feeding of lbw infants
TRANSCRIPT

Feeding of LBW Infants
Dr. L S DeshmukhDM (Neonatology)

Feeding the LBW Infant
Objectives :• Nutrient requirement• Formula choices• Options for feeding regimens• Adjuncts to feeding

“There is no finer investment for any
community than putting milk into babies”
- Winston Churchill (1943)
LBW Nutrition - Introduction
Improved survival of premies & LBWsGreater morbidity in pretermsIncreased risk of growth deficits and developmental delayIncreased risk of later adult diseaseRecent research, marked difference between LBW versus term AGA nutrition

Goals of LBW NutritionShort term :
- Mimic intrauterine growth/compositionLong term :
- Optimize neurodevelopmental outcome- Impact adult onset disease
Prevent neonatal morbidities :- Improve feed tolerance- Reduce NEC- Minimize infection

Problems of PretermPhysiological Handicaps :• Poor co-ordination of sucking & swallowing (<33 wks)• Weak Gag reflex (aspiration)• Lax esophageal sphincter• Small gastric capacity• Gastroparesis & intestinal hypomotilityBiochemical handicaps :• High energy & micronutrient requirement.• Higher fluid requirement• Increase need for proteins, minerals & vitamins• Relative deficiency of bile acids & lactase
Saili A et al, J Neonatol July-Sept 2002

Current Feeding Practices : Problems
• Volume restriction• Uncertainty about proper conc. of
nutrients • Global undernutrition of LBWs • Increased volume of feeds only after
weight plateus (inadequate growth).• Consequences : ↓ no. of brain cells,
deficit in learning, behavior and memory

Glucose• 6 to 10 mg/kg/min, higher than term.• Higher brain to body ratio• Avoid higher percentage (adiposity &
↑ Co2)
• Hypoglycemia redefined as < 45 mg/dl

Revised Recommended Protein Intake for PT Infants
26-30 wks PCA 4.4 g/kg/d30-36 wks PCA 3.6-4.0 g/kg/d36-40 wks PCA 3.0-3.4 g/kg/d
(Rigo J,J Pediatr,2006)
positive protein balance requires at least 1.5 g/kg/day – Hay ww et al, Pediatr Neonatol. 2010


Lipids• Vital ingredient • Provision of 40-50% calories in TPN• LA & ALA• Lack of AA & DHA• 0.5 gm/kg/d to prevent EFA deficiencyControversies :• Additional LC PUFA to formula/TPN• Supplemental DHA & AA

Role of LCPUFA* Breast milk has adequate conc.* Present formulae deficient* Most important DHA & AA * Major constituents of nerve cell membranes* Key role in the structural development of retinal, neural & synaptic membranes.* Important for visual & neurodevelopment
LBW Nutrition – LCPUFAs • 11 RCTs involving PTs• Many reported beneficial effects on visual,
neural and developmental outcome.• Some reports of negative effect on growth • Cochrane Review, Simmer K, 2004
- Increased early rate of visual maturation- No effect on growth - No long term benefit- Use of fish oil & borage oil in PTs
(Fewtrell MS et al, J Pediatr, 2004)

Ca & P Supplementation
• Two- third body mineral content acquired in 3rd trimester
• Fetal accretion rates 105 mg/kg/d and 70 mg/kg/d for Ca & P respectively
• PT born with low skeletal stores• Very high requirement• Human milk feeding alone-
- Hypophosphatemia- Poor bone mineralization- Elevated Alk. Phospatase- May lead to # & slow growth
Ca & P Supplementation Osteopenia of prematurity, commoner < 1000 g Ca & P deficiency, rarely vitamin D deficiency Ca & P accretion in utero equal to puberty Rates of bone formation equal to adult Ca absorption around 60% - 70%
(Hawthorne KM et al, Minerva Pediatr, 2004)

