first trimester induction protocols and complications
DESCRIPTION
FIRST TRIMESTER INDUCTION PROTOCOLS AND COMPLICATIONS. Dr.A.R.Vijayalakshmy DGO,MD,MRCOG Senior Consultant( O& G) Khoula Hospital. INTRODUCTION. - PowerPoint PPT PresentationTRANSCRIPT

FIRST TRIMESTER INDUCTION PROTOCOLS AND COMPLICATIONS
Dr.A.R.Vijayalakshmy DGO,MD,MRCOG
Senior Consultant( O& G)
Khoula Hospital
•First Trimester Induction applies to those terminations on Medical grounds and Miscarriage
•Miscarriage occurs in 10-20 %
•Surgical Evacuation – Conventional method
•Effective Non Surgical Alternatives
•Early Pregnancy Assessment Units (EPAU)
INTRODUCTION
EAPU(Bigrigg and Read 1991)•Streamlines the management of early pregnancy problems with improved efficiency and quality
•Hospital admissions reduced by 40% and 20% shorter stay
•Cited in a dedicated area with
Appropriate Staffing and Facilities
Efficient Appointment system
Direct access for GPs and selected patient groups
TVS,BHCG,Serum Progesterone •Available on all days ,minimum 5 days in the morning ,Clinical Guidelines for management

Spont.AbortionSpont.Abortion MiscarriageMiscarriage
Threatened Threatened abortionabortion
Threatened miscarriageThreatened miscarriage
Inevitable abortionInevitable abortion Inevitable miscarriageInevitable miscarriage
Incomplete abortionIncomplete abortion Incomplete miscarriageIncomplete miscarriage
Complete abortionComplete abortion Complete miscarriageComplete miscarriage
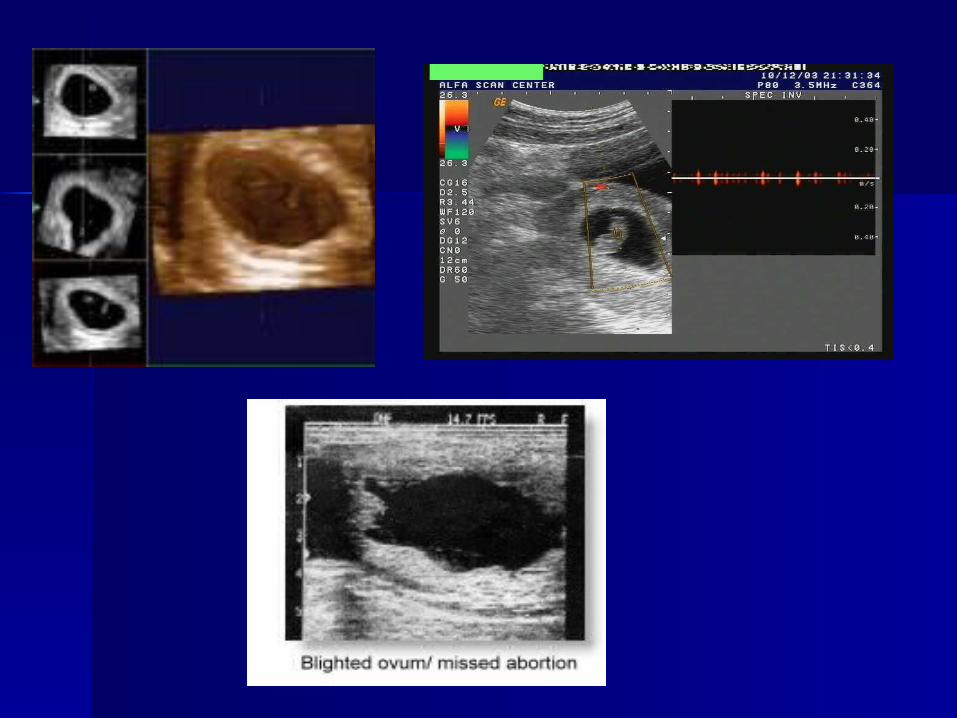
Missed abortionMissed abortion Missed miscarriageMissed miscarriage
Anembryonic Anembryonic pregnancypregnancy
Early fetal demise /Silent Early fetal demise /Silent miscarriagemiscarriage
Blighted ovumBlighted ovum Delayed miscarriageDelayed miscarriage
Septic abortionSeptic abortion Miscarriage with infectionMiscarriage with infection
Recurrent abortionRecurrent abortion Recurrent miscarriageRecurrent miscarriage
TERMINOLOGIES 33rd RCOG Study Group 1997

