fetal dna for the prediction and diagnosis of genetic...
TRANSCRIPT
Fetal DNA for the prediction and diagnosis
of genetic disorders
Uwe Werner Fass
Oman Medical College
2. International Pediatric and Neonatology Conference
Muscat 13.-15.4.2017

NIPT and NIPD
Non-Invasive Prenatal Testing and
Non-Invasive Prenatal Diagnosis
Is a genetic prenatal diagnosis possible?
Yes.

Thoughts and Reality -- 3 Statements
I
The vast majority of disorders and conditions for which prenatal testing is performed are largely incurable. This situation will not change with assessment of cell free fetal (cff) DNA in maternal blood.
Prenatal Screening for fetal abnormalities has not changed much since its introduction in the last quarter of the past century
The technical possibilities of genomic deep sequencing, the ease to obtain a blood sample from a pregnant women and isolate cffDNA in addition to commercial interests have already changed screening for aneuploidies and other genetic conditions in fetal medicine.
Thoughts and Reality -- 3 Statements
I
The vast majority of disorders and conditions for which prenatal testing is performed are largely incurable. This situation will not change with assessment of cell free fetal (cff) DNA in maternal blood.
Prenatal Screening for fetal abnormalities has not changed much since its introduction in the last quarter of the past century
The technical possibilities of genomic deep sequencing, the ease to obtain a blood sample from a pregnant women and isolate cffDNA in addition to commercial interests have already changed screening for aneuploidies and other genetic conditions in fetal medicine.
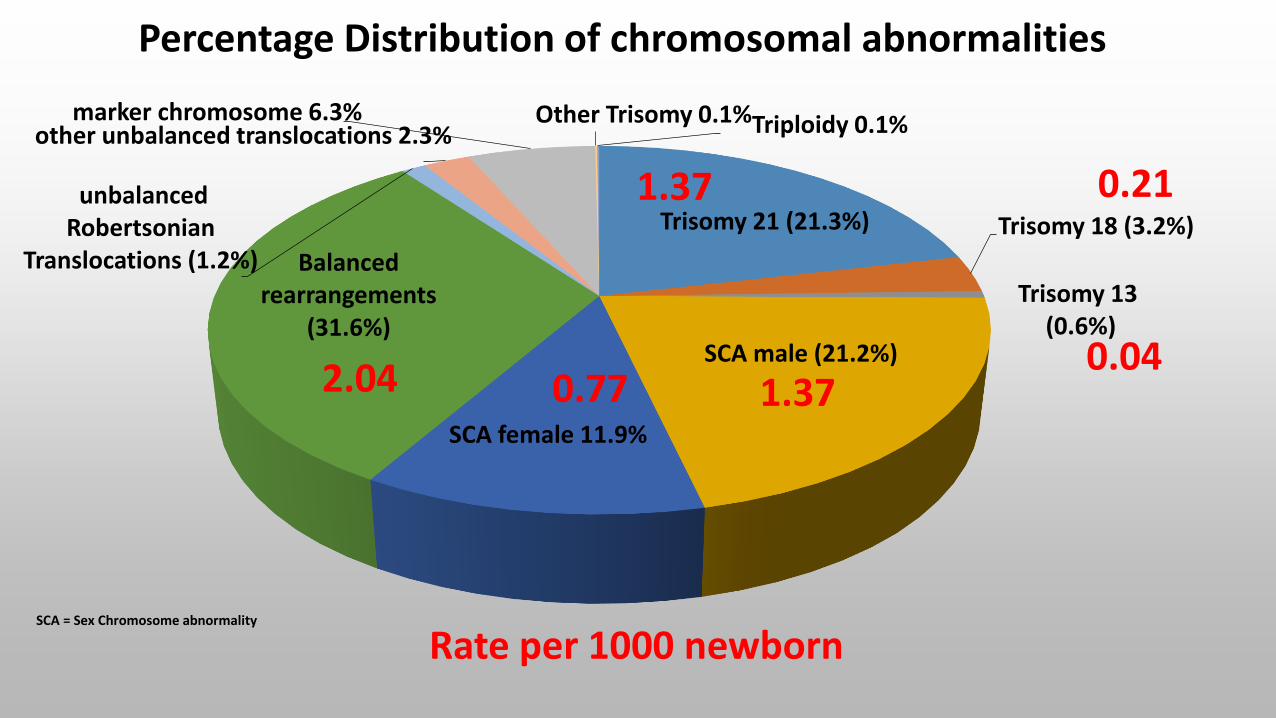
Percentage Distribution of chromosomal abnormalities
Rate per 1000 newborn
Trisomy 21 (21.3%) Trisomy 18 (3.2%)
Trisomy 13(0.6%)
SCA male (21.2%)
SCA female 11.9%
Balanced rearrangements
(31.6%)
unbalanced Robertsonian
Translocations (1.2%)
other unbalanced translocations 2.3%marker chromosome 6.3% Other Trisomy 0.1%Triploidy 0.1%
1.37 0.21
0.041.370.772.04
SCA = Sex Chromosome abnormality

