expression in balloon-ilated and stented
TRANSCRIPT

ORIGINAL ARTICLE
Nonmuscie myosin heavy chain-B
expression in balloon-ilated and stented
arteries: a study in the atherosclerotic
Yucatan micropig
B.J.G.L. de Smet, H. De Leon, J.N. Wilcox, Y.J.M. van der Helm, A. Schoneveld, C. Borst, M.J. Post
Background. Restenosis after balloon angioplastyis in part due to remodelling, whereas restenosisafter stenting is entirely due to neointima for-mation. Nonmusde myosin heavy chain-B(NMMHC-B) is expressed by vascular smoothmuscle cells and because of its overexpression inrestenotic lesions after balloon angioplasty,NMMHC-B is proposed as a potential therapeutictarget. Because the mechanisms underlyingrestenosis after balloon angioplasty or afterstenting are different we hypothesised that theexpression ofNMMHC-B would differ in balloon-dilated versus stented arteries.Metbods. To study the localisation and time courseof expression of NMMHC-B, we performedstenting or balloon dilation in peripheral arteries of16 atherosderoticYucatanmcropigW and used serialintravascular ultrasound (IVUS) and angiographyto measure geometric dimensions following balloonangioplasty or stenting. In situ hybridisation tech-niques were used to detect NMMHC-B mRNA.5'-bromo-2'-deoxyuridine (BrdU) wasadminto detect proliferating cells. By counting thenumber of silver grains in the different layers of
BJ.G.L de SmetDepartment of Cardiology, Groningen University Medical Centre,GroningenYJ.M. van der HelmA. SchoneveldDepartment of Cardiology, Utrecht University Hospital andInteruniversity Cardiology Institute of the NetherlandsC. BorstMi. PostDepartment of Cardiology, Utrecht University Hospital, UtrechtH. De LeonJ.N. WIlcoxCardiovascular Divsion, Department of Medicine,Emory University, Atlanta, GA, USA
Correspondence to: B.J.G.L. de SmetGroningen University Medical Centre,PO Box 30001, 9700 RB GroningenE-mail: [email protected]
the artery, we could compare the amount ofexpression at the different time points between thegroups.Results. In intima and media,NMMHC-B expres-sion increased after balloon dilaton and stenting andpeked at 7 days. In stented arteries, the expressionofNMMHC-B remained high for up to 42 daysafter injury, whereas in balloon-dilated arteries ithad nornalised In the adventitia ofballoon-dilatedarteries, but not of stented arteries, NMMHC-Bexpression peaked at 7 days. NMMHC-B expres-sion was not limited to proliferating cells.Conclusion. NMMHC-B is expressed near sites ofactive repair after arterial injury, but not limited toproliferating cells. The different pattern ofNMMHC-B expression after balloon dilationcompared with stenting may be related to arterialremodelling, because stented arteries that do notremodel lack this conspicuous adventitial expres-sion at 7 days. (NethHeartJ2005;6:224-32.)
Key words: balloon dilation, restenosis
Restenosis ofcoronary arteries after successful treat-ment by balloon angioplasty or stenting remains
a major limitation ofthese revascularisation procedures.Angiographically, restenosis seems to be a well-definedentity, but the mechanisms ofrestenosis after balloonangioplasty and stent placement appear to be different.In balloon-dilated arteries, restenosis is mainly theresult of geometric remodelling of the artery and, toa lesser degree, ofneointimal formation at the luminalsurface.'-9 In contrast to balloon-dilated arteries,restenosis in stented arteries is almost completely dueto neointimal formation.'0"'1 Identification of genesexpressed after balloon dilation or stenting is essentialto better understand the different mechanisms ofrestenosis.
Nonmuscle myosin heavy chain (NMMHC) playsa fundamental role in different biological events such ascell division,l2 3 alteration of cell shape,'4 chemotaxis
Netherlands Heart Journal, Volume 13, Number 6, June 2005 cC224

Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
and protein synthesis and secretion.'5'16 Two isoforms ofNMMHC have been identified,17-19 NMMHC-A andNMMHC-B. Smooth musde cells contain both non-muscle and smooth musde myosins.2022 NMMHC-Ais equally expressed in normal and restenotic arteries.23Examination of biopsies of primary and restenoticlesions revealed thatNMMHC-B mRNAwas presentin greater abundance in restenotic lesions than inprimary atherosclerotic plaques.24 In addition, theincreased expression ofNMMHC-B in atherosderoticplaques has been suggested to identify a group oflesions at high risk for restenosis after atherectomy.25Thus nonmusde myosin heavy chain-B (NMMHC-B)might be involved in postangioplasty restenosis ofatherosclerotic arteries.
In a previous study, an upregulation ofNMMHC-B expression after balloon angioplasty was shown innonatherosclerotic porcine coronary arteries.26 In situhybridisation experiments showed a higher expressionof NMMHC-B mRNA in injured versus normalarteries. However, in that study no formal quantifi-cation ofmRNA expression was performed. Becausethe mechanisms underlying restenosis after balloonangioplasty or after stenting are different, we hypo-thesised that the expression ofNMMHC-B would bedifferent in balloon-dilated versus stented arteries. Inorder to test this hypothesis we examined the local-isation and time course ofexpression ofNMMHC-Bin the atherosderotic Yucatan micropig after balloonangioplasty or stenting. We used serial intravascularultrasound and quantitative angiography to measuregeometric dimensions following balloon angioplasty orstenting and in situ hybridisation techniques were usedto detect NMMHC-B mRNA.
