final site visit report public health accreditation board
TRANSCRIPT

Final Site Visit Report
Public Health Accreditation Board (PHAB)
For the
Shawnee County Health Department
August 2020

P a g e 2 | 99
Table of Contents
Measure Score Dashboard .............................................................................................................................3 Three Greatest Strengths ................................................................................................................................4 Three Greatest Strengths .................................................................................................................................4 Three Most Serious Challenges of Opportunities for Improvement ..............................................4 Domain 1 ...............................................................................................................................................................5 Domain 2 ................................................................................................................................................................15 Domain 3 ................................................................................................................................................................27 Domain 4 ................................................................................................................................................................37 Domain 5 ................................................................................................................................................................42 Domain 6 ................................................................................................................................................................52 Domain 7 ................................................................................................................................................................61 Domain 8 ................................................................................................................................................................67 Domain 9 ................................................................................................................................................................73 Domain 10 .............................................................................................................................................................80 Domain 11 .............................................................................................................................................................84 Domain 12 .............................................................................................................................................................95
P a g e 3 | 99
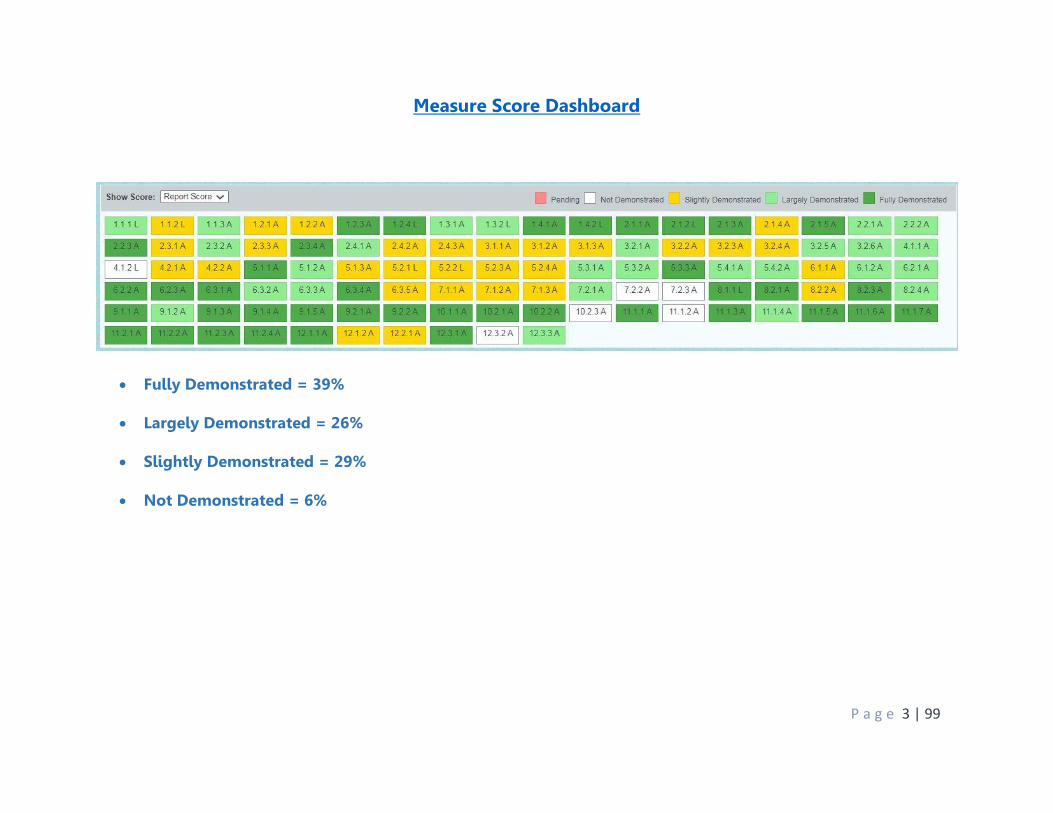
Measure Score Dashboard
Fully Demonstrated = 39%
Largely Demonstrated = 26%
Slightly Demonstrated = 29%
Not Demonstrated = 6%

P a g e 4 | 99
Site Visit Report
Overall Comments
Three greatest strengths: The Department has both traditional and non-traditional public health partners who are
committed to improving the public health of their community. Partners are involved in a county-wide coalition and are knowledgeable about Department functions and actions.
The Department links workforce development and program development to the goals listed in their strategic plan. Leadership strives to include all staff in the strategic plan.
Strong commitment by staff to meet populations where they are at and be out in the community conducting outreach and promoting public health as a profession.
Three most serious challenges or opportunities for improvement: Continue to build upon cultural competence when developing and implementing health
education programming to those in your jurisdiction. Consider developing or supporting a coalition or committee to address access to care in
the jurisdiction, identifying specific populations and, with feedback from those impacted, develop and implement strategies to address access to care.
Consider including community input in the development of health policy, education programs and initiatives, and create and implement a system for obtaining customer feedback.
Overall impression of the department as a functioning health department: Impressions: The building is clean, secure, and modern to fit the needs of the staff. Signage is
prominent. Staff is excited and passionate about public health.

P a g e 5 | 99
Domain Reports DOMAIN 1: Conduct and disseminate assessments focused on population health status and public health issues facing the community. Comments SCHD has a strong focus and appears to be committed to the assessment of the health of its population. Through efforts to systematic monitoring of health status through the collection, analysis, and dissemination of data to its stakeholder coalition (Heartland Healthy Network), they are able to use of data to inform public health policies, processes, and interventions. Their collaborative process has allowed them to develop a shared communicative procedure in sharing its health challenges, and its resources. STANDARD 1.1 – Participate in or lead a collaborative process resulting in a comprehensive community health assessment. Comments SCHD’s Community Health Assessment aims to learn about the community: the health of the population, contributing factors to higher health risks or poorer health outcomes of identified populations, and community resources available to improve the health status. In concert and collaboration with key stakeholders, community assets and resources can be mobilized to improve population health. This is a collaborative process of collecting and analyzing data and information for use in educating and mobilizing communities, developing priorities, garnering resources or using resources in different ways. Adopting or revising policies, and planning actions to improve the population’s health. SCHD’s development of a community health assessment involves the systematic collection and analysis of data and information to provide a sound basis for decision-making and action. SCHD was intentional in the development of their Community health assessments as it was conducted in partnership with other organizations and members of the community and included data and information on demographics; socioeconomic characteristics; quality of life; community resources; behavioral factors; the environment; morbidity and mortality; and other social, SCHD’s community health assessment will be the basis for development of its community health improvement plan. 1.1.1 L: Tribal/local partnership that develops a comprehensive community health assessment of the population served by the health department Score: Largely Demonstrated Conformity: RD1: SCHD provided the CHA dated November 2018 as required. The SCHD provided the RSVP/attendance roster from their Shawnee County CHNA Town Hall meeting dated September 27, 2018. The RSVP/attendance roster has a column that allowed attendees to check that they were present. The roster shows outside stakeholders representing many sectors of the local community. The documents highlight names of representatives of behavioral health, rescue mission, and Federally Qualified Health Centers (FQHC) which are the two or higher health risk populations yielding poorer health outcomes. RD2: Example 1 – Healthy Shawnee County Community Health Improvement Plan/Community Health Needs Assessment (CHIP/CHNA) Taskforce Meeting minutes dated October 25, 2017 was
P a g e 6 | 99
submitted. The notes from this meeting mentions data sources along with the continued development of data. Example 2 – Emails dated 3/6/19 from Community Health Outreach and Planning Division manager detailing plans for the next CHIP/CHNA meeting in which they discuss adding other partners to their group. Meeting minutes from 3/15/19 depict a timeline that evidences a CHNA Meeting that took place including information detailing the next steps in the CHNA process and included topics such as assets, resources, and review processes. RD3: The collaboration between Stormont Vail Health and SCHD was shown in the CHNA, dated November 2018. The collaborative process allowed the two parties to develop phases for getting the work accomplished, which included data and information being collected. The CHNA identified eight community health needs/issues to be addressed. A comprehensive inventory of community health resources and assets was provided to address health issues. Areas of Excellence: The Department has a great coalition of community stakeholders that are committed to improving the health of their community. They were able to articulate the finer points of the Community Health Assessment process during the site visit. Opportunities for Improvement: Not available 1.1.2 L: A Tribal/local community health assessment Score: Slightly Demonstrated Conformity: RD1: (1 community health assessment) a) SCHD provided their 2018 community health needs assessment (CHNA) as documentation for RD1. A SCHD used both qualitative and quantitative for their needs assessment. Primary sources (qualitative data) included interviews and town hall meetings with stakeholders. Secondary sources (quantitative data) included the Kansas Hospital Association, vital statistics, and Robert Wood Johnson County Health Rankings. b) Demographics are noted in the CHNA, including total population in the county, age, race, language, family demographics, disabilities, income, and education. c) SCHD noted a table listing a prioritized description of all the community needs identified by CHNA activities. No further information was given other than the number of attendees at a town hall meeting and votes obtained to rank the prioritized topics. SCHD also highlighted the same demographics as noted in B. Select health data, but not all, was broken down by gender (male/female), age (adult or children), and income levels. Data was not broken down by race or ethnicity. Populations with inequitable share of poor health outcomes were not identified. Areas in the county were not identified either. d) SCHD used qualitative data from town hall meetings for D. No populations are identified, just topic lists as prioritized by town hall meeting attendees, identified as weaknesses of the community. No data on health disparities or high-risk populations were addressed. No information on community factors that contribute to higher health risks and poorer outcomes of specific populations were considered. e) SCHD provided an extensive list of community resources in their CHNA. The inventory included healthcare services (those provided and not), number of providers providing care, and

P a g e 7 | 99
a Shawnee County Area Health Services directory, which included parks, youth serving organizations, housing offices, food pantries, and non-profit organizations, among others. RD2: Example 1 - SCHD provided an agenda for an “Our Health, Our Faith Community Health Forum” dated November 9, 2017. On the agenda is listed a review of the 2015 CHIP (Community Health Improvement Plan) and 2016 CHNA. This meeting was held before the November 2018 CHNA, the document provided for RD1. Example 2 - SCHD provided an agenda for a Heartland Healthy Neighborhoods annual meeting held December 10, 2018. A sign in sheet with meeting participants was included as documentation; professional groups were listed. On the agenda is a “2018 CHA Update”; minutes note that a SCHD reviewed the results of the CHA (which is dated November 2018), and reviewed the next step as developing the CHIP. The 2 examples do not demonstrate that the preliminary findings of the CHA were distributed to the community at large and that the community’s input was sought. RD3: Example 1 - SCHD provided a meeting agenda and PowerPoint presentation from a Board of County Commissioners meeting held March 21, 2019. At this meeting the SCHD presented the County Health Rankings. The PowerPoint reviews where Shawnee County stood in ranking compared from year to year, socio-economic status, behavioral risk factors, and several slides on what SCHD is doing about it. The CHNA is not mentioned at all in the PowerPoint. Age and race was broken down for suicide and homicide rates only. There is no evidence in the documentation if this data is being used to update/monitor the CHNA document. Example 2 - an agenda from a “County Health Rankings: A Community Conversation” meeting held April 8, 2019. Highlighted on the agenda are 2 items - Kujima Report Release and Prioritization of Health Needs for CHIP. The Kujima report was included; it was about the health of Black women in Topeka, KS. An extensive PowerPoint from the meeting was also provided, as well as the minutes from the meeting. There is no evidence in the documentation if this data is being used to update/monitor the CHNA document. Both examples were also from the same year; per the guidance documentation must be from 2 different years. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 1.1.3A: Accessibility of community health assessment to agencies, organizations, and the general public Score: Largely Demonstrated Conformity: RD1: Example 1 – SCHD provided emails to all the community partners. SCHD provided three ways to access the published CHNA: Heartland Healthy Neighbors website, SCHD website, and Storm View Health (hospital system) website. Example 2 – SCHD presented a screen shot of its Facebook page which is used to disseminate information. This documentation includes a post during Community Health Improvement Week and shared the location of SCHD’s Community Health Needs Assessment on their website. These actions show how they inform the general public, partners and other key stakeholders.

P a g e 8 | 99
RD2: Example 1 – SCHD produced a screen shot of its Facebook page displaying information stating the CHNA is available. SCHD posted this update to its Facebook page on 6/4/19. Example 2 – SCHD produced a screen shot of its website displaying information under their “Annual Reports” section displaying a link to the “2018 Community Health Needs Assessment”. The SCHD’s website was updated on 6/4/19. Areas of Excellence: The Department displayed its ability to deliver the results of the Community Health Needs Assessment through many different mediums. Opportunities for Improvement: Not Available STANDARD 1.2 – Collect and maintain reliable, comparable, and valid data that provide information on conditions of public health importance and on the health status of the population 1.2.1 A: 24/7 surveillance system or set of program surveillance systems Score: Slightly Demonstrated Conformity: RD1: 24/7 Surveillance System Policy presented and represents a department-wide policy and procedure. The policy states that SCHD’s surveillance system allows SCHD staff to monitor multiple systems, but only provides procedures on how a Communicable Disease Nurse will monitor the system (EpiTrax) and report outbreaks – data collection from multiple sources outside of this system is not specifically outlined. While the policy also states that data will be analyzed, the policy also does not go into detail about how data are reviewed and analyzed, other than that staff will monitor the system. RD2: SCHD’s 24/7 Surveillance System policy explains that all patient reports received through its system is considered confidential and subject to HIPAA. The policy stated that de-identified data may be released to the public but cannot lead back to the patient’s identity. The policy explains that all staff members sign confidentiality agreements as well as each accessed outside system. However, procedures for the maintaining data (both physical and electronic) in a secure and confidential manner, as the policy focuses more on staff confidentiality. RD3: SCHD’s 24/7 Communication for Reporting Public Health Emergencies and Bioterrorism Incidents clarifies SCHD’s procedure for the medical community and Kansas Department of Health and Environment to report incidents 24 hours a day/7 days a week. The Policy and Procedure details the numbers and points of contact complete with a flow chart for better clarity. However, this policy focuses more on public health emergency communication, rather than surveillance data collection, as intended by the measure. RD4: Example 1 – SCHD provided a report of testing the 24/7 contact system in the form of emails and screen shots. Specifically, the EpiTrax surveillance system was tested on 5/21/2019 and the results were disseminated to the SCHD’s leadership team and emergency preparedness staff via email on 5/30/2019. SCHD reported per their 24/7 Surveillance System Policy that reports are monitored daily by the staff. While this was only testing one method of communication, this was the main method of collection referred to in the policy provided for this measure.

P a g e 9 | 99
Example 2 – SCHD provided a report of testing the 24/7 contact system in the form of emails and a report. Specifically, the phone system was tested on 5/21/2019 and the results were disseminated to the SCHD’s leadership team and emergency preparedness staff via email on 5/29/2019. SCHD reported via the email that this was testing the 24/7 Surveillance System Policy, but this was not referenced in the policy provided. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 1.2.2 A: Communication with surveillance sites Score: Slightly Demonstrated Conformity: RD1: SCHD provided a list of surveillance data and locations on official letterhead dated June 6, 2019. However, this was a list of where data can be found, by topic, and how often they are received, and not a list of individuals or organizations that provide data to the department. RD2: Example 1 – SCHD provided copies of ESSENCE training certificates for a Division Manager along with screen shots of ESSENCE training announcement and the agenda from the training, held on May 9, 2019. SCHD also included a copy of the data use agreement. Topics for the training were presented in the agenda. However, this was a training for internal staff on using the system, rather than a training provided to surveillance site members that report to the health department, as required. Furthermore, as a training on the system, this training did not address reporting requirements, reportable diseases, and timelines. Example 2 – SCHD provided copies of a sign in sheet and email correspondences for their Mosquito Surveillance Training. The syllabus for the training was provided by the SCHD to depict the topics covered for the training which included Basics of Mosquito Control, Mosquito Trapping, and Mosquito Trap Data and Applications. However, again this was a training for internal staff, rather than a training provided to surveillance site members that report to the health department, as required. Furthermore, this training did not address reporting requirements, reportable diseases, and timelines. RD3: Example 1 - Emails depicting mosquito surveillance data sent from the Kansas Biological Survey to the SCHD Epidemiologist with the SCHD were provided. This information was dated on October 25, 2018. Example 2 - Kansas Department of Health and Environment sent STI Surveillance Data for the month of May 2019 to the SCHD’s Epidemiologist dated June 5, 2019. This is Shawnee County data. However, both examples are of the state sending data to the local health department, rather than SCHD receiving surveillance data from surveillance sites, as required. RD4: Example 1 – SCHD presented an EpiSurveillance newsletter created in-house by their Epidemiologist. Highlighted in the newsletter is data related to chlamydia surveillance in the jurisdiction. An email from the Epidemiologist notes that the newsletter was sent to all health department staff. There is no evidence of distribution outside of the health department. Example 2 – SCHD presented information on their website and Facebook page relative to flu surveillance in Shawnee County. These items are dated June 5, 2019 and March 22, 2019.
P a g e 10 | 99
Areas of Excellence: Not Available Opportunities for Improvement: Not Available 1.2.3 A: Primary data Score: Fully Demonstrated Conformity: RD1: Example 1 – SCHD provided their CHNA as evidence of primary quantitative data collection, as shown with a community stakeholder that was used in the CHNA to assess healthcare information – data was gathered from 2,324 residents. Example 2 – SCHD created a survey to gauge the need for Family Planning services in Shawnee County. An email dated February 1, 2019 was generated to the Shawnee County Board of Commissioners depicting the successful statistics and data captured from the survey. SCHD also presented a posting from their Facebook page depicting the survey results for information sharing purposes. The Facebook post was done on November 26, 2018. Areas of Excellence: Not Available Opportunities for Improvement: The site visit team has identified an opportunity for improvement that goes beyond the Standard and Measure, while qualitative data gathered for this measure met minimum requirements, SCHD should strengthen the methods used to gather qualitative data, beyond asking for comments. 1.2.4 L: Data provided to the state health department and Tribal health departments in the jurisdiction the local health department is authorized to serve Score: Fully Demonstrated Conformity: RD1: Example 1 – Primary data sent via Immunization Registry from SCHD to their State Immunization Registry was presented via screenshot from the Clinical Services Division Manager. There were updates transmitted and the SCHD was careful to redact patient names and other identifiers. The evidence submitted clearly showed that SCHD has jurisdiction that does not overlap with any Tribal Health departments. Example 2 – Primary data sent via Epitrax (Web Based infectious disease reporting system) from SCHD to their State Health Department was presented via screenshot from an SCHD staff member's computer. There was information added to an event that is automatically transmitted and the SCHD was careful to redact patient names and other identifiers. The evidence submitted clearly showed that SCHD has jurisdiction that does not overlap with any Tribal Health departments.

P a g e 11 | 99
Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 1.3 – Analyze public health data to identify trends in health problems, environmental public health hazards, and social and economic factors that affect the public’s health Comments SCHD provided evidence of analyzing public health data to identify trends in health problems that affect the public’s health. 1.3.1 A: Data analyzed and public health conclusions drawn Score: Largely Demonstrated Conformity: RD1: Example 1 – SCHD utilized the 2018 Community Feedback Conclusions from CHNA survey representing feedback from residents, community leaders, and providers via the use of an online perception survey was used to reference a qualitative analysis with conclusions drawn from data. a) The survey delivered gathered data in 2018, providing this as the reporting period. b) The 2018 Community Feedback Conclusions survey referred to the use of a “Likert Scale” in completing the survey. While the survey methodology is outlined, and the data collection process are included in the documentation, there is no specific analytic process included. c) The 2018 Community Feedback Conclusions survey no evidence of the analysis and conclusions comparability. It was difficult to determine the similar data for the same population gathered at an earlier time to establish trends. Example 2 - SCHD’s Preliminary Infant Mortality Report was used to reference a quantitative analysis with conclusions drawn from data. a) SCHD’s Preliminary Infant Mortality Report reference a period of 2008-2017 for its reporting period. b) SCHD stated that they utilized a descriptive analysis of the birth, death and linked birth-death records to summarize the issue of infant mortality in Shawnee County for their Preliminary Infant Mortality Report. c) SCHD’s Preliminary Infant Mortality Report's Fetal Infant Mortality Rate data is compared to 3 other counties in the state of Kansas and with the State of Kansas as a whole. SCHD also reviewed data for FIMR by zip codes within the report for years 2008-2017. The report is dated March 19, 2019. RD2: Example 1 – SCHD presented their CHNA’s contents (dated November 2018) which depict their town hall gatherings used to review the results of the survey and garner feedback from stakeholders. SCHD documented the sharing of data and their analysis with others. SCHD provided a list of attendees which included stakeholders from many sectors of their community. SCHD also documented the process for information gathering and results of their efforts. Example 2 - SCHD’s Preliminary Infant Mortality Report's fetal infant mortality rate data was reviewed during an April 4, 2019 Shawnee County Health Officer Meeting. Notes from the
P a g e 12 | 99
meeting were provided along with the sign in sheet noting the attendees. The report was documented on the agenda and the presentation, review, and discussion of data analysis was included in the documentation. RD3: An Epidemiology Surveillance publication with data specific to Shawnee County, KS was provided. The document presented analysis of life expectancy data that combines data from the Robert Wood Johnson County Health Rankings and the American Community Survey databases with topics including demographics, median family income, childhood poverty and percent uninsured among other items along with data sources to support their conclusion. RD4: Example 1 – SCHD documented the aggregation of primary and secondary data by presenting their Epi-Surveillance document. The data (published November 19, 2018) was compiled by Kansas Department of Health and Environment Office of Vital Statistics, National Association for Public Health Statistics and Information System, National Center for Health Statistics at the Centers for Disease Control and Prevention (CDC), and Robert Wood Johnson Foundation (RWJF). Charts were provided to enhance the information presented. SCHD also utilized GIS to target neighborhoods that are affected. The document sighted sources used in the report. The report demonstrates that data were compiled, analyzed, and conclusions drawn. Example 2 – SCHD presented a map, dated December 11, 2018, of childcare facilities overlaid with family income to represent primary and secondary data. The sources used include median family income by census tract Shawnee County, KS ACS 2016, 5 Year Estimates and the American Community Survey. While this example shows that data were compiled, there is not evidence of a specific analysis or conclusions being drawn. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 1.3.2 L: Public health data provided to various audiences on a variety of public health issues Score: Largely Demonstrated Conformity: RD1: Example 1 – SCHD presented their Epi Surveillance newsletter that covered STD trends. The document provided pictorial STD data trend graphs for Shawnee County, Kansas. The specific health issues involved were gonorrhea and chlamydia. The newsletter was shared with the health department staff and the Board of County Commissioners as evidenced by the copies of emails. The newsletter provided data analysis between the years of 2008-2018 and was compared to other counties. The data also provided a breakdown of STD rates by race and ethnicity. The evidence shows that it was distributed to their Epi Surveillance list which includes many individuals from outside of the staff and their Board. Example 2 - SCHD conducted a community stakeholder meeting on April 9, 2018 to discuss the County Health Rankings, as shown by the agenda and meeting packet provided. The meeting covered public health topics including smoking prevalence by annual household income in Shawnee County and the teen birth rate in Shawnee County. The data and minutes were captured as a county snapshot was presented by the Shawnee County Health Officer and showed that the data included both Kansas and Shawnee County. However, the county health

