final assessment report - heads of medicines … · paediatric public assessment report eu...
TRANSCRIPT

Paediatric Public Assessment Report
EU Worksharing Project - Assessment of Paediatric data
Ciproxin
Ciprofloxacin
Marketing Autorisation Holder: Bayer HealthCare AG
Rapporteur Finland
Co-rapporteur Denmark
Paediatric assessment procedure started
October 4, 2005
Deadline for Rapporteurs´s final report:
December 13, 2005
Deadline for members states final comments :
January 10, 2006
Date of this report:
15 August, 2006
1

TABLE OF CONTENT I. Introduction……………………………………………………………………………......3 I.1 Scope of the variation…………………………………………………………………....4 II. Scientific discussion……………………………………………………………………....4 II. 1 Quality aspects……………………………………………………………………….....4 II. 2 Non-clinical aspects………………………………………………………………….....4 II .3 Clinical aspects…………………………………………………………………….......11 III.Overall conclusion and benefit-risk assessment………………………………………...24 IV.Request for supplementary information as proposed by the Rapporteur……………….25 The questions raised by the Member States……………….................................................. 25 Finland (Rapporteur)………………………………………………………………………..26 Denmark (Co-rapporteur)…………………………………………………………………...27 Belgium……………………………………………………………………………………...30 France………………………………………………………………………………………..32 Germany…………………………………………………………………………………….40 Hungary……………………………………………………………………………………..46 Portugal……………………………………………………………………………………...47 Sweden……………………………………………………………………………………....47 Comments to the proposed SPC(Day 96)……………………………………………………48 Final SPC changes……………………………………………………………………………54
2

I. INTRODUCTION An “EU Worksharing Project Assessment of Paediatric Data of Existing Products” was initiated in January 2005 within EU in order to assess paediatric data of existing products. In April 2005, Bayer HealthCare AG, the MAH of Ciproxin, was requested to submit all available paediatric data to all individual EU Member States and Norway, Iceland and Liechtenstein for Ciproxin.
In August 2005, the MAH submitted data, which contained the results of following studies: an animal toxicology study, a population pharmacokinetic analysis, a paediatric pharmacokinetic study on sepsis patients, a completed clinical trial on patients with urinary tract infections or pyelonephritis and an one-going long-term safety study in patients with multiple infectious diseases. The clinical data focused on musculoskeletal and CNS safety and on efficacy in children presenting with complicated urinary tract infections or pyelonephritis. Consequently, MAH proposed the use of Ciproxin as a 2nd or 3rd line treatment of complicated urinary tract infections and pyelonephritis in paediatric patients 1 to 17 years of age.
No data on the treatment of acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa infection in paediatric patients aged 5-17 years was presented, since Bayer had submitted this data already in 1997-1998 worldwide and the indication to the treatment of acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa infection was approved throughout Europe. Furthermore, label for the prevention of anthrax for both adults and children, was approved worldwide and therefore, no data was incorporated into this submission.
Along with the application, MAH submitted PSUR from Aug 1st, 2004 through Jan 31st, 2005. The total patient exposure was 99,803 million DDD during the PSUR period compared with 97,338 million DDD during the previous interval. No new or unexpected safety concerns arose from this time period.
Ciproxin was first approved in a European market in Germany on January 31, 1987. Initially, only tablets were approved containing 250, 500 or 750 mg ciprofloxacin. Later this presentation was followed by 100 mg tablets, an intravenous infusion solution (2 mg/ml) and a suspension (50 mg/ml and 100 mg/ml). Currently, Ciproxin is approved in all member states as well as in Norway, Iceland and Liechtenstein. Suspension is available in following European countries: Austria, Belgium, Denmark, France, Germany, Greece, Italy, Luxemburg, Liechtenstein, Netherlands, Portugal, Spain, Sweden, Switzerland and United Kingdom. This Paediatric Public Assessment Report (PdPAR) consists of the proposed paediatric assessment report, the final assessment report (AR) to list of questions raised by the Member States ( Day 85), and the response to the comments to the proposed SPC raised by the Rapporteur (Finland), the Co-rapporteur (Denmark) and the Member States.
3

I.1 Scope of the variation
Ciprofloxacin (Ciproxin®) is a bactericidal antimicrobial agent that belongs to the fluoroquinolone family. It has a long history of established safety and efficacy in adults. It is registered nationally within each European country with variable indications. It is approved for the following indications in adults (varies nationally): urinary tract infections, pyelonephritis, prostatitis, gonorrhea and other sexually transmitted diseases, bacterial gastrointestinal and intra-abdominal infections, skin and skin structure infections, bone and joint infections, infections of respiratory tract including acute sinusitis, otitis media, cystic fibrosis caused by Pseudomonas aeruginosa and post-exposure inhalational anthrax and other gram-negative bacterial infections in immunocompromised hosts. For children and adolescents Ciproxin is indicated for following indications in most European countries: acute pulmonary exacerbations of patients with cystic fibrosis caused by Pseudomonas aeruginosa and in post-exposure inhalational anthrax. In addition, in three European countries (Denmark, Sweden and Finland), Ciproxin is indicated for prophylaxis of meningococcal disease in children and in one European country (Portugal), Ciproxin is indicated as a 2nd or 3rd line treatment of complicated urinary tract infections and pyelonephritis due to E. coli in children. The reasoning for caution for use in subjects of age less than 18 years has been the potential of ciprofloxacin to cause arthropathy. In non-clinical studies, ciprofloxacin has been shown to cause damage to the weight-bearing joints of juvenile animals. To date, ciprofloxacin has been the fluoroquinolone that has been used most extensively in children (mostly in adolescents) without labelling in conditions in which other antimicrobials have failed or antiobiograms have suggested quinolones as advantageous.
II. SCIENTIFIC DISCUSSION
II.1 Quality aspects NA
II.2 Non-clinical aspects II.2.1. Pharmacodynamics No new pre-clinical studies for pharmacodynamics were conducted. II.2.2.1 Subacute Oral Toxicity Study in Beagle Pups (Study No. T4071448; Report No PH 32867) The study was done to evaluate the effects of ciprofloxacin on cartilage development. It was done according to GLP except for electron microscopy that was performed under NON-GLP conditions.
Methods 24 males and 24 nulliparous non-pregnant female 13-16 weeks old beagle dogs of strain HsdCpb:DOBE from Harlan-Winkelmaan (Borchen, Germany) were used for the study. Four groups
4

of 6 males and 6 females were administered ciprofloxacin hydrochloride (Batch nro BXR026U, purity 99.0%) at 0.5% tylose solution orally by gavage once a day over a period of 14-16 days (0, 10, 30, 90 mg/kg/bw). Control group received the vehicle only. Half of the animals (3 males and 3 females from each group) were sacrificed in week 3 of the study 1 day after the last dose. For the follow-up 3 out of the 6 male and female animals per group were kept without treatment for 5 months. The necropsies were performed in week 25 of study for these animals.
During the period of dosing, two animals were housed per cage, whereas in the following recovery period animals were housed individually in the cages. All the animal, separated according to sex, were allowed to exercised daily for about 60 minutes (except at weekends and on public holidays) in a special room directly connected to the stall.
The appearance and behaviour of animals and food intake were monitored individually for each animal daily. The body weight was recorded weekly. At the sacrifice forelegs, shoulder joints (scapula/fossa glenoidalis, humeral head) and elbow joint (lateral humeral condyle, medial humeral condyle, radius, ulna) were fixed in 10 % formalin and hindlegs, hip joints (acetabulum, femoral head) and knee joints (lateral femoral condyle, medial femoral condyle, lateral tibial condyle, medial tibial condyles, patellas) in Davidson’s solution. All samples were stained with Hemalum and Eosin (H&E), safranine O/Fast Green (SOFG), Alcian blues at pH 2.5 and Alcian blue at pH 1.0 (counterstain PAS). Immunohistochemistry for alpha-5-beta-1-integrine (fibronectin receptor) was performed on native cryostate section from humeral head. Also electron microscopy was done from humeral heads. Other tissues were collected but not analysed since the aim of the study was the investigation of the articular cartilage. Gross pathologically other organs were considered normal.
Plasma samples for toxicokinetics were collected in day 1 and 14 before and 1, 2, 4, 6 and 24 h after administration (for control group only before and 2 hours after administration). The results were reported separately (Study No T 4071448; Report No PH 32688) and summary of the study is in paragraph II.2.3.1.
Results There was no mortality amongst treated or control animals. Body weight gain, food and water intake were not significantly altered. Due to treatment, redness of skin and swollen face as well as an increased incidence of vomiting and salivation during the dosing period was observed in 30 and 90 mg/kg groups. These effects were reversible in week 4 of the study. In the 90 mg/kg group also hyperextension of carpal joint during the dosing period was observed (reversible in week 5-9 of the study). One animal treated with 90 mg/kg exhibited locomotor difficulties i.e. disturbed coordination and difficulties in getting up in week 1 and 2 of the study.
At the end of the dosing in the 90 mg/kg group all animals and 30 mg/kg group half of the animals were affected by the treatment. Multiple cartilage lesions were seen in 90 mg/kg/bw and sporadic lesions in 30 mg/kg/bw group (Table 1). NOAEL for cartilage alterations according to gross pathology and histopathology was 10 mg/kg/bw. Histopathology revealed matrix degraradation, chondrocyte degeneration and cluster formation of chondrocytes in the intermediate zone articular cartilage. The humeral head was the most sensitive specimen. The amount of lesions was similar at the end of dosing and at the end of the recovery period in the 90 mg/kg group. However, in the humeral head and acetabulum the quality of lesions had changed from blisters to erosions at the end of recovery, which is a sequel of mechanical influences. Superficial erosions without cluster formations were seen
5

sporadically in all exposure groups including control animals in radius, femoral head and femoral condyles. These lesions were considered not treatment related.
Table 1. Summary of gross pathology and histopathology findings. Each group consists 3 male and 3 female beagle dogs. Group Gross pathology Histopathology 90 mg/kg/bw At the end of dosing
-Blisters and to lesser extent erosion in all animals -Humeral head, femoral head and femoral condyles were affected in all animals -Blisters in humeral condyles in one female
-Blisters and erosion developing in the intermediate zone of articular cartilage -Matrix degraradation, chondrocyte degeneration and cluster formation of chondrocytes in the intermediate zone articular cartilage
90 mg/kg/bw After recovery period
-Erosions and to a lesser extent blisters in all animals -Humeral and femoral heads affected in all animals -Humeral condyles affected in one male and one female -Femoral condyles affected in all males and one female -One animal had blisters also in ulnar cartilage
-Erosions of the articular cartilage of humeral head in all animals -Histopathologically multiple findings characterized by peripheral cluster formation
30 mg/kg/bw At the end of dosing
-Two females out of 3 and one male out of 3 showed blisters of the articular cartilage of the humeral head
-In the cartilage of the proximal humerus blister and erosion were found also in females
30 mg/kg/bw After recovery period
-One female out of 3 showed defective cartilage at both femoral heads -One male had an erosion in cartilage at scapula. (considered not treatment related)
-In one female deep erosion at the femoral head
10 mg/kg/bw At the end of dosing
Normal Normal
10 mg/kg/bw After recovery period
Normal -Superficial erosions focally without cluster formation in femoral condyles, femoral head and radius (considered not treatment related)
0 mg/kg/bw At the end of dosing
Normal Normal
0 mg/kg/bw After recovery period
Normal -One male had superficial erosions focally in both femoral condyles in (considered not treatment related)
After the recovery period all animals had complete involution of epiphyseal plates in scapula, humeral condyles and acetabulum. The involution rate for ciprofloxacin treated animals in all dose groups was
6

slightly higher in femoral head, femoral condyles, tibial condyles and radius (Table 2). In the humeral head the cartilage of the epiphyseal plate underwent partial or complete involution in females only. There was no dose-relation correlation. Eosinophilic streak/s and/or focal degeneration of the epiphyseal cartilage were observed sporadically and without dose-relation. The weight gain of the treated animals was similar to controls. No other parameters describing growth of the dogs were reported.
Table 2. Involution of epiphyseal plate. Complete involution (partial involution)
Males Females Dose (mg/kg)
0 n=3
10 n=3
30 n=3
90 n=3
0 n=3
10 n=3
30 n=3
90 n=3
Femoral head
0(0) 2 (2) 1(0) 1(2) 1(0) 3(0) 2(1) 2(1)
Femoral condyles
0(0) 1(2) 1(0) 1(2) 1(0) 3(0) 2(1) 2(1)
Tibial condyles
0(0) 0(1) 0(1) 0(1) 1(0) 3(0) 2(1) 2(1)
Radius
1(1) 3(0) 3 (1) 3 (2) 2(1) 3(0) 3(0) 3(0)
Humeral head
0(0) 0(0) 0(0) 0(0) 0(1) 0(3) 1(2) 1(2)
Scapula
3 (0) 3(0) 3(0) 3(0) 3(0) 3(0) 3(0) 3(0)
Humeral condyles
3(0) 3(0) 3(0) 3(0) 3(0) 3(0) 3(0) 3(0)
Acetabulum
3(0) 3(0) 3(0) 3(0) 3(0) 3(0) 3(0) 3(0)
Immunohistochemical staining intensity for fibronection receptor was slightly lower in some of the animal from the high dose group. A minimally increased staining of the intermediate zone was recorded in some females dosed at 30 or 90 mg/kg. Due to interindividual variation findings, a treatment effect was considered debatable. At the end of recovery there was no evidence of any differences between groups.
Transmission electron microscopical investigations were carried out on cartilage sample of the humeral head from animals on all dose groups because that location was judged to be the most sensitive by histopathological evaluation. All animals in the 10 mg/kg group and control group were selected for electron microscopy. In the groups 30 and 90 mg/kg only two animals (1 male, 1 female) per group were chosen at the end of the exposure. Initially after the recovery period 2 animals (1 male, 1 female) from group 30 mg/kg and no animal from 90 mg/kg group were chosen. No macroscopical lesions had been developed at the site of sampling. From the 90 mg/kg group additional cartilage specimens were taken from macroscopically altered areas of the formaline fixed wet tissue of two animals at the end of the exposure and two animals after the recovery period. At the end of the dosing animals in dose groups 90 and 30 mg/kg showed large pericellular areas with loss of ground substance and formation of cavities. In this area, an angulation of collagen fibers was observed. Also, formation of chondrocyte clusters, large intracytoplasmic vacuoles and the degeneration of chondrocytes were observed. The changes were also observed in recovery animals after 30 and 90 mg/kg at a slightly decreased severity. Large cavities of the cartilage ground substance only occurred in 30 and 90 mg/kg dose animals at the
7

