febrile neutropenia by dr saqib ahmad shah pg radiation oncology skims kashmir
TRANSCRIPT


GRANULOPOIESIS
GM-CSF(+)
G-CSF
CT

Neutrophils in the body
• 3-8,000/mL of blood
• ~70% of WBC
• T1/2 = 4-7 hours in blood
• T1/2 = 5-6 days in tissues
Guyton text book of physiology
Neutropenia
• Normal ANC 1500 to 8000 cells/mm³
• Neutropenia: ANC < 1500 cells / mm3
• Mild Neutropenia: 1000-1500 cells / mm3
• Moderate Neutropenia: 500-999 cells / mm3
• Severe Neutropenia: < 500 cells / mm3
• Profound Neutropenia: <100 cells/ mm³
• Ganong text book of physiology…

Infection + ABX + Immune system = cure
• Normal Gross Anatomy
• Skin Integrity
• Intact mucous membranes
• Intact ciliary function
• Absence of Foreign Bodies
• Innate Immunity
PMN,
Macrophages, NK cells, Mast cells and
basophils)
• Complement
• Adaptive immunity
T cells CD 4 and CD 8
B cells

• The life of the granulocytes after beingreleased from the bone marrow is normally 4to 8 hours circulating in the blood and another4 to 5 days in tissues where they are needed.In times of serious tissue infection, this totallife span is often shortened to only a fewhours because the granulocytes proceed evenmore rapidly to the infected area, performtheir functions,and, in the process, arethemselves destroyed.

When Does Neutropenia Occur?
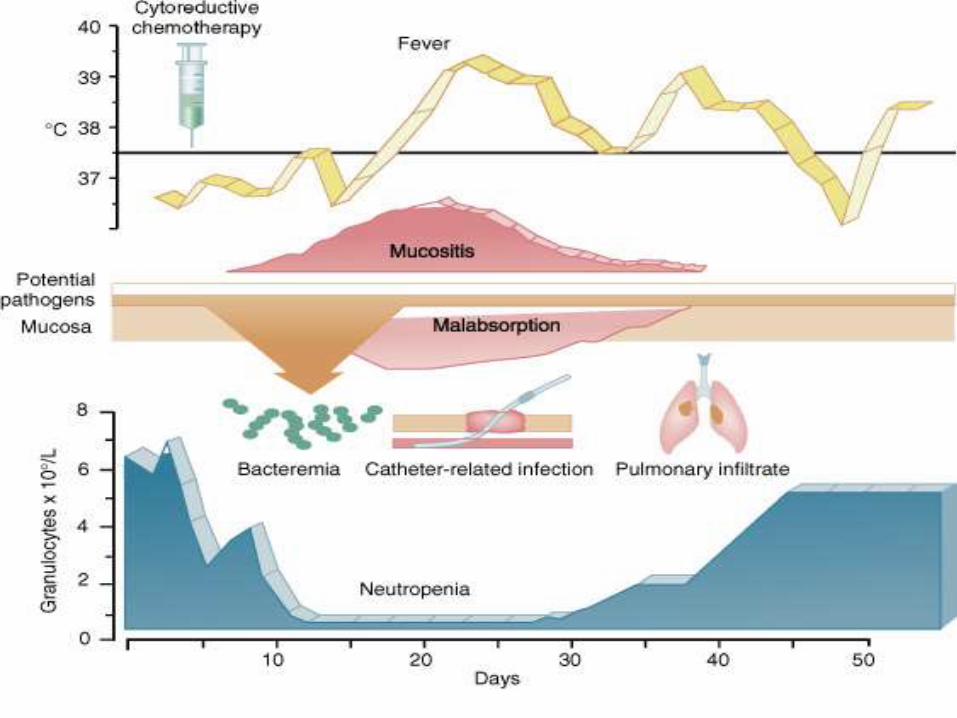
• Most chemotherapy agents/protocols cause neutropenia nadir at 10-14 days
• But can see anytime from a few days after chemotherapy to up to 4-6 weeks later depending on the agents used
• Neurtopenia is one of the risk factors in cancerpatients(others host factors hematological /solidmalignancies,aspelenia, treatment related factorsneutropenia,mucosistis ,steriods,monocolnal antibodies,RTETC)

Why is this an Oncologic emergency ??
EPIDEMIOLOGY

Morbidity and Financial Burden of Infections in Patients with Neoplasia
• Number of patients with cancer and infectious complications hospitalized (USA): 60,000 / year
• Average cost of hospitalization: $10,372
• Motality due to infection: 10%
– Solid tumors: 8% (lung: 13.4%, breast: 3.6%)
– Leukemia: 14%, Lymphoma: 9%
• Motality higher in confirmed infections:
invasive aspergillosis (39%), candidiasis (37%),
Gram (-)ve sepsis (34%), Gram (+)ve sepsis(21%)
Cagiarro et al. Cancer 2005;103:1916Kuderer et al. Cancer 2006;106:2258

Febrile Neutropenia• Appears in 10 % - 30 % of patients with solid tumors• Often characteristic signs and symptoms of infection are absent• 50% of febrile neutropenic patients have infection• 20% of febrile neutropenic patients + PMN <100 /mm3 have
septicemia• Frequent inability to identify the pathogen(motality rate 10% in solid
tumors and 14% in hematological malignancies)
• Neutopenia depends on patient factors(individalised),type of chemo/number of cycles./type of tumor.
• Crawford et al fould 96% of patients treated with CAE IN SCCLexperienced neutropenia
• Blay et al over all incidence of neutropenia (grade 4) in 51% ofpatients treated for lymphoma and solid tissue malignancies.
Sepkowitz K.A. Clin Infect Dis 2005;40 Suppl 4:S253-6Pizzo P.A. N Engl J Med 1993;328:1323

• 2142 patients with febrile neutropenia from
cancer chemotherapy
– 499 (23%) patients with bacteremia
– Gram-positive: 57%
– Gram-negative: 34%
– Polymicrobial bacteremias: 10%
Bacteremia in febrile neutropenic cancer patients
Klastersky et al. Int J Antimicrob Agents 2007; 30(Suppl 1): S51–9.

Epidemiology contd
• Changing etiology of bacteremiaIATG-EORTC 1973-2000 trials of febrile neutropenia
Gram positive dominant since mid 1980s1) More intensive chemoTx
•Mucositis2) In-dwelling catheters
• Cutaneous-IV portal3) Selective antiBx pressure
•Fluoroquinolones• Co-trimoxazole
4) Antacids•Promote oro-oesophagealcolonisation with GPC
Viscoli et al, Clin Inf Dis;40:S240-5
Gram negative resurgence

Epidemiology --NEJM, 1979;284:1061
Retrospective data have shown that
– ~ 50 % of Pseudomonas Aeruginosa Bacteremia result in death within 72 hours when ANC is < 1000
– Early trials aimed at Pseudomonas showed thatCarbapenicillin /Gentamicin decreased Mortality by 33 %

Common Microbes
Gram-positive cocci and bacilli
• Staph. aureus
• Staphylococcus epidermidis
• Enterococcus faecalis/faecium
• Corynebacterium species
Gram-negative
• bacilli and cocci
• Escherichia coli
• Klebsiella species
• Pseudomonas aeruginosa
FUNGI
• Candida- Non albicans emerging
• Aspergillus >> in HSCT

Anerobic Bacteria
• Bacteroides spp
• Clostridium spp
• Fusobacterium spp
• Propionibacterium spp
• Peptococcus spp
• Veillonella spp
• Peptostreptococcus spp

Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
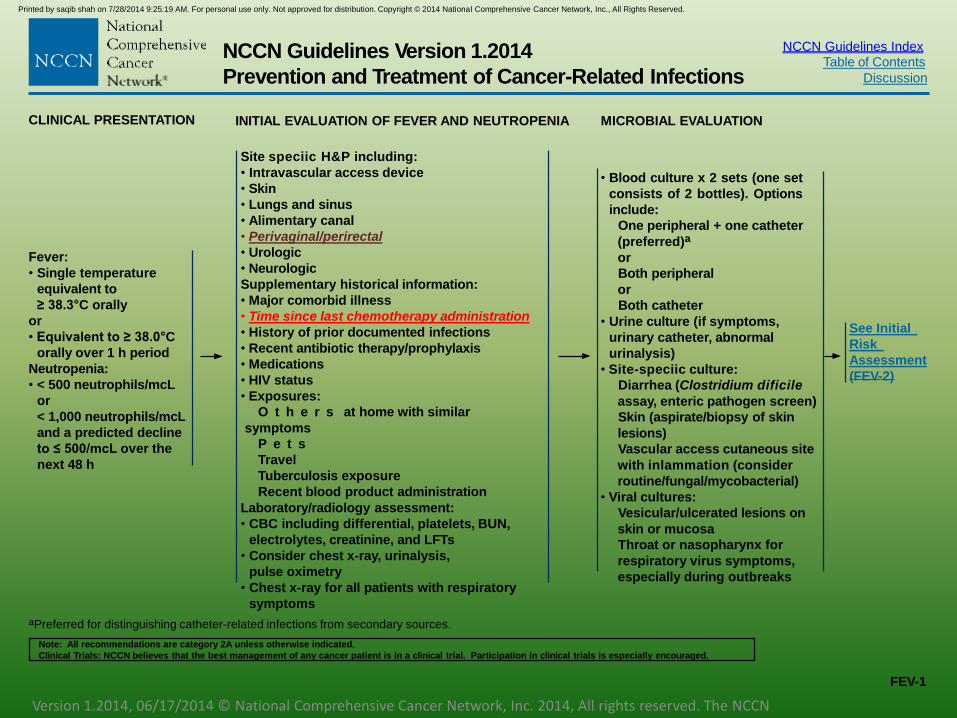
CLINICAL PRESENTATION INITIAL EVALUATION OF FEVER AND NEUTROPENIA MICROBIAL EVALUATION
Fever:
• Single temperature
equivalent to
≥ 38.3°C orally
or
• Equivalent to ≥ 38.0°C
orally over 1 h period
Neutropenia:
• < 500 neutrophils/mcL
or
< 1,000 neutrophils/mcL
and a predicted decline
to ≤ 500/mcL over the
next 48 h
Site speciic H&P including:
• Intravascular access device
• Skin
• Lungs and sinus
• Alimentary canal
• Perivaginal/perirectal
• Urologic
• Neurologic
Supplementary historical information:
• Major comorbid illness
• Time since last chemotherapy administration
• History of prior documented infections
• Recent antibiotic therapy/prophylaxis
• Medications
• HIV status
• Exposures:
O t h e r s at home with similar
symptoms
P e t s
Travel
Tuberculosis exposure
Recent blood product administration
Laboratory/radiology assessment:
• CBC including differential, platelets, BUN,
electrolytes, creatinine, and LFTs
• Consider chest x-ray, urinalysis,
pulse oximetry
• Chest x-ray for all patients with respiratory
symptoms
• Blood culture x 2 sets (one set
consists of 2 bottles). Options
include:
One peripheral + one catheter
(preferred)a
or
Both peripheral
or
Both catheter
• Urine culture (if symptoms,
urinary catheter, abnormal
urinalysis)
• Site-speciic culture:
Diarrhea (Clostridium dificile
assay, enteric pathogen screen)
Skin (aspirate/biopsy of skin
lesions)
Vascular access cutaneous site
with inlammation (consider
routine/fungal/mycobacterial)
• Viral cultures:
Vesicular/ulcerated lesions on
skin or mucosa
Throat or nasopharynx for
respiratory virus symptoms,
especially during outbreaks
See Initial
Risk
Assessment
(FEV-2)
aPreferred for distinguishing catheter-related infections from secondary sources.
FEV-1
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.

• Definition developed by infection disease society of america(IDSA) and the u.s food and drug adminstration deptt(FDA)
• Patient with neutropenia but signs and symptoms of infection (eg abdominal pain,mucositis,perirectal pain ) without fever is to be taken as active infection..
• Patient on steriods may also blunt fever response and localising signs of infection..

Febrile NeutropeniaTreatment
• Emergency situation• Treatment initiation within 2 hours
• Morbidity >70% if delay of initiation of antimicrobial chemotherapy
• A) Risk assessment
• B) Antimicrobial coverage• Wide spectrum
• Local microbial flora susceptibility pattern
• Previous antimicrobial therapy
Sepkowitz K.A. Clin Infect Dis 2005;40:S253Schimpff SC et al. N Engl J Med 1971;284:1061
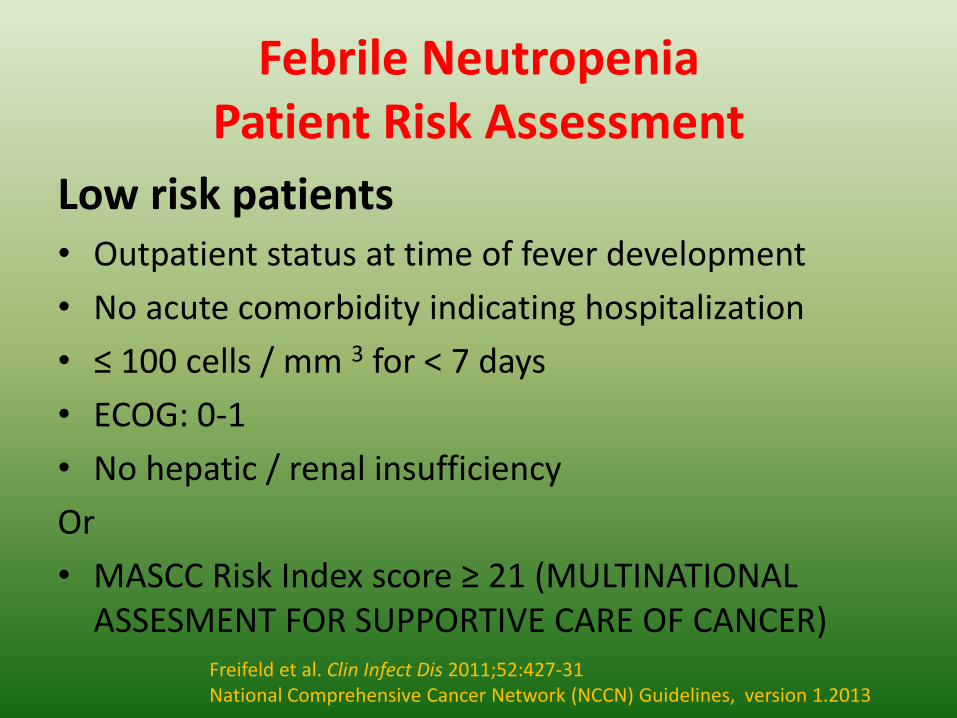
Febrile NeutropeniaPatient Risk Assessment
Low risk patients• Outpatient status at time of fever development
• No acute comorbidity indicating hospitalization
• ≤ 100 cells / mm 3 for < 7 days
• ECOG: 0-1
• No hepatic / renal insufficiency
Or
• MASCC Risk Index score ≥ 21 (MULTINATIONAL ASSESMENT FOR SUPPORTIVE CARE OF CANCER)
Freifeld et al. Clin Infect Dis 2011;52:427-31National Comprehensive Cancer Network (NCCN) Guidelines, version 1.2013
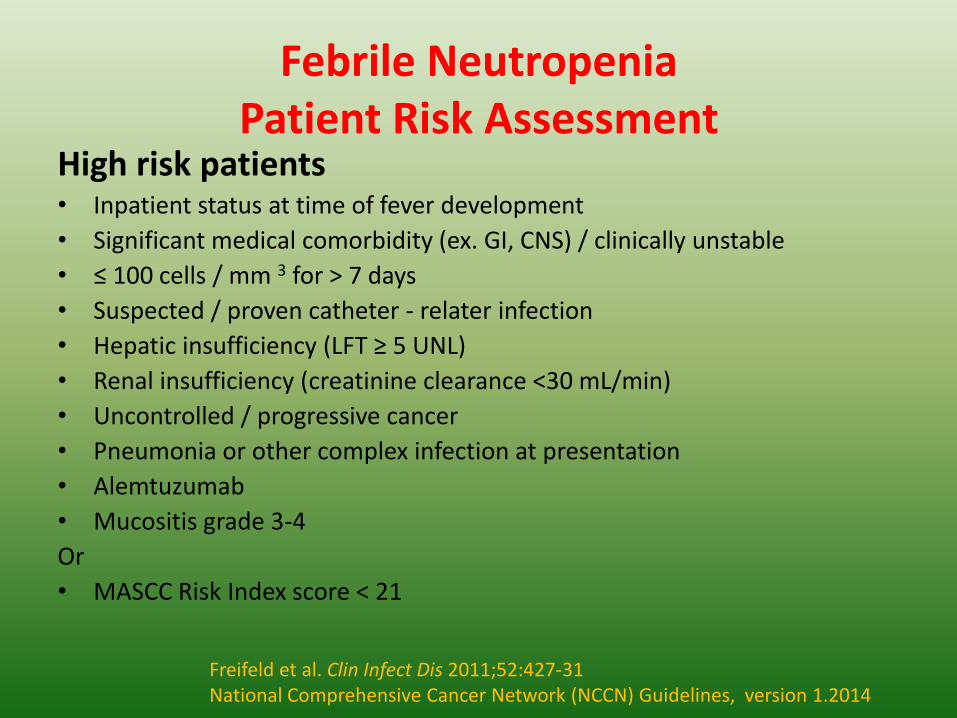
Febrile NeutropeniaPatient Risk Assessment
High risk patients• Inpatient status at time of fever development
• Significant medical comorbidity (ex. GI, CNS) / clinically unstable
• ≤ 100 cells / mm 3 for > 7 days
• Suspected / proven catheter - relater infection
• Hepatic insufficiency (LFT ≥ 5 UNL)
• Renal insufficiency (creatinine clearance <30 mL/min)
• Uncontrolled / progressive cancer
• Pneumonia or other complex infection at presentation
• Alemtuzumab
• Mucositis grade 3-4
Or
• MASCC Risk Index score < 21
Freifeld et al. Clin Infect Dis 2011;52:427-31National Comprehensive Cancer Network (NCCN) Guidelines, version 1.2014

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
RISK ASSESSMENT RESOURCES
USING THE MASCC RISK-INDEX SCORE
• Using the visual analogue score, estimate the patient's burden of illness at the time of
initial clinical evaluation. No signs or symptoms or mild signs or symptoms are scored
as 5 points, moderate signs or symptoms are scored as 3 points. These are mutually
exclusive. No points are scored for severe signs or symptoms or moribund.
• Based upon the patient's age, past medical history, present clinical features and site of
care (input/output when febrile episode occurred), score the other factors in the model
and total the sum.
MASCC RISK-INDEX SCORE/MODEL1
Characteristic
• Burden of illness
No or mild symptoms
M o d e r a t e
symptoms
• No hypotension
• No COPD
• Solid tumor or
Weight
Hematolo
gic malignancy with no
previous fungal infection
• No dehydration
• Outpatient status
• Age <60 years
BURDEN OF ILLNESS
How sick is the patient at presentation?
No signs Mild signs Moderate Severe Moribund
or or signs or signs or
symptoms symptoms symptoms symptoms
Estimate the burden of illness
considering all comorbid conditions
5
3
5
4
4
3
3
2
1Klastersky J, Paesmans M, Rubenstein EJ et al. The Multinational Association for Supportive Care in Cancer Risk Index: A Multinational Scoring System forIdentifying Low-Risk Febrile Neutropenic Cancer Patients. J Clin Oncol 2000;18:3038-51.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-D
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Duration of Neutropenia
• < 7 days LOW risk
• > 7 days HIGH RISK
• Problem with MASCC index:- duration of neutropenia not included..

