Krasov-s'kyі K.S., Andrіeіeva T.I. Zmenshennja smertnostі sered naselennja Ukraїni u 2008-2010 rokah. Zhurnal NAMN Ukraїni [Reduction of mortality among the population of Ukraine in 2008-2010. Journal of National Academy of Medical Sciences of Ukraine]. - 2013; 19: 1: 90-94.
10. Rozpodіl pomerlih za stattju, vіkovimi grupami ta prichinami smertі (tablicja S-8). Departament statistiki naselennja ta regіonal'noї statistiki. Derzhkomstat Ukraїni [Number of deaths by sex, age groups and causes of death (table С-8). Department of population statistics and regional statistics. State Statistics Service of Ukraine]., Access mode: http://www.ukrstat.gov.ua/.
11. Ruden' V.V., Timchenko N.F. Pro rol' usvіdomlenih povedіnkovih dіj ljudini pri viniknennі kardіologіchnogo bolju jak bazisu svoеchasnoї ta jakіsnoї medichnoї dopomogi pri gostromu іnfarktі mіokarda [On the role of conscious behavioural human actions at occurrence of cardiac pain as the basis for timely and qualitative medical care at acute myocardial infarction. Ukrainian Journal of Therapeutics]. - 2015; 2: 57–61.
12. Smertnіst' naselennja Ukraїni turbuє vsіh… Therapia: ukraїns'kij medichnij vіsnik [Mortality of population of Ukraine worries everybody… Therapy: Ukrainian Medical Journal]. - 2013; 9 (83))., Access mode: http://therap ia .ua / therap ia /2013- /9-83/smertnist-naselennya-ukrayiny-turbuye-vsikh
13. Ustinov O.V. Problemi nadannja medichnoї dopomogi hvorim na gostrij іnfarkt mіokarda v Ukraїnі. Ukraїns'kij medichnij chasopis [Issues of medical care provision for patients with acute myocardial infarction in Ukraine. Ukrainian Medical Journal]. - 2013; 2 (94): 8-11., Access mode: http://www.umj.com.ua/wp/wp-content/

10
uploads/2013/03/Cardiolology.pdf.upload.
14. Sen А. Mortality as an Indicator of Economic Success and Failure. Economic Journal. Royal Economic Society. - 1998; 108 (446): 1-25., Access mode: h t tp : / /on l ine l ib ra ry.wi ley.com/ . ,
https://doi.org/10.1111/1468-0297.00270
Information about authors:
1. Vasyl' Ruden' – Doctor of Medicine, Full Professor, Lviv National Medical University named after Danylo Galitsky; address: Ukraine, Lviv city; e-mail: [email protected]
2. Oksana Kovalska – Candidate of Medicine, Assistant Department of Social Medicine, Economics and
Organization of Health Lviv National Medical University named after Danylo Galitsky; address: Ukraine, Lviv city; e-mail: [email protected]
3. Natalya Timchenko – Assistant Department of Social Medicine, Economics and Organization of Health Danylo Halytsky Lviv National Medical University, address: Ukraine, Lviv city; e-mail: [email protected]
ACCREDITATIONAuthoritative accreditationProcedural accreditationStatus accreditationMembership accreditationExpert accreditation
PATENTING IOSCEAAD-775
Standart patenting
Operative patenting
CERTIFICATION «ICSQ-775»
Standart certification
Operative certification
http://academy.iuci.eu

11
Topicality
The importance of rational nutrition of people for the civil society of independent Ukraine is undeniable, because one of the main tasks in economic transformations of the current health care system provides for active formation of bases of healthy lifestyle among the country’s population [4].
An axiom of this is the scientifi c fact that irrational nutrition of a person is a source of various disease states, low physical and mental working capacity and reduction of the length of life [10]. In addition, irrational nutrition serves as the cause of more than 80 different diseases, while every third our compatriot (adult and child) suffers from various illnesses, caused by the nutrition disorders. Among the considerable part of the dead there are victims of related malignant tumors and cardiovascular diseases [8].
“Men die due to recklessness in food, drinks and intemperance, not having lived even half of life that the could live. They consume the most diffi cult to digest food, drink the poisonous drinks, and then wonder why they do not live up a hundred years age. Paul Bragg (1991) wrote, “I'm sure that 99% of patients suffer that much because of the wrong, not natural nutrition” [13].
The signifi cance of the marked words is that according to the WHO, the rational nutrition, on which the psychophysical health of the adult person depends, plays a major role among 12 mandatory conditions of healthy lifestyle [9], and in the prevention of diseases, strengthening
the health of a person. All this ultimately forms the basis of a healthy society.
Among the available information fl ows today, we attempted to entertain the importance of the biblical food in the context of the formation of bases of healthy way of human life in Ukraine of the newest format.
A motive for this is that healthy lifestyle serves as the prerequisite for the development of active participation in the labour, social, political, economic, family and household-related, recreational and other various forms of human activity [7], attainment of active longevity and full implementation of the social functions [5] with constant growth and changes in the nature of loads on human organism due to changes in political and socio-economic complexity of life of people in Ukraine and increasing risks of technological, environmental, psychological, political and military nature, which provoke negative changes in the state of health [20]. All this together makes this scientifi c research topical in its own content.
Aim
Role and place (as described in the Holy Scripture) of food as the vitally necessary thing in balanced nutrition and in the process of formation of bases of healthy way of human life.
Materials and methods
In carrying out the scientifi c work we used such methods as: bibliographical, qualimetric, historical and literary
synthesis, retrospective analysis, scientifi c abstraction and also methods of deductive awareness, structural and logical analysis with the system principles.
Results
Retrospective analysis of available information convincingly demonstrated that the connection between the person’s state of health and the quality of food was well understood by many ancient peoples. The related data was found in the works of Hippocrates, Democritus, Celsius, Galen and others [11], while the great Avicenna formulated in this context the opinion relevant for today: “If the father of the disease is unknown, the mother is always the food” [1].
However, perhaps the most topical issue in rational nutrition with regard to formation of bases of healthy lifestyle among the population of Ukraine is the pages of the Holy Scripture. From the Book of Deuteronomy 8 [19] we can fi nd that the Lord God gives seven vitally necessary products for a new generation of Israelis, destined to survive in the forty-year wandering, in order to possess the Promised Land.
In the Word of God within this context is said, “…For the Lord thy God bringeth thee into a good land, a land of brooks of water, of fountains and depths that spring out of valleys and hills; a land of wheat, and barley, and vines, and fi g trees, and pomegranates; a land of oil olive, and honey; a land wherein thou shalt eat bread without scarceness, thou shalt not lack any thing in it; a land whose stones are
U.D.C. 61:2:613.2-058
BIBLICAL LAWS ABOUT FOOD AS THE BASIS OF HEALTHY NUTRITION OF PEOPLEV. Ruden’1, Doctor of Medicine, Full Professor, Head of Department
I. Koval`ska2, Senior LecturerD. Moskviak-Lesniak3, Assistant
O.-E. Vynnytskyi4, Physician of Reanimation Department Danylo Halytsky Lviv National Medical University, Ukraine1,2,3
City Clinical Hospital of Emergency Medical Care, Ukraine4
The importance of rational nutrition in human life for the civil society of independent Ukraine is considered in the paper. Irrational nutrition of a person is a source of various disease states, low physical and mental working capacity and reduction of the length of life. The results of historical and literary synthesis of pages of the Scripture clearly confi rm that seven vitally important biblical products, namely: wheat, barley, grapes, fi gs, pomegranates, olive oil, honey and poultry, beef, lamb and eggs should be used in the daily nutrition.
Keywords: nutrition, biblical law, health, food, disease.
Conference participants,National championship in scientifi c analytics,
Open European and Asian research analytics championship
http://dx.doi.org/10.18007/gisap:msp.v0i13.1652

12
iron, and out of whose hills thou mayest dig brass. When thou hast eaten and art full, then thou shalt bless the Lord thy God for the good land which he hath given thee” (Deuteronomy 8:7-9).
Nowadays, in everyday life the consumption of seven vitally necessary products is like a blessing from fi elds of God's commandments, in this way we support both physical and spiritual health. It is important to note that modern medical science highly appreciates healing and nutritional qualities of seven important products mentioned in this passage of the Scripture.
As for the human consumption of meat it is important to refer to the Book of Genesis in the Holy Scripture, where it is said that once Abraham was sitting at the entrance of the tent during the heat of the day and saw three men in front of him. As they got to know each other, he invited them to the tent, ordered his servants to bring water to wash their feet, and ordered his wife Sarah to bake fresh breads for them. Abraham “…ran to the herd and chose a fi ne, tender calf, and gave it to a servant, who quickly prepared it. Abraham took cheese and milk, as well as the meat, and set these in front of them” (Genesis 18:6-7).
These guests told Abraham that Sarah would have a son within the next year. Indeed, next year, Sarah and Abraham had a son Isaac, despite the fact that both were not in the childbearing age.
Since then, over many generations Jewish families always kept ready fatted calf in case the “angel” comes to the house the guise of a traveler – to feed him [16].
In rich families of that time the beef and mutton were festive meals, coooked for special occasions - for banquets, weddings, soirees, sacrifi ces, but the duty was to kill lambs every year on Easter. We should also note the parable of the prodigal son, where the father was so delighted to have his son return home that commanded his servants, “…and bring the fattened calf and kill it, and let us eat and celebrate” (Luke 15:23).
Regarding such food as pork, we should refer to the Gospel of Mark that tells “... about a man with an unclean spirit who had his dwelling in the tombs”, who lived in the land under Roman rule. Upon seeing this man, Jesus said to him,
“Come out, unclean soul, of this man!” And also asked him: “What is your name?” He responded, “Legion is my name, because we are many”. There on the nearby hillside a large herd of pigs was feeding. So the demons begged Jesus, “Send us to the pigs, so that we may enter them”. He gave them permission, and the unclean spirits came out and went into the pigs, and the herd of about two thousand rushed down the steep bank into the sea and drowned in the water” (Mark 5:12).
If pigs were “clean” animals, Jesus would never allow demons to enter them. He sent the demons in pigs and only made “unclean” meat more “unclean”.
In addition, in that country controlled by the Romans, where sacrifi ces to the Roman gods were often made, cattle were usually sacrifi ced to “the gods above”, аnd pigs to “the gods at the bottom”. Jesus knew that pigs would be sacrifi ced to Satan and just sent the demons to hell in the shortest way.
In the animal world pig has always embodied gluttony. God probably appointed pig to clean the Earth from scum, while much of what pigs eat is not useful to human! In addition, they are not only gluttonous, but also very dirty animals [18].
The evidence in favor of the above-mentioned could be the work “Pork and human health” by the German physician Reckeweg Hans-Heinrichа [15]. He points that toxic substances in pork are “sutoxins” and justifi es them as risk factors in the occurrence of certain human diseases. A reason for this is that the chemical composition of pork meat is signifi cantly different from other domestic animals, because in pork meat there are large quantities of cholesterol, fatty acids, histamine and growth hormone, which are harmful to human health.
One of the diseases with which a person can be infected, after eating the undercooked pork (heat treatment lower than 100 0 С), is trichinosis, the agent – a parasite discovered in 1822 by the scientist Tiedemann and known in medicine as “tricхinella spiralis” [17]. In Muslim countries, this disease is absent among the population, which is another proof of the greatest wisdom of the Almighty.
Turning the pages of the Holy Scripture in the Book of Leviticus we can
fi nd warnings about human consumption of animal fat, “All fat is the Lord's. This is to be a lasting statute for all your generations, wherever you live. You are not to eat any fat or blood”. (Leviticus 3:16-17). And then, “Speak to the people of Israel, saying, You shall eat no fat, of ox or sheep or goat. The fat of an animal that dies of itself and the fat of one that is torn by beasts may be put to any other use, but on no account shall you eat it. For every person who eats the fat of an animal of which a food offering may be made to the Lord shall be cut off from his people” (Leviticus 7:23-25).
So the Lord God forbade eating the animal fat in any of its form. In the mentioned passage of the Scripture nothing is said about vegetable or fi sh fat, but only that fat of animals known as “clean” can be sacrifi ced to God.
Actually, it is meant that fat, sometimes called peritoneal which lines the insides of animals, was burnt as sacrifi ces in the temple. In addition, it should be noted that in the God's guideline nothing is said about fat which is the part of meat of “clean animals”, such as beef.
Nowadays, it is scientifi cally proved that any animal fats are organic substances which contain compounds of esters of triatomic alcohol / glycerol and fatty acids, namely: saturated (palmitic, stearic), unsaturated acids (oleic, linoleic, arachidonic) and F vitamin [6], known in chemistry as “triglycerides”. Excessive consumption of it leads to the risk of occurrence of arterial pressure and a number of cardiovascular diseases [23].
As for the consumption of poultry meat and eggs, the Law of Moses gives the following recommendations about birds: “These are the birds you are to regard as unclean and not eat because they are unclean: the eagle, the vulture, the black vulture, the red kite, any kind of black kite, any kind of raven, the horned owl, the screech owl, the gull, any kind of hawk, the little owl, the cormorant, the great owl, the white owl, the desert owl, the osprey, the stork, any kind of heron, the hoopoe and the bat. But all other fl ying insects that have four legs you are to regard as clean” (Leviticus 11:13-19). 24 species of birds, mostly carnivorous are forbidden to consume according to Book of Leviticus.
In Deuteronomy 14:12-18 the

