exploring attentional disruption in fibromyalgia using the attentional blink
TRANSCRIPT
This article was downloaded by: [Thammasat University Libraries]On: 06 October 2014, At: 21:18Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Psychology & HealthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/gpsh20
Exploring attentional disruption infibromyalgia using the attentional blinkK. Troy Harker a , Raymond M. Klein b , Bruce Dick a , Michelle J.Verrier a & Saifudin Rashiq aa Department of Anesthesiology and Pain Medicine , University ofAlberta , Edmonton , AB, T6G 2B7 , Canadab Psychology, Life Sciences Centre, Dalhousie University , Halifax ,NS, B3H 4J1 , CanadaPublished online: 19 May 2011.
To cite this article: K. Troy Harker , Raymond M. Klein , Bruce Dick , Michelle J. Verrier &Saifudin Rashiq (2011) Exploring attentional disruption in fibromyalgia using the attentional blink,Psychology & Health, 26:7, 915-929, DOI: 10.1080/08870446.2010.525639
To link to this article: http://dx.doi.org/10.1080/08870446.2010.525639
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Psychology and HealthVol. 26, No. 7, July 2011, 915–929
Exploring attentional disruption in fibromyalgia using the
attentional blink
K. Troy Harkera, Raymond M. Kleinb, Bruce Dicka*,Michelle J. Verriera and Saifudin Rashiqa
aDepartment of Anesthesiology and Pain Medicine, University of Alberta,Edmonton, AB, T6G 2B7, Canada; bPsychology, Life Sciences Centre,
Dalhousie University, Halifax, NS, B3H 4J1, Canada
(Received 10 March 2010; final version received 7 September 2010)
Disrupted attentional function in individuals with fibromyalgia syndrome(FMS) has been noted in a number of previous studies. The cognitivemechanisms related to this disruption are not well-understood. This studysought to identify whether differences exist in early attentional processingand attentional capacity in individuals with FMS measuring the attentionalblink (AB). Early attentional function was assessed in 16 females with FMSand compared with 16 healthy age-matched females without FMS. Simpleearly visual stimulus target detection accuracy was not significantlydifferent between groups. However, as target detection difficulty increased,individuals in the FMS group showed significantly poorer performancecompared to healthy participants. Our findings suggest that attentionaldisruption in individuals with FMS is associated with deficits in the earlyallocation of attentional resources during the completion of tasks withhigher attentional demand.
Keywords: fibromyalgia; chronic pain; attention; attentional disruption;clinical sample
Introduction
Fibromyalgia syndrome (FMS) is characterised by widespread musculoskeletal pain,stiffness and fatigue (Wolfe et al., 1990). One of the hallmark symptoms of FMS isrecurrent and widespread pain that is disproportionate to the level of objective,detectable tissue damage. Many patients with FMS also report cognitive disruptionthat can affect mental health and reduce quality of life. While researchers andclinicians have acknowledged this problem, it has not yet been systematically studied.That chronic pain disrupts cognitive functioning in FMS patients is well-documented. For example, studies of individuals with FMS have found evidenceof attentional deficits on neuropsychological tasks with high attentional demands(Grace, Nielson, Hopkins, & Berg, 1999; Sletvold, Stiles, & Landro, 1995), as well asimpairments on tasks of selective and sustained attention (Dick, Eccleston, &Crombez, 2002). More recent work (Dick, Verrier, Harker, & Rashiq, 2008) has also
*Corresponding author. Email: [email protected]
ISSN 0887–0446 print/ISSN 1476–8321 online
� 2011 Taylor & Francis
DOI: 10.1080/08870446.2010.525639
http://www.informaworld.com
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

pointed to specific difficulties with working memory in this population. While thedevelopment of neurocognitive models provide some promising theories forbiological mechanisms related to these deficits (Legrain et al., 2009), much remainsto be learned (Spaeth & Briley, 2009).
Explanations for the disruption of cognitive functioning in FMS can beunderstood using Kahneman’s (Kahneman, 1973) concept of attention as a limitedpool of resources that are available for information processing demands. Factorssuch as pain, depressed mood and fatigue have the potential to result in interruptedonline attentional processing, limiting the attentional resources available forperforming other tasks (Legrain et al., 2009; Spaeth & Briley, 2009).
While it is generally accepted that pain disrupts attentional processing, thecognitive mechanisms underlying the attentional disruption by chronic pain areunclear. Sletvold et al. (1995) proposed that the attentional disruption observed inFMS represents a disruption of information processing capacity. If the attentionaldisruption observed in FMS patients is reflective of a deficit in informationprocessing, then an examination of cognitive mechanisms with known informationprocessing capacity limits may provide important insights. These insights would berelevant to the nature of the information processing deficits in FMS and chronic painsyndromes in general.
Given the association between chronic pain and attentional functioning onbehavioural measures in previous studies, an examination of early attentionalprocessing is warranted. Rapid serial visual presentation (RSVP) and the attentionalblink (AB) paradigm are appropriate starting points for such an investigation ofearly attentional processing in a FMS population. The AB occurs early in the processof visual stimulus detection and recognition. It has been proposed to be a reflectionof the interference in target identification due to the processing of features of apreviously presented stimulus (Raymond, Shapiro, & Arnell, 1992). A recent review(Martens & Wyble, 2010) has noted that 20 years of research on the AB suggests thatit is a reflection of a generally property of perceptual awareness and improves ourunderstanding of how task relevant stimuli are perceived by the brain.