end of the treatment period. They are assessed to be initial findings of blisters that, after further development, can be detected by light microscopy or even macroscopically. The large cavities of the cartilage ground substance could not be detected after 5 months of recovery. In 10 mg/kg group no substance related changes compared to control group were observed.
In conclusion, gross pathology, light microscopy and electron microscopy revealed substance-induced cartilage alteration in animals dosed with 30 and 90 mg/kg. After follow-up period of 5 months the effects were still detectable. In the 90 mg/kg group the amount of lesions was similar at the end of dosing and at the end of the recovery period. However, according to gross pathology and light microscopy in the humeral head and acetabulum the quality of lesions had changed from blisters to erosions at the end of recovery, which is a sequel of mechanical influences. An oral dose of 10 mg/kg of ciprofloxacin hydrochloride was tolerated without any ultrastructurally, light microscopically or transmission electomicrocopically detectable treatment related changes in the cartilage of juvenile dogs. Also, 10 mg/kg dose did not induce any changes that are manifested later in older animals. The involution of epiphyseal was slightly affected by all ciprofloxacin doses.
Rapporteur’s comment: NOAEL for cartilage adverse effects was 10 mg/kg as confirmed by transmission electron microscopy done to all humeral head samples from control and 10 mg/kg animals. Females seemed more susceptible although the number of animals was small. No delayed effects on the articular cartilage in adulthood after administration of ciprofloxacin during the juvenile age were seen. However, the effects of repeated ciprofloxacin treatments have not been established. The quality of the erosions progressed during the follow up period according to gross pathology and light microscopy in the weight bearing joints of 90 mg/kg group. A deep erosion was also seen in one female treated with 30 mg/kg in the cartilage of humeral head. Because transmission electron microscopical examination was not done to all animals it cannot be used to rule out exacerbation of lesions in 30 and 90 mg/kg dose groups. The dogs were allowed to exercised daily for about 60 minutes and probably the mechanical influences exacerbated the lesions. Whether these lesions cause predisposition to degenerative joint disease later in life was not studied. The involution of epiphyseal was slightly affected by all ciprofloxacin doses without clear dose-relation. Because the study was designed to evaluate the potential for ciprofloxacin to cause latent arthrotoxicity, parameters other than weight gain for growth, were not evaluated. It is therefore unclear whether this finding has any significance. Some very limited data indicate that in animals at an early developmental phase (such as for rats at less than 3 weeks of age or dogs younger than 1 month) the epiphyseal growth plate can also be damaged by quinolones, and that these effects are associated with irreversible bone damage and growth inhibition (Stahlmann and Lode, Drugs, 1999). However, the current existing data on children exposed to ciprofloxacin does not support growth problems (see e.g. Gurnipar et al., J Int Med Res 25:302-306, 1997; Martell et al., J Perinat Med. 24: 287-291, 1996; Drossou-Agakikou et al., Pediatr Infect Dis J 23: 346-349, 2004; Bethell et al., Arch Dis Child 74:44-46, 1996; Doherty et al., Ann Trop Pediatr 20: 297-303, 2000).
8

II.2.3 Pharmacokinetics
II.2.3.1 Plasma concentrations of BAY q 3939 in a 2-week oral toxicity study on beagle dogs with BAY O 9867 (Study No T 4071448; Report No PH 32688) This study was done in conjunction with previous 2-week oral toxicity study. Beagle dogs were administered ciprofloxacin hydrochloride 10, 30 and 90 mg/kg related to 9.01, 27 and 81.1 mg/kg ciprofloxacin. Plasma samples for pharmacokinetics were collected and analyzed in day 1 and 14 before and 1, 2, 4, 6 and 24 h after administration (for control group only before and 2 hours after administration) from a peripheral vein to heparinized test tubes. The analytical part of this study was conducted in compliance with OECD Principles of Good Laboratory Practise. Ciprofloxacin concentrations were determined using HPLC with fluorescence detection after addition of acetonitrile and removal of the resulting precipitate by centrifugation.
Results showed that there were no clear gender differences. Individual Cmax was reached rapidly within 1 to 2 hours after administration. The plasma concentrations and the pharmacokinetic parameters showed interindividual variability: AUCs showed up to nearly 4-fold differences. After repeated administration in the low and the medium dose the exposure in terms of Cmax and AUC (0-24) remain approximately equal on Day 1 and Day 14. In the high dose the exposure increased by a factor of 1.41 for Cmax and 1.65 for AUC (0-24).
On Day 1 and Day 14 Cmax and AUC (0-24) increased slightly less than dose-proportionally from 10 to 30 mg/kg. Also from 30 to 90 mg/kg Cmax rose less than dose proportionally on Day 1. On Day 14 dose-proportionally effect on Cmax was seen.
No plasma concentration of test substance was found in the samples from the control group on Day 1. However, on Day 14 all plasma samples of the control animal showed predominantly low concentration of test substance just above the lower limit of quantitation (0.005 mg/L). In 3 females out of 12 animal higher concentrations up to 0.738 mg/L were determined. The highest measured concentration in the positive control samples corresponded to 28.4% of the Cmax of the low dose-group on Day 14. The arithmetic mean of the concentration of all control samples on Day 14 amounts to 0.0789 mg/L, which is 2.85% of the Cmax of the low dose group at Day 14. The source of contamination remained unclear. Rapporteur’s comment: The control animals were slightly contaminated with the study substance. Also the interindividual variation of the animals within groups was high AUCs showing up to nearly 4-fold differences. Different exposure groups showed overlap with highest and lowest concentrations. It was not possible to correlate plasma concentrations and adverse effects due to differential numbering of animals in the pathology report and the toxicokinetics report.
9

II.2.3.2 Population Pharmacokinetic modelling of Ciprofloxacin in Pediatric Patients (Report No: MRC-01209) Plasma ciprofloxacin concentration-time data were available in 357 pediatric patients (105 males, 252 females) from a total of 6 pediatric studies. The age of patients ranged from 0.27 to 16.9 years and the body weight ranged from 4.2 to 73.5 kg. Twenty-eight out of 357 patients had a history of cystic fibrosis and 207 out of 357 patients were being treated for complicated urinary tract infection / acute pyelonephritis.
The population pharmacokinetic analysis was conducted with the following objectives: 1) to estimate typical population pharmacokinetic parameters for ciprofloxacin in pediatric patients, 2) to identify covariate, demographic and clinical factors that are significant predictors of variability in ciprofloxacin pharmacokinetic parameters, and 3) to provide a dosing recommendation for pediatric patients. Analyses were performed with the NONMEM software using the First-Order Conditional Estimation (FOCE) method. Different options were considered to calculate ciprofloxacin dose for pediatric subjects. Ciprofloxacin dosing regimen employed in Study 100169 (UTI/Pyelonephritis study) was adopted and the dosing schedule proposed for complicated urinary tract infections and pyelonephritis was found acceptable: For complicated urinary tract infections or pyelonephritis the dose is 6 to 10 mg/kg i.v. every 8 hours with a maximum of 400 mg per dose or 10 to 20 mg/kg orally every 12 hours with a maximum of 750 mg per dose. The final model and simulations suggested that ciprofloxacin dose need not be adjusted for pediatric patients with mild renal impairment.
Rapporteur’s comment: The prediction is somewhat consistent with ciprofloxacin pharmacokinetic data observed in adults with normal renal function and mild renal impairment (Shah et. Al., J Antimicrob Chemother, 1996). The population based estimates for ciprofloxacin half-life (T1/2) ranged from approximately 4 to 5 hours in pediatric patients and was similar to that reported in non-cystic fibrosis patients receiving oral ciprofloxacin therapy by Peltola and co-workers (Pediatrics, 1998; 4.2 to 5.1 hours). The dosing schedule proposed by applicant for complicated urinary tract infections and pyelonephritis is as follows “For complicated urinary tract infections or pyelonephritis the dose is 6 to 10 mg/kg i.v. every 8 hours with a maximum of 400 mg per dose or 10 to 20 mg/kg orally every 12 hours with a maximum of 750 mg per dose” The proposed dosing schedule corresponds to option C was also employed in clinical trial (100169 -UTI/Pyelonephritis study), evaluating effectiveness and adverse effects of ciprofloxacin therapy in complicated urinary tract infection in children. The used dosing regimen was effective and well tolerated.
II.2.4 Overall conclusions on preclinical studies The NOAEL for cartilage adverse effects was 10 mg/kg in beagle dogs. It seemed that females were more susceptible for adverse events. The lesions in the articular cartilage were not reversible but rather
10

progressed during follow-up period. However, no delayed effects on the articular cartilage in adulthood after administration of ciprofloxacin during the juvenile age were seen. For involution of epiphyseal plate no NOAEL could be established. On the other hand, there was no dose-relation. The toxicokinetics part of the study showed slight contamination of control animals and also high variation in plasma concentrations. According to population based pharmacokinetic modelling the expected exposure of children was higher than NOAEL for cartilage adverse effects in beagle dogs (Table 5). This also supported by the Study 3939/0553 (A non-controlled study to determine the pharmacokinetic profile of ciprofloxacin 20 mg/kg/day in pediatric patients with severe sepsis, treated in the intensive care unit) in which observed Cmax values varied from 4.69 to 11.8 mg/L and AUC values from 11 to 32 mg*h/L after single dose. Overall, the highest expected human exposures to ciprofloxacin are within same magnitude as the doses producing adverse effects in beagle dogs and therefore there is no safety margin.
Table 5. Comparison of pharmacokinetic parameters obtained through population based pharmacokinetic modeling in children based and preclinical safety study in beagles.
Modelling 9 mg/kg iv single dosea
Modelling 9 mg/kg iv single doseb
Beagle dogs 10 mg/kg po Day 1
Beagle dogs 30 mg/kg po Day 1
Beagle dogs 90 mg/kg po Day 1
AUC(mg*h/L) 18.5 23.97 12.3±3.16 30.1±8.79 60.9±25.9
Cmax (mg/L) 6.63 7.2 2.63±0.572 5.68±1.26 10.8±2.4
aCreatinine clearance 130 mL/min/1.73m2; bCreatinine clearance 50 mL/min/1.73m2
In conclusion, the juvenile dog studies clearly showed adverse effects in articular cartilage, but no delayed effects on the articular cartilage in adulthood were seen. It is known that pyelonephritis may lead to renal complications. Based on conducted preclinical safety studies alone, no risk-benefit assessment of ciprofloxacin could be made. The juvenile dog is thought to be the most susceptible to quinolone induced arthropathy and according to existing data, humans seem to be far less susceptible to ciprofloxacin induced lesions. Therefore, Ciproxin cannot be approved as first line therapy for paediatric use due to safety concerns arising from animal experimentation and lack of safety margin.
II.3 Clinical aspects II.3.1 Clinical pharmacology Phase III study (3939/0553) was a non-controlled study to determine the pharmacokinetic profile of ciprofloxacin administered intravenously (IV) in paediatric patients with severe sepsis, treated in the intensive care unit. The patients (n=20) were stratified in two groups by age: Group A – patients from 3 to 11 months old; group B – patients from 1 to 5 years old. The dose of intravenous ciprofloxacin was 10 mg/kg every 12 hrs (60 min infusion). The number of enrolled patients was 20 (10 in each group). All were analysed for pharmacokinetics and safety. Fifteen patients (7 in group A, 8 in group B) completed the study. The study was conducted at one site.
11

Rapporteur`s comment: The design of the study was appropriate to study the dosing of intravenously administered ciprofloxacin.
Inclusion criteria included: 1) children requiring intensive care treatment for severe sepsis 2) assessment period of 12 hrs or less preceding enrolment 3) age between 3 months and 5 years 4) at least 3 of the following signs of symptoms:
- clinical evidence of infection - temperature >38,3°C or <35,6°C - tachycardia >100/min or adjusted for age (table) - respiratory rate >40/min (>1 yr) and >60/min (<1 yr) - WCC >12x109/l or <4x109/l - evidence for decreased perfusion (at least 1 of 3 criteria)
5) informed consent obtained from the parent or legal guardian
The design of the study is presented in Table 1:
Ciprofloxacin (test product BAY q 3939), 10 mg/kg 12-hourly, was administered intravenously during 60 min. The duration of treatment was to be between 7 and 14 days, unless the investigator considered that clinical cure
12

had been obtained in a shorter time period.Blood specimens for the determination of ciprofloxacin concentration in serum were drawn on days 0, 2 and 7. Urine sampling was also performed on days 0, 2 and 7.The following pharmacokinetic variables were calculated: Peak concentration, Cmax; Half-life, t1/2,; Area under curve, AUC (for various time periods), AUC 0-12h The pharmacokinetic profiles were similar in group A and B, for all three profiles (days 0, 2 and 7), suggesting linear pharmacokinetics, i.e. accumulation had not taken place (Table below). Cmax values were 5.81 to 9.03 mg/L in group A and 6.38 to 7.61 mg/L in group B. AUC 0-12h values 14.1 to 19.2 mg.h/L in group A and 13.2 to 18.0 mg.h/L in group B. Half-life of ciprofloxacin was 2.93 to 3.67 h in group A and 2.82 to 3.12 h in group B.
13