Thoughts and Reality -- 3 Statements
I
The vast majority of disorders and conditions for which prenatal testing is performed are largely incurable. This situation will not change with assessment of cell free fetal (cff) DNA in maternal blood.
Prenatal Screening for fetal abnormalities has not changed much since its introduction in the last quarter of the past century
The technical possibilities of genomic deep sequencing, the ease to obtain a blood sample from a pregnant women and isolate cffDNA in addition to commercial interests have already changed screening for aneuploidies and other genetic conditions in fetal medicine.

Genetic Red Flags in Pregnancies
National Coalition for Health Professional Education in Genetics. The Risk Assessment. Pregnancy and Health Profile
Advanced maternal age (>>35 years)
High risk ethnic / racial heritage (ie, Mediterranean )
Consanguinity
Family history (mother or father) of a known or suspected genetic condition
Multiple affected family members with the same or related disorder
Major malformation (ie, heart, kidney, brain) or other birth defects occurring in mother, father, grandparents, offspring or close reletives (brother/sisters)
Congenital blindness or deafness in family members
Extremely tall or short stature of mother, father, or their relatives
Developmental delays or mental retardation occurring in mother, father, offspring, or close relatives
Recurrent pregnancy losses (2 or more) for the mother
Environmental exposure to known or suspected teratogens
Infertility or premature ovarian failure
Low Risk Women / Pregnancy
High Risk Women / Pregnancy
Genetic Risk Status

Genetic Risk Status
I
Low Risk Women / Low Genetic Risk Pregnancy High Risk Women / High Genetic Risk Pregnancy
A high genetic risk is defined if any of the genetic risk factors apply - maternal age >>35 years- positive family history congenital malformation,
chromosomal disorder, monogenetic disorder
in absence of risk factors, women / pregnancy isconsidered low risk

Genetic Risk Status defines Screening Approaches
ACOG; Driscoll DA, Genet Med 2008 10(1) 73-75
Risk low
Available Options
1st Trimester Screening 2st Trimester Screening
Available Options
Mat. Serum MarkersSonogram for NT
Mat. Serum MarkersFetal anatomic sonogram
Diagnostic TestingCVS or Aminocentesis
Karyotype vs. CMA
Genetic Counselor
Final DispositionTest Results Test Results
Anticipate newborn without aneuploidy
or identifiable genetic of congenital defect
Anticipate newborn with and accurately
identified chromosomal, genetic
or congenital defect
-
+
--
+
+

Genetic Risk Status defines Screening Approaches
ACOG; Driscoll DA, Genet Med 2008 10(1) 73-75
Risk high
Available Options
1st Trimester Screening 2st Trimester Screening
Available Options
Mat. Serum MarkersSonogram for NT
Mat. Serum MarkersFetal anatomic sonogram
Final DispositionTest Results Test Results
Anticipate newborn without aneuploidy
or identifiable genetic of congenital defect
Anticipate newborn with and accurately
identified chromosomal, genetic
or congenital defect
-
+
--
+
+
Diagnostic TestingCVS or Aminocentesis
Karyotype vs. CMA
Genetic Counselor

