expert differential diagnosis · •epidural mass •cpa mass • ... epidural hematoma ... •can...
TRANSCRIPT

EXPERT DIFFERENTIAL DIAGNOSIS:
Extra-axial Spaces and Subarachnoid Cisterns
Anne G. Osborn, M.D.

EXTRA-AXIAL SPACES
• Anatomically-based ExpDDxs:• Epidural mass• CPA mass• Prepontine cistern mass• Foramen magnum mass
• Generic imaging patterns• Sulcal-cisternal enhancement• Enhancing cranial nerves
• Modality-specific ExpDDxs:• FLAIR hyperintense CSF

EPIDURAL MASS
• Common• Epidural hematoma
• Meningioma
• Skull/dural mets
• Less common• Lymphoma/leukemia
• Neurosarcoid
• Epidural empyema
• Rare but important• Tuberculoma
• Plasmacytoma
• Meningioma, Atypical/Malignant
• Hemangiopericytoma
• Extramedullary hematopoiesis
• Gliosarcoma
• Histiocytoses

EPIDURAL HEMATOMA
• Fx in 85-95%
• “Swirl sign”• Unclotted blood
• Rapid accumulation
• Arterial EDH 90%• Most adjacent to fx,
laceration of MMA
• Venous 10%• Lacerated dural
venous sinus
• Slower, more insidious
“swirl sign” crosses dura

VENOUS EDH

MENINGIOMA
• “Typical” meningioma• WHO I
• Clues to diagnosis:• Hyperdense +/- Ca++• Vascular “pedicle”• +/- hyperostosis• Isointense to GM• CSF-vascular “cleft”• Intense enhancement• Dural “tail”
• All have mimics• Metastases (esp. breast)

MENINGIOMA:Pathology/Imaging Correlation

DURAL METASTASES
• Look for skull, scalp lesions
• Often multiple
• Use T1C+FS for subtle lesions
• Can mimic meningioma!

MULTIPLE BREAST METS

SKULL/DURAL METASTASES
• Bone + dural invasion often present
• Mode of tumor spread varies with histologic type• Most common = direct spread from calvarium
to dura• Adults = Lung, breast, prostate
• Children = neuroblastoma, Ewing, hemopoietic
• Less common = hematogenous spread to dura• Lymphangitic, intravascular pulmonary tumor
• Rare• Extension from dural metastasis to brain parenchyma
• Brain parenchyma spread into dura

SKULL/DURAL METASTASES:Pathology

SKULL/DURAL METASTASES:CT
• Lytic/destructive
• Use wide windows!
• Usually enhance
• Subgaleal, dural involvement common

SKULL/DURAL METASTASES:MR
• Marrow fat replaced
• +/- Cortical destruction
• +/- Adjacent dura often thickened, enhancing
• Can be solitary or multifocal
• Often extensive, diffuse, both sub- and epidural

SKULL + DURAL METASTASES:MR

SKULL/DURAL METASTASES:CT
Leukemia

SKULL/DURAL METASTASES:MR
Neuroblastoma and “Hair on End” Pattern

DIFFUSE DURAL METASTASES:Pathology

LESS COMMON/RARE BUT IMPORTANT EPIDURAL MASSES
Lymphoma,
leukemia
Tuberculoma
Extramedullary
hematopoiesis
Plasmacytoma

CPA MASS, ADULT
• Common• Vestibular schwannoma
• Less common• Meningioma
• Epidermoid cyst
• Aneurysm
• Arachnoid cyst
• Metastasis
• Rare but important• NF2
• Sarcoidosis
• Rare (contd)• Choroid plexus papilloma
• Lipoma
• Ependymoma
• Pseudotumor
• Schwannoma, facial n.
• Schwannoma, JF
• Hemangioma
• Neurenteric cyst

CPA MASS, ADULT
• “Big kahuna” = vestibular schwannoma• 90% of all CPA-IAC masses
• Classic “ice cream on cone”
• “Small chiefs”• Meningioma, epidermoid, aneurysm, arachnoid cyst
• Together = approximately 8%
• Everything else• 10 rare dxs together = 2%

