february 13, 2007: i. sim overview medical informatics medical informatics for clinical research ida...
TRANSCRIPT

February 13, 2007: I. Sim OverviewMedical Informatics
Medical Informatics for Clinical Research
Ida Sim, MD, PhD
February 13, 2007
Division of General Internal Medicine, andCenter for Clinical and Translational Informatics
UCSF
Copyright Ida Sim, 2007. All federal and state rights reserved for all original material presented in this course through any medium, including lecture or print.

February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics

February 13, 2007: I. Sim OverviewMedical Informatics
Introduction: Ida Sim, MD, PhD• Position
– Associate Professor, General Internal Medicine– Director, Center for Clinical and Translational
Informatics
• Research areas– informatics and policy of clinical trial registration
and reporting– computer-assisted evidence-based practice– informatics for clinical research– economics of health information technology

February 13, 2007: I. Sim OverviewMedical Informatics
Health Care Quality
• Doing the right thing– based on scientific evidence
• right – without error
• to the right people– e.g., blood pressure meds by ethnicity
• at the right time– beta-blockers at hospital discharge for
heart attacks
February 13, 2007: I. Sim OverviewMedical Informatics
Doing the Right Thing...• Cusp of a “new medicine”
– genomics revolution– personalized medicine
• Human genome findings will need to be translated into population and clinical medicine
• But research findings are often not translated to practice – many examples of care that diverges from
best evidence

February 13, 2007: I. Sim OverviewMedical Informatics
...Right• Institute of Medicine (IOM) report on
medical errors (2000)– a “747” in deaths from medical errors every day
• And quality problems are endemic– Institute of Medicine (IOM) 2001 report
• “Health care today harms too frequently and
routinely fails to deliver its potential benefits…
Between the health care we have and the care
we could have lies not just a gap, but a chasm.”

February 13, 2007: I. Sim OverviewMedical Informatics
EHR to the Rescue? • To improve and transform health care
– personalized, guideline-based, error-free, 24/7 decision support
– “A nationwide effort is needed to build a technology-based information infrastructure that would lead to the elimination of most handwritten clinical data within the next 10 years…” (IOM “Chasm” report, 2001)
• To help clinical research– “Frankly, one of the biggest attractions to LastWord
(aka UCare) is going to be a boon to clinical research. Information will be accessible in a much more uniform and complete way.” ex-SOM Dean Haile Debas, UCSF Daybreak, 2001

February 13, 2007: I. Sim OverviewMedical Informatics
Yet...• Limited adoption of EHR
– 24% of outpatient clinics have an EHR [Jha, 2006]
– <10% hospitals have EHR [Leapfrog, 2003]
– only 4% hospitals have computerized physician order entry (CPOE) [Leapfrog, 2003]
• >80% of clinical research still using paper charts and forms
• Persistent under-investment in IT– only 2.5% of gross revenue on IT [Gartner Group, 2003]
– vs. ~10% in comparable information-intensive sectors (e.g., banking)

February 13, 2007: I. Sim OverviewMedical Informatics
National Policy Response• Office of the National Coordinator for Health
Information Technology (ONC for HIT), started 2004– inform clinical practice
• i.e., increase EHR use
– interconnect clinicians • through computers that “talk” to each other
• via the National Health Information Network (NHIN)
– personalize care• i.e. consumer-centric care, not “personalized” medicine
– improve population health• public health surveillance, “accelerate scientific discovery”
• Government to catalyze private-sector solutions

February 13, 2007: I. Sim OverviewMedical Informatics
IT for Clinical Research?• Attention is secondary to IT for clinical care
– ONC for HIT minor attention to clinical research– UCSF: UCare for clinical care first...
• Focused attention from– electronic clinical trials industry
• $2 billion/year (vs. $12 billion for paper-based trials)
– NIH, e.g., through Roadmap program• Clinical and Translational Science Awards (CTSA)• National Electronic Clinical Trials and Research Network
(NECTAR)• National Centers for Biomedical Computing, NCI, etc.

