fibromyalgia educational awareness
TRANSCRIPT
1/8/2019
1
z
Fibromyalgia Educational Awareness
z
Course description
This program is designed to explore the assessment required in
the diagnosis of fibromyalgia. The program also emphasizes an
overview of possible pathophysiology, treatment modalities and
management.
CEU: 1 hour
z
Learning objectives
Demonstrate the complexity of fibromyalgia in patients
Identify therapeutic pharmacological agents used in the
management of fibromyalgia
Recognize non-pharmacological treatment for fibromyalgia pain
management
z
Demonstrate the complexity of fibromyalgia in patients
Describe fibromyalgia as a clinical condition and its social
impact.
Differentiate fibromyalgia symptoms from other similar
symptoms by applying the American College of Rheumatology
diagnostic criteria.
Identify possible pathophysiology related to fibromyalgia.
z
Identify therapeutic pharmacological agents used in the management of fibromyalgia
Recognize the pharmacological choices in the management of
fibromyalgia.
z
Recognize non-pharmacological treatment for fibromyalgia pain management
Identify the role of proper nutrition, cognitive behavioral therapy,
relaxation techniques, exercise in the management of
fibromyalgia and other non-pharmacological treatments.

1/8/2019
2
z
Program Outcomes
Upon successful completion of the course, the participants will
be able to:
Identify assessment criteria to use in the diagnosis of fibromyalgia.
Apply pharmacological and non-pharmacological treatment options
in the management of fibromyalgia.
z
Learning Assessment:
One case study and 14 questions total (4 throughout the content
and 10 at the end of the course).
z
Case study
Maria, Age 35
C/O pain
Difficult to get out of bed in am
Does not feel like eating
Does not want to move
Staying in bed for hours
z
Case study continued
Tired all the time
Husband states that she cries, looks sad, cannot work due to
pain
Missing 2 out of 5 days of work
Physician not understanding, suggested acetaminophen
z
Case study continued
Referred to many different providers
Diagnosed with fibromyalgia after 2 years
Specific diagnostic tests not available to diagnose fibromyalgia
z
Complexity of fibromyalgia in patients
Choy and colleagues as discussed by Arnold (2012) found that
patients reported
2.3 years and 3.7 physicians
NMC faculty study
Evaluated nurse practitioners’ education and awareness

1/8/2019
3
z
Complexity of fibromyalgia in patients
NMC faculty study (Hughes, Adair, Feng, Maciejewski, &
Sharma, 2016).
95% of Nurse Practitioners reported difficulty diagnosing
68% were worried about labeling patients
62% aware of American College of Rheumatology criteria
76% spent time on self-education
55% wanted more education
z
Complexity of fibromyalgia in patients
Women 9x more likely to develop fibromyalgia than men
(Lawrence et al., 1998).
The mean number of physician office visits higher among
fibromyalgia patients
Patients in poorer health and had greater levels of healthcare
utilization (Robinson et al., 2003; Goldenberg, Burckhardt &
Crofford, 2004).
z
Complexity of fibromyalgia in patients
Disorder seen in families, with symptoms being displayed by
children as well as adults (National Fibromyalgia Association,
2009).
Over 5% are affected with symptoms generally appearing
between the ages of 20 and 55 years of age with a tendency to
increase with age (Berger, Dukes, Martin, Edelsber, & Oster,
2007).
May be 3-6 million American adults suffering with this condition.
z
Complexity of fibromyalgia in patients
Fibromyalgia is the third most prevalent rheumatologic disorder
in the United States (Baumstark and Buckelew, 2002)
Fibromyalgia is a common chronic widespread pain disorder that
has a worldwide prevalence between 0.55 and 5%. (Arnold,
2012),
z
History and Symptoms of Fibromyalgia
1700’s, physicians in Germany and Scandinavia were finding a
condition with pain in muscles and soft tissue.
1904, Sir William Gowers named the disorder, fibrocitis
1943, Slocumb examined connective tissue nodules and found
normal tissue without inflammation.
1981, Yunas et al. coined the condition, fibromyalgia, which
indicates the presence of pain but not necessarily, inflammation.
z
History and Symptoms of Fibromyalgia
Some physicians may not recognize fibromyalgia as a real
medical condition.
Diagnosis is based on patient history, physical examination and
the exclusion of symptoms of other conditions (Wierwille, 2012).