Duration Of Neutropenia1988,Rubin and colleagues (cancer invest journal)
• < 7 days of neutropenia
~ response rates to initial antimicrobial therapy was 95%, compared to only 32% in patients with more than 14 days of neutropenia ( <.001)
~ patients with intermediate durations of neutropenia between 7 and
14 days had response rates of 79%

Advantages of Outpatient Therapy
• Improved quality of life
• Lower incidence of nosocomial infections
• Simplification of antimicrobial therapy
• Lower cost
Uzun O and Anaizzie E.J. J Antimicrob Chemother 1999;43(3):317-320

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
OUTPATIENT THERAPY FOR LOW-RISK PATIENTS
INDICATION ASSESSMENTMANAGEMENT
Patient determined to be in low-risk
category on presentation with fever
and neutropeniab
• Careful examination
• Review lab results: no critical
values
• Review social criteria for home
therapy
Patient consents to home care
24 h home caregiver available
Home telephone
Access to emergency facilities
Adequate home environment
Distance within approximately
one hour of a medical center
or treating physician's ofice
• Assess for oral antibiotic
therapy
No nausea and vomiting
Able to tolerate oral
medications
N o t o n p r i o r
luoroquinolone
prophylaxis
Observation period (2-12 h) (category
2B) in order to:
• Conirm low-risk status and ensure
stability of patient
• Observe and administer irst dose
of antibiotics and monitor for
reaction
• Organize discharge plans to home
and follow-up
• Patient education
• Telephone follow-up within 12-24 h
See Treatment
and Follow-up
(FEV-4)
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-3Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
bRisk categorization refers to risk of serious complications, including mortality, in patients with neutropenic fever. See Risk Assessment Resources (FEV-D).
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.

ORAL vs IV
• For patients who are low risk for developing infection-related complications during the course of neutropenia,
~ Oral ciprofloxacin plus amoxicillin/clavulanate
~ Oral ciprofloxacin plus clindamycin
for PCN allergy

• Oral versus intravenous empirical antimicrobial therapy for fever inpatients with granulocytopenia who are receiving cancer chemotherapy.International Antimicrobial Therapy Cooperative Group of the EuropeanOrganization for Research and Treatment of Cancer(NEJM).
• Abstract• BACKGROUND:Intravenously administered antimicrobial agents have been the standard choice for the
empirical management of fever in patients with cancer and granulocytopenia. If orally administered empirical therapy is as effective as intravenous therapy, it would offer advantages such as improved quality of life and lower cost.
• METHODS:In a prospective, open-label, multicenter trial, we randomly assigned febrile patients with cancer who had granulocytopenia that was expected to resolve within 10 days to receive empirical therapy with either oral ciprofloxacin (750 mg twice daily) plus amoxicillin-clavulanate (625 mg three times daily) or standard daily doses of intravenous ceftriaxone plus amikacin. All patients were hospitalized until their fever resolved. The primary objective of the study was to determine whether there was equivalence between the regimens, defined as an absolute difference in the rates of success of 10 percent or less.
• RESULTS:Equivalence was demonstrated at the second interim analysis, and the trial was terminated after the enrollment of 353 patients. In the analysis of the 312 patients who were treated according to the protocol and who could be evaluated, treatment was successful in 86 percent of the patients in the oral-therapy group (95 percent confidence interval, 80 to 91 percent) and 84 percent of those in the intravenous-therapy group (95 percent confidence interval, 78 to 90 percent; P=0.02). The results were similar in the intention-to-treat analysis (80 percent and 77 percent, respectively; P=0.03), as were the duration of fever, the time to a change in the regimen, the reasons for such a change, the duration of therapy, and survival. The types of adverse events differed slightly between the groups but were similar in frequency.
• CONCLUSION:- In low-risk patients with cancer who have fever andgranulocytopenia, oral therapy with ciprofloxacin plus amoxicillin-clavulanate isas effective as intravenous therapy.

Bacteremia due to viridans streptococci in neutropenic patients: areview.(Bochud et al)
• Abstract:-Viridans streptococci have long been considered, with theexception of the ability to cause endocarditis, as minor pathogenic agents.More recently, however, these bacteria have become a major concern inneutropenic patients undergoing a chemotherapeutic treatment. In thishigh-risk population, they can be responsible for up to 39% of bacteremiacases and are the most frequent cause of this type of infection. The mostfrequently isolated species in blood cultures are Streptococcus mitis andStreptococcus sanguis II. Viridans streptococcus bacteremia can beaccompanied by serious complications, like adult respiratory distresssyndrome (ARDS) (3% to 33%), shock (7% to 18%) or endocarditis (7% to8%). Mortality rates range from 6% to 30%. Case-control studies haveidentified the following risk factors: severe neutropenia (< 100neutrophils/mm3), prophylactic antibiotic treatments with quinolone orco-trimoxazole, absence of intravenous antibiotics at the time ofbacteremia, high doses of cytosine arabinoside, oropharyngeal mucositis,and heavy colonization by viridans streptococci. The introduction ofpenicillin in prophylactic antibiotic treatments has reduced the incidenceof these infections, but the long-term use of penicillin could becompromised by the emergence of resistant strains.

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
OUTPATIENT THERAPY FOR LOW-RISK PATIENTS
TREATMENT OPTIONS FOLLOW-UP
• IV antibiotics at home
• Daily long-acting intravenous
agent ± oral therapyd
H o m e o r ofice
• Oral therapy onlye:
Ciproloxacinf plus
amoxicillin/clavulanateg
(category 1)
Moxiloxacinf,h (category 1)
hNot active against Pseudomonas.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-4Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
• Patient should be monitored daily
• Daily examination (clinic or home visit) for the
irst 72 h to assess response, toxicity, and
compliance; if responding, then telephone
follow-up daily thereafter.
• Speciic reasons to return to clinic:
Any positive culture
New signs/symptoms reported by the patient
P e r s i s t e n t or recurrent fever at
days 3-5
Inability to continue prescribed antibiotic
regimen (ie, oral intolerance)
Ofice visit for infusion of IV antibiotics
dAgents active against Pseudomonas should be included.eCriteria for oral antibiotics: no nausea or vomiting, patient able to tolerate oral medications, and patient not on prior fluoroquinolone prophylaxis.fThe fluoroquinolone chosen should be based on reliable Gram-negative bacillary activity, local antibacterial susceptibilities, and the use of quinolone prophylaxis of
fever and neutropenia.gUse clindamycin for penicillin-allergic patients.
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
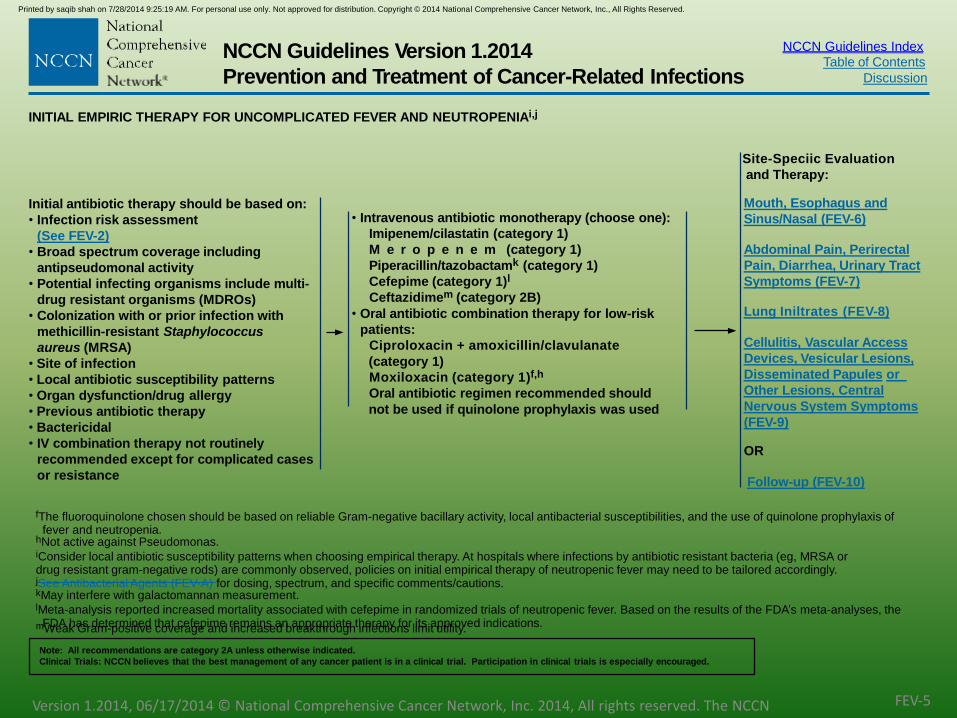
• Intravenous antibiotic monotherapy (choose one):
Imipenem/cilastatin (category 1)
M e r o p e n e m (category 1)
Piperacillin/tazobactamk (category 1)
Cefepime (category 1)l
Ceftazidimem (category 2B)
• Oral antibiotic combination therapy for low-risk
patients:
Ciproloxacin + amoxicillin/clavulanate
(category 1)
Moxiloxacin (category 1)f,h
Oral antibiotic regimen recommended should
not be used if quinolone prophylaxis was used
INITIAL EMPIRIC THERAPY FOR UNCOMPLICATED FEVER AND NEUTROPENIAi,j
Site-Speciic Evaluation
and Therapy:
Initial antibiotic therapy should be based on:
• Infection risk assessment
(See FEV-2)
• Broad spectrum coverage including
antipseudomonal activity
• Potential infecting organisms include multi-
drug resistant organisms (MDROs)
• Colonization with or prior infection with
methicillin-resistant Staphylococcus
aureus (MRSA)
• Site of infection
• Local antibiotic susceptibility patterns
• Organ dysfunction/drug allergy
• Previous antibiotic therapy
• Bactericidal
• IV combination therapy not routinely
recommended except for complicated cases
or resistance
Mouth, Esophagus and
Sinus/Nasal (FEV-6)
Abdominal Pain, Perirectal
Pain, Diarrhea, Urinary Tract
Symptoms (FEV-7)
Lung Iniltrates (FEV-8)
Cellulitis, Vascular Access
Devices, Vesicular Lesions,
Disseminated Papules or
Other Lesions, Central
Nervous System Symptoms
(FEV-9)
OR
Follow-up (FEV-10)
fThe fluoroquinolone chosen should be based on reliable Gram-negative bacillary activity, local antibacterial susceptibilities, and the use of quinolone prophylaxis offever and neutropenia.
hNot active against Pseudomonas.iConsider local antibiotic susceptibility patterns when choosing empirical therapy. At hospitals where infections by antibiotic resistant bacteria (eg, MRSA ordrug resistant gram-negative rods) are commonly observed, policies on initial empirical therapy of neutropenic fever may need to be tailored accordingly.jSee Antibacterial Agents (FEV-A) for dosing, spectrum, and specific comments/cautions.kMay interfere with galactomannan measurement.lMeta-analysis reported increased mortality associated with cefepime in randomized trials of neutropenic fever. Based on the results of the FDA’s meta-analyses, the
FDA has determined that cefepime remains an appropriate therapy for its approved indications.mWeak Gram-positive coverage and increased breakthrough infections limit utility.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-5Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.

