f v a v a l journal of vaccines & vaccination j · contagious mastitis is caused by bacterial...
TRANSCRIPT

Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
Review Article Open Access
Tiwari et al., J Vaccines Vaccin 2013, 4:2 DOI: 10.4172/2157-7560.1000176
Keywords: Bovine mastitis; Prevention; Therapy; Immunological;Non-immunological
IntroductionMajor advances in the fields of animal breeding, animal nutrition
and husbandry practices have played a significant role in increasing the global milk yield over the last 2 decades [1] meeting the overwhelming demand for milk and milk products. There have been continuous changes in the predominance of etiological of mastitis [2], greater understanding of the host responses to intra-mammary infections [3,4] and treatment regimens leading to adoption of various control and prevention measures. Regardless, the problem of mastitis continues to pose the greatest challenge to the dairy industry worldwide.
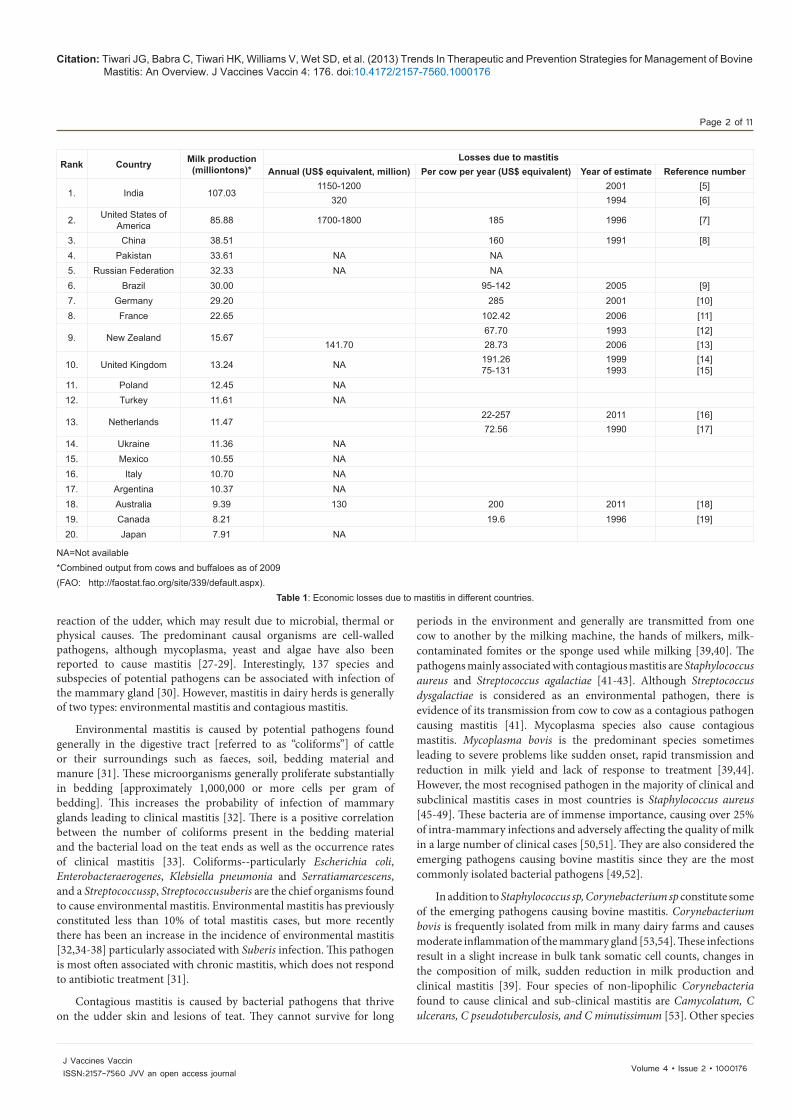
Mastitis is one of the most economically devastating diseases of dairy cattle particularly for the back yard farmers in developing world (Table 1), with different levels of economic losses reported by different countries [5-19].
More than $130 million is lost by the Australian dairy industry ($A200/cow/year) every year due to poor udder health resulting in reduced milk production that is mainly associated with mastitis [18]. A herd without an effective mastitis control programme may witness morbidity as high as 40% with infection, on an average of two quarters of the mammary gland [18]. Of the various clinical manifestations, subclinical mastitis is economically the most important due to its long term effects on milk yields [20-22]. Huge economic losses are also
incurred due to unmarketable milk or milk-products contaminated with antibiotic residues originating from treatment in the developing nations as well as from the use of antibiotics as growth promoters particularly in dairy feedlots in the developed world. The prolonged use of antibiotics in the treatment of mastitis has led to the additional problem of emergence antibiotic resistant strains, hence the constant concern about the resistant strains entering the food chain [23-25]. Many organisms associated with mastitis also have zoonotic importance and can cause diseases like brucellosis, tuberculosis, leptospirosis, Q-fever etc. [26].
Etiology of MastitisMastitis (Mast: breast, it is: inflammation) is an inflammatory
*Corresponding author: Trilochan Mukkur, School of Biomedical Sciences, Faculty of Health Sciences, Curtin Health Innovation Research Institute, Curtin University, Bentley, Perth, Western Australia 6102, Australia, E-mail: [email protected]
Received December 14, 2012; Accepted January 29, 2013; Published January 31, 2013
Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Copyright: © 2013 Tiwari JG, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview JullyGogoi Tiwari1, Charlene Babra1, Harish Kumar Tiwari2, Vincent Williams1, Sharon De Wet3, Justine Gibson4, Adrian Paxman1, Eleanor Morgan1, Paul Costantino1, Raju Sunagar5, Shrikrishna Isloor6 and Trilochan Mukkur1*1School of Biomedical Sciences, Faculty of Health Sciences, Curtin Health Innovation Research Institute, Curtin University, Bentley, Perth, Western Australia 6102, Australia2Base Victualling Yard, Homi Bhabha Road, Colaba, Mumbai 400005, India3Department of Employment, Economic Development and Innovation, Queensland Government, Brisbane 4002, Queensland, Australia4The University of Queensland, School of Veterinary Science, Gatton, Qld, 4343, Australia5Ella Foundation, Genome Valley, Shameerpet Mandal, Hyderabad 500 078, India6Veterinary College, Karnataka Veterinary, Animal and Fisheries Sciences University, Hebbal, Bangalore 560024, India
AbstractMastitis is one of the most economically significant diseases for the dairy industry for backyard farmers in
developing countries and high producing herds worldwide. Two of the major factors impeding reduction in the incidence of this disease is [a] the lack of availability of an effective vaccine capable of protecting against multiple etiological agents and [b] propensity of some of the etiological agents to develop persistent antibiotic resistance in biofilms. This is further complicated by the continuing revolving shift in the predominant etiological agents of mastitis, depending upon a multitude of factors such as variability in hygienic practices on farms, easy access leading to overuse of appropriate or inappropriate antibiotics at suboptimal concentrations, particularly in developing countries, and lack of compliance with the recommended treatment schedules. Regardless, Staphylococcus aureus and Streptococcus uberis followed by Escherichia coli, Streptococcus agalactiae has become the predominant etiological agents of bovine mastitis followed Streptococcus agalactiae, Streptococcus dysagalactiae, Klebsiella pneumonia and the newly emerging Mycoplasma bovis. Current approaches being pursued to reduce the negative economic impact of this disease are through early diagnosis of infection, immediate treatment with an antibiotic found to either inhibit or kill the pathogen(s) in vitro using planktonic cultures and the use of the currently marketed vaccines regardless of their demonstrated effectiveness. Given the limitations of breeding programs, including genetic selection to improve resistance against infectious diseases including mastitis, it is imperative to have the availability of an effective broad-spectrum, preferably cross-protective, vaccine capable of protecting against bovine mastitis for reduction in the incidence of bovine mastitis, as well as interrupting the potential cross-species transmission to humans. This overview highlights the major etiological agents, factors affecting susceptibility to mastitis, and the current status of antibiotic-based therapies and prototype vaccine candidates or commercially available vaccines against bovine mastitis as potential preventative strategies.
Journal of Vaccines & VaccinationJour
nal o
f Vaccines & Vaccination
ISSN: 2157-7560
Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 2 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
reaction of the udder, which may result due to microbial, thermal or physical causes. The predominant causal organisms are cell-walled pathogens, although mycoplasma, yeast and algae have also been reported to cause mastitis [27-29]. Interestingly, 137 species and subspecies of potential pathogens can be associated with infection of the mammary gland [30]. However, mastitis in dairy herds is generally of two types: environmental mastitis and contagious mastitis.
Environmental mastitis is caused by potential pathogens found generally in the digestive tract [referred to as “coliforms”] of cattle or their surroundings such as faeces, soil, bedding material and manure [31]. These microorganisms generally proliferate substantially in bedding [approximately 1,000,000 or more cells per gram of bedding]. This increases the probability of infection of mammary glands leading to clinical mastitis [32]. There is a positive correlation between the number of coliforms present in the bedding material and the bacterial load on the teat ends as well as the occurrence rates of clinical mastitis [33]. Coliforms--particularly Escherichia coli, Enterobacteraerogenes, Klebsiella pneumonia and Serratiamarcescens, and a Streptococcussp, Streptococcusuberis are the chief organisms found to cause environmental mastitis. Environmental mastitis has previously constituted less than 10% of total mastitis cases, but more recently there has been an increase in the incidence of environmental mastitis [32,34-38] particularly associated with Suberis infection. This pathogen is most often associated with chronic mastitis, which does not respond to antibiotic treatment [31].
