eye and vision assessment - … ocular diagnoses encountered by school nurses conjunctivitis •...
TRANSCRIPT
1
Eye and Vision Assessment
Nicole Quinn, OD, FAAONew England College of Optometry
Pediatric Health Assessment ConferenceBoston Children’s Hospital
August 16, 2017
No financial disclosures
Acknowledgment:
Kathy Majzoub, RN, MBAPrevent Blindness AmericaDirector, Northeast Region
Overview• Ocular Diagnoses Encountered By School Nurses
Conjunctivitis (Bacterial, Viral, Allergic) Contact Lens Related Red Eye Chalazion & Hordeolum Eye Trauma: Foreign Body, Abrasions, Chemical Exposure,
Contusions Sports Related Eye Injury Refractive Error: Hyperopia, Myopia, Astigmatism Strabismus Amblyopia
• Eye and Vision Assessment and Screening

2
Ocular Diagnoses Encountered By School Nurses
Conjunctivitis• “Pink Eye”
• Common cause of red, irritated eyes
• Inflammation of the thin, transparent membrane that covers the white part of the eye
• Types– Viral: Contagious!– Bacterial: Contagious!– Allergic: NOT Contagious!
3
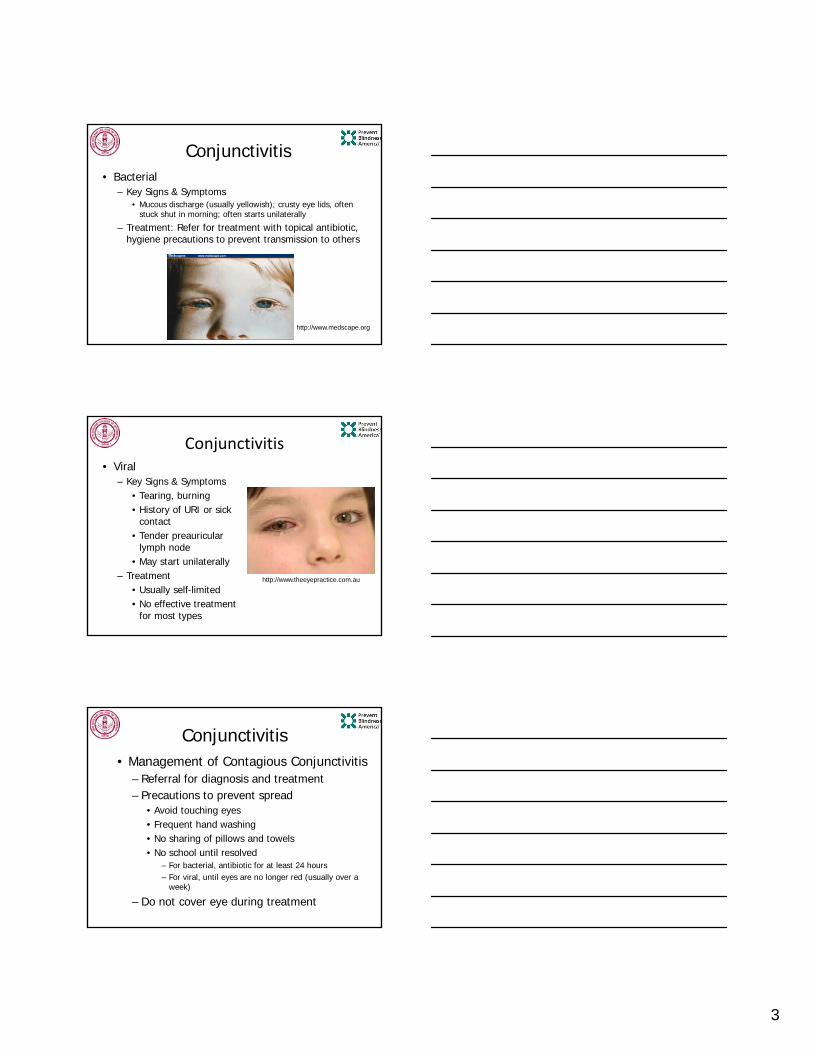
Conjunctivitis• Bacterial
– Key Signs & Symptoms• Mucous discharge (usually yellowish); crusty eye lids, often
stuck shut in morning; often starts unilaterally
– Treatment: Refer for treatment with topical antibiotic, hygiene precautions to prevent transmission to others
http://www.medscape.org
Conjunctivitis• Viral
– Key Signs & Symptoms• Tearing, burning• History of URI or sick
contact• Tender preauricular
lymph node• May start unilaterally
– Treatment• Usually self-limited• No effective treatment
for most types
http://www.theeyepractice.com.au
Conjunctivitis• Management of Contagious Conjunctivitis
– Referral for diagnosis and treatment– Precautions to prevent spread
• Avoid touching eyes• Frequent hand washing• No sharing of pillows and towels• No school until resolved
– For bacterial, antibiotic for at least 24 hours– For viral, until eyes are no longer red (usually over a
week)
– Do not cover eye during treatment

