externalization of infection prevention and quality...
TRANSCRIPT

Externalization of Infection Prevention
and Quality Metrics from Acute Care
Hospitals (ACH) to Long-term Care (LTC)
Scott Stienecker MD FACP FSHEA
Medical Director for Epidemiology and Infection Prevention
Parkview Health
Subtitle: Playing nicely in the sandbox to reduce bugs and readmits
Disclosures/Sources • Medical Director of Epidemiology and Infection
Prevention, Parkview Health System, Vibra Hospital
• Owner, LightClean Environmental Decontamination, LLC
• Speaker or Advisor (but none within past 2 years)
• Pfizer Pharmaceuticals
• Cubist Pharmaceuticals
• Research: Forest Labs, Cubist Pharmaceuticals (none
within the past 18 months)

Objectives—Why?
• Why does the government want to improve the
quality of healthcare in the US?
• Why has there been movement in CMS to cost-
sharing and Population Health?
• Why are Acute Hospitals interested in other
people’s business?
• Why were ACOs created?

Outline • Rise of government intervention
• ACA, ACO, CMS, NQF, AHRQ, CMS, NHSN
• White House National Strategy for Combating Antibiotic-
Resistant Bacteria
• Strategy to align care, coordination
• Cost sharing—CMS Models
• CMS 60 and 90 day cap program
• Continuum of care
• Local Responses
• LTC Collaborative
• Sepsis collaborative
• Infection Prevention in LTC
• CHF, Hips, Knees and money
• 30 Day Readmit Programs

SCOPE OF THE PROBLEM







GOVERNMENT RESPONSE


https://www.whitehouse.gov/sites/default/files/docs/carb_national_strategy.pdf
Key Priorities:
• CRE
• MRSA
• Ceftriaxone Resistant
N gonorrhoeae
• C difficile
Players: NSC (National
Security Council), Office of
Science and Technology
Policy, HHS, USDA, DOD,
VA, EPA, USAID

National Strategy for Combating Antibiotic-Resistant
Bacteria
1. Slow the emergence of resistant bacteria
and prevent the spread of resistant
infections
a. --Healthcare—control across the spectrum
b. --Agriculture
i. Limit antibiotics in animal feed
ii. Prevent use without a vet prescription

National Strategy for Combating Antibiotic-Resistant
Bacteria
2. Strengthen national “One-Health”
surveillance efforts to combat resistance a. Detection and Control
b. Integration of public health, veterinary, food and
environmental surveillance
c. Whole genome sequencing

National Strategy for Combating Antibiotic-Resistant
Bacteria
3. Advance development and use of rapid
and innovative diagnostic tests for
identification and characterization of
resistant bacteria a. Point of need testing
b. Drive implementation to point of care

National Strategy for Combating Antibiotic-Resistant
Bacteria
4. Accelerate basic and applied research
and development for new antibiotics, other
therapeutics and vaccines. a. Antibiotics
b. Vaccines
c. Other therapeutics and diagnostics

National Strategy for Combating Antibiotic-Resistant
Bacteria
5. Improve international collaboration and
capacities for antibiotic resistance
prevention, surveillance, control, and
antibiotic research and development

2020 Goals (Money Slide!)
• Reduce incidence of C diff by 50%
compared to 2011
• Reduce CRE by 60% compared to 2011
• Maintain CTX-resistant NG to <2%
• Reduce MDRO Pseudomonas by 35%
• Reduce MRSA by 50%
• Reduce MDR-TB by 15%

SO, HOW DO WE DO THAT?
CMS Innovation Models

http://innovation.cms.gov/initi
atives/index.html#views=mo
dels

Hovering over the item
will tell you the:
Stage
# Participants
Category
Authority
links

CMS Innovation Models • 59 programs in 6 areas – Announced, under development, ongoing,
or no longer active
• Accountable Care Organizations (shared savings programs)-11 programs
9 active
• Bundled Payments for Care Improvement (10- 5 active)
• Model 2
• Model 3
• Model 4
• Primary Care Transformation (9- 6 active)
• Initiatives focused on the Medicaid and CHIP population (8- 6 active)
• Initiatives to Accelerate the Development and Testing of New Payment
and Service Delivery Models (13- 4 active)
• Initiatives to Speed the Adoption of Best Practices (7- 4 active)
http://innovation.cms.gov/initiatives/index.html#views=models

CMS Innovation Programs of Interest
• Comprehensive ESRD Care Initiative
• Next Generation ACO Model
• Nursing Home Value-based Purchasing Demonstration
• BPCI (Bundled Payments for Care Improvement) 30, 60, 90 days
cap
• Model 2: Retrospective Acute & Post Acute Care Episodes • Money to the hospital, covers all acute services PLUS post-acute stay
• Model 3: Retrospective Post Acute Care Episodes Only • Money goes to the LTC facility and covers only the post-acute stay
• Model 4: Retrospective Acute Care Episodes Only • Money to the Acute hospital and the bundle pays everyone
• Medicare Coordinated Care Demonstration (no longer active)
• Community-based Care Transitions Program
• Partnership for Patients
Innovation.cms.gov/initiatives/bundled-payments/index.html

