fatty liver disease - acp · fatty liver disease its not just for big boys anymore ken flora, md,...
TRANSCRIPT
10/30/2017
1
Fatty liver
disease
Its not just
for big boys
anymore
Ken Flora, MD, FAASLD, FACG, AGAF
No disclosures
Common situation…Common situation…Common situation…Common situation…
• Normal ALT for men 30 IU/L 36% US males abnormal
• Normal ALT for women 20 IU/L 28% US females abnormal
Abnl ALT
Assess alcohol use/meds
Recheck in 6-8 weeks
HCV Ab HBsAg
Ferritin/TIBC
Ultrasound
still pos
10/30/2017
2
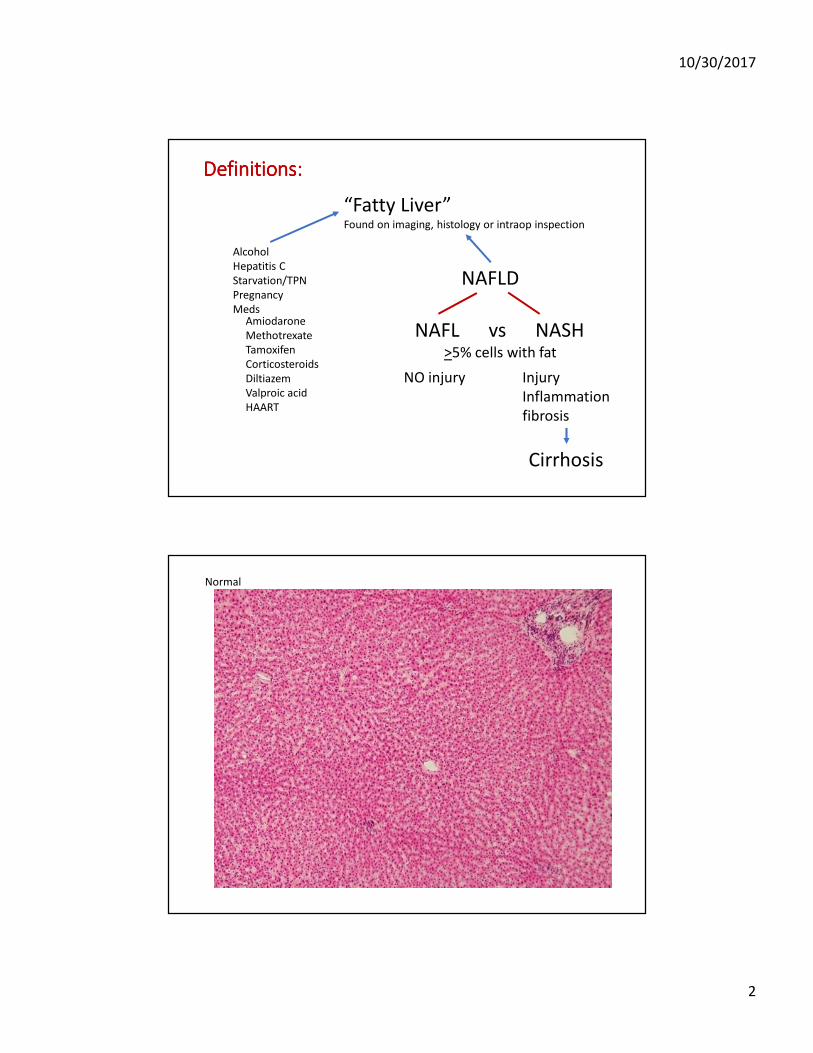
Definitions:Definitions:Definitions:Definitions:
“Fatty Liver”Found on imaging, histology or intraop inspection
Alcohol
Hepatitis C
Starvation/TPN
Pregnancy
MedsAmiodarone
Methotrexate
Tamoxifen