CPA MASS, ADULT:Imaging Protocols
• T1C+ FS MR = gold standard
• T2 FS thin-section/hi res CISS if VS suspected
• Helpful additions• FS for VS vs. lipoma
• FLAIR + DWI for epidermoid vs. arachnoid cyst
• GRE/SWI for aneurysm, blood, Ca++

VESTIBULAR SCHWANNOMA

ENHANCING CPA MASS:Helpful Clues in DDx
Meningioma
(mushroom
cap, dural tail)
Facial n. schwannoma
(geniculate ganglion)
Hemangioma
(speckled)
Metastasis
(flocculus, not
nerve)

CYSTIC CPA MASS
Arachnoid cyst
(smooth,
suppresses,
doesn’t restrict)
Epidermoid cyst
(cauliflower,
restricts, doesn’t
suppress)
Neurenteric cyst
(not like CSF)Cystic VS (extends
into IAC)

SULCAL-CISTERNAL ENHANCEMENT
• Common• Meningitis• Meningeal
carcinomatosis• Lymphoma
• Less common• Neurosarcoid• Sturge-Weber• Fungal disease• Subacute aSAH• Opportunistic
infections
• Rare but important• Leukemia• Neurocutaneous
melanosis
• Contrast

PIA-SUBARACHNOID SPACE VS.DURA-ARACHNOID
ENHANCEMENT

MENINGITIS (INFECTIOUS)
• Clinical-lab dx• Why image?
• Can be – when LP +• FLAIR may be + early• Look for complications• Agents (bacterial, TB, viral, etc)
look same
• Intense enhancement• Pia, subarachnoid space > > dura-
arachnoid pattern
• Caution: Infectious meningitis, carcinomatous may look identical!

CARCINOMATOUS MENINGITIS:Leptomeningeal Dissemination of GBM
Pathology Imaging

NCC MENINGITIS + RACEMOSE CYSTS

LESS COMMON/RARE BUT IMPORTANT
Neuroarcoid SWS
Fungal
meningitisNeurocutaneous
melanosis

ENHANCING CRANIAL NERVES
• Common• Metastases
• NF2
• NF1
• MS
• Less common• Neuritis (viral, post-
viral)
• Lyme disease
• Lymphoma
• Sarcoid
• Opportunistic infection (HIV/AIDS)
• Rare but important• Leukemia
• Ischemia (diabetes, ASVD)
• LCH
• CIDP

ENHANCING CRANIAL NERVE(S):Key Considerations
• Enhancement of cisternal, cavernous sinus CN segments always abnormal
• Solitary or multiple CNs involved?
• Which CN(s) affected?• Optic nerve: MS, NF1, viral/post-viral
• CN3, 6: Ischemia (diabetes, microvascular disease)
• CN7: Bell palsy, Herpes zoster (Ramsay Hunt), schwannoma
• CN8: Schwannoma (sporadic, NF2), metastasis

MULTIPLE ENHANCING CRANIAL NERVES
• Common• Metastases• NF2
• Less common• Viral, post-viral neuritis• Lyme disease• Lymphoma• NF1• Leukemia
• Rare but important• MS• CIDP

MULTIPLE ENHANCING CRANIAL NERVES
Metastases NF-2
Lyme disease CIDP

SOLITARY ENHANCING CRANIAL NERVE
• Common• Metastasis
• Schwannoma (VS)
• MS
• NF1 (plexiform nf, optic glioma)
• Less common• Viral, post-viral (Bell, Herpes, ADEM)
• Ischemia (diabetes, ASVD)

SOLITARY CN ENHANCEMENT
NF1,
plexiform nf
MS
Metastasis Herpes zoster

FLAIR HYPERINTENSE CSF
• Common• Subarachnoid hemorrhage
• Meningitis
• MR artifact
• Metastases (carcinomatous meningitis)
• Less common• Gadolinium in CSF
• BBB leakage
• Renal failure
• Acute cerebral infarct
• Rare but important• Dermoid cyst (ruptured)
• Moyamoya (“ivy sign”)