4
Conjunctivitis
• Allergic– Key Signs & Symptoms: Itching; history of seasonal
allergies; usually both eyes affected– Treatment: eliminate inciting agent; frequent
washing of hair, clothes, pillows; cool compresses; OTC and prescription topical medication, oral antihistamines
http://www.geteyesmart.org/eyesmart/diseases/conjunctivitis.cfm
Contact Lens-Related Red Eye• Contact lens wearers are
more likely to get severe eye infections– Red flags: eye pain,
sensitivity to light, mucous discharge, white spot on eye
– Remove contact lens immediately
– If symptoms persist, must be evaluated by an eye doctor ASAP to rule out corneal ulcer (can lead to permanent vision loss)
www.medicinenet.com
Contact Lens-Related Red Eye• Preventing eye infections in contact
lens wearers– No sleeping in contacts– No swimming– No tap or bottled water– No saliva– No sharing contacts (even colored contacts with
no prescription)– Wear contacts no longer than 12 hours per day– Use cleaning solution NOT saline solution for
disinfecting contacts

5
Hordeolum (Stye)• Infection of oil producing
glands in eye lid• Key Signs & Symptoms
– Red, tender bump on eye lid
• Treatment– Usually self-limited– Lid hygiene, warm
compresses– If multiple or severe,
refer for medication
http://www.health.state.mn.us/divs/fh/mch/webcourse/vision/chalazion.cfm
Chalazion• Bump on eye lid caused
by chronic infection of eye lid glands
• Key Signs & Symptoms– Palpable bump on eye
lid, NOT tender• Treatment
– Warm compresses– If large, consider
referral for medication or surgical removal
http://www.health.state.mn.us/divs/fh/mch/webcourse/vision/chalazion.cfm
Eye Trauma
• 1/3 of all eye injuries happen in children under 17 years of age– 75% in males
• Commonly associated with– Sports– Paintball– Fireworks– UV Exposure
• Child with monocular vision must useeyeglasses for protection

6
Sports Related Eye Injury
• 25 percent of estimated 2.4 million eye injuries that occur in the United States each year happen during sports and recreational activities
• Every 13 minutes an ER treats a sports-related eye injury
Eye Trauma
• Common symptoms
– Eye pain
– Feels like something is in eye
– Red eye
– Tearing
– Sensitivity to light
– Swelling, bruising or laceration of eyelid
• Careful history is essential in determining the type and severity of injury and the most appropriate treatment and follow‐up
Eye Trauma: Foreign Body
www.consultantlive.com
www.eyecasualty.co.uk
• Rinse eye with sterile saline• Refer for additional treatments
Ex. Removal, topical antibiotic

7
Eye Trauma: Corneal Abrasion
• Scratched cornea
• Very painful
• Treatment
– Generally, not recommended to cover eye
– Refer for topical antibiotics
– Control painwww.insighteyespecialists.com
Eye Trauma: Chemical Exposure
• IMMEDIATELY, rinse eye with sterile saline – If no sterile saline
available, then use running water
– May need to rinse for 20-30 minutes
• Refer to evaluate extent of damage
www.sharecare.com
Eye Trauma: Contusions• “Black Eye”
• Bruising of eye lid, usually due to blunt trauma
• Look for damage to eye structures
– Subconjunctival hemorrhage (bleeding under conjunctiva)
– Hyphema (bleeding inside eye)
photoree.com
casereports.bmj.com