P a g e 13 | 99
rankings are not considered an analytic report. While data were presented and to an extent discussed, a specific analysis of data, findings, implications, etc., were not included and therefore, did not meet the intent of this measure, as it was more sharing data than data analysis. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 1.4 – Provide and use the results of health data analysis to develop recommendations regarding public health policies, processes, programs, or interventions. Comments SCHD provided evidence of providing and using the results of health data to develop recommendations regarding public health policies and programs. 1.4.1 A: Data used to recommend and inform public health policy, processes, programs, and and/or interventions. Score: Fully Demonstrated Conformity: RD1: Example 1 – SCHD utilized a Family Planning survey to collect data from the community about family planning needs in their community. The survey was presented in English and Spanish. The survey results were dated January 2019 and used to impact the revision or expansion of an existing policies, processes, programs, or interventions. SCHD also provided documents presented to their governing board requesting consideration of an approval to apply for state grants for funding towards family planning thus demonstrating the use of the data received from the community. Example 2 – For this example, SCHD demonstrated the use of County Health Rankings data (as shown in a provided County Health Rankings presentation) and specifically worsening trends in their community demonstrated by the data to justify hiring a position to work on the issues presented from the County Health Rankings report. Documentation included evidence of collaboration with their community coalition, in which the SCHD is an active member as SCHD staff hold key positions, as the coalition awarded SCHD funding for the position. Documentation also included a request to their governing board to approve the creation of this position. The County Health Rankings data includes multiple data sets and sources. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
P a g e 14 | 99
1.4.2 L: Tribal/community summaries or fact sheets to support public health improvement planning processes at the Tribal or local level Score: Fully Demonstrated Conformity: RD1: Example 1 – SCHD presented a fact sheet with talking points that included public health data to provide information about raising the tobacco age to 21 (Tobacco21). Example 2 - SCHD provided an Epi Surveillance newsletter that went to providers. The document is on SCHD letterhead and was presented to the Topeka City Council Meeting in December 2017. The evidence were the emails that detailed the distribution lists. RD2: Example 1 – SCHD provided an email showing that the Tobacco 21 data and talking points were sent to community partners. Example 2 – SCHD provided an Epidemiology Surveillance Newsletter that was sent out by the health department, detailing the life expectancy in Shawnee County complete with maps detailing a census tract for births in the county. The newsletter provides a table summary with selected data points including demographics, median family income, childhood poverty, and percent uninsured. While the email original provided does not show who the report was sent to outside of internal staff, a screenshot of the website was provided to show how it was published, and a newspaper article was provided to show that it was received and used. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 15 | 99
DOMAIN 2: Investigate health problems and environmental public health hazards to protect the community Comments SCHD is bound by state statutes and has the authority to focus on the investigation of suspected or identified health problems or environmental public health hazards. These include but are not limited to epidemiologic identification or emerging health problems, monitoring disease, availability of public health laboratories, containment and mitigation of outbreaks, coordinated response to emergency situations, and communication. STANDARD 2.1 – Conduct timely investigations of health problems and environmental public health hazards Comments SCHD is charged to conduct timely investigations of suspected or identified health problems as necessary for the detection of the source of the problems, and the prevention of the further spread of the problems. SCHD’s environmental public health section investigate hazards, and aims to rectify them, thus preventing further spread of disease or illness. 2.1.1 A: Protocols for investigation process Score: Fully Demonstrated Conformity: RD1: SCHD provided their Communicable Disease/Epidemiological and Environmental and Occupational Public Health Hazards policies and procedures as evidence for RD1. The policy states that their communicable disease team will follow the Kansas Department of Health and Environment Disease (KDHE) investigation guidelines. The policy also provides a link to KDHE’s guidelines for disease investigations. SCHD did provide copies of the KDHE’s policy and procedures as evidence. The revision date for their disease investigation policy is dated 12/07/18. The revision date for the Environmental Health policy and procedures is 12/10/18. a) Specific responsibilities were shown in the SCHD’s procedures with duties being delineated in SCHD’s Communicable Disease/Epidemiologic Investigations policy. The Communicable Disease (CD) nurses are responsible for investigative activities and on-call duties while the SCHD Director and Shawnee County Health Officer will assist the nurses per the policy. The Environmental Health Policy assigns duties to Environmental Health staff, inspectors, and clerks with the Supervisor checking all paperwork. Specific responsibilities were well defined in the policy. b) SCHD provided the KDHE protocol for disease investigations. The SCHD’s Communicable Disease/Epidemiological policy indicated that they follow the policy of the State of Kansas. The KDHE guidelines provided the case investigation steps, timelines related to the problem or hazards, and reporting requirements. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 16 | 99
2.1.2 L: Capacity to conduct an investigation of an infectious disease Score: Fully Demonstrated Conformity: RD1: SCHD presented 2 after-action reports (AAR) for RD1. They also provided their written policy for disease investigation, which states that staff will utilize the Kansas Department of Health and Environment (KDHE) Disease Investigation Guidelines. A page from the KDHE Guidelines outlining investigator responsibilities was also provided and includes steps for investigation – case investigation, contact investigation, and control/prevention measures. Example 1 – The first AAR is for a shigellosis outbreak that occurred in October 2017. The document referenced a brief overview of the event, major strengths, major areas of improvement, and lessons learned/future recommendations to refine plans and procedures. It was noted in the AAR that within 24 hours SCHD staff excluded those showing symptoms, conducted case interviews, and identified contacts of the cases for excluded, which is in accordance with the KDHE Disease Investigation Guidelines provided as evidence. Example 2 – The second AAR is for a varicella contact investigation from potential exposure at a Cub Scout meeting. The document referenced a brief overview of the event, major strengths, major areas of improvement, and lessons learned/future recommendations to refine plans and procedures. It was noted in the AAR that staff were able to conduct contact tracing to determine if prophylactic vaccination was appropriate or if exclusion from work/daycare/school was needed, which is in accordance with the KDHE Disease Investigation Guidelines provided as evidence. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.1.3 A: Capacity to conduct investigations for non-infectious health problems, environmental, and/or occupational public health hazards Score: Fully Demonstrated Conformity: RD1: Example 1 – SCHD presented documentation via EpiTrax of an elevated blood lead investigation report in Shawnee County. SCHD follows the Kansas Department of Health and Environment’s (KDHE) guidelines for disease investigations. The event in EpiTrax is dated 10/25/16 thus falling within the 5-year time frame per the measure. The documentation was redacted to protect patient privacy. This activity directly involved the SCHD and did not require an MOU/MOA to be executed. The lab report for the elevated blood level investigation along with investigative notes was also provided. Example 2 - SCHD presented documentation for a nuisance complaint received by their Environmental Health program dated 10/8/18. The documentation is handwritten with redactions made to protect the identity of those involved. This activity directly involved the

P a g e 17 | 99
SCHD and did not require an MOU/MOA to be executed. The documentation provides the names of the SCHD personnel who received the complaint, details that nuisance (occupation of a travel trailer sans a functioning septic system), and a certified letter to the owners on records describing the actions needed to remedy the ordeal (abate the described nuisance IAW Shawnee County Code). Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.1.4 A: Collaborative work through established governmental and community partnerships on investigations of reportable diseases, disease outbreaks, and environmental public health issues Score: Slightly Demonstrated Conformity: RD1: Example 1 – Documentation included a request from SCHD to the Shawnee County Board of Commissioners to enter into an agreement for mosquito surveillance with the Kansas Department of Health and Environment (KDHE). The agreement, included as documentation, outlines the roles and responsibilities of both SCHD and KDHE. SCHD will collect samples via traps and use surveillance data for public education. KDHE will identify mosquitoes and test for West Nile Virus. The agreement is for surveillance, not investigations of outbreaks of disease, healthcare associated infections, or environmental public health hazards. However, the contract focuses on a partnership with the state health department, which does not meet the intent of this measure, which is to partner with other organizations; there are no other partners listed in the agreement. Example 2 – Documentation included an agreement for funding of a Tuberculosis (TB) Control Nurse and TB Control Program Activities. The agreement is between SCHD and the KDHE. There are no other partners involved in the agreement, and the agreement is not for conducting investigations of outbreaks of disease, healthcare associated infections, or environmental public health hazards, but rather the funding of a position who will coordinate care for those with TB, monitor treatment plans, and conduct TB skin testing in clinics in the field. RD2: Example 1 – SCHD presented an After-Action Review Report (AAR) of an outbreak of norovirus at a Mexican restaurant, dated January 2017, in their jurisdiction. The documentation describes that KDHE, SCHD, and the Kansas Department of Agriculture worked together when it was discovered that three people who all ate at a Mexican Restaurant experienced gastrointestinal issues. The report was published on August 14, 2017. Example 2 - SCHD presented an After-Action Review Report (AAR) of a gastroenteritis outbreak associated with a butcher shop in Shawnee County. The documentation shows that KDHE, SCHD, and the Kansas Department of Agriculture worked together when it was discovered that three different families became ill after consuming food purchased at a butcher shop in the jurisdiction. The report was published on December 18, 2015. RD3: SCHD produced their policy on laboratory testing for reportable diseases. This report details that SCHD works closely with their state laboratory, Kansas Health and Environmental

P a g e 18 | 99
Laboratory, to complete appropriate testing for reportable disease. The policy lists the reportable diseases that SCHD tests for in their laboratory. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.1.5 A: Monitored timely reporting of notifiable/reportable diseases, lab test results, and investigation results Score: Fully Demonstrated Conformity: RD1: SCHD used a fourth quarter 2018 vaccine preventable case report to represent their tracking log for investigations of reportable lab results. EpiTrax is used by SCHD for disease surveillance and reporting. EpiTrax has a reporting tool that generates reports for data analytics. The report includes columns that show the date the case was reported to public health, the date the investigation started, the date the investigation concluded, lab test results, and case classification. RD2: SCHD submitted Kansas law relating to the reporting of notifiable/reportable diseases. Kansas Administrative Regulation (K.A.R) 28-1-2 Reporting requirements for infectious or contagious diseases and conditions is what SCHD is governed by as a local health department. The statute was last amended on 10/4/18. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 2.2 – Contain/mitigate health problems and environmental public health hazards Comments Per an internal policy, SCHD follows the state health department guidelines for disease investigations. SCHD should consider adding to their policy a process for responding to environmental public health hazards. Their Emergency Operations Plan (EOP) defines what actions are to happen to activate the plan, and a separate policy defines when After Action Reports (AARs) are to be written. 2.2.1 A: Protocols for containment/mitigation of public health problems and environmental public health hazards Score: Largely Demonstrated Conformity:
P a g e 19 | 99
RD1: SCHD provided their policy on communicable diseases/epidemiologic investigations, which states that their Department follows the Kansas Department of Health and Environment’s (KDHE) guidelines for disease investigations. Also included was the KDHE’s pertussis investigation guidelines, which outlines processes for contact mitigation via control of cases and contacts, case management, contact management via detailed instructions in the protocols, immunization status, and clinical management was detailed. Also mentioned was how to communicate with the public health laboratory and legal authority for disease control, and prophylaxis and emergency biologics were included in a guidance table. There is no evidence in the documentation of environmental public health hazards in the protocol. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.2.2 A: A process for determining when the All Hazards Emergency Operations Plan (EOP) will be implemented Score: Largely Demonstrated Conformity: RD1: SCHD provided their policy on Communicable Diseases/Epidemiologic Investigations, which states that the Department follows the Kansas Department of Health and Environment’s (KDHE) guidelines for disease investigations. SCHD provided their All Hazards Emergency Operations Plan (EOP) dated May 17, 2019. The plan activation section details that the EOP will be activated in the event of an emergency, defined as any situation that is, or may expand to be, beyond their capability to respond within normal operating parameters. This section concludes by stating that the SCHD’s Director may activate the entire plan or any portion of the plan for any incident that involves Shawnee County. Activation can also occur when assisting other health districts. RD2: SCHD’s Environmental Health (EH) program procedures and their All Hazards Emergency Operations Plan (EOP) were provided. The EH program procedures details the process for complaints such as sewage, nuisance, vehicles, refuse, burning, illegal dumping, hazardous waste, and quarantine of animals. There is also information about the trapping of mosquitos. The plan activation section of the EOP describes that the plan will be activated in the event of an emergency, defined as any situation that is, or may expand to be, beyond their capability to respond within normal operating parameters. This section concludes by stating that the SCHD’s Director may activate the entire plan or any portion of the plan for any incident that involves Shawnee County. SCHD did not provide protocols that specifically address environmental public health hazards or the process for determining when the EOP will be implemented. RD3: SCHD provided their policy on Communicable Diseases/Epidemiologic Investigations, which states that the Department follows the KDHE Disease Investigation Guidelines. These guidelines were not included, and the link to the KDHE website in the policy is broken. SCHD also provided their All Hazards EOP, dated May 17, 2019. In the situations and assumptions section it lists various potential hazards that may require a public health response or might activate the use of the EOP, including “disease”. This plan activation section states the EOP will

P a g e 20 | 99
be activated in the event of an emergency. There is no evidence in the plan of protocols related to cluster evaluation. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.2.3 A: Complete After Action Reports (AAR) Score: Fully Demonstrated Conformity: RD1: SCHD provided their policy for After Action Reports. The policy lists when an AAR will be completed, including disease outbreaks, low incidence or unusual events with significant health consequences (such as active TB). An After-Action Reports (AAR) policy/procedure for SCHD was created on May 24, 2019 and provides a description of how the Department employees prepare an AAR to assess agency response to public health threats including communicable disease outbreaks, environmental health hazards, bioterrorism attacks, natural disasters and other threats as detailed within the document. RD2: SCHD’s list of significant public health events for years 2015-2020 details the list of significant events that have occurred. All other parameters were described to include the event name, date of the event, and event type. The listing was all inclusive providing outbreaks and events that threatened the public’s health. No natural disasters were listed. The events that rose to the level of significance to require an AAR were indicated with red boxes, and thus both events that did and did not require and AAR were included. RD3: Example 1 – SCHD provided an AAR for a varicella contact investigation, dated 1/7/19. The AAR detailed a brief overview of the incident, major strengths (what worked well: good coordination from SCHD team and partners, quick contact with possible suspects, responsiveness of the County Health Officer, facts sheets distribution), major areas of improvement (getting more cooperation from leader of affected areas), and conclusions (continued emphasis on communicating the purpose of the investigation as well as disease control measures and emphasizing that they strive to stop the spread of disease.) Example 2 - SCHD provided an AAR for a shigella outbreak dated 12/20/18. The AAR detailed a brief overview of the incident, major strengths (what worked well: good collaboration from SCHD team and the State of Kansas, quick contact with possible suspects, responsiveness of the County Health Officer, facts sheets distribution), major areas of improvement (use of private providers for treatment, disinfectant protocols), and conclusions (continued effort to assist families with testing-emphasis and clarification on exclusions). Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 21 | 99
STANDARD 2.3 – Ensure access to laboratory and epidemiological/environmental public health expertise and capacity to investigate and contain/mitigate public health problems and environmental public health hazards. Comments SCHD, in their Emergency Operations Plan, outlines communication procedures for support services during emergencies. It does not, however, outline this communications in 24/7 capacity. SCHD does have multiple contracts and agreement for public health emergency support, including additional locations for dispensing operations, supplies and staffing. While having limited internal lab capacity, SCHD does have access to the state lab and follows their protocol for handling and submitting specimens/ 2.3.1 A: Provisions for the health department’s 24/7 emergency access to epidemiological and environmental public health resources capable of providing rapid detection, investigation, and containment/ mitigation of public health problems and environmental public health hazards Score: Slightly Demonstrated Conformity: RD1: SCHD provided Appendix B to their Emergency Operations Plan (EOP). Highlighted in the plan are sections stating that the Department, as part of Emergency Support Function 8, will work with and contact support agencies during emergencies. The plan also states who will notify the Department during an emergency or disaster event. The plan does not mention how the Department will maintain 24/7 access to support services in emergencies. RD2: SCHD provided a Shawnee County ESF8 Public Health and Medical Services contact list. This list included contact information for EMS, various medical and surgical centers, emergency management personnel, universities, and behavioral health providers. Personnel for these locations include supervisors, directors, administrators, emergency management, and facilities directors. There are no epidemiology or environmental health contacts on the list. RD3: SCHD provided list of agreements/memorandums of understanding (MOUs) that they have established with a variety of entities. Multiple documents were included as evidence. The Points of Dispensing (POD) MOUs with community centers and high schools included language for 24/7 access during emergencies warranting mobilizing POD operations. A contract with their County Health Officer states that the provider should be available 24/7 to assist with a public health emergency. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.3.2 A: 24/7 access to laboratory resources capable of providing rapid detection, investigation and containment of health problems and environmental public health hazards Score: Largely Demonstrated

P a g e 22 | 99
Conformity: RD1: SCHD provided their CLIA certificate showing certification for Mycology and Parasitology. No other testing is provided. RD2: The laboratory policy for SCHD was presented with information on how to contact the Kansas Health and Environmental Lab (KHEL) during normal business hours and after hours. If SCHD needs to contact KHEL outside of normal business hours, staff is to utilize the 24-hour hotline for disease reporting and public health emergencies. RD3: SCHD submitted their laboratory testing policy. The policy states that all specimens collected by SCHD staff will be sent to Kansas Health and Environmental Laboratories (KHEL) for testing. SCHD included the KHEL microbiology specimen submission guidelines, which outlines out to collect and ship a variety of specimens including blood, body fluids, sputum, and stool. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.3.3 A: Access to laboratory and other support personnel and infrastructure capable of providing surge capacity Score: Slightly Demonstrated Conformity: RD1: SCHD provided the Appendix B/Emergency Support Function Annex to the Emergency Operations Plan (EOP) that serves as their protocol for surge capacity. SCHD serves as the Coordinating Agency with several support agencies listed as support personnel to include (but not limited to): American Red Cross, Shawnee County Emergency Management, and Kansas Dialysis. The protocol presented includes information on the partnership that SCHD has with the Kansas Department of Health and Environment for lab services in the event of an emergency. RD2: A staffing list for Shawnee County ESF 8 has been provided. SCHD’s call down list included contacts for the health department, medical facilities, and emergency management resources. The section on “Direction and Control” details the staffing needed for a surge response and specifies who will perform what roles during the event. An email to the essential personnel of Emergency Support Function 8 (team that performs disaster response) from the Emergency Preparedness and Community Outreach Specialist providing a contact list with names, positions, and phone numbers was entered into evidence. Finally, minutes of an ESF#8 Meeting held on 1/3/18 detail a task of sending out an updated call list to all member. RD3: SCHD uses an equipment and personnel tracking system called the Comprehensive Resource Management and Credentialing System (CRMCS). This system allows SCHD to keep track of equipment and resources purchased for preparedness efforts. Reports on the availability of deployable equipment for surge purposes can be generated to detail the availability of equipment. RD4: SCHD’s Workforce Development plan was presented which provides the core training for all staff. The Workforce Development plan also contains SCHD’s Continuity of Operation Plan (COOP) which is essential for emergency activities. A schedule of core workforce trainings was
P a g e 23 | 99
provided in the plan to include: Bloodborne Pathogens Training, Personal Protective Equipment Training, and Incident Command System training. RD5: SCHD provided a comprehensive list of agreements that are designated for surge capacity efforts. Supporting documentation included memorandums of understanding (MOU) for several point of dispensing locations and a contract for a County Health Officer. SCHD is also part of a Healthcare Coalition; the bylaws and governance structure document were included. SCHD also provided an MOU with 7 other local health departments that states the Departments will share equipment, surge personnel, and stocks of personal protective equipment in the event of an emergency. There is no mention of lab services for surge capacity in any agreement provided. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.3.4 A: Collaboration among Tribal, state, and local health departments to build capacity and share resources to address Tribal, state, and local efforts to provide for rapid detection, investigation, and containment/ mitigation of public health problems and environmental public health hazards Score: Fully Demonstrated Conformity: RD1: Example 1 – SCHD participates in the North East Kansas HealthCare Coalition. This Coalition develops the relationships, plans, and tools necessary for effective, coordinated regional responses to healthcare emergencies. SCHD provided a letter dated 10/10/16 detailing those staff members from SCHD that would participate on the coalition. SCHD produced minutes from the 2/6/18 Coalition meeting and a sign in sheet that shows the names of members from several area health departments. Example 2 – SCHD provided minutes from a regional meeting that displays multiple health departments in the region coming together to discuss preparedness activities. The Ebola Table Top Exercise was well attended and displayed how the stakeholders worked together to build capacity during the exercise. RD2: Example 1 – SCHD participated in mosquito surveillance as evidenced by an After-Action Report and Improvement Plan dated 2/1/18. The participating organizations were SCHD, Kansas Biological Survey and the Kansas Department of Health and Environment. The shared resources were funded by the CDC Epidemiology and Lab Capacity (ELC). There is not a tribe located in Shawnee County. Example 2 - After Action Report of an Ebola tabletop exercise involving SCHD, Atchison County Health Department, Brown County Health Department, Doniphan County Health Department, Jackson County Health Department, Jefferson County Health Department, Home Health, and Hospice Nemaha County Community Health Services, Marshall County Health Department, Shawnee County Emergency Management, Shawnee County Health Agency, Shawnee County Sherriff's Office, and St. Francis Health Stormont-Vail. The exercise was held on 12/4/14. There is not a tribe located in Shawnee County. Areas of Excellence:

P a g e 24 | 99
Not Available Opportunities for Improvement: Not Available STANDARD 2.4 – Maintain a plan with policies and procedures for urgent and non-urgent communications. Comments SCHD has a risk communication plan that outlines communication to city and state leadership, community stakeholders, and the public during a public health emergency. While there are considerations in the plan for those in the jurisdiction whose first language is not English, SCHD should consider adding to the plan how to communicate with those who are disable, blind or deaf. SCHD uses a health alert network to receive messages and should consider a similar system to issue messages to the community. 2.4.1 A: Written protocols for urgent 24/7 communications Score: Largely Demonstrated Conformity: RD1: SCHD provided their Risk Communication Plan which was developed for the proper management of communication activities during an emergency. The plan details the media distribution list and conveys how news would be released via multiple methods. It does not explicitly say 24/7. SCHD also provided a community contacts list, which included emails for various non-profit agencies, senior centers, healthcare centers, local EMS, and fire and police departments. RD2: SCHD was able to document how the public can reach their agency by providing a screenshot of their webpage that lists the 24/7 telephone number to call in the event of a public health emergency or environmental or occupational public health hazard. RD3: SCHD provided a screen shot of their webpage depicting the 24/7 On-Call number for the Health Department. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.4.2 A: A system to receive and provide urgent and non-urgent health alerts and to coordinate an appropriate public health response Score: Slightly Demonstrated Conformity: RD1: SCHD participates in the Health Alert Network (HAN). SCHD provided emails and a screen shot of a HAN text message (both dated 2/27/19) that was sent from the HAN to the Clinical
P a g e 25 | 99
Services Division Manager. The also provided the signed job description for the Clinical Services Division Manager. There was no documentation demonstrating SCHD using the HAN to issue alerts as required by the measure. RD2: Example 1 – SCHD provided their 24/7 Surveillance System policy, which outlines the procedure for monitoring an EpiTrax disease reporting system and internal notification process if an outbreak is noted. Also included as documentation was a memo to SCHD Leadership from the Director of Health detailing the testing of their 24/7 surveillance system’s on-call phone after-hours. The Director called on the on-call nurse after business hours and was able to connect. The example provided is for disease surveillance, not issuing urgent and non-urgent health alerts as required by the measure. Example 2 – Similar to example 1, SCHD provided their 24/7 Surveillance System policy, which outlines the procedure for monitoring an EpiTrax disease reporting system and internal notification process if an outbreak is noted. A memo from the Director to SCHD Leadership states the Director tested the monitoring of the EpiTrax disease surveillance system during normal business hours and the results of the test were attached. Again, the example provided is for disease surveillance, not issuing urgent and non-urgent health alerts as required by the measure. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 2.4.3 A: Timely communication provided to the general public during public health emergencies Score: Slightly Demonstrated Conformity: RD1: SCHD’s Risk Communication Plan was submitted as evidence. The plan states that the Public Information Office (PIO) is responsible for developing messages in formats specific to at-risk populations in the jurisdiction. Notifications will be sent out timely using the point of contact information found in the local response plan. Materials will be produced with a reading level between 3rd and 6th grade, and materials will be produced first in English and Spanish, then other languages as needed. SCHD will also provide interpreter/translator services for languages commonly spoken or read in the community. SCHD will rely on the Joint Information Center for media communications; other means of communication include social media, handwritten signs at mass care locations, and vehicle mounted loudspeaker public address systems. The plan does list alternative means of communication if there is no electricity. There was no consideration of methods of communication for those who are disabled or who require other communication considerations, such as those who are blind or deaf. RD2: Example 1 – SCHD provided a media release by their PIO regarding the investigation of cases of shigellosis at a local preschool. The media release mentions a letter from SCHD was sent home with the students of the preschool altering parents what signs to look for possible infection. A general fact sheet on shigella was included in English and Spanish. Example 2 - SCHD provided a general media release by their PIO to inform the public about precautions against whooping cough. The release outlines what whooping cough is, that the