13
prohibited species of birds are listed. Such expressions are used as “all species” and “with their species”, though the exact description of these species is not given, while at the same time in Deuteronomy 14:20 it is stated that “Every clean bird you can eat”. In this, the pure bird means game (hunting) and poultry: chickens, geese, turkeys, ducks, pigeons, partridges, quails, that Jews were allowed to eat in the time of Jesus.
In the Bible occasions when Jesus hadn’t eaten poultry were not mentioned, but He said about bird and fl edglings (in English translation “hen and chickens”) in one of the Gospel verses, “O Jerusalem, Jerusalem, the city that kills the prophets and stones those who are sent to it! How often would I have gathered your children together as a hen gathers her brood under her wings, and you were not willing!” (Matthew 23:37).
In biblical times, Laws on consumption of meat were the same for poultry: kosher poultry was prepared by soaking, salting and roasting, and kosher meat was always without blood, corresponding to the Law of Leviticus which prohibited to eat blood of “clean” animals: “Moreover, you shall eat no blood whatever, whether of fowl or animal, in any of your dwelling places.Whoever eats any blood, that person shall be cut off from his people” (Leviticus 7:26-27).
Regarding the eggs – as a food product, it should be noted that in biblical times eggs were eaten before meals, but in time of Jesus they were the usual foodstuff.
In the Book of Job we can fi nd very interesting question: “Does anyone want the tasteless white of an egg?” and then, “My appetite disappears when I look at it; I gag at the thought of eating it!” (Job 6: 6-7).
However, the attitude of Jesus to the eggs was better – He considered them well-gifts, “So I say to you: Ask and it shall be given you; seek and you will fi nd; knock, and it shall be opened to you... Which of you, fathers, when your son asks for bread, will give him a stone? Or... when he asks an egg, will offer him a scorpion? So when you, being evil, know how to give good gifts to your children, as a heavenly Father give the Holy Spirit to those who ask him!” (Luke 11:9, 11-13). It should be mentioned that in times of
Jesus eggs were cooked in different ways, including frying and boiling. In addition fried or stewed fi sh under the layer of eggs was also popular.
Nowadays, many people avoid eggs because of cholesterol and the risk of contracting salmonella (acute infectious disease from the group of zoonoses, caused by bacteria of the genus Salmonella, accompanied by the symptoms of gastroenteritis and intoxication. There are nearly 2200 Salmonella serovars, which differ by О- і Н- antigens).
Nowadays, it is scientifi cally proved that there is a lot of choline in the egg yolk, used in the human body to produce acetylcholine - one of the main neurotransmitters, providing work of brain and memory. Apart from choline eggs also contain folic acid, В group vitamins, antioxidants and polyunsaturated fatty acids. Most people do not know that egg yolks contain a lot of lecithin - substance which destroys the cholesterol [21].
The research conducted in 1999 at the Harvard University, showed that consumption of one egg a day did not increase the probability of cardiovascular diseases or a heart attack [22]. Instead, one eaten egg per day helped to prevent heart diseases.
The best way to get rid of harmful bacteria, with which eggs can be infected, is to properly cook eggs - to cook or fry the egg until the yolk becomes fi rm [2].
Another harmful factor to Human health in the context of formation of bases of a healthy way of life is the uncontrolled consumption of food and excessive weight - “overeating / hyperphagia” [12].
In addition, referring to the Bible, it should be noted that overeating is also the consumption of junk food. In the Book of Proverbs we read, “When you sit down to eat with a ruler, observe carefully what is before you, and put a knife to your throat if you are given to appetite. Do not desire his delicacies, for they are deceptive food” (Proverbs 23:1-3). It should be noted that food of rich people in some parts of the Scripture is named “delicacies”. This probably refers to fatty foods, especially fatty meat.
The consumption of meat in the Bible is often associated with overeating. Thus, “And Solomon's provision for one day was thirty measures of fi ne fl our, and sixty measures of meal. Ten fat oxen,
and twenty oxen out of the pastures, and a hundred sheep, besides harts, and deer, and fallow deer, and fatted fowl” (І Book of Kings 5:2). In the Bible it is explained that such amount of meat is excessive, because its production exhaustes the land.
Furthermore, the Scripture is against gluttony, usual overeating: “Listen, my son, and be wise, and set your heart on the right path. Do not join those who drink too much wine or gorge themselves on meat, for drunkards and gluttons become poor, and drowsiness clothes them in rags” (Proverbs 23:19-21).
The Law of Moses strictly punished gluttons. Drunkenness and gluttony were considered signs of “disobedience and rebellion” (Deuteronomy 21:20), while “... revelers and drunkards“ were sentenced to “... death by stoning” (Deuteronomy 21:21).
People who ate and drank a lot considered to be selfi sh, spoiled and undisciplined by the Jews of that time, while the pious people had to show patience, restraint and generosity towards those around [3].
In Chapter 11 of the Numbers the following interesting story is described. Wandering through the desert, the people of Israel began to murmur, not satisfi ed that they eat only manna and “people began to grumble bitterly”. “The rabble with them began to crave for other food, and again the Israelites started wailing and said: “If only we had meat to eat!?” (Numbers11:4).
The Lord God replied as follows: “Now a wind went out from the Lord and drove quail in from the sea. It scattered them up to two cubits deep all around the camp, as far as a day’s walk in any direction. All that day and night and all the next day the people went out and gathered quail. No one gathered less than ten homers. Then they spread them out all around the camp. But while the meat was still between their teeth and before it could be consumed, the anger of the Lord burned against the people, and he struck them with a severe plague.Therefore the place was named Kibroth Hattaavah, because there they buried the people who had craved for other food” (Numbers 11: 31-34). It is important to note that those, who gathered least quails gathered ten homers, that was ten and a half bushels (more than 35 cubic meters) [14].

14
The meaning of this story: people did not die because they ate birds, but due to their gluttony and disobedience.
Conclusions
1) The results of historical and literary synthesis of pages of the Scripture clearly confi rms that seven vitally important biblical products, namely: wheat, barley, grapes, fi gs, pomegranates, olive oil, honey and poultry, beef, lamb and eggs should be used in the daily nutrition with the God's blessing and benefi t for health, while pork and animal fat, overeating and drinking were prohibited by the Lord God.
2) All this, despite the millennia of years lived by people, convincingly demonstrates the relevance and appropriateness in applying the commandments of God for human health concerning the consumption of vitally important biblical products, that can make the nutrition more rational and benefi cial to human health, and can be the basis for formation of foundations of the healthy lifestyle in the social life of population of independent Ukraine.
References:
1. Avicenna. URDZhUZA - pojema o medicine [Al-Urjuzah Fi Al-Tibb - a poem about medicine]., Access mode: http://www.avicenna-sina.narod.ru /urdzhyza.html.
2. Dіagnostika terapіja і profіlaktika іnfekcіjnih hvorob v umovah polіklіnіki [Diagnostics, therapy and prevention of infectious diseases in conditions of outpatient department]., Edited by М.А. Andreichyn. - 2nd ed., revised and supplemented. - Leningrad., Medychna hazeta Ukrayiny [Medical Newspaper of Ukraine]., 1996. - 352 p.
3. Don Colbert. Biblejskie principy zdorovogo pitanija [Biblical principles of healthy nutrition]., Access mode: http://www.wmos.ru/blog/bible/1558.php.
4. Zamozhne suspіl'stvo, konkurentospromozhna ekonomіka, efektivna derzhava, Programi Ekonomіchnih reform., Komіtet z ekonomіchnih reform pri Prezidentovі Ukraїni [Prosperous society, competitive economy, effective state, program of
economic reforms., Committee on economic reforms under the president of Ukraine]., Access mode: http://www.president.gov.ua/docs/rograma_reform_FINAL_2.pdf.
5. Izutkin D.A. Formirovanie zdorovogo obraza zhizni. Sovetskoe zdravoohranenie [Formation of a healthy lifestyle. The Soviet health care]. - 1984., No. 11., pp. 8-11.
6. Lіkars'kі roslini: Encik-lopedichnij dovіdnik [Medicinal plants: Encyclopaedic Reference]., Editted by A.M. Grodzinskyi. - Кiev., Ukrayins'ka entsyklopediya im. M.P. Bazhana, Ukrayins'kyi vyrobnycho-komertsiynyi tsentr “Olimp” [Ukrainian Encyclopaedia n.a. M. Bazhan, Ukrainian industrial and commercial centre "Olympus"], 1992. - 544 p.
7. Martynenko A.V., Valentyk Yu.V., Polesskyi V.A. Formirovanie zdorovogo obraza zhizni molodezhi [Formation of healthy lifestyle of youth]., A.V. Martynenko, Yu.V. Valentyk, V.A. Polesskyi and other. - Мoscow., Medytsyna [Medicine], 1988.
8. Nepravil'noe pitanie i ego posledstvija [Improper nutrition and its consequences]., Access mode: http://humana.ua/index.hp?option=com_content&view=article&id=541%3Anepravilnoe-pitanie-i-ego-posledstvija&catid=56%3Apitanie-malysha &Itemid=208&lang=ru.
9. Nepravil'noe pitanie i ego posledstvija [Improper nutrition and its consequences]., Access mode: http://pediatriya.info/?p=89.
10. Neracional'noe pitanie [Improper nutrition]., Access mode: http://snia.ru/neracionalnoe-pitanie/1174-neracionalnoe-pitanie.html.
11. Osnovy racional'nogo pitanija [Basics of rational nutrition]., Access mode: http://www.feed.tj/racional/.
12. Pereїdannja (gіperfagіja) [Overeating (hyperphagia)]., Access mode: http://onlylife.net/gastro/745-pereyidannya-giperfagiya.html.
13. Brehh P. Chto takoe golodanie? [What is fasting?]. - Мoscow., Astrel', AST, 2007. - 160 p.
14. Principy zdorovogo pitanija [The principles of healthy nutrition]., Access mode: www.dlavseh.com/.../index.php?...
15. Relіgіja і medicina pro svininu [Religion and medicine about
pork]., Access mode: http://www.fondihlas.ru/index.php?option=com c o n t e n t & v i e w = a r t i c l e & i d = 170&Itemid=193.
16. Sv. Al'fons Marіja de Lіguorі. Jak ljubiti Іsusa Hrista [Saint Alphonsus Maria de' Liguori. How to love Jesus Christ?]., Access mode: http://dyvensvit.org/fi les/books/034_lubutu_i_h.pdf.
17. Svinina s tochki zrenija religii i mediciny [Pork from the point of view of religion and medicine]., Access mode: http://kahhar-786.livejournal.com/494600.html.
18. Svin'ja razdora: pochemu u odnih narodov i religij ona - grjaznoe zhivotnoe, u drugih, naprotiv, - svjatoe [Pig of contention: why among some nations and religions it is a dirty animal, while among others, on the contrary, it is holy?]., Access mode: http://spectr.info/science/337-svinya-razdora-dlya-odnih-narodov-ona-gryaznoe-zhivotnoe-u-drugih-svyatoe-pochemu.html.
19. Svjate pis'mo. Povnij pereklad, zdіjsnenij za origіnal'nimi evrejs'kimi, aramіjs'kimi ta grec'kimi testami [The Holy Scripture. Full translation made according to the original Hebrew, Aramaic and Greek tests]. - Кiev., Ukrayins'ke Bibliyne Tovarystvo [Ukrainian Bible Association], 1992. - 352 p.
20. Shukhatovych V.R. Zdorovyj obraz zhizni., Jenciklopedija sociologii [Healthy lifestyle., Encyclopedia of Sociology]. - Minsk., Knyzhnyy Dom [Book house], 2003.
21. Jajce (їzha) [Egg (food)]., Access mode: http://uk.wikipedia.org/wiki/Яйце(їжа).
22. Jak gramotno kontroljuvati rіven' holesterinu. Jajca [How to correctly control cholesterol level. Eggs]., Access mode: http://yaktak.com/dim_i_simya/pr int :page,1,2976-yak-gramotno-kontrolyuvati-riven-xolesterinu.html.
23. What are the disadvantages of animal fats? Access mode: http://www.answers.com/Q/What_are_the_disadvantages_of_animal_fats.
Information about author:
1. Vasyl' Ruden' – Doctor of Medicine, Full Professor, Lviv National Medical University named after Danylo Galitsky; address: Ukraine, Lviv city; e-mail: [email protected]
15
2. Iryna Koval`ska – Senior Lecturer, Lviv National Medical University named after Danylo Galitsky; address: Ukraine, Lviv city; e-mail: [email protected]
3. Dzvenyslava Moskviak-Lesniak – Assistant, Lviv National Medical University named after Danylo Galitsky; address: Ukraine, Lviv city; e-mail: [email protected]
4. Oleksiy-Evgen Vynnytskyi – Physician of Reanimation Department City Clinical Hospital of Emergency Medical Care, address: Ukraine, Lviv city; e-mail: [email protected]
RR
If you wish to know more, please visit: http://gisap.eu
WORLD RESEARCH
ANALYTICSF E D E R A T I O N