Materials and methodsSixteen Yucatan micropigs with an average weight of24 kg were used for this study. All animals were on anatherogenic diet that started at the age of7-8 months.Two weeks later, they underwent Fogarty denudationofthe internal iliac, external iliac, and femoral arteries.Atherogenic diet was continued for an additional 4-6months, after which selected arteries were balloondilated or stented. The atherogenic diet was discon-tinued and replaced with a nonatherogenic diet duringfollow-up. The animals were killed at 2, 4, 7, 14 or 42days and the artenes were harvested. The investigationconforms with the Guide for the Care and Use ofLaboratory Animals published by the US NationalInstitutes of Health (NIH Publication No. 85-23,revised 1985) and was approved by the ethics com-mittee on Animal Experiments of the Faculty ofMedicine, Utrecht University.
Atherogenic diet and anaesthesiaIn addition to essential nutrients, vitamins and salts,1.5% cholesterol, 17.5% casein, 14% lard, and 6%peanut oil formed the basic atherogenic componentsofthe diet that had a daily nutritional value equivalent
to 2400 Kcal. In pilot experiments it was shown thatthis regimen results in a sustained tenfold increase intotal cholesterol level to 14.9±4.4 mmol/l, and a 3.5-fold increase in HDL level to 2.2±0.3 mmol/l. Afterdiscontinuation of the atherogenic diet, the levels ofcholesterol andHDL cholesterol dropped to base levels(1.5±0.7 mmol/l and 0.6±0.1 mmol/l, respectively).Water intake was not restricted. The diet dunng follow-up was a regular, nonatherogenic chowwith a nutritionalvalue equal to the atherogenic diet.
For denudation, intervention and termination, theaninals were anaesthetised with intravenous metomidate(4 mg/kg) and ventilated (Servo, EM 902) with amixture of02:N20=1:2 and halothane, 1-2%. Duringeach procedure, the animals were heparinised (100IU/kg thromboliquine) to an APTI above 80 sec.Every 15 minutes, 0.25 mg atropine was given intra-venously.
One day before intervention, acetylsalicylic acid(125 mg) was given orally and continued for two weeksafter the intervention. During intervention andtermination, a continuous infusion ofnitroglycerin (20,ug/min) was given to prevent arterial spasm.
ProceduresFor denudation, intervention and termination, thearterial tree was accessed through a carotid cutdownand insertion ofan arterial 8F sheath into the descendingaorta under fluoroscopic guidance. An 8F guidingcatheterwas advanced to the aortic bifiircation. Throughthis, contrast angiography was performed and a Fogartyballoon catheter, an intravascular ultrasound catheterand a balloon angioplasty or stent catheter wereadvanced. After the denudations and the intervention,the carototomies were carefully repaired for futureinterventions.
During denudation, 3-4 cm segments (measuredby a radiopaque ruler) in the iliac and femoral arterieswere denuded by triple withdrawal of a 4F Fogartycatheter that was manually inflated with a 50/50 v/vwater contrast mixture. Four months after thedenudation, selected sites of angiographic arterialnarrowing were balloon dilated. Before and after eachintervention, angiography and intravascular ultrasoundwere performed under fluoroscopic guidance. Forballoon dilation, a standard peripheral (length 2-4 cm,diameter 4-7 mm) or coronary (length 2 cm, diameter2-4 mm) balloon catheterwas advanced over a 0.035"or a 0.014" guidewire. The balloon was inflated threetimes for one minute at a pressure of 10 atm. Forstenting we mounted the stent on a coronary ballooncatheter and the catheter was advanced over a 0.014"guidewire. The balloon was inflated for ten seconds ata pressure of10 atm.A second in-stent balloon dilationwas performed in case of inadequate stent expansionas judged by intravascular ultrasound.
After a follow-up of2, 4, 7, 14 or 42 days, the pigswere anaesthetised and angiograms and intravascularultrasound measurements were taken. The animals
Netherlands Heart Journal, Volume 13, Number 6, June 2005 225

Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
were killed after angiography and intravascular ultra-sound was performed. The arteries were removed 'enbloc' and fixed by immersion in 4% paraformaldehydein 0.1 mol/l NaPO4 buffer (pH 7.4) for two hours,followed by overnight storage in sterile 15% sucrose-PBS solution at 4°C. After fixation, the arteries weredivided into 3-4mm segments and embedded inOCTand frozen in liquid nitrogen.
Angiography and intravascular ultrasoundAngiograms were performed before and after eachintervention and at follow-up. Contrast was injectedselectively into the artery under study through an 8Fguiding catheter. The fluoroscopy was recorded at acine rate of 12 images/sec using a digital C-arm. Theimages with the highest contrast were selected andstored onDAT tape for later analysis. The angiographicdiameters ofthe arteries were measured using a semi-automated programme.27 In each artery, lumendiameters were measured at intervals of 0.5 cm,induding the treated segment and a proximal and distalreference segment. Reference lumen diameters (RLD)were chosen in angiographically normal arterialsegments at a distance of at least 1 cm proximal anddistal to the balloon-dilated site. To locate the treatedsegment repeatedly at different time points (pre- andpost-procedure and at follow-up), its position wasdocumented relative to an anatomic landmark withthe support of a radiopaque ruler placed along thespine in a reproducible manner. The ruler was alsoused for calibration ofthe angiography.27
All quantitative analyses were performed off-line.The minimum lumen diameter (MLD) of the lesionwas determined. Angiographic acute gain was definedas the difference between post- and pre-procedurelumen diameters, and angiographic late lumen loss wasdefined as the difference between post-procedure andfollow-up lumen diameters. Angiographic percentageof stenosis was calculated as (1 - MLD/RLD)x100.The site of stenosis corresponded to the MLD in thetreated segment. Dilation ratio was defined as thediameter ofthe inflated balloon on fluoroscopy dividedby the angiographic diameter ofthe reference segment.Intravascular ultrasound recordings were taken beforeand after intervention and at follow-up, using a 30-MHz ultrasound transducer, which rotated up to 16times per second within a 4.1 French catheter. Theaxial resolution ofthe system was 0.1 mm. The imageswere displayed on a monitor and recorded on VHSvideotape. Intravascular ultrasound images wereanalysed with a digital video analyser as describedpreviously.28 Fluoroscopywas performed during IVUSso that the IVUS images were documented relative toan anatomic landmark to match the IVUS images atdifferent time points (pre- and post-procedure and atfollow-up). In the IVUS images, the area circumscribedby the interface between the echodense intimal layerand the echolucent media was manually traced =media-bounded area (MBA). In addition, the lumen
area was traced and the minimum lumen area wasdetermined (MLA). Echographic acute gain wasdefined as the difference between post- and pre-intervention lumen area and echographic late lumenloss as the difference between post-intervention andfollow-up lumen area. In addition to late lumen loss,late MBA loss was introduced to measure the re-modelling after angioplasty. LateMBAloss was definedas the difference between the post-intervention MBAand follow-up MBA at either the site of the initialstenosis or the reference sites. Intimal area was definedas the difference betweenMBA and lumen area (LA).At follow-up, the intima is the sum of plaque andintimal hyperplasia. Intimal hyperplasia is thereforecalculated as the difference between the intima atfollow-up and pre-intervention. Echographic percentageof stenosis is calculated as (1 - MLA/RLA)x100.