Genetic Risk Status defines Screening Approaches
ACOG; Driscoll DA, Genet Med 2008 10(1) 73-75
Risk high
Available Options
1st Trimester Screening 2st Trimester Screening
Available Options
Mat. Serum MarkersSonogram for NT
Mat. Serum MarkersFetal anatomic sonogram
Final DispositionTest Results Test Results
Anticipate newborn without aneuploidy
or identifiable genetic of congenital defect
Anticipate newborn with and accurately
identified chromosomal, genetic
or congenital defect
-
+
-+
Diagnostic TestingCVS or Aminocentesis
Karyotype vs. CMA
Genetic Counselor
-+

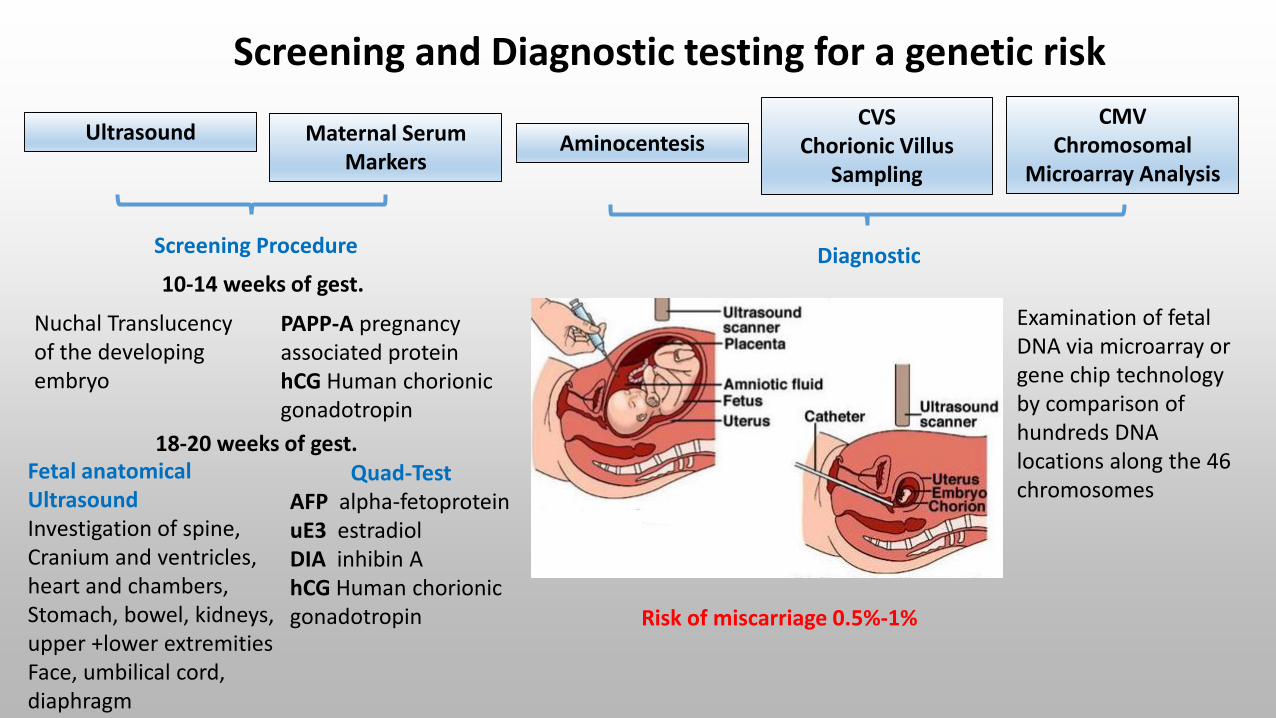
Screening and Diagnostic testing for a genetic risk
Maternal Serum Markers
UltrasoundCVS
Chorionic Villus Sampling
AminocentesisCMV
ChromosomalMicroarray Analysis
Screening Procedure Diagnostic10-14 weeks of gest.
Nuchal Translucencyof the developing embryo
PAPP-A pregnancy associated proteinhCG Human chorionicgonadotropin
18-20 weeks of gest.Fetal anatomicalUltrasoundInvestigation of spine, Cranium and ventricles, heart and chambers,Stomach, bowel, kidneys,upper +lower extremitiesFace, umbilical cord,diaphragm
Quad-TestAFP alpha-fetoproteinuE3 estradiolDIA inhibin AhCG Human chorionicgonadotropin