TermTerm DefinitionDefinitionBiochemical Biochemical preg.losspreg.loss
Pregnancy not located on scanPregnancy not located on scan
Empty sacEmpty sac Sac with absent or minimal Sac with absent or minimal structuresstructures
Fetal lossFetal loss Previous CRL measurement Previous CRL measurement with subsequent FH losswith subsequent FH loss
Early pregnancy Early pregnancy lossloss
Confirmed empty sac or sac with Confirmed empty sac or sac with absent FHA <12 wks absent FHA <12 wks
Delayed Delayed miscarriagemiscarriage
As early preg.lossAs early preg.loss
Late preg.lossLate preg.loss Loss of FHA >12 wksLoss of FHA >12 wks
Pregnancy of Pregnancy of unknown locationunknown location
No identified preg.on US ,+ve No identified preg.on US ,+ve HcgHcg
European Society for Human reproduction Special Interest Group
for Early Pregnancy - Revised Nomenclature(2005)

•History/Preexisisting conditions(Cardio resp,Coag.disorders)
•Examination ,Ultrasound
•Investigations
•Informed Consent
•Management Options
Expectant
Medical Algorithm
Surgical
MANAGEMENT

INDUCED MISCARRIAGE - FIRST TRIMESTER
Mifepristone Misoprostol /Methotrexate Misoprostol or Misoprostol alone
IPPF and WHO 2007
Mifepristone 200mg followed 36–48 hours later by 800μg misoprostol (orally, sublingually, buccally or vaginally)at once or in two doses of 400μg two hours apart, up to 9 completed weeks after last menstrual period.

US FDA
Day 1: Mifepristone 600mg (three 200mg tablets) taken as a single oral dose.
Day 3: Unless abortion has occurred and is confirmed by clinical examination or ultrasound administer misoprostol400μg (two 200μg tablets) as a single oral dose

Methotrexate/Misoprostol Protocol ( OBG Society of Canada 2008)Methotrexate 50mg/SqM Intramuscular on the deltoidOn5th,6th or 7th day afterMethotrexate, 800ugm VaginallyIf no bleeding or passage of tissue after 24 hrs, rpt 800 ugm On the D3 and D7 days •If Bhcg has fallen by >80% over 7days,procedure was successful •If not, a weekly Bhcg estimation till level reaches 0 or interval decrease is >80% • If Bhcg level plateaus or increases - Incomplete miscarriage or ongoing gestation - Suction Evacuation
Once termination is complete ,confirm a nonpregnant non tender uterus by bimanual pelvic examination

INDUCED MISCARRIAGE PROTOCOL (CONTD )MISOPROSTOL ALONE
Misoprostol 800ugm Vaginally –every 24 or 48 hrs ( Day1-5) until abortion occurs or a total of 3 doses Bhcg on Day 1 and D7 .If Fallen >80% -success. Repeat another after 1 wk to ensure continued decline .If not fallen to the desired level, rpt wkly till reaches 0 or interval decrease is > 80%If rises or plateaus -- Vacuum aspiration Ultrasound may be used instead of B hcg assays
WHO Expert Group 2007Misoprostol 800 ugm Vaginally12 hrlyx 3doses ( Ideally after 48 hrs of Mifepristone 200 mg)