The results (single dose profile) were similar to those obtained with intravenous ciprofloxacin in adults (BAY 3939/0541), whereas in a study with oral ciprofloxacin (15 mg/kg) in children (Peltola et al. 1992), the Cmax and t1/2 values were slightly lower (Table below).
14

II.3.2 Pharmacodynamics
NA II.3.3 Clinical efficacy
Main study (100169 -UTI/Pyelonephritis study)
Study 100169 (phase IIIb study) was a prospective, randomized study to compare ciprofloxacin (either as oral suspension or as IV or sequential IV → oral suspension therapy) versus control regimens (either trimethoprim/sulfamethoxazole (TMP/SMX) oral suspension, cefixime oral suspension, IV ceftazidime, sequential IV ceftazidime → trimethoprim/sulfamethoxazole oral suspension therapy or sequential IV ceftazidime → oral cefixime) in the treatment of pediatric patients with complicated urinary tract infections (UTI) or pyelonephritis. The patients were 1-17 years old. The number of patients was 684. The oral dose of ciprofloxaxin was 10 to 20 mg/kg every 12 hrs and the IV dose was 6 to 10 mg/kg every 8 hrs. The total number of enrolled patients was 689. Of these, 684 patients (335 in ciprofloxacin group and 349 in comparator group), were valid for safety analysis. The study was conducted at 61 different sites.
Inclusion criteria included: All patients eligible for enrolment were to meet the following criteria: 1) age ≥1 year but <17 years 2) written informed consent provided by parent/legal guardian and patient (as appropriate) 3) positive urine culture obtained by clean-catch MSU, intermittent catheterization, indwelling catheterization or suprapubic aspiration. 4) current episode of complicated UTI as indicated by 1 or more of the following symptoms:
- infants and children, from 12 months to <6 years: recent weight loss, failure to thrive, abdominal pain, nausea, vomiting, diarrhea, jaundice, or fever (>38°C orally, >38,6°C rectally, >37,4°C axillary, or >38,5°C tympanically) - older children and adolescents, from ≥6 years to <17 years: dysuria, urgency, urinary incontinence associated with urgency, bedwetting in a previously dry child, abdominal pain, urinary frequency/pollacisuria or foul-smelling urine or fever (defined as above)
Patient with complicated UTI were also to have 1 or more of the following criteria: 5) indwelling catheter or use of intermittent catheterization; 6) obstructive uropathy due to bladder outlet obstruction; 7) vesicoureteral reflux (VUR) or other urologic abnormalities; 8) functional of neurogenic disturbances of micturition with significant impact on bladder; emptying of pressure profile within the bladder; 9) recurrent UTI, defined as 2 or more acute UTIs over a 6-month period 10)evidence that the current UTI episode could be caused by a resistant uropathogen, including evidence that the current episode was a breakthrough infection or an older child or adolescent on chronic or intermittent antimicrobial suppression with unresolved vesicoureteral reflux 11) patients presenting with pyelonephritis had fever (defined as above).
15

Rapporteurs`s comment: The design of the study and the number of patients were appropriate to show equivalence in safety and efficacy of ciprofloxacin compared with other treatments. The study was conducted at 61 different sites in 8 countries, which may cause some variation in results.
Study treatment Ciprofloxacin was administered either intravenously or orally. The dosing is shown in Table 9-1 and Table 9-2.
Other treatments were: 1) Cefixime (PO): 4 mg/kg every 12 hours; 200 mg every 12 hours for those >50 kg or >12 years 2) Trimethoprim/sulfamethoxazole (PO): 4 mg/kg trimethoprim and 20 mg/kg sulfamethoxazole every 12 hours (maximum daily dose was 320/1600 mg) and 3) Ceftazidime (IV): 30-45 mg/kg every 8 hours.
Results
16

There were 442 patients valid for efficacy analysis, 211 in the ciprofloxacin group and 231 in the comparator group.
Co-rapporteur’s comment: Guidance 558/95: “Clinical opinion regarding who needs to be hospitalized and who needs parenteral medication, and admission policies in different healthcare systems, vary considerably on these matters. Therefore, enrolment into such studies should depend only on clear inclusion criteria.” This seems not to be the case in this study, since it was left to the investigator to decide, whether the patient should be treated IV or PO. Furthermore it was left to the decision of the investigator when to shift from IV to PO Point for clarification: Were the groups of patients from the different study sites comparable in this situation, where it was left to the investigator to decide whether the patient should be treated parenterally and if when the treatment could be changed to PO?
Clinical response Clinical response 5-9 days after the end of the therapy was the primary efficacy variable (Test-of-Cure). Definitions of clinical response were:
- Cure: resolution of signs and symptoms related to the current infection and not requiring further antibiotic therapy;
- Failure: persistent fever or flank pain or insufficient reduction in severity of the signs and symptoms of infection to qualify as resolution, requiring a modification of the antibacterial therapeutic regimen;
- Indeterminate: patients in whom a clinical assessment was not possible for various reasons, including early withdrawal for adverse events, protocol violations etc.
The overall cure rates were 95.7% and 92.6% for the ciprofloxacin and comparator groups, respectively suggesting that ciprofloxacin is equivalent to the comparator. In the oral therapy group (407 patients), the cure rate was 95.4% for ciprofloxacin and 93.4% for the comparator (211 patients). The cure rate was higher in the IV therapy group (35 patients) for ciprofloxacin (93.3%) compared to that of the comparator (85.0%).For the pyelonephritis patients, the clinical cure rates were 97% and 93% in the ciprofloxacin and comparator groups, respectively. For the complicated UTIs, the respective cure rates were 95% and 92%.
Bacteriological response was assigned on Day +5 to +9 following therapy (Test-of-Cure). Eradication was achieved in 84% of patients in the ciprofloxacin group and 79% of patients in the comparator group. The overall eradication rates (indeterminate and missing results excluded) as specified by the protocol were 86% and 81%, respectively. The eradication rates for pyelonephritis were 93% for the ciprofloxacin group and 89% for the comparator group. For complicated UTIs, the respective eradication rates were 78% and 68%.
17

In conclusion, judged by bacteriological and clinical response, Ciproxin was shown to be as efficacious as the comparator drugs in the treatment of urinary tract infections.
Co-rapporteur’s comment: 247 patients were not valid for efficacy. Validity was determined in a blinded review, and there was no bias toward either treatment group; 37% of the ciprofloxacin group and 34% of the comparator group were invalid. The description of the reasons for invalidity is sufficient.
II.3.4 Clinical safety Safety analysis is based on three studies: Sepsis study (3939/0553), UTI/Pyelonephritis study (100169) and the study with multiple infectious diagnoses (100225), of which the latter evaluates the long-term safety.
Patient exposure
Study 3939/0553 (Sepsis study): The numbers of analysed patients (groups A and B together) were 20 at Day 0, 17 at Day 2, and 14 (15) at Day 7. The mean number of days on study medication was 8 days for groups A and B combined. The mean number of doses per patient was 14.6 doses (median 17 doses).
Study 100169 (UTI/Pyelonephritis study):
Of the 689 patients enrolled, 684 received at least one dose of study drug. For 5 patients (2 Ciproxin, 3 comparator), it could not be confirmed whether study drug was taken. The mean length of treatment duration was 10.5 days for the oral treatment and 5.1 days for the intravenous treatment. There was no difference between Ciproxin and comparator groups.
Study 100225 – (Multiple infectious diagnoses)(interim report) (described later):
Of the 1029 patients enrolled, 994 received at least one dose of study drug and were valid for the safety analysis.
Adverse events
Study 3939/0553 (Sepsis study): All 20 patients were included in the safety analysis. Eight patients (40 %) had at least one adverse event and a total of 12 adverse events were reported. Three patients (30 %) in group A reported 3 adverse events and 5 patients (50 %) in group B reported 9 adverse events (Table 25). One of the adverse events was possible related and one was remotely related to the study drug, whereas 10 of the 12 adverse events were not related to the study treatment.
18
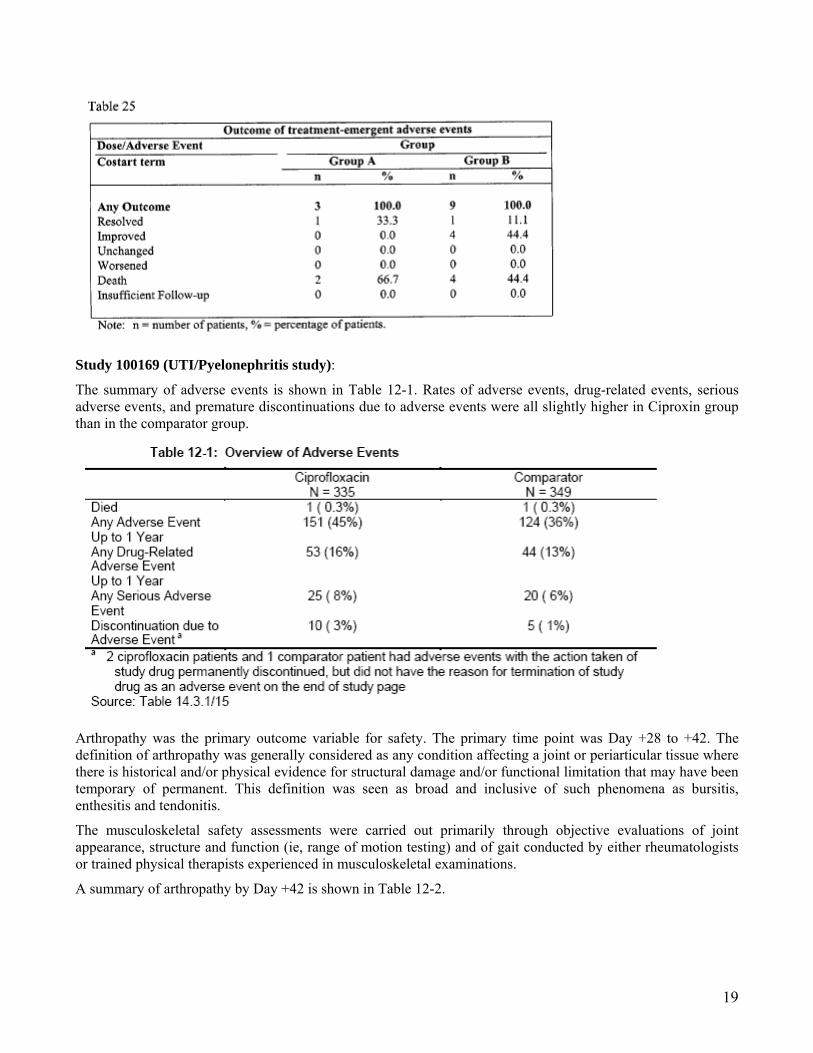
Study 100169 (UTI/Pyelonephritis study):
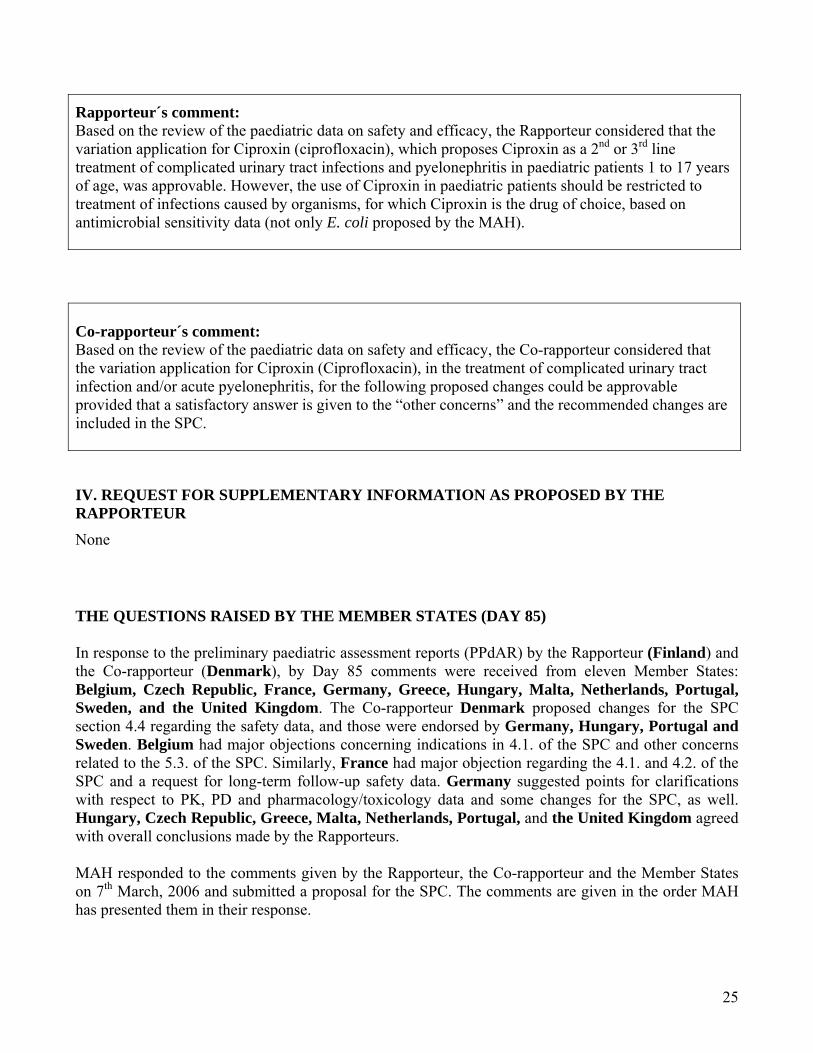
The summary of adverse events is shown in Table 12-1. Rates of adverse events, drug-related events, serious adverse events, and premature discontinuations due to adverse events were all slightly higher in Ciproxin group than in the comparator group.
Arthropathy was the primary outcome variable for safety. The primary time point was Day +28 to +42. The definition of arthropathy was generally considered as any condition affecting a joint or periarticular tissue where there is historical and/or physical evidence for structural damage and/or functional limitation that may have been temporary of permanent. This definition was seen as broad and inclusive of such phenomena as bursitis, enthesitis and tendonitis.
The musculoskeletal safety assessments were carried out primarily through objective evaluations of joint appearance, structure and function (ie, range of motion testing) and of gait conducted by either rheumatologists or trained physical therapists experienced in musculoskeletal examinations.
A summary of arthropathy by Day +42 is shown in Table 12-2.
19

