federal pharmacy 2016 - senior leaders’ perspective...
TRANSCRIPT

3/16/2016
1
Federal Pharmacy 2016: Senior Leaders’
Perspective
Ron Nosek, Department of Veterans Affairs
George Jones Jr, Defense Health Agency
COL John Spain, U.S. Army
RADM Pam Schweitzer, U.S. Public Health Service
March 4, 2016
CPE Information and DisclosuresMr. Ron Nosek, Dr. George Jones, COL John Spain and
RADM Pamela Schweitzer declare no conflicts of interest, real
or apparent, and no financial interests in any company,
product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacist Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
CPE Information
Target Audience: Pharmacists & Technicians]
ACPE#: 0202-0000-16-082-L04-P/T
Activity Type: Knowledge-based
Learning Objectives
1. Discuss two current issues that affect federal pharmacy.
2. Describe how the Defense Health Agency is improving
medication safety and effectiveness by offering medication
therapy management to its beneficiaries.
3. Explain how the Veterans Health Administration’s clinical
pharmacy program is expanding the role of pharmacists and
provide an update of the PhARMD Project.
Self-Assessment Question 1
1. The Veterans Health Administration provides care to over 8.9 million Veterans annually from 1,600 medical care sites.
True or False
Self-Assessment Question 2
2. DoD Pharmacy is implementing a Congressionally directed Medication Therapy Management pilot in:
a.) Patient Centered Medical Home based care model
b.) A Military Treatment Facility and civilian care based care model
c.) A civilian care based care model
d.) All of the above

3/16/2016
2
Self-Assessment Question 3
3. Priorities of the Army Medical Department include:
a.) Readiness and Health
b.) Healthcare Delivery
c.) Force Development
d.) Take Care of Soldiers, Civilians and Families
e.) All of the above
Self Assessment Question 4
4. What opportunities are there for pharmacists to strengthen the healthcare system infrastructure?
a.) Strategize on ways to fill gaps in healthcare
delivery
b.) Pharmacist Provider status
c.) Alignment of clinical values across healthcare
teams, and a shift to patient-centered goals within
care delivery.
d.) All of the above
Federal Pharmacy 2016: Senior Leaders’
Perspective
Ron NosekDeputy Chief Consultant, VA PBM
National Director,VA Meds by Mail Program
Veterans Health Administration
March 4, 2016
Overview and Key Initiatives in VA
• VHA and PBM
• CMOP
• Clinical Pharmacy Programs– The PhARMD Project
– Academic Detailing
– VA Pharmacy Residencies
Veterans Health Administration
• Over 1,600 sites of care including: – 167 VA Medical Centers
– Over 1,000 Community-Based Outpatient Clinics (CBOCs)
– 300 Vet Centers (Readjustment Counseling), 70 Mobile Vet Centers
– Outreach and mobile medical clinics serve the most remote rural Veterans—
all tethered to one of our medical centers
• Provides health care services to 8.9 million Veterans each year– 92.4 M OP appointments annually