Immunohistochemistty5'-bromo-2'-deoxyuridine (BrdU) was dissolved insterile lactated Ringer's solution (33 mg/ml) andadministered via the ear vein in three doses of 50mg/kg at 24, 16 and 8 hours before termination.BrdU localisation was detected in tissues using a specificBrdU monoclonal antibody (1/20 dilution, Dako)after predigestion of the tissue with proteinase K (1,g/mi) and 4N HCL. Cells were identified with thefollowing primary antibodies: SM-I directed against a-smooth muscle actin (1/800) dilution, h-caldesmon(1/1000) dilution or vimentin (1/320) dilution.Immunohistochemical detection of the preferredepitopes was performed according to the indirectalkaline phosphatase technique.29'30
In situ hybridisationIn situ hybridisation using porcine-specific 35S-labelledsense and antisense riboprobes was performed aspreviously described.32 Porcine cDNA fragmentsencoding for NMMHC-B were amplified by reverse-transcriptase polymerase chain reaction from porcineSMCs and subcloned into pCRII vectors (Invitrogen).The following primer sequences were used forpolymerase chain reaction amplification: 5'-GTGTAGGATATGGCAGAATTGAC and 3'-TGGAGTGGGAACCTFGCTCTTJG. Sequencing ofthe cDNA probe used in the present experimentsindicates that it encodes a 5' region ofthe NMMHC-B gene and that it is 93% homologous to humanNMMHC-B but only 75% homologous to humanNMMHC-A.'8
Briefly, cryosections were pretreated with para-formaldehyde and proteinase K and prehybridised in100 pd hybridisation buffer (50% formamide, 0.3 mol/ANaCL, 20 mmol/l Tris, ph 8.0, 5 mmol/l EDTA,0.02% polyvinylpyrrolidone, 0.02% Ficoll, 0.02%bovine serum albumin, 10% dextran sulphate, and 10mmol/l dithiothreitol) at 42°C. Serial sections werehybridised with 6x105 cpm of35S-labelled riboprobesat 55°C. After hybridisation, the sections were washed
Netherlands Heart Journal, Volume 13, Number 6, June 2005 t|C226

Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
Table 1. Number of days after intervention.
Number of days after Intervention
Control 2 4 7 14 42Balloon Stent Balloon Stent Balloon Stent Balloon Stent Balloon Stent
Arteries(n) 17 10 2 6 3 5 4 8 3 7 5Animals(n) 16 4 2 3 3 3 3 3 3 3 3
Note that control arteries are pooled and that balloon-dilated, stented and control arteries are obtained from the same 16 animals.
with 2xSSC (1xSSC contains 150 mmol/A NaCl and counted on the screen using a computer programme,15 mmol/l sodium citrate, pH = 7.0), 10 mmol/A - analySIS in a semi-automated fashion.mercapto-ethanol, and I mmol/A EDTA, treated withRNase A, and washed in the same buffer, followed by Statistical analysisa high-stringency wash in O.lxSSC with 10 mmol/l All data in text and tables are presented asP-mercapto-ethanol and 1 mmol/l EDTA at 55°C. mean±standard error ofthe mean. SPSS 6.1 was usedThe slides were then washed in 0.5xSSC and for all statistical calculations. To identify differencesdehydrated in graded alcohols containing 0.3 mol/l between subgroups we used one-way analysis ofNH4Ac. The sections were dried, coated with NTB2 variance and Duncan's range test. P<0.05 was con-nuclear track emulsion, and exposed in the dark at 4°C sidered statistically significant.for one to four weeks. After development, the sectionswere counterstained with haematoxylin and eosin to Resultsaid in cell identification. Balloon angioplasty was performed in 36 peripheral
Results of the in situ hybridisation were analysed arteries in 16 Yucatan micropigs. Seventeen peripheralin the following fashion. Three sections per treated site arteries were stented and 17 peripheral arteries were notwere examined. Four fields per cross-section were treated and served as controls. Complete IVUS andchosen in clockwise order (at 3, 6, 9, and 12 hours). angiographic imaging were performed in all arteries.Intima, media and adventitia were analysed separately. The numbers of arteries in each group at each timeColour video images of 240x300 ,um fields were point are given in table 1.captured and digitised by use of a x20 objective with The average echographic stenosis was 29% in thea 3CCD colour video camera. Silver grains were balloon-dilated group, 34% in the stented group and
Netherands Heart Journal, Volume 13, Number 6, June 2005
Table 2. IVUS and angiographic baseline parameters.