February 13, 2007: I. Sim OverviewMedical Informatics
NECTAR • Major barriers in clinical trials of chronic diseases
– recruitment in target population (ie community)– costs and logistics of running trials in small
geographically dispersed practices
• NECTAR vision– all US clinics on web are potential study sites– all patients in the US are potential subjects– informatics and other technologies to enhance
• recruitment, protocol administration
• standardized data reporting and data sharing
• cross-study analyses, communication, and collaboration

February 13, 2007: I. Sim OverviewMedical Informatics
GenomicsProteomicsPharmacogenomicsMetabolomics, etc.
Clinical trialsEpidemiologyMolecular Epi
Evidence-based practicePatient safetyQuality of care
Care and Research Coupled
• “Geno” - “pheno” correlations require bridging bench, bedside, clinic, and community
• Informatics is part of that bridge
Basic Discovery
Clinical Research
Clinical Care
T1
Translation
T2
Translation
Bioinformatics
Medical Informatics

February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics

February 13, 2007: I. Sim OverviewMedical Informatics
What are Computers For?
• Store
• Query and Retrieve
• Compute
• Report

February 13, 2007: I. Sim OverviewMedical Informatics
Informatics is Not Programming• The use of computation to understand and
manage complexity – Store, Query and Retrieve, Compute, and Report
complex ... stuff• Informatics is not clinical computing/IT
– clinical computing/IT uses today’s technology to meet operational needs
– informatics seeks computational advances that will lead to tomorrow’s solutions for clinical science and practice

February 13, 2007: I. Sim OverviewMedical Informatics
NIH Definition of Informatics• Includes database design, graphical interfaces,
querying approaches, data retrieval, data visualization and manipulation, data integration through the development of integrated analytical tools, and tools for electronic collaboration, as well as computational and mathematical research including the development of structural, functional, integrative, and analytical models and simulations– http://grants.nih.gov/grants/guide/pa-files/PAR-06-
411.html

February 13, 2007: I. Sim OverviewMedical Informatics
GenomicsProteomicsPharmacogenomicsMetabolomics, etc.
Clinical trialsEpidemiologyMolecular Epi
Evidence-based practicePatient safetyQuality of care
Informatics & Translation
• Informatics enables transfer and analysis of data, information, and knowledge across spectrum of clinical research to care
• ...enables the “translation” in translational research
Basic Discovery
Clinical Research
Clinical Care
T1
Translation
T2
Translation
Bioinformatics
Medical Informatics

February 13, 2007: I. Sim OverviewMedical Informatics
Why Important to You?• “Old” days
– build your own database, analyze it, publish• “New” days
– you want/need to bring together lots of data • of different types (numbers, text, images)
• from different sources (microarrays, charts, claims)
– you want/need analytic methods and models beyond statistics
– you need wide collaboration with other PIs, labs, health systems
• Querying across home-grown databases is not possible; in a networked world, informatics is key

February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics

February 13, 2007: I. Sim OverviewMedical Informatics
Course Goals
• Be familiar with core concepts in medical informatics: vocabularies, interchange standards, decision support systems
• Understand how computers are used to manage information in health care and clinical research
• Learn how information technology is being used to improve clinical care and research
• Understand how the new NIH emphasis on informatics impacts clinical research

February 13, 2007: I. Sim OverviewMedical Informatics
Outcomes
• You will be able to recognize an informatics problem when confronted with one
• You will know when you need informatics assistance in your grant (i.e., consult or collaboration)
• You will have an answer when your colleagues say “why can’t computers just ...”
February 13, 2007: I. Sim OverviewMedical Informatics
Course Structure• 6 Lecture/Discussion Sessions
– PowerPoint file up 1+ days before lecture– class participation expected
• Assignments– 5 homeworks, no final exam
• Office “hours”: [email protected]– http://www.epibiostat.ucsf.edu/courses/schedule/
med_informatics.html

February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics– Store– Query and Retrieve– Compute– Report

February 13, 2007: I. Sim OverviewMedical Informatics
CDSS Running Example• Hypertension treatment Clinical Decision Support
System (CDSS)– Clinic has an EHR
– During patient visit, CDSS notes that BP and trend is too high.
– CDSS checks patient’s Cr, diabetes status, cardiac status, current meds and allergies and recommends drug therapy change according to JNC VII guidelines and insurance coverage.
– Presents e-prescription for MD to verify. If verified, order is sent directly to pharmacy and medication list updated.