Contagious mastitis is caused by bacterial pathogens that thrive on the udder skin and lesions of teat. They cannot survive for long
periods in the environment and generally are transmitted from one cow to another by the milking machine, the hands of milkers, milk-contaminated fomites or the sponge used while milking [39,40]. The pathogens mainly associated with contagious mastitis are Staphylococcus aureus and Streptococcus agalactiae [41-43]. Although Streptococcus dysgalactiae is considered as an environmental pathogen, there is evidence of its transmission from cow to cow as a contagious pathogen causing mastitis [41]. Mycoplasma species also cause contagious mastitis. Mycoplasma bovis is the predominant species sometimes leading to severe problems like sudden onset, rapid transmission and reduction in milk yield and lack of response to treatment [39,44]. However, the most recognised pathogen in the majority of clinical and subclinical mastitis cases in most countries is Staphylococcus aureus [45-49]. These bacteria are of immense importance, causing over 25% of intra-mammary infections and adversely affecting the quality of milk in a large number of clinical cases [50,51]. They are also considered the emerging pathogens causing bovine mastitis since they are the most commonly isolated bacterial pathogens [49,52].
In addition to Staphylococcus sp, Corynebacterium sp constitute some of the emerging pathogens causing bovine mastitis. Corynebacterium bovis is frequently isolated from milk in many dairy farms and causes moderate inflammation of the mammary gland [53,54]. These infections result in a slight increase in bulk tank somatic cell counts, changes in the composition of milk, sudden reduction in milk production and clinical mastitis [39]. Four species of non-lipophilic Corynebacteria found to cause clinical and sub-clinical mastitis are Camycolatum, C ulcerans, C pseudotuberculosis, and C minutissimum [53]. Other species
Rank Country Milk production(milliontons)*
Losses due to mastitisAnnual (US$ equivalent, million) Per cow per year (US$ equivalent) Year of estimate Reference number
1. India 107.031150-1200 2001 [5]
320 1994 [6]
2. United States of America 85.88 1700-1800 185 1996 [7]
3. China 38.51 160 1991 [8]4. Pakistan 33.61 NA NA5. Russian Federation 32.33 NA NA6. Brazil 30.00 95-142 2005 [9]7. Germany 29.20 285 2001 [10]8. France 22.65 102.42 2006 [11]
9. New Zealand 15.6767.70 1993 [12]
141.70 28.73 2006 [13]
10. United Kingdom 13.24 NA 191.2675-131
19991993
[14][15]
11. Poland 12.45 NA12. Turkey 11.61 NA
13. Netherlands 11.4722-257 2011 [16]72.56 1990 [17]
14. Ukraine 11.36 NA15. Mexico 10.55 NA16. Italy 10.70 NA17. Argentina 10.37 NA18. Australia 9.39 130 200 2011 [18]19. Canada 8.21 19.6 1996 [19]20. Japan 7.91 NA
NA=Not available*Combined output from cows and buffaloes as of 2009 (FAO: http://faostat.fao.org/site/339/default.aspx).
Table 1: Economic losses due to mastitis in different countries.

Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 3 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
of Corynbacterium isolated from cases of clinical mastitis in sheep are C mastiditis and C camporealensis [55,56].
Recent studies have revealed that coagulase negative staphylococci (CoNS) isolated from teat skin, teat canal, and vagina as well as from the coat and the nostril comprises a major interest area of mastitis causal organisms [57,58]. Mastitis in heifers at calving is mainly caused by CoNS. More than 50 species and subspecies are included in this group [52]. Staphylococcus epidermidis, Staphylococcus simulans, Staphylococcus saprophyticus, Staphylococcus hyicus, Staphylococcus warneri, Staphylococcus chromogenes, Staphylococcus scrimiand Staphylococcus xylosus are the commonly encountered species of CoNS in bovine mastitis [59]. The various species of CoNS isolated from bovine mastitis cases show varied pathogenicity, antimicrobial susceptibility and virulence factors [60,61].
Mastitis caused by fungi and yeast is uncommon. The fungi commonly associated with mastitis are Candidasp, Trichosporonsp, Saccharomyces sp and Aspergillussp [62]. A very rare case of mastitis caused by yeast like fungus, Geotrichumcandidum has also been reported [62]. Though the incidence of mycotic mastitis is very low, serious problems may arise when it occurs in enzootic form [63].
Factors Affecting the Susceptibility to MastitisThe large number of predisposing factors that contribute to the
emergence of mastitis in dairy cattle may be physiological, genetic, pathological or environmental [64] described below:
Age of the cow
It has been demonstrated that occurrence of mastitis in infected quarters increases with age incows [39,65-68], being the highest at 7 years of age [69]. This may be due to an increased cellular response to intramammary infection or due to permanent udder tissue damage resulting from the primary infection. Efficient innate host defence mechanisms of the younger animals are one possibility that makes them less susceptible to infection [70]. However, at least one study conducted using 4133 cattle including both cross-bred and non-descriptive breeds revealed the highest risk of occurrence of mastitis to be between the ages of 4-6 years, followed by the age group between 2-4 years, with the least occurrence noted between 6-8 years of age [71]. Interestingly it was noted in this study that the crossbred animals were 2.55 times more susceptible to mastitis than the non-descriptive ones.
Inherited features of the bovine
Various genetic traits may also have a considerable impact upon the susceptibility of the animal to mastitis. These genetic traits include the natural resistance, teat shape and conformation, positioning of udders, relative distance between teats, milk yield and fat content of milk. High milk yielders with higher than average fat content are reported to be more susceptible to mastitis [72-74]. The conformation of the udder and shape of the teat are inherited characteristics that may also affect susceptibility to mastitis. Cows with elongated teats are more vulnerable to mastitis infection than cows with inverted teat ends [75,76]. Broad udders, lower hind-quarters and teats placed widely help the infectious agent and should be selected against it [77]. Another important predisposing factor for mastitis is super numerous teats, which provide additional reservoirs for potential pathogens leading to manifestation of mastitis.
Stage of lactation
The incidence of mastitis is reported to be higher immediately after
parturition, early lactation and during the dry period, especially the first 2-3 weeks [69,78-80] due probably to increased oxidative stress and reduced antioxidant defence mechanisms during early lactation [81]. An increase in somatic cell numbers or count (SCC) which are mainly neutrophils, is observed immediately after parturition, which remains high for a few weeks irrespective of the presence or absence of infection [82,83]. This increased SCC is the cow’s natural first line of defence to prepare for the onset of the new lactation. Relatively recent studies have revealed that cows in late lactation always show a higher than average SCC than that seen at other stages of the lactation period [84], potentially representing increased subclinical infection, leading to a fall in milk production.
Mammary regression
There are significant functional changes in the udder during the early and late lactation and dry period, which affect the cow’s susceptibility to infections. Lactating cows under stress show premature mammary regression. Such a condition compromises udder’s natural defence mechanisms [85,86] leading to invasion of the teat canals by potential pathogens. The same condition prevails during the healing process of lesions because the resistance to causal agents remains less effective.
Milking machine
Extraneous factors such as the milking habits of farmers and faulty milking machines favour the pathogens to gain access to mammary gland and proliferate, potentially leading to mastitis [87]. In farms where machines are employed for milking it is important to maintain physiologically optimal pressure [50 kPa for most machines], because pressures in excess of this may lead to injury in the teat [88]. Fluctuations in the pressure due to inadequate vacuum reserve must be avoided to prevent occurrence of mastitis. Proper installation as well as the correct maintenance of milking machines is important to avoid an inadequate vacuum level, teat and tissue damage and incomplete milking [89]. The vacuum level created by the vacuum pump is another important factor for complete and high quality milking. Experiments have shown that a teat subjected to a vacuum level of 10.5-12.5 inches at the time of peak milk flow results in rapid, complete and high quality milk yield, and the teat suffers minimum physical pressure [90]. Two-chambered teat cups are found to be better than single chambered teat cups in regard to achieving complete milking as well as fewer incidences of teat injuries [91]. However, there is a report of increased risk of both contagious and environmental mastitis causing pathogen due to machine induced changes, which widen the orifice of the teat canal in cows [92].
Nutrition
The quality and plan of nutrition appears to be an important factor that influences clinical manifestation of mastitis in heifers and cows [93] although no relationship between the incidence of mastitis and either high energy or high protein feed in cows has been reported [94,95].
Vitamin E is one of the important supplements in dairy feed to boost the immune response of cows [96] as it has been reported to enhance the neutrophil function as well as the phagocytic properties of neutrophils after parturition [97]. Vitamin E is often combined with selenium, which acts as an anti-oxidant by preventing oxidative stress [98,99]. A number of investigations have demonstrated that neutrophils of selenium fed cows are more effective at killing mastitis causing microorganisms than those not supplemented with selenium [100-102].
Beta-carotene and Vitamin A have also been found to be effective

Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 4 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
in preventing the occurrence of mastitis, most probably due to their antioxidant and immune-enhancing properties and contribution mucosal surface integrity of the mammary gland respectively [103,104]. Zinc and copper are also important nutritional elements that contribute mammary gland health by promoting cellular repair, wound healing and reduction in SCC [103,105,106] aided by increases in metallothionein synthesis with antioxidant potential. Various studies have shown that feed supplemented with copper and fed to heifers reduces the severity of subclinical mastitis as well as clinical mastitis induced by Escherichia coli [107,108].
Weather and climate
The incidence of mastitis is greatly influenced by the weather conditions and prevailing climatic conditions. Heat, humidity, cold and draught are the important predisposing factors [109-114]. A higher incidence of mastitis has been reported to occur particularly during summer rainy months [113-117]. As heat and humidity increases, so does the bacterial multiplication as well as the load of pathogens in the environment [118]. Conversely, an alternative study has reported a higher incidence of coliform mastitis during the cold months of the year when the temperature was reported to be less than 21°C [119,120].
Strategies for Therapy and Prevention of MastitisAntibiotics
Antibiotics ranging from narrow to broad spectrum have been used extensively over the past 40 years in the control of bovine mastitis [42,83]. However, because of the emerging antibiotic resistance believed to be probably due to their overuse [121-128] and the induction of prolonged persistent antibiotic resistance in biofilms by many mastitis-causing pathogens, as demonstrated recently for S aureus isolated from cases of bovine mastitis [129], effectiveness of antibiotic therapy has been compromised. As such the control of bovine mastitis has become one of the most challenging problems on dairy farms today. Cows suffering from mastitis are culled due to high SCCs and repeated occurrence of clinical mastitis. Although culling and selective antibiotic therapy have been found to cause a reduction in the manifestation of clinical mastitis [130], dairy farmers are often reluctant to cull affected the devastating financial impact on backyard farmers due to losses in milk production as is often the case in developing countries.