P a g e 26 | 99
Department offers a free vaccine, and other prevention steps to prevent spreading the illness. The release states there have been no cases in the county; this is a general press release and not related to a public health emergency as required by the measure. For both examples, there was no evidence of a media relationship in trying to reach hard-to-reach populations, such as those who are disabled, as required per the measure. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 27 | 99
Domain 3: Inform and educate about public health issues and functions Comments SCHD provides information to the public on their programs and interventions. They utilize the media to disseminate health information and information on important public health issues. SCHD has a branding plan on how to use their logo but lacks information on how the brand should be used in external and internal communications. Social media and traditional media is used to inform the public about public health issues, and materials are provided in English and Spanish. Spanish interpreters are on staff to help with translation, and SCHD has other resources to help the hearing and visually impaired. SCHD has communication plans in place for both general and risk communications. A staff person is the designated Public Information Officer (PIO) for the county. STANDARD 3.1 – Provide health education and health promotion policies, programs, processes and interventions to support prevention and wellness. Comments SCHD provides messaging to residents in their jurisdiction on health risks, health behaviors, disease prevention, and wellness. SCHD should involve the target community in the development of educational materials and messaging, before implementation. SCHD should also take into account cultural competency when providing information to the 3.1.1 A: Information provided to the public on protecting their health Score: Slightly Demonstrated Conformity: RD1: Example 1 - SCHD provided a press release, dated June 6, 2018, on the availability of free nicotine replacement therapies through the Kansas Tobacco Quitline. The press release talks about the benefit of quitting and prevalence of smoking in the county, and that smoking is one of the leading causes of cancer and chronic illness. This opportunity is a part of the Shawnee County Health Departments Chronic Disease Risk Reduction grant program. The target group is Shawnee County residents looking to quit using tobacco, who are encouraged to call the Quitline to help them quit (making this example “actionable”). The press release is written in plain language. There is no evidence how cultural competence was taken into account. Example 2 - The second example is also a press release from SCHD announcing 2 free flu shot clinics for uninsured adults in the county. The release, dated October 15, 2018, outlines steps residents can take to help minimize the spread of germs (such as hand-washing), making it actionable. The press release is written in plain language, but again there is no evidence as to how cultural competence was taken into account. RD2: Example 1 - SCHD provided an agenda from an Our Health Our Faith Community Health Forum held November 9, 2017. Highlighted on the agenda was “Community Snapshot: Health in Shawnee County” and “Opportunity for Community Discussion”. SCHD provided the accompanying PowerPoint, which smoking prevalence rates in the county and other smoking statistics highlighted. Summarized notes from the meeting note that increase access to tobacco cessation aides is needed to combat the smoking in the county. SCHD shows that data was used to identify tobacco use as an issue, but did not provide documentation that the target audience were consulted. SCHD did not provide the attendance list for the meeting. There is also no

P a g e 28 | 99
discussion of the development of educational materials/messages, nor social or environmental factors per the measure. SCHD provided an undated WIC participant survey on the use of eWIC cards and a WIC store survey on using eWIC cards. The survey results for the 2 surveys were included; only the participant survey is dated (May 22, 2019). This is a customer satisfaction survey on the WIC program and staff, and for the store survey, if they were trained in eWIC cards, not a method of soliciting input from the target audience during the development of messages and materials. SCHD did also include a eWIC educational flyer that explains the benefits of the shopper app, how to determine end of benefits, and how to read the eWIC mid-receipt and shelf labels, however this information was not included in the survey. There is no link between the survey and the eWIC educational flyer documentation. RD2, Example 1 is the same topic as the press releases in RD1. As an opportunity for improvement, SCHD should involve the target community in the development of educational materials and messaging, and document appropriately. RD3: SCHD provided an email chain between a SCHD staff person and a representative from the state health department's Quitline Coordinator (KanQuit) about a tobacco cessation lunch and learn panel invite. The KanQuit Coordinator was invited to be on the panel, was unable to make it, but provided a presentation for a SCHD staff person to present instead. The KanQuit Coordinator also provided a flyer on the program. Documentation is for the coordination of a lunch and learn, not the coordination of health education messaging. Example 2 - The second example was an email from the Kansas Perinatal Community Collaborative (KPCC) Program Coordinator to a list of unidentified persons regarding a KPCC website going live. Noted in the email is that the website is limited to promotional materials, guidance documents, curriculum handouts, lesson and activity plans, and power points. There is no evidence of SCHD coordinating a unified health education message with a local/state health department. Materials were pre-developed and distributed. Areas of Excellence: Not Available Opportunities for Improvement: The site visit team has identified an opportunity for improvement that goes beyond the Standard and Measure, SCHD should consider documenting how cultural competence is taken into account when creating educational materials and messaging. 3.1.2 A: Health promotion strategies to mitigate preventable health conditions Score: Slightly Demonstrated Conformity: RD1: SCHD provided the 2019 update to their Strategic Plan 2017-2021. Highlighted in the plan is the organizational chart, priority goals, and strategies including engaging a wide cross section of partners to progress towards health equity. SCHD also provided the position description for the Community Health Outreach and Planning Division Manager. There is no evidence in the documents of a planned approach for developing and implementing health promotion programs. RD2: Example 1 - SCHD provided what appears to be a portion of their Chronic Disease Risk Reduction FY18 application dated February 15, 2017. The application is to enact Tobacco 21 policy in the County. They also provided activity progress paperwork, suggesting that the

P a g e 29 | 99
application was accepted and implemented. Evidence Based – The application references an Institute of Medicine report referencing the
public health benefits of enacting a nationwide Tobacco 21 policy. Developed with Community – Progress paperwork notes that several meetings were held
with community stakeholders to move a Tobacco 21 policy forward, including the American Heart Association, local Chamber of Commerce, and local police department. The application mentions that students and youth will participate in activities such as education and engagement, data collection, and media advocacy. In the progress report it does mention that 2 youth provided testimony at a December 5, 2018 City Council meeting, at which Tobacco 21 passed.
Social and Environmental Factors – The application mentioned that raising the minimum legal age to 21 to purchase tobacco products has the potential to be an effective strategy to reduce tobacco use among young people. This encourages individual behavioral factors that negatively impact health.
Change Methods/Marketing – The application mentions that a partnership with students and youth will be valuable in creating opportunities for earned media and communications.
Implemented with community – Tobacco 21 was passed December 5, 2018. Several meetings are noted as being held with community stakeholders to move Tobacco 21 forward.
Example 2 - a Safe Routes to School final report for a local elementary school. It is dated 2014 and was written by the SCHD Health Promotion Coordinator. Evidence Based – The report notes that Safe Routes to School (SRTS) is an evidence-based
strategy than can help reverse the epidemic of childhood obesity. The report states that evidence shows that SRTS programs make the trip to and from school safer, increase the number of children who get to school by walking and bicycling, and promote the health of children in their communities.
Developed with Community – Feedback was obtained from both students and parents via surveys; methods are outlined in the report.
Social and Environmental Factors –The report contained maps noting environmental hazards prohibiting a “safe route to school”.
Change Methods/Marketing – There is no evidence of this in the report. Implemented with community – The report includes a SRTS implementation plan for the
school; there is no evidence it was implemented with the community. RD3: Example 1 - SCHD provided a letter to parents/guardians (dated December 1, 2014) asking them to complete and return a survey on safe routes to school by December 4. A copy of the survey, provided in English and Spanish, was included. Questions included how healthy parents/guardians through walking or biking to/from school was for their child, what issues affect decisions to allow/not allow their child to walk or bike to/from school, and if they would change their mind if the identified problem was changed or improved. A summary of survey results was included. Example 2 - SCHD provided a letter from an apartment complex manager (dated January 23, 2018) to tenants stating that the current smoking policies are going to be reviewed and updated due to continued issues with the smell of smoke traveling to adjacent apartments. Staff from SCHD held a discussion on smoke-free multi-unit housing policies and solicited feedback from residents on February 21, 2018. SCHD send the manager an email summarizing tenant feedback. The property went smoke-free April 1, 2018. A copy of the smoke-free lease addendum was provided.
P a g e 30 | 99
RD4: Example 1 - SCHD provided Safe Routes to School final report for a local elementary school. It is dated 2014 and was written by the SCHD Health Promotion Coordinator. SCHD highlights the “Recommendations” section of the report for evidence of implementation was in collaboration with stakeholders, partners, and the community. “Recommendations” implies that implementation was not completed yet. The report lists partners and their role in phased implementation, including inmate labor to remove overgrowth, Public Works, Parks and Recreation, and the local police department. Example 2 - SCHD provided a Tobacco 21 Endorsement page with multiple logos on it. It is noted in the documentation this was for marketing purposed only. SCHD and the American Heart Association are highlighted. SCHD also provided program activity progress pages for their Chronic Disease Risk Reduction Application (FY18). American Heart Association is listed as part of the Tobacco 21 taskforce. Also provided is an undated and unaddressed letter from the Heart Association encouraged adoption of Tobacco 21 policies. Attached to the letter is a fact sheet on raising the minimum legal sales age of tobacco to 21. Documentation does not describe all partners and does not go into enough detail about Tobacco 21 in the county and what role everyone played in implementation. Areas of Excellence: SCHD uses evidence-based strategies. Opportunities for Improvement: Not Available 3.1.3 A: Efforts to specifically address factors that contribute to specific populations’ higher health risks and poorer health outcomes. Score: Slightly Demonstrated Conformity: RD1: Example 1 - SCHD provided a FY20 grant application for chronic disease risk reduction programming, dated March 11, 2019. a) The community profile and statement of need is highlighted. The profile includes percentage of ethnic groups, percent overweight, food insecurity and poverty rate. The application notes the statement of need is to continue efforts on Tobacco 21 and smoke-free housing unit policies. b) In the application, SCHD outlines multi-year SMART objectives that will be taken to address their statement of need. These include working with housing complexes in the jurisdiction to help them implement smoke-free housing policies and holding lunch and learns with tenants and property owners. There is no evidence that the plans were to impact health inequities. c) SCHD provided an internal department policy outlining their mission, goals, and values. The policy states that the mission, vision, and core values should be taken into consideration for any type program development or funding proposal to ensure the inclusion of health equity considerations for the Shawnee County community. This grant was awarded in July 2019, per SCHD's reply to a pre-site visit review question. This was confirmed at the site visit. Therefore, implementation activities are occurring after the June 2019 PHAB submission. This document, while it identifies strategies, does not have an implementation component required per the measure.

P a g e 31 | 99
Example 2 - SCHD provided the same grant application as in Example 1, with sections related to SCHD facilitating the newly formed Shawnee County Farm and Food Advisory Council to ensure completion of priorities decided upon by the Council. a) The community profile and statement of need is highlighted. The profile includes number of person living in food deserts in the jurisdiction and free-reduced price lunch numbers in the school system. The application notes funds will be used to create community awareness around the initiatives of the Farm and Food Advisory Council and promote initial membership. b) In the application, SCHD outlines multi-year SMART objectives that will be taken to address their statement of need regarding the Farm and Food Advisory Council. These include finalizing the Council composition, resolution, and by-laws, develop priorities, increase utilization of healthy and locally produced food in identified food deserts, and create objectives for subcommittees. There is no evidence that the plans were to impact health inequities. c) SCHD provided a Shawnee County Community Food System Assessment document dated March 2017. Highlighted in this document is a section on equity issues in the food system and include farming and the food system, food system infrastructure, food retail, and consumer access. SCHD also provided the same policy as RD1 for this section of the requirement. This grant was awarded in July 2019, per SCHD's reply to a pre-site visit review question. Therefore, implementation activities are occurring after the June 2019 PHAB submission. This document, while it identifies strategies, does not have an implementation component required per the measure. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 3.2 – Provide information on public health issues and public health functions through multiple methods to a variety of audiences. Comments SCHD provides information to the public on their programs and interventions. They utilize the media to disseminate health information and information on important public health issues. SCHD has a branding plan on how to use their logo but lacks information on how the brand should be used in external and internal communications. Social media and traditional media is used to inform the public about public health issues and materials are provided in English and Spanish. Spanish interpreters are on staff to help with translation, and SCHD has other resources to help the hearing and visually impaired. SCHS has communications plans in place for bother general and risk communications. 3.2.1 A: Information on public health mission, roles, processes, programs, and interventions to improve the public’s health provided to the public. Score: Largely Demonstrated Conformity:
P a g e 32 | 99
RD1: SCHD provided their department’s Community Services brochure dated September 2017. The brochures lists the services available through the department, as well as the mission, vision, and aim statement of the department. SCHD also provided an outreach list of when and where the brochure was distributed. SCHD provided a published editorial written by the SCHD Manager of Community Health Outreach and Planning. The editorial, titled “Improving the Health of our Community”, discusses access to care is not the only indicator of health in a community, and that collaboration is key to creating positive impacts on health outcomes. There is no information on what public health is, its value, and/or the health department’s role, processes, programs, and interventions in the editorial. RD2: SCHD provided their 2018 Media Tracker, which lists the media source, contact date, contact person and phone number, reason for contact, and status/outcome of the contact. Some outcomes include live interviews, published press in newspapers, and being featured in taped news stories for topics including Tobacco 21 implementation, measles, and increase in flu activity. Example 2 - The second example is a published guest columnist article written by the Director of Health on preventing youth smoking. The article, published December 3, 2017, included statistics on youth smoking initiation and encourage adoption of a Tobacco 21 ordinance. Areas of Excellence: SCHD has a good working relationship with media that covers their jurisdiction. Opportunities for Improvement: Not Available 3.2.2 A: Organizational branding strategy Score: Slightly Demonstrated Conformity: RD1: SCHD provided their Public Health Marketing and Branding Style Guide dated March 2019. Guidance A: SCHD highlighted the goal of effective public health communication in the plan. SCHD Community Health Outreach and Planning Division staff lead/coordinate external communications and provides guidance and training's to develop communication skills in staff across the department. There is no evidence of how SCHD ensures that department staff have a clear understanding and commitment to the brand. Guidance B: SCHD lists target audiences including families, media partners, and community partners and provides examples of ways to communicate to each of those audiences. There is no evidence of how the brand is used for each of these audiences. Guidance C: There is no evidence in the documentation how the brand is to be used in organizational communication strategies and external communications. SCHD should add to their branding plan how the brand and logo is to be used in external and internal communications. Guidance D: SCHD highlighted 2 ways of correctly positioning the logo with additional content; a hand washing sign and a fact sheet were the examples. It is mentioned that the logo can be used as a stand-alone image on materials or in conjunction with existing state and/or community partner logos. SCHD uses the public health logo provided by the National Association of County and City Health Officials with the tagline “Prevent, Promote, Protect”.
P a g e 33 | 99
Guidance E: During the site visit, signage was noted to be prominent both inside and outside their building. The document provided does not demonstrate the steps to display appropriate signage inside and outside the building. SCHD referenced a photo of an outside sign for this requirement. Guidance F: The only mention of the marketing and branding plan being tied to the strategic plan is the statement “This plan, as alluded to earlier, is tied directly into the strategies and action items outlined in the SCHD Strategic Plan”. These strategies and action items are not mentioned. RD2: Example 1 - For the first example, SCHD provided an art proof of an outdoor tent with the SCHD logo on it. Example 2 - The second example is a media release with the SCHD logo on it. Both logos are surrounded by white space, which is part of their branding style guide. Areas of Excellence: SCHD has and utilizes a branding plan to identify themselves to those in their jurisdiction. Opportunities for Improvement: Not Available 3.2.3 A: Communication procedures to provide information outside the health department Score: Slightly Demonstrated Conformity: RD1: SCHD provided their media releases and requests for information policy. Guidance A: The policy states that any staff member designated to speak to the media should collaborate with the Public Information Officer (PIO) to establish clear messages that reflect SCHD’s position regarding the topic. There is no documentation related to the process for different audiences, nor how information is disseminated timely and appropriately. Guidance B: The policy states that any outside business, agency or organizations that are assisting in SCHD program efforts need to be mentioned in all media releases. There is no documentation of a process on how to inform and/or coordinate with community partners to promote consistent and unified public health messages that are accurate and appropriate for the audience. Guidance C: The policy contains a media distribution list. The policy states the list will be updated on a regular bases by the PIO, and that this list in the primary resource for dissemination of any media materials. Only media were listed. No key stakeholders were included in the list. Guidance D: SCHD provided the job description for the Community Health Outreach and Planning Division Manager. The job description states that 20% of this person’s responsibility is media relations and public information. This person is to serve as the media coordinator and may serve as the PIO during emergency responses. Guidance E: The policy states that any requests for information should be directed to the PIO. Also, any staff member designated to speak to the media should collaborate with the Public Information Officer (PIO) to establish clear messages that reflect SCHD’s position regarding the topic. No additional information is given regarding guidance or responsibilities.

P a g e 34 | 99
RD2: Example 1 - SCHD provided a media release, dated January 3, 2019, with the Community Health Outreach and Planning Division Manager listed as the PIO and contact person. This release is in regards to a smoke-free multi-unit housing lunch and learn. Partners are listed in the release per the media policy. Example 2 - SCHD provided a media release, dated January 23, 2019, with the Community Health Outreach and Planning Division Manager listed as the PIO and contact person. This release is in regards to a free child care licensing orientation event co-hosted by SCHD. Partners are listed in the release per the media policy. Neither example is for a chronic disease program, as required. Areas of Excellence: Not Available Opportunities for Improvement: The site visit team has identified an opportunity for improvement that goes beyond the Standard and Measure, SCHD should consider expanding the media release and requests for information policy to include requests for information from non-media sources. 3.2.4 A: Risk communication plan Score: Slightly Demonstrated Conformity: a) No protocol is mentioned for how information is provided for a given situation. The plan states that it may be used in preparation and/or response to all emergencies. The PIO will coordinate with other affected entities and the state health department to send out media releases. b) The plan notes that if there is no internet or electricity and if media access is unavailable to the public, there are alternative means of distributing information without the benefit of electoral power or internet access. These include posting of handwritten signs at disaster recovery centers and other locations, vehicle-mounted loudspeaker public address systems, and enlisting the aid of Medical Reserve Corp members. The plan mentions that the PIO is made available 24/7, however there is no information in the plan on how information is provided to the public 24/7. SCHD should add to the risk communication plan methods of how information is provided to the public 24/7. c) The plan states that the (PIO) is the Division Manager of Community Health Outreach and Planning; the back-up PIO for the SCHD is the Health Promotion Coordinator. The PIO will be activated by the SCHD Incident Commander. While chain of command is mentioned, there is no mention of their roles and responsibilities. d) The plan states additional communication methods will be employed if phone lines are unavailable, including but not limited to desktop or laptop computers, 800 MHz radios, public information, and face-to-face runners. The plan also states that the PIO might need to distribute information without the benefit of electrical power or Internet access; these methods include posting of handwritten signs and announcements made via vehicle-mounted loudspeaker public address systems. e) Before any information is released to the media, it must be cleared and approved by the Incident Commander. There is no information on how message clearance would be expedited during an emergency.

P a g e 35 | 99
f) SCHD will schedule news briefings as determined based upon the incident, and as directed by the Incident Commander. g) SCHD refers to Annex C of the plan, which contains fact sheets and links to public service announcements on various hazards and agents. These items will be used to educate the media and public about the hazard or agent, and it is noted that these materials, along with the usage of social media, will be important in reducing public alarm and misinformation. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 3.2.5 A: Information available to the public through a variety of methods Score: Largely Demonstrated Conformity: RD1: SCHD provided various screenshots of their website for this required documentation. Guidance A: SCHD has a contact number for 24/7 public health emergencies listed on their website. Guidance B: SCHD provides a link to the state health department’s reportable disease form on their website. Guidance C: SCHD provided a screen shot of mosquito surveillance in the county, with a chart showing the total number of mosquitoes caught in traps over a period of time. This does not meet the measure of providing health data. Guidance D: SCHD provided a screenshot of a webpage that had a link to the Shawnee County Code for pursuing complaints, as well as a link to the Home Rule HR2015-5 for required home refuse service. Guidance E: Information is provided for the Tobacco 21 program, with links to signage and fact sheets. Guidance F: SCHD provides web links to other public health agencies, including CDC, National Association of County and City Health Officials, Kansas Association of Local Health Departments, and the state health department. All of the links are specific to public health emergency preparedness and response. Guidance G: Links to leadership bios are provided for the Director and other leadership staff. RD2: Example 1 - For their first example SCHD provided a screenshot of their Facebook page, which shows a banner picture for National Nutrition Month 2019. Example 2 - The second example is a screenshot of a local news article (dated March 23, 2018) where a SCHD staff person reacts to the local tobacco 21 ordinance. Both are evidence that SCHD uses other methods to make information available to the general public about public health issues and/or functions. Areas of Excellence: Not Available Opportunities for Improvement:
P a g e 36 | 99
Not Available 3.2.6 A: Accessible, accurate, actionable, and current information provided in culturally sensitive and linguistically appropriate formats for target populations served by the health department. Score: Largely Demonstrated Conformity: RD1: SCHD provided information from the U.S. Census that demonstrates demographic and housing estimates for the county. Race and languages spoken in the home are listed by total households and percentage of the population. Data was downloaded March 12, 2019. RD2: SCHD provided their hearing impaired and interpretive services policy. In the policy they list several resources for those who are hearing impaired, for who English is not their first language and may need translation assistance, and a contact person for questions regarding the American with Disabilities Act. SCHD contracts with Voiance Language Services for over-the-phone translation assistance. During the site visit it was observed that SCHD had a Spanish interpreter on site, braille signs in the building, and power-assist doors at the entrance and to the public bathrooms. RD3: SCHD provided a job description for a Spanish interpreter/translator for the department. This does not demonstrate assistance for the hearing or visually impaired. RD4: Example 1 - SCHD has brochures in other languages; Example 1 is a brochure of department services in Spanish. Example 2 - SCHD provided a flyer in Spanish on 2 back to school immunization clinics being offered in the community. This is for individual health services and is out of PHAB's scope of practice. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 37 | 99
DOMAIN 4: Engage with the community to identify and address health problems Comments SCHD is a part of several community coalitions and partnerships that are addressing public health and health issues. SCHD should consider identifying those on their coalition/partnership rosters who are community members versus professional organizations. SCHD should also document any community, policy, or program changes as a result of the coalition/partnership’s work. While SCHD outlined their method of engagement with the pubic during the community need assessment process, they lacked documentation of providing consultation, technical assistance, or information to community partners or stakeholders concerning methods for collaborative community engagement. Engagement of members of the specific community or group that will be affected by a policy and/or strategy to promote the public’s health is done primarily through formal Board of Health or Committee meetings. STANDARD 4.1 – Engage with the public health system and the community in identifying and addressing health problems through collaborative processes. Comments SCHD is part of several community coalitions and partnerships that are addressing public health and health issues. SCHD should consider identifying those on their coalition/partnership rosters who are community members versus professional organizations. SCHD should document any community, policy, or program changes as a result of the coalition/partnership’s work. SCHD should provide and document technical assistance provided to community partners/stakeholders on methods of community engagement. 4.1.1 A: Establishment and/or engagement and active participation in a comprehensive community health partnership and/or coalition; or active participation in several partnerships or coalitions to address specific public health issues or populations. Score: Largely Demonstrated Conformity: RD1: SCHD provided information for 4 coalitions/taskforces they are involved with: 1. The first one is the Metropolitan Topeka Planning Organization Complete Streets Advisory
Committee. SCHD provided a meeting agenda for March 15, 2018; on the agenda the SCHD Director of Health is listed as attending. Minutes show that bike paths and speed ordinances were discussed, demonstrating this committee is addressing issues that impact on health. Additional information on the purpose, vision, and background of Complete Streets was provided, as well as a list of advisory member committees. Members of the Metropolitan Topeka Planning Organization include County Commissioners, Planning Department employees, Council people, and Transportation Planners.
2. The second set of documentation is concerned with a Farm and Food Council Taskforce. SCHD provided an agenda and minutes from a February 28, 2019 meeting. The goal of the Taskforce is to positively impact food systems changes in the county. A SCHD staff person is listed as attending. SCHD also provided a copy of the taskforce by-laws, with a statement highlighted that membership shall represent diverse food related sectors including the community at-large, youth, and senior citizens, among others. A timeline shows that this