The AB is typically evoked by dual-target RSVP paradigms in which individualsare asked to identify two target stimuli embedded within a stream of distractingstimuli. In the RSVP paradigm, when the first target (T1) has been successfullyattended to and the second target (T2) is presented within approximately 500milliseconds of T1 (Raymond et al., 1992), individuals are impaired in their ability toaccurately identify T2. This brief period of time subsequent to attending to T1 duringwhich individuals are impaired at attending to T2 is what Raymond et al. (1992) havetermed the AB. In this way, the AB is thought to represent a capacity limit forregulating the rate at which attentional resources consumed by T1 are released tohelp identify T2 (Marois & Ivanoff, 2005).
In this study, our primary aim was to investigate the early attentional processingcapacity in individuals with FMS. A secondary aim was to investigate the influenceof key factors such as pain level and mood on early attentional function. Wehypothesised that attentional processing capacity, as measured by an AB-maskingparadigm, would be reduced in individuals with FMS relative to pain-free matchedcontrols. To test this hypothesis, we specifically examined two related informationprocessing functions: (1) the ability to accurately identify target identities (T1) whenthese are presented briefly and masked; and (2) the duration of attentionalinvolvement in the processing of a first target stimulus during which time the
916 K.T. Harker et al.
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

processing of a second target stimulus is impaired (the AB). We hypothesised that ifchronic attentional disruption in individuals with FMS affects the attentionalresources needed for target letter identification, then T1 identification should beimpaired relative to the control group. Alternatively, if pain disrupts the control ofattentional resources, then we predicted that the FMS group would demonstrate anAB of greater duration and/or magnitude than that of the control group.
Methods
Participants
This study was approved by the University of Alberta Health Research Ethics Board.Informed consent was obtained from all participants. A sample of 16 femaleparticipants with a history of FMS meeting the American College of Rheumatology(ACR) diagnostic criteria for the classification of FMS (Wolfe et al., 1990) and 16age- and sex-matched pain-free controls (ranging in age from 21 to 66 years) wererecruited for this study. FMS participants were consecutively sampled from patientswho were scheduled to receive ongoing treatment at the Multidisciplinary PainCentre at the University of Alberta Hospital. Control participants were recruitedfrom the local community through hospital, campus, newspaper and televisionadvertisements. Participants in the FMS group had had pain for at least 6 months.Individuals with a medical history that included significant head injury, neurologicaldisorder or disease known to impair attentional functioning were excluded.
Measures
The following measures were recorded from all participants.
Demographics
Background demographic, medical, pain history and current medication prescriptiondetails were recorded.
Pain
Pain was recorded using a 100mm Visual Analogue Scale. Participants were requiredto draw a vertical line to represent their pain levels at the time of testing on ahorizontal line anchored with the descriptors ‘no pain’ and ‘worst pain imaginable’.
Mood
The Hospital Anxiety and Depression (HAD) scale (Zigmond & Snaith, 1983) is abrief (14-item) measure used to assess participants’ current levels of depression andanxiety. The seven items related to depression were used for this study.
AB paradigm
The stimuli, parameters and procedures for the AB paradigm are the same as thosereported by McLaughlin, Shore, and Klein (2001).1 The target stimuli consisted of
Psychology and Health 917
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

uppercase letters randomly chosen from the alphabet with the exception of the lettersI and O. The target stimuli were masked by eight different random pattern maskscreated from two masks (each composed of jumbled pieces of digits, see e.g.McLaughlin et al. (2001)) that had been rotated in four different orientations. Thefixation stimulus consisted of a black cross in the centre of the screen. Computerisedtesting was carried out using PsyScope software on an iMac Apple computer. Eachtrial was initiated by a key press from the participant and began with a fixation pointfollowed by a variable delay of 100ms, 200ms or 300ms before a 4-item sequenceconsisting of Target 1 (T1) – Mask 1 (M1) – interstimulus interval (ISI) – Target 2(T2) – Mask 2 (M2). Each target – mask pairing (i.e. T1–M1; T2–M2) had a totalduration of 105ms (including a 15ms gap between target and mask). T1 difficultywas manipulated by varying the duration of the T1 and M1 stimuli as follows: easytrials T1¼ 45ms and M1¼ 45ms; medium trials T1¼ 30ms and M1¼ 60ms; hardtrials T1¼ 15ms and M1¼ 75ms. T2 and M2 durations were held constant at themedium T1 difficulty level (T2¼ 30ms, M2¼ 60ms). T1–T2 stimulus onsetasynchrony (SOA) was varied by manipulating the ISI between T1’s mask and T2.The result was five different SOAs ranging from 120ms to 600ms in 120msincrements.
This AB-masking paradigm requires participants to identify two briefly presentedtargets within a stream of target masks. The target stimuli were presented at varyingtime intervals to change the level of difficulty. The difficulty level of this task wasmodified by altering the T1 target to mask presentation time ratio, thus allowing fora comparison of target identification ability. Identification accuracy for T2 in an AB-masking paradigm is, however, typically reduced when this target occurs between100ms to 500ms after the T1 (i.e. during the AB). Identification accuracy rate of T2as a function of the interval between targets thus provides a useful index of theduration of attentional involvement for target processing.
Procedure
Participants were instructed to sit at a comfortable distance from the computerscreen and provided with instructions on how to start a trial and enter responses.At the end of each sequence, participants entered their responses to the targets byentering the letters detected visually in the order they were detected via the computerkeyboard. Participants were instructed to guess if not sure about their target choiceand were told that their guesses would often be correct. Following a practice block of30 trials using the easiest level of difficulty, participants completed a block of 300 testtrials. Participants were encouraged to take breaks as needed during the task andwere not given any time constraints for completing the block of trials.