Intramammary infections have been traditionally treated with systemic or intramammary antibiotic therapy [131,132]. Despite scheduling treatment regimens to prolong the availability of appropriate antibiotics for an extended period of time in the infected area [131,133], the cure rates of mastitis particularly for S aureus infections have been reported to vary from 0% to 80% [131,133-135]. This is presumably due to the induction and persistence of biofilm-associated antibiotic resistance [129] depending upon the intensity of infection as reflected by SCC counts and management practices [136-139]. Milking animals with a SCC of less than 1 million showed greatest success of antibiotic therapy while those with a higher count responded poorly [134,140]. This is notwithstanding the fact that some antibiotics used for the treatment of mastitis such as penicillin, oxytetracycline, lincomycin and neomycin may affect the phagocytic properties of polymorphonuclear leukocytes (PMN) by altering the oxidative burst property of PMN [141-143] leading to a recurrence of intramammary infections.
Bacteriophage therapy for mastitis associated infections
Given the problems associated with antibiotic therapy of mastitis, development of alternative treatment strategies for management of
clinical and sub-clinical mastitis are warranted. One such alternative treatment is bacteriophage therapy, which uses pathogen specific bacteriophages in the treatment of a bacterial infection. Recent interest in phage therapy in veterinary medicine was sparked by some early success in the treatment of E. coli infections in animal models including a chicken model for respiratory infections [144], a mouse model for meningitis [145] and a calf model for diarrhoea [146,147]. However, the few studies that have been carried out using bacteriophages to treat mastitis caused by S aureus infection have yielded variable results. While intramammary infusion of bacteriophage into S aureus infected quarters of lactating dairy cattle did not show significant protection [148,149]. Kwiatek et al. [150] isolated and characterised a bacteriophage from the milk of cows suffering from mastitis with broad-spectrum activity against methicillin- resistant S aureus (MRSA). It is suggested that additional research is required to explore the therapeutic potential of bacteriophages to treat clinical and subclinical mastitis associated bacterial infections.
Mastitis vaccines
It is beyond the scope of this overview to describe detailed experimental approaches undertaken for the development of vaccines against bovine mastitis caused by the major bacterial pathogens thus far. In this overview, a brief description of the vaccines currently being formulated with the hope of reducing the incidence mastitis on-farm or backyard farming, and promising prototype vaccine candidates of the mastitis-associated pathogens, is presented. The use of vaccination particularly with autogenous killed whole cell vaccines to control infectious diseases on-farm in dairy cattle is common, and vaccination against mastitis pathogens is no exception. Several efforts have been made to develop a vaccine against mastitis, but few have claimed satisfactory outcomes [151-158], neither in the field nor on backyard farms. It is clear that a single vaccine will not prevent mastitis caused by the plethora of pathogens and their different mechanisms of pathogenesis [159].
Vaccines against Staphylococcus aureus: Numerous attempts to develop a vaccine against Staphylococcus aureus using varied approaches have been made [47]. These include whole organism vaccines [154], DNA vaccine encoding clumping factor A [156], live attenuated (aroA) S aureus [160], capsular polysaccharide (CPS)-protein conjugate vaccines [161,152] and recombinant S aureus mutated enterotoxin type C [162].
Somato-Staph®/ Lysigin vaccine has been used in the United States of America since the mid-1970s [163,164]. This is a polyvalent whole cell vaccine comprising 5 phage types of lysed cultures. It reduces the clinical severity of bovine mastitis and lowers the SCC in milk [165]. However, it failed to prevent occurrence of new infections [163,166]. “MASTIVAC-1”, which is composed of three different field strains, is another vaccine against S aureus that initially showed promising results in field trials [154]. However, various field trials of these vaccines against S aureus mastitis have shown that, although clinical severity of the disease is reduced, new infections are not prevented from taking hold. A trivalent vaccine composed of S aureus serotype 5, 8 and 336 lysates was reported to stimulate the production of IgG1 and IgG2 in serum in heifers and the vaccines formulated with adjuvant such as Freund’s incomplete or aluminium hydroxide produced more IgG2 than IgG1 [167]. However, the efficacy of the vaccine against intramammary infections caused by S aureus was not evaluated. O’Brien et al. [168] reported that a conjugate vaccine composed of S aureus capsular polysaccharide type 5, 8 and 336 combined with poly(DL-lactide-coglycolide) microspheres enhanced phagocytosis and produced high

Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 5 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
antibody titre in cows. Nour El-Din et al. [156] reported a high level of antibody response in dairy cattle when vaccinated with DNA vaccine encoding ClfA. Promising results were also reported in a vaccine trial in dairy heifers vaccinated with a virulent mutant RC122 S aureus strain [157]. Strong and specific levels of IgG were reported in both milk and blood of the vaccinated heifers. A trial of vaccine composed of extracellular component from S aureus in twelve gestating cows resulted in a reduction of multiplication of S aureus in the mammary gland [169]. However, there was no difference observed in terms of clinical symptoms in both control and vaccinated animals. In a recent study, a conjugate vaccine composed of ClfA and deacetylated poly-N-β-(1,6)-acetyl-glucosamine (dPNAG) of S aureus was reported to be highly immunogenic in a murine bacteraemia model [170]. The same combination of the vaccine was also found to be immunogenic in multiple animal species including goat, rabbit and rhesus monkey in the same laboratory [170].
Vaccines against coliform bacteria: Coliforms (Ecoli, Klebsiella sp.) are etiological agents of environmental mastitis. Coliform mastitis generally causes clinical mastitis mostly during the peri-parturient period [171,172]. Early investigations used heterogeneous oligosaccharide antigens derived from Ecoli to develop a vaccine against coliform mastitis. These vaccines were administered during the non-lactating period with the aim of preventing mastitis in subsequent lactations [173,174]. These vaccines reduced the severity of infection initially, but their effect gradually diminished over time [175]. J-5Bacterin, Mastiguard™ and J Vac® are the three vaccines available in the market against coliform mastitis [164]. A new vaccine, Startvac (Hipra), has recently been made available in the market targeting not only coliforms but also coagulase-negative staphylococci and S aureus. J-5Bacterin, also known as the E coli J5 vaccine, is composed of the J5 mutant strain of E coli. Cows vaccinated with this vaccine showed a significant reduction of clinical mastitis cases under field conditions [176,177]. Only 20% of the vaccinated animals showed clinical infections, although there was no difference in the incidence of new coliform mastitis cases among the vaccinated compared to the non-vaccinated animals [177]. However, no vaccines against mastitis caused by K pneumoniae are available in the marketplace.
Vaccines against Streptococcus uberis: The high global incidence of clinical mastitis due to S uberis, an environmental pathogen, has warranted the development of vaccines to prevent mastitis caused by this specific etiological agent [178]. Repeated immunisation in experimental animals with killed S uberis vaccine resulted in a significant reduction in the number of bacteria in milk but failed to reduce the SCC count [179]. Vaccination with bacterin from S uberis demonstrated protection against S uberis mastitis caused by the homologous strain but failed to protect against a heterologous strain [180]. In another study, plasminogen activator derived from Suberis showed promising results in reducing the severity of infection [178,181]. In a recent study, cows vaccinated with a recombinant adhesion molecule of S uberis (rSUAM) by the subcutaneous route showed an increased antibody titre in milk and serum, which was found to reduce adherence and internalisation of the organism into the epithelial cells of the mammary gland in vitro [182].
Numerous efforts to develop S uberis vaccines to prevent mastitis have not proven successful and no commercial vaccines for prevention of this infection are available in the market. No immune response is induced in the mammary gland even after intramammary infection with S uberis, which further complicates the development of a vaccine [183]. Sortase-anchored proteins derived from S uberis may
be potential candidates for vaccine as they are important potential virulence antigens contributing to the pathogenesis of bovine mastitis [184]. Recently, Denis et al. [185] reported that cows which developed mastitis after environmental exposure to S uberis developed bactericidal antibodies and T cells in blood and milk, resulting in an increased level of interferon-gamma (IFN-γ) that was specific for in-vitro killing of S uberis [185]. Clearly, research on the development of an effective vaccine against S uberis – associated mastitis is highly warranted.
Vaccines against Streptococcus agalactiae and Streptococcus dysgalactiae: Streptococcus agalactiae is an important pathogen for humans [infants, pregnant women and immune compromised elderly patients] has nine serotypes [159], each having a serologically distinct polysaccharide capsule; a capsular conjugate vaccine, using the capsule of predominant serotypes, has been evaluated in Phase 2 trials with encouraging results. However, little information available on the capsular types of this pathogen which also causes mastitis in the dairy population. Furthermore, no commercially attractive prototypevaccine candidates are available against mastitis caused by Sagalactiae or S dysgalactiae despite many attempts that have been made to develop an effective vaccine against these pathogens. Recently, a recombinant vaccine composed of S aureus cluming factor A (ClfA) and surface immunogenic protein (rSip) of S agalactiaewas shown to increase the serum IgG1 antibody titre in experimental mice immunised by an intramammary route [158]. Not much effort in developing a vaccine against bovine mastitis due to S dysagalactiae has been made either. However, the surface proteins GapC and Mig of Streptococcus dysgalactiae were reported to be potential protective antigens against bovine mastitis [186].
Genetic selection of cattle for resistance to clinical mastitis
Breeding production animals for resistance to infectious diseases is not new [187], but generally the breeding of farm animals has been confined to enhancement of production traits such as increased milk production. Such selection, while enhancing milk production, has been reported to increase the incidence of many infectious diseases including bovine mastitis [188,189]. In attempts to overcome this problem, a strategy based on enhancing the overall immune response-- including antibody-mediated immune response (AMIR) and cell-mediated immune response (CMIR)--has been proposed [190]. However, a negative genetic correlation between AMIR and CMIR [191] has been recorded, making a balanced genetic selection more complex and requiring further investigations.