Ca & P Supplementation• Recommended intakes – • Ca : 200-220 mg/kg/d,• P : 100-110mg/kg/d • Ca : P ratio > 16 wks GA 1.8:1• Supplementation with both essential
for postnatal bone mineralization.• Supplement till 42-43 wks PNA• Cochrane Review : No studies which met
selection criteria were identified(Carl A Kuschel , 2009)

LBW Nutrition - Iron
• Total body iron low at birth
• Further decrease in iron, phlebotomy losses / Epo
• Early iron deficiency – Late cognitive effects
• Dose 2-4 mg/kg/d started between 2 wks to 2 mo PNA
• 6 mg/kg/d for Epo / IDA (Rao R et al, Semin Neonatol. Oct. 2001)

Zinc Supplementation* Preterm HM has less conc. & LBW may be zinc
deficient * Better weight gain* May improve immune function* Improves mental development & behaviour ?
(Lira PI et al, Eur J Clin Nutr, 1998) Sazwal et al, Indian StudySazwal et al, Indian Study, Pediatr 2001, Pediatr 2001
- Decreased risk of death due to diarrhea- Decreased risk of death due to diarrhea- Zinc deficiency more in SGA babies- Zinc deficiency more in SGA babies
Effect on growthEffect on growth- Better weight & height gain - Better weight & height gain - Dose : 2 mg/kg/d x 6 wks- Dose : 2 mg/kg/d x 6 wks
Islam MN et al. indian pediatr, 2010Islam MN et al. indian pediatr, 2010

Vit.A Supplementation Regulates & promotes growth of many cells Maintains integrity of respiratory epithelial tract Important for visual pigment, human function and as antioxidant. 1000 IU / kg/d for all VLBWTheraupeutic use ↓ O2 requirement & BPD ↓ ROP ↓ Nosocomial sepsis Dose : 5000 IU IM 3 times a wk x 4 wks.
Oral - 4000 IU/kg/d ( Darlow BA, Cochrane Review, 2002)

Vitamin E in LBW Nutrition•Routine supplementation, ↑ses Hb marginally•↓ risk of IVH, •↓ risk of severe ROP•RD for LBW - 0.7 IU/100 kcal + 1 IU/gm
PUFA•Recommended 10 mg/d (Oral)
IM 20 mg/kg/d x 3 d•Side effects : sepsis, NEC, thrombocytosis
((Brian LP, Cochrane Review, 2006)Brian LP, Cochrane Review, 2006)

Enteral feeding - Early Gut Development
• Int. mucosal development by IInd trimester.
• Organize motility develops till 28-30 wks.
• Motility – rate limiting• Poor esophageal motility – GER• Gastric emptying slower• Only 50% <28 wks. pass mec. within
3 d.

Maturation of oral feeding skills in LBW infants
GA Maturation of feeding skills Initial feeding method
< 28 wks No proper sucking effortsNo propulsive motility in the gut
Intravenous fluid
28-31 wks Sucking bursts developNo coordination between suck/swallow and breathing
Oro-gastric (or naso-gastric) tube feeding with occasional spoon/paladai feeding
32-34 wks Slightly mature sucking patternCoordination between breathing & swallowing begins
Feeding by spoon/paladai/cup
>34 wks Mature sucking patternMore coordination between breathing and swallowing
Breast feeding

Enteral feeding - issues• what milk to feed• what nutritional supplements• how to feed• how much and how frequently• what support • how to monitor