16
Introduction. Multiforme exudative erythema (MEE) is an acute
polymorphic dermatosis, which occurs in the form of a bluish-red colour rash on the skin of the extremities, mucous membranes, sometimes in the genital area [1].
The etiology of MEE is not fully understood, so the causes of the disease are varied, but in patients with this disease there is some triggering factor which triggers the mechanism of the immune reaction of hypersensitivity. One of them is the infectious diseases caused by the herpes simplex virus [10], Chlamydia [8] and mycoplasma pneumonia [13]. Another factor is the allergens of medicamentous nature [2, 5-7].
In this regard, many local authors identify infectious-allergic (idiopathic) and toxic-allergic (symptomatic) forms of MEE. In the development of idiopathic form the main trigger factors are infections. In toxic-allergic form the hypersensitivity to different medications is revealed [3]. Toxic-allergic form is characterized by vivid hyperemia, a tendency to merging of lesions, frequent lesions of the mucous membranes, including genital, expressed epidermolytic component (vesicles), isomorphic reaction. Infectious-allergic form is often present in the form of small elements of the "stagnant" shade that do not have a tendency to merge, being preferentially localized on the extremities and less frequently on the mucous membranes [2].
In the clinical practice, the foreign
experts often distinguish two forms of MEE - big and small. Both are characterized by the same type of primary lesions, but differ in the presence or absence of mucosal lesions and general symptoms [14].
According to the International Statistical Classifi cation of Diseases and Related Health Problems, 10th Revision (ICD-10) - WHO Version (2016), the following forms of MEEt (L51 Erythema multiforme) are distinguished: L51.0 Nonbullous erythema multiforme, L51.1 Bullous erythema multiforme, Stevens-Johnson syndrome, L51.2 Toxic epidermal necrolysis [Lyell], L51.8 Other erythema multiforme, L51.9 Erythema multiforme, unspecifi ed [9].
As the disease develops acutely, it demands the treatment at an early stage. However, cystic syndrome in the oral cavity appears at a number of dermatoses (Lyell's syndrome, acantholytic and non-acantholytic pemphigus, bullous pemphigoid, Duhring’s disease, bullous form of Lichen ruber planus, vesical-vascular syndrome, acute herpetic stomatitis), which requires timely differential diagnosis of this condition. One of the methods of diagnosis of MEE is cytology. It is relatively informative, non-invasive; it takes little time and is acceptable to patients.
The aim of the study was to investigate the features of the cytological picture under toxic-allergic form of multiforme exudative erythema in oral cavity.
Materials and methods. The study included 15 patients with MEE (6 men
and 9 women), aged 26-57, directed to the department for consultation. We adhered to the domestic interpretation of the diagnosis formulation and considered the type of MEE in patients as a toxic-allergic, which corresponds to the code L51.1 Bullous erythema multiforme, Stevens-Johnson syndrome ICD-10. All patients, after removing the pellicle, underwent the sampling of the contents of erosion by scraping. The material was fi xed in a solution of methanol, stained by Romanovsky-Giemsa method. In cytological preparations the qualitative and quantitative composition of hematogenous and histiogenous cellular elements was studied.
Results. All patients reported rapid development of the disease, usually within 1-2 days. There was sharp pain in the oral cavity even at rest, worse when speaking, moving the tongue or eating. From the medical history we found out that before the development of stomatitis the patients were treated, for various reasons, with medications (antibiotics, sulfonamides, non-steroidal anti-infl ammatory drugs, tranquilizers). It should be noted that here we indicate only groups of drugs, which, according to the literature, most commonly cause the toxic and allergic reactions. However, patients took, on their own or prescribed by a doctor, not only these drugs, but others as well: vitamins, desensitization, expectorants, antacid, etc. Therefore, it is diffi cult to indicate the specifi c source of the drug-induced allergic reactions.
While examining the oral cavity we observed diffuse or limited erythema and
U.D.C. 616.511+616.31]-021-091.8-093
FEATURES OF THE CYTOLOGICAL PICTURE AT MULTIFORME EXUDATIVE ERYTHEMA IN THE ORAL CAVITY
Yu. Lakhtin1, Doctor of Medicine, Associate ProfessorP. Moskalenko2, Candidate of Medicine, Assistant
L. Karpez3, Candidate of Medicine, AssistantSumy State University, Ukraine1,2
Kharkiv Post-graduate Medical Academy, Ukraine3
Authors have studied the cytological picture of contents of the erosions in patients with toxic-allergic form of the multiforme exudative erythema in the oral cavity. It was found out that the composition of cellular elements is specifi c for the exudate of nonspecifi c infl ammation. Hematogenous and histiogenous cells are mostly not destroyed. There are numerous mononuclear type cells, polyblasts, eosinophils and epithelium frequently being in the state of hydropic degeneration.
Keywords: multiforme exudative erythema, toxic-allergic reaction, cytology, eosinophils, polyblasts, mononuclear cells.
Conference participants,National championship in scientifi c analytics,
Open European and Asian research analytics championship
http://dx.doi.org/10.18007/gisap:msp.v0i13.1653
17
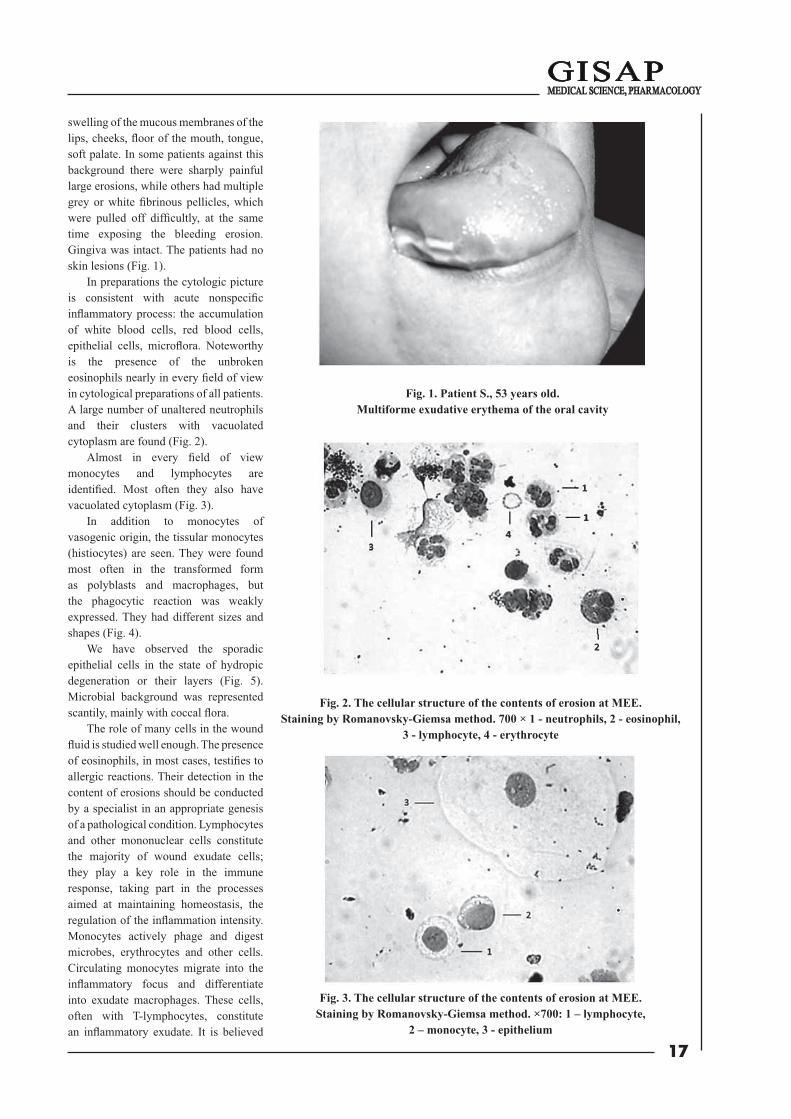
swelling of the mucous membranes of the lips, cheeks, fl oor of the mouth, tongue, soft palate. In some patients against this background there were sharply painful large erosions, while others had multiple grey or white fi brinous pellicles, which were pulled off diffi cultly, at the same time exposing the bleeding erosion. Gingiva was intact. The patients had no skin lesions (Fig. 1).
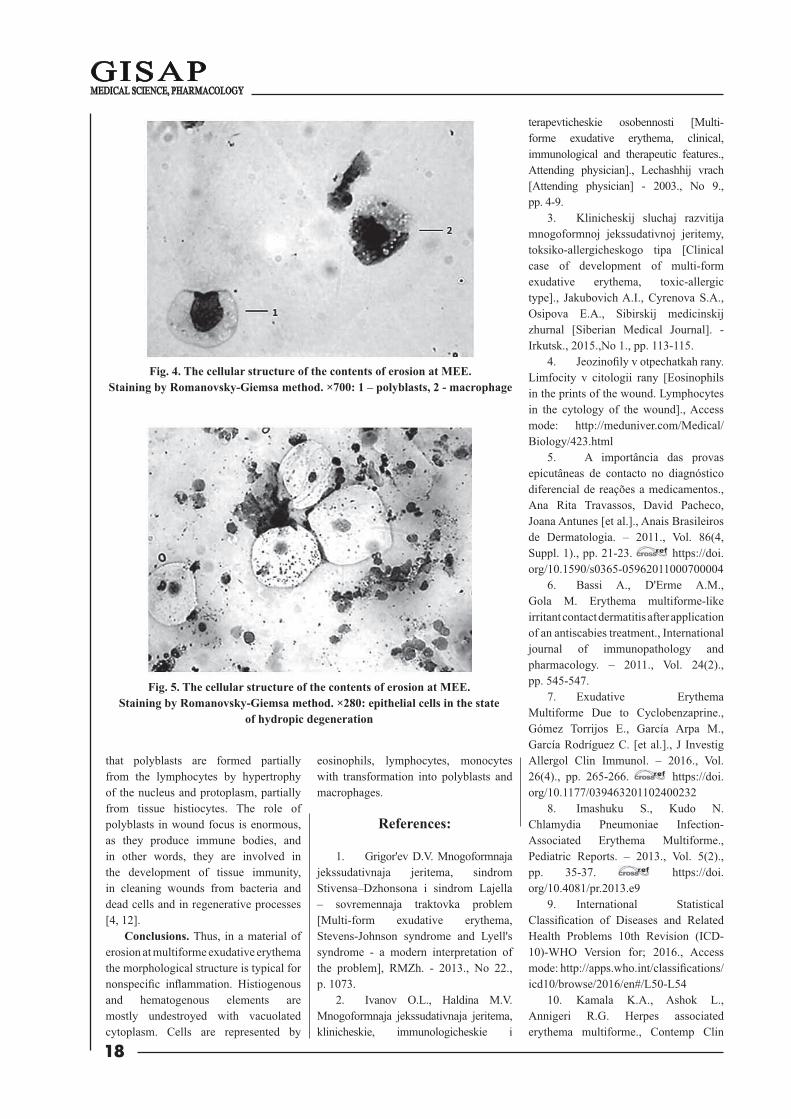
In preparations the cytologic picture is consistent with acute nonspecifi c infl ammatory process: the accumulation of white blood cells, red blood cells, epithelial cells, microfl ora. Noteworthy is the presence of the unbroken eosinophils nearly in every fi eld of view in cytological preparations of all patients. A large number of unaltered neutrophils and their clusters with vacuolated cytoplasm are found (Fig. 2).
Almost in every fi eld of view monocytes and lymphocytes are identifi ed. Most often they also have vacuolated cytoplasm (Fig. 3).
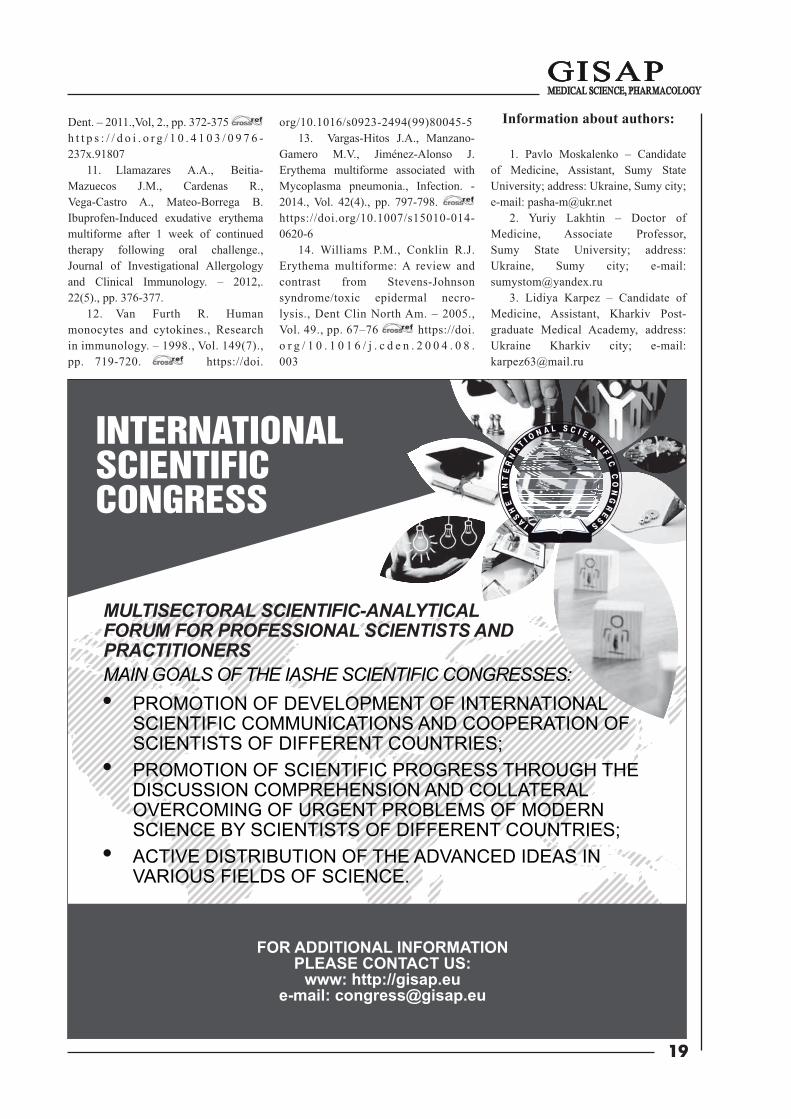
In addition to monocytes of vasogenic origin, the tissular monocytes (histiocytes) are seen. They were found most often in the transformed form as polyblasts and macrophages, but the phagocytic reaction was weakly expressed. They had different sizes and shapes (Fig. 4).
We have observed the sporadic epithelial cells in the state of hydropic degeneration or their layers (Fig. 5). Microbial background was represented scantily, mainly with coccal fl ora.
The role of many cells in the wound fl uid is studied well enough. The presence of eosinophils, in most cases, testifi es to allergic reactions. Their detection in the content of erosions should be conducted by a specialist in an appropriate genesis of a pathological condition. Lymphocytes and other mononuclear cells constitute the majority of wound exudate cells; they play a key role in the immune response, taking part in the processes aimed at maintaining homeostasis, the regulation of the infl ammation intensity. Monocytes actively phage and digest microbes, erythrocytes and other cells. Circulating monocytes migrate into the infl ammatory focus and differentiate into exudate macrophages. These cells, often with T-lymphocytes, constitute an infl ammatory exudate. It is believed
Fig. 1. Patient S., 53 years old. Multiforme exudative erythema of the oral cavity
Fig. 2. The cellular structure of the contents of erosion at MEE. Staining by Romanovsky-Giemsa method. 700 × 1 - neutrophils, 2 - eosinophil,
3 - lymphocyte, 4 - erythrocyte
Fig. 3. The cellular structure of the contents of erosion at MEE. Staining by Romanovsky-Giemsa method. ×700: 1 – lymphocyte,
2 – monocyte, 3 - epithelium
18
that polyblasts are formed partially from the lymphocytes by hypertrophy of the nucleus and protoplasm, partially from tissue histiocytes. The role of polyblasts in wound focus is enormous, as they produce immune bodies, and in other words, they are involved in the development of tissue immunity, in cleaning wounds from bacteria and dead cells and in regenerative processes [4, 12].
Conclusions. Thus, in a material of erosion at multiforme exudative erythema the morphological structure is typical for nonspecifi c infl ammation. Histiogenous and hematogenous elements are mostly undestroyed with vacuolated cytoplasm. Cells are represented by
eosinophils, lymphocytes, monocytes with transformation into polyblasts and macrophages.
References:
1. Grigor'ev D.V. Mnogoformnaja jekssudativnaja jeritema, sindrom Stivensa–Dzhonsona i sindrom Lajella – sovremennaja traktovka problem [Multi-form exudative erythema, Stevens-Johnson syndrome and Lyell's syndrome - a modern interpretation of the problem], RMZh. - 2013., No 22., p. 1073.
2. Ivanov O.L., Haldina M.V. Mnogoformnaja jekssudativnaja jeritema, klinicheskie, immunologicheskie i
terapevticheskie osobennosti [Multi-forme exudative erythema, clinical, immunological and therapeutic features., Attending physician]., Lechashhij vrach[Attending physician] - 2003., No 9., pp. 4-9.
3. Klinicheskij sluchaj razvitija mnogoformnoj jekssudativnoj jeritemy, toksiko-allergicheskogo tipa [Clinical case of development of multi-form exudative erythema, toxic-allergic type]., Jakubovich A.I., Cyrenova S.A., Osipova E.A., Sibirskij medicinskij zhurnal [Siberian Medical Journal]. - Irkutsk., 2015.,No 1., pp. 113-115.
4. Jeozinofi ly v otpechatkah rany. Limfocity v citologii rany [Eosinophils in the prints of the wound. Lymphocytes in the cytology of the wound]., Access mode: http://meduniver.com/Medical/Biology/423.html
5. A importância das provas epicutâneas de contacto no diagnóstico diferencial de reações a medicamentos., Ana Rita Travassos, David Pacheco, Joana Antunes [et al.]., Anais Brasileiros de Dermatologia. – 2011., Vol. 86(4, Suppl. 1)., pp. 21-23. https://doi.org/10.1590/s0365-05962011000700004
6. Bassi A., D'Erme A.M., Gola M. Erythema multiforme-like irritant contact dermatitis after application of an antiscabies treatment., International journal of immunopathology and pharmacology. – 2011., Vol. 24(2)., pp. 545-547.
7. Exudative Erythema Multiforme Due to Cyclobenzaprine., Gómez Torrijos E., García Arpa M., García Rodríguez C. [et al.]., J Investig Allergol Clin Immunol. – 2016., Vol. 26(4)., pp. 265-266. https://doi.org/10.1177/039463201102400232
8. Imashuku S., Kudo N. Chlamydia Pneumoniae Infection-Associated Erythema Multiforme., Pediatric Reports. – 2013., Vol. 5(2)., pp. 35-37. https://doi.org/10.4081/pr.2013.e9
9. International Statistical Classifi cation of Diseases and Related Health Problems 10th Revision (ICD-10)-WHO Version for; 2016., Access mode: http://apps.who.int/classifi cations/icd10/browse/2016/en#/L50-L54
10. Kamala K.A., Ashok L., Annigeri R.G. Herpes associated erythema multiforme., Contemp Clin
Fig. 4. The cellular structure of the contents of erosion at MEE. Staining by Romanovsky-Giemsa method. ×700: 1 – polyblasts, 2 - macrophage
F ig. 5. The cellular structure of the contents of erosion at MEE. Staining by Romanovsky-Giemsa method. ×280: epithelial cells in the state
of hydropic degeneration
19
Dent. – 2011.,Vol, 2., pp. 372-375 h t t p s : / / d o i . o r g / 1 0 . 4 1 0 3 / 0 9 7 6 -237x.91807
11. Llamazares A.A., Beitia-Mazuecos J.M., Cardenas R., Vega-Castro A., Mateo-Borrega B. Ibuprofen-Induced exudative erythema multiforme after 1 week of continued therapy following oral challenge., Journal of Investigational Allergology and Clinical Immunology. – 2012,. 22(5)., pp. 376-377.
12. Van Furth R. Human monocytes and cytokines., Research in immunology. – 1998., Vol. 149(7)., pp. 719-720. https://doi.
org/10.1016/s0923-2494(99)80045-513. Vargas-Hitos J.A., Manzano-
Gamero M.V., Jiménez-Alonso J. Erythema multiforme associated with Mycoplasma pneumonia., Infection. - 2014., Vol. 42(4)., pp. 797-798. https://doi.org/10.1007/s15010-014-0620-6
14. Williams P.M., Conklin R.J. Erythema multiforme: A review and contrast from Stevens-Johnson syndrome/toxic epidermal necro-lysis., Dent Clin North Am. – 2005., Vol. 49., pp. 67–76 https://doi.o r g / 1 0 . 1 0 1 6 / j . c d e n . 2 0 0 4 . 0 8 .003
Information about authors:
1. Pavlo Moskalenko – Candidate of Medicine, Assistant, Sumy State University; address: Ukraine, Sumy city; e-mail: [email protected]
2. Yuriy Lakhtin – Doctor of Medicine, Associate Professor, Sumy State University; address: Ukraine, Sumy city; e-mail: [email protected]
3. Lidiya Karpez – Candidate of Medicine, Assistant, Kharkiv Post-graduate Medical Academy, address: Ukraine Kharkiv city; e-mail: [email protected]
INTERNATIONALSCIENTIFICCONGRESS
MAIN GOALS OF THE IASHE SCIENTIFIC CONGRESSES: PROMOTION OF DEVELOPMENT OF INTERNATIONAL SCIENTIFIC COMMUNICATIONS AND COOPERATION OF SCIENTISTS OF DIFFERENT COUNTRIES; PROMOTION OF SCIENTIFIC PROGRESS THROUGH THE DISCUSSION COMPREHENSION AND COLLATERAL OVERCOMING OF URGENT PROBLEMS OF MODERN SCIENCE BY SCIENTISTS OF DIFFERENT COUNTRIES; ACTIVE DISTRIBUTION OF THE ADVANCED IDEAS IN VARIOUS FIELDS OF SCIENCE.
MULTISECTORAL SCIENTIFIC-ANALYTICAL FORUM FOR PROFESSIONAL SCIENTISTS AND PRACTITIONERS
FOR ADDITIONAL INFORMATIONPLEASE CONTACT US:
www: http://gisap.eu e-mail: [email protected]