•Effective and acceptable for selected group of women (Level 1b).
•Should be offered to women who have access to emergency admission if required.
•Successful in 2-6 wks without increasing complications in 80-90% of women with Incomplete miscarriage and 65-75% of women with Delayed miscarriage/Empty sac (Butler C. et al J.Fam.Practice 2005).
EXPECTANT MANAGEMENT IN MISCARRIAGES

EXPECTANT MANAGEMENT IN MISCARRIAGES (CONTD.)•Those with intact sac may take several wks and efficacy low.
•Success depends on various factors like
Type of miscarriage
Duration of follow up
Ultrasound or Clinical
•Low serum Progesterone may be used to predict outcome

SURGICAL MANAGEMENT( Suction Evacuation)
Treatment of choice for Intact sac ,Incomplete miscarriage with ET >50 mm ,Heavy bleeding, Unstable Vital signs or Infection,Suspected molar pregnancy ,Patient’s choice
Advantage of Suction Evacuation
•Safe and Quick
•Significantly reduced blood loss( Cochrane review 2001)
Need for Cervical priming assessed ( Misoprostol 400 ugm) oral or vaginaly)4 -12 hrs prior
Reduces cervical laceration and uterine perforation up to 80%
Antibiotic Prophylaxis individualised ( 1gm Metronidazole) rectally at surgery followed by oral Doxycyclin 100mg BDx 7days)

SURGICAL MANAGEMENT ( CONTD)
•Canula size in mm should be equal to or > than the Gest.age in weeks ( B)
•Use of Oxytocin associated with clinically significant decrease in mean blood loss ( 17.6 mlVS 24.5 ml ) Level 1a
•Suspected Infection – Intravenous Antibiotics for 12 hrs prior to Evacuation
•Serious Morbidity and Mortality – 2.1% and 0.5/100,000 in Induced abortion( Level 3 Evidence)
Others
Incomplete Miscarriage 2/1000, Haemorrhage,Cervical trauma,uterine trauma 1/1000

COMPLICATIONS
Cervical shock ( Vasovagal ) – Para cervical block Tonic Clonic reaction – confused with seizure
Bradycardia, rapid recovery ,absence of post ictal state – differentiates
Pre op Cervical priming – prevents the Cervical shock
Perforation –Presentation depends on the site
At Isthmic portion – May lacerate the ascending branch of uterine artery--- haematoma in the broad ligament/ intraabdominal bleed
Immediate Laparotomy and ligation of severed vessels / repair of uterine injury/Hysterectomy( rarely)

Low Cervical perforation - May injure descending branch of Uterine artery in the Cardinal ligament- due to forcible dilatation
•Deaths due to delayed bleeding can occur hrs or days later
•Management - Embolisation /Hysterectomy
•Fundal Perforation - Stop the Suction ,Laparoscopy/ Laparotomy and complete the evacuation under vision ,repair the damage
•Haemorrhage – Uterine atony,Lowlying limplantation, Perforation
•Misoprostol 1000ugm rectally /Oxytocin /IM PG f2 Alfa
•Persistent bleeding – Retained tissue,Perforation
COMPLICATIONS (CONTD )

MEDICAL MANAGEMENT - As Out patient ( Level 1b)
•Induced miscarriage
•Incomplete ,Silent/Delayed / Missed miscarriage
•Early fetal demise
Variety of regimens described including Gemeprost, Mifepristone followed by Misprostol ,Methotrexate - Misoprostol and Misoprostol alone

Misoprostol > 600 studies 90,000women
PGE1 analogue ,cheap, highly effective,acts via various routes , easy storage ,fast absorption ,peaks after 12 minutes of oral and 60minutes after vaginal Half life 20-30 minutes ( Bioavailability varies with route)
Myometrial contractions by interacting with specific receptors on myometrial cells -- Cascade of events change in calcium concentration and muscle contraction