~ A meta analysis of 33 RCTs until Feb 2005 on
Antipseudomonal B lactams as MONOtherapies showedthat ~CEFEPIME increases 30 day all cause mortality.. Asubsequent meta-analysis by the FDA, using additional databeyond what was used in the Yahav study, did not find astatistically significant increase in mortality for cefepime-treated patients compared with controls. Thus, the FDAconcluded that cefepime remains appropriate therapy forits approved indications
~ Carbapenems were associated with increased
Pseudomembranous colitis..

Febrile NeutropeniaEmpiric Monotherapy
• Ceftazidime is no longer reliable as monotherapy
decreasing potency against gram (-) ves
poor activity against gram (+)ves (streptococci)
• Aminoglycosides not to be used as monotherapy empirically due to rapid emergence of resistance
Freifeld et al. Clin Infect Dis 2011;52:427-31

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
INITIAL CLINICAL
PRESENTATION
(DAY 0)
FINDING EVALUATION ADDITIONS TO INITIAL EMPIRIC REGIMENn,o,p
All febrile neutropenic patients should receive broad-spectrum antibiotics (FEV-5)
Mouth/
mucosal
membrane
Necrotizing
ulceration
Thrush
Vesicular lesions
• Culture and Gram stains
Viral - Herpes simplex virus
(HSV)
Fungal
C o n s i d e r
l e u k e m i c iniltrate
• Biopsy suspicious lesions
• Ensure adequate anaerobic activity
• Consider anti-HSV therapy
• Consider systemic antifungal therapy
• Antifungal therapy
F l u c o n a z o l e irst-line
therapy
Voriconazole, posaconazole, or
echinocandin if refractory to luconazole
Anti-HSV therapy (category 1)
Viral cultures or PCR or
other diagnostics and DFA
direct luorescent antibody
test for HSV and Varicella-
zoster virus (VZV)
• Culture suspicious oral
lesions
HSV
Fungal
• Consider endoscopy, if no
response to therapy
• Consider CMV esophagitis
in patients at high risk for
CMV disease
Esophagus•Retrosternal burning
•Dysphagia/
odynophagia
• Initial therapy guided by clinical indings
(eg, thrush or perioral HSV)
• Antifungal therapy for thrush
F l u c o n a z o l e , irst-line
therapy
Voriconazole, posaconazole, or
echinocandin if refractory to luconazole
• Consider acyclovir for possible HSV
Sinus/
nasal
• Sinus tenderness
• Periorbital cellulitis
• Nasal ulceration
• Unilateral eye tearing
• High resolution sinus
CT/orbit MRI
• ENT/ophthalmological
urgent evaluation
• Culture and stains/
biopsy
• Add vancomycin if periorbital cellulitis noted
• Add lipid amphotericin B preparation to
cover possible aspergillosis and
mucormycosis in high-risk patients with
suspicious CT/MRI indingsq
See
Follow-up(FEV-10)
nSee Antibacterial Agents (FEV-A) for dosing, spectrum, and specific comments/cautions.oSee Antifungal Agents (FEV-B) for dosing, spectrum, and specific comments/cautions.pSee Antiviral Agents (FEV-C) for dosing, spectrum, and specific comments/cautions.qPosaconazole can be considered for patients who have invasive, refractory infections or who have intolerance to amphotericin B formulations. Posaconazole is not
approved by the FDA as either primary or invasive, refractory therapy for invasive fungal infections.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-6Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
PEARLS(NCCN guidelines)
A trial of fluconazole and acyclovir (5 mg/kg IV every 8 hours in patients withnormal renal function) should be considered in neutropenic patients andother highly immunocompromised persons with symptoms that suggestesophagitis..
Fluconazole is recommended as first If patients do not respond, the dose offluconazole can be increased up to 800 mg daily (in adults with normal renalfunction)
The sinuses are a common site of bacterial infection. Patients with severeand prolonged neutropenia (e.g., more than 10 days) and allogeneic HSCTrecipients with GVHD are particularly susceptible to invasive mold infections.

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
INITIAL CLINICAL
PRESENTATION
(DAY 0)
EVALUATIONs ADDITIONS TO INITIAL EMPIRIC REGIMENn,o,p
All febrile neutropenic patients should receive broad-spectrum antibiotics (FEV-5)
Abdominal
painr
• Abdominal CT (preferred) or ultrasound
• Alkaline phosphatase, transaminases,
bilirubin, amylase, lipase
• Oral vancomycin or
metronidazole if C. dificile
suspected
• Ensure adequate anaerobic
therapy
• Ensure adequate anaerobic
therapy
• Consider enterococcalt
coverage
• Consider local care (sitz baths,
stool softeners)
Perirectal
pain
• Perirectal inspection
• Consider abdominal/pelvic CT
Diarrhea
• C. dificile assay
• Consider testing for rotavirus and
norovirus in winter months and during
outbreaks
• Consider stool bacterial cultures and/or
parasite exam if travel/lifestyle history or
community outbreak indicate exposure
• Consider testing for adenovirus
If C. dificile suspected,
consider adding oral
metronidazole or oral
vancomycin pending assay
results: IV metronidazole
should be used in patients who
cannot take oral agents
Urinary tract
symptoms• Urine culture
• UrinalysisNo additional therapy until
speciic pathogen
identiied
SeeFollow-up(FEV-10)
nSee Antibacterial Agents (FEV-A) for dosing, spectrum, and specific comments/cautions.oSee Antifungal Agents (FEV-B) for dosing, spectrum, and specific comments/cautions.pSee Antiviral Agents (FEV-C) for dosing, spectrum, and specific comments/cautions.rSurgical and other subspecialty (eg, gastroenterology, interventional radiology) consultations should be considered for these situations as clinically indicated.sLab studies include CMV antigens/PCR and abdominal/pelvic CT.tEnterococcal colonization must be differentiated from infection. Vancomycin use must be minimized because of the risk of vancomycin resistance.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-7Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
PRINCIPLES OF DAILY FOLLOW-UP FOLLOW-UP THERAPY
• Daily site-speciic H&P
• Daily review of
laboratory tests and
cultures: document
clearance of
bacteremia, fungemia
with repeat blood
cultures
• Evaluate for response
to therapy (in 3-5 d) and
drug toxicity:
F e v e r trends
Signs and symptoms
of infection
• Evaluation of drug
toxicity including end-
organ toxicity (LFTs and
renal function tests at
least 2x/wk)
Responding/clinically stable
• Decreasing fever trend
• Signs and symptoms of
infection are stable or
improving
• Patient is
hemodynamically stable
No change in initial
empiric regimen.
If initially started
appropriately on
agent for gram-
positive resistant
infection,aa continue
course of therapy.
Initial antibiotic
regimen should be
continued at least
until neutrophil count
is ≥ 500 cells/mcL
and increasing
Documented
infection
See Duration(FEV-11)
Fever
resolved,
unknown
origin
Neutrophils
≥ 500 cells/mcL
Discontinue
therapy
Neutrophils
< 500 cells/mcLbb
Continue
current
regimen until
neutropenia
resolvescc
Non-responding/clinically unstable
• Persistently or intermittently
febrile
• Signs and symptoms of infection
are not improving
• Patient may be hemodynamically
unstable
• Persistent positive blood cultures
• Broaden coverage to
include anaerobes,
resistant Gram-negative
rods, and resistant Gram-
positive organisms, as
clinically indicated
• Consider reevaluation
with CT scans
• Consider adding G-CSF or
GM-CSF (category 2B)
• Ensure coverage for
Candida
• ID consult
• Consider antifungal
therapy with activity
against molds for fever
continuing ≥ 4 days
of empiric antibiotic
therapyaa
• Duration of therapy
depends on clinical
course, neutropenia
recovery, toxicity,
and opinions of ID
consultants
aaSee Appropriate Use of Vancomycin and Other Agents for Gram-positive Resistant Infections (FEV-F).bbIn the case of prolonged neutropenia (>14d), consider judicious assessment of empiric therapy.ccIn patients who defervesced, it may be appropriate in some cases to de-escalate to fluoroquinolone.ddThe timing to add empirical antifungal therapy varies with the risk of invasive mold infection but generally ranges between 4-7d of neutropenic fever. In patients at
high-risk for mold infection (neutropenia > 10d, allogeneic stem cell transplant recipients, high-dose corticosteroids), the Panel recommends adding empirical
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
antifungal therapy after 4th d unless patient is receiving prophylaxis directed against molds.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-10
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines

Evaluation and Follow-up Therapy in Non-responding Patients
Non infectious etiology(drug fever) nonbacterial infection (fungal or viral) abacterial infection that is resistant to empiric antibiotics, a venous access orclosed space infection, or inadequate antimicrobial serum levels,deep tissueinfections may take longer than fever of unknown etiology to respond to
antimicrobial therapy. unusual infections (e.g., toxoplasmosis) may complicateneutropenia, particularly if immunosuppressive agents (e.g., high-dosecorticosteroids) are alsoused. the panel strongly recommends an infectiousdisease consultation for these patients.
•Broaden coverage to include anaerobes, resistant Gram-negative
rods, and resistant Gram- positive organisms, as clinically indicated
•Consider reevaluation with CT scans
•Consider adding G-CSF or GM-CSF (category 2B)
•Ensure coverage for Candida
•ID consult
NCCN GUIDELINES FOR NRPs

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
FOLLOW-UP THERAPY FOR
RESPONDING DISEASE
SUGGESTED MINIMUM DURATION OF THERAPY FOR DOCUMENTED INFECTIONn,o,p
These are general guidelines and may need to be revised for individual patients.
Documented
infection
• Initial antibiotic regimen should
generally be continued until
neutrophil count is ≥ 500 cells/
mcL and increasing
• Duration of antimicrobial therapy
may be individualized based
upon:
Neutrophil recovery
Rapidity of defervescence
Speciic site of infection
Infecting pathogen
Patient's underlying illness
• Skin/soft tissue: 7-14 d
• Bloodstream infection (uncomplicated)
G r a m - n e g a t i v e : 10-14 d
G r a m - p o s i t i v e : 7-14 d
S. aureus: at least 2 weeks after irst negative blood culture; treatment
may need to be prolonged in cases of endovascular involvement
Yeast: ≥ 2 wks after irst negative blood culture
Consider catheter removal for bloodstream infections with Candida,
S. aureus, Pseudomonas aeruginosa, Corynebacterium jeikeium,
Acinetobacter, Bacillus organisms, atypical mycobacteria, yeasts,
molds, vancomycin-resistant enterococci, and Stenotrophomonas
maltophilia
• Sinusitis: 10-21 d
• Catheter removal for septic phlebitis, tunnel infection, or port pocket
infection
• Bacterial pneumonia: 10-21 d
• Fungal (mold and yeast):
Candida: minimum of 2 wks after irst negative blood culture
Mold (eg, Aspergillus): minimum of 12 wks
• Viral:
HSV/VZV: 7-10 d (category 1); acyclovir, valacyclovir, or famciclovir
(uncomplicated, localized disease to the skin)
nSee Antibacterial Agents (FEV-A) for dosing, spectrum, and specific comments/cautions.oSee Antifungal Agents (FEV-B) for dosing, spectrum, and specific comments/cautions.pSee Antiviral Agents (FEV-C) for dosing, spectrum, and specific comments/cautions.eeSome centers use higher dose (for example 150 mg).
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-11
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Febrile NeutropeniaGram positive antimicrobial coverage
Gram Positive organisms
Increasing in frequency
Central Venous Catheters (?)
Antimicrobial Chemotherapy
– vancomycin
– linezolid
– quinopristin - dalfopristin
– tigecycline
– daptomycin
• Discontinuation of empiric gram(+)ve Rx post 72 hours if susceptible bacteria are not isolated from the patient
Freifeld et al. Clin Infect Dis 2011;52:427-31Hughes at al. Clin Infect Dis 2002;34:730

• Vancomycin should be considered in thefollowing clinical situations
• Clinically apparent, serious IV catheter-related infection (tocovercoagulase-negative staphylococcal isolates, which areusually betalactam antibiotic-resistant and MRSA).
• Blood cultures positive for Gram-positive bacteria beforefinal identification and susceptibility testing;
• Known colonization with penicillin/cephalosporin–resistantpneumococci or MRSA;
• Clinical instability (e.g., hypotension or shock), pending theresults of cultures.
• Soft tissue infection (particularly in regions where MRSAinfection is common).
• management of complicated cases of Clostridium difficileinfections, oral vancomycin can be considered.

The NCCN Guidelines panel strongly recommendsthat vancomycin should not be routinely added to anempiric regimen solely based on persistentneutropenic fever of unknown etiology.(2 trials)
• In patients with neutropenic fever and severe mucositis who receivingimipenem/cilastatin, meropenem, or piperacillin/tazobactam antibiotics withactivity against oral flora), it does not appear that the addition of vancomycin is
advantageous .
• A smaller randomized, placebo-controlled study did not show any advantage after adding teicoplanin (a glycopeptide antibiotic similar to vancomycin) in patients with neutropenic fever that persisted after 3 to 4 days of empiric imipenem/cilastatin
MultiDrug Resistant (MDR) organisms
Risk Factors
– Previous infection
– Colonization
– Admission in hospital with endemic resistant bacteria
• MRSA: vancomycin, linezolid, daptomycin
• VRE: linezolid, daptomycin
• ESBLs: carbapenem
• KPCs: colistin, tigecycline

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
ANTIBACTERIAL AGENTS: GRAM-POSITIVE ACTIVITY
aThese drugs are not recommended as monotherapy for fever in the setting of neutropenia and should only be added for documentedinfection with resistant Gram-positive organisms or if certain risk factors are present. (See FEV-F)
bRequires dose adjustment in patients with renal insufficiency.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. FEV-A
(Page 1 of 4)
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Continued on next page
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Gram-positiveAgentsa
DOSE SPECTRUM COMMENTS/PRECAUTIONS
Dalfopristin/
Quinupristin
7.5 mg/kg IV every 8 h • Gram-positive
organisms
including most VRE
• Not active against
Enterococcus faecalis
• Signiicant drug interactions
• Use limited by myalgias/arthralgias (up to 47%)
• Requires central venous access delivery
• Avoid use due to toxicity although coverage is good
• Musculoskeletal pain syndrome is a potential toxicity
Daptomycin 6 mg/kg/d IV b • Gram-positive organisms
• Has in vitro activity against
VRE but is not FDA-
approved for this indication
• Weekly CPK to monitor for rhabdomyolysis
• Not indicated for pneumonia due to inactivation by
pulmonary surfactant
• Myositis is a potential toxicity
Linezolid 600 mg PO/IV
every 12 h
Gram-positive
organisms, including
VRE
• Hematologic toxicity (typically with prolonged cases, > 2 wks) may occur,
thrombocytopenia most common (0.3% to 10%)
• Serotonin syndrome rare, use cautiously with SSRI's1
• Not routinely used in fever and neutropenia although, does not impair
neutrophil recovery
• Treatment option for VRE and MRSA
• Peripheral/optic neuropathy with long-term use
Vancomycin 15 mg/kg IV every12 hb
For C.dificile: 125mg PO every 6 h
Gram-positive organisms,
with exception of VRE
and a number of rare
Gram- positive organisms
• Should not be considered as routine therapy for
neutropenia and fever unless certain risk factors present
(See-FEV-F)
• Dosing individualized with monitoring of levels