What to feed
• Nutritional sources for LBW infants Human milk Breastmilk substitutes Locally prepared animal milks
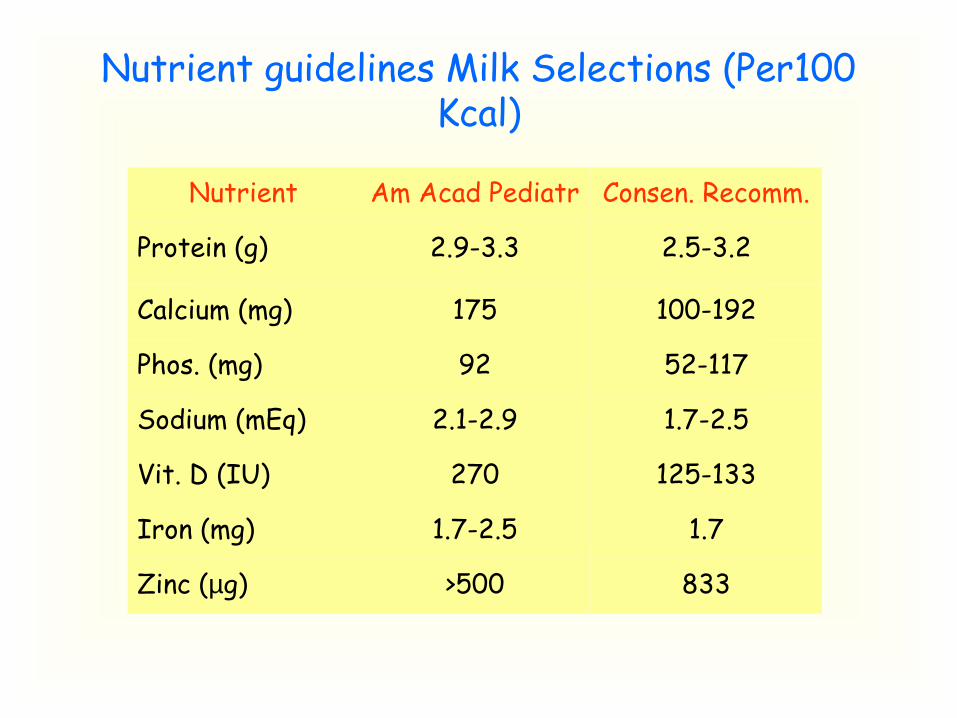
Nutrient guidelines Milk Selections (Per100 Kcal)
Nutrient Am Acad Pediatr Consen. Recomm.
Protein (g) 2.9-3.3 2.5-3.2
Calcium (mg) 175 100-192
Phos. (mg) 92 52-117
Sodium (mEq) 2.1-2.9 1.7-2.5
Vit. D (IU) 270 125-133
Iron (mg) 1.7-2.5 1.7
Zinc (µg) >500 833

