extent of asymmetry and unilaterality among juvenile onset primary open angle glaucoma patients
TRANSCRIPT

Original Article
Extent of asymmetry and unilaterality amongjuvenile onset primary open angle glaucomapatientsViney Gupta MD,1 Shikha Gupta MBBS,1 Munish Dhawan MD,1 Ajay Sharma BSc,1 Kulwant S Kapoor BSc2
and Ramanjit Sihota MD FRCS1
1Dr. Rajendra Prasad Centre for Ophthalmic Sciences, and 2Department of Biostatistics, All India Institute of Medical Sciences,New Delhi, India
ABSTRACT
Background: Juvenile onset open angle glaucoma(JOAG) due to its rarity is not well characterized. Weaimed to assess the extent of interocular asymmetryof baseline intraocular pressure (IOP), disc mor-phometry and visual field defects at presentation inpatients with primary JOAG.
Design: Retrospective, single-centre, hospital-basedstudy.
Participants: Fifty-two consecutive JOAG patientswho presented with glaucomatous optic neuropathyin at least one eye, without any secondary causes ofglaucoma.
Methods: Participants were evaluated for baselineclinical features. The optic disc parameters weremeasured using scanning laser ophthalmoscopy(Heidelberg Retina Tomograph). Reliable and repro-ducible visual field tests using standard 30-2 Hum-phrey automated perimetry were analysed.
Main Outcome Measures: Interocular asymmetry ofbaseline IOP, vertical cup:disc ratio and meandeviation.
Results: Fourteen patients (27%) had glaucomatousoptic neuropathy in only one eye at initial presenta-tion; the fellow eyes of which had IOP <21 mmHg ineight whereas six had IOP >21 mmHg. In 20 out of52 patients (39%) one eye remained perimetrically
unaffected. Patients presenting with bilateral opticneuropathy were found to be significantly younger(24.4 � 10.6 years) in age compared to thosewith unilateral optic neuropathy (32 � 8.2 years)(P = 0.02).
Conclusions: One-fourth of primary JOAG patientspresent as a unilateral optic neuropathy with 60% ofthese having normal IOP in the fellow eyes. PrimaryJOAG may present with considerable asymmetrywith a small proportion presenting as a unilateraldisease.
Key words: inter-eye asymmetry, interocular asymme-try, JOAG, juvenile glaucoma, juvenile onset glaucoma.
INTRODUCTION
Juvenile onset open angle glaucoma (JOAG) is anautosomal dominant disease. Numerous disease-causing MYOC and also CYP1B1 mutations have nowbeen identified, and additional loci on other chromo-somes have been linked to JOAG.1,2 A diagnosis ofJOAG is made when patients present with primaryopen angle glaucoma between 10 and 40 years ofage. Patients with JOAG are known to have highintraocular pressure (IOP), deep cups and diffusevisual field loss.3 However, because of its rarity,JOAG is not well characterized. It is possible thatmany of these patients may have features of congeni-tal glaucoma presenting late or adult glaucoma pre-senting early.
� Correspondence: Dr Viney Gupta, Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical sciences, Ansari Nagar, New Delhi
110029, India. Email: [email protected]
Received 13 October 2010; accepted 16 January 2011.
Clinical and Experimental Ophthalmology 2011; 39: 633–638 doi: 10.1111/j.1442-9071.2011.02522.x
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists

Adult onset primary open angle glaucoma pre-sents bilaterally and has an asymmetric presentation.Primary congenital glaucoma has been reported topresent unilaterally in almost 20–35% of cases.4,5
Poinoosawmy et al. reported unilateral field lossamong 25% of adult normal tension glaucoma (NTG)patients, whereas in the adult high pressure glau-coma group, 31% patients presented with unilateralfield loss.6 Primary angle-closure glaucoma under-standably has greater interocular asymmetry.7–9 Anextremely asymmetric or unilateral presentation in ayoung patient may indicate a reason to search forsecondary causes for glaucoma. The purpose of thisstudy was to assess structural and functional asym-metry among primary JOAG patients.