Balloon Stent Control
Number of arteries 36 17 17MLA pre (mm2) 7.5±0.4 6.6±0.8 7.7±0.9MBA pre (mm2) 9.5±0.6 9.1±1.1 8.4±1.0LA reference pre (mm2) 11.8±0.9 10.4±1.0 10.2±1.3MBA reference pre (mm2) 12.3±0.9 11.7±1.1 10.9±1.4MLD pre (mm) 2.4±0.1 2.1±0.2# 2.7±0.1LD reference pre (mm) 3.2±0.1 3.1±0.1 3.3±0.2Stenosis IVUS (%) 28.8±3.5 33.6±5.1 24.5±2.5Stenosis angiogram (%) 24.2±2.9 29.5±5.5 17.5±2.6Acute gain IVUS (mm2) 5.1±0.8 6.7±1.0Acute gain angiogram (mm2) 0.8±0.1 1.1±0.2Dilation ratio 1.2±0.0 1.1±0.0*
# stent versus control significantly different with p<O.05.* stent vs. balloon significantly different with p<O.05.MLA pre=minimum lumen area before balloon dilation or stenting, MBA=media-bounded area, LA=lumen area, MLD pre=minimum lumen diameter before balloon di-lation or stenting, LD=lumen diameter. Note that MLD, LD and dilation ratio are angiographic parameters.
227

Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
25% in the control group (table 2). The angio-graphically determined dilation ratio was 1.2±0.0 inthe balloon-dilated group and 1.1±0.0 in the stentedgroup (p<0.05). The echographic acute gain was5.1±0.8 mm2 in the balloon-dilated group vs. 6.7±1.0mm2 in the stented group. Acute gain and dilationratio are considered to reflect the severity of injuryimparted on the arterial wall. The mean pre-existingplaque area was 1.8±0.2 mm2. Echographic andangiographic percentage ofstenosis, echographic andangiographic acute gain, lumen areas and media-bounded areas were not significantly differentbetween the groups (table 2). Lumen areas, media-bounded areas and lumen diameters before balloonangioplasty or stenting are given in table 2 for boththe site of stenosis and the reference site and for thecontrol arteries.
IA NMMHC-B In Intimaj3000- #
2400
11800-
> I1200-
600
Control 2 4 7 14 42Days after Intervention
NMMHC-B mRNA expression over timeLow expression ofNMMHC-B mRNA was found incontrol atherosclerotic arteries both in the media andintima. A semi-quantitative comparison of in situhybridisation expression is only possible ifnonspecificbinding of the probe is similar in all groups. Whenusing the sense probe, the number ofsilver grains per50x103I im2 was low and not significantly different inany group at any given time point. The nonspecificbinding of the sense probe was only higher in thestented arteries than the balloon-dilated and controlarteries at 2 days.
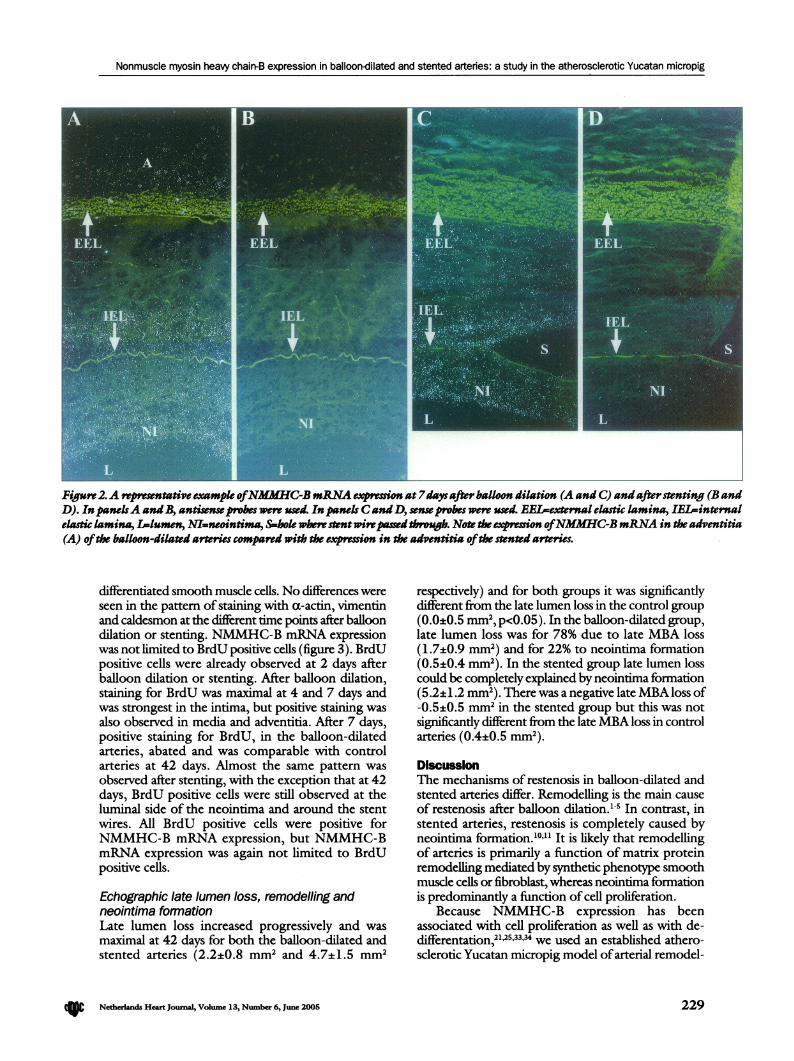
In the intima of the balloon-dilated arteries,NMMHC-B mRNA expression increased over timeand was maximal at 7 days after intervention. At 42days, NMMHC-B mRNA expression in the balloon-dilated arteries had returned to levels seen in controlarteries. In stented arteries, NMMHC-B mRNAexpression was also maximal at 7 days but remainedincreased until 42 days after intervention (figure IA).Examples of NMMHC-B mRNA expression in theintima 7 days after balloon dilation or stenting are
shown in figure 2.In the media, the increase in expression of
NMMHC-B mRNA in stented and balloon-dilatedarteries showed a similar pattern. They were bothmaximal at 7 days. However, the expression in stentedarteries at 4 days was already significantly higher thanboth control and balloon-dilated arteries. Again, medialexpression ofNMHHC-B in stented arteries remainedhigh until 42 days and was significantly higher than inthe balloon-dilated arteries at 42 days (figure 1B).