– 16,801 Average Operating Beds
– 707.4 K Admissions
– 312 K surgeries annually
• Pharmacy Services– Approximately 8,500 Pharmacists; 600 Residents/Fellows; 4,500 Technicians
– 223 outpatient pharmacies; 7 mail order pharmacies
– 146 M Rx’s (271 M 30-day Eqv) annually (80% filled by mail)
– $3.7 billion in drug cost
Pharmacy Benefits Management
• VA operates a world-class pharmacy benefits management program with demonstrated excellence in several key areas including:
– Clinical pharmacy practice (profession benchmark)
– Top Pharmacy Residency Training Programs
– Pharmacy automation (innovator)
– Medication safety (national and international reputation)
– Formulary management (sustained superior performance in access, cost and quality over the past decade)
3/16/2016
3
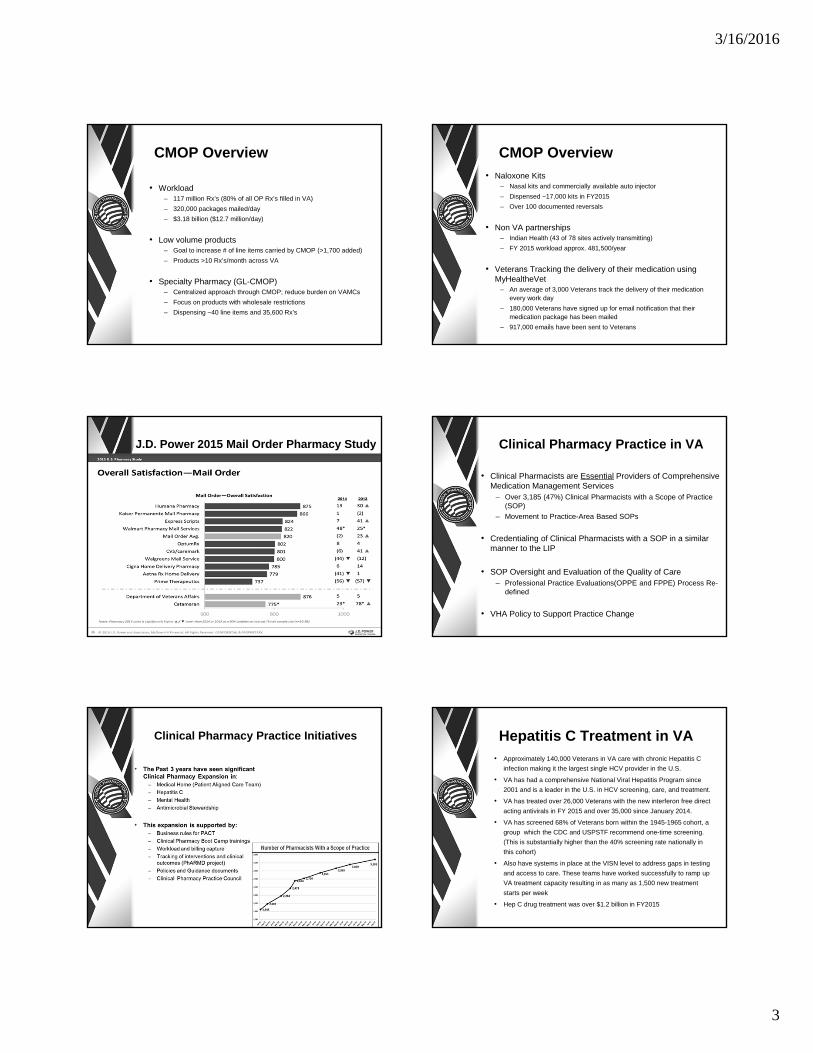
CMOP Overview
• Workload– 117 million Rx’s (80% of all OP Rx’s filled in VA)
– 320,000 packages mailed/day
– $3.18 billion ($12.7 million/day)
• Low volume products– Goal to increase # of line items carried by CMOP (>1,700 added)
– Products >10 Rx’s/month across VA
• Specialty Pharmacy (GL-CMOP)– Centralized approach through CMOP; reduce burden on VAMCs
– Focus on products with wholesale restrictions
– Dispensing ~40 line items and 35,600 Rx’s
CMOP Overview
• Naloxone Kits– Nasal kits and commercially available auto injector
– Dispensed ~17,000 kits in FY2015
– Over 100 documented reversals
• Non VA partnerships– Indian Health (43 of 78 sites actively transmitting)
– FY 2015 workload approx. 481,500/year
• Veterans Tracking the delivery of their medication using MyHealtheVet
– An average of 3,000 Veterans track the delivery of their medication every work day
– 180,000 Veterans have signed up for email notification that their medication package has been mailed
– 917,000 emails have been sent to Veterans
J.D. Power 2015 Mail Order Pharmacy Study Clinical Pharmacy Practice in VA
• Clinical Pharmacists are Essential Providers of Comprehensive Medication Management Services
– Over 3,185 (47%) Clinical Pharmacists with a Scope of Practice (SOP)
– Movement to Practice-Area Based SOPs
• Credentialing of Clinical Pharmacists with a SOP in a similar manner to the LIP
• SOP Oversight and Evaluation of the Quality of Care – Professional Practice Evaluations(OPPE and FPPE) Process Re-
defined
• VHA Policy to Support Practice Change
Clinical Pharmacy Practice Initiatives Hepatitis C Treatment in VA• Approximately 140,000 Veterans in VA care with chronic Hepatitis C
infection making it the largest single HCV provider in the U.S.
• VA has had a comprehensive National Viral Hepatitis Program since
2001 and is a leader in the U.S. in HCV screening, care, and treatment.
• VA has treated over 26,000 Veterans with the new interferon free direct
acting antivirals in FY 2015 and over 35,000 since January 2014.
• VA has screened 68% of Veterans born within the 1945-1965 cohort, a
group which the CDC and USPSTF recommend one-time screening.