Analyses
Statistical analyses were focussed on the variables of T1 accuracy (a simple measureof stimulus detection) and conditional T2 accuracy (T2 accuracy given that T1 wascorrect – a measure of the AB). The order of T1 and T2 responses was disregardedfor all analyses. All analyses were conducted with repeated measures analysis ofvariance (RM-ANOVA). Conservative degrees of freedom were employed whenviolations of sphericity were found ("5 1). Following Howell’s (1997)
918 K.T. Harker et al.
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

recommendations, the Huynh–Feldt correction was used for smaller violations ofsphericity (values between 0.75 and 1.00) while the Greenhouse–Geisser correctionwas employed for more severe violations of sphericity ("5 0.75). A 2-within1-between RM-ANOVA for T1 accuracy examined the following factors: T1difficulty (Easy, Medium, Hard) X Lag (5 levels) X Group (FMS, Control). The2-within 1-between RM-ANOVA for T2 conditional accuracy (i.e. only recorded fortrials where both targets were correctly identified) examined these same factors.
Results
Demographics and pain
Information on participants’ demographic, medical, mood and pain-related infor-mation can be found in Table 1. No between-group differences were found on anydemographic measures. Significant differences were found between groups wherehigher levels of depression (t(24)¼ 6.09, p5 0.001) were noted in the FMS group.Pain was also significantly higher in the FMS group (t(24)¼ 7.47, p5 0.001).
T1 accuracy
T1 letter identification was not impaired in the FMS participants relative to thecontrol group, suggesting that the chronic disruption of attention in FMS does notappear to affect the cognitive resources required for letter identification. The resultsof the RM-ANOVA found a significant main effect of T1 difficulty (F(2,60)¼ 61.77;p5 0.05; effect size¼ 0.67), indicating that as stimulus duration was shortened,stimulus identification became less accurate for all participants (Figure 1). TheRM-ANOVA found no other significant effects or interactions, including no maineffect of Group or Group interactions related to T1 accuracy.
Table 1. Demographic, pain and medication status, including percentages (%) means andstandard deviations (SDs) of participants with FMS and control participants (Control).
FMS Control
Demographicdata
Mean age (years) (SD) 47.56 (12.77) 47.44 (13.49)
Mean years of education (SD) 15.27 (2.57) 15.42 (2.77)Pain status Visual analogue scale mean score
(range 0–100) (SD)44.19 (25.40) 1.81 (3.72)
Mean pain chronicity (years) (SD) 10.57 (9.39) 0.0 (0.0)Mood Mean HAD score (range 0–21) (SD) 6.36 (3.53) 0.50 (0.67)Pain location (N) Joints 11 0
Back 11 0Limbs 6 0Neck and shoulders 11 0All over 5 0Other 10 0
Medication (N) Opioids 6 0Non-opioid analgesics 3 0Non-steroidal anti-inflammatory (NSAID) 2 0Other (any other prescription medication) 14 9
Psychology and Health 919
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014
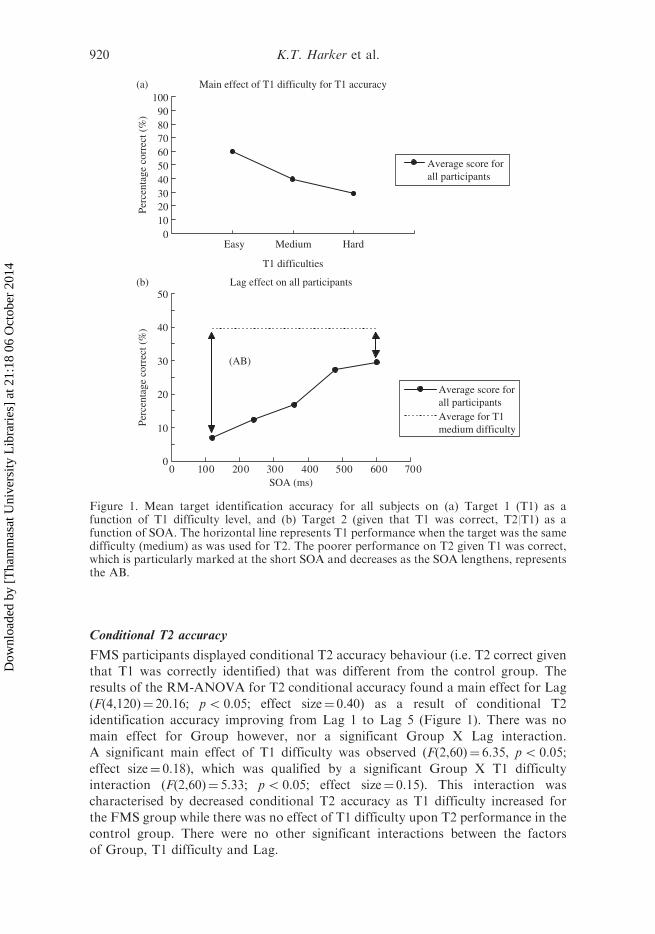
Conditional T2 accuracy
FMS participants displayed conditional T2 accuracy behaviour (i.e. T2 correct given
that T1 was correctly identified) that was different from the control group. The
results of the RM-ANOVA for T2 conditional accuracy found a main effect for Lag
(F(4,120)¼ 20.16; p5 0.05; effect size¼ 0.40) as a result of conditional T2
identification accuracy improving from Lag 1 to Lag 5 (Figure 1). There was no
main effect for Group however, nor a significant Group X Lag interaction.