P a g e 38 | 99
Taskforce has been in place since March 2018. Minutes state that a recruitment event will be held in May; there is no evidence in the documentation that representatives of the community impacted are on the Taskforce.
3. The third partnership is a Substance Abuse Task Force. SCHD provided an agenda and minutes from a January 17, 2019 meeting. Highlighted on the agenda is the SCHD providing an update on vaping. The minutes sate that the Task Force will continue to identify new methods of empowering youth and parents. If this is the Task Force’s target population, there is no evidence in the documentation of their participation on the Task Force. A print out from a Safe Streets webpage (unclear of relationship to Task Force) states that the Substance Abuse Task Force is comprised of school districts, youth serving organization, and others, however this is not evident in the documentation.
4. The fourth is a Healthy Babies Workgroup Summary, on SCHD letterhead, undated, and written for Domain 4.1.1. The summary includes the workgroup’s background, strategies, and focus. This workgroup was initiated by the Heartland Healthy Neighborhood (HHN) Coalition in 2013. A SCHD staff person is listed as the 2019 chair of the workgroup. No other workgroup members are listed; therefore there is no evidence of the community impacted being on the Healthy Babies Workgroup.
RD2: SCHD provided memberships lists for the 4 coalitions/taskforces listed in RD1. 1. The list for the Complete Streets 2018 Advisory Committee was provided. Members include
the county Park and Rec Department, the state Department of Transportation, the Area Agency on Aging, as well as the Citizen’s Advisory Committee and the local bike club, which is evidence of the community being involved.
2. The Food and Farm Task Force member list dated February 28, 2019 was provided. Members include several food stores, the school district, the American Heart Association, and the United Way. This list also includes “Community Members” and “Food Growers and Consumers”.
3. The membership list for the Substance Abuse Task Force, dated March 21, 2019, was provided. A wide sector is represented, but community members were not listed. Membership includes the faith community, Family Service and Guidance Center, Kansas Children Service League, the county sheriff, and Prevention and Recovery Services.
4. The list of Health Babies Coalition workgroup members/partners was provided. This list, dated March 18, 2019, includes healthcare agencies, the education sector (universities, local board of education), WIC, and “community members”.
RD3: Example 1 – SCHD provided documents related to the Shawnee County Farm and Food Advisory Council. A timeline highlighted that in February 2019 a resolution and bylaws were finalized, and in April 2019 a council membership application was finalized. Meeting agendas and minutes confirm that the work in the timeline was completed. The documentation provided does not reflect a community, policy, or program changed implemented through the Council, but rather steps taken to formalize the Council structure. Example 2 – SCHD provided a media release, dated October 19, 2018, for an annual community baby shower for safe sleep, happening on November 3. This event is hosted by the Heartland Healthy Neighborhoods (HHN) Healthy Babies workgroup, a partnership mentioned in RD1. SCHD also provided a flyer, booth reservation request, planning checklist, and lawn sign graphic as documentation.

P a g e 39 | 99
Areas of Excellence: Not Available Opportunities for Improvement: The site visit team has identified an opportunity for improvement that goes beyond the Standard and Measure, SCHD should consider adding organizational affiliations to meeting minutes. 4.1.2 L: Stakeholders and partners linked to technical assistance regarding methods of engaging with the community Score: Not Demonstrated Conformity: RD1: Example 1 – SCHD provided their Community Health Assessment (CHA) from November 2018, conducted by a consultant. SCHD emphasized the methodology for conducting the CHA, which included town hall meetings to gather data on wellness in the community. A press release included as documentation requested public feedback via an online survey or attendance at a town hall meeting, as well as the PowerPoint used by the consultant during the meetings. Documentation provides no evidence that the SCHD provided consultation, technical assistance, or information to community partners/stakeholders concerning methods for collaborative community engagement. Example 2 – SCHD provided an email invitation for the Director of Health to present at the 2018 Kansas Public Health Association conference because of the Department's work on Tobacco 21 policy. The conference program, provided as evidence, noted the Director was part of a panel that discussed “Loud and Local: Practical Information and Opportunities for Policy Action”. A PowerPoint presentation was included, dated June 19, 2017, and focused on how SCHD passed Tobacco 21 policy. SCHD also provided a Shawnee County Board of Health meeting agenda from June 19, 2017. On the agenda it is highlighted that the Department's County Health Officer presented “County Health Rankings – What will it Take to Improve Shawnee County Health”. No other documentation related to the agenda was provided. Documentation provides no evidence that the SCHD provided consultation, technical assistance, or information to community partners/stakeholders concerning methods for collaborative community engagement. SCHD should provide and document technical assistance provided to community partners on community engagement models. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 4.2 – Promote the community’s understanding of and support of policies and strategies that will improve the public’s health.
P a g e 40 | 99
Comments While SCHD outlined their methods of engagement with the public during the community need assessment process, they lacked documentation of providing consultation, technical assistance, or information to community partners or stakeholders concerning methods for collaborative community engagement. Engagement of members of the specific community or group that will be affected by a policy and/or strategy to promote the public’s health is done primarily through formal Board of Health or Committee meetings. 4.2.1 A: Engagement with the community about policies and/or strategies that will promote the public’s health Score: Slightly Demonstrated Conformity: RD1: Example 1 - SCHD provided a City Council agenda dated December 5, 2017. Highlighted under “Action Items” is the consideration of a resolution for a Tobacco 21 ordinance that would raise the legal age to purchase tobacco products from 18 to 21. Public comment is also listed on the agenda. Minutes from the meeting demonstrated that the Director of Health spoke in favor of the ordinance, and representatives from local convenience stores spoke in opposition. The ordinance was adopted. Example 2 – SCHD provided a memo to the Board of Shawnee County Commissioners from the County Legal Office dated February 18, 2019 regarding the possible privatization of the county Solid Waste Department. The resolution for this request was provided. Minutes from the Shawnee County Solid Waste Committee meetings held on February 27 and March 6 on this proposal showed that public comment was made from residents, and that a Committee member, who is also a SCHD employee, commented on the impact to public health if privatization occurs. The SCHD enforces the current county resolution regarding residents to have trash services. SCHD should document engagement of the community outside of formal City Council/Committee meetings, as both examples demonstrated residents engaging with councils, and not the health department. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 4.2.2 A: Engagement with governing entities, advisory boards, and elected officials about policies and/or strategies that will promote the public’s health. Score: Slightly Demonstrated Conformity: RD1: Example 1 - SCHD provided Board of County Commissioners meeting minutes from December 10, 2018. The minutes state that the Department is looking to create and hire a new position – a Community Health Planner – to help the Heartland Healthy Neighborhoods group implement and track outcomes of the 2019 Community Health Improvement Plan. A PowerPoint on the position was included as well as a news article on the search to fill the position. While the

P a g e 41 | 99
new hire will work on public health activities, there is no evidence in the documentation of a policy or strategy that will promote the public's health and the example was more informing the governing entity of actions rather than collaboration, as required. Example 2 - SCHD provided minutes from a Board of County Commissioners meeting held January 7, 2019. Highlighted in the minutes is one sentence stating that the Shawnee County Health Promotions Coordinator discussed initiatives regarding the increase in smoke-free multi-unit housing policies in the county. There is no evidence of collaboration per the measure. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
P a g e 42 | 99
DOMAIN 5: Develop public health policies and plans Comments SCHD has a central and active role in the establishment of policies and practices. SCHD’s CHIP identified 3 priority areas and goals and objectives for each, but did not address social determinants of health causes for higher health risks and poorer health outcomes of specific populations, and health inequities. SCHD has a strategic plan and involved multiple levels of staffing in the development of the plan as well as a representative of the governing body. SCHD maintains an Emergency Operations Plan for their Department. The plan clearing identified the roles and responsibilities of internal staff members. STANDARD 5.1 – Serve as a primary and expert resource for establishing and maintaining public health policies, practices, and capacity. Comments SCHD provides updates and information to their governing board, stakeholder and general public around policy development. SCHD also shared access to community and population data and information that provided knowledge. SCHD has a central and active role in the establishment of policies and practices. 5.1.1 A: The monitoring and tracking of public health issues that are being discussed by individuals and entities that set policies and practices that impact on public health Score: Fully Demonstrated Conformity: RD1: Example 1 – SCHD presented a newsletter the Director of SCHD received from the Kansas League of Municipalities on 1/5/18. The newsletter details public issues and the issue presented pertained to Tobacco 21 efforts in the State of Kansas. Example 2 - SCHD presented a newsletter the Director of SCHD received from the Kansas News Service on 4/5/19. The newsletter details public issues and the issue presented pertained to Medicaid Expansion efforts in the State of Kansas. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
5.1.2 A: Engagement in activities that contribute to the development and/or modification of policy that impacts public health Score: Largely Demonstrated Conformity: RD1: Example 1 is a published letter to the editor written by the SCHD Director in support of Topeka passing a Tobacco 21 ordinance. The contents of the letter include tobacco use

P a g e 43 | 99
statistics, and the health benefits seen by other cities that have passed a Tobacco 21 ordinance. This is a media statement and meets the first bullet point of the measure. Example 2 is a consent agenda memo from a Shawnee County Solid Waste Committee meeting with an action item of appointing new members to the Shawnee County Solid Waste Management Committee. The memo states that the Committee has reviewed the plan, written in 2015, and has no changes this year. However, this memo lists a SCHD employee as a new appointee to the Committee, after the plan was already reviewed and recommended to be adopted without changes. There is no documentation that SCHD was involved in the review of the plan, which was included for reference. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
5.1.3 A: Informed governing entities, elected officials, and/or the public of potential intended or unintended public health impacts from current and/ or proposed policies Score: Slightly Demonstrated Conformity: RD1: Example 1 – SCHD Director presented a presentation on Tobacco 21 to the Shawnee County Board of County Commissioners on August 3, 2017. The Shawnee County Board of Commissioners serves as the policy making authority for the County. The presentation by the Director touched on the health and economic impact that enacting Tobacco 21 policies would have on Shawnee County (how many people in Kansas die due to smoking; number of premature deaths in kids who start to smoke at an early age; millions in health care costs annually because of smoking). Example 2 –SCHD provided meeting minutes from a Shawnee County Solid Waste Committee meeting. It is noted in the minutes that a SCHD staff person, who is also on the Committee, spoke on potential public health impacts if trash service was to be privatized, including illegal burning of trash by people not being able to afford private trash service. Also included as documentation was a Solid Waste Management committee report to the Board of County Commissioners of Shawnee County, written by the Chair of the Committee (not a SCHD employee). This report included motions to provide 3 recommendations to the Board – hire a director of Solid Waste, study operating efficiencies, and start bargaining unit negotiations. There is no evidence of this example meeting one of the 3 bulleted items in the guidance. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
STANDARD 5.2 – Conduct a comprehensive planning process resulting in a tribal/state/community health improvement plan.
P a g e 44 | 99
Comments SCHD utilized a community group called Heartland Healthy Neighborhoods to conduct their community health improvement plan (CHIP). Their CHIP identified 3 priority areas and goals and objectives for each. However, there CHIP did not address social determinants of health, causes of higher health risks and poorer health outcomes of specific populations, and health inequities. SCHD should also consider a process to track actions to implement strategies in the CHIP, as this was lacking in the documentation. 5.2.1 L: A process to develop a state health improvement plan Score: Slightly Demonstrated Conformity: RD1: SCHD presented their 2015 Community Health Improvement Plan (CHIP) as documentation for this measure. a) The CHIP provided a wide variety of community partners ranging from 60 different agencies. Financial advisors, food banks, health care agencies, and school districts were some of the many organizations that were represented. b) Included in the CHIP is data compiled in order to determine the health issues that would be championed by the community partners. There were 14 issues that came out of the data sets and these issues were communicated to the broader group. This data and communication assisted in shaping the CHIP. c) Heartland Healthy Neighborhoods (HHN) represented the original brain trust along with the help of Healthy Shawnee County Task Force. The brain trust is the original group that came together for the purpose of making a change in the community. The HHN served as the coalition that would move forward with the CHIP. They took the issues presented in the 2013 CHNA and met to discuss and develop the 14 priority issues. The documentation shows that workgroups were formed around the public health issues identified to include: Healthy Babies, Healthy Eating/Active Living, Access-Transportation and Knowledge of Health Care Services, Complete Streets. The work groups met monthly and established objectives and strategies for getting the work accomplished. The issues identified by the community and stakeholders included: Babies in Shawnee County are dying at an alarming rate compared to state data; the obesity epidemic continues to be on the rise. It is costly to Kansans and threatens the long-term health and quality of life for residents; Public health experts and community focus groups identified access to transportation for patients and knowledge of health care services by health professionals as top issues in the 2013 Shawnee County Community Health Needs Assessment. There was no documentation of community members’ definition of health and of a healthy community as required per the measure. d) The SCHD listed their HHN Leadership Team, coalition members familiar with the CHNA and the plans for developing the CHIP as their resources. The process for identifying assets and resources was not documented. e) SCHD notes in the CHIP that the 14 priority health issues identified in the community health needs assessment were grouped into one of 3 categories to make them more manageable – infant mortality, overweight/obese, and access to health services. The categories were then used by the HHN to form workgroups that would develop plans for improvement in each area of focus. The process used to group into categories was not discussed in the documentation. Areas of Excellence:
P a g e 45 | 99
Not Available Opportunities for Improvement: Not Available
5.2.2 L: Community health improvement plan adopted as a result of the community health improvement planning process Score: Slightly Demonstrated Conformity: RD1: The SCHD presented their 2015 Community Health Improvement Plan (CHIP) as documentation for this measure. a) The CHIP lists 3 priority action areas: Healthy Babies, Healthy Eating/Active Living, and Access-Transportation and Knowledge of Health Care Services. Only the objectives under Healthy Babies and Healthy Eating/Active living had measurable objectives and a timeline (year) to reach the goal. While there are 2 data charts in the CHIP – population by race and poverty level/uninsured, there is no evidence in the CHIP of addressing social determinants of health, causes of higher health risks and poorer health outcomes of specific populations, and health inequities. b) The planners of the 2015 Community Health Improvement Plan addressed the need for policy change in their Healthy Eating objective by calling for the implementation of wellness policies and practices in organizations serving school aged children by the year 2018. As an example of a policy that has already been enacted to alleviate health inequity, SCHD presented evidence of the City of Topeka’s designation as “Bike Friendly Community” along with a report of the City of Topeka’s Pedestrian Master Plan that was taken from their website on 11/19/18. c) SCHD highlighted in their CHIP that the Heartland Healthy Neighborhood group was identified as the coalition to develop the CHIP. There is no evidence of individuals and organizations that have accepted responsibility for implementing the strategies. Under each priority area, only the strategy, outcome, and measure/indicator are listed. d) SCHD presented within the contents of the CHIP Healthy Babies Goal. Healthy Kansas 2020 and Healthy People 2020’s goal for Infant Mortality Rate (6.0 infant deaths per 1000) were also entered into evidence. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
5.2.3 A: Elements and strategies of the health improvement plan implemented in partnership with others Score: Slightly Demonstrated Conformity:

P a g e 46 | 99
RD1: SCHD provided their Strategic Plan 2019 Update, not their CHIP, for RD1. This does not meet the intent of the measure. RD2: Example 1 - SCHD presented ways in which they were able to implement an area of the plan. Strategy 1, Opportunity 5 of the 2015 CHIP called for hosting a community baby shower for safe sleep. SCHD presented a screenshot of their Facebook page that extended an invitation to the community to the shower, held November 3, 2018. SCHD was one of several hosts of this event. SCHD also provided a media release on the event that including statistics on SIDS and activities that were planned. Example 2 – In the CHIP, under the Healthy Eating/Active Living strategy, an opportunity for community action is to create a community garden network. SCHD provided a copy of the March 2019 Shawnee County K-State and Extension Newsletter in which a Shawnee County Community Gardens/Urban Farmers networking net-together event was scheduled for a date in March. There was no documentation of a specific achievement as required by the measure. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
5.2.4 A: Monitor and revise as needed, the strategies in the community health improvement plan in collaboration with broad participation from stakeholders and partners Score: Slightly Demonstrated Conformity: RD1: SCHD provided the agenda and PowerPoint from the 2018 annual meeting of the Heartland Healthy Neighborhoods group. The agenda lists “Work Group 2018 Progress” as a discussion item. The PowerPoint from the meeting was also included with bullet points and pictures of events done by each work group, but there is no comparison to the CHIP. A slide in the PowerPoint states that a “next step” is to develop the CHIP. The 2015 CHIP was also included as documentation. There is no evidence in the slides of consideration of the feasibility and the effectiveness of the strategies and/or changing priorities, resources, or community assets, as required. RD2: The same agenda and PowerPoint in RD1 was used for RD2. Also included as evidence is a contract agreement between Heartland Healthy Neighborhoods Coalition and the Kansas Health Institute to develop a new CHIP for 2019. A revised CHIP was not included in the documentation. There is no documentation of reviewing or revising the 2015 CHIP report used in RD1 as required per the measure. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 47 | 99
STANDARD 5.3 – Develop and implement a health department organizational strategic plan Comments SCHD has a strategic plan and involved multiple levels of staffing in the development of the plan as well as a representative of the governing body. They document progress towards achieving the goals and objectives contained in the plan. 5.3.1 A: Department strategic planning process Score: Largely Demonstrated Conformity: RD1: a) SCHD provided documentation listing the members of their strategic planning implementation team. Team members included the Director, a Clinic Nurse, an Epidemiologist, a Family Health Team Leader, two Office Assistants, and an Environmental Health Specialist. All-staff meetings and Supervisor/Management meetings were also held during the planning process. The document states that the SWOT analysis the goals and objectives, and the final draft of the strategic plan were sent to the County Commissioners (the governing agency) for review, and one meeting was held with one member of the governing agency to review the SWOT. A member of the governing entity is not listed on the strategic planning implementation team. b) The documentation lists the strategic planning team meeting from August 24, 2018 to February 19, 2019. The number of meetings per group was listed – for example, the strategic planning implementation team met twice, all staff met twice, and there was one meeting with a governing body representative. The documentation detailed their process including conducting a SWOT analysis, setting core values/vision/mission statements, and updating goals and objectives from the 2018 plan. The strategic plan implementation team identified stakeholders and their role, but there is no evidence of stakeholders reviewing the strategic plan. Areas of Excellence: SCHD is to be commended for their strategic planning process as it sets the course for their yearly activities. Additionally, the plan is designed so that everyone can see where they fit into the overall plan. Opportunities for Improvement: Not Available 5.3.2 A: Adopted department strategic plan Score: Largely Demonstrated Conformity: RD1: SCHD provided their Strategic Plan for 2017 to 2021. a) The Strategic Plan contains SCHD’s mission, vision, and values. b) There were 3 priority goals identified in the plan: Health Equity, Community Engagement, and Organizational Excellence. The 3 priority goals are then broken into 4 objectives and 15 strategies.

P a g e 48 | 99
c) An action plan is contained within the Strategic Plan and outlines the strategy, action steps, lists an action leader, and assigns a timeframe of “ongoing, 1-2 years, or 3-5 years”. d) SCHD’s Strategic Plan addresses capacity for and enhancement of information management within Objective 4; SCHD’s Strategic Plan addresses workforce development within Objective 4 (Create a culture of quality) Strategy 4.3 (Develop and implement plans for workforce development using PHAB standards and measures); SCHD’s Strategic Plan addresses communication (including branding) within Objective 2 (Coordinate health promotions, outreach activities, and programs to enhance community health and well-being) Strategy 2.2 (Use the SCHD Branding and Marketing Plan to implement health promotions and community outreach); SCHD’s Strategic Plan addresses financial sustainability within Objective 4 (Create a culture of quality)Strategy 4.4 (Maintain strong and sustainable fiscal management). e) SCHD performed a S.W.O.T analysis on the Department. The analysis covers the external/internal trends, events, or other factors that may the Department. f) SCHD performed a S.W.O.T analysis on the Department. The analysis covers the strengths and weaknesses of the SCHD. g) SCHD’s Strategic Plan addresses and links important goals of their CHIP. Objective 1 (Support the goals and objectives identified in CHIP Strategy 1.1 Increase Breast feeding initiation and duration rates among SCHD programs along with Objective 4 (Create a culture of quality) Strategy 4.2 (Develop and Implement plans for Performance Management and Quality Improvement using PHAB Measurements). Areas of Excellence: Not Available Opportunities for Improvement: Not Available 5.3.3 A: Implemented department strategic plan: Score: Fully Demonstrated Conformity: RD1: Example 1 - SCHD presented evidence of the evaluation of the 2017 Strategic Plan by the Strategic Planning Implementation Team dated 3/1/18. An agenda and meeting minutes of the team was provided as evidence of the development of the plan’s adoption and showing that it was reviewed and monitored to assess progress towards reaching its goals and objectives. SCHD Leadership Team Meeting minutes dated September 29, 2017 were also provided to show progress and monitoring of the strategic planning initiatives. SCHD also provided their tracking tool that they used to monitor progress. RD2: SCHD presented evidence of the evaluation of the 2018 Strategic Plan by the Strategic Planning Implementation Team dated 5/17/19. SCHD Leadership Team Meeting minutes dated February 5, 2019 were provided to show assessment and monitoring of the strategic planning initiatives. The Leadership Team Meeting also provides the documented recommendations to the strategic plan from the Leadership Team along with the dates the strategies from the 2018 plan were achieved. Monitoring of the strategic planning objectives and strategies were captured on SCHD’s Program Indicator’s Report. Areas of Excellence:

P a g e 49 | 99
Not Available Opportunities for Improvement: Not Available
STANDARD 5.4 – Maintain an all hazards emergency operations plan. Comments SCHD maintains an Emergency Operations Plan for their Department. The plan clearly identified the roles and responsibilities of internal staff members. SCHD should consider revisiting the plan after a drill or exercise and not any corrections made to the plan as a result. 5.4.1 A: Process for the development and maintenance of an All Hazards Emergency Operations Plan (EOP) Score: Largely Demonstrated Conformity: RD1: Example 1 – SCHD provided minutes from a Northeast Corner Regionalization Initiative meeting. SCHD is an active participant. The Kansas Department of Health and Environment and Doniphan County are all represented at this regional preparedness meeting. The minutes referenced past table top exercises, fit testing, and point of dispensing exercises that have been completed. Example 2 – SCHD is the coordinating agency for Emergency Support Function (ESF) #8. The minutes from a January 3, 2018 planning meeting was provided. SCHD, Shawnee County Emergency Management Team, local Hospice, Hospital and other agencies were present. At the meeting participants discussed strategies to ensure proper readiness in the event of an emergency. RD2: Example 1 – SCHD hosted an exercise titled “It’s a Long Way Home” on 10/17/18. An After-Action Report (AAR) was produced that details the exercise. a) Within the Exercise Overview are the participating organizations that included: Shawnee County Department of Emergency Management, Valeo Behavioral Health Care, Shawnee County Health Department, NEK Healthcare Coalition, and Tallgrass Surgical Center. The report details how the exercise deals with a severe weather event that requires coordination with the participants due to the threat level and possible destruction. b) The conclusions section of the AAR provides detailed, bulleted listing of primary areas for improvement, including recommendations for the participants to implement. Example 2 - SCHD participated in a Full-Scale Exercise titled “Shawnee County Operation Pegasus HazMat Plane Crash Bird Strike Full Scale Exercise (FSE)” on 7/20/17. An AAR, dated, 9/17/17, was produced and details the exercise. a) This FSE included many emergency response partners who coordinated the event. A complete list of participant is listed in Appendix B: Exercise Participants. b) Appendix A: Improvement Plan of the Official Report of the FSE provides detailed listing of primary areas for improvement, including recommendations for the participants to implement. RD3: SCHD provided their All-Hazards Emergency Operations Plan. The promulgation in the plan states that this is the Emergency Operations Plan for the SCHD of Topeka, Kansas and is a supplement to the Shawnee County Emergency Operation Plan which governs threats and

P a g e 50 | 99
emergencies within Shawnee County. SCHD did not present the County Emergency Operations Plan as required per the measure. a) SCHD minutes from an internal leadership workday meeting, where SCHD leadership was in attendance. No other county staff were in attendance. b) In the plan, Annex A lists COOP (Continuity of Operations) Teams and Responsibilities. Teams are broken down into Pandemic Team, Support, Devolution, Reconstitution, and Emergency Evacuation. All team members are SCHD employees, with the exception of a state epidemiologist on the Devolution Team. Next to each team members name is their responsibility/role. Appendix A also includes a key staff notification list with SCHD staff names, phone numbers (work, home, and cell), and emails. Only SCHD staff are listed. c) SCHD referenced the same list as in b. above, which is an internal list only. They also referenced the ESF8 – Public Health and Medical Services Partners – section of the plan, which goes into detail who is responsible for and the process of responding to medical surge, fatality management, epidemiology and surveillance, and medical countermeasure distribution, among others. A master list of primary agencies and support agencies, including SCHD as the Coordinating Agency, is included, but does not include roles and responsibilities. These are written directly into the plan. d) SCHD referenced the revision history page of the Emergency Operation Plan, which lists the date, author, and description of the change. However, this is not the revision page for the All Hazard plan as required by the measure. The full Emergency Operation Plan was also provided. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
5.4.2 A: Public health emergency operations plan (EOP) Score: Largely Demonstrated Conformity: RD1: SCHD provided their Emergency Operation Plan (EOP), dated May 17, 2019. The EOP states that it was developed using FEMA Comprehensive Planning Guide 101, Developing and Maintaining State, Territorial, Tribal and Local Government Emergency Plans. The plan states that special consideration will be addressed for unique and vulnerable populations. a) The EOP designated the SCHD Director as the person responsible for coordinating a response. b) The roles and responsibilities of SCHD staff and partners are well defined over the course of several pages within the EOP. These descriptions provide detailed information on what every member needs to do and what their role is within the EOP. c) SCHD Risk Communication Plan was presented to convey how information is communicated and disseminated during an emergency. d) SCHD’s Continuity of Operations Plan (COOP) was provided to portray their commitment to continuing operations during an emergency. The SCHD Director signed and dated the document on 3/29/19.

