fetoscopy in complicated twin pregnancies in complicated twin pregnancies basky thilaganathan fetal...
TRANSCRIPT

Fetoscopy in Complicated Fetoscopy in Complicated Fetoscopy in Complicated Fetoscopy in Complicated
Twin PregnanciesTwin PregnanciesTwin PregnanciesTwin Pregnancies
Basky ThilaganathanBasky ThilaganathanBasky ThilaganathanBasky Thilaganathan
Fetal Medicine UnitAcademic Department of
Obstetrics and Gynaecology
St.George’s Hospital Medical School
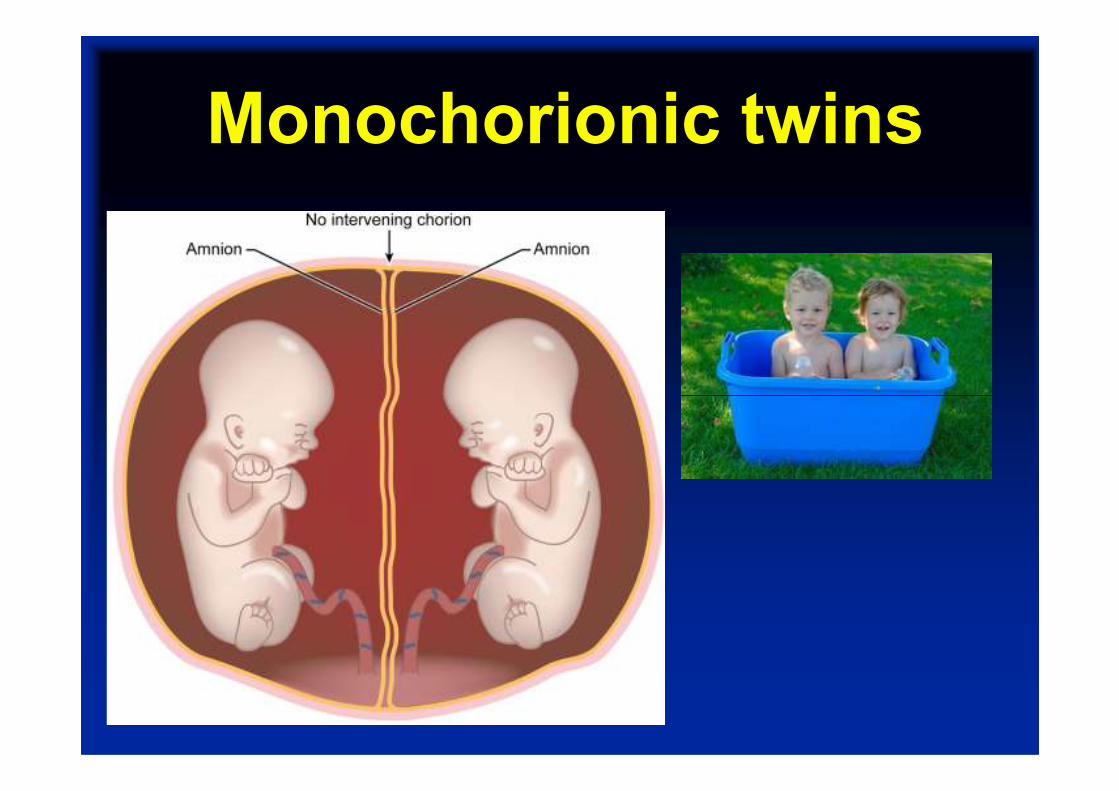
Monochorionic twins

Who needs fetoscopy?
Absolute indications
Stage 3 and 4 TTTS
Relative indicationsRelative indications
Stage 1 and 2 TTTS
Selective IUGR
Acute TTTS
Discordant severe abnormality
TRAP sequence

Complications of MCDA
twins
Size Fluid
TTTS Discrepant Poly-oligo
Acute ITT Same Poly-oligo
Selective IUGR Discrepant Normal-oligo

Selective IUGRSevere IUGR in stuck
(donor) twin
NORMAL co-twin
(no polyhydramnios)
Rarest form of twin
vascular complication
Variable UA Doppler
~30% CP risk with
co-twin death

Acute TTTSPoly-oligohydramnios
NO evidence of
growth discrepancy
Preterm delivery
15% recurrence risk
Abnormal umbilical
Doppler