Ancillary non-specific strategies for prevention of mastitis
Non-specific immunostimulants against mastitis: In the absence of the availability of effective commercial vaccines for prevention of mastitis caused by multiple pathogens, attempts are continually being made to evaluate the potential of non-specific immune stimulants for prevention of bovine mastitis [192]. Lysate of Corynebacterium cutis has been considered as one of the non-specific immune stimulants against mastitis. There are reports of a reduction in SCC [193] in the milk of dairy cows receiving a subcutaneous injection of lysate of C cutis possibly due to the boosting of the immune system of those animals [194]. Intramuscular injection of C cutis to pregnant ewes resulted in an increased level of IgG in serum on the 140th day and in colostrum up to 3 days post-parturition [195]. Clearly, further studies on the potential of the non-specific immune stimulants are warranted.
Lactation therapy: Treatment of mastitis during lactation with antibiotics is referred to as “lactation therapy”, which is used by many

Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 6 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
producers to reduce the clinical signs of mastitis and bring back the normal milk production of cows. This therapy has proven useful in reducing the SCC in milk and thereby maintains the quality of milk [196-198]. However, lactation therapy for subclinical mastitis is not suggested as it is not economically viable and shows poor efficacy [198]. Factors such as SCC in milk during treatment, stage of lactation, immune status of the animal, age of the cow and type of pathogen also play an important role in the success or failure of lactation therapy [196,199,200]. New intramammary infections in cows have been shown to respond better to antibiotic therapy than chronic infections [201,202], and young animals show better response to treatment than older animals [203-207]. Spontaneous cure by lactation therapy for clinical as well as subclinical mastitis caused by S aureus is very rare [197-208]. Lactation therapy in chronic clinical cases of mastitis caused by S aureus has been found equally ineffective [130]. However, an extended period of treatment with antibiotics at therapeutic levels has been reported to yield better cure rates for clinical mastitis caused by S aureus [205]. A serious drawback of this therapy is the loss of milk because of antibiotic residues.
Dry cow therapy: Dry cow therapy with antibiotics has been suggested as one of the options to control intramammary infections and prevent development of mastitis [209,210]. During the dry period, the cow is at the greatest risk of acquiring new intramammary infections with both gram-positive and gram-negative environmental or contagious pathogens [211-213]. It has been reported that about 61% of new infections are acquired during this period [213]. Treatment during dry period is advantageous because it allows treatment of infections with antibiotics without the need to discard milk from treated quarters. Antibiotics are administered towards the end of lactation [214] and may remain in the udder in concentrations high enough to kill pathogenic bacteria for 20-70 days, depending upon the kind of formulations that are used. The antibiotic has an enhanced penetration due to prolonged exposure and the probability of curing intramammary infections increases markedly, unless resistance to new antibiotics is acquired by the invading pathogen’s biofilm formation in the udder [129]. Dry cow therapy has been reported to eliminate almost 100% of mastitis caused by S agalactiae [210,215]. However, dry cow therapy is comparatively less successful to prevent S aureus mastitis than streptococcal mastitis [209]. The cure rate of dry cow treatment against S aureus mastitis was reported as approximately 50% and vaccination against this pathogen during the dry period may enhance the antibiotic efficacy [213]. Dry cow therapy for a period of two weeks showed significant reduction in the number of clinical mastitis cases due to infection with S dysgalactiae and S uberis [216].
Teat sealer: The development of internal and external teat sealants for use during the dry period is a promising progress towards control of mastitis and its aftermath [118,217-221]. External teat sealants such as DryFlex and Delaval also showed potential in reducing new infections of the mammary gland during the dry period [134]. However, lack of persistence is the main drawback of external teat sealers [222]. Bismuth subnitrate as an internal teat sealer used in field conditions was reported to reduce new infections upto tenfold [217,223]. Internal teat sealer used with long acting antibiotics during the dry period showed a 30% and 33% reduction in new intramammary infections and incidence of clinical mastitis, respectively [103]. Bismuth subnitrate combined with cloxacillin as dry cow therapy demonstrated reduction in both clinical and subclinical cases of mastitis [220,221]. There are several studies that have demonstrated the usefulness of OrbeSeal, an internal sealer in reducing new infections of the mammary gland in lactating animals [219,224].
ConclusionsBovine mastitis is an economically important disease due to its
involvement in the quantity and quality of milk production. The dairy industry all over the world suffers from significant economic losses incurred due to mastitis. Application of hygienic measures during milk collection, using milking machines, lactation and dry cow therapy, teat sealers, dietary supplements and culling are likely to reduce but not control the incidence of both clinical and subclinical mastitis. The effects of mastitis on dairy cattle health and milk production highlight an urgent need to develop effective strategy of prevention and control. The constantly changing predominance of etiological agents in different geographical locations must be considered while adopting and developing mastitis control strategies. Research aimed at developing an effective broad-spectrum universal vaccine capable of providing protection against the predominant environmental and contagious pathogens causing bovine mastitis is highly warranted for reduction of the incidence of bovine mastitis worldwide.
Acknowledgements
Financial support of the Australia India Strategic Research Fund, DIISR, Canberra, Australia, The Department of Biotechnology, India and the School of Biomedical Sciences, CHIRI, Curtin University, Australia is gratefully acknowledged. Special thanks are due to Dr. Nagendra Hegde of the Ella Foundation for offering suggestions on the content of this review.
References
1. Shook GE (2006) Major advances in determining appropriate selection goals. J Dairy Sci 89: 1349-1361.
2. Zadoks R, Fitzpatrick J (2009) Changing trends in mastitis. Ir Vet J 62: S59-70.
3. Oviedo-Boyso J, Valdez-Alarcon JJ, Cajero-Juarez M, Ochoa-Zarzosa A, Lopez-Meza JE, et al. (2007) Innate immune response of bovine mammary gland to pathogenic bacteria responsible for mastitis. J Infect 54: 399-409.
4. Atalla H, Wilkie B, Gyles C, Leslie K, Mutharia L, et al. (2010) Antibody and cell-mediated immune responses to Staphylococcus aureus small colony variants and their parental strains associated with bovine mastitis. Dev Comp Immunol 34: 1283-1290.
5. Dua K (2001) Incidence, aetiology and estimated loss due to mastitis in India- An update. Ind Dairy man 53: 41-48.
6. Singh PJ, Singh PB (1994) A study of economic losses due to mastitis in India. Ind J Dairy Sci 47: 265-272.
7. Bramley AJ, Cullor JS, Erskine RJ, Fox LK, Harmon RJ, et al. (1996) The mastitis problem. Current concepts of bovine mastitis. (4thedn), Madison: National Mastitis Council.
8. Fang WH, Hu SH, Jiang CS, Huang IQ, Liu HR (1991) Bovine mastitis - a Chinese approach to its prevalence, causal pathogens, losses and control. Proceedings of the 6th International Symposium on Veterinary Epidemiology and Economics.
9. Swinkels JM, Hogeveen H, Zadoks RN (2005) A partial budget model to estimate economic benefits of lactational treatment of subclinical Staphylococcus aureus mastitis. J Dairy Sci 88: 4273-4287.
10. Hamann J (2001) Mastitis notes from members countries. Germany Bullt IDF367: 18-21.IDF (1987) Bovine mastitis. Definition and guidelines for diagnosis. Bullt IDF 211: 24.
11. Fourichon C, Seegers H, Beaudeau F, Verfaille L, Bareille N (2001) Health-control costs in dairy farming systems in western France. Livest Prod Sci 68: 141-156.
12. Holdaway R (1993) Bovine mastitis in New Zealand dairy herds. A study commissioned by the National Mastitis Advisory Committee. Thesis submitted to Massey University.
13. Malcolm D, Hook I, Montgomerie B, Winkleman A, Sim S, et al. (2006) The cost of mastitis. Dairy insight research 2005/2006 report of the National Mastitis Advisory Committee.
Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 7 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
14. Bennett R, Christiansen K, Clifton-Hadley R (1999) Preliminary estimates of the direct costs associated with endemic diseases of livestock in Great Britain. Prev Vet Med 39: 155-171.
15. Esslemont RJ, Peeler EJ (1993) The scope for raising margins in dairy herds by improving fertility and health. Br Vet J 149: 537-547.
16. Hogeveen H, Pyorala S, Waller KP, Hogan JS, Lam TJGM, et al. (2011) Current status and future challenges in mastitis research. NMC Annual Meeting Proceedings.
17. Scharenraad MHW, Dijkhuizen AA (1990) Economic losses due to bovine mastitis in Dutch Dairy herds. Neth J Agric Sci 38: 89-92.
18. Dairy Australia (2011) Dairy Australia Strategic Plan 2011-2015.
19. Dekkers JC, Van Erp T, Schukken YH (1996) Economic benefits of reducing somatic cell count under the milk quality program of Ontario. J Dairy Sci 79: 396-401.
20. Rosetti CA (1993) Prevalence of subclinical mastitis caused by Staphylococcus aureus in the Buenos Aires Dairy area and its susceptibility to antibiotics. Vet Argent 10: 323-326.
21. Gogoi J (1997) Public health importance of Staphylococcus aureus isolated from cases of bovine mastitis and milkers. MVSC thesis submitted to Assam Agricultural University, India.
22. Zafalon LF, Nader Filho A, Oliveira JV, Resende FD (2007) Subclinical mastitis caused by Staphylococcus aureus: cost benefit analysis of antibiotic therapy in lactating cows. Arq Bras Med Vet Zootec 59: 577-585.
23. White DG, McDermott PF (2001) Emergence and transfer of antibiotic resistance. J Dairy Sci 84: E151-E5.
24. Virdis S, Scarano C, Cossu F, Spanu V, Spanu C, et al. (2010) Antibiotic Resistance in Staphylococcus aureus and Coagulase Negative Staphylococci Isolated from Goats with Subclinical Mastitis. Vet Med Int 2010: 517060.
25. Collins NA, Moses M, Moneoang SM, Corneleus B (2010) Antibiotic-resistant Staphylococcus aureus isolated from milk in the Mafikeng Area, North West province, South Africa. South Afr J Sci 106: 1-6.