P a g e 51 | 99
RD2: Example 1 – SCHD provided their Emergency Operations Plan (EOP) dated May 2019 and an After-Action Report for an exercise held October 17, 208 that tested several public health capabilities as part of a grant deliverable. a) SCHD provided the “Plan Maintenance and Development” section of the EOP plan. This section states that SCHD will conduct independent training, exercises, and drills and will participate in exercises and drills in coordination with the Shawnee County Dept. of Emergency Management to test components of the EOP and relevant annexes. The document will be updated as needed after these events. b) SCHD provided an After-Action Report for an exercise testing several public health capabilities as part of a grant deliverable. The report included a summary, participant list, analysis of capabilities that referenced sections of the EOP, and an improvement plan. Example 2 - SCHD provided a memo dated May 21, 2019 from the SCHD Emergency Preparedness and Community Outreach Specialist to the SCHD Director regarding the process for testing and evaluating the emergency operations plan (EOP). a) This memo references the “Plan Develop and Maintenance Section” of the EOP, which states that SCHD will conduct independent training, exercises, and drills and will participate in exercises and drills in coordination with the Shawnee County Dept. of Emergency Management to test components of the EOP and relevant annexes. The EOP will be updated as needed after these events. b) An After-Action Report (AAR) dated April 5, 2019 for a tornado drill was provided. The AAR states that the tornado drill tested the SCHD EOP, as well as 3 public health capabilities. The AAR included an executive summary, analysis of capabilities, an improvement plan, and a list of participants. RD3: SCHD provided minutes from a leadership workday meeting, held May 14, 2019. A section of the minutes is entitled “All-Hazards Emergency Operation Plan Review”. a) The minutes describe a review of the EOP by the SCHD leadership team. Changes to be made to the EOP include eliminating some references, keeping ICS 300 and 400 training courses separate, and adding information as to where binders are located and include a hyperlink to folder on HACommon. There is no reference to any changes being made as a result of an AAR as required per the measure. b) The SCHD’s revised EOP was provided. An EOP revision history page is contained within the EOP detailing the changes, dates, version, and author. There a reference in the revision history page that the EOP was revised due to a collaborative review meeting, but not due to an evaluation or drill. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 52 | 99
DOMAIN 6: Enforce public health laws Comments SCHD has created an environment in which the enforcement of public health laws is well supported by leadership, training provided, and other agencies. More comprehensive department wide plans may be needed in some areas but the overall structure of the department has a functional enforcement department. A wide variety of enforcement activities are performed by the SCHD.
STANDARD 6.1 - Review existing laws and work with governing entities and elected/appointed officials to update as needed. Comments SCHD uses current laws and public health interventions but is not active in the review and recommendation process through external partners. The department is covered through the County Counselors office and has access to legal counsel to use for recommendation of proposed law changes. Many reviews that occur at SCHD are through internal process and protocols and not externally. 6.1.1 A: Laws reviewed in order to determine the need for revisions Score: Slightly Demonstrated Conformity: RD1: Example 1 - SCHD provided a review of a proposed Tobacco 21 ordinance. a) SCHD provided a PowerPoint presentation to the County Commissioners detailing how the Tobacco 21 will affect not only the health but the health equity of the youth in Shawnee County. This example demonstrated consideration of evidence-based practices. b) The health officer provided the commissioners with rulings from other states as well as additional penalties and stipulations. Specifically, this example used standards and guides from other states-18 states and 250+ cities- in the creation of the program for T21 in Kansas as a guide developed by others. c) The health officer for the county acted as the key stakeholder for the review. SCHD presented the review to the Board of County Commissioners where the county Health Officer was present. An email was sent as follow-up to the Health Officer. The T21 Program was not open for input outside of the County Commissioners and Health Officer. d) Neither example provided collaboration/input from the state health department. Example 2 - SCHD by provided meeting minutes from the Shawnee County Commissioners meeting discussing Solid Waste Regulation and the privatization of the entities providing those services. a) Concerns for the citizens health equity is discussed due to many citizens not being able to pay for trash service and the fear that illegal dumping and burning of trash will occur. This example demonstrated consideration of evidence-based practices. b) SCHD did not provide evidence to support the use of public health law models, checklists, or templates within this example. The Shawnee County Code was also provided but no standard use of public laws, templates, or checklist were utilized in the review of the resolution.

P a g e 53 | 99
c) The Solid Waste regulation review was open for public comment and gave stakeholders the opportunity to comment on the regulation changes. Stakeholders concerns included how the privatization will affect the current employees within the Solid Waste-Public Works department. d) Neither example provided collaboration/input from the state health department. RD2: SCHD provided a screenshot of the Shawnee County website where it is highlighted that the SCHD has access to the Shawnee County Counselor. As additional documentation the SCHD provided an email from the Assistant Shawnee County Counselor stating that she also represents the department. Within the email the Assistant Counselor provides examples of the work she has done for the SCHD including assisting in creating a new position and drafting MOUs. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
6.1.2 A: Information provided to the governing entity and/or elected/appointed officials concerning needed updates/amendments to current laws and/or proposed new laws. Score: Largely Demonstrated Conformity: RD1: SCHD provided two examples of providing the governing entity or other elected officials updates concerning current and proposed laws. Example 1 - SCHD provided a presentation to adopt the Complete Streets Plan and Design Guidelines. SCHD was involved in these efforts by being on the Complete Streets Advisory Committee. The purpose of complete streets is to ensure that city and county roadways are created with the consideration of all needs for all users of the transportation system regardless of age and ability. These recommended guidelines were adopted by the County Commissioners. Example 2 - SCHD provided communication between their Department and the County Commissioners on the Raise the Age Campaign. The County Commissioners approved the endorsement of the Raise the Age Campaign. The attached endorsement sheet contained statistical information on use of tobacco products by the youth in the US and Kansas for review before approval. An email response back was included with campaign information and endorsement page giving the SCHD approval to be a partner in the statewide initiative. While there were no specific written recommendations sent to the governing entity, SCHD provided an email thanking the governing entity for its support and the completed endorsement form from the Raise the Age Kansas campaign. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 54 | 99
STANDARD 6.2 – Educate individuals and organizations on the meaning, purpose, and benefit of public health laws and how to comply. Comments SCHD makes a conscious effort to ensure that they are communicating the public health laws, enforcement activities, and their implications with the public. SCHD is active on social media and their web page to make information readily available to the public. Training to their staff within the areas of expertise are also provided to stay current on the laws and regulations they are responsible for enforcing. 6.2.1 A: Department knowledge maintained and public health laws applied in a consistent manner. Score: Largely Demonstrated Conformity: RD1: SCHD provided two examples of training their staff in related fields. Examples provide are for Rabies Laws/Regulations and Investigation and Child Care Licensing Regulations which are part of the Kansas Administrative Regulations. Example 1 - SCHD provided documentation on training that was provided to the Clinical Services Division Manager who oversees the Environmental Health and Communicable Diseases programs. The contents of the webinar are focused on the animal health aspect of the rabies disease and interventions related to the animal and not the populations health making it outside of PHAB’s scope of authority. Example 2 is an attendance record for a regional childcare licensing meeting along with the presentation that was provided by the Kansas Department of Health and Environment. The staff in attendance were staff members of the Child Care Licensing Division. Public Health is responsible for regulating child care facilities and licensing. This training was for that programming and regulations that are associated with it. RD2: SCHD provided two examples of the application of laws. Example 1 - SCHD provided a letter to local business owners and managers informing them of the new minimum age requirement for the sale of tobacco products. Additionally, SCHD sites the repercussions of not following the new mandated regulations. Flyers with the new regulations were include for business owners to display with resource hotline information to quit smoking. This example does not provide the consistent application of the law, just an initial application. Example 2 - SCHD sent a letter to a local head start during a Shigella outbreak. They are reviewing the regulations for Child Care Licensing providers, Complaint Follow-Up procedures and Regulation reminders from the KAR (Kansas Administrative Regulations). SCHD states the regulations and recommendations for the isolation and quarantine of individuals during an outbreak situation. Additional information was provided through a link to the CDC. Due to the increased reports the Health Officer required all staff and students to follow strict guidelines to ensure they were no longer contagious before returning to school. This example does not provide a specific consistent application, but does highlight within the investigation regulations provided what consistent measures would be taken in the event of an outbreak. Areas of Excellence: Not Available

P a g e 55 | 99
Opportunities for Improvement: Not Available
6.2.2 A: Laws and permit/license application requirements are accessible to the public. Score: Fully Demonstrated Conformity: RD1: SCHD provided a screenshot of the department’s website for their Child Care Licensing Program. Along with a general overview of the program, SCHD provides additional documents and links including certificate information and application, starting a childcare business, and how to find child care in Shawnee County. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 6.2.3 A: Information or education provided to regulated entities regarding their responsibilities and methods to achieve full compliance with public health related laws. Score: Fully Demonstrated Conformity: RD1: SCHD provided a screenshot of a post on the SCHD’s Facebook page. This post included an attachment of the flyer that outlines the required immunizations for the 2018-2019 school year. Included in the picture of the flyer are the ages at which the children require vaccines, how many doses they should receive, and additional notes and recommendations for vaccines that are not required for school but are still recommended. These requirements are set forth by the State of Kansas and are not individual requirements for Shawnee County. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
STANDARD 6.3 – Conduct and monitor public health enforcement activities and coordinate notification of violations among appropriate agencies. Comments SCHD conducts and monitors regulated entities on a regular basis and remains in compliance with all grantors for outside grant programs. SCHD appears to have a knowledgeable and organized staff to complete all of these mandated regulations. The procedures for these inspections, especially in the area of Environmental Health are very detailed and organized.
P a g e 56 | 99
Communication plans and efforts with other agencies and the public are lacking in terms of a comprehensive plan or policy, not just for emergency purposes and outbreak situations. 6.3.1 A: Written procedures and protocols for conducting enforcement actions Score: Fully Demonstrated Conformity: RD1: SCHD provided two areas of enforcement code activities. Example 1 - SCHD provided tuberculosis regulations for enforcement. The authority is granted by the State of Kansas for Health Officers to be able to investigate any suspected tuberculosis case given reasonable doubt. Health officers have the authority to order medical examination of the suspected case in the event that the person of interest will not comply. Example 2- SCHD provided the Shawnee County Code which gives the Department the authority to conduct and enforce environmental regulations. These regulations include sewage systems and wastewater. RD2: SCHD provided 2 examples of the policies and procedures for the tuberculosis and environmental enforcement programs. Example 1 - SCHD provided a document that outlines the tuberculosis identification and treatment procedures including screening, evaluation, infection and disease treatment. These procedures have the forms needed to complete the investigations in bold print. Example 2 - SCHD provided a document that details the procedures for environmental health enforcement areas. These areas include various types of septic systems and their installment and inspections, complaints and follow-up, school inspections, open burning, trash haulers, landfill inspections, permits, and complaints, illegal dumping, wells, audits, outreach, and quarantines. Each section of environmental code gives step by step instructions of the operational process from start to finish. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
6.3.2 A: Inspection activities of regulated entities conducted and monitored according to mandated frequency and/or a risk analysis method that guides the frequency and scheduling of inspections of regulated entities. Score: Largely Demonstrated Conformity: RD1: SCHD provided the protocol for inspections of their regulated entities. Example 1 - SCHD provided the regulations set forth by Kansas Department of Health and Environment for Child Care Licensing programs. This program is awarded to the SCHD as grant money for the services provided. Through this grant award the SCHD agrees to inspect each Child Care Licensing Inspection once every 12 months. These inspection results are then tracked through a web-based database.
P a g e 57 | 99
Example 2 - SCHD provided the regulations set forth by Kansas State Statue that gives the SCHD the authority to conduct school building inspections. Per this statute the SCHD is required to perform one inspection for each school upon the opening of the fall term of school. Also included is a check off list given to inspectors for completion and then per their internal Environmental Health procedures are required to turn the completed form into the environmental health clerk. RD2: Example 1 - SCHD provided screenshots of the CLARIS web-based database application used for their Child Care Licensing program. Each Child Care Facility has their own page within the application where inspections and their results can be recorded. The application gives the current status of each facility, inspection reports, note sections for enforcement codes, observations, and a complaint tab. The license and current licensing information along with the application are also available to view. Within the CLARIS system there are multiple tabs for each facility. Within the tabs SCHD is able to record any enforcement actions, follow ups and return inspections, and final disposition. Example 2 - A completed school inspection form was presented containing the actions of the inspection however no log of various inspections and any follow up actions or return inspections are provided. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 6.3.3 A: Procedures and protocols followed for both routine and emergency situations requiring enforcement activities and complaint follow-up. Score: Largely Demonstrated Conformity: RD1: Example 1 - SCHD provided the SCHD Environmental Health Nuisance Complaint Tracking Form. This form tracks the following data quarterly: address, date complaint received, date SCHD are on-site, staff member assigned, letter status, date letter is sent, date the investigation is closed, additional comments, and the type of complaint. The follow-up procedure, in terms of failure to abate on the owner’s behalf, is detailed and states the violations and fine amounts for the owner. However, beyond tracking the information no formal analysis is done with the tracked data. Example 2 - SCHD provided the complaint tracking log for the Child Care Licensing program. This internal database contains the following information to be tracked: date complaint received, license number, name of provider, address, staff assigned, date investigation is initiated and completed, the complaint, and any comments. Follow-up and investigation protocols are detailed within the provided procedures for the program set forth by the Kansas Department of Health and Environment. However, beyond tracking the data, no formal analysis is completed. RD2: For Examples 1 and 2, SCHD provided settlement agreements through court hearing documents between the SCHD and defendants. Example 1 - SCHD provided communications to the defendants on what nuisances on their properties needed to be abated by a certain date. Upon completion the defendants are to

P a g e 58 | 99
contact SCHD for a follow-up inspection of the property. SCHD communicates with the Shawnee County Counselors office on the progress being made by the defendants. Example 2 - SCHD provided communications with defendants through a court hearing as well. The defendants were ordered to clean up the hazardous conditions of the property. To correct this nuisance a demolition had to be scheduled and the costs of that process we sent via certified mail to the defendant as well as information on the Tax Lien issued for the property. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
6.3.4 A: Patterns or trends identified in compliance from enforcement activities and complaints. Score: Fully Demonstrated Conformity: RD1: SCHD provided two annual reports from the Environmental Health Division. Example 1 - SCHD provided annual statistics of the nuisance complaints reported to the department, a description of the investigation process, and information about the responsibility of the SCHD to conduct nuisance complaints. Trends and patterns are identified at the end of the document with an explanation of why these trends or patterns are occurring. The report included compliance from the breakdown of complaints and also within the tracking system that is used for the Child Care Licensing. Example 2 - SCHD provided statistical information on the Child Care Licensing program. A breakdown of each type of complaint received is detailed within the report. Following this breakdown statistical information on the number of each of the complaints are listed. After analysis of the complaints, trends are reported with an explanation for the trends seen. The patterns are identified within the report used. RD2: SCHD provided 2 After Action Reports (AAR) for outbreak and case investigation situations. Both examples are set up in a standard format with a summary of the event, major strengths, major areas of improvement, and actions going forward. Both investigations and AAR were done as part of SCHD’s Child Care Licensing programming, making them examples of enforcement activities. Example 1 - SCHD provided information on a Shigella outbreak at a local head start. Areas of strength for the department are noted as good coordination between the state and local health department and great teamwork efforts. Areas of improvement were identified as communication of exclusion testing was sometimes difficult to get to local providers and finding alternative disinfecting methods as the school did not allow bleach products. Additional notes are listed within the conclusions section as lessons learned and what steps and recommendations can be made to refine plans, processes, and procedures in the future. Example 2 - SCHD provided information on a Varicella case that was reported in a school aged child. Areas of strengths noted were good coordination between the school nurse and SCHD and that the immunization requirements and records were easily accessible. Major Areas for Improvement were getting other groups to provide information needed to conduct an investigation. Additional notes are listed within the conclusions section as lessons learned and
P a g e 59 | 99
what steps and recommendations can be made to refine plans, processes, and procedures in the future. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
6.3.5 A: Coordinated notification of violations to the public, when required, and coordinated sharing of information among appropriate agencies about enforcement activities, follow-up activities, and trends or patterns. Score: Slightly Demonstrated Conformity: RD1: SCHD provided two communication protocols for enforcement activities. SCHD has a policy to follow the investigation protocol put in place by the Kansas Department of Health and Environment. Example 1 - In the first investigation protocol, Shigellosis Investigation Guideline, the guide states that the local public health department will begin an investigation and enter data into the Kansas Epi-Trax system. Additional notification is made to the case patient. Per this protocol the notifications are coming from the state health department rather than the local health department with the exception of the case investigation which would be a notification to one person and not another agency. Example 2 - The second protocol provided was their Rabies Investigation Guidelines. This guide details the investigation process; highlighted within these guidelines are the use of press releases which focuses on the dissemination of information and education to the public and not another agency. RD2: SCHD provided their Risk Communication Plan. In this plan SCHD details how they will notify the public in the event of a public health emergency or outbreak but did not outline the procedure that is used to notify the public of enforcement activities conducted by the department. RD3: SCHD provided two examples of media releases to the public. Example 1 - Entitled "Health Department Investigates Cases of Shigellosis", this media release provides information to the public about the current status of the outbreak situation within the county and additional information about the disease. Recommendations for those with symptoms are detailed such as staying home if ill, washing your hands, and not sharing food or drinks. This example is for a Shigella outbreak which is an infectious disease that the SCHD monitors. Example 2 - Entitled "World Rabies Day Reminds Importance of Pet Vaccinations", this media release highlights the importance of vaccinating household pets for the rabies virus. This release gives statistical information on the amount of rabies investigations performed by the department and what you should do if you are a victim of an animal bite. The first signs and symptoms are provided as well with a link to the CDC Rabies page. Because the release is focused on the rabies vaccine for dog and cats the article is outside the scope of authority set forth by PHAB.