(This is substantially higher than the 40% screening rate nationally in
this cohort)
• Also have systems in place at the VISN level to address gaps in testing
and access to care. These teams have worked successfully to ramp up
VA treatment capacity resulting in as many as 1,500 new treatment
starts per week
• Hep C drug treatment was over $1.2 billion in FY2015

3/16/2016
4
The PhARMD Project
• Pharmacists Achieve Results with Medications Documentation
• A clinical reminder dialog template that allows pharmacists to document the spectrum of clinical pharmacy services that are provided to patients by pharmacists within the VA.
• The PhARMD tool contains interventions commonly seen in different settings
• Original tool focuses on the ambulatory setting
• Version 7.0 includes interventions in the acute care setting; released at the end of FY15
PhARMD Project Tool: How Does it Work?
• A health factor was created for each of the clinical pharmacy interventions in the tool using standardized nomenclature and these health factors are exported into the regional and corporate data warehouses
• CPPO has developed the ability to retrieve these clinical pharmacy health factors (HF) for each intervention logged by the clinical pharmacist at the local medical center
PhARMD Project Focus on Interventions
• CPPO PhARMD Reporting SharePoint available with data for all participating sites
• Summary and interventions breakdowns
– Important in describing role of the pharmacist
• Provides information related to types of patients and their therapeutic goals identified by pharmacists
• Provides granularity as to number of patients who achieved therapeutic targets
PhARMD Project Results
Academic Detailing Implementation in Veterans Health Administration
• In-person educational outreach– Information is provided interactively so the academic detailer can:
• Understand where the provider is coming from in terms of knowledge, attitudes, and behavior personal motivations for practice
• Modify the interaction to meet the needs of the provider• Engage the provider by acknowledging their expertise and
learning together rather than teaching
• Uses balanced evidence-based information and tools• Delivered by a healthcare professional specially skilled in empathic
persuasive communication• Over time, the educator and provider develop a trusted and useful
relationship
• As of March 2015, VHA mandated implementation of Academic Detailing in every Veteran Integrated Service Network to be provided by Clinical Pharmacy Specialists
Multi‐faceted Approach:Academic Detailing, Audit Feedback and Practice Facilitation
Academic Detailing VISN
Implementation Statistics as of September 2015
• 6 VISNs have fully implemented AD
• 14 VISNs are in‐progress of implementation
• 2 VISNs pending decision on waiver
Topics Covered During AD Visits (FY15 Q1-3)Topic Total Visits
Pain/Opioid Use 1171
OEND 638
Benzo in the Elderly 194
PTSD 194
Testosterone 141
AUD 51
Insomnia 43
Hepatitis C 35
Depression 25
Dual Care 18
Refractory Schizophrenia 13
Coalition Building 12
Other 39
Insomnia Pharmacotherapy Dashboard OEND Distribution Report
3/16/2016
5
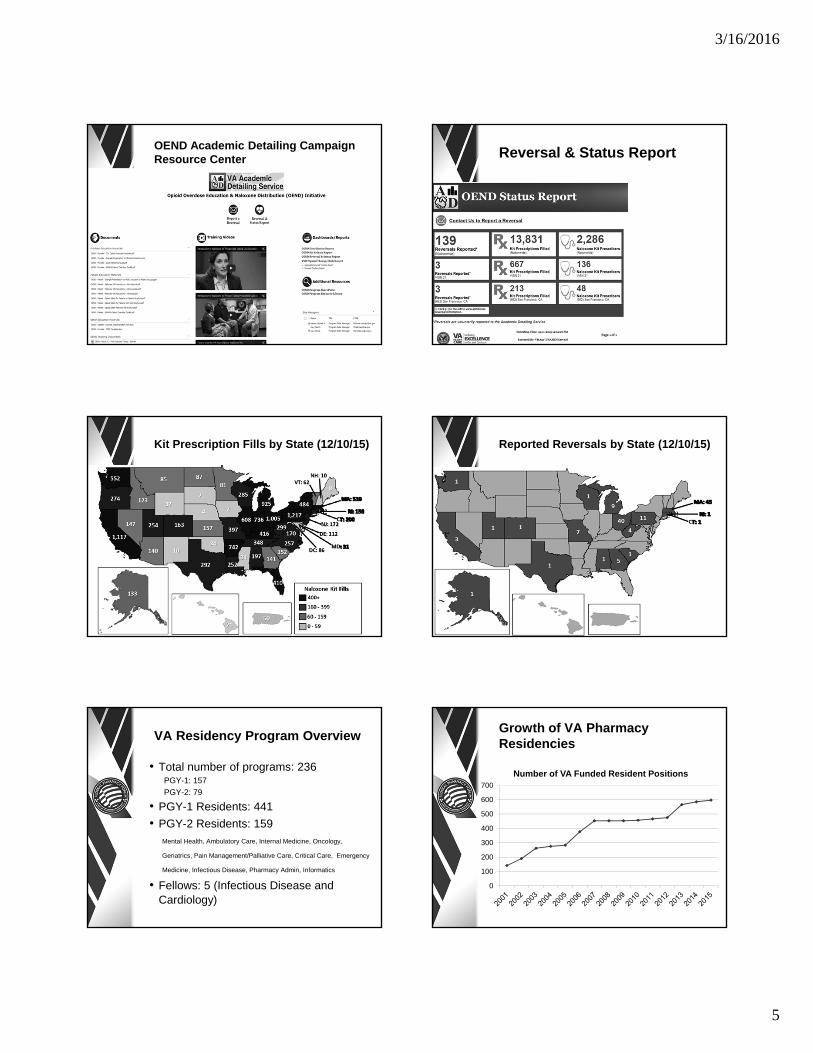