Recommended dietary allowance in preterm VLBW infants and the estimated intakes with
fortified/unfortified human milkRDA
(Units/kg/d)At daily intake of 180 ml/kg
Only expressed Breast milk
EBM fortified with lactodex-
HMF (4g/100mL)
EBM fortified with preterm
formula (4g/100mL)
Energy (kcal)Protein (g)Carbohydrates (g)Fat (g)Calcium (mg)Phosphorus (mg)Vit. A (IU)Vit. D (IU/d)Vit.E (IU)Vit B1 (mcg)Vit B2 (mcg)Bit. B6 (mcg)Folic acid (mcg)Zinc (mg)
105-130305-4.010-145.4-7.2
210110
90-270400>1.3>48>72>4239.6>0.6
1172.4611.66.8
43.222.26803.51.9
36.284.225.7
60.6
1443.2
16.847.122311233089036.379.4156.2115.71500.96
1533.4
15.589.0610352980403.6231
564.222136
0.96
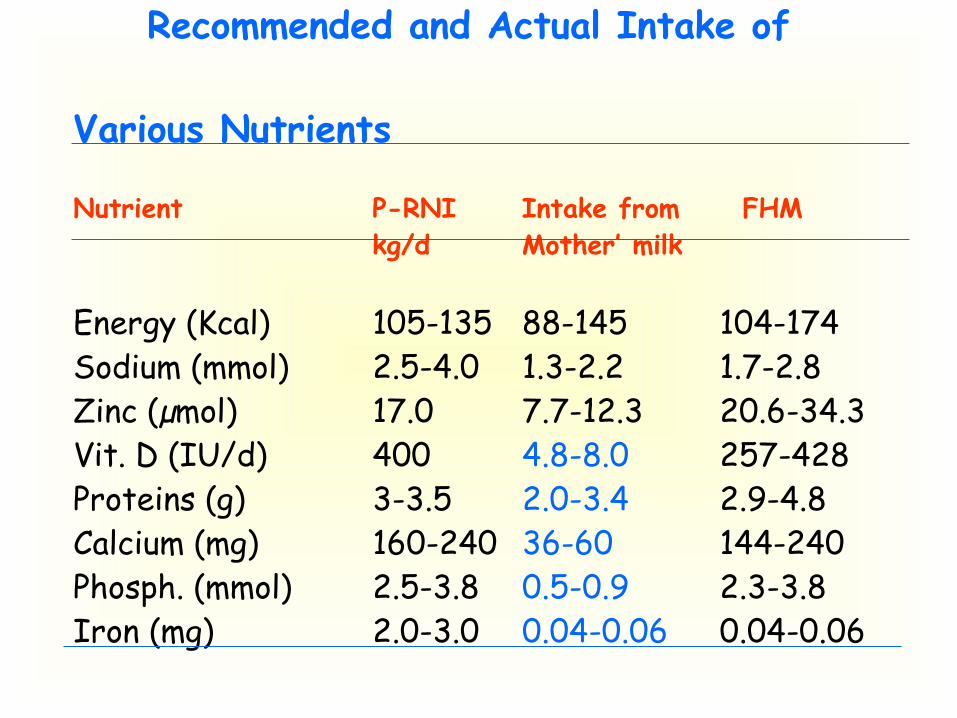
Recommended and Actual Intake of Various Nutrients
Nutrient P-RNI Intake from FHMkg/d Mother’ milk
Energy (Kcal) 105-135 88-145 104-174Sodium (mmol) 2.5-4.0 1.3-2.2 1.7-2.8Zinc (µmol) 17.0 7.7-12.3 20.6-34.3Vit. D (IU/d) 400 4.8-8.0 257-428Proteins (g) 3-3.5 2.0-3.4 2.9-4.8Calcium (mg) 160-240 36-60 144-240Phosph. (mmol) 2.5-3.8 0.5-0.9 2.3-3.8Iron (mg) 2.0-3.0 0.04-0.06 0.04-0.06

Human milk• Mother’s own milk and donor milk• Fore milk and hind milk• Drip milk and expressed milk
Storage of human milkHUMAN MILK SUPPLEMENTS

Prevents Infection & InflammationsIgA, Lactoferrin,
Lysozyme, Cytokines,
oligosaccharides
Promotes int. adoptation
sIgA, Growth factor, hormones,
oligosaccharides
Enhance function poorly expressed
in the infants
Lipids, cytokines, hormones
Promotes establishment of
beneficial microbiota
sIgA, Lactoferrin, α-LA, Oligosaccharides
Compensate for immaturity of the
intestine
Neocleotides, PAF-AH, cytokines growth factors
Beneficial effects of bioactive agents in
HM
Human milk supplementation
• Individual vitamins or minerals— Vitamin A— Vitamin D— Vitamin K— Iron— Zinc— Calcium and phosphorus• Multivitamins• Multicomponent fortifiers

Multicomponent Fortifier
• facilitate more rapid catch-up growth
• May improve neurodevelopmental outcomes.
• logistically difficult for infants fed directly
McCormick FM et al, 2010

Fortified Breast Milk : Safety
• HM – sterile product• EBM contamination at various points.
- Pumping- Storage- Transportation- Addition of fortifier- Setup & administration of feed
• Effect of iron content on bacterial growth(Dalidowitz C, J Am Diet Asso, Oct, 2005)

Breastmilk substitutes
• Pre-term infant formulas• Standard infant formulas• Nutrient enriched “post-discharge”
formulas• Soy-based formulas
ENTERAL FEEDING – Time of initiation
• Early Vs Delayed feeding• Early feeding < 4 d • Delayed > 5-7 d• Feeds delayed to dec. NEC• No evidence that delayed introduction
of progressive enteral feeds prevents NEC (Morgan J et al , cochrane, 2011 )
Delayed Feeding : Consequences
• Fewer mucosal antibody cells. • Reduction in the local immune response.• Decreased enzyme levels.• Damage to mucosal barriers.• Increased susceptibility to infections.• Morphologic injury.• Decreased secretion of IgA.• Bacterial overgrowth.