Corticosteroids
Diltiazem
Valproic acid
HAART
NAFLD
NAFL vs NASH>5% cells with fat
NO injury Injury
Inflammation
fibrosis
Cirrhosis
Normal
10/30/2017
3
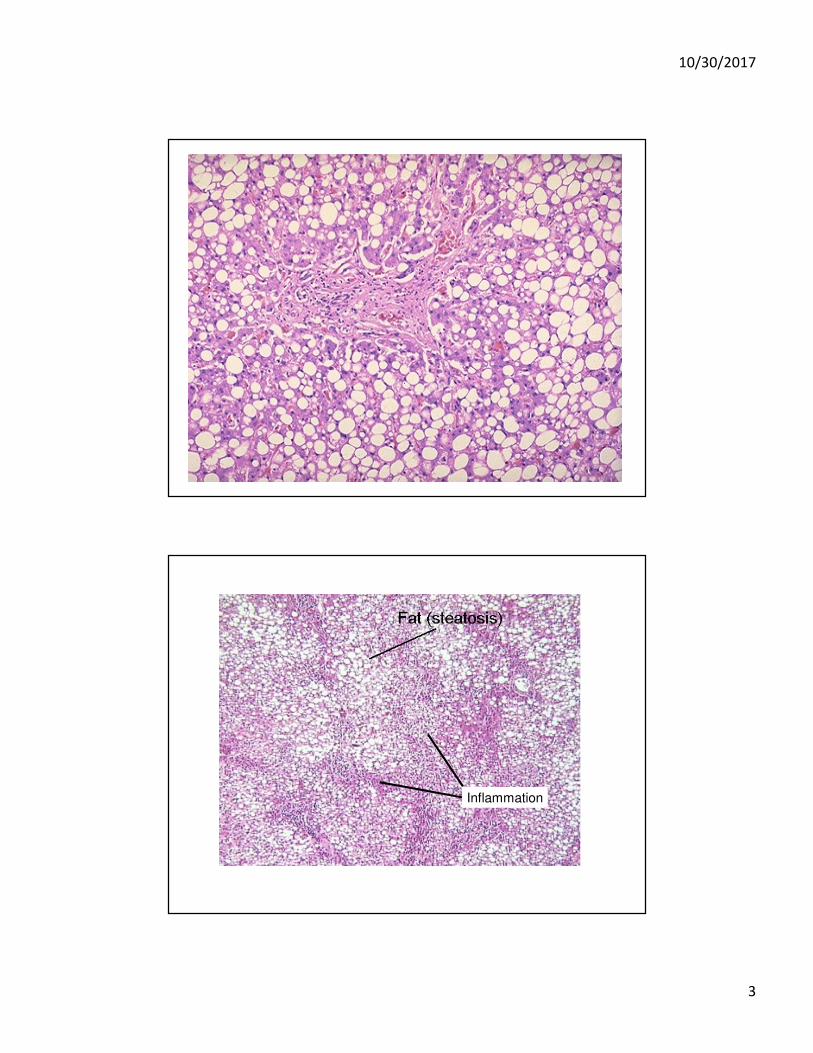
Inflammation
10/30/2017
4
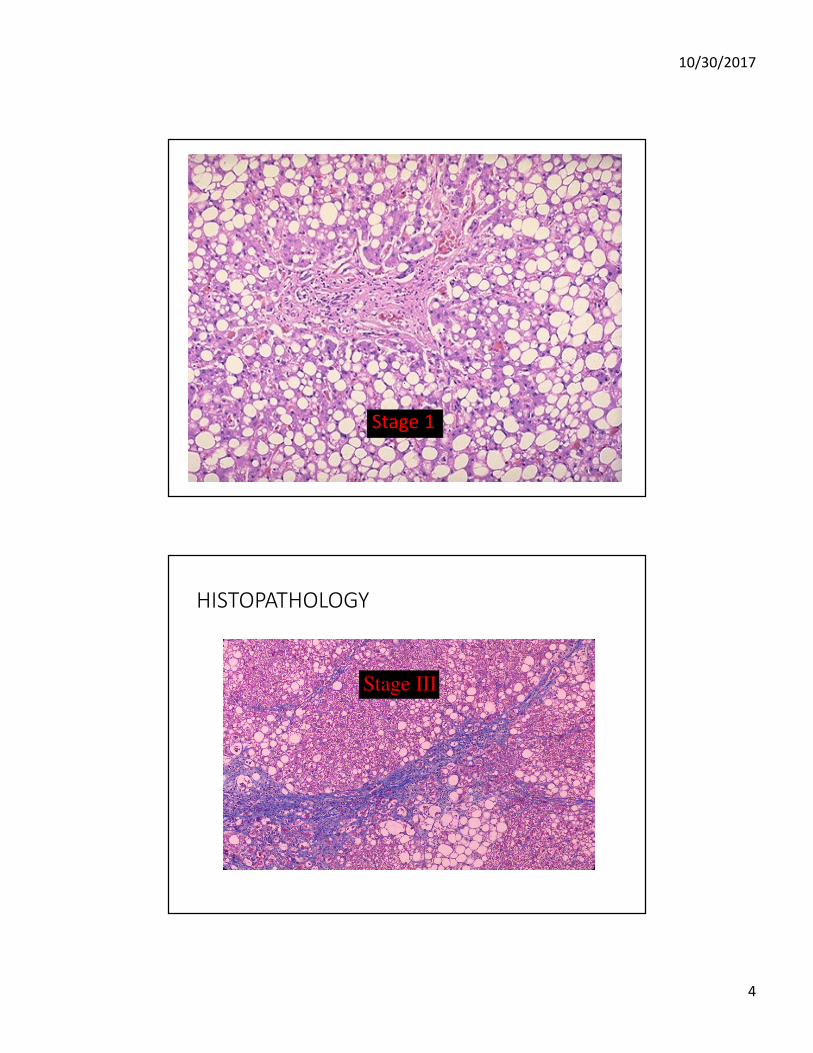
Stage 1
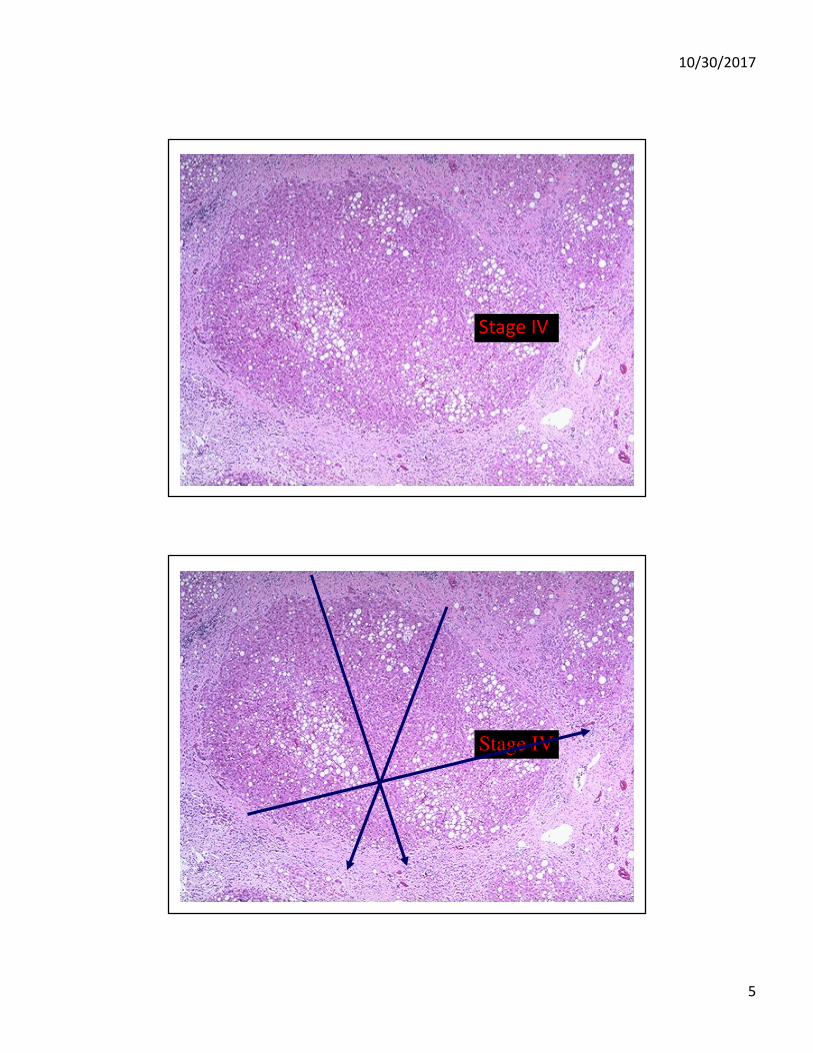
HISTOPATHOLOGY
Stage III
10/30/2017
5
Stage IV
Stage IV

10/30/2017
6
Incidence:Incidence:Incidence:Incidence:
• Not well known – no prospective biopsy studies
• Recent meta analysis suggested
• Asia 52/1000 person-years
• West 28/1000 person years
Younossi ZM Hepatology 2016. 64:73
Prevalence:Prevalence:Prevalence:Prevalence:
Global 25% NAFLD
1.5 – 6.5% NASH
Mid East/South America 30% Africa 13%
Younossi ZM Hepatology 2016. 64:73

10/30/2017