The pattern ofNMMHC-B mRNA expression inthe adventitia was similar to the pattern in the intimaand media except for a remarkable high expression at7 days after balloon angioplasty. This peak expressionwas absent in stented arteries (figure 1C).
In balloon-dilated arteries, expressionofNMMHC-B mRNA in the intima as well as the media and theadventitia was most prominent near breaks of theinternal elastic lamina.
Is NMMHC-B In Media
3000
2400
11800'
I1200-
600
Balloon
Control
~IControl
uControl 2 4 7 14 42Days aftr Intervention
ic NMMHC-B In Adventitla3000-
Z 2400-.1S 1800-
1200-
I600-
rv --
Balloon
Stent
~IControl
Control 2 4 7 14 42Dys after IntentIon
Figure 1. NMMHIC-B tipe#ion over time. Panel AXlxproion inthe intima. PanelB: Epression in the media. Panel C: lprossionin the adventitia.*=p<0.05 (stentvs. balloon), #=p<0.05 (vs. contol). Note that controlarteries arepookd.
ImmunohistochemistryCells expressing NMMHC-B mRNA stained with a-
actin or both a-actin and vimentin, but not withcaldesmon, suggesting that these cells were de-
Netherlands Heart Journal, Volume 13, Number 6, June 2005 C
Balloon
- SCnt
~~Control
228
. Ai i- dkkm -A
Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
#-t, j,$.
Figure 2.A reprewntative example ofNMMHC-BmRNA exrssion at7dys after balloon dilation (A and C) and afterstenting (B andD). InpanelsA and , antisenseprobes were used. Inpanels CandD, sense probes were used. EEL-external elastic lamina, IEL-internalelastic lamina, L-lumen, NI=neointima, Sshokewherestentwirepassed ovug. Note theexprsion ofNMMHC-B mRNA in the adventitia(A) ofthe balloon-dilated arteries compared with the eression in the adventitia ofthe stented arteries.
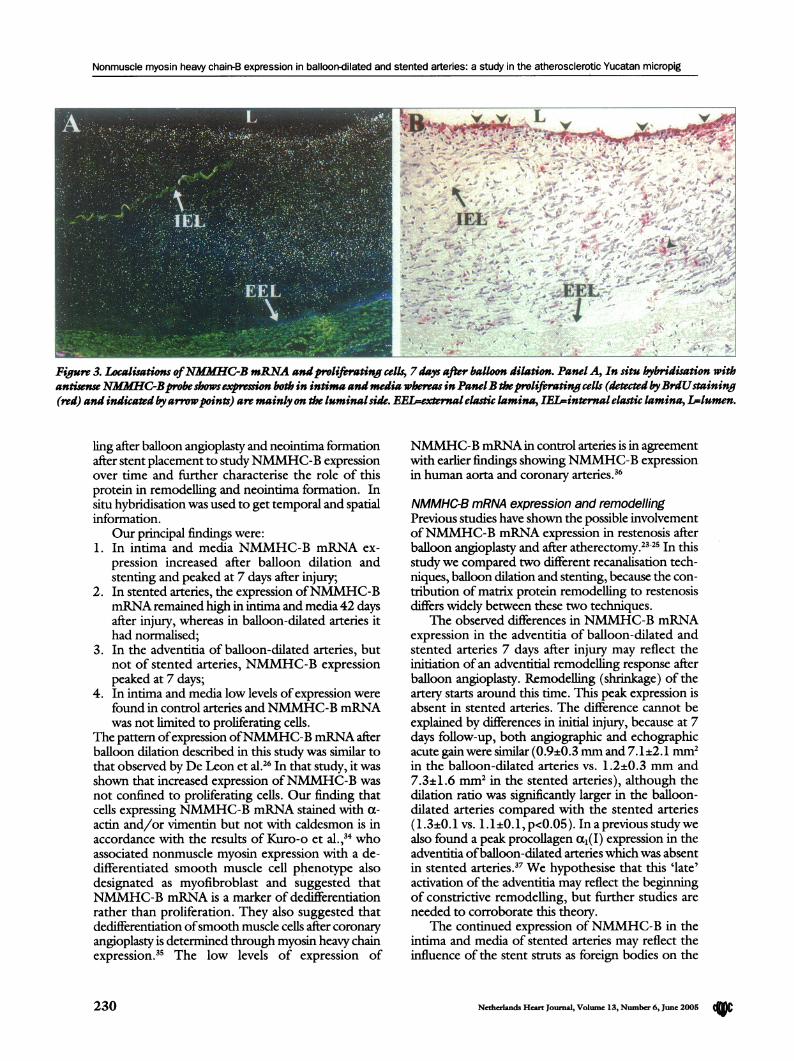
differentiated smooth musde cells. No differences wereseen in the pattern ofstaining with a-actin, vimentinand caldesmon at the different time points after balloondilation or stenting. NMMHC-B mRNA expressionwas not limited to BrdU positive cells (figure 3). BrdUpositive cells were already observed at 2 days afterballoon dilation or stenting. After balloon dilation,staining for BrdU was maximal at 4 and 7 days andwas strongest in the intima, but positive staining wasalso observed in media and adventitia. After 7 days,positive staining for BrdU, in the balloon-dilatedarteries, abated and was comparable with controlarteries at 42 days. Almost the same pattern wasobserved after stenting, with the exception that at 42days, BrdU positive cells were still observed at theluminal side of the neointima and around the stentwires. All BrdU positive cells were positive forNMMHC-B mRNA expression, but NMMHC-BmRNA expression was again not limited to BrdUpositive cells.