February 13, 2007: I. Sim OverviewMedical Informatics
Major Tasks of this CDSS• EHR has to “know”
– BP trend– patient is diabetic, has micro-albuminuria
• Apply the guideline– BP is “too high” for diabetic– diabetics with micro-albuminuria should be on an ACE
inhibitor• E-prescribing
– patient not yet on ACE inhibitor– benazapril is covered ACEI by pt insurance plan– given pts. age and weight, start at 5 mg PO QD– generate prescription and e-mail to pharmacy

February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics– Store– Query and Retrieve– Compute– Report

February 13, 2007: I. Sim OverviewMedical Informatics
Data Storage• Computers can help us
– store, retrieve, query, compute, and report data • For this to happen, we must describe the data in
such a way that the computer– “understands” the data– can manipulate the data
• e.g., sort them, graph them, add numbers, perform analyses
– can retrieve the data for later use• The computer’s ability to manage data depends
on how well the data is described

February 13, 2007: I. Sim OverviewMedical Informatics
• Types of data and detail sufficient for– real-time clinical care
• notes, orders, labs, prescriptions, xray (reports)...
– administation• demographic, billing, provider IDs...
• What about quality improvement and research?– standardized data collection, symptom scales, etc– e.g., examples?
What Data Should EHRs Store?

February 13, 2007: I. Sim OverviewMedical Informatics
How Should EHRs Store Data?
• Computers cannot read. For EHRs to “understand” the clinical content– need to code concepts into standardized terms – a standardized vocabulary acts like a dictionary
• DGIM tried to use STOR to pull out all CHF patients for quality improvement program but terms used were too varied
• Free text vs. coded entries– e.g., how to guarantee that all pneumonia
admissions will be retrieved if asked for?– “Mrs. Jones has a left bilobar pneumonia”– Pneumonia: Yes, Location: Left

February 13, 2007: I. Sim OverviewMedical Informatics
“Describing” Data: To Humans
• To describe a thought for another human to understand, we use
– symbols (words) with shared meaning• e.g., English, Chinese, Urdu words; IM lingo
– a system for codifying meaning using those words• e.g, English grammar, mathematical notation
• We must also make the coded message concrete
– e.g., skywriting “I LUV U”, drawing graph on beach
– and persistent• text on paper, an oil painting, lecture on audiotape
24142 1083.9 96

February 13, 2007: I. Sim OverviewMedical Informatics
“Describing” Data: To Computers• Computers need to be talked to also!• To describe a thought for computers to understand, use
– a controlled vocabulary for a domain, like a dictionary• e.g., ICD-9, SNOMED
– a data model that stores the “words” together in a standard format
• e.g., relational data model
– an interchange protocol, like a grammar, that codifies the meaning of “words” sent between computers
• e.g., HTTP, or FTP
• Make the thoughts concrete and persistent by storing as 1’s and 0’s on hard disks, etc.

February 13, 2007: I. Sim OverviewMedical Informatics
Notable Clinical VocabulariesVocabulary Name Domain Use
SNOMED Standardized Nomenclatureof Human and Ve t Medicine
ClinicalMedicine
EMRDocumentation
MeSH Medical Subject Heading BiomedicalIndexing
BibliographicRetrieval
ICD-9 International Classificationof Diseases
Diseases Billing
CPT Current ProceduralTerminology
MedicalProcedures
Billing
DSM-IV Diagnostic and StatisticalManual of Mental Disorders
Pyschiatry Billing,Nosology
LOINC Logical ObservationIdentifier Names and Codes
Labs Lab systems,Billing

February 13, 2007: I. Sim OverviewMedical Informatics
Problems of Controlled Vocabs• Coverage
– is the idea (e.g., SNP) included?
• Granularity– do you need left heart failure?
• Synonomy– cervical: neck or cervix related?
• Relationships between terms– lisinopril IS-A ACE-inhibitor
• Size and “post-coordination”– left heart failure vs. left + heart failure
• Usability– can’t find the right code
• Versioning– new terms (e.g., SNP), defunct terms (e.g., dropsy)