7
Prevalence in ‘high risk’ pops:Prevalence in ‘high risk’ pops:Prevalence in ‘high risk’ pops:Prevalence in ‘high risk’ pops:
AASLD Practice Guidance. Hepatology 2017
Obesity
T2DM
Dyslipidemia
Metabolic Syndrome
Polycystic Ovary Syndrome

10/30/2017
8
ObesityObesityObesityObesity
•Prevalence of NAFLD increases with BMI
•95% of bariatric surgery candidates
Sasaki. Front Endocrinol 2014;5:164
Subichin. Surg Obes Relat Dis 2015;11:137
10/30/2017
9
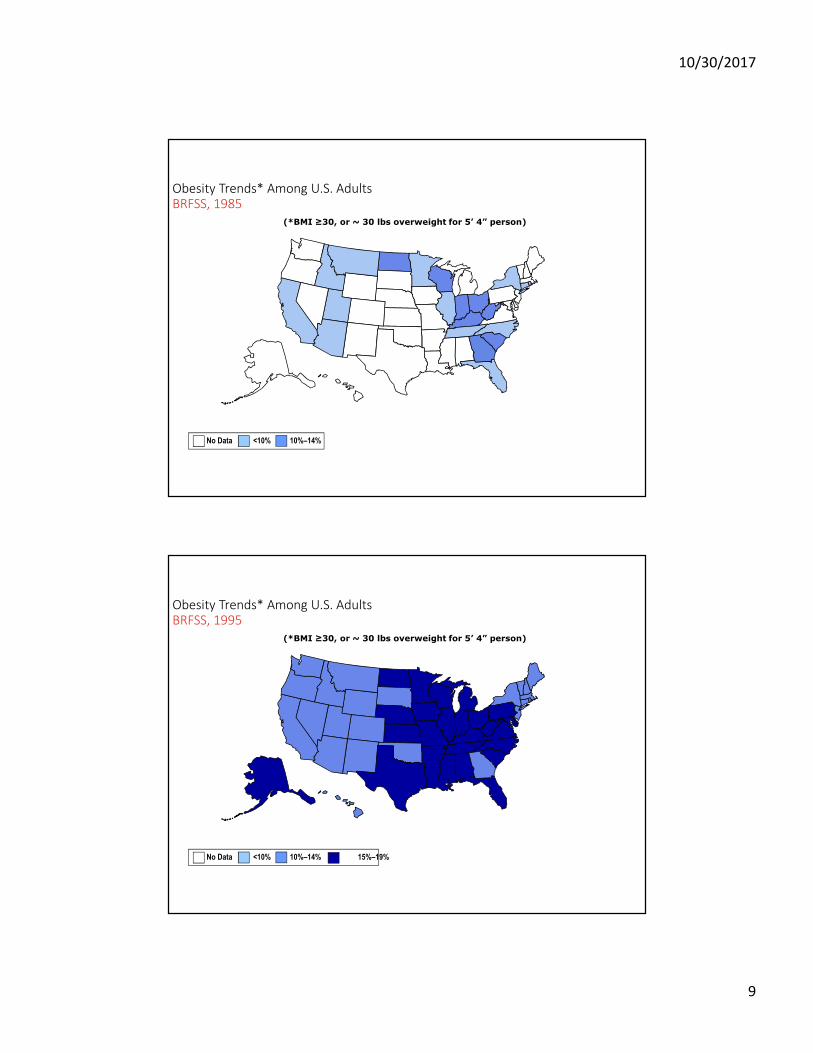
Obesity Trends* Among U.S. AdultsBRFSS, 1985
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1995
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%

10/30/2017
10
Obesity Trends* Among U.S. AdultsBRFSS, 2005
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