A significant main effect of T1 difficulty was observed (F(2,60)¼ 6.35, p5 0.05;
effect size¼ 0.18), which was qualified by a significant Group X T1 difficulty
interaction (F(2,60)¼ 5.33; p5 0.05; effect size¼ 0.15). This interaction was
characterised by decreased conditional T2 accuracy as T1 difficulty increased for
the FMS group while there was no effect of T1 difficulty upon T2 performance in the
control group. There were no other significant interactions between the factors
of Group, T1 difficulty and Lag.
Lag effect on all participants
0
10
20
30
40
50
SOA (ms)
Perc
enta
ge c
orre
ct (
%)
Average score forall participantsAverage for T1medium difficulty
(AB)
Main effect of T1 difficulty for T1 accuracy
0102030405060708090
100(a)
(b)
0 100 200 300 400 500 600 700
Easy Medium Hard
T1 difficulties
Perc
enta
ge c
orre
ct (
%)
Average score forall participants
Figure 1. Mean target identification accuracy for all subjects on (a) Target 1 (T1) as afunction of T1 difficulty level, and (b) Target 2 (given that T1 was correct, T2|T1) as afunction of SOA. The horizontal line represents T1 performance when the target was the samedifficulty (medium) as was used for T2. The poorer performance on T2 given T1 was correct,which is particularly marked at the short SOA and decreases as the SOA lengthens, representsthe AB.
920 K.T. Harker et al.
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

Age
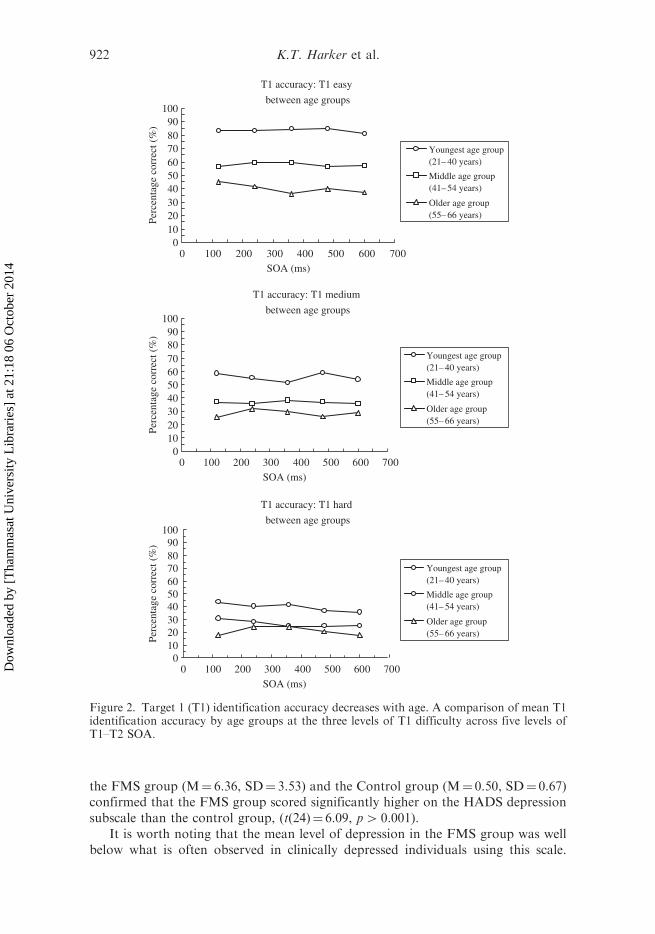
Comparison of our findings with those of McLaughlin et al.’s (2001) study revealedthat our participants were performing at a much lower level of accuracy despiteperforming the identical task. It was hypothesised that an explanation for thisdiscrepancy might lie in the fact that our participants were considerably older (range21–66 years) than those in the McLaughlin study (range 20–29 years). To explore thispossibility, we carried out a follow-up analysis of the T1 data using the variablesLag, T1 difficulty and Age. The participants were divided into three different agegroups (21 to 40, n¼ 10; 41 to 54, n¼ 12; 55 to 66, n¼ 10). An expected, main effectof T1 difficulty was observed (F(2,58)¼ 77.88, p5 0.05; effect size¼ 0.73).In addition, there was a significant main effect of Age (F(2,29)¼ 5.27, p5 0.05;effect size¼ 0.27) and a T1 difficulty X Age interaction (F(4,58)¼ 4.01, p5 0.05;effect size¼ 0.22).
A least significant difference post-hoc analysis of Age showed that the youngestage group performed significantly better than both the middle and older age groups,while the latter two groups were not significantly different from each other(Figure 2). These results strongly support the suggestion that the participants in ourstudy performed worse than the participants in the McLaughlin et al. (2001) studybecause of age differences between the two studies and a decline in performancewith age.