METHODS
This study included untreated, primary JOAGpatients presenting between January 2001 andJanuary 2005 at our centre. The study was approvedby our institutional review board. The optic disc andvisual field records on confocal scanning laser oph-thalmoscopy (Heidelberg Retina Tomograph [HRT])and 30-2 Humphrey field analyser, respectively, wereevaluated. A diagnosis of JOAG was based on thepresence of all of the following:
• Primary open angle glaucoma with an age ofonset between 10 and 40 years
• Intraocular pressure >22 mmHg in one or botheyes on more than one occasion
• Glaucomatous optic neuropathy in one or botheyes with or without visual field loss consistentwith optic nerve damage
• Open angles on gonioscopy in both eyes.
Exclusion criteria were: history of steroid use,presence of any other retinal or neurological pathol-ogy, evidence of secondary causes of raised IOP,those with any pathology detected on gonioscopylike angle recession, pigmentation of the anglegreater than grade 3 or peripheral anterior synechiaeand those who had had any ocular surgery beforepresentation.
All patients underwent a complete ophthalmicexamination including slit-lamp biomicroscopy,gonioscopy, pachymetry and dilated stereoscopicexamination of optic disc and fundus. Three base-line IOP measurements (before starting therapy),taken in each eye, using standard Goldmannapplanation tonometer, were recorded. IOP asym-metry was calculated for a difference of 2, 3–8 andgreater than 8 mmHg between the two eyes of eachpatient at presentation. To qualify, the IOP asym-metry had to be regularly present, with all of theasymmetric readings in the same direction during at
least two clinical visits, until the institution oftherapy.
A minimum of two reliable and reproduciblebaseline Humphrey 30-2 full threshold visual fieldswere evaluated. Modified Andersons criteria wereused to categorize a visual field defect as beingglaucomatous.10 The location of the defect had to beconsistent between baseline fields and with theglaucomatous optic disc damage. We categorized thedegree of interocular visual field asymmetry in eachpatient based on the difference between the meandeviation values.
Glaucomatous optic neuropathy was consideredin the presence of an excavated disc, with neuroreti-nal rim thinning/notching or localized/generalizedretinal nerve fibre layer defect as detected on HRTand confirmed by fundus evaluation by two glau-coma specialists. Confocal scanning laser ophthal-moscopy (HRT II, Heidelberg Engineering GmbH,Heidelberg, Germany) was used to image the opticnerve head in both eyes in each patient. Three 15°topographic images (obtained in the same sitting)were aligned and averaged to obtain a meantopography. An experienced optometrist outlined theoptic disc margin. One glaucoma specialist (VG)reviewed all the images. The following global HRTparameters were examined in this study: disc area,cup area, rim area, cup-to-disc area ratio, rim-to-discarea ratio, cup volume, rim volume, mean cup depth,maximum cup depth, height variation contour, cupshape measure, mean retinal nerve fibre layer thick-ness, retinal nerve fibre layer cross-sectional area,horizontal and vertical cup:disc ratios, linearcup:disc ratio, and the FSM11 and RB12 discriminantfunctions.
Statistical analysis
Interocular differences of IOP, cup:disc ratio andmean deviation were calculated and correlated usingPearson’s correlation coefficient. Continuous vari-ables were compared using Student’s t-test andcategorical variables using chi-square analysis.A P-value <0.05 was considered for statisticalsignificance. The SPSS software (version 10.0, SPSSInc., Chicago, IL, USA) was used for statisticalanalysis.
RESULTS
Baseline data of 52 consecutive, unrelated, JOAGpatients were analysed. Their follow-up records over5 years with an average of 11.2 � 3 HRT and8.3 � 2.3 visual field examinations were alsostudied. Mean age of the patients in the study was26.5 � 10 years. There were 44 male and eight
634 Gupta et al.
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists

female patients. There was no predilection for eithereye having a more severe disease (Table 1).