February 13, 2007: I. Sim OverviewMedical Informatics
Controlled Vocab for CDSS• Hypertension treatment CDSS
– During patient visit, CDSS notes that BP and trend is too high. It checks patient’s Cr, diabetes status, cardiac status, current meds and allergies and recommends drug therapy change according to JNC VII guidelines and insurance coverage. Presents e-prescription for MD to verify. If verified, order is sent directly to pharmacy and medication list updated.
• How are BP readings labelled? Systolic and diastolic?• ICD-9 for hypertension (401.1), diabetes (250.00) at each
encounter? any encounter? what if only “HTN” written in problem list? Who codes the ICD-9? Why?
• Medications, from EHR, PHR, or pharmacy– “benaz” or benazepril or Lotensin– is lisinopril an ACEI?

February 13, 2007: I. Sim OverviewMedical Informatics
Tradeoffs of Coding• The more coded your data, the more
expressive the vocabulary, the more computing you can do with the data– because the computer can “understand” more
• But coding costs time and effort– e.g., selecting billing codes
• How to make coding easier/cheaper?– pay someone other than doctor– automatic coding from text, voice recognition,
etc.

February 13, 2007: I. Sim OverviewMedical Informatics
Teaching Point: Storing Data
• The more coded your data, the more the computer can do with it
• But – controlled vocabularies are hard to build
and maintain– standardized coding is difficult and
expensive

February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics– Store– Query and Retrieve– Compute– Report

February 13, 2007: I. Sim OverviewMedical Informatics
• HTN CDSS example– During visit, CDSS notes that BP and trend is too high. It
checks patient’s Cr, HgbA1C, cardiac status, current meds and allergies and recommends drug therapy change according to JNC VII guidelines and insurance coverage. Presents e-prescription for MD to verify. If verified, order is sent directly to pharmacy and medication list updated.
• Inefficient to query multiple databases: EHR, claims, pharmacy, ADT, lab, xray, etc
• May also wish to query data collected as part of clinical research – data from research protocols, GCRCs, etc.
Beyond the EHREHR
EHRPharmacy
Admin

Query, Retrieval, Data Interchange
Clinic 2007
FrontDesk
Radiology
Claims
MedicalInformationBureau
Archive
Walgreens
Prescribing
Pharm BenefitManager
Benefits Check(RxHub)
HealthNetFormulary Check
B&TEligibility Authorization
Personal HealthRecord
UCare
Electronic MedicalRecord
Specialist
Referral
ReferralAuthorization
Internet Intranet Phone/Paper/Fax
Lab
UniLab
(HL-7)
February 13, 2007: I. Sim OverviewMedical Informatics
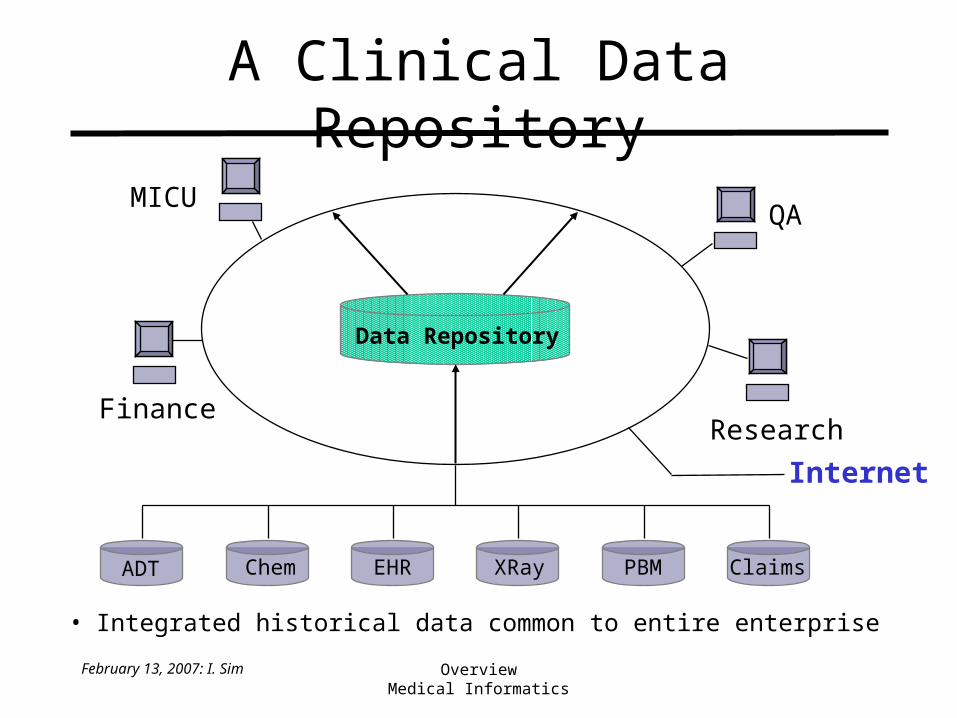
MICU
FinanceResearch
QA
Data Repository
Internet
ADT Chem EHR XRay PBM Claims
• Integrated historical data common to entire enterprise
A Clinical Data Repository