● Gestational age ●Maternal age ● Race/ethnicity ●Weight ● Presence of diabetes ● singl. vs multiple gest.
Maternal Serum MarkersPAPP-A Pregnancy Associated protein hCG human chorionic protein
AFP alfa fetoprotein uE3 estradiol DIA inhibin A
Value is influenced by…..
Reporting…….
● multiple of the median (MoM)
Individual Serum concentration Mean of the population for the specific gestational age
1 Trimester 2. Trimester
DIA High, above 95th percentile
hCG above 95th percentile above 95th percentile
PAPP-A Below 5th percentile
uE3 far below 5th percentile
AFP far below 5th percentile
High risk for chromosomal abnormality exist:
Screening and Diagnostic testing for a genetic risk
Maternal Serum Markers
UltrasoundCVS
Chorionic Villus Sampling
AminocentesisCMV
ChromosomalMicroarray Analysis
Screening Procedure Diagnostic10-14 weeks of gest.
Nuchal Translucencyof the developing embryo
PAPP-A pregnancy associated proteinhCG Human chorionicgonadotropin
18-20 weeks of gest.Fetal anatomicalUltrasoundInvestigation of spine, Cranium and ventricles, heart and chambers,Stomach, bowel, kidneys,upper +lower extremitiesFace, umbilical cord,diaphragm
Quad-TestAFP alpha-fetoproteinuE3 estradiolDIA inhibin AhCG Human chorionicgonadotropin Risk of miscarriage 0.5%-1%
Examination of fetal DNA via microarray or gene chip technologyby comparison of hundreds DNA locations along the 46chromosomes

Thoughts and Reality -- 3 Statements
I
The vast majority of disorders and conditions for which prenatal testing is performed are largely incurable. This situation will not change with assessment of cell free fetal (cff) DNA in maternal blood.
Prenatal Screening for fetal abnormalities has not changed much since its introduction in the last quarter of the past century
The technical possibilities of genomic deep sequencing, the ease to obtain a blood sample from a pregnant women and isolate cffDNA in addition to commercial interests have already changed screening for aneuploidies and other genetic conditions in fetal medicine.
Routine History Taking
I
Feb 2017, Dr. S., Gynecologist, Germany
Good MorningDr. S. Good Morning
Dr. S. What is the gestational age
Dr. S. Do you have your previous ultrasound investigations with you
Dr. S. What laboratory test have you done? Did you do a glucose tolerance test.
Dr. S. What genetic screening test of cffDNA was conducted?
Me: We did not screen cffDNA
Dr. S. Why not. Is this too expensive in Oman? The health insurance pays here half of it.
Me: What to do with the results.
Dr. S. Ok, lets see

cffDNA or cf maternal DNA or cfDNA
Nowroz H, Nature Medicine 1996 (2) 1035 Microsatelite alterations in Serum DNA of head and neck cancer patients
squamouscell carcinoma
Cancer
Chen XQ, Nature Medicine 1996 (2) 1033 Microsatelite alterations in plasma DNA of small cell lung cancer patients
Cell free fetal DNA or cell free maternal DNA or cell freeDNAWhat's this
L T S
L T S
D3S1238
D2IST245
L – LymphocyteT – TumorS - Serum
Microsatelite changeswhich are distinct to the tumorwere detected in serum

Tumor and Placenta…What are common cell-biological concepts
Image: Annu. Rev. Med. 2016 (67) 419-432 Prenatal Diagnosis Innovation:Genome Sequencing of Maternal Plasma

Lo Dennis YM (1997) Lancet (350) 485-487 Presence of fetal DNA in maternal plasma and serum
Identification of fetal DNA in Maternal Plasma, Serum and Blood
0
20
40
60
80
Plasma Serum Blood
% c
ase
s
Male Female
43 pregnant women(30m/13f)
PCR of Y-chromosomespecific marker (DNA-Sequence)
New Insights
1. Fetal DNA occurs in maternal plasma
2. Assessment of fetal cell free DNA allows the determination of gender
Isolation of DNA, in Plasma, Serum and nucleated cells
3. Implications for non-invasive prenatal screening and diagnosis
Analysis Electrophoresis
male embryo: 17, 22, 5, 25, 28