26. Sharif A, Umer M, Muhammad G (2009) Mastitis control in dairy production. J Agril Soc Sci 5: 102-105.
27. Wilson DJ, Gonzalez RN, Das HH (1997) Bovine mastitis pathogens in New York and Pennsylvania: prevalence and effects on somatic cell count and milk production. J Dairy Sci 80: 2592-2598.
28. Barkema HW, Schukken YH, Lam TJ, Beiboer ML, Wilmink H, et al. (1998) Incidence of clinical mastitis in dairy herds grouped in three categories by bulk milk somatic cell counts. J Dairy Sci 81: 411-419.
29. Fox LK, Kirk JH, Britten A (2005) Mycoplasma mastitis: a review of transmission and control. J Vet Med B Infect Dis Vet Public Health 52: 153-160.
30. Watts JL (1988) Etiological agents of bovine mastitis. Vet Microbiol 16: 41-66.
31. Jones GM (2006) Understanding the basics of mastitis. Virginia Cooperative Extension, Publication No. 404-233, Virginia State University, USA, 1-7.
32. Bradley AJ, Green MJ (1997) Clinical mastitis in dairy cows after ‘blitz’ therapy. Vet Rec 141: 179-180.
33. Hogan JS, Smith KL, Hoblet KH, Todhunter DA, Schoenberger PS, et al. (1989) Bacterial counts in bedding materials used on nine commercial dairies. J Dairy Sci 72: 250-258.
34. Boyer PJ (1997) Outbreak of clinical mastitis in dairy cows following ‘blitz’ therapy. Vet Rec 141: 55.
35. Edmondson PW (1997) Clinical mastitis in dairy cows after ‘blitz’ therapy. Vet Rec 141: 108.
36. Bradley AJ, Green MJ (2001) Adaptation of Escherichia coli to the bovine mammary gland. J Clin Microbiol 39: 1845-1849.
37. Bradley AJ, Leach KA, Breen JE, Green LE, Green MJ (2007) Survey of the incidence and aetiology of mastitis on dairy farms in England and Wales. Vet Rec160: 253-258.
38. Dairy Australia (2011) Environmental mastitis increasing.
39. Harmon RJ (1994) Physiology of mastitis and factors affecting somatic cell counts. J Dairy Sci 77: 2103-2112.
40. APHIS (Animal and Plant Health Inspection Service) Info sheet, USDA (2008) Prevalence of contagious mastitis pathogens on U.S. dairy operations, 2007.
41. Smith KL, Hogan JS (1995) Epidemiology of mastitis. Proc 3rd Int Mastitis Seminar, Tel Aviv, Israel, S6: 3-12.
42. Barkema HW, Schukken YH, Zadoks RN (2006) Invited Review: The role of cow, pathogen, and treatment regimen in the therapeutic success of bovine Staphylococcus aureus mastitis. J Dairy Sci 89: 1877-1895.
43. Monecke S, Kuhnert P, Hotzel H, Slickers P, Ehricht R (2007) Microarray based study on virulence-associated genes and resistance determinants of Staphylococcus aureus isolates from cattle. Vet Microbiol 125: 128-140.
44. van der Burgt G, Main W, Ayling R (2008) Bovine mastitis caused by Mycoplasma bovis. Vet Rec 163: 666.
45. Workineh S, Bayleyegn M, Mekonnen H, Potgieter LN (2002) Prevalence and aetiology of mastitis in cows from two major Ethiopian dairies. Trop Anim Health Prod 34: 19-25.
46. Barrett DJ, Healy AM, Leonard FC, Doherty ML (2005) Prevalence of pathogens causing subclinical mastitis in 15 dairy herds in the Republic of Ireland. Ir Vet J 58: 333-337.
47. Middleton JR (2008) Staphylococcus aureus antigens and challenges in vaccine development. Expert Rev Vaccines 7: 805-815.
48. Ericsson Unnerstad H, Lindberg A, Persson Waller K, Ekman T, Artursson K, et al. (2009) Microbial aetiology of acute clinical mastitis and agent-specific risk factors. Vet Microbiol 137: 90-97.
49. Pereira UP, Oliveira DG, Mesquita LR, Costa GM, Pereira LJ (2011) Efficacy of Staphylococcus aureus vaccines for bovine mastitis: a systematic review. Vet Microbiol 148: 117-124.
50. Owens WE, Watts JL, Boddie RL, Nickerson SC (1988) Antibiotic treatment of mastitis: comparison of intramammary and intramammary plus intramuscular therapies. J Dairy Sci 71: 3143-3147.
51. Haveri M (2008) Staphylococcus aureusin bovine intramammary infection: molecular, clinical and epidemiological characteristics. Academic dissertation, submitted to Department of Production Animal Medicine, Faculty of Veterinary Medicine, University of Helsinki, Finland.
52. Pyörälä S, Taponen S (2009) Coagulase-negative staphylococci-emerging mastitis pathogens. Vet Microbiol 134: 3-8.
53. Hommez J, Devriese LA, Vaneechoutte M, Riegel P, Butaye P, et al. (1999) Identification of nonlipophilic corynebacteria isolated from dairy cows with mastitis. J Clin Microbiol 37: 954-957.
54. Haltia L, Honkanen-Buzalski T, Spiridonova I, Olkonen A, Myllys V (2006) A study of bovine mastitis, milking procedures and management practices on 25 Estonian dairy herds. Acta Vet Scand 48: 22.
55. Fernandez-Garayzabal JF, Collins MD, Hutson RA, Fernandez E, Monasterio R, et al. (1997) Corynebacterium mastitidis sp. nov., isolated from milk of sheep with subclinical mastitis. Int J Syst Bacteriol 47: 1082-1085.
56. Fernández-Garayzábal JF, Collins MD, Hutson RA, Gonzalez I, Fernández E, et al. (1998) Corynebacterium camporealensis sp. nov., associated with subclinical mastitis in sheep. Int J Syst Bacteriol 48: 463-468.
57. Pitkälä A, Haveri M, Pyöröla S, Myllys V, Honkanen-Buzalski T (2004) Bovine mastitis in Finland 2001--prevalence, distribution of bacteria, and antimicrobial resistance. J Dairy Sci 87: 2433-2441.
58. Tenhagen BA, Köster G, Wallmann J, Heuwieser W (2006) Prevalence of mastitis pathogens and their resistance against antimicrobial agents in dairy cows in Brandenburg, Germany. J Dairy Sci 89: 2542-2551.
59. Rupp R, Beaudeau F, Boichard D (2000) Relationship between milk somatic-cell counts in the first lactation and clinical mastitis occurrence in the second lactation of French Holstein cows. Prev Vet Med 46: 99-111.
60. Zadoks RN, Schukken YH (2006) Use of molecular epidemiology in veterinary practice. Vet Clin North Am Food Anim Pract 22: 229-261.
61. Taponen S, Pyöröla S (2009) Coagulase-negative staphylococci as cause of bovine mastitis- not so different from Staphylococcus aureus? Vet Microbiol 134: 29-36.
62. Chahota R, Katoch R, Mahajan A, Verma S (2001) Clinical bovine mastitis caused by Geotrichum candidum. Vet Arh 71: 197-201.
Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 8 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
63. Sharma N, Rho GJ, Hong YH, Kang TY, Lee HK, et al. (2012) Bovine mastitis: an asian perspective. Asn J Anim Vet Adv 7: 454-476.
64. Sordillo LM (2005) Factors affecting mammary gland immunity and mastitis susceptibility. Liv Prod Sci 98: 89-99.
65. Emanuelson U, Persson E (1984) Studies on somatic cell counts in milk from Swedish dairy cows. I. Non-genetic causes of variation in monthly test-day results. Acta Agri Scand 34: 33-44.
66. Busato A, Trachsel P, Schällibaum M, Blum JW (2000) Udder health and risk factors for subclinical mastitis in organic dairy farms in Switzerland. Prev Vet Med 44: 205-220.
67. Sharma H, Maiti SK, Sharma KK (2007) Prevalence, etiology and antibiogram of microorganisms associated with sub-clinical mastitis in buffaloes in Durg, Chhattisgarh state. Intl J Dairy Sci 2: 145-151.
68. Sharma N, Maiti SK (2010) Incidence, etiology and antibiogram of sub clinical mastitis in cows in durg, Chhattisgarh. Ind J Vet Res 19: 45-54.
69. Schukken YH, Grommers FJ, Van de Geer D, Brand A (1989) Incidence of clinical mastitis on farms with low somatic cell counts in bulk milk. Vet Rec 125: 60-63.
70. Dulin AM, Paape MJ, Nickerson SC (1988) Comparison of phagocytosis and chemiluminescence by blood and mammary gland neutrophils from multiparous and nulliparous cows. Am J Vet Res 49: 172-177.
71. Mahajan S, Bhatt P, Ramakant, Kumar A, Dabas YPS (2011) Risk and occurrence of bovine mastitis in Tarai region of Uttarakhand. Vet Pract 12: 244-247.
72. Grohn YT, Erb HN, McCulloch CE, Saloniemei HS (1990) Epidemiology of mammary gland disorders in multiparous Finnish Ayrshire cows. Prev Vet Med 8: 241-252.
73. Rajala PJ, Gröhn YT (1998) Disease occurrence and risk factor analysis in Finnish Ayrshire cows. Acta Vet Scand 39: 1-13.
74. Lactation Resource Library (2009) Other Factors Affecting Milk Yield and Composition.
75. Rathore AK (1976) Relationships between teat shape, production and mastitis in Friesian cows. Br Vet J 132: 389-392.
76. Seykora AJ, McDaniel BT (1985) Udder and teat morphology related to mastitis resistance: a review. J Dairy Sci 68: 2087-2093.
77. Thomas CL, Vinson WE, Pearson RE, Dickinson FN, Johnson LP (1984) Relationships between linear type scores, objective type measures, and indicators of mastitis. J Dairy Sci 67: 1281-1292.
78. Ellis KA (2005) Studies of the composition of milk produced on organic and conventional dairy farms in the UK. PhD Thesis, University of Liverpool.