February 13, 2007: I. Sim OverviewMedical Informatics
Internet = Network of Networks
itsa
medicine
ucsf.edu
nci.nih.gov cochrane.uk myhome.com
Main Trunk Cables
local trunk cablethrough Berkeley
amazon.com
at homedial-in to itsa.ucsf.edu via modem
pacbell.net
aol.com
Internet Service Provider (ISP)via DSLor cable
LAN

February 13, 2007: I. Sim OverviewMedical Informatics
• Protocol = grammar for machines talking to each other– e.g., Hypertext transfer protocol http for web
• http://www.epibiostat.ucsf.edu/courses/schedule/med_informatics.html
• Health-specific protocols needed “on top of” http or tcp/ip– e.g., Health Level 7 (HL-7), DICOM (xrays)
What Happens Over the Cables
MSH|…message header
PID|…patient identifier
<!-OBX…observation result>
OBX|1|ST|84295^NA||150|mmol/l|136-148|H||A|F|19850301<CR>

February 13, 2007: I. Sim OverviewMedical Informatics
MICU
FinanceResearch
QA
Data Repository
Internet
ADT Chem EHR XRay PBM Claims
• Integrated historical data common to entire enterprise
What is “Data Warehouse” For?

February 13, 2007: I. Sim OverviewMedical Informatics
Types of Queries
• Clinical care
• What was Mr. Smith’s last potassium?
• Does he have an old CXR for comparison?
• What antihypertensives has he been on before?
• What did the neurology consult say about his epilepsy?
• Quality Improvement• What proportion of
diabetics with AMI admissions were discharged on -blockers?
• What was the average Medicine length of stay in 2000 compared to 1995?
• What is the trend in use of head CTs in patients with migraine?

February 13, 2007: I. Sim OverviewMedical Informatics
EHR/Data Repository Comparison
• Enterprise viewpoint more appropriate for QI and research
• Data repository cleans and aggregates data from multiple sources– need standardization of codes, definitions,
and data schemas
Viewpoint Time Queries
EHR Patient Real-Time ClinicalData Repository Enterprise Historical Ad Hoc
February 13, 2007: I. Sim OverviewMedical Informatics
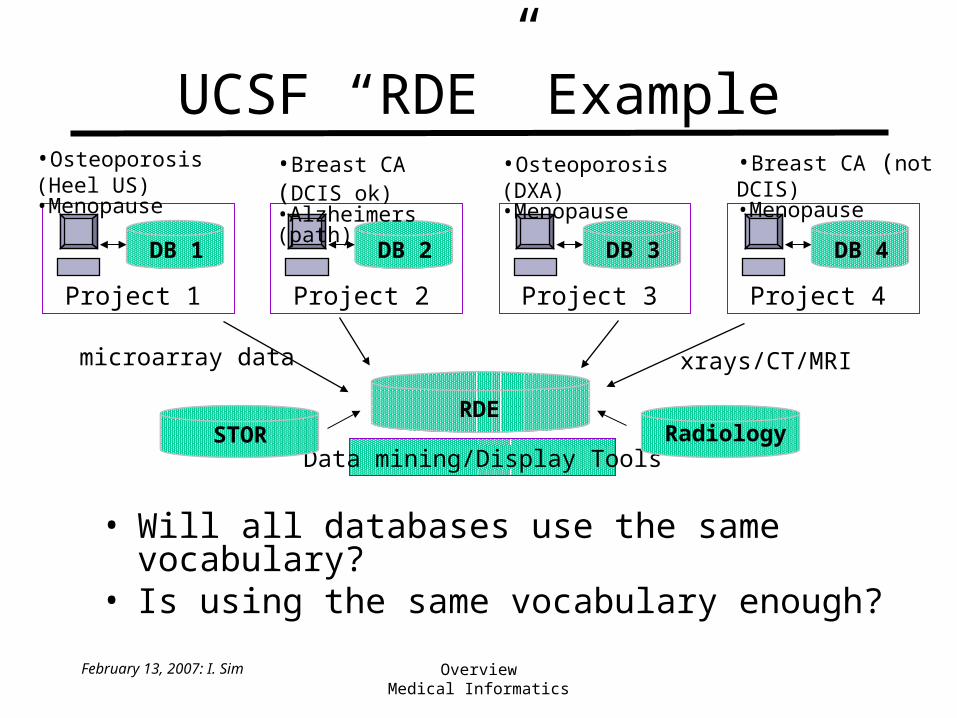
UCSF “RDE” Example
• Will all databases use the same vocabulary?• Is using the same vocabulary enough?
Project 1
DB 1
Project 2
DB 2
Project 3
DB 3
Project 4
DB 4
•Breast CA (not DCIS)•Menopause
•Osteoporosis (Heel US)•Menopause
•Osteoporosis (DXA)•Menopause
•Breast CA (DCIS ok)•Alzheimers (path)
xrays/CT/MRImicroarray data
RDE
Data mining/Display ToolsRadiologySTOR