Lo Dennis YM (1999) Am. J. Hum. Gent. (64) 218-224 Rapid clearance of fetal DNA from maternal plasma
Clearance of fetal DNA after Delivery
12 pregnant women(m)
Assessment sex determining region Y gene after deliveryin Plasma by PCR
40min
4. Half-life time for circulating fetal DNA 16.3 minutes (range 4-30 minutes)and is undetectable a few hours after delivery
New Insights

Characteristics of cell-free fetal DNA
I
● Plasma contains cell free DNA.
● 10-20% of maternal cell free DNA are of fetal origin (during gestation).
● cell-free fetal DNA is degraded immediately, within hours after birth
● cell free fetal DNA has an approximate length of around 143bp, maternal cell free DNA has an length of 166 bp
● cell free fetal DNA occurs after 9 to 10 weeks of gestation

HGD
HGD
HGD
HGD
HGD
HGD
HGD HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD HGD
HGD

HGD
HGD
HGD
HGD
HGD
HGD
HGD HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD HGD
HGD

HGD
HGD
HGD
HGD
HGD
HGD
HGD HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD HGD
HGD
HGDHGD
HGD
HGD
HGD HGDHGD
HGD
HGD HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD
HGD
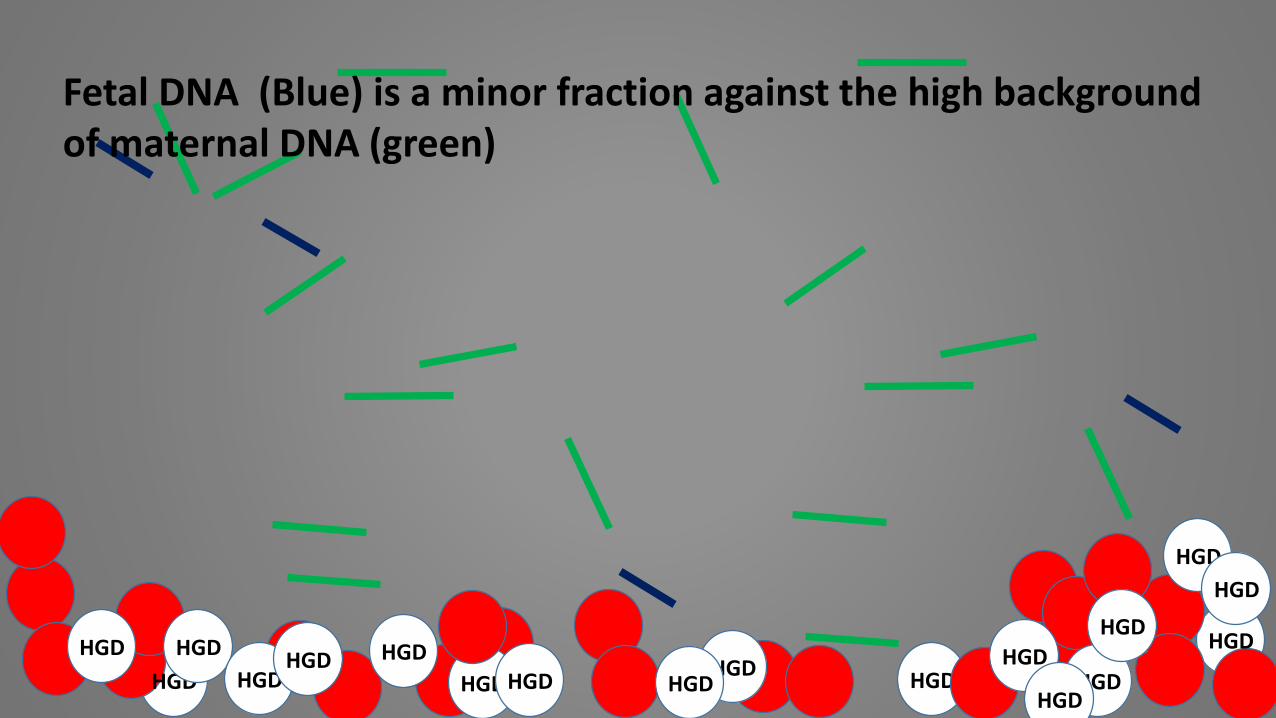
Fetal DNA (Blue) is a minor fraction against the high background of maternal DNA (green)