79. Corbett R (2009) Minimizing the effects of immunosuppression through management and nutrition. Proceedings of the 48th Annual Meeting of the NMC, January 25-28, 2009, Charlotte, NC, 113-119.
80. Fadlelmula A, Al Dughaym AM, Mohamed GE, Al Deib MK, Al Zubaidy AJ (2009) Bovine mastitis: Epidemiological, clinical and etiological study in a Saudi Arabian large dairy farm. Bulgarian J Vet Med 12: 199-206.
81. Sharma N, Singh NK, Singh OP, Pandey V, Verma PK (2011) Oxidative stress and antioxidant status during transition period in dairy cows. Asian-Aust J Anim Sci 24: 479-484.
82. Bradley A, Green MJ (2005) Use and interpretation of somatic cell count data in dairy cows. In Pract 27: 310-315.
83. Plastridge WN (1958) Bovine mastitis: A review. J Dairy Sci 41: 1141-1181.
84. Peeler EJ, Green MJ, Fitzpatrick JL, Morgan KL, Green LE (2000) Risk factors associated with clinical mastitis in low somatic cell count British dairy herds. J Dairy Sci 83: 2464-2472.
85. Giesecke WH, Du Preez JH, Petzer IM (1994) Practical Mastitis Control in Dairy Herds. Diagnosis of udder health problems, Butterworth Publishers: Durban, South Africa.
86. Capuco AV, Ellis SE, Hale SA, Long E, Erdman RA, et al. (2003) Lactation persistency: insights from mammary cell proliferation studies. J Anim Sci 81: 18-31.
87. Mein G, Reinemann D, Schuring N, Ohnstad I (2004) Milking Machines And
Mastitis Risk: A storm in a TeatcupSensortec (NZ), Werribee, Australia; 2 UW-Madison, WI, USA; 3 Westfalia -Surge, Naperville, IL, USA; 4 ADAS, Taunton, UK, Paper presented at the 2004, Meeting of the National Mastitis Council.
88. Blood DC, Radostits OM (1989) Veterinary medicine. In: textbook of the diseases of cattle, sheep, pigs, goats and horses, (7thedn), 501.
89. International Dairy Federation (1987) Bovine mastitis: Definition and guidelines for diagnosis. Bulletin of the International Dairy Federation, Document 211.
90. Jones GM (2009) The Role of Milking Equipment in Mastitis. Virginia Cooperative Extension.
91. Mein GA, Schuring N (2003) Lessons from scrapbooks and scrapheaps of history. Bulletin-International Federation.
92. Mein GA, Neijenhuis F, Morgan WF, Reinemann DJ, Hillerton JE, et al. (2001) Evaluation of bovine teat condition in commercial dairy herds: 1. Non-infectious factors. Proceedings of the 2nd International Symposium on Mastitis and Milk Quality, NMC/AABP, Vancouver, 374-351.
93. Heinrichs AJ, Costello SS, Jones CM (2009) Control of heifer mastitis by nutrition. Vet Microbiol 134: 172-176.
94. Madsen PS, Nielsen SM (1981) The influence of udder health by feeding different levels of protein. In: Proceedings of the IVth International Symposium on Mastitis Control (II): 463-476.
95. Rodenburg J (2012) Mastitis Prevention for Dairy Cattle: Environmental Control. Factsheet.
96. Spears JW, Weiss WP (2008) Role of antioxidants and trace elements in health and immunity of transition dairy cows. Vet J 176: 70-76.
97. Hogan JS, Weiss WP, Todhunter DA, Smith KL, Schoenberger PS (1992) Efficacy of an Escherichia coli J5 mastitis vaccine in an experimental challenge trial. J Dairy Sci 75: 415-422.
98. Chamberlain AT, Wilkenson JM (1996) Feeding the dairy cow. Chalcombe Publications 90-91.
99. Mustacich D, Powis G (2000) Thioredoxin reductase. Biochem J 346: 1-8.
100. Erskine RJ, Eberhart RJ, Grasso PJ, Scholz RW (1989) Induction of Escherichia coli mastitis in cows fed selenium-deficient or selenium-supplemented diets. Am J Vet Res 50: 2093-2100.
101. Grasso PJ, Scholz RW, Erskine RJ, Eberhart RJ (1990) Phagocytosis, bactericidal activity, and oxidative metabolism of milk neutrophils from dairy cows fed selenium-supplemented and selenium-deficient diets. Am J Vet Res 51: 269-274.
102. Underwood EJ, Suttle NF (1999) In: The Mineral Nutrition of Livestock. Underwood EJ and Suttle NF (eds), CABI Publishing, New York.
103. Sordillo LM, Shafer-Weaver K, DeRosa D (1997) Immunobiology of the mammary gland. J Dairy Sci 80: 1851-1865.
104. Chew BP (1993) Role of carotenoids in the immune response. J Dairy Sci 76: 2804-2811.
105. Prasad AS, Bao B, Beck FW, Kucuk O, Sarkar FH (2004) Antioxidant effect of zinc in humans. Free Radic Biol Med 37: 1182-1190.
106. Bruno DR (2010) Mastitis, Mammary Gland Immunity, and Nutrition. Mid-South Ruminant Nutrition Conference 19 Arlington, Texas.
107. Scaletti RW, Trammell DS, Smith BA, Harmon RJ (2003) Role of dietary copper in enhancing resistance to Escherichia coli mastitis. J Dairy Sci 86: 1240-1249.
108. Upadhayay AK, Gangwar P, Kumar M (2008) Supplementation to prevent subclinical mastitis. Vet World 1: 40-41.
109. Eckles CH (1913) Dairy cattle and milk production. The Macmillan Company, New York, 342.
110. Shaldon JP (1980) Dairy farming: being the theory, practice, and methods of dairying (1880). Cassell and Company, London 575.
111. Jones GM (2001) Cold weather mastitis prevention tips. Dairy Pipeline.
112. Dhakal IP, Dhakal P, Koshihara T, Nagahata H (2007) Epidemiological and bacteriological survey of buffalo mastitis in Nepal. J Vet Med Sci 69: 1241-1245.
113. Akyuz A, Boyaci S, Cayli A (2010) Determination of critical period for dairy cows using temperature humidity index. J Anim Vet Adv 9: 1824-1827.

Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 9 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
114. Reneau J (2012) Gear up for warm weather mastitis management now. Dairy Star.
115. Costa EO, Ribeiro AR, Watanabe ET, Melville PA (1998) Infectious bovine mastitis caused by environmental organisms. Zentralbl Veterinarmed B 45: 65-71.
116. Ribeiro AR, Garinojr F, Silva JAB, Watanabe ET, Vallue CR, et al. (2001) Seasonality on the occurrence of environmental bovine mastitis. Nopgama 4: 19-22.
117. Sentitula, Yadav BR, Kumar R (2012) Incidence of Staphylococci and Streptococci during winter in mastitic milk of sahiwal cow and murrah buffaloes. Ind J Microbiol 52: 153-159.
118. Godden S, Rapnicki P, Stewart S, Fetrow J, Johnson A, et al. (2003) Effectiveness of an internal teat seal in the prevention of new intramammary infections during the dry and early-lactation periods in dairy cows when used with a dry cow intramammary antibiotic. J Dairy Sci 86: 3899-3911.
119. Shathele MS (2009) Weather effect on bacterial mastitis in dairy cows. Intl J Dairy Sci 4: 57-66.
120. Ranjan R, Gupta MK, Singh KK (2011) Study of bovine mastitis in different climatic conditions in Jharkhand, India. Vet World4: 205-208.
121. Palanivel KM, Suresh RV, Jayakumarn R, Ganesan PI, Dhanapalan P (2008) Retrospective study of sub-clinical mastitis in buffaloes. Ind J Vet Med 28: 34-36.
122. Ross S, Rodriguez W, Controni G, Khan W (1974) Staphylococcal susceptibility to penicillin G. The changing pattern among community strains. JAMA 229: 1075-1077.
123. Eykyn SJ (1988) Staphylococcal sepsis. The changing pattern of disease and therapy. Lancet 1: 100-104.
124. Pearson H (2002) ‘Superbug’ hurdles key drug barrier. Nature 418: 469.
125. Shi D, Hao Y, Zhang A, Wulan B, Fan X (2010) Antimicrobial resistance of Staphylococcus aureus isolated from bovine mastitis in China. Transbound Emerg Dis 57: 221-224.
126. Shittu AO, Okon K, Adesida S, Oyedara O, Witte W, et al. (2011) Antibiotic resistance and molecular epidemiology of Staphylococcus aureus in Nigeria. BMC Microbiol 11: 92.
127. Park YK, Fox LK, Hancock DD, McMahan W, Park YH (2012) Prevalence and antibiotic resistance of mastitis pathogens isolated from dairy herds transitioning to organic management. J Vet Sci 13: 103-105.
128. Gao J, Yu FQ, Luo LP, He JZ, Hou RG, et al. (2012) Antibiotic resistance of Streptococcus agalactiae from cows with mastitis. Vet J 194: 423-424.
129. Babra C, GogoiTiwari J, Pier G, Thein TH, Sunagar R, et al. (2012) Retention of persistent antibiotic resistance, developed by bovine mastitis methicillin-sensitive Staphylococcus aureus of different capsular phenotypes in biofilms, as planktonic subcultures. Submitted for publication to Folia Microbiologia.
130. Petersson-Wolfe CS, Mullarky IK, Jones GM (2010) Staphylococcus aureus Mastitis: Cause, Detection, and Control. Virginia Cooperative Extension.
131. Owens WE, Ray CH, Boddie RL, Nickerson SC (1997a) Efficacy of sequential intramammary treatment against chronic Staphylococcus aureus. Large Anim Pract 18: 10-14.
132. Barlow J (2011) Mastitis therapy and antimicrobial susceptibility: a multispecies review with a focus on antibiotic treatment of mastitis in dairy cattle. J Mammary Gland Biol Neoplasia 16: 383-407.
133. Erskine RJ (2001) Enhancing immunity during the dry period: Pitfalls and opportunities. In: Proceeding of National Mastitis Council, 95-106.