20
One of the most perspective approaches to non-invasive
diagnostics, focused on the oral cavity and upper gastrointestinal tract diseases is to consider the examination of the oral fl uid composition.
Oral fl uid criteria should describe both the local and general reactions, i.e. covered mucous membranes of a digestive tract. Composition of the oral fl uid should change in case of infl ammatory and non-infl ammatory lesions, detected in oral cavity and in upper gastrointestinal tract.
Non-specifi c antimicrobial components of the oral fl uid are protein-carbohydrate complexes (glycoproteins). Protein and glycoproteins create the oral fl uid viscosity and a layer that protects mucous membranes of the oral cavity from infl uence of factors of the physical and chemical nature, pathogenic microfl ora.
Purpose of the research
The purpose is to study the content of the protein and glycoproteins, their
components in the oral fl uid in children with chronic gastritis or duodenitis.
Materials and methods
189 patients were examined. Among them there were 92 (48.7%) boys and 97 (51.3%) girls, aged from 12 to 17. The fi rst group included 107 patients with chronic gastritis, duodenitis. The second group (control) included 82 children with healthy oral cavity, without the somatic pathology.
Patients in the fi rst group (56 girls and 51 boys) were treated in the gastroenterological department of the regional children's clinical hospital. Period of the gastrointestinal disease in the examined patients, according to the anamnesis, varied from 1 to 6 years. Diagnosis of gastroduodenal pathology was confi rmed after clinical, endoscopic and ultrasonic examinations.
The content of glycoproteins, hexosamines, fucose and sialic acids in the oral fl uid was determined among children with chronic gastritis,
duodenitis, and among children of the control group, according to our original methods. Research of the protein was carried out by biuret method.
Results and discussion
Analysis of oral fl uid revealed the increase of protein content among children with chronic gastritis, duodenitis (table 1). Chronic gastritis and duodenitis are acid-related diseases. Their basic pathogenic link should be increasing production of the hydrochloric acid by the stomach glands. Increase of protein content in the oral fl uid of children is considered to be protective reaction of the organism against the rising gastric juice acidity and refl ux of acid stomach contents into the esophagus with concomitant motor disorders in the gastrointestinal tract.
In our opinion, increase of the protein level in the oral fl uid is the compensatory reaction, which has shown an intensive function of salivary glands at the infl ammatory processes
Тab. 1.Content of protein and glycoproteins, their components in the oral fl uid at the children in the research groups (М±m)
Groups IndicatorsTotal protein, g/l Common
glycoproteins, mg/mlSialic
acids, mmol/lFucose,mmol/l
Hexosamines, mmol/l
1(n=107)
7.33±0.43р<0.01
0.03±0.01р<0.01
0.16±0.01р<0.01
0.87±0.02р<0.01
0.23±0.01р<0.01
2(n=82)
2.57±0.06 0.10±0.01 0.14±0.01 0.61±0.01 0.49±0.02
Note. р – signifi cance of differences compare with indicators in the control group.
CONTENT OF PROTEIN AND GLYCOPROTEINS, THEIR COMPONENTS IN THE ORAL FLUID IN CHILDREN WITH CHRONIC GASTRITIS, DUODENITIS
E. Romanenko1, Doctor of MedicineA. Shtompel2, Ph.D. in Medicine, Assistant
O. Sinkovskaya3, Ph.D. in MedicineA. Matveeva4, StudentN. Mirotina5, Doctor
Dnipropetrovsk Medical Academy, Ukraine1,2,3,4
Dnipropetrovsk city children’s dental polyclinic No. 2, Ukraine5
In the oral fl uid of children with chronic gastritis, duodenitis there is the increased protein content (up to 7.33±0.43 g/l) against the background of the decreasing level of glycoproteins (up to 0.03±0.01 mg/ml). Coeffi cient of ratio protein / glycoproteins in the oral fl uid is increased by a factor of 9510, which has shown the intensive decay of protein-carbohydrate complexes and the increasing content of the protein fragments. In the composition of glycoproteins there is the reduced amount of hexosamines (up to 0.23±0.01 mmol/l), against the background of the increasing sialic acids (up to 0.16±0.01 mmol/l) and fucose (up to 0.87±0.02 mmol/l). Coeffi cient of ratio of terminal and corpus monosaccharides in the glycoproteins of the oral fl uid in patients with chronic gastritis, duodenitis is increased by a factor of 2.41 and 3.34, as compared to the same values in the control group of children, which signifi cantly modifi es the functional properties of the protein-carbohydrate complexes.
Keywords: oral fl uid, gastritis, duodenitis, glycoproteins, hexosamines, sialic acids, fucose.
Conference participants
http://dx.doi.org/10.18007/gisap:msp.v0i13.1654

21
of gastroduodenal area. Examination of the protein level using the biuret method allows us to identify its fragments, fi rstly. Secondly, we could reveal a link between the increasing total protein level and the fast disintegration in the structures of an upper digestive tract.
At the same time, content of glycoproteins was signifi cantly decreased in children with chronic gastritis, duodenitis, as the result of their rapid destruction in the oral cavity, and deterioration synthesis of the protein-carbohydrate complexes in the salivary glands.
In the course of the research the composition of glycoproteins, taken from saliva in the control group of children, revealed that average level of monosaccharides is decreasing in the following order: fucose (0.61±0.01 mmol/l), hexosamines (0.49±0.02 mmol/l), sialic acids (0.14±0.01 mmol/l) (table 1). Typical feature of biochemical disorders in the structure of glycoproteins taken from oral fl uid of children with chronic gastritis, duodenitis is the decreasing amount of hexosamines, which should demonstrate a number and length of carbohydrate chains in the glycoproteins. Decreasing level of hexosamines has shown the violation of the glycoprotein synthesis, occurring in the salivary and mucous glands.
The given trend was typical for structural changes in the epithelial cells of oral cavity, which should provoke violation of the protective properties of oral fl uid. In this case takes place the growth of concentration of the sialic acids, i.e. fucose, which should be crucially important for creation of additional links between carbohydrate connections in some parts of the glycoprotein molecule.
Finally, decrease of hexosamines demonstrates the chronic pathology in the upper digestive tract. Sialic acids and fucose in the protein-carbohydrate complexes were located terminally. Thus, the sialic acids are responsible for hydrophilic properties of the glycoproteins; fucose should support the hydrophobic sites in a molecule, thereby, ensuring their adhesion to the hydrophobic areas in the membrane epithelial cells. The demonstrated situation contributes to enhanced colonization of epithelial cells by pathogenic microorganisms. Increasing level of sialic acids in the glycoproteins should lead to the increase of the oral fl uid viscosity. In the physiologic conditions it protects the epithelium from adhesion with pathogens.
Increasing of the oral fl uid hydrophobicity was associated with high content of fucose. It contributes to its thickening at the infl ammation in the mouth and reduces its protective properties. Increasing content of the sialic acids in patients of the fi rst group, as compared to the control group, demonstrates the development of the compensatory reactions in response to tissue infl ammation in the upper digestive tract. However, taking into account the irregularities in the structure of glycoproteins as the result of the decreasing content of hexosamines the fucose is increasing. We believe in this
case, that changes of protective properties of the oral fl uid are a part of pathogenesis of the oral cavity diseases.
At the same time, despite the signifi cant differences in amounts of separate monosaccharides, the general quantity of monosaccharides in the 1st group of the studied children had no signifi cant difference from the same indicator shown by children of the control group (table 2). This fact is explained by signifi cant increasing of the terminal glycoprotein monosaccharides (sialic acids and fucose) against the background of reduction of content of the corpus monosaccharides (hexosamine). Although, the total amount of monosaccharides in a glycoprotein should not change, some changes occurred in the functional properties of protein-carbohydrate complexes.
Particular attention should be paid to examination of relationships in the content of protein and the protein-carbohydrate complexes, corpus and terminal monosaccharides in glycoproteins as the criteria, which refl ected the imbalance between damaging and protective factors in the oral fl uid
In order to determine the quality indicators of the oral fl uid we have calculated the coeffi cient of ratios of protein and the glycoproteins, the corpus and terminal monosaccharides (table 3).
Тab. 2.Indicators total amount of monosaccharides in the oral fl uid glycoproteins at
the children groups (М±m)Groups Total amount of monosaccharides, mmol/l
1(n=107)
1.23±0.02р=0.08
2(n=82)
1.24±0.02
Note. р – signifi cance of differences compare with indicators in the control group.
Тab. 3.Ratio of protein and protein-carbohydrate complexes, corpus and terminal monosaccharides in the oral fl uid (М±m)
Groups Coeffi cient of ratiosProtein / glycoproteins Sialic
acids/ hexosamines Fucose / hexosamines
1(n=107)
244.33×103±26.02р<0.01
0.70±0.12р<0.01
4.14±0.45р<0.01
2(n=82)
25.70×103±3.26 0.29±0.05 1.24±0.10
Note. р – signifi cance of differences compare with indicators in the control group.
22
It has been found out, that in the oral fl uid of children from the control group the ratio of protein to glycoproteins was 25.70×103, sialic acids to hexosamines – 0.29, fucose to hexosamines – 1.24. In the children of the 1st group, ratio of protein / glycoproteins in the oral fl uid increased by 9510 times (p<0.01), which indicates fast disintegration of glycoproteins in the oral cavity and the increasing content of protein fragments due to exposure of the microbial enzymes. Coeffi cient of ratio terminal and corpus monosaccharides in the glycoproteins of oral fl uid among the patients with chronic gastritis, duodenitis is increasing, as compared to the same indices in the control group of children, by 2.41 and 3.34 times (p<0.01).
Given changes could indicate the serious violation of biosynthesis and degradation of all components of the glycoproteins in the oral fl uid in the course of the upper gastrointestinal tract diseases.
Taking into account, that immune defence of the oral cavity (immunoglobulins, complement, interferon) is represented by the protein-carbohydrate complexes, we believe, that in order to assess the barrier properties of oral fl uid the research should be conducted, which should be focused on the level of hexosamines, because it allows us to make a qualitative assessment of maturity of glycoproteins.
Conclusions
Basic feature of biochemical indices should be focused on the oral fl uid of children with chronic gastritis, duodenitis, having the increased protein content (up to 7.33±0.43 g/l) against the background of the decreasing level of glycoproteins (up to 0.03±0.01 mg/ml). Coeffi cient of ratio protein / glycoproteins in the oral fl uid has increased by 9510 times, as compared to the same indicator in the control group of children. This indicates the fast disintegration of glycoproteins in the oral cavity. Qualitative composition of glycoproteins has changed due to the decreasing level of hexosamines (to 0.23±0.01 mmol/l), increasing concentrations of the sialic acids (to 0.16±0.01 mmol/l) and fucose (to 0.87±0.02 mmol/l). Coeffi cient of ratio for the terminal and corpus monosaccharides in the glycoproteins of oral fl uid in patients with chronic gastritis, duodenitis has increased, as compared to the same indices in the control group of children, by 2.41 and 3.34 times, and this signifi cantly modifi es the functional properties of the protein-carbohydrate complexes.
References:
1. Methods of determination glycoproteins and their components (hexosamines, fucose, sialic acids) with diagnostic purpose in the mixed saliva at the children with gastroduodenal
pathology: metodical recommendations., Yu.M. Stepanov, O.H. Romanenko, V.O. Kondratiev, et all. – Kyiv., 2015. – 20 p.
2. Tailford L.E. Mucin glycan foraging in the human gut microbiоte., E.L. Tailford, E.H. Crost, D. Kavanaugh, N. Juge., Frontal Genetics. - 2015. - Vol. 19, No. 6. pp. 81-86. https://doi.org/10.3389/fgene.2015.00081
3. Spielmann N. Saliva: diagnostics and therapeutic perspectives., N. Spielmann, D.T. Wong., Clininical Therapy. - 2015., Vol. 37, No. 3., pp. 529 - 539. https://doi.org/10.1111/j.1601-0825.2010.01773.x
Information about authors: 1. Elena Romanenko – Doctor of
Medicine, Dnipropetrovsk Medical Academy, address: Ukraine, Dnipro city; e-mail: [email protected]
2. Anna Shtompel – PhD in Medicine, Assistant, Dnipropetrovsk State Medical Academy, address: Ukraine, Dnipro city; e-mail: [email protected]
3. Olga Sinkovskaya – PhD in Medicine, Dnipropetrovsk State Medical Academy, address: Ukraine, Dnipro city; e mail: [email protected]
4. Anna Matveeva – Student, Dnipropetrovsk State Medical Academy, address: Ukraine, Dnipro city; e-mail: [email protected]
5. Natalya Mirotina – Doctor, Dnipropetrovsk city children's dental polyclinic No. 2, address: Ukraine, Dnipro city; e-mail: [email protected]