Performance deficits
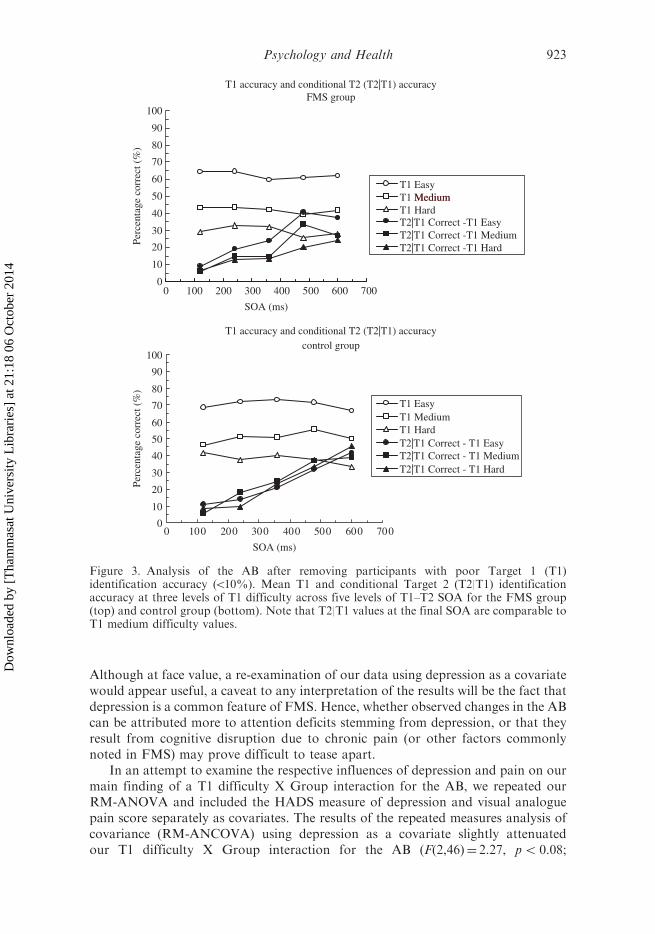
Lower T1 performances are problematic for measuring the AB in this study becausethe AB is derived from T2 performance but only when T1 has been correctlyidentified. With no or few T1 correctly identified, one cannot measure the AB. Toaddress this issue, we ran another T2 conditional correct RM-ANOVA (T1 difficultyX Lag X Group) analysis focussing on participants with no or few data blocks whereT1¼ 0 (Figure 3). This was accomplished by defining a minimum T1 performancecriterion of 10% averaged across each Lag X T1 difficulty data block. This resultedin the removal of six participants (two from the FMS group and four from thecontrol group) from the data set.
The results of this analysis were similar to the original T2 conditional correctanalysis. There was still main effect of group while the T1 difficulty effect(F(2,48)¼ 4.50, p5 0.05; effect size¼ 0.16) and the T1 difficulty X Group interaction(F(2,48)¼ 5.14, p5 0.05; effect size¼ 0.18) remained. As can be seen in Figure 4, theinteraction reflects the fact that T1 difficulty has no effect on conditional T2accuracy in the control group whereas in the FMS group, conditional T2 accuracydeclines as T1 became more difficult.
Depression
It is widely accepted that attention and concentration difficulties are commoncharacteristics of depression and previous evidence has suggested high levels ofdepression may increase the duration and the magnitude of the AB (Rokke, Arnell,Koch, & Andrews, 2002). Depression is so common in the FMS population thatmany hold it as a core feature of this disorder. As previously mentioned, a t-testcomparison (equal variances not assumed) of the mean HADS depression scores for
Psychology and Health 921
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014
the FMS group (M¼ 6.36, SD¼ 3.53) and the Control group (M¼ 0.50, SD¼ 0.67)confirmed that the FMS group scored significantly higher on the HADS depressionsubscale than the control group, (t(24)¼ 6.09, p4 0.001).
It is worth noting that the mean level of depression in the FMS group was wellbelow what is often observed in clinically depressed individuals using this scale.
T1 accuracy: T1 medium
between age groups
0102030405060708090
100
SOA (ms)
Perc
enta
ge c
orre
ct (
%)
Youngest age group(21– 40 years)
Middle age group(41– 54 years)
Older age group(55– 66 years)
T1 accuracy: T1 hard
between age groups
0102030405060708090
100
SOA (ms)
Perc
enta
ge c
orre
ct (
%)
Youngest age group(21– 40 years)
Middle age group(41– 54 years)
Older age group(55– 66 years)
T1 accuracy: T1 easy
between age groups
0102030405060708090
100
0 100 200 300 400 500 600 700
0 100 200 300 400 500 600 700
0 100 200 300 400 500 600 700SOA (ms)
Perc
enta
ge c
orre
ct (
%)
Youngest age group(21– 40 years)
Middle age group(41– 54 years)
Older age group(55– 66 years)
Figure 2. Target 1 (T1) identification accuracy decreases with age. A comparison of mean T1identification accuracy by age groups at the three levels of T1 difficulty across five levels ofT1–T2 SOA.
922 K.T. Harker et al.
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014
Although at face value, a re-examination of our data using depression as a covariatewould appear useful, a caveat to any interpretation of the results will be the fact thatdepression is a common feature of FMS. Hence, whether observed changes in the ABcan be attributed more to attention deficits stemming from depression, or that theyresult from cognitive disruption due to chronic pain (or other factors commonlynoted in FMS) may prove difficult to tease apart.