February 13, 2007: I. Sim OverviewMedical Informatics
Teaching Point: Query/Retrieve
• Data warehouses clean and aggregate data from multiple sources– health-specific “grammars” (e.g., HL7) are
used for sending clinical data over the network
• If data coding isn’t standardized across data sources, aggregation may not be meaningful
February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics– Store– Query and Retrieve– Compute– Report

February 13, 2007: I. Sim OverviewMedical Informatics
Some General Thinking Tasks
• Finding things (Google)
• Individual knowledge discovery (ie learning)
• New knowledge discovery (ie research)
• Applying knowledge to action
• Artistic creation
• ...
= clinical research
= clinical care

February 13, 2007: I. Sim OverviewMedical Informatics
Knowledge Discovery
• From Data -> Information -> Knowledge

February 13, 2007: I. Sim OverviewMedical Informatics
D-I-K...Wisdom• Data
– raw observations/objective facts, “discrete, atomistic, tiny packets (with) no inherent structure or necessary (inter)relationship”
• Information– data with meaning, formed data, processed data
• Knowledge– tacit: no codifiable (eg “expertise”, clinical sense)– vs. explicit: codifiable (eg guideline)– useful for predicting future, guiding future action

February 13, 2007: I. Sim OverviewMedical Informatics
Knowledge Discovery
• Many methods for “data mining” – statistics (classical, bayesian)– neural networks, bayes nets, clustering, classification, etc, etc.– natural language processing, information extraction, etc.
• Methods vary at at incorporating prior knowledge, causal knowledge, types of data that can be handled, etc.

February 13, 2007: I. Sim OverviewMedical Informatics
Comparing Methods (1)
To loan or not to loan...
Linear regression Linear classification

February 13, 2007: I. Sim OverviewMedical Informatics
Comparing Methods (2)
Clustering
Non-linear classifiers
Neural Network Nearest Neighbor

February 13, 2007: I. Sim OverviewMedical Informatics
Some General Thinking Tasks
• Finding things (Google)
• Individual knowledge discovery (ie learning)
• New knowledge discovery (ie research)
• Applying knowledge to action
• Artistic creation
• ...
= clinical research
= clinical care

February 13, 2007: I. Sim OverviewMedical Informatics
Knowledge to Action• Decision support
– given starting conditions and a defined set of action choices, recommend or rank action choices for user(s)
• Requires some “thinking” to recommend or rank– strictly deterministic (if-then) thinking– fuzzy and probabilistic thinking
• in starting data or reasoning procedure
• outcomes (e.g. prob. of adverse reaction)
– often thinking about concepts, not numbers• symbolic vs. quantitative computing