8
Orbital Fracture
• Signs & Symptoms
– Swollen, tender eye lid
– Eyes not moving in all directions; pain during eye movement
– Double vision
– Numbness, creptius
• Treatment
– Refer for complete eye exam and imaging (usually CT)
http://www.bheyelids.com/before_and_after_orbital_fractures_photos.asp
Penetrating Ocular Injuries
• Signs & Symptoms
– Pain, reduced vision, loss of fluid from eye
– Contents of eye outside of globe
– Abnormal pupil shape, hyphema
• Do not put pressure on eye
• Do not remove penetrating object
• Transfer to ER
http://webeye.ophth.uiowa.edu/eyeforum/trauma.htm
Tips for School Nurses: Eye Trauma
• Thorough history is essential
• Use observational skills to determine type and extent of injury
• Tools needed to evaluate/assist patient
– Sterile saline to rinse eyes
– Visual acuity chart: has vision been affected?
– Light to better observe eye structures
• Establish a plan for emergency and non‐emergency referrals

9
Vision Screening• Without early detection and
treatment, vision deficits in childhood can lead to– Permanent vision loss– Learning difficulties– Delayed sensory, motor,
cognitive & social-emotional development
• Screening is designed to detect the most common vision problems in children– Refractive error– Strabismus– Amblyopia
Screenings do not detect ALL vision problems so pay attention to the ABC’s and refer, if necessary
ABC’s: Appearance
• Crossed or misaligned eyes
• Watering eyes
• Red-rimmed, encrusted or swollen eyelids
• Drooping eyelid
• Sties or infections
• Presence of white pupil
• Possible eye injury
ABC’s: Behavior
• Squinting or frowning
• Tilting head to one side
• Excessive blinking or eye rubbing
• Closing or covering one eye
• Body rigid when looking far
• Thrusting head forward or backward

10
ABC’s: Complaints
• Headaches, nausea or dizziness
• Blurred or double vision
• Burning, scratchy, painful or itchy eyes
• Blurry vision at looking up after close work
• Unusual sensitivity to light
“Normal” Vision
• Ideally, light enters the eye and focuses exactly on the retina, allowing clear vision
• If this occurs, no glasses are needed
Refractive ErrorIf light entering the eye does not focus on the retina, blurry
vision occurs. Corrective lenses are prescribed to compensate for the refractive error in the eye’s visual system.
Hyperopia
Myopia