P a g e 60 | 99
Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 61 | 99
DOMAIN 7: Promote strategies to improve access to health care Comments SCHD, via their Community Needs Assessment, has conducted an inventory of health services offered in the county, such as ambulatory surgery centers geriatric services, and mammography, and if the service is provided by the hospital group, the health department, or “other” entity. SCHD should document data sharing of availability of health care services with community partners, and emerging issues in their jurisdiction that could impact access to care. SCHD has an ongoing collaboration to address maternal and child health in their jurisdiction. Evidence is missing, however, if this group is experiencing access to care issues. SCHD should document the collaborative implementation of strategies identified by a workgroup looking at access to care to improve access to services for those who experience barriers in their jurisdiction. SCHD should incorporate and document cultural competence, language, or literacy in their efforts to address the health care service needs of populations who experience barriers to access to health care. SCHD has data for the total uninsured population in their jurisdiction. They should work with community partners to identify populations who experience barriers to health care services and document as appropriate. STANDARD 7.1 – Assess health care service capacity and access to health care services. Comments SCHD uses their Community Needs Assessment as documentation of assessing the healthcare needs of the community, who is having trouble accessing healthcare services, and gaps/barriers to accessing needed services. This was done in collaboration with their healthcare system. The documentation is missing evidence of analysis of emerging issues that impact access to care, and who in the jurisdiction is experiencing access to care issues. Documentation is also missing evidence of service gaps and barriers to accessing care. 7.1.1 A: Process to assess the availability of health care services. Score: Slightly Demonstrated Conformity: RD1: SCHD provided select pages from their 2018 Community Health Assessment (CHA). The CHA included an inventory of health services offered in the county, such as ambulatory surgery centers, geriatric services, and mammography, and if the service is provided by the hospital group, the health department, or “other” entity. Stormont Vail Health, the local healthcare system, collaborated in the development of the CHA, and a consultant was hired to conduct the CHA. A roster of participants for the 2018 CHA includes the 3 entities (SCHD, Stormont Vail, and the consultant). RD2: Example 1 – A press release (dated July 11, 2018), sent out by SCHD and Stormont Vail Health asks for public feedback via a survey and through attendance at town hall meetings to understands the need of the community. A final town hall was held September 27, 2018; the agenda and attendee list was provided as documentation. On the agenda the topic “final vote and determine areas of focus” was highlighted. There is no evidence of data sharing of availability of health care services as required per the measure.
P a g e 62 | 99
Example 2 – A media release notes that the 2019 County Health Rankings have been released, and that SCHD, with community partners, will be hosting a community discussion on the rankings as related to Shawnee County. The agenda for the meeting was provided and “Prioritization of Health Needs for CHIP” highlighted. The slides were provided, highlighted was a slide on clinical care. This slide shows Shawnee County clinical care ranking in 2018 and 2019, the percent uninsured, and primary care physician rate compared to Kansas. As with the first example in RD2, there is no evidence of data sharing of availability of health care services as required per the measure. The examples in RD2 are not related to the process identified in RD1. RD3: Example 1 – SCHD provided their Community Health Improvement Plan (CHIP) from 2015 as documentation for example 1. Highlighted in the CHIP is a priority area for Healthy Babies, where an objective is to increase the proportion of pregnant women who receive early prenatal care in the first trimester. Several strategies to meet these objectives were also highlighted. There is no evidence of an emerging issue that impact access to care for pregnant women. Example 2 - SCHD provided the same CHIP from 2015 as documentation for example 2. Highlighted in the CHIP is a priority area of “access/transportation and knowledge of healthcare services”. A goal of promoting awareness and connectivity to allow individuals access to community health and transportation resources, with objectives of reducing gaps and centralizing resources access is also listed. There is no evidence in the documentation of emerging issues that impact access to care. The examples in RD3 are not related to the process identified in RD1 (the CHIP was before the collaborative process). SCHD should document data sharing of availability of health care services with community partners, and emerging issues in their jurisdiction that could impact access to care. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
7.1.2 A: Identification of populations who experience barriers to health care services identified. Score: Slightly Demonstrated Conformity: RD1: SCHD provided their Community Health Assessment (CHA) from November 2018. The CHA project timeline is highlighted, as well as a “Phase II – Qualify Community Need” section which includes conducting secondary research to uncover historical community health status for the service area, and gathering primary research to uncover public health needs, practices, and perceptions. A section of the CHA notes the rate of uninsured and amount of charity care provided in the community. RD2: SCHD provided a report on the health status of black women in Topeka, Kansas written by the Kujima Health organization. In the report there is a chart on the percentage of adults that did not seek care due to cost by race/ethnicity in Kansas as a state between 2011 and 2015, but not by gender (i.e. black women) or for the department's jurisdiction. An agenda for a County Health Rankings Community Conversation was included; the report was released at this meeting. There is no evidence in the report of a population that is under- or un-served.
P a g e 63 | 99
SCHD should identify populations in their jurisdiction who experience barriers to health care services and document the process appropriately. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 7.1.3 A: Identification of gaps in access to health care services and barriers to the receipt of health care services identified. Score: Slightly Demonstrated Conformity: RD1: SCHD provided their 2018 Community Needs Assessment (CHA). SCHD partnered with their local hospital to hire a consultant to complete the CHA. SCHD highlighted the methodology used to complete the CHA, which included reviewing secondary data, gathering stakeholder feedback, and holding community town hall meetings. A community survey was included as documentation. This survey was used in the 2018 CHA and asked questions about the amount of services available to address health issues, the quality of the services, and the rating of the health services on a scale from “very good to very poor”. A barrier to access question was also asked. An open-ended question asked if there are any health care services or delivery issues that need to be improved, worked on or changed. RD2: Example 1 – SCHD provided their CHA from 2018; this document was the same as used in 7.1.1 so the same partners are present. a) The same survey used in 7.1.3. RD1 was provided as documentation. A question, “what amount of services are available in our community for these issues” was highlighted. There is no evidence of assessment of capacity and distribution of healthcare providers in the jurisdiction. b) A question, “what amount of services are available in our community for these issues” was highlighted, with a scale option of no services to enough services for items such as access to primary health care, alcohol/drug abuse, and cancer. c) A question, “are there any issues that prevent you and/or your family from using he community's health care services” was highlighted in the survey. Possible answers include cannot get an appointment, fear, and don't know how to find a doctor. No results were provided, just the survey question. There is no evidence of analysis of data and conclusions drawn as required per the measure. d) SCHD highlighted a chart in the CHA that showed the zip codes of those that responded to the survey. Also highlighted was a chart with the title “How would our community rate each of the following”, with responses such as ambulance services and child care, and a percentage number next to each. There is no explanation as to what the percentage means. For (D), SCHD also highlighted an inventory chart of health services in the county. This chart lists if the service is offered in the county (Yes/No) and if the service is provided by the hospital, health department, or “other”. There is no evidence of results for those who are experiencing access to care barriers. There was no report for RD2 outside the CHA. Example 2 – The second example is a 2019 County Health Rankings and Roadmap document for Shawnee County.
P a g e 64 | 99
a) Highlighted on the Rankings document is the primary care physician, mental health provider, and dentist rate per 100,000 population in the county annually from 2015 to 2019. There was no evidence of geographic gaps in the availability of healthcare providers. b) The same content as A was highlighted for B. There was no specific assessment of availability of healthcare services. c) On the Rankings document the percentage of uninsured for those under the age of 65 is highlighted. This does not demonstrate an assessment of cause for lack of access to services and barriers to access to care. d) SCHD provided news articles that the results of the County Health Rankings were shared with Commissioners. The county Medical Advisor discussed racial disparities from the Rankings at a Kujima Collective meeting, an annual meeting held as a result of the Ranking document being released. This does not demonstrate the results of data or information gathered concerning access. Both documents for RD2 do not offer conclusions that can help develop effective strategies to address gaps in access per the measure. SCHD should assess the capacity and distribution of healthcare providers in the jurisdiction. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
STANDARD 7.2 – identify and implement strategies to improve access to health care services. Comments SCHD has an ongoing collaboration to address maternal and child care health in their jurisdiction. Evidence is missing, however, if this group is experiencing access to care issues. SCHD should document the collaborative implementation of strategies identified by a work group looking at access to care to improve access to service for those who experience barriers in their jurisdiction. SCHD should incorporate and document cultural competence, language, or literacy in their efforts to address the health care service needs of populations who experience barriers to access to health care. 7.2.1 A: Process to develop strategies to improve access to health care services. Score: Largely Demonstrated Conformity: RD1: SCHD provided a fact sheet on the Heartland Healthy Neighborhoods collaborative. On the fact sheet the guiding principles of the group are highlighted, which includes a statement on convening with partners on health issues. Also provided is a leadership list for the collaborative; SCHD and hospital staff are listed as participants. An agenda and committee report for the collaborative dated March 21, 2019 states that the Healthy Babies work group of the collaborative is “working to engage school districts in discussion to expand services to pregnant and parenting teens in regards to community resources”. After requesting additional documentation during the pre-site visit review, SCHD provided a Healthy Babies work group
P a g e 65 | 99
attendance roster, noting dates of meetings held in 2019 and those who attended the roster listing those in the work group and an additional set of meeting minutes. Healthcare access was not the focus of the group, there was no evidence of healthcare access discussion in the minutes RD2: Example 1 – SCHD provided a resource guide for mothers and families, dated October 2018 and created by the Heartland Healthy Neighborhoods Healthy Babies work group. The resource guide is not a strategy as required per the measure; i.e. it is not clear how this example improves access to health care services, as required. Example 2 - SCHD provided work group minutes from a Healthy Babies meeting. Under key points discussed is to “assess and determine what are the barriers are to receiving prenatal care and work to address them to increase the percentage of women entering early prenatal care”. A healthy babies prenatal care survey was also provided. The survey asked 2 questions: 1) about reasons for unplanned pregnancy, and 2) what prevented you from getting prenatal care before 20 weeks. A handwritten tally of answered questions was provided. There is no documentation of what strategy was developed to improve access to care services. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 7.2.2 A: Implemented strategies to increase access to health care services. Score: Not Demonstrated Conformity: RD1: Example 1 - SCHD provided a memorandum of understanding (MOU), dated April 5, 2018, between a local health clinic, SCHD and the Kansas Immunization Program for deputizing and oversight of public health department to provide vaccines for children (VFC) purchased vaccine to entitled under-insured children. The MOU allows the SCHD to provide the vaccine to those eligible per VFC guidelines. The documentation does not show a collaborative implementation of a strategy to improve access to services for those who experience barriers and seems to be a clinical example, and so is out of scope. The documentation does not list activities, scope of work, and timelines per the measure. Responsibilities of the VFC provider are listed, and include screening children for VFC program eligibility and agreement to vaccinate walk-in clients. Example 2 – SCHD provided an agenda, sign in sheet, and minutes from a Shawnee County Advisory Council meeting held January 16, 2019. The Council is part of the local federally qualified health care center (FQHC). Service updates of the FQHC are listed in the minutes. These include finding a podiatrist, a new grant that would help with Medicare enrollment of children, and 5 areas of a program called Momentum 22 (none of which are healthcare related). There is no evidence of the Advisory Council addressing cultural competence, language needs, or literacy needs of their population in any of the service updates provided. SCHD should document the collaborative implementation of strategies identified by a workgroup looking at access to care to improve access to services for those who experience barriers in their jurisdiction. Areas of Excellence: Not Available

P a g e 66 | 99
Opportunities for Improvement: Not Available
7.2.3 A: Implemented culturally competent initiatives to increase access to health care services for those who may experience barriers to care due to cultural, language, or literacy differences. Score: Not Demonstrated Conformity: RD1: Example 1 – SCHD provided their policy on hearing impaired and interpretation services. No documentation was provided demonstrating initiatives to ensure that access and barriers are addressed in a culturally competent manner. Only the policy was provided. Example 2 – SCHD provided an agenda, sign in sheet, and minutes from a Shawnee County Advisory Council meeting held January 16, 2019. The Council is part of the local federally qualified health care center (FQHC). Service updates of the FQHC are listed in the minutes, however there is no evidence of the incorporation of cultural competence, language, or literacy in efforts to address the health care service needs of populations who experience barriers to access to health care as required per the measure. SCHD should incorporate and document cultural competence, language, or literacy in their efforts to address the health care service needs of populations who experience barriers to access to health care. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
P a g e 67 | 99
DOMAIN 8: Maintain a competent public health workforce Comments In the area of Workforce Development and ensuring the department maintains a competent public health workforce the SCHD deploys programs and interventions to strategically align the needs of Shawnee County and the workforce that is recruited and employed by the SCHD. SCHD engages with local universities in Topeka area that have pre-med and nursing programs. These students are given presentations and internship opportunities through the SCHD. Along with the internship programs and presentations SCHD enlists the students in the Shawnee County Medical Reserve Corp. SCHD created and adopted a Workforce Development Plan to ensure that they were recruiting and maintaining an educated, multi-disciplinary workforce. Efforts in workforce development included competency-based position descriptions workforce development training days for the entire department, and retention activities including recognition programs. To encourage continuous development the SCHD routinely performs personal development plans and employee evaluations. STANDARD 8.1 – Encourage the development of a sufficient number of qualified public health workers. Comments SCHD engages with local universities in Topeka area that have pre-med and nursing programs. These students are given presentations and internship opportunities through the SCHD. Along with the internship programs and presentations SCHD enlists the students in the Shawnee County Medical Reserve Corp. 8.1.1 A: Relationships and collaboration with educational programs that promote the development of future public health workers Score: Fully Demonstrated Conformity: RD1: SCHD demonstrated provided a letter of support from a local university. This letter acknowledges that the SCHD is an active participant in their program which promotes education of public health to help meet the health needs in the community. More specifically SCHD assists in programs such as nursing and the Medical Reserve Corps (MRC). Areas of Excellence: SCHD promotes public health as a profession by offering long-term internships and planning with local universities to incorporate public health into the curriculum.
Opportunities for Improvement: Not Available
STANDARD 8.2 – Ensure a competent workforce through the assessment of staff competencies, the provision of individual training and profession development, and the provision of a supportive work environment.

P a g e 68 | 99
Comments SCHD created and adopted a Workforce Development Plan to ensure that they were recruiting and maintaining an educated, multi-disciplinary workforce. Efforts in workforce development included competency-based position descriptions workforce development training days for the entire department, and retention activities including recognition programs. To encourage continuous development the SCHD routinely performs personal development plans and employee evaluations. 8.2.1 A: Workforce development strategies Score: Fully Demonstrated Conformity: RD1: SCHD provided their 2019 Workforce Development Plan. The plan included an assessment of current workforce and its present capacity while also addressing the gaps and ways to address these gaps or barriers. The workforce was assessed in multiple ways including by demographics which were broken down by gender, race, age, credentialing, FTE units, and the number of employees paid by grant or contracts. Gaps addressed by the SCHD were as follows: retirement, leadership development, diversity, grant writing, quality and performance improvement, and technology and security information. On the topic of technology and information security, SCHD discussed the changing environment of public health information systems and technology. To address these changes, SCHD states the importance of continuous training and development for not only their staff but also equipment. In addition to the technology and information security, the SCHD is also aware of the evolving areas of health equity and diversity. Within the workforce development plan SCHD discusses the need for health equity training and the skill that current and future workforce will need to engage with diverse and special populations. To help develop the workforce and its needs the SCHD adopted the Council on Linkages Core Competencies for Public Health Professionals. SCHD used this as a guide in development of core competencies developed for their workforce. SCHD had each employee take a self-assessment and rate their knowledge and skill level for varying tasks and competencies. Based on this assessment results were compiled and then later were used to identify barriers in their unique environment such as cost, time, and leadership support and communication. Through efforts made by the leadership and front-line staff SCHD was able to design a curriculum for their training needs to not only develop skills within their staff but to also to allow opportunities for continued education to be used for certain credentialing purposed for professions such as nurses and emergency preparedness staff. RD2: Example 1 - SCHD provided documentation discussing the future workforce needs and competency-based needs training, specifically in the area of diversity. SCHD states that when possible their workforce will reflect the demographics of the clients it serves. Example 2 - SCHD presented documents on a Workforce Development Day for leadership and staff. The material covered at this event included sexual harassment training, which is identified in the core workforce trainings as an all-staff training needed to be completed each year according to the Workforce Development Plan. To help better identify where their workforce had gaps in training gaps were identified by surveying the staff on cross cutting competencies within their workforce. Areas that presented with gaps were cultural competency and sexual harassment. These subjects were then used to add trainings and content into their Workforce Development Plan. These examples are addressing future plans and workforce development, which is not specifically implementation activities themselves, but are part of their current plan

P a g e 69 | 99
to perform the Workforce Development Days and planning sessions. Thus, they are implementing parts of their plans through these sessions and planning. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
8.2.2 A: A competent health department workfoce Score: Slightly Demonstrated Conformity: RD1: SCHD provided two competency-based position descriptions. Both examples, although different positions, have clearly stated requirements that the applicant must meet in order to be qualified for the job. In each case the position description states the specified degree for the position and that the degree must be earned from an accredited college or university. In addition to the degree requirements, the position description also specifies that you must also meet special requirements by completing National Incident Management System (NIMS) and Incident Command System (ICS) trainings within six months of employment. Both of the examples provided were only job descriptions were posted, not the way in which they were recruiting these positions. RD2: SCHD provided two different position descriptions; Spanish Interpreter/Translator and Community Health Planner. Although both of these position description emphasize the importance of the worker being culturally diverse and pertaining to the demographic of the community, neither example provides evidence of how the individuals are being recruited or any process on how to recruit these individuals. RD3: Example 1 - SCHD provided an application and email for their department staff to be nominated for a special annual award of excellence. No leadership is allowed to receive the award. Award selection is based on leadership in furthering the mission of the SCHD, fostering collaboration to improve the health of their population, building community/workforce capacity and advancing new approaches through innovation, and achieving impact by fostering opportunities for health. The recipient is then recognized at the annual Workforce Development Day. Example 2 - SCHD provided documentation for a Health and Wellness program they started for their employees. As part of the beginning efforts, the staff was sent an email explaining why this program was useful and important for them and asked to complete a survey. The survey was done anonymously and consisted of multiple-choice questions and also short answer where staff could add their own input and responses. In this example, SCHD is using those types of programs as retention activities and as a way to keep their employees. Within the survey provided they ask the importance of health and wellness programs for employees. RD4: SCHD provided two position descriptions which included a detailed description of the work to be performed, competencies required such as knowledge, ability, and skills, minimum qualifications for education and the required field of study, and any special requirements needed to preform assigned work. While both position descriptions have the same overarching theme the position for the Health Protection Manager is a more general job description while the Emergency Preparedness and Community Outreach Specialist has more specific

P a g e 70 | 99
requirements when it comes to degree fields and special requirements. Both descriptions are available to staff on a shared local server that can be accessed from the staff computers. The last page of each example’s documentation is a screen shot of the shared server for SCHD where all job descriptions are kept. Both job descriptions provided are for public health position, but Example 2 does not require a public health degree specifically, but rather an Environmental Health or Environmental Engineering degree - both do not list specifically public health specialty needs and generalist needs. RD5: SCHD provided their application screening and qualifications process. This process included the applicant meeting the minimum qualifications and being reviewed by two sets of staff members before being scheduled for an interview. Once an interview has been scheduled driver's license, degrees, and licensure/certifications are verified for current status and in good standing. After completion of these screenings and the interview has been conducted the applicant's references are contacted and additional screenings are in place. RD6: Example 1 - SCHD provided a staff licensing log. The licensing log includes the name of each employee and the degree that each employee holds. Following this information is the license or certification number and the expiration date for the licensure. A notes category allows for other information to be stated if needed. Staff positions listed on the tracking log include nurses, dieticians, social workers, and physicians. Example 2 - SCHD demonstrated conformity by tracking the CPR certifications for each employee. The employees are listed with their original training date and the expiration date of the certification. An asterisk is placed by the employee's names that are not required to be certified in CPR. All staff are added to a licensing tracking sheet. These are verified but evidence of following the entire process outlined in RD5 was not documented. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
8.2.3 A: Professional and career development for all staff Score: Fully Demonstrated Conformity: RD1: Example 1 - SCHD provided an all-staff training agenda on Armed Assailants. Along with the training agenda, SCHD also included the sign-in sheet of all staff that were in attendance. Example 2 - SCHD provided a training request for a grant writing course. The staff member requested to attend the training by filing the paperwork and then received approval. Along with the request and approval, SCHD also provided the training participation certificate that the staff member received post-training. RD2: Example 1 - SCHD provided the approval for the offices Finance Manager to belong to several financial officer groups in which training and additional resources are provided. Funding was granted to the finance officer to apply to these organizations and to have the health department cover the expenses. SCHD also provided the paid invoice for the membership dues for the Kansas Government Finance Officers Association.

P a g e 71 | 99
Example 2 - SCHD provided documentation for a member of the leadership team to attend a state-wide public health conference. Attached with the training request were the CEU's provided upon completion. RD3: Example 1 - SCHD provided a training completion certificate for Supervisor Situational Decision Making for the Clinical Services Division Manager. Along with the training certificate SCHD also provided the training attendance and expense request form with the direct supervisor's approval signature. An informational flyer for the seminar was also attached. Example 2 - SCHD provided a training certificate for advanced level ICS training from the Kansas Emergency Management Agency awarded to a member of staff leadership. Like example one, the training attendance and expense form were also provided. Both examples were provided by others outside SCHD, Example 1 was provided by the Kansas County Human Resources Association and Example 2 was provided by Kansas Emergency Management. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
8.2.4 A: Work environment that is supportive to the workforce Score: Largely Demonstrated Conformity: RD1: Example 1 - SCHD provided a policy from their Operating Procedures Manual that explains their breastfeeding during work policy. SCHD recognizes the documented health benefits from breastfeeding as the document states and note they will provide employees who are breastfeeding the opportunity to express milk during work hours. Example 2 - SCHD provided their quality improvement plan. Within the plan the SCHD addresses how Quality Improvement projects are selected and how the staff are encouraged to be an active participant in these processes. The plan also states the departments’ intention to provide their employees with the support, skills, and information they need to do their jobs and being able to make quality decisions and comprehending their actions within the workplace. These were the only two policies that were given. SCHD did not provide any examples of a comprehensive set of policies or multiple policies. RD2: SCHD provides their policy on Consumer Feedback from their Operating Procedures Manual. Within this policy is the positive feedback clause that allows leadership take the information on the positive feedback surveys and submit the staff member it involved to the Monthly Dose Employee Newsletter. In the monthly publication staff members who have been involved in positive feedback that month receive recognition in that month's edition of the newsletter. Also provided was a copy of the newsletter recognizing three of its current employees for their positive customer service. RD3: SCHD provided their Event Healthy Food Guidelines from their Operating Procedures Manual. Within this policy the department acknowledges the importance of a healthy diet and are supportive of a workplace that provides this for its employees. The policy states that for all official SCHD functions, drug representative lunches, and fundraisers the department has adopted the 2015 Guidance in Meeting and Events from the Healthy Workplace-Food and

P a g e 72 | 99
Beverage Toolkit by the American Heart Association. Any buffet dinners provided to the staff will also have the serving sizes and nutritional information available. Areas of Excellence: Not Available Opportunities for Improvement: Not Available
P a g e 73 | 99
DOMAIN 9: Evaluate and continuously improve processes, programs, and interventions Comments SCHD uses performance management and an adopted performance management system in an effort to monitor and improve the performance of the employees and the department. A performance management dashboard is used by the SCHD to track goals, objectives, and follow up actions. The Performance Management/Quality Improvement Committee is tasked with maintain the dashboard and monitoring progress. This committee completed a self-assessment of the department’s performance management system and provided training to the staff directly involved in the PM/QI process. As an extension of performance management, the SCHD also adopted a Quality Improvement Plan. Through this plan Quality Improvement Projects and the process of these projects such as selection and project results are outlined for staff use. The Quality Improvement team monitors the progress of these projects and the actions taken after completion. All levels of staff as well as multiple disciplines are involved with the Quality Improvement committee. STANDARD 9.1 – Use a performance management system to monitor achievement of organizational objectives. Comments Incorporated into the Performance Management and Quality Improvement System the SCHD show evidence of monitoring achievement by using a specific process to analyze and collect data over a variety of areas and programs. These measures have data collected at time increments that are also outlined in their plan. Leadership and staff are both invited and encouraged to participate in the PM and QI planning process and assessment. Staff and management are also provided with the ability to gain more training and education about PM/QI. 9.1.1 A: Staff al all organizational levels engaged in establishing and/or updating a performance management system Score: Fully Demonstrated Conformity: RD1: Example 1 and 2 - SCHD providing leadership meeting minutes to two separate meetings held by the department. The meeting materials showed that the leadership and upper management staff was actively involved in completing their performance management system, especially in the area of performance indicators. Meeting minutes, agendas, and other handout such as the performance indicators and organizational chart showing leadership was also provided. RD2: Example 1 and 2 - SCHD provided the completed Quality Improvement Plan which was approved and adopted by their Domain 9 work group. This work group was made up of front line and leadership staff members. Throughout the plan it is clearly stated that the frontline staff is actively involved throughout the performance management and quality improvement process. Also provided were meeting minutes from their Domain 9 work groups. Within these meeting minutes various topics were discussed by the members of the group such as

P a g e 74 | 99
performance indicators, creating the performance management system, and how staff should be trained on these topics. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 9.1.2 A: Performance management policy/system Score: Largely Demonstrated Conformity: RD1: a) SCHD provided a written description of performance standards and performance standards communications. The leadership team is in charge of setting the standards which are determined by their current Community Health Improvement Plan (CHIP), grant requirements, and other standards set by certain program regulations. Once these standards are set as priority goals they are then communicated to the staff in a variety of methods. Staff members of SCHD are emailed the final copy of these set goals and standards while the Board of County Commissioners (SCHD Governing Body) is provided with several drafts during the process and then a finalized copy. Community partners are involved throughout the CHIP process and are given the final copy through a group known as Heartland Healthy Neighborhoods Leadership Team. b) SCHD provided the departments 2019 Inaugural Performance Management System Plan. Within this plan is a background and description of performance management systems, how the Turning Point Performance System Framework will be used in public health, the overview of their own system, and training provided. As appendices the department provides their Strategic Plan, Program Indicators, and Quality Improvement Plan.The data is collected by the SCHD Leadership Team and then reported on the Programs Indicator Spreadsheet. This data is collected quarterly on April 30, July 31, October 31, and January 31. c) SCHD provided a written description of how progress is reported as well as the analysis of data, communications of these results, and how often reporting is done. The committee meets two times throughout the year with meetings set in August and February. The purpose of these meetings is to analyze the progress made on the set performance indicators. While analyzing this data they look for trends of current improvement and areas that need improvement. Once a final report is compiled of the analyzed results, the report is then forwarded to the staff members, leadership team, and the county commissioners. d) SCHD did not demonstrate conformity on their process for using the above mentioned data results, managing change for quality improvement, and creating a learning organization. SCHD stated that the QI Committee chooses QI Projects based on the analysis of their performance management data but do not continue on to describe or provide a description of the process for doing so. Within the document there is an Analysis of Data section and a Quality Improvement Section. While for Requirement C SCHD states that they analyze data 2 times per year and look for trends of improvement and areas that need improvement, going into Requirement D the plan states that they choose QI projects based in part on the analysis of performance management for the above data. There is no clear process of how this is analysis is done or what is weighted when doing the analysis or choosing programs and indicators.