In an attempt to examine the respective influences of depression and pain on ourmain finding of a T1 difficulty X Group interaction for the AB, we repeated ourRM-ANOVA and included the HADS measure of depression and visual analoguepain score separately as covariates. The results of the repeated measures analysis ofcovariance (RM-ANCOVA) using depression as a covariate slightly attenuatedour T1 difficulty X Group interaction for the AB (F(2,46)¼ 2.27, p5 0.08;
T1 accuracy and conditional T2 (T2|T1) accuracycontrol group
0
10
20
30
40
50
60
70
80
90
100
SOA (ms)
Perc
enta
ge c
orre
ct (
%)
T1 EasyT1 MediumT1 HardT2|T1 Correct - T1 EasyT2|T1 Correct - T1 MediumT2|T1 Correct - T1 Hard
T1 accuracy and conditional T2 (T2|T1) accuracyFMS group
0
10
20
30
40
50
60
70
80
90
100
0 100 200 300 400 500 600 700
0 100 200 300 400 500 600 700
SOA (ms)
Perc
enta
ge c
orre
ct (
%)
T1 EasyMediumT1 Medium
T1 HardT2|T1 Correct -T1 EasyT2|T1 Correct -T1 MediumT2|T1 Correct -T1 Hard
Figure 3. Analysis of the AB after removing participants with poor Target 1 (T1)identification accuracy (510%). Mean T1 and conditional Target 2 (T2|T1) identificationaccuracy at three levels of T1 difficulty across five levels of T1–T2 SOA for the FMS group(top) and control group (bottom). Note that T2|T1 values at the final SOA are comparable toT1 medium difficulty values.
Psychology and Health 923
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

effect size¼ 0.11). However, the results of the RM-ANCOVA using the current painlevel as a covariate removed our significant finding of a T1 difficulty X Groupinteraction on the AB, (F(2,48)¼ 0.94, p¼ 0.40; effect size¼ 0.04). These findings areconsistent with the conclusion that pain plays a primary role in accounting for theimpaired AB in FMS.
Discussion
The purpose of this study was to examine whether attentional disruption in FMSdiminished the attentional resources needed for identifying briefly presented andmasked target stimuli and whether the control of attentional processing resourceswas impaired in individuals with FMS, in comparison to the pain-free, age- andgender-matched controls. Using the AB-masking paradigm of McLaughlin et al.(2001), we assessed both simple attention for stimulus identification (T1 accuracy)and the degree of attentional involvement in information processing as measured bythe AB (T2 accuracy conditional upon T1 being correctly identified).
As expected, T1 performance deteriorated with increasing level of T1 difficulty;however, there were no differences in T1 performance between the FMS and controlgroups. Conditional T2 accuracy was poorest at the shortest time lags and improvedwith increasing lag, as is typical for the AB. However, contrary to our predictions,there was neither significant Group difference in T2 performance nor did Groupinteract with Lag as would have occurred if attention in the FMS group becamemore deeply absorbed in T1 processing. Nonetheless, a significant Group X T1difficulty interaction was found for conditional T2 accuracy, providing evidence of
T2 accuracy at different T1 difficulties
FMS and control groups
0
10
20
30
40
50
Easy Medium Hard
Perc
enta
ge c
orre
ct (
%)
FMS groupControl group
T1 difficulties
Figure 4. FMS conditional Target 2 (T2|T1) identification accuracy decreases as Target 1 (T1)difficulty level increases relative to the control group and mean T2|T1 identification accuracyfor the FMS and control groups at each T1 difficulty level.
924 K.T. Harker et al.
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

abnormal attentional processing in individuals with FMS. It is important to notethat this effect occurred when the task of identifying T1 became more difficult. Thisfinding is consistent with previous work showing that this effect occurs in individualswith chronic pain primarily when task demands are high (Dick & Rashiq, 2007;Eccleston, 1995).
As T1 identification is considered to be a simple task of attention, the lack of T1identification deficits by the FMS group is consistent with the above-mentionedneuropsychological evidence of attentional disruption only for more demandingtasks of attention in FMS. The relationship between T1 difficulty level and T1accuracy observed in this study is comparable to that reported by McLaughlin et al.(2001) with the exception of the absolute T1 accuracy values (discussed below). Thusthis study confirms that the attentional disruption observed in FMS is notattributable to impairment in simple stimulus detection and a disruption of resourceallocation needed for letter identification.
That the AB did not differ between the FMS and control groups either inmagnitude or duration in this study might seem surprising, given that studies of otherclinical populations with attention-related cognitive impairments have reported analtered AB, such as schizophrenia (protracted duration and increased magnitude)(Li et al., 2002), ADHD (protracted duration) (Hollingsworth, McAuliffe, &Knowlton, 2001) and spatial neglect (protracted duration) (Husain, Shapiro, Martin,& Kennard, 1997). It should not be necessarily expected, however, that the attentionimpairments in these populations are equivalent to those in FMS patients. Indeed,unlike the control group in this study and the participants in the originalMcLaughlin et al. (2001) study using the same AB-masking paradigm, the AB inthe FMS group was susceptible to the influence of T1 identification difficulty.The results of this investigation nonetheless provide evidence confirming ourhypothesis of abnormal attentional processing in FMS. As T1 items became moredifficult to detect, conditional T2 accuracy decreased in the FMS group. This resultimplies that in the FMS group, factors such as chronic pain may disrupt attention viaimpairment in the allocation of attentional resources and that this effect isdependent upon the difficulty level of the task. In the control group, T1 difficultyhad no demonstrable effect on subsequent conditional T2 accuracy. In the FMSgroup, when the overall task difficulty increased by making T1 identificationmore difficult, attentional function was most disrupted compared to when T1identification was easy. That the FMS group shows impairments with increasingT1 difficulty level is consistent with the neuropsychological and behavioural reportsthat have found attentional impairment in individuals with FMS on demandingtasks of attention (Dick & Rashiq, 2007; Eccleston, 1995; Grace et al., 1999;Sletvold et al., 1995).
An important report on the effects of stimulus competition (Leavitt & Katz,2006) sheds light on our findings. They completed neuropsychological testing on agroup of individuals with FMS and found that on tasks where stimulus competitionincreased, task performance was significantly disrupted. This effect has more recentlybeen replicated and extended in a general chronic pain population (Dick & Rashiq,2007). The current findings are consistent with these previous reports and mayrepresent a very early attentional processing stage affected by stimulus competition.The results in this report are an initial step in our understanding of how early stagesof cognitive processing are affected by chronic pain and other factors. Nevertheless,they provide important corroborative evidence that the behavioural disruption
Psychology and Health 925
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

during task performance noted in previous research may have its roots invery early attentional disruption. To the best of our knowledge, this is thefirst study that has found an early cognitive mechanism that is disruptedin individuals with FMS.
We recognise that there are a number of limitations inherent to the design of thisstudy. There are a variety of factors that could be involved in the differences foundbetween our groups. Factors such as depression, fatigue and effort are known to beassociated with attentional disruption. While we were able to statistically investigatethe influence of some of the factors potentially involved, there are some importantchallenges that arise as we strive to interpret the unique effects of factors that areclearly related to each other. Further, the nature of FMS as a clinical syndrome issuch that symptoms of depression and fatigue could be easily argued to beestablished elements of FMS. When factoring out the influence of variables such asdepression, it is difficult to confidently state that depression is a key cause of thecognitive disruption. Instead, it appears far more appropriate to suggest thatcomorbid depression that frequently coexists with FMS may play an important rolein the cognitive disruption noted in individuals with FMS. Finally, unfortunately, wedid not collect data related to perceived cognitive impairment and related functionaldisability from our participant groups. Examining the magnitude of the relationbetween perceived cognitive dysfunction, actual measured dysfunction, and moreglobal pain-related disability would further enhance our understanding of theconsequences of the disruption of early attentional processes. This would be animportant factor to examine in future studies.
In addition, it is difficult, and, potentially unethical, to study the effects ofmedication on cognitive function in this population. There is little question that anumber of the medications taken by our participants have the potential to markedlyaffect cognitive function. However, we suggest that it is also worth consideringimportant evidence (Lorenz, Beck, & Bromm, 1997; Tassain et al., 2003) thatmedication, particularly analgesic medications taken by our participants, mayactually improve cognitive function. Thus, it is possible that our between groupeffects could have actually been reduced by medications taken, rather than caused orincreased by them. Much remains to be learned about the effects of medication oncognition in clinical populations with chronic pain syndromes.
Also of interest in this study were the low levels of performances on T1 andconditional T2 accuracies (Figure 1) for both the FMS and the control groups. Theparadigm we used in this study was the same paradigm employed by McLaughlinet al. (2001) that resulted in typical T1 and conditional T2 ceiling accuracies. The ABhas typically been studied in university-aged young adults, while the age range ofparticipants in this study was from 21 to 66 years of age. Our analysis of agegroupings suggested that the lower T1 accuracy scores for both groups in this studymay have been related to the age range of our participants. Indeed, the youngest agegroup achieved performance levels comparable to those typically reported in ABstudies. In addition, a previous report (Park, Glass, Minear, & Crofford, 2001) hasnoted that individuals with FMS show declines in cognitive function that are similarto those observed in older individuals. Most important to this effect however, wasthe observation that by Lag 5, performance levels of T2 approach the performancelevel of the medium T1 difficulty level. T2 conditional accuracies would not beexpected to be higher than T1 accuracy levels for the medium difficulty level as theyshare the same duration (i.e. 30ms).
926 K.T. Harker et al.
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

Attentional disruption associated with chronic pain disorders (such as FMS)affects the sufferer’s ability to work, sleep and perform other activities essential toleading a full life, and these changes generally worsen over time (Wincent, Liden, &Arner, 2003). It has been suggested that when attention has been chronicallyinterrupted by pain, even the signal or expectation of impending pain can becomesufficient to disrupt attention (Legrain et al., 2009). This suggestion predicts that asfactors that disrupt attention consume greater amounts of attentional resources, taskperformance should decline. This is an issue that would be worthwhile to explore infuture studies and could be examined through comparison of performance acrossindividuals who are pain-free, those who have chronic pain and those withexperimentally induced tonic pain.
Understanding the cognitive mechanisms mediating the attentional disruption inFMS is important for developing screening measures of information processingdeficits. Such measures will allow for the identification of FMS patients at risk ofcognitive disruption and who might benefit from cognitive rehabilitation treatmentssuch as attentional retraining. There is some evidence that show cognitive disruptioncan be remediable in clinical settings. How amenable early attentional processingwould be to such interventions is unknown but worthy of investigation in futurestudies. The results of this study suggest that the attentional disruption in FMSappears to be associated with deficits in the early allocation of attention resources intasks with higher attentional demand. These results provide a framework and guidefor future investigations of the cognitive mechanisms mediating attentionaldisruption by factors such as chronic pain.
Acknowledgement
The authors thank Canadian Institutes of Health Research (CIHR) for the HealthProfessional Student Research Award to K.T.H.
Note
1. McLaughlin et al. (2001) advanced their version of the Target-Mask–Target-Mask (TM–TM) paradigm first developed by Duncan, Ward, and Shapiro to avoid the untowardcontributions of task switching present in the RSVP in the seminal study by Duncan et al.(1994). They also demonstrated that this paradigm taps the same underlying attentionalmechanisms as does the stream paradigm.