11
Refractive Error: Myopia (Nearsightedness)
• Distant objects blurred
• Increases through school-age years and stabilizes in early adulthood
• Unable to see people’s faces from a distance or read board at school
• May squint eyes to see better
Refractive Error: Hyperopia (Farsightedness)
• Objects blurrier at near than at distance
• Mild hyperopia is normal in young children and commonly decreases as the child grows
• Only when significant amount is present are corrective glasses prescribed at a young age
Refractive Error: Astigmatism• Irregular corneal shape
causes more than one point of focus in the eye
• Distorted vision distance and near
• May get headaches or eye strain; may squint to improve vision
12
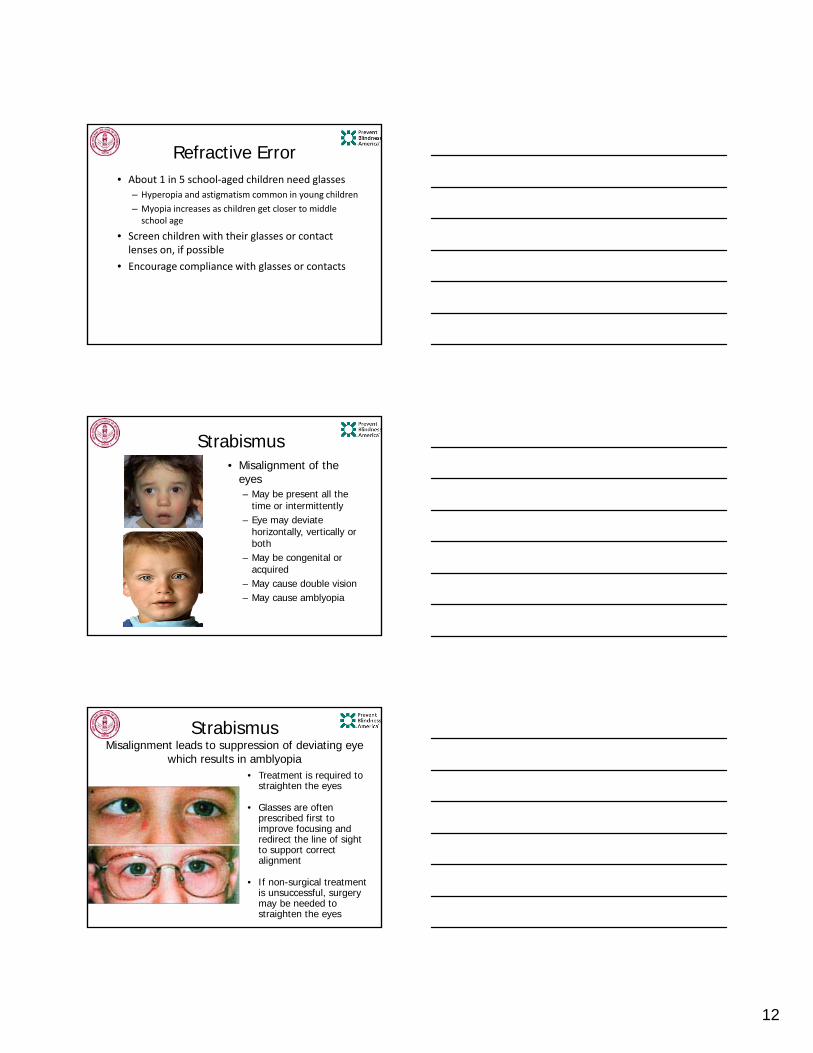
Refractive Error• About 1 in 5 school‐aged children need glasses
– Hyperopia and astigmatism common in young children
– Myopia increases as children get closer to middle school age
• Screen children with their glasses or contact lenses on, if possible
• Encourage compliance with glasses or contacts
Strabismus• Misalignment of the
eyes– May be present all the
time or intermittently– Eye may deviate
horizontally, vertically or both
– May be congenital or acquired
– May cause double vision– May cause amblyopia
StrabismusMisalignment leads to suppression of deviating eye
which results in amblyopia• Treatment is required to
straighten the eyes
• Glasses are often prescribed first to improve focusing and redirect the line of sight to support correct alignment
• If non-surgical treatment is unsuccessful, surgery may be needed to straighten the eyes

13
Amblyopia
• Amblyopia (“Lazy Eye”)– “amblyos” dull– “opia” vision
• Develops birth - 8 years
• Leading cause of blindness in children and adults under 45 years
• Any condition that causes the brain to receive images of unequal quality from the two eyes can lead to amblyopia
Amblyopia• Most common causes of amblyopia
– Refractive Error (especially if one eye has a significantly higher refractive error than the other)
– Strabismus (misalignment of eyes)– Deprivation (something blocking vision)
• Ex. Ptosis or Cataract
Amblyopia Treatment
Correct underlying vision problem (refractive error, cataract, strabismus, etc.)
Correct amblyopia by retraining the brain (ex. patching)

14
Vision Screening: Who and Where
According to the MA Mandate and AAP Guidelines:
All children beginning at birth are assessed by PCP
All children beginning at age 3 or 4 years have additional vision assessment through the use of screening protocols by PCP designee and annually thereafter
All children enrolled in Head Start beginning at age 3 years are evaluated using vision screening protocols (5% of MA preschoolers)
All children in public kindergarten, annually through elementary school, once in middle school, and once in high school, are evaluated with vision screening protocols by school nurse or designee
Primary Care Provider Bright Futures
• 0-3 Years: History, external, red reflex, light reflex, fixation, tracking, cover test
• 3-5 Years: All of the above AND visual acuity and stereopsis– Instrument-based
screening acceptable
• Age 6, 8, 10 years and three times during teen years
MA : Screening State or Exam State?
• MA: An Act Relative to Eye Examinations for Children, 2004: Within 30 days of start of K, child must show pass on vision screen or proof of eye exam conducted in previous 12 months. Children with Neurodevelopmental delay, and children who fail thevision screening, are referred for a comprehensive eye exam by an ophthalmologist or optometrist.