Minimal Enteral Nutrition (MEN) Benefits
- Stimulates secretion of GI hormones- Improved glucose tolerance (enteroinsular axis)- Stimulates motor activity- Stimulation of bile flow & ↓ cholestasis
AIIMS- NICU protocols 2008

Minimal Enteral Nutrition (MEN)•Dilute / full strength feeds < 10 to 15mL/Kg/day or no enteral nutrient intake (water only)•“Trophic” feedings
•↓ feed intolerance•? ↓ NEC•↓ hospital stay
Tyson JE, Cochrane Review, 2006,

* Can be started on ventilator and /or receiving TPN* In severe birth asphyxia, after 48-72 hours* VLBW infants born with antenatal diagnosis of altered umbilical arterial blood flow delayed for 2 to 3 days.
MEN - essentials

Initiation of Enteral Feeding : IssuesNG V/s OG Feeding :Nasogastric feeding - Pulmonary compromise - Higher A & B Orogastric Feeding :- Grooved palate- SialadenitisNo large RCTs available, insufficient
data (Cochrane Review, 2006)

Initiation of Enteral Feeding : Issues
Feeding tube placement :Size of feeding tube : Problems with larger
tube • Nasal inflammation • Throat irritation• Pressure necrosis• Pulmonary compromise • GER• Apnea & bradycardiaUse smaller feeding tubes

Initiation of Enteral Feeding : IssuesIntermittent Bolus FeedBenefits :- Promotes cyclical surge of gut
hormones- Promotes gut developmentRisk :- Feeding intolerance- Delayed gastric empty / intestinal
transit- Difficult metabolic homeostasis

Initiation of Enteral Feeding : Issues
Continuous Feeding :Benefits :- Energy efficient- Improved nutrient absorption- Reduced feed intolerance- Improved growthRisk :- Alters cyclical pattern of release of
hormones- Potential to affect metabolic homeostasis− ↑ GER

Continuous vs. intermittent feeding
• There is no difference in time to achieve full feedings
(Premji SS et al, Cochrane,2008 )

Enteral feeding - interval
• ad libitum or demand/semi demand Vs Scheduled • Some evidence - earlier hospital
discharge
(McCormick FM, Cochrane, 2010 )

Feeding volumes and frequency
Birth weight
(g)
Starting volume
(ml/kg/d)
Volume increment each day (ml/kg/d)
Maximum volume
(ml/kg/d)
Frequency of feeds
<1200 10-20 20 180 2 hrly1200-1600
60 30 180 2 hrly
>1600 60 30 150 3 hrly

Cup feeding versus Bottle / spoon
• cup fed more likely to be exclusively breastfed at hospital discharge
• no difference at 3 / 6 mo• one study feed by cup spent ten days
longer in hospital• cannot recommend cup feeding.
Flint A et al , Cochrane , 2008

Initiation of Enteral Feeding : Issues
Enteral Feeding with Umbilical Lines :• Fear of feeding problems & NEC• A prospective, RCT of 60 PT infants
with low UAC – no feeding problems• Monitor infants for signs of feeding
problems.
Breast Feeding LBW - Challenges
• Fortification of preterm HM• Establishing a milk supply• Maintaining milk supply• Transition from gavages to
breast feed• Incidence and duration of BF• Barrier to BF in PT