MEDICAL MANAGEMENT CONTD
•Alternative method- does not replace surgical evacuation
•Availability Improved choice
•20% willing to choose medical method as could avoid anesthesia and feels more in control ( Level 1 b)
•Local protocols should be developed with selection criteria ,theraputic regimen and follow up ( Good practice)
•Should be counselled that bleeding may continue for 3wks

Rule out Contraindications
Absolute Adrenal insufficiency ,Long term steroid trt , Hb<10 gm%, Hemoglobinopathies,Glaucoma,Mitral stenosis ,Coagulation disorders,Hepatorenal diseases,Acute Inflammatory bowel disease , Porphyria ,NSAIDS ingestion in the preceding 48 hrs(?) Pelvic infection/sepsis, known allergy
Relative – Hypertension, Severe Asthma

To date no standard protocol for the use of Misoprostol as single agent•Variety of doses and differing dosing schedules
Success depends on various factors like
•Type of miscarriage,Sac size ,Total dose ,Route,Duration,Clinical or US follow up
•High success rates with Incomplete ,High dose Vaginal and Clinical follow up
INCOMPLETE MISCARRIAGE (Upto 12 wks•Single oral dose of 600 ugm - Successful in > 1000 women in > 6 trials world wide ( Int.J OBG 2007)
•Vaginal 800ugm –Single dose ,Oral 400ugm Single dose
•Single and Rpted doses of oral 600ugm ,maximum 1200 ugm –found to be equally effective ,lower incidence of diarrhoea in single dose group ( Ngutyen TN etal –Contraception 2005)
•Success 61-95%,bleeding for 6 days

Sublingual 400 ugm has also been evaluated - Success of 94.5%
Both Sublingual 400 ugm and Oral 600 ugm –Equally effective for Incomplete miscarriage ( FIGO 2006 )
In many low resource countries ,with women having limited access to Secondary and Tertiary Care ,could use for Incomplete miscarriage ( 17th Expert Committee on Selection & Use of Essential Medicines, Geneva March 2009)
Cohrane Review including 19RCT on Pregnancies <14 wks reported that Vaginal Misoprostol reduces the time to expulsion when compared with Placebo Doses used 400 ,600 or 800 ugm.
Lower doses 2RCT-less effective

AuthoAuthor r
Dose& Dose& Route Route
No No SucceSuccessss
DefinDefineded
Pang 2001 Pang 2001 800Vag 2doses 800Vag 2doses 4 hrly 4 hrly
96 pt 96 pt – – 61% 61% < 24 hrs < 24 hrs
Blanchard Blanchard 20042004
600 oral 600 oral 2doses 4hrly 2doses 4hrly
87Pts87Pts 70% 70% 2 wks2 wks
Ngoc 2004 Ngoc 2004 600 oral2doses 600 oral2doses 4hrly 4hrly
150 pts 150 pts 94% 94% 9days9days
Blohm 2005 Blohm 2005 400 Vag 1dose 400 Vag 1dose 64 pts 64 pts 88% 88% 2 wks2 wks
Zhang 2005 Zhang 2005 800 Vag 48hrly800 Vag 48hrly2doses max 2doses max
30pts30pts 93% 93% 1wk1wk
Shwekerela Shwekerela 20072007
600 oral 1dose 600 oral 1dose 150pts 150pts 99% 99% 2wks2wks
Dao 2007 Dao 2007 600 oral 1dose600 oral 1dose 223 pts 223 pts 94.5% 94.5% 1wk1wk

CONTD
• Hospitalisation not necessary
• Time to expulsion varies ,bleeding heavy for 3-4 days may last >14 days with additional days of spotting
• Women with Previous CS
• No reason to withhold ,while many trials have excluded
• For Uterine size < 12 wks misoprostol reported safe with scar

• Does not increase the infection rate•Avoids surgery and anaesthesia • Emotionally easier for some women•Client controlled; more privacy and autonomy; • Better than surgical in very early gestation, or with• severe obesity (body mass index >30) without other cardiovascular risk factors, or in the case of fibroids, uterine malformations or previous cervical surgery• No risk of cervical/uterine injury
ADVANTAGES OF MEDICAL METHODS