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
ANTIBACTERIAL AGENTS: ANTI-PSEUDOMONALc
bRequires dose adjustment in patients with renal insufficiency.cEmerging data may support continuous infusion use for higher potency against resistant cases.dNone of these agents are active against MRSA or VRE.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. FEV-A
(Page 2 of 4)
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
ANTI-PSEUDOMONAL AGENTSd DOSE SPECTRUM COMMENTS/PRECAUTIONS
Cefepime 2 grams IV every 8 hb • Broad spectrum activity against most
Gram-positive and Gram-negative
organisms
• Not active against
most anaerobes and
Enterococcus spp
• Use for suspected/proven CNS infection
with susceptible organism
• Increased frequency of resistance among
Gram-negative rod isolates at some centers
• Empiric therapy for neutropenic
fever (category 1)
Ceftazidime 2 grams IV every 8 hb • Relatively poor Gram-
positive activity
• Breakthrough
streptococcal infections
reported
• Not active against
most anaerobes and
Enterococcus spp.
• Use for suspected/proven CNS
infection with susceptible organism
• Increased frequency of resistance among Gram-
negative rod isolates at some centers
• Empiric therapy for neutropenia fever
(category 2B; due to resistance
among certain Gram-negative rods)
Imipenem/cilastatin sodium 500 mg IV every 6 hb • Broad spectrum activity against most
Gram-positive, Gram-
negative and
anaerobic organisms
• Preferred against extended
spectrum beta-lactamase (ESBL) and
serious Enterobacter
infections.
• Carbapenem-resistant Gram-
negative rod infections are an
increasing problem at a
number of centers
• Use for suspected intra-
abdominal source
• Meropenem is preferred over imipenem
for suspected /proven CNS infection
• Carbapenems may lower seizure threshold in
patients with CNS malignancies or infection or with
renal insuficiency
• Effective in nonsocomial pneumonia and
intra- abdominal infections
• Empiric therapy for neutropenic
fever (category 1)
• Data is limited but we would expect that Doripenem
like Meropenem as an anti-pseudomonal
beta-lactam would be eficacious
Meropenem 1 gram IV every 8 hb
(2 g IV every 8 h for
meningitis)
Doripenem 500 mg IV every 8 hb
Piperacillin/tazobactam 4.5 grams IV every 6 hb
Some institutions use
extended infusion: 3.375
g IV every 8 h
• Broad spectrum activity
against most Gram-positive,
Gram- negative and anaerobic
organisms
• Use for suspected intra-abdominal source
• Not recommended for meningitis
• May result in false positive galactomannan2
• Empiric therapy for neutropenic fever (category 1)

NCCN Guidelines Index
eConsider adding a second agent in cases of severe infection based on local susceptibility pattern.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. FEV-A
(Page 3 of 4)Version 1.2014, 06/0172014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
Table of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
ANTIBACTERIAL AGENTS: OTHER
bRequires dose adjustment in patients with renal insufficiency.
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
OTHER ANTIBACTERIAL
AGENTS
DOSE SPECTRUM COMMENTS/CAUTIONS
Aminoglycosides
• Amikacin
• Gentamicin
• Tobramycin
Dosing
individualized with
monitoring of levelsb
• Activity primarily against Gram-negative
organisms
Often used as empiric therapy
in seriously ill or
hemodynamically unstable
patients
Ciproloxacine 500-750 mg PO every
12 hours or 400 mg
IV
every 8-12 hb
For low risk: 500
mg PO every 8 h +
amoxicillin/
clavulanate 500 mg
every 8 h
• Good activity against Gram-negative and
atypical (e.g., Legionella spp.) organisms
• Less active than “respiratory”
luoroquinolones against Gram-positive
organisms
• No activity against anaerobic organisms
• Avoid for empiric therapy if patient
recently treated with luoroquinolone
prophylaxis
• Increasing Gram-negative resistance in
many centers
• Oral antibiotic combination therapy in
low-risk patients (with
amoxicillin/clavulanate or clindamycin)
Levoloxacin 500-750 mg oral
or IV dailyb• Good activity against Gram-negative and
atypical (e.g., Legionella spp.) organisms
• Improved Gram-positive activity
compared to ciproloxacin
• Limited activity against anaerobes
• Prophylaxis in neutropenic patients3,4
• Prophylaxis may increase
bacterial resistance and
superinfection5
• Limited studies as empirical
therapy in patients with fever
and neutropenia
Trimethoprim/
sulfamethoxazol
e (TMP/SMX)
Single or double strength
daily
or
Double strength 3 times
per wk
Activity against P. jiroveccii Highly effective as prophylaxis against
P. jirovecii in high risk
patients (See INF-6)

NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related InfectionsANTIFUNGAL AGENTS: AZOLES
bTherapeutic drug monitoring (TDM) is an ongoing area of research; TDM should be considered in consultation with ID specialists. (See Discussion).
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.FEV-B
(Page 1 of 4)
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
aAzoles inhibit fungal cell membrane synthesis and inhibit cytochrome P450 isoenzymes that may lead to impaired clearance of other drugs metabolized by this pathway. Fluconazole is a
less potent inhibitor of cytochrome P450 isoenzymes than the mold-active azoles. Drug-drug interactions are common and need to be closely monitored (consult package inserts for
details). Reversible liver enzyme abnormalities are observed.
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
AZOLESa DOSE SPECTRUM COMMENTS/CAUTIONS
Fluconazole In adults with normal renal
function: 400 mg IV/PO
daily
• Active against Candida
• Active against dimorphic fungi (eg,
histoplasmosis, coccidioidomycosis)
and C. neoformans
• Candida glabrata is associated with variable resistance
in vitro and Candida krusei is always resistant
• Inactive against molds (eg, Aspergillus
species, Zygomycetes)
Itraconazoleb Oral 400 mg daily (aim for
trough of > 0.25 mcg/mL
after 7 d of therapy)
• Active against Candida, Aspergillus
sp. and some of the rarer molds
• Active against dimorphic fungi and
C. neoformans
• Itraconazole has negative inotropic properties and is
contraindicated in patients with signiicant cardiac
systolic dysfunction
Posaconazoleb • Prophylaxis: 200 mg POTID among high-riskpatients (See INF-2)
• Treatment of refractoryinfection: 400 mg POBID with high fat meal or200 mg PO QID if unableto eat, preferably withacidic beverage
• EC 300mg BID on day1 and then 300 mg POQ day
• Effective as prophylaxis in neutropenic
patients with myelodysplastic
syndrome and acute myelogenous
leukemia4, and in HSCT recipients with
signiicant GVHD5
• Active against Candida, Aspergillus
sp., some Zygomycetes sp., and some
of the rarer molds
• Active against dimorphic fungi and
C. neoformans
• Evaluated as treatment of refractory infection (but not
FDA-approved) in several invasive fungal diseases.
• Data on posaconazole as primary therapy for invasive
fungal infections are limited.
• Should be administered with a full meal or liquid
nutritional supplement or an acidic carbonated
beverage. For patients who cannot eat a full meal or
tolerate an oral nutritional supplement alternative
antifungal therapy should be considered.
• Proton pump inhibtors decrease posaconazole plasma
concentration
Voriconazoleb • IV 6 mg/kg every 12 h
x 2 doses, then 4 mg/
kg every 12 h; oral 200
mg PO BID (for invasive
aspergillosis);1
• IV 6 mg/kg every
12 h x 2, then 3
mg/kg every 12 h
for non-
neutropenic patients with
candidemia2
• Active against Candida, Aspergillus
sp. and some of the rarer molds
• Active against dimorphic fungi and
C. neoformans
• Standard of care as primary therapy for
invasive aspergillosis (category 1)1,3
• Effective in candidemia in
non- neutropenic patients2
• Poor activity against Zygomycetes
• IV formulation should be used with caution in patients
with signiicant pre-existing renal dysfunction based
on potential to worsen azotemia
NCCN Guidelines Index
effective but less toxic than 10 mg/kg/d as initial therapy for invasive mold infections.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. FEV-B
(Page 2 of 4)
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Table of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
ANTIFUNGAL AGENTS: AMPHOTERICIN B FORMULATIONS
Continued on next page
cBroad spectrum of antifungal activity. Significant infusional and renal toxicity, less so with lipid formulations.dThe vast majority of subjects in this trial had invasive aspergillosis; optimal dosing of L-AMB for other mold infections (such as mucormycosis with 3mg/kg/d IV) was as
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
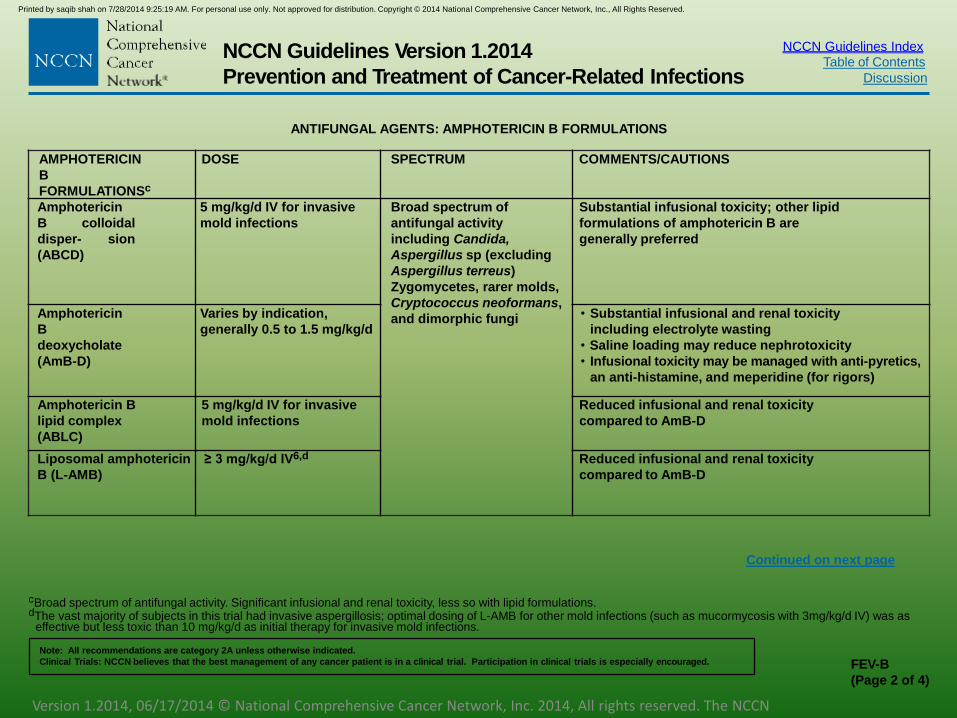
AMPHOTERICIN
B
FORMULATIONSc
DOSE SPECTRUM COMMENTS/CAUTIONS
Amphotericin
B colloidal
disper- sion
(ABCD)
5 mg/kg/d IV for invasive
mold infections
Broad spectrum of
antifungal activity
including Candida,
Aspergillus sp (excluding
Aspergillus terreus)
Zygomycetes, rarer molds,
Cryptococcus neoformans,
and dimorphic fungi
Substantial infusional toxicity; other lipid
formulations of amphotericin B are
generally preferred
Amphotericin
B
deoxycholate
(AmB-D)
Varies by indication,
generally 0.5 to 1.5 mg/kg/d
• Substantial infusional and renal toxicity
including electrolyte wasting
• Saline loading may reduce nephrotoxicity
• Infusional toxicity may be managed with anti-pyretics,
an anti-histamine, and meperidine (for rigors)
Amphotericin B
lipid complex
(ABLC)
5 mg/kg/d IV for invasive
mold infections
Reduced infusional and renal toxicity
compared to AmB-D
Liposomal amphotericin
B (L-AMB)
≥ 3 mg/kg/d IV6,d Reduced infusional and renal toxicity
compared to AmB-D