Initiation of Breast Feeding : When ? • Traditional Criteria :• Physiologic stability• Ability to tolerate bolus feeds• GA > 34 wks & BW > 1500 g
• Behaviorally based criteria :• Mother – Caregiver observations • Infant sucks on pacifier / tube• Makes rooting motions
• Has brief periods of active / quiet alert state

feeding intolerance
•Significant abdominal distension or discoloration
•Signs of perforation
•Obvious blood in stool •Gastric residuals 25% to 50% of interval volume for 2 to 3 feedings
•Bilious gastric residual or emesis
•Significant apnea/bradycardia
•Significant cardiopulmonary instability
(The Vermont Oxford Network "Got Milk" focus group ,2003)

Gastric residuals
• Prefeed aspirate, milky & > 50%, omit feeds & evaluate
• 25-50%, omit feed & monitor (AC)
• < 25% aspirate, push back, monitor & continue feeding.
(Saili A, J Neonatol, 2002)

Non-nutritive Sucking (NNS)
•Different from nutritive sucking•During gavage feeds•Pacifier (thumb size) / empty breast•Facilitates development of sucking.•Improves digestion •Decreased hospital stay
(Source : Pinelli J. Chochrane Review, 2010)•Calming as well as analgesic effect
(Source : Symington A, Chochrane Review, 1998)

Kangaroo Mother Care (KMC)
Possible Benefits:• Promotes & Prolongs Breastfeeding• Physiologic stability ( A&B, quiet sleep)• Maternal confidence & Bonding• Decreased Infection• Cost Savings
(Kirsten GF, PCNA,2001)

Oil Application / Massage
• Greater weight gain • ? Greater length gain• Better neurobehavior• Better thermoregulation
(Ramji S et al, 2005; Modkar JA et al, 2005)
• Better skin barrier function∀ ↓ sepsis (use of sunflower seed oil)
(Darmstadt GL et al, 2005)

Feed Intolerance : Oral Erythromycin
• Potent prokinetic activity• Acts through motilin receptors • Improves feed tolerance• Cochrane review, 2008- not enough evidence
to show any benefit• high-dose erythromycin probably justifiable
(Lam HS et al, Curr Opin Pediatr. 2011 Apr;23(2):156-60 )

Lactase Treated Feeds• Last of the disaccharidases to develop in PT.• first detectable in the fetal intestine by 10
weeks' gestation • At 28 to 34 weeks, lactase activity is only ~30% • often managed with soy protein, protein
hydrolysate, low lactose, or lactose-free formulas • Lactase to hydrolyse lactose for promotion of
growth & feed intolerance.• greater rate of weight gain and higher serum
albumin- indicative of improved nutritional status (J Pediatr, Oct. 2002)
• Single RCT, no significant benefit. (Ohlsson A et al, cochrane 2006),

Feed Intolerance : Adjuncts• Enteral insulin - accelerates GI develop.
- stimulates intestinal activity - increases lactate activity
Pilot study, Shulman RJ, 2002Limitation : Historic controls, need RCT
• Enteral solution (like human amniotic fluid)- Phase I trial, significant increase in milk feeding.- May be related to growth factors
(Barney CK et al, Adv Neo Care, April, 2006)• Cisapride : RCT, Kohl M et al, Biol Neonate, 2005
- No benefit (only in ELBW)- More vulnerable to side effects
• Metoclopramide : No role, adverse effects
Role of Glutamine•Increased feed tolerance•Decreased sepsis•Decreased nosocomial infections•Better short term outcome•Dose – 0.3 gm/kg/d
Van Den Berg et al, Am J Clin Nutr, 2005
• No effect on mortality, serious infection, gut complications or long term development.Tubman TRJ et al, Cochrane Review, 2006
•may lead to significant improvements in growth Korkmaz A, Turk J Pediatr. 2007

Role of Arginine
• RCT• 152 PT infants• L-arginine (1.5 mmol/kg/d)• Significant decrease in all
stage of NEC(Amin HJ et al, J Pediatr 2002)