SILENT ,DELAYED ,MISSED OR EARLY FETAL DEMISEA Confusing number of regimes using Misoprostol alone (Oral,Sublingual or Vaginal) in doses of 400,600 or 800 ugm in single or repeated doses
Oral Mifepristone 200,400 or 600 mg followed by 36-48 hrs later by Misoprostol or Gemiprost 0.5- 1mg Vaginally
Success with Mifepristone+ Misoprostol -70-84% with Induction to miscarriage time of 8hrs and Satisfaction rate of 91% ,Bleeding stopped in 8 days
Mifepristone not necessary in above miscarriages as Progesterone levels are low
Vaginal route preferred -Early expulsion than Oral
Sublingual route –Fatigue and diarrhoea higher ( Tang OS et al , Human Reproduction 2003,NgOC et al Int.J O&G 2004
Single dose Vaginal 800ugm –more effective than 400 ugm (55% VS 40.2 %) in delayed miscarriage compared with empty sac (50 % Vs 40%)
Larger and Rpt doses needed in those with Empty sac
There is no randomised evidence to guide practice in cases of 1st Trimester miscarriage particularly in cases of intact sac
Suction evacuation - high satisfaction and acceptability

•Chung et al 1995 - 400 ugm oral 4hrly 3doses ,141pt - 62%
•Nielson et al 1997 -400 mg Mifepristone -36 hrs Oral Miso 400 ugm – 31 pts , 52%
•Zalayani et al 1998 – 200 ugm Vaginally 4hrly X 4doses – 25pts -88%
•WoodSL et al 2002 - 800 ugm Vaginal ,Rpt at 24 hrs – 50 pts- 84%
•TangOS et al 2003 – 600 ugm Vag or SL 3hrlyx 3doses – 80 pts – Successs -87.5% in both , diarrhoea ,fatigue more in SL,otherwise comparable side effects ( RCT)
SOME OF THE REGIMENS IN EARLY PREG.FAILURE

•Davis AR et al 2002 – 800 ugm Vag -24 hrlyx 2 doses – 80 pts – 85%
•Ngoc et al 2004 – 800 ugm Oral or Vaginal – 200 pts 89 % and 92.9% success
•Reynold et al 2005 – 600 ugm Vaginally 4hrly x 3 doses – 44 pts – 86 %
•Zhang 2005 - 800 ugm Vaginal – Rpt at 48 hrs if POC - 652 pts ,77% after 1 dose and 84 % after 2 doses
•WHO Expert Group 2007 – 800 ugm Vaginally 3hrly or Sublingual 600ugm 3hrly – Give 2 doses and leave for 1-2 wks
CONTD.

SIDE EFFECTS AND COMPLICATIONS
Rarely mild rash
Infection rate - Not different from other methods ( 2%) Vs 3%
No adverse effect on future fertility ( Level 1a)
Nausea,VoNausea,Vomiting miting
5-33% ( resolves in 2-6 hrs)5-33% ( resolves in 2-6 hrs)
Diarrhoea Diarrhoea 3.8 % 3.8 %
Fever Fever 0.4 – 2 %0.4 – 2 %
ChillsChills 5- 8 % 5- 8 % ( Subsides in 24 hrs)( Subsides in 24 hrs)
Cramping Cramping 56 – 95%(Starts in minutes- few56 – 95%(Starts in minutes- few hrs )hrs )

Rupture up to 4% in Previous CS and High Parity after 12 wks ( 12-24 wks )

COMPARISON BETWEEN DIFFERENT MANAGEMENTS
•Only few RCT comparing Expectant ,Medical and Surgical for Incomplete Miscarriage and Early fetal demise
•MIST trial ( BMJ 2006 ) Trinder J et al. Signicantly more unplanned admissions and surgical curettage after Expectant and Medical management than Surgical
•Infection rate was low ( 2-3 % ) regardless of method

A meta analysis reported in Obst.Gyn 2005 ,Surgical had the best success rate followed by Medical and Expectant although many were of poor methodological quality
Cochrane review 2006 ,Expectant –> High risk of incomplete miscarriage,bleeding ,need for surgical evacuation .