134. Timms L (2001) Evaluation of recommended and extended pirlimycin therapy strategies in four high somatic cell count herds. In: Proceedings of Second International Mastitis Milk Quality Symposium 2001: 534-535.
135. Gruet P, Maincent P, Berthelot X, Kaltsatos V (2001) Bovine mastitis and intramammary drug delivery: review and perspectives. Adv Drug Deliv Rev 50: 245-259.
136. Prescott JF (1987) In vitro antimicrobial drug susceptibility testing in bovine mastitis therapy. In: Proceedings, International Mastitis Symposium, Canada, 1987.
137. du Preez JH (2000) Bovine mastitis therapy and why it fails. J S Afr Vet Assoc 71: 201-208.
138. Sérieys F, Raguet Y, Goby L, Schmidt H, Friton G (2005) Comparative efficacy of local and systemic antibiotic treatment in lactating cows with clinical mastitis. J Dairy Sci 88: 93-99.
139. Petrovski KR (2007) Bovine mastitis treatment failure.
140. Cattell MB, Belschner AP (1997) Efficacy of extended lactational intramammary antibiotic treatment against Staphylococcus aureus mastitis. In: Proceeding of National Mastitis Council 244-245.
141. Daley MJ, Furda G, Dougherty R, Coyle PA, Williams TJ, et al. (1992) Potentiation of antibiotic therapy for bovine mastitis by recombinant bovine interleukin-2. J Dairy Sci 75: 3330-3338.
142. Pyörälä S (2002) New strategies to prevent mastitis. Reprod Domest Anim 37: 211-216.
143. Paape MJ, Bannerman DD, Zhao X, Lee JW (2003) The bovine neutrophil: Structure and function in blood and milk. Vet Res 34: 597-627.
144. Huff WE, Huff GR, Rath NC, Balog JM, Donoghue AM (2002) Prevention of Escherichia coli infection in broiler chickens with a bacteriophage aerosol spray. Poult Sci 81: 1486-1491.
145. Smith HW, Huggins MB (1982) Successful treatment of experimental Escherichia coli infections in mice using phage: its general superiority over antibiotics. J Gen Microbiol 128: 307-318.
146. Smith HW, Huggins MB (1983) Effectiveness of phages in treating experimental Escherichia coli diarrhoea in calves, piglets and lambs. J Gen Microbiol 129: 2659-2675.
147. Smith HW, Huggins MB, Shaw KM (1987) The control of experimental Escherichia coli diarrhoea in calves by means of bacteriophages. J Gen Microbiol 133: 1111-1126.
148. Gill JJ, Pacan JC, Carson ME, Leslie KE, Griffiths MW, et al. (2006) Efficacy and pharmacokinetics of bacteriophage therapy in treatment of subclinical Staphylococcus aureus mastitis in lactating dairy cattle. Antimicrob Agents Chemother 50: 2912-2918.
149. Gill JJ, Sabour PM, Leslie KE, Griffiths MW (2006) Bovine whey proteins inhibit the interaction of Staphylococcus aureus and bacteriophage K. J Appl Microbiol 101: 377-386.
150. Kwiatek M, Parasion S, Mizak L, Gryko R, Bartoszcze M, et al. (2012) Characterization of a bacteriophage, isolated from a cow with mastitis, that is lytic against Staphylococcus aureus strains. Arch Virol 157: 225-234.
151. Lee JC, Perez NE, Hopkins CA, Pier GB (1988) Purified capsular polysaccharide-induced immunity to Staphylococcus aureus infection. J Infect Dis 157: 723-730.
152. Mamo W, Jonsson P, Flock JI, Lindberg M, Müller HP, et al. (1994) Vaccination against Staphylococcus aureus mastitis: immunological response of mice vaccinated with fibronectin-binding protein (FnBP-A) to challenge with S. aureus. Vaccine 12: 988-992.
153. Leitner G, Yadlin B, Glickman A, Chaffer M, Saran A (2000) Systemic and local immune response of cows to intramammary infection with Staphylococcus aureus. Res Vet Sci 69: 181-184.
154. Leitner G, Lubachevsky E, Glikman E, Winkler M, Saran A, et al. (2003) Development of a Staphylococcus aureus vaccine against mastitis in dairy cows. I. Challenge trials. Vet Immunol Immunopathol 93: 31-38.
155. Tenhagen BA, Edinger D, Baumgärtner B, Kalbe P, Klünder G, et al. (2001) Efficacy of a herd-specific vaccine against Staphylococcus aureus to prevent post-partum mastitis in dairy heifers. J Vet Med A Physiol Pathol Clin Med 48: 601-607.
156. Nour El-Din AN, Shkreta L, Talbot BG, Diarra MS, Lacasse P (2006) DNA immunization of dairy cows with the clumping factor A of Staphylococcus aureus. Vaccine 24: 1997-2006.
157. Pellegrino M, Giraudo J, Raspanti C, Odierno L, Bogni C (2010) Efficacy of immunization against bovine mastitis using a Staphylococcus aureus avirulent mutant vaccine. Vaccine 17: 4523-4528.
158. Xu H, Hu C, Gong R, Chen Y, Ren N, et al. (2011) Evaluation of a novel chimeric B cell epitope-based vaccine against mastitis induced by either Streptococcus agalactiae or Staphylococcus aureus in mice. Clin Vaccine Immunol 18: 893-900.
159. Heath PT (2011) An update on vaccination against group B streptococcus. Expert Rev Vaccines 10: 685-694.

Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 10 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
160. Buzzola FR, Barbagelata MS, Caccuri RL, Sordelli DO (2006) Attenuation and persistence of and ability to induce protective immunity to a Staphylococcus aureus aroA mutant in mice. Infect Immun 74: 3498-3506.
161. Poutrel B, Boutonnier A, Sutra L, Fournier JM (1988) Prevalence of capsular polysaccharide types 5 and 8 among Staphylococcus aureus isolates from cow, goat, and ewe milk. J Clin Microbiol 26: 38-40.
162. Chang BS, Moon JS, Kang HM, Kim YI, Le HK, et al. (2008) Protective effects of recombinant staphylococcal enterotoxin type C mutant vaccine against experimental bovine infection by a strain of Staphylococcus aureus isolated from subclinical mastitis in dairy cattle. Vaccine 26: 2081-91.
163. Yancey RJ Jr (1999) Vaccines and diagnostic methods for bovine mastitis: fact and fiction. Adv Vet Med 41: 257-273.
164. Ruegg RL (2005) Evaluating the effectiveness of mastitis vaccines.
165. Miltenburg JD, de Lange D, Crauwels AP, Bongers JH, Tielen MJ, et al. (1996) Incidence of clinical mastitis in a random sample of dairy herds in the southern Netherlands. Vet Rec 139: 204-207.
166. Nickerson SC (1999) Role of vaccination and treatment programs. In: Proceedings of 38th Annual Meeting National Mastitis Council, Inc. Madison, WI, 76-85.
167. Lee JW, O’Brien CN, Guidry AJ, Paape MJ, Shafer-Weaver KA, et al. (2005) Effect of a trivalent vaccine against Staphylococcus aureus mastitis lymphocyte subpopulations, antibody production, and neutrophil phagocytosis. Can J Vet Res 69: 11-18.
168. O’Brien CN, Guidry AJ, Fattom A, Shepherd S, Douglass LW, et al. (2000) Production of antibodies to Staphylococcus aureus serotypes 5, 8, and 336 using poly(DL-lactide-co-glycolide) microspheres. J Dairy Sci 83: 1758-1766.
169. Prenafeta A, March R, Foix A, Casals I, Costa L (2010) Study of the humoral immunological response after vaccination with a Staphylococcus aureus biofilm-embedded bacterin in dairy cows: possible role of the exopolysaccharide specific antibody production in the protection from Staphylococcus aureus induced mastitis. Vet Immunol Immunopathol 134: 208-217.
170. Maira-Litrán T, Bentancor LV, Bozkurt-Guzel C, O’Malley JM, Cywes-Bentley C, et al. (2012) Synthesis and evaluation of a conjugate vaccine composed of Staphylococcus aureus poly-N-acetyl-glucosamine and clumping factor A. PLoS One 7: e43813.
171. Hogan JS, Smith KL (1987) Apractical look at environmental mastitis. Compendium on Continuing Education for the Practicing Veterinarian 9: F342.
172. Jones GM (2009) Environmental Streptococcal and Coliform Mastitis. Virginia Cooperative Extension.
173. Wilson MR (1972) The influence of preparturient intramammary vaccination on bovine mamary secretions. Antibody activity and protective value against Escherichia coli enteric infections. Immunology 23: 947-955.
174. Wilson MR, Duncan JR, Heistand F, Brown P (1972) The influence of preparturient intramammary vaccination on immunoglobulin levels in bovine mammary secretions. Immunology 23: 313-320.
175. Dosogne H, Vangroenweghe F, Burvenich C (2002) Potential mechanism of action of J5 vaccine in protection against severe bovine coliform mastitis. Vet Res 33: 1-12.
176. González RN, Cullor JS, Jasper DE, Farver TB, Bushnell RB, et al. (1989) Prevention of clinical coliform mastitis in dairy cows by a mutant Escherichia coli vaccine. Can J Vet Res 53: 301-305.
177. Hogan JS, Weiss WP, Todhunter DA, Smith KL, Schoenberger PS (1992) Bovine neutrophil responses to parenteral vitamin E. J Dairy Sci 75: 399-405.
178. Leigh JA (2000) Vaccines against bovine mastitis due to Streptococcus uberis current status and future prospects. Adv Exp Med Biol 480: 307-311.
179. Finch JM, Hill AW, Field TR, Leigh JA (1994) Local vaccination with killed Streptococcus uberis protects the bovine mammary gland against experimental intramammary challenge with the homologous strain. Infect Immun 62: 3599-3603.
180. Finch JM, Winter A, Walton AW, Leigh JA (1997) Further studies on the efficacy of a live vaccine against mastitis caused by Streptococcus uberis. Vaccine 15: 1138-1143.