Analysis of cell-free fetal DNA in maternal Plasma

Detection of Aneuploidies by massively parallel genomic sequencing
I
Maternal cfDNA
cffDNA
Robertsonian TranslocationTrisomy21 Down Syndrome

Detection of Aneuploidies by massively parallel genomic sequencing
Chiu RW PNAS 2008 (105) 20458

Statements and Opinions of Professional Societies to guide NIPT
I
National Society of Gentic Counselors (NSGC)International Society for Prenatal Diagnosis (ISPD)Society for Maternal-Fetal Medicine (SMFM)American Congress of Obstetricians and Gynecologists (ACOG)American College of Medical Genetics and Genomics (ACOG)European Society of Human Genetics (ESHG)American Society of Human Genetics (ASHG)
AGREEMENT DISAGREEMENT
Pre- and Post-test genetic counselling
Clear statement that NIPT is a SCREENING TEST (no DIGNOSTIC TEST)
ACOG, ESHG and ASHGNIPT should be offered to all women
NSGC, ISPD, SMFM, ACOGNIPT should be offered to women with genetic high risk (advanced maternal age, prior affected pregnancy,positive serum screen)

Norton ME; NEJM 2015 372(17) 1589 Cell-free DNA Analysis for Noninvasive Examination of Trisomy
Cell-free DNA (cfDNA) testing for fetal trisomies is highly effective among high-risk women. However, there have been few direct, well powered studies comparing cfDNA testing with standard screening during the firstTrimester in routine prenatal population.
Standard prenatal Screening: Serum Biochemical Assays and nuchal translucency measurement
Enrollment 35 international centers Enrollment of 18955 pts, with singleton pregnancy, 10-14 weeks of gestation
Primary Outcome: comparison of cfDNA testing vs standard testing assessed as area under the receiver-operating-characteristic curve (AUC) for trisomy 21
Secondary Outcome: Evaluation of cfDNA testing and standard screening for risk for Trisomy 18 and 13

Norton ME; NEJM 2015 372(17) 1589 Cell-free DNA Analysis for Noninvasive Examination of Trisomy
Primary Outcome for Trisomy 21 Screening-Receiver-operating-characteristic curve (AUC)-
AUC for cfDNA sctreening 0.999AUC for standard screening 0.958 P=0.001
● cfDNA screening identified 38 cases out of 38 cases for Trisomy21-- sensitivity 100% (95% confidence interval (CI), 90.7 to 100
● standard screening identified 30 cases out of 38 cases for Trisomy21-- sensitivity 78.9% (95% CI, 62.7 to 90.4)