2001).
1/8/2019
4
z
History and Symptoms of Fibromyalgia
The majority of patients have symptoms of
chronic fatigue,
widespread musculoskeletal pain,
poor sleep,
morning stiffness
mood disorders such as anxiety or depression
(Park, Glass, Minear & Crofford, 2001).
Some experience “fibromyalgia fog”
z
History and Symptoms of Fibromyalgia
Hughes (2002) study of 107 fibromyalgia patients described pain
as aching, throbbing, sharp, tender, burning, gnawing, shooting,
and pulling.
The participants thought that the pain was exhausting,
sickening, wretched, and caused them to be fearful.
Participants were recorded as having up to 26 awakenings
during the course of one night’s sleep.
z
History and Symptoms of Fibromyalgia
Symptoms can appear and disappear along with the degree and
severity of pain.
Many patients feel hopeless.
Fibromyalgia patients may look healthy and move around with
no noted difficulty.
z
American College of Rheumatology Criteria used for Diagnosis
Definition of fibromyalgia is a medical condition based on the
following criteria:
At least 3 months of widespread pain
Pain occurs in all four quadrants of the body with moderate pain
sensitivity in specific tender points.
The pain should occur on digital examination (4 kg. of pressure) in
at least 11 out of 18 specified tender point sites (Wolfe et al., 1990).
z
American College of Rheumatology Criteria used for Diagnosis
1990 ACA Criteria for Fibromyalgia Main Points
1. “History of widespread pain”
left side of the body,
right side of the body,
above the waist,
below the waist.
axial skeletal pain must be present.
z
American College of Rheumatology Criteria used for Diagnosis
1990 ACA Criteria for Fibromyalgia Main Points
2. Pain in 11 of 18 tender points sites, on digital palpation.

1/8/2019
5
z
American College of Rheumatology Criteria used for Diagnosis
Tender points sites
Occiput
Low cervical
Trapezius
Supraspinatus
z
American College of Rheumatology Criteria used for Diagnosis
Tender points sites
Second rib
Lateral epicondyle
Gluteal
Greater trochanter
Knee
z
American College of Rheumatology Criteria used for Diagnosis
Digital palpation
approximate force of 4 kg for a tender point to be considered
“positive”
The subject must state that the palpation was painful. “Tender” is
not to be considered “Painful” (Wolfe et al., 1990).
z
American College of Rheumatology Criteria used for Diagnosis
Objections
The restrictiveness of the tenderpoint count was not performed at
the Primary Care Providers office
The accuracy of the tenderpoint assessment was not consistent.
Philosophically, other important patient symptoms that interfered
with a quality of life occurred, that included fatigue, cognitive
symptoms and the extent of other somatic symptoms,
(Wolfe, Clauw, Fitzcharles, Goldenbert, Katz, Mease, Russell, . . .
Yunas, 2010).
z
American College of Rheumatology Criteria used for Diagnosis
In 2010, the ACR changed the diagnostic criteria to include:
assessment of pain and symptoms over a period of a week.
symptoms lasting over three months.
ruling out any other health problem that would present the same
pain and symptomology.
z
2010 ACR Criteria for Fibromyalgia Main Points
A patient satisfies diagnostic criteria for fibromyalgia if the
following 3 conditions are met.
1. Widespread Pain Index (WPI) > 7 and Symptom Severity (SS)
scale score > 5 or WPI 3-6 and SS scale score > 9.
2. Symptoms have been present at a similar level for at least 3
months.
3. The patient does not have a disorder that would otherwise explain
the pain.

1/8/2019
6
z
2010 ACR Criteria for Fibromyalgia Main Points
Shoulder girdle
Upper arm
Lower arm
Hip (buttock, trochanter)
Upper leg
Lower leg
Jaw
Chest
Abdomen
Upper back
Lower back
Neck
z
2010 ACR Criteria for Fibromyalgia Main Points
The SS scale score includes:
1. Fatigue
2. Waking unrefreshed
3. Cognitive symptoms
z
2010 ACR Criteria for Fibromyalgia Main Points
Indicate the level of severity over the past week using the
following scale:
1. no symptoms
2. few symptoms
3. a moderate number of symptoms
4. a great deal of symptoms
( Wolfe et al., 2010)
z
2010 ACR Criteria for Fibromyalgia Main Points
The 2010 criteria will probably be utilized to a greater
extent.