NCCN Guidelines Index
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
FEV-B(Page 3 of
4)Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCN
Guidelines
Table of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
ANTIFUNGAL AGENTS: ECHINOCANDINS
Continued on next page
eA number of centers use combination voriconazole and an echinocandin for invasive aspergillosis based on in vitro, animal, and limited clinical data.
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
ECHINOCANDINSe DOSE SPECTRUM COMMENTS/CAUTIONS
Anidulafungin 200 mg IV x 1 dose,
then 100 mg/d IV
Active against Candida
and Aspergillus sp. Not
reliable or effective
against other fungal
pathogens.
• Primary therapy for candidemia and
invasive candidiasis (category 1)
• Superior eficacy compared to luconazole as primary
therapy for candidemia and invasive candidiasis11
• Excellent safety proile
Caspofungin • 70 mg IV x 1 dose, then 50 mg
IV daily; some investigators use
70 mg IV daily as therapy for
aspergillosis
• 70 mg IV x 1 dose, followed by
35 mg IV daily for patients
with moderate liver disease
• Primary therapy for candidemia and
invasive candidiasis (category 1)7
• Treatment for invasive, refractory aspergillosis.
Similar eficacy compared to AmB-D as primary
therapy for candidemia and invasive
candidiasis, but signiicantly less toxic7
• 45% success rate as therapy for invasive, refractory
aspergillosis8
• Similar eficacy, but less toxic compared with L-AMB
as empirical therapy for persistent neutropenic fever7
• Excellent safety proile
Micafungin • 100 mg/d IV for
candidemia and 50-100
mg/d IV as prophylaxis
• 150 mg/d IV used at some
centers for Aspergillus
sp. infection
• Primary therapy for candidemia and
invasive candidiasis (category 1)
• Similar eficacy compared to caspofungin9 and
compared to L-AMB10 as primary therapy for
candidemia and invasive candidiasis
• Excellent safety proile

NCCN Guidelines Index
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. FEV-C
(Page 1 of 4)
Version 1.2014, 06/17/2014 © National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCNGuidelines
Table of Contents
Discussion
NCCN Guidelines Version 1.2014
Prevention and Treatment of Cancer-Related Infections
ANTIVIRAL AGENTSa
aRequires dose adjustment in patients with renal insufficiency.bAntiviral prophylaxis should be targeted to specific high-risk patients (see INF-3). In non-transplant high-risk patients, prophylaxis should be administered to patients
seropositive for HSV or VZV (or with a history of chicken pox). In HSCT recipients, prophylaxis is only indicated if either the donor or recipient is seropositive for the virusin question. The indicated doses for antiviral agents are for adults with normal renal function; consult package insert for dose modification in pediatric patient and inpatients with renal impairment. Prophylactic antiviral doses may be higher than those routinely used in immunocompetent persons (for example, for recurrentcold sores); there is substantial variability in the prophylactic doses of acyclovir used in different clinical trials in patients with hematologic malignancies and HSCTrecipients.
cHigh-dose acyclovir and valacyclovir have been used as prophylaxis for CMV. Because these agents have weak activity against CMV, a strategy of CMV surveillanceand pre-emptive therapy with ganciclovir, valganciclovir, or foscarnet is required among patients at high risk for CMV disease.
dIn general, the strategy of CMV surveillance testing by antigenemia or PCR followed by pre-emptive anti-CMV therapy for a positive result is favored over universallong-term prophylaxis in allogeneic HSCT patients.
Printed by saqib shah on 7/28/2014 9:25:19 AM. For personal use only. Not approved for distribution. Copyright © 2014 National Comprehensive Cancer Network, Inc., All Rights Reserved.
AGENT TREATMENT SPECTRUM COMMENTS/CAUTIONS
Acyclovir • Prophylaxisb: HSV (400-800 mg PO BID); VZV in allogeneic HSCT recipients (800 mg PO
BID)1; CMV in allogeneic HSCT recipients (800 mg PO QID)c,2; for patients unable to
tolerate oral therapy, 250 mg/m2 IV every 12 h.
• Post-exposure prophylaxis: 800 mg PO 5 times daily
• Treatment: signiicant mucocutaneous HSV (5 mg/kg IV every 8 h for 7-10 days); single
dermatomal VZV (800 mg PO 5 times daily or 5 mg/kg IV every 8 h for 7-10 days);
disseminated HSV or VZV including viral encephalitis (10 mg/kg IV every 8 h)3
HSV
,
VZV
• Hydration to avoid crystal
nephropathy with high dose
• Dosing based upon
ideal body weight.
Famciclovir Prophylaxis: HSV or VZV (250 mg PO BID)
Treatment: HSV (250 mg PO TID) or VZV (500 mg PO TID)5,6HSV
,
VZV
No data for
oncologic related
prophylaxis
Ganciclovir • Prophylaxis for CMV: 5-6 mg/kg IV every day for 5 days/week from engraftment until day
100 after HSCTd,7
• Pre-emptive therapy for CMV: 5 mg/kg every 12 h for 2 weeks; if CMV remains detectable,
treat with additional 2 weeks of ganciclovir 6 mg/kg daily 5 days per week.
• Treatment: CMV disease (5 mg/kg every 12 h for 2 weeks followed by 5 to 6 mg/kg daily
for at least an additional 2-4 weeks and resolution of all symptoms). Add IVIG for CMV
pneumonia. Formulations and dosages of IVIG vary in different series
CMV,
HSV,
VZV,
HHV-
6
May cause bone
marrow
suppression
SPECIAL CASES

NEUTROPENIC SEPTIC SHOCK

Source: Adapted from the American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee

• IST HOUR OF ANTIBIOTIC THERAPY PREDICTS MOTALITY. Broad spectrum beta-lactam (e.g.,imipenem/cilastatin, meropenem,or piperacillin-tazobactam) plus an aminoglycoside and vancomycin.
• Addition of fluconazole or an echinocandin should be strongly considered in patients not receiving antifungal prophylaxis.
• Rapid interventions are needed. Fluid resuscitation, oxygen, invasive hemodynamic monitoring, and vasopressor agents may be required. Stress doses of hydrocortisone (IV 50 mg every 6 hours with or without fludrocortisone oral 50 mcg daily) have been associated with decreased mortality in patients with septic shock and with insufficient adrenal reserve.
• Stress-dose corticosteroids are recommended for patients with septic shock who require vasopressor support. High-dose corticosteroids have not shown any benefit in the setting of septic shock or severe sepsis, and may be associated with increased risks for secondary infections.(NCCN GUIDE LINES 2014)

• Stress doses of hydrocortisone reverse hyperdynamic septicshock: a prospective, randomized, double-blind, single-center study(Briejel et al) :critical care med:1999
• CONCLUSION:-Infusion of stress doses of hydrocortisone reduced the timeto cessation of vasopressor therapy in human septic shock. This wasassociated with a trend to earlier resolution of sepsis-induced organdysfunctions
• Effect of high-dose glucocorticoid therapy on mortality in patients withclinical signs of systemic sepsis. The Veterans Administration SystemicSepsis Cooperative Study Group.(NEJM:1988)
• CONCLUSION:-NO ADVANTAGES
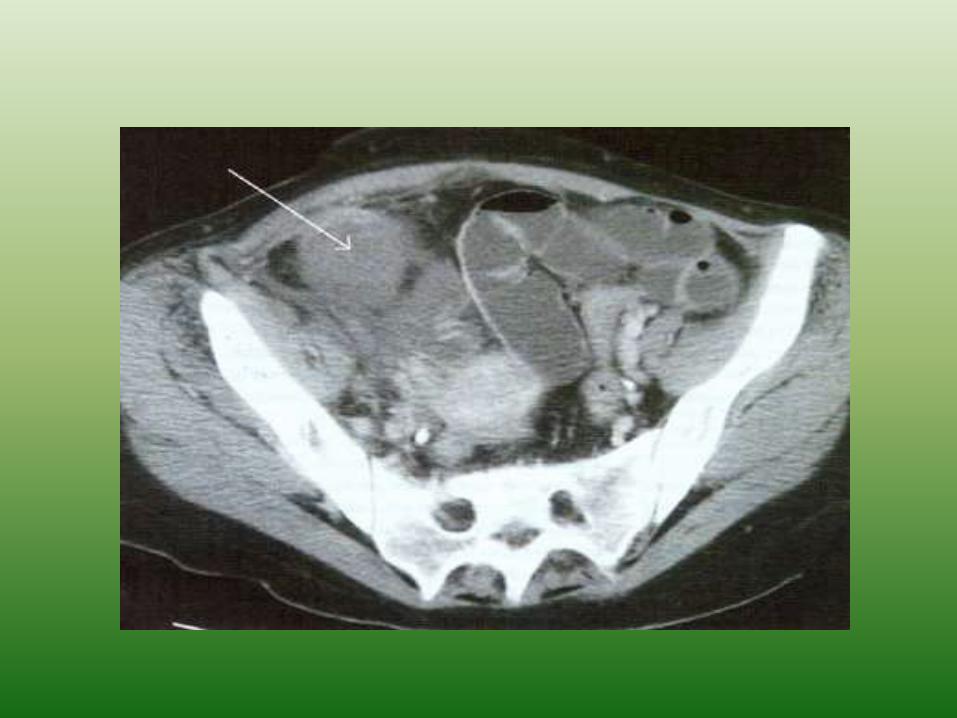
Neutropenic Enterocolitis or Typhilitis
• Inflammatory process involving colon and/or small bowel
• ischemia, necrosis, bacteremia
• ( translocation from gut) hemorrhage, and perforation.
• Fever and abdominal pain ( typically RLQ).
• Bowel wall thickening on ultrasonography or CT imaging.