February 13, 2007: I. Sim OverviewMedical Informatics
Decision Support “Thinking”• Strictly deterministic
– first-order logic rule-based systems– adhoc rule-based systems (non-mathemetical reasoning
about probability)• e.g., if high WBC AND cough AND fever AND abn. CXR
then likelihood of pneumonia is 4 out of 5
• Probabilistic/fuzzy– bayesian networks
• formal probabilistic reasoning, extension of decision analysis
– neural networks– fuzzy logic, case-based reasoning, etc., or hybrids

February 13, 2007: I. Sim OverviewMedical Informatics
HTN CDSS Example• EHR has to “know”
– BP trend– patient is diabetic, has micro-albuminuria
• Apply the guideline– BP is “too high” for diabetic– diabetics with micro-albuminuria should be on an ACE
inhibitor
• E-prescribing– patient not yet on ACE inhibitor– benazapril is covered ACEI under insurance plan– given pts. age and weight, start at 5 mg PO QD– generate prescription and e-mail to pharmacy

February 13, 2007: I. Sim OverviewMedical Informatics
Rule-Based Approach• Forward chaining/reasoning (data-driven)
– start with data, execute applicable rules, see if new conclusions trigger other rules, and so on
– example• if DX = DIABETES AND SBP > 130 => GIVE-DM-BP-MED
• if GIVE-DM-BP-MED AND MICROALBUMINURIA => GIVE-ACEI
• if GIVE-ACEI AND NOT-TAKING (ACEI) => CHECK-ACEI-COVERAGE
• IF NOT-ALLERGIC (ACEI) AND INSURANCE-COVERED (ACEI) => PRESCRIBE (ACEI)
– use if sparse data

February 13, 2007: I. Sim OverviewMedical Informatics
Discussion• Reasoning features
– includes both symbolic information (has diabetes) and quantitative information (SBP < 130)
– deterministic: if-then construct– value-based: assumes that BP drug is
worth marginal benefit– could be multi-user
• Some problems with rule-based systems?

February 13, 2007: I. Sim OverviewMedical Informatics
Broad Comparisons
• Knowledge Discovery• Clinical research• More quantitative• Values-free• Probabilistic and
deterministic
• Knowledge to Action• Clinical care• More symbolic• Values-dependent• Deterministic and
probabilistic• Multiple users
• Comparative features apply to human and computer reasoning – but implies use of different computing techniques

February 13, 2007: I. Sim OverviewMedical Informatics
Teaching Point: Compute• What is a computational problem?
– knowledge discovery: when you have data and want knowledge
– applying knowledge to action: how to figure out what to do next
• Informatics principles include– specifying the problem abstractly (e.g., D-I-K,
symbolic? probabilistic? values? domain? users?)– meaningful data coding, aggregation, interchange– choosing the best method (not just statistics)– efficient algorithms to achieve solution

February 13, 2007: I. Sim OverviewMedical Informatics
Outline
• Introduction
• What is Informatics
• Course Goals
• Functional Overview of Informatics– Store– Query and Retrieve– Compute– Report

February 13, 2007: I. Sim OverviewMedical Informatics
Visualizing Complex Information
• http://biocyc.org/ECOLI/new-image?type=OVERVIEW– the more coded and structured the underlying
information, the more powerful and flexible the visualization can be
• Best information exploration interfaces incorporate– cognitive psychology
• error mitigation techniques
– human-computer interaction principles• principle of “5-7 item” limit of human attention
– engineering design and aesthetics• “affordances,” “usability”

February 13, 2007: I. Sim OverviewMedical Informatics
Summary• Computers help us
– store, query and retrieve, compute, and report on– data, information, and knowledge
• Biomedical informatics is using computers to manage the complexity in biomedicine– complexity of concepts (e.g., findings, diagnoses)– complexity of relationships among concepts (e.g.,
disease etiology, treatment predictors)– complexity of care system (e.g., EHRs, guidelines)
• Since clinical research getting more complex, informatics has increasing role to play...

February 13, 2007: I. Sim OverviewMedical Informatics
Teaching Points• Store
– standardized coding is critical but difficult• Query and retrieve
– coding must be standardized across databases for data repositories
• Compute– formal approach to specifying computational
problems and selecting best methods• Report
– information exploration design draws from many fields