23
Introduction
Delivery of medical aid to the injured patients with the polytrauma with the prevailing abdominal and thorax injuries may assume high level of diagnostic errors, post-surgical complications, disability and mortality, which points out the need for further improvement of diagnostic algorithms and surgical treatment of this category of patients [Abacumov and co-authors, 2005; Yartsev and co-authors, 2008]. Minimally invasive operations have been widely applied in the foreign and national surgery during the last years. They have been used even more frequently for the patients with emergency surgical diseases due to the practical implementation of modern technologies. Enhanced life quality of patients, reduced time of their stay in the hospital, as well as the reduced time of their temporary disability and amount of complications are the important advantages of these surgeries.
The aim of our study was to enhance the health care effi ciency for patients in case of polytrauma with the prevailing abdominal and thorax injury.
Methods and materials
We observed 822 injured patients with polytrauma with the prevailing pathology of abdominal and thorax injuries. The age of patients varied from 17 to 70. The average age was 43.5±3.45. There were 487 men (59.25%) and 335 women (40.75%). 281 patients had associated somatic dysfunctions. In particular, 103 patients (12.5%) suffered from the coronary
heart disease accompanied by diffuse and post-infarction cardiosclerosis; 62 patients (7.5%) had chronic bronchitis and pulmonary emphysema; 57 patients (6.9%) had diabetes mellitus; 38 patients (4.6%) had chronic pyelonephritis, and 21 patients (2.6%) – chronic cerebrovascular disorder.
A certain diagnosing algorithm was used, including the laboratory tests, U/S of abdominal cavity organs, multiple-view X-ray imaging, observation catheter setting, CT, MRI, and laparoscopy.
Bleeding of parenchymal organs was stopped by our patented method of U-shaped hemostatic suturing on the mesh implant Rebound HDR with the Nitinol frame. The mesh was introduced to the abdominal cavity through the laparoscopic port, after which it unfolded in the abdominal cavity immediately thanks to the Nitinol frame. Then the mesh was put on the diaphragmatic surface of liver, and a similar mesh – on the visceral surface of liver. U-shaped sutures were put on liver through the meshes. As the mesh was in constant tension due to the Nitinol frame, the suture pressure was spread uniformly over the mesh surface, which prevented the liver tissue from being cut with sutures. This ensured safe hemostasis. For better hemostasis we used fi brin glue TachoComb in combination with the framed mesh, which was applied to the section line and was put under the mesh to the section line. In the latter case the mesh performed the plugging and fi xation function.
For the purpose of diagnosing the thorax injuries we used X-ray thorax imaging, computer tomography, and
magnetic resonance imaging. In some cases pleural puncture was done.
Upon detecting a considerable amount of blood in the pleural cavity, thoracoscopy was conducted. During the thoracoscopy we discovered the source of bleeding after the aspiration of blood and blood clots, followed by coagulation of bleeding vessels.
Thoracoscopy was conducted in 48 cases as follows: the patient lies in the lateral position on the healthy side on a roll placed between the 4th and 5th rib, which ensures maximum spreading of ribs from the intervention side and provides good visualization of the pleural cavity, all sections of diaphragm and mediastinum. Based on the data [Om and co-authors, 2005], it has 100% sensitivity, 97% specifi city, and 98% accuracy. In order to introduce the thoracoscope we used a point in the fi fth or sixth intercoastal space at the midaxillary line. After introducing the thoracoscope we also did two or three additional thorax sections, when necessary, and set ports for introduction of manipulators and instruments.
Results:
We analysed the results of diagnosing and treatment of 822 patients with polytrauma with the abdominal and thorax injuries. No major injuries were discovered in 190 patients during the examination, which allowed to treat them without surgery. In 204 cases major abdominal and thorax injuries were discovered during the examination, which served an indication for emergency laparotomy.
U.D.C. 61.831-005-073.432.19:612.13
EFFICIENCY OF LAPAROSCOPY FOR PATIENTS SUFFERING FROM POLYTRAUMA WITH PREVAILING ABDOMINAL AND CHEST INJURIES
A. Plotnikov, SurgeonYu. Hrubnyk, Doctor of Medicine, Head of Department
Odessa National Medical University, Ukraine
The author analyses the results of diagnostics and treatment of 822 patients suffering from the polytrauma with the prevailing abdominal and thorax injuries. In 428 cases the laparoscopy has been used for diagnosing and treatment. In 150 (35%) cases, no signifi cant injuries have been discovered, and the surgery ended with the abdominal drainage. In 162 (37.9%) cases the laparoscopic surgery was conducted, and in 116 (27.1%) cases the conversion (laparostomy) was done. Operative mortality was 5 (3%) cases.
Keywords: laparoscopy, surgery, injury, polytrauma.
Conference participants
http://dx.doi.org/10.18007/gisap:msp.v0i13.1655

24
In 428 cases laparoscopic diagnosing was done to ascertain the diagnosis. In 150 out of 428 video laparoscopies no major abdominal injuries were discovered, and the intervention ended with the abdominal drainage. In 162 cases laparoscopic surgeries were done. During the laparoscopic surgeries we widely used electrocoagulation in different modifi cations for the purpose of bleeding control. Besides, to stop bleeding and achieve safe hemostasis we developed and implemented in practice a method of fi xation of polypropylene and other kinds of meshes on an elastic Nitinol frame to the rupture line of parenchymal organs (patent dated December 26, 2011, No. 66396).
In some cases TachoComb was put under the mesh to the rupture line to ensure safe hemostasis.
In 41 cases, in the case of live injury degree III according to OIS (Organ Injury Scaling) with the subcapsular hematoma of over 25-50% of liver surface with the continued bleeding, the method of Nitinol frame-based mesh implant application was used. Hemostasis applied according to our methodology (application of a polypropylene mesh on an elastic Nitinol frame) turned out to be very effective in the cases of subcapsular hematomas with the continued bleeding and in the case of intrahepatic hematomas. No recurring bleeding was observed in any of 34 cases. Abdominal cavity was mandatorily drained in the dextral hypochondrium with PVC drainage.
For the purpose of mitigating the
risk of occurrence of irreversible shock and replenishing the circulating blood volume for patients with the apparent medium and heavy blood loss, we have widely used autohemotransfusions using Cell Saver 5 for 43 patients.
Cell Saver 5 allowed extending the list of indications for laparoscopy and laparoscopic surgeries even in case of hemoperitoneum of up to 1,500 ml, and limiting the scope of contraindications for laparoscopic interventions considerably, paying more attention to the state of hemodynamics and cardiovascular disorder. Based on our data we believe that the contraindications to laparoscopy in the case of abdominal injuries include terminal state of patients, multiple injuries of hollow organs, general purulent peritonitis, massive intra-abdominal bleeding (over 1,500 ml of blood), diaphragm injury, and certain combinations of injuries characterised by the crush injury of internal abdominal organs. Therefore, the use of laparoscopic technologies for abdominal injuries is appropriate. Wide diagnostic and treatment opportunities of the method determine not only its expediency, but also the need for the reasonable active surgical tactic. According to our data, laparoscopic surgeries allow to exclude unnecessary laparotomies, to perform a complete surgery in over a half of patients (62%) who need endovideolaparoscopic interventions.
As it does not seem to be possible to compare 162 patients who underwent laparoscopic surgery and 320 patients who underwent laparotomy due to a
different severity level of the general state of patients and different severity of their injuries, we took a group of 50 patients who underwent treatment before the introduction of laparoscopic surgeries and had the injuries of the degree not exceeding I-III according to OIS (which corresponds to the degree of abdominal and thorax injuries of the patients who underwent laparoscopic surgery) in order to evaluate effi ciency of laparoscopic surgeries in case of polytrauma with the prevailing abdominal and thorax injuries. In order to assess the effi ciency of laparoscopic surgeries we performed a comparative analysis of the duration of laparoscopic surgeries and similar surgeries in the control group of patients who underwent laparotomy. These data are shown in Table 1. Table 1 shows that the duration of video-laparoscopic intervention in most cases was shorter, because opening and closure of the laparotomic access takes more time.
The greatest differences between the video-laparoscopic and traditional laparotomic intervention are observed during the post-surgical period. Treatment duration in the intensive care unit after the video-laparoscopic surgery was 0.84±0.4 days; for patients who underwent laparotomic surgery it was 1.20±0.4 days (р>0,05), and for patients who underwent curative laparotomy it was 2.60±0.7 days. We should also consider the extended period of stay in the intensive care unit up to 3.08±0.7 days in case conversion is needed.
Comparison of post-surgical complications in the control groups
Tab. 1.Comparison chart of the duration of operative treatment of patients who underwent laparoscopy and laparotomy
in the case of abdominal injury
Kinds of surgeryTime of surgery
Patients with laparoscopy Patients with laparotomySurgeries in the case of liver injury degree 1-3 according to OIS 70.63±2.54 60±2.64Surgeries in the case of spleen injury degree 1-2 according to OIS
51.38±1.88 73.25±3.75
Surgeries in the case of stomach injury 62±2.2 59.25±2.58Surgeries in the case of small intestinal wound 52.88±1.82 48.63±1.82Surgeries in the case of urinary bladder wound 46.88±0.65 65.38±1.28Surgeries in the case of mesentery wound 53.38±1.91 55.25±1.26Total patients 162 50
p<0.05
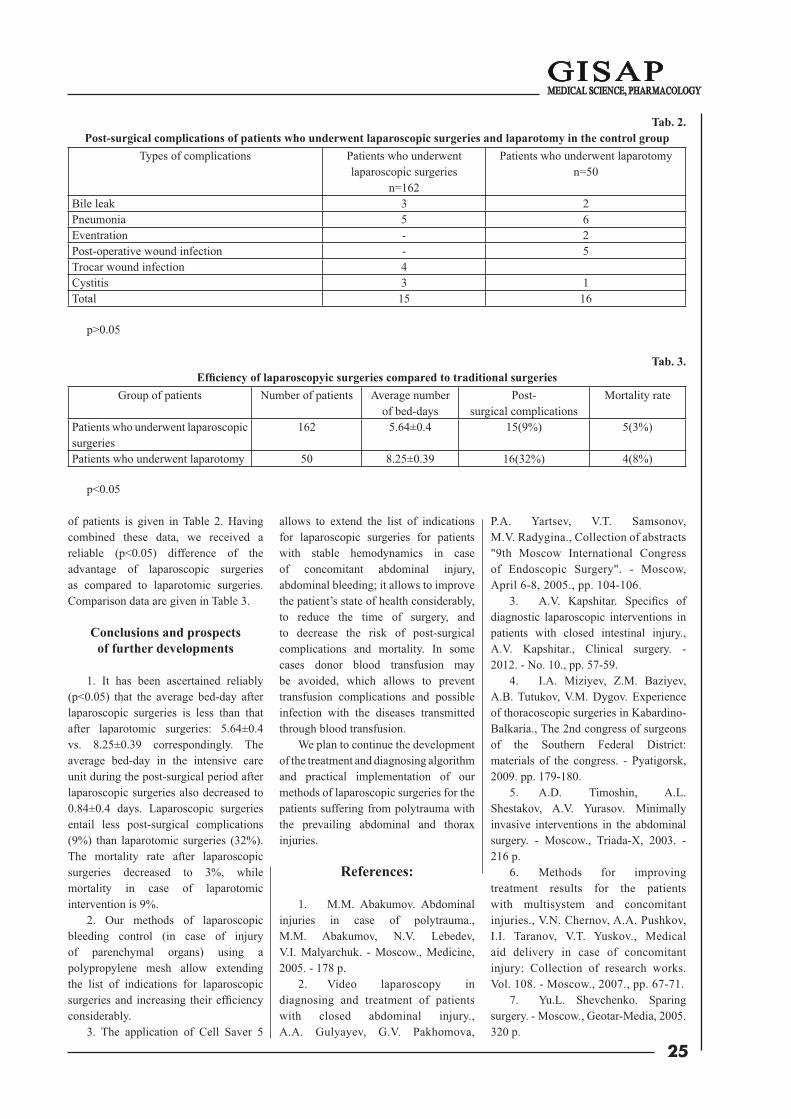
25
of patients is given in Table 2. Having combined these data, we received a reliable (p<0.05) difference of the advantage of laparoscopic surgeries as compared to laparotomic surgeries. Comparison data are given in Table 3.
Conclusions and prospects of further developments
1. It has been ascertained reliably (p<0.05) that the average bed-day after laparoscopic surgeries is less than that after laparotomic surgeries: 5.64±0.4 vs. 8.25±0.39 correspondingly. The average bed-day in the intensive care unit during the post-surgical period after laparoscopic surgeries also decreased to 0.84±0.4 days. Laparoscopic surgeries entail less post-surgical complications (9%) than laparotomic surgeries (32%). The mortality rate after laparoscopic surgeries decreased to 3%, while mortality in case of laparotomic intervention is 9%.
2. Our methods of laparoscopic bleeding control (in case of injury of parenchymal organs) using a polypropylene mesh allow extending the list of indications for laparoscopic surgeries and increasing their effi ciency considerably.
3. The application of Cell Saver 5
allows to extend the list of indications for laparoscopic surgeries for patients with stable hemodynamics in case of concomitant abdominal injury, abdominal bleeding; it allows to improve the patient’s state of health considerably, to reduce the time of surgery, and to decrease the risk of post-surgical complications and mortality. In some cases donor blood transfusion may be avoided, which allows to prevent transfusion complications and possible infection with the diseases transmitted through blood transfusion.
We plan to continue the development of the treatment and diagnosing algorithm and practical implementation of our methods of laparoscopic surgeries for the patients suffering from polytrauma with the prevailing abdominal and thorax injuries.
References:
1. M.M. Abakumov. Abdominal injuries in case of polytrauma., M.M. Abakumov, N.V. Lebedev, V.I. Malyarchuk. - Moscow., Medicine, 2005. - 178 p.
2. Video laparoscopy in diagnosing and treatment of patients with closed abdominal injury., A.A. Gulyayev, G.V. Pakhomova,
P.A. Yartsev, V.T. Samsonov, M.V. Radygina., Collection of abstracts "9th Moscow International Congress of Endoscopic Surgery". - Moscow, April 6-8, 2005., pp. 104-106.
3. A.V. Kapshitar. Specifi cs of diagnostic laparoscopic interventions in patients with closed intestinal injury., A.V. Kapshitar., Clinical surgery. - 2012. - No. 10., pp. 57-59.
4. I.A. Miziyev, Z.M. Baziyev, A.B. Tutukov, V.M. Dygov. Experience of thoracoscopic surgeries in Kabardino-Balkaria., The 2nd congress of surgeons of the Southern Federal District: materials of the congress. - Pyatigorsk, 2009. pp. 179-180.
5. A.D. Timoshin, A.L. Shestakov, A.V. Yurasov. Minimally invasive interventions in the abdominal surgery. - Moscow., Triada-X, 2003. - 216 p.
6. Methods for improving treatment results for the patients with multisystem and concomitant injuries., V.N. Chernov, A.A. Pushkov, I.I. Taranov, V.T. Yuskov., Medical aid delivery in case of concomitant injury: Collection of research works. Vol. 108. - Moscow., 2007., pp. 67-71.
7. Yu.L. Shevchenko. Sparing surgery. - Moscow., Geotar-Media, 2005. 320 p.
Tab. 3. Effi ciency of laparoscopyic surgeries compared to traditional surgeries
Group of patients Number of patients Average number of bed-days
Post-surgical complications
Mortality rate
Patients who underwent laparoscopic surgeries
162 5.64±0.4 15(9%) 5(3%)
Patients who underwent laparotomy 50 8.25±0.39 16(32%) 4(8%)
p<0.05
Tab. 2. Post-surgical complications of patients who underwent laparoscopic surgeries and laparotomy in the control group
Types of complications Patients who underwent laparoscopic surgeries
n=162
Patients who underwent laparotomy n=50
Bile leak 3 2Pneumonia 5 6Eventration - 2Post-operative wound infection - 5Trocar wound infection 4Cystitis 3 1Total 15 16
p>0.05