Within oral treatment (296 Ciproxin and 304 comparator patients), the arthropathy event rates were 9.1% (27 patients) in the Ciproxin group and 6.9% (21 patients) in the comparator group. Within IV treatment (39 Ciproxin and 45 comparator patients) the respective rates were 10.3% (4 patients) and 0% (none).
Since the upper limit of the confidence interval for the difference in arthropathy rates was greater than 6%, it could be concluded that Ciproxin is not equivalent to the comparator.
The overall adverse event rate by Day +42, shown in Table 12-4, was 41% in the Ciproxin versus 31% in the comparator group. Abdominal pain, vomiting and nausea were slightly more common in the ciprofloxaxin group than the comparator group.
Serious adverse events and deaths
Study 3939/0553 (Sepsis study):
Three patients died during the study (two in group A and one in group B) and one patient died 5 days after the end of the treatment. The deaths were considered unrelated to the study treatment. Five patients had 9 serious adverse events (two patients in group A and 3 patients in group B). Only one of the serious adverse events was possibly related to the study drug (convulsion in patient B10; resolved).
20

Study 100169 (UTI/Pyelonephritis study):
Two patients died during the study. One was a victim of infanticide and the other died from HIV infection. Both deaths were unrelated to the study treatment. In the Ciproxin group, 12 patients (3.6%) discontinued the study medication because of an adverse event, and 25 patients (7.5%) had serious adverse events. All serious adverse events were judged by the investigators to be unlikely or not related to the study drug. The most common adverse events leading to premature discontinuation of Ciproxin therapy were vomiting (3 patients), nausea (2 patients), and moniliasis (2 patients). No patient discontinued due to a musculoskeletal event. In the comparator group, 6 patients (1.7%) discontinued the treatment due to an adverse event, and 20 patients (5.7%) had serious adverse events.
Laboratory findings
Study 100169 (UTI/Pyelonephritis study):
Laboratory test abnormalities occurred at similar rates in both treatment groups (Table 12-6).
21

Long-term safety data
Study 100169 (UTI/Pyelonephritis study):
By one year, the adverse event rates were similar to those by Day +42 (Table 12-5). Ciproxin exhibited a higher overall event rate by 1 year (Ciproxin 45% versus comparator 36%) and a higher drug-related event rate by 1 year (Ciproxin 16% versus comparator 13%).
Among ciprofloxacin patients with arthropathy by one year after treatment, 65% (30/46) of cases were considered by the Independent Pediatric Safety Committee to be related to the study drug and 30% (14/46) of cases were considered to have a pre-existing condition. Among comparator patients, the respective percentages were 59% (20/34) and 41% (14/34). Table 14.3.1/4.
The mean duration of arthropathy was 44 days in the Ciproxin group and 32 days in the comparator group. The arthropathy resolved in all patients in whom the relationship of arthropathy to the study drug was possible or probable (Table 14.3.1/5; not shown here).
22

Study 100225 – Phase IIIb study (multiple infectious diagnoses)(interim report).
A prospective, open-label, non-randomized, naturalistic, long-term safety surveillance, observational study of either ciprofloxacin (either as oral suspension, oral tablets or sequential IV → oral therapy or purely IV therapy) or a non-quinolone antibiotic (either as oral suspension, oral tablets or sequential IV → oral therapy or purely IV therapy) in the treatment of paediatric patients with infectious diagnoses. The patients were 2 months - 16 years old. The number of patients was 994.
The oral dose of Ciproxin was 5-20 mg/kg every 12 hrs and the IV dose was between 6 mg/kg every 12 hrs and 12 mg/kg every 8 hrs, depending on the severity of infection. The total number of enrolled patients was 1029 of which 994 were valid for the safety analysis (487 in Ciproxin and 507 in non-quinolone group). The study was conducted at 67 study sites in the US and 1 in Canada.
The final analysis of the data is planned to occur approximately 5 years after the last paediatric patient is enrolled. This interim analysis included only 1-year post-treatment follow-up data for all patients who had been contacted by telephone by June 30, 2003.
Preliminary results of study 100225
Only the musculoskeletal and CNS events observed through one year are shown here. The data were obtained by telephone contact. Table 12-3 shows the adverse events in the Ciproxin group and Table 12-10 in the non-quinolone group.
The incidence of any musculoskeletal event by 1 year of post-treatment follow-up was 13% in the Ciproxin group and 3% in the control group. Arthralgia was reported in 9% and 1% of Ciproxin and control patients, respectively.
23

Rapporteur´s comment: The occurrence of adverse events in patients treated with Ciproxin was slightly higher than in those treated with the comparator study drugs. The difference was seen in the rates of arthropathy and gastrointestinal symptoms (abdominal pain, vomiting, nausea). Although most of the events were mild and resolved completely, the use of Ciproxin in paediatric patients should be restricted to treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data.
III. OVERALL CONCLUSION AND BENEFIT-RISK ASSESSMENT
Based on the review of submitted paediatric data on safety and efficacy, it was concluded after the first round, that the variation application for Ciproxin, proposing to use Ciproxin as a 2nd or 3rd line treatment of complicated urinary tract infections and pyelonephritis in paediatric patients 1 to 17 years of age, is approvable. Results of main study 100169 (UTI/Pyelonephritis study) showed, that Ciproxin was as efficacious as the comparator drugs in the treatment of urinary tract infections in children. The juvenile dog studies clearly showed adverse effects in articular cartilage, but no delayed effects on the articular cartilage in adulthood were seen. The occurrence of adverse events in patients treated with Ciproxin was slightly higher than in those treated with the comparator study drugs. The difference was seen in the rates of arthropathy and gastrointestinal symptoms (abdominal pain, vomiting, nausea). Most of the events were mild and resolved completely. However, due to safety concerns arising from animal experimentation and lack of safety margin, the proposal was that Ciproxin should be used as 2nd or 3rd line treatment of complicated urinary tract infections and pyelonephritis in paediatric patients 1 to 17 years of age, only. The use of Ciproxin in paediatric patients should be restricted to treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data (not only E. coli).
In addition, it was proposed that the SPC should address the issue that Ciproxin is not a drug of first choice in the pediatric population due to an increased incidence of adverse events compared to controls including events relating to joints and/or surrounding tissues. These issues should be addressed in sections 4.1, 4.2, 4.4, 4.8, 5.2, and 5.3 of the SPC.
24
Rapporteur´s comment: Based on the review of the paediatric data on safety and efficacy, the Rapporteur considered that the variation application for Ciproxin (ciprofloxacin), which proposes Ciproxin as a 2nd or 3rd line treatment of complicated urinary tract infections and pyelonephritis in paediatric patients 1 to 17 years of age, was approvable. However, the use of Ciproxin in paediatric patients should be restricted to treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data (not only E. coli proposed by the MAH).
Co-rapporteur´s comment: Based on the review of the paediatric data on safety and efficacy, the Co-rapporteur considered that the variation application for Ciproxin (Ciprofloxacin), in the treatment of complicated urinary tract infection and/or acute pyelonephritis, for the following proposed changes could be approvable provided that a satisfactory answer is given to the “other concerns” and the recommended changes are included in the SPC.
IV. REQUEST FOR SUPPLEMENTARY INFORMATION AS PROPOSED BY THE RAPPORTEUR None THE QUESTIONS RAISED BY THE MEMBER STATES (DAY 85) In response to the preliminary paediatric assessment reports (PPdAR) by the Rapporteur (Finland) and the Co-rapporteur (Denmark), by Day 85 comments were received from eleven Member States: Belgium, Czech Republic, France, Germany, Greece, Hungary, Malta, Netherlands, Portugal, Sweden, and the United Kingdom. The Co-rapporteur Denmark proposed changes for the SPC section 4.4 regarding the safety data, and those were endorsed by Germany, Hungary, Portugal and Sweden. Belgium had major objections concerning indications in 4.1. of the SPC and other concerns related to the 5.3. of the SPC. Similarly, France had major objection regarding the 4.1. and 4.2. of the SPC and a request for long-term follow-up safety data. Germany suggested points for clarifications with respect to PK, PD and pharmacology/toxicology data and some changes for the SPC, as well. Hungary, Czech Republic, Greece, Malta, Netherlands, Portugal, and the United Kingdom agreed with overall conclusions made by the Rapporteurs. MAH responded to the comments given by the Rapporteur, the Co-rapporteur and the Member States on 7th March, 2006 and submitted a proposal for the SPC. The comments are given in the order MAH has presented them in their response.
25

Questions raised by the Member States 1.1. Request to change the SPC text for the indication ( Rapporteur) “The use of Ciproxin in paediatric patients should be restricted to treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data and not only for E. coli.” MAH Response: The changes in the proposed SPC text as requested by the Rapporteur are accepted by Bayer and included in our proposal for the SPC text. The reference to section 4.4 has been taken out in the final SPC proposal. MAH`s proposal for the SPC Section 4.1. (Day 85): Section 4.1 THERAPEUTIC INDICATIONS Children Ciprofloxacin may be used in children for the 2nd and 3rd line treatment of complicated urinary tract infections and pyelonephritis due to E. coli or other susceptible pathogens (age range studied in clinical studies: 1-17 years) and for the treatment of acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa (age range applied in clinical studies: 5-17 years). Treatment should be initiated after careful benefit/risk evaluation, due to possible adverse events related to joints and/or surrounding tissues. The use of Ciproxin in pediatric patients with complicated urinary tract infections and pyelonephritis should be restricted to treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data. Inhalational anthrax (post-exposure) in adults and in children: To reduce the incidence or progression of disease following exposure to aerosolised Bacillus anthracis. Ciprofloxacin serum concentrations achieved in humans serve as a surrogate endpoint reasonably likely to predict clinical benefit and provide the basis for this indication (see also: Inhalative Anthrax – additional information in section Pharmacodynamic properties). Consideration should be given to official guidance on the appropriate use of antibacterial agents. Rapporteur’s comment: MAH has taken into consideration the request that the use of Ciproxin should be restricted to the treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on the antimicrobial sensitivity data and not E. coli. However, in the proposed form, 4.1. of the SPC is slightly confusing and repetitive. Rapporteur disapproves of deleting the cross-reference to 4.4. and endorses the proposal by France to include cross-reference also to section 5.1. Rapporteur requests the following wording for the 4.1. of the SPC concerning the use of Ciproxin in children: Children Ciprofloxacin may be used for the 2nd and 3rd line treatment of complicated urinary tract infections and pyelonephritis in children and adolescents 1-17 years of age and for the treatment of acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa in children and adolescents 5-
26

17 years of age. The use of Ciproxin in paediatric patients with complicated urinary tract infections and pyelonephritis should be restricted to treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data. Treatment should be initiated by physician, who is experienced in the treatment of severe infections in children and adolescents and after careful benefit/risk evaluation, due to possible adverse events related to joints and/or surrounding tissues. (see 4.4. and 5.1.). Inhalational anthrax (post-exposure) in adults and in children: (as approved nationally in each member state)…. Consideration should be given to official guidance on the appropriate use of antibacterial agents.” The point unresolved. Co-rapporteur comment: Agreed 2.1 Question 1, Clinical efficacy ( Co-rapporteur) “Were the groups of patients from the different study sites comparable in the situation, where it was left to the investigator to decide whether the patient should be treated parenterally, and if when the treatment could be changed to PO.” MAH Response: The patient demographics in Study 100169 are summarized in the Table 2-1 by treatment regimen and route of administration. In this study, the decision of whether to administer intravenous (IV) therapy or oral (PO) therapy only was at the Investigator’s discretion. From this table, it is clear that there was good comparability between ciprofloxacin- and comparator-treated patients who received IV therapy and also between ciprofloxacin- and comparator-treated patients who received PO therapy only. Thus, all 4 treatment groups were similar with respect to mean age, sex and race. The number of ciprofloxacin and comparator patients treated with IV or PO therapy across individual countries was also similar. Not surprisingly, patients with severe infections were more likely to receive IV therapy than patients with mild to moderate infections. However, the number of ciprofloxacin- and comparator-treated patients with moderate to severe infections who received IV therapy was very similar. In summary, the demographic characteristics of patients selected to receive IV ciprofloxacin or comparator therapy were comparable as were the demographics of ciprofloxacin or comparator patients who were selected to receive PO therapy.
27