Fourteen out of the 52 JOAG patients (27%) pre-sented with glaucomatous optic neuropathy in onlyone eye (Table 2) and an untreated IOP >22 mmHg inthat eye. Of these nine had corresponding visualfield defects (Table 2). Among these 14 patients, IOPwas consistently <21 mmHg in eight of the 14 felloweyes; the other six eyes had untreated IOP in therange of 22–28 mmHg and were subsequently con-trolled on medical therapy. None of the fellow eyes ofthese 14 patients developed glaucomatous optic neu-ropathy over a 5-year follow up. The disc morpho-metric features as measured on HRT between thefellow and affected eyes were significantly differentfor all parameters (Table 3). The mean deviation inthe involved eye of these 14 patients varied from-1.3 dB to –34 dB (average -14.5 � 14.1 dB). Noneof the fellow eyes showed any glaucomatous visualfield defects. These patients on an average were older(32 � 8.2 years) compared to those who presentedwith a bilateral optic neuropathy (24.4 � 10.6 years)(P = 0.02).
IOP asymmetry
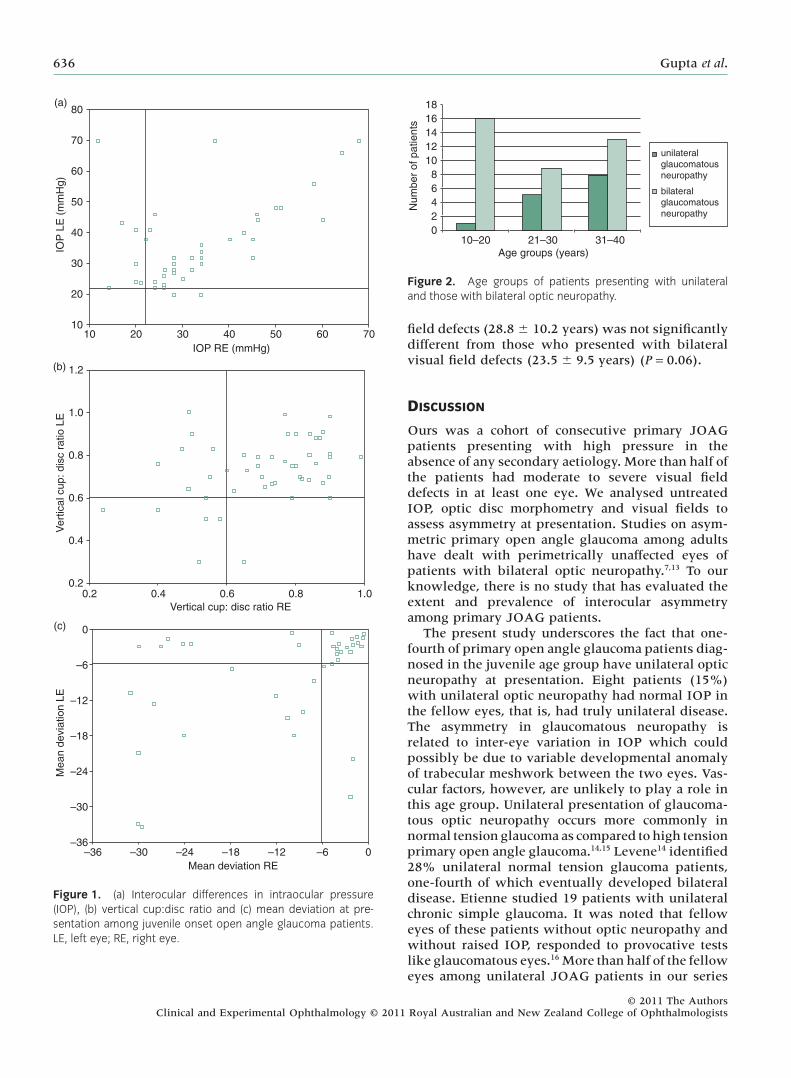
At presentation, 24 patients had an interocular IOPdifference of �2 mmHg, 15 had 3–8 mmHg differ-ence and 13 (25%) patients had an interocular IOPdifference of >8 mmHg (Fig. 1a). The differences inIOP correlated with the vertical cup:disc ratio differ-ences (r = 0.458; P = 0.01) and with the differences inmean deviation between the two eyes (r = 0.378;P = 0.032).
Optic disc asymmetry
Vertical cup:disc ratio asymmetry among JOAGpatients is depicted in Figure 1b.