26
8. V.G. Stenko. Treatment of patients with the heavy concomitant injury., V.G. Stenko., First Medical Aid. - 2004., Vol. 5., No. 3., pp. 195-196.
9. Assessment of nonoperative management of blunt spleen and liver
trauma., P.S. Om el al., Am. Surg. – 2005., Vol. 71., pp. 379-386.
Information about authors:
1. Andrii Plotnikov – Surgeon, Odessa National Medical University;
address: Ukraine, Odessa city, e-mail: [email protected]
2. Yuri Grubnik – Head of a Chair, Doctor of Medicine, Full Professor, Odessa National Medical University; address: Ukraine, Odessa city, e-mail: [email protected]
www: http://iashe.eu e-mail: [email protected] phone: +44 (20) 71939499
Issues of the IASHE are distributed across Europe and America, widely presented in catalogues of biggest scientific and public libraries of the United Kingdom.
Scientific digests of the GISAP project are available for acquaintance and purchase via such world famous book-trading resources as amazon.com and bookdepository.co.uk.
Activity of the Academy is concentrated on promoting of the scientific creativity and increasing the significance of the global science through consolidation of the international scientific society, implementation of massive innovational scientific-educational projects
While carrying out its core activities the Academy also implements effective programs in other areas of social life, directly related to the dynamics of development of civilized international scientific and educational processes in Europe and in global community.
International Academy of Science and Higher Education (IASHE, London, UK) is a scientific and educational organization that combines sectoral public activities with the implementation of commercial programs designed to promote the development of science and education as well as to create and implement innovations in various spheres of public life.
HIGHER EDUCATION
INTERNATIONAL and OF SCIENCE

27
Nowadays the study of the causes of infertility and ways to overcome
it is an important and urgent problem of modern biomedical science. Most researchers indicate that in the structure of infertile marriages male factor constitutes 20%, the cause of infertility cannot be detected in 15% of these families, and 25% of infertility index are caused by reproductive disorders in men and women [1, 4, 9].
Reduced spermatogenic and hormone-producing function of the testes can result from acute and chronic disorders of blood circulation (both local and systemic), endogenous intoxication, which occurs in many pathological conditions, and exposure to physical and chemical factors [2, 4, 8]. In recent years, environmental technological burden increases. As a result, the number of chemical substances and their metabolites, which have a negative infl uence on organs and body systems, including testicles, increase as well. Technogenic pollution with heavy metals and their derivatives is especially dangerous [2, 6, 8]. It should be noted that peculiarities of structural changes in testes under the infl uence of heavy metals are not suffi ciently studied.
The aim is to study the morphological changes in testes under the infl uence of cadmium chloride.
Materials and Methods
Testicles of 20 mature white male rats were studied morphologically. Rats were divided into 2 groups. The fi rst group included 9 healthy intact animals; the second group included 11 male rats that received cadmium chloride
subcutaneously at a dose of 6 mg/kg for 4 weeks [6].
Euthanasia of animals was performed one month after the beginning of experiment via exsanguination under thiopental anaesthesia. Pieces of the testes were fi xed in 10% neutral formalin solution and, after corresponding processing in ethyl alcohol of increasing concentrations, placed in wax. Microtome sections 5-7 microns thick were stained with hematoxylin-eosin, toluidine blue, by van Gieson, Mallory, and Veyhert [7]. Histological specimens were examined with the help of microscopes MBS-15 and Lyumam-P8.
Results and discussion
No deviations of the histological structure of testes were detected in animal specimens of the control group. In the
intact testes, spermatogenic epithelium cells, which are at different stages of development and are arranged in several concentric layers, adjoin to the proper tunic of convoluted seminiferous tubules. Between the convoluted seminiferous tubules interstitial connective tissue is localized. In the testicular stroma there are small groups of Leydig cells, which are characterized by homogeneous cytoplasm and a nucleus located eccentrically, along the blood vessels of small calibre. The nuclei of these cells are mostly irregular in shape.
Histological examination of macro-preparations of the testes of experimental animals that received cadmium chloride revealed signifi cant structural changes. In these experimental conditions, there was a slight reduction in the size of convoluted seminiferous tubules as compared to control animals.
Fig. 1. Stromal edema, partial reduction of layers and spermatogenic epithelium cells damage and desquamation, thickening of the membrane of convoluted seminal tubules in testicles of white rats under the infl uence of cadmium chloride. Staining by hematoxylin-eosin. Magnifi cation: x 140.
U.D.C. [616.618 611.631-612.616 +] 612.273.2
MORPHOLOGICAL CHANGES IN THE TESTICLES UNDER EXPOSURE OF THE ORGANISM TO CADMIUM CHLORIDE
S. Konovalenko1, MD, Ph.D., Professor of the Department of Biomedical Sciences,M. Hnatjuk2, Doctor of Medicine, Professor of the Department of Operative Surgery and Topographic Anatomy
N. Haliyash3, MD, Ph.D., Associated Professor of the Department of Pediatrics No. 2Kyiv International University, Ukraine1
Ternopil State Medical University named after I.Y. Gorbachevsky, Ukraine2,3
The authors present the results of the study of morphological changes in the testes of white rats under the infl uence of cadmium chloride. The study has revealed that long-term exposure of the organism to cadmium chloride causes severe vascular disorders in the studied organs, reduction of layers, degenerative necrobiotic changes of spermatogenic epithelium, infi ltration, sclerosis and hyalinization of stroma.
Keywords: testicles, organism, disorders, white rats, cadmium chloride.
Conference participants
http://dx.doi.org/10.18007/gisap:msp.v0i13.1656

28
Microscopically it was found out that most convoluted seminiferous tubules are in a state of devastation and degeneration of spermatogenic epithelial cells. Also often areas of dystrophic and necrotic spermatogenic epithelium were observed (Fig. 1, 2).
In testicle samples of white male rats that received cadmium chloride, in the lumen of convoluted seminiferous tubules products that appear as a result of the disintegration and necrosis of spermatogenic epithelium were found. In the testes areas with convoluted seminiferous tubules, the lumen of which was fi lled with cellular
detritus, are detected microscopically. Some researchers consider that partial or complete obliteration of the seminiferous tubules leads to thickening of their proper tunics [3, 5].
In addition to the above described changes there was revealed the desquamation of spermatogenic epithelium in convoluted seminiferous tubules of experimental animals, which received cadmium chloride, and its dislocation into the lumen. Sometimes the cells of spermatogenic epithelium were placed on the basement membrane unevenly; in some seminiferous tubules cavities appeared in
between the cells. One, sometimes two layers of dystrophic spermatoblasts and spermatocytes were attached to the proper tunic of some tubules. Between the layers of myoid cells bundles of collagen fi bres were observed.
Among the spermatogenic epithelial cells of convoluted seminiferous tubules the marked reduction of spermatocytes and early spermatids is detected. The nuclei of these cells are hyperchromic, and their cytoplasm is swollen and vacuolated. Basement membrane in most observations has signs of sclerosis. Microscopically we have observed structural changes in the interstitium of the testicles in the modelled pathology. Spaces between the convoluted seminal tubes are expanded as a result of edema and proliferation of connective tissue elements. These spaces are of different shapes and sizes, often with polymorphonuclear cell infi ltration. In interstitium the connective tissue is replaced by rough fi brous, hyalinized and scleroid structures. These effects lead to deformation of vessels and convoluted seminiferous tubules. Isolated Sertoli cells were located at the proper tunic of convoluted seminiferous tubules of the testicles.
The nuclei of Sertoli cells, which are located mostly near the basement membrane of convoluted seminiferous tubules, are deformed. The cytoplasm of these cells in the majority of observations is granular and with signs of active phagocytosis.
The cytoplasm of Leydig cells is granular and often vacuolated; their nuclei are hypochromic. In marked proliferation of connective tissue Leydig cells lose their orientation, in some of them marked nuclei lysis is detected.
In the simulated experimental conditions we have observed thickening of the proper tunic of convoluted seminiferous tubules. The basement membrane of convoluted seminiferous tubules proper tunic is wavily deformed, and unevenly expanded. It should be noted that the most common cause of thickening of convoluted seminal tubules proper tunic was the proliferation of connective tissue elements, sclerosis and hyalinization.
In the modelled pathology, arteries and veins of the testes underwent restructuring as well (Fig. 2, 3). The walls of the arteries are thickened, their lumen is narrowed;
Fig. 2. Structural changes in the vascular wall, perivascular swelling, degeneration, edema, desquamation of spermatogenic epithelial cells in the convoluted seminal
tubules of testicles of experimental animals under the infl uence of cadmium chloride. Staining by hematoxylin-eosin. Magnifi cation: x 140.
Fig. 3. Venous congestion, destructive processes in venous wall, desquamation of spermatogenic epithelium in the convoluted seminiferous tubules. Staining
by hematoxylin-eosin. Magnifi cation: x 140.

29
some endotheliocytes have got dystrophic and necrobiotic changes and signs of desquamation. Within this experiment we have observed plethora, stasis of blood and stagnation in venules and veins of the testicles. The contours of the venous walls are indistinct and thickened. There are alternating zones of edema and sclerosis with the wiggly and crooked contours; lumen of the veins is deformed. Endotheliocytes of the venous vessels are increased in size with signs of edema, dystrophy, and necrobiosis. There were islands of endothelial cells desquamation, pycnosis and lysis of their nuclei. It is known that chemicals circulating in the blood can damage endotheliocytes, which was revealed at histological examination of the testicle micro-preparations of animals exposed to cadmium chloride. It is considered that the endothelium that covers the inner surface of blood vessels is an important autocrine, paracrine and endocrine organ with numerous regulatory functions. It is known that normally functioning endotheliocytes produce nitric oxide (NO), which regulates vascular tone, affects the vascular wall remodelling processes, determines the system of antioxidant defence and peroxidation aggression, inhibits platelet aggregation and macrophages adhesion, and proliferation processes in the vascular wall. Damage of a signifi cant number of endothelial cells in the investigated arteries can lead to endothelial dysfunction, which plays a leading role in vascular remodelling and morphogenesis of the studied pathology [4, 9]. In the perivenous spaces there are marked swelling and sclerosis of perivascular tissues. The detected changes point to the disorders of the testicular venous drainage system, which were complicated by venous plethora, hypoxia, dystrophic and necrobiotic changes of cells and tissues, infi ltration and sclerosis. So, the prolonged exposure of studied animals to cadmium chloride causes severe structural reorganization of arterial and venous beds, parenchyma and stroma in testicles, thus signifi cantly impairing their spermatogenic and endocrine functions [4, 10].
Conclusions
Thus, in the course of the study it was found out that long-term administration of cadmium chloride to white male rats leads to signifi cant structural
reorganization in parenchyma and stroma of testicles, which is characterized by severe cardiovascular disorders, reduction of layers, degenerative and necrobiotic changes of spermatogenic epithelium and endotheliocytes, stromal infi ltration, sclerosis and hyalinization in the investigated organ.
References:1. Antonechko F.F. The role of
varicocele and its surgical treatment in violation of reproductive function., F.F. Antonechko, D.A. Scherbovskaya, S.A. Lelchuk., Reproductive health of children and adolescents. – 2009., No. 3., pp. 77-84.
2. Voloshin I.M. Assessment of the impact of heavy metals on human health., I.M. Voloshin., Modern ecological environment and human environmental pathology. – Lviv., B.І., 2007., pp. 10-12.
3. Hlodan O.J. Morphofunctional changes in the testis in terms of clamping blood vessels of the spermatic cord., O.J. Hlodan., Galician Drug Herald. – 2008., Vol. 15, No. 1. pp. 12-14.
4. Hrytsulyak B.V. The structure of the testes in acute ischemia., B.V. Hrytsulyak., Scientifi c Bulletin of the Uzhgorod University. The series "Medicine". – 2000., Issue 12., pp. 27-38.
5. Hrytsulyak B.V. Cytological changes in the test is under conditions of blockade of blood outfl ow in experiment., B.V. Hrytsulyak, V.B. Hrytsulyak, O.J. Hlodan., Bulletin Carpathian National University by V. Stefanik. Series Biology. – 2011., Issue XV., pp. 201-204.
6. Pryshlyak A.M. Atrial cardiomyocytes secretory activity in experimental animals with different
resistance to hypoxia in conditions of cadmium intoxication., A.M. Pryshlyak, M.S. Gnatyuk., Bulletin of scientifi c research. – 2006., No.3., pp. 62-64.
7. Sorochinnikov A.G. Histolo-gical and microscopic appliances., A.G. Sorochinnikov, A.E. Dorosevich. – Moscow., Medicine, 1997. – 448 p.
8. Trachtenberg I.M. Heavy metals as chemical pollutants of industrial and surrounding environment., I.M. Trachtenberg., Environment and Health. – 2005., No. 2., pp. 48-51.
9. Bong G.W. The adolescent varicocele: to treat or not to treat., G.W. Bong, H.P. Koo., Urol. Clin. North. Am. – 2004., No. 31 (3)., pp. 509–515.
https://doi.org/10.1016/j.ucl.2004.04.012
10. Jarow J.P. Induction of spermatogenesis in azoospermic men after varicocele repair., J.P. Jarow., J. Urol. – 2003. – 170 (2 Pt 1)., pp. 676–678.
Information about authors:1. Serhiy Konovalenko – MD, Ph.D.
in Medicine, Professor of the Department of Biomedical Sciences, Kyiv International University, address: Ukraine, Kyiv city, e-mail: [email protected]
2. Mykhailo Hnatjuk – Doctor of Medicine, Professor of the Department of Operative Surgery and Topographic Anatomy, Ternopil State Medical University named after I.Y. Gorbachevsky; address: Ukraine, Ternopil city, e-mail: [email protected]
3. Nataliya Haliyash – MD, Ph.D. in Medicine, Associated Professor of the Department of Pediatrics No. 2, Ternopil State Medical University named after I.Y. Gorbachevsky, address: Ukraine, Ternopil city, e-mail: [email protected]