OEND Academic Detailing Campaign Resource Center Reversal & Status Report
Kit Prescription Fills by State (12/10/15) Reported Reversals by State (12/10/15)
VA Residency Program Overview
• Total number of programs: 236PGY-1: 157
PGY-2: 79
• PGY-1 Residents: 441
• PGY-2 Residents: 159Mental Health, Ambulatory Care, Internal Medicine, Oncology,
Geriatrics, Pain Management/Palliative Care, Critical Care, Emergency
Medicine, Infectious Disease, Pharmacy Admin, Informatics
• Fellows: 5 (Infectious Disease and Cardiology)
Growth of VA Pharmacy Residencies
0
100
200
300
400
500
600
700
Number of VA Funded Resident Positions

3/16/2016
6
“Current Issues in DoDPharmacy Operations”
DoD Pharmacy Enterprise
Dr. George E. Jones, Jr.Chief, Pharmacy Operations Division
Defense Health Agency
Learning Objectives
• An overview of the Defense Health Agency and the DoD Pharmacy Enterprise Support Activity
• Awareness of the DoD Pharmacy implementation of a Medication Therapy Management pilot project
Military Health System Modernization
• Creating a more globally integrated health system – built on our battlefield successes
• Driving enterprise-wide shared services; standardized clinical and business processesthat produce better health and better health care
• Implementing future-oriented strategies to create a better, stronger, more relevant medical force
“Medically Ready Force…Ready Medical Force” 34
DHA Pharmacy Ops Division: Supporting the DoD Pharmacy Enterprise
“Medically Ready Force…Ready Medical Force” 35.
The DHA Pharmacy Operations Division has responsibility for corporate management and compliance oversight of enterprise-wide pharmacy initiatives enabling DoD pharmacy benefit delivery in support of the MHS.
Pharmacy Enterprise Support Activity- Guided by Pharmacy Work Group
DoD Pharmacy: Delivering!∎ Pharmacy Shared Services – from “Initial to Full”
Operating Capability 2013‐15
∎ Service Consultants/DHA Pharmacy Staff–Pharmacy Work Group
∎ Exceeded Every Target∎ Integrated Operational Framework – Dynamic Collaboration to
Address Mission Opportunities
∎ Tasked to implement Congressionally directed Medication Therapy Management pilot program∎ Assess MTM delivery and results in three practice settings
∎ Develop / track metrics to describe value to patient outcome
Delivering Today ‐ Positioned to Build on the Excellence
MTM in DoD Pharmacy –A Pilot Program
∎ NDAA 2015 Section 726 – Medication Therapy Management Pilot Program
• “…program to evaluate the feasibility and desirability of including medication therapy management as part of the TRICARE program.”
∎ Elements:
∎ 1+ chronic condition; 1+ prescribed medication
∎ Focus – improve use and outcome of medication(s)
∎ Metrics to measure the effect of MTM

3/16/2016
7
MTM Pilot Implementation
• Pilot directed in NDAA 2015 Section 726
• 2 year pilot
• Determine if MTM is feasible and desirable for deployment DoD wide
• Directed MTM Pilot Sites– Location Type 1 – Patients enrolled in PCMH
– Location Type 2 – Patients using MTF pharmacies but receiving medical care outside the MTF
– Location Type 3 – Patients receiving purchased sector care and using Retail or Mail (non MTF)
MTM Pilot Implementation, cont.