Refer to Fibromyalgia Network | www.fmnetnews.com
| (800) 853-2929 for more details about the 2010
criteria.
z
Test your knowledge
1. In 2010, the American College of Rheumatology (ACR)
identified that the pain must occur on digital exam in 11 out of
18 body parts to be considered the pain of fibromyalgia.
True or False
z
Test your knowledge
1. In 2010, the American College of Rheumatology (ACR)
identified that the pain must occur on digital exam in 11 out of
18 body parts to be considered the pain of fibromyalgia.
True or False
1/8/2019
7
z
Test your knowledge
1. In 2010, the American College of Rheumatology (ACR)
identified that the pain must occur on digital exam in 11 out of
18 body parts to be considered the pain of fibromyalgia.
True or False
Rationale: This is from the 1990, American College of
Rheumatology Diagnosis Criteria
z
Test your knowledge
2. Symptom severity (SS) score consists of the severity of pain,
decreased mobility, and cognitive symptoms.
True or False
z
Test your knowledge
2. Symptom severity (SS) score consists of the severity of pain,
decreased mobility, and cognitive symptoms.
True or False
z
Test your knowledge
2. Symptom severity (SS) score consists of the severity of pain,
decreased mobility, and cognitive symptoms.
True or False
Rationale: Incorrect symptoms are listed; it should list the following
symptoms –severity of fatigue, unrefreshed sleep and cognitive
symptoms.
z
Possible Pathophysiology of Fibromyalgia
Cause unknown
Several theories have been proposed.
Genetic predisposition with family members over several
generations being diagnosed with the condition.
First degree relatives more likely to develop fibromyalgia
(Arnold, Hudson and Hess, 2004).
Traumatic events, infection, and psychological stress
z
Possible Pathophysiology of Fibromyalgia
Clauw and Crofford (2003), suspect abnormalities in the
hypothalamic-pituitary-adrenal axis.
The concept of sensory hypersensitivity or central sensitization
has been studied resulting in increased muscle sensitivity by a
normally non-painful stimulus, and increased pain intensity
triggered by normally painful stimuli (Staud & Smitherman 2002;
Arendt-Nielsen & Graven-Nielsen, 2003).
1/8/2019
8
z
Possible Pathophysiology of Fibromyalgia
Patients have demonstrated a deficiency in the production of
cortisol.
Serotonin levels have been lower than normal.
Many have an increased level of Substance P and glutamate
accounts for an increased awareness of pain and nerve sensitivity
Increases in glutamate concentrations in specific brain regions
have been noted (Harris, Sundgren, Craig et al., 2009; Valdes,
Collado & Bargallo, 2010).
z
Possible Pathophysiology of Fibromyalgia
The functional changes and pathological mechanisms behind the
fibromyalgia chronic pain may include:
1. “central nervous system (CNS) sensitization,
2. dysfunction of the descending inhibitory pain pathways,
3. peripheral nervous system (PNS) sensitizations,
4. release of inflammatory mediators,
5. endocrine irregularity in the hypothalamic-pituitary-adrenal (HPA) axis,
and
6. neurotransmitter abnormalities”,
(Wierwille, 2012, p. 185).
z
Possible Pathophysiology of Fibromyalgia
Wierville cited evidence of demyelination of neurons and
inflammation of peripheral nerve fibers in skin biopsies from the
tender points of fibromyalgia patients which could result from
chronic stress and HPA axis dysfunction.
z
Specific steps of diagnosis and treatment of Fibromyalgia for the Healthcare Provider
According to Goldenberg, Burckhardt and Crofford (2004) found
in the article by Marter and Agruss (2008), possible steps in the
diagnosis and treatment of fibromyalgia could be the following:
z
Specific steps of diagnosis and treatment of Fibromyalgia for the Healthcare Provider
Step One
Obtain a history using the 2010 ACR Criteria.
Perform a physical examination.
Consider such diagnostic tests as Complete Blood Count,
Complete Metabolic Panel, Thyroid Stimulating Hormone, and
Erythrocyte Sedimentation Rate.
z
Specific steps of diagnosis and treatment of Fibromyalgia for the Healthcare Provider
Step Two
Provide patient education about their condition.
Assess and treat comorbid conditions that impact fibromyalgia
such as depression, anxiety, and sleep disorders.