CMS Innovations Model 3
Features CMS Innovation Models
• 48 different clinical conditions
• Triggered by acute hospital stay with
initiation of the bundle with the start of the
LTC stay
• Bundle for all services for 30, 60, or 90
days

48 Conditions covered under
Innovation Models • Acute myocardial infarction
• Amputation
• Atherosclerosis
• Automatic implantable cardiac defibrillator generator or
lead
• Back and neck except spinal fusion
• Cardiac arrhythmia
• Cardiac defibrillator
• Cardiac valve
• Cellulitis
• Cervical spinal fusion
• Chest pain
• Chronic obstructive pulmonary disease, bronchitis/asthma
• Combined anterior posterior spinal fusion
• Complex non-Cervical spinal fusion
• Congestive heart failure
• Coronary artery bypass graft surgery
• Diabetes
• Esophagitis, gastroenteritis and other digestive disorders
• Double joint replacement of the lower extremity
• Fractures femur and hip/pelvis
• Gastrointestinal hemorrhage
• Gastrointestinal obstruction
• Hip and femur procedures except major joint
• Lower extremity and humerus procedure except hip, foot,
femur
• Major bowel
• Major cardiovascular procedure
• Major joint replacement of the lower extremity
• Major joint replacement of upper extremity
• Medical non-infectious orthopedic
• Medical peripheral vascular disorders
• Nutritional and metabolic disorders
• Other knee procedures
• Other respiratory
• Other vascular surgery
• Pacemaker
• Pacemaker Device replacement or revision
• Percutaneous coronary intervention
• Red blood cell disorders
• Removal of orthopedic devices
• Renal failure
• Revision of the hip or knee
• Sepsis
• Simple pneumonia and respiratory infections
• Spinal fusion (non-Cervical)
• Stroke
• Syncope and collapse
• Transient ischemia
• Urinary tract infection

Expected Changes in Mandatory Reporting
• Crystal Ball Time!
• Mandatory Flu vaccine for all HCW
• Mandatory reporting of CRE, pan-
resistant Pseudomonas, and MDRO-
Acinetobacter
• Sepsis Bundle 3 hr.
• Sepsis Bundle 6 hr.
http://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2014-
Fact-sheets-items/2014-08-04.html

Expected Changes in Mandatory Reporting • NHSN
• CAUTI and CLABSI will move to house-wide as of 1/1/15
• Antibiotic Use will become required
• Increasing reporting of VAE requiring an EMR and electronic surveillance
• VBP
• Process indicators will decrease, outcomes and efficiency indicators will increase
• 1% withhold in 2014 will increase to 2% by 2017
• Mandatory Flu Vaccination for HCW
• IPPS and LTCH PPS update reductions for HAC, VBP and
Readmissions Reductions Programs
• Mandatory reporting of Sepsis Bundles
• Increasing demand for denominators requiring surveillance
programs

VALUE BASED PURCHASING


EXTERNALIZED INFECTION
PREVENTION IN THE ECF
Sarah Y. Won, L. Silvia Munoz-Price, Karen Lolans, Bala Hota, Robert A. Weinstein, Mary K. Hayden, and for the Centers for Disease Control and Prevention
Epicenter Program Emergence and Rapid Regional Spread of Klebsiella pneumoniae Carbapenemase–Producing Enterobacteriaceae Clin Infect Dis. (2011)
53 (6): 532-540

COMMON ECF CONCERNS

ECF, LTACH Concerns
• When to check urines
• Culture on admission
• Maximizing resident freedom—role of the
Individualized Infection Prevention
Program (IIPP)
• When to stop isolation?
• C Diff prevention—role of probiotics
• Expensive antibiotics

Acute Care Hospital concerns about ECFs
• 30 day readmission rates
• Acute Length of Stay (and early transition)
• Transmission of infections contributing to
readmission
• Sepsis
• CHF
• Quality Indicators

LTC Quality Indicators to Consider • Infection Logs, line lists
• Look for gene sequences, not just organisms
• Flu Vaccination Rates
• Staff
• Residents
• TB Conversions
• Patients with Isolation Status Changes
• Med errors
• STAC Rate—Sudden transfer to acute care
• Sepsis
• Hips/Knees—time to independent function

Long Term Care Collaborative
• Hosted at Parkview Quarterly
• Review results of initiatives
• Give all institutions an opportunity to play
in our sandbox
• Forum to determine the “community
standard”

ENVIRONMENTAL TESTING

ATP Testing
• ATP is in all living things, even if killed. It is one of the components of intracellular energy transfer. Cotton fibers will give high readings.
• <30 is considered clean.
• In my tests, 30-150 suggests that the item has been cleaned recently.
• 150-250-fairly dirty—you can do better!
• >250 is filthy!
• Although we typically grow common skin bacteria, if an item isn’t getting cleaned of those germs, think how likely you could spread pathogens, such as C diff, Acinetobacter or MRSA?