However no strong argument for either approach
•Individual woman’s preferrence - major concern
•Filmy adhesions reported in7.7% of Surgical cases
•Longterm conception rates and pregnancy outcome similar in both Medical and Surgical methods
•Median time to achieve pregnancy – 8 months
•Cost – Misoprostol least costly,followed by Expectant and Surgical Evacuation ( Pooled data)
•Other studies – Report otherwise
WOMAN’S PERSPECTIVE ABOUT DIFFERENT CHOICESA Survey done by (Molnar AM et al 2000 ) in women attending Family planning Clinics
Strong preferrence for Expectant management ,although Physician’s recommendation would infuence the decision.
No Single Best Way to treat Miscarriage to suit all women.
Largest Qualitative study of women’s views on Various management options ,concluded that Informed Choice was paramount
SATISFACTION RATES
Highly acceptable for Incomplete miscarriage – 96.8% ,would choose the same again – 94.5% ,would recommend to a friend -94%

HISTOPATHOLOGYOf Products of conception - should be sent to rule out Trophoblastic disease and Ectopic pregnancy
DISPOSAL OF THE POC Each Hospital should have clear system and protocol for sensitive disposal of the fetal remains
Record keeping poor
Should have National Guidelines for the same

ALGORITHM FOR MANAGEMENT OF MISCARRIAGE (Obstetrician and Gynaecologist 2007)
THREATENED MISCARRIAGE
Active bleeding Admit for reassurance
Follow up if
Haematoma
Decrease in Liqour
Fetal bradycardia
Rescan 2 wks
COMPLETE MISCARRIAGE – ET < 15 mm
Report if bleeding doesn’t stop in 2 wks

INCOMPLETE MISCARRIAGE - ET 15-50 OR >50 MM
Type 1 - Expectant - If bleeding is not heavy ,continue as long as per the woman’s wish ,with scan at 1-2 wkly intervals till complete miscarriage occurs.If heavy bleeding Surgical management
Medical - If woman not willing to wait – Vag.Prostaglandins Gemeprost 0.5mg, Gemeprost 1mg, Misoprostol 800 ugm
If heavy Bleeding /Infection /Changes the mind Surgical
Surgical Strong preference
Heavy bleeding Assess need for priming
Infection ( under antibiotic cover)

ET > 50 mm
Surgical Strong preference
Heavy bleeding Assess the need for
Infection priming
SILENT /MISSED/DELAYED /EARLY FETAL DEMISE Rescan1wk , If no change
Expectant As in incomplete
Medical Woman not willing to wait
Oral Mefipristone 200 mg followed by
36-48 hrs later Vag.PG ,Gemeprost 0.5mg /1mg
Misoprostol 800 Ugm ( 4 x 200 Ugm)
single dose for < 9wks , > 9wks 3hrly x 5doses