15
First Step: Screening or Exam?“Neurodevelopmental Delay”
MA School Health Manual
• Law requires proof of a comprehensive eye exam, performed by a licensed optometrist or ophthalmologist, for children diagnosed with neurodevelopmental delay
• Term “neurodevelopmental delay” may be subject to interpretation, but is likely to include children born pre-term or low birth weight and children with neurological disorders such as cerebral palsy, Down Syndrome, multiple handicaps or developmental delay
National Center for Children’s Vision and Eye Health
• Children who are at high risk, such as those born prematurely or with known neurodevelopmental disorders in any area (ex. hearing impairment, motor abnormalities such as cerebral palsy, cognitive impairment, autism spectrum disorders, and speech delay), should be referred directly to an eye care provider for further evaluation
THE O’s?
Ophthalmology• Four years post undergraduate education (MD)• Four years internship/residency• One or two year optional fellowship: cornea,
pediatric/strabismus, glaucoma, retina, ocular immunology, etc.
Optometry• Four years post undergraduate education (OD)• One year optional residency: pediatric, geriatric, low
vision rehabilitation, vision therapy
Confidentiality? • HIPAA : doctors outside of school and school nurse can
communicate about child’s health condition without parent permission
• FERPA (school health staff operate under FERPA) does not allow school nurse to communicate health information that originates in school (for example vision screening results or results of physical exam that was completed at school) to doctors outside of school unless parent gives permission
• FERPA does allow school nurse to discuss health condition with classroom teacher and others as a “need to know” issue
• MA School Health Policy states that if an eye exam was done based on results of a school screening, the eye doctor is required to send exam results to the school and school health also requests that results be sent to the PCP
16
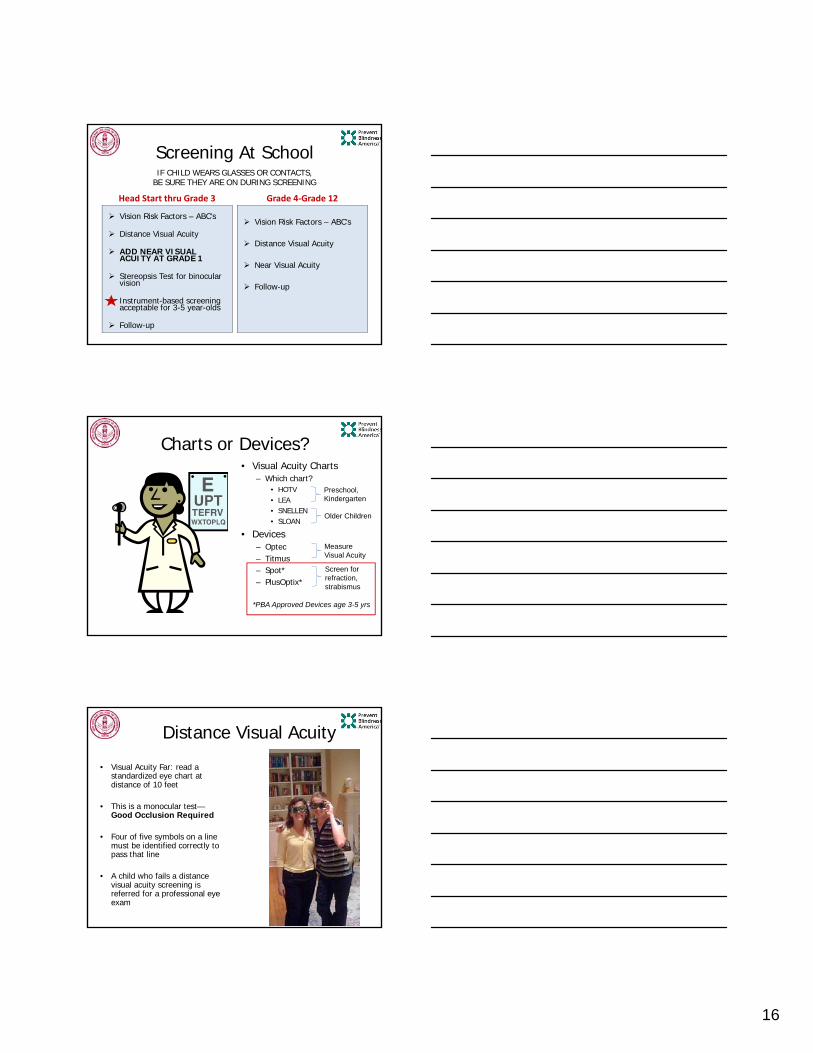
Screening At School
Head Start thru Grade 3
Vision Risk Factors – ABC’s
Distance Visual Acuity
ADD NEAR VISUAL ACUITY AT GRADE 1
Stereopsis Test for binocular vision
Instrument-based screening acceptable for 3-5 year-olds
Follow-up
Grade 4‐Grade 12
Vision Risk Factors – ABC’s
Distance Visual Acuity
Near Visual Acuity
Follow-up
IF CHILD WEARS GLASSES OR CONTACTS, BE SURE THEY ARE ON DURING SCREENING
Charts or Devices?• Visual Acuity Charts
– Which chart?• HOTV• LEA• SNELLEN• SLOAN
• Devices– Optec– Titmus– Spot*– PlusOptix*
Screen for refraction, strabismus
Measure Visual Acuity
Preschool, Kindergarten
Older Children
*PBA Approved Devices age 3-5 yrs
Distance Visual Acuity
• Visual Acuity Far: read a standardized eye chart at distance of 10 feet
• This is a monocular test—Good Occlusion Required
• Four of five symbols on a line must be identified correctly to pass that line
• A child who fails a distance visual acuity screening is referred for a professional eye exam