This keyboard looks
like it has never been
cleaned!
Nurse on a Stick. Who
cleans it, and How
does this get cleaned?

• ECG machine was filthy
• Hadn’t been cleaned recently (if
ever)
• Vitals machine with high ATP and
high colony counts suggest no
recent cleaning.
• Thermometer was dirty as well.

Phone with MSSA

Cleaned Room
Pt Call Light
ATP: 910
This call light was grossly
contaminated with skin flora
and bodily secretions. It has
coagulase negative staph and
bacilli. The ATP reading
appears indicative of picking
up living microbes on the
surface of the call light.

Hospital—Terminally
Cleaned Patient Room
• Bed rail very clean.
• Grab Bar with very high levels, but also had cotton towels hanging over the rail.
• >20 colonies, not that clean, either. Suspect that there is cotton fiber contamination as well as bacteria present.
• No pathogens recovered.

Tips and Tricks
• Test cleaned rooms to see if EVS is
missing any places
• Orphaned Equipment
• Phones, call buttons, underside of over-
bed tables
• Test dirty rooms to see how far things
spread
• Serratia—Who’s cleaning the pail?

INFECTIONS


ESBL, KPC and CRE (what are they and why do
they matter?)
• Mandatory reportable (possibly) by
September
• Health department Tracking

Figure 1: Distribution of CRE Isolates 2013
and 2014 (N=220)
0
10
20
30
40
50
60
70
80
90
100
Citrobacter
spp.
Enterobacter
spp.
E. coli K.
pneumoniae
Klebsiella spp. Proteus spp. S. marcescens
Nu
mb
er o
f Is
ola
tes
CRE Isolates
2013
2014
From: ISDH—personal communication

Figure 2: Sources Containing CRE isolates
2013 and 2014 (N=220)
0
10
20
30
40
50
60
Urine Wound Blood Respiratory
Nu
mb
er o
f Is
ola
tes
Source
2013
2014
From: ISDH—personal communication

Handouts
• ISDH CRE Submission Form
• CRE Submission Criteria
SEPSIS

February 2015- Sepsis Pilot Update
• 14 in Sepsis Pilot – 50 % participation from intent
• Pilot Participants as of February 2015:
• Ashton Creek
• Lutheran Life Villages – Kendallville
• Heritage Park
• Heritage – FW
• Millers Merry Manor
• Saint Anne’s Home
• Town House • Woodview
• Signature Care

Post Acute Care
Parkview 2014:
All patient discharge
SNF 12.87
PAC 14
For Age >65
SNF 27.6
PAC 29.99

Skilled Nursing Facility Landscape
Sg2
1/3 SNF
patients have a
care-related
adverse event
Ave $15,000/stay
Non-profit SNF
5.4% margin
For profit SNF
Margin 16.1%
Reliance on NPs
Staff shortages
Ave 83% occupancy
ACH SNF typically
at 62% loss
SNF->reducing
LOS, move home
or rehab

TRANSITIONAL CARE PILOT
FOR SEMI-ACUTE PATIENTS
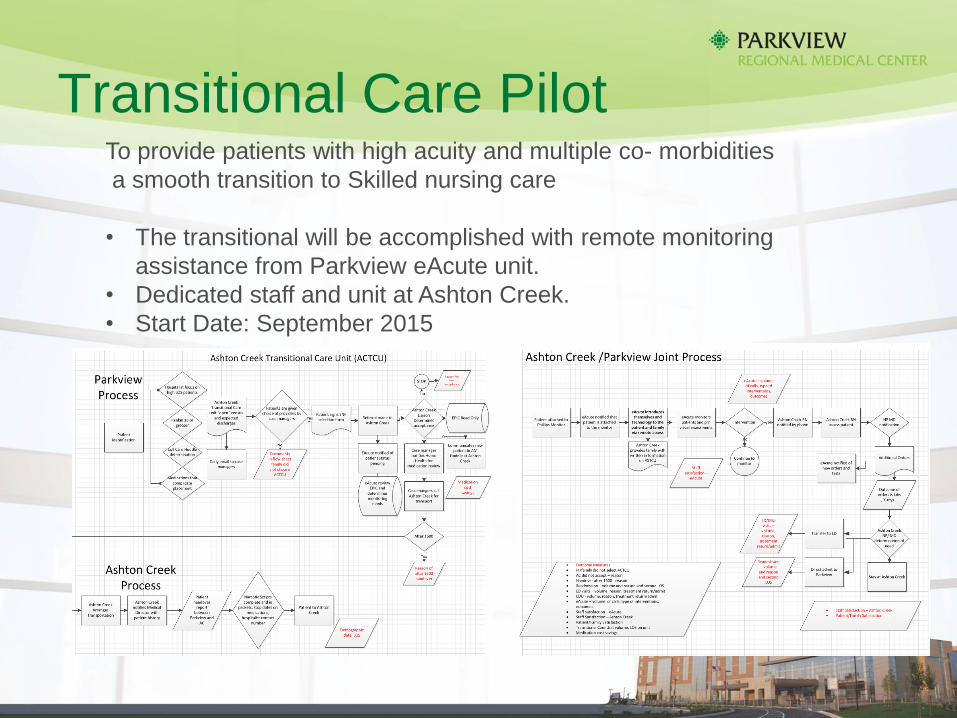
Transitional Care Pilot To provide patients with high acuity and multiple co- morbidities
a smooth transition to Skilled nursing care
• The transitional will be accomplished with remote monitoring
assistance from Parkview eAcute unit.
• Dedicated staff and unit at Ashton Creek.
• Start Date: September 2015