181. Leigh JA (1999) Streptococcus uberis: a permanent barrier to the control of bovine mastitis? Vet J 157: 225-238.
182. Prado ME, Almeida RA, Ozen C, Luther DA, Lewis MJ, et al. (2011) Vaccination of dairy cows with recombinant Streptococcus uberis adhesion molecule induces antibodies that reduce adherence to and internalization of S. uberis into bovine mammary epithelial cells. Vet Immunol Immunopathol 141: 201-208.
183. Schukken YH, Hertl J, Bar D, Bennett GJ, González RN, et al. (2009) Effects of repeated gram-positive and gram-negative clinical mastitis episodes on milk yield loss in Holstein dairy cows. J Dairy Sci 92: 3091-3105.
184. Leigh JA, Egan SA, Ward PN, Field TR, Coffey TJ (2010) Sortase anchored proteins of Streptococcus uberis play major roles in the pathogenesis of bovine mastitis in dairy cattle. Vet Res 41: 63.
185. Denis M, Lacy-Hulbert SJ, Buddle BM, Williamson JH, Wedlock DN (2011) Streptococcus uberis-specific T cells are present in mammary gland secretions of cows and can be activated to kill S. uberis. Vet Res Commun 35: 145-156.
186. Bolton A, Song XM, Willson P, Fontaine MC, Potter AA, et al. (2004) Use of the surface proteins GapC and Mig of Streptococcus dysgalactiae as potential protective antigens against bovine mastitis. Can J Microbiol 50: 423-432.
187. Adams LG, Templeton JW (1998) Genetic resistance to bacterial diseases of animals. Rev Sci Tech 17: 200-219.
188. Simianer H, Solbu H, Schaeffer LR (1991) Estimated genetic correlations between disease and yield traits in dairy cattle. J Dairy Sci 74: 4358-4365.
189. Heringstad B, Klemetsdal G, Steine T (2007) Selection responses for disease resistance in two selection experiments with Norwegian red cows. J Dairy Sci 90: 2419-2426.
190. Thompson-Crispi KA, Sewalem A, Miglior F, Mallard BA (2012) Genetic parameters of adaptive immune response traits in Canadian Holsteins. J Dairy Sci 95: 401-409.
191. Heriazon A, Yager JA, Sears W, Mallard BA (2009) Induction of delayed-type hypersensitivity and interferon-gamma to Candida albicans and anti-hen-egg white lysozyme antibody as phenotypic markers of enhanced bovine immune response. Vet Immunol Immunopathol 129: 93-100.
192. Eid G, Zaghioul WA, Awaad AHH (1995) Role of Corynebacterium cutis as an immunostimulant on the response of chickens against fowl pox virus. Vet Med J 43: 219-229.
193. Lee WC, Kim TJ, Lee SM, Kim YC, Kwon YE, et al. (1996) An observative study on the application of Corynebacterium cutis lysate (Ultracorn) in decreasing of somatic cell count of the bulk milk from a herd of dairy cows for milk hygiene. Kor J Vet Pub Hlth 20: 349-353.
194. Shalaby MA, Saleh SM, el-Atrash S, Sami AM, el-Sanousi AA, et al. (1992) Application of Corynebacterium cutis lysate as an immune stimulant in cattle. Mol Biother 4: 147-150.
195. Yilmaz OT, Kasikci G, Gunduz MC (2011) Benefits of pregnant sheep immunostimulation with Corynebacterium cutis on post-partum and early newborn’s life IgG levels, stillbirth rate and lamb’s weight. Small Rum Res 97: 146-151.
196. Sol J, Sampimon OC, Snoep JJ, Schukken YH (1997) Factors associated with bacteriological cure during lactation after therapy for subclinical mastitis caused by Staphylococcus aureus. J Dairy Sci 80: 2803-2808.
197. Oliver SP, Gillespie BE, Headrick SJ, Moorehead H, Lunn P, et al. (2004) Efficacy of extended ceftiofur intramammary therapy for treatment of subclinical mastitis in lactating dairy cows. J Dairy Sci 87: 2393-2400.
198. 198. Pyöräla S (2009) Treatment of mastitis during lactation. Ir Vet J 62 Suppl 4: S40-S44.
199. Hillerton JE, Berry EA (2003) The management and treatment of environmental streptococcal mastitis. Vet Clin North Am Food Anim Pract 19: 157-169.
200. Hektoen L, Ødegaard SA, Løken T, Larsen S (2004) Evaluation of stratification factors and score-scales in clinical trials of treatment of clinical mastitis in dairy cows. J Vet Med A Physiol Pathol Clin Med 51: 196-202.
201. Owens WE, Ray CH, Watts JL, Yancey RJ (1997) Comparison of success of antibiotic therapy during lactation and results of antimicrobial susceptibility tests for bovine mastitis. J Dairy Sci 80: 313-317.
202. Pinzon-Sanchez C, Hulland C, Ruegg PL (2010) Post treatment outcomes of clinical mastitis on commercial dairy farms. J Dairy Sci 93, E-Suppl: 1:79.
203. Pyöräla SH, Pyöräla EO (1998) Efficacy of parenteral administration of three

Citation: Tiwari JG, Babra C, Tiwari HK, Williams V, Wet SD, et al. (2013) Trends In Therapeutic and Prevention Strategies for Management of Bovine Mastitis: An Overview. J Vaccines Vaccin 4: 176. doi:10.4172/2157-7560.1000176
Page 11 of 11
Volume 4 • Issue 2 • 1000176J Vaccines VaccinISSN:2157-7560 JVV an open access journal
antimicrobial agents in treatment of clinical mastitis in lactating cows: 487 cases (1989-1995). J Am Vet Med Assoc 212: 407-412.
204. Deluyker HA, Chester ST, Van Oye SN (1999) A multilocation clinical trial in lactating dairy cows affected with clinical mastitis to compare the efficacy of treatment with intramammary infusions of a lincomysin/neomycin combination with an ampicillin/cloxacillin combination. J Vet Pharmacol Ther 22: 274-282.
205. Sol J, Sampimon OC, Barkema HW, Schukken YH (2000) Factors associated with cure after therapy of clinical mastitis caused by Staphylococcus aureus. J Dairy Sci 83: 278-284.
206. McDougall S, Arthur DG, Bryan MA, Vermunt JJ, Weir AM (2007) Clinical and bacteriological response to treatment of clinical mastitis with one of three intramammary antibiotics. N Z Vet J 55: 161-170.
207. McDougall S, Agnew KE, Cursons R, Hou XX, Compton CR (2007) Parenteral treatment of clinical mastitis with tylosin base or penethamate hydriodide in dairy cattle. J Dairy Sci 90: 779-789.
208. Zhen YH, Jin LJ, Li XY, Guo J, Li Z, et al. (2009) Efficacy of specific egg yolk immunoglobulin (IgY) to bovine mastitis caused by Staphylococcus aureus. Vet Microbiol 133: 317-322.
209. Ziv G, Storper M, Saran A (1981) Comparative efficacy of three antibiotic products for the treatment and prevention of subclinical mastitis during the dry period. Vet Q 3: 74-79.
210. Oliver SP, Sordillo LM (1988) Udder health in the periparturient period. J Dairy Sci 71: 2584-2606.
211. Murphy JM, Hanson JJ (1943) Infection of the bovine udder with coliform bacteria. Corn Vet 33: 61-77.
212. Oliver SP, Mitchell BA (1983) Susceptibility of bovine mammary gland to infections during the dry period. J Dairy Sci 66: 1162-1166.
213. Todhunter DA, Smith KL, Hogan JS, Schoenberger PS (1991) Gram-negative bacterial infections of the mammary gland in cows. Am J Vet Res 52: 184-188.
214. Janosi Sz, Huszenicza G (2001) The use of the dry cow therapy in the control of bovine mastitis. Vet Med-Czech 46: 55-60.
215. Bramley AJ, Dodd FH (1984) Reviews of the progress of dairy science: mastitis control--progress and prospects. J Dairy Res 51: 481-512.
216. Hassan Z, Daniel RC, O’Boyle D, Frost AJ (1999) Effects of dry cow intramammary therapy on quarter infections in the dry period. Vet Rec 145: 635-639.
217. Woolford MW, Williamson JH, Day AM, Copeman PJ (1998) The prophylactic effect of a teat sealer on bovine mastitis during the dry period and the following lactation. N Z Vet J 46: 12-19.
218. Twomey DP, Wheelock AI, Flynn J, Meaney WJ, Hill C, et al. (2000) Protection against Staphylococcus aureus mastitis in dairy cows using a bismuth-based teat seal containing the bacteriocin, lacticin 3147. J Dairy Sci 83: 1981-1988.
219. Sanford C, Keefe G, Leslie K, Dohoo I, Barkema H, et al. (2004) Efficacy of an internal teat sealant (OrbeSeal) for the Prevention of new Intramammary Infections during the dry period. NMC Annual Meeting Proceedings 43: 306-307.
220. Runciman DJ, Malmo J, Deighton M (2010) The use of an internal teat sealant in combination with cloxacillin dry cow therapy for the prevention of clinical and subclinical mastitis in seasonal calving dairy cows. J Dairy Sci 93: 4582-4591.
221. Izak E, Castello E, Veneranda G (2012) Mastitis in Dairy:efficacy and economic benefit of an internal teat sealant during drought and rainy weather dry period on incidence of clinical mastitis.
222. Hayton AJ, Bradley AJ (2001) An investigation of factors affecting the adherence and efficacy of an external teat sealant in organic herds. In Proceedings of the 2nd International mastitis and milk quality symposium, Vancouver.National Mastitis Council, Madison, WI, 470-471.
223. Huxley JN, Greent MJ, Green LE, Bradley AJ (2002) Evaluation of the efficacy of an internal teat sealer during the dry period. J Dairy Sci 85: 551-561.
224. Cook NB, Wilkinson A, Gajewski K, Weigel D, Sharp R, et al. (2004) The prevention of new intramammary infections during the dry period when using an internal teat sealant in conjunction with a dry cow antibiotic. Proceedings of National Mastis Council.