Rapporteur´s comment: MAH has provided the requested data, from which it can be concluded that the demographic characteristics of patients selected to receive either IV or PO ciprofloxacin therapy or comparator therapy were comparable.
28

The point resolved Co-rapporteur´s comment: Agreed 2.2 Question 2, Proposed changes to the SPC section 4.4 (Co-rapporteur) “It should be stated in the SPC section 4.4 “Special warning and precautions for use” that“ available safety data ……” disclose an incidence of drug-related arthropathy by 1-year follow-up of 8.2% among ciprofloxacin treated patients compared to 1.8% among patients treated with other antibiotics. Hence ciprofloxacin should be used only as second or third line treatment of complicated urinary infections and pyelonephritis in children.” MAH Response: Bayer agrees with the Co-rapporteur Denmark that a statement in the section 4.4 “Special Warnings and precautions for use” is appropriate and should be included in the final text proposal. Similar request were received from several Member States and these request should be discussed here as well to come to a final proposal. Other Member States who requested a similar statement are Hungary, Portugal and Sweden. A proposal for this section of the SPC based on the slightly modified proposal by MPA from Sweden is attached to this Consolidated Response Bayer believes that this SPC proposal meets the request for all countries involved: Denmark, Hungary, Portugal and Sweden. Rapporteur´s comment: MAH has taken into consideration the request to include a statement in the section 4.4. regarding the incidence of drug related arthropathy, as proposed by Sweden. Minor changes are recommended for the wording. Section 4.4 SPECIAL WARNINGS AND PRECAUTIONS FOR USE Pediatric use Ciprofloxacin has been shown to cause arthropathy in weight-bearing joints of immature animals. Safety data from a randomized double blind study on ciprofloxacin use in children (Ciprofloxacin: n=487, mean age = 6.2 y; comparators: n=507, mean age = 5.3 years; age range = 2 months to 16 years) revealed an incidence of suspected drug related arthropathy (discerned from joint-related clinical signs and symptoms) by Day +42 of 7.2% and 4.6%. Respectively, an incidence of drug-related arthropathy by 1-year follow-up was 9.0% and 5.7%. The increase of suspected drug related arthropathy over the time was not statistically significant between groups. Hence ciprofloxacin should be used only as second or third line treatment of complicated urinary infections and pyelonephritis in children. The use of ciprofloxacin for indications other than the treatment of acute pulmonary exacerbation of cystic fibrosis caused by P. aeruginosa infection (children aged 5 – 17 years), complicated urinary tract
29

infections and pyelonephritis (children aged 1 – 17 years) and for the use in inhalational anthrax (post-exposure) has not been evaluated in clinical trials and the clinical experience is limited. Inhalational anthrax (post-exposure) in adults and children…. (as proposed nationally) The point unresolved. Co-rapporteur´s comment: Agreed 3.1 Question 1, Clinical assessment (Belgium) “The statement in section 4.1 Indications “The use of Ciproxin in paediatric patients with complicated urinary tract infections and pyelonephritis should be restricted to treatment of infections caused by organisms for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data (see 4.4)” is not acceptable. Section 4.4 does not provide any information about the in vitro susceptibility of pathogens. This information should be available in section 5.1 (cf. CPMP/EWP/558/95 rev 1). Furthermore, the information related to the in vitro susceptibility does not allow to conclude that ciprofloxacin is the treatment of choice for some pathogens. Section 4.1 should clearly indicate that ciprofloxacin is a 2nd or 3rd line treatment for complicated urinary tract infections and pyelonephritis due to E.coli or other susceptible Gram negative pathogens in children aged 1-17 years, and for treatment of acute pulmonary exacerbation of cystic fibrosis associated with Pseudomonas aeruginosa in children aged 5-17 years.” MAH Response: In line with the comments by Belgium the following wording is proposed for section 4.1 Therapeutic indications: Ciprofloxacin may be used in children for the 2nd and 3rd line treatment of complicated urinary tract infections and pyelonephritis due to E. coli and other susceptible pathogens and for the treatment of acute pulmonary exacerbation of cystic fibrosis associated with Pseudomonas aeruginosa in children aged 5-17 years. This text is in line with the proposal made in the original application and slightly modified by the addition of the words “and other susceptible pathogens” for the indication complicated urinary tract infections and pyelonephritis. The word gram-negative has been deleted from this statement as Ciprofloxacin shows activity against gram-positive pathogens, e.g. staphylococci and streptococci, as well. As requested it is clearly indicated that ciprofloxacin in children should only be used as 2nd or 3rd line treatment. The reference to susceptibility data in section 4.4 ”Special warnings and precautions for use” has been deleted.
30

Rapporteur´s comment: MAH has taken into consideration the request made by Belgium to indicate clearly in 4.1 of the SPC that ciprofloxacin is a 2nd or 3rd line treatment for complicated urinary tract infections and pyelonephritis. However, the wording proposed for the SPC “due to E. coli or other susceptible Gram negative pathogens” is slightly confusing and Rapporteur proposes that the phrase “due to E. coli or other susceptible Gram negative pathogens” is left out for the reason that for urinary tract infections caused by E. coli in children in most cases benign treatment options are available and very seldom ciprofloxacin is the drug of choice in these cases. In clinical practise, ciprofloxacin is used in situations where no other treatment option is available, such as in urinary tract infection caused by Pseudomonas aerigunosa. We strongly support the request made by Belgium to provide data on in vitro susceptibility of pathogens and prevalence of acquired resistance, as stated in Note for Guidance on evaluation of medicinal products indicated for treatment of bacterial infections (cf. CPMP/EWP/558/95 rev 1) in 5.1. of the SPC. A following standard statement should be included before the table: “The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable.” The point unresolved. Co-rapporteur´s comment: Agreed 3.2 Question 2. Preclinical safety data (Belgium) “Articular tolerability studies As it is also known for other gyrase inhibitors, ciprofloxacin causes damage to the large, weight-bearing joints in immature animals. The extent of the cartilage damage varies according to age, species, and dose; the damage can be reduced by taking the weight off the joints. Studies with mature animals (rat, dog) revealed no evidence of cartilage lesions. In a study in young beagle dogs ciprofloxacin at high doses (1.3 to 3.5 times the therapeutic dose) at therapeutic and higher dose levels caused articular changes after two weeks of treatment, which were still observed after 5 months. At therapeutic doses no effects were observed.” MAH Response: A similar request for changes in the section 5.3 “Preclinical safety data” was made by BfArM (see 5.6, Question 6, Germany (With respect to pharmacology/toxicology)). The text “at high doses (1.3 to 3.5 times the therapeutic dose)” is deleted in the SPC. To indicate the doses applied in this preclinical study the following text is added: “at therapeutic doses”. As requested the sentence “At therapeutic doses no effects were observed.” has been deleted. The final wording is revised based on the comments from BfArM in Germany as well and therefore, some additional wording was added to also meet the requests by BfArM.
31

MAH proposal for section 5.3. of the SPC( Day 85): Section 5.3 PRECLINICAL SAFETY DATA Articular tolerability studies As reported for other gyrase inhibitors, ciprofloxacin causes damage to the large weight-bearing joints in immature animals. The extent of the cartilage damage varies according to age, species and dose; the damage can be reduced by taking the weight off the joints. Studies with mature animals (rat, dog) revealed no evidence of cartilage lesions. In a study in young beagle dogs ciprofloxacin caused severe articular changes at therapeutic doses after two weeks of treatment, which were still observed after 5 months. Although the juvenile dog is thought to be the most susceptible species to quinolone-induced arthropathy, a safety risk for pediatric patients cannot be excluded.” Rapporteur´s comment: MAH has taken into consideration the request and has changed the wording in 5.3. of the SPC accordingly. The point resolved. Co-rapporteur´s comment: Agreed 4. 1. Request to change the SPC text for the indication (France) “We do not agree with the proposed wording of the Therapeutic indications (section 4.1) in the ciprofloxacin SPC. We do not consider that the clinical study (study 100169) included in this dossier is sufficient to document a demonstration of efficacy in complicated UTI and results of this study should be mainly considered as additional safety paediatric data; this trial cannot be adequate to document efficacy in this indication : the qualification of complicated UTI in assessed patients is questionable because of the inclusion of UTI without fever, lower UTI with only risk factors, … ; it can be underlined that safety is the principal objective in the protocol whereas microbiological and efficacy assessments are described as second ones. Even if we consider that in exceptional severe UTI cases ciprofloxacin should be prescribed in children, we are not in favour of individualizing this infection among the whole severe infections where ciprofloxacin can be used. In fact we consider inappropriate to distinguish each severe infection, such as suggested by the inclusion of this additional indication (UTI) claimed in this paediatric dossier. Granting the indication the “UTI” indication will put emphasis on this situation whereas the use of ciprofloxacin could be considered in other future indications for which it is impossible to constitute a complete list because it will not cover all different acceptable situations which must be exceptional and very restricted. Therefore this will not be informative for prescribers. In addition, the granting of this specific indication only is particularly concerning taking into account the potential risk of a wide paediatric prescription of this antibiotic in this indication, and in consequence the associated risk of increase of bacterial resistance. In fact epidemiological consequences of a wide use of fluoroquinolones in UTI have to be taken into account regarding the risk of a rise of the percentage of E. coli resistant to quinolones. In community medicine, the widespread use of fluoroquinolones in UTI in adults has led to increased resistance in urinary bacteria as illustrated by the Spanish experience on resistance in E.coli. In countries where
32

ciprofloxacin is used in children, even if the number of prescriptions is low, the number of ciprofloxacin-resistant E.coli is growing. As a general consideration, we have to be very prudent in the paediatric prescriptions of ciprofloxacin considering the ability of common pathogens in children, to become resistant to fluoroquinolones if a medical attitude is not contained; we have to keep in mind that in adult medicine, where fluoroquinolones are widely used, the rates of fluoroquinolone resistance are increasing for most bacteria and the risk for the community is especially the emergence and dissemination of strains resistant to fluoroquinolones (pneumococci, E.coli). In line with the antibiotic policies and the good use of antibiotics, the restricted use of this pharmacological class must be promoted. Moreover, articular side-effects should be particularly considered in paediatrics with the use of fluoroquinolones. Consequently the proposed wording “second and third line treatment of complicated UTI and pyelonephritis due to E.coli ” is not satisfactory and is not acceptable regarding the submitted documentation and in view of the above microbiological considerations. Firstly the terms of “second and third line treatment” is not accurate and leaves a room for the interpretation of practioners; moreover, this information is more a result of an antibiotic strategy than an assessment of an efficacy demonstration through a clinical trial. Secondly restricting a ciprofloxacin use to pyelonephritis due to E. coli is questionable: the restricted use depends on MICs of bacteria with a particular interest for high MICs, it depends on micro-organisms other than E.coli such as P. aeruginosa, …; and we agree in this way with the Rapporteur to do not consider “E.coli” only. Finally regarding the SPC, we consider that cystic fibrosis and anthrax indications are of particular interest and should be maintained in a same wording in the section 4.1 such as already validated. UTI therapeutic indication should be deleted. Moreover we propose to delete the sentence: “The clinical trials in children were performed in the indications listed above; for other indications clinical experience is limited”, such as proposed by the Rapporteur. We propose to write in addition of both indications already allowed in children (cystic fibrosis and anthrax), a general indication targeted on exceptional severe infections, including notably UTI, with the following terms : “Ciprofloxacin may be used in children in exceptional cases of treatments for severe infections excepted in cystic fibrosis and excepted in anthrax, when other treatments cannot be used or after failure to conventional therapy, and when the microbiological documentation can justify a ciprofloxacin use.” The following sentence such as proposed by the company: “Treatment should only be initiated after careful benefit/risk evaluation due to possible adverse events related to joints and/or surrounding tissues” can be maintained and can be placed just after the above sentence. A cross reference to the section 4.4 should be introduced such as proposed by the Rapporteur. And in addition, a cross-reference to the section 5.1 should be included. In line with the “Note for guidance on evaluation of medicinal products indicated for treatment of bacterial infections” (CPMP/EWP/558/95 rev 1; october 2004) “Consideration should be given to official guidance on the appropriate use of antibacterial agents”, should be added at the end of the 4.1 SPC section. Referring to antibiotic recommendations constitutes an adequate response to the strategy of this antibiotic use and the need to promote a restricted prescription of ciprofloxacin. Finally, we propose the following structure for the paediatric paragraph of the 4.1 section of the SPC : “Children -Cystic fibrosis : … -Ciprofloxacin may be used in children in exceptional cases of treatments for severe infections, when other treatments cannot be used or after failure to conventional therapy, and when the microbiological documentation can justify a ciprofloxacin use. Treatment should only be initiated after careful
33