Twin-Twin
TransfusionTransfusion
Syndrome

Twin-to-twin transfusion

Twin-to-twin transfusion

Operative
techniquetechnique

Operative Fetoscope

Sono-endoscopic technique

Inter-twin membrane

Non-selective Technique

Selective TechniquesVascular equator
Thilaganathan B et al. 2000 Ult Obs Gyn

Laser Sequence

Posterior placenta
Donor North
Recipient South
Arteries dark
Laser Sequence
Two A-V connections
Maternal movement
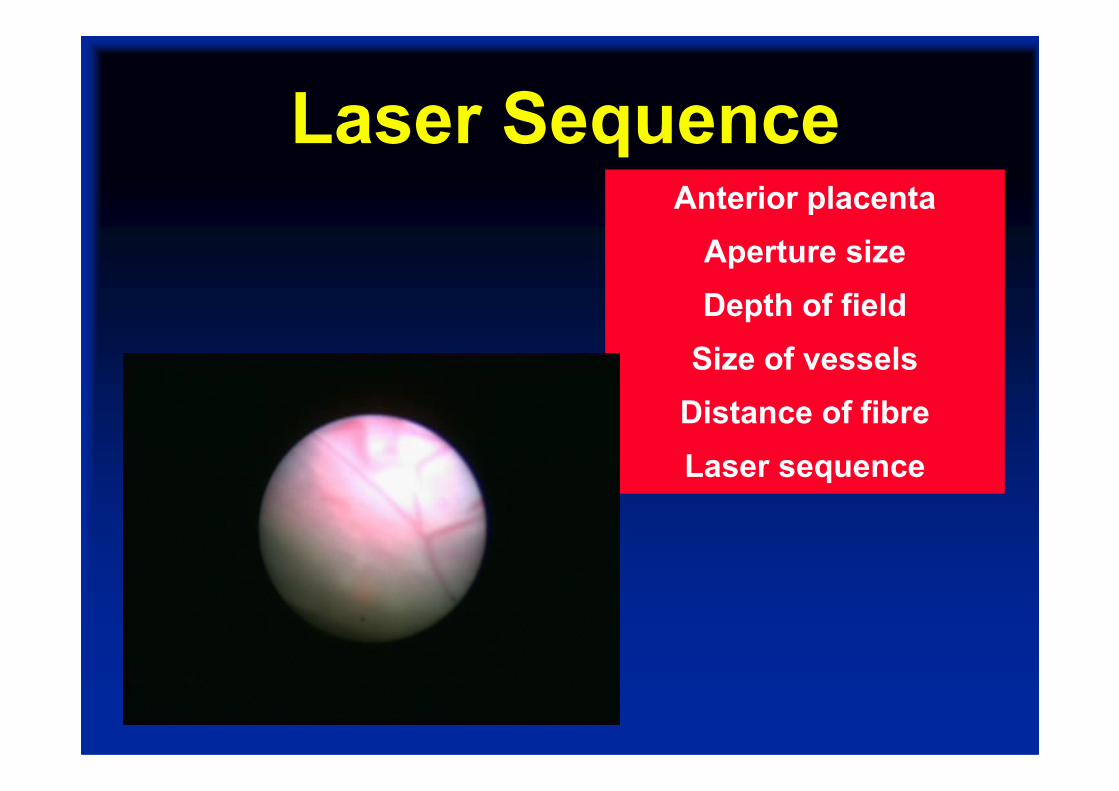
Anterior placenta
Aperture size
Depth of field
Size of vessels
Distance of fibre
Laser Sequence
Distance of fibre
Laser sequence

Results
70%
75%
80%
Non selective
Senat et al
n=35
Selective
Quintero et al
n=74
Equatorial
n=77Non selective 30-90 minutesVille et al 1995 NEJM
Selective median 73 min (range 20-178 min)Quintero et al 2000 Ultrasound OG
Equatorial median 15 min (range 5-25 min)
Survival n
No. of
pregnancies
% of total
pregnancies
0 survivors 20 26%
At least one survivor 57 74%
One survivor 26 34%
Two survivors 31 40%
77 monochorionic twin pregnancies
All severe TTTS at Quintero
stage III (n=68) or IV (n=9)
60%
65%
Ierullo A et al. BrJOG. 2007;114:689-93