Echographic late lumen loss, remodelling andneointima formationLate lumen loss increased progressively and wasmaximal at 42 days for both the balloon-dilated andstented arteries (2.2±0.8 mm2 and 4.7±1.5 mm2
respectively) and for both groups it was significantlydifferent from the late lumen loss in the control group(0.0±0.5 mm2, p<O.05). In the balloon-dilated group,late lumen loss was for 78% due to late MBA loss(1.7±0.9 mm2) and for 22% to neointima formation(0.5±0.4 mm2). In the stented group late lumen losscould be completely explained by neointima formation(5.2±1.2 mm2). There was a negative lateMBAloss of-0.5±0.5 mm2 in the stented group but this was notsignificantly different from the lateMBA loss in controlarteries (0.4±0.5 mm2).
DiscussionThe mechanisms of restenosis in balloon-dilated andstented arteries differ. Remodelling is the main causeof restenosis after balloon dilation.'"5 In contrast, instented arteries, restenosis is completely caused byneointima formation.'0"1' It is likely that remodellingof arteries is primarily a ftmction of matrix proteinremodelling mediated by synthetic phenotype smoothmuscle cells or fibroblast, whereas neointima formationis predominantly a function of cell proliferation.
Because NMMHC-B expression has beenassociated with cell proliferation as well as with de-differentation,21,25,33,3 we used an established athero-sclerotic Yucatan micropig model ofarterial remodel-
Netherlands Heart Journal, Volume 13, Number 6, June 2005 229
Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
'I_LL\. vv... vS~ ~~ - .S. - u,u
¢ 6 IEL- 'r b*' # -ik - <t - ~~~~~~~~~~~~~~, x# 1P57- ~ ~ ~ ~ ~ ~ -
- - EEL,At~
Figure 3. Localisations ofNMfMHC-B mRNA andproliferating cellf 7 days after balloon dilation. Pane A, In situ hybridisation withantiwnseNMAHC-Bprobe shows expmsionboth in intimaand media whereasinPanelB theproliferating cells (dtecdbyBrdUstaining(red) and indicated byarrowpoints) are mainly on the luminal side.EEi-exrleltic lamina, IEL-internal elastic lamina, 1-lumen.
ling after balloon angioplasty and neointima formationafter stent placement to studyNMMHC-B expressionover time and further characterise the role of thisprotein in remodelling and neointima formation. Insitu hybridisation was used to get temporal and spatialinformation.
Our principal findings were:1. In intima and media NMMHC-B mRNA ex-
pression increased after balloon dilation andstenting and peaked at 7 days after injury;
2. In stented arteries, the expression ofNMMHC-BmRNAremained high in intima and media 42 daysafter injury, whereas in balloon-dilated arteries ithad normalised;
3. In the adventitia of balloon-dilated arteries, butnot of stented arteries, NMMHC-B expressionpeaked at 7 days;
4. In intima and media low levels ofexpression werefound in control arteries andNMMHC-B mRNAwas not limited to proliferating cells.
The pattern ofexpression ofNMMHC-B mRNA afterballoon dilation described in this study was similar tothat observed by De Leon et al.26 In that study, it wasshown that increased expression ofNMMHC-B wasnot confined to proliferating cells. Our finding thatcells expressing NMMHC-B mRNA stained with a-actin and/or vimentin but not with caldesmon is inaccordance with the results of Kuro-o et al.,34 whoassociated nonmuscle myosin expression with a de-differentiated smooth muscle cell phenotype alsodesignated as myofibroblast and suggested thatNMMHC-B mRNA is a marker of dedifferentiationrather than proliferation. They also suggested thatdedifferentiation ofsmooth muscle cells after coronaryangioplasty is determined through myosin heavy chainexpression.35 The low levels of expression of
NMMHC-B mRNA in control arteries is in agreementwith earlier findings showingNMMHC-B expressionin human aorta and coronary arteries.36
NMMHC-B mRNA expression and remodellingPrevious studies have shown the possible involvementofNMMHC-B mRNA expression in restenosis afterballoon angioplasty and after atherectomy.2325 In thisstudy we compared two different recanalisation tech-niques, balloon dilation and stenting, because the con-tribution of matrix protein remodelling to restenosisdiffers widely between these two techniques.
The observed differences in NMMHC-B mRNAexpression in the adventitia of balloon-dilated andstented arteries 7 days after injury may reflect theinitiation of an adventitial remodelling response afterballoon angioplasty. Remodelling (shrinkage) of theartery starts around this time. This peak expression isabsent in stented arteries. The difference cannot beexplained by differences in initial injury, because at 7days follow-up, both angiographic and echographicacute gain were similar (0.9±0.3 mm and 7.1±2.1 mm2in the balloon-dilated arteries vs. 1.2±0.3 mm and7.3±1.6 mm2 in the stented arteries), although thedilation ratio was significantly larger in the balloon-dilated arteries compared with the stented arteries(1.3±0.1 vs. l.l±O.l, p<O.05). In a previous studywealso found a peak procollagen al(I) expression in theadventitia ofballoon-dilated arteries which was absentin stented arteries.37 We hypothesise that this 'late'activation ofthe adventitia may reflect the beginningof constrictive remodelling, but further studies areneeded to corroborate this theory.