benefit/risk evaluation due to possible adverse events related to joints and/or surrounding tissues and considering the microbiological data (see sections 4.4 and 5.1). Specific situation Anthrax: .. Consideration should be given to official guidance on the appropriate use of antibacterial agents.” MAH Response: Indication The applicant believes that study 100169 appropriately supports the use of ciprofloxacin in the indication complicated urinary tract infections and acute uncomplicated pyelonephritis. Study 100169 focused both on efficacy and safety aspects of the use of ciprofloxacin in children. However, the use of ciprofloxacin in the indications applied for has been well established in clinical trials conducted in adults and as such has been an approved indication and medical practice for almost 20 years. The main difference between children and adults is the safety profile of the compound in children and therefore, study 100169 focused on safety without neglecting clinical efficacy as a main parameter in the study. The results of the study clearly showed non-inferiority for the indication and thus, supports the proposed wording for the SPC. The applicant’s proposed indication is in line with the current guidance on the Summary of Product Characteristics and with the proposed guidance for pediatric labeling in the EU. In this guidance it is stated that only those indications can be included in the SPC that have been studied in the pediatric population. As stated in the current guidance on the Summary of Product Characteristics dated October 2005: “Indications should be stated clearly and concisely and should define the target disease or condition. When appropriate it should define the target population especially when restrictions to patient populations apply.” In this respect the applicant already in this procedure wants to adhere to the current and upcoming EU guidance. Although the SPC text proposed by AFSSAPS is in line with the current SPC for Ciprofloxacin in France (see section 4.2 of the French SPC), the applicant, based on the guidance mentioned above, would like to propose the wording for the indication as in our original proposal. The applicant is well aware of the fact that fluoroquinolones may cause arthropathy in children. This was also seen in the preclinical study in juvenile dogs included in the application. Therefore, a wide use beyond the indication in the SPC is not promoted by the applicant. The use of ciprofloxacin for the treatment of complicated urinary tract infections should only be indicated for second or third line treatment, which clearly limits the usage to those cases where other drugs were not effective. Furthermore, the proposed wording limits the indication to those infections caused by pathogens susceptible for ciprofloxacin. The applicant strongly believes that this cautious SPC proposal does not advocate a wide spread use of ciprofloxacin for the treatment of these infections in children. As part of the original application a safety review made by FDA was submitted. This review was made over the period December 22, 2003 to January 31, 2005, evaluating all reports known to FDA, as part of the granting of pediatric exclusivity for ciprofloxacin in USA. In this review it is shown that, amongst others, adverse events in relation to arthropathy have been reported in children. FDA did not identifynew safety concerns in the pediatric population that are not adequately addressed in the labeling. The US Product Information is in alignment with the wording of the SPC proposal attached to this consolidated response. In line with the Note for guidance on evaluation of medicinal products indicated for treatment of bacterial infections” (CPMP/EWP/558/95 rev 1; October 2004) “Consideration should be given to official guidance on the appropriate use of antibacterial agents”, is added at the end of the 4.1 SPC section as requested by France.
34

Rapporteur´s comment: We fully agree with the concern presented by France related to emerging drug resistance related to the over use of fluoroquinolones and therefore, need for the prudent antimicrobial use. However, we disagree with the proposal of expanding the indication beyond urinary tract infections, in which Ciprofloxacin has shown to be efficacious and relatively safe. MAH should be more over encouraged to study efficacy and safety of ciprofloxacin properly in other indications in children. Like said previously, in clinical practice, Ciprofloxacin is widely used without labeling in urinary tract infections caused by less common pathogens, such as Pseudomonas aeruginosa. In urinary tract infections caused by E. coli, other treatment options are very often available. Therefore, the Rapporteur feels that the following wording emphasizes adequately that caution should be exercised when using Ciprofloxacin in children. Information regarding in vitro data of pathogens and prevalence of resistance provides clinician additional information for the decision making. “Ciprofloxacin may be used for the 2nd and 3rd line treatment of complicated urinary tract infections and pyelonephritis in children and adolescents 1-17 years of age and for the treatment of acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa in children and adolescents 5-17 years of age. The use of Ciproxin in paediatric patients with complicated urinary tract infections and pyelonephritis should be restricted to treatment of infections caused by organisms, for which Ciproxin is the drug of choice, based on antimicrobial sensitivity data. Treatment should be initiated by physician, who is experienced in the treatment of severe infections in children and adolescents and after careful benefit/risk evaluation, due to possible adverse events related to joints and/or surrounding tissues. (see 4.4. and 5.1)” The point unresolved. Co-rapporteur´s comment: Agreed with the Rapporteur 4.2 Request to revise section 4.2 of the SPC(France) “In line with the above position, the section 4.2 of the SPC should be revised. We propose to delete the paragraph targeted to UTI and to replace it by a paragraph restricted to severe infections other than cystic fibrosis and anthrax, with the following wording : - parenteral presentations : 7.5 mg/kg IV twice daily or three times daily (maximum of 400 mg per dose, and maximum daily dose : 1200 mg) depending on severity of infections in particular in life-threatening infections (nosocomial pneumonia, septicaemia, complicated UTI, …) and the susceptibility of the considered micro-organism (notably Pseudomonas aeruginosa sp.), following by an oral ciprofloxacin treatment : 10 to 15 mg/kg orally twice daily (maximum daily dose : 1500 mg); - oral presentations : 10 to 15 mg/kg orally twice daily (maximum daily dose :1500 mg) directly or after an IV ciprofloxacin treatment. For both presentations, we suggest to add after this paragraph : “Treatment by ciprofloxacin should be started in an hospital environment.”
35

MAH Response: The adaptation of the section 4.2 of the SPC “Posology and method of administration” is directly related to the section 4.1 “Therapeutic indications”. Therefore, we would like to refer to 4.1 Question 1, France. The applicant prefers to maintain the indication for ciprofloxacin as proposed by the applicant in the original application, based on the available data and the reasons outlined in our response to question 4.1. Rapporteur´s comment: We agree with the proposal by the MAH concerning 4.2. of the SPC. However, E. coli should be deleted from the sentence “For complicated urinary tract infections or pyelonephritis due to E. coli the duration of treatment is 10-21 days.” (see below). Section 4.2 POSOLOGY AND METHOD OF ADMINISTRATION Cystic fibrosis Clinical and pharmacokinetic data support the use of ciprofloxacin in pediatric cystic fibrosis patients (aged 5-17 years) with acute pulmonary exacerbation associated with P. aeruginosa infection, at a dose of 20 mg/kg orally twice daily (maximum daily dose 1500 mg) or 10 mg/kg IV three times daily (maximum daily dose 1200 mg). Complicated urinary tract infections and pyelonephritis For complicated urinary tract infections or pyelonephritis the dose is 6 to 10 mg/kg IV every 8 hours with a maximum of 400 mg per dose or 10 to 20 mg/kg orally every 12 hours with a maximum of 750 mg per dose. Inhalational anthrax (post-exposure) Children: Oral administration: 15mg/kg twice daily. The maximum of 500mg per dose should not be exceeded (maximum daily dose of 1000mg). Intravenous administration: 10mg i.v./kg twice daily. The maximum of 400 mg i.v. per dose should not be exceeded (maximum daily dose of 800mg). Drug administration should begin as soon as possible after suspected or confirmed exposure. Duration of treatment Children: Cystic fibrosis For acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa infection in pediatric patients (aged 5-17 years), the duration of treatment is 10-14 days. Complicated urinary tract infections and pyelonephritis For complicated urinary tract infections or pyelonephritis due to E. coli the duration of treatment is 10-21 days. Inhalational anthrax (post-exposure) in adults and children: The total duration of treatment of inhalational anthrax (post-exposure) with ciprofloxacin (i.v. or oral) is 60 days. Renal and hepatic impairment
36

Children: Dosing in children with impaired renal and or hepatic function has not been studied. The point unresolved. Co-rapporteur´s comment: We agree with the Rapporteur. However, in the paragraph concerning treatment duration, if “Cystic fibrosis” is a heading the complicated urinary tract infections and pyelonephritis” should also be a heading. 4.3 Request to revise Section 4.4. of the SPC (France)
The section 4.4 of the SPC should be reviewed. We propose to delete the sentence : “The use of
AH Response: the section 4.4 of the SPC “Special warnings and precautions for use” is directly
“ciprofloxacin for indications other than the treatment of acute pulmonary exacerbation of cystic fibrosis caused by P. aeruginosa infection (children aged 5-17 years), complicated urinary tract infections and pyelonephritis due to E.coli (children aged 1-17 years) and for the use in inhalational anthrax (post-exposure), was not studied. For other indications, clinical experience is limited”. We propose the following wording for the paragraph 4.4 targeted on the paediatric use: “Paediatric use As with drugs in its class, ciprofloxacin has been shown to cause arthropathy in weightbearing joints of immature animals …. articular damage. Moreover prescription of ciprofloxacin should be very carefully considered regarding the microbiological risk of a non-restricted use of this antibiotic, and this epidemiological risk could be greater if broader use of fluoroquinolones is observed. As a matter of fact, a prudent paediatrics use of ciprofloxacin is encouraged considering the ability of pathogens common in children to become resistant to fluoroquinolones. Consequently the benefit-risk ratio should be taken into account before any ciprofloxacin paediatric prescription.” MThe adaptation ofrelated to the section 4.1 “Therapeutic indications”. Therefore, we would like to refer to 4.1, Question 1, France. The applicant prefers to maintain the indication for ciprofloxacin as proposed by the applicant in the original application, based on the available data and the reasons outlined in our response to question 4.1. Rapporteur´s comment: We agree with the proposal by the MAH concerning 4.4.of the SPC. The reasoning has been giving in responses to questions 2 and 3. Co-rapporteur´s comment: Agreed 4.4 Safety issues (France)
37

“Further to the results of the two studies submitted, two safety concerns remain :
mpany should submit
e UTI, some paediatric patients might receive repeated courses of
AH Response: low-up data for study 100225 will not be available until after study completion. The
- data on long-term follow-up related to study 100225 are not available. The cothese results as soon as available, - according to the aetiology of thciprofloxacin treatment; however, no data on repeated treatments of ciprofloxacin in paediatrics is available. A wide use of ciprofloxacin in paediatrics patients can not be excluded particularly if the claimed indications are granted. In order to monitor the use of this anti-infective, the MAH should propose a risk management plan including at least annual reports gathering cases reported in paediatric population, paediatric exposure and ciprofloxacin usage patterns in this population (indications, dosages…).” MThe long-term follast patient’s last visit for this study is scheduled to take place in 2008, after which, final results will be reported. In the meantime all relevant data are submitted according to current rules and regulations. The data on long-term follow-up from study 100225 will be submitted as soon as the final report for this study is available. Prior and post use of ciprofloxacin and other quinolones was collected during both the cUTI and observational studies. The rates of arthropathy based on previous and post quinolone use was as follows:
38

Although repeated use can not be excluded, there are no data available that allow an assessment of repeated use and inclusion of a statement in the SPC. Based on Bayer’s experience in the USA with the use of ciprofloxacin in this indication, wide spread use is not foreseen. In the USA, the usage of ciprofloxacin in pediatric patients is closely monitored and reported every year to FDA as part of the approval commitments for this indication. This is in line with the wording of the indication that ciprofloxacin should only be used for second or third line treatment of cUTI in children. The adverse event reported in pediatric patients are also presented and discussed in a separate section in the PSUR for ciprofloxacin, compiled every 6 months. Therefore, Bayer is of the opinion that based on our current activities for this indication and for ciprofloxacin in general, Bayer is adequately monitoring the pediatric use of ciprofloxacin as suggested by AFSSAPS.
39

Rapporteur´s comment: MAH has responded adequately to the question and is committed to monitor the pediatric use of ciprofloxacin as suggested by AFSSAPS. The point resolved. Co-rapporteur´s comment: We agree that the response by the MAH is adequate; however, we worry about the results presented in the tables. Children treated with quinolone before or after the study-treatment have a higher frequency of arthropathy, but the number of children is very small and it may not be possible to make any relevant statistical analysis. If the tendency becomes even more clear during the continuous observation, it should appear from the SPC. 5.1. Pharmacokinetics and pharmacodynamics (Germany) “Depending on the indication the use in children is restricted to children for 5-17 years for treatment of acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa whereas for the 2nd and 3rd line treatment of complicated urinary tract infections and pyelonephritis it is indicated for children with an age range of 1-17 years. Is there any pharmacokinetic or clinical data suggesting that children of 1-4 years should not be treated for the indication “acute pulmonary exacerbation of cystic fibrosis”?” MAH Response: At the time Bayer conducted the clinical trial in Cystic Fibrosis subjects (September 1991-April 1995), patients under the age of five were not included primarily because pulmonary function tests in children under 5 years of age are not reliable (1) and because the children had to be able to swallow tablets. The CF study preceded the development of a pediatric suspension of ciprofloxacin, which was approved in the USA in September of 1997. The current pharmacokinetic and clinical data justify a positive risk benefit assessment for ciprofloxacin in this patient group (children 1-4 year of age with ‘acute pulmonary exacerbation of cystic fibrosis'). Reference 1. Behrman RE, Kliegman RM, Jenson HB. Nelson Textbook of Pediatrics. 15th Edition, Philadelphia, Pennsylvania: WB Saunders Company; 1996: 1243. Rapporteur´s comment: MAH has responded adequately to the question and provided the knowledge that current pharmacokinetic and clinical data justify a positive risk benefit assessment for ciprofloxacin in children 1-4 year of age with acute pulmonary exacerbation of cystic fibrosis. However, in the current submission, there was no data provided for the treatment of acute pulmonary exacerbation of cystic
40