10/30/2017
11
T2DMT2DMT2DMT2DM
•30-60% have NAFLD
•Can appear simultaneously
DyslipidemiaDyslipidemiaDyslipidemiaDyslipidemia
50% NAFLD among lipid clinic patients
Assy, Dig Dis Sci 2000;45:1929
Leite. Liver Int 2009;29:113

10/30/2017
12
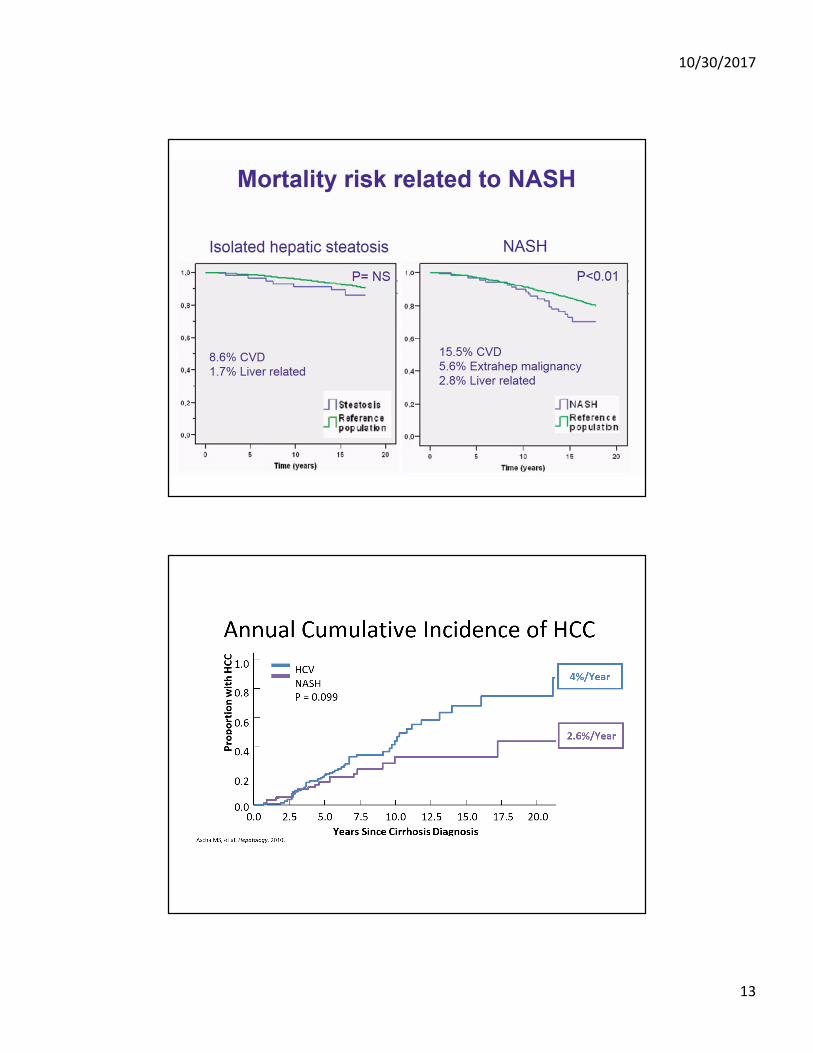
Yu, et al.Gastroenterology Research and Practice Volume 2016 (2016), Article ID 2862173
Ong JP, Younossi ZM. Clin Liver Dis 2007;11:1-16
10/30/2017
13

10/30/2017
14
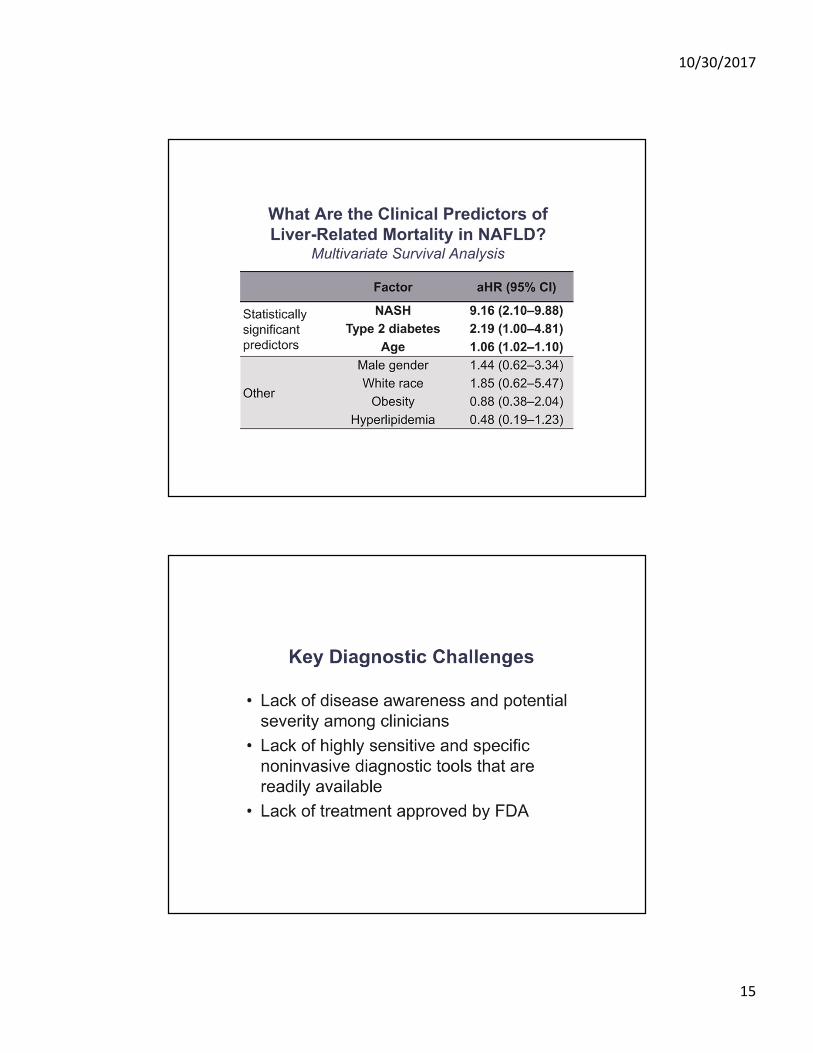
Mittal S, et al. Clin Gastroenterol Hepatol 2016;14:124-131
Predictors of “Bad” NASH:
10/30/2017
15
10/30/2017
16
10/30/2017
17
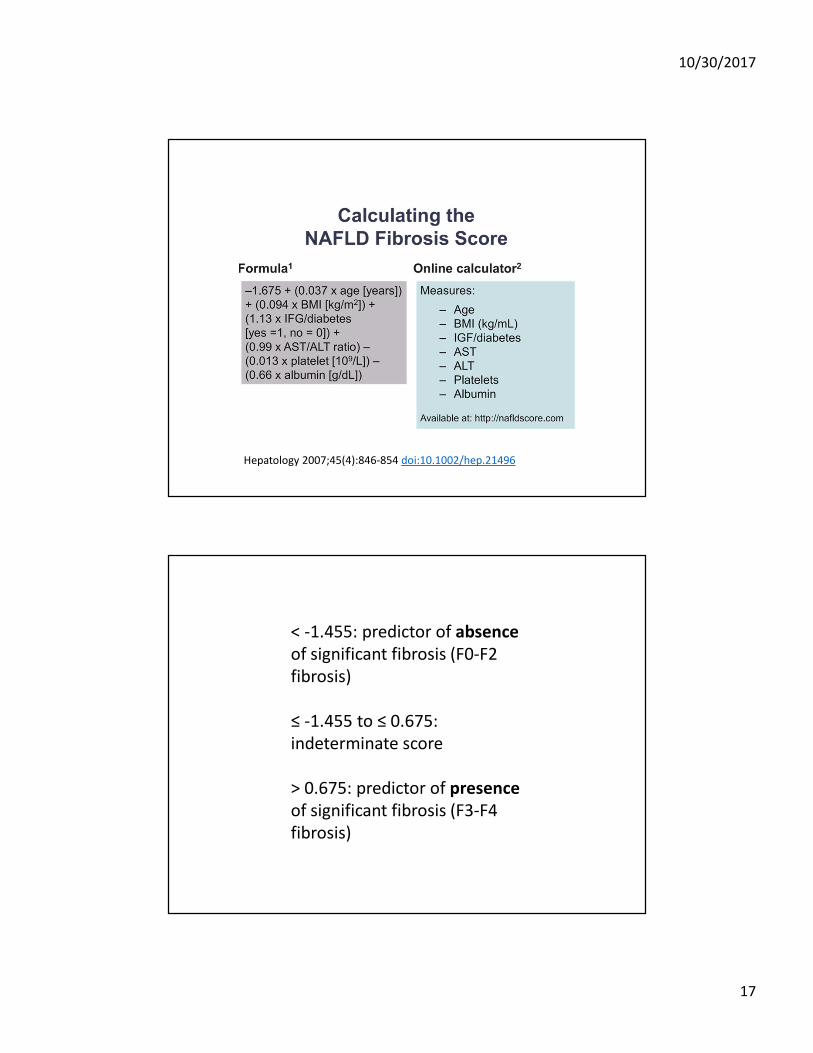
Hepatology 2007;45(4):846-854 doi:10.1002/hep.21496
< -1.455: predictor of absence