The continued expression ofNMMHC-B in theintima and media of stented arteries may reflect theinfluence of the stent struts as foreign bodies on the
Netherlands Heart Journal, Volume 13, Number 6, June 2005
I lll.I J
230

Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
surrounding tissue, which may trigger a continuedinflammation response.38'39
Umitatlons of the studyWe studied mRNA level by in situ hybridisation, so anabsolute quantification ofNMMHC-B mRNAwas notpossible. Instead, this technique enabled us to study theexpression in the different layers of the artery. Bycounting the number of silver grains in the differentlayers of the artery, we could compare the amount ofexpression at the different time points between thegroups. The nonspecific binding was low and did notdiffer between the time points examined. We thereforefeel that comparison of the absolute number of silvergrains was justified. This study was performed in peri-pheral arteries in an animal model ofcomplex athero-sclerosis and it remains to be determined ifour findingsmay be extrapolated to the human situation. Althoughthe arteries contained considerable plaques, the echo-graphic and the angiographic stensosis were mild, andthus the acute gain was partly achieved by overdilationof the arteries. However the dilation ratios used weresimilar to the clinical situation both for the balloon-dilated arteries and the stented arteries.40 So it is likelythat the amount ofinjury inflicted upon the arterial wallis similar to the human situation and not an exaggerationas in most nonatherosclerotic animal models.
ConclusionsNMMHC-B mRNA is expressed by smooth musclecells and/or myofibroblasts near sites of active repairafter arterial injury, but not limited to proliferatingcells. The different pattern ofexpression ofNMMHC-B mRNA after balloon dilation compared with stentingmay be related to arterial remodelling, because stentedarteries that do not remodel lack this conspicuousadventitial expression at 7 days. U
AcknowledgementParts of this study were presented at the 46th annualscientific session ofthe American College ofCardiologyand at the 70th scientific sessions of the AmericanHeart Association.
This studywas supported by the Netherlands HeartFoundation (grant NHS 92.365) and in part by theInteruniversity Cardiology Institute ofthe Netherlands.
References
1 Mintz GS, Popma n, Pichard AD, Kent KM, Satler LF,Wong SC,et al. Arterial remodeling after coronary angioplasty: a serial intra-vascular ultrasound study. Circulation 1996;94:35-43.
2 Di Mario C, Gil R, Camenzind E, Ozaki Y, Von Birgelen C,Umans VA, et al. Quantitative assessment with intracoronaryultrasound of the mechanisms of restenosis after percutaneoustransluminal coronary angioplasty and directional atherectomy.AmJCardiol 1995;75:772-7.
3 Post MJ, Borst C, Kuntz RE. The relative importance of arterialremodeling compared with intimal hyperplasia in lumen renarrow-ing after balloon angioplasty: A study in the normal rabbit and thehypercholesterolemic Yucatan micropig. Circulation 1994;89:2816-21.
4 Kakuta T, Currier JW, Haudenschild CC, Ryan TJ, Faxon DP.Differences in compensatory vessel enlargement, not intimalformation, accbunt for restenosis after angioplasty in the hyper-cholesterolemic rabbit model. Circulation 1994;89:2809-15.
5 Lafont A, Guzman LA, Whitlow PL, Goormastic M, Comnill JF,Chisolm GM. Restenosis after experimental angioplasty: Intimal,medial, and adventitial changes associated with constrictive re-modeling. Circ Res 1995;76:996-1002.
6 Liu MW, Roubin GS, King SB3. Restenosis after coronaryangioplasty. Potential biologic determinants and role of intimalhyperplasia. Circulation 1989;79:1374-87.
7 Nobuyoshi M, Kimura T, Ohishi H, Horiuchi H, Nosaka H,Hamasaki N, et al. Restenosis after percutaneous transluminalcoronary angioplasty: pathologic observations in 20 patients.JAmCoil Cardiol 1991;17:433-9.
8 Ellis SG, Muller DWM. Arterial injury and the enigma ofcoronaryrestenosis. jAm CoU Cardiol 1992;19:275-7.
9 Schwartz RS, Holmes DR Jr, Topol EJ. The restenosis paradigmrevisited: An alternative proposal for cellular mechanisms. JAmCoil Cardiol 1992;20:1284-93.
10 Painter JA, Mintz GS, Wong SC, Popma JJ, Pichard AD, Kent KM,et al. Serial intravascular ultrasound studies fail to show evidenceofchronic Palmaz-Schatz stent recoil. AmJCardiol 1995;75:398-400.
11 Post MJ, De Smet BJGL, van der Helm YJ, Borst C, Kuntz RE.Arterial remodeling after balloon angioplasty or stenting in anatherosclerotic experimental model. Circulation 1997;96:996-1003.
12 Pasterkamp G, Borst C, Gussenhoven EJ, Mali WP, Post MJ, TheSH, et al. Remodeling ofDe Novo atherosderotic lesions in femoralarteries: impact on mechanism of balloon angioplasty. JAm CollCardiol 1995;26:422-8.
13 Mintz GS, PichardAD, Kent KM, Satler LF, Popma JJ, Leon MB.Axial plaque redistribution as a mechanism ofpercutaneous trans-luminal coronary angioplasty. AmJCardiol 1996;77:427-30.
14 Siegel RJ, Swan K, Edwalds G, Fishbein MC. Limitations ofpost-mortem assessment of human coronary artery size and luminalnarrowing: differential effects of tissue fixation and processing onvessels with different degrees ofatherosclerosis. JAm Coll Cardiol1985;5:342-6.
15 Wessels D, Soll DR, Knecht DA, Loomis WF, DeLozanne A,Spudich JA. Cell motility and chemotaxis in Dictyostelium amebaelacking myosin heavy chain. Dep Biol 1988;128:164-77.
16 Ludowyke RI, Peleg I, Beaven MA, Adelstein RS. Antigen-inducedsecretion of histamine and the phosphorylation of inducedsecretion of histamine and the phosphorylation of myosin byprotein kinase C in rat basophilic leukemia cells.JBiol Chem 1989;264:12492-501.