Treatment( 50-70% mortality)
• Initial conservative management • bowel rest,
• intravenous fluids,
• TPN,
• broad-spectrum antibiotics
• and normalization of neutrophil counts.
• Surgical intervention • obstruction, perforation, persistent gastrointestinal
bleeding despite correction of thrombocytopenia and coagulopathy, and clinical deterioration.
Consider Pseudomonal and Clostridial coverage in Empiric therapy
• Clostridium SepticumClostridium SordelliCover with PEN G ,AMP, Clindamycin*Broad Spectrum Abx ( carbapenem )include Metronidazole if unsure of Cdiff
* resistance of Clostridia to clindamycin
reported.

Neutropenic Pneumonia
• In neutropenia, consolidation and sputum production may be absent.(lack of inflimatory response)
• Blood cultures, a chest radiograph, and, if possible, a sputum sample for Gram stain and culture should be obtained.
• (a) If community-acquired pneumonia is suspected (i.e., pneumonia present before admission or developing within 3 to 4 days of hospitalization), addition of a macrolide or fluoroquinolone to an antipseudomonal beta-lactam is warranted to treat atypical pathogens.
• (b)For nosocomial pneumonia, therapy with an antipseudomonalbetalactam is advised, and addition of an aminoglycoside and fluoroquinolone should be considered. For cases of nosocomialpneumonia in which hospital-acquired legionellosis is suspected, empiric addition of a macrolide or fluoroquinolone is also warranted.
• (C) Vancomycin or linezolid should be added for pneumonia in patients colonized with MRSA and for nosocomial pneumonia at centers in which MRSA is common..

Pcp Pneumonia• Diffuse infiltrates have a broad differential diagnosis:-
PCP,viral infections, hemorrhage, and drug-inducedpneumonitis. A diagnosis of PCP should be considered inpatients with significantly impaired cellular immunity notreceiving PCP prophylaxis who present with diffusepulmonary infiltrates. BAL is the standard approach fordiagnosing PCP. In patients with substantial respiratorydisease (e.g., labored breathing, requiring supplementaloxygen), empiric therapy should be initiated before BAL.Pending BAL results, an initial regimen can include arespiratory fluoroquinolone against community-acquiredpathogens and TMP-SMX (TMP component: 5 mg/kg every 8hours) against possible PCP. In patients with suspected PCPand with room air PaO2 of 75 mmhg or less, corticosteroids(initially prednisone 40 mg twice daily, then tapered) shouldbe added based on studies of patients withAIDS–associatedPCP.(NCCN GUIDELINES)
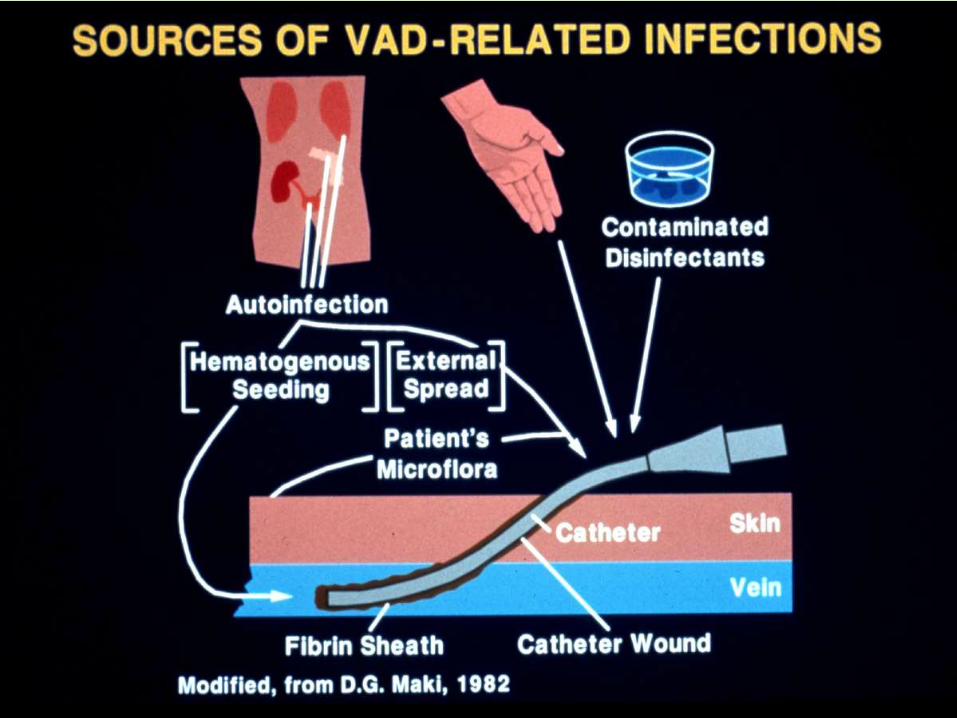
CVC related infections
• Diagnosis and treatment is a challenge
• Usual microorganisms:
CNS, S. aureus, Candida spp., gram (-)ve
• Local and disseminated complications (septic thrombophlebitis, endocarditis)
• Challenging question: Catheter removal
• Prevention is feasible

Fungal Infections
• More frequent in AML patients
• Candida spp. more likely pathogen in the first days of neutropenia if no administered prophylaxis
• If fluconazole prophylaxis then more likely – fluconazole resistant Candida (C. krusei, C. glabrata)
– Mold (Aspergillus spp., Zygomyces spp. , Fusarium spp.)
• Invasive mold infections in patients with severe (ANC ≤ 100 cells/mm 3) and prolonged (>10-15 days) neutropenia
Freifeld et al. Clin Infect Dis 2011;52:427-31

Antifungal Therapy
• Added on the 5th - 7th day of fever and neutropenia
• Increased incidence of fungal infection post day 7 of fever and neutropenia
• 40% - 50% of patients will defervesce post initiation of antifungal chemotherapy
Freifeld et al. Clin Infect Dis 2011;52:427-31

Febrile NeutropeniaEmpirical Antifungal Therapy
• Liposomal amphotericin B
• Azoles (with mold activity)
Itraconazole
Voriconazole
• Micafungin
• Caspofungin
Freifeld et al. Clin Infect Dis 2011;52:427-31
Antibacterial Prophylaxis During
Neutropenia(afebrile neutropenia)Patients with cancer and chemotherapy-induced neutropenia are at risk forsevere bacterial infections. Fluoroquinolones are the most commonly usedprophylactic antibacterial agents in adults with chemotherapy inducedNeutropenia.
In a meta-analysis that evaluated 18 trials(N=1408) in which fluoroquinoloneswere compared to either placebo or TMP/SMX, fluoroquinolone prophylaxissignificantly reduced the incidence of Gram-negative infections by about 80%compared with those without prophylaxis (relative risk=0.21; 95% CI, 0.12-0.37),leading to an overall reduction in total infections:ENGLS et al:cl oncojournal.
The NCCN Guidelines panel advises that fluoroquinolone prophylaxis(levofloxacin is preferred) be considered in patients with expected duration ofneutropenia (ANC less than 1000/mcL) for more than 7 days. In patients withneutropenia expected to last less than 7 days who are not receivingimmunosuppressive regimens (e.g., systemic corticosteroids), the panelsuggests no antibiotic prophylaxis

Antifungal Prophylaxis During Neutropenia(afebrile neutropenia)
INTERMEDIATE RISK GROUP (MM,LYMPHOMAS,AUTOLOGUSHSCT,NEUTROPENIA 7-10 DAYS AND FURADABINE BASED CHEMO) AND HIGH-RISK PATIENTS ( LONGER DURATIONS OF NEUTROPENIA(>10 DAYS) OR WITHGVHD AFTER ALLOGENEIC HSCT,ALL ):- USE FLUCONAZOLE PROPHYLAXIS ifNEUTROPENIA till recovery AND MUCOSITIS.
The NCCN Guidelines panel recommends posaconazole (category 1) for antifungalprophylaxis in neutropenic patients with AML and MDS receiving induction orreinduction chemotherapy.

Antiviral Prophylaxis During Neutropenia(afebrile neutropenia)
HSV infection/reactivation in intermediate andhigh risk use viral prophylaxis(acyclovir /famicyclovar)for neutropenia or during active therapy
Same applies for vzv.
In low risk group use only if prior hsv episode..

You can be a victim of cancer, or a survivor of cancer. It’s a mindset.” All u need brave efforts– Dave Pelzer
THANK YOU