fibrosis associated with P. aeruginosa infection in paediatric patients of any age. Therefore, this issue has to dealt separately in forthcoming procedures. The point resolved. Co-rapporteur´s comment: Agreed 5.2.Pharmacokinetics and pharmacodynamics (Germany) “Study BAY 3939/0553 (10 mg/kg ciprofloxacin infused) and the study by Peltola et al. (1992) (15 mg/kg ciprofloxacin orally) show significant differences concerning the crucial pharmacokinetic parameters (Cmax, AUC and t1/2) of children of 1-5 years. This should be discussed. As in the clinical efficacy study 100169 patients were stratified with respect to the mode of administration (oral or i.v. treatment), efficacy results should be presented respectively to the strata.” MAH Response: The two studies show indeed differences in the main pharmacokinetic parameters (Table 5-1) although one can expect similar pharmacokinetic results after a 15 mg/kg oral vs. a 10 mg/kg intravenous dose based on bioavailability considerations. They can not be explained by the different forms of administration alone. In the study by Peltola et al. (2) the exposure (AUC) and the terminal half life were lower than in the study 0553 (3), while the difference in the peak concentrations can be explained by the slower input rate following oral administration of the drug. A possible reason for this difference in exposure (AUC) could be that there was incomplete absorption of the drug in the patient population. The author himself speculates about physiological changes as a function of age and alterations in the GI tract due to the underlying disease (2), since most of his study participants were suffering from Salmonella spp. infections (e.g. impaired absorption due to expedited gastric motility or inflammatory processes in the gut). Another reason could be in the inadequacy of the dosage form which had to be used in the study for application to pediatric patients: The investigator had to crush tablets and administer them as a slurry. Since ciprofloxacin is known to exhibit a very bitter taste, compliance of the patients –although tablet ingestion was visually controlled by the study personal - could have been a problem. These hypotheses are supported by a later study of the same investigator (1998, 4) where he used a ciprofloxacin suspension, (which is a bioequivalent alternative oral dosage form) especially designed to avoid bitter taste, in a similar cohort of patients aged 2 -5 years. The resulting pharmacokinetic parameters (Table 5-2) are comparable to those in study 0553 and indicate that age related differences in the pharmacokinetics in children aged 1 -5 years seem to be unlikely. This in accord with own investigations (5). Thus, the (speculative) conclusion that impaired absorption of the ground tablet formulation occurred in the study by Peltola is the most reasonable explanation for the observed differences. The apparent differences in the half life seen between the Peltola data and the study 0533 (Table 5-1) are explained by the fact that the windows described by the data is not identical. Due to the lower concentrations measured by Peltola, the half life calculated in his study reflects partly an earlier phase in the plasma concentration time profile with fast distribution processes ongoing. In conclusion, the data indicate that in infections where one has to expect potential absorption problems due to medical reasons, intravenous administration of ciprofloxacin should be the method of choice to guarantee therapeutic drug concentrations.
41

42

MAH`s proposal for 5.2. of the SPC: Section 5.2 PHARMACOKINETIC PROPERTIES Children In a study in children Cmax and AUC were not age-dependent. No notable increase in Cmax and AUC upon multiple dosing (10 mg/kg three times daily) was observed. In 10 children with severe sepsis, less than 1 year of age Cmax was 6.1 mg/L (range 4.6 – 8.3 mg/L) after a 1-hour intravenous infusion at a dose level of 10 mg/kg; and 7.2 mg/L (range 4.7 – 11.8 mg/L) for children between 1 and 5 years of age. The AUCvalues were 17.4 mg*h/L (range 11.8 – 32.0 mg*h/L) and 16.5 mg*h/L (range 11.0 – 23.8 mg*h/L)in the respective age groups. These values are within the range reported for adults at therapeutic doses. Based on population pharmacokinetic analysis of pediatric patients with various infections, the predicted mean half-life in children is approx. 4 –5 hours and the bioavailability of the oral suspension approx. 60%. Rapporteur´s comment: The reasoning given by the MAH that the observed differences between two studies could be explained by the fact that in a study by Peltola, crushed tablets were given as a slurry for children 1-5 years of age resulting possible impaired absorption, seems reasonable. The current SPC provides adequate dosing for both oral and intravenous administration for a clinician, who ultimately determines on clinical bases whether ciprofloxacin is given orally or intravenously. The proposal for 5.2.of the SPC is adequate. The point resolved. Co-rapporteur´s comment: Agreed 5.3.Ppharmacokinetics and pharmacodynamics (Germany) “As presented on page 16 of the AR of the Rapporteur, pharmacokinetics of group A and group B in study BAY 3939/0553 seem comparable for children of 3-11 months (group A) and children of 1-5 years (group B). It should be discussed why children younger than 1 year should not be treated with ciprofloxacin.” MAH Response: Bayer does not recommend the use of ciprofloxacin in children younger than 1 year of age because of the lack of clinical efficacy and safety data for ciprofloxacin in this age group. Patients who were under 1 year of age were excluded from the 100169 cUTI study because in this age group, the patients were unlikely to be walking (and hence not weight bearing on their joints) thus making it difficult to identify the presence of drug-related arthropathy. Also, serial gait joint exams may also have been less reliable over time in these young patients. Finally, pre-verbal children are unable to articulate any subjective measure of pain. Thus, it was felt that, in an effort to obtain the most reliable safety information, children under the age of one year should not be included in the clinical trial. Furthermore, children
43

under the age of 1 year have a milk based diet and for these children oral treatment with ciprofloxacin is considered unsuitable. This is based on the fact that milk and dairy products interfere with the absorption of ciprofloxacin from the gastro-intestinal tract as described in the current SPC in the sections 4.2 “Posology and method of administration” and 4.5 “Interactions with other medicaments and other forms of interaction”. Rapporteur´s comment: MAH has responded adequately to the question and provided sufficient amount of justifications, among them the lack of efficacy and safety data, why ciprofloxacin cannot be considered adequate therapy for infants less than one year at this point. The point is resolved. Co-rapporteur´s comment: Agreed 5.4.Pharmacokinetics and pharmacodynamics (Germany) “As there was a 1-year follow-up in study 100169, safety results with confidence intervals should be presented and discussed for this late follow-up visit.” MAH Response: The rates of suspected arthropathy at one year are presented in the table below. The rate of arthropathy, as assessed by the independent safety committee was 13.73% in ciprofloxacin-treated and 9.74% in comparator-treated patients. This difference was not statistically significant as the 95% Confidence interval was: -0.8, 8.9%.
44
Rapporteur´s comment: We refer to our response in 2.2. MAH has adequately revised the 4.4. of the SPC. The point resolved. Co-rapporteur´s comment: Agreed 5.5. Request of revision of the SPC (Germany) “The safety results from study 100169 indicating a higher incidence of arthropathy in the ciprofloxacin arm than in the comparator arm should be mentioned in section 4.4 “special warnings and precautions for use”. Prophylaxis and treatment of anthrax: Indication and posology and method of administration for children should be mentioned in sections 4.1 and 4.2 of the SPC.” MAH Response: A similar request is part of the evaluation by Co-Rapporteur Denmark and is discussed in detail in 2.2, Question 2, Co-Rapporteur, Denmark (VI. Proposed changes to the SPC). The text of SPC is adapted as requested by BfArM and the frequencies as requested are included in the proposal for the SPC attached to this Consolidated Response. The indication Anthrax was not discussed as part of this application, but will be included in the final SPC proposal. Rapporteur´s comment: MAH has responded adequately to the question and has adequately revised the 4.4. of the SPC. The point is resolved. Co-rapporteur´s comment: Agreed 5.6. Pharmacology/toxicology (Germany) “Comment on the proposed wording for SPC section 5.3 Preclinical safety data In a preclinical study with juvenile beagle dogs the NOAEL for severe adverse cartilage effects was 10 mg/kg. The lesions in the articular cartilage were not reversible but rather progressed during follow-up period. According to population based pharmacokinetic modelling the expected exposure of children is higher than NOAEL for cartilage adverse effects in beagle dogs. I.e., the highest expected human exposures to ciprofloxacin are within same magnitude as the doses producing adverse effects in beagle dogs and therefore there is no safety margin. From our point of view the safety concerns arising from the juvenile dog study and the lack of any safety margin have not been adequately addressed in the proposed labeling. Therefore, we would like to propose the following wording:
45

5.3. Preclinical safety data of the SPC Articular tolerability studies As it is also known for other gyrase inhibitors, ciprofloxacin causes damage to the large, weight-bearing joints in immature animals. The extent of the cartilage damage varies according to age, species, and dose; the damage can be reduced by taking the weight off the joints. Studies with mature animals (rat, dog) revealed no evidence of cartilage lesions. In a study in young beagle dogs ciprofloxacin at high doses (1.3 to 3.5 times the therapeutic dose) caused severe articular changes at therapeutic doses after two weeks of treatment, which were still observed after 5 months. At therapeutic doses no effects were observed. Although the juvenile dog is thought to be the most susceptible species to quinolone induced arthropathy, a safety risk for pediatric patients can not be excluded.“ MAH Response: The proposal is acceptable for Bayer and is included in the final SPC proposal attached to this Consolidated Response. Rapporteur´s comment: MAH has responded adequately to the question and has adequately revised the 5.3. of the SPC. The point is resolved. Co-rapporteur´s comment: Agreed 6.1. Proposed changes to the SPC (Hungary) “Safety data from a randomized double-blinded study on ciprofloxacin use in patients less than 18 years of age disclose an incidence of drug related arthropathy by Day +42 of 7.2% and 4.6% and by 1 year follow-up of 9.0% and 5.7%, among Ciproxin treated patients and patients treated with comparator drugs, respectively.” MAH Response: A similar request is part of the evaluation by Co-rapporteur Denmark and is discussed in detail in 2.1, Question 2, Co-rapporteur. The text as requested by the Hungarian Health Authorities is accepted by Bayer and has been included in our proposal for the SPC. Rapporteur´s comment: MAH has responded adequately to the question and has adequately revised the 4.4.of the SPC. The point is resolved. Co-rapporteur´s comment: Agreed
46

7.1.Request of revision of section 4.4.(Portugal) “We are aware that there is an incidence of drug related arthropathy by 1 – year follow-up of 8.2% among ciprofloxacin treated patients compared to 1.8% among patients treated with other antibiotics. As suggested by the Co-Rapporteur this information should be mentioned in section 4.4 “Special warning and precautions of use”. MAH Response: A similar request is part of the evaluation by Co-rapporteur Denmark and is discussed in detail in 2.1, Question 2, Co-rapporteur. The text as requested by INFARMED is accepted by Bayer and has been included in our proposal for the SPC. Rapporteur´s comment: MAH has responded adequately to the question and has adequately revised the 4.4.of the SPC. The point is resolved. Co-rapporteur´s comment: Agreed 8.1. Request of revision of wording in section 4.4 (Sweden) “The following wording in section 4.4 is suggested: Pediatric use As with drugs in its class, ciprofloxacin has been shown to cause arthropathy in weightbearing joints of immature animals. Safety data from a randomized double-blinded study on ciprofloxacin use in patients less than 18 years of age disclose an incidence of drug related arthropathy by Day +42 of 7.2% and 4.6% and by 1 year follow-up of 9.0% and 5.7%, among Ciproxin treated patients and patients treated with comparator drugs, respectively. The analysis of available safety data from ciprofloxacin use in patients less than 18 years of age, the majority of whom had cystic fibrosis, did not disclose any evidence of drug related cartilage or artricular damage. The use of ciprofloxacin for indications other than the treatment of acute pulmonary exacerbation of cystic fibrosis caused by P. aeruginosa infection (children aged 5 – 17 years), complicated urinary tract infections and pyelonephritis (children aged 1 – 17 years) and for the use in inhalational anthrax (post-exposure) was not studied. For other indications clinical experience is limited.” MAH Response: A similar request is part of the evaluation by Co-rapporteur Denmark and is discussed in detail in 2.1, Question 2, Co-rapporteur, Denmark ( Proposed changes to the SPC). The text as requested by MPA is accepted by Bayer and has been included in our proposal for the SPC attached to this Consolidated Response.
47

Rapporteur´s comment: The proposal made by Sweden to include long-term safety data rather from the pivotal study 100169 than from open observational study 100225 is endorsed. MAH has responded adequately to the proposal and has adequately revised the 4.4.of the SPC. The point is resolved. Co-rapporteur´s comment: Agreed COMMENTS TO THE PROPOSED SPC (Day 96) The applicant submitted the response to Day 96 comments/requests made by Belgium, France, Germany, Netherlands and United Kingdom. In the consolidated response the applicant addressed the points raised by the Member States and submitted in the response the proposal for the revised wording of the SPC. All objections are related to the SPC proposal and are discussed in the same order as they presented in the SPC. Section 4.1. Therapeutic Indications. Belgium disagreed with the proposed revised wording of the indications. France commented on the focus on the UTI indication for which specific clinical data have been submitted. In addition France commented that they were not comfortable with the way the UTI indication is mentioned (i.e. 2nd or 3d line treatment), that such a wording might not be clinically meaningful. The UK endorsed with the proposals by Rapporteur and Co-rapporteur that the application of Ciproxin as a 2nd and 3rd line treatment of complicated urinary tract infection and pyelonephritis in paediatric patients 1 to 17 years of age is approvable. The UK also commented on the wording of the indication and agreed with the Rapporteur’s proposal to delete the phrase ‘due to E. Coli or other susceptible Gram negative pathogens’. The UK endorsed the Rapporteur’s and Co-rapporteur’s view that the expansion of the indication should not go beyond urinary tract infections were ciprofloxacin was shown to be efficacious and relatively safe. The Netherlands endorsed the change of the wording of the indication for cUTI patients and endorsed the comment by Belgium. Rapporteurs comment: MAH has addressed adequately the concerns raised by Belgium and has taken into account all the comments made by other member states, such as France, and based on those comments/requests has revised the 4.1.of the SPC. In the proposed SPC, the use of Ciproxin is restricted for extreme occasions when hardly any other options are available (“2nd or 3rd line treatment”/”complicated urinary tract infections and pyelonehritis”/”restricted to infections caused by organisms, for which Ciproxin is the drug of choice”/”based on antimicrobial susceptibility testing”/”initiated by physician, who is experienced in the treatment of severe infections in children and adolescents”/ “and after careful
48

benefit/risk evaluation”. The current wording emphasizes adequately that the process of initiating this medication should be based on very thorough decision-making taking into account all the risks and benefits. France has raised a relevant point that Ciproxin could be useful in treating other life-threatening infections, as well. However, further studies are needed to address this issue and MAH is encouraged to study efficacy and safety of ciprofloxacin properly in other indications in children. The proposed wording of the SPC, summits the comments given by different MS, such as Germany, the UK etc and therefore the Rapporteur endorses the proposed wording The point resolved Co-rapporteur´s comment: Agreed
Section 4.2. Posology and method of administration France commented that the lower doses (IV+oral) are expected to be adequate in most of the UTI considering the known susceptibility of the most common pathogen involved (E. Coli). Low doses might not be sufficient in some other Urinary Tract Infections (in particular due to Pseudomonas aeruginosa). A statement would deserve to be added for encouraging the use of the highest doses in such cases. The applicant acknowledges the valuable comments by France, which indicate that there is a medical need for individual cases of severe and life-threatening infections in children for which treatment with ciprofloxacin can be life saving. However, the clinical data as submitted by the applicant in the frame work of this EU work sharing project for the assessment of pediatric data of existing products do not substantiate the wording for the SPC as proposed here and as a consequence can not be included in the SPC. Section 4.2. proposed by France is not in accordance with the section 4.1 Indications, which is limited to complicated urinary tract infections and pyelonephritis. This point is not in line with the EU SmPC guideline. The Netherlands commented that the presently proposed advice on the posology and administration of the inhalation anthrax (post-exposure) cannot be endorsed. The applicant refers to the response on the comments by the Netherlands under section 4.1 Indications.
Rapporter´s comment: The point resolved. Co-rapporteur comment: Agreed
49