P a g e 75 | 99
Areas of Excellence: Not Available Opportunities for Improvement: Not Available 9.1.3 A: Implemented performance management system Score: Fully Demonstrated Conformity: RD1: SCHD provided their 2019 Inaugural Performance Management Plan. Within this plan they included their May 17, 2019 meeting minutes where the team, made up of all levels of staff, gave updates on various QI Projects and also reviewed and analyzed the first Quarter Program Indicators. Throughout the analysis qualitative and quantitative data was reported and ways to improve based upon the reports were made. RD2: SCHD provided two examples of goal setting and objectives for the department. Example 1 - The first example provided is a programmatic, Child Care Licensing. This programming falls under the jurisdiction of Environmental Health. The goal was set to recruit more childcare providers to license through outreach activities. Example 2 - The second example provided is administrative evaluations. The goal set was to ensure evaluations were completed on time with a target of greater or equal to 90%. Both examples demonstrate identified time frames for measurement – Example 1 has an annual timeframe (with Quarterly Reporting) and Example 2 has a quarterly timeframe. RD3: SCHD provided their Performance Management Program Indicators Dashboard. Example 1 - Within the objectives and measures data is collected on a quarterly basis and then entered into the dashboard by the assigned staff person. These results are then discussed at the quarterly meeting of the Domain 9 team. Example 2 - The second example is from the same plan but highlights a different portion of the plan. In this section the department is taking the running total of the quarterly results and comparing the data to data from 2017 and 2018. This information is then again reviewed and discussed at the quarterly meeting of the Domain 9 team. The two examples provided are the implemented processes from RD2. The examples are for Child Care Licensing and Administrative Evaluations. RD4: SCHD reviewed and performed a root cause analysis on the two goals set in RD2: Child Care Licensing and Evaluations. SCHD discussed both examples at quarterly Quality Improvement Committee Meetings. After progress made on the target goals were presented to the committee a root cause analysis of these results was performed to decide where to go and the future steps for these goals to meet their targets. For both examples, the objectives were analyzed in the correct timeframes as specified in the previous RD. RD5: SCHD had a Domain 9 team meeting where each member of the team reviewed their performance data. Through this data review, team members identified where there were opportunities to improve to increase or decrease their targets as they were set. For the specific example presented, the department is trying to increase their childcare licensing program by gaining outreach opportunities such as the county fair, community-wide events, and a Safe Sleep event. The documentation provided continued the two examples provided for the measure - Child Care Licensing and Administrative Performance Evaluations. RD6: SCHD created two self-assessments, one for front line staff and one for supervisors and managers. All staff members were emailed an invitation to take the assessment with the link
P a g e 76 | 99
that corresponded to their job classification. Once the survey link was closed the Domain 9 team members met to analyze the 2 sets of survey results and assess the data that was provided. Through this review the team determined areas for improvement in their Performance Management Processes. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 9.1.4 A: Implemented systematic process for assessing customer satisfaction with health department services Score: Fully Demonstrated Conformity: RD1: SCHD provided two customer surveys: Family Planning and Community Conversation survey. Example 1 - The first example, Family Planning, was provided in both English and Spanish, and was available in paper form, on Survey Monkey for community partners to share, and by boosting the survey post on Facebook. Results from this survey was compiled in various graph form and then shared with the County Commissioners (Governing Entity) along with a message to pay special attention to certain elements of the results. Example 1 was a satisfaction survey on the services offered for family planning at SCHD. Example 2 - The second example provided was given to community stakeholders about the facilities and event held by the SCHD after the Annual County Health Rankings. The stakeholders invited to participate in this event and survey came from a wide-range of businesses and community members including local health care providers, correctional facilities, Boy Scouts, insurance plan providers, and local educational systems and universities. The ending results were compiled and presented during a Supervisor-Manager Meeting. Results also included additional comments left by the participants as qualitative data. During their Community Conversations to discuss the Annual County Wide Health Rankings, a representative was there from the Kujima Collective for representation of a special population. This is a group that address black women’s health equity and access. For both examples, this information was analyzed and distributed by the SCHD director to the governing entity and stakeholders. Responses through Survey Monkey were compiled into graphs and charts. Through an email to the stakeholders the SCHD Director points out specific areas to look at. RD2: SCHD used the results from the surveys in RD1 to prepare interventions to improve. Example 1 - The Family Planning Survey Results were presented at the Board of County Commissioners meeting with a request to apply for funding for Family Planning grant dollars through the Kansas Department of Health and Environment. It is noted that this funding will be used to address gaps in the services available to the community as presented in the survey results. Example 2 - SCHD provided documentation on the analysis and actions going forward from the Community Conversations. Results from the survey were provided to the leadership committee. Based on these results a larger space was needed and scheduling around subgroup meeting. To correct one item of concern SCHD leadership will reserve the 3 conference rooms instead of 2

P a g e 77 | 99
for the upcoming community conversation. The first example is the SCHD applying for a family planning grant as a result of the analysis and conclusions drawn and is population-based. The second example is the actions taken based on the results of their Community Health Needs Assessment. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 9.1.5 A: Opportunities provided to staff for involvement in the department’s performance management Score: Fully Demonstrated Conformity: RD1: Example 1 - SCHD provided a prerecorded webinar on performance management. Specifically staff who are on the Domain 9-Performance Management team were present for this training. 5 speakers were presented to the staff from the Public Health Foundation through a PowerPoint entitles Performance Management: Improving the Improvement. Also presented with the staff sign in and PowerPoint were the minutes from the Domain 9 team meeting. Example 2 - SCHD provided their senior level staff and supervisors with a Domain 9/ Performance Management training in 2017. This training reviewed the basics of domain 9 and its measures and also went into detail on the process for performance management and different ways to record data and see results. A sign in sheet was not able to be provided but the department provided email RSVP confirmation pages with the meeting name and accepted messages from each staff member present. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 9.2 – Develop and implement quality improvement processes integrated into organizational practice, programs, processes, and interventions. Comments Through the development of performance management the SCHD has also developed a Quality Improvement system. This system uses data that has been collected and analyzed to choose and implement quality improvement projects and goals. To achieve this the SCHD utilizes all levels of staff to carry out the projects, collection of data, and monitoring of progress and achievements. 9.2.1 A: Established quality improvement program based on organizational policies and direction

P a g e 78 | 99
Score: Fully Demonstrated Conformity: RD1: SCHD demonstrated conformity by providing a Quality Improvement Plan that was implemented in January 2019. Within this document the department provides the reader with a glossary of commonly used terms that will be used throughout the plan. They have also provided commonly used public health acronyms that someone may need to understand certain aspects of the plan. Based on NACCHOS Roadmap to a Culture of Quality Improvement, SCHD identifies that they are currently in Phase 2 of creating a quality of culture. Due to leadership buy in they believe this will be an area that they will excel in the future. The plan included key elements of QI structure, as required. In order to make sure active participation is occurring training is mandatory for all new staff members within the first two weeks of hire. To educate existing staff, the QI team gives updates at each monthly staff meeting. The leadership staff are more extensively trained on an annual basis. In order to provide continuous quality improvement, the QI meets annually to review their Strategic Plan and the data collected by their performance management plan. Based off of this data the highest priority projects are chosen first for the reason of linking to the strategic plan and meeting the strategic goals most efficiently. The second highest priority is based on the performance data that is collected. Other considerations for project selection are the impact made in the community and the amount of energy staff have for the project. Within the plan SCHD outlines their quality goals, objectives, and implementation. SCHD had two main Quality Improvement goals: Implement plan for Quality Improvement using PHAB standards and measures and moving from phase 2 to phase 3 of a QI culture. For these two goals the department set objectives and activities on how this were going to be reaching these goals. They then set measures and timeframes for the work to be done and assigned a staff member from the QI Council or a council as a whole to be responsible for these goals. To monitor their progress on these goals and objectives the QI Council meets once a year in July. A survey is completed by the council members as well as a facilitated discussion about progress made, effectiveness of meetings, and integration of improvement into the department. To keep staff members engaged and informed on the quality improvement efforts made by the department Quality Reports are given during all staff meeting and quarterly updates are available through the Quarterly Newsletter. The Board of Health is provided an update of the improvement activities on a quarterly basis and updates are shared with the public are able to view updates online and on social media for the department. Finally, the QI Plan as a whole is evaluated at the annual meeting in July. Through this process the council looks at the phases of the Roadmap to a Culture of Quality, any lessons learned, and the clarity and effectiveness of the plan and its associated documents. A review of this evaluation will be considered and influence any revisions that may need to be made to the plan. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 9.2.2 A: Implemented quality improvement activities Score: Fully Demonstrated
P a g e 79 | 99
Conformity: RD1: SCHD demonstrated conformity by following the Quality Improvement Plan and Processes implemented by the department. One program area and one administrative area were chosen for the projects. Through the narrative (minutes) the SCHD describe how staff problem solve, select improvement areas, and determining possible causes of the problems. QI team members then work together to create the best solution and then implement the plan for improvement. For each project SCHD set time-framed targets to be improved upon by April/May. Within these timeframes the department set specific targets to be reached to show improvement. To document the continuous quality improvement the department uses the Plan-Do-Study-Act (PDSA) improvement tool. The QI team documented team communications throughout the meeting minutes and summarized within the PDSA tool. The two programs chosen were Child Care Licensing (programmatic) and Performance Evaluations (administrative). RD2: SCHD provided meeting minutes for two different QI project meetings. Within these minutes they state the particular project that the team is working on, which staff members are present, and the date and time of the meeting. For each of the minutes the team have a streamlined process for conducting these meetings. The following is the agenda and actions during the meeting from beginning to end: Introduction, Program Indicator Review, describe problem and desired outcomes, flow chart, root cause analysis, test solutions, data collection and follow-up, and next meeting review. Through the minutes template the staff also discusses and notes their key discussion points, actions, and decisions. Also noted is who is in charge of making sure these points and actions are being carried out and monitored and stated any follow-up notes and timeframes. Staff was involved in both examples provided. The standard minute’s template used list staff names involved. Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 80 | 99
DOMAIN 10: Contribute to and apply the evidence base of public health Comments SCHD uses promising practice in public health programming and interventions. They obtain IRB approval when needed. SCHD has an Epidemiologist on staff and contracts with individuals in the public health field for medical consultation and analysis of public health trends. Results of research findings and their public health implications are communicated to stakeholders, public health system partners, and/or the public. STANDARD 10.1 – Identify and use the best available evidence for making informed public health practice decisions. Comments SCHD uses and documents the use of promising practices in their programming and interventions. The practices come from reliable sources. Target audiences for the promising practices are identified. 10.1.1 A – Applicable evidence-based and/or promising practices identified and used when implementing new or revised processes, programs, and/or interventions Score: Fully Demonstrated Conformity: RD1: Example 1 - a) SCHD provides pages from the National Prevention Council's Best Practices for Comprehensive Tobacco Control Programs (undated document). Highlighted in the document is a statement that smoke-free multi-unit housing policies are a best practice in the creation of smoke free housing. SCHD also provided a printout of a County Health Rankings and Roadmaps document highlighting that smoke-free multi-unit housing policies are a suggested strategy to reduce second and third-hand smoke exposure (dated June 4, 2019). b) For inclusion in a new or revised public health process, program, or intervention SCHD provided pages from a Chronic Disease Risk Reduction SFY2019 application, noting a goal of increasing the number of multi-unit housing properties in the county with smoke-free ordinance from 3 to 5. The target population is noted to be Shawnee County residents in multi-unit housing. Example 2 - SCHD provided several documents for a Kansas Perinatal Community Collaborative “Becoming a Mom” (BAM) prenatal education curriculum. a) This is a promising practice created by the March of Dimes. Documentation includes that guidance for implementation of group prenatal education resources. SCHD also provided a BAM state aggregate report for 2017 which recommends the curriculum to address infant mortality, sudden infant death syndrome, and low birth weight. b) For inclusion in a new or revised public health process, program, or intervention SCHD provided several documents. These include a BAM implementation training agenda and PowerPoint slide deck from a 2 day training held May 2017. An email chain between the state BAM coordinator and SCHD staff demonstration that SCHD were trained in the curriculum and the BAM program was incorporated into the Shawnee County Baby Basics program. SCHD

P a g e 81 | 99
provided an action plan with due dates and staff responsible outlining the steps needed to become facilitators and implement the program. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 10.2 – Promote understanding and use of the current body of research results, evaluations, and evidence-based practices with appropriate audiences. Comments SCHD obtains IRB approval when needed. SCHD has an Epidemiologist on staff and contracts with individuals in the public health field for medical consultation and analysis of public health trends. Results of research findings and their public health implications are communicated to stakeholders, public health system partners, and/or the public. SCHD should send their research findings to the state health department. 10.2.1 A: Protection of human subjects when the health department is involved in or supports research activities Score: Fully Demonstrated Conformity: RD1: SCHD provided a letter from the State of Kansas Department of Health and Environment, Director of Science and Surveillance, granting IRB approval for a Fetal Infant Mortality Review (FIMR) project. This is a copy of the IRB approval from the institution where the IRB review was done and meets the measure. Areas of Excellence: SCHD obtains IRB approval when appropriate.
Opportunities for Improvement: Not Available
10.2.2 A: Access to expertise to analyze current research and its public health implications. Score: Fully Demonstrated Conformity: RD1: SCHD provided a list of 3 experts: their Department Epidemiologist (staff), their County Health Officer (contracted), and their Tuberculosis Consultant (contracted). Supporting documentation for the Epidemiologist included the job description and the employee's resume. In the job description is the responsibility of “analyze the status of

P a g e 82 | 99
indicators on health outcomes and risk factors in the community. Conduct epidemiological research/disease investigations and draw sound conclusions available data”. Supporting documentation for the County Health Officer included his bio, license, and contract for services. The contract states this individual will provide professional medical and health services for the County (not direct medical care). In the contact responsibilities may include “1) communicating with staff about trends and best practices at the national level to improve effectiveness and efficiency in the organization and delivery of public health essential services, 2) establishing health policy and issue public statements about the public's health, and 3) Identifying public health priorities and emerging trends”. Supporting documentation for the Tuberculosis Consultant included a resume, license, and contract for services. Services include providing SCHD nursing staff with medical supervision and orders which allow for the treatment of clients with tuberculosis infection or disease. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 10.2.3 A: Communicated research findings including public health implications Score: Not Demonstrated Conformity: RD1: Example 1: SCHD provided an Epi-Surveillance newsletter, dated November 19, 2018, developed by their department. Highlighted in the newsletter are life expectancy at birth estimated calculated by the US Small-Area Life Expectancy Estimates Project (USLEEP). The newsletter goes on to describe the datasets for Shawnee County according to the County Health Rankings model, which includes census tracks, social and economic factors, and demographics. This does not meet measure requirements of information being analyzed and conclusions drawn. SCHD also provided 15 pages of emails as a distribution list. Only emails are provided therefore there is no evidence of the document being sent to the state health department as required per the measure. Example 2: SCHD provided minutes from a Board of County Commissioners meeting held April 22, 2019. In the minutes the Director of Health reported that their Epi-Surveillance newsletter was released and that their Epidemiologist spoke to the Commission regarding the rise in sexually transmitted diseases (STDs) in the county. The newsletter, dated April 15, 2019, was included. Charts in the newsletter show rates of reported STDs for the county from 2008 to 2018. Sources of the date were the Kansas Department of Health and Environment (KDHE) STD Case Rate Report and the CDC STD Surveillance 2017 report. A question and answer part of the newsletter described public health implications of the rise of certain STDs. This does not meet measure requirements of information being analyzed and conclusions drawn. SCHD also included a distribution list for the Epi-Surveillance newsletter (dated May 21, 2019), but only emails are listed. It is unclear from the list if the document was sent to the state health department as required per the measure. Areas of Excellence: Not Available

P a g e 83 | 99
Opportunities for Improvement: The site visit team has identified an opportunity for improvement that goes beyond the Standard and Measure, SCHD should consider adding organization affiliations to their distribution lists.