Figure 2 shows the age groups of patients withunilateral and those with bilateral optic neuropathy.There was no difference in the disc size betweenthe affected (2.56 � 0.49 mm2) and normal felloweyes (2.46 � 0.4 mm2) of patients with unilateralglaucomatous neuropathy (P = 0.3) (Table 3). Aver-age asymmetry of the linear cup:disc ratio in thosewith unilateral glaucomatous neuropathy (0.25 �0.13) was significantly more than those with bilat-eral neuropathy (0.08 � 0.06) (P = 0.01).
Visual field asymmetry
Thirty of the 52(58%) patients presented with amean deviation, worse than -12 dB in at least oneeye at presentation. Twenty out of 52 patients (39%)had glaucomatous visual field defects in only oneeye. The interocular differences in mean deviation of41 patients are given in Figure 1c. In 11 patients thevisual acuity in one eye was less than 6/60 preclud-ing a visual field examination in that eye forcomparison. The age of those with no visual fielddefect in either eye or those with unilateral visual
Table 1. Differences in the clinical parameters between the right and left eyes
Patient characteristic Right eye Left eye P-value
Baseline intraocular pressure (mmHg) 30.8 � 12.3 33.6 � 13.9 0.5Vertical cup:disc ratio 0.71 � 0.16 0.73 � 0.15 0.58Average mean deviation (dB) -11.4 � 11.3 -10.71 � 0.5 0.22Pachymetry (mm) 521 � 28 534 � 31 0.21
Table 2. Laterality of optic disc and visual fields in juvenileonset open angle glaucoma patients at presentation
Visual field defect(VFD)
Optic neuropathy Total
Unilateral Bilateral
No VFD in either eye 5 4 9VFD in one eye 9 11 20VFD in both eyes 0 23 23Total 14 38 52
Table 3. Heidelberg Retina Tomograph characteristics ofaffected and fellow eyes (n = 14) of those with unilateral opticneuropathy
Global parameter Fellow eyes Affected eyes
Disc area (mm2) 2.46 � 0.4 2.56 � 0.49Cup area (mm2) 0.85 � 0.3 1.48 � 0.6†
Rim area (mm2) 1.6 � 0.3 1.2 � 0.5†
Cup disc area ratio 0.34 � 0.1 0.55 � 0.19†
Rim disc area ratio 0.65 � 0.1 0.44 � 0.2†
Cup volume (mm3) 0.27 � 0.18 0.7 � 0.5†
Rim volume (mm3) 0.43 � 0.19 0.21 � 0.2†
Cup depth (mm) 0.32 � 0.1 0.45 � 0.15†
Cup shape measure -0.15 � 0.05 -0.05 � 0.1†
RNFL thickness (mm) 0.26 � 0.07 0.12 � 0.09†
RNFL area (mm2) 1.4 � 0.5 0.9 � 0.7†
Horizontal cup:disc ratio 0.58 � 0.14 0.73 � 0.13†
Vertical cup:disc ratio 0.49 � 0.09 0.7 � 0.12†
FSM 0.96 � 2 -1.9 � 3†
RB 1.2 � 0.8 -0.2 � 1.2†
†The differences between the affected and fellow eyes weresignificant at P < 0.05. FSM and RB, discriminant functions;RNFL, retinal nerve fibre layer.
Interocular asymmetry in JOAG 635
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists
field defects (28.8 � 10.2 years) was not significantlydifferent from those who presented with bilateralvisual field defects (23.5 � 9.5 years) (P = 0.06).
DISCUSSION
Ours was a cohort of consecutive primary JOAGpatients presenting with high pressure in theabsence of any secondary aetiology. More than half ofthe patients had moderate to severe visual fielddefects in at least one eye. We analysed untreatedIOP, optic disc morphometry and visual fields toassess asymmetry at presentation. Studies on asym-metric primary open angle glaucoma among adultshave dealt with perimetrically unaffected eyes ofpatients with bilateral optic neuropathy.7,13 To ourknowledge, there is no study that has evaluated theextent and prevalence of interocular asymmetryamong primary JOAG patients.