15841 were included in analysis
15841 standard screening 15841 cfDNA screening
884 positive result 14957 negative result 15794 with low risk47 with high risk
18955 pts enrolledExclusion Criteria- No singleton pregnancy- Unknown ovum owner status- withdrew or were withdrawn - Smpl handling error- No cf-DNA results- Lost in follow up
● 30 pts had Trisomy 21● 854 pts did not have Trisomy 21
● 8 pts had Trisomy 21● 14949 pts did not have Trisomy21
● 38 pts had Trisomy 21● 9 pts did not have Trisomy21
● 0 pts had Trisomy 21● 15794 did not have Trisomy21
Norton ME; NEJM 2015 372(17) 1589 Cell-free DNA Analysis for Noninvasive Examination of Trisomy
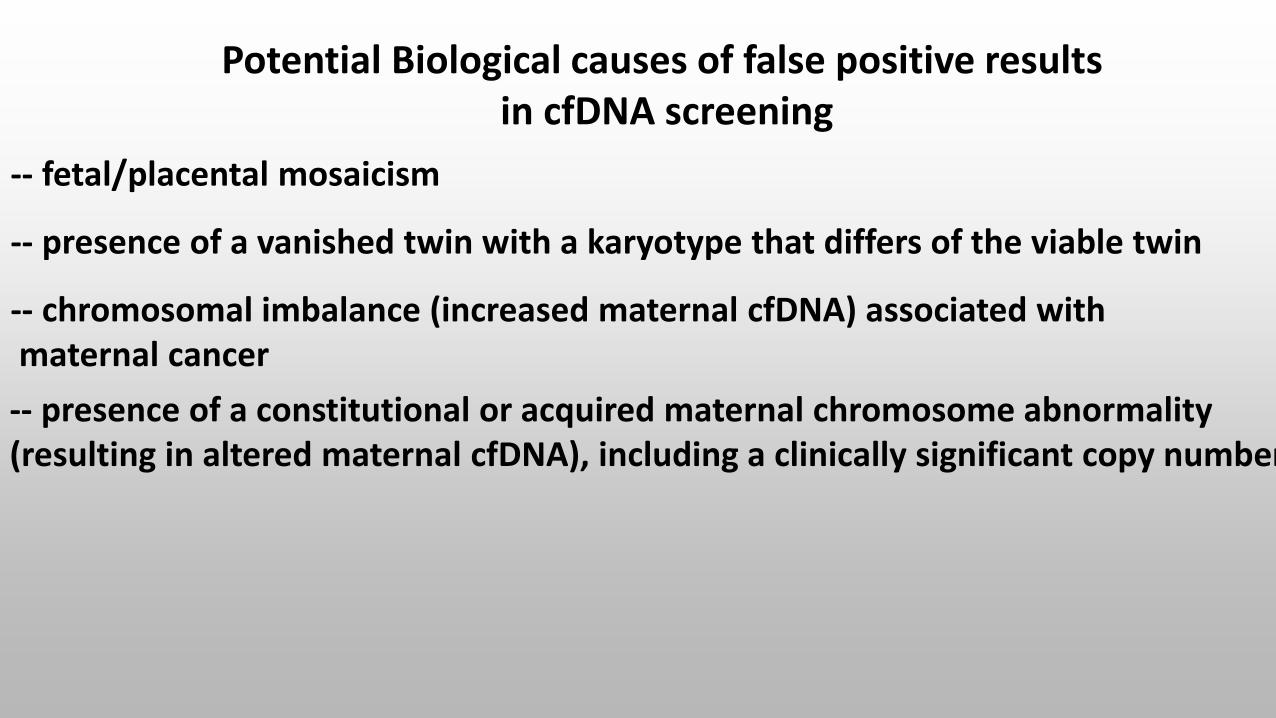
Potential Biological causes of false positive results in cfDNA screening
-- fetal/placental mosaicism
-- presence of a vanished twin with a karyotype that differs of the viable twin
-- chromosomal imbalance (increased maternal cfDNA) associated withmaternal cancer
-- presence of a constitutional or acquired maternal chromosome abnormality (resulting in altered maternal cfDNA), including a clinically significant copy number variation

Overview about available options of massive parallel sequencing (MPS) in Noninvasive Prenatal Testing
SubchromosomalDeletions
duplications
Identifications of single-
gene disorders
Fetal Methylome Fetal Transcriptome
Chromosomalaneuploidy detection
Bisulfite Sequencing
RNA Sequencing
- Example 1- - Example 2-