Post-operative AssessmentUltrasound and Doppler
assessments at 6hrs
2 weeks and 6 weeks
2 cases of fetal
anaemia post-laser
1 repeat procedure

TRAP
SyndromeSyndrome

TRAP syndromeTwin Reversed Arterial
Perfusion Syndrome
1% of MC pregnancies
1:35,000 births
Acardiac/acephalic mass
Pump twin
Close cord insertions
2-vessel cord
Retrograde blood flow
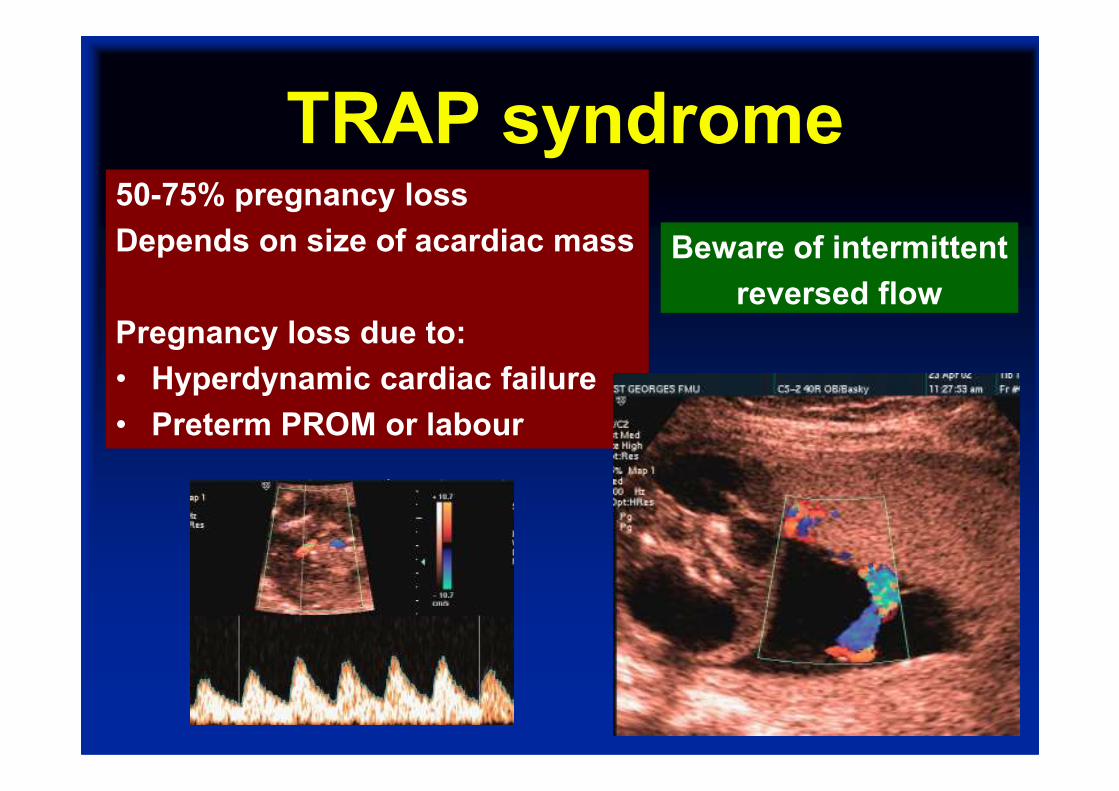
TRAP syndrome50-75% pregnancy loss
Depends on size of acardiac mass
Pregnancy loss due to:
• Hyperdynamic cardiac failure
Beware of intermittent
reversed flow
• Hyperdynamic cardiac failure
• Preterm PROM or labour

TRAP syndromeFetoscopic laser ablation
80% survival rate
Hecher K et al. Ult Obstet Gynecol
2006;28:688-91

TRAP syndromeCord occlusion of 51
patients with 65% survival
Quintero RA et al.
AmJOG 2006;194:982-91
Intrafetal techniques have:
Later gestation at delivery
Lower PROM rates
Fewer technical failures
Tan and Sepulveda
Ult Obstet Gynecol 2003;22:409-19

TRAP syndrome
Radiofrequency ablation of
29 patients with 86% survival
Lee H et al.
AmJOG 2007;196:459AmJOG 2007;196:459
First trimester ultrasound-
guided interstitial laser
All 11 cases survived
St Georges unpublished