P a g e 84 | 99
DOMAIN 11: Maintain administrative and management capacity Comments SCHD has many administrative functions in place to ensure that the organization is operating in the most effective capacity. SCHD has a multitude of policies, procedures, and interventions in place to maintain an operational infrastructure to support the department’s public health functions. SCHD has an extensive Operational and Human Resources Manual including confidentiality and being competent and linguistically appropriate. Multiple information systems and security systems are in place to keep information secure and up to date. In addition, the facilities are not only clean, safe and secure but are also in compliance with many ADA regulations. SCHD’s finances are approved and directed by the Board of County Commissioners (Governing Entity). In order to operate the department SCHD receives funds from the County Commissioners, fees, and grants for various programs. These sources of revenue are monitored by the County Commissioners, SCHD, and the agencies who are awarding the funds through program reports, MOUs, and independent audits. STANDARD 11.1 – Develop and maintain an operational infrastructure to support the performance of public health functions. Comments SCHD uses the basic human resources functions and operational infrastructure to support and run the day to day operations of the department. Policy development and staff input, as well as access is utilized often and on a regular basis. Maintenance of policies, procedures, licenses, and regulation are routinely performed and all staff are involved in these processes. 11.1.1 A: Policies and procedures regarding health department operations, reviewed regularly, and accessible to staff Score: Fully Demonstrated Conformity: RD1: SCHD provided a table of contents from their Administrative Policies and Procedures Manual. Within this manual 2 policies were highlighted. Example 1 - The first policy provided is for the use and scheduling of the meeting rooms. Within this policy the capacity for each room is listed as well as the step by step procedures on scheduling. Example 2 - The second policy provided is for the Code “E” Procedure. This procedure is provided for staff to have step by step instructions on what to do in a medical emergency. The policy lists who should be notified, location of emergency equipment, and a flow sheet to document the incident. RD2: SCHD provided two organizational charts in use for the department. The first is a functional organizational chart showing the different divisions and what functions they are responsible for performing. The second is chart provided is the organizational chart, complete with the full-time equivalents of each position listed. The chart is broken down from the director and upper management to division managers and front-line staff. Each position within the divisions are listed around to their specific job title. The current 2020 organizational chart was provided at the time of the site visit. RD3: Example 1 - SCHD provided their policy review calendar. The leadership team is responsible for reviewing a number of policies and procedures annually. Each policy is reviewed
P a g e 85 | 99
by an assigned reviewer and then determined if the policy has been reviewed, revised, or abolished. Example 2 - This example continues from Example 1 by providing meeting minutes and an agenda from the leadership meeting held. At the meeting the policies in need of a revision are discussed and the group collaborates to create the revision. The leadership is then assigned the next month's polices for review. Both examples provided evidence of policies being revised. Some were removed for being obsolete and others were revised for clarification. All policies were administrative and department wide. RD4: SCHD provided a screenshot of the availability to the staff on their shared server. Policies and procedures are also available to the staff through the county website. Upon revision and review, the policy is emailed to the staff to review and has the change made listed. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.1.2 A: Ethical issues identified and ethical decisions made Score: Not Demonstrated Conformity: RD1: SCHD provided the Vaccine Allocation Model from the University of Maryland. This model is use to help determine how many people and of which populations need to receive a vaccine within a target population. SCHD does not have a department wide ethics policy as of their June 2019 submission date. SCHD used a Vaccine Allocation Model that is only used to determine how vaccinations would be distributed during a pandemic or shortage. There was no other documentation provided to show evidence of the process to evaluate ethical situations or issues that arise. RD2: SCHD provided an example of the deliberation and resolution of a dress code violation/grievance made by an employee. In the WIC division a team leader and peer counselor had differing ideas on the dress code in place. Under the current dress code items such as nose piercing was not acceptable to be worn. However, the peer counselor had been wearing this item for over a year before it had been questioned. After a review of both party's statement's via e-mail the leadership team discussed and made the decision to amend the dress code to include jewelry that does not disrupt their job performance. However, this example does not demonstrate review and revision of an ethical issue. The employee brings up that it is unethical, but it is not truly an ethical issue, rather more of a personnel issue. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.1.3 A: Policies regarding confidentiality, including applicable HIPAA requirements
P a g e 86 | 99
Score: Fully Demonstrated Conformity: RD1: SCHD provided 2 policies - the employee confidentiality agreement and a business associate agreement. The first policy is the destruction policy and procedure of confidential records. The policy ensures that confidential information is secured during disposal and has a detailed procedure to ensure the policy is successful. The second policy is the HIPPA Confidentiality Breech policy. The policy is in place to ensure that each employee understands what information falls under the HIPPA regulations and how you could be in breech of the policies. The signed employee confidentiality agreement is an extension of the breech policy. The employee is asked to review the terms of the policy and then sign that they agree to adhere to the policy and procedures in place. The last document provided is an agreement between SCHD and an information management provider. Throughout the document the confidentiality of the clients of the department are listed. Also laid out within this contract is the information that the agency is allowed to disclose and their obligation to keep the data and information secure. Both personal information and health or other information is protected. Their confidentiality policy and HIPPA policy discuss the protocols for this. RD2: SCHD provided two examples of training offered to employees by the department. Example 1 - SCHD provided documents from a staff workforce development day. HIPPA and the employee confidentiality agreement was presented. Additionally, the staff signed the employee confidentiality agreement after the training stating that they would adhere to the confidentiality guidelines. Example 2 - The second example was from a confidentiality make-up training. This training was made available to those who has previously missed the annually scheduled training day. For both examples the PowerPoint of the training presented and a sign in sheet was provided. RD3: SCHD provided a signed copy of the employee confidentiality agreement as previously mentioned in RD1 and RD2. Also provided is a copy of the sign in sheet that was used for the training and the agenda for the training day. Both are have a signature of the employees who have attended and who have signed the agreement. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.1.4: Policies, processes, programs, and interventions provided that are socially, culturally, and linguistically appropriate to specific populations with higher health risks and poorer health outcomes. Score: Largely Demonstrated Conformity: RD1: SCHD provided two documents for RD1. The first document was the SCHD Strategic Plan. Within this plan the SCHD lists health equity as a priority goal for the SCHD to address. The second document provided is the SCHD Racial Equity Impact Analysis Workgroup. The purpose of this group is to make sure that when preparing programs and interventions they are created
P a g e 87 | 99
in the most effective way to improve the health of their community in a culturally competent manner; their purpose is also to review policies and procedures to make sure they are culturally competent and meeting the needs of the disenfranchised in the community. To do this the SCHD uses a Racial Equity Impact Analysis Tool to assess new policies, programs, and educational materials. This tool also includes a survey for the individuals who attend the workgroup meeting. These survey questions ask questions such as age, ethnic origin, gender, marital status, employment status, disabilities or impairments, and education. RD2: SCHD provided two examples of internal operational policies. Example 1 - A disaster plan for tornados policy states the reason for the protocol and the procedure for when a tornado occurs. The pre-recorded message that is played over the intercom for the staff and the clients of the department is first read in English and then is replayed in Spanish. At the beginning of the message there is a prompt stating that it is the following message is bilingual. Example 1 does not specifically apply to the programs offered, just a means of communication to the clients in the building during this disaster. Example 2 - The second example provided is a Facebook screenshot of the need for input from the public for the Community Health Needs Assessment Survey. This online survey is offered in both English and Spanish. Also provided is the Spanish version of the Community Health Needs Assessment Survey provided through the link. RD3: SCHD provided a cultural competence and knowledge of health equity self-assessment. The 64-question survey was distributed to health department staff via email. After the staff completed the survey an analysis was done of the results. Based on the analysis results the leadership team made recommendations of what needs to be done in the department to improve their cultural competence and health equity knowledge. RD4: SCHD provided an agenda for an all-staff meeting, where a speaker was invited to talk about cultural competence. Included along with the agenda is the PowerPoint presentation of the speaker’s content. Throughout the presentation staff persons were asked to text into a poll to answer questions about their organization anonymously. Attached with these materials is the all staff sign in sheet with signatures of the staff present. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.1.5 A: A human resources function Score: Fully Demonstrated Conformity: RD1: SCHD provided a human resources manual containing the following elements: 1. A resolution from the county commissioners adopting the human resources policy manual
is provided. Within the manual the first chapter states the purpose and legal requirements of the jurisdiction.
2. The next section bookmarked is the process and regulations for recruitment, hiring, and placement. This section explains the approval of positions, advertisement of postings, applications, interviews, pre-employment screenings, and new hire orientation.
P a g e 88 | 99
3. Confidentiality is also addressed in the human resources manual. This confidentiality not only covers the employee but also discusses the confidentiality of clients and their records.
4. SCHD states that they are an Equal Opportunity Employer and that the department takes affirmative action to ensure equal opportunities for employment are provided to individuals regardless of race, sex, age, religion, creed, veteran status, physical or mental disability, and nationality. These EEO/Affirmative Action Policies were adopted by SCHD in 1996 with periodic updates.
5. SCHD Human Resources Manual describes the departments salary schedule in terms of compensation ranges for full time employees, compensation of temporary employees, compensation for part-time employees, and compensation for intermittent employees.
6. For each of the salary schedules the SCHD defines the hours of work in the areas of work weeks, flextime, overtime, and off the clock work. Further explanation is detailed with how the hours of work are calculated and when the hours of work should be turned in to a supervisor or HR manager.
7. SCHD has a multitude of benefits that are provided to employees along with a detailed descriptions and procedures. These benefits include vacation leave, sick leave, military leave, funeral leave, jury duty, holiday time off, personal leave, Family and Medical Leave Act, sharing of leave, domestic violence and sexual assault leave, life insurance, health insurance and disability benefits.
8. SCHD provides employees with a performance evaluation policy and procedure for their staff to be able to measure employee’s performance and effectiveness. Also provided to the staff is a guide for developing and implementing a performance improvement plan (PIP) for employees. This guide gives staff an overview of the evaluation process and walks the employee through each step of creating and then implementing the PIP.
9. Three types of harassment have a no tolerance policy at the SCHD. These include general harassment, sexual harassment, and workplace misconduct. If any of these occur the coworker or employee receiving the harassment has a detailed complaint/grievance policy that will be followed to resolve the issue. Complaints are investigated as rapidly and fairly as possible without fear of repercussion. SCHD makes every effort to find an acceptable solution for all parties involved.
RD2: SCHD provided a screenshot of the intraweb system that is an available to all Shawnee County employees. Through this system SCHD employees are able to access human resources policies and procedures, as well as the manual and employee benefits. RD3: SCHD provided an agreement between the SCHD and the Shawnee County Commissioners, where the Teamsters Union is representing the SCHD employees. Within this documentation the Teamster Union is responsible for acting on behalf of the SCHD employees when making changes and negotiations to working relationships or manual changes for the department. RD4: SCHD provided 2 examples for RD4: Position Descriptions and the Teamster Contract. Example 1 - Two position descriptions for the Administrative Officer and Administrative Assistant were included. Both position descriptions state that the knowledge required for these positions is concentrated on human resources management including hiring practices, disciplinary procedures, terminations, etc.. The position descriptions also state the need for an ability to establish and maintain effective working relationships with employees, the public, and other County personnel. Position descriptions are used for example one showing that the department actively used and Administrative Officer and Administrative Assistant to operate in the human resources capacity. Example 2 - A contract between the SCHD and the Teamsters Local Union was provided. SCHD has employees who belong to a bargaining unit. This contract works to protect the worker’s rights and conditions. The Teamsters contracts are
P a g e 89 | 99
the employment agreements for the employee unions and the county agencies. For this example, SCHD has demonstrated that they have dedicated people working on HR functions and are actively working with a union for personnel reasons. Areas of Excellence: Very extensive HR Policy and Procedure Manual Opportunities for Improvement: Not Available 11.1.6 A: Information management function that supports the health department’s mission and workforce by providing infrastructure for data storage, protection, and management; and data analysis and reporting Score: Fully Demonstrated Conformity: RD1: SCHD provided 2 examples of information systems that support their public health functions. Example 1 - A compilation of screenshots of their access into the Kansas Grant Management System was provided. Within this system they have multiple programs including Chronic Disease Risk Reduction, CRI Public Health Preparedness, HIV Prevention Program, and Child Care Licensing Program. For each of these programs there are areas for administration, insurance and billing, and Aid to Local where program and expenditure reports are uploaded. Example 2 - An Excel spreadsheet used for documenting and tracking Environmental Health Nuisances was provided. This spreadsheet included the date the complaint is received, date the investigation is started, which staff person is responsible for follow up on the nuisances, information on communication with the property owner or location of nuisance, and the type of nuisance reports. This spreadsheet is available for staff usage on the shared server drive. This was the information system that they provided and it seemed like this was what was mainly used. While at SCHD many uses of technology were observed: intercom system throughout the entire building, WIFI access in public and private areas, charging stations for clients, climate-controlled server room with locked access, security cameras, and access to the Shawnee County IT Department. When IT services are needed a request is put in through the County Commissioners and then a member of the IT staff will look into the request to resolve the problem quickly. RD2: SCHD provided the Shawnee County Human Resources Manual. The Information Technology Policy within this manual state that each department may choose to utilize additional restrictions on technology at their own discretion but a general policy is laid out for use by all departments. This policy is shared on the Shawnee County intraweb site under the Information Technology section. Within the policy guidelines and restrictions are laid out to ensure general information technology security as well as data security. The policy is broken into 6 sections: Applicability and Exemptions, Security (General, Passwords, Physical Security and Data Security), System/Data Access (General and Remote Access), Acceptable Use (General, Personal Use, Internet Access, Social Media E-Mail, and Equipment), Audit Policy, and Policy Exemption Notification Policy. Personnel are obligated to report ant instances of misuse to the Department Head. The Shawnee County Internal Auditor has the authority to preform random audits/security reviews of the county technology resources. These audits could result in information and reports of information systems being requested by the Internal Auditor. An
P a g e 90 | 99
additional appendix is available to staff on creating strong passwords and the do’s and don’ts of selecting passwords for information systems. RD3: SCHD provided their Employee HIPPA Confidentiality Agreement. This agreement defines confidential information, protected health information, personnel information, business operations information, third party information, receive, receipt, use disclosure, health department's workforce, and computer systems for the employee to understand the definitions and examples of information that should remain confidential and secure. The policy continues to give the employee a detailed explanation of how the confidential data and information should be handled once received. Within this information the SCHD states that the use and disclosure of confidential information is governed by federal and state laws and regulations as well as the SCHD’s policies and procedures. RD4: SCHD provided the Shawnee County Information Technology Department's Strategic Plan for 2019. This plan is created to ensure that the departments in the county (including the health department) are able to execute their primary daily functions that are dependent on technology. Strategies within this plan include the continuation to implement newer technologies and methodologies to be as secure, effective, and efficient as possible and to provide a stable network infrastructure that allows access to all necessary internal and external technology resources. RD5: SCHD provided an inventory listing of the electronic data systems used by the department. For each of the data systems, an explanation of who is using these systems and what program area the electronic systems are being utilized is provided. For example EpiTrax- used in Communicable Disease and Emergency Preparedness Programming. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.1.7 A: Facilities that are clean, safe, accessible, and secure Score: Fully Demonstrated Conformity: RD1: SCHD provided their CLIA lab certificate. SCHD has a current certificate for compliance that will expire in December of 2020. Certifications for SCHD are mycology and parasitology. The Kansas State Health Department provides select agent lab services for the SCHD as documented. RD2: SCHD provided 2 examples of occupancy and inspections for their building. Example 1 - Documentation shows that the fire extinguishers in the JP Lewis Building are checked and are in active status. The checklist provided includes the locations of each fire extinguisher with the date it is checked and who is certifying the inspection. Example 2 - SCHD provided a certificate of occupancy issued by the City of Topeka to the SCHD. The certificate specifies that for the square footage of the building you can have an occupancy of 428 people. This occupancy certificate was last updated in 2017 by the City of Topeka’s Chief Building Official. While at SCHD the facilities were presented as clean, safe, accessible, and secure. Observations made were security cans through the halls and public areas, locked private access doors that can only be opened with a SCHD issued key card, handicap accessible entry doors, bathrooms, front

P a g e 91 | 99
desk, and water fountains, all guests going into private, staff-only areas are required to sign in and out at the front desk and are issued a visitors badge. SCHD also has a tornado shelter in the middle of the building due to being in a high-risk tornado area geographically. RD3: SCHD provided a completed ADA Checklist. In addition to the ADA Checklist the SCHD also provided a letter from the Schwerdt Design Group certifying that the SCHD is in compliance with the requirements of the ADA Standards and the Life Safety Code as well as zoning, building, fire, health, and other governmental laws, ordinances, and requirements in effect at the time of design and construction. This letter was provided to the county in August 2018. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 11.2 – Establish effective financial management system. Comments SCHD’s finances are approved and directed by the Board of County Commissioners (Governing Entity). In order to operate the department SCHD receives funds from the County Commissioners, fees, and grants for various programs. These sources of revenue are monitored by the County Commissioners, SCHD, and the agencies who are awarding the funds through program reports, MOUs, and independent audits. Regular audits, recording of expenses, and budgeting is done on by SCHD. SCHD is not a high-risk grantee and maintains competent financial records and audits. In an attempt to fund the public health for their county they apply for grant money to support their efforts in improving the counties health 11.2.1 A: Financial and programmatic oversight of grants and contracts Score: Fully Demonstrated Conformity: RD1: SCHD provided two examples of audited financial statements. Example 1 - Documentation was from the 2016 Shawnee County Audit. Example 2 - Documentation was from the 2017 Shawnee County Audit. While Shawnee County is audited as a whole, the SCHD has a separate breakout for the health agency fund on the balance sheets provided. These audited statements are completed by an independent auditing firm for the SCHD. RD2: SCHD provided program reports from two different areas within the department. Example 1 - SCHD provided an interim grant report submitted by the SCHD for the Fetal Infant Mortality Review (FIMR) Grant. This report is sent semi-annual to funders of the FIMR Grant. Example 2 - SCHD provided a quarterly program report submitted to the Kansas Department of Health and Environment for the Child Care Licensing Program that is administered by the SCHD. The report is submitted through the Catalyst electronic reporting and application system. RD3: SCHD provided a sworn statement from Director that the SCHD has not received any communications within the past 5 years from state or federal funders that indicate the SCHD is classified as a “high-risk” grantee.
P a g e 92 | 99
Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.2.2 A: Written agreements with entities from which the health department purchases, or to which the health department delegates, services, processes, programs, and/or interventions Score: Fully Demonstrated Conformity: RD1: SCHD provided two examples of written agreements with entities to provide a service for the SCHD. Example 1 - SCHD provided documentation of an approved MOU with the Washburn Rural High School to be used as an open Point of Dispensing (POD) location during a public health emergency. Within this agreement the Washburn Rural High School agrees to provide the usage of facilities, grounds, and equipment for dispensing purposes at no cost to the SCHD. The health department will be using the space in the agreement to provide public health services when needed to the community. The school is providing the space for the health department to be able to perform these services. Example 2 - SCHD provided documentation of the purchase of services from the Topeka Community Cycle Project. Through the MOU provided the SCHD agrees to purchase bicycle lessons, safety training enhancement, adult bike education, enhanced bicycle repair, and bicycle advocacy for the implementation of their Chronic Disease Risk Reduction grant. To fulfill grant requirements the health department has to purchase the items listed. The health department is not providing these- they are just paying for the service to be provided to fulfill the grant and receive funding. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.2.3 A: Financial management systems Score: Fully Demonstrated Conformity: RD1: SCHD provided their 2019 approved budget for the department as approved by the County Commissioners. Along with main summary sheets for the budget SCHD provided the excel worksheets that are used in computing the figures for the budget. These are broken into divisions: Administration, WIC, Immunizations, Clinic-STI, Environmental Health, Child Care Licensing, Maternal Child Health, Grant and Non-Grant Funds, Public Health Emergency
P a g e 93 | 99
Preparedness, and Community Health Outreach. Also provided is the SCHD five-year budget for the included 2019 year. Approved 2020 SCHD Budget was provided at the time of the site visit. RD2: SCHD provided monthly financial statements from June 2018 and July 2018 creating the two examples required. The monthly reports created by the SCHD contain line items for each expense and revenue item that has been accounted for during that month. Expenditures and revenues are reported separately between each of the division listed in RD1. A comparison of the budgeted expense and revenue for each of the lines are listed as well as the actual cost of operations to gauge the accuracy of the budgeting process and to track cash flow. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 11.2.4 A: Resources sought to support agency infrastructure and processes, programs, and interventions Score: Fully Demonstrated Conformity: RD1: SCHD provided 2 examples of efforts to seek funding from additional financial resources. Example 1 - SCHD provided a grant application for SFY19 to the Kansas Department of Health and Environment requesting funding for various programs through the state department including State Formula, Child Care Licensing, Chronic Disease Risk Reduction, Maternal and Child Health, Immunizations, and Public Health Emergency Preparedness- Local and Regional. SCHD requested a total of $987,367.00 in grant funds. Along with the grant application SCHD also provided the Board of County Commissioners approval to apply in the form of meeting minutes. Example 2 - SCHD provided an application for funding from the Kansas Governor's Council on Fitness- Walking Enhancement Funding to increase the accessibility and walkability of the Shawnee County trail network. This grant application requested the funding amount of $9,780.00. Accompanying the request for funding and application was the approval from the Board of County Commissioners in the form of meeting minutes. RD2: SCHD provided two communications with the public and the Board of County Commissioners pertaining to the need for financial support. Example 1 - SCHD provided a presentation to the Board of County Commissioners on the importance of having funding for a Community Health Planner to work with the Heartland Healthy Neighborhoods. Along with the presentation and meeting minutes granting approval SCHD also provided an article from the Topeka Capital Journal on the big picture of community health and the new position that needed to be filling by the department. The article details the funding structure and a description of that the position would entail putting emphasis on the community health focus. Example 2 - SCHD provided a request to enter into an agreement with Custom Data Processing (CDP) to purchase Electronic Health Record (EHR) Software. SCHD staff explained the benefits to the Board of County Commissioners of being able to use an EHR system. Also presented to the Board of County Commissioners was a PowerPoint from CDP on the company, features of the EHR system, and a breakdown of the operations of the system.

P a g e 94 | 99
Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 95 | 99
DOMAIN 12: Maintain capacity to engage the public health governing entity Comments State statute outlines SCHD’s mandated authority to conduct public health activities in the jurisdiction. SCHD provides documentation to the Board of County Commissioners concerning the health department’s responsibilities, as set forth in the health department’s authorizing documents. The Department has an extensive Board of County Commissioners orientation packet, however a written process for implementing the orientation is lacking. Communication to the Board of County Commissioners regarding important public health issues is done via email and written weekly reports. Improvements of the health department’s performance is communicated to the Governing Body via program indicator dashboards. STANDARD 12.1 – Maintain current operational definitions and statements of public health roles, responsibilities, and authorities. Comments State statute outlines SCHD’s mandated authority to conduct public health activities in the jurisdiction. SCHD communicates weekly via newsletter to Commissioners department activities, including state-mandated functions. Statue defines the County Commissioners are the Board of Health. There is, however, no written description of the Board of Health’s roles and responsibilities related to the health department. 12.1.1 A: Mandated public health operations, programs, and services provided. Score: Fully Demonstrated Conformity: RD1: SCHD provided several documents for RD1. The first was a letter dated May 2, 2018 from the Kansas Department of Health and Environment (KDHE) regarding changes to Kansas administrative regulations on the reporting of and isolation/quarantine of infectious/contagious disease. The letter is for those “mandated reporters” such as labs and physicians. A copy of the regulation was included. Local health conducts surveillance. The second document is a Local Health Department New Director Orientation packet from the Kansas Association of Local Health Departments (KALHD). In this document are several links to administrative regulations, including contagious disease and confidentiality of information, and oath and bond of local health officers. Last, SCHD provided the Shawnee County Kansas Code. In this document are citations related to nuisances, slaughterhouses, and environmental code, of which the local health department is responsible for. RD2: SCHD provided a weekly report sent to the Board of County Commissioners from the SCHD Director. The report included updates on county code and state statute mandated functions (updates are noted as such), including child care licensing, environmental health, and communicable disease surveillance and investigation. Updates included number of child care visits, number of routine inspections, and updates on long-term care norovirus outbreaks. Areas of Excellence: Not Available

P a g e 96 | 99
Opportunities for Improvement: Not Available 12.1.2 A: Operational definitions and/or statements of the public health governing entity’s roles and responsibilities. Score: Slightly Demonstrated Conformity: RD1: SCHD provided a printout from the 2015 Kansas Statutes - #65-201. The statute states that “the county Commissioners of the several counties of this state shall act as county boards of health for their respective counties”. The statute continues to state that “each county board thus created shall appoint a person licensed to practice medicine and surgery, preference being given to persons who have training in public health, who shall serve in an advisory capacity to the county board of health and as the local health officer”. There is no explanation of the governing entity's authority. SCHD should add to the statute information on how the Board of County Commissioners are chosen, and a written description of their authority, roles, and responsibilities as related to public health. RD2: SCHD provided a copy of a 2-slide PowerPoint presentation of the Shawnee County Board of Health dated April 21, 2014.The Board of County Commissioners acts as the Board of Health. The first slide is a cover slide with a picture of the Board of County Commissioners. Highlighted under the second slide is reference to Kansas statute #65-201, stating “the county Commissioners of the several counties of this state shall act as county boards of health for their respective counties”. The statute continues to state that “each county board thus created shall appoint a person licensed to practice medicine and surgery, preference being given to persons who have training in public health, who shall serve in an advisory capacity to the county board of health and as the local health officer”. No other information on the Board composition is provided. Areas of Excellence: Not Available Opportunities for Improvement: Not Available STANDARD 12.2 – Provide information to the governing entity regarding public health and the official responsibilities of the health department and of the governing entity. Comments SCHD provides documentation to the Board concerning the health department’s responsibilities, as set forth in the health department’s authorizing documents(s). The Department has an extensive Board orientation packet, however a process is lacking. 12.2.1 A: Communication with the governing entity regarding the responsibilities of the public health department and of the responsibilities of the governing entity.

P a g e 97 | 99
Score: Slightly Demonstrated Conformity: RD1: SCHD provided 2 examples for Requirement A for this measure. Example 1 - The first is a weekly report to the Board of County Commissioners from the SCHD Director, dated May 17, 2019. In this document were updates on activities the SCHD is required to do per county code and state statute (childcare licensing, environmental health, and communicable disease investigation). Updates included number of child care visits, number of routine inspections, and varicella surveillance. Updates from other sections (Finance, Emergency Preparedness) were also included. Example 2 - The second example is a weekly report to the Board of County Commissioners from the SCHD Director, dated April 28, 2019. In this document were updates on activities the SCHD is required to do per county code and state statute (childcare licensing, environmental health, and communicable disease investigation). Updates included number of child care visits, number of routine inspections, and varicella surveillance. Updates from other sections (Finance, Emergency Preparedness) were also included. SCHD should document the process for orientating new Board members. SCHD reported out on their activities, not the roles of the governing body, as required. For Requirement B, SCHD provided an Orientation to Public Health document dated November 29, 2018. Chapter 1 reviews public health, Chapter 2 reviews the governing body responsibilities, and Chapter 3 reviews the role of the health officer. In Chapter 4 includes Kansas State Code outlining the roles and responsibilities of the local health department. Subsequent chapters cover the SCHD strategic plan, budget, grants, newsletter, and accreditation. Only the Board orientation packet was provided, there is no evidence of a written process for orientating new Board members. Areas of Excellence: SCHD provides regular written communication to the Board of County Commissioners, the governing entity.
Opportunities for Improvement: Not Available STANDARD 12.3 – Encourage the governing entity’s engagement in the public health department’s overall obligations and responsibilities. Comments The Department communicates with the governing entity regarding important public health issues and/or recent actions of the health department through direct email and written weekly reports. The Department does not, however, consistently review the Board of County Commissioners patters or issues discussed per the measure. Improvement of the health department’s performance is communicated to the Governing Body via program indicator dashboards. 12.3.1 A: Information provided to the governing entity about important public health issues facing the community, the health department, and/or the recent actions of the health department.
P a g e 98 | 99
Score: Fully Demonstrated Conformity: RD1: Example 1 – SCHD provided an email from the SCHD Director to the Board of County Commissioners regarding an outbreak of shigella at a childcare center. The Director updated the Commission on the number ill, education given by SCHD staff to childcare center staff, and actions to be taken on a day when SCHD is closed but the childcare center is open. This is evidence of the local health department communicating with the governing entity regarding important public health issues. Example 2 – SCHD provided a weekly report to Board of County Commissioners from the SCHD Director (dated January 19, 2018). Highlighted in the report is that an issued nuisance complaint letter resulted in a request for hearing. The request for hearing was attached, as well as emails between SCHD staff and the Assistant Shawnee County Counselor. Documentation showed evidence of the local health department communicating with the governing entity regarding important public health issues, in this case an environmental health hazard. Areas of Excellence: Not Available Opportunities for Improvement: Not Available 12.3.2 A: Actions taken by the governing entity tracked and reviewed. Score: Not Demonstrated Conformity: RD1: Example 1 – SCHD provided an email from a County Commissioner to the Director of Health regarding the need for a narrative to go along with a video being presented by the County Commissioner. This does not meet the measure requirement of the local health department consistently reviewing the governing entity's patters of issues discussed, opinions, or positions taken. Example 2 – SCHD provided minutes from a leadership workday held May 14, 2019. Highlighted in the minutes are that the Director had an evaluation with the Board of County Commissioners, one Commissioner is concerned about teen suicide and another about high STD levels in the jurisdiction. It is mentioned in the minutes that the Commissioners also asked about succession planning. Only one set of minutes was provided. This documentation does not meet the measure requirement of the local health department consistently reviewing the governing entity's patters of issues discussed, opinions, or positions taken. SCHD should consistently review issues discussed, actions taken, and policies set by the Board of County Commissioners on a regular basis and document as such.
Areas of Excellence: Not Available Opportunities for Improvement: Not Available

P a g e 99 | 99
12.3.3 A: Communication with the governing entity about health department performance assessment and improvement. Score: Largely Demonstrated Conformity: RD1: Example 1 - SCHD provided a memo to the Board of County Commissioners regarding gaining approval to submit an application to PHAB, and to sign a letter of support. SCHD highlights benefits of PHAB accreditation to local health departments in the letter. Minutes show the Board approved the application submission. The letter of support is attached, as well a PowerPoint on PHAB and the benefits of accreditation. Example 2 - SCHD provided a 2019 update to their strategic plan. An email shows evidence it was sent to the governing body in February 2019. The plan contains a SWOT analysis, priority goals, and an action plan with goals and objectives. The documentation does not meet the intent of the measure of providing a quality improvement plan. RD2: Example 1 - SCHD provided a dashboard showing progress status on a variety of projects. Projects include accreditation documentations submission, branding plan, and workforce development plan, among others. An email to the governing body demonstrates the dashboard was distributed. Example 2 - SCHD provided a program indicator report for quarter 1 of 2019. This was distributed to the governing body via email. Each SCHD program is listed with target goals and variance from goals from date of indicator report submission. There is no documentation if the variance from goals, or met goals, are a result of performance improvement process or activities conducted by the department. Rather, individual indicators are listed under each program, such as “Number of community presentations given” under Health Outreach and Planning or “% of errors found through monthly clerical data entry audit” under Finance. Areas of Excellence: Not Available Opportunities for Improvement: Not Available