• Issuing a Request for Proposal (1st QTR CY2016)
• Mechanism to enable adding staff to deliver MTM
• Implementing purchased sector care location
• Measurement and Analytics support
• Leverage Existing Medication Optimization • Patient Centered Medical Home efforts
• Reports developed by DHA and provided to Services
• Capabilities of current pharmacy contract partner
• Initiate Pilot Program 3rd QTR CY2016
• OVERALL GOAL – Improve Medication Use; Meet Report to Congress Requirements
Key Points
• An overview of the Defense Health Agency and the DoD Pharmacy Enterprise Support Activity
• Awareness of the DoD Pharmacy implementation of a Medication Therapy Management pilot project
Federal Pharmacy 2016: Senior Leaders’
Perspective
COL John SpainU.S. Army Pharmacy Consultant and
USA MEDCOM Pharmacy Program ManagerOffice of the Army Surgeon General
March 4, 2016
Outline
• TSG 44: Intent, Priorities, Future Environment• Army Pharmacy Strategic Plan• Top 3
– Interaction at Dispensing– Clinical Pharmacy Expansion– Recapture
• Looking Forward– Clinical Pharmacy Value Proposition– Specialty Medications
• Engagement– DOD– Federal Pharmacy– Industry
• Comments/Questions/Discussion
TSG: Intent and Priorities
• TSG 44 - LTG Nadja West
• Primary mission: Support the warfighter
• Priorities– Readiness and Health
– Healthcare Delivery
– Force Development
– Take Care of Soldiers, Civilians and Families

3/16/2016
8
TSG: How I View the Future Health Care Environment
• Characteristics:– Paradigm shift in care-delivery model (i.e. phone,
internet, group visits, genetically tailored treatment)
– Super empowered healthcare consumers
– Continued rising costs reaching a potential “breaking point”
– Increasing focus on patient behavior
– Integrated information technology systems
• Health Service Challenges:– Super empowered healthcare consumers
– Fiscal constraints
– Data saturation
– Patient compliance
Strategic Plan (FY13-16)
SP: Bottoms up - iterative review - living document(SP Group >JFPS review >field review >final >revision >publish[JAN16] >interim[APR16])
1. Readiness: visibility of non-deployable medication, polypharmacy high risk
2. Stewardship: perpetual inventory, E-Rx, contract compliance, reverse distribution
3. Quality Care: polypharmacy, secret shopper, staffing model
4. Innovation/Standardization: automation, metrics, privilege/credentials
5. Service Excellence: customer feedback
6. People: job/skill expectations, certification,
training opportunity
Top 3
• Interaction at Dispensing
• Pharmacy Expansion in the Army
Medical Home
• Recapture
#1: Interaction at Dispensing
Everyone contributes to achieving Service Excellence objective MOE : >87.5% of patients rate pharmacy services as very good/ excellent
#2: Expansion in the AMH #3: Recapture
• Purchases– Brand to generic compliance ~ 93%
– National contract compliance ~ 88%
• Select Brand Prescriptions– Acute
– Maintenance
• Patients– Expanding formularies
– Increasing co-pays

3/16/2016
9
Looking Forward
• Value Proposition– Clinical
– Financial
– Readiness
• Specialty Medications
Value Proposition
• Clinical measures: • predictive modeling
• outcomes assessment
• Financial measures: • RVU generation
• Patient care time (direct & indirect)
• Readiness measures: • # high risk Polypharmacy
• # non deployable medication use
Clinical
Financial
Readiness
Value Proposition Clinical Value Proposition Financial
• RVU generation
• Patient care time (direct & indirect)
Value Proposition Readiness
• Medical Readiness Assessment Tool
• Polypharmacy Report
Specialty Medications

3/16/2016
10
DOD Pharmacy Engagement Federal Pharmacy Engagement
• DOD/VA Pharmacy Value Collaboration
• Pharmacy MTM handoff in patient transition from DOD to VA
• Aligning GS grades and position responsibilities
• Institutionalizing dispensing interaction based on Indian Health Service practices
Industry Engagement
• MTFs need access to specialty medications through DAPAs
• Opportunities for partnering can capitalize on shared goals in improving adherence and health
• Standardization and interoperability provide win-win-win prospects
Federal Pharmacy 2016: Senior Leaders’ Perspective
RADM Pam Schweitzer, Assistant Surgeon General
Chief Professional Officer for PharmacyU.S. Public Health Service
March 4, 2016
PHS Pharmacists by Agency(1266 Commissioned Corps 2/15/2016)
IHS 554 CMS 35FDA 406 CDC 21BOP 155 NIH 11SAMHSA 6 HRSA 15AHRQ 1 OS 15Coast Guard 16 DOD TMA 10ICE 20
Collaboration - Stronger together
• Indian Health Pharmacy meetings:– Oklahoma, Northern Tier, Quad (Arizona)
• Bureau of Prisons– Denver
• Subject Matter Expert (SME) teams– Chronic diseases, immunizations, geriatrics, wellness,
pain management/opioids, provider status/MTM/CPA’s
• External– Liaisons to organizations, schools of pharmacy
• Cross-category (other USPHS disciplines) collaboration
– Tobacco Cessation, Women’s support group, Wellness (early stages)

3/16/2016
11
“You can do what I cannot do. I cando what you cannot do. Together wecan do great things.”