17 Saez CG, Myers JC, Shows TB, Leinwand LA. Human nonmusclemyosin heavy chain mRNA: generation of diversity throughalternative polyadenylation. Proc Natl Acad Sci USA 1990;87:1164-8.
18 Simons M, Wang M, McBride OW, Kawamoto S, Yamakawa K,Gdula D, et al. Human nonmuscle myosin heavy chains areencoded by two genes located on different chromosomes. Circ Res1991;69:530-9.
19 Matsuoka R, Yoshida MC, Furutani Y, Imamura S, Kanda N,Yanagisawa M, et al. Human smooth muscle myosin heavy chaingene mapped to chromosomal region 16q12. AmJMed Genet1993;46:61-7.
20 Kawamoto S, Adelstein RS. Characterization of myosin heavychains in cultured aorta smooth muscle cells: A comparative study.JBiol Chem 1987;262:7282-8.
21 RovnerAS, Murphy RA, OwensGK Expression ofsmooth muscleand nonmuscle myosin heavy chains in cultured vascular smoothmuscle cells. JBiol Chem 1986;261:14740-5.
22 Gaylinn BD, Eddinger TJ, Martino PA, Monical PL, Hunt DF,Murphy RA. Expression of nonmuscle myosin heavy and lightchains in smooth muscle. AmJPhysiol 1989;257:C997-C1004.
23 Owens GK, Vernon SM, Madsen CS. Molecular regulation ofsmooth musde cell differentiation.JHyperensSuppl 1996;14:S55-64.
24 Leclerc G, Isner JM, Kearney M, Simons M, Safian RD, Baim DS,et al. Evidence implicating nonmusde myosin in restenosis: Use ofin situ hybridization to analyze human vascular lesions obtained bydirectional atherectomy. Circulation 1992;85:543-53.
Ctw Netherlands Heart Journal, Volume 13, Number 6, June 2005 231

Nonmuscle myosin heavy chain-B expression in balloon-dilated and stented arteries: a study in the atherosclerotic Yucatan micropig
25 Simons M, Leclerc G, Safian RD, Isner JM, Weir L, Baim DS.Relation between activated smooth-muscle cells in coronary-arterylesions and restenosis after atherectomy. NEnglJMed 1993;328:608-13.
26 De Leon H, Scott NA, Martin F, Simonet L, Bernstein KE, WilcoxJN. Expression ofnonmuscle myosin heavy chain-B isoform in thevessel wall of porcine coronary arteries after balloon angioplasty.Circ Res 1997;80:514-9.
27 De Smet BJGL, Kuntz RE, van der Helm YJ, Pasterkamp G, BorstC, Post MJ. Relationship between plaque mass and neointimalhyperplasia after stent placement in Yucatan micropigs. Radiolo,gy1997;203:484-8.
28 Wenguang L, Gussenhoven EJ, Zhong Y, The SH, Di Mario C,Madretsma GS, et al. Validation of quantitative analysis of intra-vascular ultrasound images. IntJ Card Imaging 1991;6:247-53.
29 Skalli 0, Ropraz P, Trzeciak A, Benzonana G, Gillessen D,Gabbiani G. A monoclonal antibody against alpha-smooth muscleactin: a new probe for smooth muscle differentiation. J Cell Biol1986;103:2787-96.
30 Frid MG, Shekhonin BV, Koteliansky VE, Glukhova MA. Pheno-typic changes ofhuman smooth muscle cells during development:late expression of heavy caldesmon and calponin. Dev Biol 1992;153:185-93.
31 Osbom M, Debus E, WeberK Monodonal antibodies specific forvimentin. Eurj Cell Biol 1984;34:137-43.
32 Wilcox JN. Fundamental principles of in situ hybridization. JHistochem Cytochem 1993;41:1725-33.
33 Simons M, Rosenberg RD. Antisense nonmuscle myosin heavychain and c-myb oligonucleotides suppress smooth musde cell pro-liferation in vitro. Circ Res 1992;70:835-43.
34 Kuro-o M, Nagai R, Nakahara K, Katoh H, Tsai RS, TsuchimochiH, et al. cDNA cloning of a myosin heavy chain isoform inembryonic smooth muscle and its expression during vasculardevelopment and in atherosclerosis. JBiol Chem 1991;266:3768-73.
35 Nikol S, Murakami N, Pickering JG, Kearney M, Leclerc G,Hofling B, et al. Differential expression ofnonmuscle myosin IIisoforms in human atherosclerotic plaque. Atherosclerosis 1997;130:71-85.
36 Aikawa M, Sivam PN, Kuro, Kimura K, Nakahara K, Takewaki S,et al. Human smooth muscle myosin heavy chain isoforms asmolecular markers for vascular development and atherosclerosis.Circ Res 1993;73:1000-12.
37 De Smet BJ, van der Helm YJ, Horowitz A, Simons M, Post MJ.Matrix remodeling in balloon dilated and stented arteries in athero-sclerotic yucatan micropigs: procollagen alphal(I), alphal(III) andMMPI expression over time [abstract]. Circulation 1996;94:I-403.
38 Karas SP, Gravanis MB, Santoian EC, Robinson KA, AnderbergKA, King SB III. Coronary intimal proliferation after balloon in-jury and stenting in swine: an animal model ofrestenosis. JAm CollCardiol 1992;20:467-74.
39 Miller DD, Karim MA, Edwards WD, Schwartz RS. Relationshipofvascular thrombosis and inflammatory leukocyte infiltration toneointimal growth following porcine coronary artery stent place-ment. Atherosclerosis 1996;124:145-55.
40 Serruys PW, De Jaegere P, Kiemeneij F, Macaya C, Rutsch W,Heyndrickx G, et al. A comparison of balloon-expandable-stentimplantation with balloon angioplasty in patients with coronaryartery disease. NEngljMed 1994;331:489-95.
232 Netherlands Heart Journal, Volume 13, Number 6, June 2005