(CONTD)SURGICAL -As with ET >50mm
AntiD Prophylaxis if Rh –ve(50ugm)
Threatened miscarriage >12 wks
<12 wks if heavy bleeding
Confirmed miscarriage >12 wks
<12 wks if Evacuation
(Medical & Surgical)
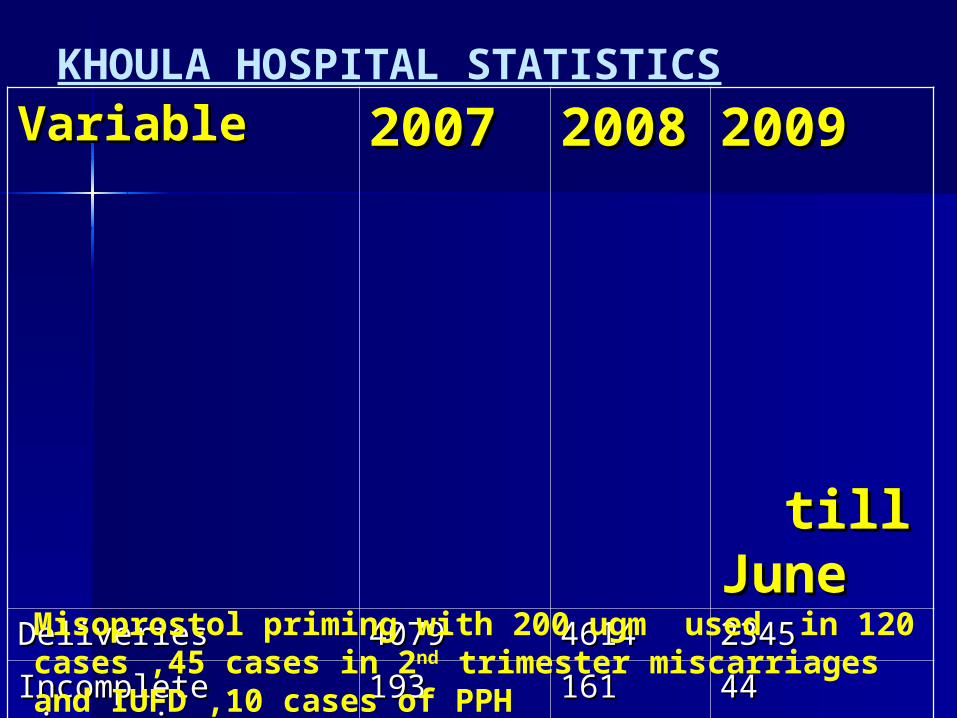
KHOULA HOSPITAL STATISTICS
VariableVariable 20072007 20020088
2009 2009 till till JuneJune
DeliveriesDeliveries 40794079 46144614 23452345
Incomplete Incomplete miscarriagemiscarriage
193193 161161 4444
Missed miscarriageMissed miscarriage 7979 123123 1616
Inevitable Inevitable miscarriagemiscarriage
5757 3131 1111
Complete Complete miscarriagemiscarriage
2525 2828 1212
E&CE&C 249249 232232 129129
Suction EvacuationSuction Evacuation 7979 9494 6262
Misoprostol priming with 200 ugm used in 120 cases ,45 cases in 2nd trimester miscarriages and IUFD ,10 cases of PPH

CONCLUSION AND RECOMMENDATION•Early Pregnancy Assessment Units
•Patient’s choice
•Counselling
•Misoprostol priming before evacuation
•Out patient management for Expectant and Medical
•Rule out Contraindications
•Prevention of Misuse – Mandatory

(CONTD)•Incomplete Miscarriage – Misoprostol 600 ugm single oral dose •Delayed Miscarriage – 800ugm Vaginally 24 hrly x 2doses
Induced miscarriage - 800 ugm Vaginally every 24-48 hrs maximum of 3 doses
•Follow up at 2 wks
•Antibiotic prophylaxis - Evacuation
•Markers to predict spontaneous resolution – IGF BP -1, Inhibin A and Inhibin Pro a-CRI
REFERRENCES1) Cochrane Database Systematic Review 2004
2)Consensus Statement – Instruction for Use- Misoprostol for Incomplete abortion and Miscarriage –Expert Meeting on Misoprostol – Reproductive Health Technology Project 2004
3)International Parenthood Federation ( First Trimester Abortion Guidelines and Protocols ) 2004
4)Greentop Guidelines No 25 -2006
5)Supplement to International Journal of Obstetrics and Gynecology 2007,Vol 99
6) Obstetrician and Gynaecologist 2007 ;9: 102-108
7)Council of the Society of Obstetrics and Gynecology of Canada ,Induced Abortion Guidelines Dec19,2008