Administer the Revised Fibromyalgia Impact Questionnaire (FIQR)
to evaluate current status.

1/8/2019
9
z
Specific steps of diagnosis and treatment of Fibromyalgia for the Healthcare Provider
Step Three
Begin pharmacologic treatment trial with pregabalin (Lyrica),
amitriptyline (Elavil), or cyclobenzaprine (Flexeril).
Begin non-pharmacologic treatment such an aerobic exercise
program, including pool-based work for deconditioned patients.
Try a multidisciplinary approach with referral for cognitive behavior
therapy.
Schedule follow-up appointments with the primary care provider
every 4-6 weeks, with re-evaluation with the FIQR.
z
Specific steps of diagnosis and treatment of Fibromyalgia for the Healthcare Provider
Step Four
If minimal or no improvement:
Consider referral to a rheumatology, pain management, or other
specialists as indicated.
Consider alternate pharmacologic treatment with selective
serotonin reuptake inhibitors (SSRI), or use of combination
serotonin and norepinephrine reuptake inhibitors, or use of
tramadol (Ultram) with acetaminophen.
Consider use of two or more pharmacologic options in
combination.
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
Revised Fibromyalgia Impact Questionnaire.
Originally, the FIQ used a visual analog scale that required the
practitioner to measure the patient response.
One question also required reverse scoring and the use of constants to convert the first 13 questions to a standardized scale
of 0 to 10.
Questions in the FIQ directed to patient function assumed that the
patient possessed a car, vacuum cleaner and a washing machine.
There were no questions directed to problems with cognition,
tenderness, balance and sensitivity to the environment.
(Bennett et al., 2009).
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
The FIQR was developed to ease the scoring, address the
limitations stated previously, and promote more widespread
clinical use.
21 individual questions based on an 11-point numeric rating
scale from 0 to 10 with 0 being the best and 10 being the worst.
The tool is framed in the context of the past 7 days in the life of
the fibromyalgia patient.
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
Divided into three sets of domains:
function with 9 questions ranging from brushing/combing hair to
shopping for groceries,
overall impact of fibromyalgia with two questions related to
accomplishment of weekly goals
impact of symptom severity, and rating of symptoms experienced
by the patient.
(Bennett et al., 2009)
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
The scoring consists of a summed score for the function (0-90
divided by 3)
the summed score for overall impact (0-20)
summed score for symptoms (0-100 divided by 2).
The total FIQR is the sum of the three modified domain scores.
The maximal score of the FIQR is 100
(Bennett et al., 2009).

1/8/2019
10
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
In the psychometric testing of the FIQR,
the total scores of the FIQR and FIQ were closely correlated (r =
0.88, P < 0.01).
The FIQR also demonstrated good correlation with comparable
instrument domains in the SF-36.
The tool had good discriminant ability between fibromyalgia
patients and healthy controls, rheumatoid arthritis, systemic lupus
erythematosus, and major depressive disorder patients
(Bennett et al. 2009)
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
The FIQR is available in paper and electronic form.
It takes 2 minutes to complete.
The authors of the instrument have published a document with
the interpretation of the FIQR results with the following scale
related to the scoring:
mild fibromyalgia (0-42),
moderate fibromyalgia (43-59),
severe fibromyalgia (60-74),
extreme fibromyalgia (75-100).
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
There is a user agreement that needs to be completed
requesting the following information:
licensee details of name etc.,
context of use,
project financing,
language translations needed
listing of the details of the user agreement.
z
Revised Fibromyalgia Impact Questionnaire (FIQR)
There is no fee for use of this tool unless the licensee is involved
with a “for profit” organization.
For further information on the use of the FIQR, the
corresponding author is Robert M. Bennett at
[email protected] at the Fibromyalgia research Unit,
Oregon Health and Science University, 3455 SW Veterans
Road, Portland Oregon 97239.
z
RevisedFibromyalgiaImpact Questionnaire (FIQR)
(Bennett et al. 2009)
z
Pharmacology in the treatment for Fibromyalgia
European League Against Rheumatism (EULAR)
Pharmacological
Non-pharmacological

1/8/2019
11
z
Pharmacology in the treatment for Fibromyalgia
Pharmacological
tramadol (Ultram)
weak opioids
Amitriptyline (Elavil)
Tropisetron (Navoban)
Pramipexole (Mirapex)
Pregabalin (Lyrica)
(Carville et al., 2008).