30
Introduction
It is known that infl ammations of the skin are accompanied by bacterial contamination and therefore require the use of prolonged antimicrobial action. This effect can be achieved by using external antimicrobial agents in the form of ointments, creams and gels. [1] In present among the large number of drugs proposed for treatment of acne the dosage form of surface action based on azelaic acid and benzoyl peroxide is stipulated. Azelaic acid (HOOC(CH2)7COOH) – the active pharmaceutical ingredient (API) of a famous cream called Skinoren® 20% (Schering) is the antibiotic drug, which is produced by the yeast Pityrosporum acne. It inhibits the growth of propionic bacteria and the formation of fatty acids contributing to the occurrence of acne. In turn the API of a drug called Ugresol 10% (Pharmascience Inc., Canada), benzoyl peroxide (C6H5C(O)OO(O)C6H5) effectively regulates the processes of keratinization in the sebaceous follicles, improves oxygenation of tissues, reduces the level of free fatty acids in the lipid tissues, and has antimicrobial effect, especially with regard to Propionibacterium acne and Staphylococcus epidermidis [2-10].
The research clarifi es the applicability of diperoxyazelaic acid as an active pharmaceutical ingredient in preparations of surface action regarding acne, which, unlike benzoyl peroxide, is not capable of radical decomposition, and therefore will not have the ability to enhance carcinogenesis by UV radiation.
The aim of the study was to conduct the comparative study of antimicrobial activity of the ointment on the basis
of our proposed new substance – diperoxyazelaic acid (hereinafter both DPAA) (Fig. 1) and two European branded drugs – AkneStop 20% (Corporation "Arterium", Kyiv) and Ugresol Lotion 10% (Brij 30, disodium EDTA, carbomer 940) (Pharmascience Inc., Canada).
Polyethylene oxide (PEO) was chosen as the basis for ointments of diperoxyazelaic acid. This is the most common excipient of all known water-soluble bases on Pharmacopoeias of the most part of the world. The advantages of PEO: satisfactory water solubility, the ability to dissolve the hydrophilic and hydrophobic drugs, well mixed with wax and glycerides to form stable pseudo-emulsion well applied to the skin, does not prevent gas exchange and does not affect the activity of glands, weak bactericidal effect due to the presence of primary osmotically active hydroxyl groups. All PEO base are neutral, non-toxic, physiologically neutral, suitable for long-term use, not damaging the skin, easy to release drugs, not being the environment for the development of microfl ora. Being actively mixed with other substances, these bases can be used for all soluble and most of water-insoluble drugs.
Mechanism of action of peroxyacids is the following. Compounds with active oxygen used in the composition of disinfectants and antimicrobial agents, represent hydrogen peroxide, perborate, persulfate, percarbonate etc., as well
as peracids, and hydrogen peroxide oxidation obtaining carboxylic acids. They can be seen as a replacement product or just the two hydrogen atoms in a molecule of hydrogen peroxide to acyl groups.
Compounds with active oxygen belong to the group of disinfectant oxidants. Under the infl uence of the Lane oxide group there goes oxide inactivation of lipids and proteins, essential elements of microorganisms, bacterial cytoplasmic membrane and membranes of the spore forms of bacteria. Lipid peroxidation, most pronounced on unsaturated fatty acids, leads to a decrease of hydrophobicity and increase of membrane permeability. And membrane proteins are changing through the formation of protein-lipid complexes, oxidation and denaturation of proteins containing -SH group and the possible formation of cross-links in amino (NH2). Inhibition of redox enzymes leads to respiratory failure of microbial cells. Study of oxygen-containing drugs on the cells of bacteria and spores of bacillus showed that all tested microorganisms lose protein up to 90%; DNA – up to 30-50%, the RNA – up to 30%, and spore forms also lose 25% of dipicolinic acid. Equally signifi cant washout of intracellular components demonstrates the rapid violation of integrity of bacterial cells and spores [11-12].
Materials and methods
Diperoxyazelaic acid was synthesized by a known method of Swern [13] according to the scheme (in the present sulphuric acid): Fig. 1. Structure of diperoxyazelaic acid
O O
OOHHOO
COMPARATIVE STUDY OF THE ANTIBACTERIAL ACTIVITY OF OINTMENT BASED ON DIPEROXYAZELAIC AND UGRESOL 10% AND ACNE STOP 20% PREPARATIONS
O. Prysiazhniuk, StudentM. Blazheyevskiy, Doctor of Chemistry, Full Professor
National University of Pharmacy, Ukraine
The diperoxyazelaic acid was synthesised. Ointment on the polyethylenoxide basis containing 1% diperoxyazelaic acid was obtained. The antimicrobial activity of the ointment and branded drugs Acne Stop and Ugresol have been explored in the comparative perspective. The shelf life of creams was clarifi ed. The conclusion was made about the prospects for further in-depth research on the issue of its application as the extemporal dosage form.
Keywords: acne, benzoyl peroxide, azelaic acid, diperoxyazelaic acid, antibacterial preparations.
Conference participants,National championship in scientifi c analytics,
Open European and Asian research analytics championship
http://dx.doi.org/10.18007/gisap:msp.v0i13.1657

31
НО(О)С(СН2)7С(О)ОН+Н2О2 = НОО(О)С(СН2)7С(О)ООН + H2O.
Diperoxyazelaic acid (nonanebis (peroxoic acid), T mp. + 90-90,5ºC (with decomp.), the content of active oxygen species (AOC) 14,2%; рКа1=8,08, рКа2=9,19.
To confi rm the stability of DPAA, one sample was kept in a self-sealing bag at room temperature (30-35 °C). The active oxygen content of the sample was determined by iodometric titration after every 10-15 days. It was found that it retains its active oxygen content over a period of 50 days (14.2-14.1%). There were no changes observed in the physical appearance, too. This confi rms the stability of DPAA at room temperature.
An ointment composition: 0.8-1.2 wt. % DPAA; Poly(ethylene oxide), MW 400 (PEO 400) (Specif. 2483 007 71150986 2006), 78,0-79,4 wt.%, Poly(ethylene oxide), MW 1500 (PEO-1500) (Specif. 2483-008-71150986-2006), 20,19-19,38 wt.%; disodium EDTA (0,1-0,02 wt.%). The content of DPAA ointment is determined experimentally. Reduction of its content in the composition of the drug leads to a marked reduction of antimicrobial activity. The composition of water-soluble hydrophilic ointment base with the specifi ed content PEO 400, PEO-1500, disodium EDTA was also chosen experimentally. Due to optimal components this framework is the most appropriate, since it promotes optimal release of active substances, chemically indifferent with respect to the drug and is convenient in terms of technology of ointments production.
The study of antimicrobial activity of the objects carried by agar diffusion was based on the ability of active substances to diffuse in the culture medium of the previously inoculated microorganisms. According to WHO recommendations we used the following museum strains for assessment of antibacterial and antifungal activity of drugs as the test cultures: gram-negative bacillus Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, Gram-positive cocci Staphylococcus aureus ATCC 25923 and spore-forming bacillus Bacillus subtilis ATCC 6633, yeast fungi Candida albicans ATCC 653/885, and clinical isolates: Candida tropicalis, Candida krusei,
Candida glabrata. In the experiment we used daily suspension of microorganisms in saline. Microbial load was 1 · 107 colony forming units in 1 ml of the nutrient medium [14,15].
Antimicrobial activity of 1% ointment DPAA was studied in 1 day 2 weeks and 1 month after preparation. The results determine the antimicrobial activity of 1% ointment DPAA. Comparison of preparations is presented in Table 1. It shows that 1% ointment DPAA manifests antimicrobial action with respect to C. albicans and C. tropicalis level comparator AkneStop 20%. While antibiotic ointment revealed the effect of DPAA against Gram-negative (E. coli, Ps. Aeruginosa) and gram-positive bacteria (St. aureus, B. subtilis) strongly exceeding the effect of other investigated drugs. As seen from the data in Table 1, ointment based of DPAA revealed high antimicrobial activity in relation to the St. aureus, E. coli,
Ps. aeruginosa and C. albicans, less pronounced – to B. subtilis, C. tropscalis, C. krusei and C. glabrata.
Consequently, studies have shown that the new DPAA ointments based on hydrophilic matrix reveal suffi ciently high antimicrobial activity (which is dominated by European brands), and therefore the further in-depth research promising.
Conclusions
The diperoxyazelaic acid was synthesised. Ointment on the polyethylenoxide basis containing 1% diperoxyazelaic acid was obtained. The antimicrobial effects of the ointment and branded drugs Acne Stop and Ugresol have been examined in comparative perspective. The shelf life of creams was clarifi ed, and the conclusion was made about the prospects for further in-depth study of the issue of its application as an extemporal dosage form.
Tab. 1. The results determine the antimicrobial activity
Testculture Zones of growth inhibition test cultures mm (n = 3)
Ointment based DPAA 1% After 1 month of storageStaphylococcus aureus 45,4±1,3
Escherichia coli 45,0±0,4Pseudomonas aeruginosa 38,8±2,6
Bacillus subtilis 22,7±2,8Candida tropscalis 23,7±1,4Candida albicans 31,3±3,7Candida krusei 21,5±1,5
Candida glabrata 14,8±1,7Aknestop 20%
Staphylococcus aureus 35,1±0,4Escherichia coli 21,3±0,7
Pseudomonas aeruginosa 29,0±1,2Bacillus subtilis 15,0±0,7
Candida tropscalis 22,3±0,3Candida albicans 27,1±1,1Candida krusei 22,4±0,6
Candida glabrata 9,0±0,5Ugresol 10%
Staphylococcus aureus 15,1±1,2Escherichia coli 12,8±1,3
Pseudomonas aeruginosa -Bacillus subtilis 16,1±1,2
Candida tropscalis 17,7±0,5Candida albicans 24,5±0,5Candida krusei -
Candida glabrata -
Note. “-” - A zone of stunted growth of microorganisms available.

32
References:
1. Drohovoz S.M, Shchokina K.G. Pharmacology in palms. Handbook for pharmacists, doctors and students of medical and pharmaceutical universities. - Kharkiv., 2009. - 110 p.
2. Fluhr J.W., Degitz K., J. Dtsth. Dermatol. Ges. – 2010., Vol. 8, Suppl. 1., pp. 24-30. https://doi.org/10.1111/j.1610-0387.2009.07169.x
3. Worret W.I., Fluhr J.W., J. Dtsth. Dermatol. Ges. – 2006., Vol. 4, No. 4., pp. 293-300. https://doi.org/10.1111/j.1610-0387.2006.05931.x
4. Harper J.C., J. Dtsth. Dermatol. Ges. – 2010., Vol. 9, No. 5., pp. 482-487.
5. Usenko G.D., Zupanets I.A., Bezdetko N.V. pharmacist. - 2002., No. 19., Access mode: http://www.provisor.com.ua/archive/2002/N19/art_17.php
6. Potekaev N.N., Andreeva L.V. A Journal of Dermatology and Venereology - 2001., No. 6., pp. 32-35.
7. T. Protsenko, A. Kaplan. Ukrainian Journal of Dermatology, Venereology, Сosmetology - 2007., No. 2 (25)., pp. 12-14.
8. Kolyadenko V.G., Usenko G.D. Weekly Pharmacy. - 1997., No. 27., pp. 42-43.
9. Stepanenko V.І. Klіnіchna іmunologіya, alergіya, іnsektologіya. - 2010., No. 1., pp. 86-96.
10. Usenko G.D. Practitioners Magazine - 1997., No. 2., pp. 11-14.
11. Paly H.K., Antiseptics in the prevention and treatment of infections., Authors; Ed. G.K. Paly. - Kyiv., Health. - 1997. - 201 p.
12. Krasilnikov A.P. Handbook on antiseptic. - App.: High society. HQ., 1995. - 367 p.
13. Winfred E., Witnauer L.P., Swern D., J. Am. Chem. Soc. - 1957.- Vol. 79, No. 8., pp. 1929-1931. https://doi.org/10.1021/ja01565a043
14. Guidelines "Studying the specifi c activity of antimicrobial drugs". - Kyiv., 2004. - 38 p.
15. A Guidance Ministry of Health in Ukraine "Determination of the sensitivity of microorganisms to antibiotics". - Kyiv., 2007, No. 167. MB 9.9.5 - 143-2007.
Information about authors:1. Oleksandr Prysiazhniuk - Student,
National University of Pharmacy; address: Ukraine, Kharkiv city; e-mail: [email protected]
2. Mykola Blazheyevskiy – Doctor of Chemistry, Full Professor, National University of Pharmacy; address: Ukraine, Kharkiv city; e-mail: [email protected]
http://platonick.com
Possibility of the informal communication with colleagues from various countries;
Demonstration and recognition of creative potential;
Promulgation and presentation of author's scientific works and artworks of various
formats for everyone interested to review.
International intellectual
portal «PlatoNick» is a
multilingual, open resource
intended to facilitate the organization
of multifaceted communication of
scientists and intellectuals, promulgate their
authoritative expert conclusions and
consultations. «Platonick» ensures
familiarization of wide international public
with works of representatives of
scientific and pedagogic
community. An innovation
news line will also be
presented on the
«Platonick»
portal.
International multilingual
social network
for scientists and
intellectuals.