Overview about available options of massive parallel sequencing (MPS) in Noninvasive Prenatal Testing (cont.)
- Example 1-The NHS RAPID project (Reliable Accurate Prenatal Diagnosis)
Apert SyndromeFGFR3-related skeletal dysplasias: achondroplasia, thanatrophic dysplasiaCystic Fibrosis
- Example 2-Panorama®
●The panel includes the following standard NIPT screening options.Trisomy13, 18, 21, Turner 45X, Klienefelder 47XXY, 47XXX, 47XYY, 48XXYY,
●The panel can be extended for the following opt-in versions1p36, 5p- (cri-du-chat syndrome), 22q11.2 (DiGeorge syndrome or velo-cardio-facial syndrome), 15q11.2 Prader-Willi Angelman Syndrome
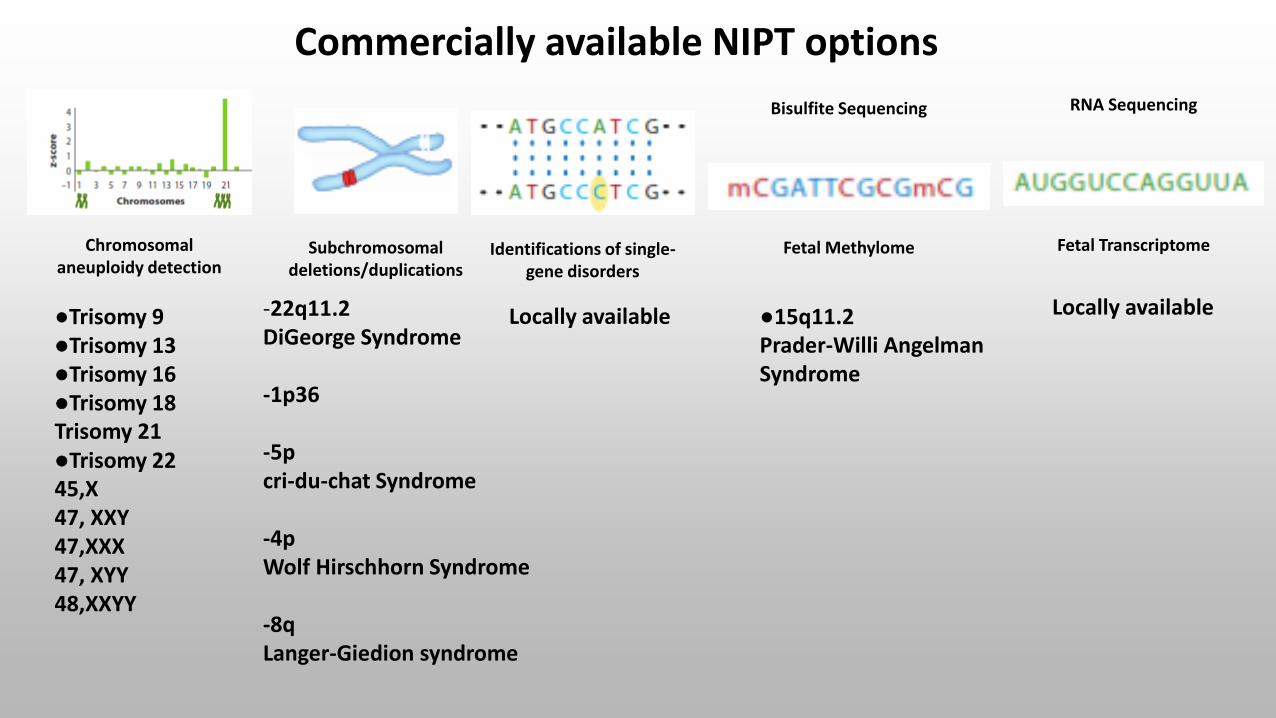
Commercially available NIPT options
Subchromosomaldeletions/duplications
Identifications of single-gene disorders
Fetal Methylome Fetal TranscriptomeChromosomalaneuploidy detection
Bisulfite Sequencing RNA Sequencing
●Trisomy 9●Trisomy 13●Trisomy 16●Trisomy 18Trisomy 21●Trisomy 2245,X47, XXY47,XXX47, XYY48,XXYY
●15q11.2Prader-Willi AngelmanSyndrome
Locally available-22q11.2 DiGeorge Syndrome
-1p36
-5p cri-du-chat Syndrome
-4pWolf Hirschhorn Syndrome
-8qLanger-Giedion syndrome
Locally available

Final Thoughts about NIPT
● Regulation and Test Dissemination● Return of fetal sex information (India China Jurisdiction)
● low genetic literacy may limit informed decision making
● cultural frameworks: Family consent vs infomed consentRender families to fraudulent providers and financial exploitation
● equity to access

THANK YOU