17
Distance Visual Acuity:Passing Lines
Age Passing Line
MA: 48 months and younger 20/40
MA: Older than 48 months 20/30
2 Line or Greater Difference in Acuity
RDE Stereopsis Test• In the child whose eyes are not
working together, the brain is unable to fuse the two images from each eye into one clear image
• Child must identify the card with the “E” four consecutive times at a distance of 48 inches– Must use polarized glasses– Test at correct distance!
Near Acuity-Add at 1st Grade
• LEA, HOTV, SNELLEN
• Distance: 14-16 inches (string)
• Allowed to miss one per line
• Passing line is 20/30
• Both eyes together

18
Red Flags for School Nurses:When to Refer to Eye Doctor
• When child is suspected of having contagious conjunctivitis, contact lens related red eye or sustains an eye injury
– Referral ASAP if vision loss, eye pain, structural damage has occurred
• At diagnosis of “neurodevelopmental delay” or other diagnoses associated with vision problems
• Appearance, Behavior, Complaint related to vision
• Fail on MA Vision Screening Protocol
Resources
Healthy Eyes Eyeglass Program: [email protected]
For approved vision screening equipment:www.goodlite.com/Details.cfm?ProdID=502&category=7&Secondary=37www.schoolhealth.com/preventblindness
References‐www.childrensvisionmassachusetts.org‐www.nationalcenter.preventblindness.org‐www.preventblindness.org‐http://www.aao.org/eye‐health/tips‐prevention/injuries‐Gerstenblith AT, Rabinowitz MP. (2012) The Wills eye manual: office and emergency room diagnosis and treatment of eye disease. 6th edition. Philadelphia:Wolters Kluwer/Lippincott Williams & Wilkins.‐Kaiser PK, Neil J, Pineda III R. (2014) The Massachusetts eye and ear infirmary illustrated manual of ophthalmology. 4th edition. New York: Elsevier, Saunders.
Questions