Mother Teresa
Ongoing…
• Limited distribution drug products
• Health information technology – connecting health, interoperability
• Federal Pharmacy – House of Delegates– Introduced two new business items:
• NBI #9 - Medication Assisted Treatment (MAT)
• NBI #10 - Opioid Overdose Prevention
U.S. Surgeon General Initiatives New
• National Adult Immunization Plan - released
• Surgeon General’s Opioids campaign – coming soon
• Tobacco cessation training program – Rx for Change
– RX for Change: Tobacco Cessation Intervention for Clinicians (Five A Model)
– RX for Change: Basic Tobacco Intervention Program for busy clinicians and non-clinicians (Ask-Advise-Refer)
National Adult Immunization Plan
• http://www.hhs.gov/nvpo/national-adult-immunization-plan/index.html
National Adult Immunization Plan (NAIP) Goals
• Goal 1: Strengthen the adult immunization infrastructure.
• Goal 2: Improve access to adult vaccines.
• Goal 3: Increase community demand for adult immunizations.
• Goal 4: Foster innovation in adult vaccine development and vaccination-related technologies.

3/16/2016
12
Recommended vaccines
• The CDC and its Advisory Committee on Immunization
Practices (ACIP) currently recommend 13 different
vaccines for adults age 18 and older to prevent a host of
diseases:
• Includes:– vaccines that are universally recommended (e.g., influenza)– recommended for certain age groups (e.g., human papilloma
virus [HPV]), – targeted to individuals with specific risk factors (e.g., hepatitis A
and B).– catch-up vaccinations for those adults who never initiated or did
not complete a multi-dose series when vaccination was first recommended during childhood.
National “Network of Networks”
Mission: Engage volunteers to strengthen public health, reduce vulnerability and disaster risk, build resiliency, and improve community preparedness, response and recovery capabilities
Keys to success:
Dedicated volunteers and leaders
Supportive housing organizations
Strong partnerships
Medical Reserve Corps
http://www.naccho.org/topics/emergency/MRC/networkprofile
Mt Kilimanjaro
Key Points
• Mission first
• Support our federal delegates (house of delegates)
• Smoking cessation training
• Develop strategies to improve adult vaccinations
• Your health is important!
Answer to Self-Assessment Question 1
1. The Veterans Health Administration provides care to over 8.9 million Veterans annually from 1,600 medical care sites.
True
3/16/2016
13
Answer to Self-Assessment Question 2
2. DoD Pharmacy is implementing a Congressionally directed Medication Therapy Management pilot in:
a.) Patient Centered Medical Home based care model
b.) A Military Treatment Facility and civilian care based care model
c.) A civilian care based care model
d.) All of the above
Answer to Self-Assessment Question 3
3. Priorities of the Army Medical Department include:
a.) Readiness and Health
b.) Healthcare Delivery
c.) Force Development
d.) Take Care of Soldiers, Civilians and Families
e.) All of the above
Answer to Self Assessment Question 4
4. What opportunities are there for pharmacists to strengthen the healthcare system infrastructure?
a.) Strategize on ways to fill gaps in healthcare delivery
b.) Pharmacist Provider status
c.) Alignment of clinical values across healthcare teams, and a shift to patient-centered goals within care delivery.
d.) All of the above
Closing Remarks
Dr. George E. Jones, [email protected]
COL John [email protected]
RADM Pamela [email protected]