33
Introduction
«Aqua-rinosol» is a medicine for treatment of dryness inside the nose (nasal passages). It helps add moisture inside the nose in order to dissolve and soften thick or crusty mucus. In babies and young children with blocked nostrils who cannot blow their noses, this product helps to make the mucus easier to remove with a nasal bulb syringe. This helps relieve stuffi ness and makes breathing easier. This product contains the purifi ed gentle salt solution (also called saline or sodium chloride solution) and Benzalkonium chloride (BAC) as the preservative (w=0,015 %). It is a mixture of a l k y l b e n z y l d i m e t h y l a m m o n i u m chlorides of various even numbered alkyl chain lengths (R=С8, С10, С12, С14, С18). This product is a nitrogenous cationic surface-acting agent belonging to the quaternary ammonium group, especially inhibitors of acetylcholinesterase.
Considering the widespread use in pharmaceutical formulation the determination of low concentration preservative constitutes a challenging problem in current pharmaceutical analysis and is a topic of global interest. The standard method for determination of BAC in pharmaceutical compositions is reversed-phase high performance liquid chromatography [1-6].
Experimental section
Instruments and apparatusAll the spectral absorbance
measurements were made using the “photoelectric concentration colorimeter (CPC-2) (Zagorsky Optical & Mechanical plant, Russia).
pH value was measured with the laboratory ionomer I–160M (Belarus) by using EGL 43-07 pH glass electrode together with the auxiliary chloride silver electrode of EAL-1m3.1 type, standard with potassium chloride.
Materials and reagents All chemicals and reagents used
were of analytical grade: Pharmacopoeial acetylcholine chloride medication – 0.2 g per amp/5 ml (manufactured by “VECTOR” – State Science Center of virology and biotechnology of the Russian Federation” (Russia); dry protein drug of cholinesterase from horse serum – 8 mg / L (IV class) 22AE / mg (SMU “Biomed”, Russia). N - phenetidine (4 - ethoxyaniline - 98%) (SIGMA - ALDRICH); Series: A0281408s, New Jersey, USA; “Stabilized Hydrogen Peroxide 30-40%” (LLC “Inter - Synthes”, Boryslav, Ukraine). The content of hydrogen peroxide was determined by SPU according to the monograph “High-test hydrogen peroxide solution 27.5-31.0%.
High purity double distilled water was used throughout.
Preparation of the standard stock solution
Standard stock solution was prepared in the double distilled water: 0.09910 g of standard solution of Benzalkonium chloride (50%) were added into the 500 ml volumetric fl ask, and it was diluted up to the mark x (ppm). 0.1 ml of this solution were added into a 10 ml volumetric fl ask and was diluted up to 10 ml. From the standard stock solution, a standard solution was prepared containing 2.12·10-5 mol/L. Alternatively, derived from the corresponding regression equation.
Preparation of the solution of Cholinesterase (ChE)
It was prepared in the double distilled water by adding 80mg of dry cholinesterase drug in volumetric fl ask, and it was shaken and diluted up to the mark. After that it was kept in the thermostate for 10 minutes at 38 ºC above Zero [7].
Phosphate buffer solution (pH 8.35) preparation
It was prepared by dissolving: 35.75 g of sodium hydrogen phosphate were added to 500 ml fl ask, then 300 ml of double-distilled water were added; the mixture was dissolved; Then 19 ml of 0.1 mol/L solution of hydrochloric acid were added, stirred and diluted with the double distilled water to 500.0 ml. The prepared pH solution is potentiometrically controlled.
U.D.C. 543.395: 543.23: 543.422.7
APPLICATION OF THE KINETIC ENZYMATIC METHOD FOR BENZALKONIUM CHLORIDE DETERMINATION IN AEROSOL PREPARATION
O. Koval’ska, AssistantM. Blazheyevskiy, Doctor of Chemistry, Full Professor
National University of Pharmacy, Ukraine
A new kinetic photometric method for BAC determination based on an inhibition of the enzymatic (cholinesterase) reaction was proposed. The reaction rate was detected at unhydrolised acetylcholine residue, which is determined by the amount of peracetic acid, producted during the impact of H2O2 on it. Indicator reaction is a reaction of peracetic acid with 4-ethoxyaniline interaction that leads to the formation of azoxyphenetole with λmax = 358 nm (lgε =4.18). The measurement velocity of changing of light absorption vs. time (∆А/∆t, min-1) give a chance to quantitatively determination of BAC. The results confi rmed that the method is linear at concentrations ranging from 1.0×10-6 mol/L to 5.0 ×10 -6 mol/L. Depending calibration equation ΔA/Δt, min-1 from the village BAC has the form: tgα = 5093 c + 0.0075 (r = 0,999). LOD was 0.4× 10-6 mol/L. The method was satisfactorily applied to the determination of BAC in nasal pharmaceutical preparation «Aqua-rinosol». The recovery was 99.9%, RSD = 2.7 % (n=5, P=0.95). This method is benefi cial because high sensitivity and selectivity can be achieved using relatively simple technical equipment.
Keywords: Benzalkonium chloride, kinetic photometric method, determination, aerosol preparation.
Conference participants,National championship in scientifi c analytics,
Open European and Asian research analytics championship
http://dx.doi.org/10.18007/gisap:msp.v0i13.1658

34
Hydrogen peroxide solution (10%). It was prepared by dilution of
the appropriate high-test hydrogen peroxide with double-distilled water. The exact hydrogen peroxide content in prepared 10% solution is determined permanganatometrically.
P-phenetidine hydrochloride solution preparation (1%).
N - phenetidine hydrochloride (Ph) was extracted from the base by hydrogen chloride precipitation in the chloroform solution. Dissolve 1.00g p-phenetidine hydrochloride in 80 ml of double-distilled water in 100 ml capacity measuring bottle and dilute it to volume.
Preparation of the enzyme substrate of the acetylcholine chloride solution (ACh).
The content of an ampoule of pharmacopoeia drug acetylcholine chloride (0.2 g) is dissolved in 200 ml of double-distilled water. For that, open an ampoule, add 4.0 ml of water with pipette, and shake until acetylcholine is completely dissolved. Then pour the acetylcholine solution into 200 ml capacity measuring bottle and dilute with the double-distilled water to the volume.
General recommended procedure.10.0 ml of 0.2 mol/L phosphate
buffer solution (pH=8.3) were transferred in 20 ml graduated test tube with ground plug consistently. The accurate volumes of test solution (BAC or “Aqua-rinosol”) over the concentration range of x mol/L were added into a standard fl ask.
After that, 2.0 ml of cholinesterase were added while stirring; a timer was switched on; each solution was thoroughly shaken up and thermostated for 15 min. Then 1.0 mL of 1% acetylcholine solution was added quickly; a timer was switched on; it was shaken thoroughly and thermostated for 10 min again. Then 2.0 ml of 10% hydrogen peroxide solution were added; kept for 10 min in the thermostat, and then 1.0 ml of 1% p-phenetidine solution (Ph) was added. The mix was diluted with the distilled water to volume of 20 ml. 5 ml drop of the solution was transferred to a 100 ml volumetric fl ask and made up to the mark with water. Suitable dilution was made to fi t the applicable concentration range and the above described procedures were followed.
The nominal concentration of the bottles was calculated either from calibration graph or using the regression equation.
Results and discussion
The proposed method for BAC detection is based on an enzymatic (cholinesterase) reaction. Mechanism of analytical reaction and sensitivity of this method are the same as (or similar to) those in the human body. The conventional enzymatic method is based on the ability of cholinesterase to accelerate hydrolytic
decomposition of the neurotransmitter (substrate) acetylcholine to choline and acetic acid. The reaction rate is detected at unhydrolised acetylcholine residue, which is determined by the amount of peracetic acid, produced during the impact of H2O2 on it. Indicator reaction is a reaction of peracetic acid with 4-ethoxyaniline interaction, which leads to the formation of azoxyphenetole with λmax=358 nm (lgε =4.18). The measurement velocity of changing of light absorption vs time (∆А/∆t, min-1) gives a chance to perform quantitative determination of BAC.
Fig. 1: Kinetic curves of couple oxidation of p-phenetidine by hydrogen peroxide in presence of the system: 1 – ACh+ChE, 2- 5 – ACh+(ChE+BAC), 6
– AСh. Initial concentrations: pH 8.3 (phosphate buffer), w(Ph) = 0.05% (w/v), c(H2O2) = 1.5· 10-2 mol /L, w(ACh) = 0.05% (w/v), c(ChE=2.2 AE/mL) t = 37 ±
0.1 °C, λ = 358 nm.
Fig. 2: Dependence of the relative reaction rate on BAC concentration. Initial concentrations: pH 8.3 (phosphate buffer),w(Ph) = 0.05% (w/v), c(H2O2)
= 1.5· 10-2 mol /L, w(ACh) = 0.05% (w/v), c(ChE=2.2 AE/mL) t = 37 ± 0.1 °C, λ = 358 nm.
00,05
0,10,15
0,20,25
0,30,35
0,40,45
0,5
0 5 10 15
A
t, min
1
6
01234567
0,01 0,015 0,02 0,025
100t
g ,
-1
c,10-4 mol/L
35
According to the optical-time relations, the kinetic curves are plotted and the slope of the fi rst 15 min is found (Fig. 1). According to the data received a slope - fi nite analyte concentration calibrated relation is obtained, c, μmol / L.
A calibration curve equation is solved by the least squares method (Linear regression): tgα=bс+a, where a, b are Y-axis intercept and slope, (tgα, min -1) respectively. Switch on timer and every other minute scan photometrically each solution for 15 min on photoelectric colorimeter CPC-2, use colour fi lter №2 and 1.0 cm cuvette (Fig. 2).
The results confi rmed that the method is linear at concentrations ranging from 1.0×10-6 mol/L to 5.0 × 10-6 mol/L. Depending on the calibration equation ΔA / Δt (tgα), min-1 the BAC has the form: tgα = = 5093c + 0.0075 (r = 0,999). LOD was 0.4×10-6 mol /L. The precision and accuracy of the proposed method was studied by performing the experiment fi ve times at three different concentration levels (low, medium and high) of BAC (table 1).
The method was satisfactorily applied to the determination of BAC in
nasal pharmaceutical preparation «Aqua-rinosol». The recovery was 99.9%, RSD = 2.7 % (n=5, P=0.95).
Conclusion
The proposed kinetic-spectrophotometric method for the determination of BAC in pharmaceutical samples of “Agua-rinosol” preparation described in this paper is simple, quick, inexpensive, and thus appropriate for routine quality control analysis of active drugs in the laboratories of hospitals, pharmaceutical companies and research institutions. It should also be suitable for the developing countries. The validation of the method shows that the results obtained are in good agreement with the standard Pharmacopoeial method.
References:
1. Hashem A.l. Aani., J. Appl. Pharm. Sci. – 2016., Vol. 6, No. 5., pp. 80-89.
2. Kostić D.E., J. Chem. – 2012., Vol. 9, No. 3., pp. 1599-1604.
3. Gubin M., Pivovarova S.,
Pharmacy. – 2012., Vol. 4., pp. 9-12.4. Kabeer AS, Ashish TP.,
J. Trace Anal. Food & Drugs. – 2013., Vol. 21, No. 1., pp. 14-21. https://doi.org/10.7726/jtafd.2013.1002
5. Hanni M.H. at all., Euras. J. Anal Chem. – 2015., Vol. 10, No. 1., pp. 46-67.
6. Metha J., Patidar K., Vyas N., E-Jornal Chem. – 2010., Vol. 7, No. 1., pp. 11-20. https://doi.org/10.1155/2010/312379
7. Blazheyevskiy M.Ye., Dyadchenko V.V., Pharm. J. - 2004., Vol. 2., pp. 52-58 (Ukrainian).
Information about authors:
1. Mykola Blazheyevskiy – Doctor of Chemistry, Full Professor, National University of Pharmacy; address: Ukraine, Kharkiv city; e-mail: [email protected]
2. Olena Koval’ska – Ph.D. of Pharmaceutics, Assistant, National University of Pharmacy; address: Ukraine, Kharkiv city; e-mail: [email protected]
Tab. 1.Accuracy and precision of the proposed method
No.BAC taken*,
mol /LBAC found,
X ±ΔX, mol /LN
RSD(Р=0.95) (X -μ)·100% /μ
1. 1.065· 10-6 (1.059±0.015)·10-6 5 2.52% 0.56%2. 3.195· 10-6 (3.179±0.05)·10-6 5 1.49% 0.50%3. 4.26· 10-6 (4.244±0.03)·10-6 5 0.63% 0.42%
*calculated according to the certifi cate.
36
DOCTORAL DYNAMIC SCIENTIFIC AND ANALYTICAL PROGRAMS
SCIENTIFIC AND ANALYTICAL PROGRAM OF THE EDUCATIONAL AND PROFESSIONAL QUALIFICATION IMPROVEMENT
INTERNATIONAL ATTESTATION-BASED LEGALIZATION OF QUALIFICATIONS
DOCTORAL DISSERTATIONAL SCIENTIFIC AND ANALYTICAL PROGRAMS
ACADEMIC SCIENTIFIC AND ANALYTICAL PROGRAMS
BIBLIOGRAPHIC SCIENTIFIC-ANALYTICAL ACADEMIC PROGRAMS
BIBLIOGRAPHIC SCIENTIFIC-ANALYTICAL DOCTORAL PROGRAMS
AUTHORITATIVE PROGRAMS
http://university.iashe.eu e-mail: [email protected] Phone: + 44 (20) 71939499
OF SCIENTIFIC AND INNOVATIVE ANALYTICS OF THE IASHE
INTERNATIONALINTERNATIONALUNIVERSITYUNIVERSITY

CURRENTS ISSUES IN DEVELOPMENT OF METHODS OF PREVENTION AND
TREATMENT OF DISEASES OF HUMAN BEINGS, ANIMALS AND PLANTS:
TRADITIONS AND EXPERIMENTAL TRENDS
02-08.11Medicine, Pharmaceutics / Biology, Veterinary Medicine and Agricultural sciences
3 stage
INNOVATIVE APPROACHES TO OVERCOMING THE GAPS IN OUR
KNOWLEDGE ABOUT PHYSICAL AND CHEMICAL PROPERTIES OF MATTER, AS
WELL AS CONDITIONS OF THEIR MEASUREMENT
02-08.11Physics, Mathematics and
Chemistry / Earth and Space
Sciences
3FACTORS OF FUNCTIONALITY, SAFETY, EFFICIENCY AND AESTHETIC VALUE IN
MANUFACTURING TECHNICAL DEVICES AND ERECTING BUILDINGS: STANDARDS
AND INNOVATIONS
02-08.11Technical Science, Architecture and Construction
3 stagestage
CURRENT RESEARCH ON MATERIAL OBJECTS AND INTERACTION OF
SUBSTANCES: EXPANDING THE LIMITS OF KNOWLEDGE AND DETERMINING THE
FUTURE OF MANKIND
03-09.08
Physics, Mathematics and Chemistry / Earth and Space Sciences
2 stage
CURRENT PROBLEMS IN THE PROCESS OF MEETING THE EXPANDING DEMAND OF
THE POPULATION FOR THE MODERN HIGH TECH PRODUCTS
03-09.08Technical Science, Architecture and Construction
2PROBLEMS OF INTERPERSONAL
RELATIONS IN CONDITIONS OF MODERN REQUIREMENTS TO QUALITY OF EDUCATION AND THE LEVEL OF
PROFESSIONAL SKILLS OF EXPERTS
14-19.09Educational sciences and Psychology
3 stagestage
CREATIVITY AS A PERSONAL SELF-EXPRESSION MECHANISM AND A
WAY TO REVEAL THE LEVEL OF SOCIOCULTURAL DEVELOPMENT
08-13.06Culturology, Physical cultureand Sports, Art History / History and Philosophy
2 stage
CHRONIC AND INFECTIOUS HUMAN DISEASES, EPIZOOTIC OUTBREAKS AND
EPIPHYTOTY AS THE RESULTS OF CHANGES IN CONDITIONS OF
BIOLOGICAL LIFE AND THE MAJOR DIRECTIONS OF SCIENTIFIC RESEARCH
04-10.07Medicine, Pharmaceutics / Biology, Veterinary Medicine and Agricultural sciences
2 stage
CORRELATION BETWEEN INDIVIDUAL AND COLLECTIVE NEEDS IN THE CONTEXT
OF IMPROVING THE EFFECTIVENESS OF SOCIAL PROCESSES
20-26.06Economics, Jurisprudence and Management / Sociology, Political and Military Sciences
2 stage
RATIO BETWEEN THE ROLES OF AN INDICATOR OF SOCIAL CULTURE,
INSTRUMENT OF COMMUNICATION, AND MECHANISM OF PRESERVATION AND
TRANSFER OF INFORMATION IN MODERN LANGUAGE SYSTEMS
10-16.10Philology
3 stage
ORGANIC COMBINATION OF SOCIAL PARTNERSHIP AND INDIVIDUAL IDENTITY AS THE MAIN FACTOR IN ENSURING THE
SELF-PRESERVATION AND DEVELOPMENT OF THE SOCIETY
24-31.10Economics, Jurisprudence and Management / Sociology, Political and Military Sciences
3 stage
PHENOMENON OF MASS CULTURE AGAINST THE BACKGROUND OF
EXPANSION OF LIBERAL PREREQUISITES FOR DEVELOPMENT OF PERSONAL
SELF-EXPRESSION FORMS
10-16.10Culturology, Physical culture and Sports, Art History / History and Philosophy
3 stage
GISAP CHAMPIONSHIP AND CONFERENCES 2017
Website: http://gisap.eu/ Email: [email protected]