Role of probiotics• Two Meta-analyses
• reduced the risk of death due to all causes
• Significant decrease in NEC
• No effect on sepsis
• No significant adverse effects
• strain specific Szajewska H, Early Hum Dev. 2010

Prebiotic supplementation
• galacto-oligosaccharides• fructo-oligosaccharides• supplementation appears safe• may benefit enteral tolerance in the most immature infants.
Modi N et al, Pediatr Res. 2010 Nov;

Antenatal corticosteroids –
Role in PT nutrition.• Early introduction of enteral feeding• Enhanced intestinal motility, integrity
and growth• Maturation of intestinal arginine
synthesis• Shortened hospital stay
Wu G et al, J Nutr Biochem Aug. 2004.

Feeding of LBW : Poor Weight Gain
Diet Considerations :• Incorrect calculations of actual
intakes• Milk prepared incorrectly• Volume intakes not advanced for
weight gain.• Increased nutrient demands• Feed intolerance
Feeding of LBW : Poor Weight Gain
Use of Human Milk Consideration :• Greater vol. production than intake
(foremilk V/s hindmilk)• Incorrect proportion of HMF• Need for sodium supplementation• Need for increased vol. or protein
supple.

Approximate Daily Weight Gain for InfantsGestational age g/kg/d24-28 wk 15-2029-32 wk 17-2133-36 wk 14-1537-40 wk 7-9
Corrected age g/d40 wk – 3 mo 303-6 mo 206-9 mo 159-12 mo 1012-24mo 6
Care of high-risk infant, Klaus,2000

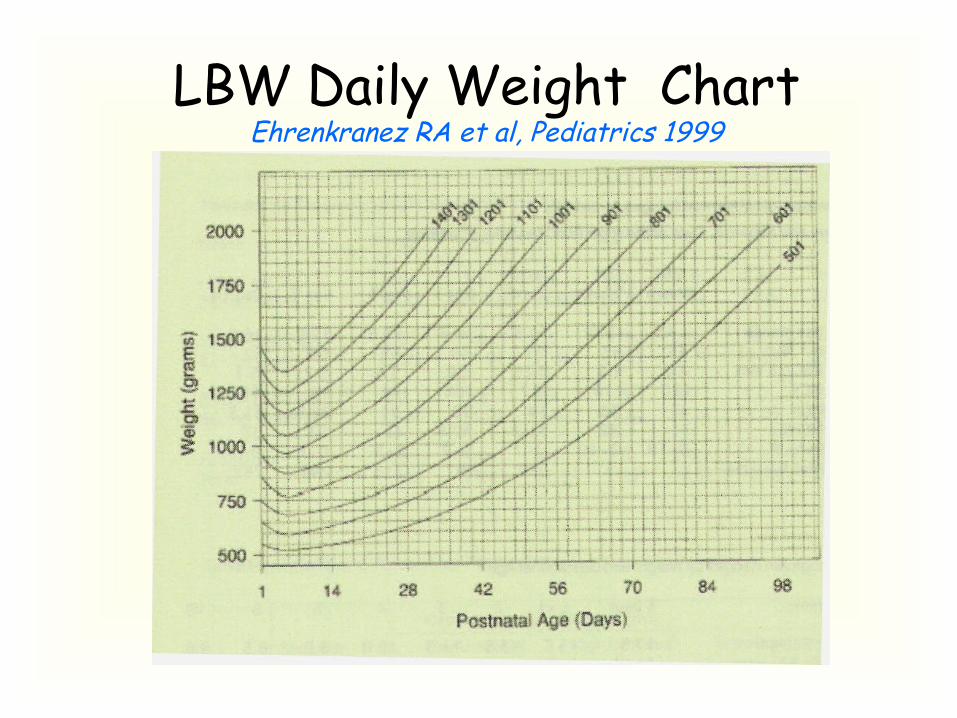
LBW Daily Weight ChartEhrenkranez RA et al, Pediatrics 1999