z
Pharmacology in the treatment for Fibromyalgia
Pharmacological
Pregabalin (Lyrica) – 450 mg/day
Amitriptyline (Elavil) – as well as duloxetine (Cymbalta) and
milnacipran (Savella)
Gabapentin (Neurontin)
Cyclobenzaprine (Flexeril)
Not recommended: Zolpidem (Ambien) or benzodiazepine
medications
z
Pharmacology in the treatment for Fibromyalgia
Also Not recommended:
Corticosteroids
Strong Opioids
NSAIDS
z
Pharmacology in the treatment for Fibromyalgia
High Benefit:
Duloxetine (Cymbalta)
Alprazolam (Xanax), lorazepam (Ativan), and clonazepam
(Klonopin)
Pregabalin (Lyrica)
Tizanidine (Zanaflex) and carisoprodol (Soma)
Modafinil (Provigil)
Tramadol hydrochloride (Ultram)
z
Non-Pharmacologic treatments for Fibromyalgia
EULAR recommended the following non-pharmacologic
approaches:
Heated pool therapy
Exercise programs
Cognitive behavioral therapy
Relaxation and psychological support
Education about the syndrome
Eat proper nutrition to manage weight
Moderate exercise and stress-relieving techniques
z
Non-Pharmacologic treatments for Fibromyalgia
The American College of Rheumatology self-care tips:
Making time to relax each day,
Set a sleep routine and exercise often
“start low, go slow”
1/8/2019
12
z
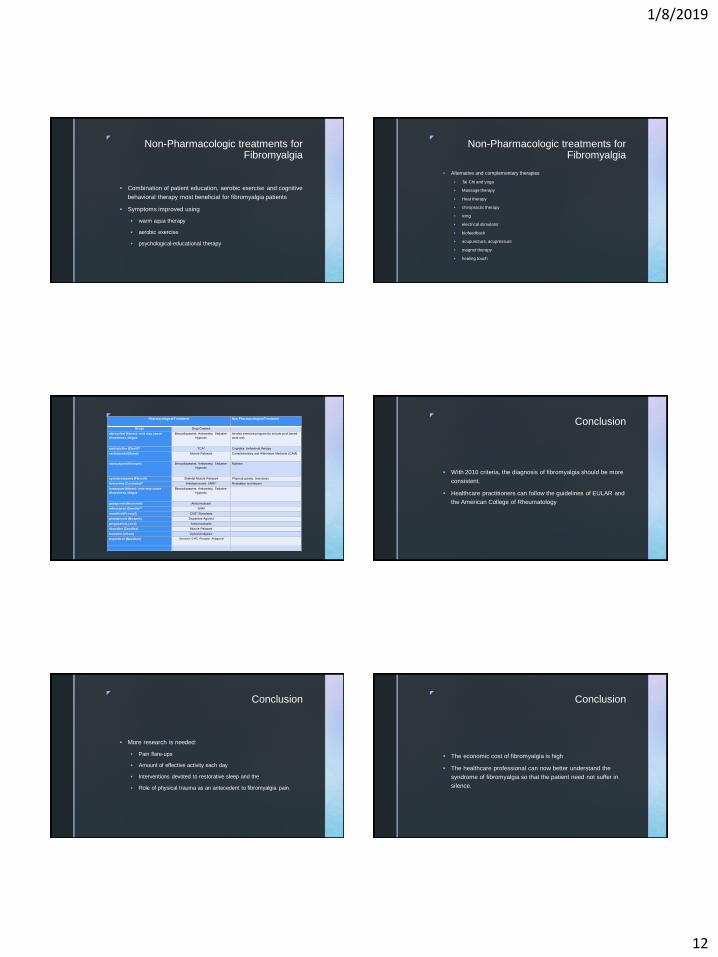
Non-Pharmacologic treatments for Fibromyalgia
Combination of patient education, aerobic exercise and cognitive
behavioral therapy most beneficial for fibromyalgia patients
Symptoms improved using
warm aqua therapy
aerobic exercise
psychological-educational therapy
z
Non-Pharmacologic treatments for Fibromyalgia
Alternative and complementary therapies
Tai Chi and yoga
Massage therapy
Heat therapy
chiropractic therapy
icing
electrical stimulator
biofeedback
acupuncture, acupressure
magnet therapy
healing touch
zPharmacological Treatment Non Pharmacological Treatment
Drugs Drug Classes
alprazolam (Xanax)- note may cause
drowsiness, fatigue
Benzodiazepine, Antianxiety, Sedative-
Hypnotic
Aerobic exercise program (to include pool based
work out)
amitriptyline (Elavil)** TCA* Cognitive behavioral therapy
carisoprodal (Soma) Muscle Relaxant Complementary and Alternative Medicine (CAM)
clonazepam (Klonipin) Benzodiazepine, Antianxiety, Sedative-
Hypnotic
Nutrition
cyclobenzaprine (Flexeril) Skeletal Muscle Relaxant Physical activity (exercise)
duloxetine (Cymbalta)** Antidepressant, SNRI* Relaxation techniques
lorazepam (Ativan)- note may cause
drowsiness, fatigue
Benzodiazepine, Antianxiety, Sedative-
Hypnotic
gabapentin (Neurontin) Anticonvulsant
milnacipran (Savella)** SNRI
modafinil (Provigil) CNS* Stimulants
pramipexole (Mirapex) Dopamine Agonist
pregabalin (Lyrica) Anticonvulsants
tizanidine (Zanaflex) Muscle Relaxant
tramadol (Ultram) Opioid Analgesic
tropisetron (Navoban) Serotonin 5-HT₃ Receptor Antagonist
z
Conclusion
With 2010 criteria, the diagnosis of fibromyalgia should be more
consistent.
Healthcare practitioners can follow the guidelines of EULAR and
the American College of Rheumatology
z
Conclusion
More research is needed:
Pain flare-ups
Amount of effective activity each day
Interventions devoted to restorative sleep and the
Role of physical trauma as an antecedent to fibromyalgia pain.
z
Conclusion
The economic cost of fibromyalgia is high
The healthcare professional can now better understand the
syndrome of fibromyalgia so that the patient need not suffer in
silence.
1/8/2019
13
z
References
Argoff, C. (2011). Mechanisms of pain transmission and pharmacologic management. Current Medical Research and
Opinion, 27(10), 2019-2031.
Arendt-Nielsen, L., & Graven-Nielsen, T. (2003). Central sensitization in fibromyalgia and other musculoskeletal disorders.
Current Pain and Headache Reports, 7(5), 355-361.
Arnold, L., Clauw, D., Dunegan, J., & Turk, D. (2012). A framework for fibromyalgia management for primary care
providers. Mayo Clinical Proceeding, 87(5), 488-496.
Baumstark, K. E., & Buckelew, S. P. (2002). Fibromyalgia: Clinical signs, research findings, treatment implications, and
future directions. Annals of Behavioral Medicine, 14, 282–291.doi:10.1016/j.mayocp.2012.02.010.
Bennett, R., Friend, R., Jones, K., Ward, R., Han, B., & Ross, R. (2009). The revised fibromyalgia impact questionnaire
(FIQR): validation and psychometric properties. Arthritis research & Therapy, 11(5), 415. doi: 10.1186/ar2783.
Berger, A., Dukes, E., Martin, S., Edelsberg, J., & Oster, G. (2007). Characteristics and health care cost of patients with
fibromyalgia syndrome. Internal Journal of Clinical Practice, 61(9), 1498-1508.
Busch, A., Schachter, C., Overend, T., Peloso, P., & Barber, K. (2008). Exercise for fibromyalgia : a systematic review.
Journal of Rheumatology, 35(6), 1130-1144
z
References
Carbonell-Baeza, A., Aparicio, V., Chillon, P., Femia, P., Delgado-Fernandez, M., & Ruiz, J. (2011). Effectiveness of
multidisciplinary therapy on symptomatology and quality of life in women with fibromyalgia. Clinical Experimental
Rheumatology, 29(6), S97-103.
Carvill, S., Arendt-Nielsen, S., Bliddal, H., Blotman, F., Branco, J., Buskila, D., . . . Choy, E. (2008). EULAR evidence-based
recommendations for the management of fibromyalgia syndrome. Annals of Rheumatology Disease, 67, 536-541.
Clauw, D. J., & Crofford, L. J. (2003). Chronic widespread pain and fibromyalgia: What we know, and what we need to
know. Best Practice & Research Clinical Rheumatology, 17, 685–701.
Crofford, L. (2013).Fibromyalgia. American College of Rheumatology. Retrieved from
http://www.rheumatology.org/Practic/Clinical/Patients/Diseases_And_Conditions/Fibromyagia.Fibromyalgia Network.
(2006). Retrieved from http://fmnetnews.iraherman.com.
Goldenberg, D., Burckhardt, C., & Crofford, L. (2004). Management of fibromyalgia syndrome. JAMA, 292(19), 2393.
Harris, R., Sundgren, P., Craig, A., Kirshenbaum, E., Sen, A., Napadow, V., & Clauw, D. (2009). Elevated insular glutamate
(Glu) in Fibromyalgia (FM) is associated with experimental pain. Arthritis and Rheumatology, 60 (10), 3146-3154.
Hauser, W., Wolfe, F., Tolle, T., Uceyler, N., & Sommer, C. (2012). The role of antidepressants in the management of
fibromyalgia syndrome. CNS Drugs, 26 (4), 297-307.
z
References
Hughes, L. (2002). Sociocultural, physiologic, and psychologic variables that influence pain in the fibromyalgia patient.
Unpublished dissertation, University of Nebraska Medical Center.
Hughes, L., Adair, J. Feng, F., Maciejewski, S. & Sharma, H. (2016). Nurse practitioners’ education, awareness, and
therapeutic approaches for the management of fibromyalgia. Othropaedic Nursing, 35(5), 317-322.
Lawrence, R., Helmick, C., Arnett, F., Deyo, R., Felson, D., Giannini, E., … Wolfe, F. (1998). Estimates of the prevalence of
arthritis and selected musculoskeletal disorders in the United States. Arthritis and Rheumatism, 41(5), 778-799. doi:
10.1002/art.23176.
Marter, A. & Agruss, J. (2008). Solving the riddle of fibromyalgia: An evidence-based practice protocol for the advanced
practice nurse. The Journal for Nurse Practitioners, 424-437.
National Fribromyalgia Association. (2009). Fibromyalgia fact sheet {online}.Retrieved from
http://www.Fmaware.org/prevalence.html.
Park, D. Glass, J.,, Minear, M.,& Crofford, L. (2001). Cognitive function in fibromyalgia patients. Arthritis and Rheumatology,
44(9):2125-33.
Robinson, R., Birnbaum, H., Morley, M., Sisitsky, T., Geenberg, P. & Claxton, A. (2003). Economic cost and
epidemiological characteristics of patients with fibromyalgia claims. Journal of Rheumatology, 30 (6), 1318-1325.
z
References
Staud, R. & Smitherman, M. (2002). Peripheral and central sensitization in fibromyalgia; Pathogenetic role. Current Pain
and Headache Reports, 6(4), 259-266.
Tzellos, T., Toulis, K., goulis, D., Papazisis, G., Zampeli, V., & Vakfari, A. (2010). Gabapentin and pregabalin in the
treatment of fibromyalgia: a systematic review and a meta-analysis. Journal of Clinical Pharmacy and Therapeutics, 35,
639-656.
Valdes, M., Collado, A., Bargallo, N., Vazquez, M., Rami, L., Gomez, E., & Salamero, M. (2010). Increased
glutamate/glutamine compounds in the brains of patients with fibromyalgia: a magnetic resonance spectroscopy study.
Arthritis and Rheumaticism, 62 (6), 1829-1836.
Wierwille, L. (2012). Fibromyalgia: Diagnosing and managing a complex syndrome. Journal of American Academy of Nurse
Practitioner, 24(4):184-92. doi: 10.1111/j.1745-7599.2011.00671.
Wolfe, F., Clauw, D., Fitzcharles, M., Golderberg, D., Katz, R., Mease, P., . . . Yunas, M. (2010). The American College of
Rheumatolgoy preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care
Research, 62(5), 600-610.
Wolfe, F., Smythe, H., Yunas, M., Bennett, R., Bombardier, C., Goldenberg, D., . . . . Sheon, R. (1990). The American
College of Rheumatology 10990 criteria for the classification of fibromyalgia: Report of the multicenter criteria committee.
Arthritis and Rheumatology, 33(2), 160-172.
Yunas, M., Masi, A., Calabro, J., Miller, K., & Feibenbaum, S. (1981). Primary fibromyalgia (fibrocitis): Clinical study of 50
patients with matched normal controls. Seminars in Arthritis and Rheumaticsm, 11, 151-171.