4.4 Special warnings and precautions for use Belgium commented on that in section 4.4 the differences observed in the incidence of drug-related arthropathy when compared with other antibiotics (8.2% versus 1.8%) should be mentioned..
Bayer agrees with the assessor that information on the incidence rate of drug-related arthropathy in children should be included in the section 4.4 Warnings and precautions of the SPC to reflect that this adverse event occurs more frequent in children than in adults. In the SPC proposal attached to the final assessment report for this procedure, numbers have been included in this section. Additionally, to reflect the dependence of the occurrence of this adverse event, data at two points in time were included in this section of the SPC.
Rapporteur´s comment: MAH has adequately addressed the issue and has revised the SPC accordingly. The point resolved. Co-rapporteur´s comment: Agreed France commented on the incidences of athropathy that were proposed to be added in section 4.4. The applicant proposes to replace the last sentence by a wording indicating that for the initiation of the treatment of children with ciprofloxacin a careful risk/benefit evaluation is needed to improve consistency within the SPC.
The Netherlands commented on: Inhalational anthrax (post-exposure) in adults and children…. (as proposed nationally) The response on the Comments by the Netherlands under section 4.1 Indications. The applicant agrees with the proposal in the final assessment report by the Rapporteur and the Co-rapporteur and the SPC has been revised. Rapporteur´s comment: MAH has adequately addressed the issue raised by France and revised the SPC. Comments related to inhalational anthrax are dealt separately within each MS. The point resolved. Co-rapporteur´s comment: Agreed
4.8 Adverse events Belgium commented on that the incidences of adverse events are based on information overwhelmingly collected from adults, not from children. Since the incidence of arthropathy is linked to age, the incidence of this particular adverse event should be given separately for adults on one hand and subjects up to 17 years old on the other. The applicant agrees with the assessor that this section is based on clinical trials in adults and that it is appropriate to state the higher incidence rate of arthropathy in the pediatric population in the SPC.
50

Rapporteur´s comment: Belgium has raised an adequate point and MAH has responded by revising the SPC in section 4.8. The point resolved. Co-rapporteur comment: Agreed
5.2 Pharmacokinetic properties
Belgium raised the issue of that when administering ciprofloxacin intravenously to children 1-5 years old in a dose of 10 mg/kg over 60 minutes, peak levels equal to or above 10 mg/l were observed. How many children in this age group demonstrated such levels and safety problem when exceeding plasma levels equal to or above 10 mg/l.
Applicant’s response: The data presented in section 5.2 for pediatric pharmacokinetics indicate that values for Cmax are observed between 4.7 and 11.8 mg/l after administration of ciprofloxacin at a dose level of 10 mg/kg to children in the age of 1 to 5 years. Until now a concentration threshold for ciprofloxacin has only been discussed in papers dealing with safety of ciprofloxacin in CAPD patients. Since these patients exhibit a longer ciprofloxacin plasma half life, due to the missing renal clearance, they are at higher risk compared to patients with normal renal function when exceeding a certain threshold level. This level may be considered as a good surrogate for total drug exposure in this special subpopulation; however, its use has never been validated in other patient groups and may therefore be probably not applicable. In the pharmacovigilance database for ciprofloxacin adverse events are related to dose, but not to plasma levels.
The data in this section of the SPC present the values for AUC and Cmax observed in a limited number of severely ill patients. The main objective of this study was to show that pharmacokinetical behaviour of ciprofloxacin in this small patient group is consistent with that generally known for ciprofloxacin in adults.
Overall, pharmacokinetic data in children receiving 10 mg/kg bid intravenous ciprofloxacin were collected in 357 patients participating in six clinical trials. Seventeen of these 357 patients were in the age range of 1 to 5 years. Only two patients (both in the 1-5 year age range) had plasma concentrations above 10 mg/L (corresponds to 12%). These were not associated with drug related serious adverse events. In view of the low number of cases obtained from these clinical trials a PK evaluation based on population pharmacokinetic methods was performed to get a better estimate of the percentage of patients exceeding the 10 mg/L threshold [1]. The results of the evaluation are given in figure 1. They indicate that approximately 6.3 % of 1 year old patients, 8.4 % of 3 year old patients and 9.6 % of 5 year old patients are expected to exhibit peak ciprofloxacin plasma levels greater than 10 mg/L after a 1 hour infusion of 10 mg/kg of ciprofloxacin. This rate can be reduced significantly by applying longer infusion times (e.g. the rate of patients beyond 10mg/L will drop below 1% for an infusion time of 2h)
51

Clinical data did not reveal any major adverse reactions with any of the doses applied in these studies and therefore, the risk benefit assessment of these doses in these indications is positive (for reference see the expert report presented as part of this application.
Rapporteur´s comment: MAH has presented additional distribution data and references that show Ciproxin does not cause any additional safety concerns. The point can be considered resolved. Co-rapporteur´s comment: Agreed.
Comments made by France regarding revision in SPC were regarding age dependence and that the pharmacokinetic parameters proposed are derived from studies suffering from significant limitations, and that this should be made it clear for prescribers, that the values mentioned might not be accurate. For bioavailability of the oral suspension it was suggested to be more appropriate to mention a range rather than a value.
The comments made by France are included in the SPC.
Rapporteur´s comment: France has raised some valuable comments and MAH has responded to them adequately. The point can be considered resolved. Co-rapporteur´s comment: Agreed.
5.3 Preclinical Safety Data
France commented that the last sentence of the paragraph pertaining to Articular tolerability studies (in particular the statement “a safety risk for pediatric patients cannot be excluded”) is falsely reassuring and should be deleted.
The applicant agreed to take out the sentence from the paragraph. The text in the SPC is revised.
Rapporter´s comment: MAH has adequately revised the 5.3.of the SPC. The proposed wording is acceptable. The point can be considered resolved. Co-rapporteur´s comment: Agreed.
52

CONCLUSION: The EU Worksharing Project assessment of Paediatric data for Ciproxin ended on June 15th, 2006, (Day 120) succesfully. All the MSs agreed with the proposed SPC. It was agreed that the applicant is requested to submit national Type II variation to MSs to implement the amendments to the SPC agreed upon during the procedure. The SPC with the final changes is enclosed (Attachment 1).
53

Attachment 1
FINAL SPC CHANGES 4.1 THERAPEUTIC INDICATIONS
“Children Ciprofloxacin may be used for the 2nd and 3rd line treatment of complicated urinary tract infections and pyelonephritis in children and adolescents 1-17 years of age and for the treatment of acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa in children and adolescents 5-17 years of age. The use of Ciproxin in paediatric patients with complicated urinary tract infections and pyelonephritis should be restricted to infections caused by organisms, for which Ciproxin is the drug of choice, based on the results of antimicrobial susceptibility testing. Treatment should be initiated by physician, who is experienced in the treatment of severe infections in children and adolescents and after careful benefit/risk evaluation, due to possible adverse events related to joints and/or surrounding tissues. (see 4.4. and 5.1.).
Inhalational anthrax (post-exposure) in adults and in children: (as approved nationally in each member state)….
[Last sentence of the paragraph:] Consideration should be given to official guidance on the appropriate use of antibacterial agents.”
4.2 POSOLOGY AND METHOD OF ADMINISTRATION
Cystic fibrosis Clinical and pharmacokinetic data support the use of ciprofloxacin in pediatric cystic fibrosis patients (aged 5-17 years) with acute pulmonary exacerbation associated with P. aeruginosa infection, at a dose of 20 mg/kg orally twice daily (maximum daily dose 1500 mg) or 10 mg/kg IV three times daily (maximum daily dose 1200 mg).
Complicated urinary tract infections and pyelonephritis For complicated urinary tract infections or pyelonephritis the dose is 6 to 10 mg/kg IV every 8 hours with a maximum of 400 mg per dose or 10 to 20 mg/kg orally every 12 hours with a maximum of 750 mg per dose.
Inhalational anthrax (post-exposure) (as approved nationally in each member state)….
Duration of treatment
Children: Cystic fibrosis
54

For acute pulmonary exacerbation of cystic fibrosis associated with P. aeruginosa infection in pediatric patients (aged 5-17 years), the duration of treatment is 10-14 days.
Complicated urinary tract infections and pyelonephritis For complicated urinary tract infections or pyelonephritis the duration of treatment is 10-21 days.
Inhalational anthrax (post-exposure) in adults and children: (as approved nationally in each member state)….
Renal and hepatic impairment Children: Dosing in children with impaired renal and or hepatic function has not been studied.
4.4 SPECIAL WARNINGS AND PRECAUTIONS FOR USE
Pediatric use Ciprofloxacin has been shown to cause arthropathy in weight-bearing joints of immature animals. Safety data from a randomized double blind study on ciprofloxacin use in children (Ciprofloxacin: n=335, mean age = 6.3 years; comparators: n=349, mean age = 6.2 years; age range = 1 to 17 years) revealed an incidence of suspected drug related arthropathy (discerned from joint-related clinical signs and symptoms) by Day +42 of 7.2% and 4.6%. Respectively, an incidence of drug-related arthropathy by 1-year follow-up was 9.0% and 5.7%. The increase of suspected drug related arthropathy over the time was not statistically significant between groups. Treatment should only be initiated after a careful benefit/risk evaluation, due to possible adverse events related to joints and/or surrounding tissue.
The use of ciprofloxacin for indications other than the treatment of acute pulmonary exacerbation of cystic fibrosis caused by P. aeruginosa infection (children aged 5 – 17 years), complicated urinary tract infections and pyelonephritis (children aged 1 – 17 years) and for the use in inhalational anthrax (post-exposure) has not been evaluated in clinical trials and the clinical experience is limited. The use of Ciprofloxacin should follow the official guidance.
Inhalational anthrax (post-exposure) in adults and children…. (as approved nationally in each member state)….
4.5. Updating of 4.5. according to the guidelines.
4.8. Updating of 4.8 according to the guidelines.
The incidence of arthropathy, mentioned above, is referring to data collected in studies with adults. In children, arthropathy is reported to occur commonly (See also 4.4 Special warning and precautions for use).
5.1. Updating of 5.1 according to the guidelines.
5.2 PHARMACOKINETIC PROPERTIES
Children
55

The data available to substantiate the pharmacokinetic data in children are limited. In a study in children Cmax and AUC were not age-dependent (above one year of age). No notable increase in Cmax and AUC upon multiple dosing (10 mg/kg three times daily) was observed. In 10 children with severe sepsis, less than 1 year of age Cmax was 6.1 mg/L (range 4.6 – 8.3 mg/L) after a 1-hour intravenous infusion at a dose level of 10 mg/kg; and 7.2 mg/L (range 4.7 – 11.8 mg/L) for children between 1 and 5 years of age. The AUC values were 17.4 mg*h/L (range 11.8 – 32.0 mg*h/L) and 16.5 mg*h/L (range 11.0 – 23.8 mg*h/L) in the respective age groups. These values are within the range reported for adults at therapeutic doses. Based on population pharmacokinetic analysis of pediatric patients with various infections, the predicted mean half-life in children is approx. 4 –5 hours and the bioavailability of the oral suspension ranges from 50 to 80%.
5.3 PRECLINICAL SAFETY DATA
Articular tolerability studies
As reported for other gyrase inhibitors, ciprofloxacin causes damage to the large weight-bearing joints in immature animals. The extent of the cartilage damage varies according to age, species and dose; the damage can be reduced by taking the weight off the joints. Studies with mature animals (rat, dog) revealed no evidence of cartilage lesions. In a study in young beagle dogs ciprofloxacin caused severe articular changes at therapeutic doses after two weeks of treatment, which were still observed after 5 months.
EU work sharing project pediatric data Ciprofloxacin Final SPC Changes, June 2006
56