of significant fibrosis (F0-F2
fibrosis)
≤ -1.455 to ≤ 0.675:
indeterminate score
> 0.675: predictor of presence
of significant fibrosis (F3-F4
fibrosis)
10/30/2017
18
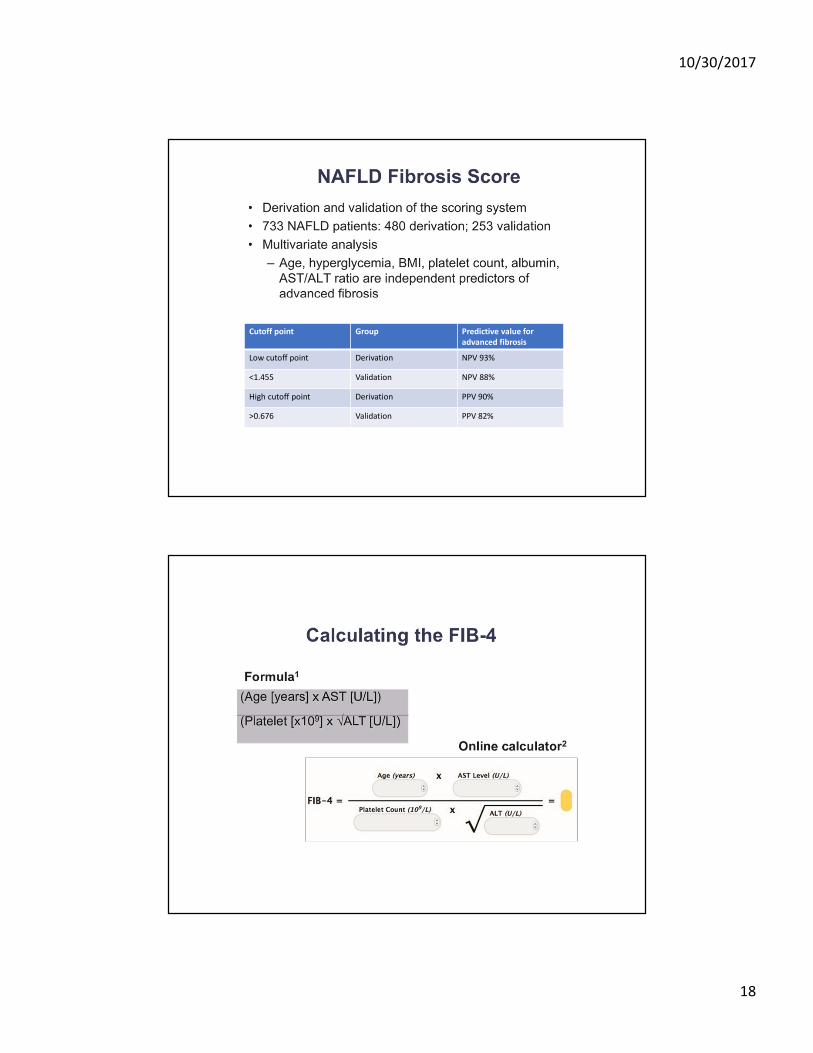
Cutoff point Group Predictive value for
advanced fibrosis
Low cutoff point Derivation NPV 93%
<1.455 Validation NPV 88%
High cutoff point Derivation PPV 90%
>0.676 Validation PPV 82%
10/30/2017
19
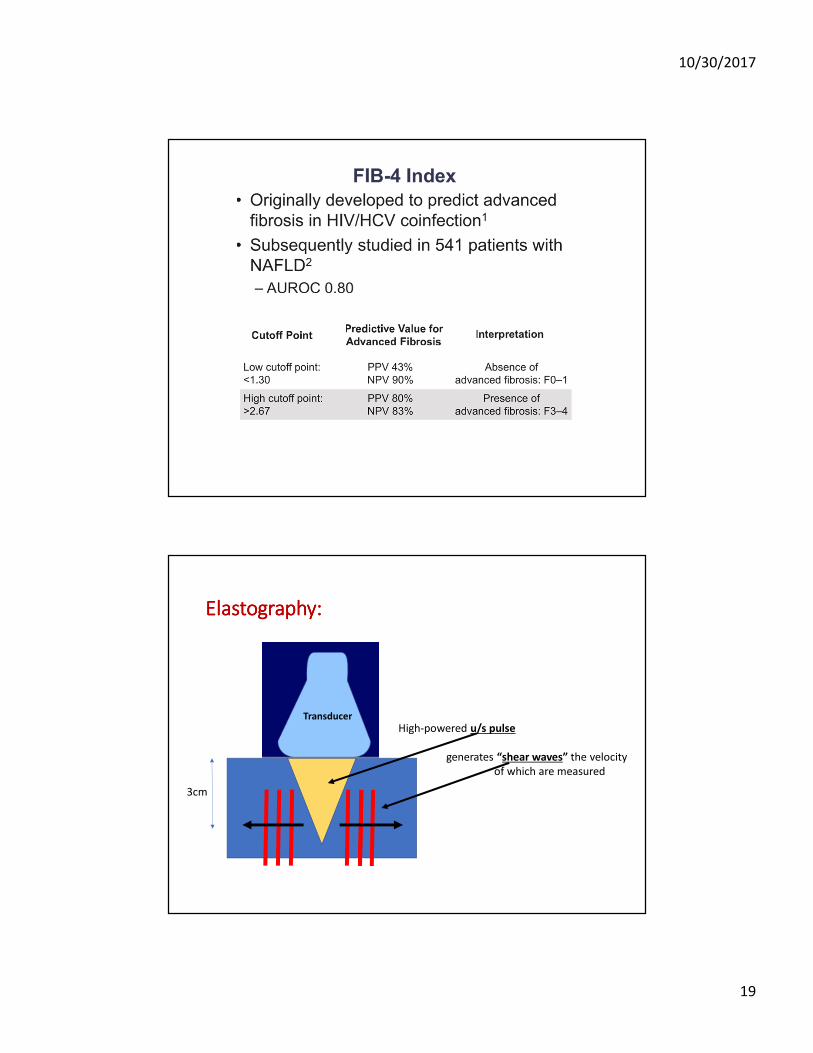
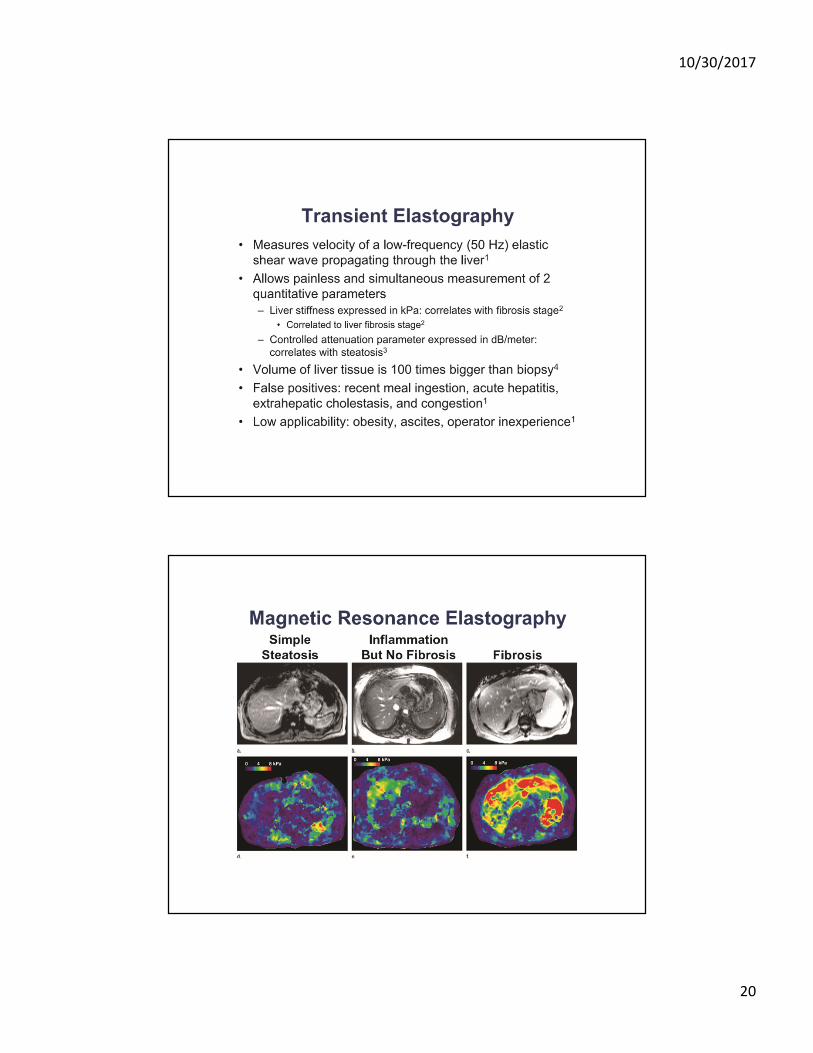
Transducer
High-powered u/s pulse
generates “shear waves” the velocity
of which are measured
3cm
Elastography:Elastography:Elastography:Elastography:
10/30/2017
20

10/30/2017
21
Liver biopsy:Liver biopsy:Liver biopsy:Liver biopsy:
• AASLD Practice Guidance for NAFLD 2017