The present study underscores the fact that one-fourth of primary open angle glaucoma patients diag-nosed in the juvenile age group have unilateral opticneuropathy at presentation. Eight patients (15%)with unilateral optic neuropathy had normal IOP inthe fellow eyes, that is, had truly unilateral disease.The asymmetry in glaucomatous neuropathy isrelated to inter-eye variation in IOP which couldpossibly be due to variable developmental anomalyof trabecular meshwork between the two eyes. Vas-cular factors, however, are unlikely to play a role inthis age group. Unilateral presentation of glaucoma-tous optic neuropathy occurs more commonly innormal tension glaucoma as compared to high tensionprimary open angle glaucoma.14,15 Levene14 identified28% unilateral normal tension glaucoma patients,one-fourth of which eventually developed bilateraldisease. Etienne studied 19 patients with unilateralchronic simple glaucoma. It was noted that felloweyes of these patients without optic neuropathy andwithout raised IOP, responded to provocative testslike glaucomatous eyes.16 More than half of the felloweyes among unilateral JOAG patients in our series
10 20 30IOP RE (mmHg)
IOP
LE
(m
mH
g)
40 50 60 7010
20
30
40
50
60
70
80(a)
0.2 0.4 0.6 0.8 1.00.2
0.4
0.6
Ver
tical
cup
: dis
c ra
tio L
E
0.8
1.0
1.2
Vertical cup: disc ratio RE
Mean deviation RE
Mea
n de
viat
ion
LE
–36 –30 –24 –18 –12 –6 0–36
–30
–24
–18
–12
–6
0
(b)
(c)
Figure 1. (a) Interocular differences in intraocular pressure(IOP), (b) vertical cup:disc ratio and (c) mean deviation at pre-sentation among juvenile onset open angle glaucoma patients.LE, left eye; RE, right eye.
02468
1012141618
10–20 21–30Age groups (years)
unilateral glaucomatousneuropathy
bilateral glaucomatousneuropathy
Num
ber
of p
atie
nts
31–40
Figure 2. Age groups of patients presenting with unilateraland those with bilateral optic neuropathy.
636 Gupta et al.
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists

were normotensive and all remained perimetricallyunaffected.
What was interesting was that greater bilateralitywas seen among younger patients, whereas thosewith a unilateral optic neuropathy in our study wereolder in age. The pathogenesis of raised IOP in JOAGis ascribed to a goniodysgenesis involving lack ofmaturity of trabecular meshwork and thickened tra-becular beams.17,18 It is reported that developmentalabnormalities of the angle tend to be less obvious asthe age of onset increases.19 It is probable that thosepresenting at a later age may have less severe devel-opmental anomalies of the trabecular meshwork andhence tend to have only one eye involved.
Notably one-fourth of the high pressure JOAGpatients in our study presented with a significantinterocular IOP asymmetry of >8 mmHg at base-line. There was a direct correlation of the asymmetricIOP with disc and visual field asymmetry. UnequalIOP has also been found to correlate with asym-metric visual field defects even in low-tensionglaucoma.1,20,21
Unilateral visual field loss, as defined by theabsence of scotoma in one eye, was seen in 39% ofour JOAG patients. There was a trend towards thosewith bilateral field defects to be younger comparedto those who presented with no defects or with uni-lateral visual field defects. This again could possiblybe due to greater severity of goniodysgenesis amongthose presenting at a younger age. Poinoosawmyet al.6 in contrast found that among adult glaucomapatients (median age 68–70 years), those with uni-lateral field loss at presentation were younger. Theirpatients belonged to an older age group where age-related changes of the trabecular meshwork are thecause of progressive glaucoma.
Characteristics of the visual field defects amongJOAG patients have been described as being sym-metrical with almost equal involvement of the supe-rior and inferior hemifields correlating with thediffuse rim loss secondary to high IOP. The authorsof this study,22 however, did not comment on theinterocular asymmetry in their series. The presentstudy for the first time demonstrates that the extentof structural and functional asymmetry at presenta-tion among primary JOAG patients is considerable.A few JOAG patients like those with primary con-genital glaucoma may present unilaterally. Causativefactors for such a unilateral presentation in JOAGpatients are not fully understood, and furtherresearch is needed to investigate this.