References
Dick, B., Eccleston, C., & Crombez, G. (2002). Attentional functioning in fibromyalgia,
rheumatoid arthritis, and musculoskeletal pain patients. Arthritis & Rheumatism, 47,
639–644.Dick, B.D., & Rashiq, S. (2007). Disruption of attention and working memory traces in
individuals with chronic pain. Anesthesia & Analgesia, 104, 1223–1229.Dick, B.D., Verrier, M.J., Harker, K.T., & Rashiq, S. (2008). Disruption of cognitive function
in fibromyalgia syndrome. Pain, 139, 610–616.Duncan, J., Ward, R., & Shapiro, K. (1994). Direct measurement of attentional dwell time in
human vision. Nature, 369, 313–315.
Psychology and Health 927
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014

Eccleston, C. (1995). Chronic pain and distraction: An experimental investigation into the role
of sustained and shifting attention in the processing of chronic persistent pain. Behaviour
Research and Therapy, 33, 391–405.Grace, G.M., Nielson, W.R., Hopkins, M., & Berg, M.A. (1999). Concentration and memory
deficits in patients with fibromyalgia syndrome. Journal of Clinical and Experimental
Neuropsychology, 21, 477–487.Hollingsworth, D.E., McAuliffe, S.P., & Knowlton, B.J. (2001). Temporal allocation of visual
attention in adult attention deficit hyperactivity disorder. Journal of Cognitive
Neuroscience, 13, 298–305.
Howell, D.C. (1997). Statistical methods for psychology (4th ed.). Belmont, CA: Duxbury
Press, Wadsworth Publishing Company.
Husain, M., Shapiro, K., Martin, J., & Kennard, C. (1997). Abnormal temporal dynamics
of visual attention in spatial neglect patients. Nature, 385, 154–156. doi: 10.1038/
385154a0.Kahneman, D. (1973). Attention and effort. Englewood-Cliffs, NJ: Prentice-Hall.
Leavitt, F., & Katz, R.S. (2006). Distraction as a key determinant of impaired
memory in patients with fibromyalgia. Journal of Rheumatology, 33, 127–132.
Retrieved from http://www.jrheum.org.login.ezproxy.library.ualberta.ca/content/33/1/
127.longLegrain, V., Damme, S.V., Eccleston, C., Davis, K.D., Seminowicz, D.A., & Crombez, G.
(2009). A neurocognitive model of attention to pain: Behavioral and neuroimaging
evidence. Pain, 144, 230–232.
Li, C.S., Lin, W.H., Yang, Y.Y., Huang, C.C., Chen, T.W., & Chen, Y.C. (2002). Impairment
of temporal attention in patients with schizophrenia. NeuroReport, 13, 1427–1430. ISSN:
0959-4965.Lorenz, J., Beck, H., & Bromm, B. (1997). Cognitive performance, mood and experimental
pain before and during morphine-induced analgesia in patients with chronic non-
malignant pain. Pain, 73, 369–375.Marois, R., & Ivanoff, J. (2005). Capacity limits of information processing in the brain.
Trends in Cognitive Sciences, 9, 296–305.Martens, S., & Wyble, B. (2010). The attentional blink: Past, present, and future
of a blind spot in perceptual awareness. Neuroscience and Biobehavioral Reviews,
34, 947–957.McLaughlin, E.N., Shore, D.I., & Klein, R.M. (2001). The attentional blink is immune
to masking-induced data limits. Quarterly Journal of Experimental Psychology-A, 54,
169–196.
Park, D.C., Glass, J.M., Minear, M., & Crofford, L.J. (2001). Cognitive function in
fibromyalgia patients. Arthritis and Rheumatism, 44, 2125–2133.
Raymond, J.E., Shapiro, K.L., & Arnell, K.M. (1992). Temporary suppression of visual
processing in an RSVP task: An attentional blink? Journal of Experimental Psychology:
Human Perception and Performance, 18, 849–860. ISSN: 0096-1523.Rokke, P.D., Arnell, K.M., Koch, M.D., & Andrews, J.T. (2002). Dual-task
attention deficits in dysphoric mood. Journal of Abnormal Psychology, 111,
370–379. ISSN: 0021-843X.Sletvold, H., Stiles, T.C., & Landro, N.I. (1995). Information processing in
primary fibromyalgia, major depression and healthy controls. Journal of Rheumatology,
22, 137–142. ISSN: 0315-162X.
Spaeth, M., & Briley, M. (2009). Fibromyalgia: A complex syndrome requiring
a multidisciplinary approach. Human Psychopharmacology: Clinical and Experimental,
24, S3–S10.
928 K.T. Harker et al.
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014
Tassain, V., Attal, N., Fletcher, D., Brasseur, L., Degieux, P., Chauvin, M., &Bouhassira, D. (2003). Long term effects of oral sustained release morphineon neuropsychological performance in patients with chronic non-cancer pain.Pain, 104, 389–400.
Wincent, A., Liden, Y., & Arner, S. (2003). Pain questionnaires in the analysis of long lasting(chronic) pain conditions. European Journal of Pain, 7, 311–321.
Wolfe, F., Smythe, H.A., Yunus, M.B., Bennett, R.M., Bombardier, C.,
Goldenberg, D.L., . . . , Sheon, R.P. (1990). The American college ofrheumatology criteria for the classification of fibromyalgia. Arthritis andRheumatism, 33, 160–172.
Zigmond, A.S., & Snaith, R.P. (1983). The hospital anxiety and depression scale.Acta Psychiatrica Scandinavica, 67, 361–370.
Psychology and Health 929
Dow
nloa
ded
by [
Tha
mm
asat
Uni
vers
ity L
ibra
ries
] at
21:
18 0
6 O
ctob
er 2
014