MCT oil for wt gain
• primarily of energy• Increased weight-length ratio• producing obesity• RCT, PE Vs MCT oil’• Significantly higher protein intake • better growth
Brumberg HL et al, J Perinatol. 2010

Postdischarge Nutrition• Often neglected • Mostly only breast fed• More attention beneficialImportant for : Who can’t consume ad libitum quantities Poor growth Abnormal biochemical screen of nutritional
statusImportant – monitor just before and at least one
month after discharge and consider fortification
Lucas A et al, Pediatr 2001.

Weaning Preterm Infants
• Early onset of weaning
• Use of foods with higher energy and protein
• Foods rich in iron and zinc
• Beneficial effect on length & iron status
Marriott LD et al, Arch Dis Child Fetal Neonatal ed. Nov. 2003

Feeding Options for PTsDuring stable growth phaseFirst Choice : preterm human milk +
Lactodex – HMF (if affordable) + Fe supplements from 2 wks.
ORPreterm human milk + Ca/P +
multivitamins, Zinc + Fe supplement.Second Choice : LBW formula milk +
multivitamins, Zinc + Fe supplements.Third Choice : Undiluted cow’s milk +
mltivitamins, Zinc + Fe supplement.

Potentially Better Practices
• Monitoring of growth & nutrition• Early initiation of enteral nutrition• Consistent systematic advancement of feeds.• Uniformity & clarity as to withholding feeds.• HM is the preferred nutrient for PT• Use of appropriate enteral products• Early initiation of TPN, when feasible
(The Vermont Oxford Network "Got Milk" focus group ,2003)

Thank You

Developmental signs that show readiness for feeding
Behaviour at the breast
Response when offered expressed breat mild by cup
Range of gestational or post-menstrual age (wks)
Feeding readiness
Range of birth weight
No definite mouthing
No extrusion of tongue, no licking
< 28 No readiness IV feeding neededIntragastric tube may be possible
< 1000 g

Developmental signs that show readiness for feeding
Behaviour at the breast
Response when offered expressed breast milk by cup
Range of gestational or post-menstrual age (wks)
Feeding readiness Range of birth weight
Occasional, ineffective suckling attempts
Opning mouth, tongue out of the mouth, licking milk. Not able to coordinate breathing and swallowing well
28-31 First signs of oral readiness.Intragastric feeding appropriate Can try small amount of direct expression or cup feeding to gain oral experience
1000-1500g

Developmental signs that show readiness for feeding
Behaviour at the breast
Response when offered expressed breast mild by cup
Range of gestational or post-menstrual age (wks)
Feeding readiness Range of birth weight
May root and attach to breast. Weak suckling attempts
Opening mouth, tongue forward, licking milkAble to coordinate breathing and swallowing well
32-34 Can now use cup or other alternative feeding method for most feeds.Allow baby to attach to breast for part of feed or for some feeds
1300-1800g

Developmental signs that show readiness for feeding
Behaviour at the breast
Response when offered expressed breast mild by cup
Range of gestational or post-menstrual age (wks)
Feeding readiness
Range of birth weight
Able to root and attach to the breast
May have periods of organized suckling with long pauses
Opening mouth, tongue forward, licking milk, coordinating breasting and swallowingCoordinating breathing and swallowing wellAn now able to suck at the milk from the cup and other alternatives
33-35 Breast feed for part of feedor some complete feeds
Cup or alternative supplement most feeds to ensure adequate intake
1600-2000g

Developmental signs that show readiness for feeding
Behaviour at the breast
Response when offered expressed breast mild by cup
Range of gestational or post-menstrual age (wks)
Feeding readiness
Range of birth weight
Able to suckle effectively at the breast
Able to suck at milk from the cup and other alternative feeding methods
34-36 Breastfeed, and may need some supplements by cup or other alternative
1800-2200g