REFERENCES
1. Bayat B, Yazdani S, Alavi A et al. Contributions ofMYOC and CYP1B1 mutations to JOAG. Mol Vis 2008;14: 508–17.
2. Turalba AV, Chen TC. Clinical and genetic character-istics of primary juvenile-onset open-angle glaucoma(JOAG). Semin Ophthalmol 2008; 23: 19–25.
3. Jonas JB, Grundler A. Optic disc morphology in juve-nile primary open-angle glaucoma. Graefes Arch Clin ExpOphthalmol 1996; 234: 750–4.
4. Elder SD. Congenital Deformities. St Louis: CV Mosby,1969.
5. Krieglstein GK. Congenital glaucoma – diagnosis andmanagement. Trans Ophthalmol Soc UK 1986; 105: 549–54.
6. Poinoosawmy D, Fontana L, Wu JX, Bunce CV,Hitchings RA. Frequency of asymmetric visual fielddefects in normal-tension and high-tension glaucoma.Ophthalmology 1998; 105: 988–91.
7. Wang JC, Gazzard G, Foster PJ et al. Interocular asym-metry of visual field defects in primary open angleglaucoma and primary angle-closure glaucoma. Eye2004; 18: 365–8.
8. Gazzard G, Foster PJ, Viswanathan AC et al. The sever-ity and spatial distribution of visual field defects inprimary glaucoma: a comparison of primary open-angle glaucoma and primary angle-closure glaucoma.Arch Ophthalmol 2002; 120: 1636–43.
9. Rhee K, Kim YY, Nam DH, Jung HR. Comparison ofvisual field defects between primary open-angle glau-coma and chronic primary angle-closure glaucoma inthe early or moderate stage of the disease. Korean JOphthalmol 2001; 15: 27–31.
10. Anderson DR. Automated Static Perimetry, 1st edn. StLouis: CV Mosby, 1992.
11. Iester M, Swindale NV, Mikelberg FS. Sector-basedanalysis of optic nerve head shape parameters andvisual field indices in healthy and glaucomatous eyes.J Glaucoma 1997; 6: 370–6.
12. Bathija R, Zangwill L, Berry CC, Sample PA, WeinrebRN. Detection of early glaucomatous structural damagewith confocal scanning laser tomography. J Glaucoma1998; 7: 121–7.
13. Caprioli J, Nouri-Mahdavi K, Law SK, Badala F. Opticdisc imaging in perimetrically normal eyes of glau-coma patients with unilateral field loss. Trans Am Oph-thalmol Soc 2006; 104: 202–11.
14. Levene RZ. Low tension glaucoma: a critical reviewand new material. Surv Ophthalmol 1980; 24: 621–64.
15. Kitizawa Y. Unilateral normal-tension glaucoma.J Glaucoma 1997; 6: 50–5.
16. Etienne R. Unilateral glaucoma. Br J Ophthalmol 1972;56: 254–8.
17. Jerndal T. Goniodysgenesis and hereditary juvenileglaucoma. A clinical study of a Swedish pedigree. ActaOphthalmol Suppl 1970; 107: 3–100.
18. Tawara A, Inomata H. Developmental immaturity ofthe trabecular meshwork in juvenile glaucoma. Am JOphthalmol 1984; 98: 82–97.
19. Jerndal T. Congenital glaucoma due to dominantgoniodysgenesis. A new concept of the heredity ofglaucoma. Am J Hum Genet 1983; 35: 645–51.
20. Crichton A, Drance SM, Douglas GR, SchulzerM. Unequal intraocular pressure and its relation to
Interocular asymmetry in JOAG 637
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists

asymmetric visual field defects in low-tensionglaucoma. Ophthalmology 1989; 96: 1312–14.
21. Cartwright MJ, Anderson DR. Correlation of asym-metric damage with asymmetric intraocular pressurein normal-tension glaucoma (low-tension glaucoma).Arch Ophthalmol 1988; 106: 898–900.
22. Ko YC, Liu CJ, Chou JC, Chen MR, Hsu WM, Liu JH.Comparisons of risk factors and visual field changesbetween juvenile-onset and late-onset primary open-angle glaucoma. Ophthalmologica 2002; 216: 27–32.
638 Gupta et al.
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists