fibromyalgia research: from neurasthenia to central processing abnormalities laurence a. bradley,...
TRANSCRIPT

Fibromyalgia Research: From Neurasthenia to
Central Processing Abnormalities
Laurence A. Bradley, PhDDivision of Clinical Immunology and Rheumatology
University of Alabama at Birmingham
Introduction
Fibromyalgia is characterized by several symptoms: Widespread pain Abnormal pain sensitivity evoked by
diverse stimuli Headache Fatigue Sleep disturbance

Introduction
Fibromyalgia symptoms are associated with several behavioral disturbances: Reduced activity, social interaction, function Avoidance of events that evoke pain Affective distress Increased usage of health services

Introduction
Abnormalities in pain sensitivity, functional ability, and affect, in the absence of biological markers led to different research and clinical pathways: Search for single source of symptoms Attribution of symptoms to psychiatric
illness

Diagnostic Labels For Fibromyalgia Syndrome
DaCosta Syndrome/Shell Shock (brain) Neurasthenia (nerves) Chronic Brucellosis (viral) Failure to Cope (psychological) Fibrositis (muscle inflammation) Affective Spectrum Disorder (depressive
disorder) Fibromyalgia

Theoretical and Empirical Contributions To Fibromyalgia Research and Clinical
Care
Gate control theory (1965)
Psychosocial factors influence health care seeking behavior (1988)
Identification of altered biological factors associated with pain, distress, and related symptoms in fibromyalgia (1992)

Gate Control Theory
Multiple biological and psychosocial factors influence pain perception and pain behavior
It is no longer appropriate to identify pain and related symptoms as “organic” or “functional”

Pain Perception
Pain Behavior
Neuromatrix
Psychosocial andHealth Status
FactorsAttention
Central NervousSystem Plasticity
PathologicInput
MedullaryDescending
Inhibition
Endocrine, Immune,and AutonomicSystem Activity
AfferentInput
0
2
4
6
8
FM patients DepressedSubjects
Healthycontrols
kg/
1.54
cm
2
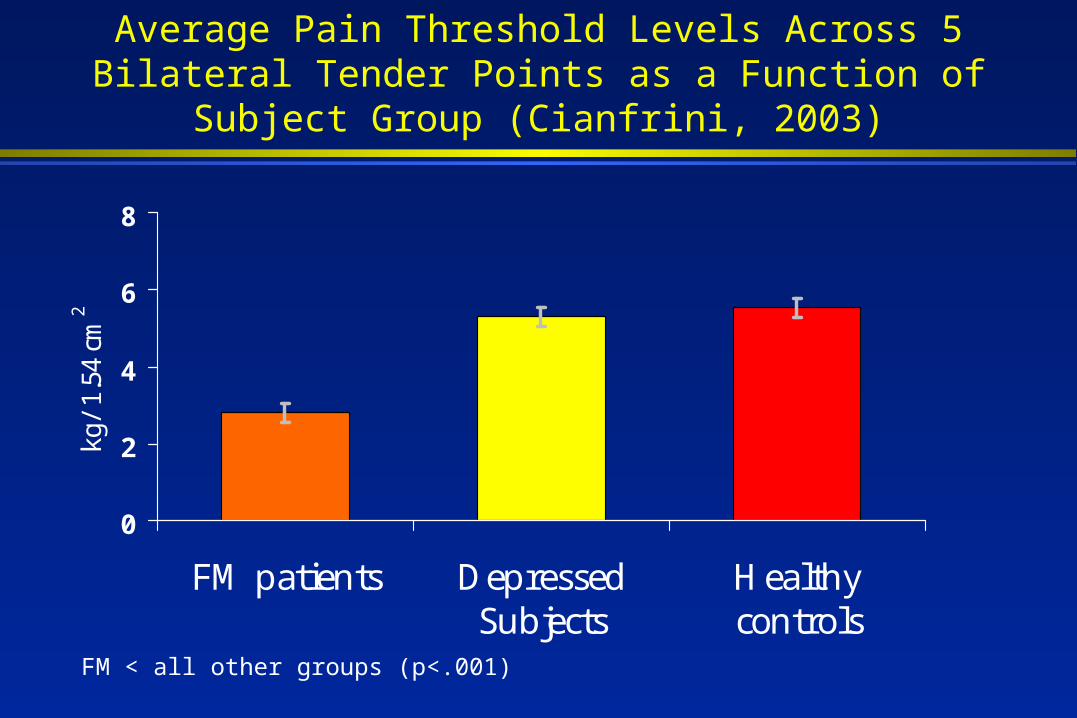
Average Pain Threshold Levels Across 5 Bilateral Tender Points as a Function of Subject Group (Cianfrini,
2003)
FM < all other groups (p<.001)
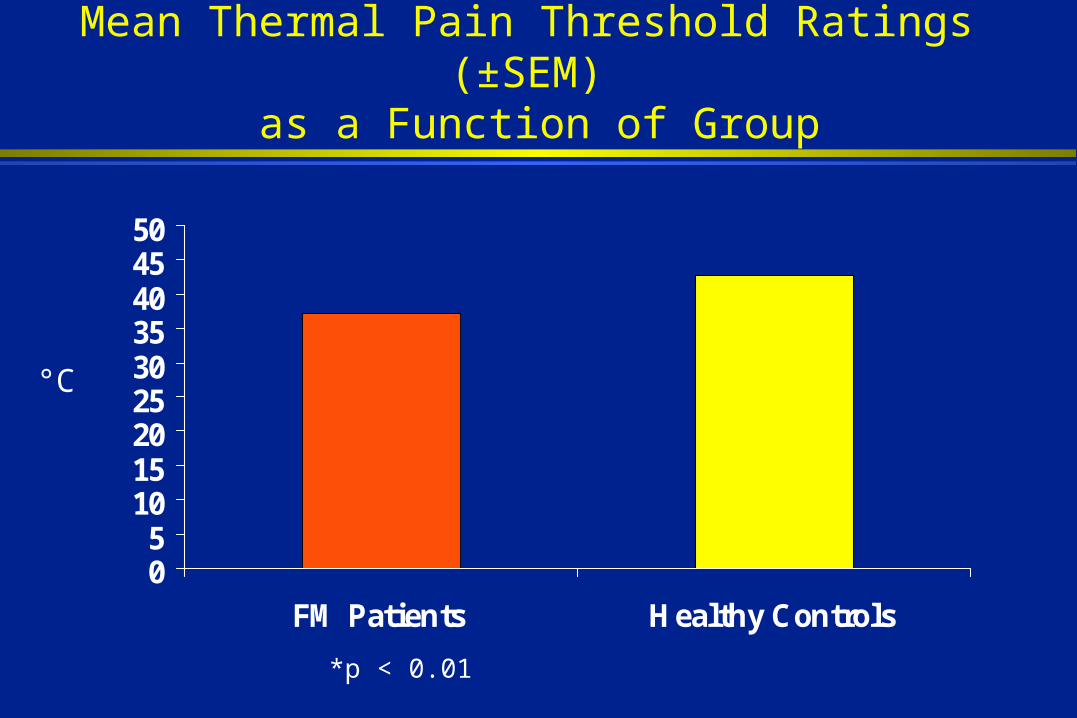
Mean Thermal Pain Threshold Ratings (±SEM) as a Function of Group
05
101520253035404550
FM Patients Healthy Controls
*p < 0.01
°C
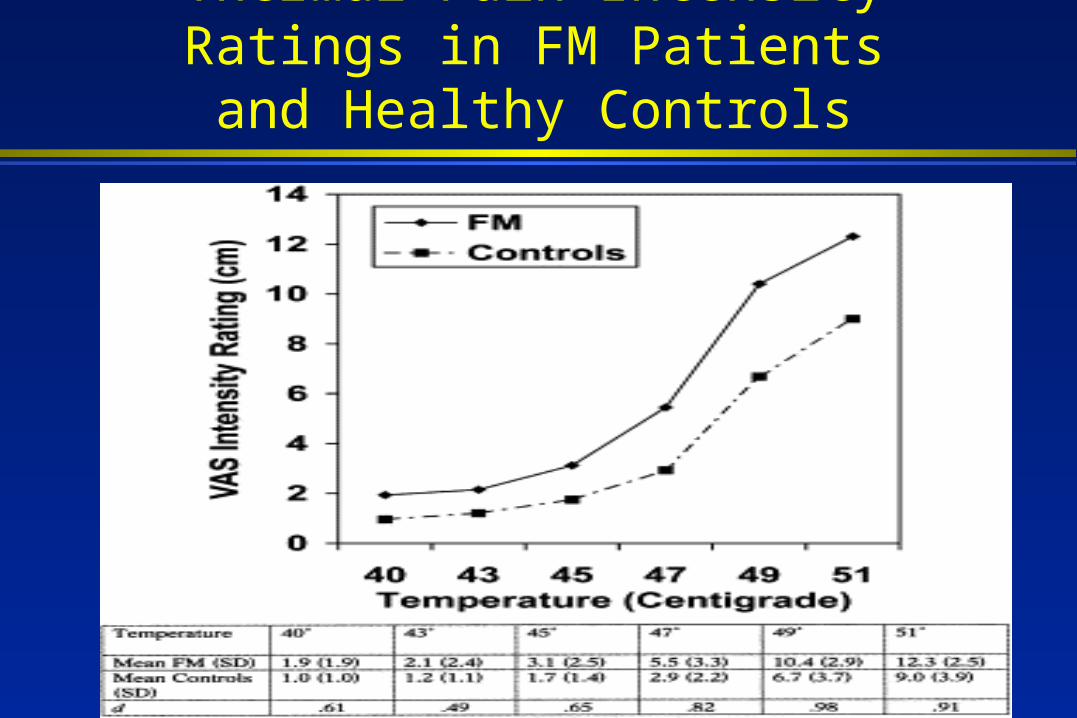
Thermal Pain Intensity Ratings in FM Patients and Healthy Controls

Altered Temporal Summation of Thermal and Mechanical Stimulation
Psychosocial Factors and Health Care Behavior
Psychological distress or psychiatric illness is associated with greater health care seeking behavior at tertiary care facilities
Psychological factors are not necessary or sufficient to produce fibromyalgia symptoms




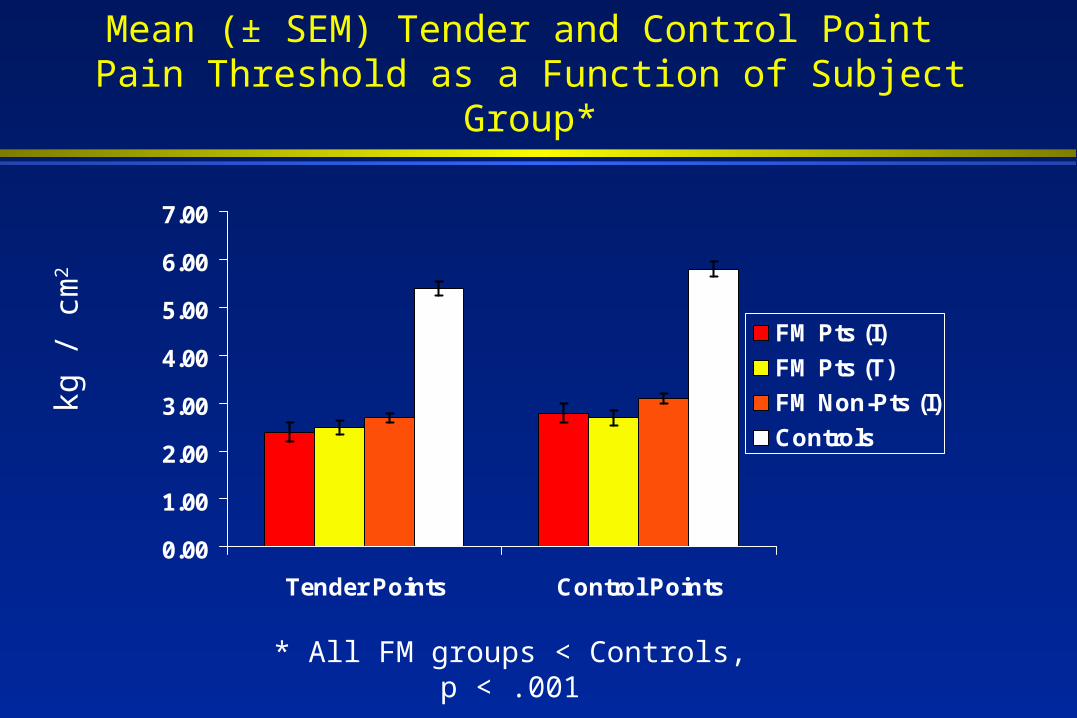
Mean (± SEM) Tender and Control Point Pain Threshold as a Function of Subject Group*
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
Tender Points Control Points
FM Pts (I)
FM Pts (T)
FM Non-Pts (I)
Controls
kg /
cm
2
* All FM groups < Controls, p < .001

Mean (± SEM) CSF Levels of Substance P*
5.00
7.00
9.00
11.00
13.00
15.00
17.00
19.00
21.00
23.00
25.00
FM Pts (I)
FM Pts (T)
FM Non-Pts (I)
Controlsf mol
es/m
l
* All FM groups > Controls, p < .05
Effects of Stress on FM Pain
Patients frequently report that their FM symptoms are intensified by physical and emotional stress
Personally-relevant stressful imagery is associated with increased clinical pain in patients with fibromyalgia (Davis et al., 2001)

Mean Stress-Induced Changes in Pain Unpleasantness Ratings as a Function of Thermal Stimulus and Group
-10
-5
0
5
10
FM Patients Healthy Controls
45°C 47°C 49°C 51°C
Δ M
VA
S R
a tin
g (
stre
ss -
ne u
t ra l
)
Stimulus Temperature
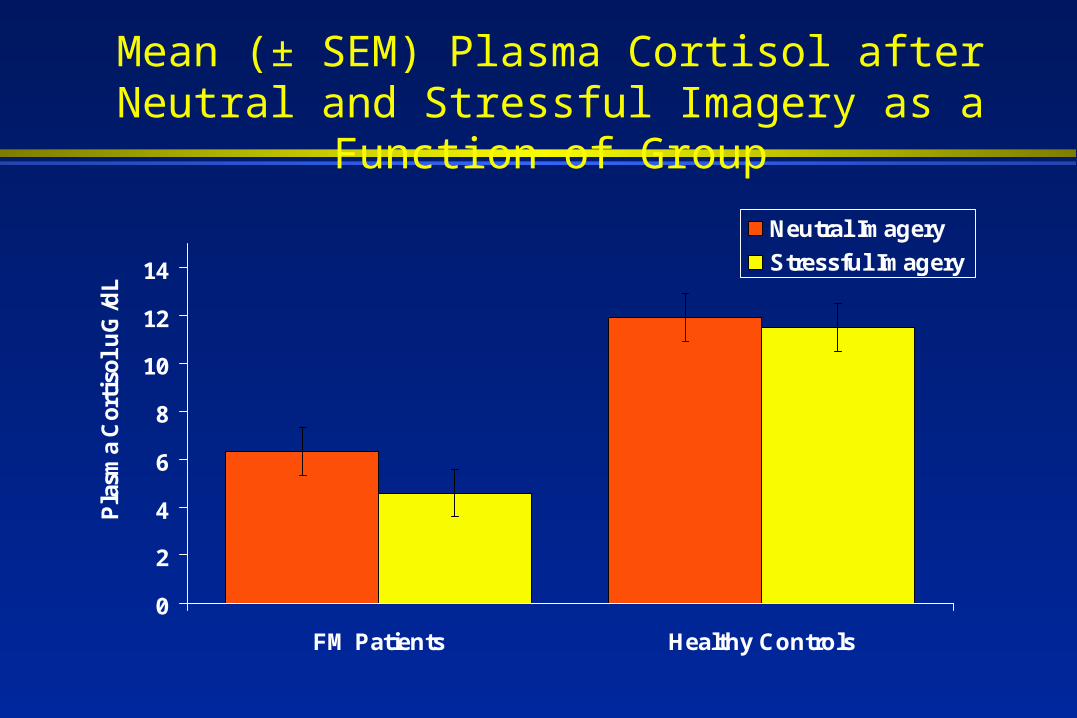
Mean (± SEM) Plasma Cortisol after Neutral and Stressful Imagery as a Function of Group
0
2
4
6
8
10
12
14
FM Patients Healthy Controls
Pla
sma
Cor
tiso
l uG
/dL
Neutral Imagery
Stressful Imagery

Altered Biological Factors Associated with Pain and Distress
Genetic influences on pain and analgesia
Altered central processing of sensory input

Distribution of 5-HTT Promoter Region Polymorphism in FM Patients and Controls
0
10
20
30
40
50
60
L/L L/S S/S
Fre
quency
(%
)
Controls (559 W/ 0 M)
Patients (99 W/ 0 M)
Cohen et al., Arthritis Rheum, 2002

Pentazocine analgesia by sex and MC1R genotype: Thermal and Ischemic Stimulation
(Mogil et al., 2003)

Imaging of Cerebral Responses to Mechanical
Stimulation (Gracely et al., 2002)

Imaging of Cerebral Responses to Mechanical Stimulation (Gracely et al., 2002)
Conclusions
Pain sensitivity, pain-related symptoms, and behavioral disturbances in fibromyalgia are reliably observed:
By different investigators or clinicians
Using different measurement techniques

Conclusions
Pain sensitivity and related symptoms are influenced by biological factors:
There may be a genetic predisposition for development of fibromyalgia, headache, and anxiety disorders
Abnormal pain sensitivity is associated with elevated CSF levels of substance P Abnormal pain sensitivity in fibromyalgia is associated with augmented sensory
neural input

Conclusions
Pain sensitivity and CSF substance P do not vary as a function of affective illness (i.e., major depression) or lifetime psychiatric morbidity
However, plasma cortisol levels, reports of pain unpleasantness, and other symptoms or behaviors (e.g., function, health care seeking) are influenced by psychosocial factors (e.g., stressors) and affective disturbance
Implications for Clinical Trials
Pharmacologic interventions that alter central processing of sensory neural input are likely to modify pain intensity and related symptoms (e.g., sleep, fatigue) in fibromyalgia
These interventions may also modify pain
behavior through alterations in pain intensity and secondary effects on affective disturbance and other psychosocial factors
Implications for Clinical Trials
Cognitive-behavioral and other psychosocial interventions are likely to modify affective responses, health care behavior, and functional ability
Cognitive-behavioral interventions may prove to be most effective when they are used in conjunction with effective pharmacologic therapy