ECF INTERVENTION
PROGRAM

Response Time Month Patients Average
time of
notified to
order in
hours
Numbers
orders written
at time of
notification
(%)
Time from X-
ray
performed to
results in
hours
Time from lab
drawn to
results in
hours
Time for
antibiotic
from order
given in
hours
Time from lab
results to
antibiotics
given in hours
December
2014
26 1.8 10 (38%) 1.6 2.1 8.4 4
January
2015
19 1.5 8 (42%) .78 (47
minutes)
2.9 4.6 2.6
February
2015
16 .75 6 (37%) .88 (53
minutes)
1.4 9.3 1.78
ECF Chart review and focused intervention:
Marked decrease in time to notification, time to X-ray, time from lab draw to
antibiotic.
Time for antibiotic from order to “given” didn’t change, but overall time to antibiotic
did drop

Lactic Acid Tests
Month Patients Lactic Acid
Test
performed
Lactic Acids
results 2 or
greater
December 2014 26 32 11
January
2015
19 15 6
February
2015
16 17 7

Sepsis Long Term Care Data
Note increase in
sepsis cases, but
marked decrease in
septic shock.
CMI dropped. A lot.

December – February 2014
Resident Data N = 61 December 2014 increase in respiratory illness in Fort Wayne
• Parkview volume statistics by Sepsis ICD9 codes stable – no increase in volume
• 3 Hospitalizations • 2 – Hospice
• 1-Cardiac
• Long Term Care Volumes • Sepsis (lowest sepsis ICD9) – increased by 4%
• Sever Sepsis (mid range Sepsis ICD9) decreased by 4%
• Septic Shock(highest sepsis level ICD9) – decreased by 9%

Case Study
• Long term care resident
• 12-26-15 Lactic Acid 4.2 • Protocol started with IV and fluids and antibiotic
• 12-27-15 Lactic Acid 3.6
• 12-29-15 Lactic Acid 1.8
Resident remained at facility

Heart Failure Unit • 6 bed dedicated unit – Heritage Park
• Estimated start date July 2015
• Maintain 80% occupancy
• Parkview Medical Director
• Parkview protocols
• Aggressive post acute discharge Care Advising

Bibliography
• 1. White House Strategy for Combating Antibiotic-
Resistant Bugs
https://www.whitehouse.gov/sites/default/files/docs/carb_
national_strategy.pdf
• 2. http://innovation.cms.gov/initiatives/Advance-
Payment-ACO-Model/
• 3. Parkview Health—Internal Data
• 4. https://www.federalregister.gov/articles
/2015/02/27/2015-03751/patient-protection-and-
affordable-care-act-hhs-notice-of-benefit-and-payment-
parameters-for-2016

Bibliography
• 5. http://innovation.cms.gov/initiatives/BPCI-Model-2/
• 6. http://innovation.cms.gov/initiatives/BPCI-Model-3/
• 7. Fiscal Year 2015 Policy and Payment Changes for Inpatient
Stays in Acute-Care Hospitals and Long-Term Care Hospitals --
http://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-
sheets/2014-Fact-sheets-items/2014-08-04.html
• 8. Special Section: Aging and Infectious Diseases: Robert A. Bonomo
Multiple Antibiotic-resistant Bacteria in Long-term-care Facilities: An
Emerging Problem in the Practice of Infectious Diseases Clin Infect Dis.
(2000) 31 (6): 1414-1422
• 9. http://www.health.gov/hai/prevent_hai.asp#hai_plan.
• 10. Indiana State Department of Health