“Liver biopsy should be considered in patients with NAFLD who are at increased risk to have steatohepatitis and advanced fibrosis.”
“Liver biopsy should be considered in patients with suspected NAFLD in whom competing etiologies for hepatic steatosis and the presence and/or severity of (the) co-existing chronic liver diseases cannot be excluded without a liver biopsy.”
Chalasani, Younossi, Lavine, et al. Hepatology 2017
Management:Management:Management:Management:
Hannah WN, et al. Clin Liver Dis. 201.
Vilar-Gomez, et al. Gastroenterology 2015; 149:367-378.
Treatment: % Weight Loss Associated with Histological
Improvement
Life style- dietary change and exercise

10/30/2017
22
Romero-Gomez et al. J Hepatol 2017;67:829
Diet:
• Long-term compliance is important
• The specific composition of the diet less important- decrease caloric intake by >30% (~750-1,000 kcal/day)
• Not enough data to recommend a specific diet though the Mediterranean-style diet seems best currently and that advised by societies.

10/30/2017
23
Exercise:
• Exercise, without weight loss, improves LFTs and prevents/improves NAFL somewhat–effect on NASH unknown. Only vigorous activity seems to do that.
• Real effect is on the heart
Medications:
• Metformin – not recommended- ineffective for NASH
• Rosiglitazone – not recommended- helped NAFL, not NASH
• Pioglitazone – improvement (signif in some studies) in NASH with or without T2DM- wt gain most sig SE
• Vitamin E (pure rrr α-tocopherol) 800IU/day better for NASH than placebo or metformin. Concern over all-cause mortality and higher risk of prostate CA at higher doses.
• Urso – not recommended- ineffective
• Omega-3 Fas – not recommended- ineffective- may help hyperTGemia
• Statins are OK

10/30/2017
24
Nonalcoholic Fatty Liver Disease: Epidemiology, Natural History, and Diagnostic ChallengesNonalcoholic Fatty Liver Disease: Epidemiology, Natural History, and Diagnostic ChallengesNonalcoholic Fatty Liver Disease: Epidemiology, Natural History, and Diagnostic ChallengesNonalcoholic Fatty Liver Disease: Epidemiology, Natural History, and Diagnostic Challenges
Hepatology
Volume 64, Issue 3, pages 954-954, 2 AUG 2016 DOI: 10.1002/hep.28719
http://onlinelibrary.wiley.com/doi/10.1002/hep.28719/full#hep28719-fig-0001