SUBARACHNOID HEMORRHAGE
• Trauma > aneurysm
• Other etiologies• Nonaneurysmal
perimesencephalic SAH
• Vein, dural sinus occlusion
• Vascular malformation
• CT > MR
• Hyperintense CSF in basal cisterns, sulci

MENINGITIS
• Sulcal exudate
• Basilar > convexity
• Can be so FLAIR hyperintense that mimics nl T2WI!
• Look for• Sulcal effacement on T1WI
• Ventriculitis
• Enhancement on T1C+

MR ARTIFACTS:Magnetic Susceptibility
• Metal (braces, root canal, aneurysm clips)
• Air interfaces
• Incomplete suppression
• Local magnetic field alterations →• Null point for fluid (T1)
altered
• Inappropriate high signal intensity
2 hr later
? abnormal
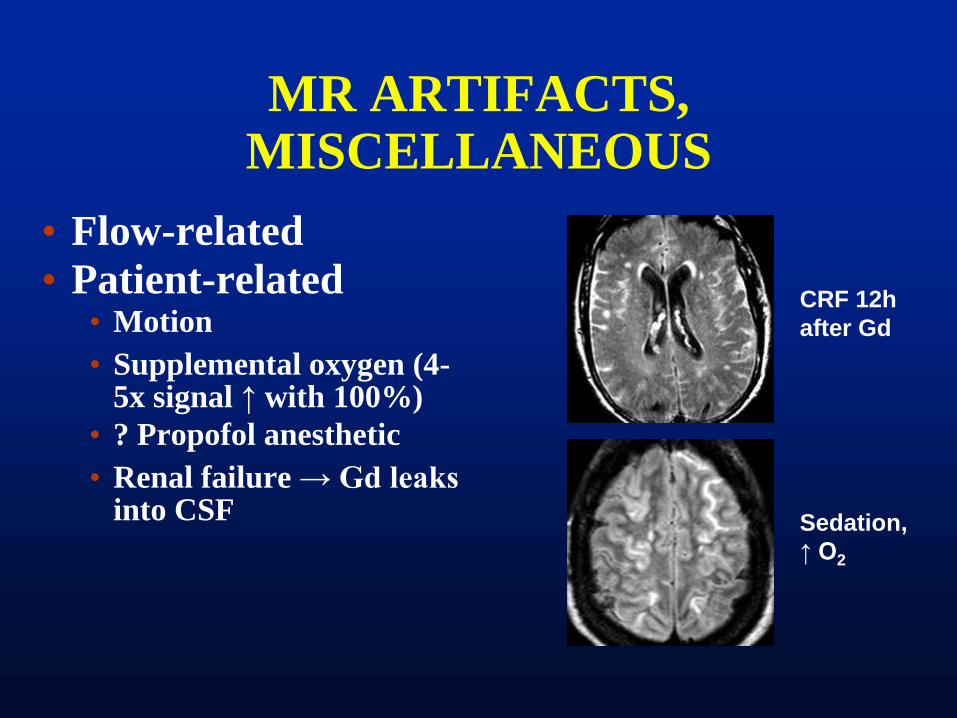
MR ARTIFACTS, MISCELLANEOUS
• Flow-related
• Patient-related• Motion
• Supplemental oxygen (4-5x signal ↑ with 100%)
• ? Propofol anesthetic
• Renal failure → Gd leaks into CSF
CRF 12h
after Gd
Sedation,
↑ O2

METASTASES (CARCINOMATOUS MENINGITIS)
• Causes of hyperintense CSF• ↑ cellularity
• ↑ protein
• Can be focal, regional or diffuse
• Pial enhancement in sulci
• Breast, lung most common

LESS COMMON/RARE CAUSES OF FLAIR HYPERINTENSE CSF
Cerebritis
post contrastCerebral ischemia
(slow flow)
Moya-moya (ivy
sign)
PRES

SUMMARY
• Extra-axial vs. intra-axial• Look for:
• Displaced gray-white interface
• CSF-vascular “cleft”
• Displaced dura (thin black line on MR) = epidural location
• Supra- or infratentorial
• CSF-like or not?
• Adult vs. child